Fiebre Mandell.7

of 14
-
Upload
enrique-swayne -
Category
Documents
-
view
215 -
download
0
Transcript of Fiebre Mandell.7
-
7/28/2019 Fiebre Mandell.7
1/14
76
Temperature Regulation andthe Pathogenesis of FeverPHILIP A. MACKOWIAK
5050
The oldest known written reerence to ever exists in Akkadian cunei-orm inscriptions rom the 6th centurybc, most likely derived roman ancient Sumerian pictogram o a aming brazier used to symbolizeboth ever and the local warmth o inammation.1 Theoretical con-structs o the pathogenesis o ever did not emerge until severalcenturies later, when hippocratic physicians proposed that body tem-perature, and physiologic harmony in general, involved a delicatebalance among our corporal humorsblood, phlegm, black bile, andyellow bile.2 Fever was then believed to result rom an excess o yellowbile, a concept in concert with the act that many inections o that eracaused both ever and jaundice. During the Middle Ages, demonic
possession was added to the list o mechanisms thought to be respon-sible or ever. By the 18th century, Harveys discovery o the circula-tion o blood and the birth o clinical chemistry led iatrophysicists andiatrochemists to hypothesize alternatively that body heat and everresulted rom riction associated with the ow o blood through thevascular system and that they resulted rom ermentation and putre-action occurring in the blood and intestines.3 Ultimately, as a resulto the work o Claude Bernard, the metabolic processes occurringwithin the body came to be recognized as the true source o body heat.Subsequent work established that body temperature is tightly con-trolled within a narrow range by mechanisms regulating the rate atwhich such heat is allowed to dissipate rom the body.
The origin o the practice o monitoring body temperature as an aidto diagnosis is uncertain. The oldest known reerences to devices usedto measure temperature date to the 1st or 2nd centurybc, when Philo
o Byzantium and Hero o Alexandria are believed to have inventedseveral such devices.4 It is reasonably certain that Galileo manuac-tured a primitive (air) thermometer at about the time that he assumedthe chair in mathematics at Padua in 1592.5 However, thermometrywas not ully assimilated into medical practice until 1868, when CarlReinhold August Wunderlich published a magnum opus entitled DasVerhalten der Eigenwrme in Krankenheiten (The Course o Tempera-ture in Diseases).6
Through Das Verhalten der Eigenwrme in Krankenheiten, Wun-derlich gave 37 C (98.6 F) special signifcance with respect to normalbody temperature.7 He described the diurnal variation o body tem-perature and, in the process, alerted clinicians to the act that normalbody temperature is actually a temperature range, rather than a spe-cifc temperature.
TminologyAccording to the International Union o Physiological Sciences Com-mission or Thermal Physiology, ever is a state o elevated core tem-perature, which is oten, but not necessarily, part o the deensiveresponses o multicellular organisms (host) to the invasion o live(microorganisms) or inanimate matter recognized as pathogenic oralien by the host.8 The ebrile response, o which the temperature riseis a component, is a complex physiologic reaction to disease, involvingnot only a cytokine-mediated rise in core temperature but also thegeneration o acute-phase reactants and the activation o numerousphysiologic, endocrinologic, and immunologic systems. The regulatedrise in temperature during ever is to be distinguished rom that occur-ring during episodes o heat stroke and other orms o orced hyper-
thermia, in which inammatory cytokines play only a minor rolThermophysiologists defne the term hyperthermia as the condition oa temperature regulator when core temperature is above the rangspecifed or the normal active state o the species.8 It may be regulateas in ever, or orced, as in heat stroke, when heat production exceethe capacity o heat loss. Heat stroke and other orms o orced hypethermia are characterized by a sustained elevation in core temperatulacking the diurnal uctuation typical o ever and normal body temperature, and do not respond to antipyretic therapy.9
In the clinical setting, ever is typically defned as a pyrogen-medated rise in body temperature above the normal range. Although con
sistent with the publics perception o ever, the defnition ignores thact that a rise in body temperature is but one component o thmultiaceted response. This standard clinical defnition is urthawed, because it implies that body temperature is a single entitwhen, in act, it is a pastiche o many dierent temperatures, eacrepresentative o a particular body part, and each varying throughouthe day in response to activities o daily living and the inuence oendogenous diurnal rhythms.
Clinical ThmomtyFor over a century, the thermometer has been preeminent amonclinical instruments used to distinguish health rom disease and monitor the course o illness. Unortunately, thermometric measurments are inuenced by a host o variables, all too requently ignore
when interpreting the signifcance o clinical temperature readings.
ANATOMIC VARIABILITY
Although clinicians requently regard temperature readings romvarious anatomic sites as equivalent approximations o body temperture,1 no one temperature characterizes the thermal status o thhuman body. This is because the body has many dierent temperatures, each representative o a particular body part. Nevertheleswithin the body, there are two basic thermal compartments worthy special considerationthe core and the shell.10
The shell, which consists o skin and subcutaneous at, insulates thcore rom the external environment. The core, o which the viscerand muscles are major components, although insulated by the shehas temperature gradients o its own resulting rom dierences in thmetabolic rates and blood ow patterns o the various organs contained therein. Even during baseline conditions, organs with highmetabolic rates have slightly higher temperatures than those wilower metabolic rates; in general, tissues close to the skin have lowetemperatures than those at deeper locations.11 Although such dieences are normally small, muscle temperatures rise during vigorouexercise markedly in comparison with those o less metabolically activorgans. During shock and under extreme environmental conditionregional anatomic variations in temperature may also bexaggerated.
Rectal measurements were once regarded as the most practical anaccurate means o obtaining routine estimates o core temperaturBenzinger and Benzinger, however, have pointed out that no knowthermoregulatory system exists at this particular anatomic site.11 Rect
SecTion A ever
-
7/28/2019 Fiebre Mandell.7
2/14
766 PART II Major Clinical Syndromes
Their fndings concerning the relationship between rectal and oralreadings were in agreement with those o several earlier investiga-tions.37-40 Their fndings with respect to the relationship between oraland TM readings, however, diered rom earlier reports,12 which hadgenerally shown TM readings to be higher than simultaneouslyobtained oral measurements. This discrepancy most likely reected theact that unadjusted-mode TM thermometersor example, the IVACCoregenerally give lower readings than adjusted-mode TM ther-mometers, such as those used in earlier studies.23
PHYSIOLOGIC VARIABLES
Wunderlich and Seguin41 believed that old people have lower bodytemperatures than younger persons, and their views in this regard werecorroborated by Howell in a report published in Lancet in 1948.42There is also a substantial body o data suggesting that thermoregula-tion is impaired in older persons because o various eects o aging onthe autonomic nervous system.43 Nevertheless, more recent work hasnot shown lower average core temperatures among healthy older sub-jects (mean age, 80.3 years; range, 62 to 99 years) than among healthyyounger subjects.44 Comparisons o simultaneous oral, axillary, andrectal temperature readings rom these subjects have shown loweraverage oral and axillary readings in older persons but comparableaverage rectal temperatures in older and younger subjects.
It has long been known that women exhibit increases in body tem-perature o about 0.5 C (0.9 F) at the time o ovulation.14 Wunderlichand Seguin also maintained that women have slightly higher normaltemperatures than men overall and oten show greater and moresudden changes in temperature.41 Two other studies have corroboratedWunderlich and Seguins ormer but not latter observation.45,46
Body temperature, like most physiologic unctions, exhibits circa-dian rhythmicity that is linked to the sleep-wake cycle.47 Duringnormal sleep-wake cycles (i.e., asleep during the night and awakeduring the day), the core temperature reaches its zenith in the lateaternoon or early evening and its nadir in the early morning.45 Adap-tation to night shit work causes a reversal o this pattern. Thermo-regulation has also been reported to be altered in patients withneuropsychiatric disorders, such as chronic depression.48 Thereore,when interpreting clinical thermometric measurements, it is impor-
tant to consider not only the time o the measurement and the site atwhich the temperature was taken, but also the sleep-wake cycle andmental health o the subject being studied.
In addition to these physiologic variables, exercise, digestion, andunderlying disorders such as chronic renal ailure, shock, and localinammation at the site o the thermometric measurement (e.g.,proctitis, external otitis, or stomatitis) may alter thermoregulatoryresponses, local temperature, or both. It has, or example, been shownthat the core temperature varies by as much as 3 C (36 to 39 C) instates ranging rom sleep to moderately high levels o sustained exer-cise, and this continuum o body temperature is related to a contin-uum o activity.49 Ambient temperature and humidity have beenshown experimentally to aect both human sleep stages and bodytemperature,50 suggesting that body temperature might also varyaccording to the time o year and local climate. It is pertinent in thisregard that Cheng and Partridge have shown that bundling and warmenvironments can elevate rectal temperatures o newborns to theebrile range.51
Normal Body TemperatureA survey o physicians perceptions o body temperature published in1995 indicated widespread conusion regarding key eatures o thehuman body temperature.52 O 268 physicians and medical studentssurveyed, 75% gave 37 C (98.6 F) as their defnition o normal bodytemperature. An additional 13% defned the normal temperature as anarrow range o temperatures about a mean o 37 C (98.6 F). Only10 (4%) subjects in the group as a whole specifed a particular bodysite (e.g., oral or rectal) or temperature measurements in their defni-tion. Also, 98% percent thought that the normal temperature varies
temperature readings are consistently higher than those obtained atother sites (even pulmonary artery blood), which some authoritieshave suggested might be caused by heat generated as a result o themetabolic activity o ecal bacteria.11 However, an early study showedno signifcant decrease in the rectal temperature ater a reduction inthe colonic bacterial content.11 There is also concern that stool in therectum acts as a heat sink to delay or mitigate changes in the rectaltemperature, particularly i the thermometer is inserted directly intostool.12 During shock, perusion o the rectum may be markedly
impaired, causing the rectal temperature to lag signifcantly behind arapidly rising or alling core temperature.13 For this reason, Houdasand Ring have concluded that the rectal temperature provides a reli-able approximation o the core temperature only i the patient is inthermal balance.14 In neonates, even in the absence o shock, the rectaltemperature measured by standard technique has been reported tocorrelate poorly with the core temperature as measured by a deeprectal probe.15
The right atrium is the ideal site or measuring core temperature,because it is the nexus at which venous blood rom all anatomicregions joins. However, because it is relatively inaccessible, the tem-peratures o other sites are more oten used as approximations o coretemperature. The tympanic membrane (TM) temperature is thoughtby some to be particularly useul in this regard, because the TM isperused by a tributary o the artery that supplies the bodys thermo-
regulatory center.22
This act, and the ease with which TM measure-ments can be obtained using modern inrared TM thermometers, havemade these instruments the thermometers o choice in many clinicsand intensive care units. There are two basic types o inrared TMthermometers. One type detects radiant energy emitted rom the TMand portions o the ear canal, processes the inormation, and thendisplays a value representing tissue temperature in the ear canal (unad-justed mode).23 The other displays an (adjusted) estimate o the coretemperature (e.g., pulmonary arterial blood temperature) based oncomparison data obtained rom selected study samples. Readingsobtained using the ormer type o TM thermometer tend to be lowerthan simultaneously obtained oral readings, whereas those obtainedwith the latter type are generally higher.22 Unortunately, numerousstudies o many dierent TM thermometers have shown that althoughconvenient, such instruments tend to give highly variable readings
that correlate poorly with simultaneously obtained oral or rectalreadings.19,23-26
Several studies have shown that monitoring the skin temperatureusing temperature-sensitive crystals incorporated into plastic stripsplaced on the orehead is an insensitive technique or detecting eleva-tions in the core temperature.32,33 The detection o ever by palpationis similarly insensitive. Bergeson and Stieneld ound that 42% o 138ebrile children (as defned by a body temperature o 38 C or higher)were judged to be aebrile by nurse assistants using palpation to detectever.34 Only 1.8% o over 1000 aebrile children were judged to beebrile using this same technique. In an evaluation o a mothers abilityto assess the temperature o her child by palpation, Banco and Veltriound mothers to have a sensitivity o 73.9% and a specifcity o 85.6%or detecting ever higher than 38 C (100.4 F).35 Thus, palpation bymothers was more sensitive than that by nurse assistants but was lessspecifc or detecting the ebrile state. Finally, Bonadio and co-workershave reported that among inants younger than 2 months presentingto the emergency room with a history o ever, those in whom everhad been documented at home by rectal thermometer were twice aslikely to be ebrile on presentation or during hospitalization than thosewhose ever had been documented by palpation alone (92% vs. 46%;P< .001).36
Because the temperature o the rectum, mouth, and tympanic mem-brane are related but not identical, it would be useul to have a reliableormula or converting data rom one site to another. In a study ohealthy young adults, Rabinowitz and associates determined that onaverage, rectal readings exceed concurrent oral readings by 0.4 C(0.8 F) and exceed TM readings (obtained with the IVAC Core) by0.8 C (1.6 F).19 However, these relationships were extremely variable.
-
7/28/2019 Fiebre Mandell.7
3/14
50 Temperature Regulation and the Pathogenesis o Fever 76
1 C (2.44 beats/min or each 1 F) rise in temperature over the rango temperatures examined (96.0 to 100.8 F).
According to Wunderlich and Seguin, When the organism (manis in a normal condition, the general temperature o the body main
tains itsel at the physiologic point: 37 C= 98.6 F.41
Although seversubsequent investigations have recorded mean temperatures o normadult populations closer to 36.6 C (98.0 F),53 Wunderlichs intimtion that 37 C (98.6 F) is the most normal o temperatures 54 persisto this day in lay thinking, although to a lessening extent in the thinking o health care workers.
The data reviewed earlier suggest that 37 C (98.6 F) has no specisignifcance vis--vis body temperature in healthy young adults whesuch temperature is measured orally using modern thermometers. Ithe population examined, 37 C (98.6 F) was not the overall meatemperature, the mean temperature o any o the time periods studiethe median temperature, or the single most requent temperaturrecorded. Furthermore, it did not all within the 99.9% confdenclimits or the sample mean (36.7 to 36.8 C; 98.1 to 98.2 F).
Wunderlich identifed 38.0 C (100.4 F) as the upper limit o norm
body temperature in his patient population and thereore regarded antemperature higher than 38.0 C (100.4 F) as ever.41 However, thupper limit o normal body temperature varies among individuathereby limiting the applicability o mean values derived rom popultion studies (even those as large as Wunderlichs) to individual subjects. However, the maximal temperature, like the mean temperaturexhibited by a population varies according to the time o day and th
during the day, with quantitative estimates o such diurnal variabilityranging rom 0.2 C (0.4 F) to 2.8 C (5 F) (mean SD, 0.8 0.4 C[1.6 0.8 F]).
The origin o these perceptions o body temperature is uncertain,
but in all likelihood it lies in Carl Wunderlichs 1868 book on clinicalthermometry (see earlier), which many regard to this day as the defni-tive work on the subject.6 Unortunately, several o Wunderlichsdictums concerning body temperature, such as the perceptions omodern-day physicians, appear to be in error.
A 1992 descriptive analysis o 700 baseline oral temperature obser-vations rom 148 healthy men and women ound a range o 35.6 C(96.0 F) to 38.2 C (100.8 F), with an overall mean o 36.8 0.4 C(98.2 [0.7 F]); 37 C (98.6 F) accounted or only 56 (8%) o the 700oral temperature observations recorded (Fig. 50-1).45 The mean tem-perature varied diurnally, with a 6 am nadir and a 4 to 6 pm peak (Fig.50-2). The maximal temperature (as reected by the 99th percentile)varied rom a low o 37.2 C (98.9 F) at 6 am to a high o 37.7 C(99.9 F) at 4 pm. Age did not signifcantly inuence temperaturewithin the age range studied (18 to 40 years) (linear regression, P=
.99). Women had a slightly higher average oral temperature than men(36.9 C [98.4 F] vs. 36.7 C [98.1 F]; t test, P < .001, degrees oreedom [d] = 698) but did not exhibit higher average diurnaltemperature oscillations than male counterparts (0.56 C [1.0 F] vs.0.54 C [0.97 F]). There was a statistically signifcant linear relation-ship between temperature and pulse rate (regression analysis, P
-
7/28/2019 Fiebre Mandell.7
4/14
768 PART II Major Clinical Syndromes
convert adenosine diphosphate to adenosine triphosphate (ATP). Atrest, more than hal o the bodys heat is generated as a result o theinefciency o the biochemical processes that convert ood energy intothe ree energy pool (e.g., ATP). Even i no external work is beingperormed, heat is generated as a result o both internal work (e.g.,peristalsis, myocardial contractions, and the circulation o blood) andbiochemical reactions involved in maintaining the structural and unc-tional integrity o the various organ systems (i.e., the uptake and resyn-thesis o ATP). When external work is perormed, additional heat is
generated as a byproduct o skeletal muscle contractions.In adult humans and most other large mammals, shivering is the
primary means whereby heat production is enhanced. Nonshiveringthermogenesis is more important in smaller mammals, newborns(including humans), and cold-acclimated mammals.60,61 Althoughseveral tissues (e.g., the heart, respiratory muscles, and adipose tissue)contribute to the process, brown adipose tissue has been most closelyassociated with nonshivering thermogenesis. This highly specializedorm o adipose tissue located near the shoulder blades, neck, adrenals,and deep blood vessels (adjacent to vital organs) is characterized by itsbrownish color, a prouse vascular system, and an abundance omitochondria.60,62
Heat generated primarily in vital organs lying deep within the bodycore is distributed throughout the body via the circulatory system. Inresponse to input rom the nervous system, the circulatory system
determines both the temperature o the various body parts and the rateat which heat is lost rom body suraces to the environmentby con-duction, convection, radiation, and evaporation.63 In a warm environ-ment, or in response to an elevation in the core temperature resultingrom exercise, cutaneous blood ow increases so that heat is trans-ported rom the core to be dissipated at the skin surace. Simultaneousactivation o sweating enhances such heat loss via evaporation. Inanesthetized animals, increases in cutaneous blood ow in response tohypothalamic warming are oset by concomitant reductions in gas-trointestinal blood ow.64 In a cold environment or in response toa reduction in core temperature, cutaneous blood ow normallydecreases as a means o conserving heat within the body core.
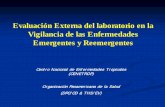
Thermoregulation is a process that involves a continuum o neuralstructures and connections extending to and rom the hypothalamusand limbic system through the lower brain stem and reticular orma-
tion to the spinal cord and sympathetic ganglia (Fig. 50-3).
60
Neverthe-less, an area o the brain located in and near the rostral hypothalamus
site at which the temperature measurement is taken. Because o suchvariability, no single temperature can be designated as the upper limito normal. In the study population considered earlier, 37.2 C (98.9 F)was the maximal oral temperature (i.e., the 99th percentile) recordedat 6 am, whereas at 4 pm, the maximal oral temperature observedreached 37.7 C (99.9 F). Thus, these data suggest that when modernthermometers are used to monitor oral temperature in young or mid-dle-aged adults, ever is roughly defned as an early-morning tempera-ture o 37.2 C (99.0 F) or higher or a temperature o 37.8 C (100 F)
or higher at any time during the day.Wunderlich wrote in 1868 that [temperature] oscillates even in
healthy persons according to time o day by 0.5 C = 0.9 F. The nextyear, Wunderlich and Reeve wrote, The lowest point is reached in themorning hours between two and eight, and the highest in the ater-noon between our and nine.55 Modern authorities have generallyconcurred with these observations. However, Tauber has suggestedthat the amplitude o diurnal variation might be as high as 1 C(1.8 F).56 The data described earlier are more consistent with the viewso Wunderlich and colleagues. Nevertheless, the subjects examined inthat study exhibited considerable individual variability, with somehaving daily temperature oscillations as wide as 1.3 C (2.4 F) andothers having oscillations as narrow as 0.1 C (0.2 F).
According to Wunderlich and Seguin, women have slightly highernormal temperatures than men and oten show greater and more
sudden changes o temperature.41
In a study o nine healthy youngadults (six male and three emale), Dinarello and Wol corroboratedboth observations.46 The investigation described earlier, which did notcontrol or the eects o ovulation on thermal observations, was ableto corroborate only the ormer observation o Wunderlich andSeguin.45
It has been maintained or over a century that older persons havelower body temperatures than younger persons.41 Howells 1948 study(see earlier) seemed to substantiate this belie.42 Although there areconsiderable data suggesting that thermoregulation is impaired inolder persons because o various eects o aging on the autonomicsystem,43 as noted, more recent investigation has not shown loweraverage core temperatures among healthy older persons than amonghealthy young people.44
As a result o work conducted earlier this century, 38,57 it is widely
believed that the heart rate increases 10 beats/min or each 1 F rise inbody temperature. More recent data (see earlier) indicate that the heartrate increases only 2.44 beats/min or each 1 F rise in temperature.45The dierence between the earlier and more recent investigations mostlikely reects the act that in the latter study, subjects were aebrile andwere examined seated, whereas those examined in earlier investiga-tions were mostly ebrile and rested reclining on a couch or 20 minutesbeore examination.
The normal range o body temperature in children is not well delin-eated. Lorin has written that the range is higher in children than inadults and that a decrease toward adult levels begins at about 1 year oage, continues through puberty, and stabilizes at 13 to 14 years o agein girls and at 17 to 18 years o age in boys.58 He has oered a 1937publication by Bayley and Stolz as documentation o his views on thematter.59 Unortunately, these early investigators did not control orvariables such as the time o day, bundling, and the thermometer dwelltime, each o which might have signifcantly aected the results o theirsurvey. It has also been maintained that the circadian rhythm thatcharacterizes body temperature in the adult is less evident in the frstew months o lie, is well established by the second birthday, and tendsto be more pronounced during childhood than during adulthood.58This concept, like many concerned with the normal temperature ochildren, is difcult to substantiate with published data.
ThmogulationHeat is derived rom biochemical reactions occurring in all livingcells.60 At the mitochondrial level, energy derived rom the catabolismo metabolites such as glucose is used in oxidative phosphorylation to
Septalnucleus
Preopticnucleus OVLT
Anteriorhypothalamus
RF
STt
igu 50-3 Sagittal view o the brain and upper spinal cordshowing the multisynaptic pathway o skin and spinal thermorecep-tors through the spinothalamic tract (STt) and reticular ormation(RF) to the anterior hypothalamus, preoptic region, and the septum.OVLT, organum vasculosum o the lamina terminalis. (From MackowiakPA. Concepts of fever. Arch Intern Med. 1998;158:1870-1881.)
-
7/28/2019 Fiebre Mandell.7
5/14
50 Temperature Regulation and the Pathogenesis o Fever 76
enous pyrogens, regardless o their physicochemical structure, initiaever by inducing host cells (primarily macrophages) to producendogenous pyrogens. Such concepts notwithstanding, certain endoenous molecules also have the capacity to induce endogenous pyrogens. These include, among others, antigen-antibody complexes in thpresence o complement,74,75 certain androgenic steroid metabolites,76-78 inammatory bile acids,79 complement,80 and various lymphocyte-derived molecules.81,82 Similarly, data recently obtained romguinea pig studies have suggested that bacterial lipopolysaccharid
(LPS) induces ever directly (rather than indirectly through the indution o pyrogenic cytokines) by interacting with Kupers cells, therebinitiating pyrogenic signals that are transmitted to the preoptic area othe hypothalamus via the hepatic branch o the vagus nerve. 83 Thuthe distinction between endogenous and exogenous pyrogens is artifcial at best.
Complete understanding o the unction o individual pyrogencytokines has been hampered by the act that one cytokine oten inences the expression o other cytokines, their receptors, or both, anmay also induce more distal co-mediators o cytokine-related bioativities (e.g., prostaglandins and platelet-activating actor).84 In shorcytokines unction within a complex regulatory network in whicinormation is conveyed to cells by combinations, and perhaps bsequences, o a host o cytokines and other hormones.85 Like the wordo human communication, individual cytokines are basic units o
inormation. On occasion, a single cytokine, like a single word, macommunicate a complete message. More oten, however, complemessages received by cells probably resemble sentences, in which combinations and sequences o cytokines convey inormation. Because osuch interactions, it has been difcult to ascertain the direct in vivbioactivities o particular cytokines. Nevertheless, several cytokinhave the capacity to induce ever in common. On the basis o thcharacteristic, they have been codifed together as so-called pyrogencytokines.
The list o currently recognized pyrogenic cytokines includes inteleukin-1 (IL-1 [IL-1 and IL-]), tumor necrosis actor- (TNF-IL-6, ciliary neurotropic actor (CNF), and intereron (IFN).86-94 Eveamong these ew cytokines, complex relationships exist, with certaimembers upregulating the expression o other members or their receptors in certain situations and downregulating them in others.84 Th
our major pyrogenic cytokines have monomeric molecular massthat range rom 17 to 30 kDa. Undetectable under basal conditions ihealthy subjects, they are produced by many dierent tissues response to appropriate stimuli. Once released, pyrogenic cytokinhave short intravascular hal-lives. They are pleiotropic, in that theinteract with receptors present on many dierent host cells. They aractive in picomolar quantities, induce maximal cellular responses eveat low receptor occupancy, and exert local (autocrine-paracrine) well as systemic (endocrine) eects.84
It has long been suspected that interactions between pyrogenic cytokines and their receptors in the preoptic region o the anterior hypothalamus activate phospholipase A2, liberating plasma membranarachidonic acid as a substrate or the cyclooxygenase (COX) pathwaSome cytokines appear to do so by increasing COX expression directcausing liberation o the arachidonate metabolite PGE2. Because thsmall lipid molecule easily diuses across the blood-brain barrier, it thought by some to be the local mediator that activates thermosenstive neurons. In the case o ever induced by circulating IL-6, thcytokines pyrogenic eect appears to be mediated by PGE2 produceby nuclear signal transducer and activator o transcription (STAT)3positive cells involved in the COX-2dependent ever pathway in thcerebral microvasculature.95 Although it is not yet widely accepteadditional studies have indicated that the C5a component o the complement cascade is integral to LPS-induced ever96 and that in somsituations, thermal inormation involved in the ebrile response transmitted rom the periphery to the thermoregulatory center vvagal pathways (see earlier).97
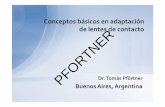
Figure 50-4 depicts the current hypothetical model or the ebriresponse,98 in which pyrogenic cytokines released by phagocytic leu
appears to be especially important to the process o thermoregulation.Although generally reerred to as the preoptic area, it actually includesthe medial and lateral aspects o the preoptic area, anterior hypothala-mus, and septum. Numerous studies extending over 60 years haveestablished that a synaptic network o neurons located in this areaexerts at least partial control over physiologic and behavioral thermo-regulatory responses.63,65 The network encompasses our dierenttypes o neuronswarm-sensitive, temperature-insensitive, heat loss,and heat production eector neuronsthat regulate core tempera-
ture. Hypothalamic warm-sensitive neurons integrate core and periph-eral thermal inormation, orienting their dendrites medially andlaterally to receive aerent input rom cutaneous thermoreceptors.Temperature-insensitive neurons have a dierent dendritic orienta-tion and appear to provide constant reerence signals that determinethermoregulatory setpoints. The temperature-sensitive and tempera-ture-insensitive neurons send mutually antagonistic inputs to eectorneurons controlling thermoregulatory responses, with warm-sensitiveneurons exciting heat loss through eector neurons and inhibitingheat production neurons.65
Many, although not all, thermophysiologists believe that the tem-perature-sensitive preoptic area regulates body temperature by inte-grating thermal input signals rom thermosensors in the skin and coreareas, including the central nervous system.66 One o the more widelyheld theories is that such integration involves a designated thermal
setpoint or the preoptic area that is maintained by a negative eedbacksystem. According to this theory, i the preoptic temperature risesabove its setpoint, or whatever reason (e.g., during exercise), heat lossresponses are activated to lower the body temperature and return thetemperature o the preoptic area to the thermal setpoint (e.g., 37 C).67The thermal setpoint o a particular heat loss response is thus themaximal temperature tolerated by the preoptic area beore the heatloss response is evoked. I, on the other hand, the preoptic temperaturealls below its thermal setpoint (e.g., as a result o cold exposure),various heat retention and heat production responses are activated toraise body temperature and, with it, the temperature o the preopticarea, to its thermal setpoint. The thermal setpoint o a particular heatproduction response is thus the minimal temperature tolerated by thepreoptic area beore the response is evoked.
Although a convenient explanation o the means whereby tempera-
ture elevations are coordinated during ever, the concept o a singlecentral setpoint temperature is regarded by many thermophysiologistsas oversimplifed. At least some physiologists preer to think o bodytemperature as regulated within a narrow range o temperatures by acomposite setpoint o several thermosensitive areas and several dier-ent thermoregulatory responses.68-70
Various endogenous substances and drugs appear to aect tempera-ture regulation by altering the activity o hypothalamic neurons.Perhaps the best examples o such substances are the pyrogenic cyto-kines (see later). These are released by mononuclear phagocytes inresponse to a wide array o stimuli and have the capacity to raise thethermoregulatory centers thermal setpoint. Whether they cross theblood-brain barrier to do so71,72 or act by evoking the release o othermediators (e.g., prostaglandin E2 [PGE2]) in circumventricular organs,such as the organum vasculosum o the lamina terminalis (OVLT), 71is uncertain. Whatever the precise endogenous mediators o ever,their primary eect appears to be to decrease the fring rate o preopticwarm-sensitive neurons, leading to the activation o responses designedto decrease heat loss and increase heat production.
endognous PyognsTraditionally, pyrogens have been divided into two general categories,those that originate outside the body (exogenous pyrogens) and thosethat are derived rom host cells (endogenous pyrogens). Exogenouspyrogens are, or the most part, microorganisms and toxins or otherproducts o microbial origin, whereas endogenous pyrogens are hostcellderived (pyrogenic) cytokines that are the principal central medi-ators o the ebrile response.73 According to traditional concepts, exog-
-
7/28/2019 Fiebre Mandell.7
6/14
770 PART II Major Clinical Syndromes
vidual cytokines in response to various stimuli; or how the upper limito the ebrile range is set.84
Acut-Phas rspons
As noted, a cytokine-mediated rise in the core temperature is but oneo many eatures o the ebrile response. Numerous other physiologicreactions, collectively reerred to as the acute-phase response, aremediated by members o the same group o pyrogenic cytokines thatactivate the thermal response o ever. Such reactions include a hosto behavioral, physiologic, biochemical, and nutritional alterations(Table 50-1).101 Stimuli capable o inducing an acute-phase responseinclude bacterial and (to a lesser extent) viral inections, trauma,malignant neoplasms, burns, tissue inarction, immunologically medi-ated and crystal-induced inammatory states, strenuous exercise, andchildbirth.85,102 There is also evidence that major depression,103 schizo-phrenia,104 and psychological stress105 are capable o inducing an acute-phase response.
Traditionally, the term acute-phase response has been used to denotechanges in plasma concentrations o a number o secretory proteinsderived rom hepatocytes. Acute-phase proteins, o which there aremany (Table 50-2),101 exhibit increased synthesis (positive acute-phaseproteins) or decreased synthesis (negative acute-phase proteins)during the acute-phase response. IL-6 is the chie stimulator o theproduction o most acute-phase proteins. Other pyrogenic cytokines,however, also inuence the production o various subgroups o theseproteins.101
Many o the acute-phase proteins are believed to modulate inam-mation and tissue repair.106 A major unction o C-reactive protein(CRP), or example, is presumed to involve binding o phosphocholineon pathogenic microorganisms, as well as phospholipid constituentson damaged or necrotic host cells. Through such binding, CRP mightactivate the complement system and promote phagocyte adherence,thereby initiating the process whereby pathogenic microbes or necrotic
kocytes into the bloodstream in response to exogenous pyrogens fndtheir way to the OVLT, where they induce synthesis o prostaglandinsmediating the ebrile response. The model has several shortcomingsthat have caused thermophysiologists to suspect that multiple path-ways might be involved in the induction o ever (e.g., the vagal path-ways reerred to earlier, local production o pyrogenic cytokines in thehypothalamus itsel, participation o membrane-bound cytokines asmediators, and Toll-like receptor signal transduction), with dierentpathways or combinations o pathways being responsible or ever indierent situations.97,99,100 All the models proposed to date have beenconcerned with mechanisms responsible or the induction phase oever. None has considered the plateau or ascending phases o ever orexplained why a disorder such as endocarditis, in which exogenouspyrogens (i.e., bacteria) are present continuously in the blood, is asso-ciated with a remittent rather than a continuous ever pattern. As aconsequence, our understanding o the ebrile response remainsincomplete and largely speculative. As noted, the ollowing are not yetclear: whether circulating cytokines cross the blood-brain barrier orhave to be produced within the central nervous system to activatethermosensitive neurons; whether each o the pyrogenic cytokines iscapable o raising the thermoregulatory setpoint independently ormust exert this eect through some fnal common pathway (see Fig.50-4); whether PGE2 or other local mediators are a sine qua non o theebrile response; what determines the magnitude o expression o indi-
Exogenous pyrogen
Temperature-dependent
feedback oncytokine
expression
Activatedleukocytes
IL-6
IL-6
Pyrogenic cytokines(IL-1, TNF-, IFN-)
Circumventricular organs
PGE2
Fever
103 F
igu 50-4 Hypothetical model or the ebrile response. (FromMackowiak PA. Concepts of fever. Arch Intern Med. 1998;158:1870-1881.)
Neuroendocrine Changes
Fever, somnolence, and anorexiaIncreased secretion o corticotropin-releasing hormone, corticotropin, and
cortisolIncreased secretion o arginine vasopressinDecreased production o insulin-like growth actor IIncreased adrenal secretion o catecholamines
Hematooietic ChangesAnemia o chronic diseaseLeukocytosisThrombocytosis
Metabolic Changes
Loss o muscle and negative nitrogen balanceDecreased gluconeogenesisOsteoporosisIncreased hepatic lipogenesisIncreased lipolysis in adipose tissueDecreased lipoprotein lipase activity in muscle and adipose tissueCachexia
Heatic Changes
Increased metallothionein, inducible nitric oxide synthase, heme oxygenase,manganese superoxide dismutase, and tissue inhibitor ometalloproteinase-1
Decreased phosphoenolpyruvate carboxykinase activity
Changes in Nonprotein Plasma Constituents
Hypozincemia, hypoerremia, and hypercupremiaDecreased plasma retinol concentrationsIncreased plasma glutathione concentrations
From Gabay C, Kushner I. Acute-phase proteins and other systemic responses toinammation.N Engl J Med. 1999;340:448-454. Copyright 1999 MassachusettsMedical Society. All rights reserved.
TABLE
50-1 Acut-Phas Physiologic ractions
-
7/28/2019 Fiebre Mandell.7
7/14
50 Temperature Regulation and the Pathogenesis o Fever 77
play important roles in modulating inammation. However, the untional capacity o such proteins is broad. There is also a growing literture concerned with the acute-phase protein LPS-binding proteiwhich appears both to enhance and neutralize the biologic activio LPS through its interaction with the CD14 receptor omacrophages.115
Although closely associated with ever, the acute-phase response not an invariable component o the ebrile response.101 Some ebripatients (e.g., those with certain viral inections) have normal bloo
levels o CRP. Moreover, patients with elevated blood levels o CRare not always ebrile. The acute-phase response, like the ebriresponse, is a complex response consisting o numerous integratethough separately regulated, components. The particular componenexpressed in response to a given disease process more than likely reethe specifc cytokines induced by the disease.
endognous AntipyticsHippocrates maintained that heat is the immortal substance o liendowed with intelligence. However, heat must also be rerigerateby respiration and kept within bounds i the source or principle o liis to persist; or i rerigeration is not provided, the heat will consumitsel.116 Modern-day clinicians also generally subscribe to the notiothat the ebrile range has an upper limit but do not agree on a precis
temperature defning this limit.52
The lack o a consensus in this regaris understandable, because body temperature profles exhibit consideable individual, anatomic, and diurnal variability. Thus, the upplimit o the ebrile range cannot be defned as a single temperaturapplicable to all body sites o all people at all times during the daNevertheless, the ebrile response is a regulated physiologic responsin which the temperature is maintained within a specifc range, thupper limit o which almost never exceeds 41 C in adult humanregardless o the cause o the ever or the site at which the temperatumeasurement is taken.117 The physiologic necessity o this upper limis supported by considerable experimental data demonstrating adverphysiologic consequences o core temperatures higher than 42 (107.6 F).118
The mechanisms regulating evers upper limit have yet to be ulelucidated. They could lie with the intrinsic properties o the neuron
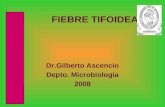
themselves or involve the release o endogenous antipyretic substancthat antagonize the eects o pyrogens on thermosensitive neuronWith regard to the ormer possibility, plots o the fring rates oneurons coordinating thermoregulatory responses and heat prodution tend to converge at 42 C (107.6 F; Fig. 50-5).118 At this temperture, the sustained fring rates o warm-sensitive neurons reach thezenith and cannot be increased urther in response to higher tempertures. Similarly, the fring rates o cold-sensitive neurons reach thenadir at 42 C (107.6 F) and cannot decrease urther, even i the temperature continues to increase. Thus, regardless o the pyrogen concentration, thermosensitive neurons appear to be incapable oproviding additional thermoregulatory signals once the temperatureaches 42 C (107.6 F).
These same thermosensitive neurons are inuenced by variouendogenous substances, at least some o which appear to unction aendogenous antipyretics.118 One such substance is arginine vasopresin. Studies rom several laboratories using various animal modehave established that arginine vasopressin is present in the fbers anterminals o the ventral septal area o the hypothalamus, is releaseinto the ventral septal area during ever, reduces ever by its action type 1 vasopressin receptors when introduced into the ventral septarea, and, when inhibited, prolongs ever.119-121
Melanocyte-stimulating hormone (-MSH) is another neuropeptide exhibiting endogenous antipyretic activity.122 Unlike some the other antipyretic peptides, -MSH has not been identifed in fbeprojecting into the dorsolateral septal area.123 It does, neverthelesreduce pyrogen-induced ever when administered to experimentanimals in doses below those aecting the basal body temperature.124-
When given centrally, -MSH is more than 25,000 times more poten
cells are cleared rom the host. Such activities are most likely potenti-ated by CRP-induced production o inammatory cytokines107 andtissue actor108 by monocytes. Nevertheless, the ultimate unction oCRP is uncertain, in that several in vivo studies have shown it to haveanti-inammatory properties.109-111
Another major human acute-phase protein, serum amyloid A, hasbeen reported to potentiate adhesiveness and chemotaxis o phagocyticcells and lymphocytes.112 There is also evidence that macrophages bearspecifc binding sites or serum amyloid A; serum amyloid Arich,high-density lipoproteins mediate the transer o cholesterol to mac-rophages at sites o inammation;113 and serum amyloid A enhanceslow-density lipoprotein oxidation in arterial walls.114
Complement components, many o which are acute-phase reac-tants, induce pyrogenic cytokines and PGE2; modulate chemotaxis,opsonization, vascular permeability, and vascular dilation; and havecytotoxic eects.101 Haptoglobin, hemopexin, and ceruloplasmin areall antioxidants. It is thereore reasonable to assume that, like theantiproteases 1-antichymotrypsin and C1-esterase inhibitor, they
proteins Whose plasma Concentrations Increase
Complement systemC3C4C5C9MACFactor BC1 inhibitorC4b-binding proteinMannose-binding lectin
Coagulation and fbrinolytic systemFibrinogenPlasminogenTissue plasminogen activatorUrokinaseProtein SVitronectinPlasminogen-activator inhibitor IKininogen
Antiproteases1-Protease inhibitor1-AntichymotrypsinPancreatic secretory trypsin inhibitorInter--trypsin inhibitors
Transport proteins
CeruloplasminHaptoglobinHemopexin
Participants in inammatory responsesSecreted phospholipase A2Lipopolysaccharide-binding proteinInterleukin-1 receptor antagonistGranulocyte colony-stimulating actor
OthersC-reactive proteinSerum amyloid A1-Acid glycoproteinFibronectinFerritinAngiotensinogen
proteins Whose plasma Concentrations Decrease
AlbuminTranserrin
Transthyretin2-HS glycoproteinAlpha-etoproteinThyroxine-binding globulinInsulin-like growth actor IFactor XIIRetinol-binding protein
Adapted rom Gabay C, Kushner I. Acute-phase proteins and other systemicresponses to inammation.N Engl J Med. 1999;340:448-454. Copyright 1999Massachusetts Medical Society. All rights reserved.
TABLE
50-2 Human Acut-Phas Potins
-
7/28/2019 Fiebre Mandell.7
8/14
772 PART II Major Clinical Syndromes
in the appropriate physiologic milieu, pyrogenic cytokines unction
paradoxically as endogenous antipyretics.A growing body o literature has indicated that the release o pyro-genic cytokines such as IL-1 is ollowed by increased shedding osoluble receptors or such cytokines, which unction as endogenousscavengers o these pyrogens.148 In the case o IL-1, a 22- to 25-kDamolecule identifed in supernates o human monocytes blocks bindingo IL-1 to its receptors.149 The IL-1 receptor antagonist is structurallyrelated to IL-1 and IL-1150 and binds to types I and II receptors onvarious target cells without inducing a specifc biologic response.151,152Shedding o soluble receptors o TNF- that bind to circulating TNF-and thereby inhibit binding to cell-associated receptors has also beendescribed.153-157 The precise biologic unction o such circulating recep-tor antagonists and soluble receptors is not known. However, it ispossible that one unction is to serve as a natural braking system orthe ebrile response.
risk-Bnft ConsidationsQuestions concerning evers risk-beneft quotient have generatedconsiderable controversy.158 The controversy arises because o dataindicating both potentiating and inhibitory eects o the response onresistance to inection. As a result, there is as yet no consensus as tothe appropriate clinical situations (i any) in which ever or its media-tors should be suppressed.
Evidence illustrating evers benefcial eects originate rom severalsources. Studies o the phylogeny o ever have shown the response tobe widespread within the animal kingdom.159 With ew exceptions,mammals, reptiles, amphibians, and fsh, as well as several invertebratespecies, have been shown to elevate their core temperature in response
as an antipyretic than acetaminophen.122 Repeated central administra-
tion o-MSH does not induce tolerance to its antipyretic eect.
129
Inaddition, injection o anti-MSH antiserum into the cerebral ven-tricles has augmented the ebrile response o experimental animals toIL-1.130
Glucocorticoids and their inducers (e.g., corticotropin-releasinghormone [CRH] and corticotropin) inhibit the synthesis o pyrogeniccytokines such as IL-6 and TNF-.131-133 Through such eects, they arebelieved to exert inhibitory eedback on LPS-induced ever.134 Lipo-cortin 1, a putative mediator o glucocorticoid unction, has also beenshown to inhibit the pyrogenic actions o IL-1 and IFN.135 Injection oCRH into the third ventricle o experimental animals produces similarantipyretic eects.136
Thyrotropin-releasing hormone,137 gastric-inhibitory peptide,138neuropeptide Y,139 nitric oxide,140 carbon monoxide,141 and bombe-sin142 similarly exhibit antipyretic properties under certain conditions.O these, bombesin has exhibited the highest potency in that it consis-tently produces hypothermia associated with changes in heat dissipa-tion and heat production when injected into the preoptic area oranterior hypothalamus o conscious goats and rabbits.142-144 Bombesinis believed to exert its hypothermic eect by decreasing the sensitivityo warm-sensitive neurons.144
IL-10 has been shown to mediate deervescence o ever evoked byboth LPS-induced and Staphylococcus aureusinduced inammationin rats.145 Moreover, pyrogenic cytokines, the mediators o the ebrileresponse, might themselves have a role in determining evers upperlimit, in that under certain conditions (e.g., with intracerebral injec-tion o recombinant human TNF- in Zucker rats), TNF- acts tolower rather than raise body temperature,146,147 although only in thepresence o LPS. Thus, it is possible that at certain concentrations or
Th 37 C 42 C
FR
Th 37 C 42 C
FR
Th 37 C 42 C
Heat
production
N
N
N
P1
P2
P1
P1
P2
P2
Maximum
Pyrogen
A
B
C
w
c
igu 50-5 Model showing responses (A, B) o the neuronal fringrate (FR) in the preoptic region and anterior hypothalamus andwhole-body metabolic heat production (C) during changes in hypo-thalamic temperature (Th). Thermosensitivity is refected by the slopeo each plot. The letters inside the cells indicate a warm-sensitive (w)neuron and cold-sensitive (c) neuron. With increases in T h, warm-sensitive neurons raise their FRs and heat production decreases. Pyro-gens inhibit () the FRs o warm-sensitive neurons, thereby resulting inaccelerated FRs o cold-sensitive neurons and increased heat produc-tion. The plots show FR and heat production responses during normalconditions in the absence o pyrogens (N) and in the presence o lowconcentrations (P1) and high concentrations (P2) o pyrogens. (FromMackowiak PA, Boulant JA. Fevers glass ceiling. Clin Inect Dis.1996;22:525-536.)
Mammalia
Aves
Reptilia
Amphibia
Pisces
Crustacea
Chelicerata
Insecta
Hirudinea
Gastropoda
Arthropoda
Vertebrata
Chordata
Urochordata
Aechinodermata
Brachiopoda
Ectoprocta
Phoronidea
Sipunculida
Coelenterata
Ctenophora
ANIMALIA
Annelida
Mollusca
Platyhelminthes
igu 50-6 Evolutionary tree o animals. A ebrile response hasbeen documented in the Vertebrata, Arthropoda, and Annelida. Theseobservations suggest that the ebrile response evolved more than400,000,000 years ago at about the time that evolutionary lines leadingto arthropods and annelids diverged.
-
7/28/2019 Fiebre Mandell.7
9/14
50 Temperature Regulation and the Pathogenesis o Fever 77
might theoretically enhance resistance to inection.84,182 In vitro and vivo investigations o these cytokines have provided evidence o protective eect o IFN, TNF-, or IL-1, or all o these, against Plamodium,183-185Toxoplasma gondii,186Leishmania major,187Trypanosomcruzi,188 and Cryptosporidium.189
Several reports have also shown enhancement o resistance tviral190-192 and bacterial inections193,194 by pyrogenic cytokines. Treament o normal and granulocytopenic animals with IL-1 has beeshown to prevent death in some gram-positive and gram-negativ
bacterial inections.194 However, IL-1 is eective only i administerean appreciable time (e.g., 24 hours) beore the initiation o inectionhaving rapidly atal courses. In less acute inections, IL-1 administration can be delayed until shortly ater the inectious challenge. Sucobservations suggest that those physiologic eects o the ebriresponse that enhance resistance to inection might be limited to locaized inections or systemic inections o only mild to moderaseverity.
The ebrile responses potential or harm was reected in a urry oreports suggesting that IL-1, TNF-, IL-6, and IFN mediate the physologic abnormalities o certain inections. Although proo o aadverse eect o ever on the clinical outcome o these inections hyet to be established, the implication is that i pyrogenic cytokincontribute to the pathophysiologic burden o inections, both thmediators themselves and the ebrile response are potentially deleter
ous. The most persuasive evidence in this regard derives rom studio gram-negative bacterial sepsis.195 It has long been suspected thbacterial LPS is involved in the pathophysiology o the syndromPurifed LPS induces a spectrum o physiologic abnormalities similto those occurring in patients with gram-negative bacterial sepsis. Iexperimental animals, challenge with LPS causes TNF- and IL-1 be released into the bloodstream coincident with the appearance osigns o sepsis.196 Furthermore, patients with the septic syndrome havdetectable levels o circulatory TNF-, IL-1, and IL-6 independent oculture-documented inection, and these levels correlate inversely witsurvival.197 IL-1, alone or in combination with other cytokines, inducmany o the same physiologic abnormalities (e.g., ever, hypoglycemishock, and death) seen ater the administration o purifed LPS.198
a murine experimental model or septic shock, IFN administerebeore or as long as 4 hours ater LPS challenge increases mortalit
whereas pretreatment with anti-IFN antibody signifcantly reducmortality.199 In several investigations, the adverse eects o gramnegative bacterial sepsis, LPS injections, or both, have been attenuateby pretreating experimental animals with IL-1 antagonists200,201 anmonoclonal antibodies directed against TNF-.202,203 Furthermoranimals rendered tolerant to TNF- by repeated injections o threcombinant cytokine are protected against the hypotension, hypothermia, and lethality o gram-negative bacterial sepsis.204
The theory derived rom these observationsthat death rom sepsis the consequence o cytokine-mediated overstimulation o thimmune systemunortunately correlates only loosely with thclinical picture in humans, most likely because the studies cited uselarge doses o endotoxin or bacteria that induced levels o circulatinpyrogenic cytokines exponentially higher than those detected ipatients with sepsis.205 Thus, the cytokine storm created in sucanimals most likely has only limited relevance or human sepsis. Thperhaps explains why in clinical trials, inhibition o pyrogenic cytokines in septic patients has had only modest success, improvinoutcome in patients with a high risk or death but not those with a lorisk.206
Antipytic ThapyAlthough clinicians have long had at their disposal eective means olowering the core temperature in ebrile patients, the actual beneft osuch reductions in temperature is still uncertain. Moreover, it has yto be shown in humans that increases in the core temperature encountered during ever are actually harmul. Certainly, during the couro heat stroke and other orms o hyperthermia, the core temperatur
to a challenge with microorganisms or other known pyrogens (Fig.50-6). It has been assumed, although not established conclusively, thatsuch elevations in temperature are the poikilothermic corollary oever. The prevalence o such ebrile responses has been oered assome o the strongest evidence that ever is an adaptive response, basedon the argument that the metabolically expensive increase in bodytemperature that accompanies the ebrile response would not haveevolved and been so aithully preserved in the animal kingdom unlessever had some net beneft to the host.
Further evidence o evers benefcial eects can be ound in numer-ous investigations demonstrating enhanced resistance o animals toinection with increases in body temperature within the physiologicrange.159 In classic studies involving experimental inection o thereptile Dipsosaurus dorsalis with Aeromonas hydrophila, Kluger andassociates demonstrated a direct correlation between body tempera-ture and survival.160,161 They also showed in their model that suppres-sion o the ebrile response with sodium salicylate is associated with asubstantial increase in mortality.161 Covert and Reynolds corroboratedthese fndings in an experimental model involving goldfsh.162
In mammalian experimental models, increasing the body tempera-ture by artifcial means has been reported to enhance the resistance omice to herpes simplex virus,163 poliovirus,164 coxsackie B virus,165rabies virus,166 and Cryptococcus neoormans167 but to decrease resis-tance to Streptococcus pneumoniae.168 Increased resistance o rabbits to
S. pneumoniae169
and C. neoormans,170
dogs to herpesvirus,171
pigletsto gastroenteritis virus,172 and errets to inuenza virus173 has also beenobserved ater the induction o artifcial ever. Unortunately, becauseraising the body temperature by artifcial means does not duplicate thephysiologic alterations that occur during ever in homeotherms (and,indeed, entails a number o opposite physiologic responses174), evi-dence obtained using mammalian experimental models must be inter-preted with caution when used to understand the ebrile response.
Clinical data supporting an adaptive role or ever have accumulatedslowly. Like animal data, clinical data include evidence o the benefcialeects o ever and adverse eects o antipyretics on the outcome oinections. In a retrospective analysis o 218 patients with gram-nega-tive bacteremia, Bryant and associates reported a positive correlationbetween maximal temperature on the day bacteremia was diagnosedand survival.175 A similar relationship has been observed in patients
with polymicrobial sepsis and mild (but not severe) underlying dis-eases.176 In an examination o actors inuencing the prognosis ospontaneous bacterial peritonitis, Weinstein and co-workers identifeda positive correlation between a temperature reading higher than 38 C(100.4 F) and survival.177
It has been reported that children with chickenpox who are treatedwith acetaminophen have a longer time to total crusting o lesions thanplacebo-treated controls.178 Stanley and colleagues have reported thatadults inected with rhinovirus exhibit more nasal viral shedding whenthey receive aspirin than when given placebo.179 Furthermore, Grahamand colleagues have reported a trend toward a longer duration orhinovirus shedding in association with antipyretic therapy and haveshown that the use o aspirin or acetaminophen is associated withsuppression o the serum-neutralizing antibody response and withincreased nasal symptoms and signs.180 A more recent retrospectiveobservational analysis o studies o human volunteers inected withinuenza A has ound a relationship between antipyretic therapy andprolonged illness.181 These data, like those reviewed earlier, are subjectto several interpretations and do not prove a causal relationshipbetween ever and improved prognosis during inection. Nevertheless,they are consistent with such a relationship and, when considered inconcert with the phylogeny o the ebrile response and the animal datasummarized earlier, constitute strong circumstantial evidence thatever is an adaptive response in most situations.
Whereas many o the oregoing investigations examined the rela-tionship between elevation o the core temperature and outcome oinection, others have considered the endogenous mediators o theebrile response. In such studies, all the principal pyrogenic cytokineshave been shown to have immune-potentiating capabilities, which
-
7/28/2019 Fiebre Mandell.7
10/14
774 PART II Major Clinical Syndromes
only 10% as potent in this regard as indomethacin. Acetaminophenselectively inhibits a third COX variant, a close relative o COX-1derived rom the same gene and reerred to as COX-3.217 The impor-tance o the discovery o COX-3 is that it explains the pharmacologicactions o acetaminophen and other antipyretic analgesic drugs, whichare weak inhibitors o COX-1 and COX-2 but penetrate easily into thecentral nervous system. NSAIDs such as dicloenac or ibuproen arealso potent inhibitors o COX-3 expressed in cultured cells but, beinghighly polar, are unlikely to reach brain COX-3 in eective concentra-
tions.218 Only aspirin irreversibly inhibits COX via acetylation withinthe active site o the enzyme. Other NSAIDs and acetaminopheninhibit COX reversibly.219
Studies have shown that aspirin and the NSAIDs also have COX-independent antipyretic activity. Aspirin induces cytochrome P-450,which might augment its antipyretic eect by shiting arachidonic acidmetabolism toward cytochrome P-450mediated production o anti-pyretic epoxyeicosanoids. Additionally, acetylation o COX-2 byaspirin increases the production o 15R-hydroxyeicosatetraenoic acid,which neutrophils use to orm aspirin-triggered lipoxins. These lipox-ins have potent anti-inammatory activity independent o aspirin.Heat shock proteins have been shown to reduce the transcription oIL-1B in vitro, and therapeutic doses o aspirin and certain NSAIDsincrease heat shock actor 1 concentration in vitro. These same drugsalso diminish the activity o transcriptional activator nuclear actor
kappa B (NF-B),219
which is involved in the transcription o pyro-genic cytokines, adhesion molecules, inducible nitric oxide synthase,and COX-2 in certain cell lines. Production o adenosine, an anti-inammatory mediator produced by leukocytes, is enhanced by aspirinand NSAIDs. The clinical implications o these alternative antipyreticpathways remain to be determined.
PHYSICAL METHODS OF ANTIPYRESIS
Various physical techniques are used to cool ebrile patients. Theseinclude sponging with various solutions (e.g., tepid water or alcohol),the application o ice packs or cooling blankets, and exposure to cir-culating ans (most oten in conjunction with sponging). With thelatter method, Helox (80% helium, 20% oxygen) has been shown tobe superior to air in lowering core temperature, at least in experimen-
tal animals, because o the greater thermal conductivity o heliumcompared with that o nitrogen.220 In contrast to antipyretic drugs,external cooling lowers the temperature o ebrile patients by over-whelming eector mechanisms that have been evoked by an elevatedthermoregulatory setpoint, rather than by lowering that setpoint.Thereore, unless concomitant antipyretic agents are used, or shiveringis inhibited by other pharmacologic means, external cooling is vigor-ously opposed in the ebrile patient by thermoregulatory mechanismsendeavoring to maintain the elevated body temperature.
Physical methods o antipyresis promote heat loss by conduction,convection, and evaporation. Evaporative methods have traditionallybeen touted as the most eective physical means o promoting heatloss in ebrile patients, because these methods are deemed to be leastlikely to induce shivering.221 However, careully designed comparativetrials have not yet established any one physical method o antipyresisas superior.
Similarly, direct comparisons o pharmacologic and physicalmethods o antipyresis are all but nonexistent. In the only extant con-trolled study, Wenzel and Werner reported that salicylates reduced thesecond phase o endotoxin-induced ever in rabbits, whereas abdomi-nal cooling increased heat production and did not lower the coretemperature unless the animals were simultaneously exposed to envi-ronmental hyperthermia.222 Neither antipyretic modality abolished theinitial ebrile response.
The ew available clinical studies o the efcacy o physical methodso antipyresis have diered in their conclusions. Interpretation o theresults o these studies has been difcult, because pharmacologicagents have almost invariably been administered concomitantly withexternal cooling. Steele and co-workers ound acetaminophen (in age-
can, and requently does, rise to levels that are inherently harmul. 207However, as noted, such levels are almost never reached during eversregulated rise in temperature, which probably never exceeds 41 C(105.8 F) in humans.118 Nevertheless, whereas healthy volunteers havebeen reported to withstand core temperatures o 42 C (107.6 F) orperiods o as long as 4 hours without apparent ill eects,208 the possibil-ity remains that in certain patients, even the relatively modest increasesin core temperature encountered during ever are deleterious andshould thereore be suppressed.
One such category o patients includes children, primarily thosebetween the ages o 3 months and 5 years. In such children, seizureshave been reported to occur during episodes o ever at a requency ashigh as 14% in select populations.209 Although most children withebrile seizures have temperatures o 39 C (102.2 F) or higher at thetime o their seizure,210 many tolerate even higher evers at later dateswithout convulsing.211 Unortunately, antipyretic therapy has not beenshown to protect against recurrences o ebrile seizures in the ewcontrolled trials conducted thus ar (see later).212
It has also been suggested that patients with underlying cardiovas-cular or pulmonary disorders might be especially susceptible to theadverse eects o ever because o metabolic demands imposed by theelevated temperature.213 Such demands are particularly high duringthe chill phase i shivering is present, as evidenced by increases in thesympathetic tone,174 oxygen consumption, respiratory minute volume,
and respiratory quotient.214
As a result o the associated increase inmetabolic demand, the chill phase o ever might be expected to addto the burden o cardiac or pulmonary disorders. Although this pos-sibility has been oered as justifcation or antipyretic therapy inpatients with these disorders, the risk-beneft ratio o such therapy hasyet to be determined.
Antipyretic therapy might also be justifed, at least in theory, ievers physiologic beneft exceeded its metabolic cost, i the treatmentprovided symptomatic relie without adversely aecting the course othe ebrile illness, or i the toxicity (side eects) o the antipyreticregimen were appreciably lower than its benefcial eects. Unortu-nately, although clinicians have long argued the validity o each othese propositions as justifcation or antipyretic therapy, ew scientifcdata exist to support any o these arguments.
Antipyretic drugs can be grouped into three general categories on
the basis o their mechanisms o action. These include corticosteroids,aspirin and the other nonsteroidal anti-inammatory drugs (NSAIDs),and acetaminophen. Each exerts its eects at dierent points in theebrile response pathway.
Although not generally used or antipyresis, corticosteroids suppressever through direct and indirect mechanisms. They block the tran-scription o pyrogenic cytokines and inducible COX via interactionsinvolving the glucocorticoid receptor.73,215 They downregulate the syn-thesis o cytokine receptors and, by inducing lipocortin-1, they sec-ondarily inhibit the activity o phospholipase A2, a critical enzyme inthe prostaglandin synthetic pathway.215
Acetaminophen and aspirin and the other NSAIDs all inhibit COX-mediated synthesis o inammatory thromboxanes and prostaglandinsrom arachidonic acid. Cyclooxygenase has at least two distinct iso-orms, COX-1 and COX-2. The ormer was long regarded as a consti-tutively expressed cellular enzyme involved in various housekeepingunctions, whereas the latter was touted as an inducible enzymeresponsible or hypothalamus-mediated ever and produced as part othe inammatory process by various cell lines, including macrophages,synoviocytes, and endothelial cells. However, this dichotomousconcept o a constitutive COX-1 and an inducible proinammatoryCOX-2 has proved to be oversimplifed. Not only do some cells expressCOX-2 constitutively but, under certain conditions, COX-2 has alsobeen shown to promote healing o mucosal lesions and resolution oinammation.216
The distinctive afnities o the various categories o antipyreticdrugs or the dierent COX variants are thought to determine theirrelative antipyretic and analgesic potencies. Acetaminophen andaspirin, or example, are equally potent inhibitors o central COX but
-
7/28/2019 Fiebre Mandell.7
11/14
-
7/28/2019 Fiebre Mandell.7
12/14
776 PART II Major Clinical Syndromes
cardiovascular and pulmonary disorders, and possibly prevent or alle-viate ever-induced mental dysunction in older patients. To minimizeantipyretic-induced uctuations in temperature, as well as the risk orrecurrent shivering with its associated increased metabolic demands,antipyretic agents should be administered to ebrile patients at regularintervals that preclude abrupt recurrences o ever, rather than asneeded or temperatures above some arbitrary level. Whenever suchmedications are prescribed, it should also be recognized that eachcarries its own risk or toxicity and might prolong the course o the
illness responsible or the ever while reducing the intensity o itssymptoms.
In view o the capacity o external cooling measures to induce a coldpressor response, it is questionable whether this orm o antipyretictherapy should ever be administered to ebrile patients, much less tointensive care unit patients or whom it is so requently prescribed. Iexternal cooling is used to treat ever, care must be taken to preventshivering because o its associated increased oxygen consumption.Unortunately, even i shivering is prevented, there is no guarantee thata cold pressor response will be averted. In view o indomethacinscapacity to cause coronary vasoconstriction in patients with coronaryartery disease and the possible increased risk or cardiovascular throm-botic events associated with COX-2selective NSAIDs, it should beused cautiously to suppress ever in such patients.
hours o IV therapy with the COX inhibitor ibuproen lowered thecore temperature, heart rate, oxygen consumption, and lactic acidblood levels but did not decrease the incidence o organ ailure ormortality at 30 days.251 In a more recent retrospective analysis o sepsistrials, Eichacker and co-workers ound evidence o a benefcial eecto antipyretic agents only in septic patients with a high risk or death(see earlier).206 Thus, in spite o promising results obtained in someexperimental models, antipyretic agents have been shown to be o onlylimited value clinically or the treatment o bacterial sepsis.
INDICATIONS
Although clinicians have long resorted to various orms o antipyretictherapy, there is a dearth o scientifc data concerning the actual ben-efts and relative risks o such treatments.252 Nevertheless, several tenta-tive conclusions regarding antipyretic therapy seem warranted in lighto the limited data available. It is clear, or example, that short courseso approved doses o standard antipyretic drugs carry a low risk ortoxicity. Most o these drugs have analgesic as well as antipyretic prop-erties. Thereore, i not otherwise contraindicated (e.g., aspirin inyoung children because o the risk or Reyes syndrome), such drugscan be prescribed to provide symptomatic relie in ebrile patients,reduce the metabolic demands o ever in patients with underlying
reereNCeS1. Majno G. The Healing Hand: Man and Wound in the Ancient
World. Cambridge, Mass: Harvard University Press; 1975:57.2. Galen. Opera omnia. In: Siegel RE, ed. Galens System o Physiol-
ogy and Medicine, vol 11. New York: Karger; 1968.3. Atkins E. Fever: Its history, cause and unction. Yale J Biol Med.
1982;55:283-287.4. Berger RL, Clem TR, Harden VA, et al. Historic al development
and newer means o temperature measurements in biochemis-try.Methods Biochem Anal. 1984;30:269-331.
5. Bolton HC. Evolution o the Thermometer 1592-1743. Easton, Pa:Chemical; 1900:18, 98.
6. Wunderli ch C. Das Verhalten der Eigenwrme in Krankenheiten.Leipzig, Germany: Otto Wigard; 1868.
7. Mackowiak PA, Worden G. Carl Reinhold August Wunderlichand the evolution o clinical thermometry. Clin Inect Dis.1994;18:458-467.
8. Commission or Thermal Physiology o the International Uniono Physiological Sciences (IUPS Thermal Commission). Glos-sary o terms or thermal physiology. 3rd ed. Japanese J Physiol.
2001;51:245-280.9. Bouchama A, Knochel JP. Heat stroke. N Engl J Med.2002;346:1978-1988.
10. Benzinger M, Benzinger TH.National Bureau o Standards FithSymposium on Temperature. Pittsburgh, Pa: Instrument Societyo America. 1971:2080-2102.
11. Blainey CG. Site selection in taking body temperature. Am JNurs. 1974;74:1859-1861.
12. Lorin MI. Measurement o body temperature. Semin PediatrInect Dis. 1993;4:4-8.
13. Buck SH, Zaritsky AL. Occult core hyperthermia complicatingcardiogenic shock. Pediatrics. 1989;83:782-783.
14. Houdas Y, Ring EFJ. Human Body Temperature. New York:Plenum; 1982:57-141.
15. Mayfeld SR, Bhatia J, Nakamura KT, et al. Temperaturemeasurement in term and preterm neonates. J Pediatr.1984;104:271-275.
16. Fonkalsrud E, Clathworthy HW. Accidental peroration othe colon and rectum in newborn inants. N Engl J Med.1965;272:1097-1100.
17. Horwitz MA, Bennett JV. Nursery outbreak o peritonitis withpneumoperitonium probably caused by thermometer-induced
peroration.Am J Epidemiol. 1976;104:632-644.18. McAllister TA, Roud JA, Marshall A, et al. Outbreak oSalmo-nella eimsbuettelin newborn inants spread by rectal thermom-eters. Lancet. 1986;1:1262-1264.
19. Rabinowitz RP, Cookson ST, Wasserman SS, et al. Eects oanatomic site, oral stimulation and body position on estimateso body temperature.Arch Intern Med. 1996;156:777-780.
20. Tandberg D, Sklar D. Eect o tachypnea on the estimationo body temperature by an oral thermometer. N Engl J Med.1983;308:945-946.
21. Ne J, Ayoub J, Longman A, Noyes A. Eect o respi ratory ra te,respiratory depth, and open versus closed mouth breathing onsublingual temperature. Res Nurs Health. 1989;12:195-202.
22. Klein DG, Mitchell C, Petrinec A, et al. A comparison o pulmo-nary artery, rectal, and tympanic membrane temperature mea-surements in the ICU. Heart Lung. 1993;22:435-441.
23. Erickson RA, Kirklin SK. Comparison o ear-based, bladder, oraland axillary methods or core temperature measurement. CritCare Med. 1993;21:1528-1534.
24. Giuliano KK, Scott SS, Elliot S, et al. Temperature measure-ments in critically ill orally intubated adults: A comparison opulmonary artery core, tympanic, and oral methods. Crit CareMed. 1999;27:2188-2193.
25. Modell JG, Katnoli CR, Kumaramangalam SM, et al. Unreli-ability o the inrared t ympanic thermometer in clinical practice:A comparative study with oral mercury and oral electronic ther-mometers. South Med J. 1998;91:649-654.
26. Peterson-Smith A, Barber N, Coody DK, et al. Comparison oaural inrared with traditional rectal temperatures in childrenrom birth to age three years. J Pediatr. 1994;125:83-85.
27. Buntain WI, Pregler M, OBrien PC, et al. Axillary versus rectaltemperature: A comparative study. J Louisiana State Med Soc.1977;129:5-8.
28. Schiman RF. Temperature monitoring in the neonate: Acomparison o axillary and rectal temperatures. Nurs Res.1982;31:274-277.
29. Loudon ISL. On taking the temperature in the mouth and axilla.Lancet. 1957;268:233-235.
30. Nichols GA, Kulvi RL, Lie HR, et al. Measuring oral and rectaltemperatures o ebrile children. Nurs Res. 1972;21:261-264.31. Ogren JM. The inaccuracy o axillary temperatures measured
with an electronic thermometer. Am J Dis Child. 1990;144:109-111.
32. Reisinger KS, Kao J, Grant DM. Inaccuracy o the Clinitemp skinthermometer. Pediatrics. 1979;64:4-6.
33. Scholefeld JH, Gerber MA, Dwyer P. Liquid crystal oreheadtemperature strips.Am J Dis Child. 1982;136:198-201.
34. Bergeson PS, Stieneld HJ. How dependable is palpation as ascreening method or ever? Clin Pediatr. 1974;13:350-351.
35. Banco L, Veltri D. Ability o mothers to subjectively assessthe presence o ever in their children. Am J Dis Child.1984;138:976-978.
36. Bonadio WA, Hegenbarth M, Zachariason M. Correlatingreported ever in young inants with subsequent temperaturepatterns and rate o serious bacterial inections. Pediatr InectDis J. 1990;9:158-160.
37. Linder FE, Carmichael HY. A biometric study o the relationbetween oral and rectal temperatures in normal and schizo-phrenic subjects. Hum Biol. 1935;7:24-46.
38. Tanner JM. The relationship between the requency o the heart,
oral temperature and rectal temperature in man at rest.J Physiol.1951;115:391-409.39. Togawa T. Body temperature measurement. Clin Phys Physiol
Meas. 1985;6:83-108.40. Anagnostakis D, Matsaniotis N, Graakos S, et al. Rectal-axillary
temperature dierence in ebrile and aebrile inants and chil-dren. Clin Pediatr. 1993;32:268-272.
41. Wunder lich KRA, Seguin E. Medical Thermometry and HumanTemperature. New York: William Wood; 1871.
42. Howell TH. Normal temperature in old age. Lancet. 1948;1:517-518.
43. Weitzman ED, Moline ML, Czeisler CA, et al. Chronobiology oaging: Temperature, sleep-wake rhythms, and entrainment.Neurobiol Aging. 1982;3:299-309.
44. Jones SR. Fever in the elderly. In: Mackowiak PA, ed.Fever: BasicMechanisms and Management. New York: Raven Press;1991:233-242.
45. Mackowiak PA, Wasserman SS, Levine MM. A critical appraisalo 98.6 F, the upper limit o the normal body temperature, and
other legacies o Carl Reinhold August Wunderlich. JAMA.1992;268:1578-1580.
46. Dinarello CA, Wol SM. Pathogenesis o ever in man.N Engl JMed. 1978;298:607-612.
47. Stephenson LA. Circadian timekeeping. In: Mackowiak PA, ed.Fever: Basic Mechanisms and Management. 2nd ed. Philadelphia:Lippincott-Raven; 1997:59-77.
48. Avery DH, Shah SH, Eder DN, et al. Nocturnal sweatingand temperature in depression. Acta Psychiatric Scand.1999;100:295-301.
49. Webb P. Daily activit y and body temperature. Eur J Appl Physiol.1993;66:174-177.
50. Okamoto-Mizuno K, Mizuno K, Michie S, et al. Eects o humidheat exposure on human sleep stages and bodytemperature. Sleep. 1999;22:767-773.
51. Cheng TL, Partridge JC. Eect o bundling and high environ-mental temperature on neonatal body temperature. Pediatrics.1993;92:238-240.
52. Mac kowiak PA, Wasserman SS . A study o physicians percep-
tions o body temperature in health and disease. South Med J.1995;88:934-938.53. Horvath SM, Menduke H, Piersol GM. Oral and rectal tempera-
tures o man.JAMA. 1950;144:1562-1565.54. Wunderlich CA, Woodman WB.On the Temperature in Diseases:
A Manual o Medical Thermometry. London: New SydenhamSociety; 1871:71.
55. Wunderlich CA, Reeve JC. The course o the temperature indiseases: A guide to clinical thermometry. Am J Med Sci.1869;57:425-447.
56. Tauber MG. Fever o unknown origin. In: Stein JH, ed. InternalMedicine. 3rd ed. Boston: Little Brown; 1990:1240-1246.
57. Lyon DM. The relation o pulse-rate to temperature in ebrileconditions. Q J Med. 1927;20:205-218.
58. Lorin MI. Fever: Pathogenesis and treatment. In: Feigin RD,Cherry JD, eds. Textbook o Pediatric Inectious Diseases. 4th ed.Philadelphia: Saunders; 1998:89.
59. Bayley N, Stolz HR. Maturational changes in rectal temperatureso 61 inants rom 1 to 36 months. Child Dev. 1937;8:195-206.
60. Boulant JA. Thermoregulation. In: Mackowiak PA, ed. Fever:Basic Mechanisms and Management. 2nd ed. Philadelphia: Lip-pincott-Raven; 1997:35-58.
61. Bruck K. Heat balance and the regulation o body temperature.In: Schmidt RF, Thews G, eds. Human Physiology. Berlin:Springer-Verlag; 1983:531-547.
62. S tanier MW, Mount LE, Bligh J. Energy Balance and Tempera-ture Regulation. Cambridge, England: Cambridge UniversityPress, 1984.
63. Boulant JA. Hypothalamic control o thermoregulation: Neuro-physiological basis. In: Morgane PJ, Pankepp J, eds. Handbooko the Hypothalamus, vol 3, pt A. New York: Marcel Dekker;1980:1-82.
64. Schonung W, Wagner H, Jessen C, et al. Dierentiation ocutaneous and intestinal blood ow during hypothalamicheating and cooling in anesthetized dogs. Pfugers Arch.1971;328:145-154.
65. Boulant JA. Neuronal basis o Hammelss model o set-pointthermoregulation.J Appl Physiol. 2006;100:1547-1554.
66. Hammel HT, Jackson DC, Stolwijk JAJ, et al. Temperature regu-lation by hypothalamic proportional control with an adjustableset point.J Appl Physiol. 1963;18:1146-1154.
-
7/28/2019 Fiebre Mandell.7
13/14
50 Temperature Regulation and the Pathogenesis o Fever 77
67. Hammel HT. Neurons and temperature regulation. In:Yamamoto WS, Brobeck JR, eds. Physiological Controls andRegulations. Philadelphia: WB Saunders; 1965:71-97.
68. Sawka MN, Wenger CB. Physiolog ical responses to acute exer-cise-heat stress. In: Pandol KB, Sawka MN, Gonzalez RR, eds.Human Perormance Physiology and Environmental Medicineat Terrestrial Extremes. Indianapolis, Ind: Benchmark;1988:97-151.
69. Bligh J. Temperature Regulation in Mammals and Other Verte-brates. Amsterdam: North Holland; 1973.
70. Benzinger TH, Kitzinger C, Pratt AW. The human thermostat .In: Hardy JD, ed. TemperatureIts Measurement and Control inScience and Industry, v. 3, pt. 5: Biology and Medicine. New York:
Reinhold; 1963:637-665.71. Stitt JT. Prostaglandin E as the mediator o the ebrile response.
Yale J Biol Med. 1986;59:137-149.72. Mitchell D, Laburn HP, Cooper KE, et al. Is prostaglandin E the
neural mediator o the ebrile response? The case against aproven obligatory role. Yale J Biol Med. 1986;59:159-168.
73. Dinarello CA. Cytokines as endogenous pyrogens. In: Mack-owiak PA, ed. Fever: Basic Mechanisms and Management. 2nded. Philadelphia: Lippincott-Raven; 1997:87-116.
74. Mickenberg ID, Snyderman R, Root RK, et al. The relationshipo complement consumption to immune ever. J Immunol.1971;107:1466-1476.
75. Arend WP, Joslin FG, Massoni RJ. Eects o immune complexeson production by human monocytes o interleukin 1 or aninterleukin 1 inhibitor.J Immunol. 1985;134:3868-3875.
76. Dillard GM, Bodel P. Studies on steroid ever. II. Pyrogenic andanti-pyrogenic activity in vitro o some endogenous steroids oman.J Clin Invest. 1970;49:2418-2426.
77. Kappas A, Hellman L, Fukushima DK, et al. The pyrogeniceect o etiocholanolone [letter]. J Clin Endocrinol Metab.1957;17:451-453.
78. Wol SM, Kimball HR, Perry S, et al. The biological propertieso etiocholanolone.Ann Intern Med. 1967;67:1268-1295.
79. Bondy PK, Bodel P. Mechanism o action o pyrogenic and anti-pyretic steroids in vitro. In: Wolstenholme GEW, Birch J, eds.Pyrogens and Fever. Edinburgh: Churchill Livingstone;1971:101-113.
80. Goodman MG, Chenoweth DE, Weigle WO. Induction o inter-leukin 1 secretion and enhancement o humoral immunity bybinding o human C5a to macrophage surace C5a receptors.J Exp Med. 1982;156:912-917.
81. Bernheim HA, Block LH, Francis L, et al. Release o endogenouspyrogen-activating actor rom concanavalin A-stimulatedhuman lymphocytes.J Exp Med. 1980;152:1811-1816.
82. Dinarello CA. Demonstration o a human pyrogen-inducingactor during mixed leukocyte reactions. J Exp Med. 1981;153:1215-1224.
83. Li Z, Blatteis CM. Fever onset is linked to the appearance olipopolysaccharide in the liver.J Endotoxin Res. 2004;10:39-53.
84. Mackowiak PA, Barlett JG, Borden EC, et al. Concepts oever: Recent advances and lingering dogma. Clin Inect Dis.1997;25:119-138.
85. Kushner I, Rzewnicki DL. The acute phase response. In: Mack-owiak PA, ed. Fever: Basic Mechanisms and Management. 2nded. Philadelphia: Lippincott-Raven; 1997:165-176.
86. Dinarello CA, Wol SM. The role o interleukin-1 in disease.NEngl J Med. 1993;328:106-113.
87. Dinarello C. The interleukin-1 amily: 10 years o discovery.FASEB J. 1994;8:1314-1325.
88. Dinarello C. Interleukin-1.Adv Pharmacol. 1994;25:21-51.89. Fiers W. Tumor necrosis actor: Characterization at the
molecular, cellular and in vivo level. FEBS Lett. 1991;285:199-212.
90. Vassalli P. The pathophysiol ogy o tumor necrosis actors .AnnuRev Immunol. 1992;10:411-452.
91. Tracey K, Cerami A. Tumor necrosis actor: A pleiotropic cyto-kine and therapeutic target. Annu Rev Med. 1994;45:491-503.
92. Brach M, Herrman F. Interleukin 6: Presence and uture. Int JClin Lab Res. 1992;22:143-151.
93. Lotz M. Interleukin-6. Cancer Invest. 1993;11:731-742.94. Jones T. Interleukin-6, an endocrine cytokine. Clin Endocrinol.
1994;40:703-713.95. Rummel C, Poole S, Luheshi GN. Circulating interleukin-6
induces ever through a STAT3-linked activation o COX-2in the brain. Am J Physiol Regul Integr Comp Physiol.
2006;291:R1316-1326.96. Li S, Holers VM, Boackle SA, Blatteis CM. Modulation omouse endotoxic ever by complement. Inect Immun.2002;70:2519-2525.
97. Szekely M, Romanovsky AA. Pyretic and antipyretic signalswithin and without ever: A possible interplay.Med Hypotheses.1998;50:213-218.
98. Mackowiak PA. Concepts o ever. Arch Intern Med.1998;158:1870-1881.
99. Netea MG, Kullberg BJ, Van der Meer JWM. Do only circulat ingpyrogenic cytokines act as mediators in the ebrile response? Ahypothesis. Eur J Clin Invest. 1999;29:351-356.
100. Dinarella CA. Inection, ever, and exogenous and endogenouspyrogens: Some concepts have changed. J Endotoxin Res.2004;10:201-222.
101. Gabay C, Kushner I. Acute-phase proteins and other sys temicresponses to inammation.N Engl J Med. 1999;340:448-454.
102. Ernst E, Saradeth T, Achhammer G. n-3 atty acids and acute-phase proteins. Eur J Clin Invest. 1991;21:77-82.
103. Joyce PR, Hawes CR, Mulder RT, et al. Elevated leve ls o acutephase plasma proteins in major depression. Biol Psychiatry.1992;32:1035-1041.
104. Ganguli R, Yang Z, Shurin G, et al. Serum interleukin-6 concen-tration in schizophrenia: Elevation associated with duration oillness. Psychiatry Res. 1994;51:1-10.
105. LeMay LG, Vander AJ, Kluger MJ. The eects o psychologicalstress on plasma interleukin-6 activity in rats. Phys Behav.1990;47:957-961.
106. Volanakis JE. Acute phase proteins. In: McCarty DJ, KoopmanWJ, eds.Arthritis and Allied Conditions: A Textbook o Rheuma-tology. Malvern, Pa: Lea & Febiger; 1993:469-477.
107. Ballou SP, Lozanski G. Induction o inammatory cytokines
release rom cultured human monocytes by C-reactive protein.Cytokine. 1992;4:361-368.
108. Cermak J, Key NS, Bach RR, et al. C-reactive protein induceshuman peripheral blood monocytes to synthesize tissue actor.Blood. 1993;82:513-520.
109. Tilg H, Vannier E, Vachine G, et al. Antiinammatory propertieso hepatic acute phase proteins: Preerential induction o inter-leukin 1 (IL-1) receptor antagonist over IL-1 synthesisby human peripheral blood mononuclear cells. J Exp Med.1993;178:1629-1636.
110. Dobrinich R, Spagnuolo PJ. Binding o C-reactive protein tohuman neutrophils: Inhibition o respiratory burst activity.Arthritis Rheum. 1991;34:1031-1038.
111. Ahmed N, Thorley R, Xia D, et al. Transgenic mice expressingrabbit C-reactive protein exhibit diminished chemotacticactor-induced alveolitis. Am J Respir Crit Care Med.1996;153:1141-1147.
112. Xu L, Badolato R, Murphy WJ, et al. A novel biologic unctiono serum amyloid A-induction o T lymphocyte migration andadhesion.J Immunol. 1995;155:1184-1190.
113. Kisilevsky R, Subrahmanyan L. Serum amyloid A changes highdensity lipoproteins cellular afnity. Lab Invest. 1992;66:778.
114. Berliner JA, Navab M, Fogelman AM, et al. Atherosclerosis: Basicmechanismsoxidation, inammation, and genetics.Circulation. 1995;91:2488-2496.
115. Wurel MM, Monks BG, Ingalls RR, et al. Targeted delet ion othe lipopolysaccharide (LPS)-binding protein gene leads to pro-ound suppression o LPS responses ex vivo, whereas in vivoresponses remain intact.J Exp Med. 1997;186:2051-2056.
116. May MT. Galen on t