Controversias en DM2. Actualización de enero de 2015
44
Controversias en el tratamiento de la DM2 por Carlos Fernández Oropesa se distribuye bajo una Licencia Creative Commons Atribución-NoComercial-CompartirIgual 4.0 Internacional.
-
Upload
carlos-fernandez-oropesa -
Category
Health & Medicine
-
view
758 -
download
1
Transcript of Controversias en DM2. Actualización de enero de 2015

Con
trov
ers
ias
en
el t
rata
mie
nto
de la
DM
2 p
or C
arlo
s F
ern
ánd
ez O
rope
sa s
e d
istr
ibu
ye b
ajo
una
Li
cen
cia
Cre
ativ
e C
om
mo
ns A
trib
uci
ón-
No
Co
me
rcia
l-C
om
par
tirIg
ual 4
.0 I
nter
naci
onal
.




13 noviembre 2014
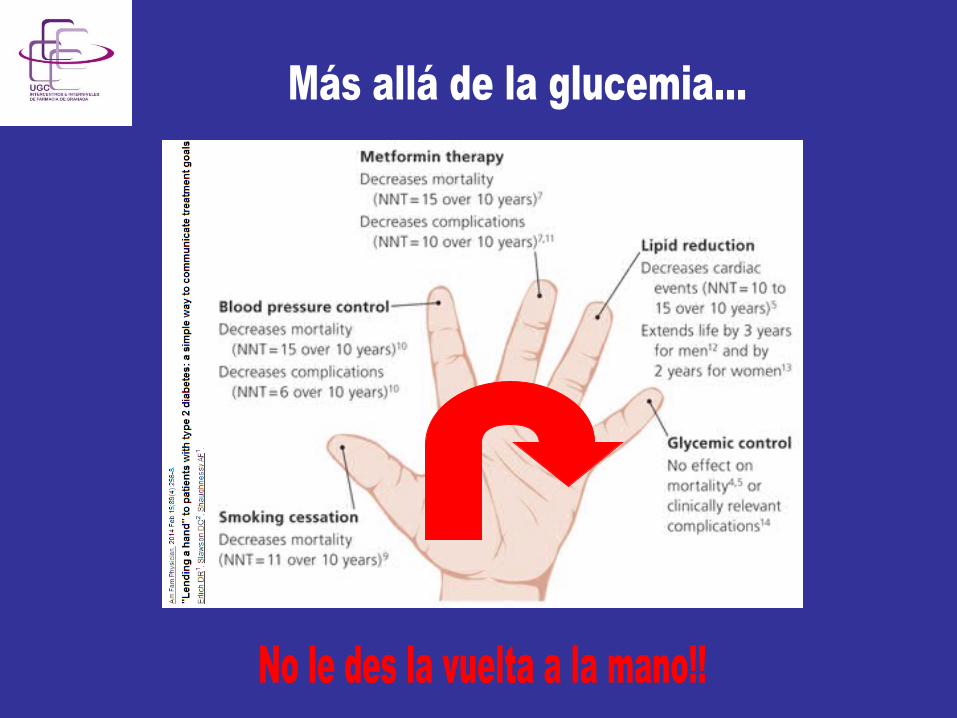

- Abordaje multifactorial y multidisciplinar
- Huir de la perspectiva glucocéntrica
- La base del tratamiento es NO farmacológica
- Paciente empoderado – ¿paciente maduro?



















Verás tú que de las gliptinas no va a decir ná…





Management of Hyperglycemia in Type 2 Diabetes, 2015:
A Patient-Centered ApproachUpdate to a Position Statement of the American Diabetes Association (ADA)
and the European Association for the Study of Diabetes (EASD)
Diabetes Care 2015;38:140–149Diabetologia 2015;10.1077/s00125-014-3460-0

Healthy eating, weight control, increased physical activity & diabetes education
Metformin high low risk neutral/loss GI / lactic acidosis low
If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (order not meant to denote any specific preference - choice dependent on a variety of patient- & disease-specific factors):
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
high low risk gain edema, HF, fxs
low
Thiazolidine- dione
intermediate low risk neutral rare
high
DPP-4 inhibitor
highest high risk gain hypoglycemia variable
Insulin (basal)
Metformin +
Metformin +
Metformin +
Metformin +
Metformin +
Basal Insulin +
Sulfonylurea
+ TZD
DPP-4-i
GLP-1-RA
Insulin§
or
or
or
or
Thiazolidine-dione +
SU
DPP-4-i
GLP-1-RA
Insulin§
TZD
DPP-4-i
GLP-1-RA
high low risk loss GI
high
GLP-1 receptor agonist
Sulfonylurea
high moderate risk gain hypoglycemia low
SGLT2 inhibitor intermediate low risk loss GU, dehydration high
SU
TZD
Insulin§
GLP-1 receptor agonist +
SGLT-2 Inhibitor +
SU
TZD
Insulin§
Metformin +
Metformin +
or
or
or
or
SGLT2-i
or
or
or
SGLT2-i
Mono- therapy
Efficacy* Hypo risk Weight Side effects Costs
Dual therapy†
Efficacy* Hypo risk Weight Side effects Costs
Triple therapy
or
or
DPP-4 Inhibitor +
SU
TZD
Insulin§
SGLT2-i
or
or
or
SGLT2-i
or
DPP-4-i
If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (order not meant to denote any specific preference - choice dependent on a variety of patient- & disease-specific factors):
If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on oral combination, move to injectables, (2) on GLP-1 RA, add basal insulin, or (3) on optimally titrated basal insulin, add GLP-1-RA or mealtime insulin. In refractory patients consider adding TZD or SGL T2-i:
Metformin +
Combination injectable therapy‡
GLP-1-RA Mealtime Insulin
HbA1c≥9%
Me orminintolerance or
contraindica on
Uncontrolledhyperglycemia
(catabolicfeatures,BG≥300-350mg/ dl,HbA1c≥10-12%)
Insulin (basal)
+
or
or
or
Diabetes Care 2015;38:140-149; Diabetologia 2015;10.1077/s00125-014-3460-0







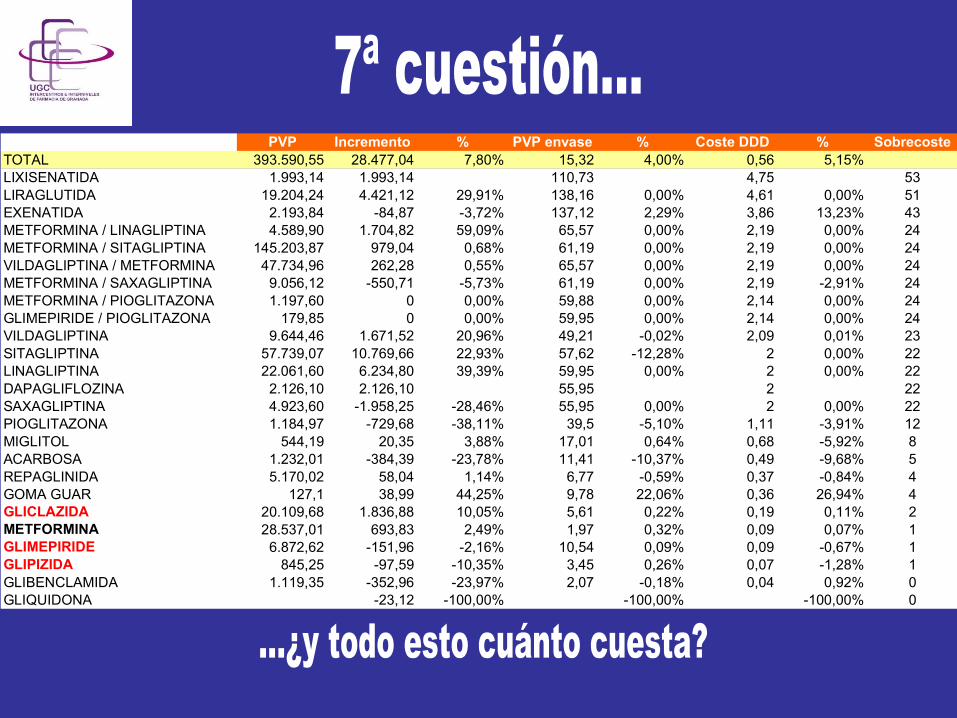
PVP Incremento % PVP envase % Coste DDD % SobrecosteTOTAL 393.590,55 28.477,04 7,80% 15,32 4,00% 0,56 5,15%LIXISENATIDA 1.993,14 1.993,14 110,73 4,75 53LIRAGLUTIDA 19.204,24 4.421,12 29,91% 138,16 0,00% 4,61 0,00% 51EXENATIDA 2.193,84 -84,87 -3,72% 137,12 2,29% 3,86 13,23% 43METFORMINA / LINAGLIPTINA 4.589,90 1.704,82 59,09% 65,57 0,00% 2,19 0,00% 24METFORMINA / SITAGLIPTINA 145.203,87 979,04 0,68% 61,19 0,00% 2,19 0,00% 24VILDAGLIPTINA / METFORMINA 47.734,96 262,28 0,55% 65,57 0,00% 2,19 0,00% 24METFORMINA / SAXAGLIPTINA 9.056,12 -550,71 -5,73% 61,19 0,00% 2,19 -2,91% 24METFORMINA / PIOGLITAZONA 1.197,60 0 0,00% 59,88 0,00% 2,14 0,00% 24GLIMEPIRIDE / PIOGLITAZONA 179,85 0 0,00% 59,95 0,00% 2,14 0,00% 24VILDAGLIPTINA 9.644,46 1.671,52 20,96% 49,21 -0,02% 2,09 0,01% 23SITAGLIPTINA 57.739,07 10.769,66 22,93% 57,62 -12,28% 2 0,00% 22LINAGLIPTINA 22.061,60 6.234,80 39,39% 59,95 0,00% 2 0,00% 22DAPAGLIFLOZINA 2.126,10 2.126,10 55,95 2 22SAXAGLIPTINA 4.923,60 -1.958,25 -28,46% 55,95 0,00% 2 0,00% 22PIOGLITAZONA 1.184,97 -729,68 -38,11% 39,5 -5,10% 1,11 -3,91% 12MIGLITOL 544,19 20,35 3,88% 17,01 0,64% 0,68 -5,92% 8ACARBOSA 1.232,01 -384,39 -23,78% 11,41 -10,37% 0,49 -9,68% 5REPAGLINIDA 5.170,02 58,04 1,14% 6,77 -0,59% 0,37 -0,84% 4GOMA GUAR 127,1 38,99 44,25% 9,78 22,06% 0,36 26,94% 4GLICLAZIDA 20.109,68 1.836,88 10,05% 5,61 0,22% 0,19 0,11% 2METFORMINA 28.537,01 693,83 2,49% 1,97 0,32% 0,09 0,07% 1GLIMEPIRIDE 6.872,62 -151,96 -2,16% 10,54 0,09% 0,09 -0,67% 1GLIPIZIDA 845,25 -97,59 -10,35% 3,45 0,26% 0,07 -1,28% 1GLIBENCLAMIDA 1.119,35 -352,96 -23,97% 2,07 -0,18% 0,04 0,92% 0GLIQUIDONA -23,12 -100,00% -100,00% -100,00% 0

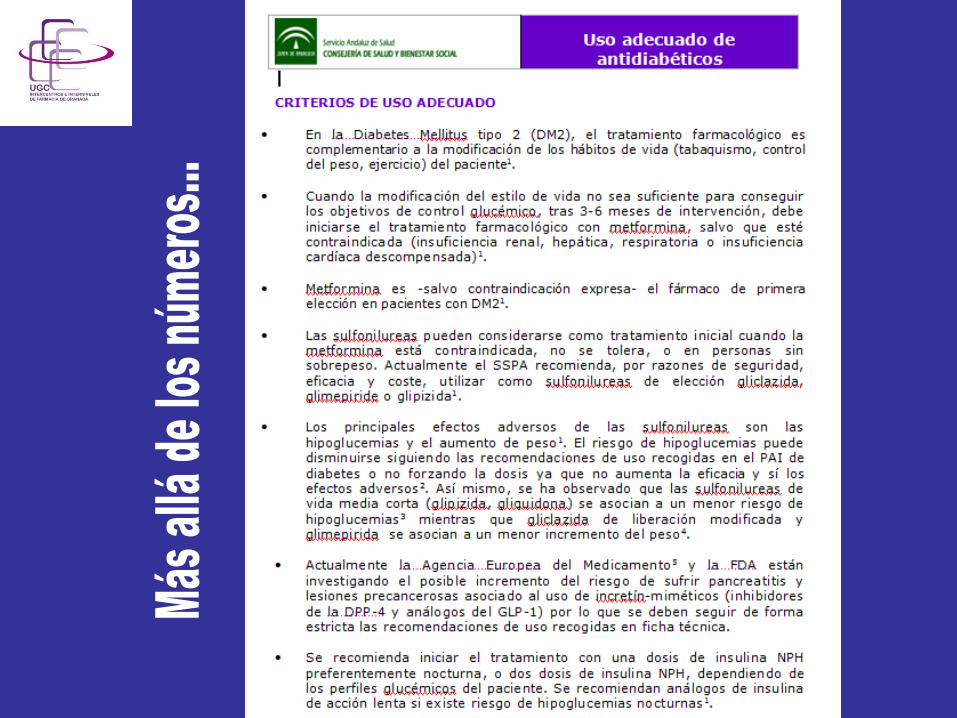
1.- Las SU constituyen un grupo heterogéneo de fármacos entre los que hay diferencias importantes de seguridad, no así de eficacia. Las más seguras son gliclazida, glimepiride y gliquidona.
2.- De forma general, su lugar en la terapéutica, por razones de seguridad, eficacia y coste es la 2ª línea de tto, asociadas a metformina.
3.- No obstante lo anterior, existe un perfil idóneo de paciente candidato al tto con SU. Y un perfil de paciente no candidato al tto con SU, sobre todo con glibenclamida, cuyo uso actualmente no se recomienda.
4.- En los últimos años se han magnificado, posiblemente de forma interesada, los efectos adversos de las SU. La incidencia y la gravedad, son bajas, aunque hay que gestionar de forma adecuada los riesgos.
5.- Las incretinas y los inhibidores del cotransportador sodio-glucosa, por los mismos motivos (no han demostrado utilidad en variables de resultado orientadas al paciente, su reciente comercialización y su precio) quedan relegados a la 3ª línea de tto o a la 2ª en pacientes que no puedan/deban tomar SU.
6.- A la vista de las últimas evidencias, las recomendaciones del PAI de diabetes continúan siendo vigentes.