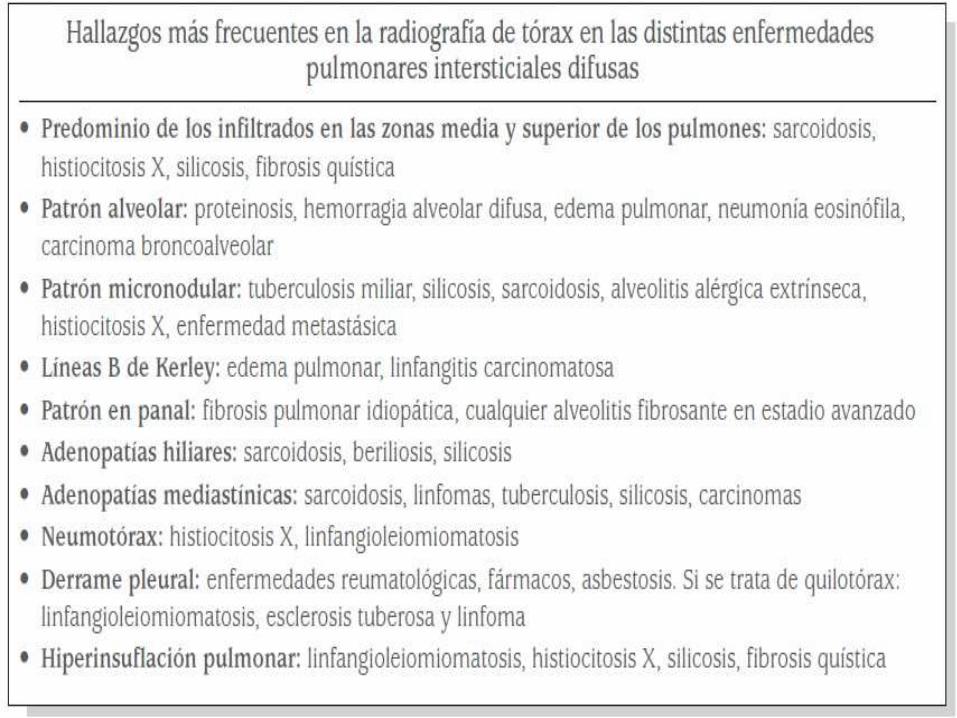
Lesiones intersticiales
60
Lesiones Intersticiales Radiología Ramos R1MF
-
Upload
anell-ramos -
Category
Economy & Finance
-
view
1.618 -
download
2
Transcript of Lesiones intersticiales

Lesiones IntersticialesRadiología
Ramos R1MF

ENFERMEDADES INTERSTICIALES PULMONARES
DEFINICIÓN
Conjunto de afecciones con manifestaciones clínicas, radiológicas y funcionales respiratorias similares, en las que las principales alteraciones anatomopatológicas afectan a las estructuras alveolointersticiales.
Generalidades:







PRONÓSTICO
El pronóstico es muy variable, en dependencia de la enfermedad que el paciente presente. Dentro de las enfermedades mas frecuentes como puedan ser la fibrosis pulmonar idiopática o la sarcoidosis, podemos encontrar un claro ejemplo de esta discordancia, ya el pronóstico es excelente en la sarcoidosis y decepcionante en la fibrosis pulmonar idiopática.
TRATAMIENTO
En general la mayoría de estas enfermedades se tratan con corticoides a dosis de 0,5-1 mg/Kg/d durante 4-8 semanas, continuando con una dosis de mantenimiento de 0,125-0,25 mg/Kg/7d. Si no hay respuesta se asocian inmunosupresores (azatioprina, ciclofosfamida) aunque en algunas enfermedades, estos ya se asocian de entrada.

Fibrosis Pulmonar IdiopaticaRADIOLOGÍALa radiografía de tórax convencional (RT) muestra típicamente un patrón intersticial oinfiltrados reticulonodulares de distribución bibasal y periférica (subpleural). La mayoríade los pacientes presentan una RT anormal en el momento del diagnóstico.







OTRAS NEUMONÍAS INTERSTICIALES IDIOPÁTICAS (NII)

Neumonía Intersticial Aguda NIA
Vidrio deslustrado,Aparición progresiva.
La radiografía de tórax muestra infiltradosalveolares bilaterales y el TACAR muestra desdeimágenes en “vidrio deslustrado” a consolidaciónconfluente y difusa de los espacios.En las fases proliferativa y fibrótica,pueden aparecer imágenes de bronquiectasiasde tracción y panalización pulmonar.

Neumonía Intersticial No especifica NINE
Muestran generalmente una ausencia de panalización, predominando las imágenes de opacidades en “vidrio deslustrado”,generalmente bilaterales, con una distribución subpleural y asociadas a pérdidade volumen de los lóbulos inferiores. Tambiénpueden estar presentes imágenes reticulares,de distribución simétrica y basal

Neumonía Intersticial Descamativa NID
predominan las imágenes difusasde atenuación en
“vidrio deslustrado”
aunquepuede haber
engrosamiento difuso de los
septos alveolares con líneas reticulares.20% normal
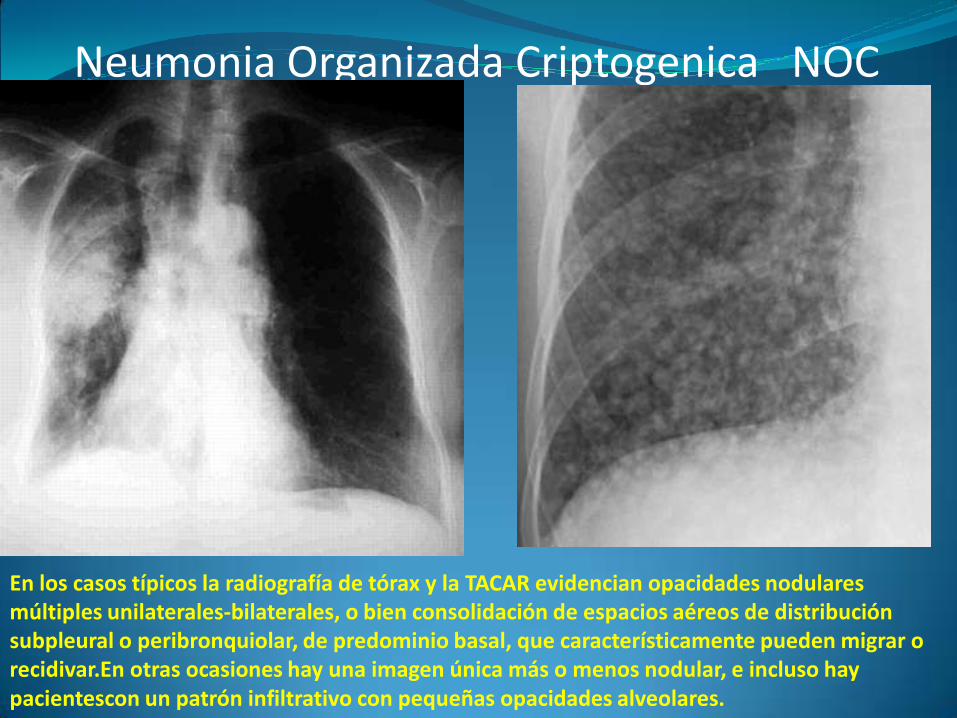
Neumonia Organizada Criptogenica NOC
En los casos típicos la radiografía de tórax y la TACAR evidencian opacidades nodulares múltiples unilaterales-bilaterales, o bien consolidación de espacios aéreos de distribución subpleural o peribronquiolar, de predominio basal, que característicamente pueden migrar o recidivar.En otras ocasiones hay una imagen única más o menos nodular, e incluso hay pacientescon un patrón infiltrativo con pequeñas opacidades alveolares.

Neumonia Intersticial Linfocitica NIL
La radiografía de tórax y la TACAR muestranimágenes en vidrio deslustrado, aunquepueden observarse imágenes reticulares ynodulares-micronodulares difusas.

ENFERMEDAD PULMONAR INTERSTICIAL ASOCIADA A TRASTORNOS DEL TEJIDO CONECTIVO.

Artritis Reumatoide
Los hallazgos radiológicos son similares ala neumonía intersticial usual (NIU), incluyendoengrosamiento de septos interlobulillares,opacidades irregulares reticulares, vidriodeslustrado,panalización, bronquiectasias portracción y bronquioloectasias


Rheumatoid arthritis with thoracic bone changes. Posteroanterior radiograph shows resorption of the distal clavicles and humeral heads.
Rheumatoid arthritis with pulmonaryfibrosis and lung cancer. Posteroanteriorradiograph shows bilateral peripheral areasof coarse reticulation and an irregular lungmass in the left upper lobe. The diagnosis of lung cancer was proved at surgery.

Lupus Eritematoso sistemico

Hemorragia Pulmonar

Hipertension Pulmonar

Tromboembolia Pulmonar

opacidad triangular con base pleural (“joroba deHampton”), ascenso hemidiafragma, derrame pleural de escasa cuantía, oligohemia periférica yatelectasias subsegmentarias.
TromboemboliaPulmonar

Systemic lupus erythematosus withdiaphragmatic dysfunction. Posteroanteriorradiograph shows decreased lung volumesrelated to diaphragmatic dysfunction and bibasilar atelectasis.
Systemic lupus erythematosus with tumoral calcinosis. Posteroanterior radiograph of a patient with systemic lupus erythematosusand renal failure shows a large amorphoussoft-tissue calcification projecting into theright supraclavicular region and right axilla.

Systemic lupus erythematosus with lupus pneumonitis. Posteroanterior radiograph shows patchy bilateral areas of air-space consolidation.
La radiología muestra generalmente afectación alveolar bilateral, más frecuente en bases pulmonares. Se asocia derrame pleural en el 50% de los pacientes(21). Estos hallazgos son inespecíficos y pueden ser indistinguibles de otras causas de infiltrados pulmonares enpacientes con LES, como infección, edema o hemorragia.

Esclerosis Sistemica
derrame pleuralneumonía aspirativaneumotórax espontáneobronquiectasiasneumonitis secundariaa toxicidad porfármacos y cáncer pulmonar

Esclerosis Sistemica
Los hallazgos radiológicos pueden incluir: osteopenia, acroosteolisis (p.ej.: falanges distales), calcinosis. En el tórax: fibrosis intersticial pulmonar (nodular o lineal) en las dos terceras partes inferiores de los campos pulmonares; en casos avanzados puede observarse una imagen denominada "panal de abejas"

Derrame Pleural Derecho

Neumonía por aspiración

Neumotórax Espontaneo

Bronquiectasias

Neumonitis

Scleroderma with aspiration pneumonia. (a)High-resolution CT scan shows air-space consolidation in the superior segments of both lower lobes. (b) High-resolution CT scan (mediastinal windows) shows a dilated, fluid-filled esophagus.
Scleroderma with nonspecific interstitialpneumonitis. High-resolution CT scanobtained through the lung bases shows bibasilar areas of consolidation. Video-assisted thoracoscopic surgical biopsyshowed nonspecific interstitialpneumonitis.

Scleroderma with pulmonary fibrosis. (a) Posteroanterior radiograph shows low lungvolumes and bibasilar, coarse reticular markings. (b, c) High-resolution CT scansshow patchy areas of peripheralhoneycombing (b) and diffusehoneycombing at the lung bases (c).

POLIMIOSITIS/DERMATOMIOSITIS
Afectación pulmonar45%
Pacientes con DM/PMComplicaciones pulmonares:•enfermedad intersticial Pulmonar• hipoventilación• insuficiencia respiratoriapor debilidad de los músculos respiratorios,•neumonía por aspiración y toxicidadpor drogas.

POLIMIOSITIS/DERMATOMIOSITIS

Dermatomyositis with bronchiolitisobliterans organizing pneumonia. High-resolution CT scans show a peripheral area of consolidation in the right middle lobe (a)and peribronchial consolidation in both lung bases (b).
Dermatomyositis with bronchiolitisobliterans organizing pneumonia. High-resolution CT scans show a peripheral area of consolidation in the right middle lobe (a)and peribronchial consolidation in both lung bases (b).

Polymyositis with pulmonary fibrosis (usual interstitial pneumonia). High-resolution CT scan shows peripheral architecturaldistortion and bilateral tractionbronchiectasis.

SÍNDROME DE SJÖGREN
Hallazgo radiológico más frecuente:afectación intersticial pulmonar,10-14% de pacientes en Rx y 34% Asociación con neumonía intersticial linfocitaria (NIL) Se manifiesta como un patrón reticulonodular predominio en lóbulos inferiores o como extensas áreas de afectación en vidrio deslustrado y múltiples quistes de paredes finas. Sjögren syndrome with lymphocytic
interstitial pneumonitis. High-resolution CT scan shows scattered bilateral thin-walledcysts.

Sjögren syndrome with bronchiectasis. High-resolution CT scan shows extensivebilateral cylindrical bronchiectasis.

Neumoconiosis
Las neumoconiosis engloban un grupo muyamplio de enfermedades pulmonares causadas por la inhalación de polvo inorgánico en concentraciones altas y muchas veces de origen ocupacional.
La lesión pulmonar desencadenada por lainhalación de estas partículas va a depender de muchos factores como son: naturaleza química, tamaño y forma de éstas, concentración en el aire ambiente, duración de la exposición,distribución y mecanismos de depuración yvariaciones individuales en la respuesta inmune e inflamatoria.
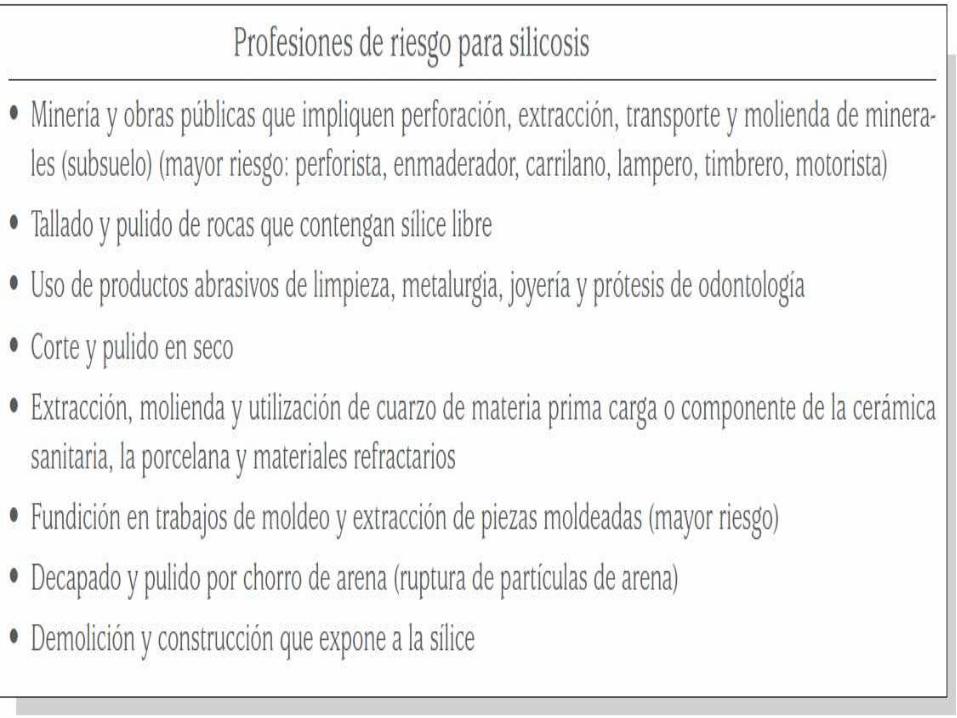

Silicosis
Silicosis in a 54-year-old man who worked for 20 years as a stonecutter. (a) Chest radiograph shows multiple small nodules in both lungs, predominantly in the upper and middle zones.
Silicosis in a 56-year-old man who worked for 25 years as a stonecutter. (a) Chest radiograph shows multiple variable-sized nodular lesions in both lungs, predominantly in the upper and middle zones.

Silicosis and progressive massive fibrosis in a 58-year-old man who worked for 30 years as a stoneworker. (a) Chest radiograph shows multiple small nodules and masses in both lungs, predominantly in the upper and middle zones, and eggshell calcifications (arrows) in the lung hilum and the mediastinum.

Silicosis and progressive massive fibrosis in a 66-year-old man who worked for 10 years crushing rock with a high quartz content. (a) Chest radiograph shows large bilateral opacities (arrows) in the upper zones of the lung, as well as upward elevation of both hila.

NEUMOCONIOSIS DE LOS TRABAJADORES DEL CARBÓN
Progressive massive fibrosis in a 59-year-old man who worked for 20 years in a coal mine. (a) Composite of axial thin-section CT scans (1.0-mm-thick sections) obtained at various levels of the distal trachea shows irregularly marginated 20–30-mm nodules (arrows) accompanied by smaller satellite nodules and surrounding reticulation in the upper lobe of both lungs
Progressive massive fibrosis in a 59-year-old man who worked for 20 years in a coal mine. (a) Composite of axial thin-section CT scans (1.0-mm-thick sections) obtained at various levels of the distal trachea shows irregularly marginated 20–30-mm nodules (arrows) accompanied by smaller satellite nodules and surrounding reticulation in the upper lobe of both lungs.

ASBESTOSISEl término asbesto es de origen griego ysignifica inextinguible. Desde tiempo antes deCristo se conoce este material resistente al fuego
Asbestosis in a 58-year-old man who worked for 25 years in building construction. Chest radiograph shows small reticular opacities (arrows) at the costophrenic sulcusin the lower zone of both lungs.
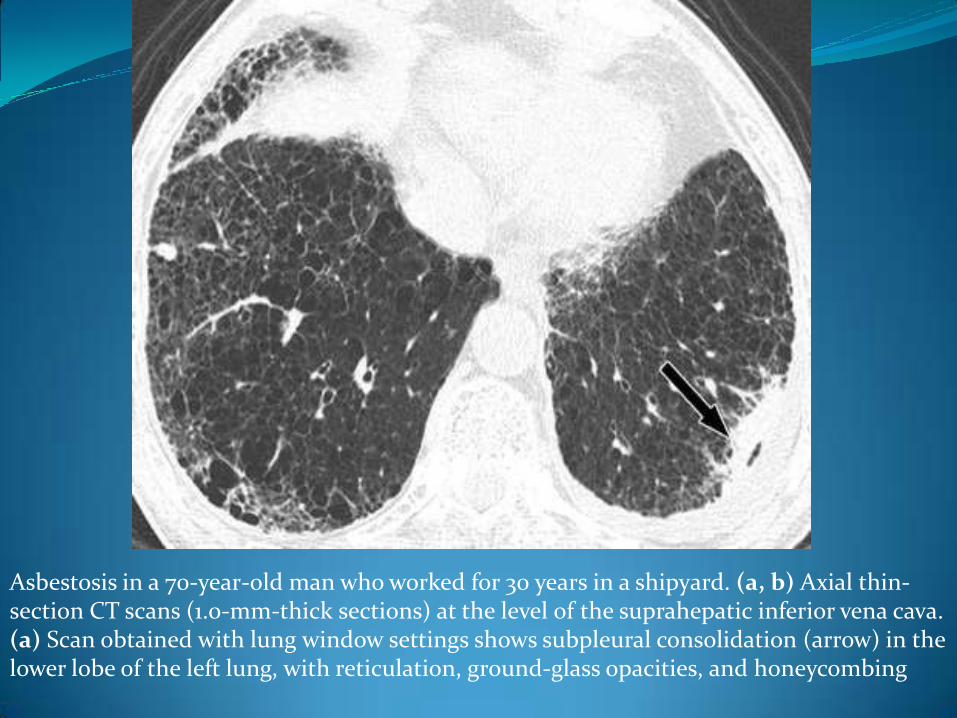
Asbestosis in a 70-year-old man who worked for 30 years in a shipyard. (a, b) Axial thin-section CT scans (1.0-mm-thick sections) at the level of the suprahepatic inferior vena cava. (a) Scan obtained with lung window settings shows subpleural consolidation (arrow) in the lower lobe of the left lung, with reticulation, ground-glass opacities, and honeycombing


BERILIOSISLa radiografía de tórax no muestra un patrón específico. Es posible que sea normal(hasta en un 25% de casos con demostración histológica) o con un patrón de opacidadesdifusas, granular, que respeta los vértices y las bases. Se pueden observar adenopatías hiliares y nódulos, en ocasiones calcificados.
Berylliosis in a 49-year-old man who worked for 7 years in metal polishing. (a) Chest radiograph shows bilateral mediastinal and hilar lymph node enlargement, as well as internal fixation of a right clavicular fracture

Berylliosis in a 49-year-old man who worked for 7 years in metal polishingAxial thin-section CT scans (1.0-mm-thick-sections) obtained at the levels of the bronchus intermedius (b) and the basal segmental bronchus (c) show multiple small nodules along the bronchovascular bundles (straight arrows) and in subfissural regions (arrowheads) and enlarged hilar lymph nodes (curved arrows).