Conferencia - Taller Insulinas en atención primaria
30
Taller de insulinas: De la teoría a la práctica Dra. Lina P Pradilla S MD Internista - endocrinóloga Presidente Capítulo Nororiental ACE Profesora Medicina Interna UIS Bucaramanga, Noviembre 2015
-
Upload
lina-patricia-pradilla -
Category
Health & Medicine
-
view
612 -
download
3
Transcript of Conferencia - Taller Insulinas en atención primaria

Taller de insulinas: De la teoría a la práctica
Dra. Lina P Pradilla S MD Internista - endocrinóloga
Presidente Capítulo Nororiental ACE Profesora Medicina Interna UIS Bucaramanga, Noviembre 2015

Conflicto de intereses•Conferencista:
•Eli-Lilly •Novonordisk •Sanofi-Aventis
•Educación Médica continuada: •Eli-Lilly •Merck Serono •Novonordisk
•Investigación: MSD, Novonordisk
Agenda• Guías actuales de manejo
• Casos clínicos
• Insulina basal
• Agregando ultrarrápida
• Intensificando insulina
• Conclusiones
• P&R

¿De qué disponemos?
NPH DETEMIR GLARGINA DEGLUDEC
Insulina BasalPOS NO POS
Insulina Prandial
CRISTALINA ASPART LISPRO
POS
GLULISINA

Guías actuales de manejo• Disponemos de al menos 3 guías conocidas por la
mayoría de los médicos
• ADA= el cuadrado
• AACE= azul
• ALAD= según glicosilada
• ¿Cuál usan en su institución?

iDPP4

or punishment. Equipping patients withan algorithm for self-titration of insulindoses based on self-monitoring of bloodglucose (SMBG) improves glycemic con-trol in type 2 diabetic patients initiatinginsulin (18).Basal insulin alone is the most conve-
nient initial insulin regimen, beginningat 10 U or 0.1–0.2 U/kg, depending onthe degree of hyperglycemia. Basal in-sulin is usually prescribed in conjunctionwith metformin and possibly one addi-tional noninsulin agent. If basal insulinhas been titrated to an acceptable fast-ing blood glucose level, but A1C remainsabove target, consider advancing to
combination injectable therapy (Fig. 7.2)to cover postprandial glucose excur-sions. Options include adding a GLP-1receptor agonist or mealtime insulin,consisting of one to three injections ofrapid-acting insulin analog (lispro, as-part, or glulisine) administered just be-fore eating. A less studied alternative,transitioning from basal insulin totwice-daily premixed (or biphasic) insu-lin analog (70/30 aspart mix, 75/25or 50/50 lispro mix), could also be con-sidered. Regular human insulin andhuman NPH-Regular premixed formula-tions (70/30) are less costly alternativesto rapid-acting insulin analogs and
premixed insulin analogs, respectively,but their pharmacodynamic profilesmake them suboptimal for the coverageof postprandial glucose excursions. Aless commonly used and more costlyalternative to “basal–bolus” therapywith multiple daily injections is CSII(insulin pump). In addition to the sug-gestions provided for determiningthe starting dose of mealtime insulinunder a basal–bolus regimen, anothermethod consists of adding up the totalcurrent insulin dose and then providingone-half of this amount as basal andone-half as mealtime insulin, the lattersplit evenly between three meals.
Figure 7.1—Antihyperglycemic therapy in type 2 diabetes: general recommendations (15). The order in the chart was determined by historicalavailability and the route of administration, with injectables to the right; it is not meant to denote any specific preference. Potential sequences ofantihyperglycemic therapy for patients with type 2 diabetes are displayed, with the usual transition moving vertically from top to bottom (althoughhorizontal movement within therapy stages is also possible, depending on the circumstances). DPP-4-i, DPP-4 inhibitor; fxs, fractures; GI, gastro-intestinal; GLP-1-RA, GLP-1 receptor agonist; GU, genitourinary; HF, heart failure; Hypo, hypoglycemia; SGLT2-i, SGLT2 inhibitor; SU, sulfonylurea;TZD, thiazolidinedione. *See ref. 15 for description of efficacy categorization. †Consider starting at this stage when A1C is$9%. ‡Consider starting atthis stage when blood glucose is$300–350 mg/dL (16.7–19.4 mmol/L) and/or A1C is$10–12%, especially if symptomatic or catabolic features arepresent, in which case basal insulin 1 mealtime insulin is the preferred initial regimen. §Usually a basal insulin (NPH, glargine, detemir, degludec).Adapted with permission from Inzucchi et al. (15).
care.diabetesjournals.org Position Statement S43



Iniciar'insulina'basal'(insulina'de'larga'acción)'
A1c$<8%$
Dosis%total%diaria%0.1.0.2U/Kg%
Titulación*de*insulina*c/203*días*para*alcanzar*la*meta:"# Régimen"fijo:"Aumente"2"UI"# Régimen"ajustable:"
# GA">180:"Aumente"4UI"# GA"140#180:"Aumente"2"UI"# GA"110#139:"Aumente"1"UI"
Si"hay"hipoglucemia"reduzca"la"dosis:"# <70mg/dl:"10#20%"# <40mg/dl:"20#40%"
A1c$>8%$
Dosis%total%diaria%0.2.0.3U/Kg%
Si#no#alcanza#la#meta:#INTENSIFIQUE#
Considere)suspender)o)reducir)sulfonilurea)cuando)inicia)insulina)basal.)Metas:)A1c)<7%)para)la)mayoría)de)pacientes)y)GA)y)preprandiales)<110mg/dl,))sin)hipoglucemia.)Ajuste)por)edad)del)pac,)Dempo)de)evolución,)comorbilidades,)complicaciones)de)DM)y)riesgo)de)hipoglucemia)

Ajustes de la basal: en ensayos clínicos
• Aumentos diarios de 1UI cada día hasta llegar a la meta.
• Si está muy lejos de la meta, se puede aumentar 2UI al día.
• Aumentos cada 3 días de 2UI según el promedio o la mediana

� Aumentar según el PROMEDIO de los últimos 3 días � Ej. 100-120-180 = 133mg/dl
� Una alternativa es usar la MEDIANA � Ej. 120
� El valor en que se aumenta la dosis de insulina puede ser fijo (generalmente 2-3 UI) o variable según lo lejos que esté de la meta

Si#no#alcanza#la#m
eta:#
INTENSIFIQUE#
Intensificar+(control+prandial)+
Agregue&&RA&GLP+1&o&SGLT+2&o&Inh&DPP+IV& Agregue&insulina&prandial&
Dosis%total%diaria%0.3.0.5%U/Kg%%50%%Análogo%basal%
50%%Análoga%prandial%Menos%deseables:%NPH,%regular%o%premezclas%
Titulación*de*insulina*cada*2/3*días*para*alcanzar*la*meta*glucémica,*así:*• Incremente*DTD*como*sigue:*
• Régimen*fijo:*Aumente*2UI*la*DTD*• Régimen*ajustable:*
*GA>180mg/dl:*Agregue*4UI**GA*140/180mg/dl:*Agregue*2*UI**GA*100/139mg/dl:*Agregue*1*UI*
• Incremente*la*dosis*prandial*10%*para*cualquier*comida*si*la*GLC*2h/post*o*la*siguiente*precomida*es*>180mg/dl*• Premezcla:*Aumente*DTD*10%*si*la*GLC*>180*en*ayunas*o*precomidas*• Si*hay*hipoglucemia*de*ayuno,*reduzca*dosis*basal*• Si*hay*hipoglucemia*nocturna,*reduzca*basal*y*/o*insulina*rápida*precomida*o*presnack*nocturno*• Si*hay*hipoglucemia*entre*comidas*en*el*día,*reduzca*insulina*ultrarápida*precomida*

Ajustes de análogas rápidas al momento de cada comida Momento de aplicación
Cuándo controlar?
Glucometría (mg/dl)
Cambio de dosis
Cada cuánto ajustar?
Desayuno Antes de almuerzo
<80 80-130 >131
- 2 UI 0
+ 2UI
Cada 3 a 5 días
Almuerzo Antes de comida
<80 80-130 >131
- 2UI 0
+ 2UI
Cada 3 a 5 días
Cena Antes de ir a dormir
<125 125-150
>150
-2UI 0
+2UI
Cada 3 a 5 días

CAMBIOS EN ESTILO DE VIDA + METFORMINA + OTROS ADOS
INSULINA LENTA + ADOS= BASAL
INSULINA BASAL + ADOS (NO SU) + INSULINA ULTRARRAPIDA UNA DOSIS
(BASAL PLUS)
INSULINA BASAL + ADOS (NO SU) + ULTARRAPIDA 3 DOSIS
(BASAL BOLO O INTENSIVO)
DETERIORO DE CELULA BETA
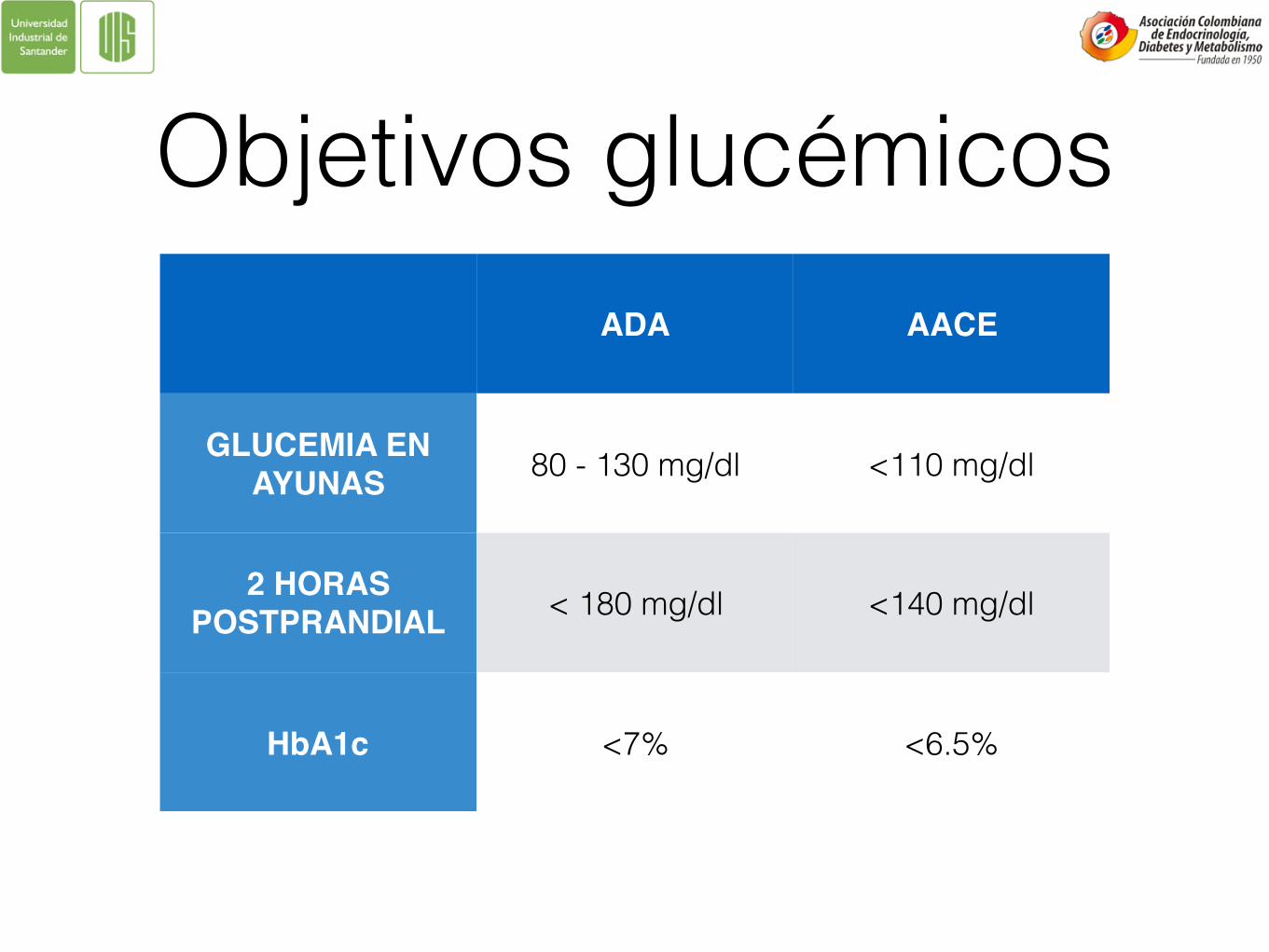
Objetivos glucémicosADA AACE
GLUCEMIA EN AYUNAS 80 - 130 mg/dl <110 mg/dl
2 HORAS POSTPRANDIAL < 180 mg/dl <140 mg/dl
HbA1c <7% <6.5%


Caso clínico No.1: Insulina Basal

• Mujer de 55 años, con HTA hace 3 años, diagnóstico de DM2 hace 5 años. Recibe actualmente GLB 5*2, MTF 850*3 y usa productos naturales para “el azúcar”. Además toma losartan 50*2 y atorvastatina 20*1. Dice hacer dieta y caminar 30 min 2v/sem.
• Al ExF Peso 75kg, IMC 31.2kg/m2, PA 132/80, cintura 94cm. No datos de complicaciones crónicas de la DM.
• Laboratorios: GLC pre y post= 198 y 234mg/dl, respectivamente. HbA1c=9.2%. Función renal y hepática normales.
Propuestas caso 1


Glucometrías post inicio de insulina basal
• Ayunas= 190- 175- 90- 153- 186- 138- 157mg/dl
• Prealmuerzo= 256 - 210 - 150mg/dl.
• Precomida= 194 - 190 - 186mg/dl.

Propuestas de ajustes a la basal…

Caso clínico No. 2: Iniciando ultrarrápida

• Hombre 66 años, DM2 hace 12 años, manejado desde hace 4 años con insulina. Tratamiento actual NPH 30-0-0-10, glibenclamida 5*4 y MTF 850*1. No falla renal, no alteración hepática. No complicaciones crónicas reconocidas en el seguimiento. Mal seguimiento de dieta. Caminata diaria 1-2 horas, incluido fin de semana.
• Al ExF: Peso 65Kg, IMC 28,4kg/m2, PA 126/74, cintura 92cm.
• Laboratorios: Glc pre 210 post 314mg/dl, HbA1c 10.2%, glucometrías en ayunas entre 176 y hasta >400mg/dl. Las hace ocasionalmente. Creatinina 1.4mg/dl.

Propuestas caso 2

• A pesar del cambio hecho presenta en control a los 3 meses: glicemia pre 160 postdesayuno 280mg/dl, HbA1c 9.4%.
• Glucometrías en ayunas entre 90 y 174mg/dl, nocturnas entre 234 y 350mg/dl

Conclusiones• Iniciar insulina no es la solución: requiere ajuste.
• Elección del candidato a ajuste.
• Todo esquema funciona: escoja uno y familiarícese con él.
• Las guías son eso: GUÍAS. Lo mejor es individualizar la terapia.