Inmunoterapia aplicada al linfoma no Hodgkin · Inmunoterapia aplicada al linfoma no Hodgkin...
54
Transcript of Inmunoterapia aplicada al linfoma no Hodgkin · Inmunoterapia aplicada al linfoma no Hodgkin...


Inmunoterapia aplicada al linfoma no Hodgkin
Andrés LópezServicio de Hematología
Hospital Universitario Vall d’Hebron

1. Monoclonal antibodies2. Antibody-drug conjugates3. Bispecific monoclonal antibodies:
Bispecific T-cell engager (BiTE), and Dual Affinity Re-Targeting (DART)
4. CAR T-cells5. Immune checkpoints inhibitors

Antibodies, modified T-cells, and immune check points blockade

Monoclonal antibodies

Anti-CD20 antibodies Type Comments
Rituximab I First in human
Ofatumumab I Approved by FDA in cases of CLL in whichFludarabine is not appropriate
Veltuzumab I Exibits a greatter CDCIn FL previously exposed to Rituximab, ORR of 44% and CR of 27%In FL no previously exposed to Rituximab, ORR of 57% and CR of 43%
LY469298 I 13-20 fold higher affinity to CD20 thanRituximabIt is active in patients carrying FcyRIIIa alleleIn FL with this allele the ORR was 22-50% in a phase I trial
Obinutuzumab II In november 2013 FDA approved fortreatment of CLL in combination withChlorambucil (ORR:78%, CD 21%)
Monoclonal antibodies

Other antibodies Phase Lymphoma Response
Epratuzumab(anti-CD22)
I/II R/R FLR/R DLBCL
ORR: 24%ORR: 15%
Epratuzumab + Rituximab
II R/R B-NHL
1stLine FL
ORR: 67% CR: (60% in FL, 50% in DLBCL)
ORR: 88%
MEDI-551(anti-CD19)
I/II R/R B-NHL ORR: 24%
Lucatumumab(anti-CD40)
I/II R/R B-NHL ORR in FL: 33%ORR in DLBCL: 11%
Dacetumumab(anti-CD40) + R-Gemcitabine
II R/R DLBCL ORR: 47%CR: 20%
Monoclonal antibodies

Antibody-drug conjugates

Antibody(Target)
Ph. Lymphoma N Response DoR (median) PFS (median) OS (median)
PolatuzumabVedotin(CD22)
I/II R/R B-NHL 95 ORR: 19%CR: 7%
- - -
InutuzumabOzogamicin(CD22)
I R/R B-NHL 79 ORR: 38%CR: 15%
- FL: 317 daysDLBCL: 49 days
FL: NRDLBCL: 193 d.
SAR3419(CD19) +Maitensina
I/II R/R B-NHL 42 ORR: 30%CR: 15%
10 m (5-77) - -
BrentuximabVedotin(CD30)
II R/R ALTCL 58 ORR: 86%CR: 57%
- 13.3 m. NR
Conjugated monoclonal antibodies

Antibodies(Target)
Phase Lymphoma N Response PFS (median) OS (median)
InutuzumabOzogamicin(CD22) +Rituximab(CD20)
I/II R/R B-NHL 119 FL(ORR:87%, CR: 62%)DLBCL (ORR:74%, CR: 50%)Refr./Agrs.(ORR:20%, CR: 3%)
FL: NR
DLBCL: 17.1 m.
Refr./Agrs.: 1.9 m.
FL: NR
DLBCL: NR
Refr./Agrs.: 8.8 m.
Milatumumab(CD74) +Vetuzumab(CD20 type 2)
I/II R/R B-NHL 34 ORR: 24%CR: 6%
2 m. 16 m.
Monoclonal antibodies combinations

Bispecific monoclonal antibodies


BiTE vs DART
Moore et al. Blood, 2011; 117: 4142-51

Blinatumumab (ant CD19 x CD3) in NHL: Final analysis
1. Nagorsen et al. Leuk lymphoma 2009. 2. Goebeler et al. JCO 2016. 3. Viardot et al. Blood 2016
Disease Phase Dosing n Results Reference
R/R NHL/CLL
I Rapid infusion 13 µg/Kg 3 t/w
22 No responses Nagorsen(1)
R/R NHL I CI: 0.5-90 µg/Kg for 4-8 w
76 ORR: 69%(DLBCL: 55%)
Goebeler(2)
R/R DLBCL II CI: 112 µg/Kg for 4-8 w
25 ORR: 43%CR: 19%
Viardot(3)

Blinatumumab (ant CD19 x CD3) in NHL: Safety
AE Frequency (%)
Pyrexia 62
Headache 36
Peripheral edema 25
Febrile Neutropenia 25
Nausea 25
Hypokalemia 23
Rash 21
Tremor 20
Constipation 20
AE with a frequency < 20%
Pneumonia
Tremor
Device-related infections
Encephalopathy
Confusion
Leukoencephalopathy: mainly in patients with previous radiotherapy and chemotherapy used to CNS

Phase I76 patientsmAge: 65 (20-80) years
Histology:DLBCL: 14iNHL: 52Other: 10
Blinatumumab (BiTE: CD19xCD3) in R/R NHL
Goebeler et al. JCO 2016; 34: 1104-11
Medication with Prednisolone and/or Dexamethasone
MTD: 60 mg/m2/day n CR PR
DLBCL 11 4 2
FL 15 6 6
MCL 7 3 2

CAR T-cells

CAR T-cell therapy (ant CD19).First reported “on the road”
Centers: City of Hope, Baylor, Pennsylvania University, MSKCC, NCI, Children Hospital Philadelphia, Fred Hutchinson, BMC, Beijing, MDACC
TTR/P (Weeks)
FL 2 Refractory4 Relapsed
No response2 PR 7 - 18+
DLBCL 5 Relapsed No response
SLL/CLL 15 Relapsed 3 CR5 PR
2+ - 15+

CAR T-cell therapy in LPS

Anti-CD19 CAR T-cells in R/R B-cell NHL
Kochenderfer et al. Haematologica 2016; 101: s1 (#S792)
22 patients
Histology:- DLBCL: 19- FL: 2- MCL: 1
Lymphodepletiontherapy with:Cyclophosphamide + Fludarabine
Response DLBCL (n=19) FL (n=2) MCL (n=1)
CR 8 2 1
PR 5
ORR 13 2 1
DoR: 1-20 months (with 10 in ongoing CR)
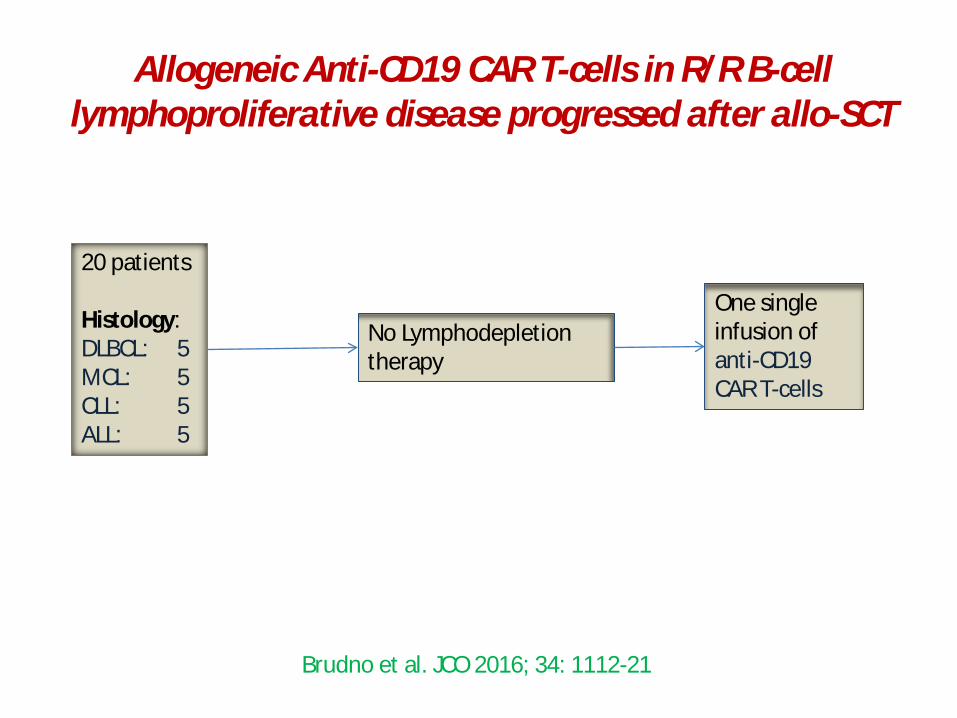
20 patients
Histology:DLBCL: 5MCL: 5CLL: 5ALL: 5
No Lymphodepletiontherapy
One single infusion of anti-CD19 CAR T-cells
Allogeneic Anti-CD19 CAR T-cells in R/R B-cell lymphoproliferative disease progressed after allo-SCT
Brudno et al. JCO 2016; 34: 1112-21

Allogeneic Anti-CD19 CAR T-cells in R/R B-cell lymphoproliferative disease progressed after allo-SCT
CR: 6 (30%)PR: 2 (10%)SD: 7 (35%)
DoR (m): 1-30+
NO new onset of
GVHD in any case was
seen
Brudno et al. JCO 2016; 34: 1112-21
In ALL 4/5 cases CR with MRD neg.

Allogeneic Anti-CD19 CAR T-cells in R/R B-cell lymphoproliferative disease progressed after allo-SCT
Brudno et al. JCO 2016; 34: 1112-21
- CD8 CAR T-cells expressing PD1 increased form 12% at time of infusion to 82% at peak blood CAR T-cells
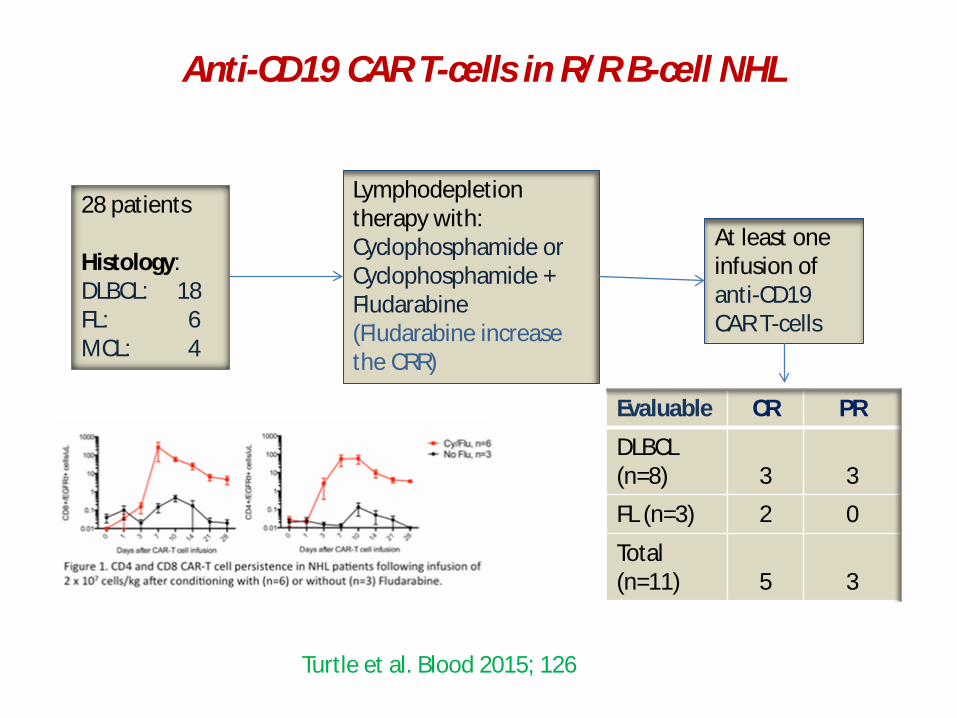
Anti-CD19 CAR T-cells in R/R B-cell NHL
Turtle et al. Blood 2015; 126
28 patients
Histology:DLBCL: 18FL: 6MCL: 4
Lymphodepletiontherapy with:Cyclophosphamide or Cyclophosphamide + Fludarabine(Fludarabine increase the CRR)
At least one infusion of anti-CD19 CAR T-cells
Evaluable CR PR
DLBCL (n=8) 3 3
FL (n=3) 2 0
Total (n=11) 5 3

Central memory derived CD19 specific T-cell after ASCT in High-risk B-NHL
Popplewell et al. Blood 2015; 126
Phase I studyTwo types:
NHL1: CD8pos. Tcm (derived CD19;zeta T-cells)NHL2: CD4/CD8 pos.Tcm (derived CD19R;zeta/EGFR pos. T-cells)
NHL1:mAge: 62 (50-75) yearsm prior lines: 3 (2-4)
Histology:-DLBCL: 7- MCL: 1
NHL2:mAge: 58 (23-71) yearsm prior lines: 2 (1-3)
Histology:-DLBCL: 4- MCL: 4

Central memory derived CD19 specific T-cell after ASCT in High-risk B-NHL
Popplewell et al. Blood 2015; 126
NHL1 CR PFS Progression
DLBCL (n=7)MCL (n=1)
5 (62.5%) 50% @1 & 2 y.(mFU: > 2y.)
4 (50%)
NHL2 CR PFS Progression
DLBCL (n=4)MCL (n=3)
8 (100%)100% @ 6 m. (mFU: > 1y.)
2 (25%)@6.4 & 12.6 m.
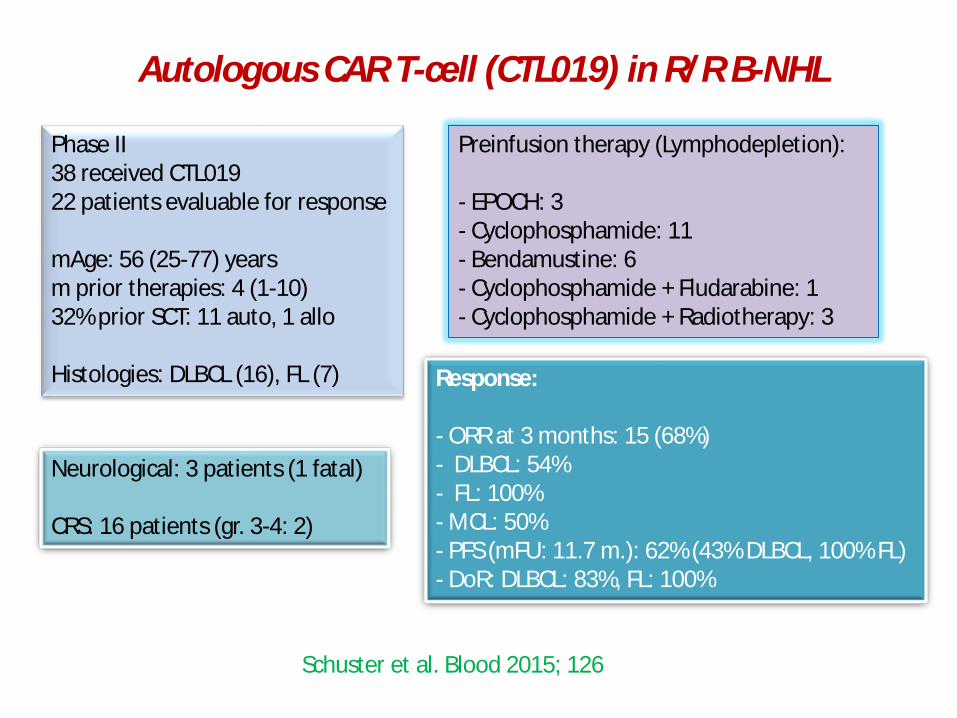
Autologous CAR T-cell (CTL019) in R/R B-NHL
Schuster et al. Blood 2015; 126
Phase II38 received CTL01922 patients evaluable for response
mAge: 56 (25-77) yearsm prior therapies: 4 (1-10)32% prior SCT: 11 auto, 1 allo
Histologies: DLBCL (16), FL (7)
Neurological: 3 patients (1 fatal)
CRS: 16 patients (gr. 3-4: 2)
Response:
- ORR at 3 months: 15 (68%)- DLBCL: 54%- FL: 100%- MCL: 50%- PFS (mFU: 11.7 m.): 62% (43% DLBCL, 100% FL)- DoR: DLBCL: 83%, FL: 100%
Preinfusion therapy (Lymphodepletion):
- EPOCH: 3- Cyclophosphamide: 11- Bendamustine: 6- Cyclophosphamide + Fludarabine: 1- Cyclophosphamide + Radiotherapy: 3

High-dose chemotherapy à ASCTà CAR (19-28z CAR T-cells) in R/R aggressive B-cell NHL
Schuster et al. Blood 2015; 126
Phase I6 patientsmAge: 61 (34-68) years
Histologies: DLBCL (3), tFL (2 -1 DH-), tMZL (1)
CRS in 2 patients
Outcome:(@ mFU of 6 months)
-All in CR (2 with > 2 years)

Two syndromes:
- Cytokine release syndrome (CRS)- Macrophage activation syndrome (MAS)
It is possible that IL6 is produced by dying B-cells, dying tumor cells or activated macrophages
Two questions:
- Correlates with the antitumor activity?- The use of anti-IL6 and corticosteroids can affect the
antitumor response?
Reversible Neurotoxicity: Obtundation, seizures, aphasia, mental status changes
CAR T-cells toxicity

Challanges for CAR T-cells1. Exhaustion due to excessive TCR signaling
2. 20% of ALL develops resistance due to loss of CD19 epitope
3. Immuneresponse induced by CAR’s can lead to a rejection of CD19 CAR’s
4. Side effects:a) CRS, associated with tumor burdenb) Neuropathy (encephalopathy, seizures, focal motors
deficits, aphasia) c) B-cell aplasia
5. Technical graft failure
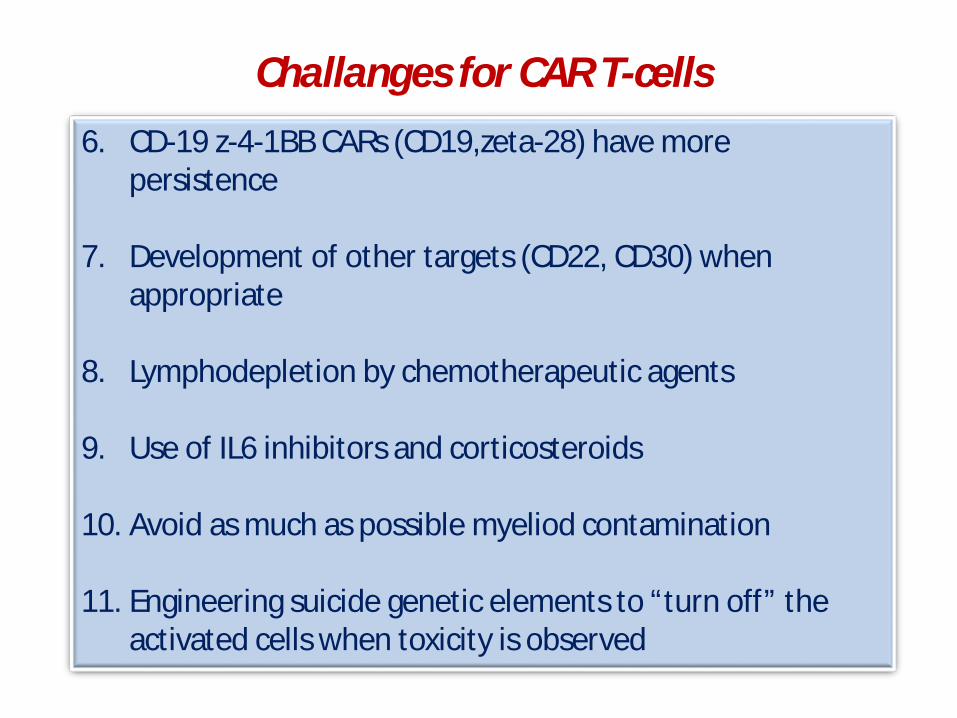
Challanges for CAR T-cells6. CD-19 z-4-1BB CARs (CD19,zeta-28) have more
persistence
7. Development of other targets (CD22, CD30) when appropriate
8. Lymphodepletion by chemotherapeutic agents
9. Use of IL6 inhibitors and corticosteroids
10. Avoid as much as possible myeliod contamination
11. Engineering suicide genetic elements to “turn off” the activated cells when toxicity is observed

A. CARs are susceptible to PD1-PDL1 interactions. So, CARs in combination with PD1 blockade is testing together in clinical trials
B. Need for universal CARs (UCAR): allogeneic donors based on knockdown of the HLA genes coupled with enforced expression of non-classical HLA molecules to avoid NK recognition and lysis
CAR T-cells challanges

Immune checkpoints inhibitors
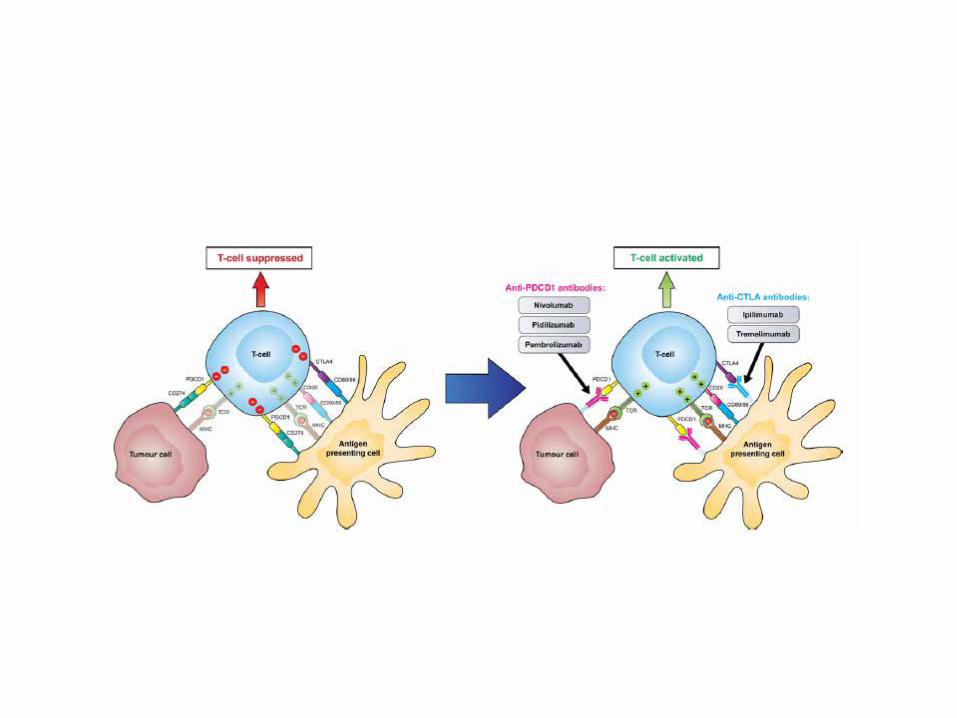

Potential activity of anti-PD1 in lymphoma
B-cell lymphomas:
Ø PMBCLØ THRBCLØ EBV-associated B-cell lymphomaØ PlasmablasticØ Primary effussionØ Primary testicularØ Primary CNSØ PTLD
T-cell lymphomas:
Ø FTH lymphomas (including AIBL)Ø Cutaneous T-cellØ S. SezaryØ Primary cutaneous CD4+ small-cellØ Double negative MFØ ALK+ anaplasticØ T/NK nasal type

Pidilizumab in relapsed Follicular Lymphomaa
Westing et al. Lancet Oncol, 2014; 15: 69-77
Patient’s characteristics Toxicity
§Phase II trial§32 patients

Westing et al. Lancet Oncol, 2014; 15: 69-77
Response
Pidilizumab in relapsed Follicular Lymphomaa

Westing et al. Lancet Oncol, 2014; 15: 69-77
FLIPI1
FLIPI2
Outcome
Pidilizumab in relapsed Follicular Lymphomaa

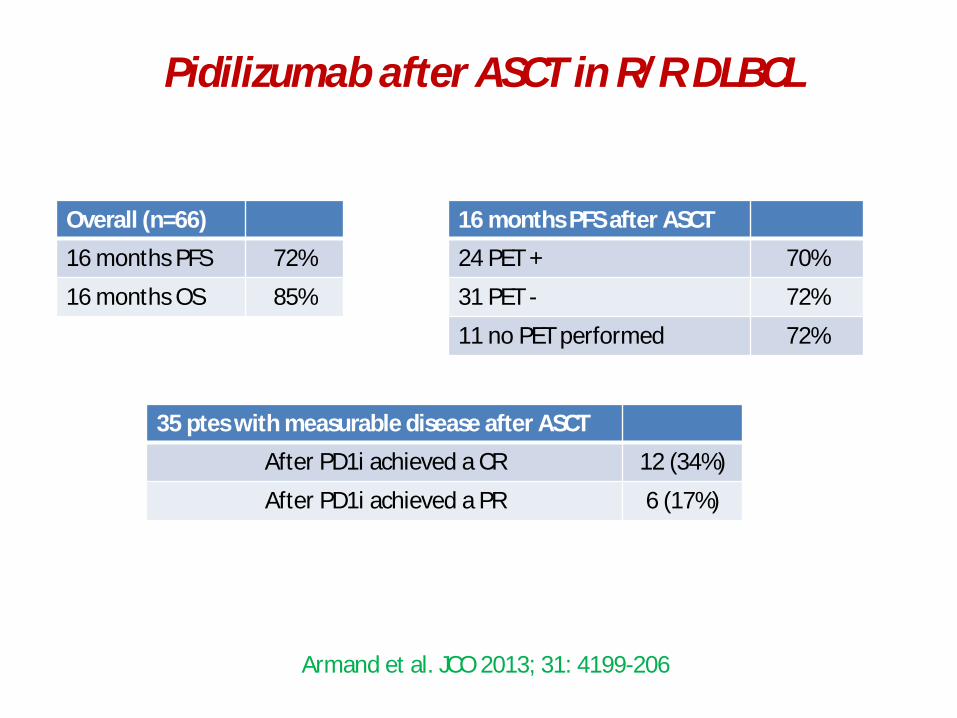
Pidilizumab after ASCT in R/R DLBCL
Armand et al. JCO 2013; 31: 4199-206
Phase IIR/R DLBCL66 patientsmAge: 57 (19-80)
Histologies:- DLBCL: 49- tFL: 13- PMLBCL: 4
Toxicity
Pidilizumab after ASCT in R/R DLBCL
Armand et al. JCO 2013; 31: 4199-206
Overall (n=66)
16 months PFS 72%
16 months OS 85%
16 months PFS after ASCT
24 PET + 70%
31 PET - 72%
11 no PET performed 72%
35 ptes with measurable disease after ASCT
After PD1i achieved a CR 12 (34%)
After PD1i achieved a PR 6 (17%)

All patients (n=97) Patients who remain PET positive after salvage treatment (n=24)
Armand et al. JCO 2013; 31: 4199-206
Pidilizumab after ASCT in R/R DLBCL

Westin et al. Lancet Oncol, 2014; 15: 69-77
Phase IIN = 30
Toxicity
Pidilizumab + Rituximab in R/R FL

Westin et al. Lancet Oncol, 2014; 15: 69-77
Responses (n=29)
CR 15 (52%)
PR 4 (14%)FLIPI1
FLIPI2
Pidilizumab + Rituximab in R/R FL

Lesokhin al. Blood, 2015; 126 (ASH)
Phase I studyies of Nivolumab in R/R lymphoid malignancies
Tumor N Complete Response
n (%)
Partial Responsen (%)
Stable Disease(SD)n (%)
Progression Free Survival Rate at 24
Weeks (%)Diffuse Large B Cell Lymphoma (DLBCL)
11 1 (9) 3 (27) 3 (27) (24)
Follicular Lymphoma (FL)
10 1 (10) 3 (30) 6 (60) (68)
Other B Cell Lymphoma
8 0 0 5 (63) (38)
Primary Mediastinal B Cell Lymphoma
2 0 0 2 (100) (0)
Mycosis Fungoides (MF)
13 0 2 (15) 9 (69) (39)
Peripheral T Cell Lymphoma (PTCL)
5 0 2 (40) 0 (30)
Other T Cell Lymphoma
5 0 0 1 (20) (0)
Dose: 1-3 mg/Kg w1/w4 and every 3w

Zinzani al. Haematologica, 2016; 101; s1 (#S797)
Phase I16 patientsmAge: 30 (22-62) years44% ≥ 4 lines75% Radiotherapy
Outcome (n=10) Results
CR 6%
ORR 37.5%
More frequent toxicity grade 1-2:- Diarrhea- Artralgia- Edema- PyrexiaNo grade 3-5 AEs
With a median FU of 5 months (0.8-22) 5 patients continue on response (0.03+ to 17+ months)
Pembrolizumab in R/R PMBCL

Kawano et al. Intern Med, 2016; 55: 1439-45
Refractory ATLL (HTLV-1)Phase II14 ptes (10 acute)Dose: 1 mg/Kg
Response (n=14) After 4 cycles After 8 cycles
CR 6 (43%) 6 (43%)
PR 3 (21%) 0
ORR 9 (64%) 6 (43%)
Mogamulizumab (anti-CCR4) in R/R ATLL

Tokunaga et al. Blood, 2015; 126
Refractory ATLL (HTLV-1)Phase II77 patientsmAge: 65.6 (44-83) yearsDose: 1 mg/Kg
Outcome (n=77) Results
CR 18 (23%)
PR 15 (19%)
ORR 33 (43%)
mOS 7.7 months (5-11)
3 y. OS 18%
More frequent initial therapy:- VCAP-AMP-VECP: 41- CHOP: 19
Mogamulizumab (anti-CCR4) in R/R ATLL

Ansell et al. Clin Cancer Res, 2009; 15: 6446-53
18 patients3à1 Mg/Kg x 3 doses
Response (n=14) %
CR 5.6
ORR 11
Ipilimumab (anti-CCR4) in R/R B-NHL

Houot et al. Oncoimmunology, 2012; 1: 957-8
Anti-CD137 stimulatory antibody
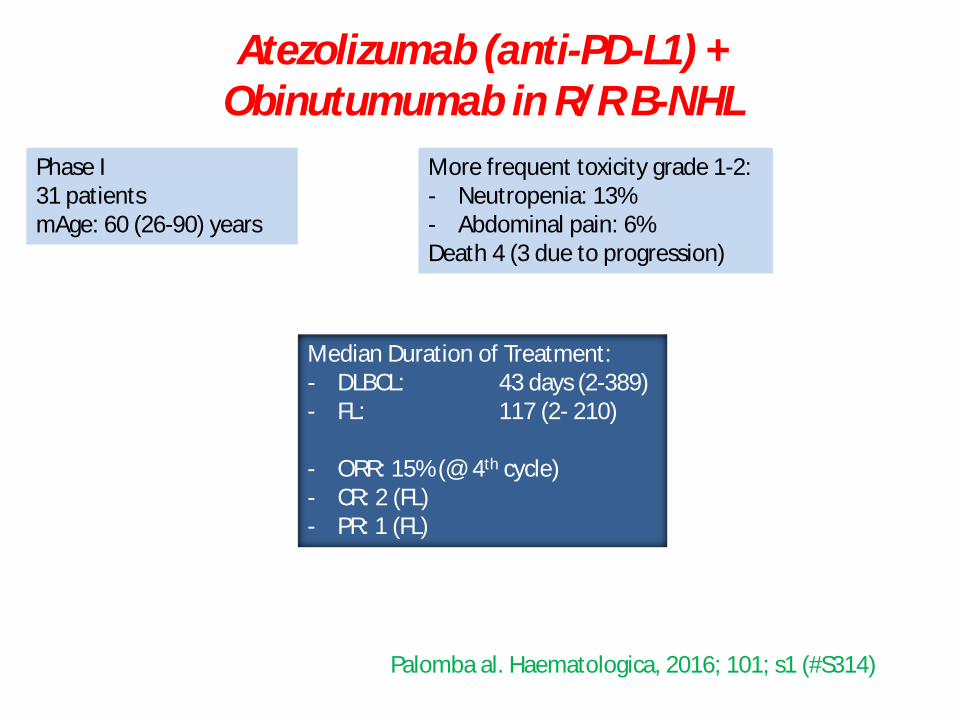
Palomba al. Haematologica, 2016; 101; s1 (#S314)
Phase I31 patientsmAge: 60 (26-90) years
More frequent toxicity grade 1-2:- Neutropenia: 13%- Abdominal pain: 6%Death 4 (3 due to progression)
Median Duration of Treatment: - DLBCL: 43 days (2-389)- FL: 117 (2- 210)
- ORR: 15% (@ 4th cycle)- CR: 2 (FL)- PR: 1 (FL)
Atezolizumab (anti-PD-L1) + Obinutumumab in R/R B-NHL
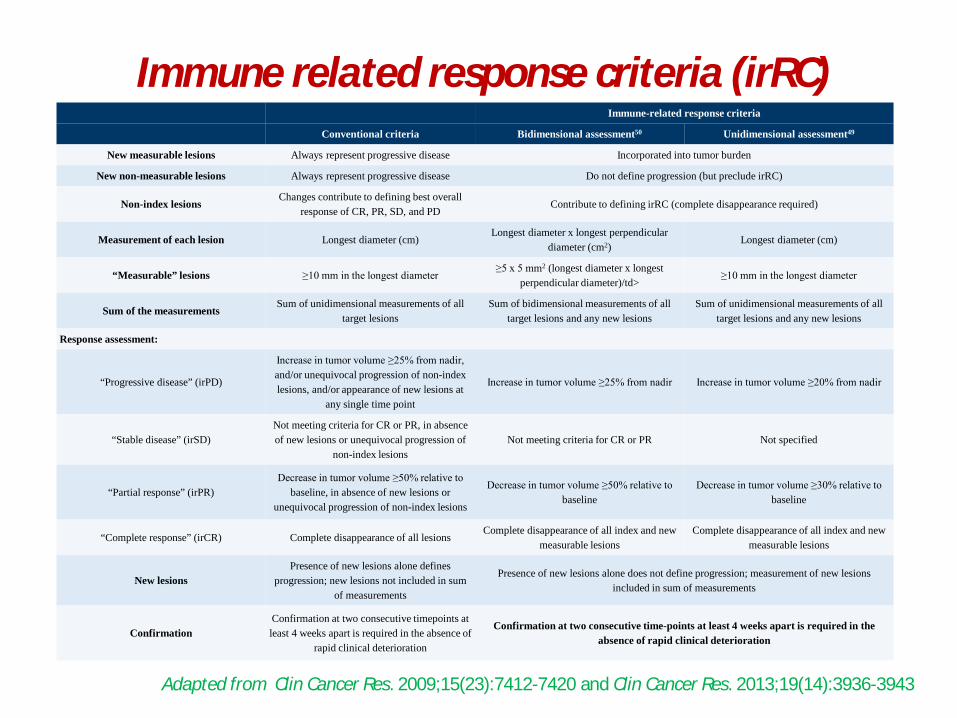
Immune related response criteria (irRC)Immune-related response criteria
Conventional criteria Bidimensional assessment50 Unidimensional assessment49
New measurable lesions Always represent progressive disease Incorporated into tumor burden
New non-measurable lesions Always represent progressive disease Do not define progression (but preclude irRC)
Non-index lesionsChanges contribute to defining best overall
response of CR, PR, SD, and PDContribute to defining irRC (complete disappearance required)
Measurement of each lesion Longest diameter (cm)Longest diameter x longest perpendicular
diameter (cm2)Longest diameter (cm)
“Measurable” lesions ≥10 mm in the longest diameter≥5 x 5 mm2 (longest diameter x longest
perpendicular diameter)/td>≥10 mm in the longest diameter
Sum of the measurementsSum of unidimensional measurements of all
target lesionsSum of bidimensional measurements of all
target lesions and any new lesionsSum of unidimensional measurements of all
target lesions and any new lesions
Response assessment:
“Progressive disease” (irPD)
Increase in tumor volume ≥25% from nadir, and/or unequivocal progression of non-index lesions, and/or appearance of new lesions at
any single time point
Increase in tumor volume ≥25% from nadir Increase in tumor volume ≥20% from nadir
“Stable disease” (irSD)Not meeting criteria for CR or PR, in absence of new lesions or unequivocal progression of
non-index lesionsNot meeting criteria for CR or PR Not specified
“Partial response” (irPR)Decrease in tumor volume ≥50% relative to
baseline, in absence of new lesions or unequivocal progression of non-index lesions
Decrease in tumor volume ≥50% relative to baseline
Decrease in tumor volume ≥30% relative to baseline
“Complete response” (irCR) Complete disappearance of all lesionsComplete disappearance of all index and new
measurable lesionsComplete disappearance of all index and new
measurable lesions
New lesionsPresence of new lesions alone defines
progression; new lesions not included in sum of measurements
Presence of new lesions alone does not define progression; measurement of new lesions included in sum of measurements
ConfirmationConfirmation at two consecutive timepoints at least 4 weeks apart is required in the absence of
rapid clinical deterioration
Confirmation at two consecutive time-points at least 4 weeks apart is required in the absence of rapid clinical deterioration
Adapted from Clin Cancer Res. 2009;15(23):7412-7420 and Clin Cancer Res. 2013;19(14):3936-3943


Summary
Wow!!!

Thanks a lot…
for your attention!