1 Proceso Mujer en la sexta década de la vida. Mujer en la sexta década de la vida. Antecedentes...
83
1 Proceso Proceso Mujer en la sexta década de la vida. Mujer en la sexta década de la vida. Antecedentes médicos conocidos de Antecedentes médicos conocidos de Hipertensión Arterial sisto-diastólica de Hipertensión Arterial sisto-diastólica de clase clase I I (NYHA). Hiperlipemia. Alteraciones (NYHA). Hiperlipemia. Alteraciones tiroideas. (Todas ellas en tratamiento). tiroideas. (Todas ellas en tratamiento). Comienza brusca , inesperadamente y sin Comienza brusca , inesperadamente y sin antecedentes previos, con un cuadro antecedentes previos, con un cuadro sintomatológico sintomatológico nocturno caracterizado por: caracterizado por: - Sensación de falta de aire (disnea) Sensación de falta de aire (disnea) - Palpitaciones. Palpitaciones. - Malestar general. Malestar general.
-
Upload
roldan-zaragosa -
Category
Documents
-
view
221 -
download
0
Transcript of 1 Proceso Mujer en la sexta década de la vida. Mujer en la sexta década de la vida. Antecedentes...
11
Proceso Proceso Mujer en la sexta década de la vida.Mujer en la sexta década de la vida. Antecedentes médicos conocidos de Hipertensión Antecedentes médicos conocidos de Hipertensión
Arterial sisto-diastólica de Arterial sisto-diastólica de claseclase I I (NYHA). (NYHA). Hiperlipemia. Alteraciones tiroideas. (Todas ellas Hiperlipemia. Alteraciones tiroideas. (Todas ellas en tratamiento).en tratamiento).
Comienza brusca , inesperadamente y sin Comienza brusca , inesperadamente y sin antecedentes previos, con un cuadro antecedentes previos, con un cuadro sintomatológico sintomatológico nocturno caracterizado por: caracterizado por:
- Sensación de falta de aire (disnea)Sensación de falta de aire (disnea)- Palpitaciones.Palpitaciones.- Malestar general.Malestar general.
22
Es atendida en su Hospital de Es atendida en su Hospital de Referencia,donde es diagnosticada de un Referencia,donde es diagnosticada de un cuadro de cuadro de Fibrilación AuricularFibrilación Auricular no no compensadacompensada (frecuencia ventricular (frecuencia ventricular rápida): rápida):
Frecuencia cardiaca máxima de 160 bpm.Frecuencia cardiaca máxima de 160 bpm. Consciente y orientada temporo-Consciente y orientada temporo-
espacialmente.espacialmente. Agitación Psico-motriz.Agitación Psico-motriz. Sin cortejo neuro-vegetativo manifiesto.Sin cortejo neuro-vegetativo manifiesto. Constantes vitalesConstantes vitales aceptables, sin aceptables, sin
compromiso hemodinámico.compromiso hemodinámico.
33
Inician una cardioversión farmacológica:Inician una cardioversión farmacológica:
AMIODARONAAMIODARONA vía i.v. (AA clase III) que, según vía i.v. (AA clase III) que, según me refiere la paciente, no tolera, empeorando el me refiere la paciente, no tolera, empeorando el cuadro subjetivo.cuadro subjetivo.
Se clasifica la reacción como un cuadro de Se clasifica la reacción como un cuadro de “hipersensibilidad al fármaco y/o sus “hipersensibilidad al fármaco y/o sus componentes (Yodo)”.componentes (Yodo)”.
Administran Administran PROPAFENONA PROPAFENONA (AA clase IC) a (AA clase IC) a dosis de 600 mgrs/ 4 horas por dosis de 600 mgrs/ 4 horas por vía oralvía oral..
(La paciente no indica el tiempo transcurrido desde (La paciente no indica el tiempo transcurrido desde la ingesta del fármaco hasta la recuperación la ingesta del fármaco hasta la recuperación sinusal y de síntomas)sinusal y de síntomas)
44
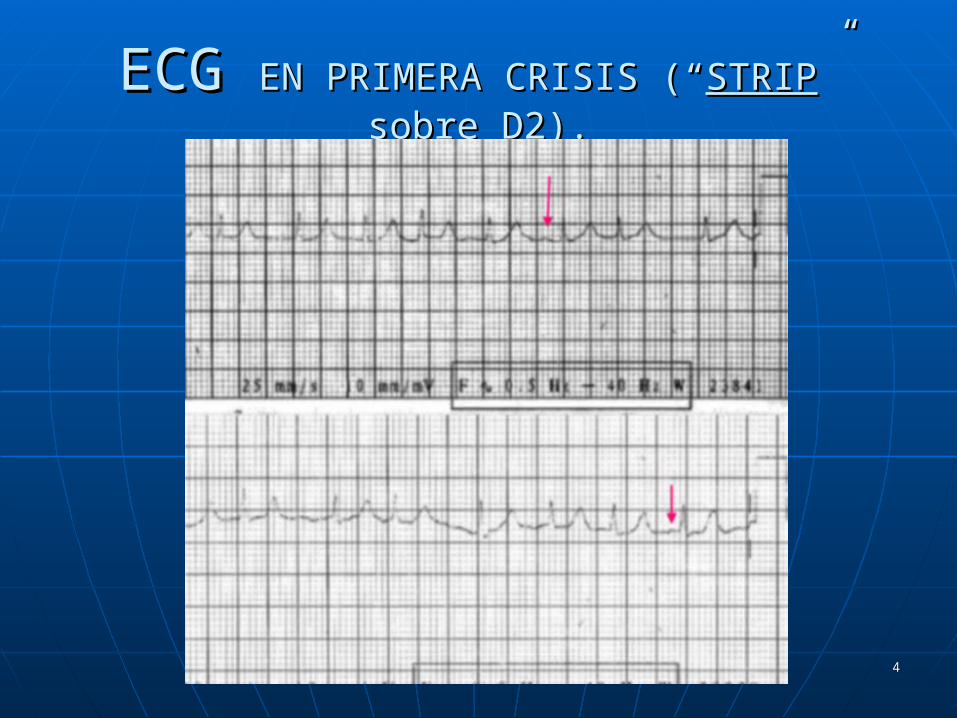
ECG ECG EN PRIMERA CRISIS (“EN PRIMERA CRISIS (“STRIPSTRIP” sobre ” sobre D2).D2).
55
Características básicas del “strip”Características básicas del “strip” Ritmo rápido con frecuencia cardiaca entre Ritmo rápido con frecuencia cardiaca entre 9595 y y
150 bpm150 bpm (esta última en “salvas de 2-3). (esta última en “salvas de 2-3).
Ondas P visibles Ondas P visibles aisladamenteaisladamente (flechas rojas). (flechas rojas).
Línea de base isoeléctrica y sin espículas.Línea de base isoeléctrica y sin espículas.
Complejos QRS de duración y amplitud normales.Complejos QRS de duración y amplitud normales.
(Taquicardia suprahisiana con frecuencia (Taquicardia suprahisiana con frecuencia moderadamente alta (máximo 150 bpm)moderadamente alta (máximo 150 bpm)
66
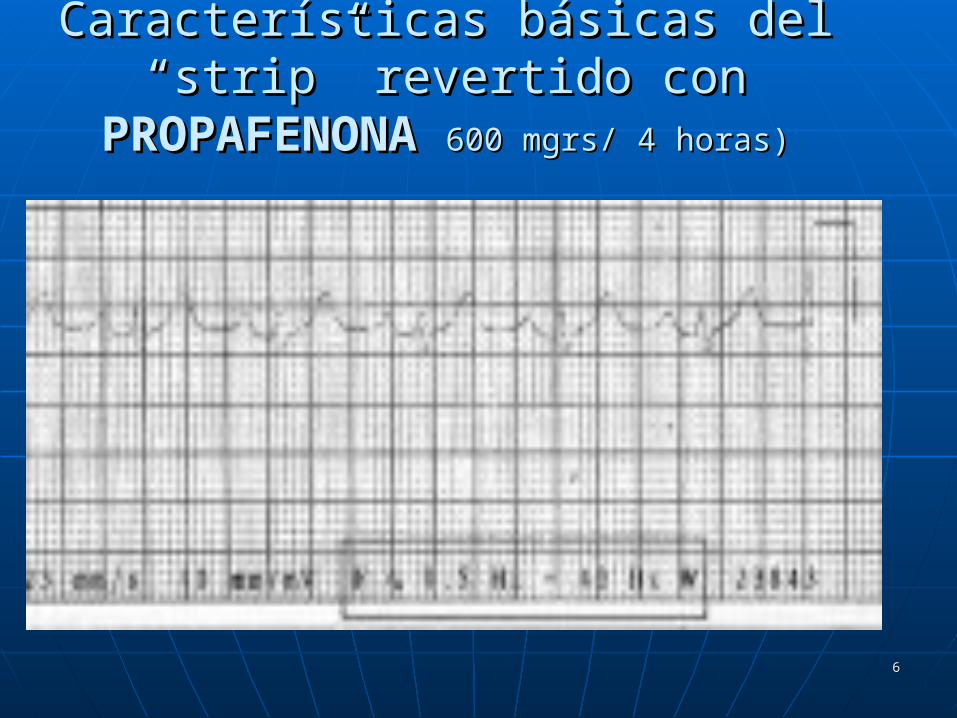
Características básicas del “strip” Características básicas del “strip” revertido con revertido con PROPAFENONAPROPAFENONA 600 mgrs/ 4 600 mgrs/ 4
horas)horas)
77
Medidas Medidas
Ritmo Sinusal a 87-88 bpm.Ritmo Sinusal a 87-88 bpm. Ondas P: 130 mseg.Ondas P: 130 mseg. Intervalo PR: Entre Intervalo PR: Entre 213-221 mseg213-221 mseg.. Intervalo QT: Entre 373-400 msegIntervalo QT: Entre 373-400 mseg Intervalo RR: 689 mseg.Intervalo RR: 689 mseg. Intervalo QT corregido (Bazett): Entre Intervalo QT corregido (Bazett): Entre
449- 481 mseg.449- 481 mseg.
88
Interpretación de StripInterpretación de Strip
Recuperación de ritmo sinusal.Recuperación de ritmo sinusal. Recuperación de frecuencia cardiaca Recuperación de frecuencia cardiaca
(87-88 bpm).(87-88 bpm). Intervalo PR Intervalo PR mayormayor de 200 mseg. de 200 mseg. Intervalo QTcB Intervalo QTcB mayormayor de 440 mseg. de 440 mseg.
BloqueoBloqueo AV de primer grado junto a AV de primer grado junto a una una ProlongaciónProlongación del intervalo QTcB. del intervalo QTcB.

99
REFLEXIONES SOBRE EL EVENTOREFLEXIONES SOBRE EL EVENTO
Taquicardia supraventricular Taquicardia supraventricular moderada de complejo QRS moderada de complejo QRS estrecho, sin repercusión estrecho, sin repercusión hemodinámica grave.hemodinámica grave.
1010
PosiblePosible : :
““fibrilación–flutter” auricularfibrilación–flutter” auricular
levemente descompensado levemente descompensado (máx. (máx. 150150 bpm en salvas; con bpm en salvas; con media y moda estadística de media y moda estadística de 95-105 bpm).95-105 bpm).
1111
Mala respuesta a perfusión de Mala respuesta a perfusión de Amiodarona Amiodarona (Hipersensibilidad???).(Hipersensibilidad???).
1212
Aceptable respuesta a la Aceptable respuesta a la cardioversión farmacológica con cardioversión farmacológica con Propafenona.Propafenona.
1313
Persistencia de intervalo PR y QTcB Persistencia de intervalo PR y QTcB ProlongadosProlongados
1414
No consta ningún intento de No consta ningún intento de cardioversión farmacológica con:cardioversión farmacológica con:
AdenosinaAdenosina en bolos i.v, de 6 mgrs (indicada en toda en bolos i.v, de 6 mgrs (indicada en toda TSV de complejo estrecho).TSV de complejo estrecho).
VernakalantVernakalant ** en perfusión i.v. en perfusión i.v.
1515
*VERNAKALANT:*VERNAKALANT: • Difiere en su farmacología de otros antiarrítmicos ya que Difiere en su farmacología de otros antiarrítmicos ya que
bloquea el potencial de acción de los canales de sodio y bloquea el potencial de acción de los canales de sodio y potasio. potasio.
• Parece tener una acción directa sobre los canales de potasio Parece tener una acción directa sobre los canales de potasio auriculares con el resultado de un alargamiento del potencial auriculares con el resultado de un alargamiento del potencial de acción auricular y una prolongación de la meseta de acción auricular y una prolongación de la meseta sin sin afectar significativamente al intervalo QTafectar significativamente al intervalo QT ó al periodo ó al periodo refractario ventricular. refractario ventricular.
• Como resultado de este mecanismo de acción, los efectos Como resultado de este mecanismo de acción, los efectos proarritmicos observados con otros agentes aprobados para el proarritmicos observados con otros agentes aprobados para el tratamiento de la F.A desaparecen. tratamiento de la F.A desaparecen.
• Para pacientes con F.A permanente durante 3-72 h, en tiempo Para pacientes con F.A permanente durante 3-72 h, en tiempo de conversión se encontró entre 8-14 minutos, de los cuales el de conversión se encontró entre 8-14 minutos, de los cuales el 79% permanecieron en ritmo sinusal a las 24 h.79% permanecieron en ritmo sinusal a las 24 h.
Los autores concluyen que la administración de vernakalant, nuevo antiarrítmico auricular Los autores concluyen que la administración de vernakalant, nuevo antiarrítmico auricular relativamente selectivo, parece ofrecer efectividad y un enfoque seguro par la conversión relativamente selectivo, parece ofrecer efectividad y un enfoque seguro par la conversión rápida de la FA a ritmo sinusalrápida de la FA a ritmo sinusal. .
Am J Health-Syst Pharm. 2010;67:1157-64Am J Health-Syst Pharm. 2010;67:1157-64
1616
Actualmente, este tipo de Actualmente, este tipo de fármacos están fármacos están considerados ,de una manera considerados ,de una manera consensuada ,como de consensuada ,como de “primera línea”“primera línea” para el control para el control de frecuencia-ritmo ante toda de frecuencia-ritmo ante toda Taquicardia Supraventricular Taquicardia Supraventricular mayor de 150 bpm, y cuyo mayor de 150 bpm, y cuyo proceso de base es todavía proceso de base es todavía desconocidodesconocido..
1717
Proceso de ALTA HospitalariaProceso de ALTA Hospitalaria
Después de la recuperación clínica y Después de la recuperación clínica y electrocardiográfica, es dada de Alta electrocardiográfica, es dada de Alta Hospitalaria con:Hospitalaria con:
- ARA IIIARA III, tipo , tipo ValsartanValsartan..
- Beta-bloqueadores Beta-bloqueadores (AA tipo II),(AA tipo II), tipo tipo AtenololAtenolol..
1818
PatocróniaPatocrónia Tras esta primera crisis de palpitaciones-Tras esta primera crisis de palpitaciones-
disnea- taquicardia suprahisiana, la disnea- taquicardia suprahisiana, la paciente refiere paciente refiere 5 episodios más5 episodios más : :
Parecidas características.Parecidas características.
Frecuencia Cardiaca media fue de Frecuencia Cardiaca media fue de 95- 100 95- 100 bpmbpm./ crisis../ crisis.
Es tratada con diferentes fármacos y combinación de Es tratada con diferentes fármacos y combinación de ellos.ellos.

1919
2ª Crisis2ª Crisis: : Cardioversión farmacológica con Cardioversión farmacológica con
PROPAFENONA 600 mgrs/ 4 horas. Vía PROPAFENONA 600 mgrs/ 4 horas. Vía oral.oral.
Alta Hospitalaria con Metoprolol 25 Alta Hospitalaria con Metoprolol 25
mgrs /8 horas.mgrs /8 horas.
2020
3ª Crisis:3ª Crisis: Misma técnica de Cardioversión. Misma técnica de Cardioversión.
Alta Hospitalaria con Metropolol 25 mgrs Alta Hospitalaria con Metropolol 25 mgrs /8 horas + Propafenona 300 mgrs / 12 /8 horas + Propafenona 300 mgrs / 12 horas.horas.

2121
Resto de crisis hasta la 5ª:Resto de crisis hasta la 5ª:
Misma técnica de cardioversión Misma técnica de cardioversión farmacológica intrahospitalaria. farmacológica intrahospitalaria.
Alta Hospitalaria con Propafenona 300 Alta Hospitalaria con Propafenona 300 mgrs/ 12 horas junto a diferentes Beta-mgrs/ 12 horas junto a diferentes Beta-bloqueadores. bloqueadores.
(Mezcla de AA: Grupo IC+ Grupo II)(Mezcla de AA: Grupo IC+ Grupo II)

2222
Propuesta de RADIOABLACIÓNPropuesta de RADIOABLACIÓN
A partir de la A partir de la 5ª crisis5ª crisis, , es considerada es considerada como accesos de como accesos de FIBRILACIÓN FIBRILACIÓN AURICULAR PAROXÍSTICA AURICULAR PAROXÍSTICA RECURRENTERECURRENTE y se propone: y se propone:
ABLACIÓN ABLACIÓN de focos arritmógenosde focos arritmógenos por por Radiofrecuencia sobre Venas Radiofrecuencia sobre Venas Pulmonares.Pulmonares.
La paciente La paciente aceptaacepta dicha intervención, la cual, es dicha intervención, la cual, es realizadarealizada..

2323
ECG previo a Radio-ablaciónECG previo a Radio-ablación
..
2424
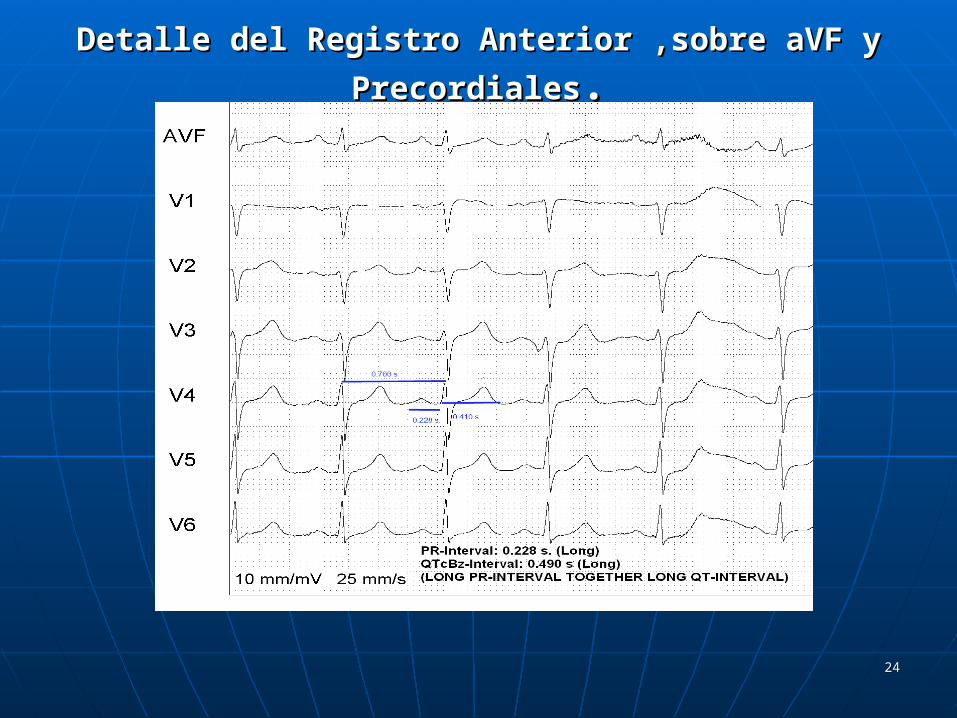
Detalle del Registro Anterior ,sobre aVF y PrecordialesDetalle del Registro Anterior ,sobre aVF y Precordiales..
2525
INTERPRETACIÓN BÁSICA DEL REGISTRO.INTERPRETACIÓN BÁSICA DEL REGISTRO.
Ritmo sinusal a 85 bpm aprox. Ondas P presentes positivas en general,
regulares, suficientes y seguidas de complejos QRS de amplitud y voltaje en valores normales. Onda P bifásica en V1 (signo de HAD)
Persistencia de “Onda S” en precordiales izquierdas
(unidas a presencia de onda S en D2-D3): Signos de HVD.- RV2+SV5 > 1.05 mV).
Eje eléctrico normal- verticalizado. Aceptable progresión de ondas R en
precordiales. Puntos J y ondas T preferentemente positivos. Segmentos ST fundamentalmente
isoeléctricos..
2626
Medidas de Intervalos Medidas de Intervalos
Intervalo PR medio: Intervalo PR medio: 0.228 segundos0.228 segundos.. Intervalo RR medio: 0.700 segundos. (85 Intervalo RR medio: 0.700 segundos. (85
bpm)bpm) Intervalo QT: 0.410 segundos.Intervalo QT: 0.410 segundos. Intervalo QT corregido (Bazett): Intervalo QT corregido (Bazett): 0.490 0.490
segundos.segundos.
PROLONGACIÓN de intervalos PR Y QTc.PROLONGACIÓN de intervalos PR Y QTc.
2727
Informe Post-ablaciónInforme Post-ablaciónO procedimento foi realizado no dia 27/07/10 com a
paciente sob anestesia geral. Por meio de punção da veia femoral direita, foram introduzidos três cateteres eletrodos multipolares e posicionados sob visão fluoroscópica no seio coronário e no átrio esquerdo (AE) através de dupla punção transeptal. O ritmo de base era sinusal.
Na transição do AE com as veias pulmonares foram realizadas aplicações de RF guiadas por mapeamento eletroanatômico (CARTO) e eletrofisiológico, utilizando cateter irrigado com ponta de 3,5mm que resultaram na desconexão elétrica das quatro veias pulmonares. Observou-se indução de FA com manipulação de cateteres revertida após cardioversão elétrica. A seguir foi realizada linha de bloqueio no Istmo Cavotricuspídeo.
O procedimento foi bem tolerado e não houve complicações
2828
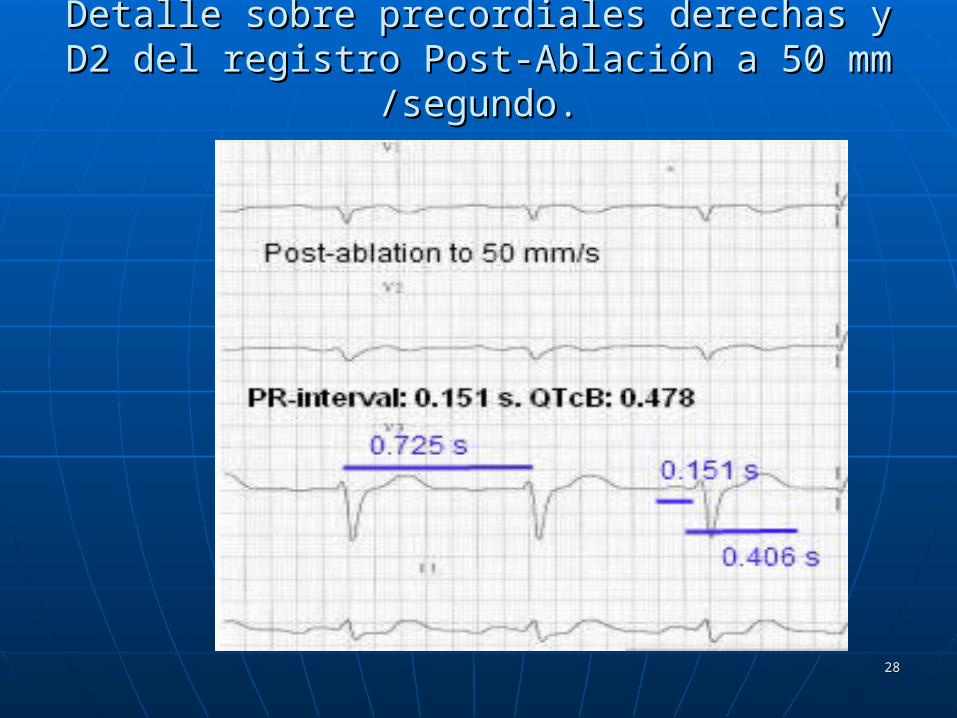
Detalle sobre precordiales derechas y D2 del Detalle sobre precordiales derechas y D2 del registro Post-Ablación a 50 mm /segundo.registro Post-Ablación a 50 mm /segundo.
2929
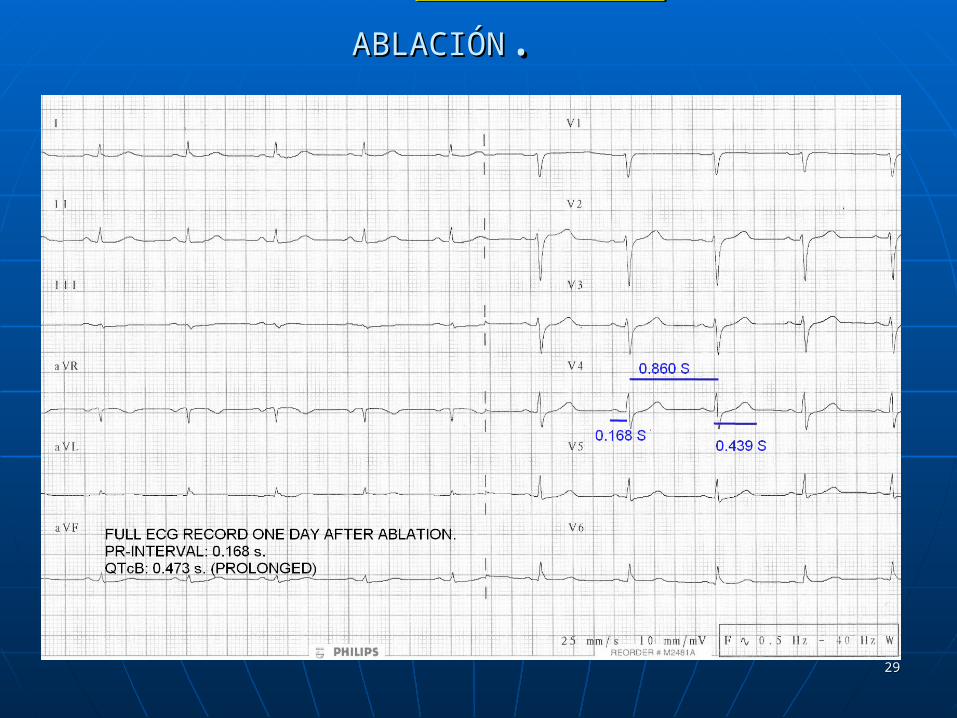
ECG COMPLETO AL ECG COMPLETO AL DIA SIGUIENTEDIA SIGUIENTE DE LA DE LA
ABLACIÓNABLACIÓN..
3030
Valoración del ECG Post. (50 mm/s)Valoración del ECG Post. (50 mm/s)• Ritmo Ritmo sinusalsinusal. . • Frecuencia cardiaca Frecuencia cardiaca 7070 bpm. bpm.• Ondas P aplanadasOndas P aplanadas..• Medidas de Intervalos.Medidas de Intervalos. Intervalo PR Intervalo PR menor menor de 200 milisegundos.de 200 milisegundos. Intervalo QT: 406 segundos.Intervalo QT: 406 segundos. Intervalo RR: 725 segundos. (82-83 bpm)Intervalo RR: 725 segundos. (82-83 bpm) Intervalo QTcB: Intervalo QTcB: 0.473-0.476 segundos0.473-0.476 segundos
((ProlongadoProlongado) )
3131
Puede observarse una Puede observarse una mejoría- control en:en:
Ritmo.- Permanece en sinusal.Ritmo.- Permanece en sinusal. Frecuencia Cardiaca.- Estable en 70-75 Frecuencia Cardiaca.- Estable en 70-75
bpm. bpm. Longitud del intervalo PR, desapareciendo Longitud del intervalo PR, desapareciendo
el Bloqueo AV.el Bloqueo AV.
Sin embargo, el intervalo QTcB persiste Sin embargo, el intervalo QTcB persiste siendo siendo prolongadoprolongado (> 440 mseg(> 440 mseg))
3232
MANEJO DE LA PACIETE POST-MANEJO DE LA PACIETE POST-ABLACIÓNABLACIÓN
Propafenona 300 mgrs.(AA tipo IC) Propafenona 300 mgrs.(AA tipo IC)
Bisoprolol 5 mgrs. (Beta-bloqueante. Bisoprolol 5 mgrs. (Beta-bloqueante. AA tipo II).AA tipo II).
3333
Evolución clínica Post-AblaciónEvolución clínica Post-AblaciónDespués de Ablación por Radio-Después de Ablación por Radio-
frecuencia de focos pulmonares frecuencia de focos pulmonares arritmogénicos, la paciente refiere:arritmogénicos, la paciente refiere:
Dos nuevos cuadros similares a la Dos nuevos cuadros similares a la primera crisis.primera crisis.
Predominio de sensación de disnea y Predominio de sensación de disnea y palpitaciones.palpitaciones.
Necesidad de Necesidad de CARDIOVERSIÓN CARDIOVERSIÓN ELÉCTRICAELÉCTRICA en ambas recaídas en ambas recaídas (no se (no se indica la energía utilizada para reversión).indica la energía utilizada para reversión).
3434
Interacciones entre ambos Interacciones entre ambos
FármacosFármacos.. Propafenona posee propiedades Propafenona posee propiedades antiarrítmicas y betabloqueantes antiarrítmicas y betabloqueantes moderadas. moderadas. La asociación puede entrañar problemas de La asociación puede entrañar problemas de la contractilidad, del automatismo y de la la contractilidad, del automatismo y de la conducción, con supresión de los conducción, con supresión de los mecanismos simpáticos compensadores.mecanismos simpáticos compensadores. PropafenonaPropafenona tiene una capacidad tiene una capacidad intrínseca para producir una prolongación intrínseca para producir una prolongación del intervalo QT. del intervalo QT.

3535
Medicación de ALTA Hospitalaria Medicación de ALTA Hospitalaria post recaída post recaída
Después de la primera crisis post-ablación Después de la primera crisis post-ablación y cardioversión eléctrica:y cardioversión eléctrica:
• Propafenona 300 mgrs.Propafenona 300 mgrs.• Verapamilo Verapamilo ¿120 mgrs?¿120 mgrs?• Atenolol 25 mgrs.Atenolol 25 mgrs.Después de la segunda crisis post-ablación Después de la segunda crisis post-ablación
y cardioversión eléctrica:y cardioversión eléctrica:• Dronedarona 800 mgrs./día.Dronedarona 800 mgrs./día.• Ivabradina 2.5 mgrs./día.Ivabradina 2.5 mgrs./día.
3636
EVOLUCIÓN CLÍNICO-EVOLUCIÓN CLÍNICO-ECG.ECG.
Periodos comprendidos desde Periodos comprendidos desde antes de ningún tipo de antes de ningún tipo de
manifestación cardiológica manifestación cardiológica hasta la fecha.hasta la fecha.
3737
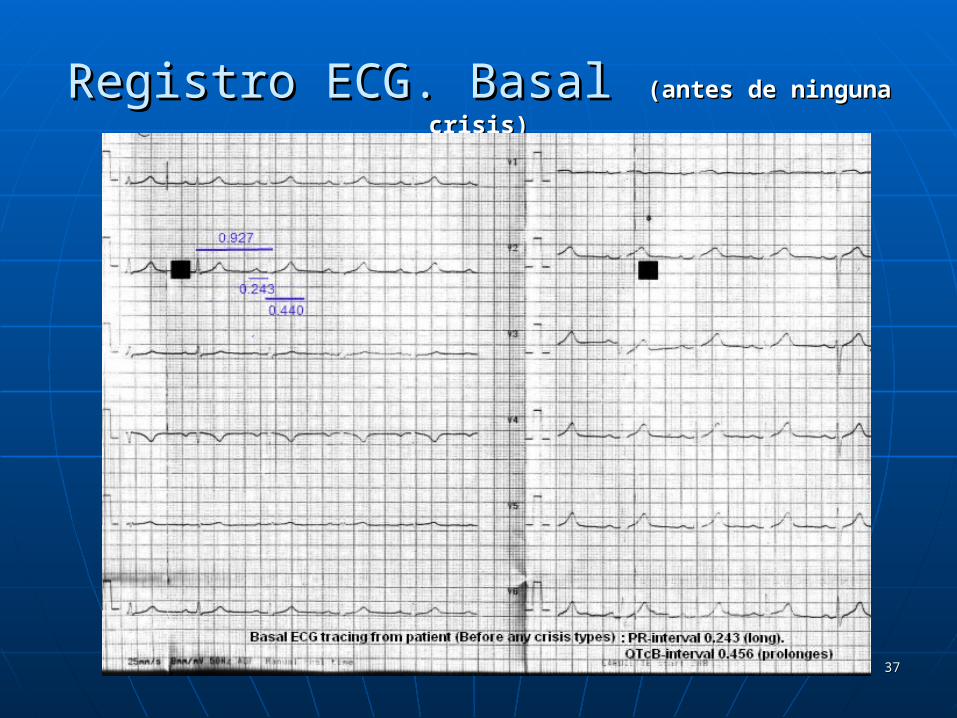
Registro ECG. BasalRegistro ECG. Basal (antes de ninguna crisis)(antes de ninguna crisis)

3838
Interpretación básica ECG Interpretación básica ECG basalbasal
Estimulación constante y regular. Estimulación constante y regular. Ritmo sinusal a 65 bpm aprox.Ritmo sinusal a 65 bpm aprox. Ondas P constantes, regulares, positivas, suficientes, Ondas P constantes, regulares, positivas, suficientes,
seguidas de complejos QRS. seguidas de complejos QRS. Intervalo PR de Intervalo PR de 0.243 seg0.243 seg.. como media (Bloqueo AV 1º como media (Bloqueo AV 1º
grado).grado). Eje eléctrico normal-verticalizado con presencia de patrón Eje eléctrico normal-verticalizado con presencia de patrón
S2S3S2S3. (Sobrecarga discreta derecha). (Sobrecarga discreta derecha) Complejos QRS normales en longitud y voltaje.Complejos QRS normales en longitud y voltaje. Progresión aceptable en ondas R en precordiales.Progresión aceptable en ondas R en precordiales. Persistencia de onda S en precordiales izquierdas.Persistencia de onda S en precordiales izquierdas. RV2+ SV5 > 1.05 mV, (Sokolov-Lyon): HVD.RV2+ SV5 > 1.05 mV, (Sokolov-Lyon): HVD. Ausencia de ondas Q patológicas. Segmentos ST y Puntos J Ausencia de ondas Q patológicas. Segmentos ST y Puntos J
isoeléctricos. Ondas T fundamentalmente positivas.isoeléctricos. Ondas T fundamentalmente positivas. Intervalo QTc Bazett de Intervalo QTc Bazett de 0.456 segundos0.456 segundos ( (ProlongadoProlongado))
3939
Juicio diagnóstico de ECG Juicio diagnóstico de ECG basalbasal
Signos discretos de Signos discretos de sobrecargasobrecarga en en cavidades derechas.cavidades derechas.
Signos de Signos de bloqueo AV de primer gradobloqueo AV de primer grado: : Intervalo PR > 0.200 seg. (0.243 seg.)Intervalo PR > 0.200 seg. (0.243 seg.)
ProlongaciónProlongación del intervalo QT con del intervalo QT con método Bazett: > 0.440 seg. (0.456 método Bazett: > 0.440 seg. (0.456 seg.)seg.)
4040
Algunas reflexiones sobre ECG BasalAlgunas reflexiones sobre ECG Basal She was diagnosed with "recurrent paroxysmal tachycardia crisis" and She was diagnosed with "recurrent paroxysmal tachycardia crisis" and
her cardiologists suggested a radio-frequency ablation from the her cardiologists suggested a radio-frequency ablation from the pulmonary veins.pulmonary veins.
Nevertheless, can be seen, in all leads, images of P- waves (more or Nevertheless, can be seen, in all leads, images of P- waves (more or less distorted) - both in basal ECG, in crisis ECG and post-ablation ECG.less distorted) - both in basal ECG, in crisis ECG and post-ablation ECG.
Cannot be seen the typical Rhythm of "irregularly irregular" of atrial Cannot be seen the typical Rhythm of "irregularly irregular" of atrial fibrillation. The heart rate did not reach - in any moment, to values fibrillation. The heart rate did not reach - in any moment, to values "alarming”, since are ever with a "moderately ventricular response "alarming”, since are ever with a "moderately ventricular response (less than 160 bpm).(less than 160 bpm).
If can be observed "bouts" of images for a typical atrial flutter.If can be observed "bouts" of images for a typical atrial flutter. Clearly, on the first recorded ECG, can be seen a Clearly, on the first recorded ECG, can be seen a prolonged PR
interval and QT interval (we have framed on the derivation V4, with (we have framed on the derivation V4, with the corresponding values in seconds).the corresponding values in seconds).
Both entities (isolated) are susceptible to cause serious problems in Both entities (isolated) are susceptible to cause serious problems in heart rhythm since the myocardial cells are extremely vulnerable and heart rhythm since the myocardial cells are extremely vulnerable and susceptible to produce these arrhythmia episodes when present each susceptible to produce these arrhythmia episodes when present each of the separate entities. This fact makes us deduced that, when there is of the separate entities. This fact makes us deduced that, when there is a coexistence of both in a same ECG recording, the possibilities and a coexistence of both in a same ECG recording, the possibilities and severity for the occurrence of these arrhythmia types are greatly severity for the occurrence of these arrhythmia types are greatly increased.increased.
4141
MeasuredMeasured by " Calipers" technique: by " Calipers" technique:
Length of PR interval: 0.220 to 0.230 seconds. (First-degree AV block). Length of PR interval: 0.220 to 0.230 seconds. (First-degree AV block).
Length of RR interval: 0.744 seconds. (Heart rate: 80-81 bpm). Length of RR interval: 0.744 seconds. (Heart rate: 80-81 bpm).
Length of QT interval: 0408-0412 seconds.Length of QT interval: 0408-0412 seconds.
QTc values: a. Bazett: 0473-0477 seconds (prolonged). b. Fridericia: 0450-0455 QTc values: a. Bazett: 0473-0477 seconds (prolonged). b. Fridericia: 0450-0455 seconds (prolonged). c. Framingham: 0450-0451 seconds (prolonged).seconds (prolonged). c. Framingham: 0450-0451 seconds (prolonged).
In all leads can be seen a prolonged PR interval alongside a In all leads can be seen a prolonged PR interval alongside a prolonged QT interval (corrected by different methods.). prolonged QT interval (corrected by different methods.).
This might be the basal problem true.This might be the basal problem true.
4242
Técnicas de Medidas utilizadas.Técnicas de Medidas utilizadas.

4343
Registro ECG en CrisisRegistro ECG en Crisis

4444
ValoraciónValoración Ritmo discretamente “irregularmente irregular”.Ritmo discretamente “irregularmente irregular”. Frecuencia cardiaca máxima de Frecuencia cardiaca máxima de 105 bpm105 bpm.. Visualización de Visualización de ondas P aisladasondas P aisladas (flechas). (flechas). Línea basal isoeléctrica en “espigas” del tipo Línea basal isoeléctrica en “espigas” del tipo
“ondas F”“ondas F” de Flutter. de Flutter. Bloqueo AVBloqueo AV de 1º grado con intervalo PR > 0.200 de 1º grado con intervalo PR > 0.200
seg. (seg. (0.223 seg0.223 seg.)..). Intervalo QT corregido no valorable.Intervalo QT corregido no valorable.
IMPRESIÓN DIAGNÓSTICA ECG:IMPRESIÓN DIAGNÓSTICA ECG: Crisis de Crisis de Flutter auricularFlutter auricular a frecuencia máxima de a frecuencia máxima de
105 bpm. 105 bpm.
4545
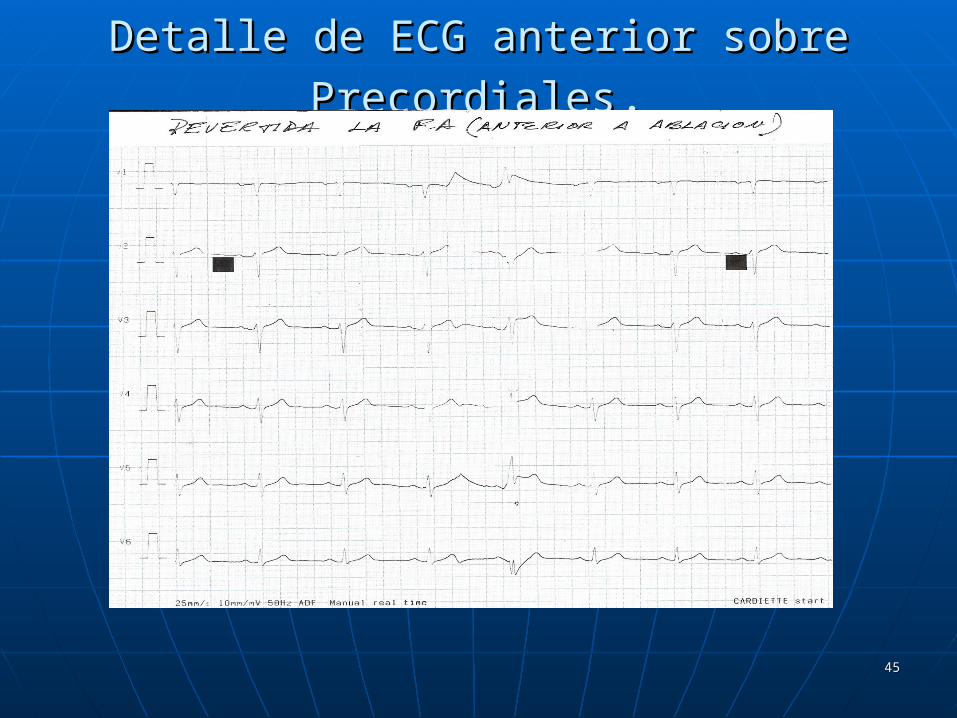
Detalle de ECG anterior sobre PrecordialesDetalle de ECG anterior sobre Precordiales..

4646
Recuperación de ritmo y frecuencia.Recuperación de ritmo y frecuencia. Regularización del intervalo QTcB a Regularización del intervalo QTcB a
0.987 seg. de valor RR.0.987 seg. de valor RR. Persistencia de intervalo PR Persistencia de intervalo PR
prolongado > 0.200 seg.prolongado > 0.200 seg.

4747
ECG post-ablación ECG post-ablación estableestable
4848
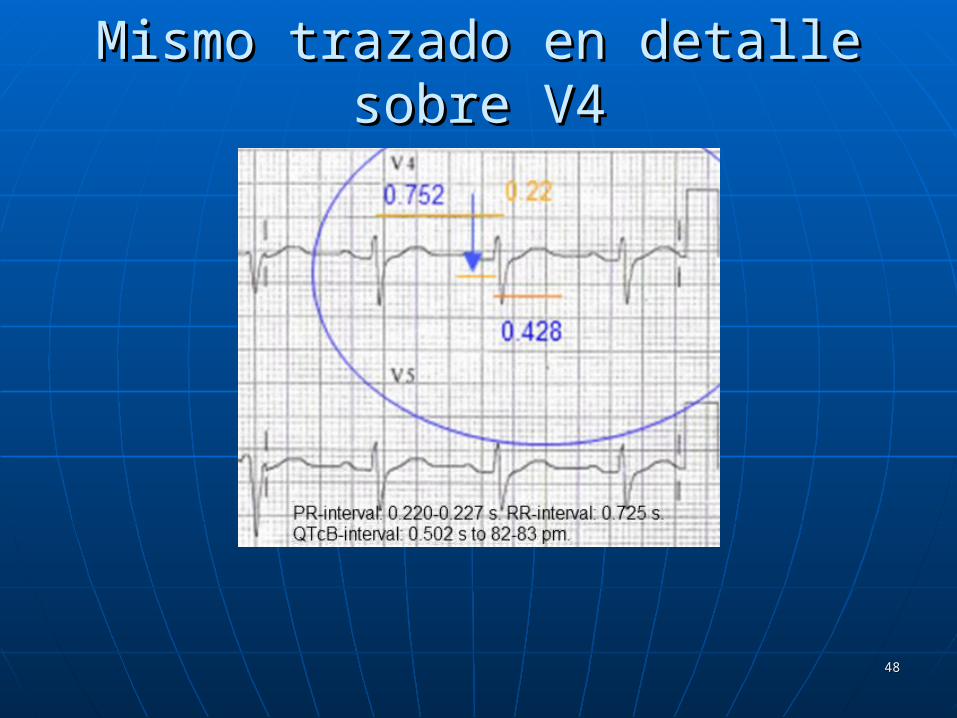
Mismo trazado en detalle sobre V4Mismo trazado en detalle sobre V4

4949
ConsideracionesConsideraciones Ritmo sinusal a 79-81 bpm.Ritmo sinusal a 79-81 bpm. Onda P en D2 de 0.31 mV.Onda P en D2 de 0.31 mV. Permanece la onda S en precordiales Permanece la onda S en precordiales
izquierdas con un Sokolow-Lyon derecho izquierdas con un Sokolow-Lyon derecho aumentado.aumentado.
Intervalo PR: Intervalo PR: 0.2220.222 seg. seg. Intervalo QT: 0.408-0.428 seg.Intervalo QT: 0.408-0.428 seg. Intervalo RR: 0.759- 0.740.Intervalo RR: 0.759- 0.740. Intervalo QTcB: Intervalo QTcB: 0.468- 0.4970.468- 0.497 seg. seg.Permanece la Permanece la prolongaciónprolongación de PR y QTc de PR y QTc

5050

5151
Ultimo trazado ECGUltimo trazado ECG

5252
Situación actual (2011)Situación actual (2011) Paciente actualmente Paciente actualmente estableestable (>18 (>18
meses).meses). Persiste la Persiste la prolongaciónprolongación de intervalos de intervalos
PR (0.212 seg.) y de QTcB (0.451 seg.) PR (0.212 seg.) y de QTcB (0.451 seg.) valorado en D2.valorado en D2.
Medicación actual:Medicación actual: Dronedarona *Dronedarona * 400 mgrs/ 12 horas. 400 mgrs/ 12 horas. Dabigratan**Dabigratan**110 mgrs/ día(???).110 mgrs/ día(???). Telmisartan (ARA III).Telmisartan (ARA III).

5353
* DRONEDARONA* DRONEDARONApreviene la fibrilación auricular o restablece el ritmo previene la fibrilación auricular o restablece el ritmo
sinusal normal dependiendo del modelo utilizado. sinusal normal dependiendo del modelo utilizado. En varios modelos animales también previene la En varios modelos animales también previene la taquicardia ventricular y la fibrilación ventricular. taquicardia ventricular y la fibrilación ventricular. Lo más probable es que estos efectos resulten de Lo más probable es que estos efectos resulten de sus propiedades electrofisiológicas que sus propiedades electrofisiológicas que pertenecen a las cuatro clases de Vaughan-pertenecen a las cuatro clases de Vaughan-Williams. Dronedarona es un bloqueante Williams. Dronedarona es un bloqueante multicanal que inhibe las corrientes de potasio multicanal que inhibe las corrientes de potasio (incluyendo IK(Ach), IKur, IKr, IKs) y que por lo (incluyendo IK(Ach), IKur, IKr, IKs) y que por lo tanto prolonga el potencial de acción cardíaca y tanto prolonga el potencial de acción cardíaca y los periodos refractarios (Clase III). También los periodos refractarios (Clase III). También inhibe las corrientes de sodio (Clase Ib) y las inhibe las corrientes de sodio (Clase Ib) y las corrientes de calcio (Clase IV). Y antagoniza de corrientes de calcio (Clase IV). Y antagoniza de forma no competitiva las actividades forma no competitiva las actividades adrenérgicas (Clase II). adrenérgicas (Clase II).
5454
Propiedades farmacodinámicasPropiedades farmacodinámicas En modelos animales, Dronedarona reduce la frecuencia En modelos animales, Dronedarona reduce la frecuencia
cardíaca. cardíaca. Prolonga la longitud del ciclo de Wenckebach Prolonga la longitud del ciclo de Wenckebach y los intervalos AH-, PQ-, QT-y los intervalos AH-, PQ-, QT-; sin ningún efecto marcado ; sin ningún efecto marcado o un incremento débil en los intervalos QTc-, y sin ningún o un incremento débil en los intervalos QTc-, y sin ningún cambio en los intervalos HV- y QRS-. cambio en los intervalos HV- y QRS-.
Aumenta los periodos efectivos refractarios (PER) de la Aumenta los periodos efectivos refractarios (PER) de la aurícula, del nódulo aurículo ventricular, y prolonga aurícula, del nódulo aurículo ventricular, y prolonga ligeramente el PER ventricular con un grado mínimo de ligeramente el PER ventricular con un grado mínimo de dependencia de frecuencia invertida.dependencia de frecuencia invertida.
Dronedarona disminuye la presión arterial sanguínea y la Dronedarona disminuye la presión arterial sanguínea y la contractilidad del miocardio (dP/dt máx) sin ningún cambio contractilidad del miocardio (dP/dt máx) sin ningún cambio en la fracción de eyección ventricular izquierda y reduce el en la fracción de eyección ventricular izquierda y reduce el consumo miocárdico de oxígeno.consumo miocárdico de oxígeno.
Dronedarona tiene propiedades vasodilatadoras en arterias Dronedarona tiene propiedades vasodilatadoras en arterias coronarias (relacionadas con la activación de la vía del óxido coronarias (relacionadas con la activación de la vía del óxido nítrico) y en arterias periféricas.nítrico) y en arterias periféricas.
Dronedarona presenta efectos antiadrenérgicos indirectos y Dronedarona presenta efectos antiadrenérgicos indirectos y antagonismo parcial a la estimulación adrenérgica. Reduce la antagonismo parcial a la estimulación adrenérgica. Reduce la respuesta alfa-adrenérgica de la presión arterial a la respuesta alfa-adrenérgica de la presión arterial a la epinefrina y las respuestas beta 1 y beta 2 al isoproterenol.epinefrina y las respuestas beta 1 y beta 2 al isoproterenol.
5555
** DABIGRATAN** DABIGRATAN::
Su uso concomitante con Su uso concomitante con AmiodaronaAmiodarona. (AA tipo III).. (AA tipo III). ProfanenonaProfanenona. (AA tipo Ic). (AA tipo Ic) DronedaronaDronedarona.. Quinidina (AA tipo Ia)Quinidina (AA tipo Ia) Verapamilo (AA tipo IV): Verapamilo (AA tipo IV):
Reducir dosis a más del30 % mg/día Reducir dosis a más del30 % mg/día de la dosis recomendada (tomar a la de la dosis recomendada (tomar a la vez). vez).

5656
Dabigratan está, actualmente, en periodo III-b de Dabigratan está, actualmente, en periodo III-b de experimentación clínica. experimentación clínica.
Actualmente está “Actualmente está “paralizadoparalizado” su uso por la F.D.A. debido al ” su uso por la F.D.A. debido al mal ajuste del I.N.R. mal ajuste del I.N.R.
Hemos visto demasiadas controversias acerca de su uso como Hemos visto demasiadas controversias acerca de su uso como anticoagulante de elección en la Fibrilación auricular- anticoagulante de elección en la Fibrilación auricular-
independientemente del estadio de la mismaindependientemente del estadio de la misma..
ReferencesReferences
Baruch L, Sherman O. Potential inaccuracy of point-of-care INR in dabigatran-treated patients.Baruch L, Sherman O. Potential inaccuracy of point-of-care INR in dabigatran-treated patients. Ann PharmacotherAnn Pharmacother 2011; DOI: 10.1345/aph.1Q105. 2011; DOI: 10.1345/aph.1Q105. Available at: Available at: httphttp://://www.theannals.comwww.theannals.com..AbstractAbstract
DeRemer CE, Gujral JS, Thornton JW, Sorrentino RA. Clinical communication to the editor. Dabigatran falsely elevates point-of-care international DeRemer CE, Gujral JS, Thornton JW, Sorrentino RA. Clinical communication to the editor. Dabigatran falsely elevates point-of-care international normalized ratio results. normalized ratio results. Am J Med Am J Med 2011; DOI: 10.1016/j.amjmed.2011.02.009. Available at: 2011; DOI: 10.1016/j.amjmed.2011.02.009. Available at: httphttp://://www.amjmed.comwww.amjmed.com. . AbstractAbstract
5757
Definición (AHA y ESC) de Fibrilación AuricularDefinición (AHA y ESC) de Fibrilación Auricular FA se define como una arritmia cardíaca con las FA se define como una arritmia cardíaca con las
siguientes características:siguientes características:
El ECG de superficie muestra "absolutamente El ECG de superficie muestra "absolutamente irregularidadirregularidad de los intervalos RR (a veces de los intervalos RR (a veces conocida como conocida como arritmia absolutaarritmia absoluta ), es decir, los ), es decir, los intervalos RR que no siguen un patrón repetitivo.intervalos RR que no siguen un patrón repetitivo.
No hay ondas PNo hay ondas P en el ECG de superficie. Algunos en el ECG de superficie. Algunos aparentemente regular la actividad eléctrica aparentemente regular la actividad eléctrica auricular puede ser visto en algunas derivaciones auricular puede ser visto en algunas derivaciones del ECG, con mayor frecuencia en la derivación V1.del ECG, con mayor frecuencia en la derivación V1.
La longitud del ciclo auricular (cuando es visible), La longitud del ciclo auricular (cuando es visible), es decir, el intervalo entre dos activaciones es decir, el intervalo entre dos activaciones auriculares, suele ser variable y <200 ms (> 300 auriculares, suele ser variable y <200 ms (> 300 lpm).lpm).
5858
Conclusiones finalesConclusiones finales No estamos seguros de que los eventos No estamos seguros de que los eventos
fueran debidos a una Fibrilación Auricular. fueran debidos a una Fibrilación Auricular. Nos inclinamos a pensar en crisis de Flutter Nos inclinamos a pensar en crisis de Flutter Auricular compensado.Auricular compensado.
Nos planteamos si hubo una “gran disociación Nos planteamos si hubo una “gran disociación sintomatico- electrocardiográfica.sintomatico- electrocardiográfica.
Posiblemente, el Posiblemente, el problema de base problema de base ((PrimarioPrimario)) fuera un patrón mixto de fuera un patrón mixto de prolongación de los intervalos PR y QT.prolongación de los intervalos PR y QT.
5959
La máxima frecuencia cardíaca La máxima frecuencia cardíaca alcanzada- según los datos de que alcanzada- según los datos de que disponemos- fue de 150 bpm. Y en disponemos- fue de 150 bpm. Y en salvas.salvas.
No observamos la típica imagen de No observamos la típica imagen de ciclos “irregularmente-irregulares” ciclos “irregularmente-irregulares” en ninguno de los registros.en ninguno de los registros.
Incluso en periodos de crisis, hemos Incluso en periodos de crisis, hemos podido observar la presencia de podido observar la presencia de ondas P.ondas P.
6060
En ningún momento hemos podido En ningún momento hemos podido observar que se “agotasen” todos los observar que se “agotasen” todos los recursos farmacológicos para recursos farmacológicos para obtener una correcta y satisfactoria obtener una correcta y satisfactoria cardioversión medicamentosa antes cardioversión medicamentosa antes de la Radio-ablación de venas de la Radio-ablación de venas Pulmonares.Pulmonares.
En base a esto,, la decisión de En base a esto,, la decisión de Ablación con Radiofrecuencia Ablación con Radiofrecuencia después de sólo 5 crisis y máxime sin después de sólo 5 crisis y máxime sin agotar las posibilidades terapéuticas agotar las posibilidades terapéuticas incruentas, nos parece incruentas, nos parece PrematuraPrematura..

6161
La paciente presentaba una prolongación del La paciente presentaba una prolongación del intervalo PR y del QTcB desde el principio intervalo PR y del QTcB desde el principio (antes de la primera crisis).(antes de la primera crisis).
Esta prolongación no desapareció ni con Esta prolongación no desapareció ni con medidas farmacológicas, ni intervencionistas medidas farmacológicas, ni intervencionistas ni mixtas.ni mixtas.
No obstante, no hemos visto que dicha No obstante, no hemos visto que dicha situación (prolongación de intervalos) se situación (prolongación de intervalos) se contemplaseen ningún momento.contemplaseen ningún momento.

6262
Está ampliamente demostrado la Está ampliamente demostrado la relación que existe entre el Bloqueo relación que existe entre el Bloqueo AV de primer grado y la aparición de AV de primer grado y la aparición de crisis de Fibrilación auricular:crisis de Fibrilación auricular:
Michael O'Riordan. PR-Interval Prolongation Increases Risk of Atrial Fibrillation and Pacemaker Michael O'Riordan. PR-Interval Prolongation Increases Risk of Atrial Fibrillation and Pacemaker ImplantationImplantation... . JAMA JAMA 2009;2009; 302: 2324-2332 302: 2324-2332. .
Cheng S, Keyes WJ, Larson MG, et al. Long-term outcomes in individuals with prolonged PR interval or Cheng S, Keyes WJ, Larson MG, et al. Long-term outcomes in individuals with prolonged PR interval or
first-degree atrioventricular block. first-degree atrioventricular block. JAMAJAMA 2009; 301: 2571-2577 2009; 301: 2571-2577. .
6363
También está ampliamente También está ampliamente demostrada esta asociación junto demostrada esta asociación junto con la de un QTc prolongado:con la de un QTc prolongado:
Breijo-Marquez FR, Pardo Ríos M (2011) Wolff-Parkinson-White and Prolonged “Q-T” Patterns in the Breijo-Marquez FR, Pardo Ríos M (2011) Wolff-Parkinson-White and Prolonged “Q-T” Patterns in the Same Electrocardiographic Record. Same Electrocardiographic Record. J Clinic Experiment Cardiol 2:118. doi:10.4172/2155-J Clinic Experiment Cardiol 2:118. doi:10.4172/2155-9880.1000118.9880.1000118.
Breijo-Márquez FR, Ríos MP, Baños MA. Presence of a critical stenosis in left anterior descending Breijo-Márquez FR, Ríos MP, Baños MA. Presence of a critical stenosis in left anterior descending coronary artery alongside a short "P-R" and "Q-T" pattern, in the same electrocardiographic record. coronary artery alongside a short "P-R" and "Q-T" pattern, in the same electrocardiographic record. JJ ElectrocardiolElectrocardiol.. 2010;43(5):422-4. 2010;43(5):422-4.
Breijo-Márquez FR, Pardo Ríos M, Alcaraz Baños M. Association of short PR interval, long QT interval and sudden cardiac death in a young male. Rev Esp Cardiol. 2010 Mar;63(3):362-4.
Breijo-Marquez FR, Rios MP. Variability and diversity of the electrical cardiac systole. BMJ Case Rep. 2009;2009. pii: bcr06.2008.0284.
Breijo-Marquez FR .Decrease of electrical cardiac systole. Int J Cardiol. 2008 May 23;126(2):e36-8.
6464
REFERENCESREFERENCES1.1. Stewart S, Hart CL, Hole DJ, McMurray JJ. Population prevalence, incidence, and predictors of atrial Stewart S, Hart CL, Hole DJ, McMurray JJ. Population prevalence, incidence, and predictors of atrial
fibrillation in the Renfrew/Paisley study. fibrillation in the Renfrew/Paisley study. HeartHeart 2001;86:516–521. 2001;86:516–521.2.2. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed
atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMAJAMA2001;285:2370–2375.2001;285:2370–2375.
3.3. Kirchhof P, Auricchio A, Bax J, Crijns H, Camm J, Diener HC, Goette A, Hindricks G, Hohnloser S, Kirchhof P, Auricchio A, Bax J, Crijns H, Camm J, Diener HC, Goette A, Hindricks G, Hohnloser S, Kappenberger L, Kuck KH, Lip GY, Olsson B, Meinertz T, Priori S, Ravens U, Steinbeck G, Svernhage Kappenberger L, Kuck KH, Lip GY, Olsson B, Meinertz T, Priori S, Ravens U, Steinbeck G, Svernhage E, Tijssen J, Vincent A, Breithardt G. Outcome parameters for trials in atrial fibrillation: executive E, Tijssen J, Vincent A, Breithardt G. Outcome parameters for trials in atrial fibrillation: executive summary. Recommendations from a consensus conference organized by the German Atrial summary. Recommendations from a consensus conference organized by the German Atrial Fibrillation Competence NETwork (AFNET) and the European Heart Rhythm Association (EHRA). Fibrillation Competence NETwork (AFNET) and the European Heart Rhythm Association (EHRA). Eur Eur Heart JHeart J 2007;28:2803–2817. 2007;28:2803–2817.
4.4. Lip GY, Golding DJ, Nazir M, Beevers DG, Child DL, Fletcher RI. A survey of atrial fibrillation in Lip GY, Golding DJ, Nazir M, Beevers DG, Child DL, Fletcher RI. A survey of atrial fibrillation in general practice: the West Birmingham Atrial Fibrillation Project. general practice: the West Birmingham Atrial Fibrillation Project. Br J Gen PractBr J Gen Pract1997;47:285–289.1997;47:285–289.
5.5. Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. implications on the projections for future prevalence. CirculationCirculation 2006;114:119–125. 2006;114:119–125.
6.6. Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, Stricker BH, Stijnen T, Lip GY, Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, Stricker BH, Stijnen T, Lip GY, Witteman JC. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Witteman JC. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Eur Heart JHeart J 2006;27:949–953. 2006;27:949–953.
7.7. Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. the United States. Am J CardiolAm J Cardiol 2009;104:1534–1539. 2009;104:1534–1539.
8.8. Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, D'Agostino RB, Massaro JM, Beiser Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, D'Agostino RB, Massaro JM, Beiser A, Wolf PA, Benjamin EJ. A, Wolf PA, Benjamin EJ. Lifetime risk for development of atrial fibrillation: the Framingham Heart Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Study. CirculationCirculation 2004;110:1042–1046. 2004;110:1042–1046.
9.9. Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J MedAm J Med2002;113:359–364.2002;113:359–364.
10.10. Hylek EM, Go AS, Chang Y, Jensvold NG, Henault LE, Selby JV, Singer DE. Effect of intensity of oral Hylek EM, Go AS, Chang Y, Jensvold NG, Henault LE, Selby JV, Singer DE. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J MedN Engl J Med2003;349:1019–2003;349:1019–1026.1026.
6565
11.11. Knecht S, Oelschlager C, Duning T, Lohmann H, Albers J, Stehling C, Heindel W, Breithardt G, Knecht S, Oelschlager C, Duning T, Lohmann H, Albers J, Stehling C, Heindel W, Breithardt G, Berger K, Ringelstein EB, Kirchhof P, Wersching H. Atrial fibrillation in stroke-free patients is Berger K, Ringelstein EB, Kirchhof P, Wersching H. Atrial fibrillation in stroke-free patients is associated with memory impairment and hippocampal atrophy. associated with memory impairment and hippocampal atrophy. Eur Heart JEur Heart J 2008;29:2125–2132. 2008;29:2125–2132.
12.12. Friberg L, Hammar N, Rosenqvist M. Stroke in paroxysmal atrial fibrillation: report from the Friberg L, Hammar N, Rosenqvist M. Stroke in paroxysmal atrial fibrillation: report from the Stockholm Cohort of Atrial Fibrillation. Stockholm Cohort of Atrial Fibrillation. Eur Heart JEur Heart J 2010;31:967–975. 2010;31:967–975.
13.13. Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic review. review. Am J MedAm J Med 2006;119(448 e1–e19). 2006;119(448 e1–e19).
14.14. Nieuwlaat R, Capucci A, Camm AJ, Olsson SB, Andresen D, Davies DW, Cobbe S, Breithardt G, Le Nieuwlaat R, Capucci A, Camm AJ, Olsson SB, Andresen D, Davies DW, Cobbe S, Breithardt G, Le Heuzey JY, Prins MH, Levy S, Crijns HJ. Heuzey JY, Prins MH, Levy S, Crijns HJ. Atrial fibrillation management: a prospective survey in Atrial fibrillation management: a prospective survey in ESC member countries: the Euro Heart Survey on Atrial Fibrillation. ESC member countries: the Euro Heart Survey on Atrial Fibrillation. Eur Heart JEur Heart J 2005;26:2422– 2005;26:2422–2434.2434.
15.15. Nabauer M, Gerth A, Limbourg T, Schneider S, Oeff M, Kirchhof P, Goette A, Lewalter T, Ravens Nabauer M, Gerth A, Limbourg T, Schneider S, Oeff M, Kirchhof P, Goette A, Lewalter T, Ravens U, Meinertz T, Breithardt G, Steinbeck G. The Registry of the German Competence NETwork on U, Meinertz T, Breithardt G, Steinbeck G. The Registry of the German Competence NETwork on Atrial Fibrillation: patient characteristics and initial management. Atrial Fibrillation: patient characteristics and initial management. EuropaceEuropace2009;11:423–434.2009;11:423–434.
16.16. Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB. Contemporary definitions and classification of the cardiomyopathies: an American Heart JB. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Prevention. CirculationCirculation 2006;113:1807–1816. 2006;113:1807–1816.
17.17. Goette A, Bukowska A, Dobrev D, Pfeiffenberger J, Morawietz H, Strugala D, Wiswedel I, Rohl FW, Goette A, Bukowska A, Dobrev D, Pfeiffenberger J, Morawietz H, Strugala D, Wiswedel I, Rohl FW, Wolke C, Bergmann S, Bramlage P, Ravens U, Lendeckel U. Acute atrial tachyarrhythmia induces Wolke C, Bergmann S, Bramlage P, Ravens U, Lendeckel U. Acute atrial tachyarrhythmia induces angiotensin II type 1 receptor-mediated oxidative stress and microvascular flow abnormalities in angiotensin II type 1 receptor-mediated oxidative stress and microvascular flow abnormalities in the ventricles. the ventricles. Eur Heart JEur Heart J 2009;30:1411–1420. 2009;30:1411–1420.
18.18. Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillationSchotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation—a translational appraisal. —a translational appraisal. Physiol RevPhysiol Rev 2010. 2010.
19.19. Daoud EG, Bogun F, Goyal R, Harvey M, Man KC, Strickberger SA, Morady F. Effect of atrial Daoud EG, Bogun F, Goyal R, Harvey M, Man KC, Strickberger SA, Morady F. Effect of atrial fibrillation on atrial refractoriness in humans. fibrillation on atrial refractoriness in humans. CirculationCirculation 1996;94:1600–1606. 1996;94:1600–1606.
20.20. Frustaci A, Chimenti C, Bellocci F, Morgante E, Russo MA, Maseri A. Histological substrate of Frustaci A, Chimenti C, Bellocci F, Morgante E, Russo MA, Maseri A. Histological substrate of atrial biopsies in patients with lone atrial fibrillation. atrial biopsies in patients with lone atrial fibrillation. CirculationCirculation 1997;96:1180–1184. 1997;96:1180–1184.
21.21. Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, LeMouroux A, Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, LeMouroux A, LeMetayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating LeMetayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. in the pulmonary veins. N Engl J MedN Engl J Med 1998;339:659–666. 1998;339:659–666.
6666
22.22. Fox CS, Parise H, D'Agostino RB Sr., Lloyd-Jones DM, Vasan RS, Wang TJ, Levy D, Wolf PA, Benjamin EJ. Fox CS, Parise H, D'Agostino RB Sr., Lloyd-Jones DM, Vasan RS, Wang TJ, Levy D, Wolf PA, Benjamin EJ. Parental atrial Parental atrial fibrillation as a risk factor for atrial fibrillation in offspring.fibrillation as a risk factor for atrial fibrillation in offspring.JAMAJAMA 2004;291:2851–2855. 2004;291:2851–2855.
23.23. Kirchhof P, Bax J, Blomstrom-Lundquist C, Calkins H, Camm AJ, Cappato R, Cosio F, Crijns H, Diener HC, Goette A, Israel Kirchhof P, Bax J, Blomstrom-Lundquist C, Calkins H, Camm AJ, Cappato R, Cosio F, Crijns H, Diener HC, Goette A, Israel CW, Kuck KH, Lip GY, Nattel S, Page RL, Ravens U, Schotten U, Steinbeck G, Vardas P, Waldo A, Wegscheider K, Willems CW, Kuck KH, Lip GY, Nattel S, Page RL, Ravens U, Schotten U, Steinbeck G, Vardas P, Waldo A, Wegscheider K, Willems S, Breithardt G. Early and comprehensive management of atrial fibrillation: executive summary of the proceedings from S, Breithardt G. Early and comprehensive management of atrial fibrillation: executive summary of the proceedings from the 2nd AFNET-EHRA consensus conference 'Research perspectives in AF. the 2nd AFNET-EHRA consensus conference 'Research perspectives in AF. Eur Heart JEur Heart J2009;30:2969-2977c.2009;30:2969-2977c.
24.24. Hodgson-Zingman DM, Karst ML, Zingman LV, Heublein DM, Darbar D, Herron KJ, Ballew JD, de Andrade M, Burnett JC Jr., Hodgson-Zingman DM, Karst ML, Zingman LV, Heublein DM, Darbar D, Herron KJ, Ballew JD, de Andrade M, Burnett JC Jr., Olson TM. Atrial natriuretic peptide frameshift mutation in familial atrial fibrillation. Olson TM. Atrial natriuretic peptide frameshift mutation in familial atrial fibrillation. N Engl J MedN Engl J Med 2008;359:158–165. 2008;359:158–165.
25.25. Olson TM, Michels VV, Ballew JD, Reyna SP, Karst ML, Herron KJ, Horton SC, Rodeheffer RJ, Anderson JL. Sodium channel Olson TM, Michels VV, Ballew JD, Reyna SP, Karst ML, Herron KJ, Horton SC, Rodeheffer RJ, Anderson JL. Sodium channel mutations and susceptibility to heart failure and atrial fibrillation. mutations and susceptibility to heart failure and atrial fibrillation. JAMAJAMA 2005;293:447–454. 2005;293:447–454.
26.26. Chen YH, Xu SJ, Bendahhou S, Wang XL, Wang Y, Xu WY, Jin HW, Sun H, Su XY, Zhuang QN, Yang YQ, Li YB, Liu Y, Xu HJ, Chen YH, Xu SJ, Bendahhou S, Wang XL, Wang Y, Xu WY, Jin HW, Sun H, Su XY, Zhuang QN, Yang YQ, Li YB, Liu Y, Xu HJ, Li XF, Ma N, Mou CP, Chen Z, Barhanin J, Huang W. KCNQ1 gain-of-function mutation in familial atrial Li XF, Ma N, Mou CP, Chen Z, Barhanin J, Huang W. KCNQ1 gain-of-function mutation in familial atrial fibrillation. fibrillation. ScienceScience 2003;299:251–254. 2003;299:251–254.
27.27. Gudbjartsson DF, Holm H, Gretarsdottir S, Thorleifsson G, Walters GB, Thorgeirsson G, Gulcher J, Mathiesen EB, Njolstad Gudbjartsson DF, Holm H, Gretarsdottir S, Thorleifsson G, Walters GB, Thorgeirsson G, Gulcher J, Mathiesen EB, Njolstad I, Nyrnes A, Wilsgaard T, Hald EM, Hveem K, Stoltenberg C, Kucera G, Stubblefield T, Carter S, Roden D, Ng MC, Baum L, I, Nyrnes A, Wilsgaard T, Hald EM, Hveem K, Stoltenberg C, Kucera G, Stubblefield T, Carter S, Roden D, Ng MC, Baum L, So WY, Wong KS, Chan JC, Gieger C, Wichmann HE, Gschwendtner A, Dichgans M, Kuhlenbaumer G, Berger K, So WY, Wong KS, Chan JC, Gieger C, Wichmann HE, Gschwendtner A, Dichgans M, Kuhlenbaumer G, Berger K, Ringelstein EB, Bevan S, Markus HS, Kostulas K, Hillert J, Sveinbjornsdottir S, Valdimarsson EM, Lochen ML, Ma RC, Ringelstein EB, Bevan S, Markus HS, Kostulas K, Hillert J, Sveinbjornsdottir S, Valdimarsson EM, Lochen ML, Ma RC, Darbar D, Kong A, Arnar DO, Thorsteinsdottir U, Stefansson K. A sequence variant in ZFHX3 on 16q22 associates with Darbar D, Kong A, Arnar DO, Thorsteinsdottir U, Stefansson K. A sequence variant in ZFHX3 on 16q22 associates with atrial fibrillation and ischemic stroke.atrial fibrillation and ischemic stroke.Nat GenetNat Genet 2009;41:876–878. 2009;41:876–878.
28.28. Packer DL, Bardy GH, Worley SJ, Smith MS, Cobb FR, Coleman RE, Gallagher JJ, German LD. Tachycardia-induced Packer DL, Bardy GH, Worley SJ, Smith MS, Cobb FR, Coleman RE, Gallagher JJ, German LD. Tachycardia-induced cardiomyopathy: a reversible form of left ventricular dysfunction. cardiomyopathy: a reversible form of left ventricular dysfunction. Am J CardiolAm J Cardiol 1986;57:563–570. 1986;57:563–570.
29.29. Watson T, Shantsila E, Lip GY. Mechanisms of thrombogenesis in atrial fibrillation: Virchow's triad Watson T, Shantsila E, Lip GY. Mechanisms of thrombogenesis in atrial fibrillation: Virchow's triad revisited. revisited. LancetLancet 2009;373:155–166. 2009;373:155–166.
30.30. Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF, Antman EM, Smith SC Jr., Faxon DP, Fuster V, Gibbons Lerman BB, Miller DD, Shaeffer CW, Stevenson WG, Tomaselli GF, Antman EM, Smith SC Jr., Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO Jr., Priori SG, Blanc JJ, Budaj A, Burgos EF, Cowie M, Deckers RJ, Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO Jr., Priori SG, Blanc JJ, Budaj A, Burgos EF, Cowie M, Deckers JW, Garcia MA, Klein WW, Lekakis J, Lindahl B, Mazzotta G, Morais JC, Oto A, Smiseth O, Trappe HJ. JW, Garcia MA, Klein WW, Lekakis J, Lindahl B, Mazzotta G, Morais JC, Oto A, Smiseth O, Trappe HJ. ACC/AHA/ESC ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias—executive summary. a report of the guidelines for the management of patients with supraventricular arrhythmias—executive summary. a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the European Society American College of Cardiology/American Heart Association task force on practice guidelines and the European Society of Cardiology committee for practice guidelines (writing committee to develop guidelines for the management of of Cardiology committee for practice guidelines (writing committee to develop guidelines for the management of patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. patients with supraventricular arrhythmias) developed in collaboration with NASPE-Heart Rhythm Society. J Am Coll J Am Coll CardiolCardiol 2003;42:1493–14531. 2003;42:1493–14531.
31.31. Hobbs FD, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, Raftery J, Davies M, Lip G. A randomised controlled trial Hobbs FD, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, Raftery J, Davies M, Lip G. A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. for the detection of atrial fibrillation in people aged 65 and over. The SAFE study. The SAFE study. Health Technol AssessHealth Technol Assess 2005;9:iii–iv. 2005;9:iii–iv.
6767
32.32. Jahangir A, Lee V, Friedman PA, Trusty JM, Hodge DO, Kopecky SL, Packer DL, Hammill SC, Shen WK, Gersh BJ. Long-term progression Jahangir A, Lee V, Friedman PA, Trusty JM, Hodge DO, Kopecky SL, Packer DL, Hammill SC, Shen WK, Gersh BJ. Long-term progression and outcomes with aging in patients with lone atrial fibrillation: a 30-year follow-up study. and outcomes with aging in patients with lone atrial fibrillation: a 30-year follow-up study. CirculationCirculation 2007;115:3050–3056. 2007;115:3050–3056.
33.33. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ Jr., Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ Jr., Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ, Calkins H, Brugada J, Chen SA, Prystowsky EN, Kuck KH, Natale A, Haines Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ, Calkins H, Brugada J, Chen SA, Prystowsky EN, Kuck KH, Natale A, Haines DE, Marchlinski FE, Calkins H, Davies DW, Lindsay BD, McCarthy PM, Packer DL, Cappato R, Crijns HJ, Damiano RJ Jr., Haissaguerre M, DE, Marchlinski FE, Calkins H, Davies DW, Lindsay BD, McCarthy PM, Packer DL, Cappato R, Crijns HJ, Damiano RJ Jr., Haissaguerre M, Jackman WM, Jais P, Iesaka Y, Kottkamp H, Mont L, Morady F, Nademanee K, Pappone C, Raviele A, Ruskin JN, Shemin RJ. Jackman WM, Jais P, Iesaka Y, Kottkamp H, Mont L, Morady F, Nademanee K, Pappone C, Raviele A, Ruskin JN, Shemin RJ. HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for Personnel, Policy, Procedures and Follow-Up: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Personnel, Policy, Procedures and Follow-Up: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the the Society of Thoracic Surgeons (STS). Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Thoracic Surgeons, and the Heart Rhythm Society. EuropaceEuropace 2007;9:335–379. 2007;9:335–379.
34.34. Jabaudon D, Sztajzel J, Sievert K, Landis T, Sztajzel R. Usefulness of ambulatory 7-day ECG monitoring for the detection of atrial Jabaudon D, Sztajzel J, Sievert K, Landis T, Sztajzel R. Usefulness of ambulatory 7-day ECG monitoring for the detection of atrial fibrillation and flutter after acute stroke and transient ischemic attack. fibrillation and flutter after acute stroke and transient ischemic attack. StrokeStroke 2004;35:1647–1651. 2004;35:1647–1651.
35.35. Hindricks G, Piorkowski C, Tanner H, Kobza R, Gerds-Li JH, Carbucicchio C, Kottkamp H. Perception of atrial fibrillation before and Hindricks G, Piorkowski C, Tanner H, Kobza R, Gerds-Li JH, Carbucicchio C, Kottkamp H. Perception of atrial fibrillation before and after radiofrequency catheter ablation: relevance of asymptomatic arrhythmia recurrence. after radiofrequency catheter ablation: relevance of asymptomatic arrhythmia recurrence. CirculationCirculation 2005;112:307–313. 2005;112:307–313.
36.36. Israel CW, Gronefeld G, Ehrlich JR, Li YG, Hohnloser SH. Israel CW, Gronefeld G, Ehrlich JR, Li YG, Hohnloser SH. Long-term risk of recurrent atrial fibrillation as documented by an implantable Long-term risk of recurrent atrial fibrillation as documented by an implantable monitoring device: implications for optimal patient care. monitoring device: implications for optimal patient care. J Am Coll CardiolJ Am Coll Cardiol 2004;43:47–52. 2004;43:47–52.
37.37. Ziegler PD, Koehler JL, Mehra R. Comparison of continuous versus intermittent monitoring of atrial arrhythmias. Ziegler PD, Koehler JL, Mehra R. Comparison of continuous versus intermittent monitoring of atrial arrhythmias. Heart Heart RhythmRhythm 2006;3:1445–1452. 2006;3:1445–1452.
38.38. Binici Z, Intzilakis T, Nielsen OW, Kober L, Sajadieh A. Excessive Supraventricular ectopic activity and increased risk of atrial Binici Z, Intzilakis T, Nielsen OW, Kober L, Sajadieh A. Excessive Supraventricular ectopic activity and increased risk of atrial fibrillation and stroke. fibrillation and stroke. CirculationCirculation 2010;121:1904–1911. 2010;121:1904–1911.
39.39. Brignole M, Vardas P, Hoffman E, Huikuri H, Moya A, Ricci R, Sulke N, Wieling W, Auricchio A, Lip GY, Almendral J, Kirchhof P, Aliot E, Brignole M, Vardas P, Hoffman E, Huikuri H, Moya A, Ricci R, Sulke N, Wieling W, Auricchio A, Lip GY, Almendral J, Kirchhof P, Aliot E, Gasparini M, Braunschweig F, Botto GL. Gasparini M, Braunschweig F, Botto GL. Indications for the use of diagnostic implantable and external ECG loop Indications for the use of diagnostic implantable and external ECG loop recorders. recorders. EuropaceEuropace2009;11:671–687.2009;11:671–687.
40.40. Hindricks G, Pokushalov E, Urban L, Taborsky M, Kuck KH, Lebedev D, Rieger G, Purerfellner H. Performance of a new leadless Hindricks G, Pokushalov E, Urban L, Taborsky M, Kuck KH, Lebedev D, Rieger G, Purerfellner H. Performance of a new leadless implantable cardiac monitor in detecting and quantifying atrial fibrillation—results of the XPECT trial. implantable cardiac monitor in detecting and quantifying atrial fibrillation—results of the XPECT trial. Circ Arrhythm Circ Arrhythm ElectrophysiolElectrophysiol 2010;3:141–147. 2010;3:141–147.
41.41. Dorian P, Guerra PG, Kerr CR, O'Donnell SS, Crystal E, Gillis AM, Mitchell LB, Roy D, Skanes AC, Rose MS, Wyse DG. Validation of a Dorian P, Guerra PG, Kerr CR, O'Donnell SS, Crystal E, Gillis AM, Mitchell LB, Roy D, Skanes AC, Rose MS, Wyse DG. Validation of a new simple scale to measure symptoms in atrial fibrillation: the Canadian Cardiovascular Society Severity in Atrial Fibrillation new simple scale to measure symptoms in atrial fibrillation: the Canadian Cardiovascular Society Severity in Atrial Fibrillation scale. scale. Circ Arrhythm ElectrophysiolCirc Arrhythm Electrophysiol 2009;2:218–224. 2009;2:218–224.
42.42. Klein AL, Grimm RA, Murray RD, Apperson-Hansen C, Asinger RW, Black IW, Davidoff R, Erbel R, Halperin JL, Orsinelli DA, Porter TR, Klein AL, Grimm RA, Murray RD, Apperson-Hansen C, Asinger RW, Black IW, Davidoff R, Erbel R, Halperin JL, Orsinelli DA, Porter TR, Stoddard MF. Use of transesophageal echocardiography to guide cardioversion in patients with atrial fibrillation. Stoddard MF. Use of transesophageal echocardiography to guide cardioversion in patients with atrial fibrillation. N Engl J N Engl J MedMed2001;344:1411–1420.2001;344:1411–1420.
43.43. Fitzmaurice DA, Hobbs FD, Jowett S, Mant J, Murray ET, Holder R, Raftery JP, Bryan S, Davies M, Lip GY, Allan TF. Screening versus Fitzmaurice DA, Hobbs FD, Jowett S, Mant J, Murray ET, Holder R, Raftery JP, Bryan S, Davies M, Lip GY, Allan TF. Screening versus routine practice in detection of atrial fibrillation in patients aged 65 or over: cluster randomised controlled trial. routine practice in detection of atrial fibrillation in patients aged 65 or over: cluster randomised controlled trial. BMJBMJ 2007;335(383). 2007;335(383).
44.44. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, Stromberg A, van Veldhuisen DJ, Atar D, Hoes Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, Stromberg A, van Veldhuisen DJ, Atar D, Hoes AW, Keren A, Mebazaa A, Nieminen M, Priori SG, Swedberg K, Vahanian A, Camm J, De Caterina R, Dean V, Funck-Brentano C, AW, Keren A, Mebazaa A, Nieminen M, Priori SG, Swedberg K, Vahanian A, Camm J, De Caterina R, Dean V, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL. Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL. ESC Guidelines for the diagnosis ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J 2008Eur Heart J 200829:2388–2442.29:2388–2442.
6868
45.45. Haverkamp W, Breithardt G, Camm AJ, Janse MJ, Rosen MR, Antzelevitch C, Escande D, Franz M, Malik M, Moss A, Shah R. Haverkamp W, Breithardt G, Camm AJ, Janse MJ, Rosen MR, Antzelevitch C, Escande D, Franz M, Malik M, Moss A, Shah R. The potential for QT prolongation and proarrhythmia by non-antiarrhythmic drugs: clinical and regulatory implications. The potential for QT prolongation and proarrhythmia by non-antiarrhythmic drugs: clinical and regulatory implications. Report on a policy conference of the European Society of Cardiology. Report on a policy conference of the European Society of Cardiology. Eur Heart JEur Heart J 2000;21:1216–1231. 2000;21:1216–1231.
46.46. Singh BN, Singh SN, Reda DJ, Tang XC, Lopez B, Harris CL, Fletcher RD, Sharma SC, Atwood JE, Jacobson AK, Lewis HD Jr., Singh BN, Singh SN, Reda DJ, Tang XC, Lopez B, Harris CL, Fletcher RD, Sharma SC, Atwood JE, Jacobson AK, Lewis HD Jr., Raisch DW, Ezekowitz MD. Amiodarone versus sotalol for atrial fibrillation. Raisch DW, Ezekowitz MD. Amiodarone versus sotalol for atrial fibrillation. N Engl J MedN Engl J Med 2005;352:1861–1872. 2005;352:1861–1872.
47.47. Hughes M, Lip GY. Stroke and thromboembolism in atrial fibrillation: a systematic review of stroke risk factors, risk Hughes M, Lip GY. Stroke and thromboembolism in atrial fibrillation: a systematic review of stroke risk factors, risk stratification schema and cost effectiveness data. stratification schema and cost effectiveness data. Thromb HaemostThromb Haemost2008;99:295–304.2008;99:295–304.
48.48. Stroke in AF working group. Independent predictors of stroke in patients with atrial fibrillation: a systematic Stroke in AF working group. Independent predictors of stroke in patients with atrial fibrillation: a systematic review. review. NeurologyNeurology 2007;69:546–554. 2007;69:546–554.
49.49. Schmitt J, Duray G, Gersh BJ, Hohnloser SH. Atrial fibrillation in acute myocardial infarction: a systematic review of the Schmitt J, Duray G, Gersh BJ, Hohnloser SH. Atrial fibrillation in acute myocardial infarction: a systematic review of the incidence, clinical features and prognostic implications. incidence, clinical features and prognostic implications. Eur Heart JEur Heart J2009;30:1038–1045.2009;30:1038–1045.
50.50. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. predicting stroke: results from the National Registry of Atrial Fibrillation. JAMAJAMA 2001;285:2864–2870. 2001;285:2864–2870.
51.51. Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, Jensvold NG, Selby JV, Singer DE. Anticoagulation therapy Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, Jensvold NG, Selby JV, Singer DE. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? practice? JAMAJAMA 2003;290:2685–2692. 2003;290:2685–2692.
52.52. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on atrial thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on atrial fibrillation. fibrillation. ChestChest 2010;137:263–272. 2010;137:263–272.
53.53. Lip GY, Frison L, Halperin J, Lane D. Identifying patients at risk of stroke despite anticoagulation. Lip GY, Frison L, Halperin J, Lane D. Identifying patients at risk of stroke despite anticoagulation. StrokeStroke 2010. 2010.54.54. Hart RG, Pearce LA, Aguilar MI. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have Meta-analysis: antithrombotic therapy to prevent stroke in patients who have
nonvalvular atrial fibrillation. nonvalvular atrial fibrillation. Ann Intern MedAnn Intern Med 2007;146:857–867. 2007;146:857–867.55.55. Sato H, Ishikawa K, Kitabatake A, Ogawa S, Maruyama Y, Yokota Y, Fukuyama T, Doi Y, Mochizuki S, Izumi T, Takekoshi Sato H, Ishikawa K, Kitabatake A, Ogawa S, Maruyama Y, Yokota Y, Fukuyama T, Doi Y, Mochizuki S, Izumi T, Takekoshi
N, Yoshida K, Hiramori K, Origasa H, Uchiyama S, Matsumoto M, Yamaguchi T, Hori M. Low-dose aspirin for prevention of N, Yoshida K, Hiramori K, Origasa H, Uchiyama S, Matsumoto M, Yamaguchi T, Hori M. Low-dose aspirin for prevention of stroke in low-risk patients with atrial fibrillation: Japan Atrial Fibrillation Stroke Trial. stroke in low-risk patients with atrial fibrillation: Japan Atrial Fibrillation Stroke Trial. StrokeStroke 2006;37:447–451. 2006;37:447–451.
56.56. Mant J, Hobbs FD, Fletcher K, Roalfe A, Fitzmaurice D, Lip GY, Murray E. Warfarin versus aspirin for stroke prevention in Mant J, Hobbs FD, Fletcher K, Roalfe A, Fitzmaurice D, Lip GY, Murray E. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a randomised controlled trial. BAFTA): a randomised controlled trial. LancetLancet 2007;370:493–503. 2007;370:493–503.
57.57. Connolly S, Pogue J, Hart R, Pfeffer M, Hohnloser S, Chrolavicius S, Yusuf S. Clopidogrel plus aspirin versus oral Connolly S, Pogue J, Hart R, Pfeffer M, Hohnloser S, Chrolavicius S, Yusuf S. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial.Events (ACTIVE W): a randomised controlled trial.LancetLancet 2006;367:1903–1912. 2006;367:1903–1912.
58.58. Connolly SJ, Pogue J, Hart RG, Hohnloser SH, Pfeffer M, Chrolavicius S, Yusuf S. Effect of clopidogrel added to aspirin in Connolly SJ, Pogue J, Hart RG, Hohnloser SH, Pfeffer M, Chrolavicius S, Yusuf S. Effect of clopidogrel added to aspirin in patients with atrial fibrillation. patients with atrial fibrillation. N Engl J MedN Engl J Med 2009;360:2066–2078. 2009;360:2066–2078.
59.59. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L. Dabigatran versus warfarin in Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L. Dabigatran versus warfarin in patients with atrial fibrillation. patients with atrial fibrillation. N Engl J MedN Engl J Med 2009;361:1139–1151. 2009;361:1139–1151.
60.60. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess one-year A novel user-friendly score (HAS-BLED) to assess one-year risk of major bleeding in atrial fibrillation patients: The Euro Heart Survey. risk of major bleeding in atrial fibrillation patients: The Euro Heart Survey. ChestChest 2010. 2010.
6969
61.61. Lip GY, Huber K, Andreotti F, Arnesen H, Airaksinen KJ, Cuisset T, Kirchhof P, Marin F. Management of antithrombotic therapy in atrial fibrillation Lip GY, Huber K, Andreotti F, Arnesen H, Airaksinen KJ, Cuisset T, Kirchhof P, Marin F. Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary intervention/stenting. patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary intervention/stenting. Thromb HaemostThromb Haemost 2010;103:13– 2010;103:13–28.28.
62.62. Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P. Percutaneous closure of the left atrial appendage versus Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. LancetLancet2009;374:534–542.2009;374:534–542.
63.63. Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ. Antithrombotic therapy in atrial fibrillation: American College of Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). ChestChest 2008;133(546S–592S). 2008;133(546S–592S).
64.64. Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A. Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A. Guidelines on the management of valvular heart disease: the Task Force on the Management of Valvular Heart Disease of the European Society of Guidelines on the management of valvular heart disease: the Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Cardiology. Eur Heart JEur Heart J 2007;28:230–268. 2007;28:230–268.
65.65. Fang MC, Go AS, Hylek EM, Chang Y, Henault LE, Jensvold NG, Singer DE. Age and the risk of warfarin-associated hemorrhage: the anticoagulation Fang MC, Go AS, Hylek EM, Chang Y, Henault LE, Jensvold NG, Singer DE. Age and the risk of warfarin-associated hemorrhage: the anticoagulation and risk factors in atrial fibrillation study. and risk factors in atrial fibrillation study. J Am Geriatr SocJ Am Geriatr Soc 2006;54:1231–1236. 2006;54:1231–1236.
66.66. Poldermans D, Bax JJ, Boersma E, De Hert S, Eeckhout E, Fowkes G, Gorenek B, Hennerici MG, Iung B, Kelm M, Kjeldsen KP, Kristensen SD, Lopez-Poldermans D, Bax JJ, Boersma E, De Hert S, Eeckhout E, Fowkes G, Gorenek B, Hennerici MG, Iung B, Kelm M, Kjeldsen KP, Kristensen SD, Lopez-Sendon J, Pelosi P, Philippe F, Pierard L, Ponikowski P, Schmid JP, Sellevold OF, Sicari R, Van den Berghe G, Vermassen F, Hoeks SE, Vanhorebeek I, Sendon J, Pelosi P, Philippe F, Pierard L, Ponikowski P, Schmid JP, Sellevold OF, Sicari R, Van den Berghe G, Vermassen F, Hoeks SE, Vanhorebeek I, Vahanian A, Auricchio A, Ceconi C, Dean V, Filippatos G, Funck-Brentano C, Hobbs R, Kearn P, McDonag T, McGregor K, Popescu BA, Reiner Z, Vahanian A, Auricchio A, Ceconi C, Dean V, Filippatos G, Funck-Brentano C, Hobbs R, Kearn P, McDonag T, McGregor K, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Vardas P, Widimsky P, De Caterina R, Agewall S, Al Attar N, Andreotti F, Anker SD, Baron-Esquivias G, Berkenboom Sechtem U, Sirnes PA, Tendera M, Vardas P, Widimsky P, De Caterina R, Agewall S, Al Attar N, Andreotti F, Anker SD, Baron-Esquivias G, Berkenboom G, Chapoutot L, Cifkova R, Faggiano P, Gibbs S, Hansen HS, Iserin L, Israel CW, Kornowski R, Eizagaechevarria NM, Pepi M, Piepoli M, Priebe HJ, G, Chapoutot L, Cifkova R, Faggiano P, Gibbs S, Hansen HS, Iserin L, Israel CW, Kornowski R, Eizagaechevarria NM, Pepi M, Piepoli M, Priebe HJ, Scherer M, Stepinska J, Taggart D, Tubaro M. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-Scherer M, Stepinska J, Taggart D, Tubaro M. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery: the Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery of the cardiac surgery: the Task Force for Preoperative Cardiac Risk Assessment and Perioperative Cardiac Management in Non-cardiac Surgery of the European Society of Cardiology (ESC) and endorsed by the European Society of Anaesthesiology (ESA). European Society of Cardiology (ESC) and endorsed by the European Society of Anaesthesiology (ESA). Eur J AnaesthesiolEur J Anaesthesiol2010;27:92–137.2010;27:92–137.
67.67. Alboni P, Botto GL, Baldi N, Luzi M, Russo V, Gianfranchi L, Marchi P, Calzolari M, Solano A, Baroffio R, Gaggioli G. Outpatient treatment of recent-Alboni P, Botto GL, Baldi N, Luzi M, Russo V, Gianfranchi L, Marchi P, Calzolari M, Solano A, Baroffio R, Gaggioli G. Outpatient treatment of recent-onset atrial fibrillation with the 'pill-in-the-pocket' approach. onset atrial fibrillation with the 'pill-in-the-pocket' approach. N Engl J MedN Engl J Med 2004;351:2384–2391. 2004;351:2384–2391.
68.68. Kowey PR, Dorian P, Mitchell LB, Pratt CM, Roy D, Schwartz PJ, Sadowski J, Sobczyk D, Bochenek A, Toft E. Vernakalant hydrochloride for the rapid Kowey PR, Dorian P, Mitchell LB, Pratt CM, Roy D, Schwartz PJ, Sadowski J, Sobczyk D, Bochenek A, Toft E. Vernakalant hydrochloride for the rapid conversion of atrial fibrillation after cardiac surgery: a randomized, double-blind, placebo-controlled trial. conversion of atrial fibrillation after cardiac surgery: a randomized, double-blind, placebo-controlled trial. Circ Arrhythm ElectrophysiolCirc Arrhythm Electrophysiol 2009;2:652– 2009;2:652–659.659.
69.69. Roy D, Pratt CM, Torp-Pedersen C, Wyse DG, Toft E, Juul-Moller S, Nielsen T, Rasmussen SL, Stiell IG, Coutu B, Ip JH, Pritchett EL, Camm AJ. Roy D, Pratt CM, Torp-Pedersen C, Wyse DG, Toft E, Juul-Moller S, Nielsen T, Rasmussen SL, Stiell IG, Coutu B, Ip JH, Pritchett EL, Camm AJ. Vernakalant hydrochloride for rapid conversion of atrial fibrillation: a phase 3, randomized, placebo-controlled trial. Vernakalant hydrochloride for rapid conversion of atrial fibrillation: a phase 3, randomized, placebo-controlled trial. CirculationCirculation2008;117:1518–1525.2008;117:1518–1525.
70.70. Camm AJ, Capucci A, Hohnloser S, Torp-Pedersen C, Van Gelder IC, Mangal B, Beatch GN. A randomized active-controlled study comparing the Camm AJ, Capucci A, Hohnloser S, Torp-Pedersen C, Van Gelder IC, Mangal B, Beatch GN. A randomized active-controlled study comparing the efficacy and safety of vernakalant to amiodarone in recent onset atrial fibrillation. efficacy and safety of vernakalant to amiodarone in recent onset atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2010. 2010.
71.71. Reisinger J, Gatterer E, Lang W, Vanicek T, Eisserer G, Bachleitner T, Niemeth C, Aicher F, Grander W, Heinze G, Kuhn P, Siostrzonek P. Flecainide Reisinger J, Gatterer E, Lang W, Vanicek T, Eisserer G, Bachleitner T, Niemeth C, Aicher F, Grander W, Heinze G, Kuhn P, Siostrzonek P. Flecainide versus ibutilide for immediate cardioversion of atrial fibrillation of recent onset. versus ibutilide for immediate cardioversion of atrial fibrillation of recent onset. Eur Heart JEur Heart J 2004;25:1318–1324. 2004;25:1318–1324.
72.72. Khan IA. Single oral loading dose of propafenone for pharmacological cardioversion of recent-onset atrial fibrillation. Khan IA. Single oral loading dose of propafenone for pharmacological cardioversion of recent-onset atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2001;37:542– 2001;37:542–547.547.
73.73. Martinez-Marcos FJ, Garcia-Garmendia JL, Ortega-Carpio A, Fernandez- Gomez JM, Santos JM, Camacho C. Comparison of intravenous flecainide, Martinez-Marcos FJ, Garcia-Garmendia JL, Ortega-Carpio A, Fernandez- Gomez JM, Santos JM, Camacho C. Comparison of intravenous flecainide, propafenone, and amiodarone for conversion of acute atrial fibrillation to sinus rhythm. propafenone, and amiodarone for conversion of acute atrial fibrillation to sinus rhythm. Am J CardiolAm J Cardiol 2000;86:950–953. 2000;86:950–953.
74.74. Chevalier P, Durand-Dubief A, Burri H, Cucherat M, Kirkorian G, Touboul P. Amiodarone versus placebo and class Ic drugs for cardioversion of recent-Chevalier P, Durand-Dubief A, Burri H, Cucherat M, Kirkorian G, Touboul P. Amiodarone versus placebo and class Ic drugs for cardioversion of recent-onset atrial fibrillation: a meta-analysis. onset atrial fibrillation: a meta-analysis. J Am Coll CardiolJ Am Coll Cardiol 2003;41:255–262. 2003;41:255–262.
75.75. Vardas PE, Kochiadakis GE, Igoumenidis NE, Tsatsakis AM, Simantirakis EN, Chlouverakis GI. Vardas PE, Kochiadakis GE, Igoumenidis NE, Tsatsakis AM, Simantirakis EN, Chlouverakis GI. Amiodarone as a first-choice drug for restoring sinus Amiodarone as a first-choice drug for restoring sinus rhythm in patients with atrial fibrillation: a randomized, controlled study. rhythm in patients with atrial fibrillation: a randomized, controlled study. ChestChest 2000;117:1538–1545. 2000;117:1538–1545.
76.76. Bianconi L, Castro A, Dinelli M, Alboni P, Pappalardo A, Richiardi E, Santini M. Comparison of intravenously administered dofetilide versus amiodarone Bianconi L, Castro A, Dinelli M, Alboni P, Pappalardo A, Richiardi E, Santini M. Comparison of intravenously administered dofetilide versus amiodarone in the acute termination of atrial fibrillation and flutter. A multicentre, randomized, double-blind, placebo-controlled study. in the acute termination of atrial fibrillation and flutter. A multicentre, randomized, double-blind, placebo-controlled study. Eur Heart JEur Heart J 2000;21:1265– 2000;21:1265–1273.1273.
77.77. Stambler BS, Wood MA, Ellenbogen KA. Antiarrhythmic actions of intravenous ibutilide compared with procainamide during human atrial flutter and Stambler BS, Wood MA, Ellenbogen KA. Antiarrhythmic actions of intravenous ibutilide compared with procainamide during human atrial flutter and fibrillation: electrophysiological determinants of enhanced conversion efficacy. fibrillation: electrophysiological determinants of enhanced conversion efficacy. CirculationCirculation 1997;96:4298–4306. 1997;96:4298–4306.
7070
78.78. Kirchhof P, Eckardt L, Loh P, Weber K, Fischer RJ, Seidl KH, Böcker D, Breithardt G, Haverkamp W, Borggrefe M. Anterior–posterior versus anterior–lateral electrode positions Kirchhof P, Eckardt L, Loh P, Weber K, Fischer RJ, Seidl KH, Böcker D, Breithardt G, Haverkamp W, Borggrefe M. Anterior–posterior versus anterior–lateral electrode positions for external cardioversion of atrial fibrillation: a randomised trial. for external cardioversion of atrial fibrillation: a randomised trial. LancetLancet 2002;360:1275–1279. 2002;360:1275–1279.
79.79. Oral H, Souza JJ, Michaud GF, Knight BP, Goyal R, Strickberger SA, Morady F. Facilitating transthoracic cardioversion of atrial fibrillation with ibutilide pretreatment. Oral H, Souza JJ, Michaud GF, Knight BP, Goyal R, Strickberger SA, Morady F. Facilitating transthoracic cardioversion of atrial fibrillation with ibutilide pretreatment. N Engl J N Engl J MedMed1999;340:1849–1854.1999;340:1849–1854.
80.80. Manios EG, Mavrakis HE, Kanoupakis EM, Kallergis EM, Dermitzaki DN, Kambouraki DC, Vardas PE. Manios EG, Mavrakis HE, Kanoupakis EM, Kallergis EM, Dermitzaki DN, Kambouraki DC, Vardas PE. Effects of amiodarone and diltiazem on persistent atrial fibrillation Effects of amiodarone and diltiazem on persistent atrial fibrillation conversion and recurrence rates: a randomized controlled study. conversion and recurrence rates: a randomized controlled study. Cardiovasc Drugs TherCardiovasc Drugs Ther 2003;17:31–39. 2003;17:31–39.
81.81. Bianconi L, Mennuni M, Lukic V, Castro A, Chieffi M, Santini M. Effects of oral propafenone administration before electrical cardioversion of chronic atrial fibrillation: a placebo-Bianconi L, Mennuni M, Lukic V, Castro A, Chieffi M, Santini M. Effects of oral propafenone administration before electrical cardioversion of chronic atrial fibrillation: a placebo-controlled study. controlled study. J Am Coll CardiolJ Am Coll Cardiol 1996;28:700–706. 1996;28:700–706.
82.82. Gulamhusein S, Ko P, Carruthers SG, Klein GJ. Acceleration of the ventricular response during atrial fibrillation in the Wolff–Parkinson–White syndrome after Gulamhusein S, Ko P, Carruthers SG, Klein GJ. Acceleration of the ventricular response during atrial fibrillation in the Wolff–Parkinson–White syndrome after verapamil. verapamil. CirculationCirculation1982;65:348–354.1982;65:348–354.
83.83. Fetsch T, Bauer P, Engberding R, Koch HP, Lukl J, Meinertz T, Oeff M, Seipel L, Trappe HJ, Treese N, Breithardt G. Prevention of atrial fibrillation after cardioversion: results of Fetsch T, Bauer P, Engberding R, Koch HP, Lukl J, Meinertz T, Oeff M, Seipel L, Trappe HJ, Treese N, Breithardt G. Prevention of atrial fibrillation after cardioversion: results of the PAFAC trial. the PAFAC trial. Eur Heart JEur Heart J 2004;25:1385–1394. 2004;25:1385–1394.
84.84. Cosio FG, Aliot E, Botto GL, Heidbuchel H, Geller CJ, Kirchhof P, De Haro JC, Frank R, Villacastin JP, Vijgen J, Crijns H. Delayed rhythm control of atrial fibrillation may be a cause Cosio FG, Aliot E, Botto GL, Heidbuchel H, Geller CJ, Kirchhof P, De Haro JC, Frank R, Villacastin JP, Vijgen J, Crijns H. Delayed rhythm control of atrial fibrillation may be a cause of failure to prevent recurrences: reasons for change to active antiarrhythmic treatment at the time of the first detected episode. of failure to prevent recurrences: reasons for change to active antiarrhythmic treatment at the time of the first detected episode. EuropaceEuropace 2008;10:21–27. 2008;10:21–27.
85.85. Kirchhof P. Can we improve outcomes in atrial fibrillation patients by early therapy? Kirchhof P. Can we improve outcomes in atrial fibrillation patients by early therapy? BMC MedBMC Med2009;7(72).2009;7(72).86.86. AFFIRM Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. AFFIRM Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J MedN Engl J Med 2002;347:1825–1833. 2002;347:1825–1833.87.87. Van Gelder IC, Hagens VE, Bosker HA, Kingma H, Kamp O, Kingma T, Said SA, Darmanata JI, Timmermanns AJM, Tijssen JGP, Crijns HJ. Van Gelder IC, Hagens VE, Bosker HA, Kingma H, Kamp O, Kingma T, Said SA, Darmanata JI, Timmermanns AJM, Tijssen JGP, Crijns HJ. A comparison of rate control and rhythm A comparison of rate control and rhythm
control in patients with recurrent persistent atrial fibrillation. control in patients with recurrent persistent atrial fibrillation. N Engl J MedN Engl J Med 2002;347:1834–1840. 2002;347:1834–1840.88.88. Carlsson J, Miketic S, Windeler J, Cuneo A, Haun S, Micus S, Walter S, Tebbe U; and the STAF Investigators. Randomized trial of rate-control versus rhythm-control in persistent Carlsson J, Miketic S, Windeler J, Cuneo A, Haun S, Micus S, Walter S, Tebbe U; and the STAF Investigators. Randomized trial of rate-control versus rhythm-control in persistent
atrial fibrillation. atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2003;41:1690–1696. 2003;41:1690–1696.89.89. Opolski G, Torbicki A, Kosior DA, Szulc M, Wozakowska-Kaplon B, Kolodziej P, Achremczyk P. Rate control vs rhythm control in patients with nonvalvular persistent atrial Opolski G, Torbicki A, Kosior DA, Szulc M, Wozakowska-Kaplon B, Kolodziej P, Achremczyk P. Rate control vs rhythm control in patients with nonvalvular persistent atrial
fibrillation: the results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFE) Study. fibrillation: the results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFE) Study. ChestChest2004;126:476–486.2004;126:476–486.90.90. Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, Bourassa MG, Arnold JM, Buxton AE, Camm AJ, Connolly SJ, Dubuc M, Ducharme A, Guerra PG, Hohnloser SH, Lambert J, Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, Bourassa MG, Arnold JM, Buxton AE, Camm AJ, Connolly SJ, Dubuc M, Ducharme A, Guerra PG, Hohnloser SH, Lambert J,
Le Heuzey JY, O'Hara G, Pedersen OD, Rouleau JL, Singh BN, Stevenson LW, Stevenson WG, Thibault B, Waldo AL. Le Heuzey JY, O'Hara G, Pedersen OD, Rouleau JL, Singh BN, Stevenson LW, Stevenson WG, Thibault B, Waldo AL. Rhythm control versus rate control for atrial fibrillation and Rhythm control versus rate control for atrial fibrillation and heart failure.heart failure.N Engl J MedN Engl J Med 2008;358:2667–2677. 2008;358:2667–2677.
91.91. Ogawa S, Yamashita T, Yamazaki T, Aizawa Y, Atarashi H, Inoue H, Ohe T, Ohtsu H, Okumura K, Katoh T, Kamakura S, Kumagai K, Kurachi Y, Kodama I, Koretsune Y, Saikawa Ogawa S, Yamashita T, Yamazaki T, Aizawa Y, Atarashi H, Inoue H, Ohe T, Ohtsu H, Okumura K, Katoh T, Kamakura S, Kumagai K, Kurachi Y, Kodama I, Koretsune Y, Saikawa T, Sakurai M, Sugi K, Tabuchi T, Nakaya H, Nakayama T, Hirai M, Fukatani M, Mitamura H. Optimal treatment strategy for patients with paroxysmal atrial fibrillation: J-RHYTHM T, Sakurai M, Sugi K, Tabuchi T, Nakaya H, Nakayama T, Hirai M, Fukatani M, Mitamura H. Optimal treatment strategy for patients with paroxysmal atrial fibrillation: J-RHYTHM Study. Study. Circ JCirc J2009;73:242–248.2009;73:242–248.
92.92. Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation—Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation—Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised trial. trial. LancetLancet2000;356:1789–1794.2000;356:1789–1794.
93.93. Hsu LF, Jais P, Sanders P, Garrigue S, Hocini M, Sacher F, Takahashi Y, Rotter M, Pasquie JL, Scavee C, Bordachar P, Clementy J, Haissaguerre M. Catheter ablation for atrial Hsu LF, Jais P, Sanders P, Garrigue S, Hocini M, Sacher F, Takahashi Y, Rotter M, Pasquie JL, Scavee C, Bordachar P, Clementy J, Haissaguerre M. Catheter ablation for atrial fibrillation in congestive heart failure. fibrillation in congestive heart failure. N Engl J MedN Engl J Med 2004;351:2373–2383. 2004;351:2373–2383.
94.94. Khan MN, Jais P, Cummings J, Di Biase L, Sanders P, Martin DO, Kautzner J, Hao S, Themistoclakis S, Fanelli R, Potenza D, Massaro R, Wazni O, Schweikert R, Saliba W, Wang P, Khan MN, Jais P, Cummings J, Di Biase L, Sanders P, Martin DO, Kautzner J, Hao S, Themistoclakis S, Fanelli R, Potenza D, Massaro R, Wazni O, Schweikert R, Saliba W, Wang P, Al-Ahmad A, Beheiry S, Santarelli P, Starling RC, Dello Russo A, Pelargonio G, Brachmann J, Schibgilla V, Bonso A, Casella M, Raviele A, Haissaguerre M, Natale A. Pulmonary-Al-Ahmad A, Beheiry S, Santarelli P, Starling RC, Dello Russo A, Pelargonio G, Brachmann J, Schibgilla V, Bonso A, Casella M, Raviele A, Haissaguerre M, Natale A. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. vein isolation for atrial fibrillation in patients with heart failure. N Engl J MedN Engl J Med 2008;359:1778–1785. 2008;359:1778–1785.
95.95. Hohnloser SH, Crijns HJ, van Eickels M, Gaudin C, Page RL, Torp-Pedersen C, Connolly SJ. Effect of dronedarone on cardiovascular events in atrial fibrillation. Hohnloser SH, Crijns HJ, van Eickels M, Gaudin C, Page RL, Torp-Pedersen C, Connolly SJ. Effect of dronedarone on cardiovascular events in atrial fibrillation. N Engl J N Engl J MedMed2009;360:668–678.2009;360:668–678.
96.96. Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, Reddy V, Augello G, Reynolds MR, Vinekar C, Liu CY, Berry SM, Berry Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, Reddy V, Augello G, Reynolds MR, Vinekar C, Liu CY, Berry SM, Berry DA. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled DA. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. trial. JAMAJAMA 2010;303:333–340. 2010;303:333–340.
97.97. Talajic M, Khairy P, Levesque S, Connolly SJ, Dorian P, Dubuc M, Guerra PG, Hohnloser SH, Lee KL, Macle L, Nattel S, Pedersen OD, Stevenson LW, Thibault B, Waldo AL, Wyse Talajic M, Khairy P, Levesque S, Connolly SJ, Dorian P, Dubuc M, Guerra PG, Hohnloser SH, Lee KL, Macle L, Nattel S, Pedersen OD, Stevenson LW, Thibault B, Waldo AL, Wyse DG, Roy D. Maintenance of sinus rhythm and survival in patients with heart failure and atrial fibrillation. DG, Roy D. Maintenance of sinus rhythm and survival in patients with heart failure and atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2010;55:1796–1802. 2010;55:1796–1802.
98.98. Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, Bergsma-Kadijk JA, Cornel JH, Kamp O, Tukkie R, Bosker HA, Van Veldhuisen DJ, Van den Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, Bergsma-Kadijk JA, Cornel JH, Kamp O, Tukkie R, Bosker HA, Van Veldhuisen DJ, Van den Berg MP. Berg MP. Lenient versus strict rate control in patients with atrial fibrillation. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J MedN Engl J Med2010;362:1363–1373.2010;362:1363–1373.
99.99. Singh BN, Connolly SJ, Crijns HJ, Roy D, Kowey PR, Capucci A, Radzik D, Aliot EM, Hohnloser SH. Singh BN, Connolly SJ, Crijns HJ, Roy D, Kowey PR, Capucci A, Radzik D, Aliot EM, Hohnloser SH. Dronedarone for maintenance of sinus rhythm in atrial fibrillation or flutter. Dronedarone for maintenance of sinus rhythm in atrial fibrillation or flutter. N N Engl J MedEngl J Med 2007;357:987–999. 2007;357:987–999.
100.100. Segal JB, McNamara RL, Miller MR, Kim N, Goodman SN, Powe NR, Robinson K, Yu D, Bass EB. The evidence regarding the drugs used for ventricular rate control. Segal JB, McNamara RL, Miller MR, Kim N, Goodman SN, Powe NR, Robinson K, Yu D, Bass EB. The evidence regarding the drugs used for ventricular rate control. J Fam J Fam PractPract2000;49:47–59.2000;49:47–59.
7171
101.101. Hou ZY, Chang MS, Chen CY, Tu MS, Lin SL, Chiang HT, Woosley RL. Acute treatment of recent-onset atrial fibrillation and flutter with a tailored dosing Hou ZY, Chang MS, Chen CY, Tu MS, Lin SL, Chiang HT, Woosley RL. Acute treatment of recent-onset atrial fibrillation and flutter with a tailored dosing regimen of intravenous amiodarone. regimen of intravenous amiodarone. A randomized, digoxin-controlled study. A randomized, digoxin-controlled study. Eur Heart JEur Heart J 1995;16:521–528. 1995;16:521–528.
102.102. Redfearn DP, Krahn AD, Skanes AC, Yee R, Klein GJ. Use of medications in Wolff–Parkinson–White syndrome. Redfearn DP, Krahn AD, Skanes AC, Yee R, Klein GJ. Use of medications in Wolff–Parkinson–White syndrome. Expert Opin PharmacotherExpert Opin Pharmacother 2005;6:955– 2005;6:955–963.963.
103.103. Davy JM, Herold M, Hoglund C, Timmermans A, Alings A, Radzik D, Van Kempen L. Dronedarone for the control of ventricular rate in permanent atrial Davy JM, Herold M, Hoglund C, Timmermans A, Alings A, Radzik D, Van Kempen L. Dronedarone for the control of ventricular rate in permanent atrial fibrillation: the Efficacy and safety of dRonedArone for the cOntrol of ventricular rate during atrial fibrillation (ERATO) study.fibrillation: the Efficacy and safety of dRonedArone for the cOntrol of ventricular rate during atrial fibrillation (ERATO) study.Am Heart Am Heart JJ 2008;156(527.e1–527.e9). 2008;156(527.e1–527.e9).
104.104. Murgatroyd FD, Gibson SM, Baiyan X, O'Nunain S, Poloniecki JD, Ward DE, Malik M, Camm AJ. Double-blind placebo-controlled trial of digoxin in Murgatroyd FD, Gibson SM, Baiyan X, O'Nunain S, Poloniecki JD, Ward DE, Malik M, Camm AJ. Double-blind placebo-controlled trial of digoxin in symptomatic paroxysmal atrial fibrillation. symptomatic paroxysmal atrial fibrillation. CirculationCirculation 1999;99:2765–2770. 1999;99:2765–2770.
105.105. Gasparini M, Auricchio A, Metra M, Regoli F, Fantoni C, Lamp B, Curnis A, Vogt J, Klersy C. Long-term survival in patients undergoing cardiac Gasparini M, Auricchio A, Metra M, Regoli F, Fantoni C, Lamp B, Curnis A, Vogt J, Klersy C. Long-term survival in patients undergoing cardiac resynchronization therapy: the importance of performing atrio-ventricular junction ablation in patients with permanent atrial fibrillation. resynchronization therapy: the importance of performing atrio-ventricular junction ablation in patients with permanent atrial fibrillation. Eur Heart Eur Heart JJ 2008;29:1644–1652. 2008;29:1644–1652.
106.106. Ozcan C, Jahangir A, Friedman PA, Patel PJ, Munger TM, Rea RF, Lloyd MA, Packer DL, Hodge DO, Gersh BJ, Hammill SC, Shen WK. Long-term survival Ozcan C, Jahangir A, Friedman PA, Patel PJ, Munger TM, Rea RF, Lloyd MA, Packer DL, Hodge DO, Gersh BJ, Hammill SC, Shen WK. Long-term survival after ablation of the atrioventricular node and implantation of a permanent pacemaker in patients with atrial fibrillation. after ablation of the atrioventricular node and implantation of a permanent pacemaker in patients with atrial fibrillation. N Engl J MedN Engl J Med 2001;344:1043– 2001;344:1043–1051.1051.
107.107. Weerasooriya R, Davis M, Powell A, Szili-Torok T, Shah C, Whalley D, Kanagaratnam L, Heddle W, Leitch J, Perks A, Ferguson L, Bulsara M. The Weerasooriya R, Davis M, Powell A, Szili-Torok T, Shah C, Whalley D, Kanagaratnam L, Heddle W, Leitch J, Perks A, Ferguson L, Bulsara M. The Australian intervention randomized control of rate in atrial fibrillation trial (AIRCRAFT). Australian intervention randomized control of rate in atrial fibrillation trial (AIRCRAFT). J Am Coll CardiolJ Am Coll Cardiol 2003;41:1697–1702. 2003;41:1697–1702.
108.108. Upadhyay GA, Choudhry NK, Auricchio A, Ruskin J, Singh JP. Upadhyay GA, Choudhry NK, Auricchio A, Ruskin J, Singh JP. Cardiac resynchronization in patients with atrial fibrillation: a meta-analysis of Cardiac resynchronization in patients with atrial fibrillation: a meta-analysis of prospective cohort studies. prospective cohort studies. J Am Coll CardiolJ Am Coll Cardiol2008;52:1239–1246.2008;52:1239–1246.
109.109. Auricchio A, Metra M, Gasparini M, Lamp B, Klersy C, Curnis A, Fantoni C, Gronda E, Vogt J. Long-term survival of patients with heart failure and Auricchio A, Metra M, Gasparini M, Lamp B, Klersy C, Curnis A, Fantoni C, Gronda E, Vogt J. Long-term survival of patients with heart failure and ventricular conduction delay treated with cardiac resynchronization therapy. ventricular conduction delay treated with cardiac resynchronization therapy. Am J CardiolAm J Cardiol 2007;99:232–238. 2007;99:232–238.
110.110. Dong K, Shen WK, Powell BD, Dong YX, Rea RF, Friedman PA, Hodge DO, Wiste HJ, Webster T, Hayes DL, Cha YM. Atrioventricular nodal ablation Dong K, Shen WK, Powell BD, Dong YX, Rea RF, Friedman PA, Hodge DO, Wiste HJ, Webster T, Hayes DL, Cha YM. Atrioventricular nodal ablation predicts survival benefit in patients with atrial fibrillation receiving cardiac resynchronization therapy. predicts survival benefit in patients with atrial fibrillation receiving cardiac resynchronization therapy. Heart RhythmHeart Rhythm 2010. 2010.
111.111. Lafuente-Lafuente C, Mouly S, Longas-Tejero MA, Bergmann JF. Lafuente-Lafuente C, Mouly S, Longas-Tejero MA, Bergmann JF. Antiarrhythmics for maintaining sinus rhythm after cardioversion of atrial Antiarrhythmics for maintaining sinus rhythm after cardioversion of atrial fibrillation. fibrillation. Cochrane Database Syst RevCochrane Database Syst Rev2007;4.2007;4.
112.112. McNamara RL, Bass EB, Miller MR, Segal JB, Goodman SN, Kim NL, Robinson KA, Powe NR. Management of new onset atrial fibrillation (evidence McNamara RL, Bass EB, Miller MR, Segal JB, Goodman SN, Kim NL, Robinson KA, Powe NR. Management of new onset atrial fibrillation (evidence report/Technology assessment).report/Technology assessment).Agency for Heathcare Research and QualityAgency for Heathcare Research and Quality 2001. 2001.
113.113. Connolly SJ. Evidence-based analysis of amiodarone efficacy and safety. Connolly SJ. Evidence-based analysis of amiodarone efficacy and safety. CirculationCirculation1999;100:2025–2034.1999;100:2025–2034.114.114. Kirchhof P, Franz MR, Bardai A, Wilde AM. Giant T–U waves precede torsades de pointes in long QT syndrome. A systematic electrocardiographic Kirchhof P, Franz MR, Bardai A, Wilde AM. Giant T–U waves precede torsades de pointes in long QT syndrome. A systematic electrocardiographic
analysis in patients with acquired and congenital QT prolongation. analysis in patients with acquired and congenital QT prolongation. J Am Coll CardiolJ Am Coll Cardiol 2009;54:143–149. 2009;54:143–149.115.115. Kääb S, Hinterseer M, Näbauer M, Steinbeck G. Sotalol testing unmasks altered repolarization in patients with suspected acquired long-QT-syndrome-Kääb S, Hinterseer M, Näbauer M, Steinbeck G. Sotalol testing unmasks altered repolarization in patients with suspected acquired long-QT-syndrome-
a case-control pilot study using i.v. sotalol. a case-control pilot study using i.v. sotalol. Eur Heart JEur Heart J 2003;24:649–657. 2003;24:649–657.116.116. Le Heuzey J, De Ferrari GM, Radzik D, Santini M, Zhu J, Davy JM. Le Heuzey J, De Ferrari GM, Radzik D, Santini M, Zhu J, Davy JM. A short-term, randomized, double-blind, parallel-group study to evaluate the efficacy A short-term, randomized, double-blind, parallel-group study to evaluate the efficacy
and safety of dronedarone versus amiodarone in patients with persistent atrial fibrillation: the DIONYSOS study. and safety of dronedarone versus amiodarone in patients with persistent atrial fibrillation: the DIONYSOS study. J Cardiovasc J Cardiovasc ElectrophysiolElectrophysiol 2010;21:597–605. 2010;21:597–605.
117.117. Kober L, Torp-Pedersen C, McMurray JJ, Gotzsche O, Levy S, Crijns H, Amlie J, Carlsen J. Increased mortality after dronedarone therapy for severe Kober L, Torp-Pedersen C, McMurray JJ, Gotzsche O, Levy S, Crijns H, Amlie J, Carlsen J. Increased mortality after dronedarone therapy for severe heart failure. heart failure. N Engl J MedN Engl J Med2008;358:2678–2687.2008;358:2678–2687.
118.118. Karlson BW, Torstensson I, Abjorn C, Jansson SO, Peterson LE. Disopyramide in the maintenance of sinus rhythm after electroconversion of atrial Karlson BW, Torstensson I, Abjorn C, Jansson SO, Peterson LE. Disopyramide in the maintenance of sinus rhythm after electroconversion of atrial fibrillation. A placebo-controlled one-year follow-up study. fibrillation. A placebo-controlled one-year follow-up study. Eur Heart JEur Heart J 1988;9:284–290. 1988;9:284–290.
119.119. Crijns HJ, Gosselink AT, Lie KI. Propafenone versus disopyramide for maintenance of sinus rhythm after electrical cardioversion of chronic atrial Crijns HJ, Gosselink AT, Lie KI. Propafenone versus disopyramide for maintenance of sinus rhythm after electrical cardioversion of chronic atrial fibrillation: a randomized, double-blind study. fibrillation: a randomized, double-blind study. PRODIS Study Group. PRODIS Study Group. Cardiovasc Drugs TherCardiovasc Drugs Ther 1996;10:145–152. 1996;10:145–152.
120.120. Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl N Engl J MedJ Med 2005;352:225–237 2005;352:225–237
7272
121.121. Piccini JP, Hasselblad V, Peterson ED, Washam JB, Califf RM, Kong DF. Comparative efficacy of dronedarone and amiodarone for the maintenance of Piccini JP, Hasselblad V, Peterson ED, Washam JB, Califf RM, Kong DF. Comparative efficacy of dronedarone and amiodarone for the maintenance of sinus rhythm in patients with atrial fibrillation. sinus rhythm in patients with atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2009;54:1089–1095. 2009;54:1089–1095.
122.122. Singh D, Cingolani E, Diamon GA, Kaul S. Dronedarone for atrial fibrillation: have we expanded the antiarrhythmic armamentarium. Singh D, Cingolani E, Diamon GA, Kaul S. Dronedarone for atrial fibrillation: have we expanded the antiarrhythmic armamentarium. J Am Coll J Am Coll CardiolCardiol 2010;55:1569–1576. 2010;55:1569–1576.
123.123. Freemantle N, Mitchell S, Orme M, Eckert L, Reynolds MR. Morbidity and mortality associated with anti-arrhythmic drugs in atrial fibrillation: a Freemantle N, Mitchell S, Orme M, Eckert L, Reynolds MR. Morbidity and mortality associated with anti-arrhythmic drugs in atrial fibrillation: a systematic review and mixed treatment meta-analysis (abstract). systematic review and mixed treatment meta-analysis (abstract). CirculationCirculation 2009;120:S691–S692. 2009;120:S691–S692.
124.124. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, Huther ML, Richardson DW; Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, Huther ML, Richardson DW; Investigators and the CAST investigators. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. Investigators and the CAST investigators. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia The Cardiac Arrhythmia Suppression Trial. Suppression Trial. N Engl J MedN Engl J Med 1991;324:781–788. 1991;324:781–788.
125.125. Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T, Lambert J, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone to prevent Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T, Lambert J, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone to prevent recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. N Engl J MedN Engl J Med 2000;342:913–920. 2000;342:913–920.
126.126. Singh SN, Fletcher RD, Fisher SG, Singh BN, Lewis HD, Deedwania PC, Massie BM, Colling C, Lazzeri D. Amiodarone in patients with congestive heart Singh SN, Fletcher RD, Fisher SG, Singh BN, Lewis HD, Deedwania PC, Massie BM, Colling C, Lazzeri D. Amiodarone in patients with congestive heart failure and asymptomatic ventricular arrhythmia. Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure. failure and asymptomatic ventricular arrhythmia. Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure. N Engl J MedN Engl J Med 1995;333:77–82. 1995;333:77–82.
127.127. Van Gelder IC, Crijns HJ, Van Gilst WH, Van Wijk LM, Hamer HP, Lie KI. Efficacy and safety of flecainide acetate in the maintenance of sinus rhythm Van Gelder IC, Crijns HJ, Van Gilst WH, Van Wijk LM, Hamer HP, Lie KI. Efficacy and safety of flecainide acetate in the maintenance of sinus rhythm after electrical cardioversion of chronic atrial fibrillation or atrial flutter. after electrical cardioversion of chronic atrial fibrillation or atrial flutter. Am J CardiolAm J Cardiol 1989;64:1317–1321. 1989;64:1317–1321.
128.128. Shah AN, Mittal S, Sichrovsky TC, Cotiga D, Arshad A, Maleki K, Pierce WJ, Steinberg JS. Long-term outcome following successful pulmonary vein Shah AN, Mittal S, Sichrovsky TC, Cotiga D, Arshad A, Maleki K, Pierce WJ, Steinberg JS. Long-term outcome following successful pulmonary vein isolation: pattern and prediction of very late recurrence. isolation: pattern and prediction of very late recurrence. J Cardiovasc ElectrophysiolJ Cardiovasc Electrophysiol 2008;19:661–667. 2008;19:661–667.
129.129. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. safety of catheter ablation for human atrial fibrillation. CirculationCirculation 2005;111:1100–1105. 2005;111:1100–1105.
130.130. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, Skanes A. Prevalence and causes of fatal outcome Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, Skanes A. Prevalence and causes of fatal outcome in catheter ablation of atrial fibrillation. in catheter ablation of atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2009;53:1798–1803. 2009;53:1798–1803.
131.131. Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Treatment of atrial fibrillation with antiarrhythmic drugs or Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm ElectrophysiolCirc Arrhythm Electrophysiol 2009;2:349–361. 2009;2:349–361.
132.132. Noheria A, Kumar A, Wylie JV Jr., Josephson ME. Catheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic review. Noheria A, Kumar A, Wylie JV Jr., Josephson ME. Catheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic review. Arch Arch Intern MedIntern Med 2008;168:581–586. 2008;168:581–586.
133.133. Jais P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, Klein G, Weerasooriya R, Clementy J, Jais P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, Klein G, Weerasooriya R, Clementy J, Haissaguerre M. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Haissaguerre M. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. CirculationCirculation2008;118:2498–2505.2008;118:2498–2505.
134.134. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Potenza D, Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Potenza D, Fanelli R, Raviele A, Themistoclakis S, Rossillo A, Bonso A, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of Fanelli R, Raviele A, Themistoclakis S, Rossillo A, Bonso A, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. symptomatic atrial fibrillation: a randomized trial. JAMAJAMA2005;293:2634–2640.2005;293:2634–2640.
135.135. Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L, Pappone N, Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L, Pappone N, Radinovic A, Manguso F, Santinelli V. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal Radinovic A, Manguso F, Santinelli V. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF Study. atrial fibrillation: the APAF Study. J Am Coll CardiolJ Am Coll Cardiol 2006;48:2340–2347. 2006;48:2340–2347.
136.136. Blanc JJ, Almendral J, Brignole M, Fatemi M, Gjesdal K, Gonzalez-Torrecilla E, Kulakowski P, Lip GY, Shah D, Wolpert C. Consensus document on Blanc JJ, Almendral J, Brignole M, Fatemi M, Gjesdal K, Gonzalez-Torrecilla E, Kulakowski P, Lip GY, Shah D, Wolpert C. Consensus document on antithrombotic therapy in the setting of electrophysiological procedures. antithrombotic therapy in the setting of electrophysiological procedures. EuropaceEuropace 2008;10:513–527. 2008;10:513–527.
137.137. Piccini JP, Lopes RD, Kong MH, Hasselblad V, Jackson K, Al-Khatib SM. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with Piccini JP, Lopes RD, Kong MH, Hasselblad V, Jackson K, Al-Khatib SM. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with atrial fibrillation: a meta-analysis of randomized, controlled trials. atrial fibrillation: a meta-analysis of randomized, controlled trials. Circ Arrhythm ElectrophysiolCirc Arrhythm Electrophysiol 2009;2:626–633. 2009;2:626–633.
138.138. Nair GM, Nery PB, Diwakaramenon S, Healey JS, Connolly SJ, Morillo CA. A systematic review of randomized trials comparing radiofrequency ablation Nair GM, Nery PB, Diwakaramenon S, Healey JS, Connolly SJ, Morillo CA. A systematic review of randomized trials comparing radiofrequency ablation with antiarrhythmic medications in patients with atrial fibrillation. with antiarrhythmic medications in patients with atrial fibrillation. J Cardiovasc ElectrophysiolJ Cardiovasc Electrophysiol 2009;20:138–144. 2009;20:138–144.
139.139. Ngaage DL, Schaff HV, Mullany CJ, Barnes S, Dearani JA, Daly RC, Orszulak TA, Sundt TM 3rd.. Influence of preoperative atrial fibrillation on late Ngaage DL, Schaff HV, Mullany CJ, Barnes S, Dearani JA, Daly RC, Orszulak TA, Sundt TM 3rd.. Influence of preoperative atrial fibrillation on late results of mitral repair: is concomitant ablation justified? results of mitral repair: is concomitant ablation justified? Ann Thorac SurgAnn Thorac Surg 2007;84:434–442. 2007;84:434–442.
140.140. Gaita F, Riccardi R, Caponi D, Shah D, Garberoglio L, Vivalda L, Dulio A, Chiecchio A, Manasse E, Gallotti R. Linear cryoablation of the left atrium Gaita F, Riccardi R, Caponi D, Shah D, Garberoglio L, Vivalda L, Dulio A, Chiecchio A, Manasse E, Gallotti R. Linear cryoablation of the left atrium versus pulmonary vein cryoisolation in patients with permanent atrial fibrillation and valvular heart disease: correlation of electroanatomic mapping versus pulmonary vein cryoisolation in patients with permanent atrial fibrillation and valvular heart disease: correlation of electroanatomic mapping and long-term clinical results. and long-term clinical results. CirculationCirculation 2005;111:136–142. 2005;111:136–142.

7373
141.141. Piccini JP, Hasselblad V, Peterson ED, Washam JB, Califf RM, Kong DF. Comparative efficacy of dronedarone and amiodarone for the maintenance Piccini JP, Hasselblad V, Peterson ED, Washam JB, Califf RM, Kong DF. Comparative efficacy of dronedarone and amiodarone for the maintenance of sinus rhythm in patients with atrial fibrillation. of sinus rhythm in patients with atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2009;54:1089–1095. 2009;54:1089–1095.
142.142. Singh D, Cingolani E, Diamon GA, Kaul S. Dronedarone for atrial fibrillation: have we expanded the antiarrhythmic armamentarium. Singh D, Cingolani E, Diamon GA, Kaul S. Dronedarone for atrial fibrillation: have we expanded the antiarrhythmic armamentarium. J Am Coll J Am Coll CardiolCardiol 2010;55:1569–1576. 2010;55:1569–1576.
143.143. Freemantle N, Mitchell S, Orme M, Eckert L, Reynolds MR. Morbidity and mortality associated with anti-arrhythmic drugs in atrial fibrillation: a Freemantle N, Mitchell S, Orme M, Eckert L, Reynolds MR. Morbidity and mortality associated with anti-arrhythmic drugs in atrial fibrillation: a systematic review and mixed treatment meta-analysis (abstract). systematic review and mixed treatment meta-analysis (abstract). CirculationCirculation 2009;120:S691–S692. 2009;120:S691–S692.
144.144. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, Huther ML, Richardson Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, Barker AH, Arensberg D, Baker A, Friedman L, Greene HL, Huther ML, Richardson DW; Investigators and the CAST investigators. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. DW; Investigators and the CAST investigators. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac The Cardiac Arrhythmia Suppression Trial. Arrhythmia Suppression Trial. N Engl J MedN Engl J Med 1991;324:781–788. 1991;324:781–788.
145.145. Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T, Lambert J, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone to prevent Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T, Lambert J, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone to prevent recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. N Engl J MedN Engl J Med 2000;342:913–920. 2000;342:913–920.
146.146. Singh SN, Fletcher RD, Fisher SG, Singh BN, Lewis HD, Deedwania PC, Massie BM, Colling C, Lazzeri D. Amiodarone in patients with congestive Singh SN, Fletcher RD, Fisher SG, Singh BN, Lewis HD, Deedwania PC, Massie BM, Colling C, Lazzeri D. Amiodarone in patients with congestive heart failure and asymptomatic ventricular arrhythmia. Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure. heart failure and asymptomatic ventricular arrhythmia. Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure. N Engl J N Engl J MedMed 1995;333:77–82. 1995;333:77–82.
147.147. Van Gelder IC, Crijns HJ, Van Gilst WH, Van Wijk LM, Hamer HP, Lie KI. Efficacy and safety of flecainide acetate in the maintenance of sinus Van Gelder IC, Crijns HJ, Van Gilst WH, Van Wijk LM, Hamer HP, Lie KI. Efficacy and safety of flecainide acetate in the maintenance of sinus rhythm after electrical cardioversion of chronic atrial fibrillation or atrial flutter. rhythm after electrical cardioversion of chronic atrial fibrillation or atrial flutter. Am J CardiolAm J Cardiol 1989;64:1317–1321. 1989;64:1317–1321.
148.148. Shah AN, Mittal S, Sichrovsky TC, Cotiga D, Arshad A, Maleki K, Pierce WJ, Steinberg JS. Long-term outcome following successful pulmonary vein Shah AN, Mittal S, Sichrovsky TC, Cotiga D, Arshad A, Maleki K, Pierce WJ, Steinberg JS. Long-term outcome following successful pulmonary vein isolation: pattern and prediction of very late recurrence. isolation: pattern and prediction of very late recurrence. J Cardiovasc ElectrophysiolJ Cardiovasc Electrophysiol 2008;19:661–667. 2008;19:661–667.
149.149. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Packer D, Skanes A. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. and safety of catheter ablation for human atrial fibrillation. CirculationCirculation 2005;111:1100–1105. 2005;111:1100–1105.
150.150. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, Skanes A. Prevalence and causes of fatal Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, Kim YH, Klein G, Natale A, Packer D, Skanes A. Prevalence and causes of fatal outcome in catheter ablation of atrial fibrillation. outcome in catheter ablation of atrial fibrillation. J Am Coll CardiolJ Am Coll Cardiol 2009;53:1798–1803. 2009;53:1798–1803.
151.151. Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Treatment of atrial fibrillation with antiarrhythmic drugs or Calkins H, Reynolds MR, Spector P, Sondhi M, Xu Y, Martin A, Williams CJ, Sledge I. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm ElectrophysiolCirc Arrhythm Electrophysiol 2009;2:349–361. 2009;2:349–361.
152.152. Noheria A, Kumar A, Wylie JV Jr., Josephson ME. Catheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic review. Noheria A, Kumar A, Wylie JV Jr., Josephson ME. Catheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic review. Arch Arch Intern MedIntern Med 2008;168:581–586. 2008;168:581–586.
153.153. Jais P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, Klein G, Weerasooriya R, Clementy J, Jais P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, Klein G, Weerasooriya R, Clementy J, Haissaguerre M. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Haissaguerre M. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. CirculationCirculation2008;118:2498–2505.2008;118:2498–2505.
154.154. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K, Pisano E, Potenza D, Fanelli R, Raviele A, Themistoclakis S, Rossillo A, Bonso A, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line Potenza D, Fanelli R, Raviele A, Themistoclakis S, Rossillo A, Bonso A, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. treatment of symptomatic atrial fibrillation: a randomized trial. JAMAJAMA2005;293:2634–2640.2005;293:2634–2640.
155.155. Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L, Pappone N, Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A, LiVolsi L, Pappone N, Radinovic A, Manguso F, Santinelli V. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in Radinovic A, Manguso F, Santinelli V. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF Study. paroxysmal atrial fibrillation: the APAF Study. J Am Coll CardiolJ Am Coll Cardiol 2006;48:2340–2347. 2006;48:2340–2347.
156.156. Blanc JJ, Almendral J, Brignole M, Fatemi M, Gjesdal K, Gonzalez-Torrecilla E, Kulakowski P, Lip GY, Shah D, Wolpert C. Consensus document on Blanc JJ, Almendral J, Brignole M, Fatemi M, Gjesdal K, Gonzalez-Torrecilla E, Kulakowski P, Lip GY, Shah D, Wolpert C. Consensus document on antithrombotic therapy in the setting of electrophysiological procedures. antithrombotic therapy in the setting of electrophysiological procedures. EuropaceEuropace 2008;10:513–527. 2008;10:513–527.
157.157. Piccini JP, Lopes RD, Kong MH, Hasselblad V, Jackson K, Al-Khatib SM. Pulmonary vein isolation for the maintenance of sinus rhythm in patients Piccini JP, Lopes RD, Kong MH, Hasselblad V, Jackson K, Al-Khatib SM. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with atrial fibrillation: a meta-analysis of randomized, controlled trials. with atrial fibrillation: a meta-analysis of randomized, controlled trials. Circ Arrhythm ElectrophysiolCirc Arrhythm Electrophysiol 2009;2:626–633. 2009;2:626–633.
158.158. Nair GM, Nery PB, Diwakaramenon S, Healey JS, Connolly SJ, Morillo CA. A systematic review of randomized trials comparing radiofrequency Nair GM, Nery PB, Diwakaramenon S, Healey JS, Connolly SJ, Morillo CA. A systematic review of randomized trials comparing radiofrequency ablation with antiarrhythmic medications in patients with atrial fibrillation. ablation with antiarrhythmic medications in patients with atrial fibrillation. J Cardiovasc ElectrophysiolJ Cardiovasc Electrophysiol 2009;20:138–144. 2009;20:138–144.
7474
Algunos Ejemplos de Algunos Ejemplos de SUBDIAGNÓSTICOSUBDIAGNÓSTICO

7575
TAKOSUBOTAKOSUBOLa presentación típica de una persona La presentación típica de una persona
con miocardiopatía de takotsubo es con miocardiopatía de takotsubo es una aparición repentina de una aparición repentina de
• IInsuficiencia nsuficiencia cardíacacardíaca congestivacongestiva • Y/o Y/o dolordolor torácicotorácico . .• Alteraciones en el ECG que sugierenAlteraciones en el ECG que sugierenun un infartoinfarto agudo de agudo de miocardiomiocardio de dela la paredpared anterior anterior. .

7676
Imagen típica de TakosuboImagen típica de Takosubo
7777
Se trata de un varón con dicho Se trata de un varón con dicho diagnóstico.diagnóstico.
El diagnóstico es completo???El diagnóstico es completo???
Si observamos y medimos Si observamos y medimos detenidamente, valoraremos:detenidamente, valoraremos:
PR-interval muy Corto: 0.107-0.110 PR-interval muy Corto: 0.107-0.110 seg.seg.
QTcB-interval Largo: 0.479 seg.QTcB-interval Largo: 0.479 seg.
7878
WELLENS’ SYNDROMEWELLENS’ SYNDROMEWellens síndrome fue descrito por primera vez de Wellens síndrome fue descrito por primera vez de
Zwaan, Wellens, y sus colegas en la década de Zwaan, Wellens, y sus colegas en la década de 1980 cuando se dieron cuenta de un subconjunto 1980 cuando se dieron cuenta de un subconjunto de pacientes con angina inestable que tenian de pacientes con angina inestable que tenian cambios específicos de la onda T en cambios específicos de la onda T en precordiales y, posteriormente,desarrollaron precordiales y, posteriormente,desarrollaron una gran infarto de miocardio en la pared anterior una gran infarto de miocardio en la pared anterior del ventriculo.del ventriculo.
Síndrome Wellens se refiere a estas Síndrome Wellens se refiere a estas anormalidades electrocardiográficas específicas danormalidades electrocardiográficas específicas de la onda T precordial del segmento, que se e la onda T precordial del segmento, que se asocian con asocian con estenosis crítica de estenosis crítica de la descendente anterior izquierda la descendente anterior izquierda proximal (LAD) arteria coronaria. proximal (LAD) arteria coronaria.
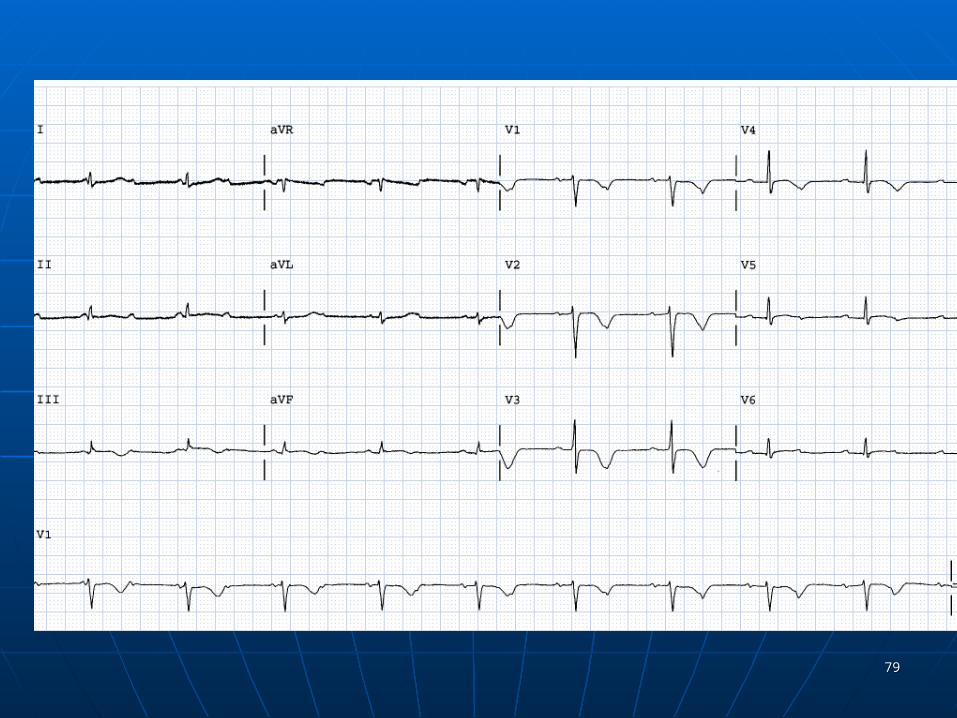
7979
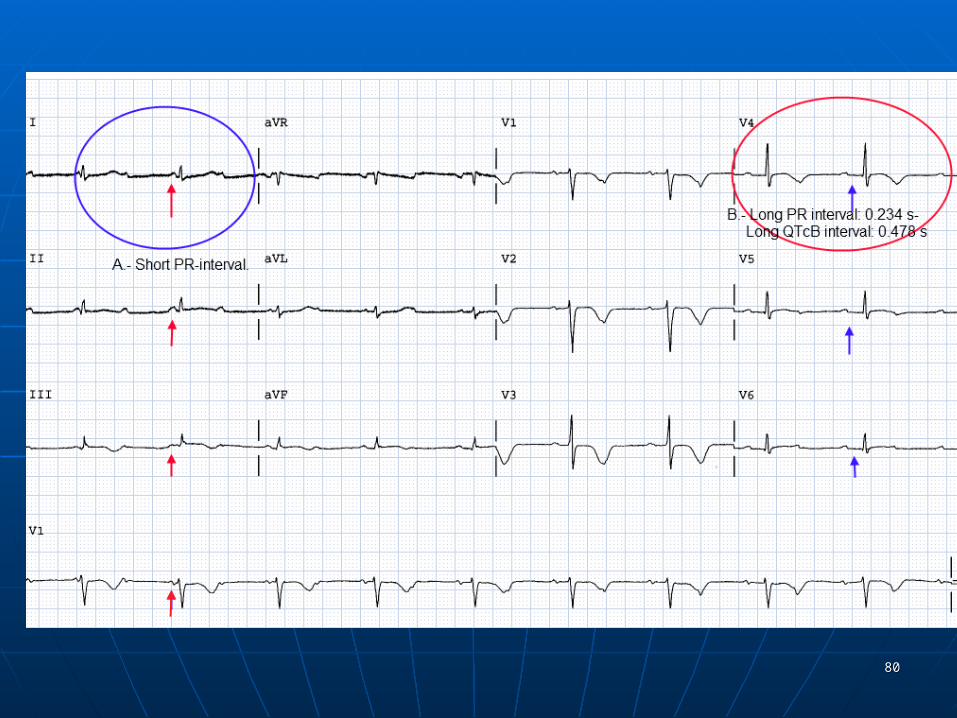
8080
8181
WOLFF-PARKINSON- WHITE.WOLFF-PARKINSON- WHITE.
Síndrome de preexcitación de los Síndrome de preexcitación de los ventrículosventrículos del del corazóncorazón debido a una vía accesoria debido a una vía accesoria conocida como conocida como hazhaz de de KentKent. Esta vía es una . Esta vía es una comunicación eléctrica anormal de la comunicación eléctrica anormal de la aurículaaurícula al ventrículo. al ventrículo.
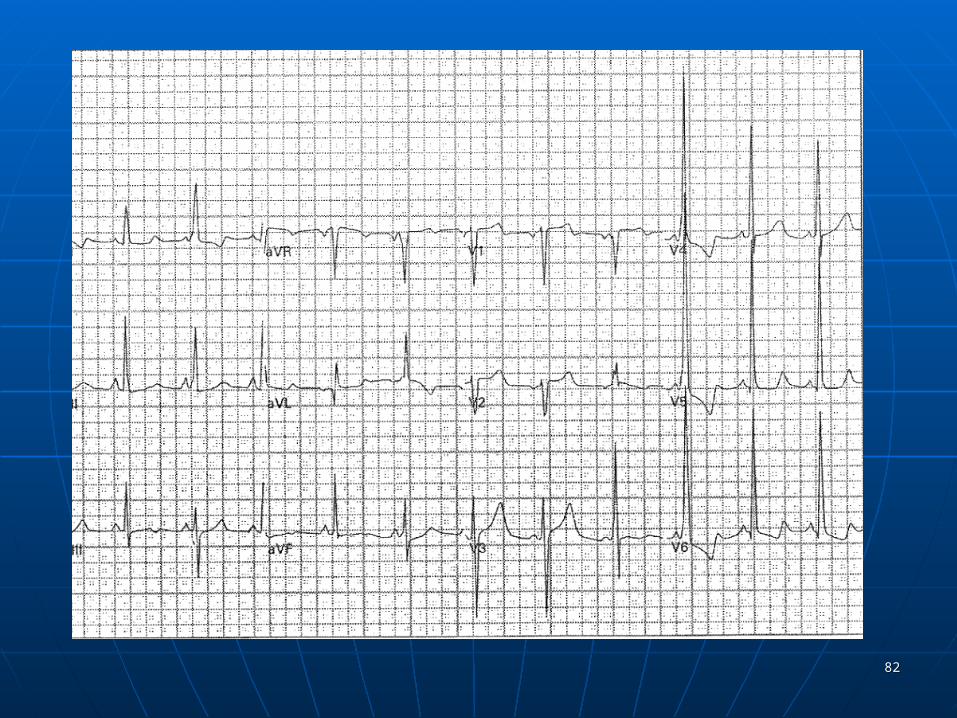
8282

8383
Además de los signos típicos de WPW Además de los signos típicos de WPW es obvia la presencia de un QTc es obvia la presencia de un QTc Largo.Largo.