Clase Isquemia Arterial Aguda

of 18
Transcript of Clase Isquemia Arterial Aguda
-
8/18/2019 Clase Isquemia Arterial Aguda
1/18
-
8/18/2019 Clase Isquemia Arterial Aguda
2/18
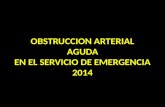
Figure 66-1 Chronic superfcial emoral artery occlusion. Numerous collateralchannels prevent the occurrence o acute ischemia despite a total occlusion.
PATHOPHYSIOLOGY
Acute limb ischemia may occur as the result o embolization or in-situ
thrombosis ( Table 66– !. "mboli ori#inate rom the heart in more than $%& o
cases') and normally lod#e at the site o an arterial biurcation ( *i#. 66– ! such
as the distal common emoral or popliteal arteries. The decreasin# prevalence
o rheumatic heart disease underlies a diminishin# proportion o embolic versus
thrombotic causes or acute limb ischemia. +hen embolization occurs, it
usually does soin the setting of atrial fibrillation or acute myocardial infarction, when
portions of atrial or ventricular mural thrombus detach and embolie to the arterial tree! t isoften difficult to distinguish embolus from thrombosis, but embolic occlusions should be
suspected in patients with the following features6 (- acute onset where the patient is often
able to accurately time the moment of the event% (2- prior history of embolism% (7- nown
embolic source, such as cardiac arrhythmias% (3- no prior history of intermittent
claudication% and (5- normal pulse and 8oppler examination in the unaffected limb!
#hrombosis as an etiology for acute limb ischemia is a much more diverse category than
emboliation! 9ith the increased use of peripheral arterial bypass grafts for chronic limbischemia, and noting the finite patency rate of any bypass graft conduit, it is not surprising
that acute graft occlusion is now the most freuent cause of acute lower extremity ischemiain most centers ( )ig! **+7 -! :; "ymptoms may be less dramatic than embolic occlusion,depending on the extent of collateral flow across the site of occlusion! n addition to the
presence of collateral channels, the location of the occlusion may also play a critical role in
the severity of limb ischemia! )or example, occlusion of the popliteal artery results in profound limb ischemia, since it is the only artery crossing at the level of the nee ( )ig!
**+3 -!
-
8/18/2019 Clase Isquemia Arterial Aguda
3/18
-
8/18/2019 Clase Isquemia Arterial Aguda
4/18
-
8/18/2019 Clase Isquemia Arterial Aguda
5/18
rrespective of the etiology of ischemia, the end result is the build'up of toxic byproducts
within the ischemic tissue bed! #hese toxins include the free radicals, which are oxygen'
derived, chemically reactive molecules that are responsible for the inGury that occurs afterischemia and reperfusion! schemia induces leaage of protein and fluid from the capillary
bed, resulting in tissue edema!:5; Hydrodynamic pressure in the extravascular space rises to a
level that competes with venous outflow, perpetuating a vicious cycle that can eventually
impede arterial inflow! $t first, this process occurs at a microscopic level, but it may progress to the development of high tissue pressures at a regional level and the clinical
entity nown as the compartment syndrome! #he development of a compartment syndrome
is hastened by the abrupt reperfusion of a previously ischemic tissue bed, a phenomenonthat explains the relatively freuent need for fasciotomy after lower extremity surgical
revasculariation for severe limb ischemia! :*;
reveals the absence of palpable pulses, and the location of the pulse deficit allows one to
predict the site of arterial occlusion! #he .5 &s/ have been used as a mnemonic toremember the presentation of a patient with acute limb ischemia1 paresthesia, pain, pallor,
pulselessness, and paralysis! n some cases, a sixth & is added1 poiilothermia, meaning
euilibration of the temperature of the limb to that of the ambient environment (coolness-!#he process is sometimes confused with deep venous thrombosis by an inexperienced
observer! $lthough a deep venous thrombosis may manifest as limb ischemia when severe
(phlegmasia cerulea dolens-, profound lower extremity edema is uncommon in pure arterialischemia! =ccasionally, a patient with arterial ischemia and pain at rest eeps the extremity
in a dependent position and edema may develop% such a scenario may be apparent if an
adeuate history is obtained ( )ig! **+5 -! &ain may either be constant or elicited by passivemovement of the involved extremity! History should include a description of the duration,
-
8/18/2019 Clase Isquemia Arterial Aguda
6/18
location, intensity, and suddenness of the onset of pain and change over time! Embolic
occlusions are usually uite sudden and of great intensity, such that patients often presentwithin a few hours of onset! #he past history should state whether or not the patient has a
history of intermittent claudication, previous leg bypass or other vascular procedures, and
history suggestive of embolic sources such as cardiac arrhythmias and aortic aneurysms!
Ieneral atherosclerotic ris factors (smoing, hypertension, diabetes, hyperlipidemia,family history of cardiac or vascular events- should be recorded because these can be
predictors of periprocedural mortality!
n an effort to classify the extent of acute ischemia for standardiation reporting of
outcome, the "ociety for Jascular "urgeryKnternational "ociety for Cardiovascular "urgery
("J"K"CJ"- (now "J"- ad hoc committee was established and published what has now
come to be nown as the Rutherford criteria, after 8r! obert utherford, the lead author of
the article!:@; #he following three classes were defined6
Class 6 the limb is viable and remains so even without therapeutic intervention!
Class 26 the limbs are threatened and reuire revasculariation for salvage!
Class 76 those limbs that are irreversibly ischemic and infarction has developedsuch that salvage is not possible!
Figure 66-4 Acute in-situ thrombotic occlusion o the popliteal artery. Note theabsence o si#nifcant collateral channels. The patient had no oppler pedalsi#nals.
-
8/18/2019 Clase Isquemia Arterial Aguda
7/18
Figure 66-5 ependent edema and ischemic blisters seen in a patient ithacute limb ischemia.
The initial or/ o the reportin# standards committee as revisedseveral years later, dividin# the middle cate#ory into two subclassifications6 class
2$ for limbs that are not immediately threatened and class 2< for those limbs that are
severely threatened to the point where urgent revasculariation is necessary for salvage!:A;
$s examples, a patient with a palpable femoral pulse but an absent popliteal pulse is liely
to have a superficial femoral artery occlusion! $bsence of a femoral pulse signifies disease
-
8/18/2019 Clase Isquemia Arterial Aguda
8/18
-
8/18/2019 Clase Isquemia Arterial Aguda
9/18
popliteal or anle pulses below, whereas patients with aortoiliac disease have absent
femoral pulses as well! 8oppler segmental pressures are also useful in defining the level ofinvolvement% a drop in pressure of 70 mm Hg or more between two segments predicts
arterial occlusion between the two levels!:7; )or example, a superficial femoral arterial
occlusion would be suggested in a patient with a systolic pressure of 20 mm Hg at the
proximal thigh pressure cuff and ?0 mm Hg at the above'nee cuff!
Contrast arteriography remains the gold standard with which all other tests must be
compared! Even today, standard arteriography is the most accurate test for all but the
occasional patient with such slow flow in the tibial or foot vessels that digital subtractionimaging fails to demonstrate a patent artery! $rteriography is, however, a semi'invasive
modality, and as such its use should be confined to those patients for whom a surgical or
percutaneous intervention is contemplated! &atients with borderline renal function mayexperience contrast'induced nephrotoxicity, and in this subgroup the use of alternate
contrast agents such as gadolinium and carbon dioxide have been employed! :3; :5;
8uplex ultrasound has been used in some centers to define the anatomic extent of peripheral arterial disease!:*; $lthough duplex has been useful in documenting the patencyof a single arterial segment such as a stented superficial femoral artery or a bypass graft,
evaluation of the entire lower extremity arterial tree remains imprecise, and its adeuacy as
the sole diagnostic modality for planning a percutaneous or open surgical intervention
remains controversial! Pagnetic resonance (P- angiography is being used with greaterfreuency in patients with peripheral arterial disease! :@; Nsing gadolinium as an P contrast
agent, the specificity and sensitivity of the test exceed that of duplex ultrasonography and
approach the accuracy of standard arteriography! P angiography has been effective indemonstrating patent tibial arteries undetected with less sensitive conventional
arteriography, identifying potential target vessels for an otherwise unfeasible lower
extremity reconstructive bypass procedure! #oday, P angiography is widely employed in patients with chronic renal insufficiency to limit the dye load! $nother noninvasive imaging
modality, computed tomographic (C#- angiography, is gaining appeal as a means of
delineating anatomy to provide a means of localiing the extent and severity of occlusivedisease!:A; 9ith future improvements in hardware and software technology, it is liely that
P and C# angiography will effectively replace conventional diagnostic arteriography, and
arterial cannulation will be reserved solely for percutaneous interventional therapies!
TREATMENT
Nnlie the situation in patients with chronic limb ischemia where observation alone is a
common and uite appropriate treatment option, patients presenting with acute limbischemia often reuire revasculariation to salvage the leg! n fact, this is why they present
acutely and are often able to identify the precise time of the occlusive event, similar to the
manner that a patient with a perforated peptic ulcer nows exactly when it occurred! n
many cases, the paucity of preexisting collateral channels renders the limb very ischemic
-
8/18/2019 Clase Isquemia Arterial Aguda
10/18
after thrombotic or embolic occlusion of the main arterial segment! "ymptoms occur with
severity and rapidity, forcing the patient to see treatment almost immediately!
=nce the diagnosis is made, adeuate systemic anticoagulation is instituted! $ bolus ofunfractionated heparin is standard, followed by a continuous infusion to maintain the
activated partial thromboplastin time (a#- in a therapeutic range! #he goal ofanticoagulation is twofold6 (- to decrease the ris of thrombus propagation and (2- in thecase of presumed embolic occlusion, to prevent recurrent emboliation! =ccasionally, if
early angiographic evaluation is feasible, hepariniation can be withheld, pending the
establishment of arterial access! =therwise, a micropuncture techniue (small localiingneedle :2 gauge;, guide wire :0!0A inch;, and a 3')rench sheath- is used to gain access or
the anticoagulation is withheld to allow the a# to fall to within !5 times control!
#he severity of the ischemic limb based on the earlier'mentioned utherford classification
dictates the extent of diagnostic tests performed for systemic ris factor assessment!outine blood studies and coagulation tests should be drawn before heparin is
administered! Correction of underlying electrolyte imbalances and systemic anticoagulationshould proceed concomitant with the other investigations! $ plain chest radiograph andelectrocardiogram should be obtained in every patient! n patients with suspected
embolism, an echocardiogram should be obtained as soon as time allows! 8espite the desire
for a complete worup, the treatment of an ischemic limb must tae priority over other
more complex and time'consuming investigations!
Nnfortunately, the threat is not only to the limb, but these patients are also at a high ris for
death! Limb hypoperfusion results in systemic acid'base and electrolyte abnormalities that
impair cardiopulmonary and renal function! "uccessful reperfusion may result in the releaseof highly toxic free radicals further compromising these critically ill patients! #herapeutic
choices are often few, and patient expectations are not always realistic! #he management of
acute limb ischemia reuires a thorough understanding of the anatomy of the arterial
occlusion and the open surgical and percutaneous options for restoring limb perfusion!
#here exist several basic therapeutic options to pursue in patients with acute limb ischemia
( )ig! **+* -!
0. The frst option is anticoa#ulation alone. 1 the ischemia isnonthreatenin# (e.#., 2utherord class 0 or A!, such a nona##ressivecourse may be appropriate. An#io#raphic evaluation and electiverevascularization may then be underta/en ater the patient has beenully prepared and other co-morbidities such as concurrent coronary
artery disease have been addressed.. 3atients ho present ith more severe ischemia (2utherord class 4!
re5uire some orm o intervention to prevent pro#ression to irreversibleischemia and limb loss. These patients should under#o earlyan#io#raphic evaluation ith ade5uate ima#in# o the aected and theunaected e7tremity. Arterial access is accomplished at a site distantrom the ischemic e7tremity usin# a contralateral emoral artery orbrachial approach to avoid the creation o needle entry sites in an arterythat mi#ht subse5uently be inused ith a thrombolytic a#ent.
-
8/18/2019 Clase Isquemia Arterial Aguda
11/18
Early angiographic imaging should be undertaen in all patients, with the sole exception of
those patients with common femoral emboli! #hese individuals can be taen directly to the
operating room for embolectomy, but intraoperative completion angiography is necessary
to rule out retained thromboembolic material!:?;
=nce adeuate diagnostic information has been obtained from the angiogram, the clinician
is in a position to mae a decision on whether to pursue a percutaneous or open surgical
option!
#hrombolytic therapy6 #hrombolytic therapy with the plasminogen activators(uroinase, alteplase, or reteplase- has been demonstrated to lower the morbidity
and mortality when compared with a traditional approach of immediate operative
revasculariation!:2; :7; #hese benefits appear to be especially prominent in patientswith medical co'morbidities when early revasculariation is necessary! #he
complication rate is high when such patients are taen urgently to open surgical
revasculariation without the ability to adeuately prepare the patient for operation!
Pechanical thrombectomy6 emoval of intra'arterial thrombus with a mechanicaldevice has gained popularity over the last several years!:20; :2; "ome devices rely on
hydrodynamic, rheolytic forces to extract the thrombus, whereas others use rotating
components to fragment the clot! Pechanical thrombectomy devices can be used inconGunction with pharmacologic thrombolysis! $lthough the devices do result in
clearing of much of the occluding thrombus, an infusion of thrombolytic agent is
still necessary in many cases to remove smaller amounts of retained mural clot! mmediate open surgical revasculariation6 Early operation has been remarably
effective in restoring adeuate blood flow to an ischemic extremity! #he relatively
simple procedure of balloon catheter thromboembolectomy, however, has fallen intodisfavor for all but embolic occlusions! #he underlying lesion responsible for the
thrombotic event must be identified and corrected to avoid early reocclusion! )or
this reason, long atherosclerotic occlusions are best treated with the placement of a
bypass graft!:22; $s well, patients with occlusion of a bypass graft as the cause ofischemia are best served with the placement of a new bypass graft, if at all possible!:27;
Open Surgical Revascularization
8nortunately, immediate open sur#ical interventions have been
associated ith an une7pectedly hi#h ris/ o ma9or morbidity and mortality.
4laisdell and associates frst reported this fndin#, notin# a :%& perioperative
mortality rate in a revie o more than :%%% patients in the published or/srom the 0$6%s and 0$;%s.') Althou#h the results have improved since the
publication o 4laisdell
-
8/18/2019 Clase Isquemia Arterial Aguda
12/18
preparation of the patient, and complications such as perioperative myocardial infarction,
cardiac arrhythmia, or pneumonia appear to underlie the unacceptable mortality rate in
these patients! $dditionally, wound complications ( )ig! **+@ - and delayed healing are
common in these patients! Hence, despite successful limb salvage, patient dissatisfaction is
freuent!
#he mortality rate from open surgical treatment of acute limb ischemia has beenreconfirmed in numerous studies published after
-
8/18/2019 Clase Isquemia Arterial Aguda
13/18
Figure 66-7 >/in ed#e necrosis in a patient ith open sur#icalrevascularization or acute limb ischemia
-
8/18/2019 Clase Isquemia Arterial Aguda
14/18
Pharmacologic Thrombolytic Therapy
Notin# the hi#h morbidity rom primary open sur#ical revascularization in
patients suerin# rom true limb-threatenin# loer limb ischemia, three
randomized, prospective clinical trials ere or#anized to compare thrombolytic
therapy and immediate open sur#ical revascularization. The frst study, the
2ochester series, compared uro/inase to primary operation in a sin#le-centere7perience o 00 patients presentin# ith hat has subse5uently been called
hyperacute ischemia. ') 3atients enrolled in this trial all had severely threatened
limbs (2utherord class b! ith mean symptom duration o appro7imately
days. Ater 0 year o ollo-up, ?& o patients randomized to uro/inase ere
alive compared ith only =?& o patients randomized to primary operation
( *i#. 66–? !. 4y contrast, the rate o limb salva#e as identical at ?%& in the
to #roups. A closer inspection o the data revealed that the defnin# variable
or mortality dierences as the development o cardiopulmonary
complications durin# the periprocedural period. The rate o lon#-term mortality
as hi#h hen such periprocedural complications occurred but was relatively low when
they did not occur! t was only the fact that such complications occurred more commonly in
patients taen directly to operation that explained the greater long'term mortality rate in the
surgical group!
#he second prospective, randomied analysis of thrombolysis versus surgery was the
"urgery or #hrombolysis for the schemic Lower Extremity ("#LE- trial!:7; Ienentech, themanufacturer of the $ctivase brand of recombinant tissue plasminogen activator (rt'&$-,
funded the study! $t its termination, 7?7 patients were randomied to one of three treatment
groups6 rt'&$, uroinase, or primary operation! "ubseuently, the two thrombolytic groupswere combined for purposes of data analysis when the outcome was found to be similar!
$lthough the rate of the composite endpoint of untoward events was higher in thethrombolytic patients, the rates of the more relevant and obGective endpoints of amputation
and death were euivalent ( )ig! **+? -! "ubseuently, two subgroup analyses of the "#LEdata were published, one relating to native artery occlusions:2A;
Figure 66-8 The rate o amputation as identical in the to treatment #roupsin the 2ochester Trial, ') but the mortality rate as si#nifcantly loer in patients
-
8/18/2019 Clase Isquemia Arterial Aguda
15/18
assi#ned to the thrombolytic arm.
Figure 66-9 @utcome measures rom the >T1" data ater :% days o ollo-up.':) The rates o death and amputation are similar.
and one to bypass #rat occlusions. '$) Thrombolysis appeared more
eective in patients ith #rat occlusions. The rate o ma9or amputation as
hi#her in native arterial occlusions treated ith thrombolysis (0%&
thrombolysis vs. %& sur#ery at 0 year!. 4y contrast, amputation as loer in
patients ith acute #rat occlusions treated ith thrombolysis. These data
su##est that thrombolysis may be o #reatest beneft in patients ith acute
bypass #rat occlusions o less than 0 days.
#he third and final randomied comparison of thrombolysis and surgery was the
#hrombolysis or &eripheral $rterial "urgery (#=&$"- trial, funded by $bbott Laboratories!
)ollowing completion of a preliminary dose'ranging trial in 27 patients,:70; 533 patientswere randomied to a recombinant form of uroinase or primary operative intervention! :;
$fter a mean follow'up period of year, the rate of amputation'free survival was similar in
the two treatment groups6 *AQ and *?Q in the uroinase and surgical patients, respectively
( #able **+3 -! $lthough this trial failed to document improvement in survival or limbsalvage with
-
8/18/2019 Clase Isquemia Arterial Aguda
16/18
TABLE 66-4 -- 2esults in the T@3A> Trial'0)
o 2ecombinant 8ro/inase
Bersus >ur#ery or Acute 3eripheral Arterial @cclusion
INTERVENTIO
N OR OT!OME
RO"INASE
GROP #N $ %7%&
SRGERY GROP
#N $ %7%&
6
M'()*+ 1 Ye,r
6
M'()*+ 1 Ye,r
Oer,)i.e I()er.e()i'(/ N'0
Amputation ? =? 0 =0
Above the
/nee
= 0$ 6
4elo the
/nee
6 :: =
@pen sur#ical
procedures
:0= :=0 ==0 =$%
Da9or 0% 006 0;; 0$:
Doderate ?$ $? 0:6 0=
Dinor 0 0:; :? =
3ercutaneous
procedures
0? 0:= == ;%
'r+) Ou)2'3e/ ' P,)ie()+ E
eath 06.% %.% 0.: 0;.%
Amputation 0. 0=.% 0.$ 0:.0
Above the
/nee
=.6 6.= 6.0 ;.=
4elo the
/nee
6.6 ?.= 6.? =.6
-
8/18/2019 Clase Isquemia Arterial Aguda
17/18
TABLE 66-4 -- 2esults in the T@3A> Trial'0)
o 2ecombinant 8ro/inase
Bersus >ur#ery or Acute 3eripheral Arterial @cclusion
INTERVENTIO
N OR OT!OME
RO"INASE
GROP #N $ %7%&
SRGERY GROP
#N $ %7%&
6
M'()*+ 1 Ye,r
6
M'()*+ 1 Ye,r
@pen sur#ical
procedures
%.: :$.: 6$.% 6=.
Da9or :.6 .: :$.: :$.:
Doderate 0%.: ?.; 06.: 0:.
Dinor 6. 6.: 0:. 0.;
"ndovascular
procedures
06.$ 0=. .0 0.;
Dedical
treatment alone
0.6 0%.: :.; .?
> 9orst outcome is the most severe event that occurred over the specified time period!
(66
-
8/18/2019 Clase Isquemia Arterial Aguda
18/18
TABLE 66-5 -- 2esults o 3harmacolo#ic Thrombolysis Compared ith
@pen >ur#ical 2evascularization
TRIAL
THROMBOLYSIS/ OPERATION/
A3u),)i'( e,)*
A3u),)i'( e,)*
2ochester 0? 06 0?
>T1" 0 6.= 00 ?.=
T@3A> 11 0= % 0:.0 0;
thrombolysis, ully :& o the thrombolytic patients ere alive ithoutamputation ith nothin# more than a percutaneous procedure ater 6 months
o ollo-up. Ater 0 year, this number had decreased only sli#htly, ith 6&
alive, ithout amputation, and ith only percutaneous interventions. The
ori#inal #oal o the T@3A> trial, to #enerate data on hich re#ulatory approval
o recombinant uro/inase ould be based, as not achieved. Nevertheless, the
fndin#s confrmed that acute limb ischemia could be mana#ed ith catheter-
directed thrombolysis, achievin# similar amputation and mortality rates but
avoidin# the need or open sur#ical procedures in a si#nifcant percenta#e o
patients.