Inmunologia de la HTA.pdf

of 6
Transcript of Inmunologia de la HTA.pdf
-
8/11/2019 Inmunologia de la HTA.pdf
1/6
doi:10.1152/advan.00063.201338:20-24, 2014.Advan in Physiol EduDaniel W. Trott and David G. HarrisonThe immune system in hypertension
You might find this additional info useful...
59 articles, 23 of which can be accessed free at:This article cites
/content/38/1/20.full.html#ref-list-1
1 other HighWire hosted articlesThis article has been cited by
[PDF][Full Text]2014; 129 (25): 2629-2632.Circulation
Francesca Seta and Richard A. CohenThe Endothelium: Paracrine Mediator of Aortic Dissection
including high resolution figures, can be found at:Updated information and services
/content/38/1/20.full.html
can be found at:Advances in Physiology EducationaboutAdditional material and information
http://www.the-aps.org/publications/advan
This information is current as of September 5, 2014.
American Physiological Society. ISSN: 1043-4046, ESSN: 1522-1229. Visit our website at http://www.the-aps.org/.December by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright 2014 by the
courses and in the broader context of general biology education. It is published four times a year in March, June, September andis dedicated to the improvement of teaching and learning physiology, both in specializedAdvances in Physiology Education
http://-/?-http://circ.ahajournals.org/content/129/25/2629.full.pdfhttp://circ.ahajournals.org/content/129/25/2629.full.htmlhttp://circ.ahajournals.org/content/129/25/2629.full.pdfhttp://circ.ahajournals.org/content/129/25/2629.full.htmlhttp://-/?-http://www.the-aps.org/publications/advanhttp://www.the-aps.org/publications/advanhttp://-/?-http://circ.ahajournals.org/content/129/25/2629.full.pdfhttp://circ.ahajournals.org/content/129/25/2629.full.htmlhttp://-/?- -
8/11/2019 Inmunologia de la HTA.pdf
2/6
Refresher Course
The immune system in hypertension
Daniel W. Trott and David G. Harrison
Division of Clinical Pharmacology, Department of Medicine, Vanderbilt University School of Medicine, Nashville, Tennessee
Submitted 13 June 2013; accepted in final form 20 December 2013
Trott DW, Harrison DG. The immune system in hypertension. AdvPhysiol Educ 38: 20 24, 2014; doi:10.1152/advan.00063.2013.Whilehypertension has predominantly been attributed to perturbations of thevasculature, kidney, and central nervous system, research for almost50 yr has shown that the immune system also contributes to thisdisease. Inflammatory cells accumulate in the kidneys and vasculatureof humans and experimental animals with hypertension and likelycontribute to end-organ damage. We and others have shown that micelacking adaptive immune cells, including recombinase-activatinggene-deficient mice and rats and mice with severe combined immu-nodeficiency have blunted hypertension to stimuli such as ANG II,high salt, and norepinephrine. Adoptive transfer of T cells restores theblood pressure response to these stimuli. Agonistic antibodies to theANG II receptor, produced by B cells, contribute to hypertension in
experimental models of preeclampsia. The central nervous systemseems important in immune cell activation, because lesions in theanteroventral third ventricle block hypertension and T cell activationin response to ANG II. Likewise, genetic manipulation of reactiveoxygen species in the subfornical organ modulates both hypertensionand immune cell activation. Current evidence indicates that theproduction of cytokines, including tumor necrosis factor-, interleu-kin-17, and interleukin-6, contribute to hypertension, likely via effectson both the kidney and vasculature. In addition, the innate immunesystem also appears to contribute to hypertension. We propose aworking hypothesis linking the sympathetic nervous system, immunecells, production of cytokines, and, ultimately, vascular and renaldysfunction, leading to the augmentation of hypertension. Studies ofimmune cell activation will clearly be useful in understanding thiscommon yet complex disease.
T cell; cytokines; angiotensin; subfornical organ; costimulation
IN THE1960S, a role for the immune system in the developmentof hypertension was first discovered. Several recent investiga-tions have further defined the role of immune system, partic-ularly the adaptive immune system, in hypertension, providednovel insights into the genesis of hypertension, and identifiednovel targets for the treatment of hypertension. The purpose ofthis review was to summarize recent discoveries by our labo-ratory and others on the role of the immune system in hyper-tension.
Early Studies in Immunity and Hypertension
The concept that the immune system contributes to hyper-tension had its genesis in the 1960s, when Grollman et al. (40,56) demonstrated that immunosuppression blunted hyperten-sion in a model of renal infarction and that transfer of lym-phocytes from rats with renal infarction induced hypertensionin previously nonhypertensive animals. Later, Svenson foundthat hypertension was not maintained in thymectiomized or
athymic nude mice with renal infarction (46). In the 1980s, Baet al. (2) found that transplanting the thymus from a Wistar-Kyoto (WKY) rat to a spontaneously hypertensive rat (SHR)resulted in a decrease in blood pressure in the SHR (2). Bloodpressure was also lowered in SHRs with treatment by eitheranti-thymocyte serum or the immunosuppressive drug cyclo-phosphamide (5, 12). Nerve growth in the thymus of SHR wasfound to be greater than that of WKY rats, suggesting a neuralcomponent of immune cell activation in hypertension (42).Rodruiguez-Iturbe et al. (43) found that immunsupression withmycophenlate mofetil blunted salt-induced hypertension afterANG II infusion. In the early 2000s, Muller and Luft (35, 36,49) conducted a series of investigations showing that NF-B
and ROS play roles in ANG II-induced end-organ damage.More recently, advances in genetic mouse models and knowl-edge of immunology prepared the way for discoveries thatwould lead to further understanding of the importance of theimmune system in hypertension.
T Cells and Hypertension
In 2007, our laboratory (18) published a study demonstratingthat T cells contribute to the development of hypertension. Inthis study, mice lacking recombinase-activating gene 1 (Rag-1/ mice) were used as these mice cannot generate functionalT cell receptors or B cell antibodies and thus lack both T andB lymphocytes. The increase in blood pressure caused by
either ANG II or DOCA salt was significantly blunted inRag-1/ mice, suggesting that either T or B cells mediateovert hypertension. Rag-1/ mice did not exhibit increasedvascular superoxide production and endothelial dysfunction.The hypertensive response to ANG II was restored whenRag-1/ mice received adoptive transfer of T cells but not Bcells. In wild-type mice, ANG II increased circulating CD69,CCR5, and CD44high T cells, markers of effector memory Tcells. In addition, T cells accumulated in the perivascularadipose tissue of the aorta. The results of this study indicatethat T cells play a major role in hypertension. Supporting therole of T cells in hypertension, severe combined immunodefi-cieny mice have also been shown to be protected againsthypertension and exhibit reduced albuminuria and renal dam-age (10). Recently, Mattson et al. (32) deleted the Rag1 gene inDahl salt-sensitive rat using zinc finger nuclease technologyand have shown that this attenuates blood pressure, albumin-uria, and kidney damage. Thus, T cells seem to contribute tothe development of various forms of hypertension in differentstrains of mice and in rats.
Role of the Central Nervous System in Immune-MediatedHypertension
The blood vessels, kidney, and central nervous system(CNS) have all been shown to contribute to the development ofhypertension. Interestingly, T cells may represent a link be-
Address for reprint requests and other correspondence: D. G. Harrison,Division of Clinical Pharmacology, Dept. of Medicine, Robinson ResearchBldg., Rm. 536, Vanderbilt Univ., Nashville, TN 37232-6602 (e-mail: [email protected]).
Adv Physiol Educ 38: 2024, 2014;doi:10.1152/advan.00063.2013.
20 1043-4046/14 Copyright 2014 The American Physiological Society
-
8/11/2019 Inmunologia de la HTA.pdf
3/6
tween these tissues. Lymphoid tissues are rich in sympatheticnerves (14). Ganta et al. (17) have shown that intracerebroven-tricular infusion of ANG II increased sympathetic nerve activ-ity to the spleen and increased expression of multiple cytokinesin the spleen. Our laboratory has preformed a series of inves-tigations on the role of the CNS in mediating T cell activation.
The circumventricular organs (CVO) are highly vascularized
and have an incomplete blood-brain barrier and can thereforebe influenced by circulating hormones like ANG II. In addi-tion, the CVO, and in particular, the subfornical organ (SFO),are important in both sending and receiving central signals thatregulate cardiovascular function and electrolyte balance. De-letion of CVO extracellular (ec)SOD, using Cre-lox technol-ogy, provides a model to determine the role of central oxidativestress in hypertension. ecSOD deletion increased ROS levels inthe CVO, increased heart low-frequency to high-frequencyheart rate variability (indicative of increased sympathetic ner-vous activity), and elevated blood pressure (25). In addition,when mice with ecSOD deleted in the CVO were infused withANG II at a dose that does not cause hypertension in normalmice (140 ngkg1min1), blood pressure was significantlyelevated and was accompanied by aortic T cell infiltration.Interestingly, in a separate investigation, when ecSOD wasspecifically deleted in vascular smooth muscle, despite in-creases in vascular ROS, blood pressure and T cell responseswere not altered compared with controls (27).
NADPH oxidases are major sources of superoxide anionproduction in mammalian cells. The subunit p22phox mediatestrafficking of NADPH oxidase catalytic subunits to the cellmembrane and is required for enzyme complex assembly and,ultimately, superoxide production. Complementing the studiesthat used deletion of ecSOD, our laboratory (26) also deletedp22phox in the SFO in a similar manner. Deletion of p22phox inthe SFO blunted the pressor response to ANG II and decreased
sympathetic outflow as assessed by heart rate variability. Inaddition, p22phox deletion abolished ANG II-induced aortic Tcell infiltration. This study is in keeping with findings thatintracerebroventricular injections of a superoxide scavengerreduces sympathetic drive, blood pressure, and renal damage insalt-induced hypertension in rats (16).
Supporting the role of the central nervous system, lesions inthe anteroventral third cerebral ventricle (AV3V), a regionwhich includes the SFO, can prevent ANG II-induced hyper-tension (7, 30). In addition, AV3V lesions protect against Tcell activation and aortic infiltration in response to ANG II(30). This is of particular importance as it demonstrates thatANG II-induced T cell activation is not due to direct actions ofANG II on T cells but rather that central signals are required
for T cell activation. Interestingly, mice infused with norepi-nephrine become hypertensive and exhibit T cell activation andaortic infiltration even after AV3V lesions. This supports theconcept that sympathetic drive, and its attendant release ofnorepinephrine, likely mediates T cell activation and hyperten-sion. In addition to the important role of the CNS, peripheralmechanisms appear to also contribute to T cell activation andvascular inflammation. Treatment with the vasodilator hydral-zine to normalize blood pressure prevents T cell activation andvascular inflammation induced by ANG II infusion (30). Thissuggests that T cells may respond to elevations in pressure andthat afferent nerves may activate central mechanisms in afeedforward manner to induce CVO oxidative stress, sympa-
thetic outflow, further T cell activation, and overt hypertension.More recently, T cells have been shown to contribute tostress-induced hypertension (31). We exposed mice to 7 daysof stress using a combination of restraint and cage switching.This stress paradigm resulted in increased blood pressure,activation of circulating T cells, and aortic T cell infiltration.Rag-1/ mice were protected from stress-induced hyperten-
sion, and adoptive transfer of T cells restored the hypertensiveresponse. These findings underscore the crucial role of theCNS in orchestrating the T cell response leading to hyperten-sion.
T Cell Subtypes, Cytokines, and Mechanisms of Activation
The above studies demonstrated that T cells contribute to thedevelopment of hypertension; however, they do not provideextensive insights into the subsets of T cells involved. CD4 Tcells have been generally classified as either T helper (Th)1 orTh2, depending on their activation markers and cytokine pro-duction (34). Th17 cells are a newly characterized subset of Tcells; these cells produce the cytokine IL-17 and contribute to
numerous autoimmune diseases, obesity, and cardiovasculardisease (13, 48, 57). To investigate the role of IL-17 inhypertension, our group studied IL-17a/ mice. These miceexhibited a similar initial increase in blood pressure as wild-type mice in response to ANG II; however, after 7 days, bloodpressure dropped in IL-17a/ mice (28). The ANG II-inducedaortic T cell infiltration observed in wild-type mice was abol-ished in IL-17a/ mice, as were increases in vascular oxida-tive stress and endothelial dysfunction. Recent reports haveshown that direct infusion of IL-17a mediated hypertensionand endothelial dysfunction in mice (37) and that IL-17 medi-ated placental oxidative stress, resulting in hypertension duringpregnancy in rats (11).
In addition to IL-17, other cytokines have been implicated inthe pathogenesis of hypertension. Etanrecept, a TNF- antag-onist, is effective in preventing hypertension (18, 50, 52). IL-6knockout mice are also protected from ANG II-induced hyper-tension (6, 24, 45). Interferon (IFN)- is upregulated in thekidneys of hypertensive mice (10), and inhibition of IFN-prevents ANG II-induced end-organ damage (29). Taken to-gether, these observations suggest that hypertension is medi-ated by multiple proinflammatory T cell subsets. In accordancewith this concept, T regulatory (Tregs) cells, which act torestrain proinflammatory T cells, attenuate hypertension-in-duced end-organ damage in mice (22) and blunt hypertensionin rats (53).
Classically, T cells require two signals for activation: 1) interaction
of the T cell receptor with an antigen presented in the contextof a major histocompatibilty complex and 2) stimulation ofcostimulatory molecules on the T cell by ligands on theantigen-presenting cell (1). A major costimulatory molecule onT cells is CD28, which is bound by the B7 ligands CD80 andCD86 of the antigen-presenting cell. Ligation of the T cellreceptor in the absence of costimulation leads to T cell apo-ptosis (15). The pharmacological agent CTLA4-Ig inhibitscostimulation by binding to B7 ligands on antigen-presentingcells. To determine whether costimulation plays a role inhypertension, our laboratory used both pharmacological inhi-bition of costimulation with CTLA4-Ig and a genetic approachwith B7-deficient (B7/) mice. CTLA4-Ig treatment blunted
Refresher Course
21IMMUNE CELLS AND HYPERTENSION
Advances in Physiology Education doi:10.1152/advan.00063.2013 http://advan.physiology.org
-
8/11/2019 Inmunologia de la HTA.pdf
4/6
blood pressure, T cell activation, and vascular infiltration inboth ANG II- and DOCA salt-induced hypertension (54).CTLA4-Ig treatment also abolished T cell production ofTNF- and IFN- induced by ANG II. Similar results wereobserved in B7/ mice, which lack B7 ligands. These obser-vations suggest that T cell receptor ligation and costimulationare necessary for T cell activation in hypertension.
The Innate Immune System and Hypertension
The role of the adaptive immune system in experimentalhypertension has been well characterized; however, less isknown about the role of the innate immune system. Recently,Abboud et al. (19) demonstrated that, in WKY rats, the chole-neric agonist nicotine results in an anti-inflammatory responsein splenic macrophages; in contrast, nicotine induced a proin-flammatory response in macrophages from SHRs and enhancedToll-like receptor-mediated cytokine release. In addition,perivascular macrophage infiltration has been observed in ex-perimental hypertension in mice (3). Inflammatory cytokines,IL-1, and IL-6 are elevated in SHRs compared with WKY
rats; this can be reversed by treatment with an angiotensin-converting enzyme inhibitor (33). Similarly, ANG II receptorblockade prevented lipopolysaccharide-induced inflammatoryresponses of innate immune cells in the rat spleen (44). Inhumans, white blood cells from essential hypertensive patientsproduced more IL-1and IL-6 when stimulated with lipopoly-saccharide compared with controls (41). These observationsare consistent with monocyte activation in hypertension. Howthe innate and adaptive immune systems interact in the devel-opment of hypertension is not well understood and is animportant topic for future study.
The Immune System and Preeclampsia
Preeclampsia is characterized by the onset of hypertensionduring pregnancy accompanied by proteinuriea. Preeclampsiais associated with the production of autoantibodies that stim-ulate the ANG II type 1 (AT1) receptor (55), and infusion ofthese antibodies can induce preeclampsia-like symptomps inpregnant mice (60). More recently, it has been shown that aspecific subset of B cells produces these antibodies (21).Depletion of B cells using the anti-CD20 antibody rituximabblunts the blood pressure response in the reduced uterineperfusion pressure rat model of preeclampsia (23). Adoptivetransfer of CD4 T cells from reduced uterine perfusionpressure rats to normal pregnant rats results in increased bloodpressure (39). This response is blunted by either rituximab orAT1 antagonism, suggesting an important role of cross-talk
between T and B cells in preeclampsia. Supporting the role ofT cells in preeclampsia, mice deficient in the cytokines IL-4 orIL-10, which skew T cells to an anti-inflammatory phenotype,develop preeclampsia-like symptoms when pregnant (8, 9).The proinflammatory cytokine IL-17 mediates placental oxi-dative stress and increases in blood pressure in pregnant rats(11). Together, these observations support a role for the adap-tive immune system in preeclampsia where T and B cells act ina synergistic manner.
Pulmonary Hypertension and the Immune System
It has long been postulated that autoimmunity and inflam-mation is involved in pulmonary hypertension (38). In addi-
tion, T cells, B cells, and macrophages are present in the lungsof patients with pulmonary hypertension (51). Recently, a roleof anti-inflammatory Tregs cells has been indentified in exper-imental pulmonary hypertension (47). In this study, in responseto VEGF receptor 2 antagonism, athymic rats, which lack Tcells, developed perivascular inflammation, including infiltra-tion of B cells and macrophages in the lung and pulmonary
hypertension. The authors then reconstituted different T cellsubsets in these animals and found that CD4 Tregscells actedto blunt pulmonary vascular inflammation and the developmentof pulmonary hypertension. In a similar manner, Tregs cellsappear to act to restrain experimental systemic hypertension inboth mice and rats (3, 22, 53).
The Immune System in Human Hypertension
Although the majority of studies implicating the immunesystem in hypertension have been performed in experimentalanimals, a limited number of investigations have examined therole of the immune system in human hypertension. IL-6 andTNF- are positively correlated with blood pressure in humans
(4). In a small study, patients with either rheumatoid arthritis orpsoriasis who also had essential hypertension were treated withmycophenlate mofetil, resulting in significantly lowered sys-tolic and diastolic blood pressure (20). Recently, circulatingproinflammatory CD8 T cells have been indentified in hyper-tensive patients (58). These cells generate IFN- and TNF-and exhibit loss of CD28 and gain of CD57, which is consistentwith a proinflammatory, senescent T cell phenotype. Thesepatients also exhibited increased circulating chemokines,which serve as T cell attractants.
Conclusions and Future Directions
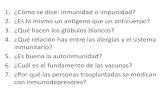
In summary, it has been known for almost 50 yr that immunecells contribute to hypertension; in the last several years,investigations from our group and others have demonstratedthe importance of T cells in the development of hypertension.In light of the data discussed here, we have formulated aworking hypothesis for the development of overt hypertension.As shown in Fig. 1, hypertensive stimuli, such as ANG II orsalt, leads to an initial elevation in blood pressure, consistent
T cell
Hypertensive stimuli
ANG II, salt, stress, aldosterone
CNS inflammation and
oxidative stress
Vasoconstriction
Vascular hypertrophy
Sympathetic outflow
Sodium
Volume Retention
Pre-hypertension - Barotrauma
Neoantigen formation and
presentation by dendritic cells
Severe hypertension
Fig. 1. Working hypothesis describing the role of immune cells in hyperten-sion. CNS, central nervous system.
Refresher Course
22 IMMUNE CELLS AND HYPERTENSION
Advances in Physiology Education doi:10.1152/advan.00063.2013 http://advan.physiology.org
-
8/11/2019 Inmunologia de la HTA.pdf
5/6
with clinical prehypertension, which results in protein mod-ifications, possibly due to oxidative modifications. These al-tered proteins serve as neoantigens that no longer recognized asself, are processed and presented by dendritic cells, and pro-mote T cell activation. In concert, afferent signals to the CNSresult in increased sympathetic outflow contributing to T cellactivation. Activated T cells infiltrate the kidney and vascula-
ture and produce cytokines that promote renal Na
and waterretention and, in the vasculature, vasoconstriction and remod-eling. Together, these alterations result in overt hypertension.The observation that hydralizine treatment abolished the T cellresponse suggests that signals from the periphery operate in afeedforward manner to signal the CNS to increase centralsympathetic drive and mediate overt hypertension. An impor-tant point is that the T cell response is independent of themodel of experimental hypertension, T cell responses havebeen observed in mice in response to ANG II, DOCA salt, andnorepinephrine. In rats, this response has been observed in bothsalt-sensitive and genetic models. Emphasizing this point is therecent study of Zhang et al. (59), where ANG II receptors werespecifically deleted in mouse T cells using Cre-lox technology.These mice were not protected against ANG II-induced hyper-tension, and, surprisingly, kidney damage in response to ANGII was exacerbated (59). These observations indicate that the Tcell response in hypertension is independent of direct actions ofANG II on T cells. We believe, based on the studies of theCNS, that central signals mediate T cell activation in a varietyof hypertension models. Recent observations by Abboud et al.(19) have suggested that central signals regulate the innateimmune system in hypertension as well. It should be noted thatthe model for the immue system in hypertension outlined hereis a working hypothesis; the precise mechanisms, particularlythe initiating factors in the development of hypertension, are asyet unknown. Our hypothesis will almost certainly require
refinement as new information comes available.
DISCLOSURES
No conflicts of interest, financial or otherwise, are declared by the author(s).
AUTHOR CONTRIBUTIONS
Author contributions: D.W.T. and D.G.H. conception and design of re-search; D.W.T. and D.G.H. prepared figures; D.W.T. and D.G.H. draftedmanuscript; D.W.T. and D.G.H. approved final version of manuscript.
REFERENCES
1. Abbas AK, Lichtman AH, Pillai S.Cellular and Molecular Immunology.Philadelphia, PA: Saunders Elsevier, 2007, p. viii.
2. Ba D, Takeichi N, Kodama T, Kobayashi H. Restoration of T celldepression and suppression of blood pressure in spontaneously hyperten-
sive rats (SHR) by thymus grafts or thymus extracts. J Immunol 128:12111216, 1982.
3. Barhoumi T, Kasal DA, Li MW, Shbat L, Laurant P, Neves MF,Paradis P, Schiffrin EL. T regulatory lymphocytes prevent angiotensinII-induced hypertension and vascular injury. Hypertension 57: 469476,2011.
4. Bautista LE, Vera LM, Arenas IA, Gamarra G. Independent associa-tion between inflammatory markers (C-reactive protein, interleukin-6, andTNF-) and essential hypertension. J Hum Hypertens19: 149154, 2005.
5. Bendich A, Belisle EH, Strausser HR. Immune system modulation andits effect on the blood pressure of the spontaneously hypertensive male andfemale rat. Biochem Biophys Res Commun 99: 600607, 1981.
6. Brands MW, Banes-Berceli AK, Inscho EW, Al-Azawi H, Allen AJ,Labazi H. Interleukin 6 knockout prevents angiotensin II hypertension:role of renal vasoconstriction and janus kinase 2/signal transducer andactivator of transcription 3 activation. Hypertension 56: 879 884, 2010.
7. Brody M, Fink G, Buggy J, Haywood J, Gordon F, Knuepfer M, MowM, Mahoney L, Johnson A. Critical role of the anteroventral thirdventricle (AV3V) region in development and maintenance of experimentalhypertension.Perspect Nephrol Hypertens 6: 7684, 1979.
8. Chatterjee P, Chiasson VL, Kopriva SE, Young KJ, Chatterjee V,Jones KA, Mitchell BM. Interleukin 10 deficiency exacerbates toll-likereceptor 3-induced preeclampsia-like symptoms in mice.Hypertension58:489496, 2011.
9. Chatterjee P, Kopriva SE, Chiasson VL, Young KJ, Tobin RP,Newell-Rogers K, Mitchell BM. Interleukin-4 deficiency induces mildpreeclampsia in mice. J Hypertens 31: 14141423, 2013.
10. Crowley SD, Song YS, Lin EE, Griffiths R, Kim HS, Ruiz P. Lym-phocyte responses exacerbate angiotensin II-dependent hypertension. Am
J Physiol Regul Integr Comp Physiol298: R1089R1097, 2010.11. Dhillion P, Wallace K, Herse F, Scott J, Wallukat G, Heath J, Mosely
J, Martin JN Jr, Dechend R, LaMarca B. IL-17-mediated oxidativestress is an important stimulator of AT1-AA and hypertension duringpregnancy. Am J Physiol Regul Integr Comp Physiol 303: R353R358,2012.
12. Dzielak DJ. Immune mechanisms in experimental and essential hyper-tension.Am J Physiol Regul Integr Comp Physiol 260: R459 R467, 1991.
13. Eid RE, Rao DA, Zhou J, Lo SF, Ranjbaran H, Gallo A, Sokol SI,Pfau S, Pober JS, Tellides G. Interleukin-17 and interferon- are pro-duced concomitantly by human coronary artery-infiltrating T cells and actsynergistically on vascular smooth muscle cells. Circulation 119: 1424
1432, 2009.14. Felten DL, Livnat S, Felten SY, Carlson SL, Bellinger DL, Yeh P.
Sympathetic innervation of lymph nodes in mice. Brain Res Bull 13:693699, 1984.
15. Frauwirth KA, Thompson CB.Activation and inhibition of lymphocytesby costimulation. J Clin Invest109: 295299, 2002.
16. Fujita M, Ando K, Kawarazaki H, Kawarasaki C, Muraoka K, OhtsuH, Shimizu H, Fujita T. Sympathoexcitation by brain oxidative stressmediates arterial pressure elevation in salt-induced chronic kidney disease.
Hypertension59: 105112, 2012.17. Ganta CK, Lu N, Helwig BG, Blecha F, Ganta RR, Zheng L, Ross CR,
Musch TI, Fels RJ, Kenney MJ. Central angiotensin II-enhanced spleniccytokine gene expression is mediated by the sympathetic nervous system.
Am J Physiol Heart Circ Physiol 289: H1683H1691, 2005.18. Guzik TJ, Hoch NE, Brown KA, McCann LA, Rahman A, Dikalov S,
Goronzy J, Weyand C, Harrison DG. Role of the T cell in the genesisof angiotensin II induced hypertension and vascular dysfunction. J Exp
Med204: 24492460, 2007.19. Harwani SC, Chapleau MW, Legge KL, Ballas ZK, Abboud FM.
Neurohormonal modulation of the innate immune system is proinflamma-tory in the prehypertensive spontaneously hypertensive rat, a geneticmodel of essential hypertension. Circ Res 111: 11901202, 2012.
20. Herrera J, Ferrebuz A, MacGregor EG, Rodriguez-Iturbe B. Myco-phenolate mofetil treatment improves hypertension in patients with pso-riasis and rheumatoid arthritis. J Am Soc Nephrol 17: S218225, 2006.
21. Jensen F, Wallukat G, Herse F, Budner O, El-Mousleh T, Costa SD,Dechend R, Zenclussen AC. CD19CD5 cells as indicators of pre-eclampsia.Hypertension 59: 861868, 2012.
22. Kvakan H, Kleinewietfeld M, Qadri F, Park JK, Fischer R, SchwarzI, Rahn HP, Plehm R, Wellner M, Elitok S, Gratze P, Dechend R, LuftFC, Muller DN. Regulatory T cells ameliorate angiotensin II-inducedcardiac damage. Circulation 119: 29042912, 2009.
23. LaMarca B, Wallace K, Herse F, Wallukat G, Martin JN Jr, Weimer
A, Dechend R. Hypertension in response to placental ischemia duringpregnancy: role of B lymphocytes. Hypertension 57: 865871, 2011.24. Lee DL, Sturgis LC, Labazi H, Osborne JB Jr, Fleming C, Pollock JS,
Manhiani M, Imig JD, Brands MW. Angiotensin II hypertension isattenuated in interleukin-6 knockout mice. Am J Physiol Heart CircPhysiol 290: H935H940, 2006.
25. Lob HE, Marvar PJ, Guzik TJ, Sharma S, McCann LA, Weyand C,Gordon FJ, Harrison DG. Induction of hypertension and peripheralinflammation by reduction of extracellular superoxide dismutase in thecentral nervous system. Hypertension 55: 277283, 2010.
26. Lob HE, Schultz D, Marvar PJ, Davisson RL, Harrison DG. Role ofthe NADPH oxidases in the subfornical organ in angiotensin II-inducedhypertension.Hypertension 61: 382387, 2013.
27. Lob HE, Vinh A, Li L, Blinder Y, Offermanns S, Harrison DG. Roleof vascular extracellular superoxide dismutase in hypertension.Hyperten-sion58: 232239, 2011.
Refresher Course
23IMMUNE CELLS AND HYPERTENSION
Advances in Physiology Education doi:10.1152/advan.00063.2013 http://advan.physiology.org
-
8/11/2019 Inmunologia de la HTA.pdf
6/6
28. Madhur MS, Lob HE, McCann LA, Iwakura Y, Blinder Y, Guzik TJ,Harrison DG. Interleukin 17 promotes angiotensin II-induced hyperten-sion and vascular dysfunction. Hypertension 55: 500507, 2010.
29. Marko L, Kvakan H, Park JK, Qadri F, Spallek B, Binger KJ,Bowman EP, Kleinewietfeld M, Fokuhl V, Dechend R, Muller DN.Interferon- signaling inhibition ameliorates angiotensin II-induced car-diac damage. Hypertension 60: 14301436, 2012.
30. Marvar PJ, Thabet SR, Guzik TJ, Lob HE, McCann LA, Weyand C,Gordon FJ, Harrison DG. Central and peripheral mechanisms of T-lym-phocyte activation and vascular inflammation produced by angiotensinII-induced hypertension. Circ Res 107: 263270, 2010.
31. Marvar PJ, Vinh A, Thabet S, Lob HE, Geem D, Ressler KJ, HarrisonDG. T lymphocytes and vascular inflammation contribute to stress-dependent hypertension. Biol Psychiatry 71: 774782, 2012.
32. Mattson DL, Lund H, Guo C, Rudemiller N, Geurts AM, Jacob H.Genetic mutation of recombination activating gene 1 in Dahl salt-sensitiverats attenuates hypertension and renal damage. Am J Physiol Regul IntegrComp Physiol 304: R407R414, 2013.
33. Miguel-Carrasco JL, Zambrano S, Blanca AJ, Mate A, Vazquez CM.Captopril reduces cardiac inflammatory markers in spontaneously hyper-tensive rats by inactivation of NF-B. J Inflamm (Lond) 7: 21, 2010.
34. Mosmann TR, Cherwinski H, Bond MW, Giedlin MA, Coffman RL.Two types of murine helper T cell clone. I. Definition according to profilesof lymphokine activities and secreted proteins. J Immunol 136: 23482357, 1986.
35. Muller DN, Dechend R, Mervaala EM, Park JK, Schmidt F, FiebelerA, Theuer J, Breu V, Ganten D, Haller H, Luft FC. NF-B inhibitionameliorates angiotensin II-induced inflammatory damage in rats. Hyper-tension35: 193201, 2000.
36. Muller DN, Mervaala EM, Schmidt F, Park JK, Dechend R, GenerschE, Breu V, Loffler BM, Ganten D, Schneider W, Haller H, Luft FC.Effect of bosentan on NF-B, inflammation, and tissue factor in angio-tensin II-induced end-organ damage. Hypertension 36: 282290, 2000.
37. Nguyen H, Chiasson VL, Chatterjee P, Kopriva SE, Young KJ,Mitchell BM. Interleukin-17 causes Rho-kinase-mediated endothelialdysfunction and hypertension. Cardiovasc Res 97: 696704, 2013.
38. Nicolls MR, Taraseviciene-Stewart L, Rai PR, Badesch DB, VoelkelNF. Autoimmunity and pulmonary hypertension: a perspective. Eur Re-spir J26: 11101118, 2005.
39. Novotny SR, Wallace K, Heath J, Moseley J, Dhillon P, Weimer A,Wallukat G, Herse F, Wenzel K, Martin JN Jr, Dechend R, LamarcaB. Activating autoantibodies to the angiotensin II type I receptor play an
important role in mediating hypertension in response to adoptive transferof CD4 T lymphocytes from placental ischemic rats. Am J Physiol Regul
Integr Comp Physiol 302: R1197R1201, 2012.40. Okuda T, Grollman A. Passive transfer of autoimmune induced hyper-
tension in the rat by lymph node cells. Tex Rep Biol Med25: 257264,1967.
41. Peeters AC, Netea MG, Janssen MC, Kullberg BJ, Van der Meer JW,Thien T. Pro-inflammatory cytokines in patients with essential hyperten-sion.Eur J Clin Invest31: 3136, 2001.
42. Purcell ES, Gattone VH, 2nd. Immune system of the spontaneouslyhypertensive rat. I. Sympathetic innervation. Exp Neurol 117: 44 50,1992.
43. Rodriguez-Iturbe B, Pons H, Quiroz Y, Gordon K, Rincon J, ChavezM, Parra G, Herrera-Acosta J, Gomez-Garre D, Largo R, Egido J,
Johnson RJ. Mycophenolate mofetil prevents salt-sensitive hypertensionresulting from angiotensin II exposure. Kidney Int 59: 22222232, 2001.
44. Sanchez-Lemus E, Benicky J, Pavel J, Larrayoz IM, Zhou J, Baliova
M, Nishioku T, Saavedra JM. Angiotensin II AT1 blockade reduces the
lipopolysaccharide-induced innate immune response in rat spleen. Am JPhysiol Regul Integr Comp Physiol 296: R1376R1384, 2009.
45. Schrader LI, Kinzenbaw DA, Johnson AW, Faraci FM, Didion SP.IL-6 deficiency protects against angiotensin II induced endothelial dys-function and hypertrophy. Arterioscler Thromb Vasc Biol27: 2576 2581,2007.
46. Svendsen UG. The role of thymus for the development and prognosis ofhypertension and hypertensive vascular disease in mice following renalinfarction. Acta Pathol Microbiol Scand A 84: 235243, 1976.
47. Tamosiuniene R, Tian W, Dhillon G, Wang L, Sung YK, Gera L,Patterson AJ, Agrawal R, Rabinovitch M, Ambler K, Long CS,
Voelkel NF, Nicolls MR. Regulatory T cells limit vascular endothelialinjury and prevent pulmonary hypertension. Circ Res109: 867 879, 2011.
48. Tesmer LA, Lundy SK, Sarkar S, Fox DA. Th17 cells in human disease.Immunol Rev223: 87113, 2008.
49. Theuer J, Dechend R, Muller DN, Park JK, Fiebeler A, Barta P,Ganten D, Haller H, Dietz R, Luft FC. Angiotensin II induced inflam-mation in the kidney and in the heart of double transgenic rats. BMCCardiovasc Disord2: 3, 2002.
50. Tran LT, MacLeod KM, McNeill JH. Chronic etanercept treatmentprevents the development of hypertension in fructose-fed rats. Mol Cell
Biochem330: 219228, 2009.51. Tuder RM, Groves B, Badesch DB, Voelkel NF.Exuberant endothelial
cell growth and elements of inflammation are present in plexiform lesionsof pulmonary hypertension. Am J Pathol 144: 275285, 1994.
52. Venegas-Pont M, Manigrasso MB, Grifoni SC, LaMarca BB, MaricC, Racusen LC, Glover PH, Jones AV, Drummond HA, Ryan MJ.
Tumor necrosis factor- antagonist etanercept decreases blood pressureand protects the kidney in a mouse model of systemic lupus erythemato-sus.Hypertension 56: 643649, 2010.
53. Viel EC, Lemarie CA, Benkirane K, Paradis P, Schiffrin EL. Immuneregulation and vascular inflammation in genetic hypertension. Am JPhysiol Heart Circ Physiol 298: H938H944, 2010.
54. Vinh A, Chen W, Blinder Y, Weiss D, Taylor WR, Goronzy JJ,Weyand CM, Harrison DG, Guzik TJ.Inhibition and genetic ablation ofthe B7/CD28 T-cell costimulation axis prevents experimental hyperten-sion.Circulation 122: 25292537, 2010.
55. Wallukat G, Homuth V, Fischer T, Lindschau C, Horstkamp B,Jupner A, Baur E, Nissen E, Vetter K, Neichel D, Dudenhausen JW,Haller H, Luft FC. Patients with preeclampsia develop agonistic auto-antibodies against the angiotensin AT1 receptor. J Clin Invest103: 945952, 1999.
56. White FN, Grollman A. Autoimmune factors associated with infarctionof the kidney. Nephron 1: 93102, 1964.
57. Winer S, Paltser G, Chan Y, Tsui H, Engleman E, Winer D, DoschHM. Obesity predisposes to Th17 bias. Eur J Immunol 39: 26292635,2009.
58. Youn JC, Yu HT, Lim BJ, Koh MJ, Lee J, Chang DY, Choi YS, LeeSH, Kang SM, Jang Y, Yoo OJ, Shin EC, Park S. ImmunosenescentCD8 T cells and C-X-C chemokine receptor type 3 chemokines areincreased in human hypertension. Hypertension 62: 126133, 2013.
59. Zhang JD, Patel MB, Song YS, Griffiths R, Burchette J, Ruiz P,Sparks MA, Yan M, Howell DN, Gomez JA, Spurney RF, CoffmanTM, Crowley SD. A novel role for type 1 angiotensin receptors on Tlymphocytes to limit target organ damage in hypertension. Circ Res 110:16041617, 2012.
60. Zhou CC, Zhang Y, Irani RA, Zhang H, Mi T, Popek EJ, Hicks MJ,Ramin SM, Kellems RE, Xia Y. Angiotensin receptor agonistic autoan-tibodies induce pre-eclampsia in pregnant mice. Nat Med 14: 855862,
2008.
Refresher Course
24 IMMUNE CELLS AND HYPERTENSION
Advances in Physiology Education doi:10.1152/advan.00063.2013 http://advan.physiology.org