TRATAMIENTO ANTIOSTEOPORÓTICO ¿Desde Cuándo y Cuál? Patricia Alonso Fernández Facultativo...
47
TRATAMIENTO ANTIOSTEOPORÓTICO ¿Desde Cuándo y Cuál? Patricia Alonso Fernández Facultativo Especialista en Geriatría Hospital Clínico San Carlos (Madrid)
-
Upload
cruzita-arena -
Category
Documents
-
view
219 -
download
1
Transcript of TRATAMIENTO ANTIOSTEOPORÓTICO ¿Desde Cuándo y Cuál? Patricia Alonso Fernández Facultativo...

TRATAMIENTO ANTIOSTEOPORÓTICO
¿Desde Cuándo y Cuál?Patricia Alonso Fernández
Facultativo Especialista en GeriatríaHospital Clínico San Carlos (Madrid)

PROTOCOLO DE TRATAMIENTO

¿Hay que tratar?¿Cuándo hay que tratar?
¿Con qué tratar?¿Hasta cuándo tratar?

¿QUÉ hay que tratar?¿Cuándo hay que tratar?
¿Con qué tratar?¿Hasta cuándo tratar?

La osteoporosis afecta a más de 200 millones de mujeres en el mundo
Afecta a 1 de cada 10 mujeres en la década de los 60, una de cada 5 en los 70, 2 de cada 5 de 80 y dos de cada 3 de cada una en la década de los 90.
España: 2,5 millones de mujeres con osteoporosis.
Johnell O el al. Osteoporos Int 2006;17:1726.
Melton LJ et al. J Bone Miner Res 1998;13:1915.
Kanis JA et al. Osteoporos Int 2000;11:669.
Algunos datos epidemiológicos…

Se traduce en que 1 de cada 3 mujeres y 1 de cada 5 hombres mayores de 50 años sufrirá una fractura osteoporótica (riesgo de fractura similar al de padecer una enfermedad cardiovascular).
El riesgo de que una mujer sufra una fractura de cadera (1 de cada 6) es mayor que el de sufrir cáncer de mama (1 de cada 9)
Burge R, Dawson-Hughes B, Solomon DH et al. J Bone Min Res 2007;22:465–475. Cummings SR et al. Lancet 2002; 359:1761. Kanis JA Lancet 2002;359:1929.
La trascendencia de la osteoporosis radica en ser un factor de riesgo de fracturas

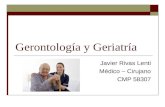
La prevalencia más alta de fractura se produce en mujeres con puntuaciones T correspondientes a osteopenia
Las tasas de fracturas aumentan a medida que disminuye la DMO. Sin embargo, el número absoluto de mujeres con fracturas es mayor en mujeres con puntuaciones T de
rango medio.
Siris ES, et al. Arch Intern Med 2004;164:1108-1112.
DMO / Puntuación T
Fracturas/1.000 personas-años Número de mujeres con fracturas
1,0 0,5 0,0 -0,5 -1,0 -1,5 -2,0 -2,5 -3,0 -3,5
Tasa de fracturas
Mujeres con fracturas
0
10
20
30
40
50
0
100
200
300
400

Cummings et al. NEJM 1995;332:767-773
Incidencia de fracturas por 1.000 mujeres / año
Lo importante... los factores de riesgo de fractura

TRATAMIENTO ANTIFRACTURAS
¿Desde Cuándo y Cuál?

Riesgo Absoluto
Riesgo
Modificable
Riesgo
No Modificable

Beneficio Absoluto
Riesgo Absoluto
Riesgo
Inmodificable
Riesgo
Modificable


>70-80 añosIMC <19
perder >10% pesoinactividad
fractura previabaja DMO
antecedentes fract. familiarfármacos
diabetes tipo 1anorexia nerviosa
gastrectomía anemia perniciosa
tabacoalcohol
escasa exposición solarmenopausia precoz
artritis reumatoideingesta de calcio <500 mg
diabetes tipo 2Hipertiroidismo
hiperparatiroidismo
Factores de RIESGO de fracturas
MAYORES MENORES

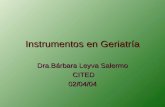
Si queremos prevenir las fracturas de cadera...
En el Nurse’s Health Study…
Sólo con caminar cuatro horas a la semana se DISMINUYE un 41% el riesgo de fractura de cadera
JAMA. 2002;288 (18) 2300-2306)

TRATAMIENTO ANTIFRACTURAS
¿Cuándo?


Otras herramientas para valorar el riesgo de fractura
Women’s Health InitiativeEscala de Black o índice Fracture


Osteoporos Int. 2014 Aug 8. [Epub ahead of print]A Frailty Index predicts 10-year fracture risk in adults age 25 years and older: results from the Canadian Multicentre Osteoporosis Study (CaMos).Kennedy CC1, Ioannidis G, Rockwood K, Thabane L, Adachi JD, Kirkland S, Pickard LE, Papaioannou A.AbstractWe created a 30-item Frailty Index in the Canadian Multicentre Osteoporosis Study. A Frailty Index is a sensitive measure that can quantify fracture risk according to degree of frailty. Our results indicated that at any age, frailty was an important independent risk factor for fracture over 10 years.INTRODUCTION:In later life, frailty has been linked to fractures. It is likely that the antecedents of fracture are seen across the life course, in ways not entirely captured by traditional osteoporosis risk factors. Using data collected from the prospective, population-based Canadian Multicentre Osteoporosis Study (CaMos), we created the 30-item CaMos Frailty Index and examined whether it was associated with incident fractures over 10 years.METHODS:All CaMos participants aged 25 years and older (n = 9,423) were included in the analysis. To examine the relationship between baseline Frailty Index scores and incident fractures, a competing risk proportional sub-distribution hazards model was used with death considered a competing risk. Analyses were adjusted for age, sex, body mass index, education level, femoral neck T-score, and antiresorptive therapy.RESULTS:At baseline, the mean age was 62.1 years [standard deviation (SD) 13.4], and 69.4 % were women. The mean Frailty Index score was 0.13 (SD 0.11), ranging from 0 to 0.66. For every 0.10 increase in Frailty Index scores (approximately one SD), the hazard ratio was 1.25 (p < 0.001) for all fractures, 1.18 (p = 0.043) for hip fractures, and 1.30 (p ≤ 0.001) for clinical vertebral fractures.
CONCLUSION:The CaMos Frailty Index quantified fracture risk according to degree of frailty. Irrespective of age and bone mineral density, the Frailty Index was associated with hip, vertebral, and all-type clinical fractures. Predicting late onset illnesses may have to consider overall health status and not just traditional risk factors.

Risk factors for fracture are, at least partly independent of BMD, parental history of hip fracture, alcohol intake of 4 or more units per day, prior fracture, long-term systemic use of corticosteroids (the latter two of which are not covered in this guidance), and rheumatoid arthritis.
Indicators of low BMD are low body mass index (defined as less than 22 kg/m2), medical conditions such as ankylosing spondylitis, Crohn’s disease, conditions that result in prolonged immobility, and untreated premature menopause
Postmenopausal women aged
Independent clinical risk factor for fracture
Indicator of low BMD Osteoporosis confirmed
Younger than65 years
1 or more and at least oneadditional indicator
Required
65–69 years 1 or more n/a Required
70 years and older 1 or more or Yes Required
In women ≥ 75 years: not required if two or more clinical risk factors or indicators of low BMD
NICE eligibility criteria for Primary Prevention
¿Desde CUÁNDO hay que tratar?

Las mujeres con fractura previa presentan un aumento del riesgo del 86% de sufrir nuevas fracturas1
Una de cada 5 mujeres posmenopáusicas con fractura vertebral previa presentará otra fractura vertebral en el plazo de 1 año2
El 45% de las mujeres con fractura de cadera sufrieron previamente una fractura por fragilidad3-5
Las mujeres con fractura previa tienen aproximadamente el doble de riesgo de sufrir una fractura de cadera6
1. Kanis JA, et al. Bone 2004; 285: 375-382; 2. Lindsay R, et al. JAMA 2001; 285: 320-323; 3. Lyles KW, et al. ASBMR 2006; 4. Edwards BJ, et al. Clin Orthop Rel Res 2007; 461: 226-230; 5. McLellan AR, et al. (2004) Effectiveness of Strategies for the Secondary Prevention of Osteoporotic Fractures in Scotland (CEPS 99/03). NHS Quality Improvement Scotland; 6. Klotzbuecher CM, et al. J Bone Min Res 2000;15:721-739.
Las fracturas previas predicen las fracturas futuras

¿Desde CUÁNDO hay que tratar?
Age Eligibility criteria
Less than 75 years T-score –2.5 or less
75 years or older T-score –2.5 or less*
* In women aged 75 years or older, a dual energy X-ray absorptiometry (DXA) scan may not be required if the responsible clinician considers it to be clinically inappropriate or unfeasible. Source [NICE, 2011a]
NICE eligibility criteria for postmenopausal women with an Osteoporotic Fragility Fracture

Recomendaciones para la valoración y tratamiento de la osteoporosis primaria de la Com.
Madrid 2007


*
*
*
*
*
*

TRATAMIENTO ANTIFRACTURAS
¿Cuándo?
Valoremos el riesgo de FRACTURA o sigamos las guías si ya existe fractura
…y decidamos qué tratamiento farmacológico

TRATAMIENTO ANTIFRACTURA
¿Con QUÉ tratar?



La “Cuarta Garantía”
Mientras que en Estados Unidos para que un medicamento esté en el mercado basta con demostrar calidad, seguridad y eficacia en comparación con placebo.
La incorporación efectiva del medicamento a la prestación farmacéutica en los países con sistemas públicos de salud requiere que haya una demostración también en términos de coste-efectividad

Initial treatment offered: alendronate
• Postmenopausal women with confirmed osteoporosis• A DXA scan may not be required in women aged 75 or over
SECONDARY PREVENTION
FIRST TREATMENT OPTION


9973


It reviews the risk assessment and intervention thresholds, the impact of nutritional deficiencies, fall prevention strategies, pharmacological treatments and their safety considerations, the risks of sub-optimal treatment adherence and strategies for its improvement.
Anti-fracture efficacy already by 12 months.The safety profiles of these pharmacological agents are generally satisfactory in this patient segment provided a few precautions are followed.
CONCLUSION: These patients should be considered for particular consultation/follow-up procedures in the effort to convince on the benefits of treatment and to allay fears of adverse drug reactions, since poor adherence is a major problem for the success of a strategy for osteoporosis and limits cost-effectiveness.

Secondary prevention: alternative treatment option (1)
Alternative treatment – risedronate or etidronate when women:• are unable to comply with administration of, or have
a contraindication to or are intolerant of alendronate and • have a combination of T-score, age and number of clinical risk factors
as outlined in the table.
Number of independent clinical risk factors for fracture
Age (years) 0 1 2
50–54 a −3.0 −2.5
55–59 −3.0 −3.0 −2.5
60–64 −3.0 −3.0 −2.5
65–69 −3.0 −2.5 −2.5
70 or older −2.5 −2.5 −2.5a Treatment with risedronate or etidronate is not recommended.

Secondary prevention: alternative treatment option (2)
Denosumab is recommended as:
• in postmenopausal women at increase risk of fractures who are unable to comply with the special instructions for administering alendronate and either risedronate or etidronate,
• or have an intolerance of, or a contraindication to, those treatments.

MÉTODOS INDIRECTOS DE VALORACIÓN DE LA ADHERENCIA
Test de Morisky - Green
Valora si el paciente adopta actitudes correctas en relación con la terapéutica.
1. ¿Se olvida alguna vez de tomar los medicamentos?
2. ¿Toma los medicamentos a las horas indicadas?
3. Cuando se encuentra bien, ¿deja alguna vez de tomarlos?
4. Si alguna vez le sientan mal, ¿deja de tomar la medicación?
Para considerar una buena adherencia, la respuesta de todas las preguntas debe ser adecuada (no, sí, no, no)

Teriparatide when:• have a combination of T-score, age and number of fractures
as outlined in the table:
• are unable to take, have a contraindication to or are intolerant of alendronate and either risedronate or etidronate, strontium ranelate
• have had an unsatisfactory response to treatment with alendronate, risedronate or etidronate
Secondary prevention: alternative treatment option (3)
Age (years) T-score Fractures
> 65 years −4.0 SD or below –
> 65 years −3.5 SD or below More than two
55–64 years −4 SD or below More than two


INTOLERANCIA O CONTRAINDICACIÓN (NICE, 2010): Esofagitis, dificultades para la deglución, incapacidad para permanecer erguido 30-60 min tras la administración del bifosfonato, Insuficiencia Renal (aclaramiento de creatinina <35%)
RESPUESTA INADECUADA: fractura por fragilidad a pesar de tratamiento durante un año (con adherencia superior al 80%) o disminución de la DMO por debajo de la basal

*
*
**



CONCLUSIONES
Las fracturas osteoporóticas son un problema sanitario grave
El tratamiento de la OP de acuerdo a las GPC está dentro de los costes aceptables
A partir de los 70 años el tratamiento es coste efectivo
Paradójicamente en este grupo el tratamiento está por debajo de las recomendaciones de la GPC
Los grandes problemas en el tratamiento de la OP son: la adherencia al tratamiento el fracaso terapéutico
Existen fármacos que dan respuesta a dicho problema

Nuestros pacientes…
Son los más viejos
Son los que más se caen
Son los que tienen menores posibilidades de recuperación funcional
Son los de mayor riesgo de fractura de cadera
Menor riesgo de efectos secundarios a largo plazo

GRACIASPatricia Alonso Fernández
Facultativo Especialista en GeriatríaHospital Clínico San Carlos (Madrid)