Neurobiomecanica de Pelvis
34
Neurobiomecánica de Pelvis y Ar7culaciones Sacroiliaca Profesores: Angelo Bartsch J. Cristián Cuadra G.
-
Upload
paula-bustamante-munoz -
Category
Documents
-
view
224 -
download
0
description
Biomecànica de pelvis
Transcript of Neurobiomecanica de Pelvis
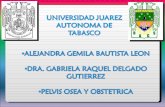
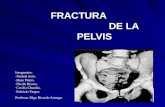
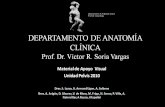
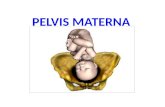
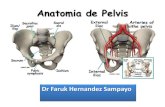
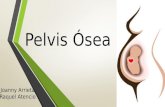
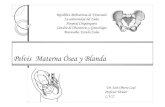
neuroblomecnlca de elvls y Aruculaclones Sacrolllaca Profesores: Angelo Bartsch J. Cristin Cuadra G. 8ecuerdo AnaLmlco !"#$%&'" )"&$'*+,-%'" 3 Grados de Libertad Movilidad Rgida Estable Vs 8ecuerdo AnaLmlco !"#$%&'" )"&$'*+,-%'" 8ecuerdo AnaLmlco !"#$%&'" )"&$'*+,-%'" 8ecuerdo AnaLmlco !"#$%&'" )"&$'*+,-%'" Allneacln de las LsLrucLuras !"#$%&'" )"&$'*+,-%'" 635 Chapter 35| STRUCTURE AND FUNCTION OF THE BONES AND JOINTS OF THE PELVISdifferencescanbeseeninthepelvicjoints:theacetabulumandauricularsurfacesoftheiliaandsacrumaresmaller[20,149],andthesymphysealsurfaceofthepubicbodyisshorter [164].Android (male) Gynecoid (female)Platypelloid AnthropoidA BC DPELVIC DIAMETERS AND TYPES OF PELVES:Assessment of the overall size of the female pelvis and thedimensions of its apertures is important in obstetrical prac-tice. Two openings are significant: one is situated above andserves as the pelvic inlet (superior aperture), and the otheris positioned below and functions as the pelvic outlet (inferi-or aperture) (Fig. 35.19). The size of the pelvic cavity posi-tioned between these two bony boundaries is the limitingfactor in obstetric considerations; no attempts are made toaccount for the fascial and muscular contributions made tothis space [135].The pelvic brim borders the pelvic inlet (Fig. 35.20). Oneach side, it is formed posteriorly by the sacral ala, laterallyby the arcuate line of the ilium and pecten of the pubis(together forming the linea terminalis), and anteriorly by thepubic crest. The circle is completed in the posterior midlineby the sacral promontory and anteriorly by the symphysispubis. The border of the pelvic outlet is formed anteriorly bythe pubic arch, laterally by the ischial tuberosities andsacrotuberous ligaments, and in the posterior midline by thecoccyx. The plane of the pelvic inlet is approximately 60 offthe horizontal, while the plane of the outlet is nearly hori-zontal [135] (Fig. 35.19). Owing to the different orientationsof the two apertures, the axis of the pelvic cavity, runningthrough the centers of the inlet and outlet, follows a curvedcourse that nearly parallels the sacrococcygeal curvature.During parturition (childbirth), the fetus follows this curva-ture in its passage through the pelvic cavity.For obstetrical purposes, three diameters of the superioraperture of the pelvis are measured commonly to deter-mine the prospective mothers pelvic type prior to delivery(Fig. 35.21). The true conjugate diameter is the distancebetween the superior border of the symphysis pubis to thesacral promontory; the diagonal conjugate diameter issimilar but has a starting point inferior to the symphysispubis. The former is measured radiographically, but thelatter can be assessed during the vaginal examination. Thetransverse diameter, the greatest distance between sym-metrical points on the pelvic brim, is deduced from exter-nal pelvic dimensions or the distance between the ischialspines, which are palpable through the vagina. Four typesof pelves are described on the basis of the ratio betweenthe transverse and conjugate diameters (Fig. 35.22). Theseare gynecoid (female), anthropoid (ape), android (male),and platypelloid (flat). The transverse diameter is greaterthan the conjugate in the gynecoid, android, and platypel-loid pelves, while the opposite is true in the anthropoidpelvis. Gynecoid and android pelves predominate inCaucasian females, while gynecoid and anthropoid typesare more common in Negroid females; few females haveplatypelloid pelves [8,147]. All pelvic types except thegynecoid type hamper engagement of the fetal headduring labor [135].Clinical Relevance Figure 35.22: Shapes of four major types of pelves are based on the ratio between the transverse and conjugate diameters. AC. The transverse diameter is greater than the conjugate. D. The opposite is true.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 635Allneacln de las LsLrucLuras !"#$%&'" )"&$'*+,-%'" 637 Chapter 35| STRUCTURE AND FUNCTION OF THE BONES AND JOINTS OF THE PELVISscientific studies has found its way into clinical and basic sci-ence textbooks. Inclusion in this section of all of the studiesthathavecontributedtotheknowledgebaseofthepelvicjoints is neither possible nor appropriate. Following a descrip-tionofeachofthejoints,thestudiesmostcriticaltoourunderstanding are offered.Lumbosacral JunctionThe basic components of the L5 and S1 articulations do notdiffer significantly from the other intervertebral unions. Thebodies are joined by an amphiarthrodial symphysis, whichconsists of thin layers of hyaline cartilage on either side of thelargestfibrocartilaginousdiscinthespine;thediscistalleranteriorlythanposteriorly,amatchingfeaturefoundintheL5body.Thesynovialzygapophysealjointshavefacetsori-entedinthecoronalplanewhosesurfacesaremorewidelyseparated than those above [147]. The sacrum sits below L5with its base tilted forward and its apex backward. The sacralinclination thusformedconsistsofthebaseofthesacrumbeingtiltedforwardoffthehorizontalbyapproximately30(Fig. 35.26). There is tremendous variability, however, with areportedrangeof20to90 [58,59,81];itisgreaterin the female [9,147]. The sacral inclination, as well a wedge-shapedL5vertebralbodyandIVD,eachcontributeto the lumbosacral angle (between the long axes of L5 and thesacrum) [81,136]; it is greater in males.Body weight forcebWa30140Figure 35.25: Medial aspect of the left hemipelvis. In standing,the sacral promontory tends to tilt down and forward while theilia tend to tilt backward because the center of gravity passesanterior to the sacroiliac joints (SIJs) and posterior to the hipjoints. These tendencies are resisted by the interosseous sacroiliac,sacrotuberous and sacrospinous ligaments, and the inherent morphology of the SIJ.Figure 35.26: The lumbosacral angle (a) is formed by the intersec-tion of lines drawn between the long axis of the fifth lumbarvertebra and the sacrum. It results from a forward sacral inclina-tion (b) and wedge-shaped lower lumbar intervertebral discs andbodies. As the sacral inclination and lumbar lordosis increase, thelumbosacral angle decreases, and vice versa. The sacral inclina-tion is greater in the female, while the lumbosacral angle isgreater in the male. W, superincumbent weight.LUMBOSACRAL ANGLE: The sacral inclination and thelumbosacral angle are intimately related to the lumbar lor-dosis. An increase in the sacral inclination along with adecrease in the lumbosacral angle necessitates an increasein the lumbar lordosis.Clinical Relevance Oatis_CH35_620-653.qxd4/15/072:06 PMPage 637Allneacln de las LsLrucLuras !"#$%&'" )"&$'*+,-%'" 638 Part IIII KINESIOLOGY OF THE HEAD AND SPINEManymuscularandligamentousentitiescrossandrein-forcethelumbosacraljunction.Themusclesbelongtothetrunk and lower limbs. Essentially any muscle that moves thetrunk across the joints of the lumbar spine stabilizes the joint,including the anterior and anterolateral abdominal wall mus-cles, posterior abdominal wall muscles, and lumbar deep backmuscles. These are described in greater detail in Chapter 33.Ligamentoussupportisprovidedbycontinuationofthevertebral ligaments that are found at higher levels of the spineandincludetheanteriorandposteriorlongitudinal,inter-transverse,interspinous,andsupraspinousligaments,alongwith the ligamentum flavum and zygapophyseal capsular ele-mentsattheL5S1interspace.Inaddition,theiliolumbarligaments reinforce the junction laterally (Fig. 35.27). Eachextends from the tip of the transverse process of L5 (and fre-quently L4) and spreads laterally to connect to the pelvis byway of two bands, both of which pass anterior to the SIJ. Anupper band attaches to the iliac crest, where it is continuousabovewiththethoracolumbarfascia;alowerband(some-timesreferredtoasthelumbosacralligament,thoughnotrecognized in the N.A. [45]) passes to the upper surface of thesacralala,whereitblendswiththeanteriorsacroiliacliga-ment [27,91,94,123,147].The iliolumbar ligament is not present in the newborn; itdevelops over the first two decades by metaplasia of fibers ofthequadratuslumborumandundergoesdegenerationfromthe fourth decade on [94]. Researchers theorize that the liga-ment develops when the lumbosacral junction is stressed byassumptionoftheuprightposture[27,94]andsuggestthatthe different bands of the ligament serve different functions[27,91]. The lower band is positioned in the coronal plane; itservestosquareL5onthesacrumandthuscontrollateralflexion. The upper band runs obliquely backward; it exerts aposteriorpullonL5topreventanteriorslippageduringweightbearing,anditcontrolsflexion.Theiliolumbarliga-ments, as a whole, appear to also control axial rotation [180].Apparently,theligamentassumesgreaterfunctionalsignifi-cance in contributing to lumbosacral stability when the lum-bosacral disc degenerates; it may protect the disc from exces-sive torque, particularly if the facet joints are defective [27].As already indicated, the lumbosacral junction is a regionof high variability, as well as the point of greatest stress in theentire vertebral column. Being one of the levels most subjecttointernalderangement[33],Kapandjireferstoitastheweak link [81]. As a result of the body weight bearing downon L5 and the anterior inclination of the sacrum, an anteroin-feriorshearstressisproducedattheL5S1junction;theresultant force vector, acting through the pars interarticularis,is an anterior one [81] (Fig. 35.28). Subsequently, L5 tends toslide forward on the sacral promontory. This tendency is resis-ted,andL5isrestrained,however,bythevertebrasbonyhook, formed by its pedicles, pars interarticulares, and inferiorarticular processes, fitting over the superior articular processesof the sacrum below [59] (Fig. 35.28).4th vertebraIliolumbar ligamentsLumbosacralligamentVentralsacroiliacligamentsPars interarticularis fracturePars interarticularis fractureABFigure 35.27: Iliolumbar ligaments, both passing anterior to thesacroiliac joint, are shown connecting both the fourth and fifthlumbar vertebrae to the ilium. Although not recognized by theNomina Anatomica, a lumbosacral ligament is shown.Figure 35.28: The bony hook of L5 consists of its pedicle, parsinterarticularis, and inferior articular process; it fits over thesuperior articular process of the sacrum below. A. Disruption ofthe bony hook mechanism between L5 and S1 can be caused byfracture of the pars interarticularis (spondylolysis) and can resultin spondylolisthesis. B. Pars interarticularis defect seen fromabove L5.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 638639 Chapter 35| STRUCTURE AND FUNCTION OF THE BONES AND JOINTS OF THE PELVISSacrococcygeal JunctionAsymphysisconsistingofasmallfibrocartilaginousIVDsandwiched between thin layers of hyaline cartilage unites theapex of the sacrum and the superior surface of the first coc-cygealsegment(Fig.35.7).Anterior,lateral,andposteriorsacrococcygeal ligaments complete the union. Successive seg-ments are nodular and generally fused to one another; occa-sionally, there is a synovial joint between the second and thirdsegments. In the young, all intercoccygeal joints are symphy-seal,buttheyfuseinadulthood,earlierinmalesthaninfemales;withadvancingage,thesacrococcygealjointfuses[80,147].Thetipofthecoccyxisanchoredtotheoverlyingskin and can be palpated easily in the intergluteal cleft [113].DorsalprimaryramiofS4-5andCo1anastomosewithoneanotherandformloopsthatinnervatethesacralapexandcoccyx, as well as the overlying skin [147].PARS INTERARTICULARIS DEFECTS: Various anom-alies and pathological or congenital conditions, over time andunder stress, may weaken or destroy the integrity of the resist-ing hook mechanism; such defects include congenital aplasia(or dysplasia) of the sacral facets, near-sagittal orientation ofone or both of the lumbosacral facet joints (Fig. 35.9), exces-sive anterior tilt of the sacrum resulting in increased lum-bosacral shear, and spondylolysis. Disruption of the parsinterarticularis (spondylolysis) can occur unilaterally (up to30%), with or without slipping (olisthesis), and although ithas been observed at L3, L4, and L5, it is most frequent at L5[59,60,100,136]. Although 5% of individuals with this condi-tion are asymptomatic [100], spondylolisthesis can be a seri-ous consequence of spondylolysis. The Belgian obstetricianHerbineaux [72] is credited with describing the first cases ofspondylolisthesis when he noted that, on occasion, a bonyprominence on the anterior surface of the sacrum interferedwith labor. Because of the location of the spondylolytic defect,the body, pedicles, and superior articular processes slip for-ward, leaving the inferior articular processes, laminae, andspinous process in their normal position.Spondylolisthesis is diagnosed on the oblique radi-ographic projection; the disrupted pars interarticularis (isth-mus) appears as a translucent area in the vicinity of theneck of the Scottie dog, described earlier in this chapter[101] (Fig. 35.5). The degree of slip of L5 on the sacrum isassessed on the lateral radiographic view as a percentagebased on a grading system of Myerding [115]: grade 1, 25%;grade 2, 2550%; grade 3, 5075%; grade 4, 75100%overhang (Fig. 35.29). Spondyloptosis occurs when theposterior edge of L5 moves anterior to the sacral promontory[100]. IVD degeneration, cauda equina compression, andsevere pain are serious potential sequelae of this disorder[59,61,100,101].Clinical Relevance COCCYX AND SACROCOCCYGEAL JUNCTION: Duringchildbirth, the coccyx moves posteriorly, allowing anincrease in the diameter of the pelvic outlet, thus facilitatingmovement of the fetus through the birth canal [113].Presumably, the movement is passive and secondary to pas-sage of the fetus and made possible by relative relaxation ofthe ligaments surrounding the coccyx. It is stimulated by anincrease in circulating sex hormones and the hormonerelaxin (more on this later) [97,113].Most injuries to the coccyx occur in women, probablyowing to its more posterior position in the broader pelvicoutlet of the female [33]. Injuries can occur during obstetri-cal and gynecological maneuvers, but most result fromother traumas [107,119]. An extension strain or fracture ofthe coccyx can result from childbirth; flexion injury, fracture,or a direct contusion can result from a fall on an unevensurface or in the half-sitting position (allowing some of theforce to be absorbed by the coccyx away from the ischialtuberosities) [33,49,80]. In extremely lean individuals withoutsufficient gluteal mass, the coccyx may be vulnerable in sit-ting [130]. Coccygodynia (coccygeal pain; also known ascoccydynia, coccyalgia) from any of the aforementionedmechanisms is always localized to the coccyx. Pain can beexperienced with activation of muscular fibers attaching tothe coccyx (i.e., gluteus maximus, iliococcygeus and coc-cygeus). Consequently, walking, especially uphill or upstairs,and sitting, particularly going from standing to seated, areusually painful; defecation and coitus may be noxious inClinical Relevance L54321Figure 35.29: Spondylolistheses is graded on the basis of theamount of forward movement of L5 on the sacrum. In grades 1,2, 3, and 4, some 25, 50, 75, and 100% of the body of L5 is posi-tioned anterior to the sacral promontory, respectively.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 6398elacln mecnlca !"#$%&'" )"&$'*+,-%'" 636 Part IIII KINESIOLOGY OF THE HEAD AND SPINEPELVIC JOINTS AND PERIARTICULARSTRUCTURESIn the erect posture, the superincumbent weight of the head,upperlimbs,andtrunkistransmittedontothesacrumthroughthelastlumbarvertebraanditsdisc.Weightisfurther transmitted through the paired SIJs and distributed totheischialtuberositiesinsittingorthefemorainstanding.Completedanteriorlywiththeunionofthepubicbodiesatthesymphysispubis,thisosteoligamentousring issubdi-videdintotwoanatomicalandfunctionalarchestodescribethetransmissionofforcesinthestandingposture[3,9,80,81,147];acoronalplanepassingthroughtheacetabulaseparates the bony pelvis into anterior and posterior arches(Fig.35.23).Theupperthreesegmentsofthesacrumandpaired pillars of iliac bone passing from both SIJs to the pos-terosuperior acetabula form the posterior arch, which servesmainly to transfer weight from above to the lower limbs. Theanterior arch is a tie beam or counter arch and consists of thesuperiorpubicrami,pubicbodies,andinterpubicdisc;itservesthedualfunctionofconnectingtheanteriorendsofthe iliac pillars to prevent separation of the posterior arch atthe SIJs, as well as acting as a compression strut against thegroundreactionforcesfromthefemorabelow.Thesittingarchesaresomewhatdifferent.Weightistransmittedfromabove through the SIJs, inferior parts of the iliac pillars, andthen to the ischial tuberosities. The tie beam or counter archfor the sitting arch includes the ischial tuberosities, ischiopu-bicrami,pubicbodies,andinterpubicdisc[9].Thehigheststresses and greatest bone densities of the pelvic bones occuralongthelinesofthetheseanteriorandposteriorarches[34,35,75] (Fig. 35.24).Thebonesandjointsofthepelvisareinherentlystable.The line of transmission of both the trunk force from aboveandthegroundreactionforcesfrombelowpassanteriortothe SIJs (Fig. 35.25). The former force tends to tilt the sacrumforward, and the latter tends to rotate the innominate bonesbackward;bothareresistedbythenumerousstrongliga-ments of the pelvic joints, as well as, in the SIJs particularly,theinherentmorphologyoftheirarticulatingsurfaces[30,147].Together,thetwoforcesprovideaself-locking,screw-homemechanismformaximalstability[3,59,81,147].Thelevelofpelvicstabilityachievedbythisarrangementrequiresthousandsofpoundsofforcetodisrupt[30,137].Furthermore,whenlargeforcesareappliedtothepelvis,either in vivo or in vitro, the sacrum or ilium often fracturesbefore the ligaments rupture or avulse.The reader should be warned that many aspects of pelvicjoint morphology, mechanics, and pathology have been debatedheavilyovertheyears.Mostofthequestionssurroundingthese joints appear to have been adequately probed to allowmostcliniciansandscientiststoarriveatwell-documentedconclusions regarding the issues around which controversy hasthrived.Althoughnaggingquestionspersist,especiallyasregards the amount and type of motion present at these joints,only a few diehards remain who are skeptical about the otherissues.Twothingsaccountforthechangingperspectivetowardthesejoints:first,technologicaladvancesinresearchtechniqueshaveproducedless-equivocalevidence,andsec-ond,thebodyofevidencefromnumerouswell-designedFigure 35.23: In standing, the posterior arch passes through thesacrum, paired iliac pillars, posterosuperior acetabula, and femora,while the anterior (counter) arch passes through the femora,superior pubic rami, pubic bodies, and interpubic disc (solid lines).In sitting, the posterior arch passes through the sacrum, inferiorpart of the iliac pillars, to the ischial tuberosities, while theanterior (counter) arch passes through the ischial tuberosities,ischiopubic rami, pubic bodies, and interpubic disc (broken lines).StandingtransferSittingtransferFigure 35.24: Bony trabecular system of the right innominatebone and proximal femur. The transfer of weight via the SIJ isthrough the arcuate line to the acetabulum in standing, andthrough the arcuate line to the ischial tuberosities when sitting.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 6368elacln mecnlca !"#$%&'" )"&$'*+,-%'" Cpsula Arucular- LlgamenLos !"#$%&'" !.&.'*+,-%'" Cpsula Arucular- LlgamenLos !"#$%&'" !.&.'*+,-%'" (c) 2001 Primal Pictures Ltd.(c) 2001 Primal Pictures Ltd.Cpsula Arucular- LlgamenLos !"#$%&'" !.&.'*+,-%'" 642 Part IIII KINESIOLOGY OF THE HEAD AND SPINEAuricularsurfacesoffemalesaresmallerandflatterthanthose in males [20,149,151,163].Starting in the middle of the third decade, surfaces of thesynovialpartoftheSIJbegintoshowsignsofdegeneration[19].Jointdegenerationprogressesfromthefourththroughthe eighth decade and is characterized by thickening and stiff-eningofthecapsule,severelossofcartilagethickness,sub-chondral bone erosion, increasing surface irregularity, intraar-ticular fibrosis of joint surfaces and, in a few individuals, totalankylosis. The degenerative changes that develop on the iliacside appear first and are more severe than those on the sacralside[19,20,168];furthermore,theyappearatanearlier ageandadvancemorerapidlyinmalesthanfemales[20,21,29,96,131,151,168].Oneauthor[138]reportssevere,advanced degenerative changes in over 90% of the SIJs fromaged males (over 80 years old).SUPPORTING STRUCTURES OF THE SIJThe SIJ is reinforced by some of the strongest and most mas-siveligamentsinthebody[6,147,169,175].Threeligamentsareinintimatecontactwiththejoint,andthreeothers,though better termed accessory, make important contribu-tions to the joints integrity.TheSIJcapsuleiscloselyattachedtothejointsmargins;ventral and dorsal sacroiliac ligaments (VSIL, DSIL) crossthejoint,andtheinterosseoussacroiliacligament (ISIL)connects the sacral and iliac tuberosities (Figs. 35.31, 35.32).The VSIL is little more than a thickening of the anterior jointcapsule;thecranialpartisthinandreinforcedbyiliolumbarligament fibers, while the caudal half is well developed belowonly as far as the iliac arcuate line [147,159]. It assists the sym-physis pubis in resisting separation or horizontal movement oftheinnominatebonesattheSIJs.TheDSILisheavierandDorsal sacroiliacligamentSacrospinousligamentSacrotuberousligament SacrospinousligamentSacrotuberousligamentIliolumbarligamentLumbosacralligamentVentralsacroiliacligamentABCFigure 35.32: Ligaments of the sacroiliac joint. A. Dorsal view. B. Medial view. C. Ventral view.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 642Cpsula Arucular- LlgamenLos !"#$%&'" !.&.'*+,-%'" L[es y lanos de MovlmlenLo )"&$'%-/$012%3 645 Chapter 35| STRUCTURE AND FUNCTION OF THE BONES AND JOINTS OF THE PELVISoppositedirection,duringtrunkextensionorbilateralhipextension. Nutation and counternutation are accompanied byseveralmillimetersoftranslation.Inthistypeofmotion,theinnominate bones move symmetrically, as a unit, in the absenceof motion at their anterior union, the symphysis pubis [67].The sacral base always moves further than the apex [173].Furthermore,itoccursaboutaninstantaneousaxislocated510 cm below the sacral promontory (Fig. 35.35). The com-bination of rotation and translation is angular movement of thesacrum,duringwhichtheiliaccrestsmoveclosertogetherwhiletheiliactuberositiesmovefurtherapart(Fig.35.36).Sagittal plane angular sacral movement is essentially the sameinmalesasinfemales,exceptduringpregnancy,whenitincreasesinfemales.Thegreatestamountofmovement,asmuch as 5.6 1.4 mm, occurs when going from recumbent tostanding and reverses in direction when moving from standingtorecumbent[173].Rotationisaccompaniedbytranslation,which results in increased ligamentous tension and absorptionof energy [176]. The SIJs thereby function as shock absorbers.Asymmetrical MotionAsecondtypeofmotionoccursattheSIJswhenasym-metricalforcesareappliedtothepelvis,asinstaticone-legged stance and the one-legged stance that occurs duringgaitandasymmetricalfalls.Applicationofunbalancedforces to the pelvis results in asymmetrical and antagonis-tic movements at the SIJs [20,125,175], resulting in pelvictorsion. Thesemovementsarealwaysaccompaniedbymovementatthesymphysispubis[67,125],despitethefactthatverylittlemovementoccursinthesymphysispubis, except in pregnancy. The experienced clinician canassessmanuallytheendpositionthatresultsfromFigure 35.34: Sagittal plane motion of the sacrum. In nutation,the base of the sacrum moves ventrocaudally and its apex movesdorsocranially; this occurs when the sacrum is loaded fromabove, in trunk flexion, or in bilateral hip flexion. The base ofthe sacrum moves in the opposite direction during trunk exten-sion and bilateral hip extension, when it counternutates.FarabeufBonnaireWeislFigure 35.35: Medial view of the innominate bone shows threeprimary sites proposed as the location of the axis of rotationbetween the sacrum and the ilium.Figure 35.36: Movement of the innominate bones during nuta-tion of the sacrum. The ilia move closer together, and the ischiamove farther apart.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 645L[es y lanos de MovlmlenLo )"&$'%-/$012%3 SlmeLrlcos )"&$'%-/$012%3 articular surfaces are very irregular. It is this irregular-ity that helps to lock the two surfaces together.Thefunctionofthesacroiliacjointistotransmitweightfromtheupperbodythroughthevertebralcol-umntothehipbones.Itisdesignedforgreatstabilityand has very little mobility. Like other synovial joints, itsarticular surface is lined with hyaline cartilage. Synovialmembrane lines the nonarticular portions of the joint. Ithas a fibrous capsule reinforced by ligaments.SI Joint MotionThe actual type and amount of movement occurring attheSIjointisthesubjectofconsiderablecontroversy.However, it is generally accepted that the motions thatdo occur at the SI joint are nutation and counternuta-tion (Fig. 17-4).Nutation, sometimesreferredtoassacral flexion,occurswhenthebaseofthesacrum(onthesuperiorend)movesanteriorlyandinferiorly.Thiscausestheinferiorportionofthesacrumandthecoccyxtomoveposteriorly. The pelvic outlet becomes larger and can bevisualizedbydrawingalinefromthetipofthecoccyxto the bottom surface of the pubic symphysis.CHAPTER 17 Pelvic Girdle 249Counternutation, sometimescalledsacralextension,referstotheoppositemotion.Thebaseofthesacrummovesposteriorlyandsuperiorly,causingthetipofthecoccyx to move anteriorly. The pelvic inlet becomes larg-er.Thepelvicinletcanbevisualizedbydrawingalinefrom the base of the sacrum across to the top of the sym-physis pubis.The amount of motion that occurs in nutation andcounternutationisminimal,anditcanoccuronly inconjunctionwithotherjointmotions.Nutationoccurs with trunk flexion or hip extension. Conversely,counternutationoccurswithtrunkextensionorhipflexion.Thesemotionsarealsoimportantduringchildbirth.Whenthebabymovesthroughthepelvicinletduringtheearlystagesoflabor,theanterior-posterior (A-P) diameter needs to be larger. Therefore,theSIjointsareincounternutation.Inthelaterstagesoflabor,whenthebabypassesthroughthepelvicoutlet,itisimportantthatthisA-Pdiameterhasincreased.PuttingtheSIjointsinnutationincreases the A-P diameter.Bones and LandmarksThetwobonesoftheSIjointarethesacrumandtheilium, the latter of which is the superior portion of thehip bone. The sacrum is wedge-shaped and consists offive fused sacral vertebrae. It is located between the twohipbonesandmakesuptheposteriorborderofthebonypelvis.Itsanteriorsurface,oftencalledthepelvicsurface, isconcave(Fig.17-5).Becauseitistilted,thesacrum articulates with the fifth lumbar vertebra at anangle referred to as the lumbosacral angle. The significantlandmarks are as follows (Figs. 17-5 and 17-6):BaseSuperior surface of S1.PromontoryRidge projecting along the anterior edge of the body of S1.Superior Articular ProcessLocated posteriorly on the base, it articulates withthe inferior articular process of L5.AlaLateral flared wings that are actually fused transverse processes.ForaminaLocated on the anterior (pelvic) and dorsal surfaces are four pair of foramina. They serve as the exit for the anterior and posteriordivisions of the sacral nerves. The anteriorforamina are larger.Figure 17-4. Sacroiliac joint motions. (A) Nutation occurswhen the sacral promontory moves anteriorly and inferiorlywhile the tip of the coccyx moves in the opposite direction.(B) Counternutation occurs when the sacral promontorymoves posteriorly and superiorly while the tip of the coccyxmoves in the opposite direction.Counternutation NutationA B2363_Ch17-247-258.qxd12/10/1012:32 PMPage 249AslmeLrlcos )"&$'%-/$012%3 646 Part IIII KINESIOLOGY OF THE HEAD AND SPINEmovementofoneinnominatebonerelativetotheother bypalpatingtherelativeprominenceoftherightand leftASISsandPSISs[33,39,58,90,99,104,152,179].Forinstance,iftheleftASISmovesupward,therightASISandtheleftPSISbecomemoreprominentwhiletheleftASISandrightPSISbecomelessprominent(Fig.35.37).Alternating, asymmetrical forces are applied transiently tothepelvisduringeachgaitcycle[20].Theproposedaxisfor pelvic torsion is transverse and passes through the sym-physispubis[125],thoughthisremainsequivocal.AbnormalmobilityorinstabilityineithertheSIJorsym-physispubisoftenisaccompanied,however,byasecond-ary stress lesion in the other [69].Lumbopelvic RhythmThelumbarspineandinnominatebonescanalsomoveasaunit.Inasmuchasmovementsofthespinearecoupledwiththoseofthepelvis,alumbopelvicrhythm (discussedinChapter32),similartothescapulothoracicrhythm,hasbeenpostulated [22] (Fig. 35.38). The specific rhythm varies amongindividuals,butflexionofthetrunkfromstandingcombinesflexion of the lumbar vertebrae and at the lumbosacral junctionwith forward rotation of the pelvis on the fixed femora[3,139].Disturbancesinthelumbopelvicrhythmcancontribute to low back pain [3,121,139].Figure 35.37: Application of unbalanced forces on the pelvis, asin static one-legged stance on the left, results in asymmetrical,antagonistic movement at the SIJs along with movement at thesymphysis pubis. This type of movement can be assessed clinicallyby palpating movement of the ASIS and PSIS.A B CFigure 35.38: Common lumbopelvic rhythm. A. Normal standing posture. B. During the first 45 of trunk flexion, most motion resultsfrom lumbar and sacral flexion causing the sacrum to nutate and the lumbar curve to flatten. C. In extreme trunk flexion, the lumbarspine continues to flatten and the pelvis rotates about the femoral heads, while the sacrum paradoxically counternutates.2Oatis_CH35_620-653.qxd4/15/072:06 PMPage 6468lLmo Lumbopelvlco )"&$'%-/$012%3 646 Part IIII KINESIOLOGY OF THE HEAD AND SPINEmovementofoneinnominatebonerelativetotheother bypalpatingtherelativeprominenceoftherightand leftASISsandPSISs[33,39,58,90,99,104,152,179].Forinstance,iftheleftASISmovesupward,therightASISandtheleftPSISbecomemoreprominentwhiletheleftASISandrightPSISbecomelessprominent(Fig.35.37).Alternating, asymmetrical forces are applied transiently tothepelvisduringeachgaitcycle[20].Theproposedaxisfor pelvic torsion is transverse and passes through the sym-physispubis[125],thoughthisremainsequivocal.AbnormalmobilityorinstabilityineithertheSIJorsym-physispubisoftenisaccompanied,however,byasecond-ary stress lesion in the other [69].Lumbopelvic RhythmThelumbarspineandinnominatebonescanalsomoveasaunit.Inasmuchasmovementsofthespinearecoupledwiththoseofthepelvis,alumbopelvicrhythm (discussedinChapter32),similartothescapulothoracicrhythm,hasbeenpostulated [22] (Fig. 35.38). The specific rhythm varies amongindividuals,butflexionofthetrunkfromstandingcombinesflexion of the lumbar vertebrae and at the lumbosacral junctionwith forward rotation of the pelvis on the fixed femora[3,139].Disturbancesinthelumbopelvicrhythmcancontribute to low back pain [3,121,139].Figure 35.37: Application of unbalanced forces on the pelvis, asin static one-legged stance on the left, results in asymmetrical,antagonistic movement at the SIJs along with movement at thesymphysis pubis. This type of movement can be assessed clinicallyby palpating movement of the ASIS and PSIS.A B CFigure 35.38: Common lumbopelvic rhythm. A. Normal standing posture. B. During the first 45 of trunk flexion, most motion resultsfrom lumbar and sacral flexion causing the sacrum to nutate and the lumbar curve to flatten. C. In extreme trunk flexion, the lumbarspine continues to flatten and the pelvis rotates about the femoral heads, while the sacrum paradoxically counternutates.2Oatis_CH35_620-653.qxd4/15/072:06 PMPage 646MovlmlenLo elvlco )"&$'%-/$012%3 walk,thepelvisislevelwhenbothlegsareincontactwiththeground.However,whenonelegleavestheground (swing phase), it becomes unsupported, and thepelvisonthatsidedropsslightly.Itisimpossibletodropthepelvisontheweight-bearingside.Therefore,the point of reference for lateral tilt is the unsupported254 PART III Clinical Kinesiology and Anatomy of the Trunkorlesssupportedside,orthesidefarthestfromtheweight-bearing joint axis. Figure 17-16 illustrates a leftlateraltilt.Thepersonbearsweightontherightlegwhile lifting the left leg from the ground. The left sideof the pelvis becomes unsupported and drops, or later-ally tilts to the left.NeutralASISPubic symphysisAAnterior tiltASISPubic symphysisBPosterior tiltASISPubic symphysisCFigure 17-13. Pelvic movement in the sagittal plane. (A) The anterior superior iliac spine (ASIS) and the pubic symphysisshould be in the same vertical plane. (B) Anterior tilt occurs when the pelvis tilts forward, moving the ASIS anterior to thepubic symphysis. (C) Posterior tilt occurs when the pelvis tilts backward, moving the ASIS posterior to the pubic symphysis.ASIS ASISFigure 17-14. Pelvic movement in the frontal plane. Whenstanding upright on both feet, the iliac crests and the ASISsshould be level.Figure 17-15. Lateral tilt (anterior view). One side of thepelvis moves up while the other side moves down.2363_Ch17-247-258.qxd12/10/1012:32 PMPage 254MovlmlenLo elvlco )"&$'%-/$012%3 CHAPTER 17 Pelvic Girdle 257Figure 17-20. Force couple causing posterior pelvic tilt(lateral view). The trunk flexors pulling up (anteriorly) andthe hip extensors pulling down (posteriorly) cause the pelvisto tilt posteriorly.Figure 17-21. Force couple keeps the pelvis level in thefrontal plane. In a reversal of muscle action, the left trunklateral benders pull up while the right hip abductors pulldown. This keeps the pelvis fairly level as opposed to lettingthe pelvis drop on the unsupported side.Trunk flexorsHip extensorsPelvis tilts posteriorlyRight hip abductorsPelvis remainsfairly levelLeft trunklateral bendersAnterior ViewGeneral Anatomy Questions1. What pelvic girdle motions occur in the following?a. The sagittal plane around the frontal axisb. The frontal plane around the sagittal axisc. The transverse plane around the vertical axis2. Concentric contraction of the right quadratus lum-borum would cause the pelvis to laterally tilt towhich side?3. Motion occurs at the lumbosacral joint when thepelvis tilts anteriorly and posteriorly and at whatother distal joint?4. What associated hip motion occurs when the pelvistiltsa. anteriorly?b. posteriorly?c. laterally?5. What associated hip motions occur when the leftside of the pelvis rotatesa. forward?b. backward?Review Questions(continued on next page)2363_Ch17-247-258.qxd12/10/1012:32 PMPage 257256 PART III Clinical Kinesiology and Anatomy of the TrunkTable 17-1 Associated Motions of the Pelvic Girdle, Vertebral Column, and Hip JointsPelvic Girdle Vertebral Column HipAnterior tilt Hyperextension FlexionPosterior tilt Flexion ExtensionLateral tilt (unsupported side) Lateral bending (to supported side) Adduction: weight-bearing sideAbduction: non-weight-bearing sideRotation (forward) Rotation: to opposite side Medial rotation: weight-bearing sideRotation (backward) Rotation: to opposite side Lateral rotation: weight-bearing sideBack extensorsHip flexorsPelvis tilts anteriorlyFigure 17-19. Force couple causing anterior pelvic tilt (lateral view). The trunk extensors pulling up (posteriorly)and the hip flexors anterior pulling down (anteriorly) causethe pelvis to tilt anteriorly.the left leg is weight-bearing and the right leg is swing-ing forward. Once again, the unsupported side is the point ofreference. Thisactioncausestherightsideofthepelvisto rotate forward, moving the right ASIS in front of theleft ASIS. If the right leg swung backward (Fig. 17-18C),the pelvis would rotate backward. Stated another way, ifyou bear weight on your left leg and swing your right legbackward, the right side of your pelvis rotates backward.Thispelvicrotationoccursbecausethepelvismoveson the weight-bearing hip joint. If there is right forwardrotation of the pelvis, there is left hip medial rotation (seeFig. 17-18B). Remember that hip medial rotation occursbecause the pelvis moves on the femoral head rather than,more commonly, the other way around. With right back-ward rotation of the pelvis, there is left hip lateral rotation(see Fig. 17-18C). The combinations of joint motions thatoccurduringwalkingaredescribedingreaterdetailinChapter 22. However, a summary of some of the associat-ed joint motions are listed in Table 17-1.Muscle ControlThe pelvis is moved and controlled by groups of musclesactingasforcecouples.Asthepelvistiltsintheanteri-or/posterior direction, the opposing muscle groups pro-videmovementandcontrol(Fig.17-19).Totiltthepelvisanteriorly,thelumbartrunkextensors,primarilythe erector spinae, pull up posteriorly while the hip flex-orspulldownanteriorly.Conversely,totiltthepelvisposteriorly, the abdominals pull up anteriorly while thegluteus maximus and hamstrings pull down posteriorly(Fig. 17-20). In both cases, these muscle groups are act-ingasaforcecouplebypullinginoppositedirectionsand causing the pelvis to tilt.Withoutanymuscleaction,theforceofgravitycantiltthepelvislaterallywhenthatlegbecomesunsup-ported. However, to control or limit the amount of lat-eral tilting, muscle groups on opposite sides of the bodyalso work as a force couple. Using the example shown inFigure17-21,inareversalofmuscleaction,thelefttrunklateralbenders(primarilytheerectorspinaeandquadratuslumborum)pullupontheleftsideofthepelvis,whiletherighthipabductors(gluteusmediusandminimus)pulldownontherightsidetokeepthepelvis fairly level.By preventing pelvic motion, all of these same mus-clegroupscanworktogethertoprovidestability.Pelvicandtrunkcontrolarenecessarytoprovidethestablefoundationuponwhichtheheadandextremi-ties can move.2363_Ch17-247-258.qxd12/10/1012:32 PMPage 2568angos de MovlmlenLo normal )"&$'%-/$012%3 644 Part IIII KINESIOLOGY OF THE HEAD AND SPINE Intheabsenceoftrauma,thegreatestamountofSIJmotion is present in the young, especially the young preg-nant female [12]. ThephysiologicalandclinicalsignificanceofSIJmotionhas been, in the main, ignored by all except obstetriciansand clinicians who regularly deal with SIJ syndromes.Ingeneral,threetypesofmotionareavailabletotheinnominatebones:symmetricalmotion ismovementofbothinnominatesasaunitinrelationtothesacrum;asym-metrical motion consists of antagonistic movement of eachinnominate bone with relation to the sacrum, which includesmovement at the symphysis pubis; and lumbopelvic motionconsistsofrotationofthespineandbothinnominatesasaunit around the femoral heads.Symmetrical MotionSymmetrical trunk and hip movements result in paired, sym-metricalmovementsattheSIJs[43,138,173,175].Duringtrunkflexionorbilateralhipflexion,thesacrumnutates (L.nutatio, nodding) or rotates anteriorly, so that the promontorymovesventrocaudallywhiletheapexmovesdorsocranially(Fig.35.34).Thesacrumcounternutates, ormovesintheTABLE 35.6: Movement of Sacroiliac JointAuthor(s) Method(s) Subjects Joint Motion ConclusionsPitkin andInclinometry Living subjects Unilateral antagonistic movement of the ilium around Pheasanttransverse axis through the symphysis pubis averaged 1936 11 (319), or 5.5 on each sideStrachan et al.Mechanical testing of sacralCadavers During trunk movements, sacral rotation was 151938 rotation when one ilium was immobilized and the other was fixed to the sacrumWeisl 1955 Movement of sacralLiving subjects Max ventral movement of the sacral promontory was promontory via radiography 5.6 1.4 mm with standing from recumbent Axis of angular movement was 510 cm below the sacral promontoryMennell 1960 Changes in distance betweenLiving subjects PSISs came 0.5 in. closer in horizontal planePSISs via palpationColachis et al.Measured distance betweenLiving subjects Maximum movement of PSISs was 5 mm with flexion 1963 Kirschner wires implanted in PSISs from standingThe axis was not fixedKapandji 1974 Theorized based on writings ofNone In nutation the ilia approximate and the iliac Farabeuf and Bonnaire tuberosities separateOpposite in counternutationFrigerio 1974 Biplanar radiography Cadavers andMaximum movement between ilium and sacrum was living subjects 12 mm (mean ~2.7 mm)Maximum movement between innominates was 15.5 mmEgund et al.Roentgen stereophotogrammetry Living subjectsMaximum rotation was 21978 with hypo-Axis of sacral rotation was through the iliac tuberosities or hypermobile SIJs at the level of S2Translations were ~2 mmWilder et al.Theoretical best-fit axes ofDried bonyJoint rotation cannot occur exclusively about any 1980 rotation based on topographicspecimens previously proposed axisanalysis of joint surfaces An important function of the SIJ may be to absorb energyReynolds 1980 Stereoradiography Cadaver Sacral rotations were 12Miller et al.Mechanical testing with oneCadavers Both ilia fixed: 1.9 rotation, 0.5 mm translation One ilium 1987 or both ilia fixed fixed: rotation 27.8 greater and translation3 greaterScholten et al.Biomechanical model Model Model relative pelvic motions rarely exceeded 121988 rotation and 3 mm translationSturesson et al.Stereoradiography Living subjects Mean rotation 2.5 0.51989 Mean translation 0.7 mm (0.11.6 mm)Smidt et al.Metrecom skeletal analysisLiving subjects Composite sacroiliac motion (relative motion between 1995 system R/L innominates) was 9 6.5 in oblique sagittal plane and 5 3.9 in transverse planeSmidt et al.Computed tomography Cadavers Sagittal plane sacral rotation was 781997 Translation was 48 mmPSISs, posterior superior iliac spines; SIJ, sacroiliac joint.Oatis_CH35_620-653.qxd4/15/072:06 PMPage 644En el plano sagital entre 1 a 8, con la media de 2 y 3. Traslacin caudal del sacro entre 0,5 y 8mm, con media 2-3mm 8angos de MovlmlenLo normal )"&$'%-/$012%3 0.2- 2 Grados de Rotacin 1-2 mm de traslacin Movimientos Pasivos de 7 a 8 grados 345Movement of the sacroiliac joint with special reference to the effect of loadCorrectpositioningofthepatientismandatory to achieve measurable radiographs. For example, if thelowerlimbissuperimposedonthepelvis,the markerscannotbedistinctlyvisualized.Forthis reason,onlyafewmea surableexaminationswere madeinthesittingposition.Whenanalyzingthe position with the hip maximally exed it was neces-sarytorstmaximallyexthehipandafterthat rotatethelegawayfromtheradiationbeams.A similarprocedurewasusedwhenanalyzingthe lms in the study of the effect of the external xator. InsomepatientsthesteelrodsoftheHoffmannSltis frame obscured the markers.Thesacrumwasdenedasthexedsegment andthemovementsweredescribedasrotation aroundandtranslationalongthethreeorthogonal axes, as illustrated in Fig.23.2. The rotation around the helical axis was also analyzed. The movements givenareforthecenterofgravityofthemarkers in each iliac bone. The mean error for rotation and translation was 0.10.2 and 0.1mm, respectively.Patient population of the RSA studiesIn total, 41 patients (34 women 1945 years of age, and 7 men aged 1845 years) were included in the RSA studies by Sturesson et al (1989, 1999a, 2000a, 2000b). The studies were focused on various issues butthebasicmovementanalysiswasusedinall studies to make the groups in the different studies comparable in a wider perspective. In all, 21 patients hadunilateralsacroiliacpainand20patientshad bilateralsymptoms.ThestudiesbyTullbergetal (1998) comprised 10 patients.Movement analysisSupine to standingIn the supine position the load on the SIJ is less than in the standing position, when the weight of the upper bodyistransmittedthroughtheSIJ.Consequently the sacrum was shown to rotate forwards relative to the ilia (nutation) when standing up from a supine position. AsshowninTable23.1,therotationwas equalonbothsides,andthemeanrotationwas 1.3aroundthehelicalaxis. Althoughtherotation was rather small, more than 90% of the movement occurredaroundtheX-axis.Themeanrotation around the sagittal axis (Z) and the rotation around the longitudinal axis (Y) were close to zero. The range reectsinsomecasesawideningintheposterior part of the SIJ and in other cases a closing movement (Y-axis).Thewideningorclosingpatternisalso seenaroundtheZ-axis,buttoalesserdegree. ProbablythesemovementsaroundtheY-andZ-axesreectthewidevariationintheanatomyof the SIJ (Solonen 1957). The movements around the X-axisandthehelicalaxisdidnotshowstatistical differences, thus it can be said that the innominates movearoundthesacrumasaunitorthesacrum moves symmetrically between the ilia.Supine to sittingComparedwiththemovementpatternfrom supinetostanding,themovementfromsupine tositting,botharoundthehelicalandtheX-axis showsanincreaseofabout25%.However,the most interesting observation is a small but constant inwardmovementoftheiliaccrests,notedas positivevaluesaroundtheZ-axisfortheleftside and negative values for the right (Table 23.2).Standing to prone with hyperextensionThe largest movement in the SIJ was found between the standingtopronewithhyperextension positions (Tables 23.3 and 23.4). In the prone position with hyperextension the load on the SIJ is low and incontrasttotheotherpositions,themovement ZYXFig. 23.2 The pelvis with the rotational axes.Ch23-F10178.indd 345 12/27/06 9:35:37 AM1raslacln !&.'%-/$012%3 womenfrom19to45yearsofageandfourmenfrom 18 to 45 years of age. They found only 2.5 ofinnominaterotation(coupledwith0.51.6mmoftranslation). This in vivo study was conducted in theweight-bearingposition.Sturessonetal(2000)feltthattheotherauthors(Weisl1954,1955,Colachis etal1963,Lavignolle et al 1983) had overestimatedthe mobility of the SIJ.Jacob & Kisslings (1995) findings of SIJ mobilityusingtheRSA techniquesupportedthoseofSturesson et al (1989, 2000). The average values forrotation and translation were low, being 1.8 of rota-tion (coupled with 0.7mm of translation) for the menand 1.9 of rotation (coupled with 0.9mm translation)for the women. No statistical differences were notedfor either age or gender. They postulated that morethan6 ofrotationand2mmoftranslationshouldbe considered pathologic (Jacob & Kissling 1995).In1995,Buyruketal(1995a,b)establishedthatthe Doppler imaging system could be used to meas-urestiffnessoftheSIJ.ThisresearchhasrecentlybeenrepeatedandconfirmedbyLeonieDamen et al (2002a). Doppler imaging of vibrations acrossthe SIJ has shown (Buyruk et al 1995a, b, 1997, 1999,Damen et al 2002a) that stiffness of the SIJ is variablebetween subjects and therefore the range of motionis potentially variable. This research has also revealedthat stiffness of the SIJ is symmetric when the left andright sides are compared in subjects without pelvicpainandasymmetricinsubjectswithpelvicpain.Thesestudieswillbediscussedingreaterdepthlater. In conclusion, we know that the SIJs are capableof a small amount of both angular (14) and transla-toric motion(13 mm),thattheamplitudeofthismotion is variable between subjects; however, withinone subject it should be symmetric between sides.NUTATION/COUNTERNUTATION OF THESACRUMNutationandcounternutationareosteokinematicterms that describe how the sacrum moves relativeto the innominates regardless of how the pelvic girdleis moving relative to the lumbar spine and femora.Nutationofthesacrumoccurswhenthesacralpromontory moves forward into the pelvis about acoronalaxisthroughtheinterosseousligament(Fig. 6.7). Conversely, counternutation of the sacrumoccurs when the sacral promontory moves backwardaboutthiscoronalaxis(Fig.6.8).Thesacrumiscounternutatedinsupinelying(Sturessonetal2000)andnutatesinsittingorstanding(Sturessonet al 2000). In other words, whenever an individualisvertical,thesacrumisnutatedrelativetotheinnominates.Theamountofsacralnutationdependsonhow theindividualissittingorstand-ing.Inanoptimalposture,thesacrumshouldbesuspendedbetweenthetwoinnominatesinslightnutationbutnotcompletelynutated(Levin1997).Duringtheinitialstagesofforwardorbackwardbending, the sacrum completely nutates between theinnominatesandshouldremaintherethroughoutthe full range of motion. On returning to standing, theTHE PELVIC GIRDLE 60Sacral NutationInferoposteriorGlideFigure 6.7 When the sacrum nutates, its articular surfaceglides inferoposteriorly relative to the innominate.Sacral counter-NutationAnterosuperiorGlideFigure 6.8 When the sacrum counternutates, its articularsurface glides anterosuperiorly relative to the innominate.Chap-06.qxd3/27/0412:33Page 60womenfrom19to45yearsofageandfourmenfrom 18 to 45 years of age. They found only 2.5 ofinnominaterotation(coupledwith0.51.6mmoftranslation). This in vivo study was conducted in theweight-bearingposition.Sturessonetal(2000)feltthattheotherauthors(Weisl1954,1955,Colachis etal1963,Lavignolle et al 1983) had overestimatedthe mobility of the SIJ.Jacob & Kisslings (1995) findings of SIJ mobilityusingtheRSA techniquesupportedthoseofSturesson et al (1989, 2000). The average values forrotation and translation were low, being 1.8 of rota-tion (coupled with 0.7mm of translation) for the menand 1.9 of rotation (coupled with 0.9mm translation)for the women. No statistical differences were notedfor either age or gender. They postulated that morethan6 ofrotationand2 mmoftranslationshouldbe considered pathologic (Jacob & Kissling 1995).In1995,Buyruketal(1995a,b)establishedthatthe Doppler imaging system could be used to meas-urestiffnessoftheSIJ.ThisresearchhasrecentlybeenrepeatedandconfirmedbyLeonieDamen et al (2002a). Doppler imaging of vibrations acrossthe SIJ has shown (Buyruk et al 1995a, b, 1997, 1999,Damen et al 2002a) that stiffness of the SIJ is variablebetween subjects and therefore the range of motionis potentially variable. This research has also revealedthat stiffness of the SIJ is symmetric when the left andright sides are compared in subjects without pelvicpainandasymmetricinsubjectswithpelvicpain.Thesestudieswillbediscussedingreaterdepthlater. In conclusion, we know that the SIJs are capableof a small amount of both angular (14) and transla-toric motion(13mm),thattheamplitudeofthismotion is variable between subjects; however, withinone subject it should be symmetric between sides.NUTATION/COUNTERNUTATION OF THESACRUMNutationandcounternutationareosteokinematicterms that describe how the sacrum moves relativeto the innominates regardless of how the pelvic girdleis moving relative to the lumbar spine and femora.Nutationofthesacrumoccurswhenthesacralpromontory moves forward into the pelvis about acoronalaxisthroughtheinterosseousligament(Fig. 6.7). Conversely, counternutation of the sacrumoccurs when the sacral promontory moves backwardaboutthiscoronalaxis(Fig.6.8).Thesacrumiscounternutatedinsupinelying(Sturessonetal2000)andnutatesinsittingorstanding(Sturessonet al 2000). In other words, whenever an individualisvertical,thesacrumisnutatedrelativetotheinnominates.Theamountofsacralnutationdependsonhow theindividualissittingorstand-ing.Inanoptimalposture,thesacrumshouldbesuspendedbetweenthetwoinnominatesinslightnutationbutnotcompletelynutated(Levin1997).Duringtheinitialstagesofforwardorbackwardbending, the sacrum completely nutates between theinnominatesandshouldremaintherethroughoutthe full range of motion. On returning to standing, theTHE PELVIC GIRDLE 60Sacral NutationInferoposteriorGlideFigure 6.7 When the sacrum nutates, its articular surfaceglides inferoposteriorly relative to the innominate.Sacral counter-NutationAnterosuperiorGlideFigure 6.8 When the sacrum counternutates, its articularsurface glides anterosuperiorly relative to the innominate.Chap-06.qxd3/27/0412:33Page 60LlmlLanLes del MovlmlenLo )"&$'%-/$012%3 45"%6*'" 76$ .$86$.93/ : $"&3;-*-93/ *3 3.2%6*3%-+/ "3%.'-*-3%3 1.- LrecLor Lsplnal 2.- Muludo Lumbar 3.- Crupo Muscular Abdomlnal a. Cbllcuos lnLernos y exLernos b. 8ecLos Abdomlnal c. 1ransverso abdomlnal 4.- lsquloublales aLrones de 8ecluLamlenLo 4$%1/-%3 46"%6*3. lnLeraccln de 1orques 4$%1/-%3 46"%6*3. Apllcacln de ConoclmlenLos Adqulrldos