Anestesia pediatrica. Mitos, dogmas y evidencia.
116
Transcript of Anestesia pediatrica. Mitos, dogmas y evidencia.



ANESTESIA PEDIATRICA

ANESTESIA PEDIATRICA
MITOS, DOGMAS Y EVIDENCIAS.
DR. LUIS VERA LINARESLIMA 2011
email: [email protected]

SOBRE EVALUAR UN
MITO...

SOBRE EVALUAR UN
MITO...
• PROBAR LA VALIDEZ SOBRE EL MITO DANES DE QUE EL ALCOHOL PUEDE SER ABSORBIDO A TRAVES DE LOS PIES: ESTUDIO EXPERIMENTAL DE TIPO ABIERTO.

RESEARCH
CHRISTMAS 2010: RESEARCH
Testing thevalidityof theDanishurbanmyth thatalcohol canbe absorbed through feet: open labelled self experimentalstudy
Christian Stevns Hansen, doctor Louise Holmsgaard Færch, doctor Peter Lommer Kristensen, doctor andresearch fellow
ABSTRACTObjective To determine the validity of the Danish urban
myth that it is possible to get drunk by submerging feet in
alcohol.
Design Open labelled, self experimental study, with no
control group.
Setting Office of a Danish hospital.
Participants Three adults, median age 32 (range 31-35),
free of chronic skin and liver disease and non-dependent
on alcohol and psychoactive drugs.
Main outcome measures The primary end point was the
concentration of plasma ethanol (detection limit
2.2mmol/L (10mg/100mL)),measured every 30minutes
for three hours while feet were submerged in a washing-
upbowl containing the contents of three700mLbottles of
vodka. The secondary outcome was self assessment of
intoxication related symptoms (self confidence, urge to
speak, and number of spontaneous hugs), scored on a
scale of 0 to 10.
Results Plasma ethanol concentrations were below the
detection limit of 2.2mmol/L (10mg/100mL) throughout
the experiment. No significant changes were observed in
the intoxication related symptoms, although self
confidence and urge to speak increased slightly at the
start of the study, probably due to the setup.
Conclusion Our results suggest that feet are impenetrable
to the alcohol component of vodka.We therefore conclude
that the Danish urban myth of being able to get drunk by
submerging feet in alcoholic beverages is just that; amyth.
The implications of the study are many though.
INTRODUCTION
According to Danish urban folklore, it is possible tobecome drunk by submerging feet in alcoholic bev-erages. Furthermore, claims exist of urine becomingredwhen feet are submerged in beetroot juice. Becausethe transcutaneous transport of alcohol to the circula-tion may have widespread implications, such urbanmyths need to be investigated in a scientific setting.We determined whether alcohol can be detected in
the circulation of humans after submersion of their feet
in vodka; the Peace On Earth (Percutaneous EthanolAbsorption Could Evoke Ongoing NationwideEuphoria And Random Tender Hugs) study. Theresults could have great implications, by freeinghuman resources for other, relevant, activities.
METHODS
The Peace on Earth study was open labelled and selfexperimental, with no control group. It evaluated theeffect of submerging feet in 2100mLof vodka (three bot-tles’worth) on the concentration of plasma ethanol. Sec-ondary end points were intoxication related symptoms.Three healthy adults (all authors, CSH, LHF, and
PLK) agreed to participate. None had any chronic skinor liver disease or was dependent on alcohol or psy-choactive drugs.Nonewasmembers of localAlcoholicsAnonymous communities or had been implicated inserious incidents or socially embarrassing events relatedto alcohol during the week before the experiment.
Study protocol
The participants abstained from consuming alcohol24 hours before the experiment. The evening beforethe experiment they rubbed their feet with a loofah toremove skin debris. On the day of the experiment, abaseline blood sample was taken through a venousline. The participants then submerged their feet in awashing-up bowl containing the contents of three700mL bottles of vodka (Karloff vodka;MR tefánika,Cífer, Slovakia, 37.5% by volume). Before each bloodsample was taken the venous catheter and cannulawere flushed with saline by a trained study nurse.Plasma ethanol concentrations were determinedevery 30 minutes for three hours. Blood sampleswere taken to the laboratory for immediate analysisby the study nurse. Plasma ethanol concentrations,measured as soon as possible in case of rapid andpotentially fatal increases, were determined using aphotometric method, with a detection limit of2.2 mmol/L (10 mg/100 mL, corresponding to0.010% weight/volume). Participants simultaneously
Endocrinology Section, Departmentof Cardiology and Endocrinology,Hillerød Hospital, Dyrehavevej 29,DK-3400 Hillerød, DenmarkCorrespondence to: P L [email protected]
Cite this as: BMJ 2010;341:c6812doi:10.1136/bmj.c6812
BMJ | ONLINE FIRST | bmj.com page 1 of 3

• HANSEN ET AL. BMJ 2010; 341:C6812.
• POBLACION DE ESTUDIO: 3 MDS.
• METODO: PIES INMERSOS EN VODKA DURANTE 3 HORAS.
• RESULTADOS: NIVELES DE ETANOL, SINTOMAS SUBJETIVOS.

SINTOMAS DE INTOXICACION
• HANSEN. BMJ 2010

CONCLUSIONES
• NUESTROS RESULTADOS SUGIEREN QUE LOS PIES SON IMPENETRABLES AL COMPONENTE ALCOHOLICO DEL VODKA Y EN TANTO CONCLUIMOS QUE ESTE MITO DANES ES TAN
SOLO ESO... UN MITO

OBJETIVOS DE ESTA CONFERENCIA
• EVALUAR ALGUNOS MITOS Y CREENCIAS ACTUALES DE LA PRACTICA ANESTESICA PEDIATRICA.

OBJETIVOS DE ESTA CONFERENCIA
• USAR LA EVIDENCIA ACTUAL PARA DAR SOPORTE O RECHAZAR ALGUNAS PRACTICAS EN ANESTESIA PEDIATRICA:
• VIA AEREA
• AGENTES INHALADOS
• OTRAS DROGAS
• MISCELANEAS
• “CREER A CIEGAS ES PELIGROSO” - LUYIA

DOGMAS SOBRE VIA AEREA EN
PEDIATRIA

DOGMAS SOBRE VIA AEREA EN
PEDIATRIA
• LA PARTE MAS ESTRECHA DE LA VIA AEREA EN NIÑOS ESTA A NIVEL DEL CARTILAGO CRICOIDES.

DOGMAS SOBRE VIA AEREA EN
PEDIATRIA
• LA PARTE MAS ESTRECHA DE LA VIA AEREA EN NIÑOS ESTA A NIVEL DEL CARTILAGO CRICOIDES.
• EL DIAMETRO DEL DEDO MEÑIQUE PREDICE DE FORMA MUY PRECISA EL TAMAÑO DEL TUBO ENDOTRAQUEAL.

DOGMAS SOBRE VIA AEREA EN
PEDIATRIA
• LA PARTE MAS ESTRECHA DE LA VIA AEREA EN NIÑOS ESTA A NIVEL DEL CARTILAGO CRICOIDES.
• EL DIAMETRO DEL DEDO MEÑIQUE PREDICE DE FORMA MUY PRECISA EL TAMAÑO DEL TUBO ENDOTRAQUEAL.
• LA PRESION DEL CARTILAGO CRICOIDES ES UN COMPONENTE IMPORTANTE EN LA INDUCCION DE SECUENCIA RAPIDA.

DOGMAS SOBRE VIA AEREA EN
PEDIATRIA
• LA PARTE MAS ESTRECHA DE LA VIA AEREA EN NIÑOS ESTA A NIVEL DEL CARTILAGO CRICOIDES.
• EL DIAMETRO DEL DEDO MEÑIQUE PREDICE DE FORMA MUY PRECISA EL TAMAÑO DEL TUBO ENDOTRAQUEAL.
• LA PRESION DEL CARTILAGO CRICOIDES ES UN COMPONENTE IMPORTANTE EN LA INDUCCION DE SECUENCIA RAPIDA.
• LOS TUBOS ENDOTRAQUEALES CON CUFF SON SEGUROS/PELIGROSOS EN NIÑOS.

ANATOMIA DE LA VIA AEREA EN PEDIATRIA:TRABAJO INICIAL
• “EN EL INFANTE... EL ANILLO CRICOIDEO PUEDE SER MAS PEQUEÑO QUE LA GLOTIS O QUE EL DIAMETRO INTERNO DE LA TRAQUEA”
• “EN INFANTES Y NIÑOS, BAYEUX, USANDO CADAVERES Y SECCIONES ANATOMICAS, ENCONTRO QUE LA CIRCUNFERENCIA DEL ANILLO CRICOIDEO ERA MAS ESTRECHA QUE EL DE LA TRAQUEA O QUE EL DE LA GLOTIS”.
• (BAYEUX PRESS MED. 1897: ECKENHOFF, ANESTHESIOLOGY 1951)

Anesthesiology 2003; 98:41–5 © 2003 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Developmental Changes of Laryngeal Dimensions inUnparalyzed, Sedated ChildrenRonald S. Litman, D.O.,* Eric E. Weissend, M.D.,† Dean Shibata, M.D.,‡ Per-Lennart Westesson, M.D., Ph.D., D.D.S.§
Background: Knowledge of the influence of age on laryngealdimensions is essential for all practitioners whose interest isthe pediatric airway. Early cadaver studies documented that thelarynx is conically shaped, with the apex of the cone caudallypositioned at the nondistensible cricoid cartilage. These dimen-sions change during childhood, as the larynx assumes a morecylindrical shape. The authors analyzed laryngeal dimensionsduring development to determine if this relationship continuesin unparalyzed children in whom laryngeal muscles are toni-cally active. The authors determined the relationships betweenthe vocal cord, sub–vocal cord, and cricoid ring dimensions andthe influence of age on these relationships.
Methods: Infants and children undergoing magnetic reso-nance imaging with propofol sedation had determinations ofthe transverse and anterior–posterior (AP) dimensions of thelarynx at the most cephalad level of the larynx (vocal cords)and the most caudad level (cricoid). Most patients had an addi-tional measurement (sub–vocal cord) at a level between thevocal cords and the cricoid ring. Relationships were obtainedby plotting age against laryngeal dimensions and the ratio oflaryngeal dimensions at different levels within the larynx.
Results: The authors measured transverse and AP laryngealdimensions in 99 children, aged 2 months–13 yr. The relation-ship between the transverse and AP dimensions at all levels ofthe larynx did not change during development. Transverse andAP dimensions increased linearly with age at all levels of thelarynx. In all children studied, the narrowest portion of thelarynx was the transverse dimension at the level of the vocalcords. Transverse dimensions increased linearly in a caudaddirection through the larynx (P < 0.001), while AP dimensionsdid not change relative to laryngeal level. The shape of thecricoid ring did not change throughout childhood.
Conclusions: In sedated, unparalyzed children, the narrowestportions of the larynx are the glottic opening (vocal cord level)and the immediate sub–vocal cord level, and there is no changein the relationships of these dimensions relative to cricoiddimensions throughout childhood.
THE development and growth of the larynx during child-hood has been a subject of interest for over a century.1
Knowledge of the influence of the age of the child onlaryngeal dimensions is essential for all practitionerswhose interest is the pediatric airway. Early studies incadaver specimens documented the cartilaginous and
bony framework of the larynx throughout childhood.1–3
These studies determined that the larynx is conicallyshaped, with the apex of the “cone” caudally positionedat the nondistensible cricoid cartilage. These dimensionschange during childhood as the larynx assumes a cylin-drical, rather than a conical shape.4 It is unknown if thisrelationship continues to exist in unparalyzed children inwhom laryngeal muscles demonstrate tonic activity.5
Therefore, we undertook this study to determine the influ-ence of age on laryngeal dimensions. Most specifically, wewere interested in the relationships between vocal cord,sub–vocal cord, and cricoid ring dimensions, and howthese relationships change as children grow. We hypothe-sized that these relationships change during developmentand may influence clinical airway management.
Materials and Methods
The Research Subjects’ Review Board of the Universityof Rochester (Rochester, New York) approved thisstudy, and written informed consent was obtained fromall parents of children in the study. Children who wereold enough to understand that they were participating ina research study gave their assent. Children aged 0–14 yrwho presented for an elective magnetic resonance im-aging scan with deep sedation were eligible to partici-pate. Consecutive children were enrolled within thelimits of investigator-related and clinical situations. Ex-clusion criteria included obvious anatomical deformitiesof the head or neck, or any other condition the investi-gators felt would cause abnormal laryngeal anatomy.Children who received airway management with either alaryngeal mask airway or endotracheal tube were alsoexcluded.
The study was performed in children who were deeplysedated with 200 !g · kg!1 · min!1 propofol. Mostchildren did not previously have an indwelling intrave-nous catheter and therefore initially received a maskanesthetic with sevoflurane and nitrous oxide, both ofwhich were discontinued after intravenous catheterplacement. Spontaneous ventilation was maintainedthroughout the procedure. A nasal cannula providedoxygen, usually at 2 l/min. Monitors included continuouselectrocardiography, pulse oximetry, capnography (viathe nasal cannula), and intermittent automated bloodpressure determinations (Medrad, Inc., Indianola, PA). Abest attempt was made to position the child’s head in theneutral position, usually with a folded sheet beneath theneck or shoulders. Occasionally, a nasal or oral airwaydevice was used to assist with maintenance of upper
* Associate Professor of Anesthesiology and Pediatrics, University of Pennsyl-vania School of Medicine, Philadelphia, Pennsylvania. † Staff Anesthesiologist,Lackland Air Force Medical Center, San Antonio, Texas. ‡ Assistant Professor ofRadiology, University of Washington School of Medicine, Seattle, Washington.§ Professor of Radiology, University of Rochester School of Medicine andDentistry.
Received from the Departments of Anesthesiology and Radiology, Universityof Rochester School of Medicine and Dentistry, Rochester, New York. Submittedfor publication February 27, 2002. Accepted for publication August 20, 2002.Supported by the Departments of Anesthesiology and Radiology, University ofRochester School of Medicine and Dentistry, Rochester, New York.
Address reprint requests to Dr. Litman: Department of Anesthesiology andCritical Care Medicine, Children’s Hospital of Philadelphia, 34th Street and CivicCenter Boulevard, Philadelphia, Pennsylvania 19104. Address electronic mail to:[email protected]. Individual article reprints may be purchased throughthe Journal Web site, www.anesthesiology.org.
Anesthesiology, V 98, No 1, Jan 2003 41
Anesthesiology 2003; 98:41–5 © 2003 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Developmental Changes of Laryngeal Dimensions inUnparalyzed, Sedated ChildrenRonald S. Litman, D.O.,* Eric E. Weissend, M.D.,† Dean Shibata, M.D.,‡ Per-Lennart Westesson, M.D., Ph.D., D.D.S.§
Background: Knowledge of the influence of age on laryngealdimensions is essential for all practitioners whose interest isthe pediatric airway. Early cadaver studies documented that thelarynx is conically shaped, with the apex of the cone caudallypositioned at the nondistensible cricoid cartilage. These dimen-sions change during childhood, as the larynx assumes a morecylindrical shape. The authors analyzed laryngeal dimensionsduring development to determine if this relationship continuesin unparalyzed children in whom laryngeal muscles are toni-cally active. The authors determined the relationships betweenthe vocal cord, sub–vocal cord, and cricoid ring dimensions andthe influence of age on these relationships.
Methods: Infants and children undergoing magnetic reso-nance imaging with propofol sedation had determinations ofthe transverse and anterior–posterior (AP) dimensions of thelarynx at the most cephalad level of the larynx (vocal cords)and the most caudad level (cricoid). Most patients had an addi-tional measurement (sub–vocal cord) at a level between thevocal cords and the cricoid ring. Relationships were obtainedby plotting age against laryngeal dimensions and the ratio oflaryngeal dimensions at different levels within the larynx.
Results: The authors measured transverse and AP laryngealdimensions in 99 children, aged 2 months–13 yr. The relation-ship between the transverse and AP dimensions at all levels ofthe larynx did not change during development. Transverse andAP dimensions increased linearly with age at all levels of thelarynx. In all children studied, the narrowest portion of thelarynx was the transverse dimension at the level of the vocalcords. Transverse dimensions increased linearly in a caudaddirection through the larynx (P < 0.001), while AP dimensionsdid not change relative to laryngeal level. The shape of thecricoid ring did not change throughout childhood.
Conclusions: In sedated, unparalyzed children, the narrowestportions of the larynx are the glottic opening (vocal cord level)and the immediate sub–vocal cord level, and there is no changein the relationships of these dimensions relative to cricoiddimensions throughout childhood.
THE development and growth of the larynx during child-hood has been a subject of interest for over a century.1
Knowledge of the influence of the age of the child onlaryngeal dimensions is essential for all practitionerswhose interest is the pediatric airway. Early studies incadaver specimens documented the cartilaginous and
bony framework of the larynx throughout childhood.1–3
These studies determined that the larynx is conicallyshaped, with the apex of the “cone” caudally positionedat the nondistensible cricoid cartilage. These dimensionschange during childhood as the larynx assumes a cylin-drical, rather than a conical shape.4 It is unknown if thisrelationship continues to exist in unparalyzed children inwhom laryngeal muscles demonstrate tonic activity.5
Therefore, we undertook this study to determine the influ-ence of age on laryngeal dimensions. Most specifically, wewere interested in the relationships between vocal cord,sub–vocal cord, and cricoid ring dimensions, and howthese relationships change as children grow. We hypothe-sized that these relationships change during developmentand may influence clinical airway management.
Materials and Methods
The Research Subjects’ Review Board of the Universityof Rochester (Rochester, New York) approved thisstudy, and written informed consent was obtained fromall parents of children in the study. Children who wereold enough to understand that they were participating ina research study gave their assent. Children aged 0–14 yrwho presented for an elective magnetic resonance im-aging scan with deep sedation were eligible to partici-pate. Consecutive children were enrolled within thelimits of investigator-related and clinical situations. Ex-clusion criteria included obvious anatomical deformitiesof the head or neck, or any other condition the investi-gators felt would cause abnormal laryngeal anatomy.Children who received airway management with either alaryngeal mask airway or endotracheal tube were alsoexcluded.
The study was performed in children who were deeplysedated with 200 !g · kg!1 · min!1 propofol. Mostchildren did not previously have an indwelling intrave-nous catheter and therefore initially received a maskanesthetic with sevoflurane and nitrous oxide, both ofwhich were discontinued after intravenous catheterplacement. Spontaneous ventilation was maintainedthroughout the procedure. A nasal cannula providedoxygen, usually at 2 l/min. Monitors included continuouselectrocardiography, pulse oximetry, capnography (viathe nasal cannula), and intermittent automated bloodpressure determinations (Medrad, Inc., Indianola, PA). Abest attempt was made to position the child’s head in theneutral position, usually with a folded sheet beneath theneck or shoulders. Occasionally, a nasal or oral airwaydevice was used to assist with maintenance of upper
* Associate Professor of Anesthesiology and Pediatrics, University of Pennsyl-vania School of Medicine, Philadelphia, Pennsylvania. † Staff Anesthesiologist,Lackland Air Force Medical Center, San Antonio, Texas. ‡ Assistant Professor ofRadiology, University of Washington School of Medicine, Seattle, Washington.§ Professor of Radiology, University of Rochester School of Medicine andDentistry.
Received from the Departments of Anesthesiology and Radiology, Universityof Rochester School of Medicine and Dentistry, Rochester, New York. Submittedfor publication February 27, 2002. Accepted for publication August 20, 2002.Supported by the Departments of Anesthesiology and Radiology, University ofRochester School of Medicine and Dentistry, Rochester, New York.
Address reprint requests to Dr. Litman: Department of Anesthesiology andCritical Care Medicine, Children’s Hospital of Philadelphia, 34th Street and CivicCenter Boulevard, Philadelphia, Pennsylvania 19104. Address electronic mail to:[email protected]. Individual article reprints may be purchased throughthe Journal Web site, www.anesthesiology.org.
Anesthesiology, V 98, No 1, Jan 2003 41

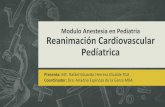
EVALUACION POR RMN DE LA VIA AEREA PEDIATRICA
• A: CUERDAS VOCALES
• B: NIVEL SUBGLOTICO
• C: NIVEL SUBGLOTICO
• ANILLO CRICOIDEO
in spontaneously breathing, unparalyzed children, therigid cricoid ring is functionally the narrowest portion ofthe larynx.
A limitation of these findings is that we did not attemptto image the larynx in any particular phase of respira-tion. Since vocal cord dimensions likely change in spon-taneously breathing, sedated children, the dimensionsthat we measured should be considered to be an averagemeasurement during movement of the vocal cords dur-ing spontaneous respiration. Therefore, it is possible thatin some children, the vocal cords were “captured” in amore adducted state than usual, as in expiration. If thisoccurred in a significant number of our subjects, theshape of the larynx in the transverse direction would bemore cylindrical than conical. An alternative explanationfor our findings is the possible influence of propofol onvocal cord position. In dogs, propofol depresses vocalcord abductor (posterior cricoarytenoid muscle) and vo-cal cord tensor (cricothyroid muscle) activity8 and may
have influenced vocal cord positions in the children westudied.
In 1951, Eckenhoff4 published a seminal article oncharacteristics of the infant larynx and their influence onendotracheal anesthesia. This article was one of the firstto emphasize that the cricoid cartilage is functionally thenarrowest point of the upper respiratory tract of thechild. Eckenhoff described the cricoid plate as “inclinedposteriorly at its superior aspect, so that the larynx isfunnel shaped with the narrowest point of the funnel atthe laryngeal exit.” This narrowest point is described aspossibly smaller than more cephalad portions of thetrachea. Eckenhoff stated that as the child grows, thecricoid plate becomes vertical, and the larynx becomesmore cylindrical shaped. He derived this informationfrom Bayeux,1 who used moulages and anatomic sec-tions of 15 children, aged 4 months to 14 yr. Bayeuxdocumented that the circumference of the cricoid ringwas narrower than that of the trachea or the glottis. Ourresults do not allow us to make direct comparisons withthe findings of Eckenhoff and Bayeux since we measureddimensions in the tonically active larynx.
The clinical importance of our findings is speculative.On one hand, our results indicate that choosing an en-dotracheal tube based on the size of the cricoid ring maynot prevent mucosal damage to the larynx cephalad tothe cricoid ring in unparalyzed children. On the otherhand, these more cephalad portions of the larynx consistof yielding structures that distend with placement of arelatively larger endotracheal tube. The cricoid ring isunyielding and prone to development of edema andscarring in response to excessive mucosal pressures.
Fig. 4. Representative sample of axial magnetic resonance im-aging slices through the vocal cords (A), subglottic levels (B andC), and cricoid ring (D). Transverse diameters increase in acaudad direction.
Fig. 3. Box plots demonstrating the relationship between tra-cheal transverse (top) and anterior–posterior (A-P; bottom) di-ameters at the levels of the vocal cords, subglottic area, andcricoid ring. Transverse diameters increased linearly in acaudad direction (P < 0.001). The middle line of the box is the50th percentile, the ends of the boxes are the 25th and 75thpercentiles, and the whiskers represent the 5th and 95th per-centiles. The square box represents the mean, the 1st and 99thpercentiles are denoted by Xs, and the dashed lines are theminimum and maximum values.
44 LITMAN ET AL.
Anesthesiology, V 98, No 1, Jan 2003 Litman, Anesthesiology 2003

EVALUACION POR RMN DE LA VIA AREA PEDIATRICA
in spontaneously breathing, unparalyzed children, therigid cricoid ring is functionally the narrowest portion ofthe larynx.
A limitation of these findings is that we did not attemptto image the larynx in any particular phase of respira-tion. Since vocal cord dimensions likely change in spon-taneously breathing, sedated children, the dimensionsthat we measured should be considered to be an averagemeasurement during movement of the vocal cords dur-ing spontaneous respiration. Therefore, it is possible thatin some children, the vocal cords were “captured” in amore adducted state than usual, as in expiration. If thisoccurred in a significant number of our subjects, theshape of the larynx in the transverse direction would bemore cylindrical than conical. An alternative explanationfor our findings is the possible influence of propofol onvocal cord position. In dogs, propofol depresses vocalcord abductor (posterior cricoarytenoid muscle) and vo-cal cord tensor (cricothyroid muscle) activity8 and may
have influenced vocal cord positions in the children westudied.
In 1951, Eckenhoff4 published a seminal article oncharacteristics of the infant larynx and their influence onendotracheal anesthesia. This article was one of the firstto emphasize that the cricoid cartilage is functionally thenarrowest point of the upper respiratory tract of thechild. Eckenhoff described the cricoid plate as “inclinedposteriorly at its superior aspect, so that the larynx isfunnel shaped with the narrowest point of the funnel atthe laryngeal exit.” This narrowest point is described aspossibly smaller than more cephalad portions of thetrachea. Eckenhoff stated that as the child grows, thecricoid plate becomes vertical, and the larynx becomesmore cylindrical shaped. He derived this informationfrom Bayeux,1 who used moulages and anatomic sec-tions of 15 children, aged 4 months to 14 yr. Bayeuxdocumented that the circumference of the cricoid ringwas narrower than that of the trachea or the glottis. Ourresults do not allow us to make direct comparisons withthe findings of Eckenhoff and Bayeux since we measureddimensions in the tonically active larynx.
The clinical importance of our findings is speculative.On one hand, our results indicate that choosing an en-dotracheal tube based on the size of the cricoid ring maynot prevent mucosal damage to the larynx cephalad tothe cricoid ring in unparalyzed children. On the otherhand, these more cephalad portions of the larynx consistof yielding structures that distend with placement of arelatively larger endotracheal tube. The cricoid ring isunyielding and prone to development of edema andscarring in response to excessive mucosal pressures.
Fig. 4. Representative sample of axial magnetic resonance im-aging slices through the vocal cords (A), subglottic levels (B andC), and cricoid ring (D). Transverse diameters increase in acaudad direction.
Fig. 3. Box plots demonstrating the relationship between tra-cheal transverse (top) and anterior–posterior (A-P; bottom) di-ameters at the levels of the vocal cords, subglottic area, andcricoid ring. Transverse diameters increased linearly in acaudad direction (P < 0.001). The middle line of the box is the50th percentile, the ends of the boxes are the 25th and 75thpercentiles, and the whiskers represent the 5th and 95th per-centiles. The square box represents the mean, the 1st and 99thpercentiles are denoted by Xs, and the dashed lines are theminimum and maximum values.
44 LITMAN ET AL.
Anesthesiology, V 98, No 1, Jan 2003
Respirando espontaneamenteSedadoNiños sin paralisis
Litman, Anesthesiology 2003

Pediatric AnesthesiologySection Editor; Peter J. Davis
Pediatric Laryngeal Dimensions: An Age-Based Analysis
Priti G. Dalal, MD, FRCA*
David Murray, MD†
Anna H. Messner, MD‡
Angela Feng, MD!
John McAllister, MD¶
David Molter, MD#
BACKGROUND: In children, the cricoid is considered the narrowest portion of the“funnel-shaped” airway. Growth and development lead to a transition to the morecylindrical adult airway. A number of airway decisions in pediatric airway practiceare based on this transition from the pediatric to the adult airway. Our primary aimin this study was to measure airway dimensions in children of various ages. Themeasures of the glottis and cricoid regions were used to determine whether atransition from the funnel-shaped pediatric airway to the cylindrical adult airwaycould be identified based on images obtained from video bronchoscopy.METHODS: One hundred thirty-five children (ASA physical status 1 or 2) aged 6 mo to13 yr were enrolled for measurement of laryngeal dimensions, including cross-sectional area (G-CSA), anteroposterior and transverse diameters at the level of theglottis and the cricoid (C-CSA), using the video bronchoscopic technique undergeneral anesthesia.RESULTS: Of the 135 children enrolled in the study, seven patients were excludedfrom the analysis mainly because of poor image quality. Of the 128 children studied(79 boys and 49 girls), mean values (!standard deviation) for the demographicdata were age 5.9 (!3.3) yr, height 113.5 (!22.2) cm and weight 23.5 (!13) kg.Overall, the mean C-CSA was larger than the G-CSA (48.9 ! 15.5 mm2 vs 30 ! 16.5mm2, respectively). This relationship was maintained throughout the study popu-lation starting from 6 mo of age (P " 0.001, r # 0.45, power # 1). The mean ratiofor C-CSA: G-CSA was 2.1 ! 1.2. There was a positive correlation between G- andthe C-CSA versus age (r # 0.36, P " 0.001; r # 0.27, P # 0.001, respectively), height(r # 0.34, P " 0.001; r # 0.29, P " 0.001, respectively), and weight (r # 0.35, P "0.001; r # 0.25, P # 0.003, respectively). No significant gender differences in themean values of the studied variables were observed.CONCLUSION: In this study of infants and children, the glottis rather than cricoid wasthe narrowest portion of the pediatric airway. Similar to adults, the pediatricairway is more cylindrical than funnel shaped based on these video bronchoscopicimages. Further studies are needed to determine whether these static airwaymeasurements in anesthetized and paralyzed children reflect the dynamic charac-teristics of the glottis and cricoid in children.(Anesth Analg 2009;108:1475–9)
The pediatric laryngeal and cricoid relationship hasbeen described as “funnel-shaped” with the apex ofthe funnel at the level of the cricoid.1 This funnel-shaped airway description, based on a limited number
of postmortem airway measurements, forms the ana-tomical basis for a number of pediatric airway man-agement decisions.1–3 Recent clinical studies conductedusing different measurement techniques measuredairway dimensions using two different techniques(magnetic resonance imaging and videobronchos-copy) and found that the glottis is narrower than thecricoid.4,5 Anatomic airway dimensions in a range ofpediatric age groups would help resolve the contrast-ing airway descriptions and determine whether, andwhen, a transition occurs from the funnel-shapedpediatric airway to the more cylindrical adult airway.In addition, a method to measure the airway might
This article has supplementary material on the Web site:www.anesthesia-analgesia.org.
From the *Department of Anesthesiology, Penn State Milton S HersheyMedical Center, Hershey, Pennsylvania; †Department of Anesthesiology,Washington University School of Medicine, St Louis Children’s Hospital,St Louis, Missouri; ‡Department of Otolaryngology/Head and NeckSurgery Lucile Packard Children’s Hospital, Stanford University,Palo Alto, California; !Kaiser Foundation Hospital, Oakland, Cali-fornia; ¶Department of Anesthesiology, Washington UniversitySchool of Medicine, St Louis Children’s Hospital, St Louis, Missouri;and #Department of Otolaryngology, Washington UniversitySchool of Medicine, St Louis Children’s Hospital, St Louis, Missouri.
Accepted for publication December 8, 2008.Dr. David Murray funded by NIH AHRQ 1 U18 HS016652-01
(Murray, PI); and the Division of Clinical and Translation Research,Department of Anesthesiology, Washington University School ofMedicine, St Louis, MO 63110.
This study is attributed to the Department of Anesthesiology, StLouis Children’s Hospital, No. 5S31, Washington University Schoolof Medicine, St Louis, MO 63110.
Partly presented as poster at the Society for Pediatric Anesthesia,Fort Myers, FL, February 2006 and at the IARS 81st Clinical andScientific Congress, Orlando, FL, March 2007.
Address correspondence and reprint requests to Dr. Priti G. Dalal,Department of Anesthesiology, H187, Penn State Milton S HersheyMedical Center, Hershey, PA 17033. Address e-mail to [email protected].
Copyright © 2009 International Anesthesia Research SocietyDOI: 10.1213/ane.0b013e31819d1d99
Vol. 108, No. 5, May 2009 1475

MIDIENDO LAS DIMENSIONES LARINGEAS POR VIDEO BRONCOSCOPIA...
gender differences analyses, the unpaired t-test (para-metric data) and the Mann–Whitney Rank Sum test(nonparametric data) were applied to analyze thedifferences in values of each of the variables betweenmale and female children. A P value !0.05 wasconsidered as significant.
RESULTSOverall, 135 patients were enrolled in the study. Of
these, seven patients were excluded from the analysismainly because of poor image quality. Of the 128children studied (79 boys and 49 girls), mean values("sd) for the demographic data were age 5.9 ("3.3) yr,height 113.5 ("22.2) cm, and weight 23.5 ("13) kg. Therelationship between C-CSA and the G-CSA wasgiven by the equation C-CSA # 36.157 $ (0.426 %G-CSA), r # 0.45, P ! 0.001, power # 1. The C-CSA
Figure 1. Measuring laryngeal dimen-sions. The catheter tip touching thegraph paper (a), the glottis (b), andcricoid (c) regions.
Figure 2. Scatterplot with regression line and confidenceinterval lines for the cross-sectional areas (CSA) versus age.C-CSA # cricoid cross-sectional area; G-CSA # glotticcross-sectional area.
Figure 3. Box and whiskers plot for the diameter measure-ments in the study population, n # 128. G-AP # glotticanteroposterior diameter; G-trans # glottic transverse diam-eter; C-AP # cricoid anteroposterior diameter; C-Trans #cricoid transverse diameter.
Table 1. Results of the Linear Regression Analysis for LaryngealDimensions Versus Age, Height, and Weight, Respectively,in 128 Patients
Age Height WeightG-CSA r # 0.36 r # 0.34 r # 0.35
P ! 0.001 P ! 0.001 P ! 0.001G-AP r # 0.38 r # 0.36 r # 0.39
P ! 0.001 P ! 0.001 P ! 0.001G-trans r # 0.24 r # 0.22 r # 0.17
P # 0.005 P # 0.009 P # 0.047C-CSA r # 0.27 r # 0.29 r # 0.25
P # 0.001 P ! 0.001 P # 0.003C-AP r # 0.13 r # 0.12 r # 0.12
P # 0.129 P # 0.167 P # 0.14C-trans r # 0.13 r # 0.19 r # 0.12
P # 0.117 P # 0.03 P # 0.18Cricoid:glottic CSA r # 0.18 r # 0.11 r # 0.14
P # 0.04 P # 0.18 P # 0.11G-CSA # glottic cross-sectional area; G-AP # glottic anteroposterior diameter; G-trans # glottictransverse diameter; C-CSA # cricoid crosssectional area; C-AP # cricoid anteroposterior diam-eter; C-Trans # cricoid transverse diameter.
Vol. 108, No. 5, May 2009 © 2009 International Anesthesia Research Society 1477
Dalal, Anesth Anag 2009

DIAGRAMA DE DISPERSION DE LAS SECCIONES CRUZADAS DE AREA GLOTICA Y CRICOIDEA
gender differences analyses, the unpaired t-test (para-metric data) and the Mann–Whitney Rank Sum test(nonparametric data) were applied to analyze thedifferences in values of each of the variables betweenmale and female children. A P value !0.05 wasconsidered as significant.
RESULTSOverall, 135 patients were enrolled in the study. Of
these, seven patients were excluded from the analysismainly because of poor image quality. Of the 128children studied (79 boys and 49 girls), mean values("sd) for the demographic data were age 5.9 ("3.3) yr,height 113.5 ("22.2) cm, and weight 23.5 ("13) kg. Therelationship between C-CSA and the G-CSA wasgiven by the equation C-CSA # 36.157 $ (0.426 %G-CSA), r # 0.45, P ! 0.001, power # 1. The C-CSA
Figure 1. Measuring laryngeal dimen-sions. The catheter tip touching thegraph paper (a), the glottis (b), andcricoid (c) regions.
Figure 2. Scatterplot with regression line and confidenceinterval lines for the cross-sectional areas (CSA) versus age.C-CSA # cricoid cross-sectional area; G-CSA # glotticcross-sectional area.
Figure 3. Box and whiskers plot for the diameter measure-ments in the study population, n # 128. G-AP # glotticanteroposterior diameter; G-trans # glottic transverse diam-eter; C-AP # cricoid anteroposterior diameter; C-Trans #cricoid transverse diameter.
Table 1. Results of the Linear Regression Analysis for LaryngealDimensions Versus Age, Height, and Weight, Respectively,in 128 Patients
Age Height WeightG-CSA r # 0.36 r # 0.34 r # 0.35
P ! 0.001 P ! 0.001 P ! 0.001G-AP r # 0.38 r # 0.36 r # 0.39
P ! 0.001 P ! 0.001 P ! 0.001G-trans r # 0.24 r # 0.22 r # 0.17
P # 0.005 P # 0.009 P # 0.047C-CSA r # 0.27 r # 0.29 r # 0.25
P # 0.001 P ! 0.001 P # 0.003C-AP r # 0.13 r # 0.12 r # 0.12
P # 0.129 P # 0.167 P # 0.14C-trans r # 0.13 r # 0.19 r # 0.12
P # 0.117 P # 0.03 P # 0.18Cricoid:glottic CSA r # 0.18 r # 0.11 r # 0.14
P # 0.04 P # 0.18 P # 0.11G-CSA # glottic cross-sectional area; G-AP # glottic anteroposterior diameter; G-trans # glottictransverse diameter; C-CSA # cricoid crosssectional area; C-AP # cricoid anteroposterior diam-eter; C-Trans # cricoid transverse diameter.
Vol. 108, No. 5, May 2009 © 2009 International Anesthesia Research Society 1477
Dalal, Anesth Analg 2009

MITO O REALIDADLA TRAQUEA PEDIATRICA Y EL DEDO
MEÑIQUE
• ¿PREDICE EL DIAMETRO DEL DEDO MEÑIQUE LA TALLA DEL TUBO ENDOTRAQUEAL?

QUE NOS DICEN LOS LIBROS?
• “OTRO METODO NO COMPROBADO CIENTIFICAMENTE , CLINICAMENTE UTIL USADO POR ALGUNOS ANESTESIOLOGOS ES COMPARAR EL DIAMETRO EXTERNO DEL TUBO ET CON EL DEL DEDO MEÑIQUE”

383 M.E.J. ANESTH 20 (3), 2009
THE ‘BEST FIT’ ENDOTRACHEAL TUBE IN CHILDREN
- Comparison of Four Formulae -
TURKISTANI A*, ABDULLAH KM***, DELVI B** AND AL-MAZROUA KA****
AbstractBackground: Uncuffed endotracheal tubes are still being recommended by most pediatric
anesthetists at our Institutes. Different algorithms and formulae have been proposed to choose the best-fitting size of the tracheal tube. The most widely accepted is related to the age of the child [inner diameter [ID] in mm = (age in yr/4) +4; the second is a body, length-related formula (ID in mm = 2 + height in cm/30); the third, a multivariate formula (ID in mm = 2.44 + age in yr � 0.1 + height in cm � 0.02 + weight in kg � 0.016]5; the fourth, the width of the 5th fingernail is used for ID prediction of the ETT (ID in mm = maximum width of the 5th fingernail).
The primary endpoint of this prospective study was to compare the size of the ‘best fit’ tracheal tube with the size predicted using each of the above mentioned formulae.
Patients and Methods: With Institutional Ethics Committee approval and parental consent, 27 boys, 23 girls, ASA I-III, 2-10 years, scheduled for different surgical procedures requiring general anesthesia and endotracheal intubation, were enrolled in the study. The size of ‘best fit’ endotracheal tubes in those children were compared. The internal diameter considered the ‘best fit’ by the attending pediatric anesthesiologist was compared to age-based, length-based, multivariate-based and 5th fingernail width-based formulae. For all tests, P < 0.05 was considered to be statistically significant.
Results: The mean (SD) IDs for the ‘best fit’, age-based, length-based, multivariate and 5th fingernail techniques were 5.31 (0.691), 5.54 (0.622), 5.82 (0.572), 5.71 (0.67) and 5.43 (0.821) mm, respectively.
Conclusions: The age-based and 5th fingernail width-based predictions of ETT size are more accurate than length-based and multivariate-based formulae in terms of mean value and case matching.
Key Words: pediatric, endotracheal tube, age, length, multivariate, 5th fingernail, formula
From College of Medicine, King Saud University, Riyadh 11461, P.O. Box: 2925, Riyadh, S.A.* MD, Assoc. Prof. of Anaesthesia. ** MD, Assist. Prof. of Anaesth. **** MD, FAAP, Assoc. Prof. Ped. Otolaryngology.From King Abdul-Aziz Medical City, Riyadh 11426, P.O. Box: 22490, Riyadh, S.A.*** MD, Arab Board, Consultant Cardiac Anaesthetist.Address for correspondence: Dr. Khaled M Abdullah, Consultant Cardiac Anaesthetist, King Abdul-Aziz Medical City.E-mail [email protected]

383 M.E.J. ANESTH 20 (3), 2009
THE ‘BEST FIT’ ENDOTRACHEAL TUBE IN CHILDREN
- Comparison of Four Formulae -
TURKISTANI A*, ABDULLAH KM***, DELVI B** AND AL-MAZROUA KA****
AbstractBackground: Uncuffed endotracheal tubes are still being recommended by most pediatric
anesthetists at our Institutes. Different algorithms and formulae have been proposed to choose the best-fitting size of the tracheal tube. The most widely accepted is related to the age of the child [inner diameter [ID] in mm = (age in yr/4) +4; the second is a body, length-related formula (ID in mm = 2 + height in cm/30); the third, a multivariate formula (ID in mm = 2.44 + age in yr � 0.1 + height in cm � 0.02 + weight in kg � 0.016]5; the fourth, the width of the 5th fingernail is used for ID prediction of the ETT (ID in mm = maximum width of the 5th fingernail).
The primary endpoint of this prospective study was to compare the size of the ‘best fit’ tracheal tube with the size predicted using each of the above mentioned formulae.
Patients and Methods: With Institutional Ethics Committee approval and parental consent, 27 boys, 23 girls, ASA I-III, 2-10 years, scheduled for different surgical procedures requiring general anesthesia and endotracheal intubation, were enrolled in the study. The size of ‘best fit’ endotracheal tubes in those children were compared. The internal diameter considered the ‘best fit’ by the attending pediatric anesthesiologist was compared to age-based, length-based, multivariate-based and 5th fingernail width-based formulae. For all tests, P < 0.05 was considered to be statistically significant.
Results: The mean (SD) IDs for the ‘best fit’, age-based, length-based, multivariate and 5th fingernail techniques were 5.31 (0.691), 5.54 (0.622), 5.82 (0.572), 5.71 (0.67) and 5.43 (0.821) mm, respectively.
Conclusions: The age-based and 5th fingernail width-based predictions of ETT size are more accurate than length-based and multivariate-based formulae in terms of mean value and case matching.
Key Words: pediatric, endotracheal tube, age, length, multivariate, 5th fingernail, formula
From College of Medicine, King Saud University, Riyadh 11461, P.O. Box: 2925, Riyadh, S.A.* MD, Assoc. Prof. of Anaesthesia. ** MD, Assist. Prof. of Anaesth. **** MD, FAAP, Assoc. Prof. Ped. Otolaryngology.From King Abdul-Aziz Medical City, Riyadh 11426, P.O. Box: 22490, Riyadh, S.A.*** MD, Arab Board, Consultant Cardiac Anaesthetist.Address for correspondence: Dr. Khaled M Abdullah, Consultant Cardiac Anaesthetist, King Abdul-Aziz Medical City.E-mail [email protected]

as determined by ultrasonography, better predicts optimalETT size than existing methods.
Materials and MethodsThis study was approved by the Review Board for Human Exper-iments atKyotoPrefecturalUniversityofMedicine (Kyoto, Japan).Written informed consent was obtained from custodial adults. Weenrolled a total of 192 patients aged 1 mo to 6 yr, split into devel-opment and validation phases. Each patient was scheduled for sur-gery requiring general endotracheal anesthesia. Those with condi-tions known or suspected to predispose them to laryngeal ortracheal pathology were excluded. General anesthesia was inducedby inhalation of sevoflurane or intravenous administration of thio-pental. Vecuronium was given to all patients for muscle relaxation.
Our primary endpoint was a regression of outer ETTdiameter against subglottic diameter as determined by ultra-sonography. In a pilot study, the SD of subglottic diameterwas 2.9 mm, the correlation coefficient between ETT outerdiameter (OD) and subglottic diameter was 0.7. The slopeestimate obtained from regression equation was 0.5. Assum-ing a true regression slope of 0.5, a total of 19 subjects wererequired to reject the null hypothesis that this slope equalszero with 90% power at an ! level of 0.01.13 Our primarygoal, though, was to determine the extent to which variabilityin optimal ETT size can be explained by the variability in thetracheal dimension as assessed by ultrasonography. Wetherefore increased the number of subjects to 48 each for thecuffed and uncuffed ETT groups (n ! 96).
Development PhaseIn the development phase, we evaluated 48 patients who wereintubated with a cuffed ETT and an additional 48 who wereintubated with an uncuffed ETT. Selection of cuffed versus un-cuffed ETT was determined solely by the preference of the an-esthesiologists. Within each study group, an equal number ofpatients were recruited from three weight subgroups: 3 to lessthan 9 kg, 9 to less than 15 kg, and 15 to less than 21 kg.
Subglottic diameter was estimated with B-mode ultrasonog-raphy (SonoSite 180, SonoSite, Inc., Tokyo, Japan) with a5–10-MHz linear probe positioned on the midline of the ante-rior neck (fig. 1). To avoid any confusion between the cricoidcartilage and a tracheal ring, ultrasonography began with local-
ization of the true vocal folds as paired hyperechoic linear struc-tures that moved with respiration and swallowing before pa-tients were paralyzed. The probe was then moved caudally tovisualize the cricoid arch (i.e., round hypoechoic structure withhyperechoic edges). The transverse air-column diameter wasmeasured at the lower edge of the cricoid cartilage after patientswere paralyzed, and was considered tracheal diameter. These mea-surements were performed without ventilation or positive end-ex-piratory pressure to minimize fluctuation in tracheal diameter.
The ultrasonographer had considerable experience performinglaryngeal ultrasonography before the starting this investigation.Typically, the ultrasound measurements took approximately 30 s.
The trachea was then intubated using direct laryngos-copy. Size of the initial tube was selected as follows: (1)uncuffed tubes, with the Cole formulas: ID (inner diameter)in mm ! 0.25 " (age in years) # 4; (2) cuffed ETTs inchildren aged 2 yr or older, with the Motoyama formulas: IDin mm ! 0.25 " (age in years) # 3.5; (3) cuffed ETTs inchildren younger than 2 yr, with the Khine formulas: ID inmm ! 0.25 " (age in years) # 3.0.
If there was resistance to ETT passage into the trachea, orthere was no audible leak when the lungs were inflated to apressure of 20–30 cm H2O, the tube was exchanged with onethat was 0.5 mm smaller. In contrast, the ETT was exchangedfor one that was 0.5 mm larger if a leak occurred at an inflationpressure less than 10 cm H2O.12,14 Tube size was consideredoptimal when a tracheal leak was detected at an inflation pres-sure between 10–20 cm H2O with either uncuffed tubes ordeflated cuffed tubes. Cuff leak evaluation was performed by thesame two well-trained investigators. Interrater variability of thecuff leak pressure values between the two observers was less than10%(intraclasscoefficientof theselectedcuff leakpressure!0.88).
After intubation with an appropriately sized tube, trachealdiameter was measured again, as was ETT OD (i.e., roundhyperechoic structure, fig. 2). Ultrasonic estimates of trachealdiameter and airway leak pressure measurement were performedby different investigators, each of whom was blinded to theother’s data. Ultrasonography and airway leak pressure measure-ment were performed in the supine position, with the head in aneutral position with slight extension.15
Linear regression was used to determine the relationshipbetween subglottic diameter and the OD of optimally sized
Fig. 1. Photograph and illustration of ultrasonography of the neck to measure subglottic diameter. Patient consent was obtainedfor use of this photograph.
PERIOPERATIVE MEDICINE
820 Anesthesiology, V 113 • No 4 • October 2010 Shibasaki et al.
transverse subglottic diameter, suggesting that ultrasono-graphic measurement could adequately assess the subglotticdiameter.11
The subglottis, as bound by the complete cartilaginousring of the cricoid cartilage, was long believed to be thenarrowest part of the pediatric larynx. A recent report, how-ever, identified the narrowest portion to be at the vocal cordand subvocal cord level in unparalyzed children.19 However,measuring the tracheal diameter consistently at these levels inall patients was difficult because of the blurred ultrasonicvisualization of the vocal cord. Therefore, we measured sub-glottic diameter at the lower edge of the hypoechogenic cri-coid cartilage. This measure represented a reliable and con-sistent value that could be compared among patients.Increasing discrepancy between uncuffed ETT OD and sub-glottic diameter in proportion as a function of subglotticdiameter indicates that the narrowest part of the pediatriclarynx must lie above the cricoid ring level even among par-alyzed patients (fig. 3).
Although ultrasonography is an operator-dependenttechnique, it is relatively simple to learn. A total of approxi-mately 15 procedures are required for operators to obtainreliable and reproducible measurements.11 Another concernabout ultrasonic measurements is that age-dependent physi-ologic calcification of the larynx creates an acoustic shadow.However, as calcification begins to occur in the laryngealcartilage during the third decade of life, ultrasonography canbe applied with few problems in pediatrics.20
Optimal ETT size could be selected from measurement ofthe tracheal diameter on chest radiography.21 A good corre-lation in tracheal diameter between computed tomographyand chest radiography indicates that the latter could give arepresentative measurement of tracheal diameter.22 A lengthof approximately 70% (uncuffed) or 60% (cuffed) of the
tracheal diameter on chest radiography is reported to be apossible indicator of ETT ID. However tracheal diameter onchest radiography does not necessarily reflect the subglotticdiameter, the narrowest part of the pediatric larynx.
In clinical anesthesia practice, we usually select pediatricETT sizes based on ID. However, the relationship between IDand OD differs among manufacturers, complicating age-basedpediatric ETT size selection. Further, although there are nodifferences in the OD between cuffed and uncuffed ETTs usedin the present study (table 2), selected ODs have a tendency tobe smaller in cuffed than uncuffed ETTs (fig. 3).
Cuffed ETTs can safely be used in pediatric populations,resulting in fewer adverse effects than uncuffed ETTs. Arecent study found that there were no significant differencesin the use of racemic epinephrine for postextubation subglot-tic edema, the rate of successful extubation, or the need fortracheotomy between intubations with cuffed versus un-cuffed ETTs.16–18
In summary, previous established formulas based on agepoorly predicted pediatric ETT size. In contrast, subglotticupper airway diameter measured by ultrasonography was agood predictor of correct cuffed and uncuffed ETT sizes forpediatric patients.
References1. Browning DH, Graves SA: Incidence of aspiration with
endotracheal tubes in children. J Pediatr 1983; 102:582– 42. Oshodi A, Dysart K, Cook A, Rodriguez E, Zhu Y, Shaffer
TH, Miller TL: Airway injury resulting from repeated en-dotracheal intubation: Possible prevention strategies. Pe-diatr Crit Care Med 2010 Apr 1. [Epub ahead of print]
3. Roy WL: Intraoperative aspiration in a paediatric patient.Can Anaesth Soc J 1985; 32:639 – 41
4. Sherman JM, Nelson H: Decreased incidence of subglotticstenosis using an “appropriate-sized” endotracheal tube inneonates. Pediatr Pulmonol 1989; 6:183–5
5. Dillier CM, Trachsel D, Baulig W, Gysin C, Gerber AC,Weiss M: Laryngeal damage due to an unexpectedly largeand inappropriately designed cuffed pediatric trachealtube in a 13-month-old child. Can J Anaesth 2004; 51:72–5
6. Cole F: Pediatric formulas for the anesthesiologist. AMA JDis Child 1957; 94:672–3
7. Motoyama EK: Endotracheal intubation. In Smith’s Anes-thesia for Infants and Children. St Louis, CV Mosby 1990;269 –75.
8. Luten RC, Wears RL, Broselow J, Zaritsky A, Barnett TM,Lee T, Bailey A, Vally R, Brown R, Rosenthal B: Length-based endotracheal tube and emergency equipment inpediatrics. Ann Emerg Med 1992; 21:900 – 4
Table 1. Continued
9–15 kg Group 15–21 kg Group
Validation Phase(n ! 32)
P Value
Development Phase(n ! 32)
Validation Phase(n ! 32)
P ValueCuffed Uncuffed Cuffed Uncuffed Cuffed Uncuffed
82 " 10 87 " 7 0.29 107 " 8 105 " 8 106 " 10 106 " 7 0.9610.6 " 1.2 11.6 " 1.6 0.14 17.4 " 1.8 17.8 " 2.3 17.4 " 2.3 17.2 " 2.3 0.87
27 " 15 30 " 10 0.57 62 " 16 60 " 14 60 " 13 61 " 11 0.95
Table 2. Endotracheal Tube Size as Determined byUltrasonography for Pediatric Patients
Inner Diameter, mm Outer Diameter, mm
3.0 4.33.5 4.94.0 5.64.5 6.25.0 6.95.5 7.5
Prediction of Pediatric Endotracheal Tube Size
Shibasaki et al. Anesthesiology, V 113 • No 4 • October 2010 823

PERIOPERATIVE MEDICINE Anesthesiology 2010; 113:819 –24
Copyright © 2010, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins
Prediction of Pediatric Endotracheal Tube Sizeby UltrasonographyMasayuki Shibasaki, M.D.,* Yasufumi Nakajima, M.D., Ph.D.,† Sachiyo Ishii, M.D.,*Fumihiro Shimizu, M.D.,* Nobuaki Shime, M.D., Ph.D.,‡ Daniel I. Sessler, M.D.§
ABSTRACTBackground: Formulas based on age and height often fail toreliably predict the proper endotracheal tube (ETT) size inpediatric patients. We, thus, tested the hypothesis that sub-glottic diameter, as determined by ultrasonography, betterpredicts optimal ETT size than existing methods.Methods: A total of 192 patients, aged 1 month to 6 yr,who were scheduled for surgery and undergoing generalanesthesia were enrolled and divided into developmentand validation phases. In the development group, the op-timal ETT size was selected according to standard age-based formulas for cuffed and uncuffed tubes. Tubes werereplaced as necessary until a good clinical fit was obtained.Via ultrasonography, the subglottic upper airway diame-ter was determined before tracheal intubation. We con-structed a regression equation between the subglottic up-per airway diameter and the outer diameter of the ETTfinally selected. In the validation group, ETT size wasselected after ultrasonography using this regression equa-tion. The primary outcome was the fraction of initialcuffed and uncuffed tube sizes, as selected through theregression formula, that proved clinically optimal.Results: Subglottic upper airway diameter was highly corre-lated with outer ETT diameter deemed optimal on clinicalgrounds. The rate of agreement between the predicted ETTsize based on ultrasonic measurement and the final ETT sizeselected clinically was 98% for cuffed ETTs and 96% foruncuffed ETTs.
Conclusions: Measuring subglottic airway diameter with ul-trasonography facilitates the selection of appropriately sizedETTs in pediatric patients. This selection method better pre-dicted optimal outer ETT diameter than standard age- andheight-based formulas.
INTUBATION of pediatric patients with an endotrachealtube (ETT) that is too small may result in insufficient
ventilation, poor reliability of end-tidal gas monitoring, leak-age of anesthetic gases into the operating room environment,and an enhanced risk of aspiration.1–3 In contrast, an ETTthat is too large can cause upper airway damage (e.g., localischemia, ulceration, scar formation) and the potential forsubsequent subglottic stenosis.4,5
Age-based formulas, such as those of Cole and Mo-toyama, have been used to estimate optimal ETT size formore than half a century.6,7 Predictive formulas for ap-propriate ETT size have also been based on patient weightand height.8 –10 However, none of these systems workespecially well. The result is that repeated laryngoscopiesare often necessary to identify the appropriate tube forindividual patients.
Recent reports suggest that the diameter of the subglotticupper airway can be determined by ultrasonography inhealthy young adults and pediatric patients.11,12 However,the extent to which ultrasonography can predict optimalETT size in pediatric patients remains to be determined.Therefore, we tested the hypothesis that subglottic diameter,
* Instructor, ‡ Assistant Professor, Department of Anesthesiologyand Intensive Care, Kyoto Prefectural University of Medicine, Kyoto,Japan. † Assistant Professor, Department of Anesthesiology and In-tensive Care, Kyoto Prefectural University of Medicine, and Member,OUTCOMES RESEARCH Consortium/Group. § Professor and Chair, Depart-ment of OUTCOMES RESEARCH, Cleveland Clinic, Cleveland, Ohio.
Received from the Department of Anesthesiology and IntensiveCare, Kyoto Prefectural University of Medicine, Kyoto, Japan. Sub-mitted for publication August 6, 2009. Accepted for publication May27, 2010. Support was provided solely from institutional and/ordepartmental sources.
Address correspondence to Dr. Shibasaki: Department of Anesthe-siology, Kyoto Prefectural University of Medicine, Kamigyo-ku, Kyoto602-8566 Japan. [email protected]. This article may be ac-cessed for personal use at no charge through the Journal Web site,www.anesthesiology.org.
! This article is featured in “This Month in Anesthesiology.”Please see this issue of ANESTHESIOLOGY, page 9A.
What We Already Know about This Topic
❖ The proper endotracheal tube size for children is poorly pre-dicted by formulas relying on age and height.
What This Article Tells Us That Is New
❖ In 192 children aged 1 month to 6 yr, ultrasound measure-ment of subglottic airway diameter better predicted appropri-ately sized endotracheal tube than traditional formulas usingage and height.
Anesthesiology, V 113 • No 4 • October 2010 819

MITO O REALIDADPRESION CRICOIDEA
• ¿ES LA PRESION CRICOIDEA UN COMPONENTE IMPORTANTE EN LA INDUCCION DE SECUENCIA RAPIDA EN NIÑOS?

DOCUMENTO DE SELLICK
• EN EL ENFERMO CRITICO, SE PUEDE PREFERIR LA INDUCCION INHALADA.
• TAN PRONTO COMO SE PIERDA LA CONCIENCIA, UNA PRESION FIRME DEBE SER APLICADA.
• DURANTE LA PRESION CRICOIDEA, LOS PULMONES PUEDEN SER VENTILADOS.
• LA ANTIGUA INDUCCION INHALADA... CON LA CABEZA DIRIGIDA HACIA ABAJO, TIENE ALGO QUE RECOMENDAR...

Sellick’s Maneuver: To Do or Not Do
Andranik Ovassapian, MD*
M. Ramez Salem, MD†
The introduction of cricoid pressure (CP) by Sellick1 in 1961 “to controlregurgitation until intubation with a cuffed endotracheal tube was com-pleted” was met with an enthusiastic reception worldwide and rapidlybecame an integral component of the rapid sequence induction/intubationtechnique (RSII). The maneuver consisted of “occlusion of the upperesophagus by backward pressure on the cricoid ring against the bodies ofcervical vertebrae to prevent gastric contents from reaching the pharynx.”1
Sellick1 provided evidence that extension of the neck and application of CPobliterated the esophageal lumen at the level of the 5th cervical vertebra, asseen in a previously placed soft latex tube distended with contrast mediato a pressure of 100 cm H2O. He also confirmed the value of CP inpreventing saline (run into the esophagus from a height of 100 cm H2O)from reaching the pharynx in a patient undergoing gastroesophagectomy.2
Sellick1,2 emphasized that the lungs can be ventilated by intermittentpositive pressure and that CP can prevent inflation of the stomach duringpositive pressure ventilation. References to CP were found in the literaturemore than 230 yr ago.3 In a letter from Dr. W. Cullen to Lord Cathcartdated August 8, 1774, concerning the recovery of persons “drowned andseemingly dead,” the use of CP by Dr. Monro was referred to as a meansof preventing gastric distension during inflation of the lungs.3
Before Sellick described CP, several techniques were used in patients atrisk of aspiration of gastric contents: awake intubation, induced hyperven-tilation with carbon dioxide during inhaled induction,4 and RSII per-formed with the patient in a 40° head-up tilt.5 The rationale behind thehead-up tilt was that gastric contents could not reach the laryngeal leveleven if contents were moved up into the esophagus.5 The RSII with CP wasextended not only to emergency surgical and obstetrical procedures andthe critical care setting, but also to elective procedures in patients at risk ofaspiration of gastric contents. The plethora of manuscripts, correspon-dence, and reviews on CP is a testimony to its relevance to anestheticpractice and continuing interest to clinicians.6
In the last 2 decades, clinicians have questioned the efficacy of CP andtherefore the necessity of the maneuver.7,8 Some suggested abandoning iton the following grounds: (a) Its effectiveness has been demonstrated onlyin cadavers,9–11 and therefore its efficacy lacks scientific validation. (b) Itinduces relaxation of the lower esophageal sphincter.8,12 (c) There havebeen reports of regurgitation of gastric contents and aspiration despite CP.13
(d) The esophagus is not exactly posterior to the cricoid, and thus themaneuver is unreliable in producing midline esophageal compression.14 (e) Itis associated with nausea/vomiting and also with esophageal rupture.15 (f) Itmakes tracheal intubation and mask ventilation difficult or impossible.15–18
Because of ethical considerations, a controlled study of the efficacy of CP isnot feasible. Even if such a study were conducted, it would probably yieldlittle information, given the low incidence of pulmonary aspiration. Thecompelling evidence supporting the effectiveness of CP comes from studiesthat unequivocally demonstrate its efficacy in preventing gastric inflation inanesthetized children and adults.19–21 It is inconceivable that a maneuvereffective in preventing gastric inflation during manual ventilation would notbe effective in preventing esophageal contents from reaching the pharynx.
The study by Rice et al.22 in the current issue sheds new light on theefficacy of CP. In 24 awake volunteers, magnetic resonance imaging was
From the *Department of Anesthesia andCritical Care, Airway Study and TrainingCenter, University of Chicago; and †Depart-ment of Anesthesiology, Advocate IllinoisMasonic Medical Center, Department of An-esthesiology, University of Illinois College ofMedicine, Chicago, Illinois.
Accepted for publication June 18, 2009.Address correspondence and reprint re-
quests to Andranik Ovassapian, MD, Depart-ment of Anesthesia and Critical Care, AirwayStudy and Training Center, University of Chi-cago, 5841 South Maryland Ave., Chicago, IL60637. Address e-mail to [email protected].
Copyright © 2009 International Anesthe-sia Research SocietyDOI: 10.1213/ANE.0b013e3181b763c0
Vol. 109, No. 5, November 20091360
Editorial

Sellick’s Maneuver: To Do or Not Do
Andranik Ovassapian, MD*
M. Ramez Salem, MD†
The introduction of cricoid pressure (CP) by Sellick1 in 1961 “to controlregurgitation until intubation with a cuffed endotracheal tube was com-pleted” was met with an enthusiastic reception worldwide and rapidlybecame an integral component of the rapid sequence induction/intubationtechnique (RSII). The maneuver consisted of “occlusion of the upperesophagus by backward pressure on the cricoid ring against the bodies ofcervical vertebrae to prevent gastric contents from reaching the pharynx.”1
Sellick1 provided evidence that extension of the neck and application of CPobliterated the esophageal lumen at the level of the 5th cervical vertebra, asseen in a previously placed soft latex tube distended with contrast mediato a pressure of 100 cm H2O. He also confirmed the value of CP inpreventing saline (run into the esophagus from a height of 100 cm H2O)from reaching the pharynx in a patient undergoing gastroesophagectomy.2
Sellick1,2 emphasized that the lungs can be ventilated by intermittentpositive pressure and that CP can prevent inflation of the stomach duringpositive pressure ventilation. References to CP were found in the literaturemore than 230 yr ago.3 In a letter from Dr. W. Cullen to Lord Cathcartdated August 8, 1774, concerning the recovery of persons “drowned andseemingly dead,” the use of CP by Dr. Monro was referred to as a meansof preventing gastric distension during inflation of the lungs.3
Before Sellick described CP, several techniques were used in patients atrisk of aspiration of gastric contents: awake intubation, induced hyperven-tilation with carbon dioxide during inhaled induction,4 and RSII per-formed with the patient in a 40° head-up tilt.5 The rationale behind thehead-up tilt was that gastric contents could not reach the laryngeal leveleven if contents were moved up into the esophagus.5 The RSII with CP wasextended not only to emergency surgical and obstetrical procedures andthe critical care setting, but also to elective procedures in patients at risk ofaspiration of gastric contents. The plethora of manuscripts, correspon-dence, and reviews on CP is a testimony to its relevance to anestheticpractice and continuing interest to clinicians.6
In the last 2 decades, clinicians have questioned the efficacy of CP andtherefore the necessity of the maneuver.7,8 Some suggested abandoning iton the following grounds: (a) Its effectiveness has been demonstrated onlyin cadavers,9–11 and therefore its efficacy lacks scientific validation. (b) Itinduces relaxation of the lower esophageal sphincter.8,12 (c) There havebeen reports of regurgitation of gastric contents and aspiration despite CP.13
(d) The esophagus is not exactly posterior to the cricoid, and thus themaneuver is unreliable in producing midline esophageal compression.14 (e) Itis associated with nausea/vomiting and also with esophageal rupture.15 (f) Itmakes tracheal intubation and mask ventilation difficult or impossible.15–18
Because of ethical considerations, a controlled study of the efficacy of CP isnot feasible. Even if such a study were conducted, it would probably yieldlittle information, given the low incidence of pulmonary aspiration. Thecompelling evidence supporting the effectiveness of CP comes from studiesthat unequivocally demonstrate its efficacy in preventing gastric inflation inanesthetized children and adults.19–21 It is inconceivable that a maneuvereffective in preventing gastric inflation during manual ventilation would notbe effective in preventing esophageal contents from reaching the pharynx.
The study by Rice et al.22 in the current issue sheds new light on theefficacy of CP. In 24 awake volunteers, magnetic resonance imaging was
From the *Department of Anesthesia andCritical Care, Airway Study and TrainingCenter, University of Chicago; and †Depart-ment of Anesthesiology, Advocate IllinoisMasonic Medical Center, Department of An-esthesiology, University of Illinois College ofMedicine, Chicago, Illinois.
Accepted for publication June 18, 2009.Address correspondence and reprint re-
quests to Andranik Ovassapian, MD, Depart-ment of Anesthesia and Critical Care, AirwayStudy and Training Center, University of Chi-cago, 5841 South Maryland Ave., Chicago, IL60637. Address e-mail to [email protected].
Copyright © 2009 International Anesthe-sia Research SocietyDOI: 10.1213/ANE.0b013e3181b763c0
Vol. 109, No. 5, November 20091360
Editorial

PRESION CRICOIDEA
• FUE USADA POR PRIMERA VEZ EN 1774 POR MONRO, Y DESCRITA POR CULLEN EN UNA CARTA DIRIGIDA A LORD CATHCART, PRESIDENTE DEL COMITE POLICIAL DE ESCOCIA.
• CULLEN ABOGA QUE LA PRESION CRICOIDEA ES UN MEDIO PARA PREVENIR LA INSUFLACION GASTRICA CUANDO SE DA REANIMACION A “PERSONAS AHOGADAS O QUE PARECEN MUERTAS”.

LA ISR CONTEMPORANEA EN ADULTOS
• PREOXIGENACION
• INYECCION RAPIDA DEL ANESTESICO Y RELAJANTE.
• PRESION CRICOIDEA.
• EVITAR LA VENTILACION MANUAL.
• INSERCION DEL TUBO ET, INFLADO DEL CUFF, CONFIRMACION DE LA POSICION.
• LIBERACION DE LA PRESION CRICOIDEA.


ISR PEDIATRICA
• “... LAS CARACTERISTICAS CLAVES DE UNA ISR PEDIATRICA MENCIONA UNA INDUCCION EFECTIVA DE UNA ANESTESIA PROFUNDA, EVITAR LA PRESION CRICOIDEA Y LA CONFIRMACION DE LA PARALISIS MUSCULAR COMPLETA...”.
• “... SE DEBE ABANDONAR LA PRESION CRICOIDEA EN TODOS LOS PACIENTES CON EXCEPCION DE LOS PEDIATRICOS...”

ISR PEDIATRICA
• “... LAS CARACTERISTICAS CLAVES DE UNA ISR PEDIATRICA MENCIONA UNA INDUCCION EFECTIVA DE UNA ANESTESIA PROFUNDA, EVITAR LA PRESION CRICOIDEA Y LA CONFIRMACION DE LA PARALISIS MUSCULAR COMPLETA...”.
• “... SE DEBE ABANDONAR LA PRESION CRICOIDEA EN TODOS LOS PACIENTES CON EXCEPCION DE LOS PEDIATRICOS...”

¿POR QUE ESTA CONTROVERSIA?
• NO HA SIDO LLEVADO A CABO UN ENSAYO CLINICO RANDOMIZADO SOBRE ISR CLASICA.
• EL HECHO DE SER REALIZADO EN ADULTOS NO PUEDE SER APLICADO A NIÑOS, DE TAL MODO QUE:
• LA PREOXIGENACION RARAMENTE ES ADECUADA.
• DESATURACION OCURRE MAS RAPIDAMENTE.
• LA APLICACION DE PRESION CRICOIDEA PUEDE HACER DEL PROCEDIMIENTO DE INTUBACION UN PROCEDIMIENTO MAS DIFICIL.

Complications during rapid sequence induction ofgeneral anesthesia in children: a benchmark study
FRANK J. GENCORELLI MDMD*, RYAN G. FIELDS DO, MBADO, MBA†AND RONALD S. LITMAN DODO‡*Department of Anesthesiology, Hospital of the University of Pennsylvania School of Medicine,Philadelphia, PA, USA, †Jersey Shore University Medical Center, Neptune, NJ, USA and‡Department of Anesthesiology and Critical Care, The Children’s Hospital of Philadelphia,Professor of Anesthesiology and Pediatrics, University of Pennsylvania School of Medicine, PA,USA
Section Editor: Dr Andrew Davidson
SummaryObjectives: Determine incidence of complications such as difficult orfailed intubation, hypoxemia, hypotension, and bradycardia in chil-dren undergoing rapid sequence intubation (RSI) in a pediatricanesthesia department in a tertiary care children’s hospital.Aim: To establish a benchmark to be used by other institutions andnonanesthesiologists performing RSI in children.Background: RSI is being increasingly performed in the nonoperatingroom setting by nonanesthesiologists. No published studies exist toestablish a benchmark of intubation success or failure and complica-tions in this patient population.Methods ⁄Materials: Retrospective cohort analysis of children aged 3–12 undergoing RSI from 2001 to 2006.Results: One thousand seventy children underwent RSI from 2001 to2006. Twenty (1.9%) developed moderate hypoxemia (SpO2 80–89%),18 (1.7%) demonstrated severe hypoxemia (SpO2 < 80%), 5 (0.5%)developed bradycardia (heart rate <60), and 8 (0.8%) developedhypotension (systolic blood pressure <70 mmHg). One patient hademesis of gastric contents but no evidence of pulmonary aspiration orhypoxemia. Eighteen (1.7%) children were noted to be difficult tointubate and required more than one intubation attempt. All wereeventually intubated without significant complications. Patientsbetween 10 and 19 kg had a higher incidence of severe hypoxemiawhen compared with older children (P < 0.001). There was noassociation between choice of muscle relaxant and any complication.Conclusions: In our cohort of 1070 children who underwent RSI,difficult intubation was encountered in 1.7% and transient oxy-hemoglobin desaturation occurred in 3.6%. Severe hypoxemia wasmore likely in children <20 kg. There were no children who could notbe intubated, and there were no long-term or permanent complica-tions.
Correspondence to: Ronald S. Litman, DO, Department of Anesthesiology & Critical Care, The Children’s Hospital of Philadelphia, 34th St. &Civic Center Blvd, Philadelphia, PA 19104, USA (email: [email protected]).
Pediatric Anesthesia 2010 20: 421–424 doi:10.1111/j.1460-9592.2010.03287.x
! 2010 Blackwell Publishing Ltd 421

Complications during rapid sequence induction ofgeneral anesthesia in children: a benchmark study
FRANK J. GENCORELLI MDMD*, RYAN G. FIELDS DO, MBADO, MBA†AND RONALD S. LITMAN DODO‡*Department of Anesthesiology, Hospital of the University of Pennsylvania School of Medicine,Philadelphia, PA, USA, †Jersey Shore University Medical Center, Neptune, NJ, USA and‡Department of Anesthesiology and Critical Care, The Children’s Hospital of Philadelphia,Professor of Anesthesiology and Pediatrics, University of Pennsylvania School of Medicine, PA,USA
Section Editor: Dr Andrew Davidson
SummaryObjectives: Determine incidence of complications such as difficult orfailed intubation, hypoxemia, hypotension, and bradycardia in chil-dren undergoing rapid sequence intubation (RSI) in a pediatricanesthesia department in a tertiary care children’s hospital.Aim: To establish a benchmark to be used by other institutions andnonanesthesiologists performing RSI in children.Background: RSI is being increasingly performed in the nonoperatingroom setting by nonanesthesiologists. No published studies exist toestablish a benchmark of intubation success or failure and complica-tions in this patient population.Methods ⁄Materials: Retrospective cohort analysis of children aged 3–12 undergoing RSI from 2001 to 2006.Results: One thousand seventy children underwent RSI from 2001 to2006. Twenty (1.9%) developed moderate hypoxemia (SpO2 80–89%),18 (1.7%) demonstrated severe hypoxemia (SpO2 < 80%), 5 (0.5%)developed bradycardia (heart rate <60), and 8 (0.8%) developedhypotension (systolic blood pressure <70 mmHg). One patient hademesis of gastric contents but no evidence of pulmonary aspiration orhypoxemia. Eighteen (1.7%) children were noted to be difficult tointubate and required more than one intubation attempt. All wereeventually intubated without significant complications. Patientsbetween 10 and 19 kg had a higher incidence of severe hypoxemiawhen compared with older children (P < 0.001). There was noassociation between choice of muscle relaxant and any complication.Conclusions: In our cohort of 1070 children who underwent RSI,difficult intubation was encountered in 1.7% and transient oxy-hemoglobin desaturation occurred in 3.6%. Severe hypoxemia wasmore likely in children <20 kg. There were no children who could notbe intubated, and there were no long-term or permanent complica-tions.
Correspondence to: Ronald S. Litman, DO, Department of Anesthesiology & Critical Care, The Children’s Hospital of Philadelphia, 34th St. &Civic Center Blvd, Philadelphia, PA 19104, USA (email: [email protected]).
Pediatric Anesthesia 2010 20: 421–424 doi:10.1111/j.1460-9592.2010.03287.x
! 2010 Blackwell Publishing Ltd 421

ISR PEDIATRICA Y DESATURACION
• 1070 ISR.
• 1.7 % casos dificiles.
• 3.6 % de pacientes mostraron desaturacion.
• Pacientes entre 10 y 19 kg no demostraron hipoxemia moderada comparado con los demas grupos.
• Pacientes entre 10 y 19 kg SI demostraron hipoxemia mas severa que los demas grupos
children (1.7%) were noted by the anesthesia prac-titioner to be difficult to intubate as evidenced by acomment on the electronic record indicating morethan one intubation attempt because of difficultyvisualizing the vocal cords. One patient requiredintubation with a lighted stylet. All were eventuallyintubated without significant complications. Onepatient, a 9-year-old male with an open tibia frac-ture, had an esophageal intubation with emesis ofgastric contents and no evidence of pulmonaryaspiration. This patient was manually ventilatedfollowing removal of the esophageal endotrachealtube and did not develop hypoxemia.
Of the 20 children with moderate hypoxemia, onehad an accompanying comment describing arequired second laryngoscopic attempt, but there
were no further details. Of the 18 children whodeveloped severe hypoxemia, there were accompa-nying comments on four. One was noted to bedifficult to intubate but only one attempt wasrequired. A second patient required a second intu-bation attempt because of difficulty visualizing thelarynx. A third patient required two intubationattempts without an apparent cause. A fourthpatient developed emesis during induction, fol-lowed by laryngospasm. Succinylcholine wasadministered and mask ventilation restored a nor-mal SpO2 prior to endotracheal intubation. Therewere no comments that accompanied the patientswho developed bradycardia or hypotension.
When we analyzed the incidence of moderate orsevere hypoxemia based on the weight of the child,we found that the patients between 10 and 19 kgwere not more likely to demonstrate moderatehypoxemia than patients weighing 20 kg or greater(P = 0.19). However, patients between 10 and 19 kgwere more likely to demonstrate severe hypoxemiathan patients weighing 20 kg or greater (P < 0.0001)(Figure 1). There was no association between the
Table 1Patient characteristics (n = 1070)
Mean ± SD (range)
Age (years) 8.13 ± 2.92 (3–12)Weight (kg) 31.1 ± 16.5 (10–180)
Type of surgerya N (%)
General surgery 677 (63.3)Neurosurgery 61 (5.7)Ophthalmology 18 (1.7)ENT 21 (2.0)Orthopedics 262 (24.6)G ⁄U 29 (2.7)
Muscle relaxantb N (%)
Succinylcholine 911 (85.1)Vecuronium 77 (7.2)Rocuronium 64 (6.0)Mivacurium 10 (0.9)
aTwo cases did not have the procedure documented in theelectronic record.bEight cases did not include documentation of the muscle relaxantused.
Table 2Complications associated with rapid sequence intubation
Complication N (%)
Moderate hypoxemia (SpO2 80–89%) 20 (1.9)Severe hypoxemia (SpO2 < 80%) 18 (1.7)Bradycardia (HR < 60 bpm) 5 (0.5)Hypotension (SBP < 70 mmHg) 8 (0.8)Difficult intubation 18 (1.7)
Total 69 (6.4)
(a)
(b)
Figure 1(a) Patients between 10 and 19 kg were not more likely todemonstrate moderate hypoxemia (SpO2 80–89%) than patientsweighing 20 kg or greater (P = 0.19). (b) Patients between 10 and19 kg were more likely to demonstrate severe hypoxemia thanpatients weighing 20 kg or greater (SpO2 < 80%) (P < 0.0001).
PEDIATRIC RAPID SEQUENCE INDUCTION 423
! 2010 Blackwell Publishing Ltd, Pediatric Anesthesia, 20, 421–424
Gencorelli, Ped Anesth 2010

EL ESTUDIO WARNER

EL ESTUDIO WARNER
• 63180 ANESTESIAS GENERALES EN NIÑOS MENORES DE 18 AÑOS.
• ASPIRACION PULMONAR EN 24 PACIENTES. (0.04%).
• NO HUBO MUERTES. SOLO 3 PACIENTES QUE REQUIRIERON IPPV POR MAS DE 48 H.
• ASPIRACION OCURRIO MAYORMENTE EN EL MOMENTO DE INDUCCION, A PESAR DEL USO DE LA PRESION CRICOIDEA.
• EN RIESGO: PACIENTES MENORES DE 3A CON CUADROS OBSTRUCTIVOS INTESTINALES.
Warner X 5, Anesthesiology 1999

ISR MODIFICADA EN NIÑOS
• PREOXIGENAR DE LA MEJOR MANERA POSIBLE.
• ASEGURAR UN PLANO PROFUNDO DE ANESTESIA Y PARALISIS MUSCULAR COMPLETA.
• VENTILACION CON PRESION POSITIVA GENEROSA.
• NO APLICAR PRESION CRICOIDEA DE RUTINA.
• PRESION CRICOIDEA EN CIRCUNSTANCIAS ESPECIALES. EJ: DISTENSION ABDOMINAL SEVERA.

MITO O REALIDADTUBOS ENDOTRAQUEALES EN PEDIATRIA: ¿CON
CUFF O SIN CUFF?
• EL USO DE TUBOS ET SIN CUFF, YA SEA DE BAJA O ALTA PRESION, NO ESTA RECOMENDADO EN INFANTES Y NIÑOS MENORES DE 8 AÑOS DE EDAD.
Bissonnette y Dalens, Ped Anesthesia 2002

.$B1D664&2$,6??$+%0136+(
`1: JXXX*+,"##$%&f&RX&<$02(
Z1: JXX`*+,"##$%&f&Z&<$02(
V1: JXXS&!"##$%&^U&$'$+&3+&3+#0+1(

.$B1D664&2$,6??$+%0136+(
\2% JXXR*+,"##$%&f&]&<$02(
T1: JXXS.20%3136+0A&������ �� �������]&<$02(
���� ��������
.$B1D664&2$,6??$+%0136+(
\2% JXXR*+,"##$%&f&]&<$02(
T1: JXXS.20%3136+0A&������ �� �������]&<$02(
���� ��������

.$B1D664&2$,6??$+%0136+(
Z1: RSSZ&*+,"##$%&f&]&<$02(
V1: JXXZ*+,"##$%&1"D$(&?0<&D$&^U

-B,$AA$+1&F+(3C:1
@(&D0,4&0(&1:$&\2%
-%3136+&3+&RSST&1:$&"($&6#&,"##$%&1"D$(&3(&,6+(3%$2$%)
!:0=1$2&D<&9$++3(&K3(:$27&89

¿TUBOS ET CON CUFF O SIN CUFF EN NIÑOS?
• HISTORICAMENTE, UNA ALTA INCIDENCIA DE COMPLICACIONES EN VIA AEREA, NOTABLE EDEMA SUB GLOTICO Y ESTENOSIS, CON EL USO DE LOS TUBOS ET CON CUFF DE LATEX ROJO.
• LOS DATOS PICU (NEWTH,2004) SUGIEREN Q NO HAY DIFERENCIAS EN CUANTO A COMPLICACIONES CON EL USO DE TUBOS ET CON CUFF.
• LOS NUEVOS DISEÑOS DE LOS TUBOS ET HAN PERMITIDO EL INCREMENTO EN EL USO DE MANERA SEGURA DE LOS TUBOS ET CON CUFF.


Evidence-Based Positive Clinical Outcomes
Prospective Randomized Multi-Center Study
24 centros hospitalarios en Europa: n = 2,249 patients
Promedio de edad de pctes: 1.9 years (3.0mm-4.5mm tubos ET)
Recambio de Tubo: 2.1% MICROCUFF, 29.9% Tubos sin cuff
Estridor Post extubacion: 4.38% MICROCUFF, 4.69% Tubos sin cuff
Pressure del cuff para sellar la traquea: 10.6 cm H2O

EL ESTUDIO WEISS METODOS
• TAMAÑO MUESTRAL GRANDE.
• RAMDOMIZADO DE FORMA ADECUADA.
• CIEGO.
• INCLUYO ESTRIDOR DE VARIAS CAUSAS.
• SOLO USO UN TIPO DE TUBO ET: MICROCUFF.
• USO INSUFLACION MINIMA DEL CUFF CON MEDICION DE PRESION DE CUFF.

SOBRE TUBOS ET SIN CUFF...
3.0mm 3.5mm 4.0mm
Presion sobre cricoidesFuga en Via Aerea
Tubo muy pequeño Tubo muy grande
- Ventilacion dificil - Alto riesgo de estenosis subglotica

Glotis
CrIcoides
Carina
TextoFuga de Aire
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Alto riesgo de aspiracion
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Alto riesgo de aspiracion
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Alto riesgo de aspiracion
Dificultad para ventilacion
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Alto riesgo de aspiracion
Dificultad para ventilacion
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Alto riesgo de aspiracion
Dificultad para ventilacion
Alto Flujo de gas fresco
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Monitoreo Inadecuado
Alto riesgo de aspiracion
Dificultad para ventilacion
Alto Flujo de gas fresco
Glotis
CrIcoides
Carina
TextoFuga de Aire
Tubos Pequeños Tubos Grandes
2.8 veces mas posibilidades de desarrollar eventos adversos.
Cause primaria (92%) de trauma laringeo en un estudio con 65 pacientes.
Diferencias de Sellado con Tubo ET sin Cuff
Suominen P et al. Paediatric Anaesthesia, 2006.Holzki J. Paediatric Anaesthesia, 1997.Weiss and Gerber. Pediatric Anesthesia, 2006.

Carina
Cricoides
Glotis
TraqueaMedia
Posicion Adecuada del cuff
Cortos, cuff cilíndrico localizado cerca de la punta del tubo ET.
Localización del Cuff en la traquea, y no en la laringe que es sensible a los cambios de presión del cuff.
Marca de profundidad basada anatómicamente lo que resulta en una correcta posición.
La punta debe situarse en la mitad de la traquea para evitar la migración endobronquial.
Debe tener un cuff de baja presión para reducir los riesgos de trauma a la via aerea.
Localización Ideal y Características de los Tubos ET Pediatricos con Cuff

Posición del cuff muy alta, cuffs muy largos.
Ausencia de marcas de profundidad.
No tienen recomendaciones para la selección de tamaño.
Cuff position should avoid pressure-sensitive vocal cords and cricoid ring
Muchos Tubos ET tienen diseños no adecuados para uso pediatrico
Weiss M et al, BJA 2004Texto

The Solution:KIMBERLY-CLARK* MICROCUFF* ET Tube
Finally, a cuffed ET tube specifically designed
Dullenkopf A et al. Pediatric Anesthesia, 2004.

The Solution:KIMBERLY-CLARK* MICROCUFF* ET Tube
Finally, a cuffed ET tube specifically designed
Short, distally-placed cuff
Introducing a microthin
polyurethane cuff
Clinically verified, anatomically correct vocal
cord depth mark
Ensures correct placement, avoiding repeated
intubations
Superior seal at ultra-low pressures
Confidence in a sealed airway
Dullenkopf A et al. Pediatric Anesthesia, 2004.

Fit and seal characteristics of a new paediatric trachealtube with high volume—low pressure polyurethane cuff
A. DULLENKOPF, A. C. GERBER and M. WEISS
Department of Anaesthesia, University Children’s Hospital Zurich, Zurich, Switzerland
Background: To evaluate a new paediatric tracheal tube(Microcuff, Weinheim, Germany) with an ultrathin highvolume—low pressure polyurethane cuff.Methods: With approval of the Hospital Ethics Committeetracheas of children undergoing general anaesthesia were intub-ated using a Microcuff tube. Tube sizes were selected accord-ing to: internal diameter (mm)! age/4" 3.5 in children aged#2 years. In newborns (#3 kg) $1 year, ID 3.0-mm tubes, and inchildren from 1 to 2 years, internal diameter 3.5-mm tubes wereused. Tubes were classified too large if no air leakage wasobtained at an airway pressure of 20 cm H2O with the cuff notinflated. Sealing pressure was assessed by auscultation. Post-extubation croup requiring therapy was noted.Results: Five-hundred children were studied. In eight childrenthe tubes were too large. Sealing pressure was 9.7% 2.5 cm H2O
(4—20). In two patients postextubation croup required singularshort-term therapy.Conclusions: Microcuff paediatric tracheal tubes provided tra-cheal sealing with cuff pressures considerably lower thanusually accepted. The rate of tube exchange was very low(1.6%), as was the rate of airway morbidity (croup requiringtherapy; 0.4%).
Accepted for publication 1 October 2004
Key words: Children, paediatric; croup, sealing, tracheal;cuff, high volume-low pressure; morbidity; tracheal tube.
# Acta Anaesthesiologica Scandinavica 49 (2005)
THE use of cuffed tracheal tubes is a controversialtopic in paediatric anaesthesia and intensive care
(1, 2). Whereas traditionally recommended for chil-dren older than 8—10years, during the past decadeseveral authors have argued for the use of cuffedtracheal tubes in younger children and infants (3—7).The advantages known from adult anaesthesia are
less gas leakage around the tube cuff, with improvedefficiency of ventilation (8), reduced environmentalpollution (4, 9), more reliable end-tidal gas monitoring(1), less aspiration, and the possibility for low-flowanaesthesia and for lung function and oxygen con-sumption testing.Specific advantages of the use of cuffed tracheal
tubes in children are a reduced need to replace ill-fitting tracheal tubes and a lower risk of using over-
sized uncuffed tubes in order to avoid air leakage (4).Oversized tracheal tubes in children are the maincause of subglottic mucosal ischemia and ulcerationleading to subglottic stenosis (1, 10, 11).The selection of cuffed tubes with a smaller internal
diameter compared to uncuffed tubes implicates ahigher chance for adequate fit of the tube at the cricoidring. The tube cuff allows compensation for the result-ing air leak as required. Despite this, cuffed trachealtubes in children younger than 8years are only usedroutinely by a minority of paediatric anaesthetists (2).A frequently cited argument against their use is thefear of cuff-induced tracheal and laryngeal airwayinjury. Cuff-related airway damage can be caused bycuff hyperinflation (12) and by inadequatelydesigned cuffed paediatric tracheal tubes (13—15).The aim of this study was to clinically evaluate a
newly designed paediatric tracheal tube with highvolume—low pressure polyurethane cuff (MPTT;Microcuff paediatric tracheal tube, Magill-tip, micro-thin-walled high volume—low pressure cuff; Micro-cuff GmbH, Weinheim, Germany) with respect to theadequacy of the proposed tube size selection, mini-mal cuff pressure required to seal the trachea and
Weiss and Gerber are involved in the development of thepresented Microcuff P. E. T. in co-operation with MicrocuffGmbH, Weinheim, Germany.Financial Disclosure Statement: no agreements or financial
benefits arose from this co-operation. Dr A. Dullenkopfobtained a Clinical Research Grant from Microcuff GmbH,Weinheim, Germany, for the presented study.
Acta Anaesthesiol Scand 2005; 49: 232—237 Copyright # Acta Anaesthesiol Scand 2005Printed in Denmark. All rights reserved
ACTA ANAESTHESIOLOGICA SCANDINAVICA
doi: 10.1111/j.1399-6576.2004.00599.x
232

TUBOS ET CON CUFF EN NIÑOS
• NO HAY ALTA INCIDENCIA DE COMPLICACIONES EN TANTO SE ELIJA :
• UN TAMAÑO ADECUADO DEL TUBO ET PARA SER USADO.
• UN DISEÑO DE TUBO ET ADECUADO.
• EVITE LA SOBREDISTENSION DEL CUFF.

USO DE TUBOS ET EN NIÑOS
• ENCUESTA POSTAL EN 2001:
• > 80 % USO 25%
• 20% − 80% USO 38%
• < 20% USO 18%
• EXCEPCIONALMENTE 19%
• ENCUESTA POR EMAIL EN REINO UNIDO, 2008:
• RARAMENTE 13%
• OCASIONALMENTE 60%
• DE RUTINA 27%
Flynn, Eur Jour Anesth 2008

SOBRE AGENTES INHALADOS...

AGENTES INHALADOS...
• ES SEVOFLUORANO EL CAUSANTE DEL DELIRIO AL DESPERTAR?
• EL OXIDO NITROSO. REALMENTE CONTRIBUYE A LAS NAUSEAS Y VOMITOS POSTOPERATORIOS?

SOBRE LA AGITACION AL DESPERTAR...
• QUIEN CAUSA MAS AGITACION AL DESPERTAR: SEVOFLUORANO? ISOFLUORANO?

AD: SEVOFLUORANO VS HALOTANO
Anesthesiology 2008; 109:225–32 Copyright © 2008, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc.
Greater Incidence of Emergence Agitation in Children afterSevoflurane Anesthesia as Compared with Halothane
A Meta-analysis of Randomized Controlled TrialsNorifumi Kuratani, M.D., Ph.D.,* Yumiko Oi, M.D.†
Background: Sevoflurane is a popular inhalational anestheticfor general anesthesia in children. The higher incidence ofemergence agitation has been suspected after sevoflurane an-esthesia as compared with halothane, whereas some controlledstudies showed conflicting results. In this report, the authorsperformed a meta-analysis of randomized controlled trials tocompare the incidence of emergence agitation in children aftersevoflurane or halothane anesthesia.
Methods: A comprehensive literature search was conductedto identify clinical trials that compared the incidence of emer-gence agitation in children anesthetized with sevoflurane ver-sus halothane. Two reviewers independently assessed each re-port to meet the authors inclusion criteria and extracted data.The data from each trial were combined using the Mantel-Haenszel fixed-effect model to calculate the pooled odds ratioand 95% confidence interval. Funnel plots were used to assesspublication bias. Subgroup analysis was used to clarify the ef-fects of age, surgical procedure, pain treatment, and premedi-cation on the incidence of emergence agitation.
Results: The authors identified 23 studies that met theirinclusion criteria. Overall, 1,252 patients received sevofluraneand 1,111 had halothane. Heterogeneity of data was statisticallyrefuted. The pooled odds ratio for all studies was 2.21, with a95% confidence interval of 1.77–2.77 (P < 0.0001). Publicationbias was not apparent in a funnel plot. All subgroup analysesshowed a higher incidence of agitation after sevofluraneanesthesia.
Conclusions: This meta-analysis revealed that emergence ag-itation occurred more frequently with sevoflurane than withhalothane anesthesia in children.
SEVOFLURANE is a popular inhalational anesthetic forgeneral anesthesia in children. It is especially character-ized by a lower blood/gas partition coefficient, less irri-tation to the airway, less cardiodepressive effect, andless toxicity to the liver or kidney as compared withother volatile anesthetics. Anesthesiologists prefer thosecharacteristics for pediatric use. However, concern hasbeen raised over its propensity to result in significantexcitatory emergence in the immediate recovery phaseof sevoflurane anesthesia. Emergence agitation is a major
source of dissatisfaction for parents, nurses, and otherstaking care of these children. The irritable, uncoopera-tive, incoherent child who is inconsolably crying, moan-ing, kicking, or thrashing is at risk for injury and requiresextra nursing care and supplemental sedative and/oranalgesic medications, which may delay patient dis-charge from hospital.
Pediatric anesthesiologists mostly agree that sevoflu-rane causes a higher incidence of emergence agita-tion,1–3 whereas some controlled studies comparingsevoflurane and halothane showed conflicting results.4,5
The conflicting results may arise from the differences ofstudy design, the background of study patients, andstudy quality. Under the existence of many confoundingfactors regarding emergence agitation, it is hard to drawfrom a single study a definitive answer about whethersevoflurane results in a higher probability of emergenceagitation in children. Various methods, including treat-ments against surgical pain and prescriptions of sedativepremedication, have been tried to prevent emergenceagitation after sevoflurane anesthesia, but their validitieshave not been well clarified.
Meta-analysis is a statistical tool that can be used toevaluate the literature in both qualitative and quantita-tive ways, accounting for variations in characteristicsthat can influence the overall estimate of outcomes ofinterest. Statistical aggregation of randomized trialsthrough meta-analysis allows for increased power to de-tect potential differences in clinical outcomes. In thisreport, we performed a meta-analysis of randomizedcontrolled trials to compare the incidence of emergenceagitation in children after sevoflurane or halothaneanesthesia.
Materials and Methods
We conducted a systematic review according to the Qual-ity of Reporting of Meta-analyses (QUOROM) recommen-dations for improving the quality of meta-analyses.6
A comprehensive literature search was performed us-ing MEDLINE, EMBASE, American College of PhysiciansJournal Club database, Cochrane Database of SystematicReviews, Cochrane Central Register of Controlled Trials,and Database of Abstracts of Reviews of Effects. Everyeffort was made to find studies reporting on emergenceagitation or equivalent state after sevoflurane or halo-thane anesthesia in children. Although there seemed tobe no widely accepted definition of emergence agitation
* Assistant Professor, Department of Anesthesiology, Saitama Medical Univer-sity. † Anesthesiologist, Department of Anesthesia, National Mie Hospital, Mie,Japan.
Received from the Department of Anesthesiology, Saitama Medical University,Saitama, Japan. Submitted for publication December 12, 2007. Accepted forpublication April 14, 2008. Support was provided solely from institutional and/ordepartmental sources. A preliminary report of this research was presented at theAnnual Meeting of the American Society of Anesthesiologists, Chicago, Illinois,October 16, 2006.
Address correspondence to Dr. Kuratani: Department of Anesthesiology,Saitama Medical University, 38 Morohongo, Moroyama-machi, Iruma-gun, Saitama350-0495, Japan. [email protected]. Information on purchasing reprintsmay be found at www.anesthesiology.org or on the masthead page at thebeginning of this issue. ANESTHESIOLOGY’s articles are made freely accessible to allreaders, for personal use only, 6 months from the cover date of the issue.
Anesthesiology, V 109, No 2, Aug 2008 225

HISTORIA CON ISOFLUORANO
• EXPERIENCIA INICIAL CON 100 PACIENTES EN LOS AÑOS 70. (DRIPPS Y PAUCA).
• USO GENERAL EN NORTEAMERICA DESDE 1982.
• INTRODUCCION EN REINO UNIDO EN EL AÑO 1983.
• NUNN PUBLICO UNA SERIE DE CASOS SOBRE LA EXPERIENCIA EN REINO UNIDO EN EL AÑO 1983 Y 1984.
• 135 PACIENTES EN EL HOSPITAL GENERAL DEL DISTRITO.
• 2 MESES A 95 AÑOS.
Dripps, Nunn, BJA 1973 y 1985

QUE DIJO NUNN SOBRE ISOFLUORANO?
• “EL UNICO GRAN PROBLEMA FUE EL DELIRIO, LO QUE REQUIRIO LA INTERVENCION MAS DE 1 ENFERMERA Y NO RESPONDIA A MORFINA EV”.
• “ESTOY DE ACUERDO CON LO VISTO POR DRIPPS Y PAUCA, DE QUE LA CONDICION (DELIRIO) ES CAUSADO POR LA PERCEPCION SUBITA DEL DOLOR POSTOPERATORIO COMO RESULTADO DE LA RAPIDA ELIMINACION DEL ISOFLUORANO”.
Nunn, British Journal of Anesthesia 1985

ISOFLUORANO VS SEVOFLUORANO
• ENSAYO CLINICO RANDOMIZADO, 40 NIÑOS, DE 4 MESES A 14 AÑOS, CIRUGIA DE ABDOMEN INFERIOR CON BLOQUEO REGIONAL.
Tracheal Extubation of Deeply Anesthetized PediatricPatients: A Comparison of Isoflurane and SevofluraneRobert D. Valley, MD, Justin T. Ramza, MD, Pauletta Calhoun, RN,Eugene B. Freid, MD, FCCM, Ann G. Bailey, MD, Vincent J. Kopp, MD, andLinda S. Georges, MD
Department of Anesthesiology, University of North Carolina School of Medicine, Chapel Hill, North Carolina
We studied the emergence characteristics of unpre-medicated children tracheally extubated while deeplyanesthetized (“deep extubation”) with isoflurane orsevoflurane. Forty children were assigned to one of twogroups, Group I or Group S. At the end of the operation,Group I patients were extubated while breathing 1.5times the minimum alveolar anesthetic concentration(MAC) of isoflurane. Group S patients were tracheallyextubated while breathing 1.5 times the MAC ofsevoflurane. Recovery characteristics and complica-tions were noted. Group S patients were arousablesooner than Group I patients (10.1 ! 6.5 vs 16.3 !9.9 min). Later arousal scores and times to dischargewere the same. There were no serious complications in
either group. Breath-holding was more common inGroup I. We conclude that the overall incidence of air-way problems and desaturation episodes was similarbetween groups. Emergency delirium was common inboth groups (32% overall: 40% for Group I, 25% forGroup S). Implications: Deep extubation of childrencan be safely performed with either isoflurane orsevoflurane. After deep tracheal extubation, airwayproblems occur but are easily managed. Return to anarousable state occurred more quickly with sevoflu-rane, although time to meeting discharge criteria wasnot different between the two groups. Emergence delir-ium occurs frequently with either technique.
(Anesth Analg 1999;88:742–5)
T racheal extubation of patients while deeply anes-thetized (deep extubation) has the advantage ofremoving a potent stimulus to coughing and
breath-holding before the return of upper airway re-activity (1,2). This technique may provide a smootheremergence from anesthesia and may reduce bleedingafter airway procedures, reduce the chance of wounddehiscence, or lower the likelihood of bronchospasm.In 1991, Pounder et al. (3) reported that children un-dergoing tracheal extubation while deeply anesthe-tized with either isoflurane or halothane had signifi-cantly fewer episodes of hemoglobin desaturationthan those who were tracheally extubated awake.
Leaving the patient with an unprotected airway isthe primary reservation to extubating patients whiledeeply anesthetized. Techniques that reduce the timefrom tracheal extubation to return of protective airwayreflexes would minimize the risk of aspiration or air-way obstruction secondary to obtundation.
Because sevoflurane is easily tolerated for inhaledinduction of anesthesia and has a relatively low blood-gas solubility partition coefficient, we hypothesizedthat sevoflurane may be more effective for deep extu-bation than isoflurane (4,5).
MethodsAfter obtaining institutional review board approvaland written, informed consent, forty ASA physicalstatus I or II children were enrolled. They ranged inage from 4 mo to 14 yr and were all scheduled forelective surgical procedures below the umbilicus.Children with a history of airway disease were ex-cluded from the study. Children underwent either anIV induction with propofol or an inhaled inductionwith sevoflurane and nitrous oxide; all were tracheallyintubated with the use of muscle relaxants. Mainte-nance anesthesia was determined by random assign-ment to either the isoflurane (I) or sevoflurane (S)group and consisted of the assigned potent inhaledanesthetic and nitrous oxide in oxygen. Exhaled anes-thetics were monitored using side-stream sampling toan infrared analyzer (Datex Ultima; Datex-Engstrom,Inc., Tewksbury, MA). No systemic analgesics were
Accepted for publication December 23, 1998.Address correspondence to Robert D. Valley, MD, Department of
Anesthesiology, University of North Carolina at Chapel Hill, CB#7010 223 Burnett-Womack Building, Chapel Hill, NC 27599-7010.
©1999 by the International Anesthesia Research Society742 Anesth Analg 1999;88:742–5 0003-2999/99/$5.00

ISOFLUORANO VS SEVOFLUORANO
• ENSAYO CLINICO RANDOMIZADO, 40 NIÑOS, DE 2 MESES A 6 AÑOS, CIRUGIA DE ABDOMEN INFERIOR CON BLOQUEO CAUDAL.
AGENTE AGITACION AL DESPERTAR
ISOFLUORANO ? 0
SEVOFLUORANO 6/20 ( 30% )
Le Berre, Pediatric Anesthesia 2001

AGITACION AL DESPERTAR POR AGENTE ANESTESICO
AGENTEAGITACION AL
DESPERTARVALOR P RR
SEVOFLUORANO 57/236 (24%) 0.002 1.77
ISOFLUORANO 68/300 (23%) 0.004 1.78
HALOTANO 44/282 (16%) 0.07 NA
PROPOFOL 6/62 (10%) 0.06 NA
Voepel Lewis, Anesth Analg 2003

ISOFLUORANO VS SEVOFLUORANO
• ENSAYO CLINICO ALEATORIZADO, 59 NIÑOS, DE 1 AÑO A 6 AÑOS,CIRUGIA DE HERNIA INGUINAL O CIRCUNCISION CON BLOQUEO CAUDAL.
AGENTE AGITACION AL DESPERTAR
ISOFLUORANO 10/29 (34%)
SEVOFLUORANO 9/30 (30%)
Meyer, Pediatric Anesth 2007

AGITACION AL DESPERTAR: SEVOFLUORANO VS ISOFLUORANO
• LA MAYORIA DE LA EVIDENCIA CONCERNIENTE A LA AGITACION AL DESPERTAR RELACIONADA CON SEVOFLUORANO USO HALOTANO COMO EL AGENTE A COMPARAR.
• EN REALIDAD HAY MAS AGITACION AL DESPERTAR CON SEVOFLUORANO COMPARADO A HALOTANO. ESPECIALMENTE EN NIÑOS EN EDAD PRE ESCOLAR.
• LA EVIDENCIA SUGIERE QUE EL ISOFLUORANO ES SIMILAR AL SEVOFLUORANO CON RESPECTO A ESTE PUNTO.

MITO O REALIDADOXIDO NITROSO
• ES EL OXIDO NITROSO UNA CAUSA POTENTE DE NAUSEAS Y VOMITOS POST OPERATORIOS EN NIÑOS?

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
• 4598 PCTES, 30 ESTUDIOS.
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
• 4598 PCTES, 30 ESTUDIOS.
• REVISION SISTEMATICA Y META ANALISIS.
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y NAUSEAS Y VOMITOS POSTOPERATORIOS EN ADULTOS
• 4598 PCTES, 30 ESTUDIOS.
• REVISION SISTEMATICA Y META ANALISIS.
• NVPO: CON OXIDO NITROSO: 33% SIN OXIDO NITROSO: 27%
REVIEW ARTICLE
Association between nitrous oxide and the incidence ofpostoperative nausea and vomiting in adults: a systematicreview and meta-analysis
J. Fernandez-Guisasola,1 J. I. Gomez-Arnau,2 Y. Cabrera3 and S. Garcıa del Valle4
1 Staff Anaesthesiologist, Anaesthesia Department, Hospital Ruber, 2 Chief, Anaesthesia and Critical Care Department,4 Chief, Unit of Anaesthesia, Hospital Universitario Fundacion Alcorcon, 3 Staff Gynaecologist, Obstetrics and
Gynaecology Department, Hospital Infanta Sofıa, San Sebastian de los Reyes, Madrid, Spain
SummarySome, but not all studies have suggested intra-operative use of nitrous oxide is correlated withpostoperative nausea and vomiting. We performed a meta-analysis of randomised controlled trialsto compare the incidence of nausea and vomiting in adults following general anaesthesia withor without nitrous oxide. We retrieved 30 studies (incorporating 33 separate trials) that investigateda ‘nitrous oxide group’ (total 2297 patients) vs a ‘no-nitrous oxide group’ (2301 patients). Omittingnitrous oxide significantly reduced postoperative nausea and vomiting (pooled relative risk 0.80,95% CI 0.71–0.90, p = 0.0003). However, the absolute incidence of nausea and vomiting washigh in both the nitrous oxide and no-nitrous oxide groups (33% vs 27%, respectively). In sub-group analysis, the maximal risk reduction was obtained in female patients (pooled relative risk0.76, 95% CI 0.60–0.96). When nitrous oxide was used in combination with propofol, the ant-iemetic effect of the latter appeared to compensate the emetogenic effect of nitrous oxide (pooledrelative risk 0.94, 95% CI 0.77–1.15). We conclude that avoiding nitrous oxide does reduce therisk of postoperative nausea and vomiting, especially in women, but the overall impact is modest.
........................................................................................................
Correspondence to: Jaime Fernandez-Guisasola MascıasE-mail: [email protected]
Accepted 27 December 2009
Postoperative nausea and vomiting (PONV) is probablythe most common cause of morbidity followinganaesthesia [1], occurring in 20–30% of patients (butin up to 70% of those with certain risk factors [2]).Sometimes considered a minor, unavoidable com-plication, many patients perceive PONV as highlyunpleasant, and some even describe it as worse thanpostoperative pain [3]. PONV increases the cost ofprocedure because anti-emetic medication becomesnecessary, or because discharge from hospital isdelayed.Marked advances have been made in our knowledge of
risk factors associated with PONV, and predictive scoringsystems have been developed [4]. However, the patho-physiology of PONV is still not well established. Manystudies are essentially epidemiological [5], and genetic or
molecular mechanisms have not been extensively exam-ined [6].It has been suggested that nitrous oxide (N2O)
contributes significantly to PONV [7–9], perhaps influ-encing the vestibular system by its diffusion into theclosed cavity of the middle ear, or by expanding theintestinal wall or releasing endogenous opioid peptidesand activating the area postrema of the brain [10]. Whilemany studies have demonstrated a positive correlationbetween N2O and PONV [11–13], others have found noassociation [14–16].When trials reach differing conclusions, a systematic
quantitative review of the original randomised clinicaltrials is a useful method of assessing the evidence. Ourmain purpose, therefore, was to compare the incidence ofPONV in adults following general anaesthesia with or
Anaesthesia, 2010, 65, pages 379–387 doi:10.1111/j.1365-2044.2010.06249.x.....................................................................................................................................................................................................................
! 2010 The AuthorsJournal compilation ! 2010 The Association of Anaesthetists of Great Britain and Ireland 379

OXIDO NITROSO Y MIRINGOTOMIA
• N20/O2/HALOTANO (n=158) 13% NVPO
• 02/HALOTANO (n=162) 13% NVPO
• EFECTO DE LA EDAD
Edad (Años) % Vomito
0.5 a 2.9 4%
3.0 a 5.9 11%
6.0 a 8.9 17%
9.0 a 12.9 31%
Splinter, Can J Anesth 1995

OXIDO NITROSO Y CIRUGIA DENTAL
• n= 330, no antiemeticos
Resultado Oxido Nitroso Control
NV en Hospital 24% 15%
Vomito luego del alta (mismo dia)
23% 20%
Vomito luego del alta (dia siguiente)
4% 3%
Total 35% 30%
Splinter, Anesth Analg 1997

NVPO Y CIRUGIA DENTAL
• DEXAMETASONA/ONDANSETRON (n=87)
• SOLO ONDANSETRON (n=91)
• TODOS LOS SUJETOS DE ESTUDIO RECIBIERON N2O, ISOFLUORANO, FENTANILO Y 20 ML/KG DE LACTACTO RINGER.
• NINGUNO DE LOS SUJETOS ESTUDIADOS VOMITO EN EL HOSPITAL.
• LUEGO DE 24 H:
• 1/87 VOMITO EN GRUPO DEXA/ONDA
• 8/91 VOMITO EN GRUPO SOLO ONDA
McIntyre, SPA 2010

NVPO Y TONSILECTOMIA
• n = 60 , no recibieron antiemeticos
Resultado Oxido Nitroso Control
NV en URPA 50% 40%
NV luego del Alta 60% 53%
Total 67% 60%
Pandit, Anesth Analg 1995

OXIDO NITROSO Y NVPO EN NIÑOS
• NO HAY EVIDENCIA PERSUASIVA QUE EVITE QUE EL OXIDO NITROSO EN NIÑOS DE RIESGO BAJO O MODERADO EVITE NVPO.
• OTROS FACTORES SON IMPORTANTES (EJ. CARGA HIDRICA).
• LOS ANTIEMETICOS SI FUNCIONAN...!!!

PUNTOS SOBRE OTROS MEDICAMENTOS
• PROBLEMAS DE SEGURIDAD:
• DEXAMETASONA
• KETOROLACO

DEXAMETASONA Y TONSILECTOMIA
• EXISTEN RIESGOS?
• SANGRADO?
• NECROSIS AVASCULAR?
• OTROS?

SANGRADO EN AMIGDALAS Y DEXAMETASONAPRELIMINARY
COMMUNICATION
Dexamethasone and Risk of Nauseaand Vomiting and Postoperative BleedingAfter Tonsillectomy in ChildrenA Randomized TrialChristoph Czarnetzki, MD, MBANadia Elia, MD, MScChristopher Lysakowski, MDLionel Dumont, MDBasile N. Landis, MDRoland Giger, MDPavel Dulguerov, MDJules Desmeules, MDMartin R. Tramèr, MD, DPhil
TONSILLECTOMY IS ONE OF THEmost frequently performed sur-gical procedures in children. In1998, the rate varied from 19
per 10 000 children in Canada to 118per 10 000 in Northern Ireland.1 In theUnited States, about 186 000 proce-dures are performed on an outpatientbasis every year.2 Common complica-tions of tonsillectomy are postopera-tive nausea and vomiting (PONV), pain,and bleeding.3 Nonsteroidal anti-inflammatory drugs (NSAIDs) havebeen widely used in this setting for theirpronounced analgesic efficacy and alack of the emetogenic effect inherentto opioids. However, classic NSAIDs,through reversible platelet inhibition,further increase the risk of bleeding af-ter tonsillectomy.4,5
Dexamethasone has antiemeticproperties in the surgical setting.6 Aninternational expert panel recom-mended dexamethasone, alone or aspart of a multimodal regimen, for
Author Affiliations: Divisions of Anesthesiology (DrsCzarnetzki, Elia, Lysakowski, Dumont, and Tramèr); Oto-laryngology–Head and Neck Surgery (Drs Landis, Giger,and Dulguerov), and Clinical Pharmacology and Toxi-cology (Dr Desmeules), University Hospitals of Geneva,Institute of Social and Preventive Medicine (Dr Elia), and
Medical Faculty, University of Geneva (Drs Dulguerov,Desmeules, and Tramèr), Geneva, Switzerland.Corresponding Author: Martin R. Tramèr, MD, DPhil,Division of Anesthesiology, University Hospitals ofGeneva, 24 rue Micheli-du-Crest, CH-1211 Geneva14, Switzerland ([email protected]).
Context Dexamethasone is widely used to prevent postoperative nausea and vom-iting (PONV) in pediatric tonsillectomy.
Objective To assess whether dexamethasone dose-dependently reduces the risk ofPONV at 24 hours after tonsillectomy.
Design, Setting, and Patients Randomized placebo-controlled trial conducted among215 children undergoing elective tonsillectomy at a major public teaching hospital inSwitzerland from February 2005 to December 2007.
Interventions Children were randomly assigned to receive dexamethasone (0.05,0.15, or 0.5 mg/kg) or placebo intravenously after induction of anesthesia. Acetami-nophen-codeine and ibuprofen were given as postoperative analgesia. Follow-up con-tinued until the 10th postoperative day.
Main Outcome Measures The primary end point was prevention of PONV at 24hours; secondary end points were decrease in the need for ibuprofen at 24 hours andevaluation of adverse effects.
Results At 24 hours, 24 of 54 participants who received placebo (44%; 95% con-fidence interval [CI], 31%-59%) had experienced PONV compared with 20 of 53 (38%;95% CI, 25%-52%), 13 of 54 (24%; 95% CI, 13%-38%), and 6 of 52 (12%; 95%CI, 4%-23%) who received dexamethasone at 0.05, 0.15, and 0.5 mg/kg, respec-tively (P!.001 for linear trend). Children who received dexamethasone received sig-nificantly less ibuprofen. There were 26 postoperative bleeding episodes in 22 chil-dren. Two of 53 (4%; 95% CI, 0.5%-13%) children who received placebo had bleedingcompared with 6 of 53 (11%; 95% CI, 4%-23%), 2 of 51 (4%; 95% CI, 0.5%-13%), and 12 of 50 (24%; 95% CI, 13%-38%) who received dexamethasone at 0.05,0.15, and 0.5 mg/kg, respectively (P=.003). Dexamethasone, 0.5 mg/kg, was asso-ciated with the highest bleeding risk (adjusted relative risk, 6.80; 95% CI, 1.77-16.5).Eight children had to undergo emergency reoperation because of bleeding, all of whomhad received dexamethasone. The trial was stopped early for safety reasons.
Conclusion In this study of children undergoing tonsillectomy, dexamethasone de-creased the risk of PONV dose dependently but was associated with an increased riskof postoperative bleeding.
Trial Registration clinicaltrials.gov Identifier: NCT00403806JAMA. 2008;300(22):2621-2630 www.jama.com
©2008 American Medical Association. All rights reserved. (Reprinted) JAMA, December 10, 2008—Vol 300, No. 22 2621
by guest on November 5, 2011jama.ama-assn.orgDownloaded from

RESULTADOS: INCIDENCIA TOTAL DE EPISODIOS DE SANGRADO
0
2
4
6
8
10
12
14
16
18
20
Placebo 0.05 0.15 0.5
% Sangrado
Dexametasona (mg/kg)
Czarnetszki, JAMA 2008

RESULTADOS: INCIDENCIA DE REOPERACION POR SANGRADO
0
4
8
12
16
20
Placebo 0.05 0.15 0.5
% Reop
Dexametasona (mg/kg)
Czarnetzki, JAMA 2008

PUNTOS SOBRE EL ESTUDIO DE CZARNETZKI
• ¿POR QUE TAN ALTA TASA DE SANGRADO?
• ¿POR QUE EL SANGRADO NO PARECE ESTAR LIGADO A LA DOSIS?
• ¿EL TERMINO TEMPRANO DEL ESTUDIO LE RESTO PODER A LOS RESULTADOS?
• COMO EL SANGRADO NO ERA SU PRIMER OBJETIVO, ¿ESTABA EL ESTUDIO DISEÑADO PARA HACER CONCLUSIONES FINALES SOBRE ESTA COMPLICACION?
Czarnetzki, JAMA 2008

EL ESTUDIO BRIGGER
2778 Tonsilectomias 2 a 18 a
1237 Dex 0.5 mg/kg 1551 Dex 1 mg/kg
4.53% ED Rx
3.6% Admitted
2.75% Reop
2.45% ED Rx
2.06% Admitted
1.55% Reop

DEXAMETASONA Y OTRAS COMPLICACIONES
• NO EXISTE EVIDENCIA DE QUE EL USO DE DEXAMETASONA CAUSE NECROSIS AVASCULAR DE CADERA CUANDO SEA USADO COMO DOSIS UNICA EN INTRAOPERATORIO.
• REPORTE RARO DE CASOS DE LISIS TUMORAL EN NIÑOS:
• NIÑO DE 8 AÑOS CON DX DE LLA, SE RECUPERO.
• NIÑO DE 3 AÑOS SIN DX DE LLA, FALLECIO.
McDonell, Anesthesia 2008

KETOROLACO Y CONSOLIDACION OSEA
• LA EVIDENCIA ACTUAL SE LIMITA A ESTUDIOS ANIMALES Y A ESTUDIOS EN ADULTOS SANOS.
• NO EXISTE EVIDENCIA EN NIÑOS A EXCEPCION DE LOS ESTUDIOS EN CIRUGIA DE ESCOLIOSIS.
• EN CIRUGIA DE ESCOLIOSIS IDIOPATICA, NO CONSOLIDACION OSEA :
• KETOROLACO 1.9%
• NO KETOROLACO 3.1%
Sucato, Spine 2008

MISCELANEAS
• ¿ES NECESARIO EL USO DE ULTRASONIDO EN LA INSERCION DEL CATETER VENOSO CENTRAL?
• LOS PADRES... ¿CUANDO DEBEN SER REUNIDOS CON SUS NIÑOS?

INSERCION DE VIA CENTRAL
• ¿EL ULTRASONIDO MEJORA LA TASA DE EXITO EN NIÑOS?

VIAS CENTRALES Y ULTRASONIDO
• NICE MENCIONA:
• EL ULTRASONIDO QUE MUESTRE IMAGENES EN 2D DEBE SER EL METODO DE ELECCION CUANDO SE INSERTE CATETERES VENOSOS CENTRALES EN VENA YUGULAR INTERNA EN ADULTOS Y NIÑOS EN “SITUACIONES ELECTIVAS”.
• EL ULTRASONIDO QUE MUESTRE IMAGENES EN 2D DEBE SER CONSIDERADO EN LA MAYORIA DE SITUACIONES CLINICAS EN LAS CUALES LA INSERCION DEL CVC SEA NECESARIA SEA ESTA UNA SITUACION ELECTIVA O DE EMERGENCIA.

META ANALISIS SOBRE USO DE US PARA CVC VIA YUGULAR INTERNA EN NIÑOS
• 5 RCT IDENTIFICADOS, 359 PACIENTES.
• NO SE DEMOSTRO DIFERENCIAS EN CUANTO A TASA DE EXITO, AL TIEMPO DE CANULACION, A PUNCION CAROTIDEA, HEMATOMA, HEMOTORAX O NEUMOTORAX.
• LA TASA DE FALLA Y PUNCION CAROTIDEA FUE MENOR EN NOVATOS QUE USARON ULTRASONIDO.
Ultrasound guided internal jugular vein access inchildren and infant: A meta-analysis of publishedstudies
STEPHANIE SIGAUT MDMD*, ALIA SKHIRI MDMD*, IDA STANYMDMD*, JONATHAN GOLMAR MDMD*, YVES NIVOCHE MD PMD PhDhD†,ISABELLE CONSTANT MD PMD PhDhD‡, ISABELLE MURAT MD PMD PhDhD§AND SOUHAYL DAHMANI MD PMD PhDhD**Assistant Professor of Anesthesia, Robert Debre University Hospital, †Professor of Anesthesia,Head of Department, Robert Debre University Hospital, ‡Professor of Anesthesia, TrousseauUniversity Hospital and §Professor of Anesthesia, Head of Department, Trousseau UniversityHospital, Paris, France
SummaryIntroduction: Central venous catheter placement is technically difficultin pediatric population especially in the younger patients. Ultrasoundprelocation and ⁄ or guidance (UPG) of internal jugular vein (IJV)access has been shown to decrease failure rate and complicationsrelated to this invasive procedure. The goal of the present study was toperform a systematic review of the advantages of UPG overanatomical landmarks (AL) during IJV access in children and infants.Material and methods: A comprehensive literature search was con-ducted to identify clinical trials that focused on the comparison of UPGto AL techniques during IJV access in children and infants. Tworeviewers independently assessed each study to meet inclusion criteriaand extracted data. Data from each trial were combined to calculatethe pooled odds ratio (OR) or themean differences (MD), and their 95%confidence intervals [CI 95%]. I2 statistics were used to assess statisticsheterogeneity and to guide the use of fixed or random effect forcomputation of overall effects. Subgroupanalysiswasused to clarify theeffects of the techniques used (prelocation or guidance) or theexperience of practitioners.Results: Literature found five articles. Most of the patients werecardiac surgery patients. In comparison with AL, UPG had no effecton IJV access failure rate (OR = 0.28 [0.05, 1.47], I2 = 75%, P = 0.003),the rate of carotid artery puncture (OR = 0.32 [0.06, 1.62], I2 = 68%,P = 0.01), haematoma, haemothorax, or pneumothorax occurrence(OR = 0.40 [0.14, 1.13], I2 = 17%, P = 0.30, OR = 0.72, OR = 0.81 [0.18,3.73], I2 = 0%, P = 0.94, respectively) and time to IJV access andhaemothorax ⁄pneumothorax occurrence. Subgroup analysis found anefficacy of ultrasound when used by novice operators or duringintraoperative use.
Correspondence to: Souhayl Dahmani, MD, PhD, Department of anesthesiology Robert Debre Hospital, 48 Bd Serurier, 75019 Paris, France(email: [email protected] ⁄ [email protected]).Received from the Department of anesthesiology Robert Debre Hospital, Assistance Publique des Hopitaux de Paris (APHP), 48 BoulevardSerurier, 75019 Paris, France.
Pediatric Anesthesia 2009 19: 1199–1206 doi:10.1111/j.1460-9592.2009.03171.x
! 2009 Blackwell Publishing Ltd 1199

CVC EN PEDIATRIA Y ULTRASONIDO
• DEBE ESTAR DISPONIBLE EL EQUIPO DE ULTRASONIDO.
• LA EVIDENCIA SUGIERE QUE ES MAS UTIL EN PACIENTES PEQUEÑOS (MENORES DE 10 KG), EN AQUELLOS CON ENFERMEDAD CARDIACA CONGENITA Y EN AQUELLOS QUE SON RECIEN INICIAN SU ENTRENAMIENTO EN CVC.
• EN PERSONAL ENTRENADO Y CON EXPERIENCIA SE HA VISTO RESULTADOS Y TASAS DE COMPLICACIONES SIMILARES USANDO O NO EL EQUIPO DE ULTRASONIDO.
• LA EVIDENCIA ESTA BASADA EN LA CANULACION VENOSA CENTRAL POR ACCESO YUGULAR, MAS NO POR VIA SUBCLAVIA.

PADRES EN LA URPA
• ¿EXISTE ALGUNA EVIDENCIA DE QUE LA PRESENCIA DE LOS PADRES EN LA URPA (RECUPERACION FASE 1) MEJORE LOS RESULTADOS OPREATORIOS?

RCT DE PADRES EN URPA
The Effects of Parental Presence in the PostanestheticCare Unit on Children’s Postoperative Behavior: AProspective, Randomized, Controlled StudyDavid R. Lardner, MBChB, FANZCA,* Bruce D. Dick, PhD, R. Psych,† and Susan Crawford, MSc‡
BACKGROUND: The effects on children of parental presence in the postanesthesia care unit(PACU) have not been extensively studied. The few published studies are retrospective,nonrandomized, or lack adequate controls. They suggest that parental presence in the PACUdecreases crying and negative behavior change postoperatively. We performed this prospective,randomized, controlled study to determine whether the presence of a parent affected cryingbehaviors in the PACU and behavior change 2 weeks postoperatively.METHODS: Randomly selected patients, aged 2.0 to 8 years 11 months, ASA physical status Ior II, and scheduled for elective outpatient surgery with an anticipated PACU stay of !10 minuteswere randomly assigned to the parent present group (n " 150) or parent absent group (n " 150)in the PACU. All parents underwent the same preparation program. Reunification occurred oncechildren’s eyes had opened for the parent present group. In the PACU, crying was scored eachminute after eye opening using a 5-point scale. Negative behavior change 2 weeks afterdischarge was determined using the Post Hospitalization Behavior Questionnaire. Because theanesthesia technique to be used was not determined a priori, data on the technique used werecollected to ensure that groups were similar. Multiple and logistic regression techniques wereused to determine predictors of crying in the PACU and behavior change 2 weeks postoperatively.RESULTS: Parental presence in the PACU made no difference in crying in the PACU. Negativebehavior change 2 weeks postoperatively occurred more frequently in the parent absent groupthan the parent present group (45.8% vs 29.3%; P " 0.007). Multiple regression identified thefollowing significant factors as predictive of larger proportion of time spent crying in the PACU(R2 " 0.256, F[5, 273] " 15.66, P # 0.001): age #5 years (P # 0.001) and higher Children’sHospital of Eastern Ontario Pain Scale score at 15 minutes after arrival in day surgery (P #0.001). Parental presence or absence from the PACU was not predictive of crying in the PACU,and neither were socioeconomic status nor intraoperative opioid analgesia. Logistic regressionidentified the following factors (!2[4] " 26.62, P # 0.001) as predictive of negative behaviorchange at 2 weeks postoperatively: being younger than 5 years (P # 0.001) and being in theparent absent group (P " 0.003).CONCLUSION: For fit healthy children undergoing outpatient surgery, parental presence in thePACU decreases negative behavior change at 2 weeks postoperatively but makes no differencein crying in the PACU. Future studies of behavior change postoperatively should consider parentalpresence in the PACU a factor and determine whether the effect persists with other interventions.(Anesth Analg 2010;110:1102–8)
Success of anesthesia is no longer determined solely bythe avoidance of mortality and major morbidity.Quality of recovery, speed of return to perioperative
function, and patient/family satisfaction are increasinglyimportant. A greater emphasis on family-centered care isdeveloping with parents, administrators, and cliniciansquestioning the validity of excluding parents from compo-nents of their child’s care.
It is clear that perioperative anxiety has been found to berelated to higher levels of postoperative pain, sleep distur-bance, and other behavioral problems.1 It is also evidentthat younger children, those with more severe illness, andthose having undergone more invasive procedures tend toexperience more medical fears and continuing behavioralindicators of stress after hospitalization.2
There is an excellent body of research concerning theeffects of parental presence during anesthetic induction.Randomized trials have shown that overall, parental pres-ence during anesthetic induction is not beneficial in reduc-ing children’s anxiety3; however, subgroups of children dobenefit from parental presence: older children, childrenwho were less active, children with calmer parents, andparents who reported higher levels of valuing preparationfor medical procedures.4
There has been considerable research on the effects ofperioperative preparation for children having surgery.Younger children tend to not benefit as much from periop-erative psychoeducational teaching programs.5 Children’sages, the timing of the preparation program, and children’stemperaments predicted children’s anxiety.6 A more recent
From the *Division of Pediatric Anesthesia, Alberta Children’s Hospital atthe University of Calgary, Calgary; †Department of Anesthesiology and PainMedicine, University of Alberta, Edmonton; and ‡Behavior Research Unit,Alberta Children’s Hospital at the University of Calgary, Calgary, Alberta,Canada.Accepted for publication November 16, 2009.Study funding: Funding information is provided at the end of the article.Disclosure: The authors report no conflict of interest.Reprints will not be available from the author.Address correspondence to David R. Lardner, MBChB, FANZCA, Divisionof Pediatric Anesthesia, Alberta Children’s Hospital at the University ofCalgary, 2888 Shaganappi Trail NW, Calgary, Alberta T3B 6A8, Canada.Address e-mail to [email protected] © 2010 International Anesthesia Research SocietyDOI: 10.1213/ANE.0b013e3181cccba8
1102 www.anesthesia-analgesia.org April 2010 • Volume 110 • Number 4

EN CONCLUSION...
• EL MENSAJE ES QUE HAY CONOCIMIENTOS CONOCIDOS. HAY COSAS QUE SABEMOS QUE CONOCEMOS. TAMBIEN HAY COSAS QUE CONOCEMOS QUE DESCONOCEMOS. ES DECIR QUE HAY COSAS QUE AHORA SABEMOS QUE NO CONOCEMOS. PERO TAMBIEN HAY COSAS NO CONOCIDAS QUE NO CONOCEMOS. FINALMENTE HAY COSAS QUE NO CONOCEMOS Y QUE NO LAS SABEMOS.