Cáncer de Páncreas estadio IV - academia.cat€¦ · Cáncer de Páncreas estadio IV Barcelona 19...
40
Cáncer de Páncreas estadio IV Barcelona 19 de noviembre 2013 Dra. Antonieta Salud Salvia Servicio de Oncología Médica Hospital Universitari Arnau de Vilanova de LLeida
Transcript of Cáncer de Páncreas estadio IV - academia.cat€¦ · Cáncer de Páncreas estadio IV Barcelona 19...

Cáncer de Páncreas estadio IV
Barcelona 19 de noviembre 2013
Dra. Antonieta Salud Salvia
Servicio de Oncología Médica
Hospital Universitari Arnau de Vilanova de LLeida
EPIDEMIOLOGIA
• 4ª causa de muerte por cáncer en países desarrollados• En Europa en 2000 60.139 nuevos casos, con 64.801 muertos• En USA en 2010 36.800 muertos• Incidencia en aumento
• Etiología desconocida: obesidad, pancreatitis crónica, cirrosis hepática, alcohol, factores genéticos , tabaco, café
• Baja tasa de curaciones• Tasa global de supervivencia a los 5 años <5% • Enfermedad metastática tiene un pronóstico muy pobre
– Mediana Supervivencia Global sin tratamiento es 3 - 6 meses
• No posibilidad de screening eficaz
1. 1.Hariharan D. HPB (Oxford). 2008;10(1):58-62.2. 2.Cancer Facts & Figures 2010. Atlanta, Ga: American Cancer Society; 2010.3. 3.Willett CG, et al. J Clin Oncol. 2005;23(20):4538-4544.

CLINICA
• Síntomas iniciales escasos diagnóstico en estadios avanzados
• Tumor de cabeza el más frecuente- Ictericia afecta al coledoco intrapancreático
• Tumor de cuerpo y cola diagnóstico más tardío
- Dolor epigástrico profundo - Síndrome constitucional, pérdida de peso y anorexia
• Diabetes de nueva aparición 10 % de pacientes

ESTADIFICACIÓN
• Estadio IA (T1N0)• Estadio IB (T2N0)• Estadio IIA (T3N0)
• Estadio IIB (T1,2,3N1)• Estadio III (T4N0,1)• Estadio IV (TNM1)
ENFERMEDAD RESECABLE
L. AVANZADO
IRRESECABLEquimioterapia
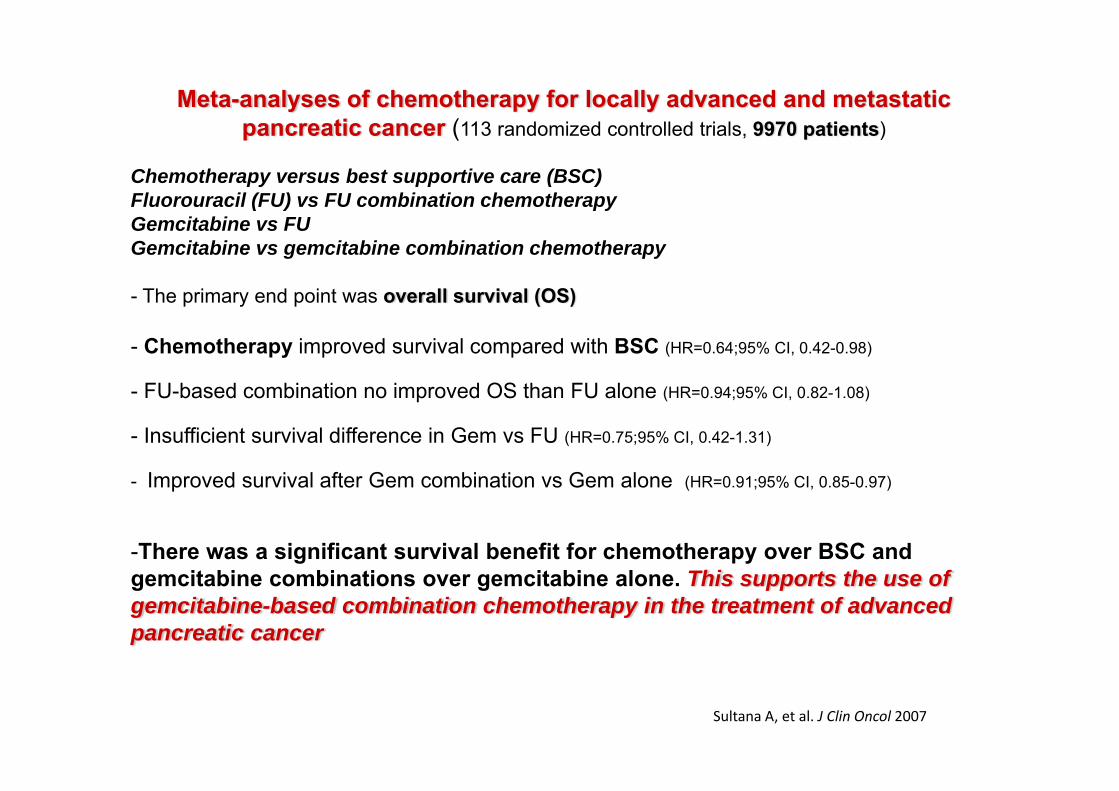
Sultana A, et al. J Clin Oncol 2007
Meta-analyses of chemotherapy for locally advanced and metastaticpancreatic cancer (113 randomized controlled trials, 9970 patients)
Chemotherapy versus best supportive care (BSC)Fluorouracil (FU) vs FU combination chemotherapyGemcitabine vs FUGemcitabine vs gemcitabine combination chemotherapy
- The primary end point was overall survival (OS)
- Chemotherapy improved survival compared with BSC (HR=0.64;95% CI, 0.42-0.98)
- FU-based combination no improved OS than FU alone (HR=0.94;95% CI, 0.82-1.08)
- Insufficient survival difference in Gem vs FU (HR=0.75;95% CI, 0.42-1.31)
- Improved survival after Gem combination vs Gem alone (HR=0.91;95% CI, 0.85-0.97)
-There was a significant survival benefit for chemotherapy over BSC and gemcitabine combinations over gemcitabine alone. This supports the use of gemcitabine-based combination chemotherapy in the treatment of advancedpancreatic cancer
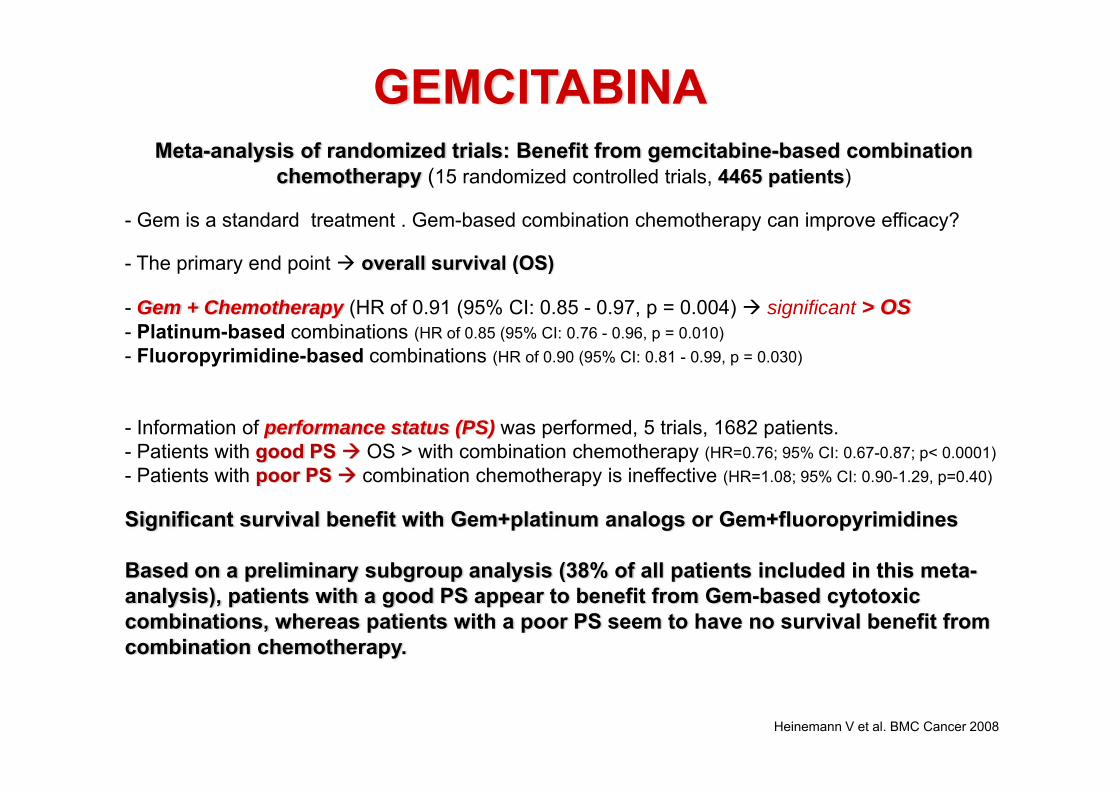
GEMCITABINAMeta-analysis of randomized trials: Benefit from gemcitabine-based combination
chemotherapy (15 randomized controlled trials, 4465 patients)
- Gem is a standard treatment . Gem-based combination chemotherapy can improve efficacy?
- The primary end point overall survival (OS)
- Gem + Chemotherapy (HR of 0.91 (95% CI: 0.85 - 0.97, p = 0.004) significant > OS- Platinum-based combinations (HR of 0.85 (95% CI: 0.76 - 0.96, p = 0.010)- Fluoropyrimidine-based combinations (HR of 0.90 (95% CI: 0.81 - 0.99, p = 0.030)
- Information of performance status (PS) was performed, 5 trials, 1682 patients.- Patients with good PS OS > with combination chemotherapy (HR=0.76; 95% CI: 0.67-0.87; p< 0.0001) - Patients with poor PS combination chemotherapy is ineffective (HR=1.08; 95% CI: 0.90-1.29, p=0.40)
Significant survival benefit with Gem+platinum analogs or Gem+fluoropyrimidines
Based on a preliminary subgroup analysis (38% of all patients included in this meta-analysis), patients with a good PS appear to benefit from Gem-based cytotoxic combinations, whereas patients with a poor PS seem to have no survival benefit from combination chemotherapy.
Heinemann V et al. BMC Cancer 2008
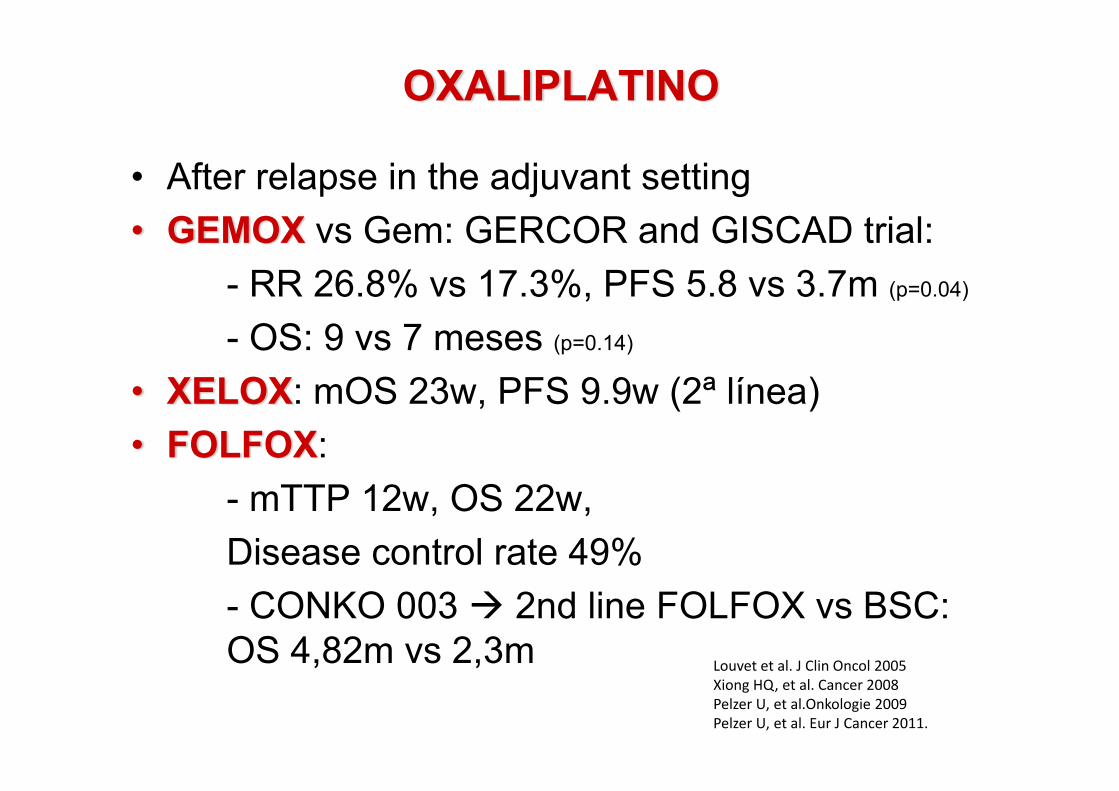
OXALIPLATINO
• After relapse in the adjuvant setting• GEMOX vs Gem: GERCOR and GISCAD trial:
- RR 26.8% vs 17.3%, PFS 5.8 vs 3.7m (p=0.04)
- OS: 9 vs 7 meses (p=0.14)
• XELOX: mOS 23w, PFS 9.9w (2ª línea)• FOLFOX:
- mTTP 12w, OS 22w, Disease control rate 49% - CONKO 003 2nd line FOLFOX vs BSC: OS 4,82m vs 2,3m Louvet et al. J Clin Oncol 2005
Xiong HQ, et al. Cancer 2008Pelzer U, et al.Onkologie 2009Pelzer U, et al. Eur J Cancer 2011.

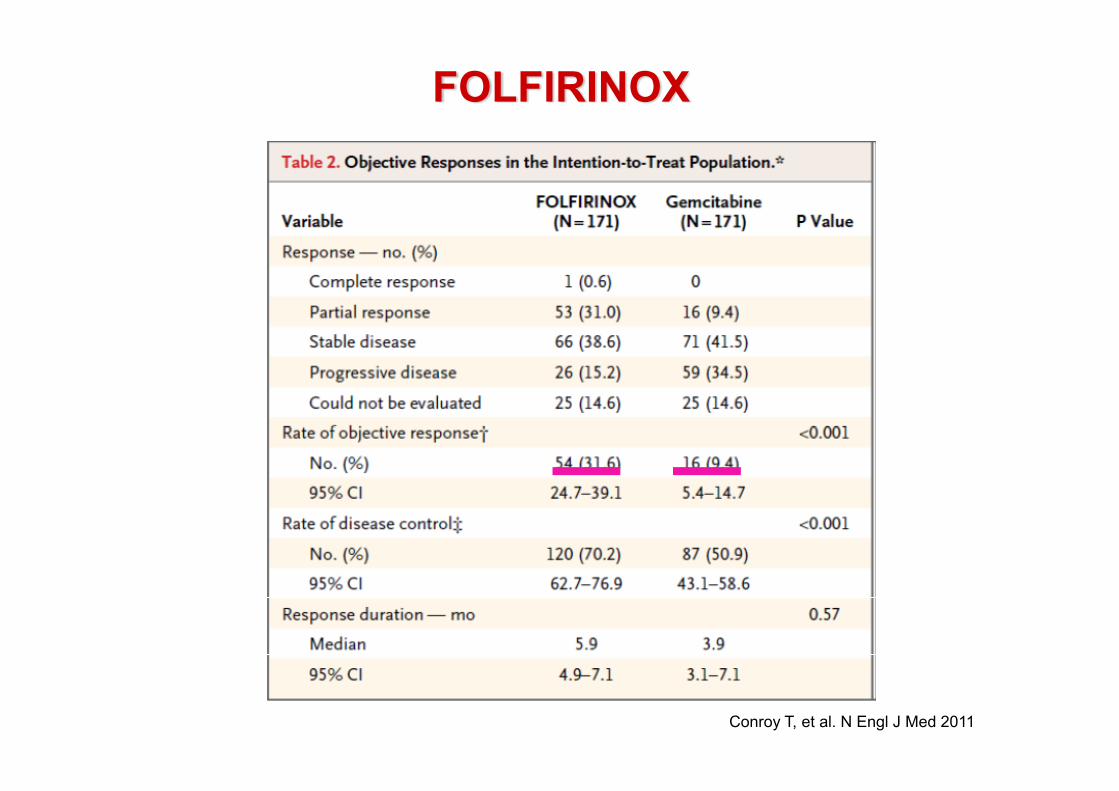
FOLFIRINOX
– Phase II/III– 342 patients– ECOG 0-1– FOLFIRINOX (N=171) vs GEM 1000mg/m2 (N=171)– Median number cycles
• FOLFIRINOX 10 (1-47) vs GEM 6 (1-26)– Disease progression before 12 cycles
• FOLFIRINOX 54.6% vs GEM 79.9%Conroy T, et al. N Engl J Med 2011
Oxaliplatin 85mg/m2
Irinotecan 180mg/m2
5FU bolus 400mg/m2
Ci 2400mg/m2 46h
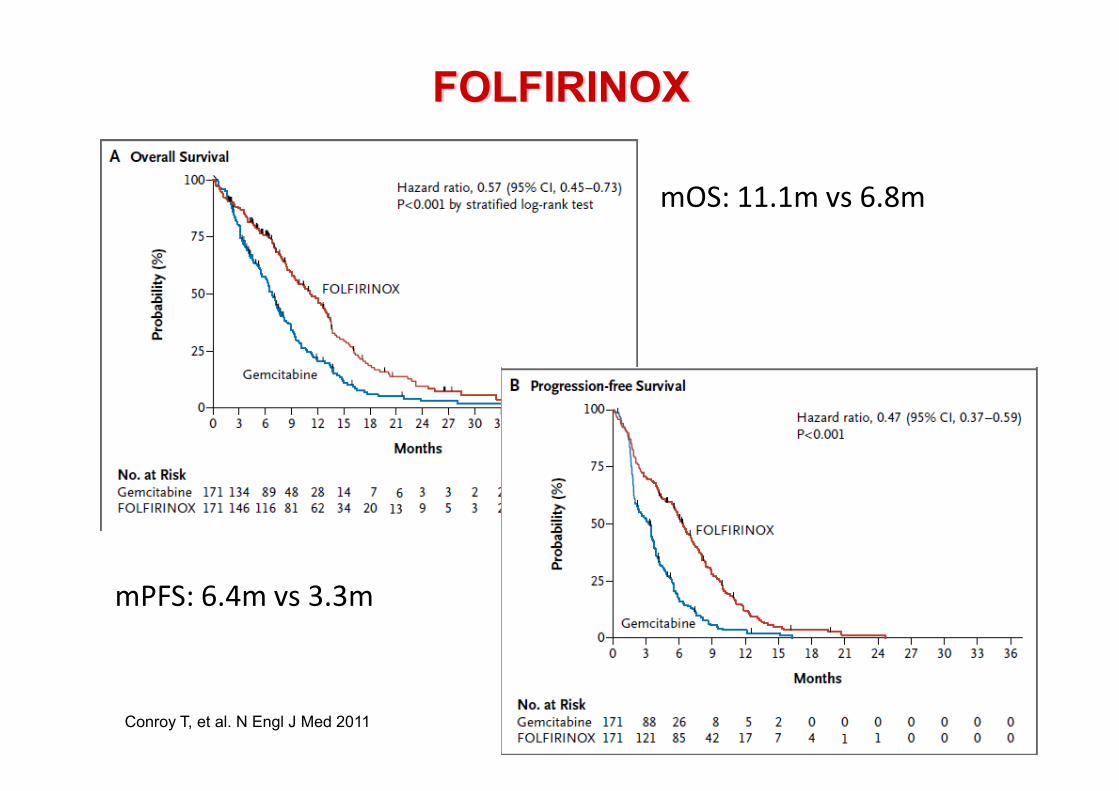
FOLFIRINOX
Conroy T, et al. N Engl J Med 2011
FOLFIRINOX
Conroy T, et al. N Engl J Med 2011
mOS: 11.1m vs 6.8m
mPFS: 6.4m vs 3.3m
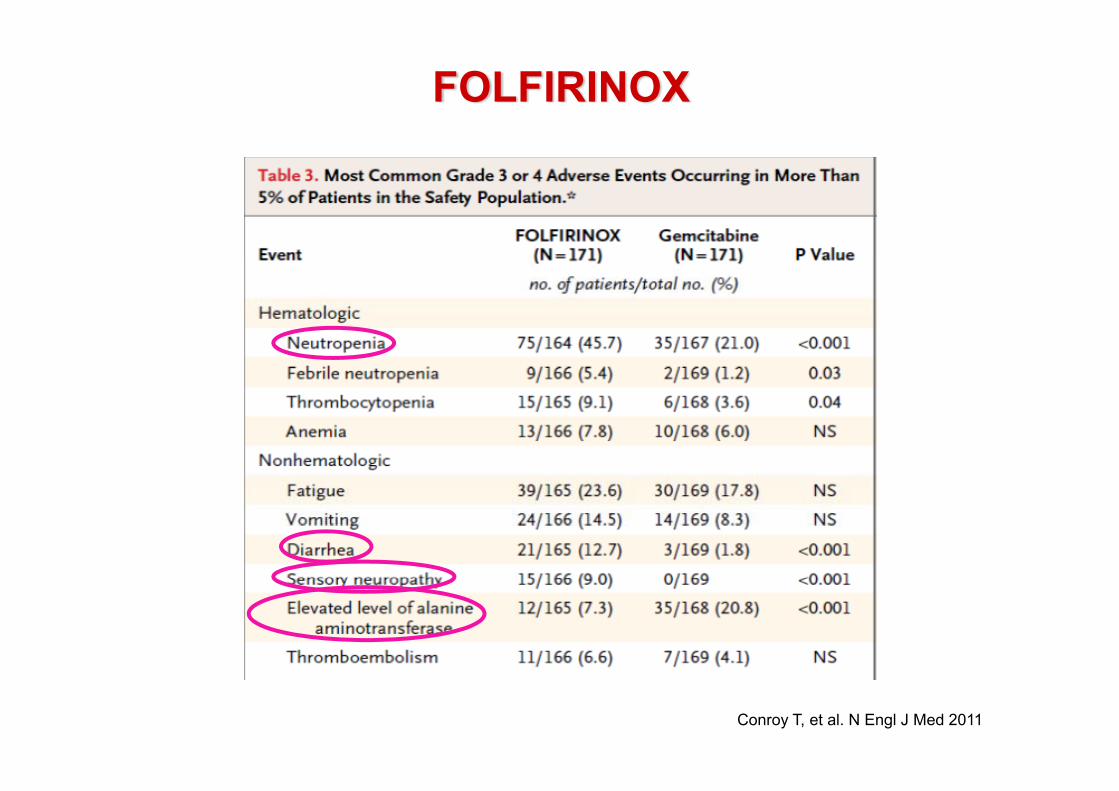
FOLFIRINOX
Conroy T, et al. N Engl J Med 2011
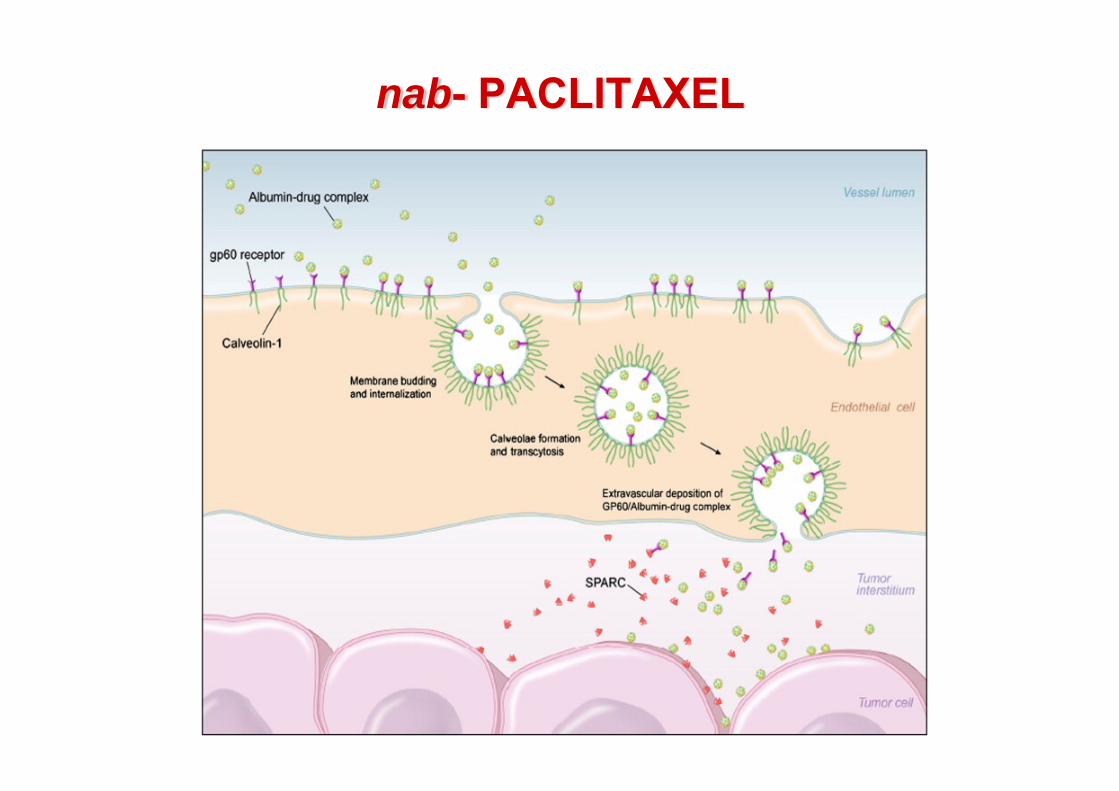
nab- PACLITAXEL
IV, intravenous; MTD, maximum tolerated dose.
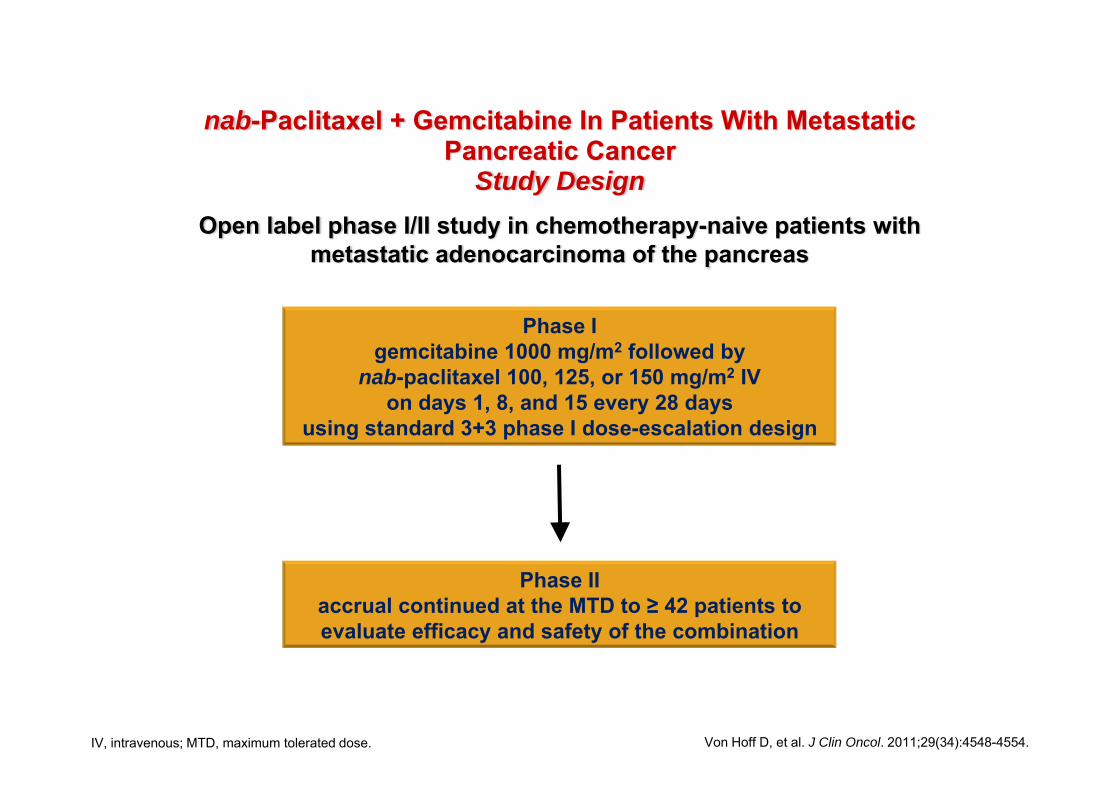
Open label phase I/II study in chemotherapy-naive patients with metastatic adenocarcinoma of the pancreas
Phase Igemcitabine 1000 mg/m2 followed by
nab-paclitaxel 100, 125, or 150 mg/m2 IV on days 1, 8, and 15 every 28 days
using standard 3+3 phase I dose-escalation design
Phase II accrual continued at the MTD to ≥ 42 patients to evaluate efficacy and safety of the combination
Von Hoff D, et al. J Clin Oncol. 2011;29(34):4548-4554.
nab-Paclitaxel + Gemcitabine In Patients With Metastatic Pancreatic Cancer
Study Design

nab-Paclitaxel + Gemcitabine in Pancreatic Cancer
• - Preclinical models– . nab-Paclitaxel (nab-P) active as single agent– . Synergistic activity in combination with gemcitabine– nab-Paclitaxel improved intratumoral concentration of
gemcitabine• - In a 67-patient phase I/II trial of nab-P + Gem
– . MTD: nab-P 125 mg/m2 + Gem 1000 mg/m2 days 1, 8, and 15 every 28 days
– . Promising activity at MTD• ORR: 48%• Median PFS: 7.9 months• Median OS: 12.2 months
1. Von Hoff DD, et al. J Clin Oncol. 2011;29:4548-4554. 2. Frese KK, et al. Cancer Discov. 2012;2:260-269.Gem, gemcitabine; MTD, maximum tolerated dose; OS, overall survival.
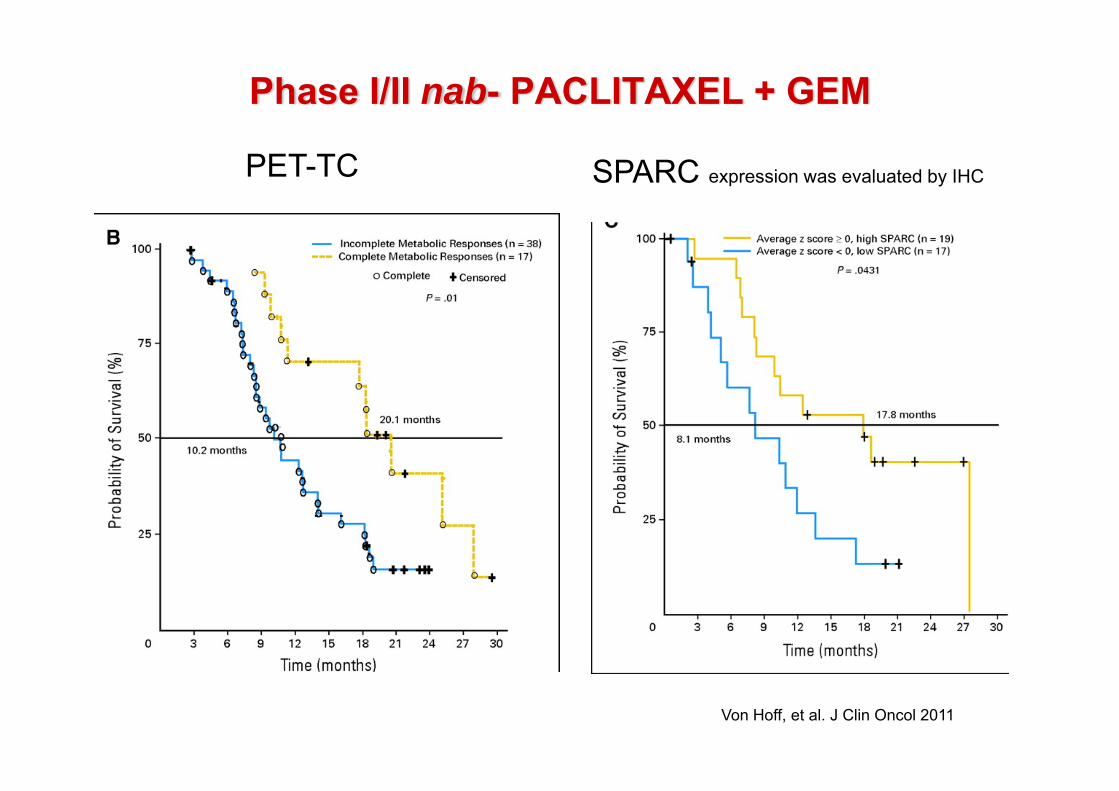
Phase I/II nab- PACLITAXEL + GEM
Von Hoff, et al. J Clin Oncol 2011
PET-TC SPARC expression was evaluated by IHCby IHC

Personalized Treatment: SPARC as a Biomarker
Marker Effect
SPARC
• . High SPARC mRNA expression in the stroma was associated with a poorer prognosis than low SPARC, historically
• . Inverse correlation between SPARC expression in distal stromal cells and survival
• . Stromal SPARC expression may be an important marker of early activity of gemcitabine plus nab-paclitaxel combination regimens
PaC, advanecd pancreatic cancer; SPARC, secreted protein acidic and rich in cysteine.
1.Infante JR, et al. J Clin Oncol. 2007;25:319-325.2.Miyoshi K, et al. Anticancer Res. 2010;30:867-871.
3.Mantoni TS, et al. Cancer Biol Ther. 2008;7:1806-1815.4.Von Hoff D, et al. J Clin Oncol. 2011;29:4548-4554.
IHC, immunohistochemistry. 1.Von Hoff D, et al. J Clin Oncol. 2011;29(34):4548-4554.
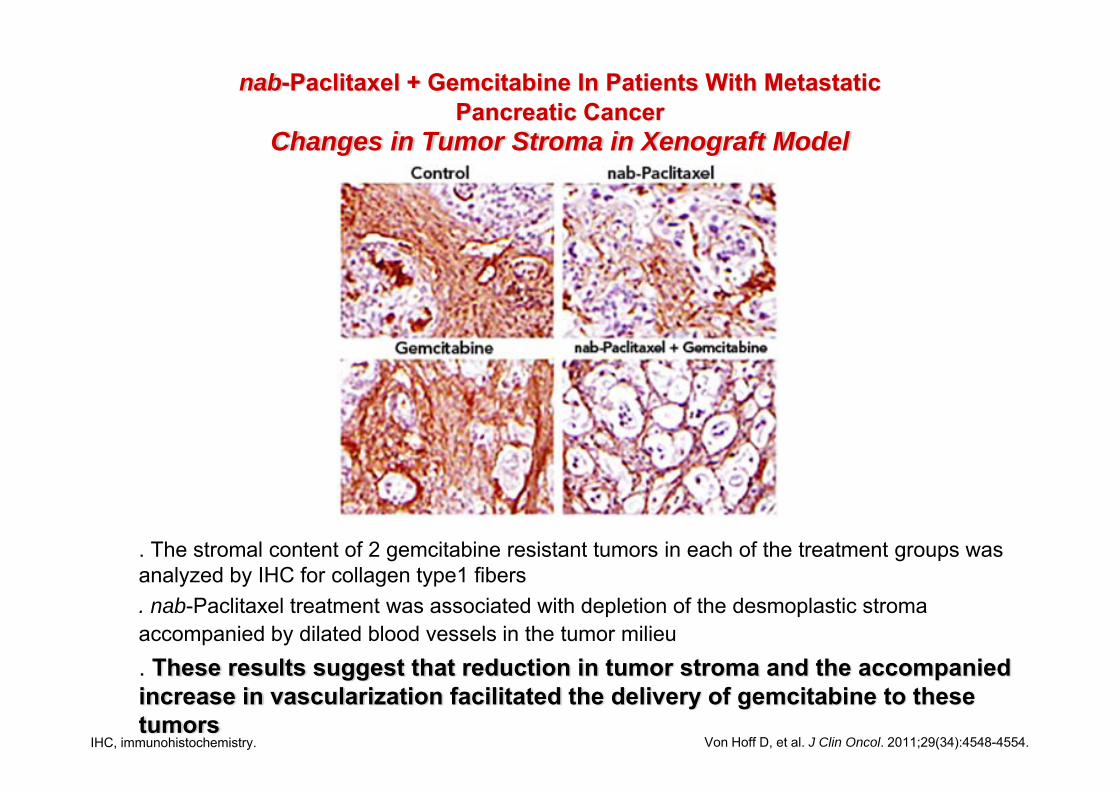
nab-Paclitaxel + Gemcitabine In Patients With Metastatic Pancreatic Cancer
Changes in Tumor Stroma in Xenograft Model
• . The stromal content of 2 gemcitabine resistant tumors in each of the treatment groups was analyzed by IHC for collagen type1 fibers
• . nab-Paclitaxel treatment was associated with depletion of the desmoplastic stroma accompanied by dilated blood vessels in the tumor milieu
• . These results suggest that reduction in tumor stroma and the accompanied increase in vascularization facilitated the delivery of gemcitabine to these tumors
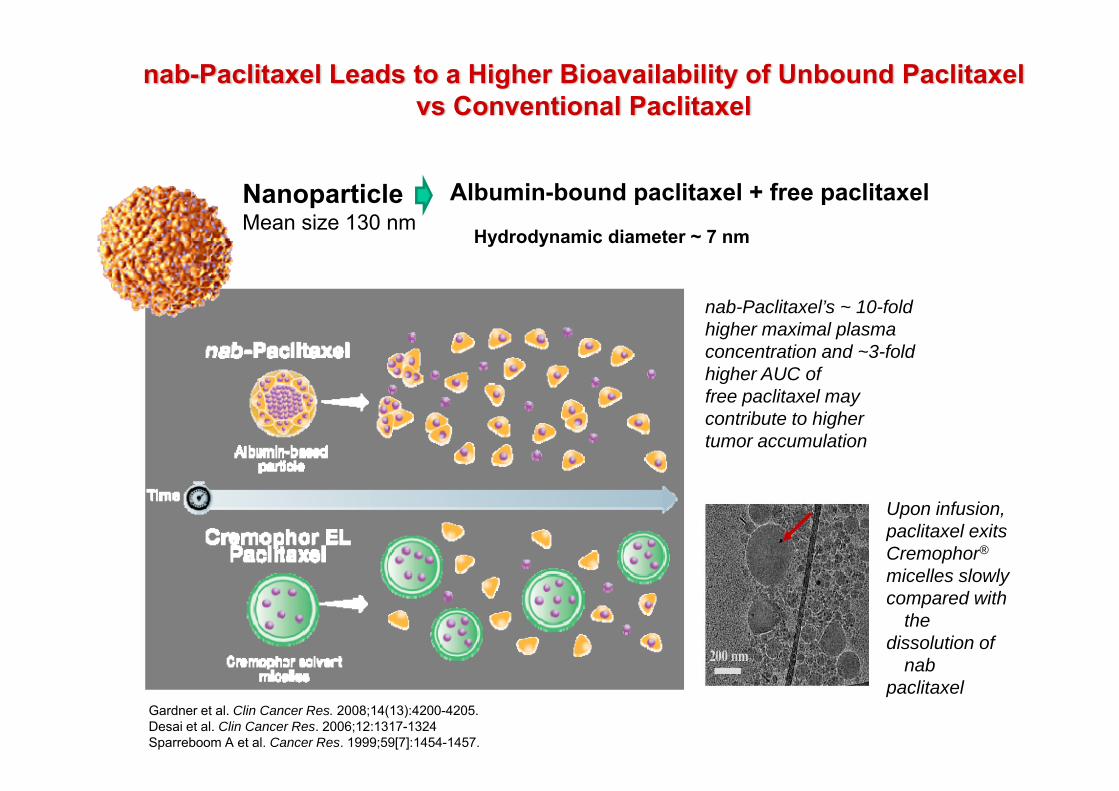
nab-Paclitaxel Leads to a Higher Bioavailability of Unbound Paclitaxel vs Conventional Paclitaxel
NanoparticleMean size 130 nm
Albumin-bound paclitaxel + free paclitaxel
Hydrodynamic diameter ~ 7 nm
nab-Paclitaxel’s ~ 10-fold higher maximal plasma concentration and ~3-fold higher AUC offree paclitaxel may contribute to higher tumor accumulation
Upon infusion,paclitaxel exitsCremophor®
micelles slowlycompared with
thedissolution of
nabpaclitaxel
Gardner et al. Clin Cancer Res. 2008;14(13):4200-4205. Desai et al. Clin Cancer Res. 2006;12:1317-1324 Sparreboom A et al. Cancer Res. 1999;59[7]:1454-1457.
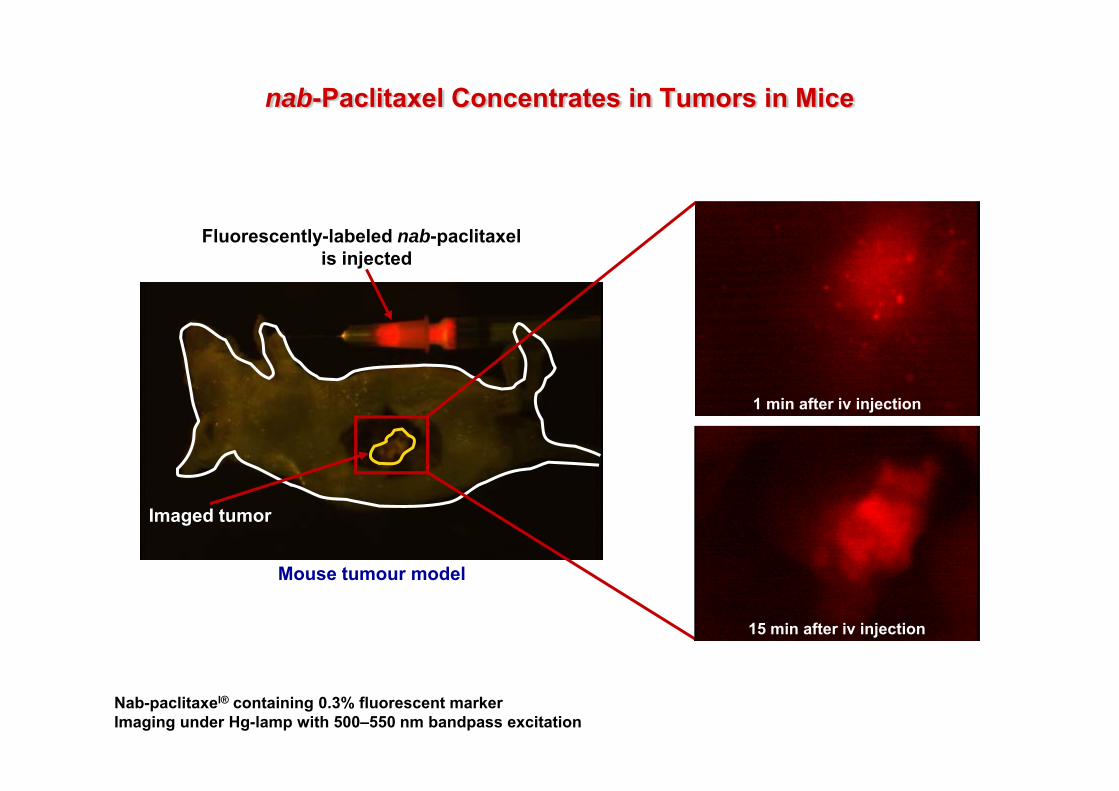
nab-Paclitaxel Concentrates in Tumors in Mice
Nab-paclitaxel® containing 0.3% fluorescent markerImaging under Hg-lamp with 500–550 nm bandpass excitation
Mouse tumour model
1 min after iv injection
Imaged tumor
Fluorescently-labeled nab-paclitaxel is injected
15 min after iv injection

nab-Paclitaxel Demonstrates Greater Tumor Selectivity
Rel
ativ
e co
ncen
trat
ion
(nab
-Pac
litax
el/C
onve
ntio
nal p
aclit
axel
)
0
0.5
1.0
1.5
• Comparative tissue distribution (ratio) of radiolabeled drug in mice bearing human breast tumor xenografts 1 hour after dose
nab®-Paclitaxel > Conv paclitaxel
<nab®-Paclitaxel Conv paclitaxel
=nab®-Paclitaxel Conv paclitaxel
nab® is a registered trademark of Celgene Corporation.conv, conventional.
1. Hawkins et al. AACR. 2003. Poster 1189.2. Scheff . Community Oncol. 2008;5(7 suppl 8):7-13.
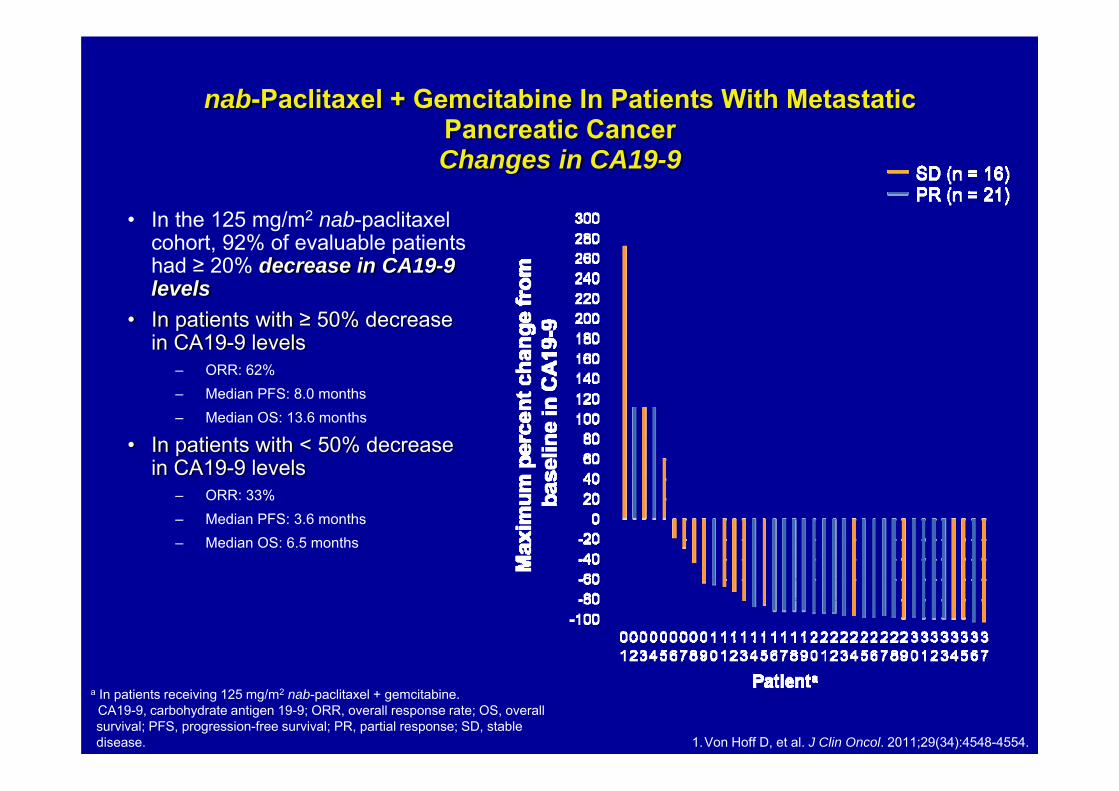
nab-Paclitaxel + Gemcitabine In Patients With Metastatic Pancreatic Cancer Changes in CA19-9
• In the 125 mg/m2 nab-paclitaxel cohort, 92% of evaluable patients had ≥ 20% decrease in CA19-9 levels
• In patients with ≥ 50% decrease in CA19-9 levels
– ORR: 62%– Median PFS: 8.0 months– Median OS: 13.6 months
• In patients with < 50% decrease in CA19-9 levels
– ORR: 33%– Median PFS: 3.6 months– Median OS: 6.5 months
a In patients receiving 125 mg/m2 nab-paclitaxel + gemcitabine.CA19-9, carbohydrate antigen 19-9; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; SD, stable disease. 1.Von Hoff D, et al. J Clin Oncol. 2011;29(34):4548-4554.

nab®-Paclitaxel + Gemcitabine In Patients With Metastatic Pancreatic Cancer
(Phase I/II)Conclusions
• - nab-Paclitaxel + gemcitabine was generally well tolerated in patients with advanced pancreatic cancer
– MTD established as nab-paclitaxel 125 mg/m2 + gemcitabine 1000 mg/m2
• - nab-Paclitaxel + gemcitabine demonstrated substantial activity in pancreatic cancer
• - Preliminary analysis suggested that SPARC positivity correlated with increased median OS
• - Decrease in serum CA19-9 levels ≥ 50% was observed in a majority of patients and correlated with median PFS and OS
CA19-9, carbohydrate antigen 19-9; MTD, maximum tolerated dose; OS, overall survival; PFS, progression-free survival; SPARC, secreted protein acidic and rich in cysteine. Von Hoff D, et al. J Clin Oncol. 2011;29(34):4548-4554

Randomized Phase III Study of Weekly nab-Paclitaxel Plus Gemcitabine vs Gemcitabine Alone in Patients With Metastatic Adenocarcinoma of the
Pancreas (MPACT)
DD Von Hoff, T Ervin, FP Arena, EG Chiorean, J Infante, M Moore,T Seay, SA Tjulandin, W Ma, MN Saleh, M Harris, M Reni, RK Ramanathan, J Tabernero, M Hidalgo, E Van Cutsem,
D Goldstein, X Wei, J Iglesias, MF Renschler
Von Hoff DD, et al. N Engl J Med. 2013

1:1, stratified by KPS, region, liver metastasis
Planned N = 842
• Stage IV• No prior treatment for metastatic disease• KPS ≥ 70 • Measurable disease• Total bilirubin ≤ ULN
431: nab-Paclitaxel125 mg/m2 IV qw 3/4 weeks
+Gemcitabine
1000 mg/m2 IV qw 3/4 weeks
430: Gemcitabine1000 mg/m2 IV qw for 7/8 weeks
then qw 3/4 weeks
24
Primary endpoint: – OSSecondary endpoints:– PFS and ORR by independent
review (RECIST)Safety and tolerability– by NCI CTCAE v3.0
• With 608 events, 90% power to detect OS HR = 0.769 (2-sided α = 0.049)
• One interim analysis for futility• Treat until progression• CT scans every 8 weeks
Phase III MPACT: Study Design
Von Hoff DD, et al. N Engl J Med. 2013
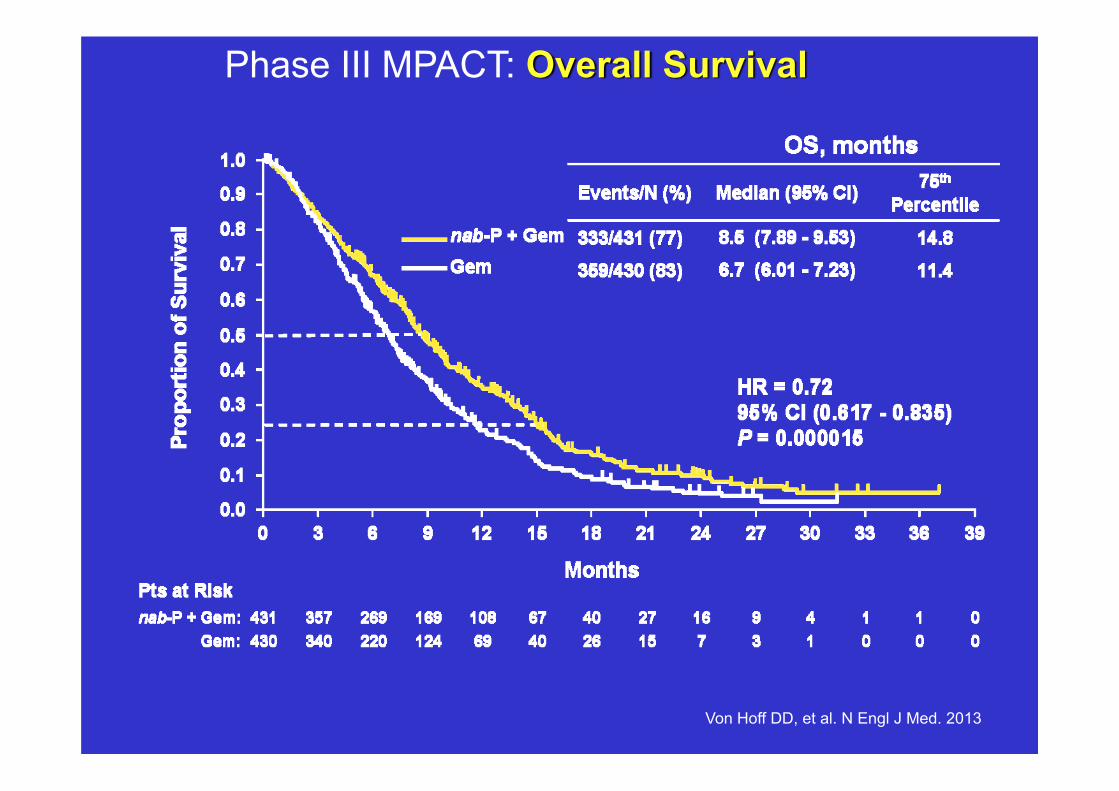
Phase III MPACT: Overall Survival
Von Hoff DD, et al. N Engl J Med. 2013
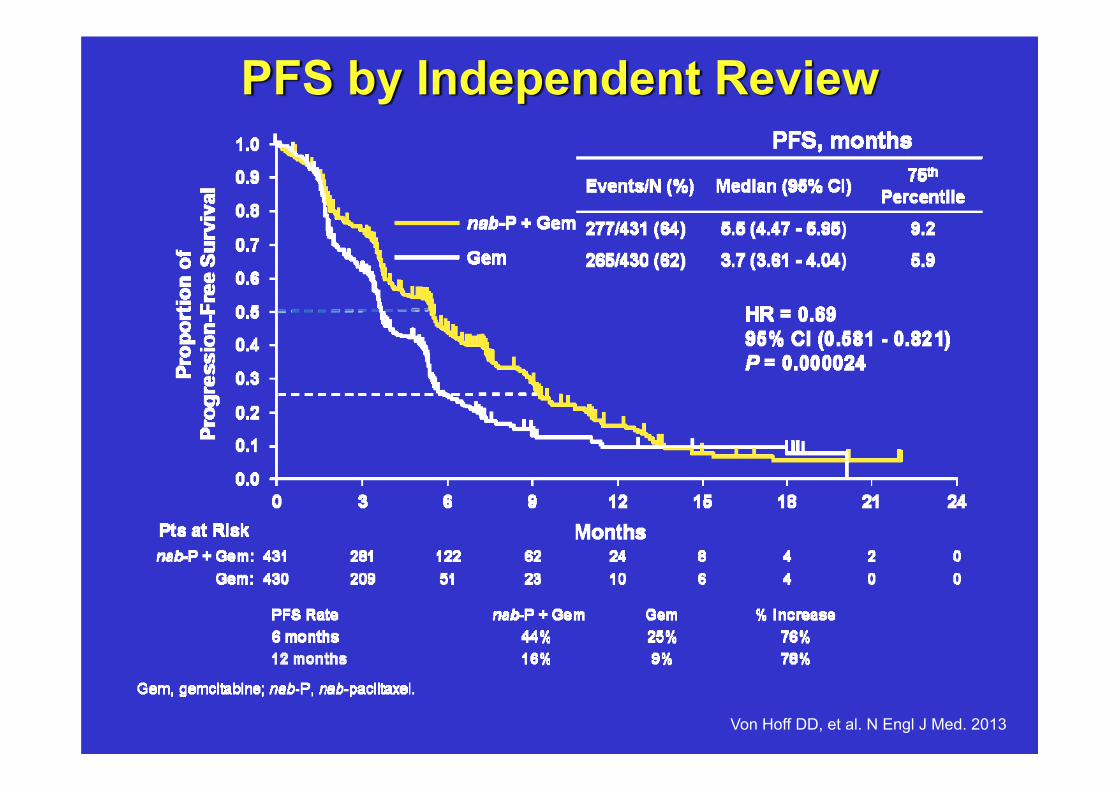
PFS by Independent Review
Von Hoff DD, et al. N Engl J Med. 2013

Phase III MPACT: Response Rate
Variablenab-P +
Gemn = 431
Gemn = 430 P Value
Overall response rateIndependent review %
(95% CI)Investigator assessment
%(95% CI)
23 (19.1 - 27.2)
29 (25.0 - 33.8)
7 (5.0 - 10.1)
8 (5.3 - 10.6)
<0.001
3.3 × 10−16
Disease control rateindependent review %
(95% CI)48
(43.0 - 52.6)33
(28.4 - 37.5)
7.2 × 10−6
Von Hoff DD, et al. N Engl J Med. 2013
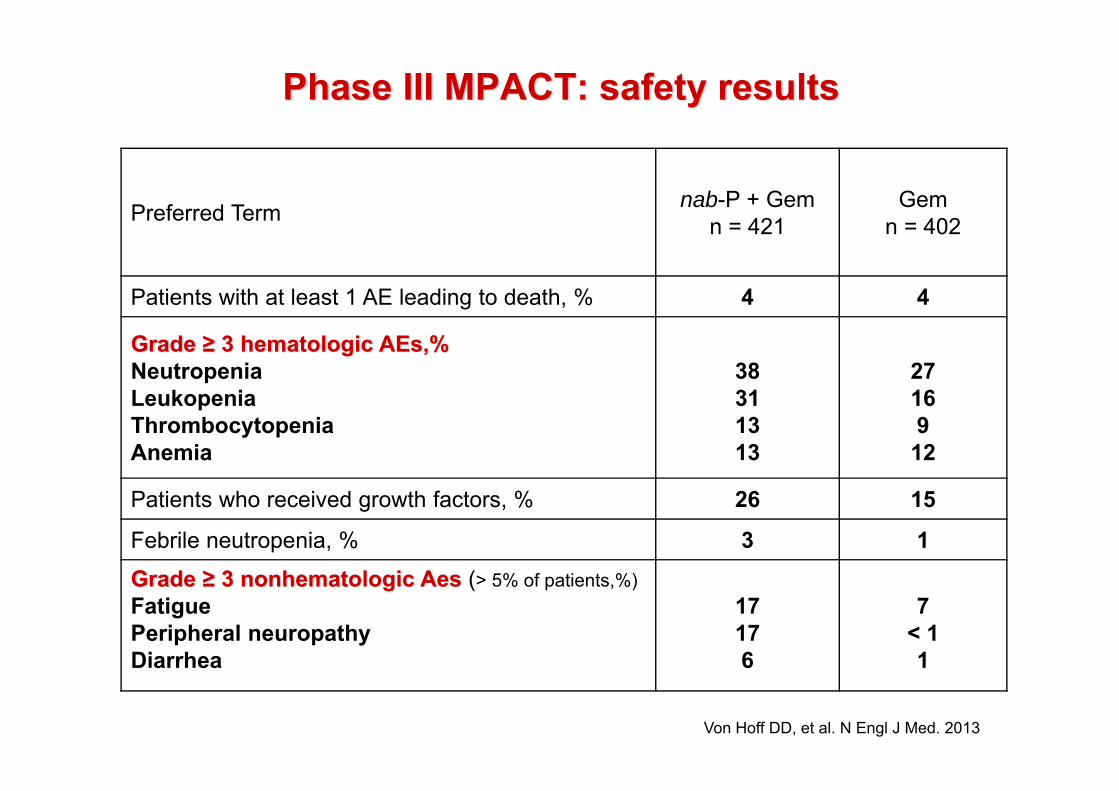
Phase III MPACT: safety results
Preferred Term nab-P + Gemn = 421
Gemn = 402
Patients with at least 1 AE leading to death, % 4 4
Grade ≥ 3 hematologic AEs,%Neutropenia Leukopenia ThrombocytopeniaAnemia
38311313
2716912
Patients who received growth factors, % 26 15
Febrile neutropenia, % 3 1Grade ≥ 3 nonhematologic Aes (> 5% of patients,%)FatiguePeripheral neuropathyDiarrhea
17176
7< 11
Von Hoff DD, et al. N Engl J Med. 2013
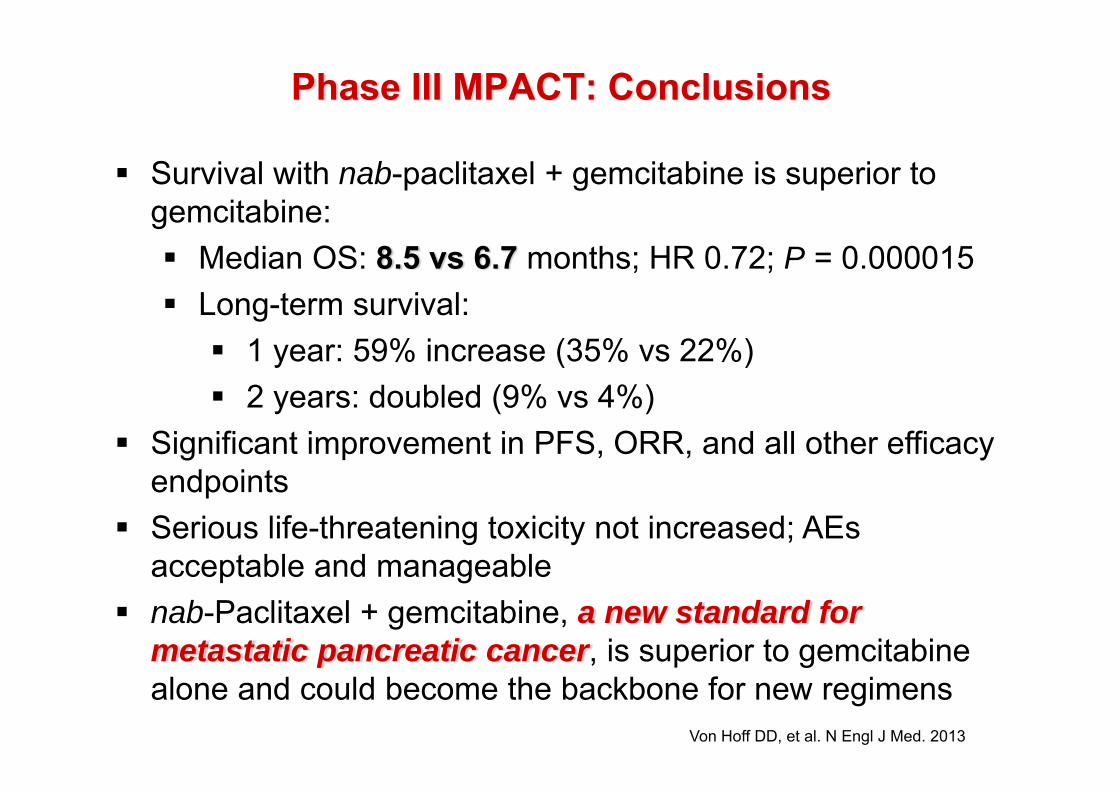
Phase III MPACT: Conclusions
Survival with nab-paclitaxel + gemcitabine is superior to gemcitabine:
Median OS: 8.5 vs 6.7 months; HR 0.72; P = 0.000015Long-term survival:
1 year: 59% increase (35% vs 22%)2 years: doubled (9% vs 4%)
Significant improvement in PFS, ORR, and all other efficacy endpointsSerious life-threatening toxicity not increased; AEs acceptable and manageablenab-Paclitaxel + gemcitabine, a new standard for metastatic pancreatic cancer, is superior to gemcitabine alone and could become the backbone for new regimens
Von Hoff DD, et al. N Engl J Med. 2013
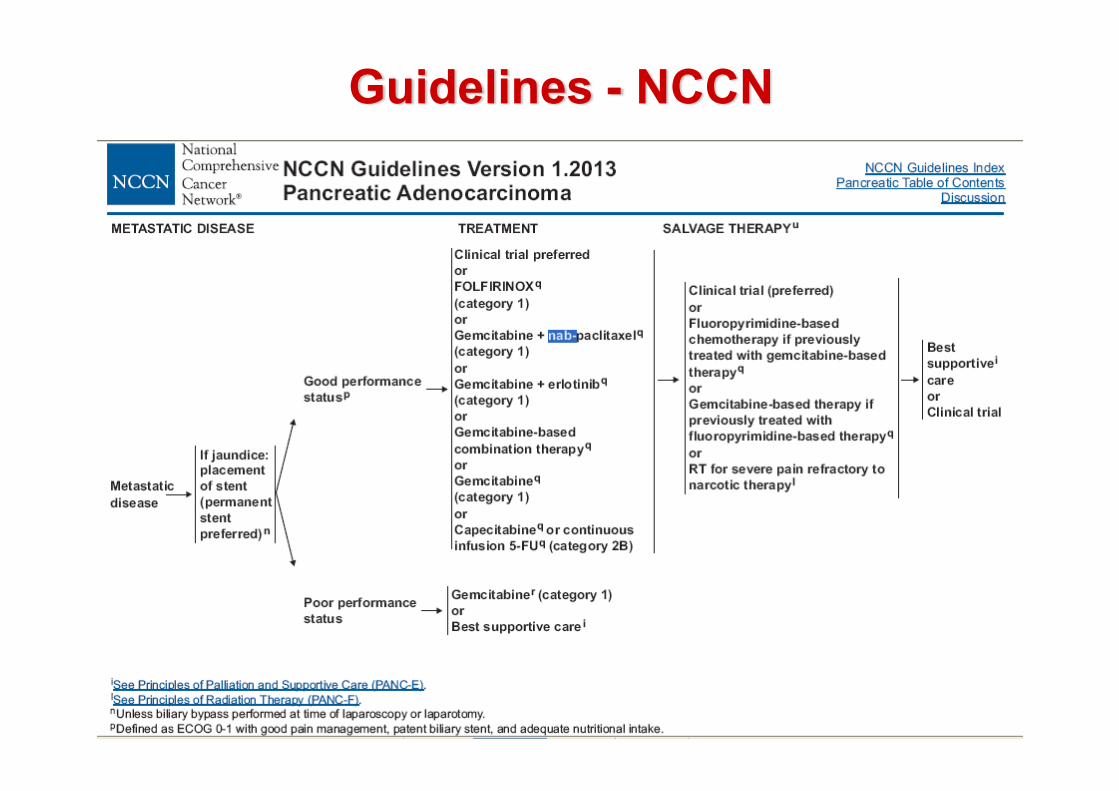
Guidelines - NCCN

Treatment Options: Overview of NCCN Guidelines
• - Metastatic: Acceptable chemotherapy combinations for patients with good performance status
– FOLFIRINOX (Category 1)– Gemcitabine + nab-paclitaxel (Category 1)– Gemcitabine + erlotinib (Category 1)– Gemcitabine + capecitabine (Category 2A)– Gemcitabine + cisplatin (Category 2A)– Fixed-dose rate gemcitabine + docetaxel + capecitabine (GTX regimen) (Category 2B)– Fluropyrimidine + oxaliplatin (Category 2B)
• - Metastatic: Acceptable monotherapy options for patients with poor performance status
– Gemcitabine at 1000 mg/m2 over 30 minutes, weekly for 3 weeks every 28 days (Category 1)
– Capecitabine or continuous infusion 5-FU (Category 2B)
• - The NCCN strongly encourages patients with pancreatic cancer to enroll in clinical trials
1.NCCN Clinical Practice Guidelines in Oncology, Pancreatic Adenocarcinoma, v1.2013.
5-FU, 5-fluorouracil; FOLFIRINOX, 5-FU/LV + irinotecan + oxaliplatin; LV, leucovorin; NCCN, National Comprehensive Cancer Network.
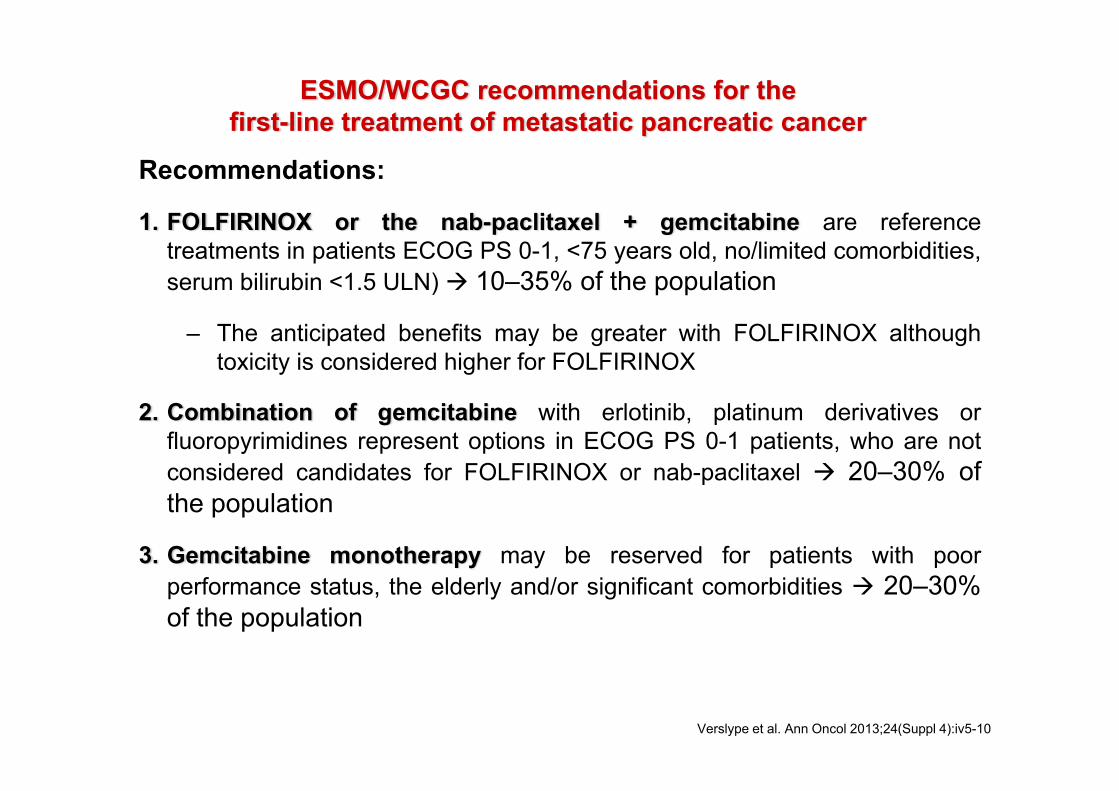
ESMO/WCGC recommendations for the first-line treatment of metastatic pancreatic cancer
Recommendations:
1. FOLFIRINOX or the nab-paclitaxel + gemcitabine are referencetreatments in patients ECOG PS 0-1, <75 years old, no/limited comorbidities,serum bilirubin <1.5 ULN) 10–35% of the population
– The anticipated benefits may be greater with FOLFIRINOX althoughtoxicity is considered higher for FOLFIRINOX
2. Combination of gemcitabine with erlotinib, platinum derivatives orfluoropyrimidines represent options in ECOG PS 0-1 patients, who are notconsidered candidates for FOLFIRINOX or nab-paclitaxel 20–30% ofthe population
3. Gemcitabine monotherapy may be reserved for patients with poorperformance status, the elderly and/or significant comorbidities 20–30%of the population
Verslype et al. Ann Oncol 2013;24(Suppl 4):iv5-10

Nab-paclitaxel + Gem or FOLFIRINOX?Summary results of MPACT study and FOLFIRINOX
Efficacy parameters Nab-paclitaxel + gemcitabine
FOLFIRINOX
Median overall survival 8.7 months 11.1 monthsMedian progression free survival 5.5 months 6.4 monthsResponse rate 23% 32.9%
Toxicities of MPACT study and FOLFIRINOX
Adverse events (grade ≥3) Nab-paclitaxel + gemcitabine
FOLFIRINOX
Fatigue 17% 24%Diarrhea 6% 13%Neutropenia 38% 46%Febrile neutropenia 3% 5%Peripheral neuropathy 17% 9%Thrombocytopenia 13% 9%

Farmacoeconomía

FOLFIRINOX
Gemcitabina Gemcitabina Abraxane ® Oxaliplatino Leucovorin Irinotecan5‐FU (bolo)
5‐FU (infusión contínua)
PVL 50.20 € 50.20 € 240 165.2 6.8 245 3.67 3.67
PVL ‐7,5% RD 8/2010 (marcas) 222
mg/vial o mg/comp 1000 1000 100 100 100 500 100 100
Pauta de tratamiento (mg/m²) 1000 1000 125 85 400 180 400 2400
Superficie corporal (m²) 1.7 1.7 1.7 1.7 1.7 1.7 1.7 1.7
Dosis/dia (mg) 1700 1700 212.5 170 680 306 680 4080
Viales/dia 1.7 1.7 2 1.7 6.8 0.6 6.8 40.8
Dias tratamiento/ciclo 3 3 3 2 2 2 2 2
Numero de ciclos (PFS) 3.7 5.5 5.5 6.4 6.4 6.4 6.4 6.4
Coste tratamiento (reutilización vial) 947.27 1,408.11 € 7783.88 3594.75 592 1919.23 319 1916.62
Coste tratamiento (reutilización vial) 947 € 9191,99 € 8341,91 €

36Abraxane® Gemcitabina Tarceva (erlotinib) Gemcitabina
PVL 240 50.2 2045.4 50.2
PVL ‐ 7,5% RD 8/2010 (marcas)
222 1892
Mg per vial o mg/comp 100 1000 150 1000
Pauta de tratamiento (mg/m2)
125 1000 100 1000
Superficie corporal (m2)
1.7 1.7 1.7 1.7
Dosis/día (mg) 212.5 1700 100 1700Viales/día 2.1 1.7 1.7
Días tratamiento/ciclo 3 3 28 3
Número de ciclos 5.5 5.5 3.75 3.75
Coste por tratamiento (reutilización vial)
€7,783.88
€1,408.11
€6,622.35
€960.08
Coste por tratamiento(reutilización vial) 9191,99 € 7582,43 €
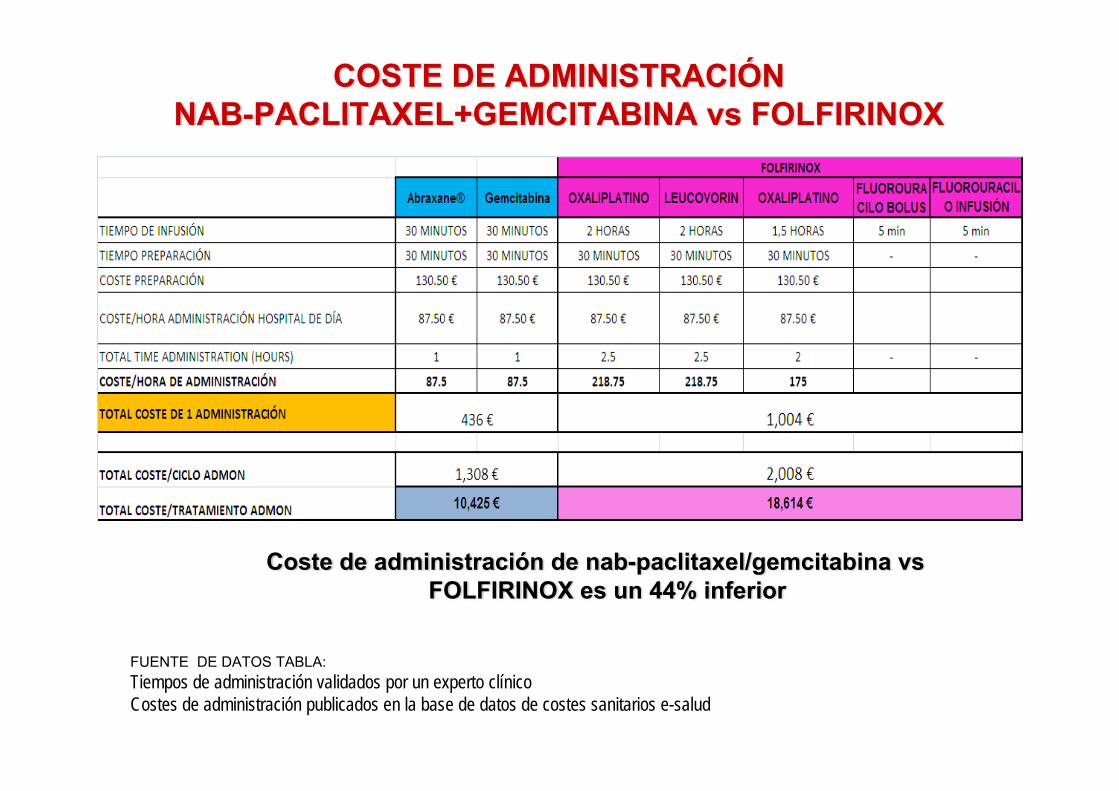
COSTE DE ADMINISTRACIÓN NAB-PACLITAXEL+GEMCITABINA vs FOLFIRINOX
Coste de administración de nab-paclitaxel/gemcitabina vs FOLFIRINOX es un 44% inferior
FUENTE DE DATOS TABLA:Tiempos de administración validados por un experto clínicoCostes de administración publicados en la base de datos de costes sanitarios e-salud
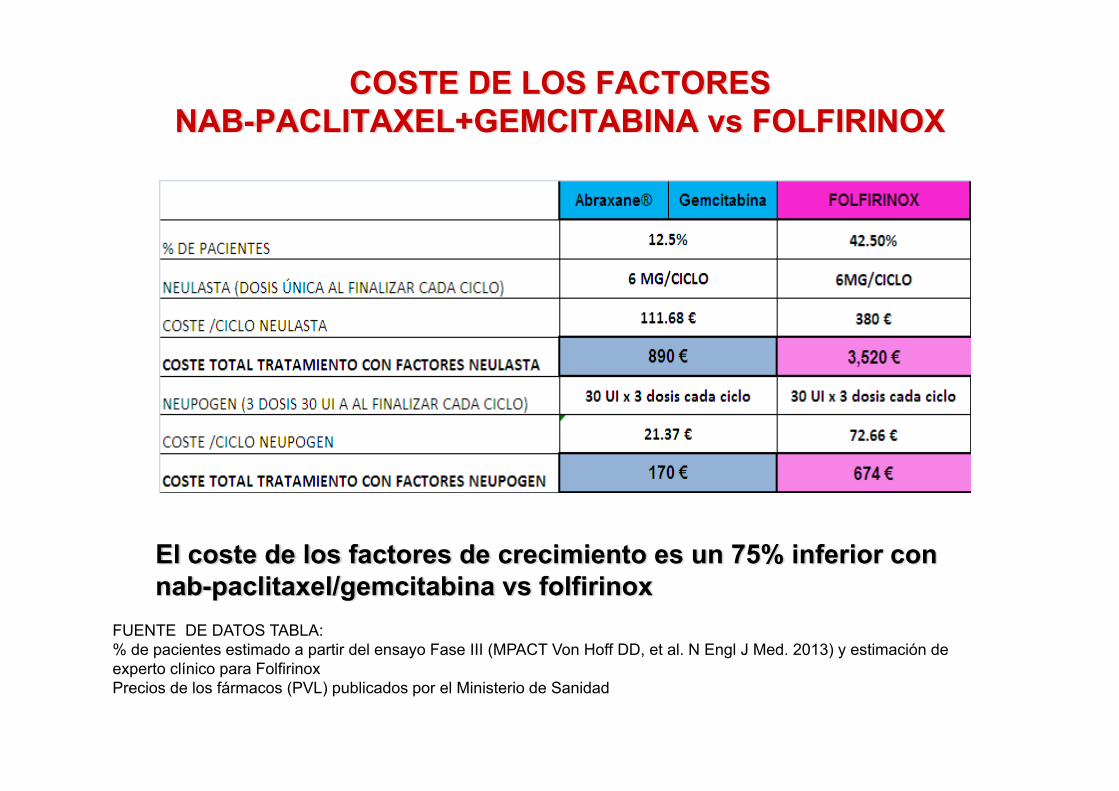
COSTE DE LOS FACTORES NAB-PACLITAXEL+GEMCITABINA vs FOLFIRINOX
El coste de los factores de crecimiento es un 75% inferior con nab-paclitaxel/gemcitabina vs folfirinox
FUENTE DE DATOS TABLA:% de pacientes estimado a partir del ensayo Fase III (MPACT Von Hoff DD, et al. N Engl J Med. 2013) y estimación de experto clínico para FolfirinoxPrecios de los fármacos (PVL) publicados por el Ministerio de Sanidad
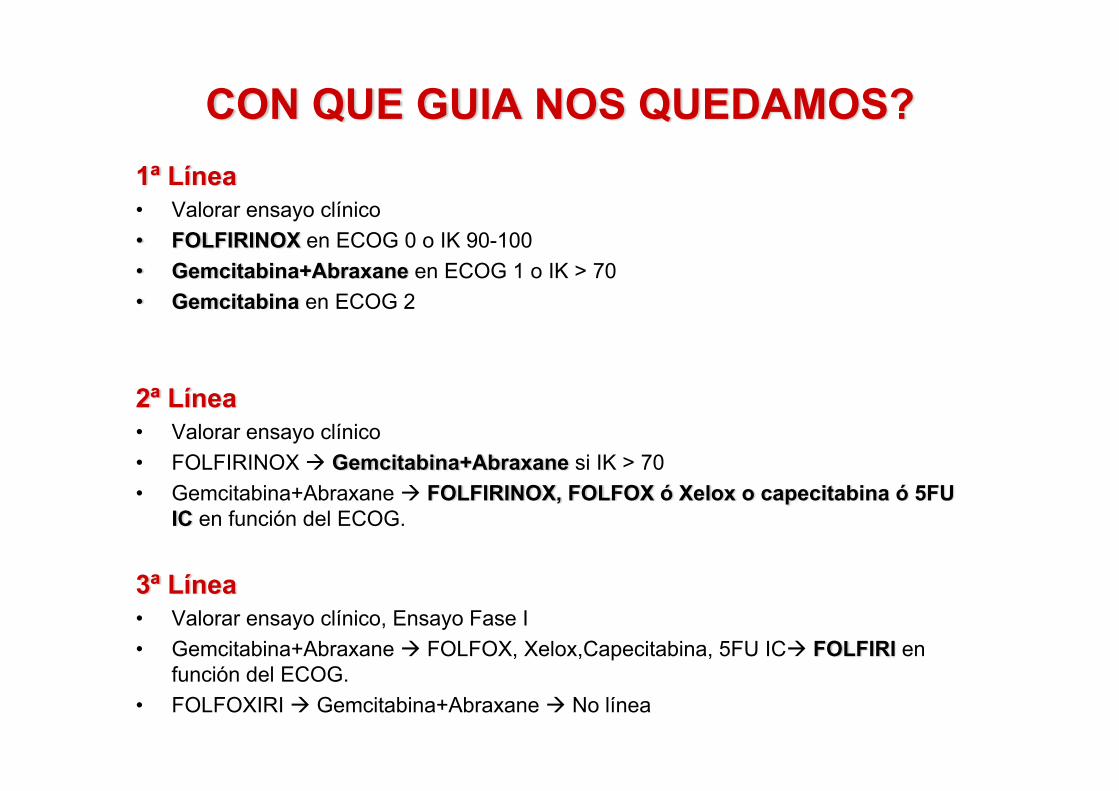
CON QUE GUIA NOS QUEDAMOS?1ª Línea• Valorar ensayo clínico• FOLFIRINOX en ECOG 0 o IK 90-100• Gemcitabina+Abraxane en ECOG 1 o IK > 70 • Gemcitabina en ECOG 2
2ª Línea• Valorar ensayo clínico• FOLFIRINOX Gemcitabina+Abraxane si IK > 70• Gemcitabina+Abraxane FOLFIRINOX, FOLFOX ó Xelox o capecitabina ó 5FU
IC en función del ECOG.
3ª Línea• Valorar ensayo clínico, Ensayo Fase I• Gemcitabina+Abraxane FOLFOX, Xelox,Capecitabina, 5FU IC FOLFIRI en
función del ECOG.• FOLFOXIRI Gemcitabina+Abraxane No línea
MOLTES GRÀCIES