CPRC: CPRC M0, opciones terapéuticas...Papel de distintas técnicas de imagen en la valoración...
69
CPRC: CPRC M0, opciones terapéuticas J Cassinello. Oncología Médica. Hospital Universitario de Guadalajara
Transcript of CPRC: CPRC M0, opciones terapéuticas...Papel de distintas técnicas de imagen en la valoración...

CPRC: CPRC M0, opciones terapéuticas
J Cassinello.
Oncología Médica.
Hospital Universitario de Guadalajara
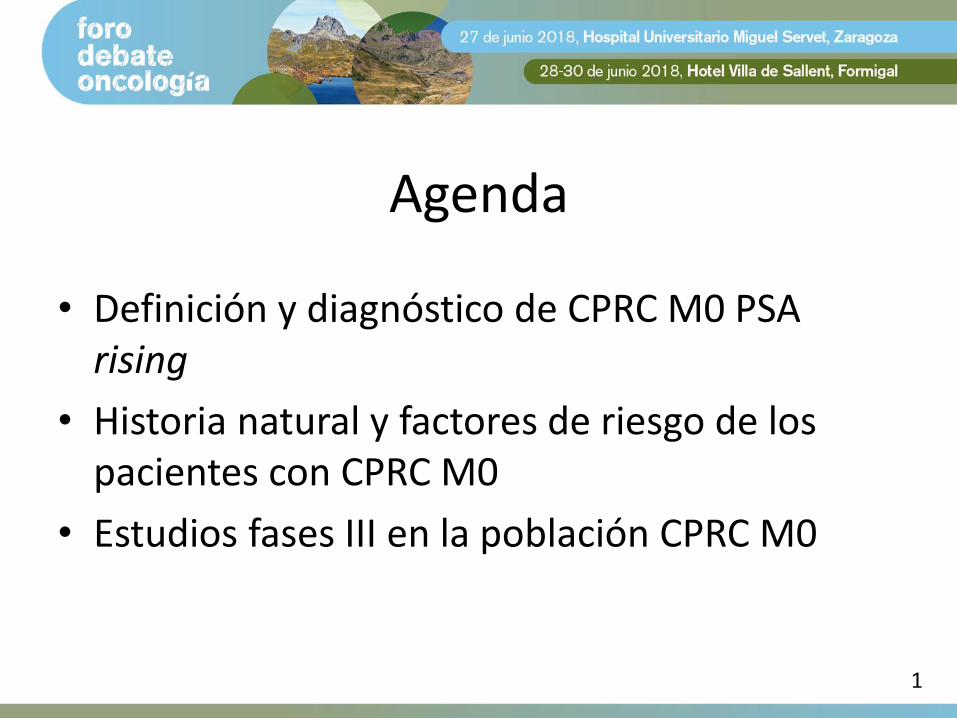
Agenda
• Definición y diagnóstico de CPRC M0 PSA rising
• Historia natural y factores de riesgo de los pacientes con CPRC M0
• Estudios fases III en la población CPRC M0
1

Agenda
• Definición y diagnóstico de CPRC M0 PSA rising
• Historia natural y factores de riesgo de los pacientes con CPRC M0
• Estudios fases III en la población CPRC M0
1
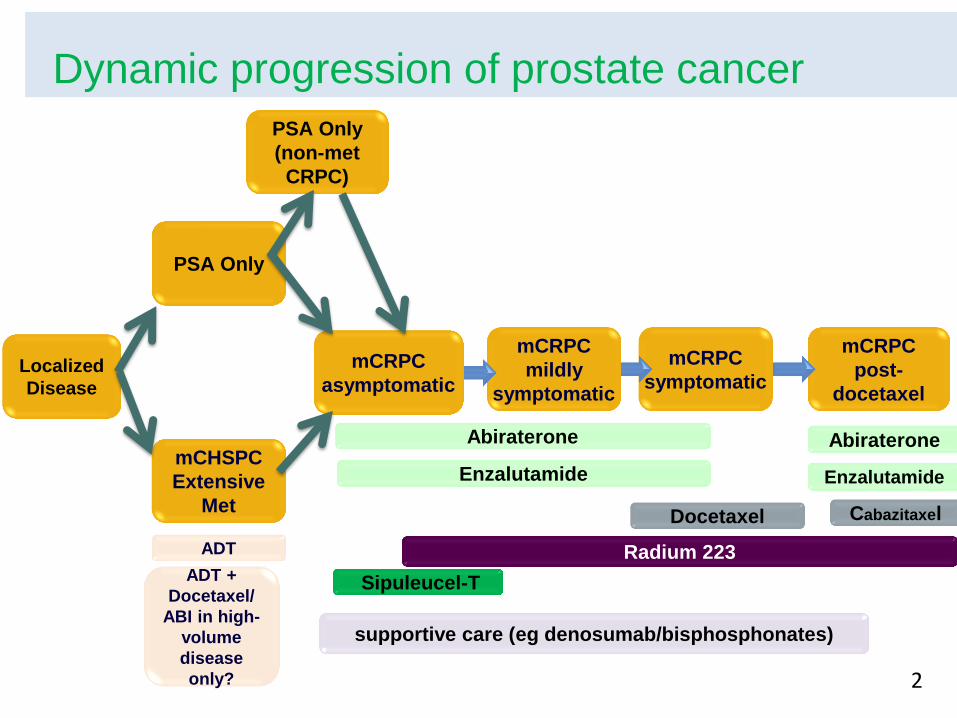
Dynamic progression of prostate cancer
ADT
supportive care (eg denosumab/bisphosphonates)
mCRPC
post-
docetaxel
mCRPC
symptomatic
mCRPC
mildly
symptomatic
mCRPC
asymptomatic
Localized
Disease
Sipuleucel-T
Enzalutamide
Abiraterone Abiraterone
Docetaxel Cabazitaxel
Radium 223
Enzalutamide
ADT +
Docetaxel/
ABI in high-
volume
disease
only?
mCHSPC
Extensive
Met
PSA Only
PSA Only
(non-met
CRPC)
2

Dynamic progression of prostate cancer
ADT
supportive care (eg denosumab/bisphosphonates)
mCRPC
post-
docetaxel
mCRPC
symptomatic
mCRPC
mildly
symptomatic
mCRPC
asymptomatic
Localized
Disease
Sipuleucel-T
Enzalutamide
Abiraterone Abiraterone
Docetaxel Cabazitaxel
Radium 223
Enzalutamide
ADT +
Docetaxel/
ABI in high-
volume
disease
only?
mCHSPC
Extensive
Met
PSA Only
PSA Only
(non-met
CRPC)
3
Tratamiento ADT ?????
Definición de CPRC M0
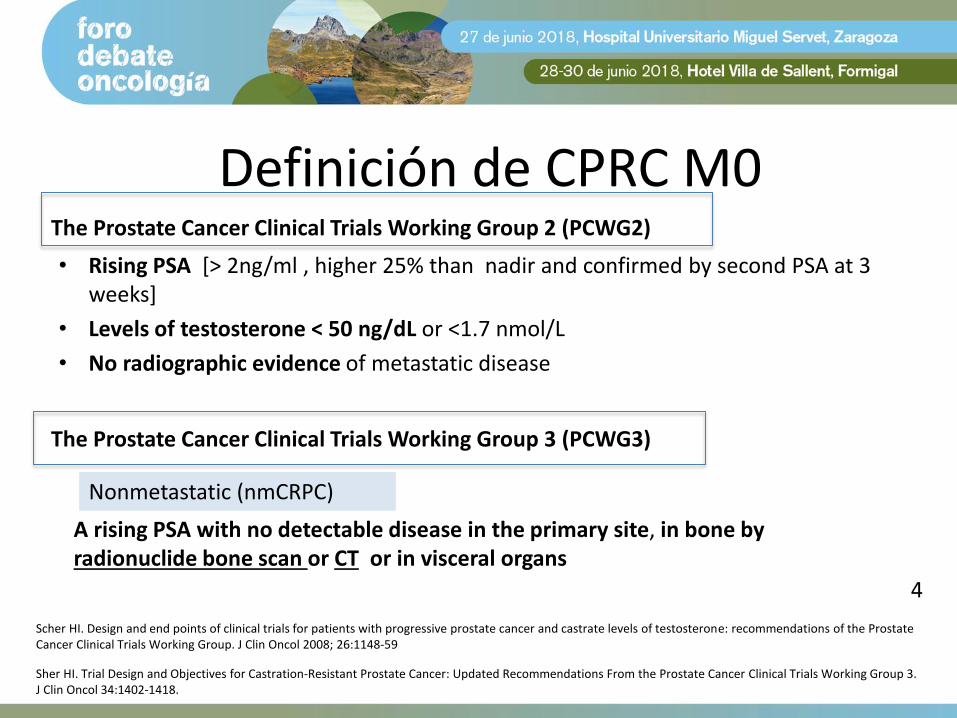
• Rising PSA [> 2ng/ml , higher 25% than nadir and confirmed by second PSA at 3 weeks]
• Levels of testosterone < 50 ng/dL or <1.7 nmol/L
• No radiographic evidence of metastatic disease
The Prostate Cancer Clinical Trials Working Group 2 (PCWG2)
The Prostate Cancer Clinical Trials Working Group 3 (PCWG3)
A rising PSA with no detectable disease in the primary site, in bone by radionuclide bone scan or CT or in visceral organs
Nonmetastatic (nmCRPC)
Scher HI. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol 2008; 26:1148-59
Sher HI. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol 34:1402-1418.
4
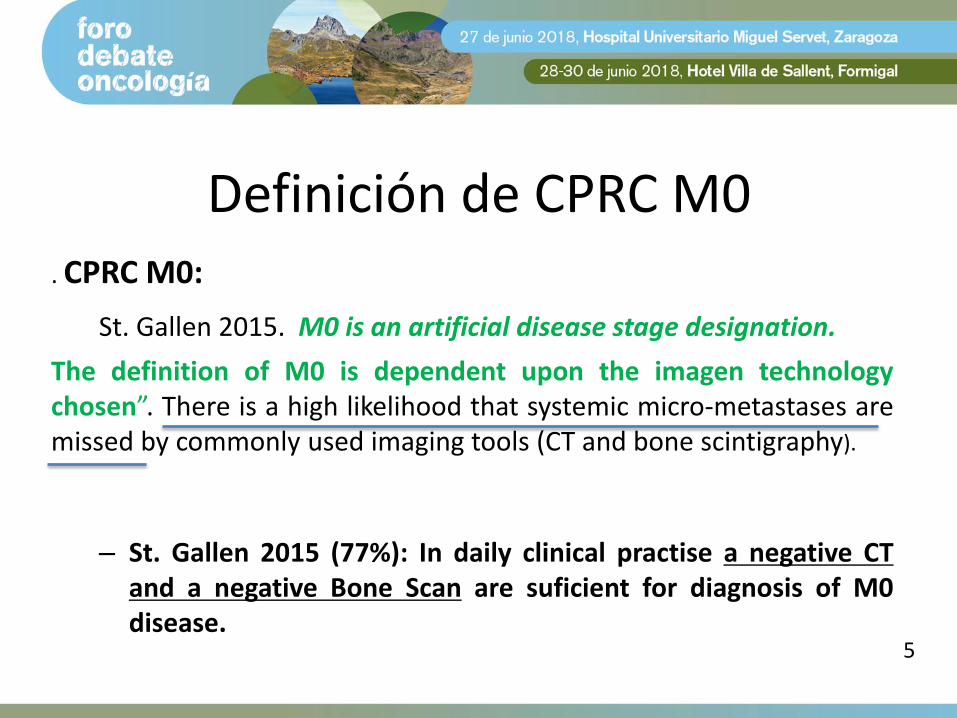
Definición de CPRC M0 . CPRC M0:
St. Gallen 2015. M0 is an artificial disease stage designation.
The definition of M0 is dependent upon the imagen technology chosen”. There is a high likelihood that systemic micro-metastases are missed by commonly used imaging tools (CT and bone scintigraphy).
– St. Gallen 2015 (77%): In daily clinical practise a negative CT and a negative Bone Scan are suficient for diagnosis of M0 disease.
5
Only technology limits our detection of the extremely small or the extremely remote.
Eric Small, 2017
6
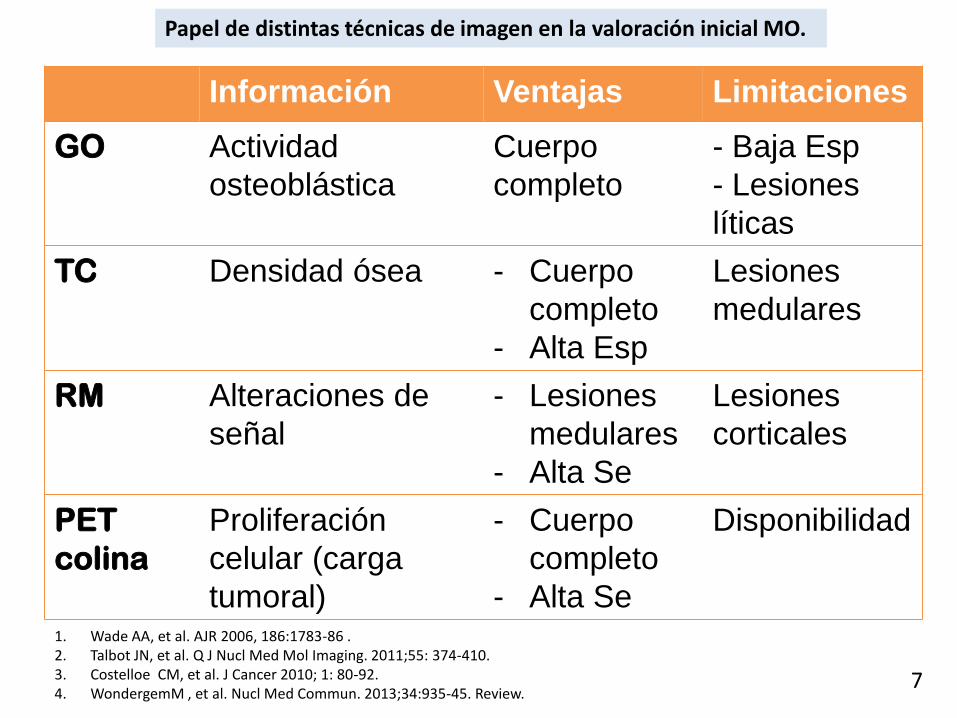
Información Ventajas Limitaciones
GO
Actividad
osteoblástica
Cuerpo
completo
- Baja Esp
- Lesiones
líticas
TC
Densidad ósea - Cuerpo
completo
- Alta Esp
Lesiones
medulares
RM
Alteraciones de
señal
- Lesiones
medulares
- Alta Se
Lesiones
corticales
PET
colina
Proliferación
celular (carga
tumoral)
- Cuerpo
completo
- Alta Se
Disponibilidad
1. Wade AA, et al. AJR 2006, 186:1783-86 . 2. Talbot JN, et al. Q J Nucl Med Mol Imaging. 2011;55: 374-410. 3. Costelloe CM, et al. J Cancer 2010; 1: 80-92. 4. WondergemM , et al. Nucl Med Commun. 2013;34:935-45. Review.
Papel de distintas técnicas de imagen en la valoración inicial MO.
7
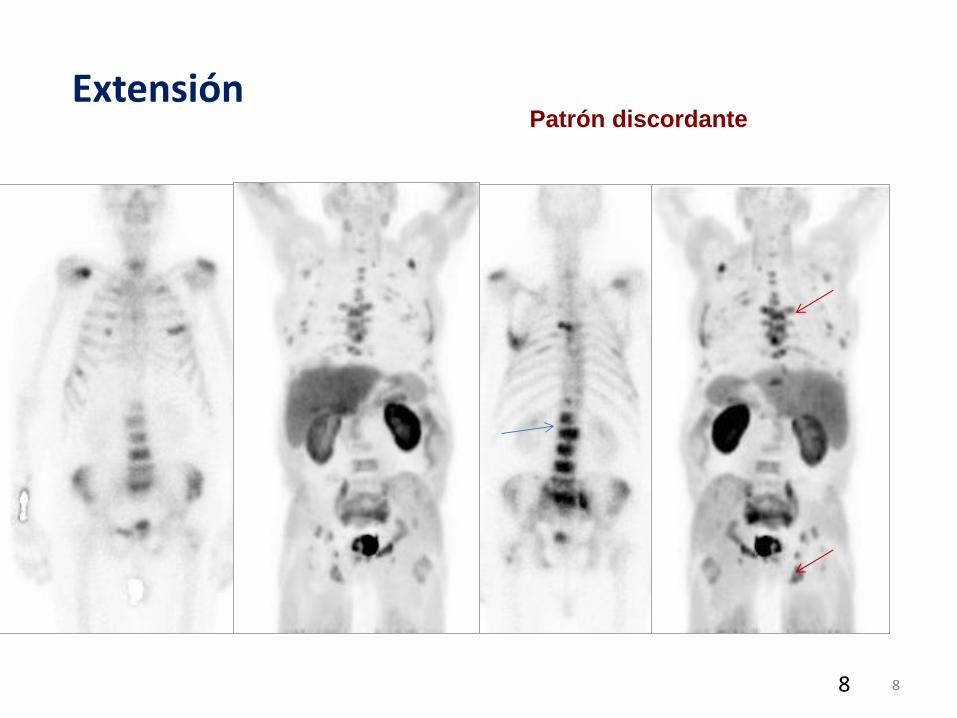
8
Extensión Patrón discordante
8
Diagnóstico de M0.
• PET con análogos de colina
- Especialmente si los niveles de PSA son > 2 ng/ml o los tiempos de duplicación son bajos (<6 meses) o el Gleason inicial es > 71.
• ¿PSMA?
– Elevada sensibilidad con niveles de PSA de 0,5 ng/ml [ASCO 2018]
•
Lo que debiera hacerse según la evidencia.
Bauman G, et al. 18F-fluorocholine for prostate cancer imaging: a systematic review of the literature. Prostate cancer and prostatic diseases. 2011:1-11.
9
Agenda
• Definición y diagnóstico de CPRC M0 PSA rising
• Historia natural y factores de riesgo de los pacientes con CPRC M0
• Estudios fases III en la población CPRC M0
10
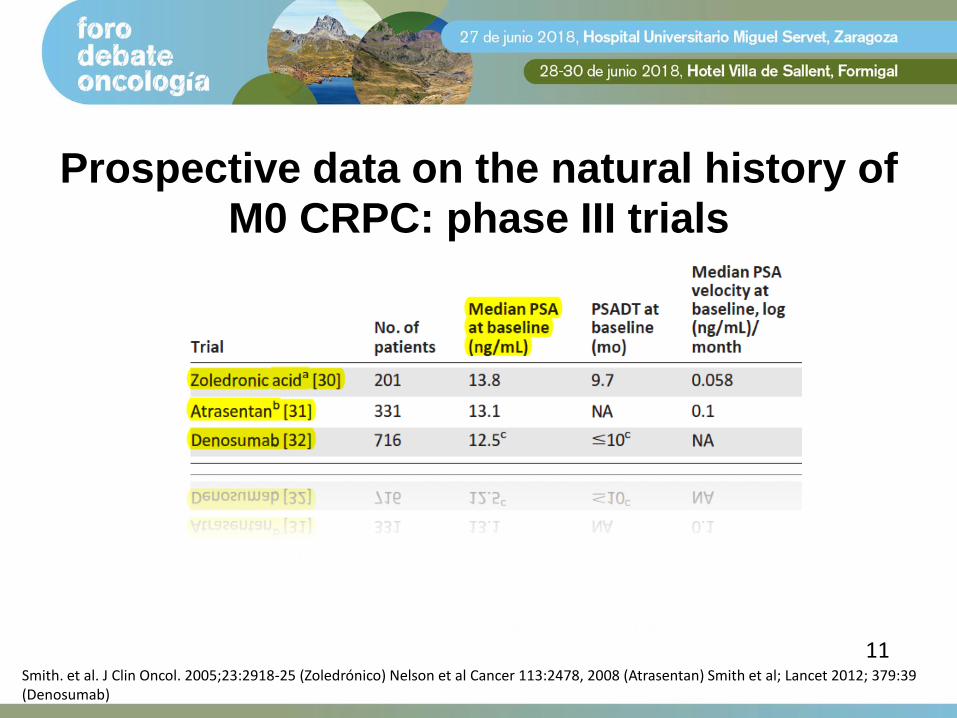
Prospective data on the natural history of
M0 CRPC: phase III trials
Smith. et al. J Clin Oncol. 2005;23:2918-25 (Zoledrónico) Nelson et al Cancer 113:2478, 2008 (Atrasentan) Smith et al; Lancet 2012; 379:39 (Denosumab)
11
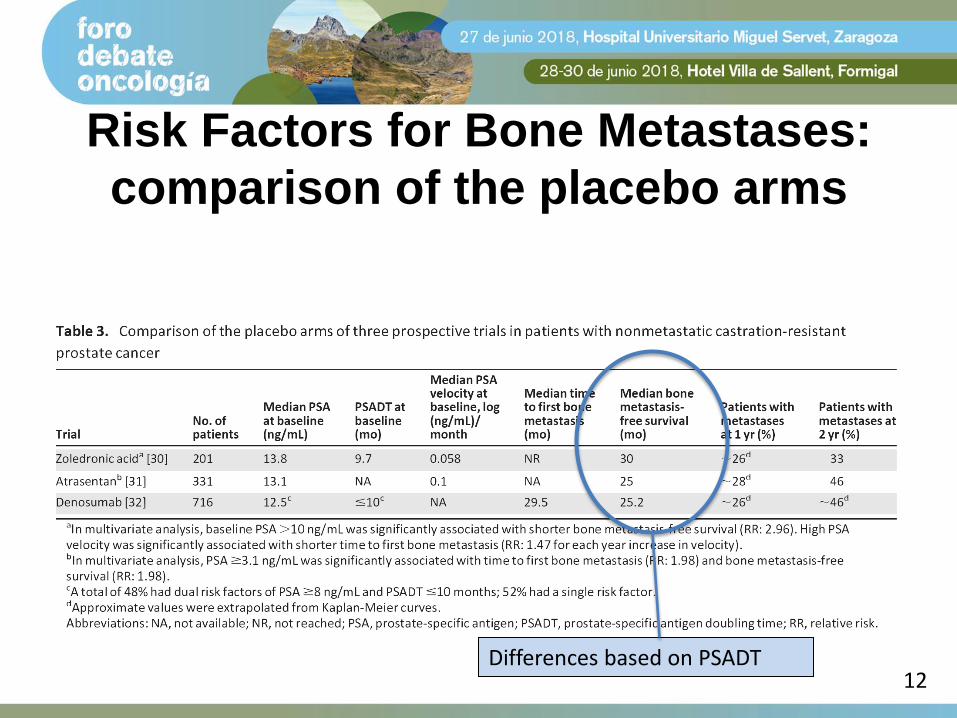
Risk Factors for Bone Metastases:
comparison of the placebo arms
12 Differences based on PSADT

Smith MR et al. Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial. Lancet 2013; 379: 39-46
1.432 CPRC
PSA ≥ 8 ng/mL PSA-DT ≤ 10 meses
Factores de estratificación:
• PSA ≥ 8 ng/mL y PSA-DT ≤ 10 meses (sí o no)
• QT previa o actual para CaP (sí o no)
A L E A T O R I Z A C I Ó N
1:1
Denosumab 120 mg sc cada 4 semanas
N=716
Placebo 120 mg sc cada 4 semanas
N=716
Objetivo principal: • Supervivencia libre
de metástasis ósea o muerte
13

Shorter PSA Doubling Time is a Predictor of Increasing Risk for Bone Metastasis and Death
PSA Doubling Time in Months
Rela
tive R
isk f
or
Bo
ne M
eta
sta
sis
or
Death
Median
PSA DT at
study
entry
1.4
1.6
1.8
2.0
2.2
2.4
2.6
2.8
3.0
20 18 16 14 12 10 8 6 4 2
PSA DT
eligibility
criteria
Placebo arm, N = 716
• Placebo arm of the Denosumab study demonstrates shortening PSA doubling time as a
predictor of increasing risk for bone metastases development
• In a separate study, PSA was a key risk factor for bone metastasis and a PSADT ≤
6 months was significantly associated with shorter bone metastasis-free survival1
Smith et al 15

Shorter PSA Doubling Time is a Predictor of Increasing Risk for Bone Metastasis and Death
PSA Doubling Time in Months
Rela
tive R
isk f
or
Bo
ne M
eta
sta
sis
or
Death
Median
PSA DT at
study
entry
1.4
1.6
1.8
2.0
2.2
2.4
2.6
2.8
3.0
20 18 16 14 12 10 8 6 4 2
PSA DT
eligibility
criteria
Placebo arm, N = 716
• Placebo arm of the Denosumab study demonstrates shortening PSA doubling time as a
predictor of increasing risk for bone metastases development
• In a separate study, PSA was a key risk factor for bone metastasis and a PSADT ≤
6 months was significantly associated with shorter bone metastasis-free survival1
Smith et al (2005)
16
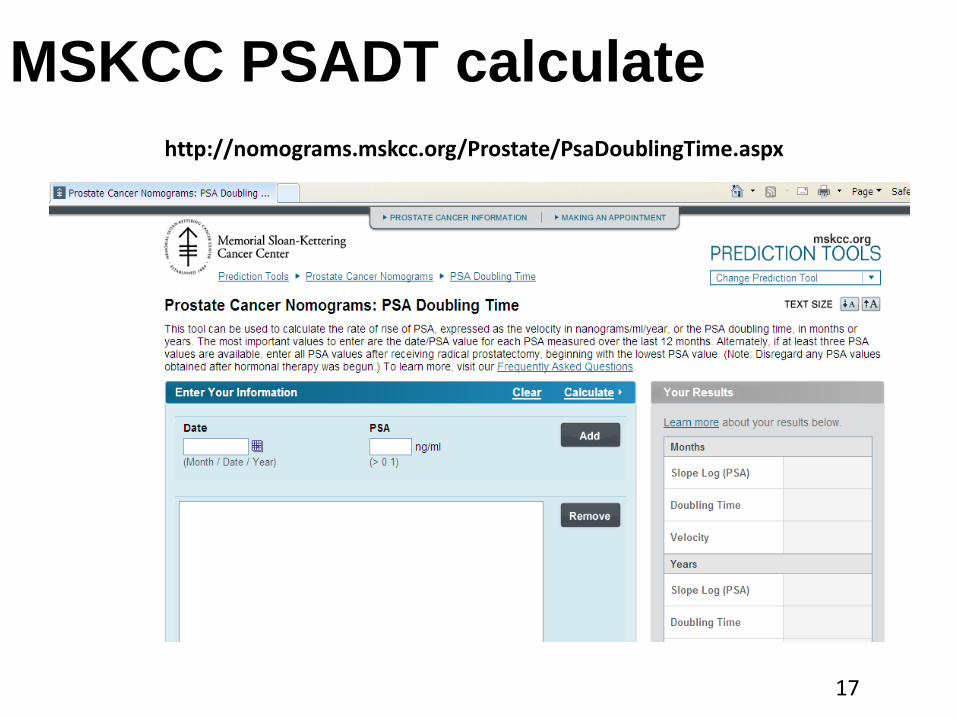
MSKCC PSADT calculate
http://nomograms.mskcc.org/Prostate/PsaDoublingTime.aspx
17
Agenda
• Definición y diagnóstico de CPRC M0 PSA rising
• Historia natural y factores de riesgo de los pacientes con CPRC M0
• Estudios fases fases III en la población CPRC M0
18
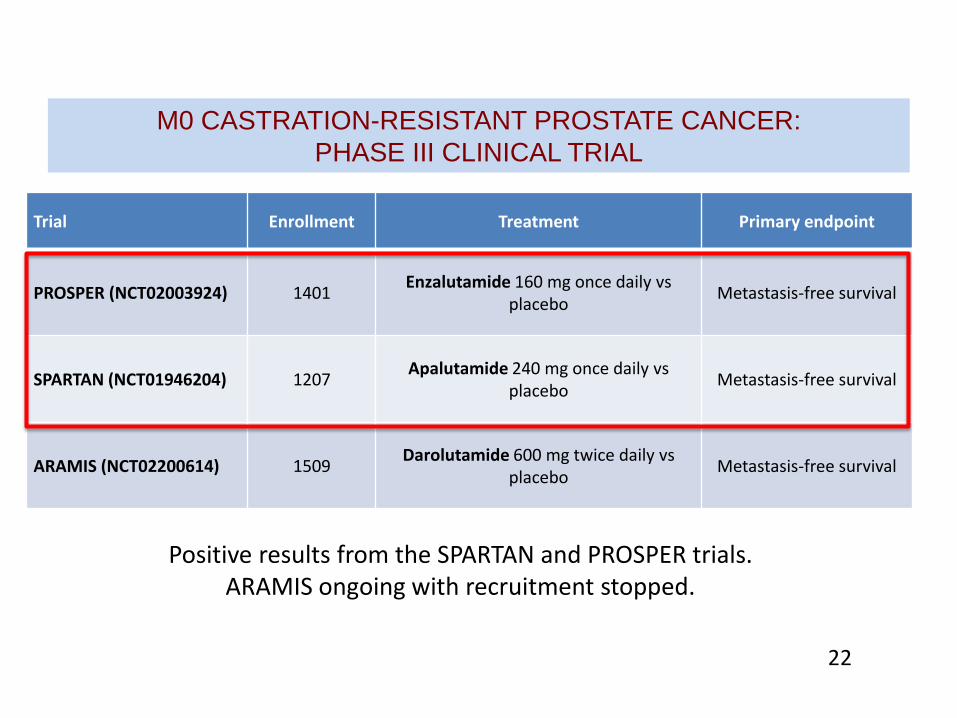
Trial Enrollment Treatment Primary endpoint
PROSPER (NCT02003924) 1401 Enzalutamide 160 mg once daily vs
placebo Metastasis-free survival
SPARTAN (NCT01946204) 1207 Apalutamide 240 mg once daily vs
placebo Metastasis-free survival
ARAMIS (NCT02200614) 1509 Darolutamide 600 mg twice daily vs
placebo Metastasis-free survival
Positive results from the SPARTAN and PROSPER trials. ARAMIS ongoing with recruitment stopped.
M0 CASTRATION-RESISTANT PROSTATE CANCER:
PHASE III CLINICAL TRIAL
22

SPARTAN, a Phase 3 Double-Blind, Randomized Study of Apalutamide vs Placebo in Patients With Nonmetastatic Castration-Resistant Prostate Cancer
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
23
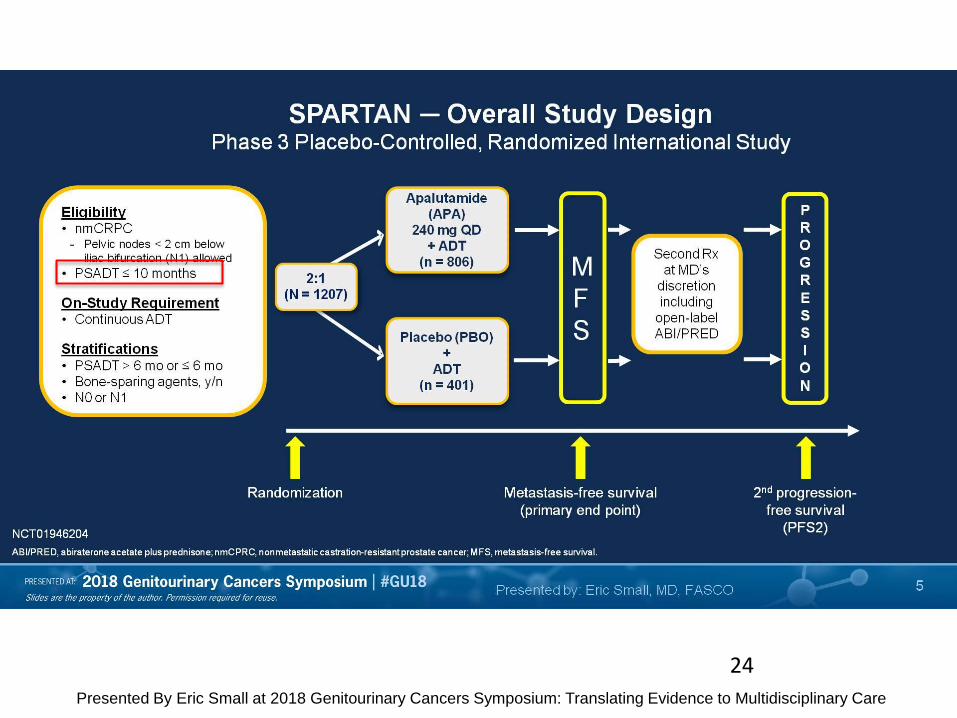
Slide 5
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
24
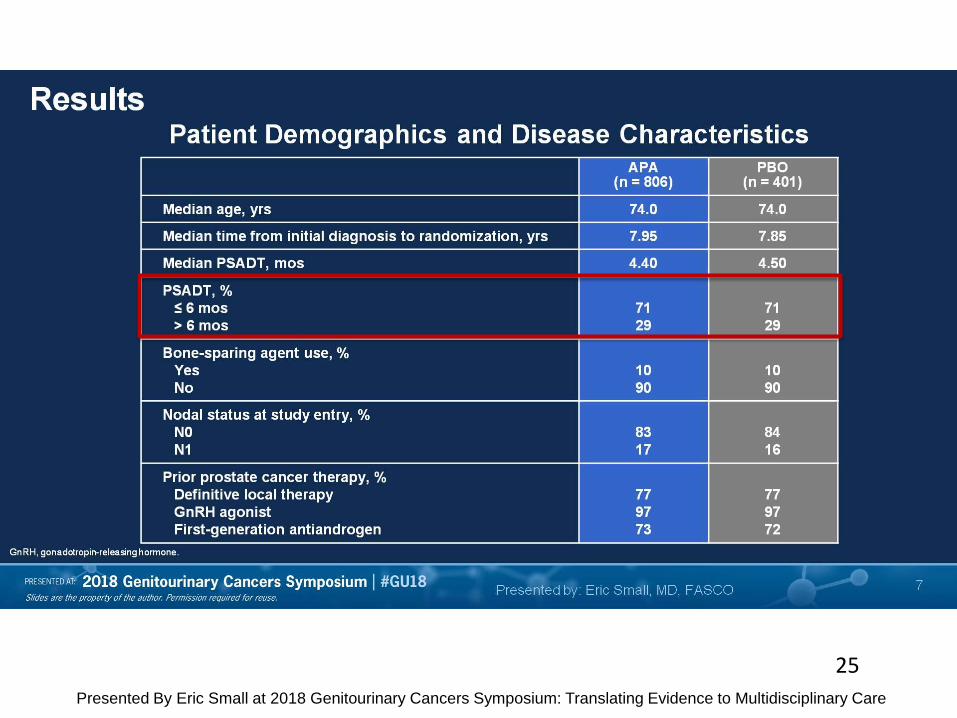
Slide 7
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
25
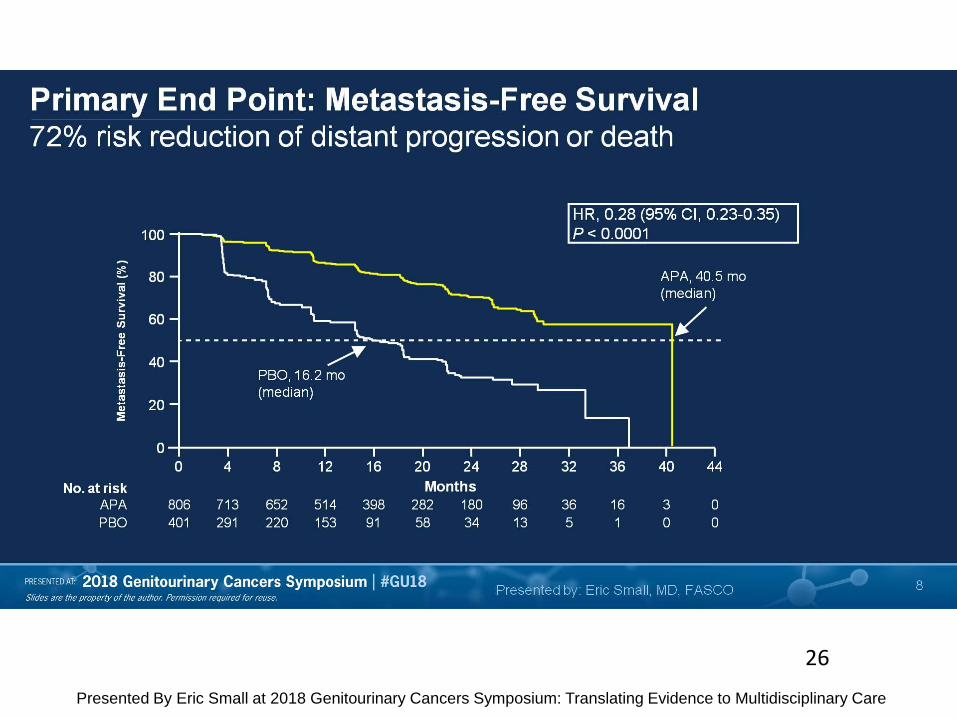
Slide 8
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
26
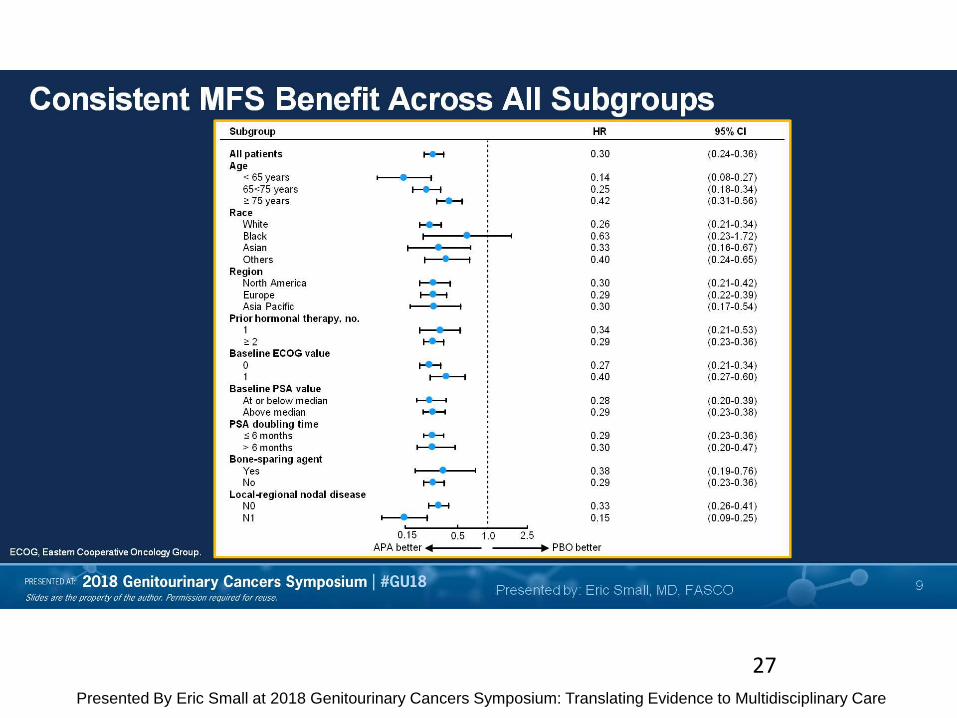
Slide 9
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
27

Slide 10
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
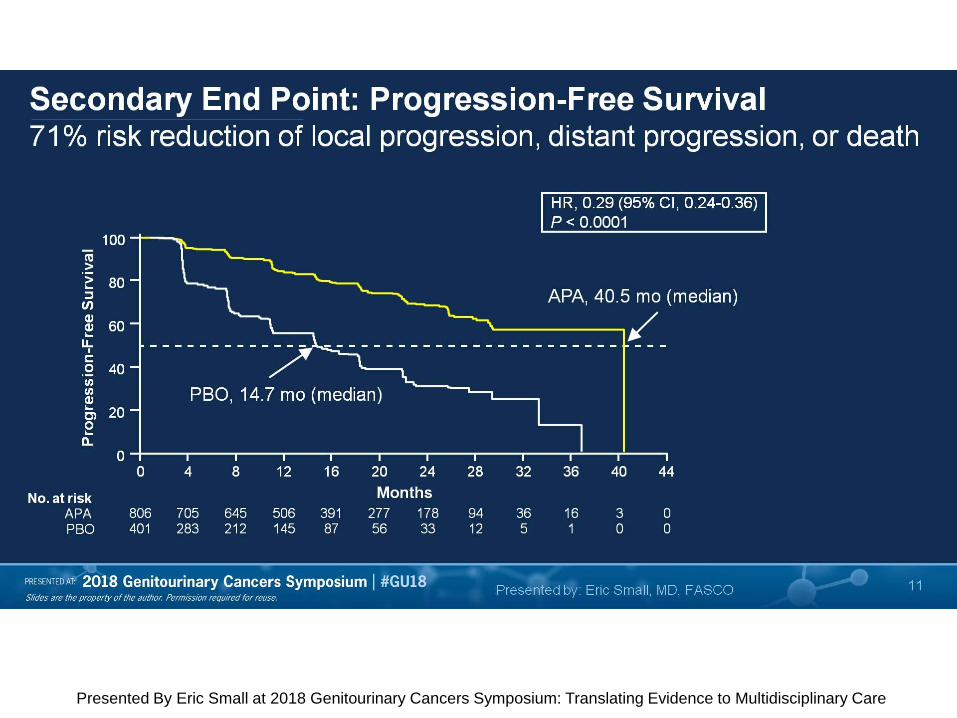
Slide 11
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
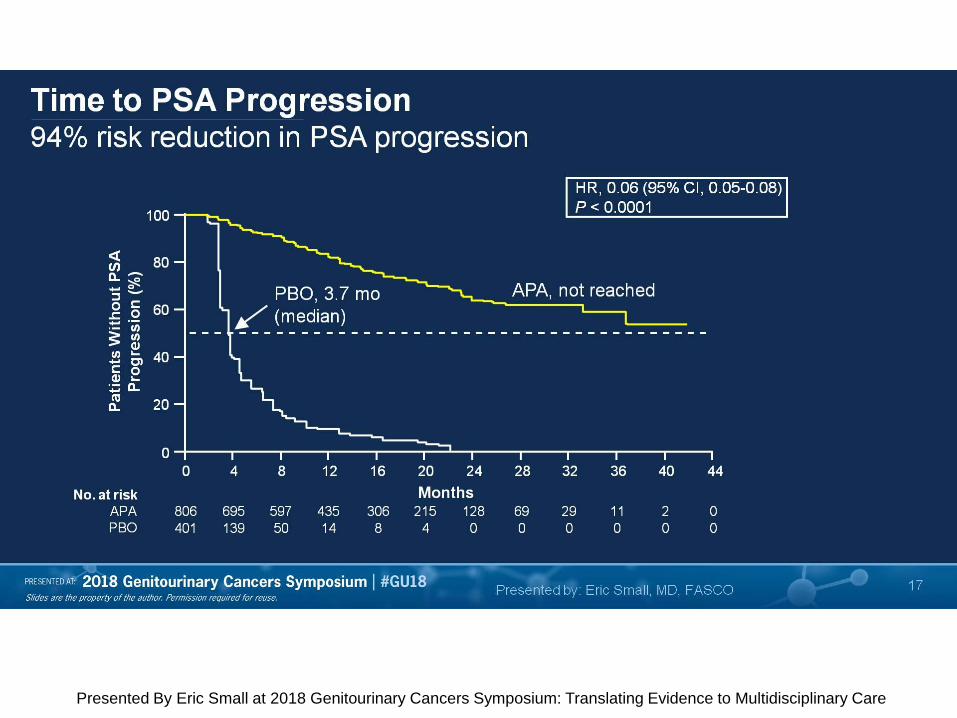
Slide 17
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
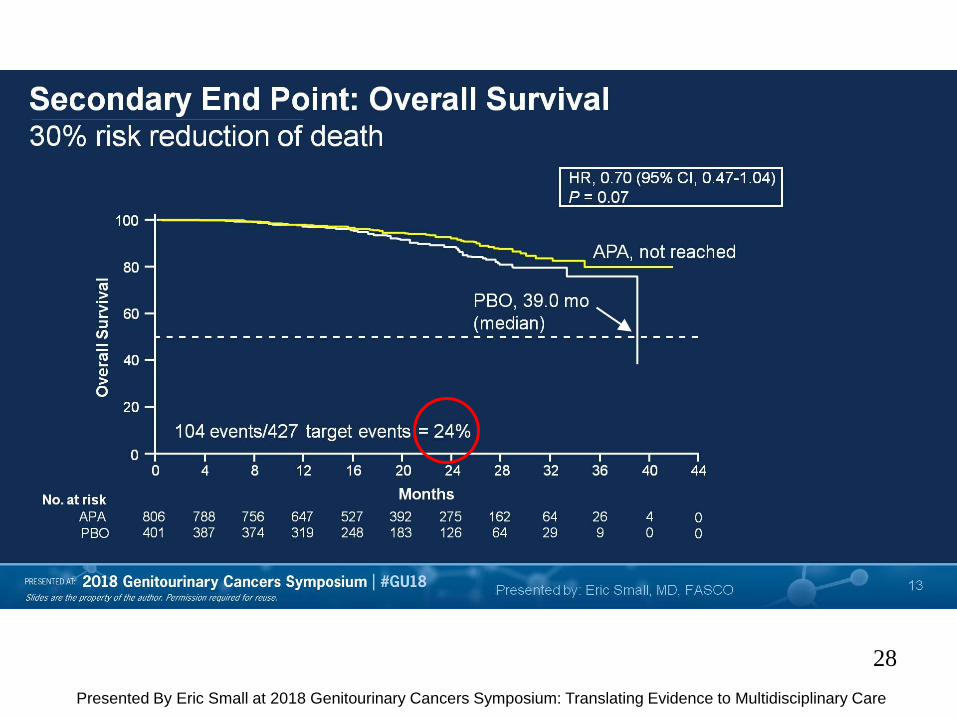
Slide 13
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
28
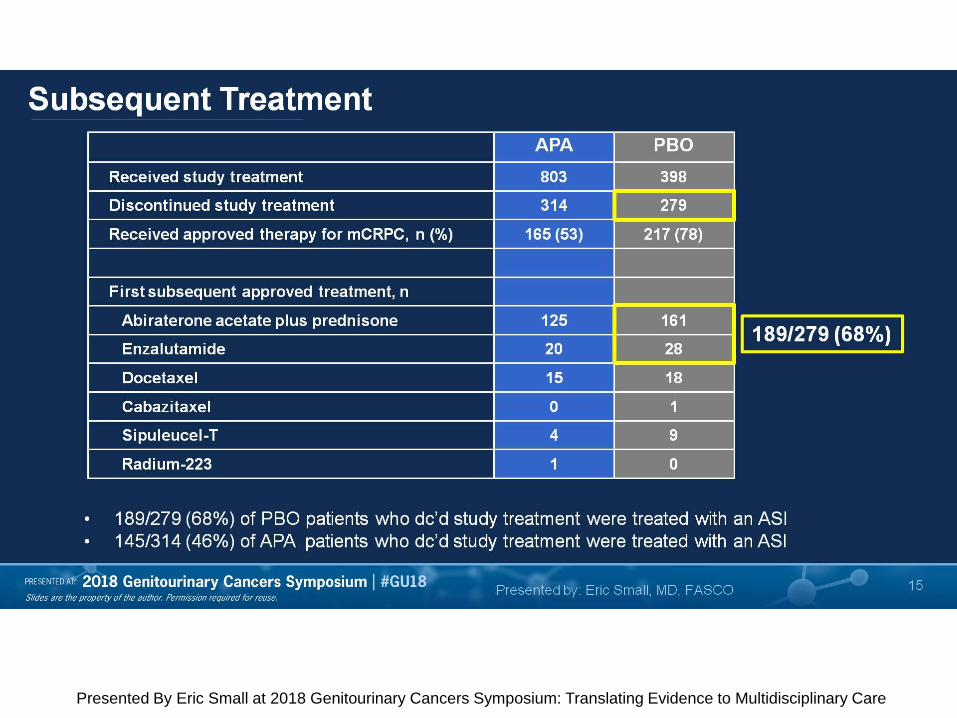
Slide 15
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Slide 16
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
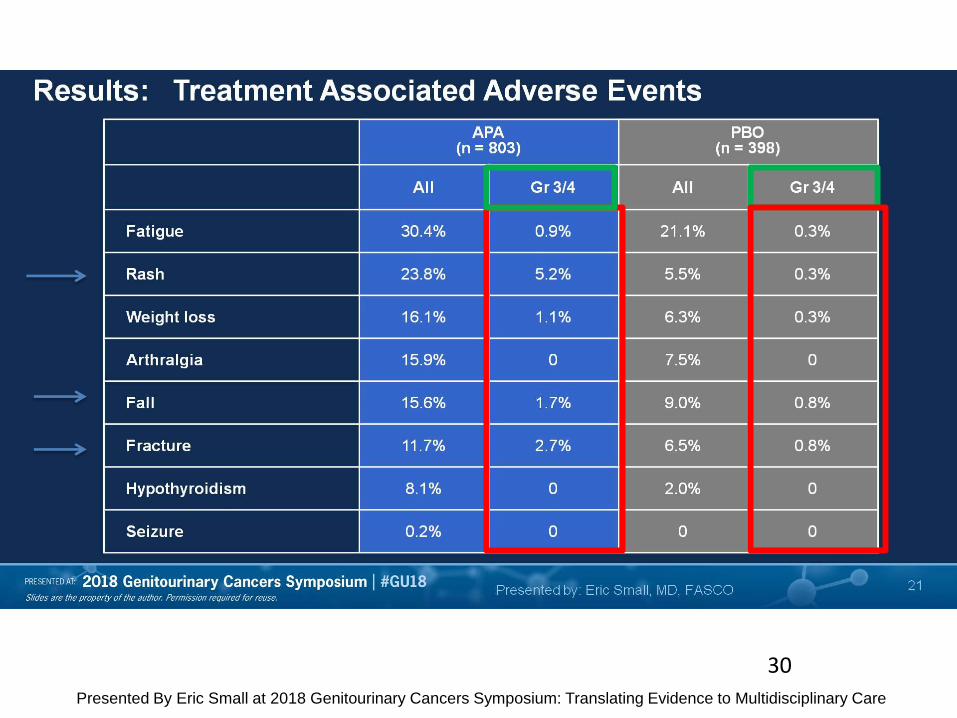
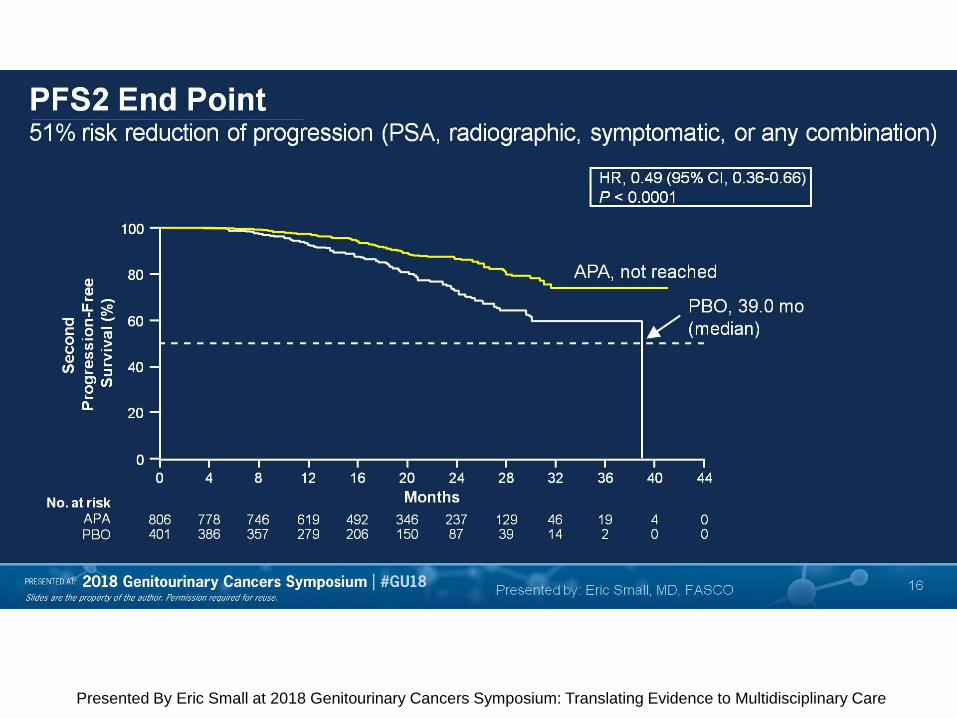
Slide 21
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
30
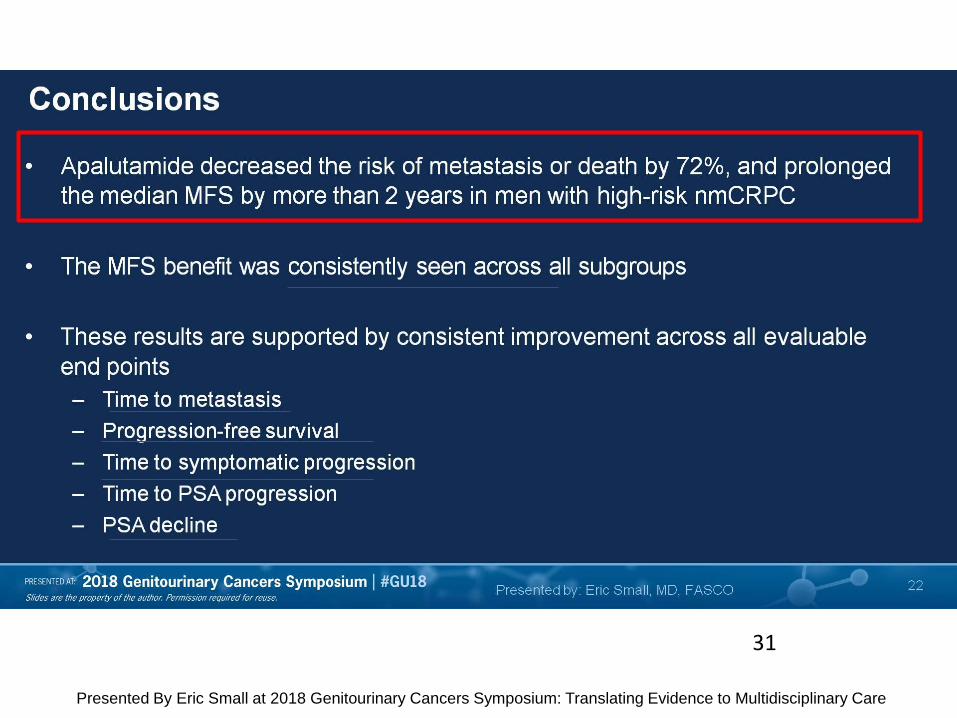
Conclusions
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
31
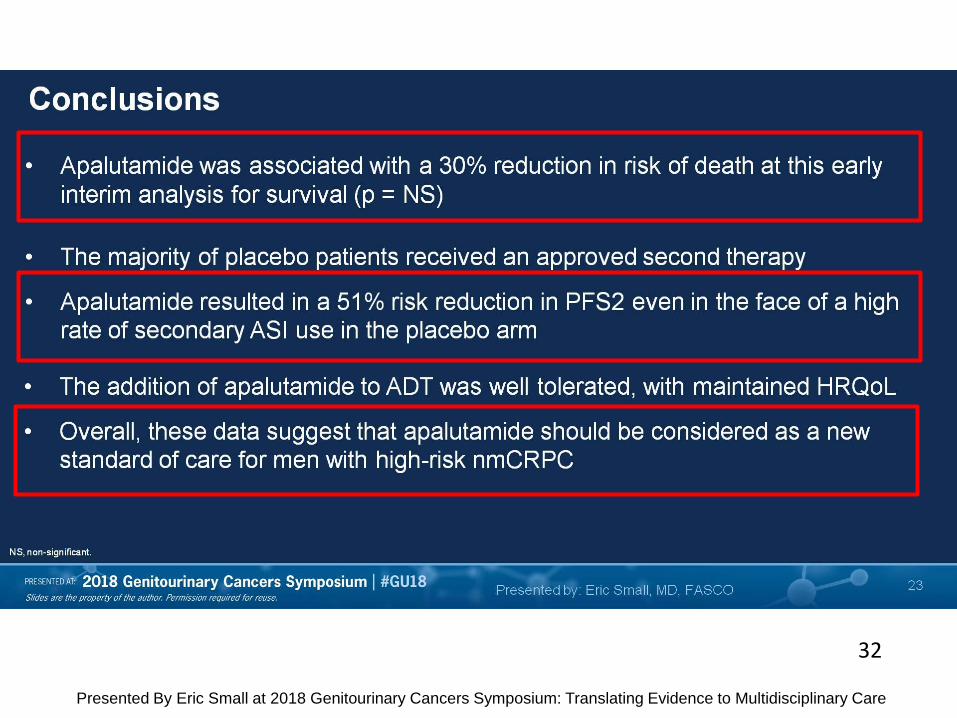
Slide 23
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
32
PROSPER: A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study of Enzalutamide in Men With Nonmetastatic Castration-Resistant Prostate Cancer
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
33

PROSPER Study Design
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
34
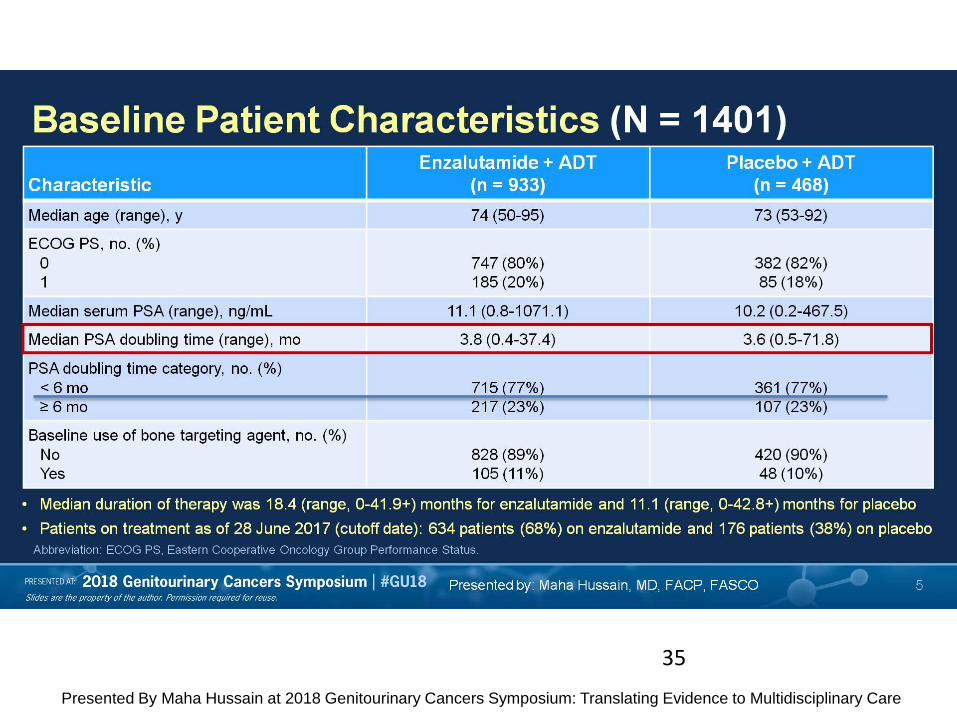
Baseline Patient Characteristics (N = 1401)
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
35
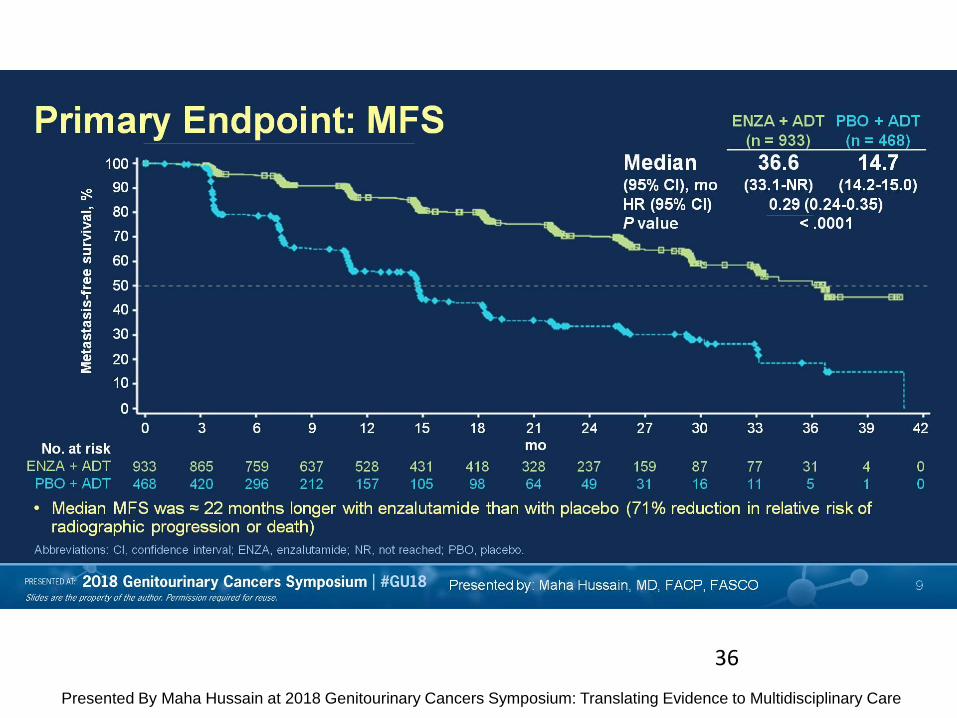
Primary Endpoint: MFS
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
36
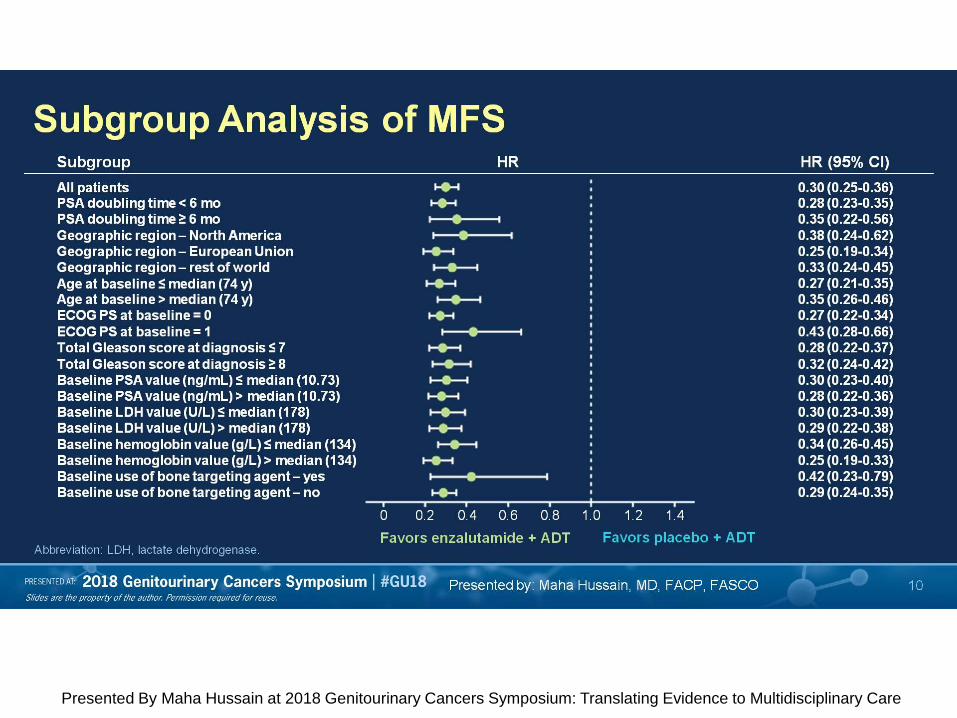
Subgroup Analysis of MFS
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Time to PSA Progression
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
37
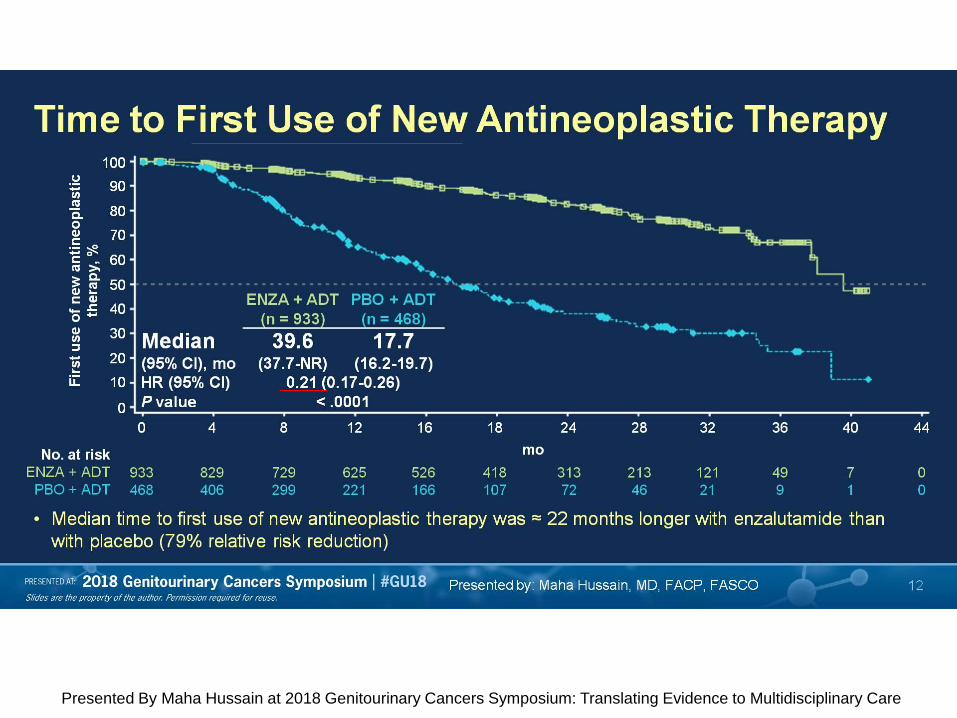
Time to First Use of New Antineoplastic Therapy
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
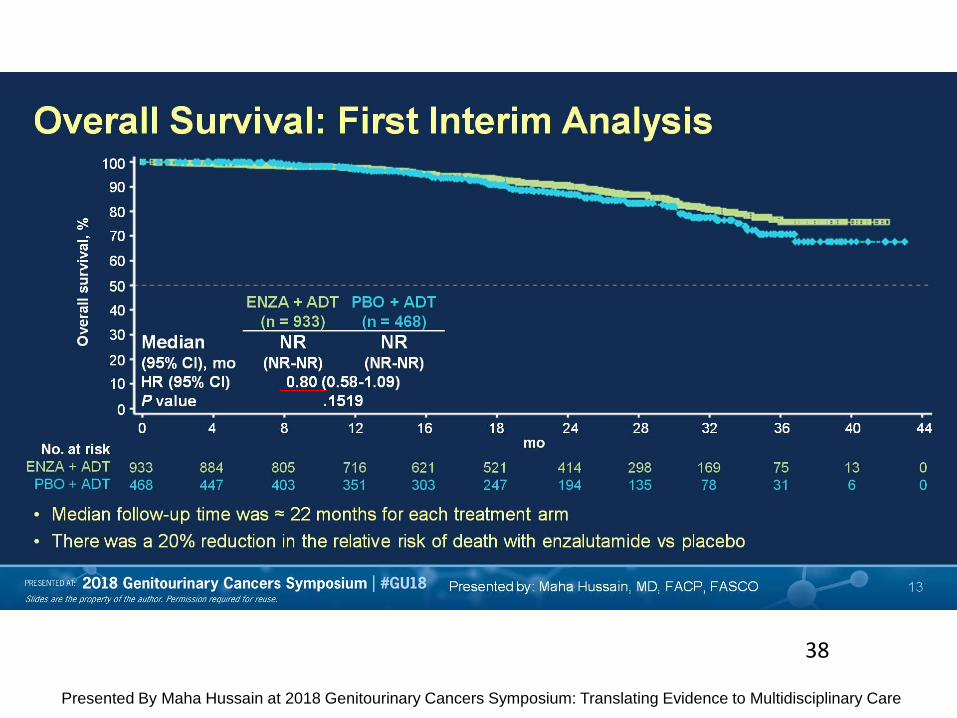
Overall Survival: First Interim Analysis
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
38
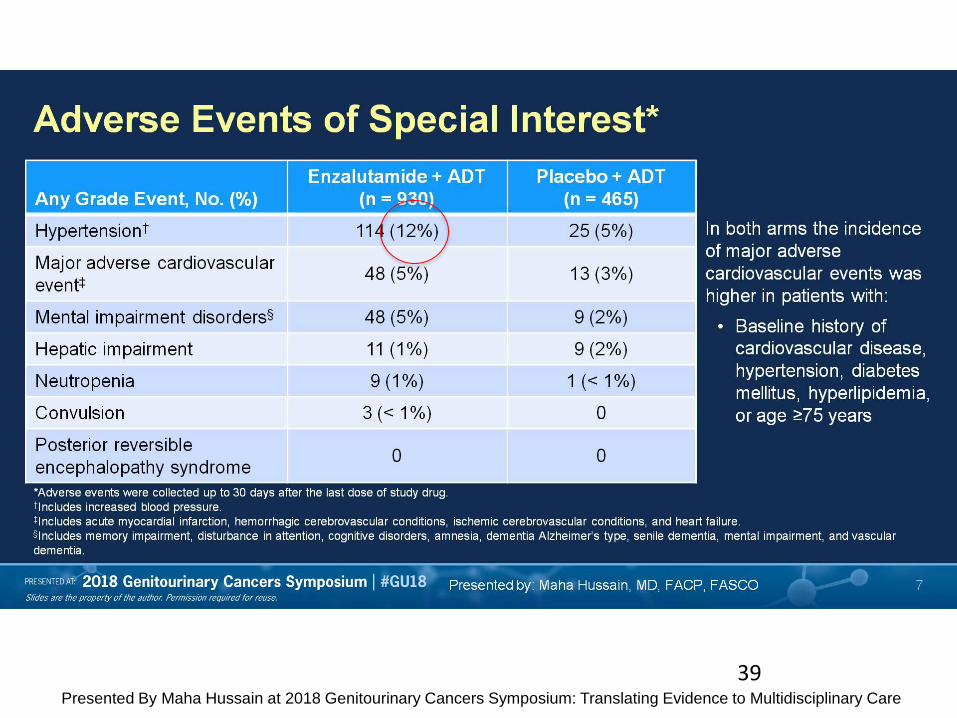
Adverse Events of Special Interest*
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
39
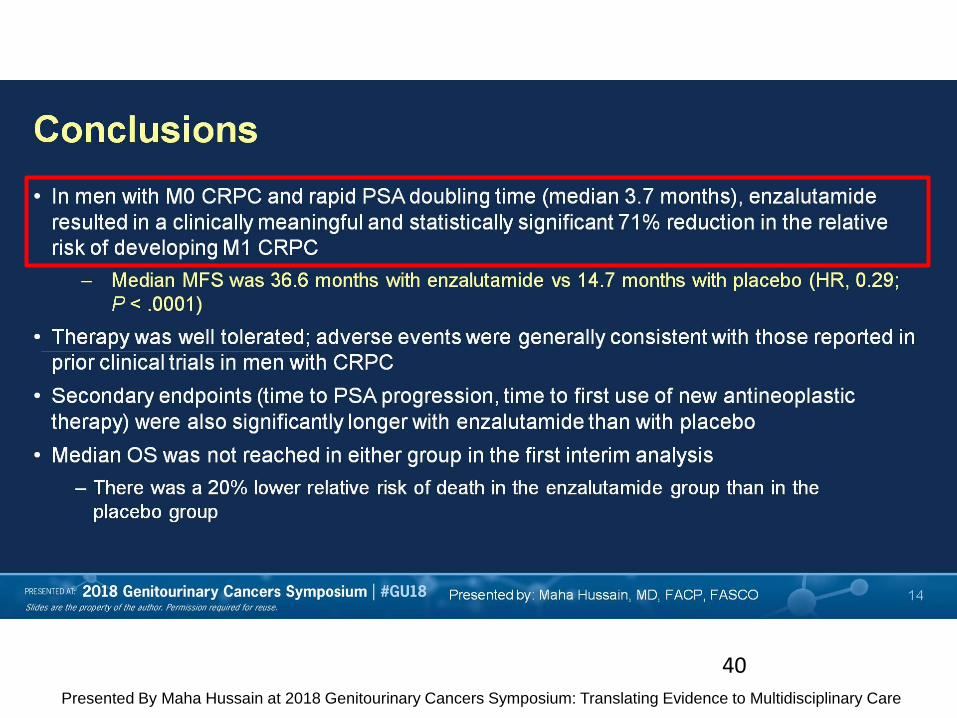
Conclusions
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
40
Is MFS a surrogate for OS?
Presented By Philip Kantoff at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
41
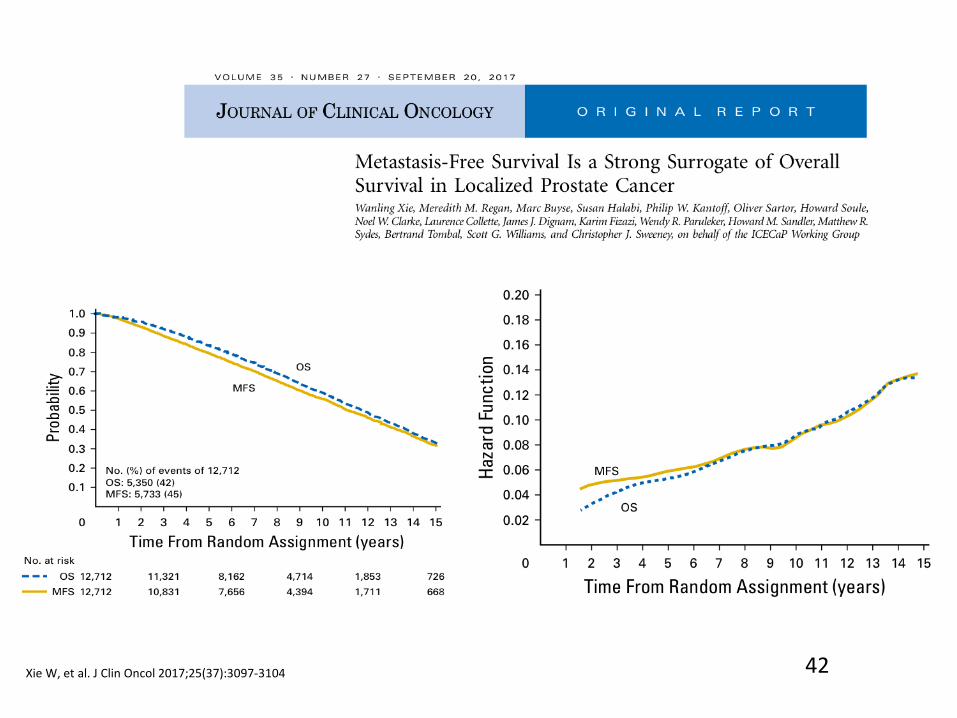
Xie W, et al. J Clin Oncol 2017;25(37):3097-3104 42
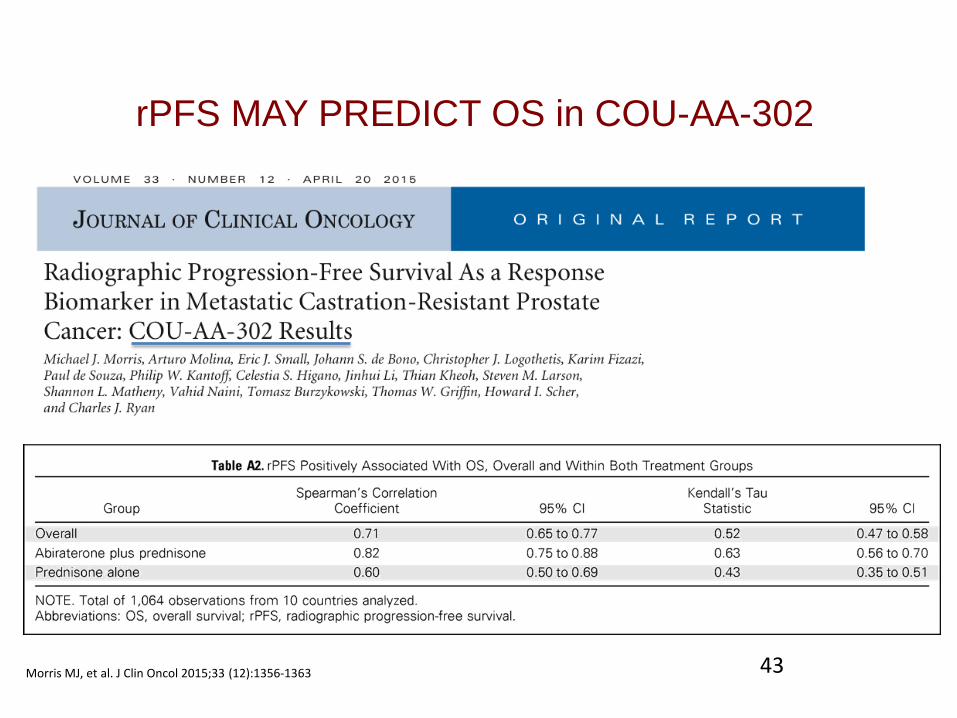
Morris MJ, et al. J Clin Oncol 2015;33 (12):1356-1363
rPFS MAY PREDICT OS in COU-AA-302
43
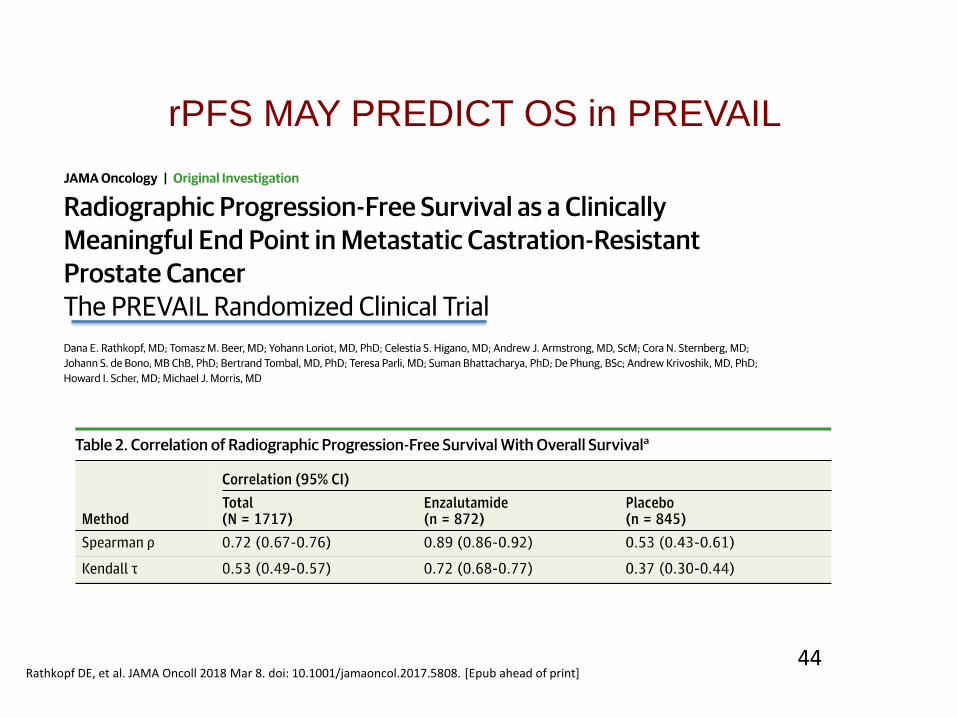
Rathkopf DE, et al. JAMA Oncoll 2018 Mar 8. doi: 10.1001/jamaoncol.2017.5808. [Epub ahead of print]
rPFS MAY PREDICT OS in PREVAIL
44
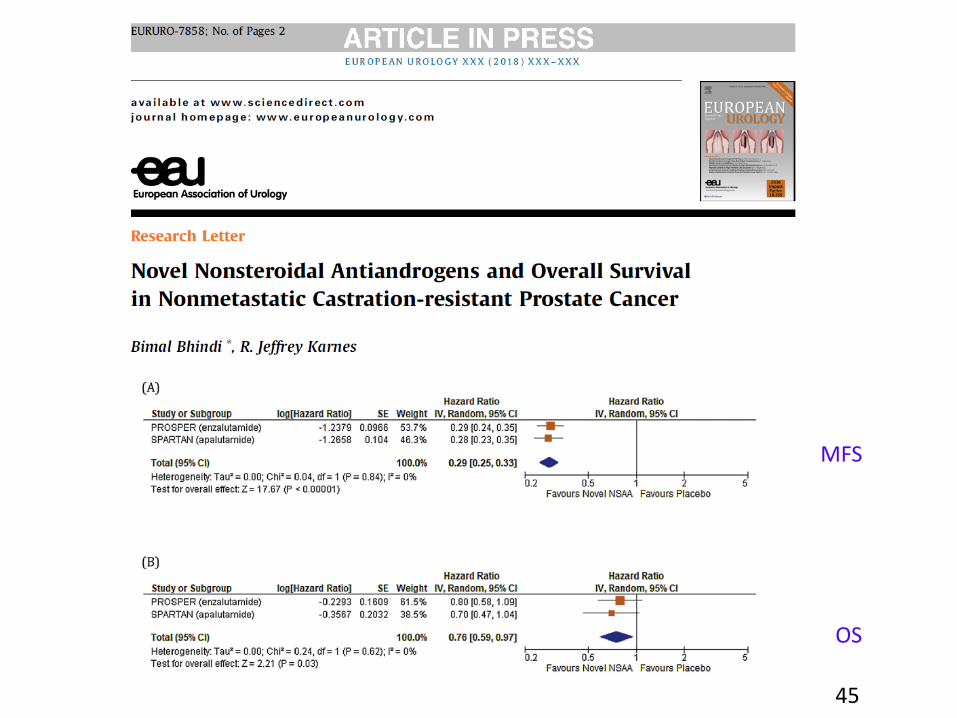
MFS
OS
45
46

Slide 27
Presented By Philip Kantoff at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Efectos adversos
47
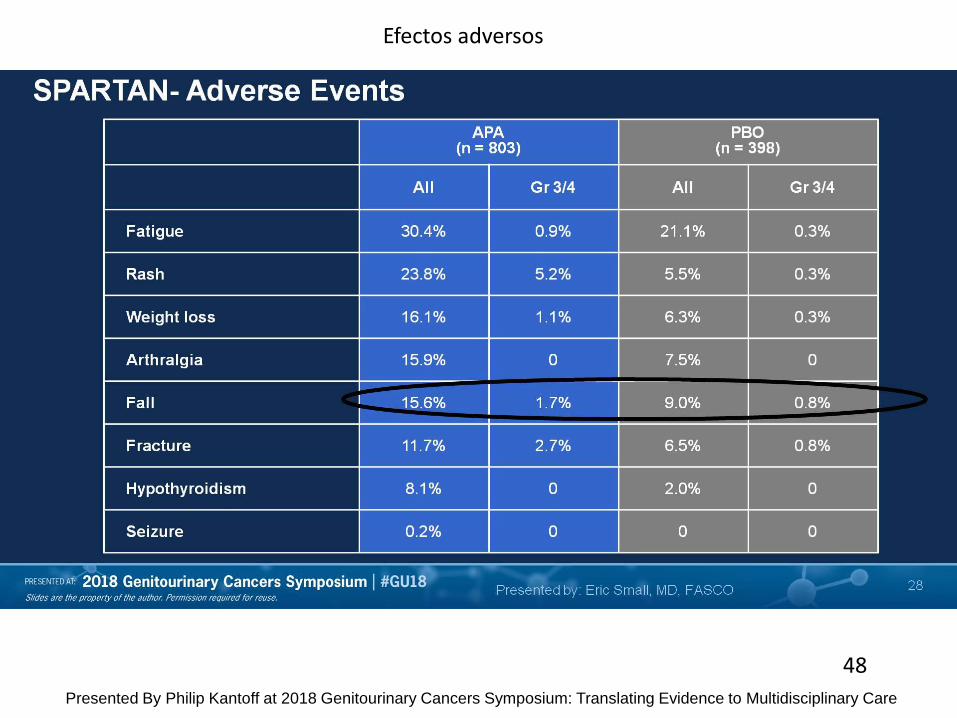
Slide 28
Presented By Philip Kantoff at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Efectos adversos
48
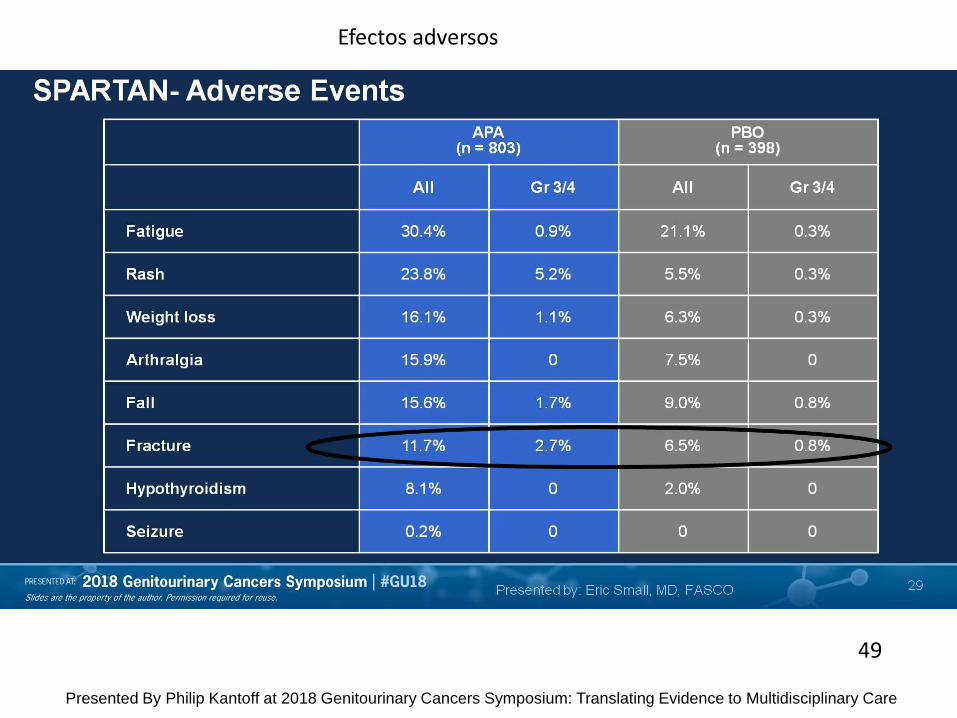
Slide 29
Presented By Philip Kantoff at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Efectos adversos
49
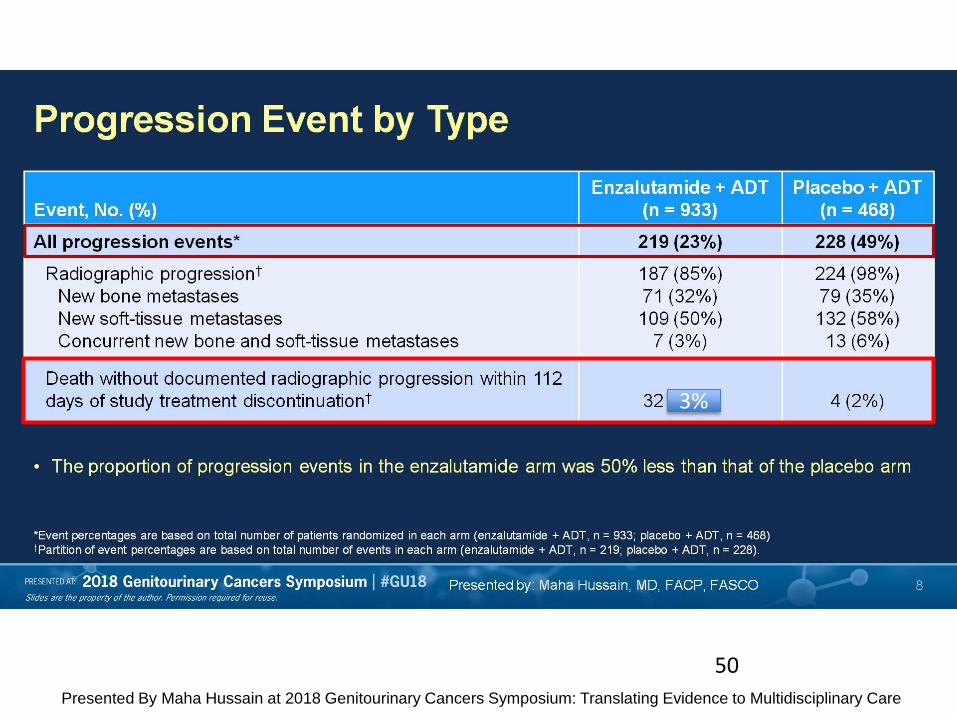
Progression Event by Type
Presented By Maha Hussain at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
50
3%
Conclusions
Presented By Philip Kantoff at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
66

• 1. Ambos estudios positivos, demostrando que la inhibición precoz (M0) de la señalización androgénica es eficaz
• 2. SG todavía no madura. Numerosos análisis apoyan la asociación entre SLM y SG.
• 3. Los efectos secundarios deben monitorizarse y explicarse de manera adecuada. Esto implica elegir muy bien el tipo de paciente a tratarse con estos agentes.
Conclusiones aceptadas sobre SPARTAN y PROSPER
Slide 25
Presented By Eric Small at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Estudio PROSPER
SPARTAN y PROSPER
¿Alguna novedad en ASCO 2018?
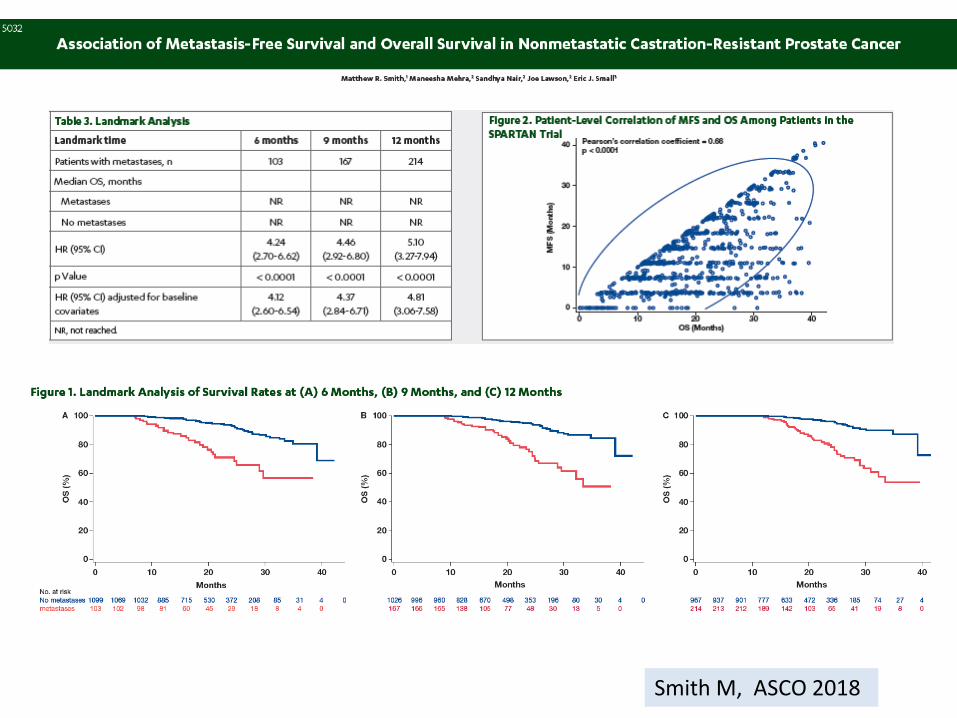
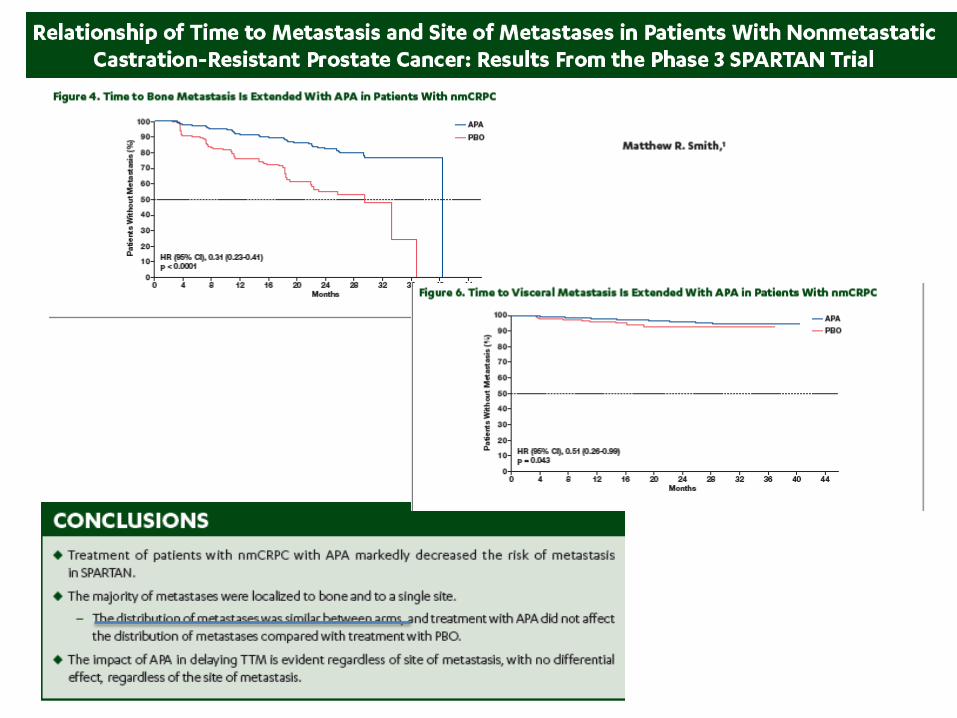
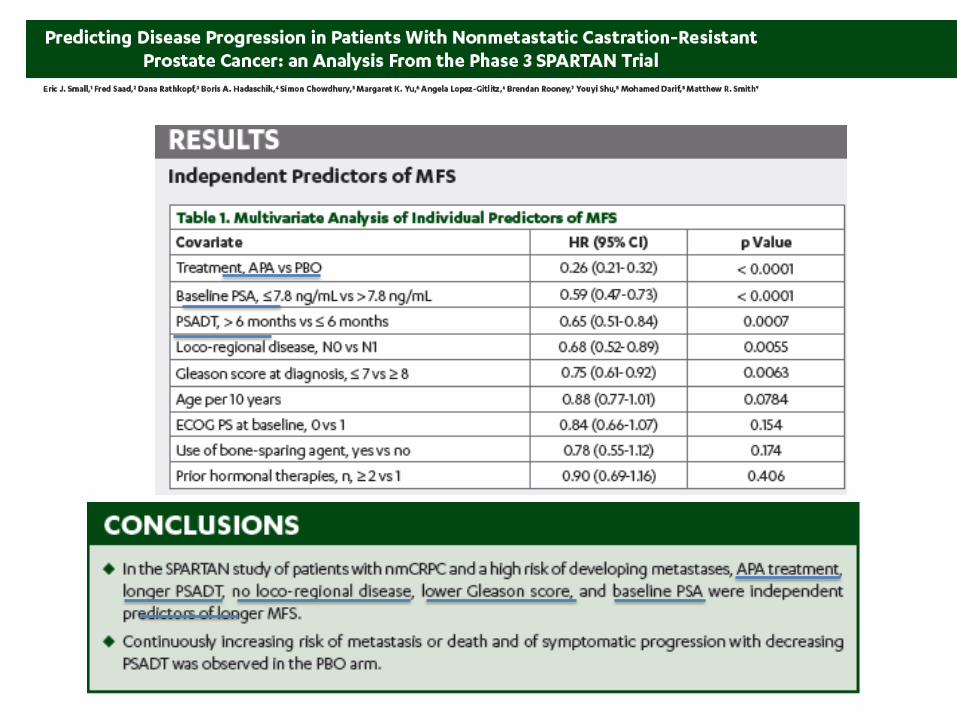
Smith M, ASCO 2018

Smith M, ASCO 2018

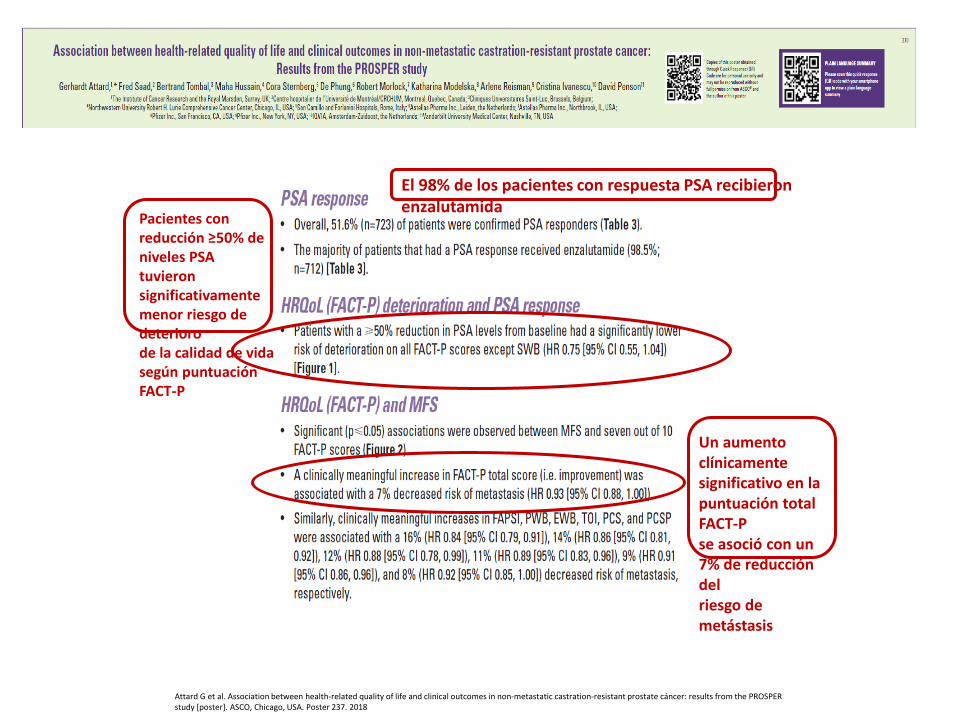
Attard G et al. Association between health-related quality of life and clinical outcomes in non-metastatic castration-resistant prostate cáncer: results from the PROSPER study [poster]. ASCO, Chicago, USA. Poster 237. 2018
Pacientes con reducción ≥50% de niveles PSA tuvieron significativamente menor riesgo de deterioro de la calidad de vida según puntuación FACT-P
Un aumento clínicamente significativo en la puntuación total FACT-P se asoció con un 7% de reducción del riesgo de metástasis
El 98% de los pacientes con respuesta PSA recibieron enzalutamida
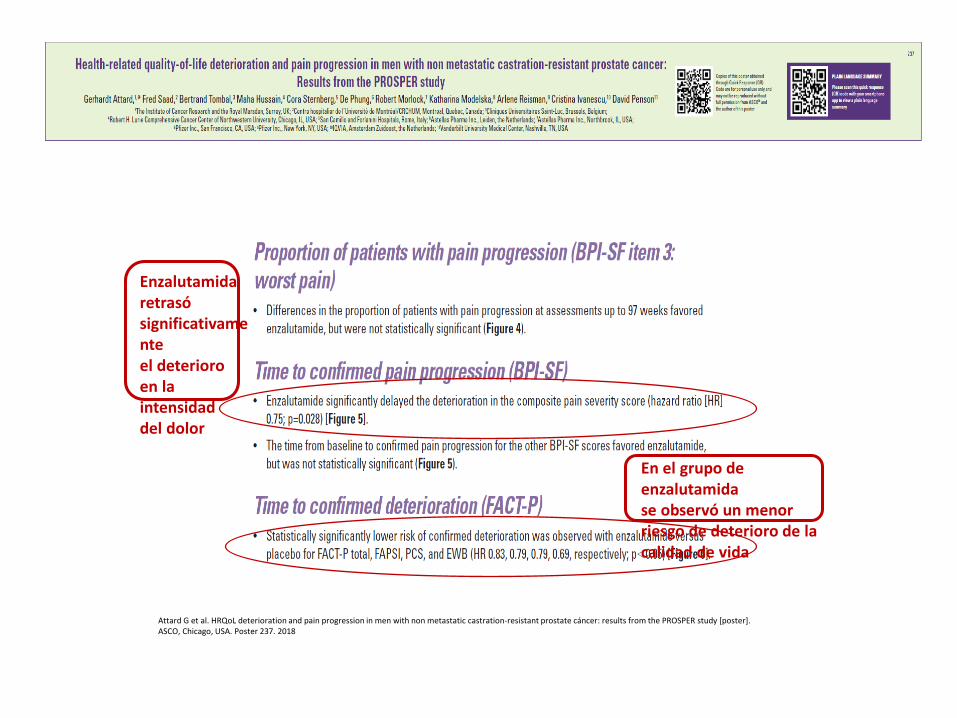
Attard G et al. HRQoL deterioration and pain progression in men with non metastatic castration-resistant prostate cáncer: results from the PROSPER study [poster]. ASCO, Chicago, USA. Poster 237. 2018
Enzalutamida retrasó significativamente el deterioro en la intensidad del dolor
En el grupo de enzalutamida se observó un menor riesgo de deterioro de la calidad de vida

FACT-P: mean change over time (PMM analysis)
PMM assumes data missing not at random
As expected, patients in both treatment arms experienced meaningful decline in FACT-P total score (>10 points) over time; the rate of decline was significantly slower in patients treated with enzalutamide
PROSPER: longitudinal analysis of FACT-P total scores in patients with nm-CRPC
Median FACT-P value over time
In PROSPER, good HRQoL was maintained during the treatment period in both groups
Deterioration in HRQoL would be expected as patients progress and age
PMM=pattern mixed model
Tombal B, et al. 2018 EAU Meeting, Copnehagen 60
CONCLUSIONES • Enzalutamida y apalutamida son nuevos agentes
indicados en pacientes CRPC M0 de alto riesgo ( ¡nuevo tratamiento estándar¡)
• El objetivo de Supervivencia libre de Metástasis ( SLM) parece adecuado, al mostrar una cada vez mayor evidencia de una estrecha asociación con la SG en este contexto.
• Buena tolerancia a ambos tratamientos, aunque deben tenerse en cuenta la exposición a largo plazo y las toxicidades específicas de cada agente
Gracias por su atención












![Bezirksärztesitzung CRC Sept. 2013.ppt [Kompatibilitätsmodus] · 2017. 7. 25. · Tumor Stadium (UICC-Klassifikation) Stadium I T1 N0 M0 T2 N0 M0 Stadium IIA T3 N0 M0 IIB T4a N0](https://static.fdocuments.ec/doc/165x107/6100eaec99e229501e68abe3/bezirksrztesitzung-crc-sept-2013ppt-kompatibilittsmodus-2017-7-25-tumor.jpg)