Desarrollos Terapéutico en Cáncer - Laboratorio de ...cronos.unq.edu.ar/farmaco/Farmaco Desarrollo...
51
Desarrollos Terapéutico en Cáncer Laboratorio de Oncología Molecular Universidad Nacional de Quilmes http//: cancer.unq.edu.ar
Transcript of Desarrollos Terapéutico en Cáncer - Laboratorio de ...cronos.unq.edu.ar/farmaco/Farmaco Desarrollo...

Desarrollos Terapéutico en Cáncer
Laboratorio de Oncología MolecularUniversidad Nacional de Quilmes
http//: cancer.unq.edu.ar
Transformación neoplásica:
Implica alteraciones en proto-oncogenes y genes supresores de tumor. De tal manera, se pierde el control del ciclo celular y la población adquiere rasgos de crecimiento autónomo.
NEOPLASIA: “Nuevo Crecimiento”Nuevo = Independiente o autónomo
Bases moleculares del cáncerOncogenes y Genes Supresores
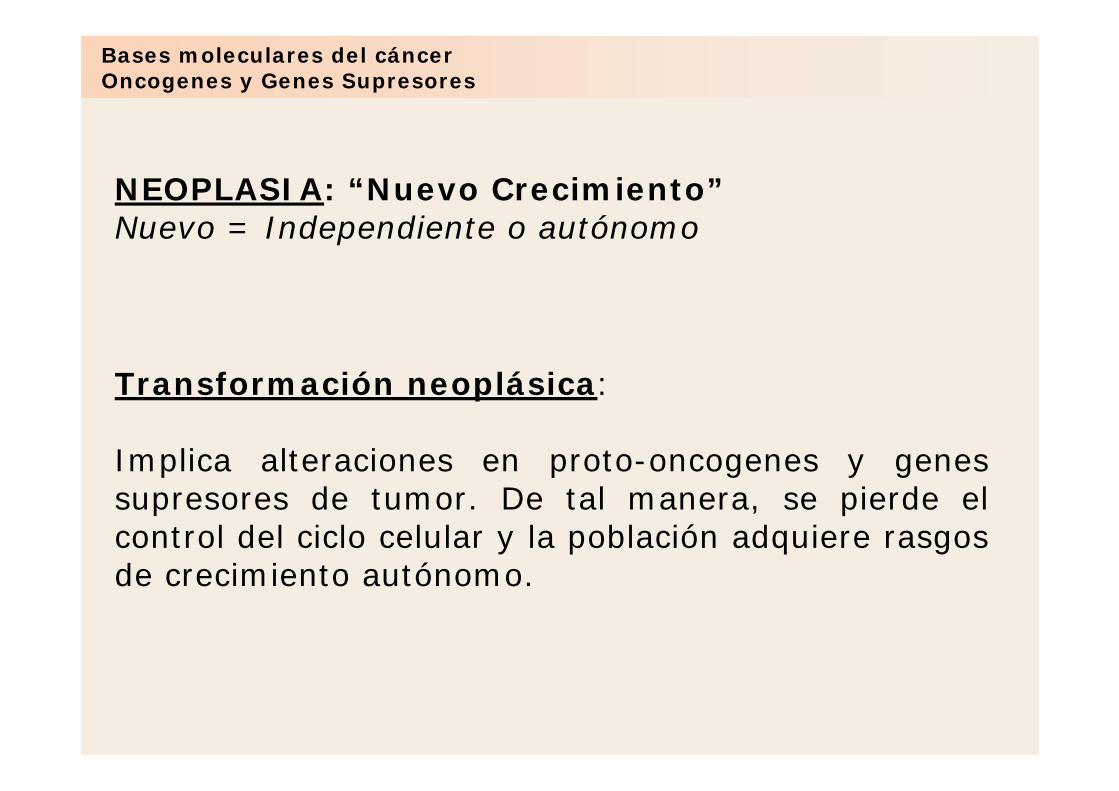
Transformación celular
Proliferación
Degradación de membrana basal
Invasión
Crecimiento tumoralLoco-regional
Intravasación
Diseminaciónsistémica
-- Crecimiento tumoral Crecimiento tumoral --Progresión Tumoral
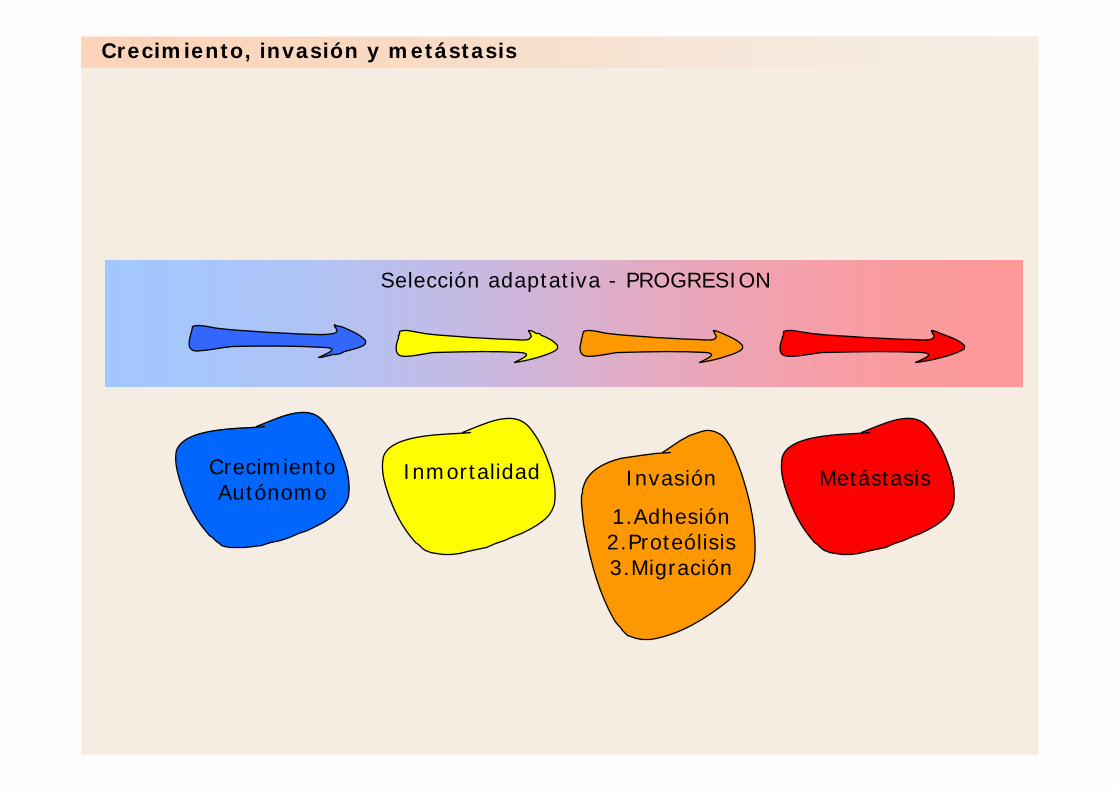
Crecimiento, invasión y metástasis
Crecimiento Autónomo
Inmortalidad Invasión
1.Adhesión 2.Proteólisis 3.Migración
Metástasis
Selección adaptativa - PROGRESION
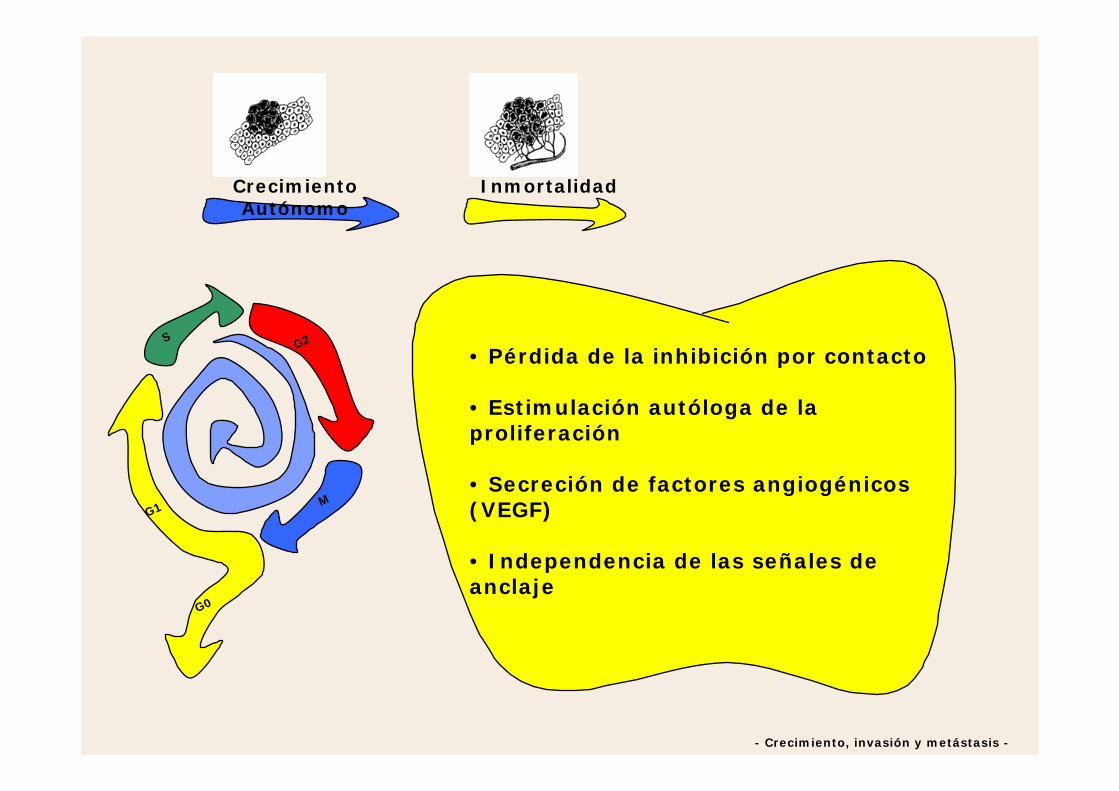
Crecimiento Autónomo
Inmortalidad
MG1
G0
S G2
• Pérdida de la inhibición por contacto
• Estimulación autóloga de la proliferación
• Secreción de factores angiogénicos (VEGF)
• Independencia de las señales de anclaje
- Crecimiento, invasión y metástasis -
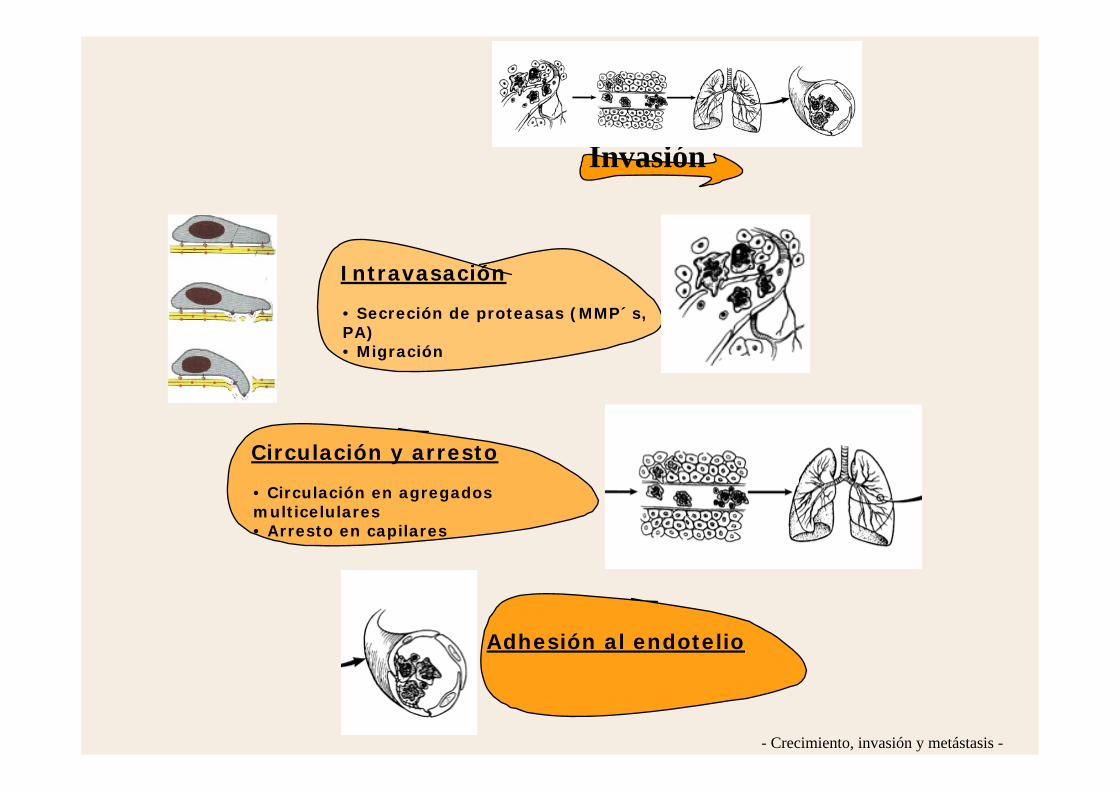
Invasión
Circulación y arresto
• Circulación en agregados multicelulares• Arresto en capilares
Adhesión al endotelio
- Crecimiento, invasión y metástasis -
Intravasación
• Secreción de proteasas (MMP´s, PA)• Migración
- Crecimiento, invasión y metástasis -
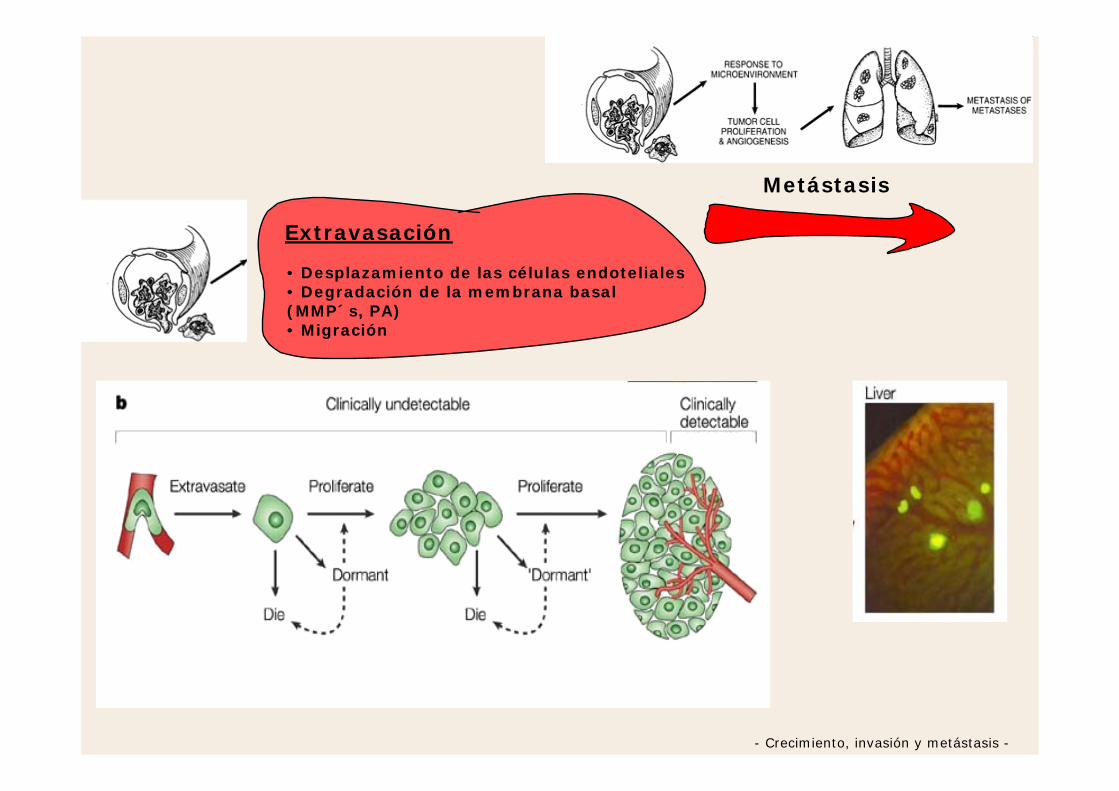
Metástasis
Extravasación
• Desplazamiento de las células endoteliales• Degradación de la membrana basal (MMP´s, PA)• Migración
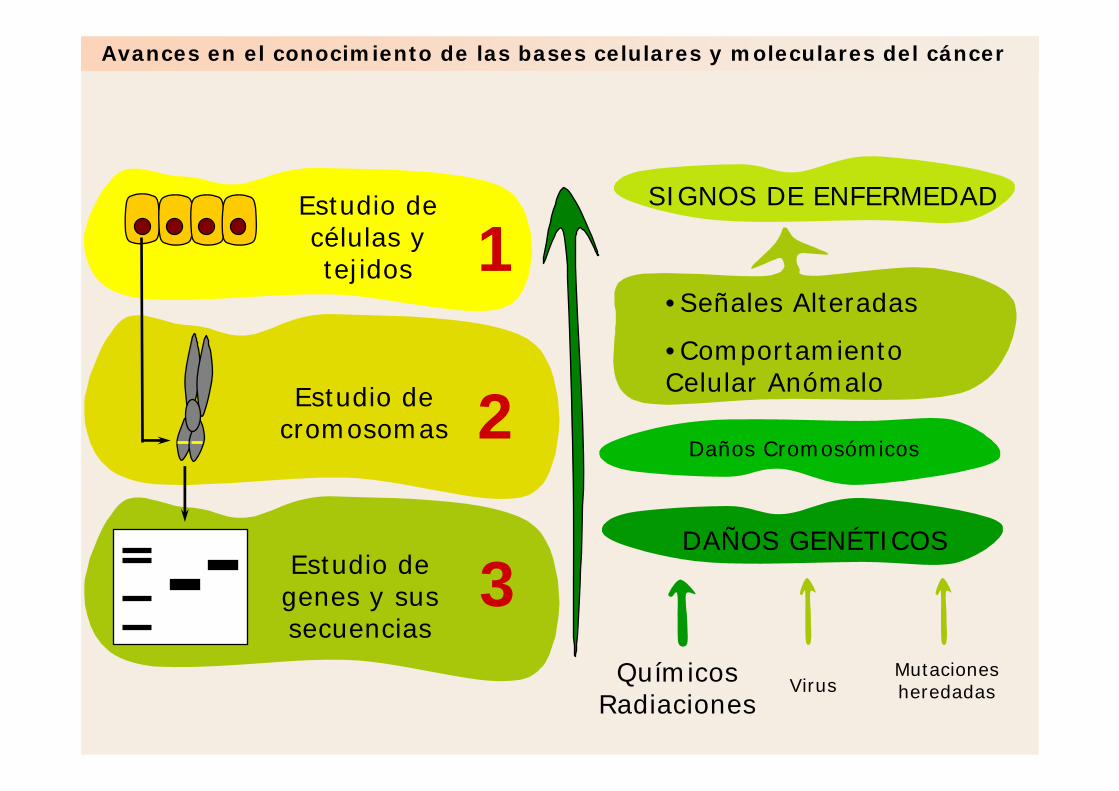
Estudio de células y tejidos 1
Daños Cromosómicos
•Señales Alteradas
•Comportamiento Celular Anómalo
SIGNOS DE ENFERMEDAD
Estudio de cromosomas 2
Químicos Radiaciones
Mutaciones heredadasVirus
DAÑOS GENÉTICOSEstudio de genes y sus secuencias
3
Avances en el conocimiento de las bases celulares y moleculares del cáncer
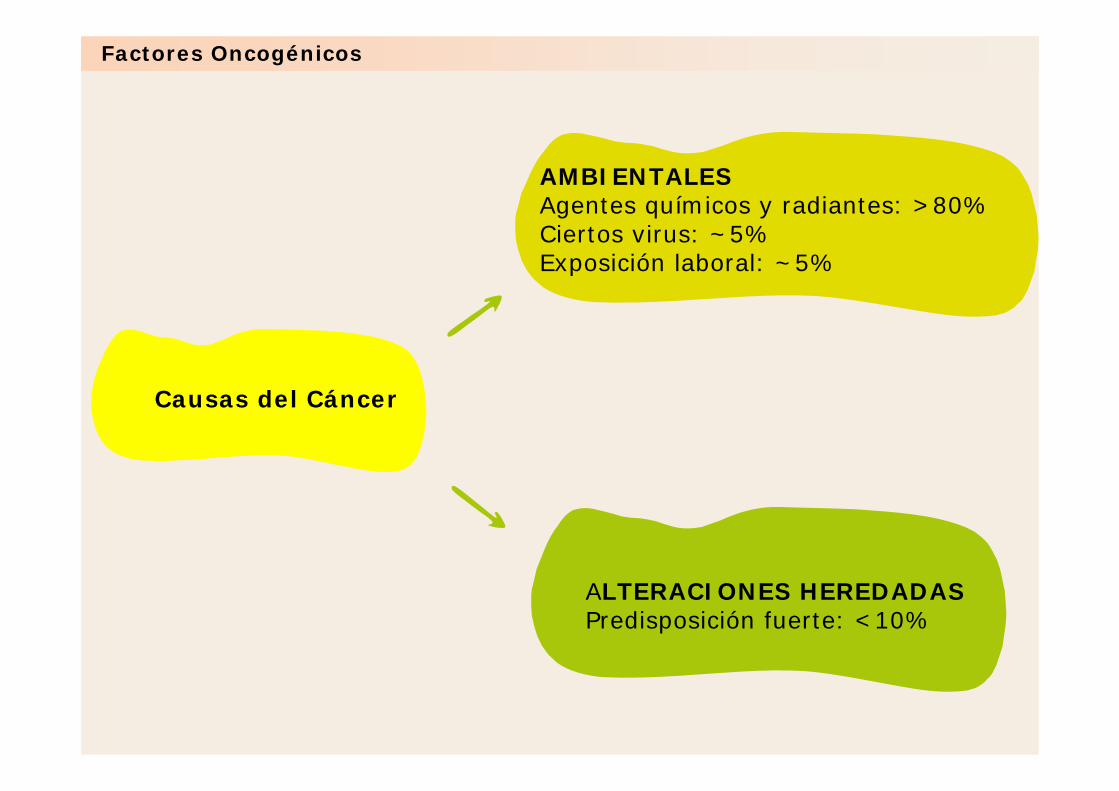
Factores Oncogénicos
AMBIENTALESAgentes químicos y radiantes: >80%Ciertos virus: ~5%Exposición laboral: ~5%
ALTERACIONES HEREDADASPredisposición fuerte: <10%
Causas del Cáncer
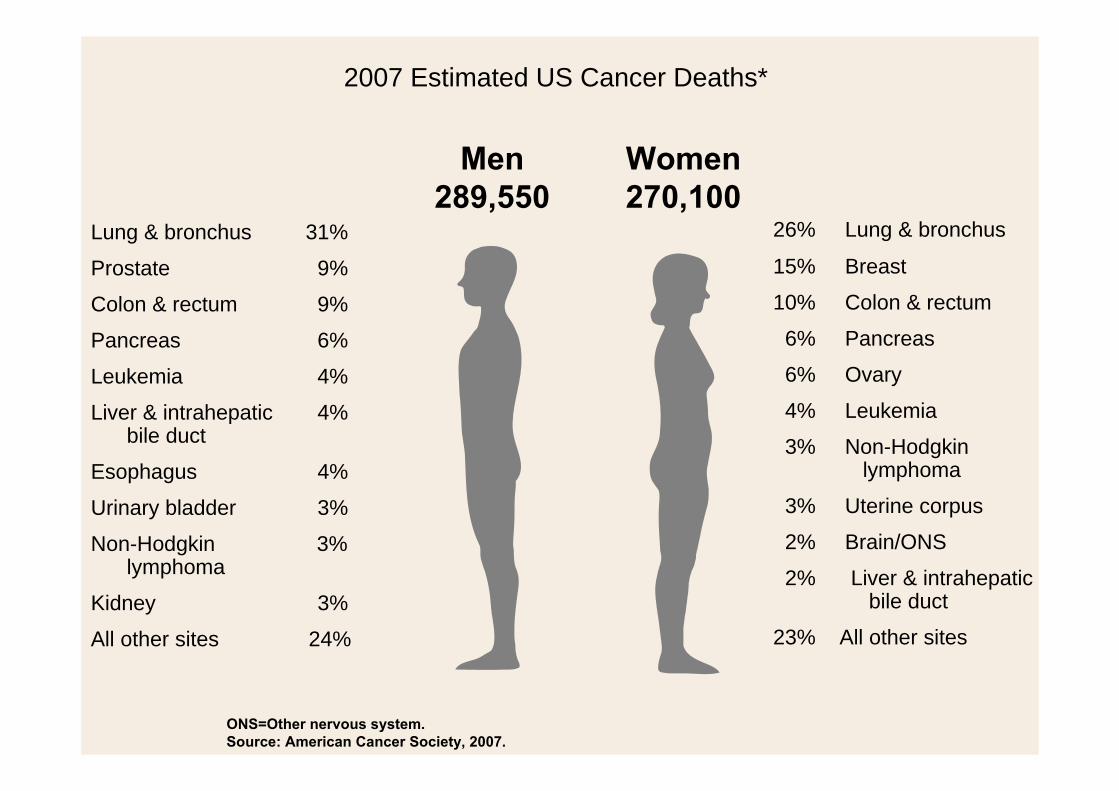
2007 Estimated US Cancer Deaths*
ONS=Other nervous system.Source: American Cancer Society, 2007.
Men289,550
Women270,100
26% Lung & bronchus
15% Breast
10% Colon & rectum
6% Pancreas
6% Ovary
4% Leukemia
3% Non-Hodgkinlymphoma
3% Uterine corpus
2% Brain/ONS
2% Liver & intrahepaticbile duct
23% All other sites
Lung & bronchus 31%
Prostate 9%
Colon & rectum 9%
Pancreas 6%
Leukemia 4%
Liver & intrahepatic 4%bile duct
Esophagus 4%
Urinary bladder 3%
Non-Hodgkin 3% lymphoma
Kidney 3%
All other sites 24%
Bases Moleculares del Cáncer
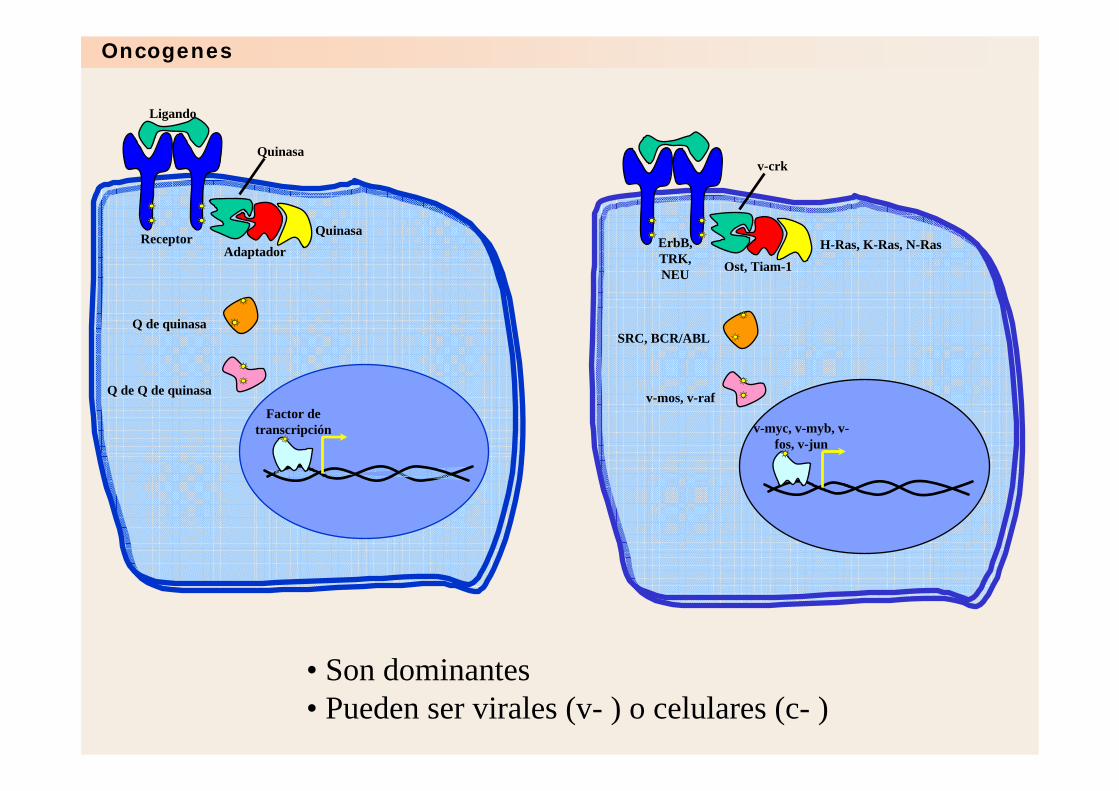
Ligando
Receptor Quinasa
Q de quinasa
Q de Q de quinasa
Factor de transcripción
Adaptador
Quinasa
ErbB, TRK, NEU
H-Ras, K-Ras, N-Ras
SRC, BCR/ABL
v-mos, v-raf
v-myc, v-myb, v-fos, v-jun
Ost, Tiam-1
v-crk
Oncogenes
• Son dominantes• Pueden ser virales (v- ) o celulares (c- )
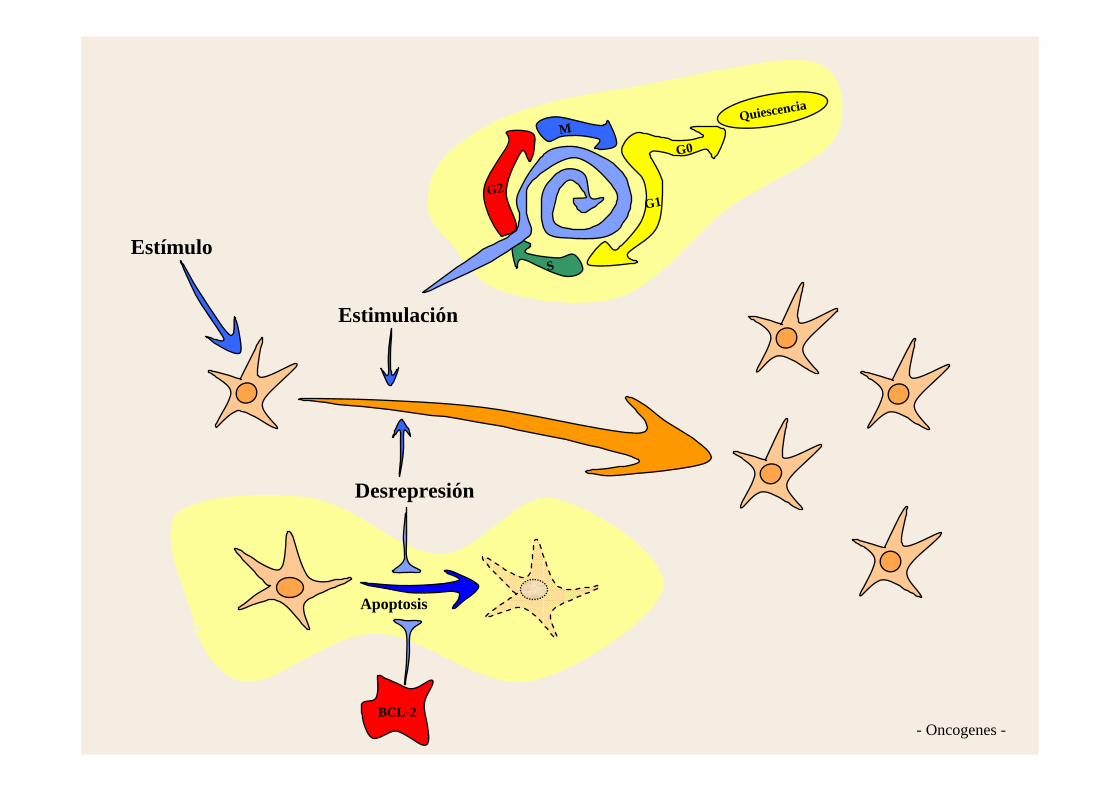
Apoptosis
BCL-2
M
G1
G0
S
Quiescencia
G2
Estímulo
Estimulación
Desrepresión
- Oncogenes -
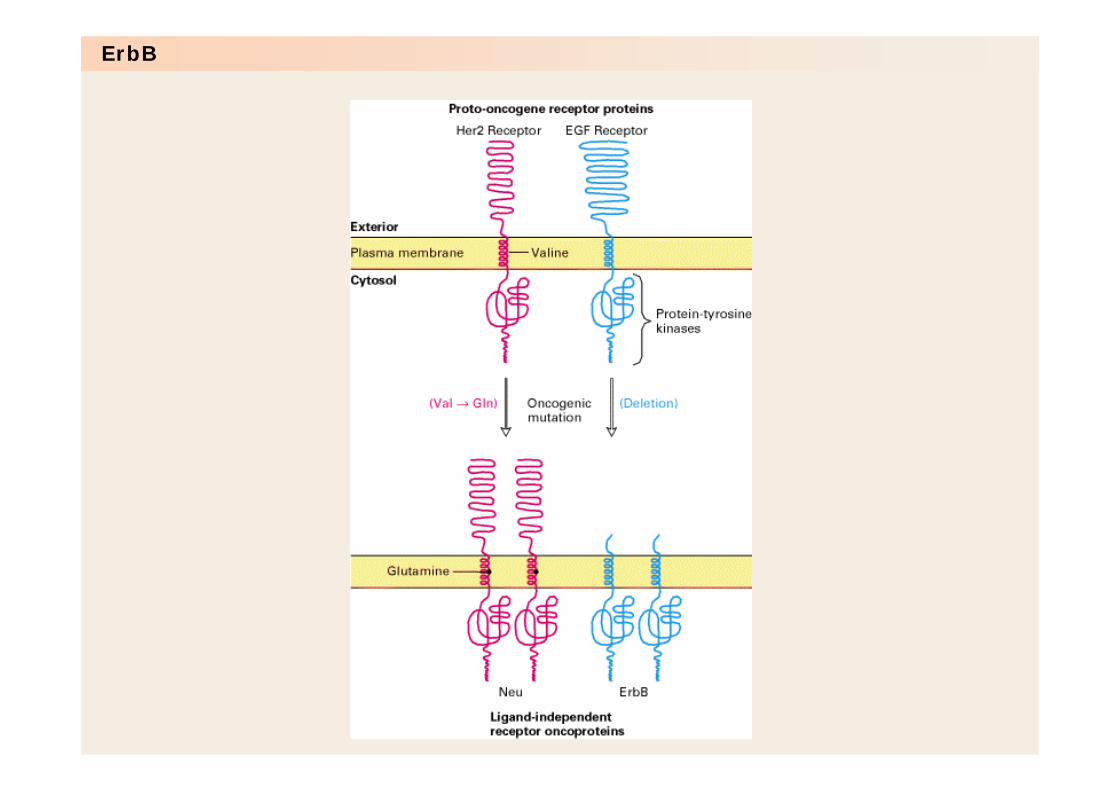
ErbB
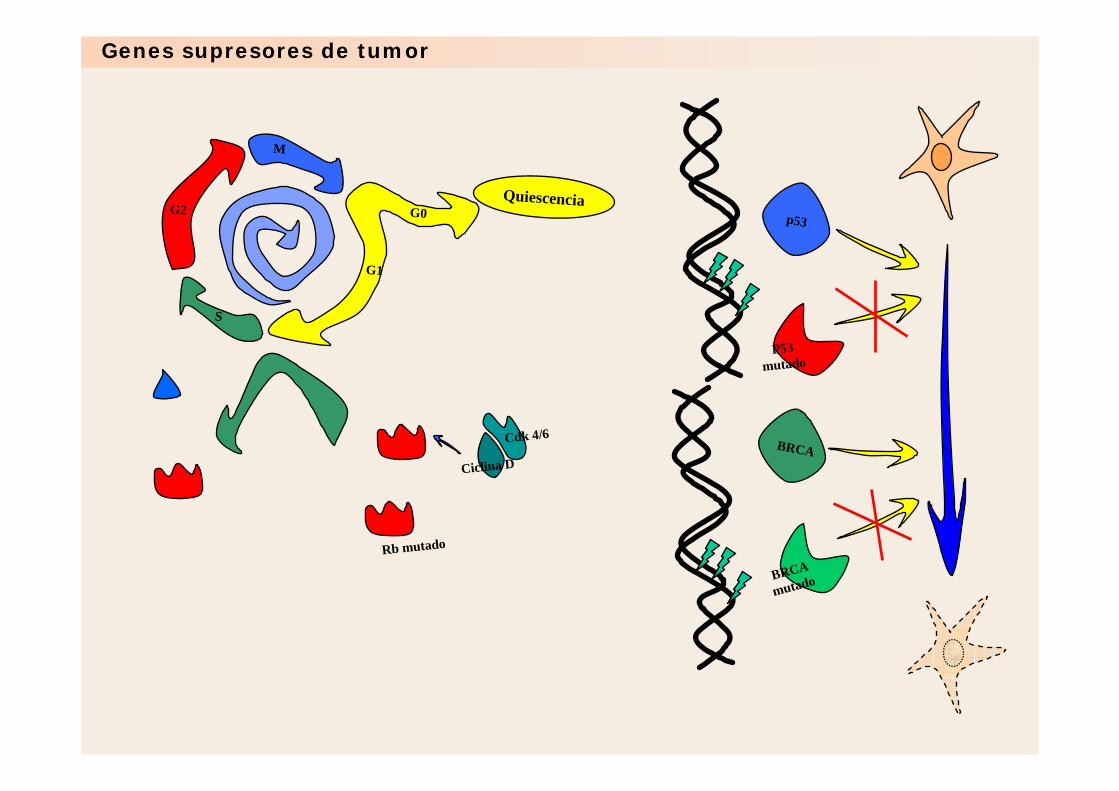
Genes supresores de tumor
M
G1
G0
S
QuiescenciaG2
E2F
Rb
Rb mutado
p53
P53mutado
BRCA
BRCA
mutado
Cdk 4/6
Ciclina D
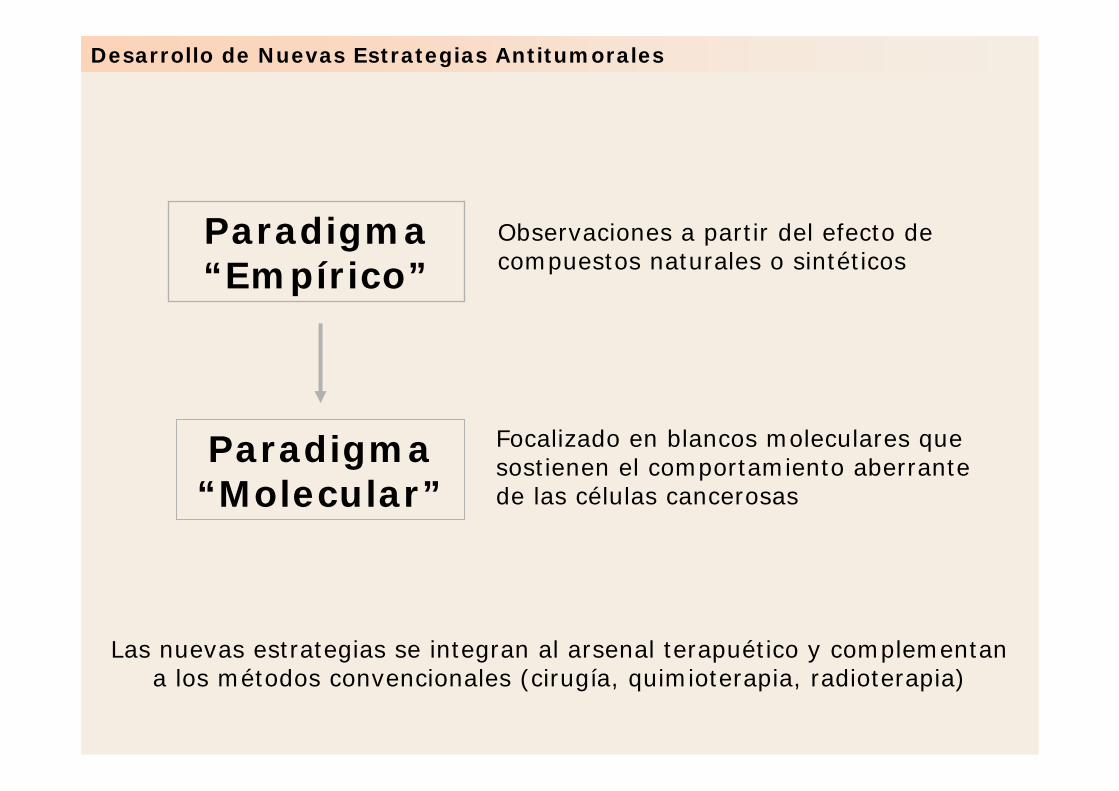
Paradigma “Empírico”
Paradigma “Molecular”
Focalizado en blancos moleculares que sostienen el comportamiento aberrante de las células cancerosas
Observaciones a partir del efecto de compuestos naturales o sintéticos
Las nuevas estrategias se integran al arsenal terapuético y complementan a los métodos convencionales (cirugía, quimioterapia, radioterapia)
Desarrollo de Nuevas Estrategias Antitumorales
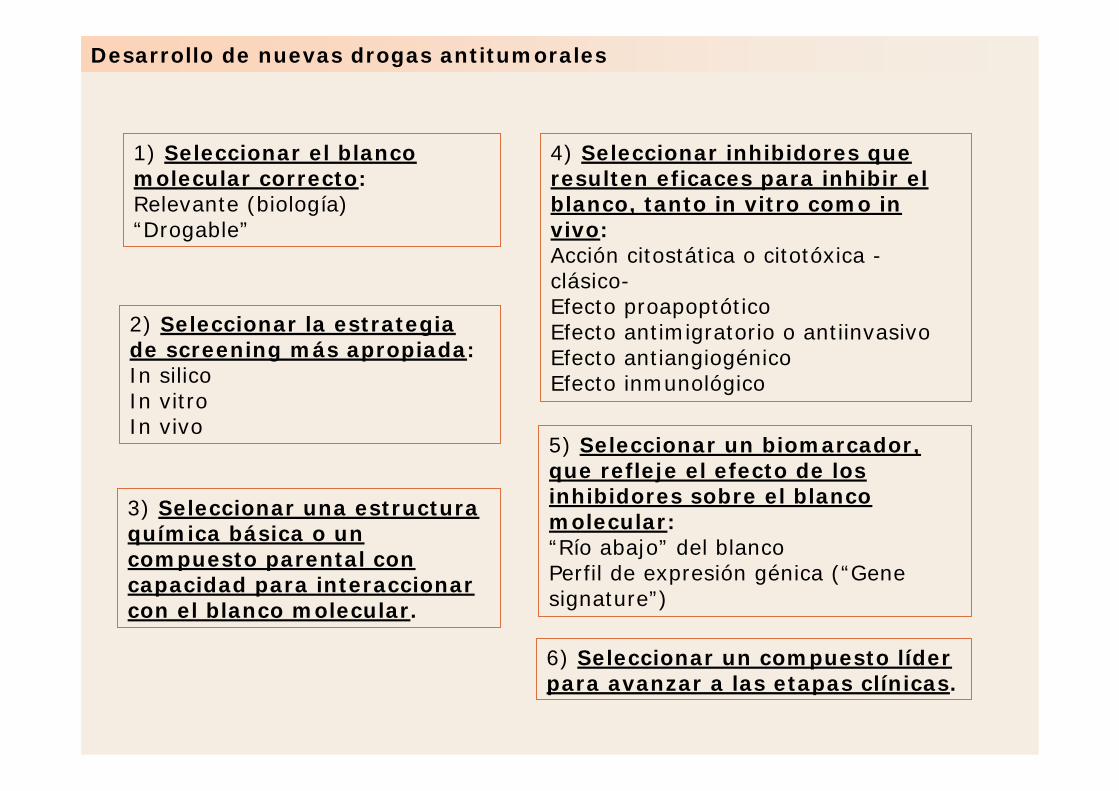
1) Seleccionar el blanco molecular correcto:Relevante (biología)“Drogable”
2) Seleccionar la estrategia de screening más apropiada:In silicoIn vitroIn vivo
3) Seleccionar una estructura química básica o un compuesto parental con capacidad para interaccionar con el blanco molecular.
4) Seleccionar inhibidores que resulten eficaces para inhibir el blanco, tanto in vitro como in vivo:Acción citostática o citotóxica -clásico-Efecto proapoptóticoEfecto antimigratorio o antiinvasivoEfecto antiangiogénicoEfecto inmunológico
5) Seleccionar un biomarcador, que refleje el efecto de los inhibidores sobre el blanco molecular:“Río abajo” del blancoPerfil de expresión génica (“Gene signature”)
6) Seleccionar un compuesto líder para avanzar a las etapas clínicas.
Desarrollo de nuevas drogas antitumorales
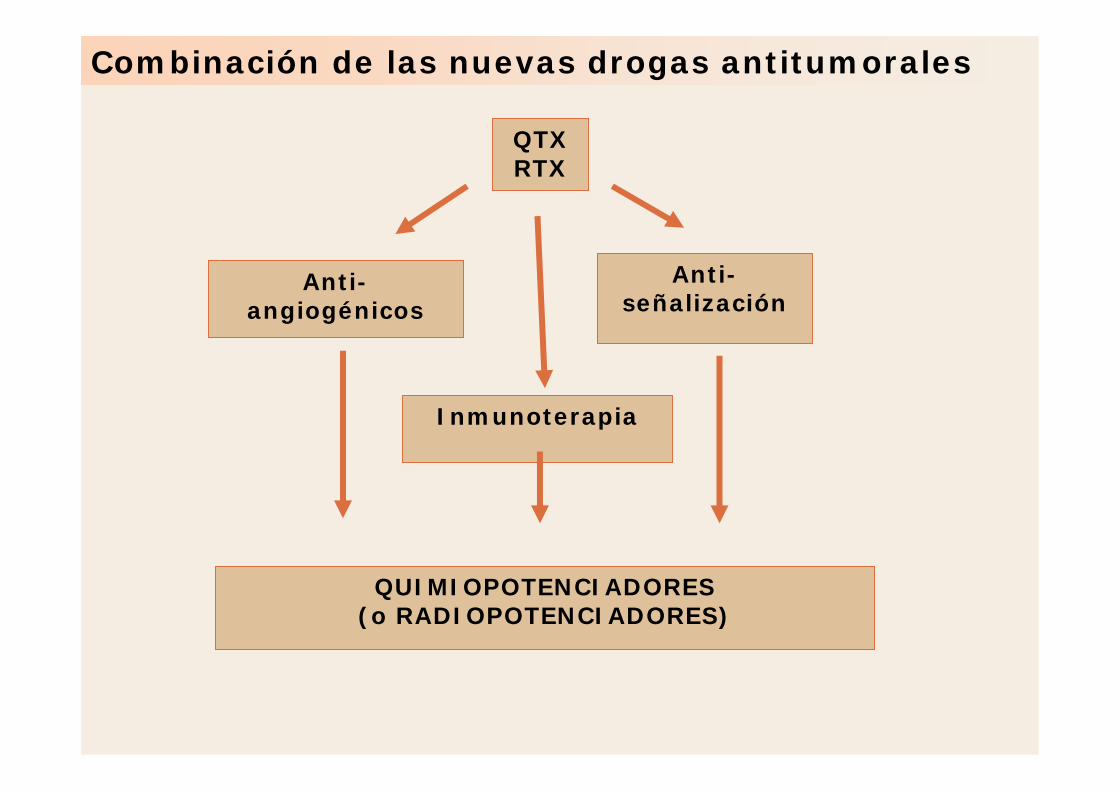
QTXRTX
Anti-angiogénicos
Inmunoterapia
Anti-señalización
QUIMIOPOTENCIADORES(o RADIOPOTENCIADORES)
Combinación de las nuevas drogas antitumorales
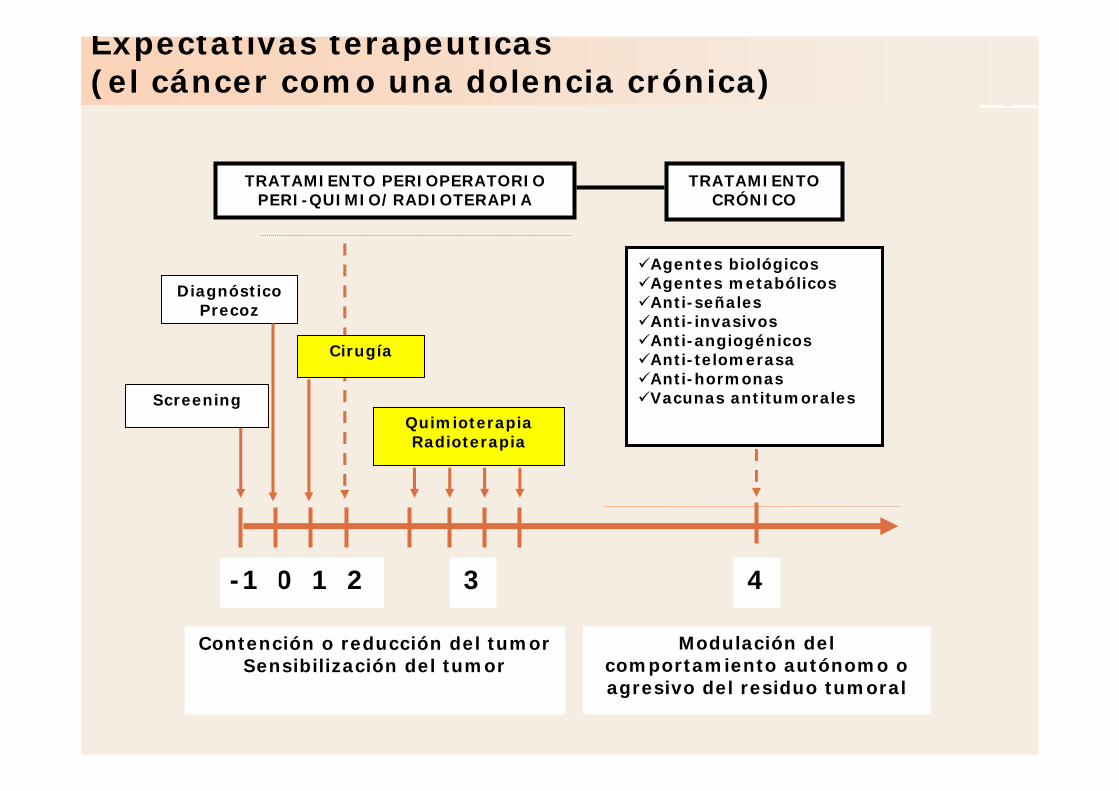
0 1 3
DiagnósticoPrecoz
Cirugía
QuimioterapiaRadioterapia
TRATAMIENTO PERIOPERATORIOPERI-QUIMIO/RADIOTERAPIA
2
TRATAMIENTOCRÓNICO
4
Agentes biológicosAgentes metabólicosAnti-señalesAnti-invasivosAnti-angiogénicosAnti-telomerasaAnti-hormonasVacunas antitumorales
Modulación del comportamiento autónomo o agresivo del residuo tumoral
-1
Screening
Contención o reducción del tumorSensibilización del tumor
Expectativas terapéuticas (el cáncer como una dolencia crónica)

ANMAT
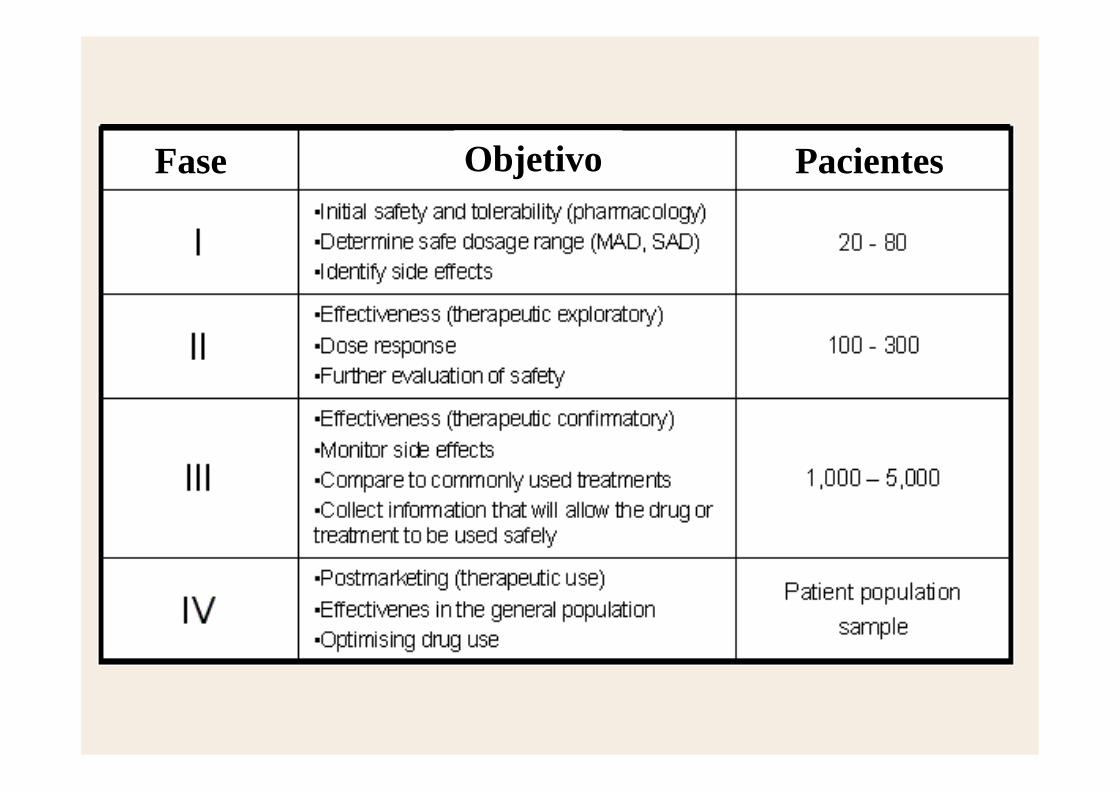
Fase Objetivo Pacientes
Inmunología del Cáncer y Vacunas Oncológicas
Dr. Mariano R. Gabri
CANCER Y SISTEMA INMUNOLOGICOCANCER Y SISTEMA INMUNOLOGICO
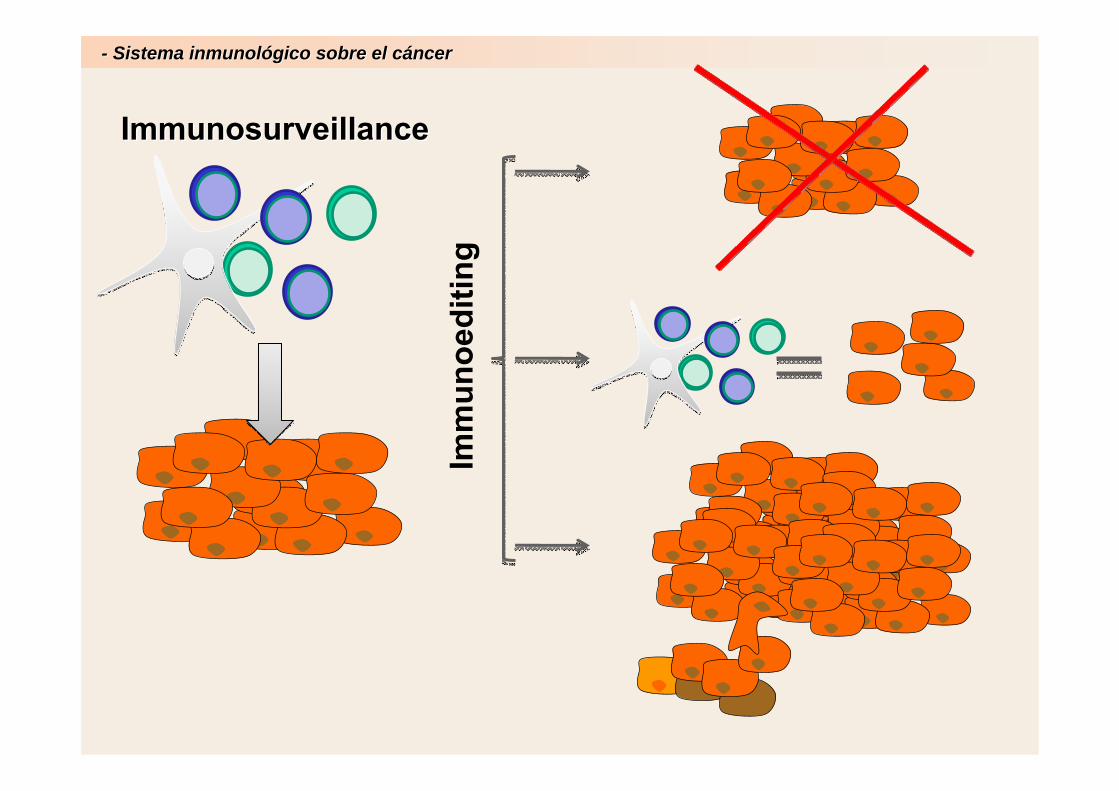
-- Sistema inmunolSistema inmunolóógico sobre el cgico sobre el cááncerncer
Imm
unoe
ditin
g
ImmunosurveillanceImmunosurveillance
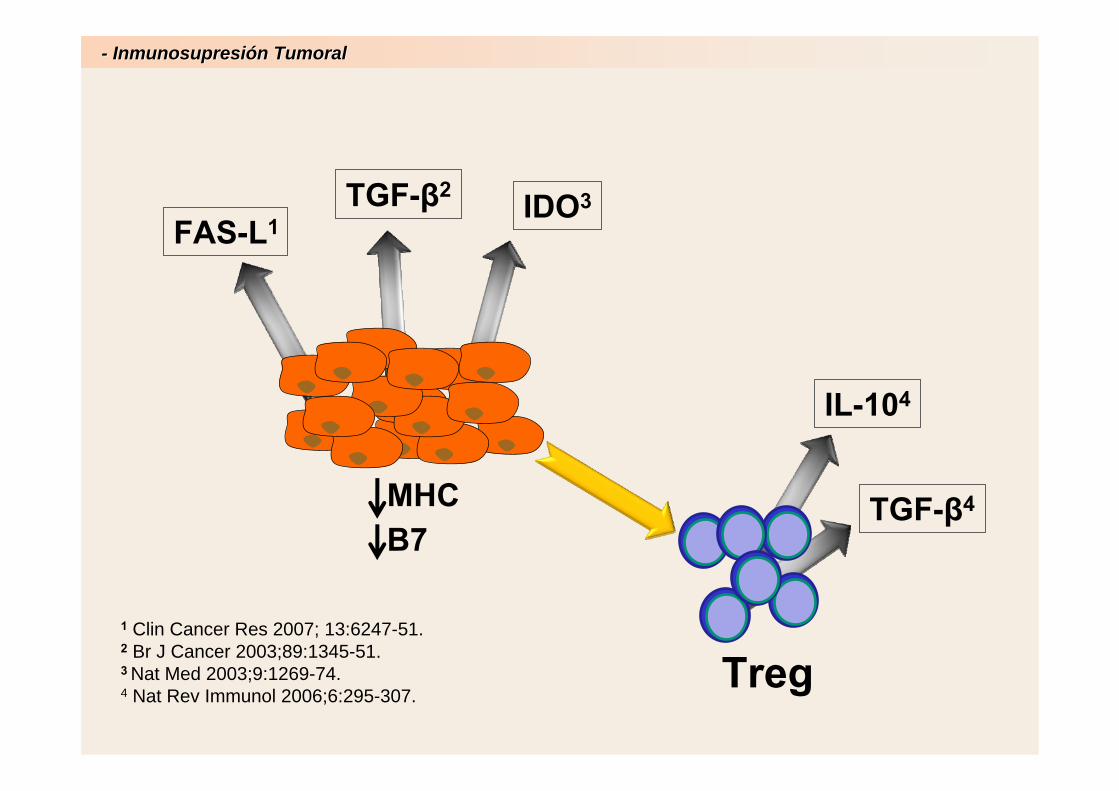
FAS-L1TGF-β2 IDO3
TGF-β4
IL-104
Treg1 Clin Cancer Res 2007; 13:6247-51.2 Br J Cancer 2003;89:1345-51.3 Nat Med 2003;9:1269-74.4 Nat Rev Immunol 2006;6:295-307.
MHCB7
-- InmunosupresiInmunosupresióón Tumoraln Tumoral
ANTIGENOS TUMORALESANTIGENOS TUMORALES
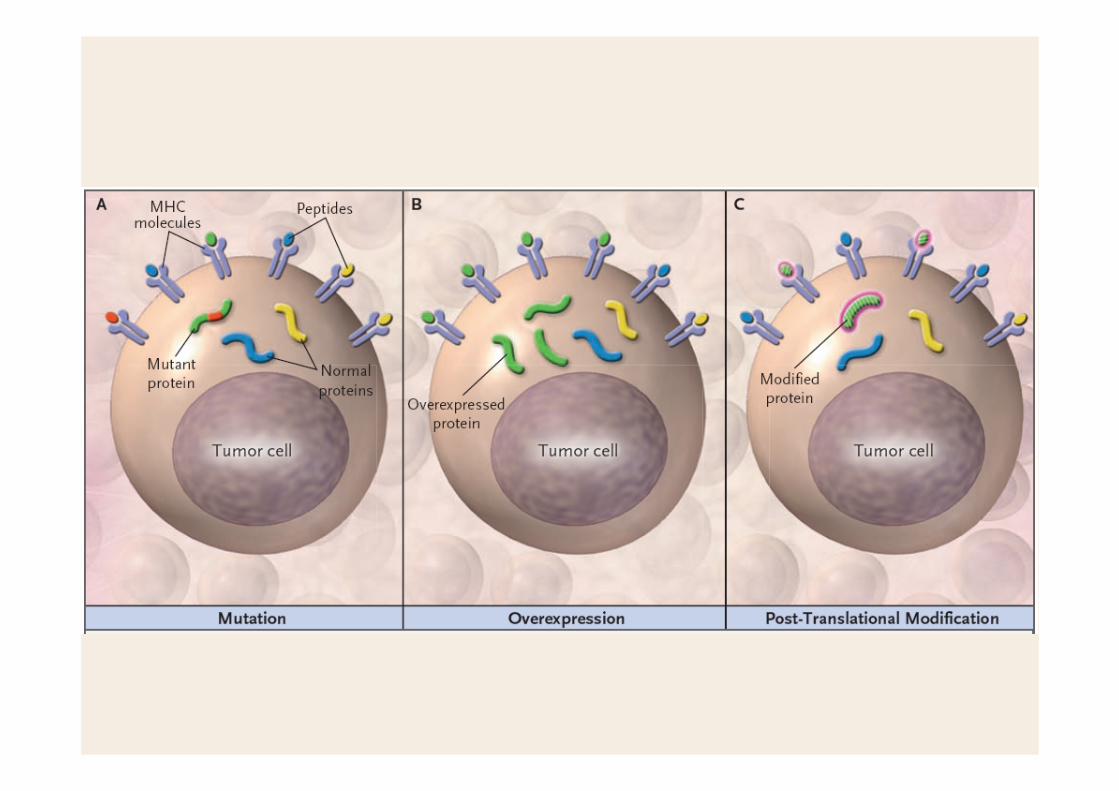
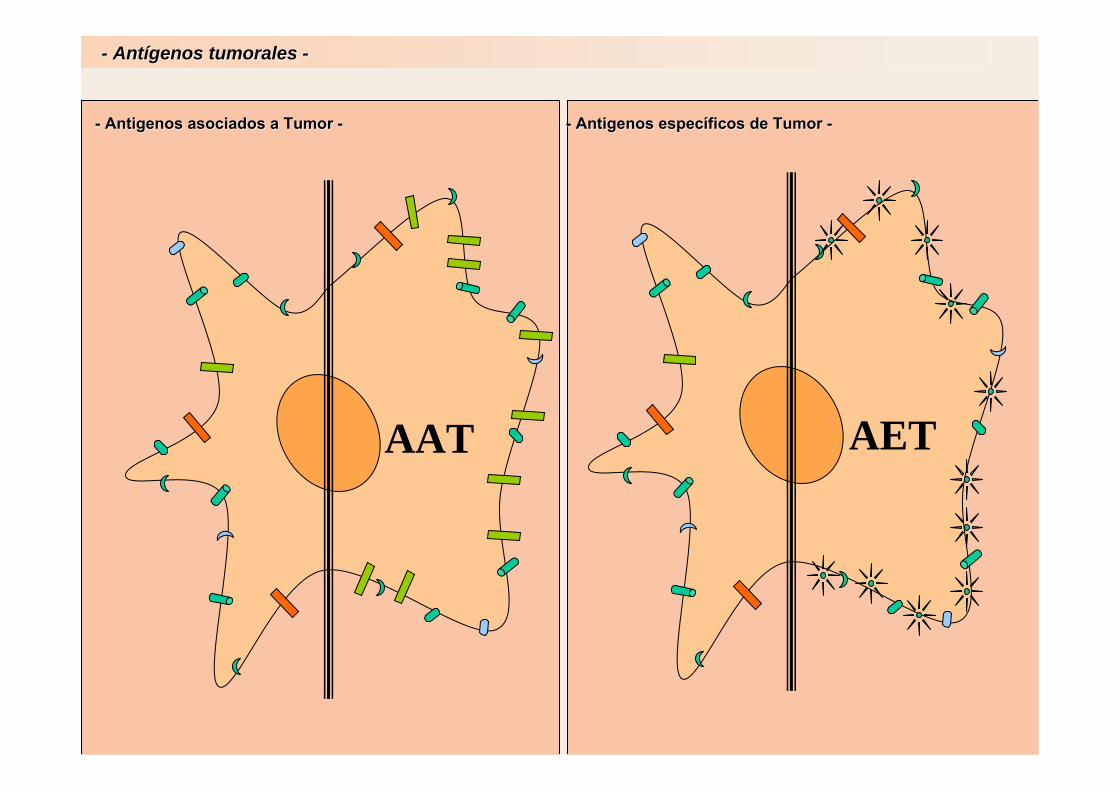
-- AntAntíígenos tumorales genos tumorales --
-- Antigenos asociados a Tumor Antigenos asociados a Tumor -- -- Antigenos especAntigenos especííficos de Tumor ficos de Tumor --
AAT AET
VACUNAS ONCOLOGICASVACUNAS ONCOLOGICAS
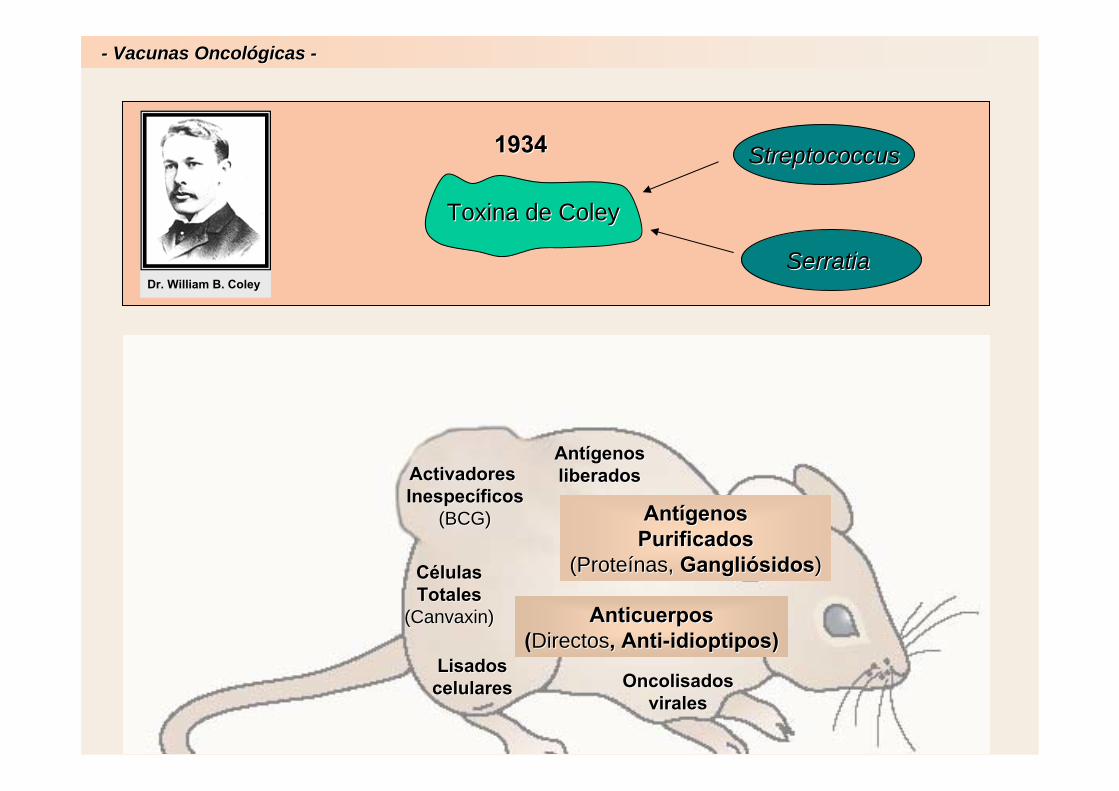
Dr. William B. Coley
Toxina de ColeyToxina de Coley
19341934 StreptococcusStreptococcus
SerratiaSerratia
Activadores Activadores InespecInespecííficosficos
(BCG)(BCG)
CCéélulaslulasTotalesTotales
(Canvaxin)(Canvaxin)
LisadosLisadoscelularescelulares
AntAntíígenosgenosliberadosliberados
AntAntíígenosgenosPurificadosPurificados
(Prote(Proteíínas, nas, GangliGanglióósidossidos))
OncolisadosOncolisadosviralesvirales
AnticuerposAnticuerpos((DirectosDirectos, Anti, Anti--idioptipos)idioptipos)
-- Vacunas OncolVacunas Oncolóógicas gicas --
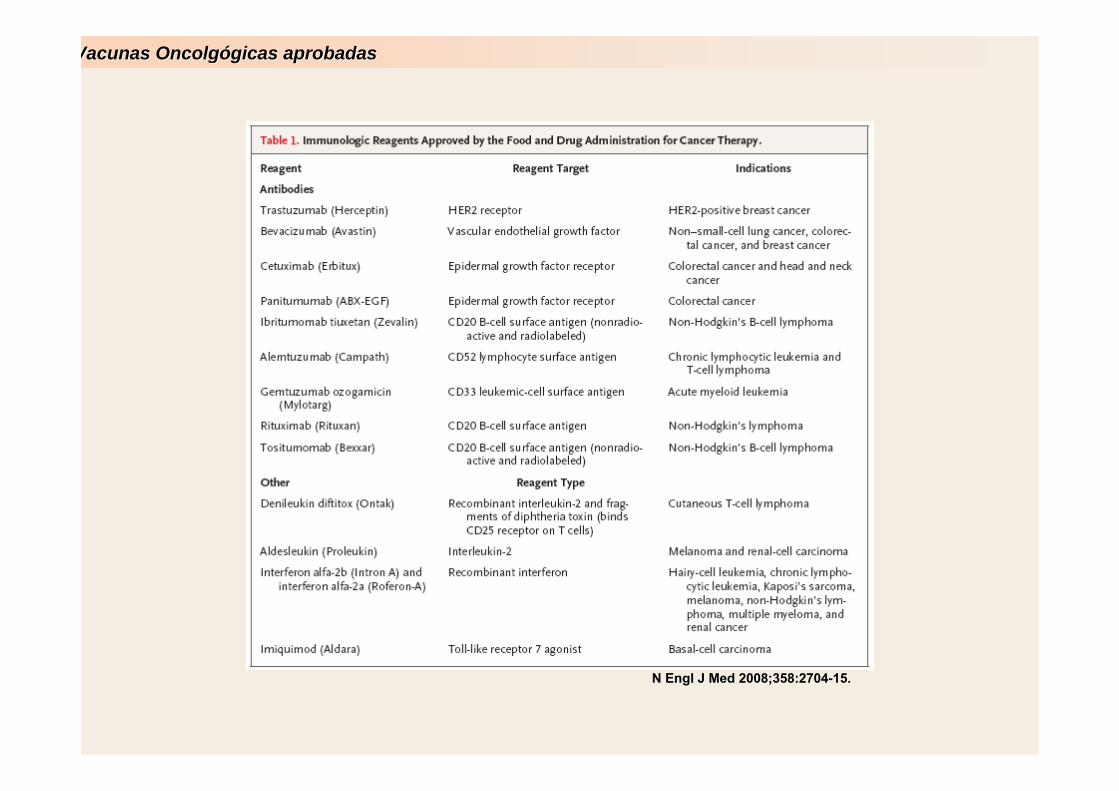
N Engl J Med 2008;358:2704-15.
Vacunas OncolgVacunas Oncolgóógicas aprobadasgicas aprobadas

Vacuna
RACOTUMOMAB®
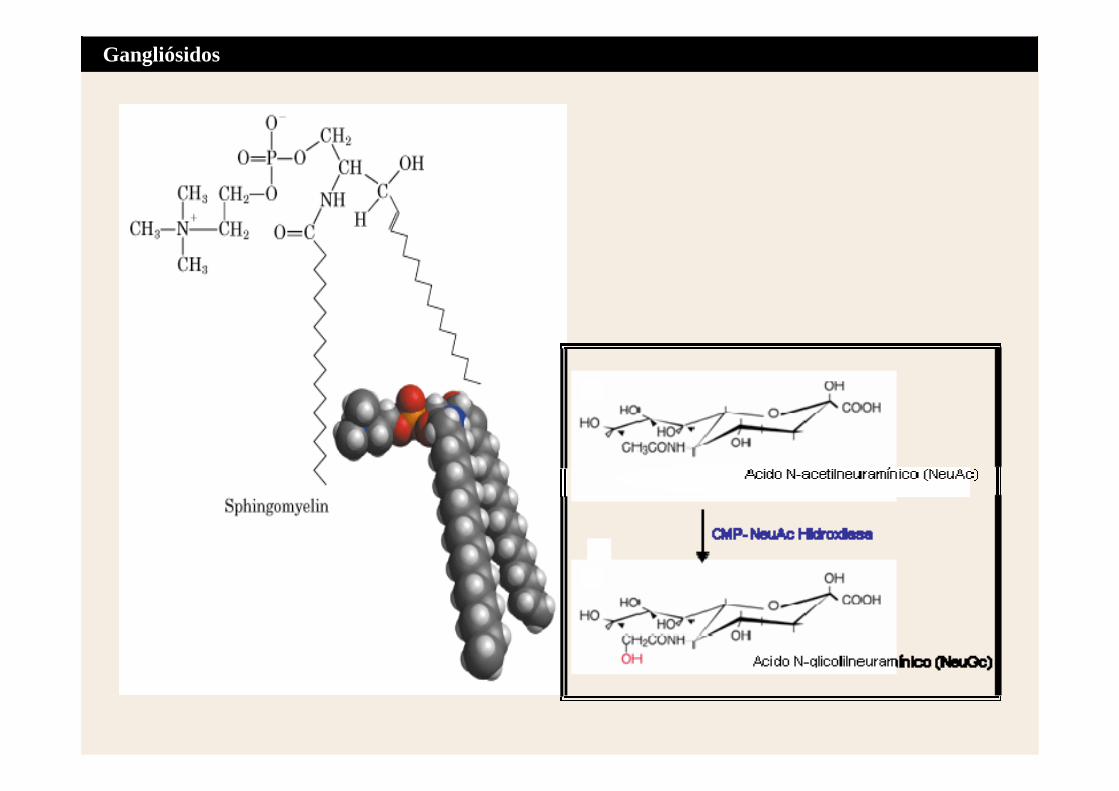
Gangliósidos
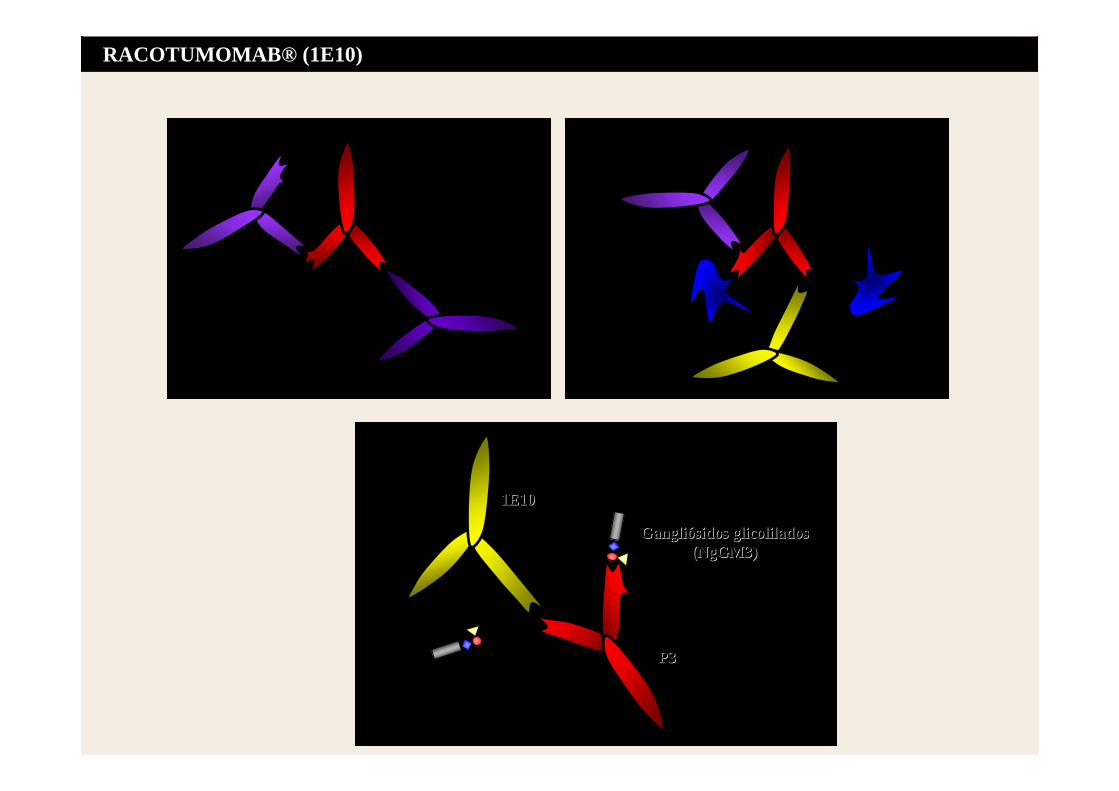
Ac2 αAc1
Ac2 β
Ac2 α
Ac1
Ac2 γ
GangliGanglióósidos glicoliladossidos glicolilados(NgGM3)(NgGM3)
P3P3
1E101E10
RACOTUMOMAB® (1E10)
Evaluación preclínica
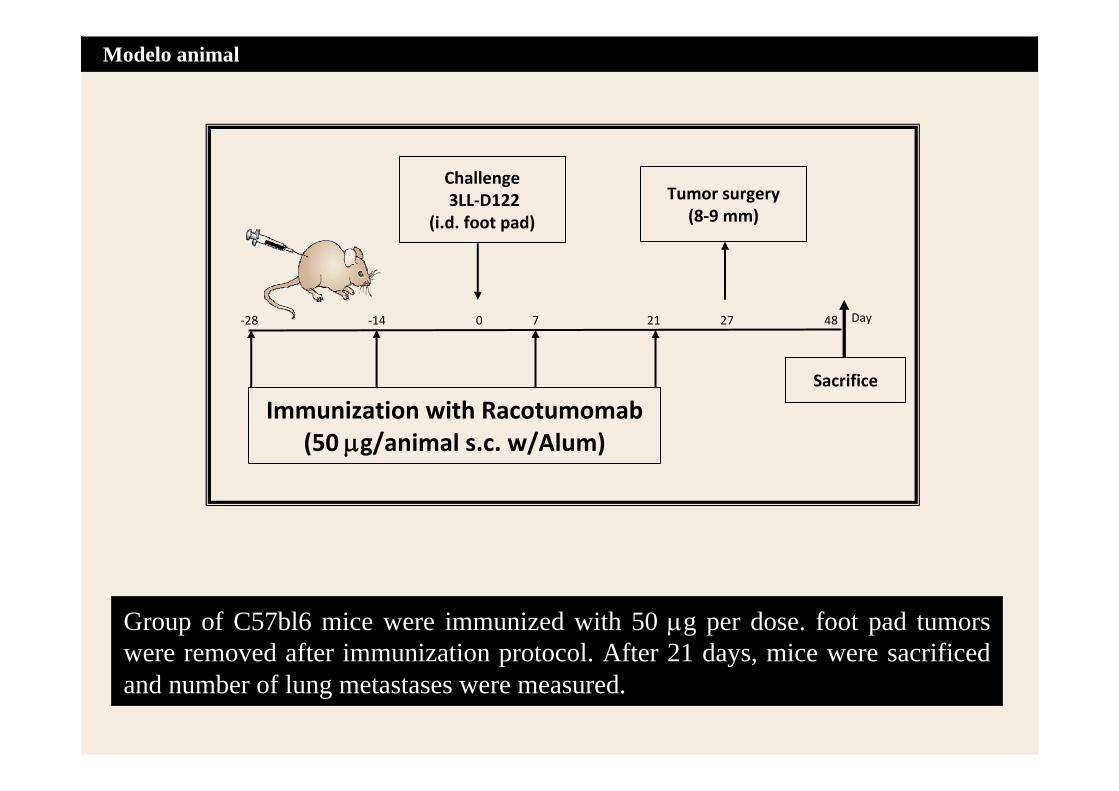
Group of C57bl6 mice were immunized with 50 μg per dose. foot pad tumors were removed after immunization protocol. After 21 days, mice were sacrificed and number of lung metastases were measured.
Immunization with Racotumomab(50 μg/animal s.c. w/Alum)
Challenge3LL‐D122
(i.d. foot pad)
Tumor surgery(8‐9 mm)
Sacrifice
Day‐28 ‐14 0 7 21 27 48
Modelo animal
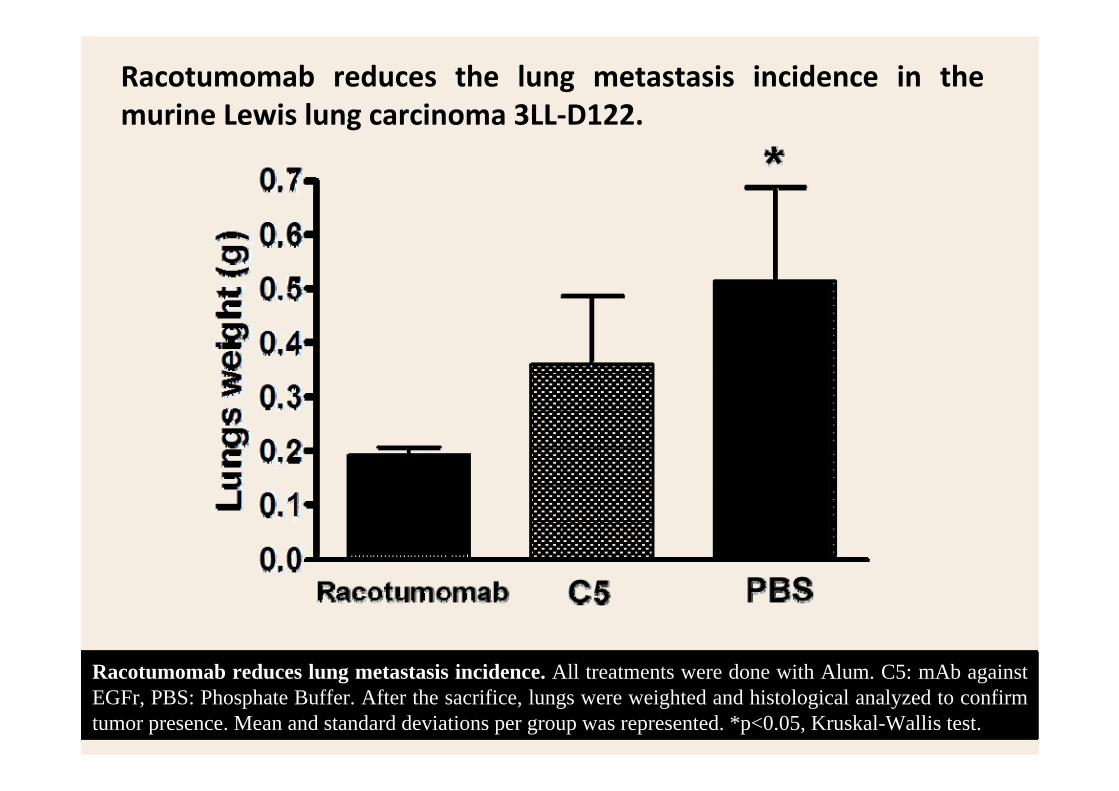
Racotumomab reduces the lung metastasis incidence in the murine Lewis lung carcinoma 3LL‐D122.
Racotumomab reduces lung metastasis incidence. All treatments were done with Alum. C5: mAb against EGFr, PBS: Phosphate Buffer. After the sacrifice, lungs were weighted and histological analyzed to confirm tumor presence. Mean and standard deviations per group was represented. *p<0.05, Kruskal-Wallis test.
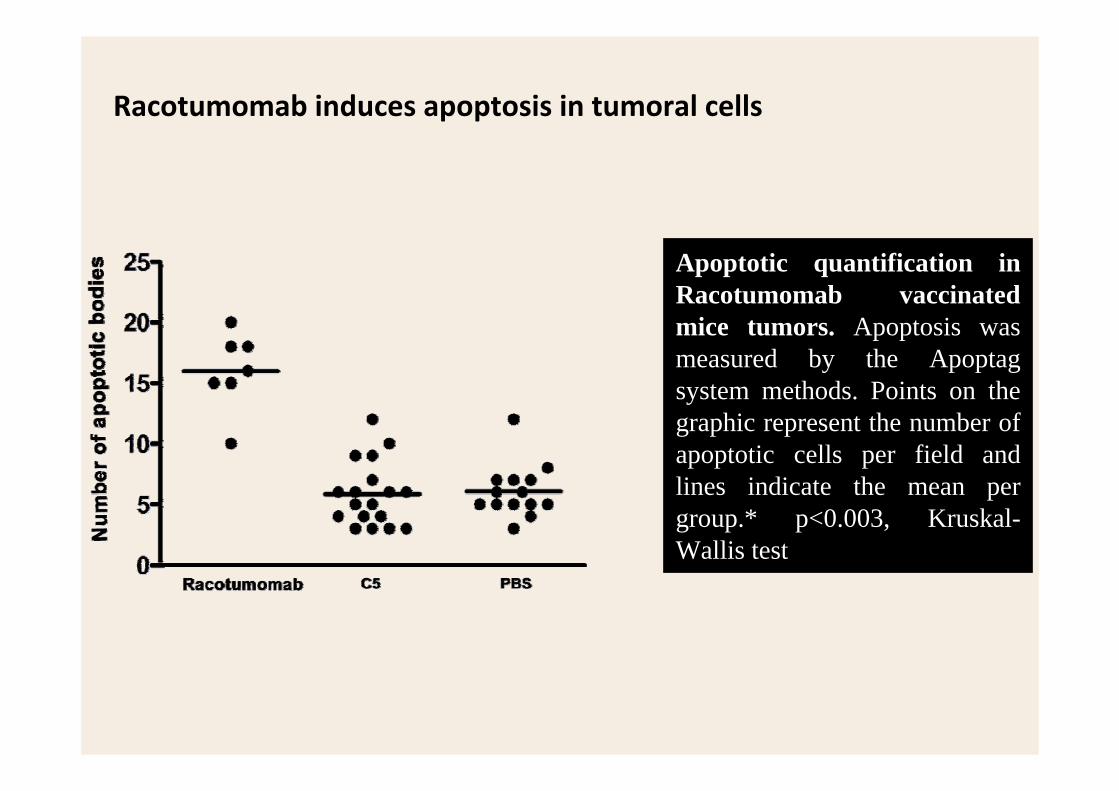
Apoptotic quantification in Racotumomab vaccinated mice tumors. Apoptosis was measured by the Apoptag system methods. Points on the graphic represent the number of apoptotic cells per field and lines indicate the mean per group.* p<0.003, Kruskal-Wallis test
Racotumomab induces apoptosis in tumoral cells
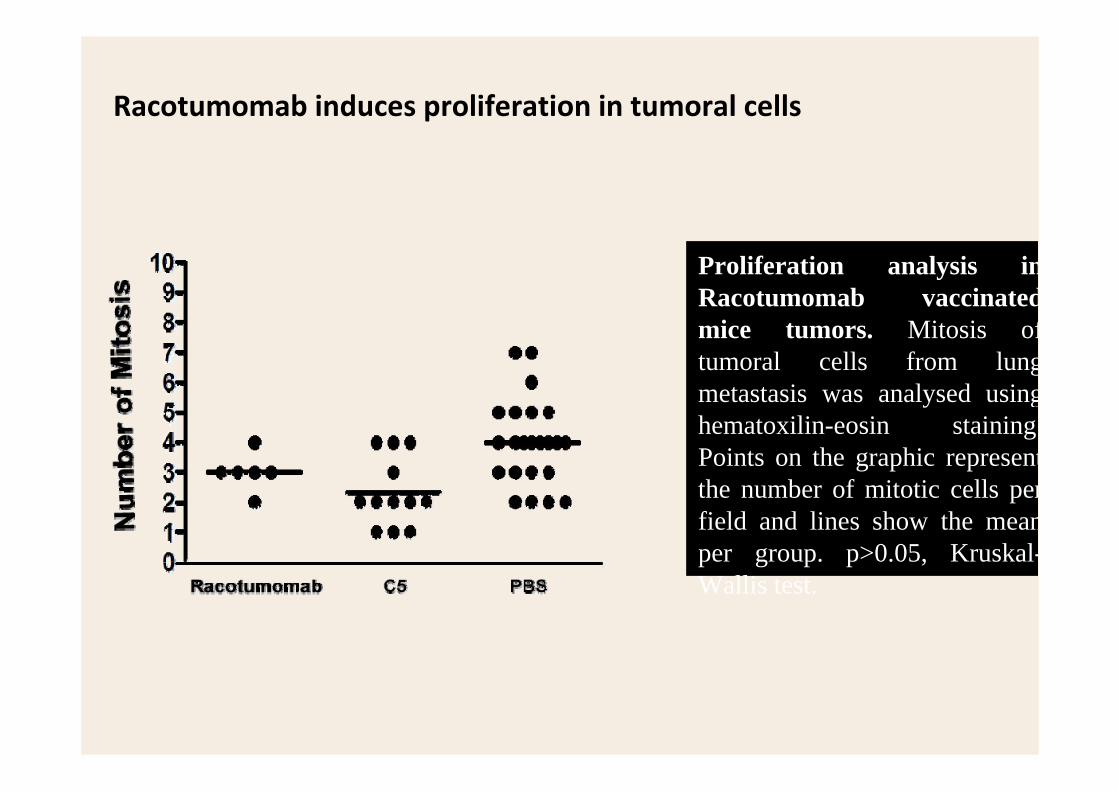
Proliferation analysis inRacotumomab vaccinatedmice tumors. Mitosis oftumoral cells from lungmetastasis was analysed usinghematoxilin-eosin staining.Points on the graphic representthe number of mitotic cells perfield and lines show the meanper group. p>0.05, Kruskal-Wallis test.
Racotumomab induces proliferation in tumoral cells
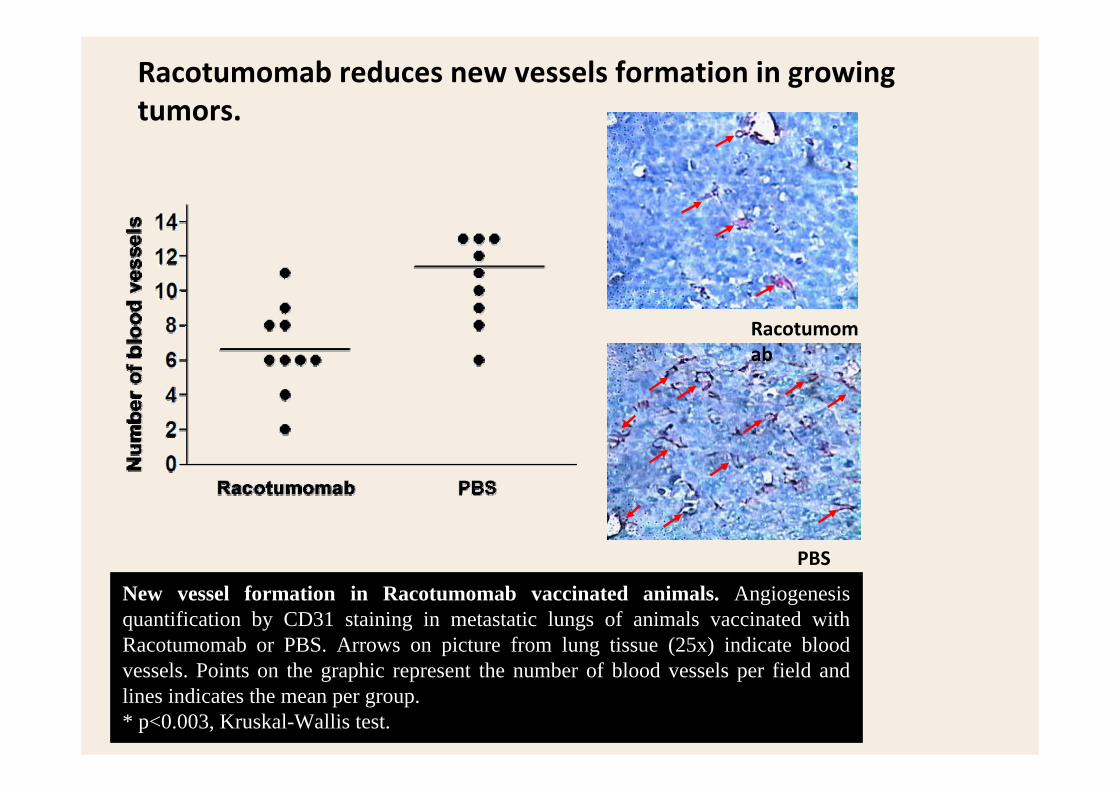
Racotumomab reduces new vessels formation in growing tumors.
PBS
Racotumomab
New vessel formation in Racotumomab vaccinated animals. Angiogenesis quantification by CD31 staining in metastatic lungs of animals vaccinated with Racotumomab or PBS. Arrows on picture from lung tissue (25x) indicate blood vessels. Points on the graphic represent the number of blood vessels per field and lines indicates the mean per group.* p<0.003, Kruskal-Wallis test.
Evaluación Clínica
Evaluación Clínica
• Ensayo piloto en melanoma de ocular y epidérmico (No. IIC RD-EC030)
• Ensayo Clínico de Fase I en pacientes con cáncer de mama avanzado (No. IIC RD-EC 044)
• Ensayo Clínico de Fase I en pacientes con Cáncer de Pulmón a Células Pequéñas (No. IICP- EC O43)
• Ensayo Clínico de Fase I en pacientes con cáncer de mama avanzado con alto riesgo de recaída
• Ensayo Clínico compasional en pacientes con Cáncer de Pulmón a Células No Pequeñas
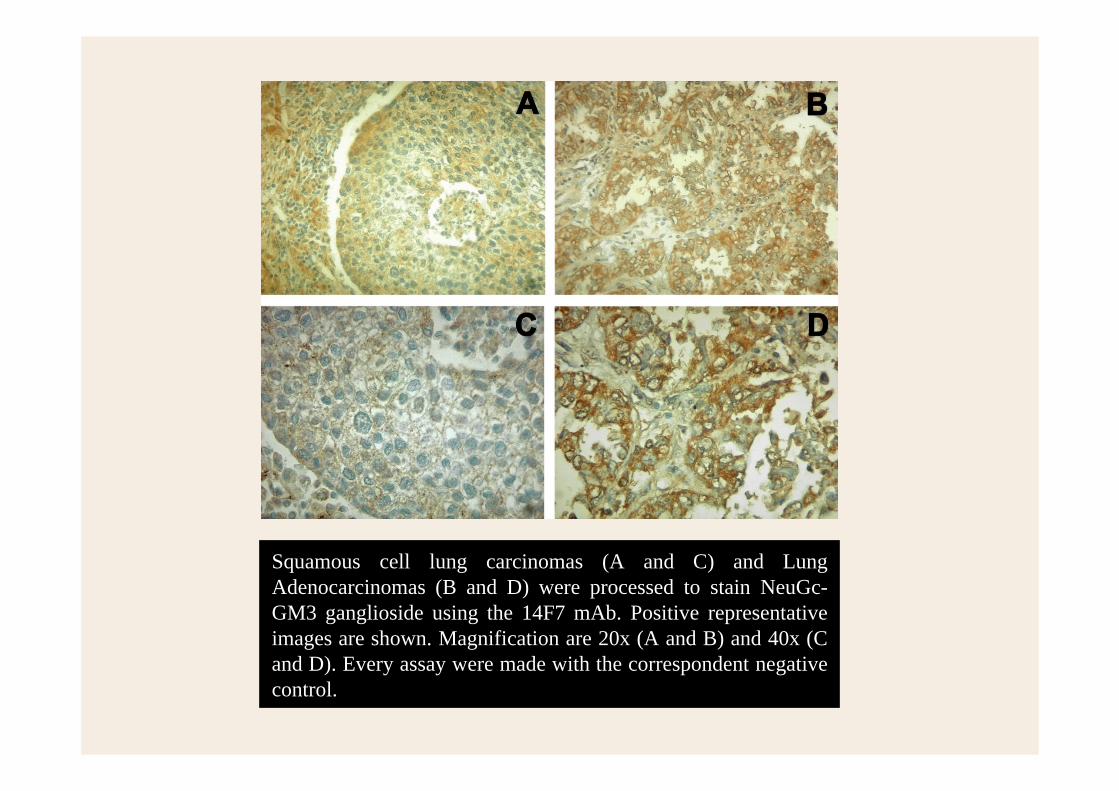
Squamous cell lung carcinomas (A and C) and Lung Adenocarcinomas (B and D) were processed to stain NeuGc-GM3 ganglioside using the 14F7 mAb. Positive representative images are shown. Magnification are 20x (A and B) and 40x (C and D). Every assay were made with the correspondent negative control.
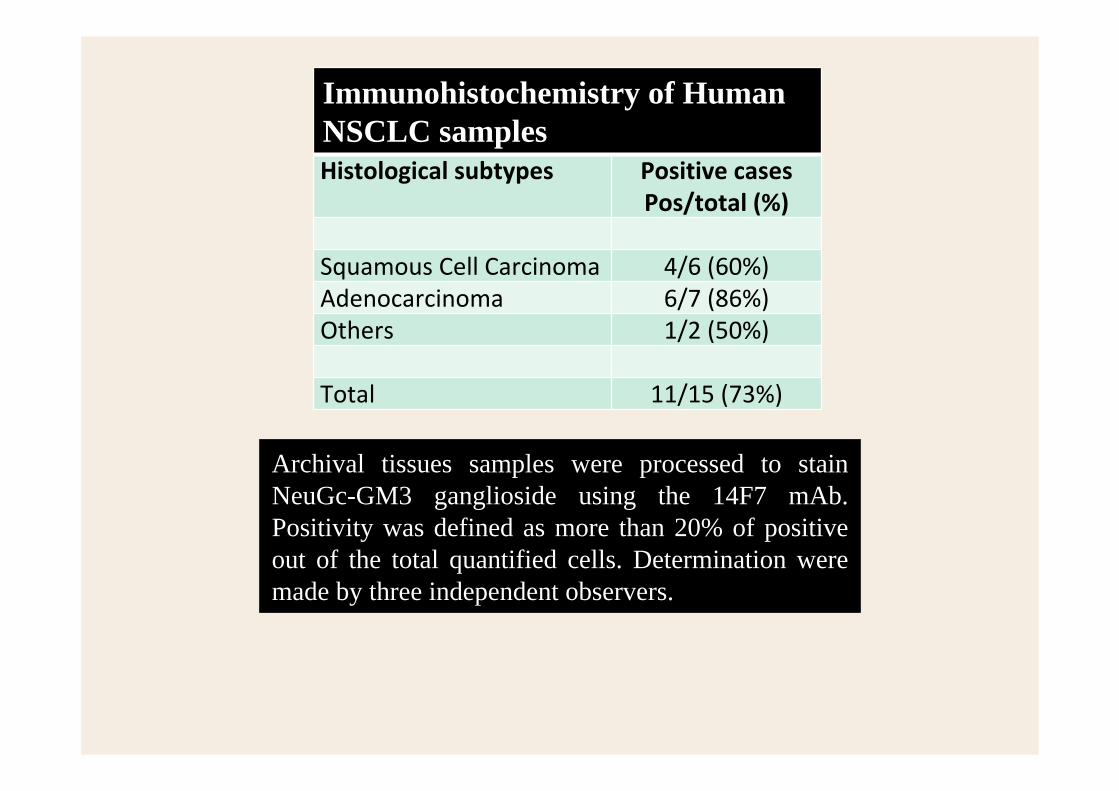
Archival tissues samples were processed to stain NeuGc-GM3 ganglioside using the 14F7 mAb. Positivity was defined as more than 20% of positive out of the total quantified cells. Determination were made by three independent observers.
Immunohistochemistry of Human NSCLC samplesHistological subtypes Positive cases
Pos/total (%)
Squamous Cell Carcinoma 4/6 (60%)Adenocarcinoma 6/7 (86%)Others 1/2 (50%)
Total 11/15 (73%)
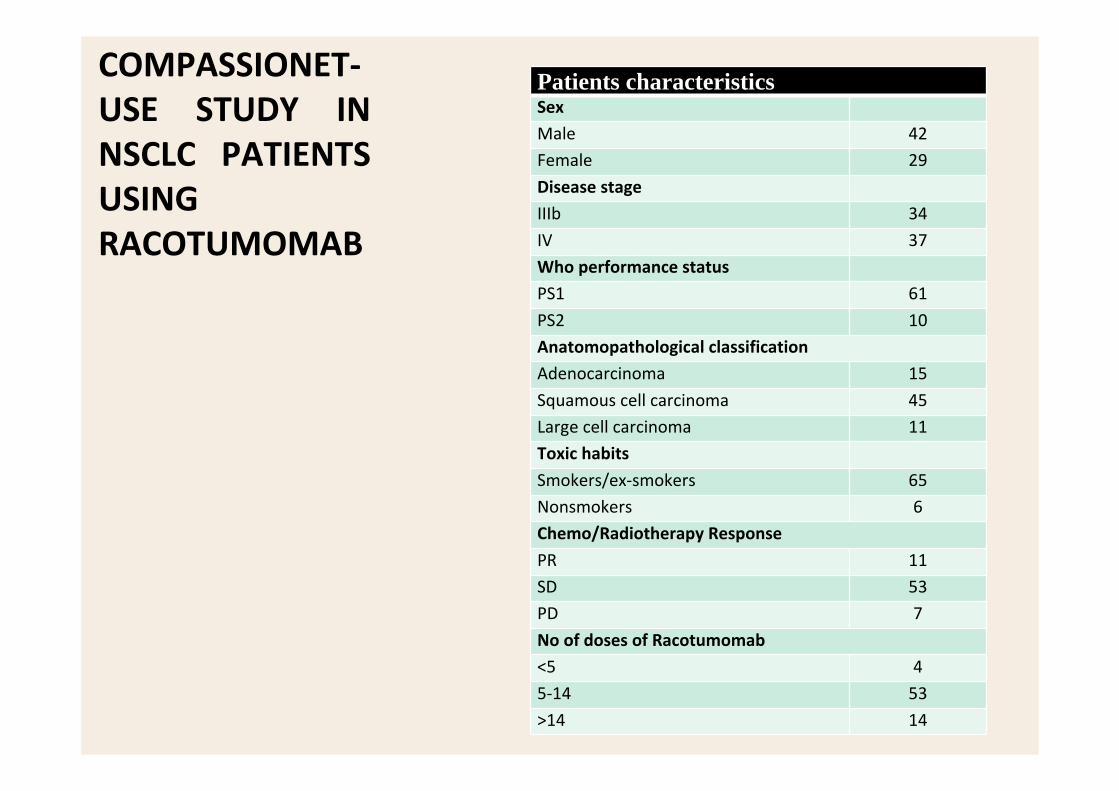
Patients characteristicsSexMale 42Female 29
Disease stageIIIb 34
IV 37
Who performance statusPS1 61
PS2 10Anatomopathological classification Adenocarcinoma 15
Squamous cell carcinoma 45Large cell carcinoma 11Toxic habits
Smokers/ex‐smokers 65Nonsmokers 6Chemo/Radiotherapy Response
PR 11SD 53PD 7
No of doses of Racotumomab<5 4
5‐14 53
>14 14
COMPASSIONET‐USE STUDY IN NSCLC PATIENTS USING RACOTUMOMAB
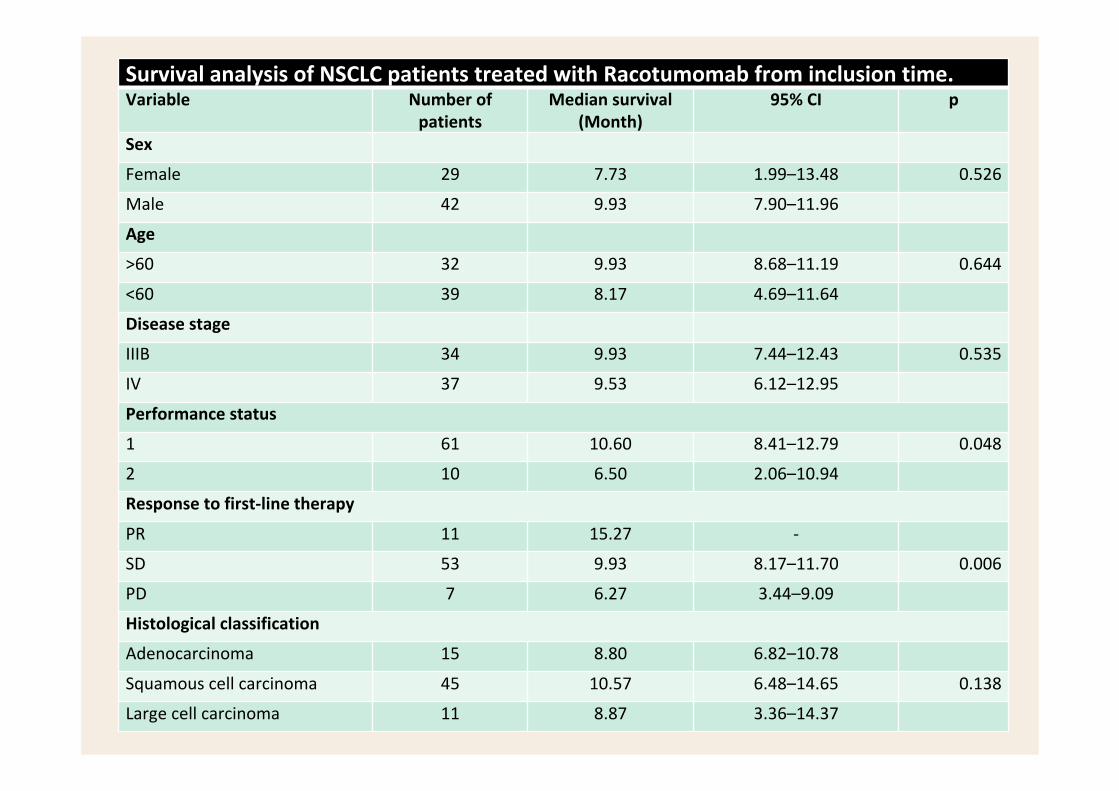
Survival analysis of NSCLC patients treated with Racotumomab from inclusion time.Variable Number of
patientsMedian survival
(Month)95% CI p
Sex
Female 29 7.73 1.99–13.48 0.526
Male 42 9.93 7.90–11.96
Age
>60 32 9.93 8.68–11.19 0.644
<60 39 8.17 4.69–11.64
Disease stage
IIIB 34 9.93 7.44–12.43 0.535
IV 37 9.53 6.12–12.95
Performance status
1 61 10.60 8.41–12.79 0.048
2 10 6.50 2.06–10.94
Response to first‐line therapy
PR 11 15.27 ‐
SD 53 9.93 8.17–11.70 0.006
PD 7 6.27 3.44–9.09
Histological classification
Adenocarcinoma 15 8.80 6.82–10.78
Squamous cell carcinoma 45 10.57 6.48–14.65 0.138
Large cell carcinoma 11 8.87 3.36–14.37
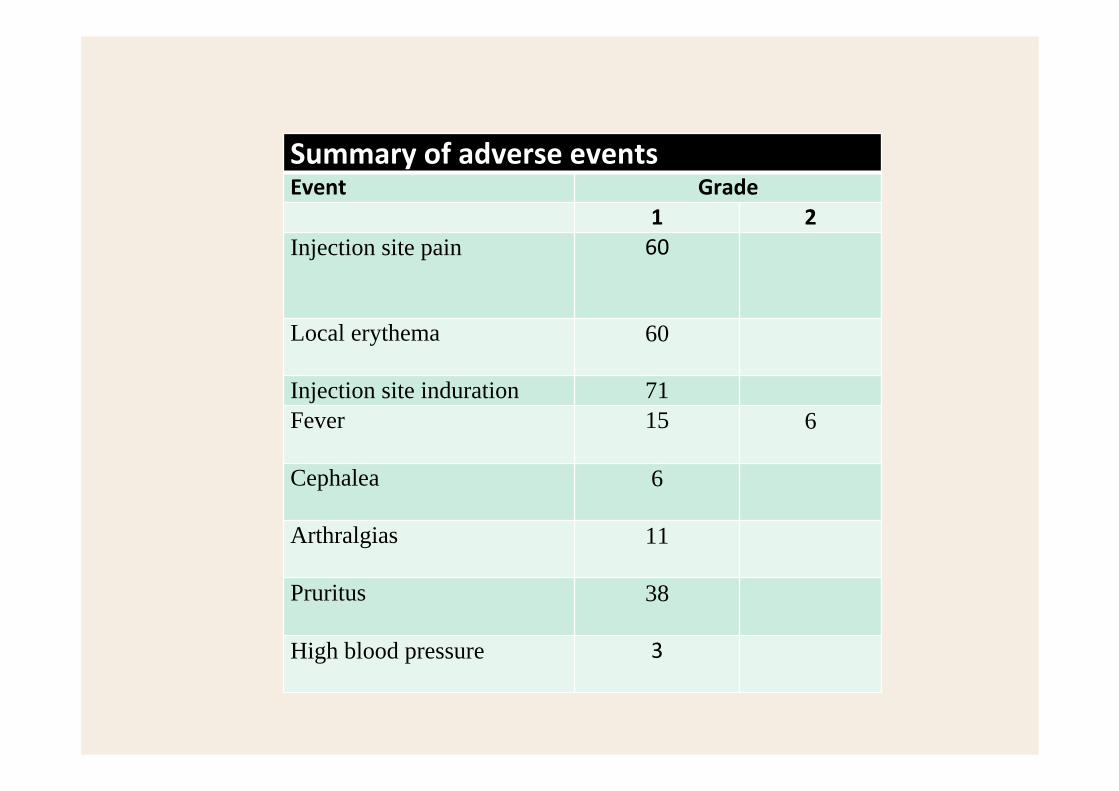
Summary of adverse eventsEvent Grade
1 2Injection site pain 60
Local erythema 60
Injection site induration 71Fever 15 6
Cephalea 6
Arthralgias 11
Pruritus 38
High blood pressure 3
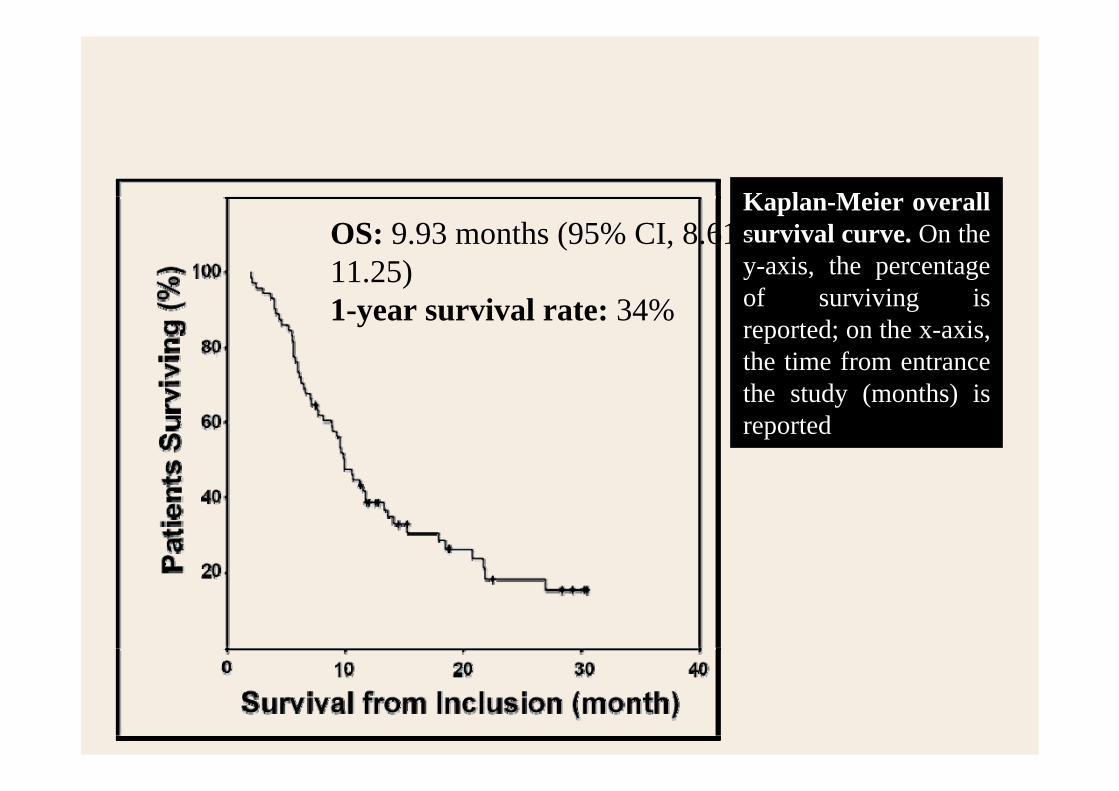
Kaplan-Meier overall survival curve. On the y-axis, the percentage of surviving is reported; on the x-axis, the time from entrance the study (months) is reported
OS: 9.93 months (95% CI, 8.61–11.25)1-year survival rate: 34%
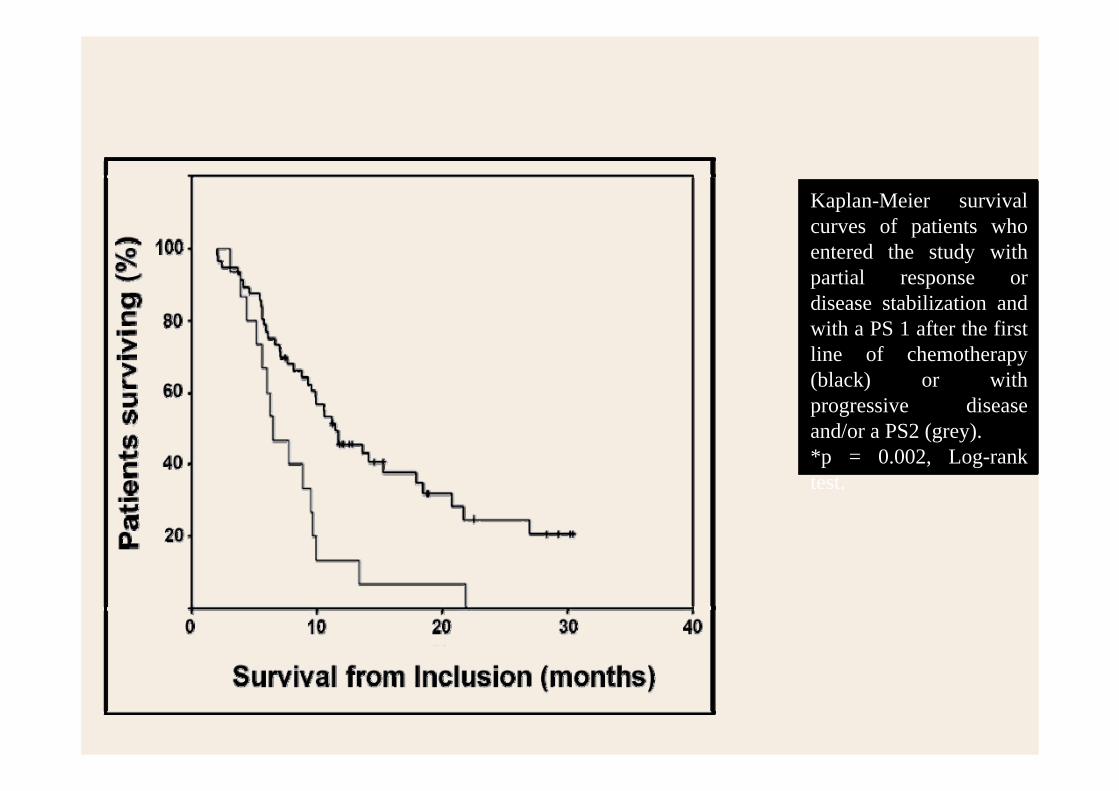
Kaplan-Meier survival curves of patients who entered the study with partial response or disease stabilization and with a PS 1 after the first line of chemotherapy (black) or with progressive disease and/or a PS2 (grey). *p = 0.002, Log-rank test.