Pancreas anat,phy,cong.anamolies
61
PANCREAS: Anatomy ,Physiology &CongenitalAnomalies
-
Upload
pradeep-pande -
Category
Education
-
view
1.011 -
download
1
Transcript of Pancreas anat,phy,cong.anamolies

PANCREAS: Anatomy ,Physiology
&CongenitalAnomalies

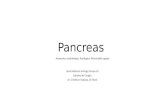
Pancreas

Pancreas
• Gland with both exocrine and endocrine functions
• 6-10 inch in length• 60-100 gram in weight

Pancreas
• Location: Retro-peritoneum, 2nd lumbar vertebral level
• Extends in an oblique, transverse position
• Parts of pancreas: head, neck, body and tail


Head of Pancreas
• Includes uncinate process• Flattened structure, 2 – 3 cm thick• Attached to the 2nd and 3rd portions of duodenum
on the right• Merges into neck on the left• SPDA and IPDA anastamose between the
duodenum and the rt. lateral border

Neck of Pancreas• 2.5 cm in length• Straddles SMV and PV• Superior border relates to the pylorus• Superior mesenteric vessels emerge from the
inferior border• Posteriorly, SMV and splenic vein confluence
to form portal vein

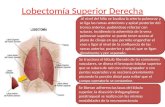
Body of Pancreas• Elongated, long structure• Anterior surface, separated from stomach
by lesser sac• Posterior surface, related to aorta, Lt.
adrenal gland, Lt. renal vessels and upper 1/3rd of Lt. kidney
• Splenic vein runs embedded in the post. surface closer to the superior border
• Inferior surface is covered by transverse mesocolon

-

Anterior Relations
• From Right to Left-– Transverse colon– Attachment of transverse mesocolon– The lesser sac– Stomach

Tail of Pancreas
• Narrow, short segment• Lies at the level of the 12th thoracic vertebra• Ends within the splenic hilum• Lies in the splenophrenic ligament• Anteriorly, related to splenic flexure of
colon• May be injured during splenectomy (fistula)

Tail of Pancreas
• Narrow, short segment• Lies at the level of the 12th thoracic vertebra• Ends within the splenic hilum• Lies in the splenophrenic ligament• Anteriorly, related to splenic flexure of
colon• May be injured during splenectomy (fistula)

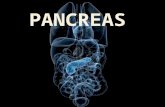
Arterial Supply of Pancreas
• Variety of major arterial sources (Celiac, SMA and Splenic)
• Celiac Common Hepatic Artery Gastroduodenal Artery Superior pancreaticoduodenal artery which divides into anterior and posterior branches
• SMA Inferior pancreaticoduodenal artery which divides into anterior and posterior branches

Arterial Supply of Pancreas
Body and tail supplied by splenic artery by about 10 branches
Three big branches from splenic are– Dorsal pancreatic artery– Pancreatica Magna (midportion of body)– Caudal pancreatic artery (tail)

Venous Drainage of the Pancreas
• Follows arterial supply• Anterior and posterior arcades drain head and
the body• Splenic vein drains the body and tail• Ultimately, into portal vein

Lymphatic Drainage
• Rich periacinar network that drain into 5 nodal groups– Superior nodes– Anterior nodes– Inferior nodes– Posterior PD nodes– Splenic nodesUltimately drain into Celiac and Superior mesenteric Lymph nodes

Innervation of Pancreas• Sympathetic fibers from the splanchnic
nerves• Parasympathetic fibers from the vagus• Both give rise to intrapancreatic periacinar
plexuses• Parasympathetic fibers stimulate both
exocrine and endocrine secretion• Sympathetic fibers have a predominantly
inhibitory effect

Innervation of Pancreas
• Rich afferent sensory fiber network• Ganglionectomy or celiac ganglion
blockade interrupt these somatic fibers (pancreatic pain)
• However the origin of pancreatic pain is difficult to explain anatomically

Histology-Exocrine Pancreas• 2 major components – Acinar cells and Ducts• They constitute 80% to 90% of the pancreatic
mass• 20 to 40 acinar cells coalesce into a unit
called the acinus• Acinar cells secrete the digestive enzymes• Centroacinar cell (2nd cell type in the acinus)
is responsible for fluid and electrolyte secretion by the pancreas

-

Physiology – Exocrine Pancreas
• 500 to 800 ml pancreatic fluid secreted per day
• Alkaline pH results from secreted bicarbonate which serves to neutralize gastric acid and regulate the pH of the intestine
• Enzymes digest carbohydrates, proteins, and fats

Bicarbonate Secretion• Bicarbonate is formed from carbonic acid
by the enzyme carbonic anhydrase• Major stimulants
Secretin, Cholecystokinin, Gastrin, Acetylcholine
• Major inhibitorsAtropine, Somatostatin, Pancreatic polypeptide and Glucagon
• Secretin - released from the duodenal mucosa in response to a duodenal luminal pH < 3

Enzyme Secretion
• Acinar cells secrete isozymes– amylases, lipases, and proteases
• Major stimulants– Cholecystokinin, Acetylcholine, Secretin, VIP

Enzymes
• Amylase– only digestive enzyme secreted by the pancreas in
an active form– hydrolyzes starch and glycogen to glucose,
maltose, maltotriose, and dextrins• Lipase
– emulsify and hydrolyze fat in the presence of bile salts

--
Physiology – Endocrine Pancreas

Insulin
• Synthesized in the B cells of the islets of Langerhans
• Stimulates transport of glucose from serum into cells.

Insulin
• Major stimulants– Glucose, amino acids, glucagon, GIP, CCK,
sulfonylurea compounds, β-Sympathetic fibers• Major inhibitors
– somatostatin, amylin, pancreastatin, α-sympathetic fibers

Glucagon
• Secreted by the A cells of the islet• Glucagon elevates blood glucose levels through the
stimulation of glycogenolysis and gluconeogenesis• Major stimulants
– Aminoacids, Cholinergic fibers, β-Sympathetic fibers• Major inhibitors
– Glucose, insulin, somatostatin, α-sympathetic fibers

Somatostatin
• Secreted by the D cells of the islet• Inhibits the release of growth hormone• Inhibits the release of almost all peptide
hormones• Inhibits gastric, pancreatic, and biliary
secretion• Used to treat both endocrine and exocrine
disorders

Pancreatic Function Tests Secretin Test
• Overnight fast• Double lumen tube• Basal secretion• 2u/kg of Secretin• Four 20 min collections of secretions• Test for volume, bicarbonate, amylase• Useful for diagnosing gastrinomas

Fecal fat test
• Distinguish between pancreatic dysfunction and intestinal malabsorption
• In Pancreatic disease when lipase secretion is reduced by 90%- 24-hour fecal fat content is elevated to more than 20 g.
• Intestinal dysfunction - Steatorrhea with low levels of fecal fat
• Use- Efficacy of pancreatic enzyme replacement

Paraaminobenzoic(PABA) acid test
• Noninvasive test of pancreatic insufficiency• N-benzoyl-l-tyrosyl-PABA is cleaved by
chymotrypsin to form PABA. • PABA is absorbed from the small intestine
excreted in the urine• One gram of BT-PABA in 300 mL of water is
given orally, and urine collections are obtained for 6 hours.
• Patients with chronic pancreatitis excrete less than 60% of the ingested dose of BT-PABA.

Embryology of Pancreas

Embryology• Endodermal in origin• Develops from ventral and dorsal
pancreatic buds• Ventral bud rotates posteriorly and
becomes the uncinate process and inferior head of pancreas
• Dorsal bud becomes superior head, neck, body and tail
• Ventral bud duct fuses with dorsal bud duct to become main pancreatic duct (Wirsung)

-

---

Annular PancreasAnnular pancreas is a rare condition in
which the second part of the duodenum is surrounded by a ring of pancreatic tissue continuous with the head of the pancreas. This portion of the pancreas can constrict the duodenum and block or impair the flow of food to the rest of the intestines.
It is estimated to occur in 1 out of 12,000 to 15,000 newborns.
The ambiguity arises from the fact that not all cases are symptomatic

-

Classification• Annular pancreas can be either 'complete' or
'incomplete'.• Complete annular pancreas is the condition
when pancreatic parenchyma or annular duct is seen to completely surround the 2nd part of duodenum.
• Incomplete annular pancreas is a condition where the annulus does not surround the duodenum completely, giving a 'crocodile jaw' appearance1

Embryology• The pancreas develops from a single dorsal and two ventral buds,
which appear as outgrowths of primitive foregut at 5 weeks of gestation.
• Ventral buds fuse rapidly.• In 7th week of gestation, duodenum expands, and rotates the ventral
bud from right to left, and causes fusion with dorsal bud. • THe ventral bud forms the inferior part of uncinate process and
inferior head of pancreas while the dorsal bud gives rise to tail and body of pancreas.
• Annular pancreas develops due to failure of ventral bud to rotate with duodenum, causing encasement of duodenum.

Annular pancreas associated with
• annular pancreas is associated with other congenital disorders, including:
• Down syndrome• tracheoesophageal fistula—an abnormal
connection (fistula) between the esophagus and the trachea
• intestinal atresia—the failure of a portion of the intestinal tract to completely form
• pancreas divisum—birth defect in which ducts of the pancreas fail to join together

Presentation• Prenatal • Maternal polyhydroamniosChildren/neonates (usually present in neonates)• bilious vomiting ( due to severe duodenal obstruction)• Feeding difficulties• upper abdominal distentionAdults
Approximately 50% of the patients may be asymptomatic for life, anomaly discovered incidentally
• When symptomatic, presentation is usually in third to sixth decade with 1)abdominal pain 2) postprandial fullness and vomiting resulting from gastric outlet obstruction 3) pancreatitis, 4)PUD,5) obstructive jaundice ,6) upper gastrointestinal bleeding from peptic ulceration,

DIAGNOSIS
Postnatal diagnostic procedures include • abdominal x-ray (Dilated stomach and
dilated duodenum i.e.), (double bubble sign).
• ultrasound,• CT scan, and • upper GI and small bowel series.

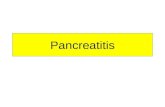
Double bubble sign• Radiographic views of the abdomen
revealed 2 gas bubbles in the upper abdomen with an absence of bowel gas distally .
• The "double-bubble" sign represents dilatation of the stomach in the left upper quadrant and the proximal duodenum in the right upper quadrant.

Double bubble sign

Treatment • surgery to bypass the pancreatic tissue. • The goal of treatment is to remove the
obstruction so that small intestine can function normally.
• Typically, the pancreatic tissue cannot be removed from the duodenum.
• Destruction of the pancreatic tissue can cause damage to the pancreas.

Treatment
• Surgical options for annular pancreas include gastrojejunostomy or duodenojejunostomy.
• These procedures will require to cut the intestine at the site of the blockage and reconnect the two parts of the intestine in an area below the obstruction.

Operative Technique

Operative Technique

Operative Technique

Pancreatic divisum
• Pancreas or Pancreatic divisum is a congenital anomaly in the anatomy of the ducts of the pancreas in which a single pancreatic duct is not formed, but rather remains as two distinct dorsal and ventral ducts
• Occurs in approximately 10% of embryos

-

-

Symptoms• A majority of individuals born with pancreas divisum will
not have symptoms. • In some cases, pancreas divisum is only detected during
autopsy. • A small group of individuals will develop symptoms which
commonly include• abdominal pain, • nausea, • vomiting, and • chronic pancreatitis.

Diagnosis
• The most common and accurate way of diagnosing an individual with this anomaly is by an MRCP or ERCP.
• This test can demonstrate the presence of two separately draining ducts within the pancreas.
• Other tests diagnosis with, such as a CT scan and an MRI.

treatmentPancreas divisum in individuals with no symptoms
does not require treatment. Treatment of those with symptoms varies and has
not been well established. A surgeon may attempt a sphincterotomy by
cutting the minor papilla to enlarge the opening and allow pancreatic enzymes to flow normally. During surgery, a stent may be inserted into the duct to ensure that the duct will not close causing a blockage.

Ectopic pancreasIs where pancreatic tissue has grown outside
its normal location and without vascular or other anatomical connections to the pancreas.
It is a congenital diseaseAlso known as heterotopic, accessory, or
aberrant pancreas.[

-Pancreas hyperplasiaPathologic hyperplasia of various pancreatic endocrine cells is rare but has been long -known. β cell hyperplasia contributes to persistent hyperinsulinemic hypoglycemia of infancy, which is commonly caused by mutations in the islet ATP-sensitive
potassium channel, and to non-insulinoma pancreatogenous hypoglycemia in adults, which may or may not be associated with bariatric surgery. α cell hyperplasia may cause glucagonoma syndrome or induce pancreatic
neuroendocrine tumors. An inactivating mutation of the glucagon receptor causes α cell
hyperplasia and asymptomatic hyperglucagonemia.

MCQ
• Most common site of ectopic pancreatic tissue is
• Stomach• Jejunum• Appendix• Hilum of spleen

MCQ
2. Dorsal bud of developing pancreas forms all of the following structures except -
• Body• Upper part of head of pancreas• Lower part of head of pancreas• Tail

MCQ
3.Treatment of choice for annular pancreas is-
• Gastro jejunostomy• Pancreatectomy• Whipple's procedure• Duodeno duodenostomy