Hodgkin lymphoma presentation
93
-
Upload
mostafa-selim -
Category
Health & Medicine
-
view
523 -
download
4
Transcript of Hodgkin lymphoma presentation
Lymphoma ???
Hetrogenous group of lymphoproliferative malignancies.
It results from clonal expansion from B, T, or NKcells .
85-90% derived from B-cell.
Variable clinical presentation (asymptomatic→medical emergency).
Hodgkin Lymphoma ???
It is the most commen childhood cancer (15-19 Y).
It was named after Thomas hodgkin (1832).
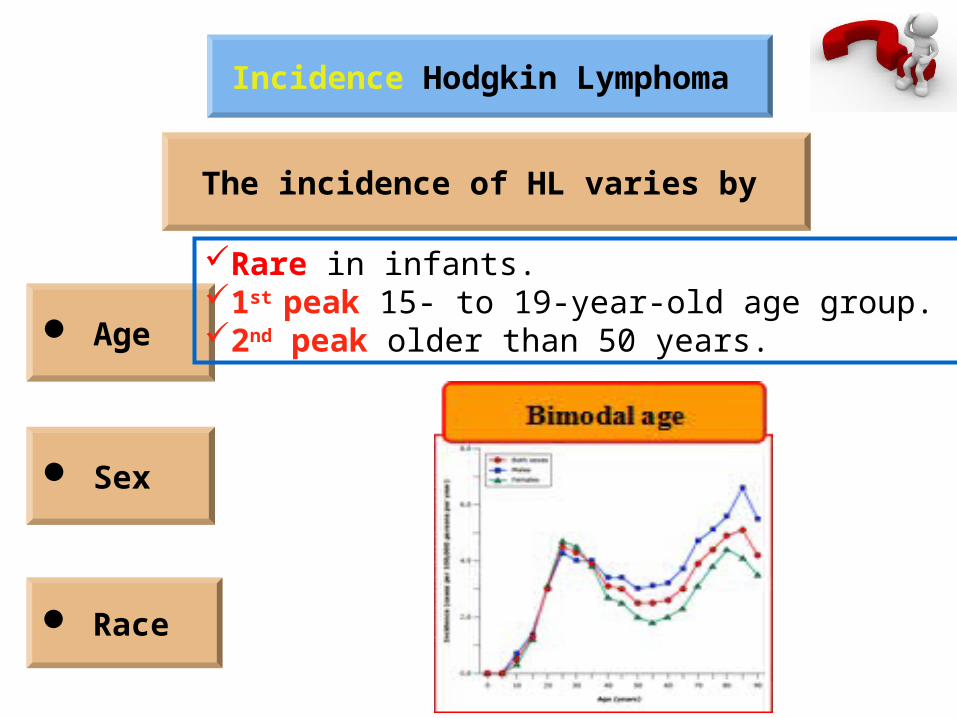
Incidence Hodgkin Lymphoma
The incidence of HL varies by
Age
Sex
Race
Rare in infants. 1st peak 15- to 19-year-old age group. 2nd peak older than 50 years.
Incidence Hodgkin Lymphoma
The incidence of HL varies by
Age
Sex
Race
In adolescents is greater in females than in males.Under age 15 boys have higher incidence than girls.
Incidence Hodgkin Lymphoma
The incidence of HL varies by
Age
Sex
Race
Younger than 10 years the incidence of HL is similar among white and African American children. Older than 10 years is increased among white children (ratio of 1.4:1).
Incidence Hodgkin Lymphoma
Familial HL
It has been estimated to represent 4.5 % of all cases of HL.
This familial association may include:
Shared environmental factors,
Exposure to viruses, and
Genetic including inherited immunodeficiency states.
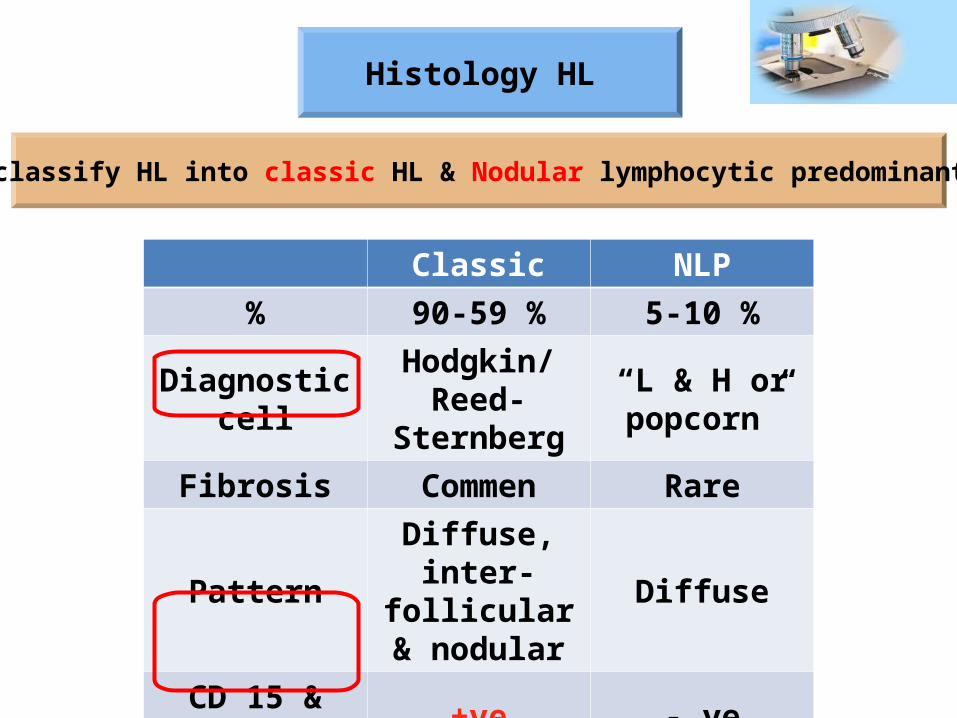
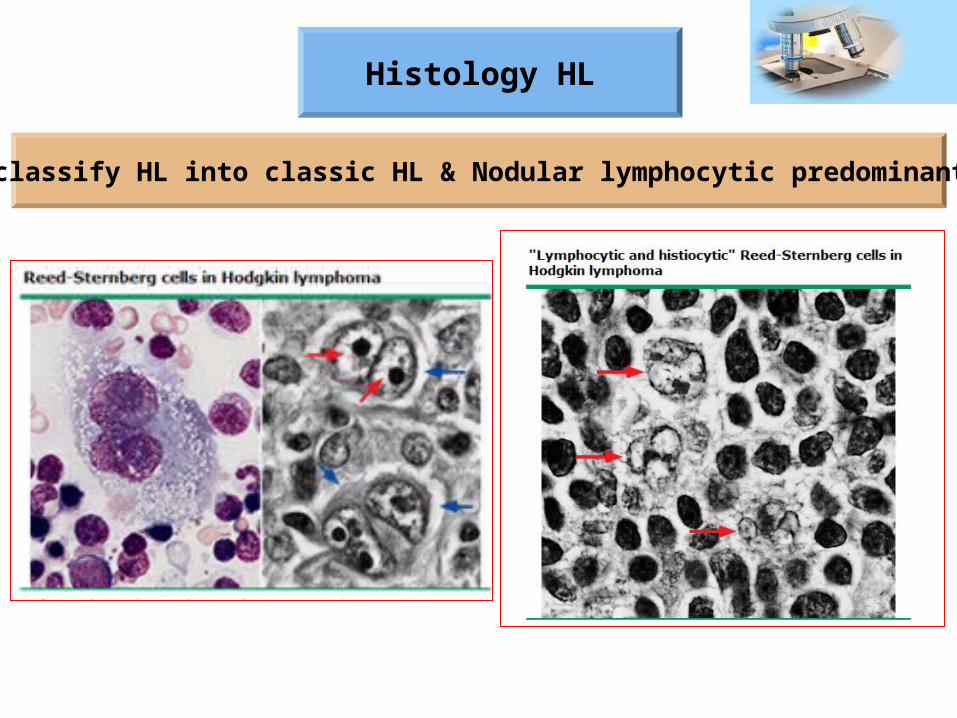
Histology HL
WHO classify HL into classic HL & Nodular lymphocytic predominant HL
Classic NLP% 90-59 % 5-10 %
Diagnostic cell Hodgkin/Reed-Sternberg
“L & H or popcorn”
Fibrosis Commen Rare
PatternDiffuse, inter-
follicular & nodular
Diffuse
CD 15 & CD30 +ve - veCD 45 & EMA - ve + ve
Histology HL
WHO classify HL into classic HL & Nodular lymphocytic predominant HL
Histology HL
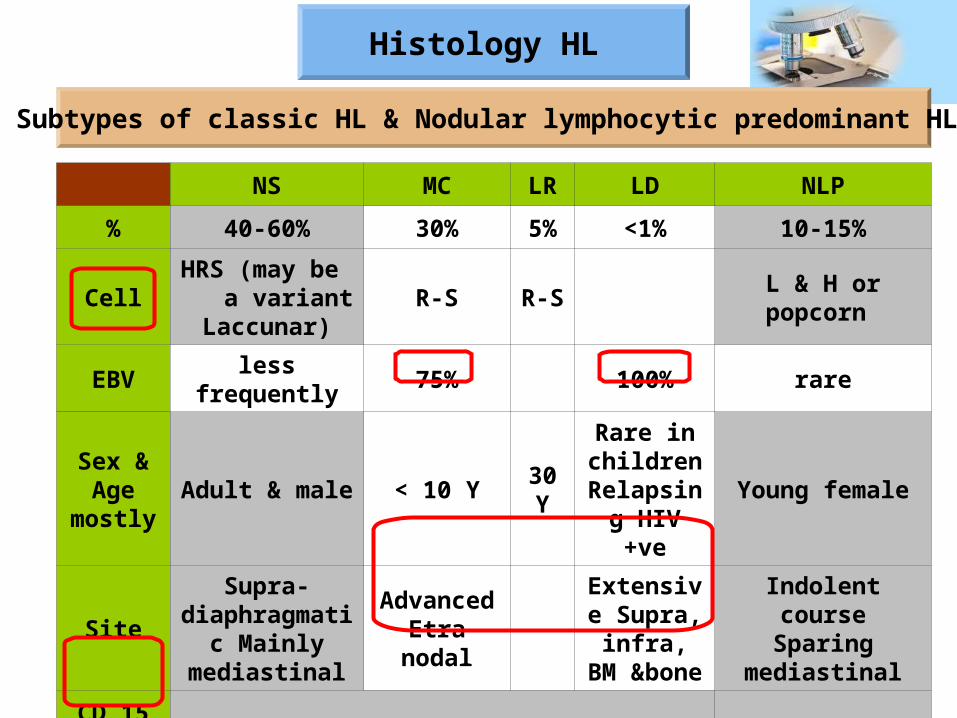
Subtypes of classic HL & Nodular lymphocytic predominant HL
NS MC LR LD NLP
% 40-60% 30% 5% <1% 10-15%
CellHRS (may be
a variant Laccunar)
R-S R-S L & H or popcorn
EBV less frequently 75% 100% rare
Sex & Age
mostlyAdult & male < 10 Y 30
Y
Rare in children
Relapsing HIV +ve
Young female
Site
Supra-diaphragmatic
Mainly mediastinal
Advanced Etra nodal
Extensive Supra,
infra, BM &bone
Indolent course Sparing
mediastinal
CD 15 & 30 +ve -ve
Factors suggesting association with HL ?
HL & EBV
Post BMT
Immunosuppression
nNucleic acids and proteins from EBV are detected in the malignant cells.
The peak incidence of HL is ≥ 4 years.
An increased incidence is observed in HIV patients.
Factors suggesting association with HL ?
HL & EBV
Nucleic acids and proteins from EBV are detected in HL cells:
20 to 50 % of cases of classical HL
> 50 % of mixed cellularity and lymphocyte depleted HL cases.
Less frequently with nodular sclerosis HL.
EBV infected tumour cells express a subset of EBV genes including:
Latent membrane protein 1(LMP1)
Latent membrane protein 2a (LMP2a)
EBV nuclear antigen 1 (EBNA1)
Factors suggesting association with HL ?
HL & EBV
Through the activation of nuclear factor kappa B (NF-kB).Up-regulation bcl-2 & MHC-I (anti apoptotic factors).
produces a tonic survival signal
Prevent apoptosis of pre-B cells that fail to express Ig molecules.
Integral membrane protein
Expression is required for the replication and maintenance of the viral genome in proliferating cell.
Biology of HL
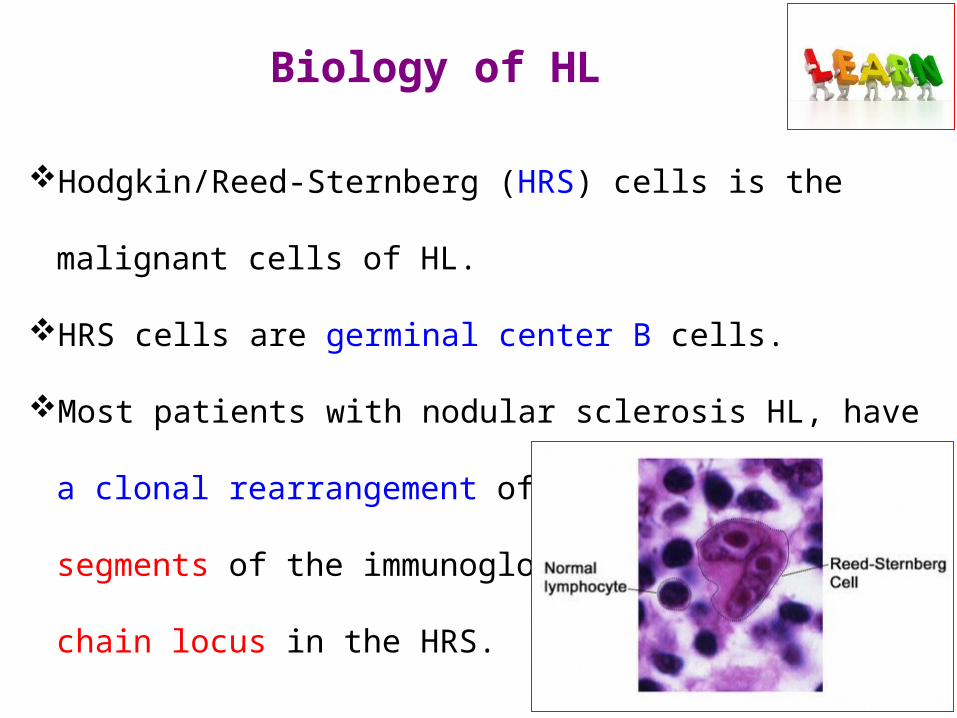
Hodgkin/Reed-Sternberg (HRS) cells is the malignant cells of HL.
HRS cells are germinal center B cells.
Most patients with nodular sclerosis HL, have a clonal
rearrangement of the V, D, and J segments of the immunoglobulin
(Ig) heavy chain locus in the HRS.
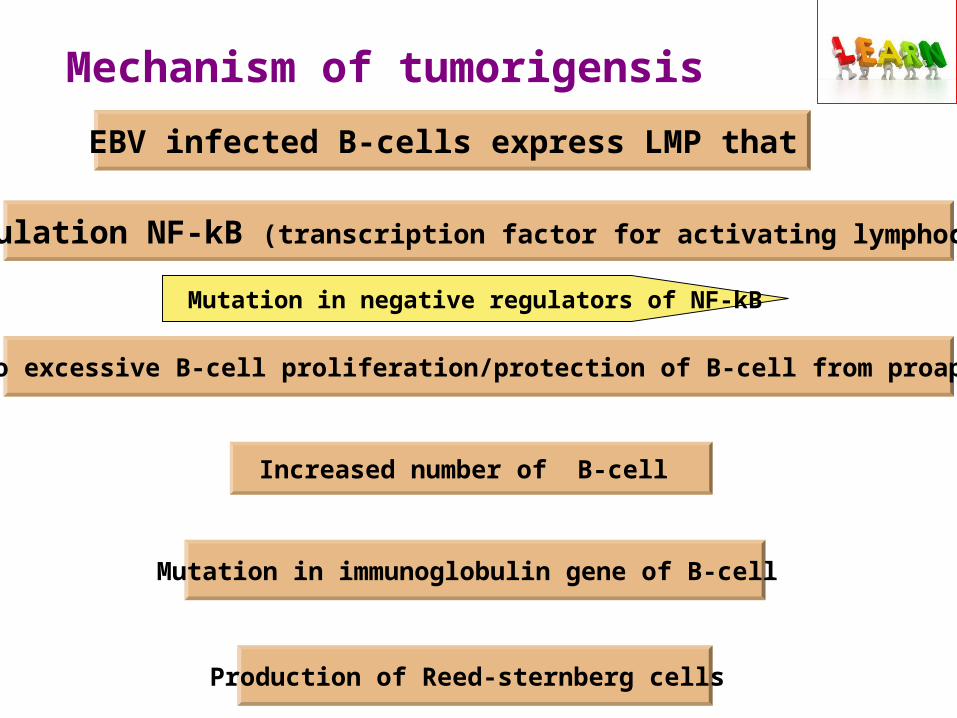
Mechanism of tumorigensis EBV infected B-cells express LMP that
Upregulation NF-kB (transcription factor for activating lymphocytes)
Leads to excessive B-cell proliferation/protection of B-cell from proapoptotic
Increased number of B-cell
Mutation in immunoglobulin gene of B-cell
Production of Reed-sternberg cells
Mutation in negative regulators of NF-kB
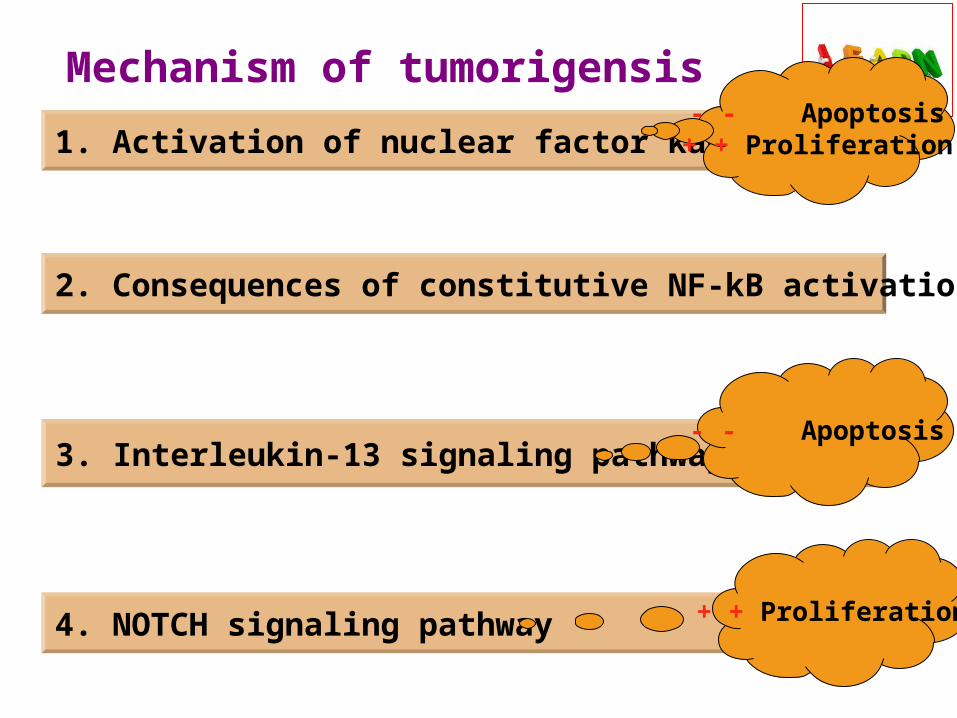
Mechanism of tumorigensis 1. Activation of nuclear factor kappa B
2. Consequences of constitutive NF-kB activation
3. Interleukin-13 signaling pathway
4. NOTCH signaling pathway
- - Apoptosis+ + Proliferation
- - Apoptosis
+ + Proliferation
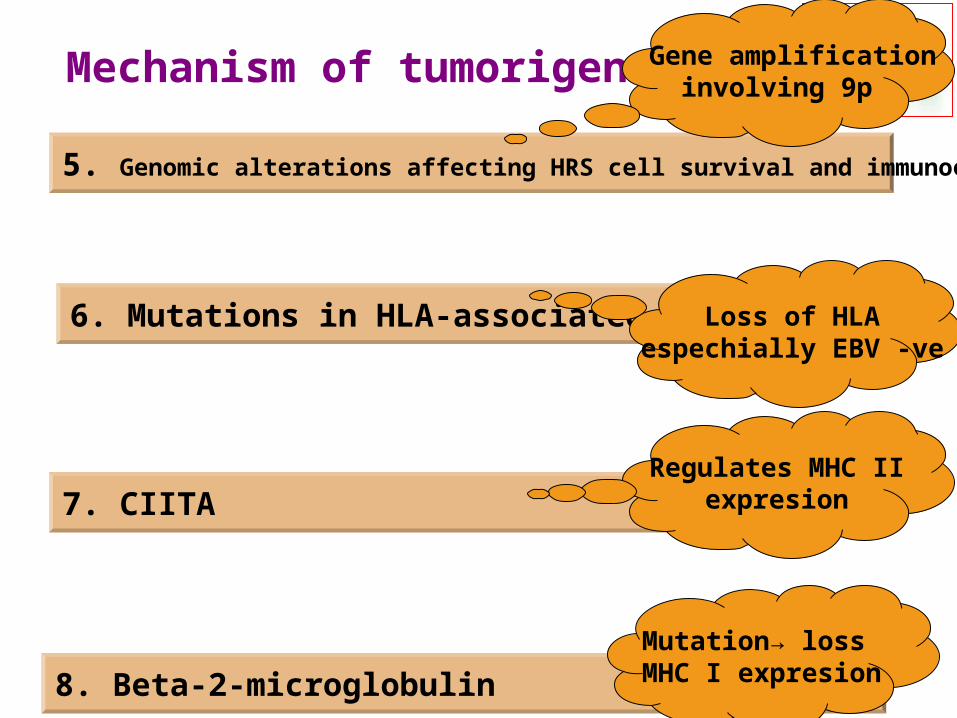
Mechanism of tumorigensis
5. Genomic alterations affecting HRS cell survival and immunoevasion
6. Mutations in HLA-associated genes
7. CIITA
8. Beta-2-microglobulin
Gene amplificationinvolving 9p
Loss of HLA espechially EBV -ve
Regulates MHC IIexpresion
Mutation→ loss MHC I expresion
80 to 85 % of pediatric HL patients (stage I to III) The remaining are stage IV.
Lymphadenopathy
Symptoms & signs
Mediastinal mass Systemic symptoms
S & S
Lymphadenopathy
Symptoms & signs
• Painless lymphadenopathy in most of cases (80%),
• Usually cervical, supraclavicular, axillary,
• Less often, inguinal.
• Lymph nodes feel rubbery and more firm than inflammatory adenopathy.
• Bulky lymphadenopathy→ (aggregates of lymph nodes 4 to 6 cm)
are considered in the risk-stratification for therapy.
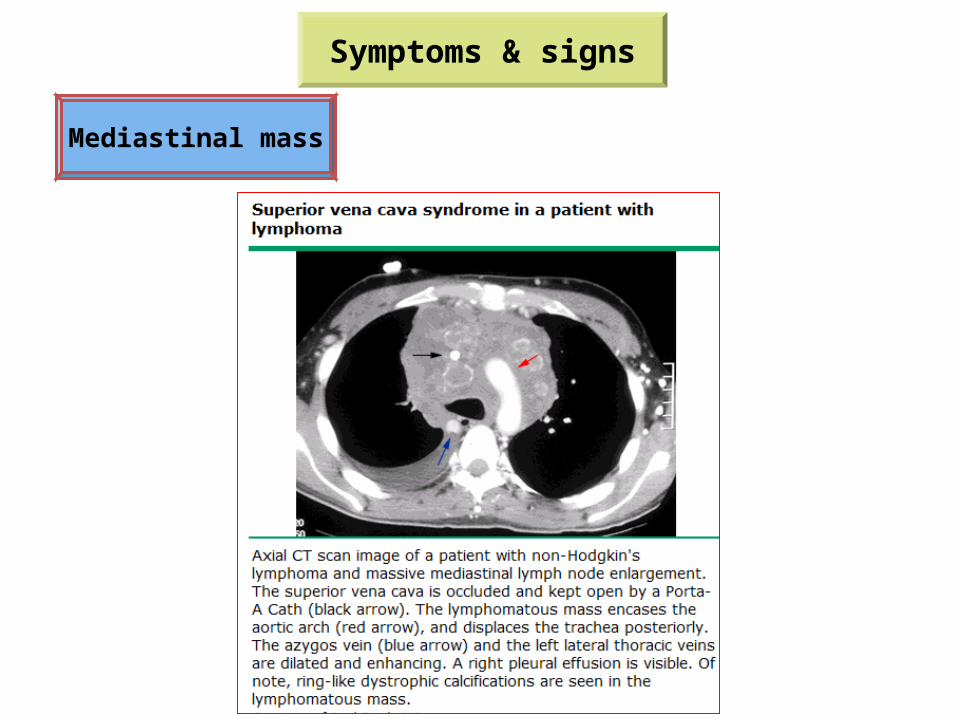
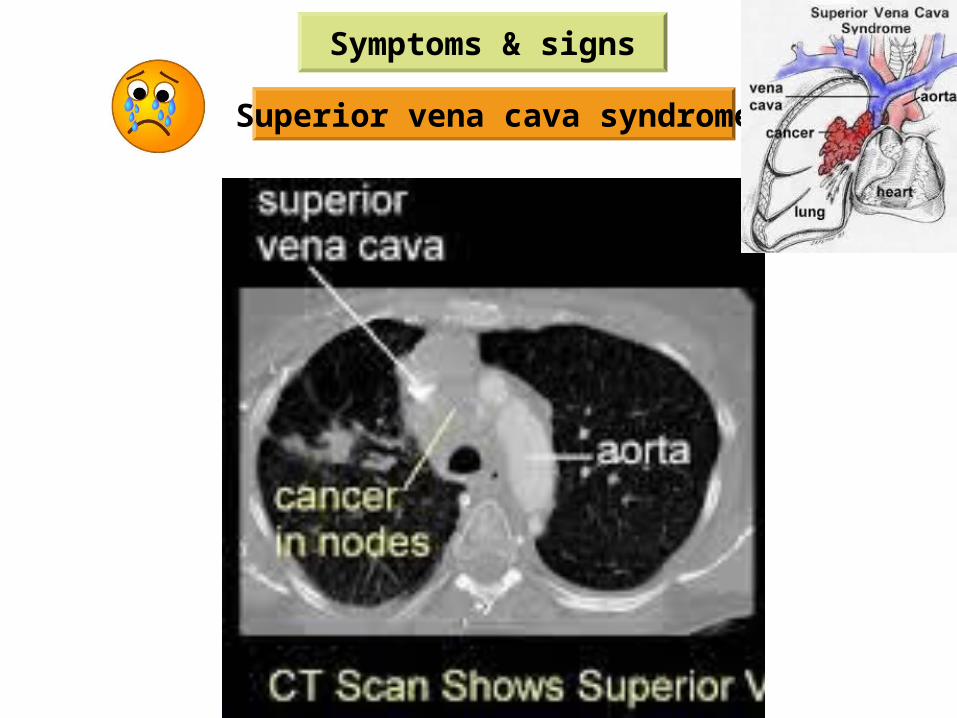
Mediastinal mass
• At the time of presentation present in 75% of cases.
• They are more common among children >12 years of age.
• Bulky mediastinal disease {masses greater than one-third the
diameter of the intrathoracic cavity} may cause dysphagia,
dyspnea, cough, stridor, or the superior vena cava (SVC)
syndrome.
Symptoms & signs
Mediastinal mass
Symptoms & signs
Symptoms & signs
Bulky disease defintion
Lugano classification A nodal mass of 10 cm or > one-third of the transthoracic diameter at any level of thoracic vertebrae as determined by CT.
Stanford V protocolDefined as ≥5 cm, required the use of involved field irradiation following completion of chemotherapy.
Ann Arbor Staging system1. An abdominal node or nodal mass that is ≥10 cm in largest dimension as determined by CT, MRI, or ultrasound.2. A mediastinal mass which has a maximum width ≥ 1/3 of the internal transverse diameter of the thorax (at the pleural surfaces) at the level of T5/6 as determined on a posteroanterior chest radiograph.
• Obstruction of blood flow through the SVC.
• Caused by:
→Invasion or external compression of the SVC.
→Thrombosis of blood within the SVC.
• Symptoms of SVC syndrome within weeks because rapid
tumor growth.
Symptoms & signs
Superior vena cava syndrome
Dyspnea is the most common symptom,
Dysphagia,
Cough,
Chest pain,
Facial swelling, Fullness of face, Arm swelling,
Patients with cerebral edema may have headaches,
confusion, or possibly coma,
Symptoms & signs
Superior vena cava syndrome
Symptoms & signs
Superior vena cava syndrome
Systemic symptoms
Symptoms & signs
Non specific
Specific
Adults
Fatigue and anorexia
Fever (>38.0°C) during the previous month,
Drenching night sweats during the previous month,
Weight loss (≥10 % loss within 6 months before
diagnosis),
B symptoms
B symptoms correlate with:Advanced stage,Bulky disease,Worse prognosis.
Systemic symptoms
Symptoms & signs
Non specific
Specific
Adults
Fatigue and anorexia
Fever (>38.0°C) during the previous month,
Drenching night sweats during the previous month,
Weight loss (≥10 % loss within 6 months before
diagnosis),
B symptoms
Pruritus and alcohol-induced pain, which typically resolve with TTT
Symptoms & signs
S & S
Autoimmune disorders such as: (after diagnosis or after remission)
Autoimmune hemolytic anemia, thrombocytopenia, or
neutropenia.
Nephropathy.
Hypertrophic osteoarthropathy:
Children & intrathoracic HL may rarely present with this.
Characterized by digital clubbing and painful periostosis of tubular bones.
Evaluation
Goal
Extent of disease (stage)
Risk stratification
Prognosis
Intensity of treatment
Evaluation
History
B symptoms
Previuos infection
Exposure to toxins
Immune deficiencies
Familial
Evaluation
Examination
Lymph node "size & location"
Liver & spleen "size"
Pulmonary findings
Skin infiltration
Neurological signs
Evaluation
Laboratory
CBC with differential count
Liver and renal functions
HIV serology
ESR & LDH
Immunologic evaluation if....Pregnancy test if ♀ married
Evaluation
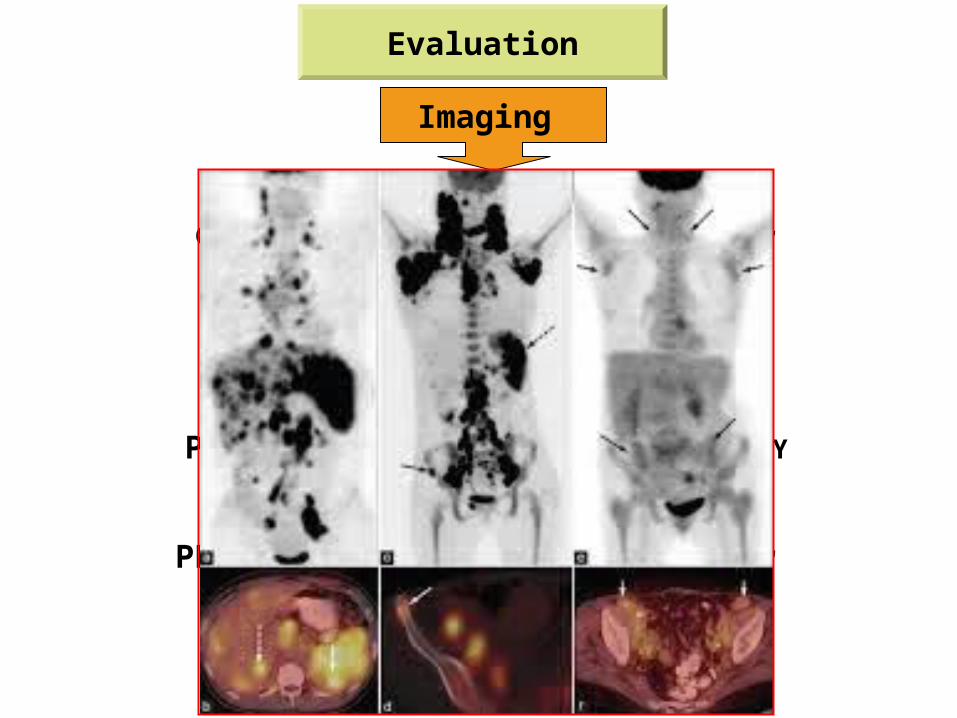
Imaging
CT with contrast "neck, chest, abdomen, pelvis"
Echo
PET-CT "after pathological confirmation"
Pulmonary function if patient >6 Y
Evaluation
Imaging
CT with contrast "neck, chest, abdomen, pelvis"
Echo
PET-CT "after pathological confirmation"
Pulmonary function if patient >6 Y
Evaluation
PET-CT
It is the examination of choice for detecting disease activity during and after treatment.
PET/CT scanning distinguish between active tumour and necrosis or fibrosis in residual masses.
The negative predictive value of PET-CT averages 80-90%.
The positive predictive value of PET-CT averages 65%.
Evaluation
PET-CT
Up to 40% of patients with positive PET-CT will not relapse.
Poor tumour shrinkage and Positive PET-CT after chemotherapy have a higher risk of relapse or progression despite the use of RTH.
The causes of false positive PET-CT: Post-inflammatory changes after chemotherapy and RTH, Rebound thymic hyperplasia, Infectious and inflammatory processes, Brown fat (neck muscles).
So tissue biopsy is must prior to giving more therapy.
Evaluation
Tissue biopsy
Excisional biopsy "not FNAC"
Why excisional biopsy not FNAC ???
Fine needle aspirates do not provide adequate amounts of material for proper histologic classification nor for molecular studies needed in the evaluation. Subclassification of HL depends upon whether the tumoral architecture is nodular, diffuse, or both, and whether "classic" or variant Reed-Sternberg cells are present, as well as the composition of the cellular infiltrate (eg, non-neoplastic small lymphocytes, eosinophils, plasma cells, fibroblasts, histiocytes, neutrophils, and collagen fibers).
Evaluation
Tissue biopsy
BMA & BMB
Excisional biopsy "not FNAC"
Should we do BMA & BMB for every case ???
BMA & BMB are recommended only for patients with:Advanced stage disease (stage III, IV), B symptoms, or Any abnormality on CBC that is suspicious for bone marrow involvement (anaemia).
Evaluation
Fertility counseling
Options for women are limited. Men can often participate in sperm banking.
Evaluation
Differential diagnosis
Malignant
Infectious
Inflammatory
Non-Hodgkin lymphoma, Metastatic adenopathy from other primary tumors (eg, nasopharyngeal carcinoma, soft tissue sarcoma). Toxoplasmosis, Typical and atypical mycobacterium infections, EBV infection.
Systemic lupus erythematosus.
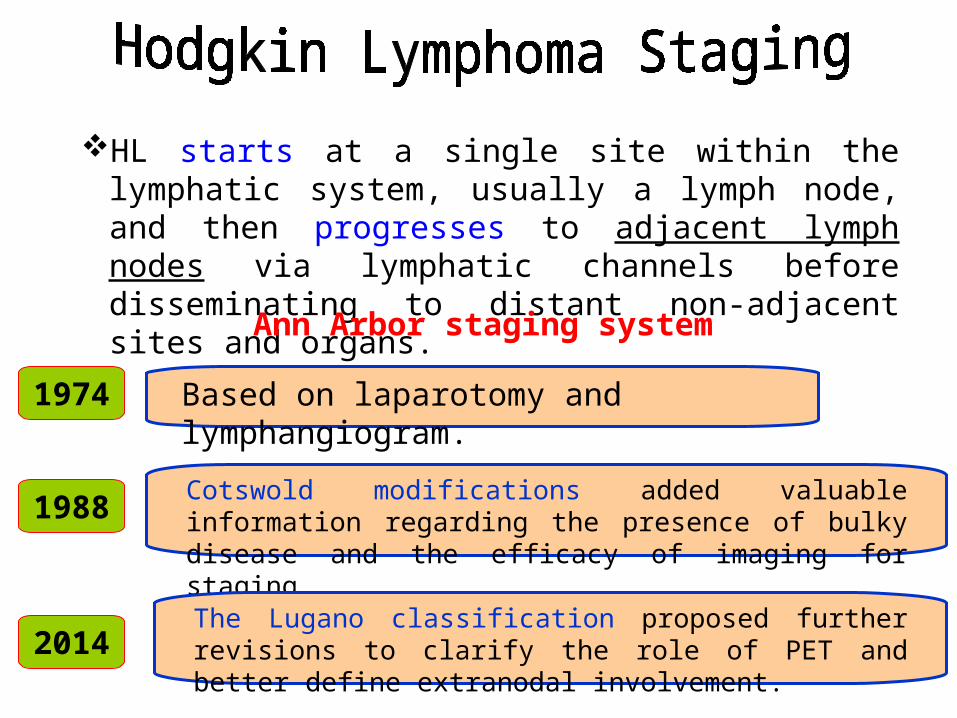
HL starts at a single site within the lymphatic system, usually a lymph node, and then progresses to adjacent lymph nodes via lymphatic channels before disseminating to distant non-adjacent sites and organs.
Based on laparotomy and lymphangiogram.
1974
Ann Arbor staging system
Cotswold modifications added valuable information regarding the presence of bulky disease and the efficacy of imaging for staging.
1988
The Lugano classification proposed further revisions to clarify the role of PET and better define extranodal involvement.
2014
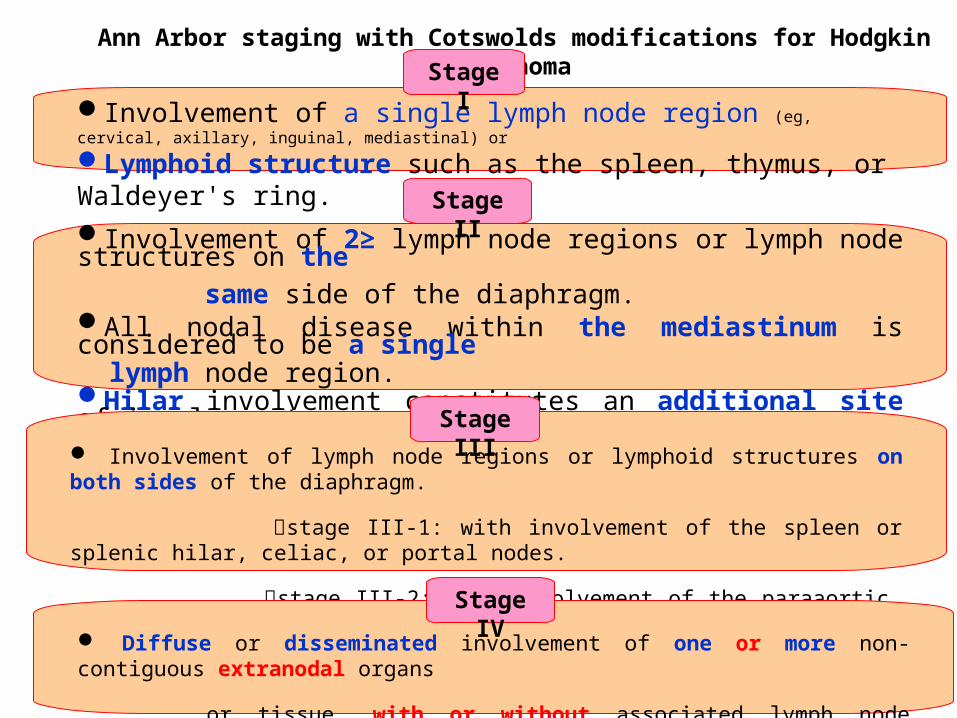
Ann Arbor staging with Cotswolds modifications for Hodgkin lymphoma
Involvement of a single lymph node region (eg, cervical, axillary, inguinal, mediastinal) or Lymphoid structure such as the spleen, thymus, or Waldeyer's ring.Involvement of 2≥ lymph node regions or lymph node structures on the same side of the diaphragm.All nodal disease within the mediastinum is considered to be a single lymph node region.Hilar involvement constitutes an additional site of involvement.
Stage I
Stage II
Involvement of lymph node regions or lymphoid structures on both sides of the diaphragm.
stage III-1: with involvement of the spleen or splenic hilar, celiac, or portal nodes.
stage III-2: with involvement of the paraaortic, iliac, inguinal, or mesenteric nodes.
Stage III
Diffuse or disseminated involvement of one or more non-contiguous extranodal organs
or tissue, with or without associated lymph node involvement.
Stage IV
Prognostic factors
Patients with stage III or IV disease are → advanced stage.
Patients with stage I or II disease are → early (limited) stage.
Early stages are further stratified for treatment purposes into
favorable and unfavorable prognosis varies by region.
It is based upon the presence or absence of certain clinical
features.
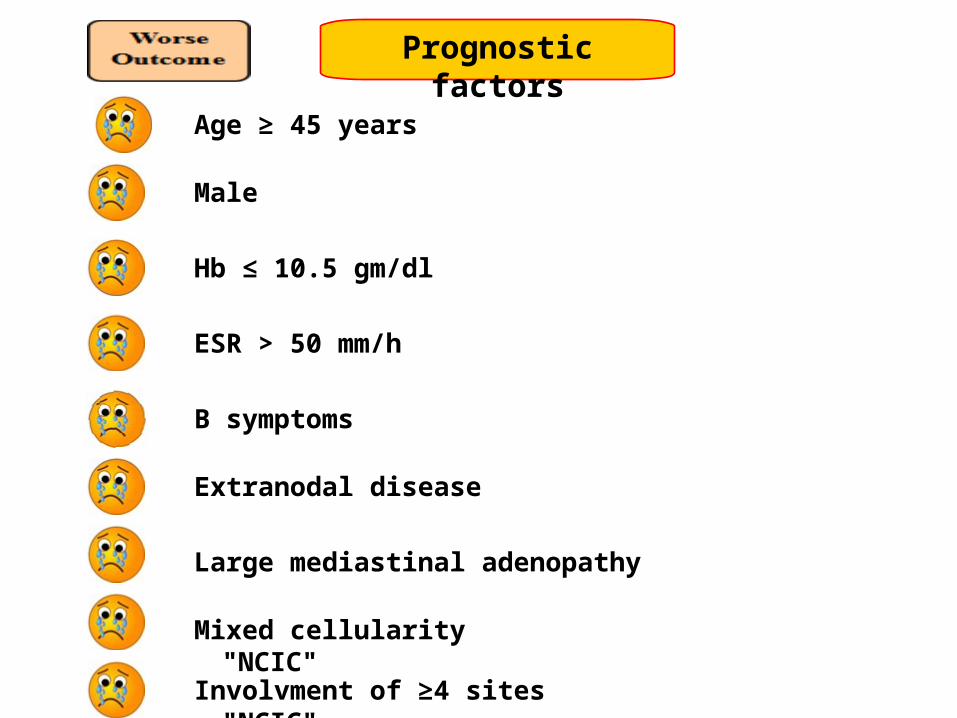
Prognostic factors
Age ≥ 45 years
Male
Hb ≤ 10.5 gm/dl
ESR > 50 mm/h
B symptoms
Extranodal disease
Mixed cellularity "NCIC"
Large mediastinal adenopathy
Involvment of ≥4 sites "NCIC"
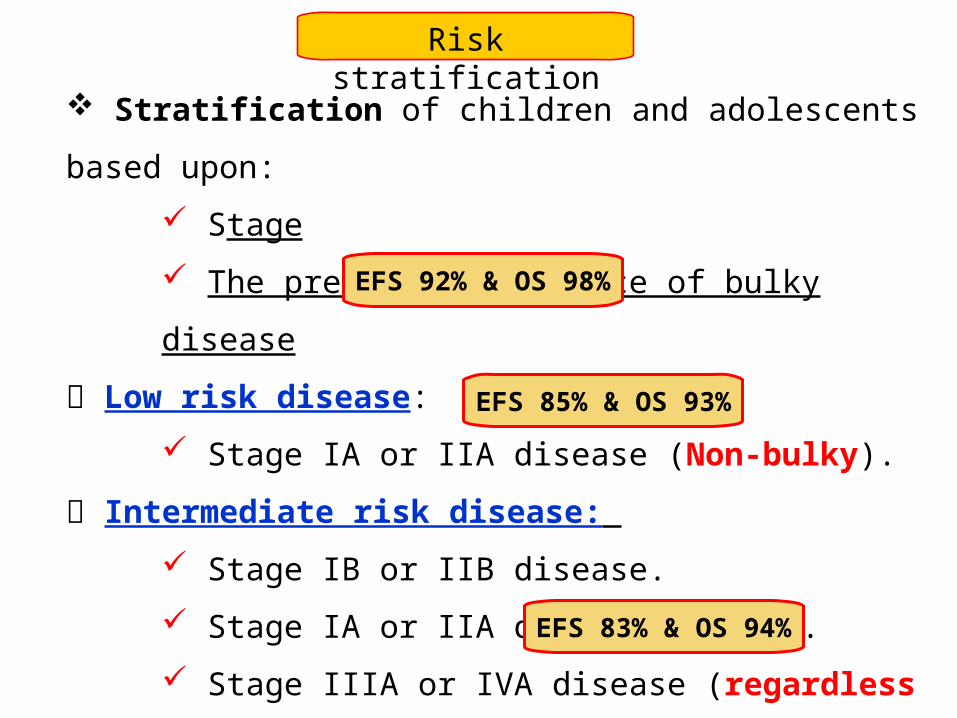
Risk stratification
Stratification of children and adolescents based upon:
Stage
The presence or absence of bulky disease
Low risk disease:
Stage IA or IIA disease (Non-bulky).
Intermediate risk disease: Stage IB or IIB disease.
Stage IA or IIA disease (Bulky).
Stage IIIA or IVA disease (regardless of bulk).
High risk disease: Stage IIIB or stage IVB disease.
EFS 92% & OS 98%
EFS 85% & OS 93%
EFS 83% & OS 94%
Response assessment
Complete remissionNo clinical evidence of disease or disease-related symptoms.
The post-treatment PET is negative (residual mass of any size is permitted).
Spleen and liver must be non-palpable and without nodules.
If a pre-treatment bone marrow biopsy was positive, an adequate bone
marrow biopsy from the same site must be cleared of infiltrate; if this
is indeterminate by morphology, immunohistochemistry should be
negative.
Response assessmentPartial remission
A decrease by at least 50 % in the sum of the products of the largest
perpendicular diameters (SPD) of up to six of the largest measurable
lesions.
Splenic or hepatic nodules must decrease by at least 50 % in the
SPD or in the greatest transverse diameter for single nodules).
The post-treatment PET should be positive in at least one previously
involved site.
There is no increase in the size of other nodes, liver, or spleen.
No new areas of disease.
Bone marrow biopsy results are not useful in determining PR.
Response assessment
Stable disease Failure to attain a CR or PR.
No evidence of progressive disease. The post-treatment PET should be positive at prior sites of disease.
No new sites should be present on PET or CT.
Response assessment
Progressive diseaseDevelopment of a new lesion is defined by the appearance of
Any new lesion >1.5 cm in long axis.
If the long axis diameter is from 1.1 to 1.5 cm, the lesion
should only be considered abnormal if its short axis is > 1.0 cm.
Progressive disease is also defined as an increase of at least
50 % in the longest diameter of a previously identified node.
Lesions should be PET positive unless they are below a
detectable size (ie, <1.5 cm in long axis by CT).
Response assessment
Rapid early responders: patients who achieved ≥ 60 % reduction
in node diameters by CT scan post two cycles of chemotherapy.
Slow early responders: patients who achieved < 40 % reduction
in node diameters by CT scan post two cycles of chemotherapy.
Response assessment
Refractory (resistant) HL: is a failure to achieve a complete
or partial response. Primary :failure to respond to initial therapy
(eg, chemotherapy ± RTH)
Secondary: initial response but failure to respond after
disease relapse.
Relapsed HL is the reappearance of disease in sites of prior
disease and/or in new sites after initial therapy and attainment
of complete response (CR).
A combination of chemotherapy and radiotherapy
Non-cross resistant: different mechanism of
action for each drug.
Non-dependant: each drug is individually
active.
No toxicity overlap: to allow full dose of each
drug.
Rules for combination TTT
Commonly used regimens
ABV (doxorubicin, bleomycin, vinblastine)
ABVE (doxorubicin, bleomycin, vinblastine, etoposide)
ABVD (doxorubicin, bleomycin, vinblastine, DTC)
VAMP (vinblastine, doxorubicin, methotrexate, prednisone)
MOPP (mechlorethamin, vincristine, procarbazine, prednisone)
COPP (cyclophosphamide, vincristine, procarbazine, prednisone)
OEPA (vincristine, etoposide, prednisone, doxorubicin; for ♂)
OPPA (vincristine, procarbazine, prednisone, doxorubicin; for ♀)
AVPC (doxorubicin, vincristine, prednisone, cyclophosphamide)
A combination of chemotherapy and radiotherapy
Several paediatric study groups have evaluated treatment de-escalation in an attempt to avoid toxicities that can be associated with treatment. As examples COG trial observed 52 children with stage IA:
* Non-bulky single node disease &* A negative PET/CT scan after complete resection.
At a median follow-up of 39 months: * Nine patients (17 %) relapsed. * All of these patients attained CR after three cycles of AV-PC. * No patients required radiation therapy.
The 3-year estimated PFS & OS rates were 82 & 100%, respectively.
A combination of chemotherapy and radiotherapy
Several paediatric study groups have evaluated treatment de-escalation in an attempt to avoid toxicities that can be associated with treatment. As examples COG trial evaluate use 3 cycles AV-PC 137 children with:
* Stage IA or IIA non-bulky single node disease.
Folowing chemotherapy alone: * 126 patients (92 %) CR. * 11 children had PR that was successfully converted to CR after IFRT.
The 4-year estimated PFS & OS rates were 88 & 100%, respectively.
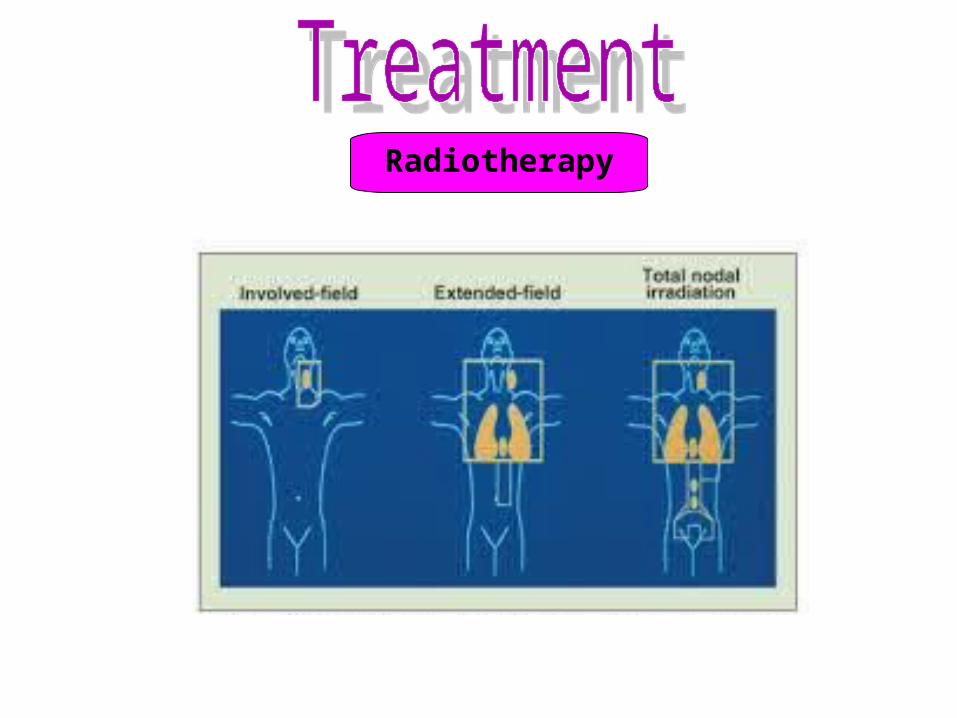
Radiotherapy
Volume
Dose
Involved field radiation therapy (LD-IFRT).
Depth of radiation varied according different trials.
Mainly on areas of bulky disease or those with poor
response to chemotherapy.
Ranging from 15-25 Gy / 10-15 fraction
Radiotherapy
A combination of chemotherapy and radiotherapy
Radiotherapy
COG trial investigated whether (AVPC) without radiotherapy would be curative in patients with CR at end of therapy.
Though preliminary data in those patients with PET-avid disease after one cycle of therapy and who did not receive radiotherapy due to complete remission at end of treatment.
→ showed two-year OS & EFS 100 %, 65 % respectivelly.
A combination of chemotherapy and radiotherapy
Risk adapted treatment
WHY?
Standard RTH & Alkylating-CHT→Significant toxicity. So tailor amount & intensitiy of treatmnt to severity of disease.
Low-Risk adapted treatment
Four cycles followed by LD-IFRT.
{VAMP or COPP or ABVE or OEPA or OPPA}
A non-randomized prospective international trial (GPOH-HD95)
suggested that omission of radiation did not compromise survival
rates among children with early stage HL who attained a CR on
CT or MRI following initial treatment with OEPA or OPPA.
Intermediate-Risk adapted treatment
Six cycles COPP or 5 cycles ABVE-PC plus LD-IFRT.
PC = (prednisone,cyclophosphamide) Results from the COG AHOD0031 trial suggest that therapy may be
modified (escalated or deescalated) based on initial response to ABVE-PC:
The omission of IFRT in rapid early responders (60 %reduction
in node diameters by CT scan post two cycles) who achieve PET-
negative CR after four cycles of ABVE-PC.
The escalation of therapy in slow early responders with PET +ve
disease.EFS 85%OS 93%
High-Risk adapted treatment
Most protocols incorporate high intensity combination
chemotherapy + low dose or standard dose IFRD
Six cycles ABVE-PC or
Two cycles of OEPA for ♂, followed by four cycles of
COPDAC.
Two cycles of OPPA for ♀, followed by four cycles of COPP.
6 cycles+LD or SD-RTH
EFS 83% OS 94%
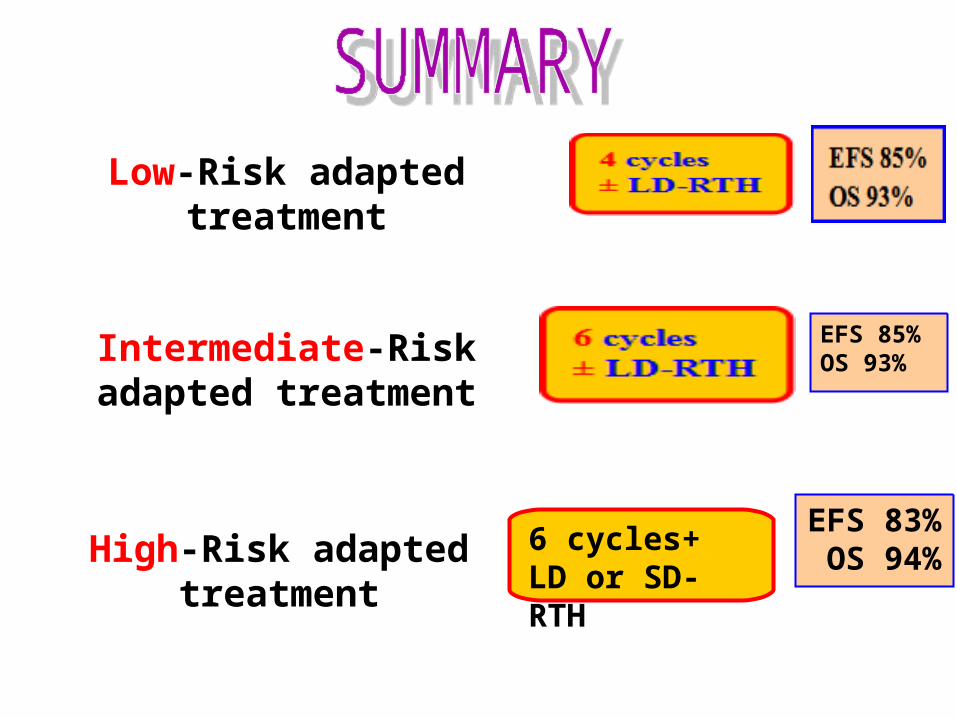
Low-Risk adapted treatment
Intermediate-Risk adapted treatment
High-Risk adapted treatment
EFS 85%OS 93%
6 cycles+LD or SD-RTH
EFS 83% OS 94%
Treatment of Nodular lymphocyte-predominant HL
NLPHL represents a more indolent disease than classical HL. Patients with stage III/IV are treated in a similar fashion to patients with classical HL. In contrast, patients with stage I/II NLPHL without B symptoms are treated with less intensive therapy than patients with classical
HL. Small studies have evaluated the use of in stage I/II NLPHL:Chemotherapy alone.Observation without treatment following excision.
The current strategies for treating NLPHL in children areModest intensity chemotherapy regimens, Some without anthracyclines, With or without involved field radiation.
Favourable outcome
Progression of disease after a partial initial response was seen in 10-15 %.
Relapse rates range from:
10 to 20 % in favorable prognosis localized (stage I-II) disease.
30 to 40 % in patients with more advanced disease (stages IIB-IV).
Failed induction therapy (resistant disease) (relapse in 30- 40 %),
Relapsed <12 months after having obtained a CR (relapse 27-
38%),
Relapsed > one year after attaining a CR (relapse in 24-40%).
%
The most favourable for successful salvage
The majority of relapses following an apparent CR will occur:
Within the first 12 months in 42%Within one to three years in 24% Late relapses (ie, >3 years following treatment) occur at the rate of
a few %/ year, extending up to 12 years post-treatment.
Time
Site
Relapse will more likely occur in previously uninvolved nodal regions or extranodal sites such as the liver or lungs.
Confirmation of relapse
Diagnosis of recurrence is generally made with biopsy of a mass.
This is especially true in case of late relapse, since there is
a significant risk for second cancers (non-Hodgkin lymphoma
or solid tumours) in these patients.
Evaluation of relapse
PET scans have added considerably to the assessment of
remission or persistent disease following salvage therapy prior to
high-dose chemotherapy and HCT.
Residual fibrotic, necrotic masses on CT scan suggest incomplete
response.
However, case series have demonstrated a relapse rate of only:
20 % if the PET scan is negative prior to HCT.
76 % if the PET scan is positive prior to HCT.
Goal of treatment
The goal of therapy is to attain a second complete response
(as defined by CT/PET negative) or an unconfirmed complete
response (as defined by CT) prior to autologous HCT.
Salvage therapy with second (or third) line regimens can
achieve responses in approximately 50 % of these
patients.
The decision to use a more aggressive treatment
approach in relapsed or refractory HL is typically based
on the presence of predictors of poor outcome.
Treatment
Predictors of better outcome in Relapsed patients:
Relapse >12 months from the end of initial TTT or
Patients who had reduced dose chemotherapy and no
RTH.
Predictors of poor outcome in Relapsed patients:
B symptoms,
Relapse between 3-12 months from the end of TTT.
Poor response to second-line therapy.
Treatment
Chemotherapy regimens
At a median follow-up of 45 months, patients with none of these
factors had a freedom from second progression of 48 % as
compared with 17 % for patients with three factors:Short time to relapse (≤12 months from end of primary TTT).
Clinical stage III or IV at relapse.
Anemia.
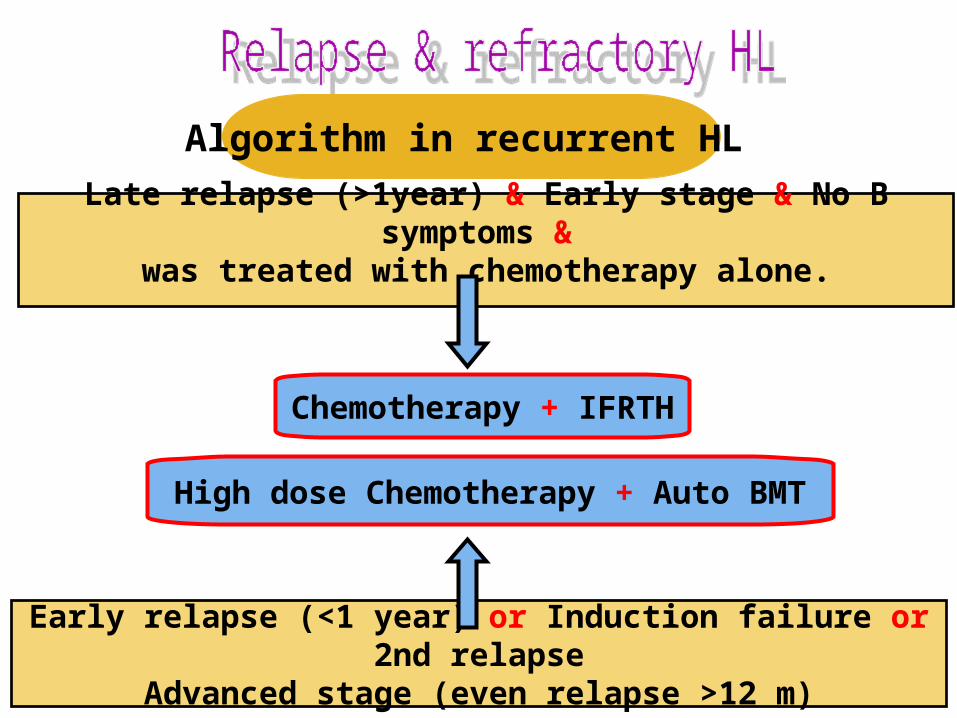
Algorithm in recurrent HL
Late relapse (>1year) & Early stage & No B symptoms & was treated with chemotherapy alone.
Chemotherapy + IFRTH
Early relapse (<1 year) or Induction failure or 2nd relapse
Advanced stage (even relapse >12 m)
High dose Chemotherapy + Auto BMT
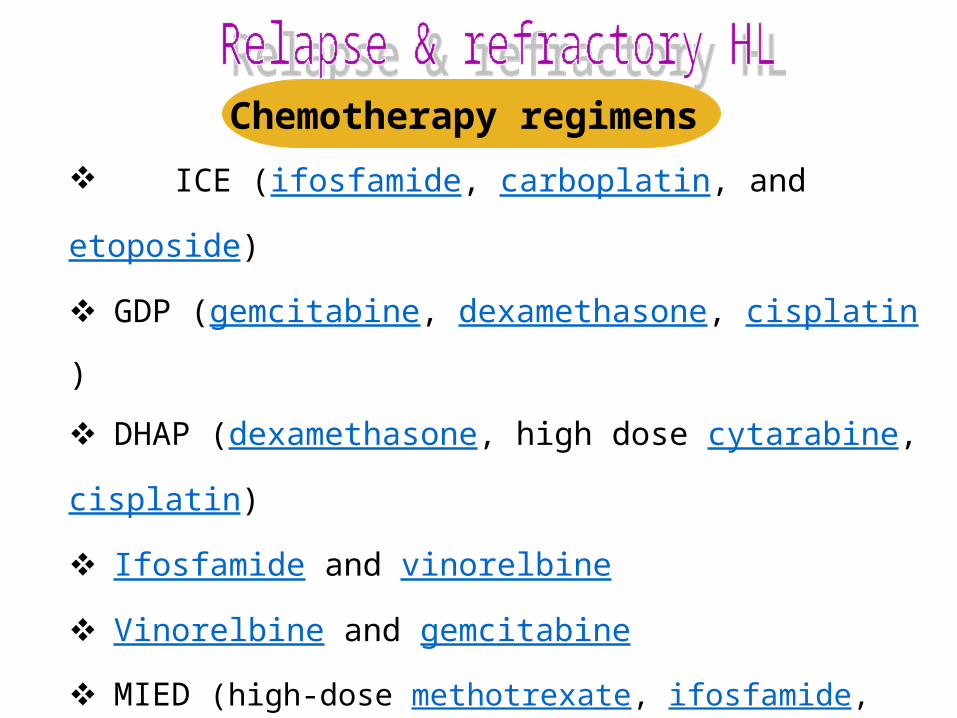
Chemotherapy regimens
ICE (ifosfamide, carboplatin, and etoposide)
GDP (gemcitabine, dexamethasone, cisplatin)
DHAP (dexamethasone, high dose cytarabine, cisplatin)
Ifosfamide and vinorelbine
Vinorelbine and gemcitabine
MIED (high-dose methotrexate, ifosfamide, etoposide, and dexa)
Biologic therapy:
Immunotherapy,
Immunotoxins, and
Adoptive immunotherapy.
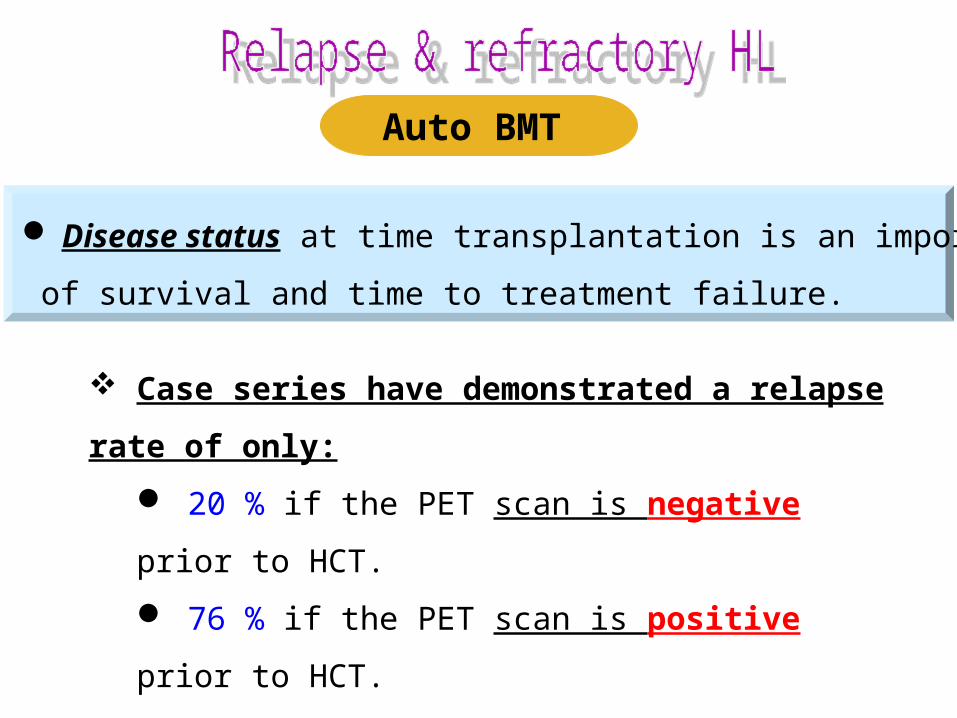
Auto BMT
Disease status at time transplantation is an important predictor
of survival and time to treatment failure.
Case series have demonstrated a relapse rate of only: 20 % if the PET scan is negative prior to HCT.
76 % if the PET scan is positive prior to HCT.
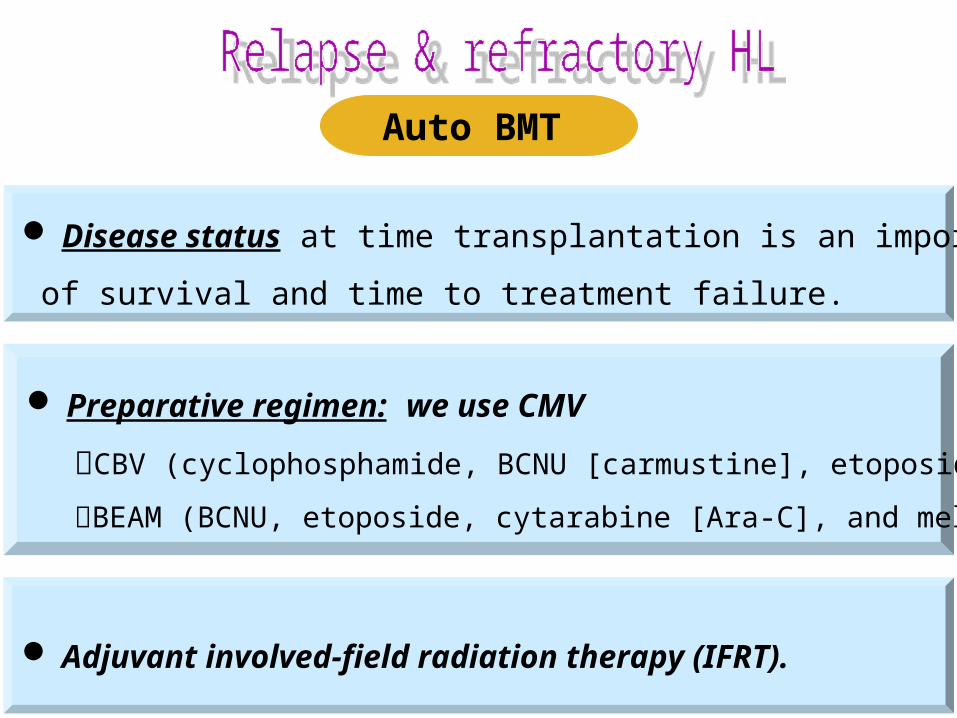
Auto BMT
Disease status at time transplantation is an important predictor
of survival and time to treatment failure.
Preparative regimen: we use CMV
CBV (cyclophosphamide, BCNU [carmustine], etoposide [VP-16]).
BEAM (BCNU, etoposide, cytarabine [Ara-C], and melphalan).
Adjuvant involved-field radiation therapy (IFRT).
What about relapse post Auto BMT ???
Other options include the use of :
Brentuximab vedotin,bendamustine,
Mtor inhibitors (eg, everolimus, gemcitabine, vinorelbine),
Immunomodulators (eg, lenalidomide),
Local regional irradiation,
Allogeneic HCT,
■ Anti PD-1 antibody nivolumab.
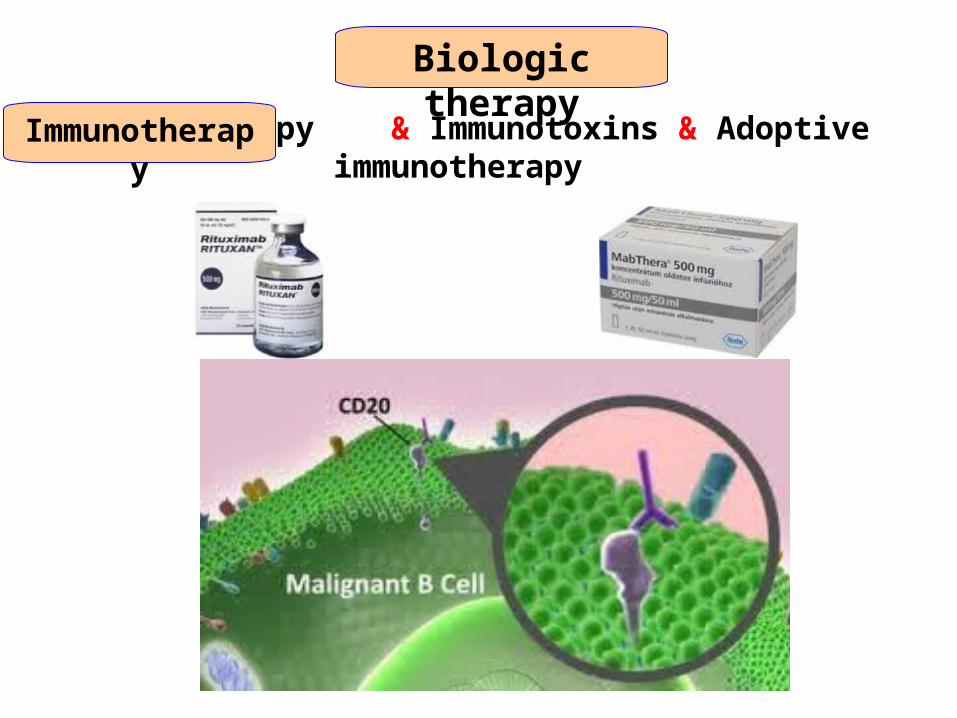
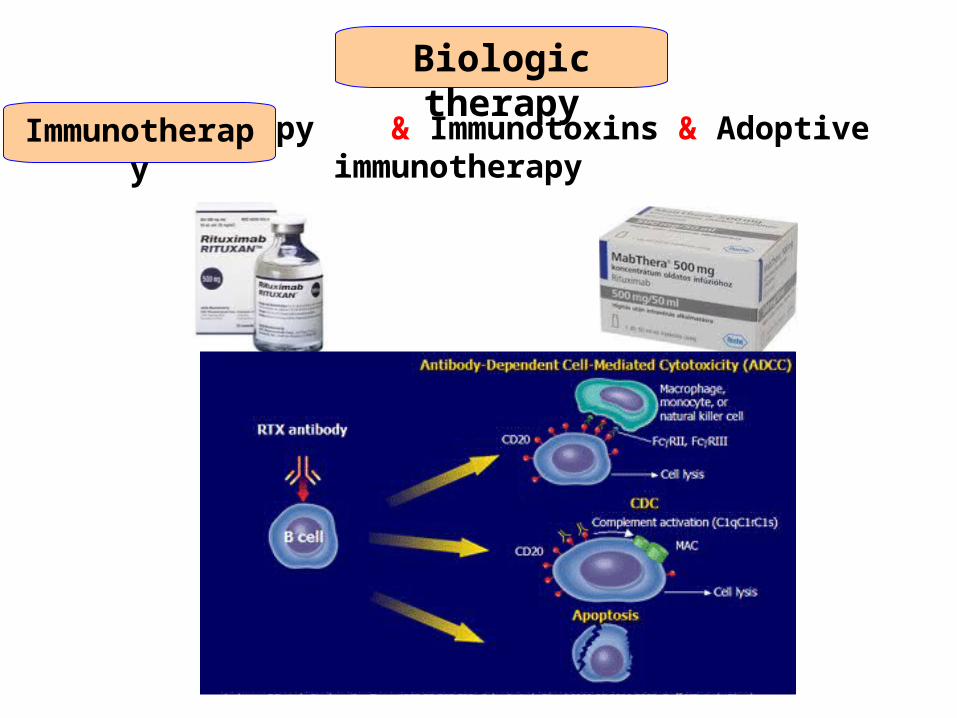
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Immunotherapy
Rituximab
It is a recombinant anti-CD20 antibody is used in the treatment of
many hematologic malignancies that express CD20.
It binds to antigen CD20 (antigen)→activating complement-dependent
B-cell cytotoxicity.
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Immunotherapy
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Immunotherapy
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Immunotherapy
It is more useful in the TTT of nodular lymphocyte predominant HL.
The value of rituximab in classic HL is uncertain.
Alone or with other second-line chemotherapy.
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Immunotoxins
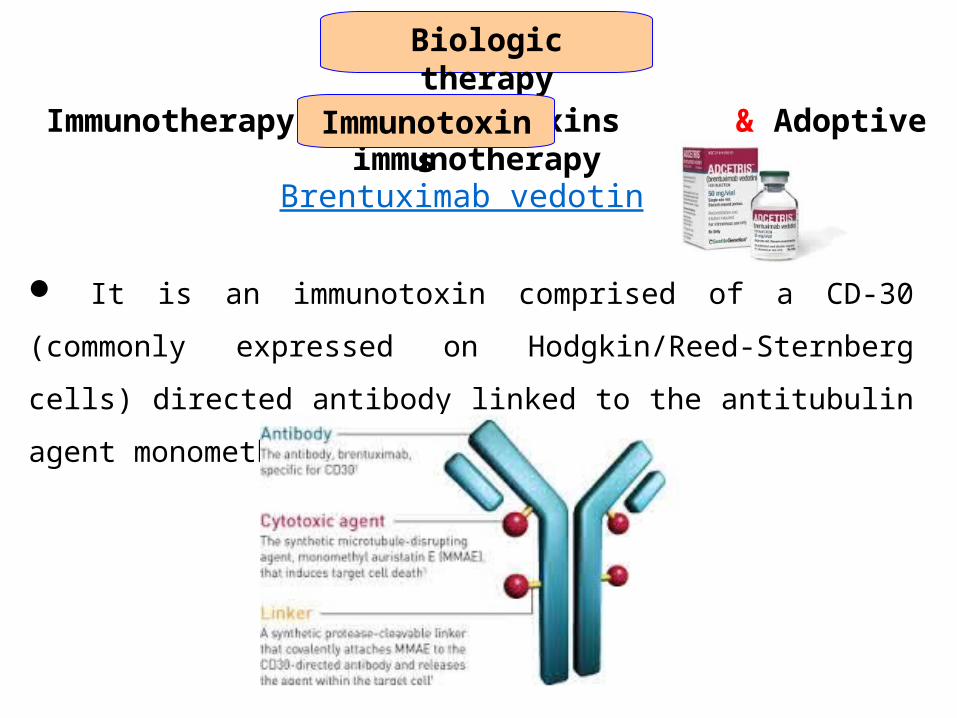
Brentuximab vedotin
It is an immunotoxin comprised of a CD-30 (commonly expressed on
Hodgkin/Reed-Sternberg cells) directed antibody linked to the antitubulin
agent monomethyl auristatin E (MMAE).
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Immunotoxins
A phase II trial of brentuximab in adults who had relapsed status post
autologous hematopoietic cell transplantation demonstrated a 75 % overall
response rate, with median progression-free survival of 5.6 months.
Pediatric phase I and II studies are ongoing, both with brentuximab as a
single agent and in combination with gemcitabine.
Brentuximab vedotin
It is an immunotoxin comprised of a CD-30 (commonly expressed on
Hodgkin/Reed-Sternberg cells) directed antibody linked to the antitubulin
agent monomethyl auristatin E (MMAE).
Biologic therapy
Immunotherapy & Immunotoxins & Adoptive immunotherapy Adoptive immunotherapy
Cytotoxic T lymphocytes (CTLs)Cytotoxic T lymphocytes (CTLs) has antitumor activity.
Cytotoxic T-lymphocytes that are specific for Epstein-Barr virus
latent antigens LMP1 and LMP2 or Reed-Sternberg cells.
Expanded clones of these cells may have a therapeutic role in those
patients with HL whose Reed-Sternberg cells express Epstein-Barr
viral antigens.
PD-1 blockade
Nivolumab, Pembrolizumab
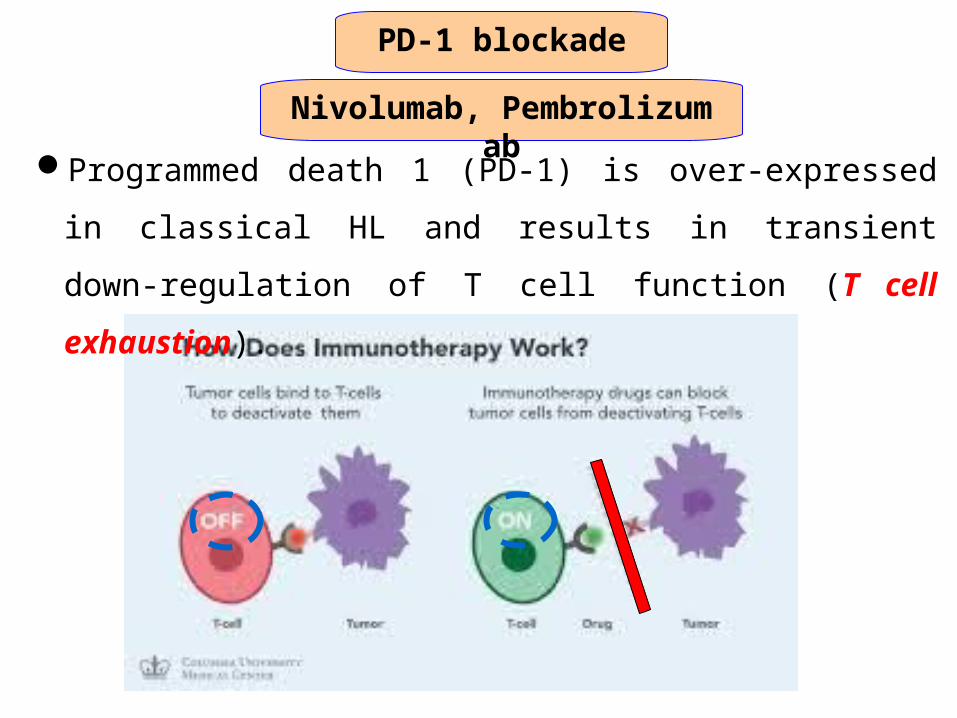
Programmed death 1 (PD-1) is over-expressed in classical HL and
results in transient down-regulation of T cell function (T cell
exhaustion).
PD-1 blockade
Nivolumab, Pembrolizumab
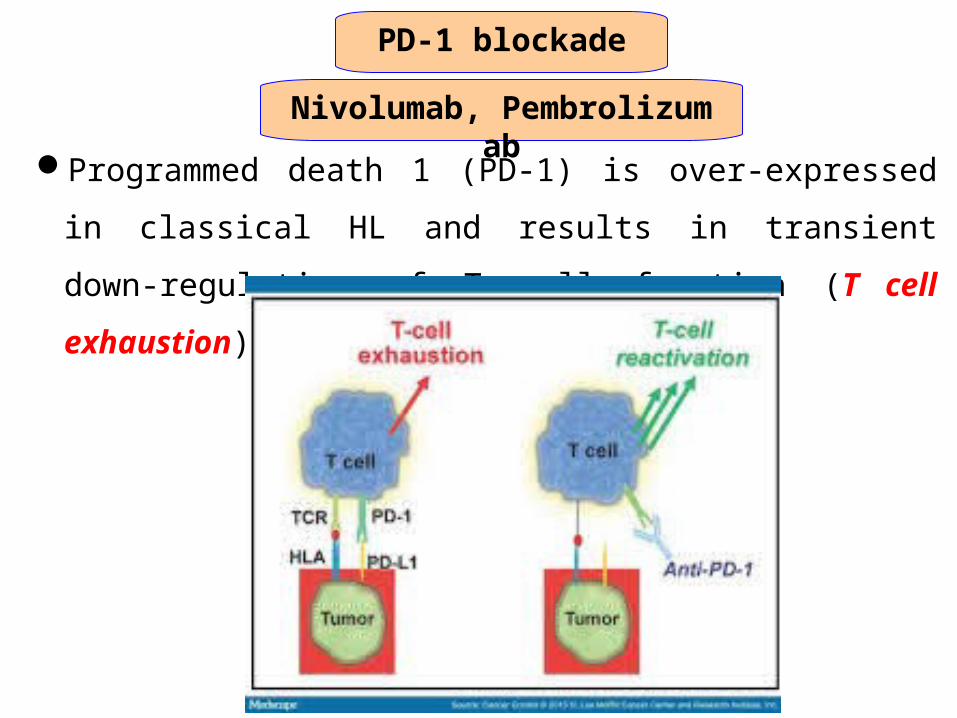
Programmed death 1 (PD-1) is over-expressed in classical HL and
results in transient down-regulation of T cell function (T cell
exhaustion).
PD-1 blockade
Nivolumab, Pembrolizumab
Programmed death 1 (PD-1) is over-expressed in classical HL and
results in transient down-regulation of T cell function (T cell
exhaustion).
Small prospective studies have reported high response rates
with PD-1 inhibitors (eg, nivolumab, pembrolizumab).
Nivolumab (3 mg/kg) was administered
At week 1 and week 4, and
Then every two weeks
Until disease progression or complete response or for
a maximum of two years.
PD-1 blockade
Nivolumab, Pembrolizumab
The most common toxicities were:
Rash (22 %),
Thrombocytopenia (17 %),
Fatigue, pyrexia,diarrhea,nausea, and pruritus (13 %each)
Overall and complete response rates were 87 and 17 %,
respectively.
Further studies are needed to further define efficacy and
toxicity prior to their general clinical use in this setting.
Effects of treatment
Acute effects
1. Radiotherapy effects
2. Chemotherapy effects
Skin: redness & hyper-pigmentation & transient hair thinning in exposed fields.
GIT: Mild nausea and vomiting & dry mouth or mucositis or taste alterationHaematological : neutropenia & thrombocytopenia.
Nausea and vomiting.Reversible alopecia.Myelosuppression and immunosuppresion.Other specific for each drug (VCR→neurotoxicity).
Effects of treatment
Late effects
1. Impaired growth of soft tissue and bone.
2. Thyroid dysfunction
Many of these long-term effects were described initially following treatment regimens that are no longer used in children.
3. Gonadal dysfunction
4. Pulmonary toxicity
5. Cardiac toxicity
6. Secondary malignancies
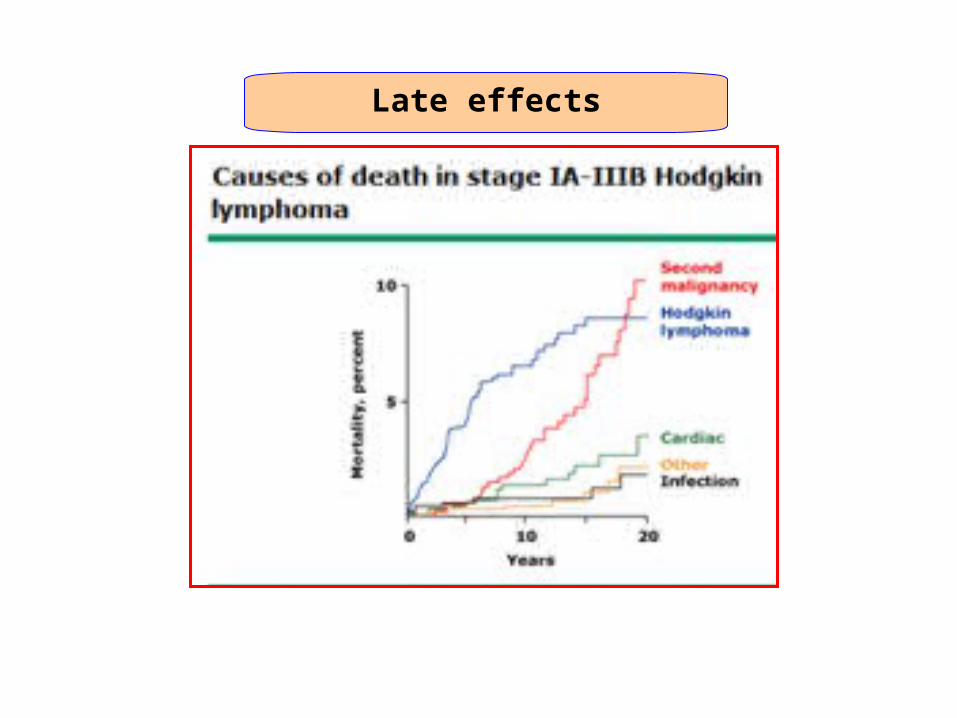
Late effects

THANL YOU