Aterosclerosis y dishematopoiesis · Células mieloides en la evolución de la aterosclerosis ....
35
José A. Páramo Servicio Hematología y Hemoterapia Laboratorio Aterotrombosis. CIMA ATEROSCLEROSIS Y HEMATOPOYESIS CLONAL
Transcript of Aterosclerosis y dishematopoiesis · Células mieloides en la evolución de la aterosclerosis ....

José A. Páramo Servicio Hematología y Hemoterapia
Laboratorio Aterotrombosis. CIMA
ATEROSCLEROSIS Y
HEMATOPOYESIS CLONAL
Esquema
• Aterosclerosis como enfermedad inflamatoria
• Componente mieloide en la aterosclerosis
• ¿Qué es CHIP?
• Hematopoyesis clonal relacionada con la edad
• Hematopoyesis clonal relacionada con la aterosclerosis

3
ENFERMEDADES CARDIOVASCULARES
PRIMERA CAUSA DE MUERTE EN EL MUNDO OCCIDENTAL
Más de 20 millones de muertes en el mundo en 2030
PREDICCIÓN MORTALIDAD ECV


DEFINICIÓN
enfermedad sistémica crónica caracterizada por la formación de placas de ateroma que provocan estenosis y obstrucción de la luz de las arterias de mediano y gran calibre (concepto anatómico)
ATEROSCLEROSIS: Sustrato fisiopatológico de las enfermedades vasculares
isquémicas y sus complicaciones trombóticas

Inflamación crónica de la capa íntima de las arterias de mediano y gran calibre Inestabilidad inflamatoria puede generar la ruptura de la placa de ateroma (placa vulnerable) formación de un trombo y el infarto de la zona afecta (concepto funcional)
ATEROSCLEROSIS

Moore KJ et al. Cell 2011
Fisiopatología: Progresión aterosclerosis
Erosión Ruptura Placa estable


La aterosclerosis es una enfermedad inflamatoria
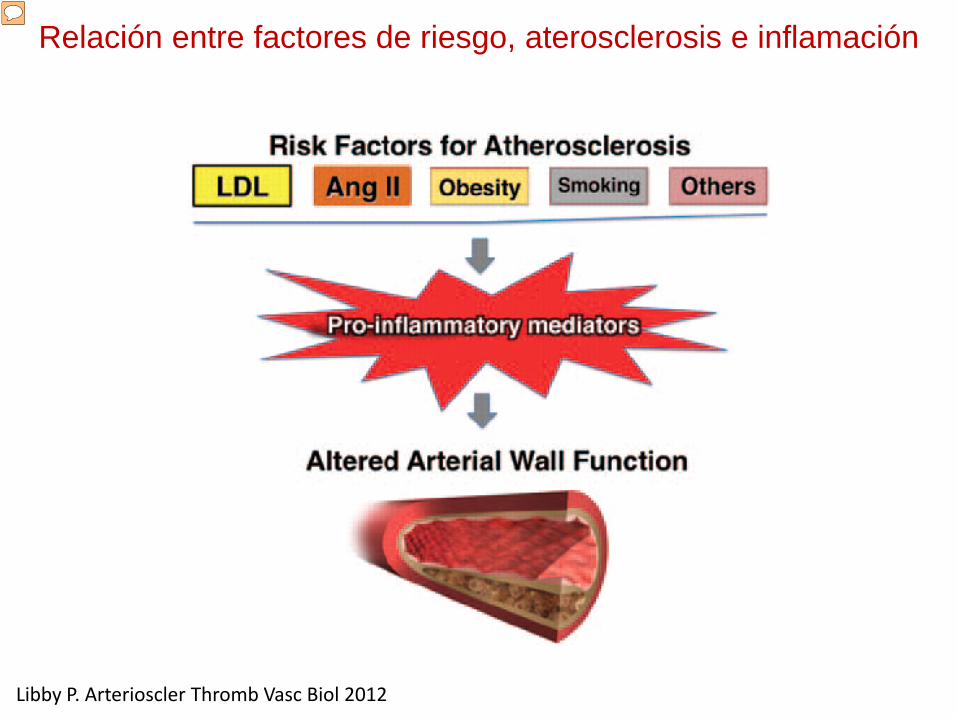
Relación entre factores de riesgo, aterosclerosis e inflamación
Libby P. Arterioscler Thromb Vasc Biol 2012
Moderador
Notas de la presentación
The relationship between traditional risk factors for atherosclerosis and inflammation. The concept of inflammation in atherosclerosis in no way diminishes the importance of the traditional risk factors for atherosclerosis depicted at the top of this diagram, including low-density lipoprotein (LDL) and angiotensin II (Ang II). Rather, the concept of inflammatory signaling and the participation of proinflammatory cytokines provides a mechanistic link between traditional risk factors and altered biological responses of the artery wall that drive atherosclerosis and its complications.

Células mieloides en la evolución de la aterosclerosis
Swirski FK. 2016

Libby P. Circ Res. 2014
Inflamación, ruptura y trombosis
Moderador
Notas de la presentación
Inflammation in plaque rupture and thrombosis. This diagram shows a cross-section of the intima of part of an artery affected by atherosclerosis. Altered hydrodynamics, illustrated in the top left, cause loss of atheroprotective functions of endothelial cells—including vasodilator, anti-inflammatory, profibrinolytic, and anticoagulant properties. Antigens presented on antigen-presenting cells such as dendritic cells (DCs) can activate TH1 lymphocytes to produce interferon-γ (IFN-γ), which activates macrophages (MΦ, yellow). Other subtypes of lymphocytes (shown in blue) include TH2 lymphocytes, which can elaborate the anti-inflammatory cytokine interleukin 10 (IL-10) and regulatory T cells that secrete the anti-inflammatory cytokine transforming growth factor-β (TFG-β). On its surface, the macrophage contains Toll-like receptors (TLRs) 2 and 4, which can bind pathogen-associated molecular patterns and damage-associated molecular patterns (see text). The intracellular TLRs 3, 7, and 9 may also contribute to lipid accumulation and other proatherogenic functions of the macrophage. Macrophages can undergo stress of the endoplasmic reticulum (ER) under atherogenic conditions. Cholesterol crystals found in plaques can activate the NOD-, LRR- and pyrin domain-containing 3 inflammasome (see text) that can generate mature IL-1β from its inactive precursor. The activated macrophage secretes collagenases that can degrade the triple helical interstitial collagen that lends strength to the plaque’s fibrous cap. Activated macrophages also express tissue factor, a potent procoagulant, and elaborate proinflammatory cytokines that amplify and sustain the inflammatory process in the plaque. When the plaque ruptures because of a collagen-poor, weakened fibrous cap, blood in the lumen can contact tissue factor in the lipid core, triggering thrombus formation (red). When the thrombus forms, polymorphonuclear leukocytes (PMNs) can accumulate and elaborate myeloperoxidase (MPO), which in turn elaborates the potent pro-oxidant hypochlorous acid. Dying PMNs extrude DNA that can form neutrophil extracellular traps (NETs), which can entrap leukocytes and propagate thrombosis. Other inflammatory cells modulate atherosclerosis. B1 lymphocytes secrete natural antibody that can inhibit plaque inflammation. On the contrary, B2 lymphocytes, in part via B-cell activating factor (BAFF), can promote inflammation and plaque complication. Mast cells can augment atherogenesis by releasing histamine and the cytokines IFN-γ and IL-6. The consequences of a given plaque rupture depend not only on the solid state of the intimal plaque but also on the fluid phase of blood, as depicted in the top right. Systemic inflammation can give rise to cytokines, culminating in the overproduction of IL-6, the trigger of the hepatic acute phase response. The acute phase reactant fibrinogen (not shown) participates directly in thrombus formation. Another acute phase reactant, plasminogen activator inhibitor-1 (PAI-1), can impair fibrinolysis by inhibiting the endogenous fibrinolytic mediators, urokinase- and tissue-type plasminogen activators (uPA and tPA). (Illustration credit: Ben Smith.)


Concepto de hematopoyesis clonal de potencial indeterminado (CHIP)
Steensma DP. Blood 2015
Expansión de clones hematopoyéticos portando mutaciones somáticas
Moderador
Notas de la presentación
CHIP as a precursor state for hematological neoplasms. (A) A model for evolution from normal hematopoiesis to CHIP and then, in some cases, to MDS or AML. (B) Comparison of evolution patterns of MGUS, MBL, and CHIP. Hematopoietic progenitor or stem cells commonly acquire mutations throughout the human lifespan; most of these are passenger mutations that have no consequence for hematopoiesis. Certain mutations, however, confer a survival advantage to the mutated cell and its progeny and allow clonal expansion. Serial acquisition of mutations in an expanded clone can lead to a disease phenotype and ultimately morbidity and mortality. Although this article primarily discusses CHIP in the context of its distinction from MDS, CHIP can also directly progress to AML without an intervening MDS stage, and CHIP can progress to other conditions such as myeloproliferative neoplasms or lymphoid neoplasms. Just as with MGUS and MBL, the majority of patients with CHIP will never develop an overt neoplasm, and patients will eventually die of unrelated causes.

Clonal hematopoiesis of indetermined potential (CHIP)
Presencia de mutaciones somáticas en cel. Stem hematopoyéticas
Ventaja selectiva
Expansión celular, sin otras anomalías hematológicas (común con edad avanzada)
Granulocitos Linfocitos Monocitos
Mayor riesgo (x2) de ECV: EAC y calcificación Mayor riesgo (x10) neoplasias hematológicas
DNMT3A TET2
ASXl1 JAK-2

Primeras descripciones hematopoyesis clonal
NEJM 2014
NEJM 2014
Nature Med 2014

Hematopoyesis clonal relacionada con la edad
• N=17.182 sujetos • Secuenciación exoma en busca de mutaciones somáticas
- <40 años= Raras - 70-79 años= 9,5% - 80-89 años =11,7% -90-108 años=18,4%
Jaiswall S. NEJM 2014
Mutaciones en 3 genes: DNMT3A TET2 ASXL1
Riesgo de neoplasias hematológicas, HR 11,1 Mortalidad, HR1,4 EAC, HR 2 Ictus, HR 2,6

NEJM 2014

EDAD
Predictor independiente de enfermedad cardiovascular
Factores de riesgo cardiovascular Obesidad Diabetes HiperTA Hipercolesterolemia
CHIP ( 10% de sujetos > 70 años Steensma DP, Blood 2015)
Mayor incidencia de neoplasias hematológicas

¿Es CHIP un factor etiológico en el desarrollo de la enfermedad vascular aterosclerótica?

¿Es CHIP un factor etiológico en el desarrollo de la enfermedad vascular aterosclerótica?
Jaiswall S. NEJM 2017
• Estudio clínico
• N=4726 pacientes con EAC
Prospectivo: BIOIMAGE (EEUU)- MDC (Suecia)
Caso-control: ATVB (Suecia)-PROMIS (Pakistan)
• N= 3529 controles sanos
Mutaciones en ASXL1, DNMT3A, JAK-2 y TET2
Asociadas de manera individual con la EAC

N Engl J Med 2017

Asociación entre mutaciones y eventos coronarios
Jaiswall S. NEJM 2017
Asociación entre mutaciones y calcificación coronaria
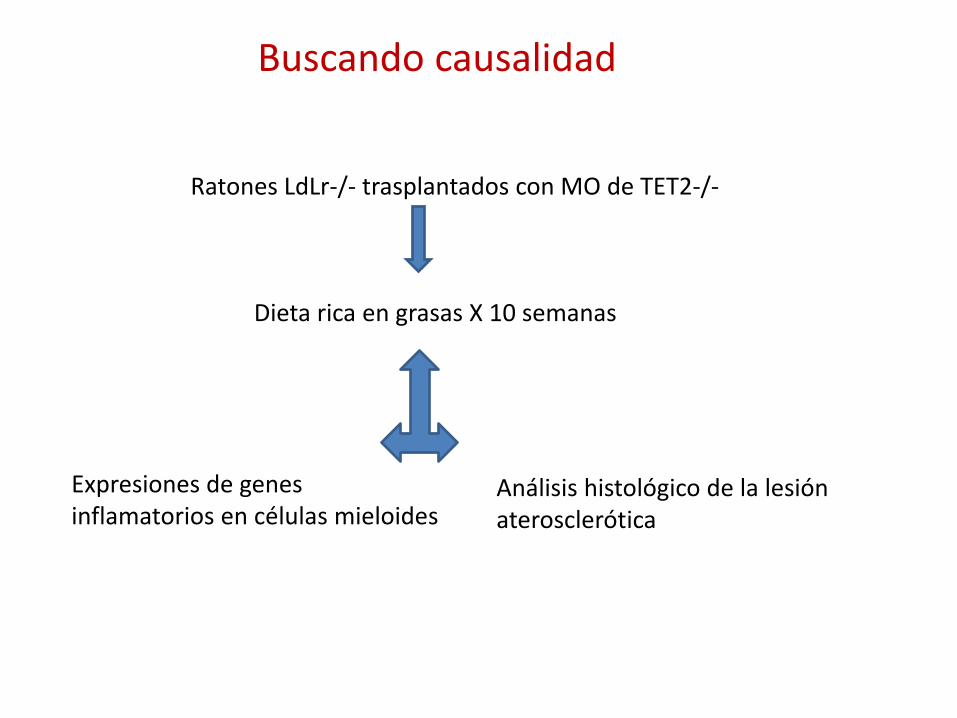
Buscando causalidad
Ratones LdLr-/- trasplantados con MO de TET2-/-
Dieta rica en grasas X 10 semanas
Expresiones de genes inflamatorios en células mieloides
Análisis histológico de la lesión aterosclerótica

Jaiswal S. N Engl J Med 2017
Loss of Tet2 in Hematopoietic Cells and Atherosclerosis in a Murine Model.
Alteraciones en Tet2 en células hemopoyéticas y aterosclerosis en un modelo murino
Moderador
Notas de la presentación
Figure 4. Loss of Tet2 in Hematopoietic Cells and Atherosclerosis in a Murine Model. Shown are the effects of the transplantation of bone marrow into female, atherosclerosis-prone Ldlr knockout mice, according to whether the donor mice had wild-type (WT) Tet2, heterozygous (HET) Tet2, or knockout (KO) Tet2. Deletions in Tet2 were obtained by using Cre recombinase expressed from the Vav1 promoter. Panel A shows aortic-root sections obtained from mice that had received transplants from WT or KO Tet2 mice after the mice had received a high-cholesterol diet for 5 weeks and 9 weeks (oil red O staining at 5 weeks and Masson’s trichrome staining at 9 weeks). The dashed lines indicate the lesion areas. Panel B shows the quantification of aortic-root lesions in mice that had received transplants from WT or KO Tet2 mice at 5 weeks and 9 weeks. P values were obtained with the use of the Wilcoxon rank-sum test. Panel C shows lesions in the descending aorta that were stained with oil red O at 17 weeks in mice that had received transplants from WT, HET, or KO Tet2 mice. The amount of red dye that is visible indicates the degree of atherosclerosis, according to Tet2 status. Panel D shows the quantification of lesions in the descending aorta at 17 weeks, according to Tet2 status. P values were obtained with the use of Dunn’s Kruskal–Wallis test for multiple comparisons and the Benjamini–Hochberg correction. In Panels B and D, the black horizontal lines represent the median values.

Science 2017

Ruparelia N. Nat Rev Cardiol 2016
IL-1β, Inflamasoma y aterosclerosis

Conclusiones
• Existe una relación de causalidad entre CHIP y EAC Experimental Clínica: Aumento de eventos en relación con tamaño clon
• Mutaciones en múltiples genes asociados con CHIP incrementan el riesgo de eventos coronarios Mayor respuesta inflamatoria mediada por macrófagos Mayor reclutamiento de monocitos al subendotelio Activación inflamasoma
• ¿Se puede modificar la hematopoyesis clonal? Hipolipemiantes Antiinflamatorios Vitamina C

Dieta Control de stress Ejercicio físico
Reducción Riesgo cardiovascular
Efecto beneficioso sobre hematopoyesis

Cimmino L. Cell 2017

Vitamina C y aterosclerosis



CHIP
Edad avanzada
Neoplasia hematológicas Enfermedad cardiovascular
¿El nexo entre cáncer y ECV? ¿Nueva diana terapéutica en aterosclerosis?