Volumen 1 Numero 8 OCTUBRE 2011 BOLETIN ALACE · Volumen 1 Numero 8 Un fenómeno digno de destacar,...
12
EDITORIAL NOTES: que hemos aprendido?: Eduardo M Targarona Servicio de cirugía Hospital Santpau Universidad Autonoma Barcelona GUIA DE LECTURA OCTUBRE 2011 Volumen 1 Numero 8 BOLETIN ALACE Hace pocos meses se publicó la revisión actualizada del White Paper sobre N.O.T.E.S(1). Dicho White Paper, publicado por primera vez en 2006(2), es la ‘hoja de ruta’ planteada por NOSCAR (Natural Orifice Surgery Consortium for Assesment and Research), el consorcio establecido entre la Sociedad Americana de Cirugía Endoscópica (SAGES) y la Sociedad Americana de Endoscopia Flexible (ASGE) para coordinar el desarrollo de NOTES. La idea de NOTES, cuyos primeros casos de cirugía transvaginal (apendicetomía, colecistectomía) pasaron desapercibidos en manos de ginecólogos (3), no fructificó hasta que el grupo Apollo, un task force liderado por A. Kalloo y dedicado al desarrollo de la endoscopia flexible no se lo planteó a finales de los años 90 (4). Sin duda, de forma similar a la primera colecistecto- mía laparoscópica, presentada por Perissat en un congreso del American College of Surgeons, que encendió la mecha explosiva de la cirugía laparoscópica en USA, el vídeo de G.V. Rao and N. Reddy (5) presentando una apendicetomía transgástrica fue también el catalizador que favoreció la difusión e interés en NOTES. CONTINUA EN LA SIGUIENTE PAGINA SECCION VIDEOS SECCION IRRE- VERENTE SECCION GALERIA SECCION EDITORIAL SECCION CASOS CURIOSOS SECCION CON- TROVERSIAS SECCION ANALI- SIS CRITICO SECCION:LO QUE NUNCA ME ENSEÑARON SECCION: CIRU- GIA BASADA EN EVIDENCIAS 2 3 4 5 6 Y 7 COMITÉ EDITORIAL DR: JOSE DE VINATEA DR: CARLOS BENAVIDES DR: AURELIO GAMBIRA- ZIO DR: EDGAR GONZALES ING. MIGUEL PRADA DR: GUSTAVO REAÑO DRA: MONICA URIBE DR: DAVID ORTEGA PUBLICACION OFICIAL DE LA ASOCIACION LATINOAMERICANA DE CIRUGIA ENDOSCOPICA ARCHIVOS ADJUNTOS HAZ CLICK AQUI
Transcript of Volumen 1 Numero 8 OCTUBRE 2011 BOLETIN ALACE · Volumen 1 Numero 8 Un fenómeno digno de destacar,...

EDITORIAL NOTES: que hemos aprendido?: Eduardo M Targarona Servicio de cirugía Hospital Santpau Universidad Autonoma Barcelona
GUIA DE LECTURA
OCTUBRE 2011 Volumen 1 Numero 8
BOLETIN ALACE
Hace pocos meses se publicó la revisión actualizada del White Paper sobre N.O.T.E.S(1).
Dicho White Paper, publicado por primera vez en 2006(2), es la ‘hoja de ruta’ planteada por
NOSCAR (Natural Orifice Surgery Consortium for Assesment and Research), el consorcio
establecido entre la Sociedad Americana de Cirugía Endoscópica (SAGES) y la Sociedad
Americana de Endoscopia Flexible (ASGE) para coordinar el desarrollo de NOTES. La idea
de NOTES, cuyos primeros casos de cirugía transvaginal (apendicetomía, colecistectomía)
pasaron desapercibidos en manos de ginecólogos (3), no fructificó hasta que el grupo Apollo,
un task force liderado por A. Kalloo y dedicado al desarrollo de la endoscopia flexible no se
lo planteó a finales de los años 90 (4). Sin duda, de forma similar a la primera colecistecto-
mía laparoscópica, presentada por Perissat en un congreso del American College of Surgeons,
que encendió la mecha explosiva de la cirugía laparoscópica en USA, el vídeo de G.V. Rao
and N. Reddy (5) presentando una apendicetomía transgástrica fue también el catalizador que
favoreció la difusión e interés en NOTES.
CONTINUA EN LA SIGUIENTE PAGINA
SECCION VIDEOS
SECCION IRRE-
VERENTE
SECCION
GALERIA
SECCION EDITORIAL
SECCION CASOS
CURIOSOS
SECCION CON-
TROVERSIAS
SECCION ANALI-
SIS CRITICO
SECCION:LO QUE
NUNCA ME
ENSEÑARON
SECCION: CIRU-
GIA BASADA EN
EVIDENCIAS
2
3
4
5
6 Y 7
COMITÉ
EDITORIAL
DR: JOSE DE VINATEA
DR: CARLOS BENAVIDES
DR: AURELIO GAMBIRA-
ZIO
DR: EDGAR GONZALES
ING. MIGUEL PRADA
DR: GUSTAVO REAÑO
DRA: MONICA URIBE
DR: DAVID ORTEGA
PUBLICACION OFICIAL DE LA
ASOCIACION LATINOAMERICANA
DE CIRUGIA ENDOSCOPICA
ARCHIVOS
ADJUNTOS
HAZ
CLICK
AQUI

NOTES: que hemos aprendido?: Eduardo M Targarona Servicio de cirugía Hospital Santpau Universidad Autonoma Barcelona
Página 2
Volumen 1 Numero 8
Hace pocos meses se publicó la revisión actualizada del White Paper sobre N.O.T.E.S(1). Dicho White Paper, publi-cado por primera vez en 2006(2), es la ‘hoja de ruta’ planteada por NOSCAR (Natural Orifice Surgery Consortium for Assesment and Research), el consorcio establecido entre la Sociedad Americana de Cirugía Endoscópica (SAGES) y la Sociedad Americana de Endoscopia Flexible (ASGE) para coordinar el desarrollo de NOTES. La idea de NOTES, cuyos primeros casos de cirugía transvaginal (apendicetomía, colecistectomía) pasaron desapercibidos en manos de ginecólogos (3), no fructificó hasta que el grupo Apollo, un task force liderado por A. Kalloo y dedicado al desarrollo de la endoscopia flexible no se lo planteó a finales de los años 90 (4). Sin duda, de forma similar a la primera colecis-tectomía laparoscópica, presentada por Perissat en un congreso del American College of Surgeons, que encendió la mecha explosiva de la cirugía laparoscópica en USA, el vídeo de G.V. Rao and N. Reddy (5) presentando una apendi-cetomía transgástrica fue también el catalizador que favoreció la difusión e interés en NOTES. En el momento actual muchos cirujanos pueden considerar NOTES como un concepto acabado. Es inevitable decir que las optimistas y tal vez exageradas expectativas iniciales en su aplicación clínica no se han cumplido, pero sin embargo, la forma en que se ha desarrollado en los últimos 6 años así como las posibles perspectivas futuras me-rece una reflexión en el momento actual. NOTES apareció 20 años después del desarrollo desordenado de la cirugía laparoscópica. Además, la percepción inmediata del grupo promotor fue que la aplicación clínica de este concepto podía ser peligrosa y con potenciales im-portantes complicaciones. Desde un punto de vista quirúrgico ‘clásico’, la perforación de la pared del tubo digestivo se entiende como una grave complicación, y lógicamente, la hipótesis de que una perforación controlada para efectuar una intervención a su través es potencialmente beneficiosa conlleva un radical cambio de paradigma lo que indujo en su inicio múltiples y razonables dudas y controversias (6-8). Es por ello que la iniciativa de ambas sociedades (SAGES y ASGE) en la creación de un grupo de interés que intentara ordenar y que además planificara el posible desarrollo de lo que inicialmente era simplemente una idea es digna de valoración y es un modelo de desarrollo pre-viamente no considerado en el mundo de la cirugía mínimamente invasiva en particular y en la comunidad quirúrgica en general. Las recomendaciones de NOSCAR incluían la necesidad de disponer modelos experimentales, trabajar en equipo entre cirujanos y gastroenterólogos y la vez recomendaba que toda actividad clínica o publicación relativa fuera realizada bajo la autorización del comité de investigación del hospital donde se realizaba la intervención. De forma mimética, se establecieron alianzas similares en los diferentes continentes (Euro-NOTES, NOSLA (Latinoamérica), Asia NOTES) e incluso se creó una sociedad específica (EATS, www.eats.org). El primer White Pa-per definía perfectamente los escollos o puntos sobre los que se debía investigar para poder efectuar cualquier pro-cedimiento tipo NOTES (tabla I), y probablemente una de las lecciones aprendidas más interesantes es que todos estos puntos han sido investigados y existe una respuesta objetiva a cada una de las cuestiones planteadas. Así, es posible acceder a través de estómago, vagina o recto a la cavidad peritoneal, es posible navegar por el interior del abdomen, disecar una vesícula o manipular un asa intestinal, y es posible cerrar la viscerotomia de forma segura, sin que este tipo de abordaje incremente o signifique un mayor riego infeccioso (9). A la vez, también durante estos cinco años ha sido posible, de una forma mayoritariamente ordenada y bajo la supervisión de los comités de investigación hospitalarios en la mayoría de los casos, trasladar estas técnicas al ser humano, aunque con un balance menos satis-factorio, habiéndose practicado unos 2000 casos mediante técnicas NOTES en la clínica humana, una cifra mínima si comparamos con el número de colecistectomías laparoscópicas efectuadas en los primeros meses tras su descrip-ción. Ello es consecuencia, y también es otra lección aprendida, de que NOTES es conceptualmente interesante y factible, pero es excepcionalmente complejo y técnicamente demasiado demandante con el instrumental actualmente disponible. Prueba de ello es que la intervención globalmente mejor aceptada y más frecuentemente realizada ha sido la colecistectomía transvaginal, la técnica que es más sencilla desde el punto de vista de acceso y cierre, y además, en la mayoría de las ocasiones se ha llevado a cabo de forma hibrida ante la imposibilidad de efectuarla de forma NO-TES pura por la falta de plataformas estables e instrumental adecuado que permitan a la vez exponer y disecar de forma eficiente (10-13). El registro voluntario de los casos incluidos en bases de datos auditadas por sociedades y grupos con interés también ha permitido conocer la incidencia de complicaciones, y es destacable la baja incidencia de las mismas, cuando se efectuado de forma controlada y estrictamente supervisado por los comités de investiga-ción de los hospitales.

NOTES: que hemos aprendido?: Eduardo M Targarona Servicio de cirugía Hospital Santpau Universidad Autonoma Barcelona
Página 3
Volumen 1 Numero 8
Un fenómeno digno de destacar, obvia consecuencia de la intuitiva percepción de un mayor riesgo, ha sido la necesi-dad de reevaluar la forma en que se implementa la ‘innovación quirúrgica’ en la práctica clínica. Son bien conocidas las dificultades para llevar a cabo estudios prospectivos y randomizados en cirugía, y por otra parte, la ‘innovación’, entendida como una modificación que potencialmente puede mejorar un procedimiento, es fácilmente llevado a la práctica sin necesidad de una exhausta evaluación previa. La EAES (European Association of Endoscopic Surgery) desarrolló una conferencia de consenso que constituye una lúcida reflexión ante el cambio cada vez más rápido y sin alternativas hacia una cirugía marcadamente tecnológico dependiente (14). Por otra parte, se ha desarrollado el con-cepto IDEAL (15, tabla II) como paradigma del método científico, de forma similar al desarrollo de fármacos, en la evaluación de nuevos procedimientos quirúrgicos. Finalmente, el estudio prospectivo randomizado es la confirmación definitiva de las posibles ventajas de un procedimiento, y en la actualidad existen varios estudios en marcha, que se pueden consultar fácilmente en www.trial.gov, que podrán orientar de forma definitiva en algunos puntos de NOTES.
Al valorar el estado actual de NOTES, en la que probablemente la opinión generalizada es de un enlenteci-miento y/o estancamiento en su avance, es necesario considerar dos puntos, que probablemente se viven de forma diferente, al menos uno de ellos, entre USA y el resto del mundo. Una dificultad universal es el momento de recesión económica y la conciencia de que los avances necesarios desde el punto de vista tecnológico son enormemente cos-tosos y probablemente poco rentables lo que frena a la industria en su inversión. La necesidad de una plataforma es-table, concepto totalmente diferente del endoscopio flexible conlleva un gran esfuerzo tecnológico, cuyo ejemplo ini-cial es Endosamurai (Olympus), Anubiscope (Storz) o Direct drive endoscopic system (DDES; Boston Scientific) y que probablemente no se parecerán en nada a opciones futuras tele manipuladas o bajo control robótico, extensión lógica de esta tecnología. Otro punto de conflicto es la dificultad incrementada en los Estados Unidos en la traslación de las técnicas endoscópicas desarrolladas en el laboratorio a la práctica clínica ante la imposibilidad de su remuneración adecuada al coste tecnológico o su aceptación como procedimiento remunerable por los proveedores sanitarios norte-americanos. Sin embargo, este panorama tan poco definido, ha significado un estímulo para el desarrollo de otros modelos de cirugía mínimamente invasiva que tienen como objetivo la reducción a un mínimo de la agresión quirúrgica. La filo-sofía y la dificultad técnica de NOTES ha estimulado sin duda el concepto del acceso de incisión única transumbilical, opción técnica que intuitivamente se considera más fácilmente adaptable y que en este momento está en plena fase de desarrollo (16). Es fácil prever que durante los próximos meses, el concepto de Reduced Port Surgery, limitando el tamaño y numero de trocares junto a una tecnología mejorada (cámaras intrabdominales con control magnético per-cutáneo o instrumental percutáneo) favorecerá una cirugía mínimamente invasiva todavía menos agresiva (17).
Una duda inicial fue predecir quien efectuaría esta cirugía, y aparecía en el horizonte el cirujano/gastroenterólogo hibrido. Otros opinaban que sería una buena manera de que el cirujano general recuperara o adqui-riera habilidades necesarias en endoscopia flexible, idea sugerente que debería ser implementada en los centros de formación quirúrgica. Parece que NOTES ha interesado básicamente a cirujanos, con escasos endoscopistas que se hayan sumado al proyecto. Otro punto de conflicto es la dificultad incrementada en los Estados Unidos en la trasla-ción de las técnicas endoscópicas desarrolladas en el laboratorio a la práctica clínica ante la imposibilidad de su re-muneración adecuada al coste tecnológico o su aceptación como procedimiento remunerable por los proveedores sanitarios norteamericanos. Sin embargo, este panorama tan poco definido, ha significado un estímulo para el desarrollo de otros modelos de cirugía mínimamente invasiva que tienen como objetivo la reducción a un mínimo de la agresión quirúrgica. La filo-sofía y la dificultad técnica de NOTES ha estimulado sin duda el concepto del acceso de incisión única transumbilical, opción técnica que intuitivamente se considera más fácilmente adaptable y que en este momento está en plena fase de desarrollo (16). Es fácil prever que durante los próximos meses, el concepto de Reduced Port Surgery, limitando el tamaño y numero de trocares junto a una tecnología mejorada (cámaras intrabdominales con control magnético per-cutáneo o instrumental percutáneo) favorecerá una cirugía mínimamente invasiva todavía menos agresiva (17).
Una duda inicial fue predecir quien efectuaría esta cirugía, y aparecía en el horizonte el cirujano/gastroenterólogo hibrido. Otros opinaban que sería una buena manera de que el cirujano general recuperara o adqui-riera habilidades necesarias en endoscopia flexible, idea sugerente que debería ser implementada en los centros de formación quirúrgica. Parece que NOTES ha interesado básicamente a cirujanos, con escasos endoscopistas que se hayan sumado al proyecto.

NOTES: que hemos aprendido?: Eduardo M Targarona Servicio de cirugía Hospital Santpau Universidad Autonoma Barcelona
Página 4
Volumen 1 Numero 8
Otro punto de conflicto es la dificultad incrementada en los Estados Unidos en la traslación de las técnicas endoscópicas desarrolladas en el laboratorio a la práctica clínica ante la imposibilidad de su remuneración adecuada al coste tecnológico o su aceptación como procedimiento remunerable por los proveedores sanitarios norteamerica-nos. Sin embargo, este panorama tan poco definido, ha significado un estímulo para el desarrollo de otros modelos de cirugía mínimamente invasiva que tienen como objetivo la reducción a un mínimo de la agresión quirúrgica. La filo-sofía y la dificultad técnica de NOTES ha estimulado sin duda el concepto del acceso de incisión única transumbilical, opción técnica que intuitivamente se considera más fácilmente adaptable y que en este momento está en plena fase de desarrollo (16). Es fácil prever que durante los próximos meses, el concepto de Reduced Port Surgery, limitando el tamaño y numero de trocares junto a una tecnología mejorada (cámaras intrabdominales con control magnético per-cutáneo o instrumental percutáneo) favorecerá una cirugía mínimamente invasiva todavía menos agresiva (17).
Una duda inicial fue predecir quien efectuaría esta cirugía, y aparecía en el horizonte el cirujano/gastroenterólogo hibrido. Otros opinaban que sería una buena manera de que el cirujano general recuperara o adqui-riera habilidades necesarias en endoscopia flexible, idea sugerente que debería ser implementada en los centros de formación quirúrgica. Parece que NOTES ha interesado básicamente a cirujanos, con escasos endoscopistas que se hayan sumado al proyecto.
Correspondencia: Prof. EM Targarona Servicio de Cirugía Hospital d Santpau Universidad Autónoma de Barcelona Padre Claret, 167 08025 Barcelona [email protected]
Les invitamos a enviar su opinión , comentarios o las críticas al Email :[email protected]

SECCION CASOS CURIOSOS:
SINDROME DE COTARD
Página 5
Volumen 1 Numero 8
La característica más llamativa del síndrome de Cotard es que los pacientes que lo su-
fren tienen la creencia que están muertos , que no tienen nervios, ni sangre ni cerebro ni
otros órganos, creen que se están pudriendo, incluso dicen oler como se pudre su carne.
Se perciben como muertos vivientes o zombies. Otras veces creen ser inmortales aunque
solo sean piel y huesos. Creen ser muertos vivientes. Los aquejados con este síndrome tienen delirio nihilistico o de negación. Comienzan con la negación de la existencia del
exterior y llegan luego a negar su propia existencia. Se aíslan del mundo.
Principales síntomas:
Depresión, Pensamientos suicidas, Creencia que no existe su cuerpo. Es un delirio el
paciente cree estar viviendo algo de forma real cuando solo se da en su imaginación
Creencia que se están quedando sin sangre, Pensamientos negativos, Creencia que ya
están muertos- Con delirios olfativos ellos incluso huelen que se están pudriendo, Creencia que los gusanos están bajo su
piel, Creencia que son inmortales, Creencia que se están descomponiendo, Creencia que no tienen órganos internos. Anal-
gesia o ausencia de dolor, Automutilaciones
PRESENTACION DE CASO:
Paciente mujer Edad 48 años, Estado civil: Lleva viuda desde los 24 años, lugar de residencia: Estados Unidos y Co-
lombia.
Trastornos del estado de ánimo: durante su estancia en los Estados Unidos sufrió episodios depresivos recurrentes, fue
tratada con distintos antidepresivos. Al perder su trabajo presenta síntomas depresivos, insomnio recurrente, incapacidad
para sentir placer, ansiedad, sentimiento de culpa y minusvalía. Después aparecieron las ideas suicidas, hubo varios inten-
tos de suicidio (cortes superficiales en las muñecas). Al parecer al darse cuenta no era capaz de suicidarse aparecieron otros síntomas. Comenta: “El 20 de febrero vi que salía un humo por mi boca, al día siguiente me miré al espejo y mis ojos habían cam-
biado, no tenían vida. Me di cuenta que ese humo que salía por mi boca era mi alma saliendo de mi cuerpo”.
A partir de ese momento, creencia de ser una muerta viviente, se veía como una zombie. comenzó a desarrollar
alucinaciones olfativas, decía su cuerpo se estaba pudriendo y ella lo olía. Sensacion cosquilleo bajo la piel como si l
os gusanos la estuvieran devorando. Al ser consciente de que estaba muerta dejo
de comer, porque decía que “los muertos no comen”, esto provocó un drástico
descenso de peso. Se le realizaron estudios de neuroimagen para detectar si
había algún problema cerebral, pero todos dieron negativos. A ser un caso extraño y no haber muchos casos descritos en en mundo no se sabía
bien que tratamiento ponerle a la paciente. Algo había que hacer, el descenso de peso era preocupante. Se comienza a tratar con distintos medicamentos antipsicóticos
(como Prozac , flouxetina). Pasaron unos meses y aparentemente no había señales de mejora. Se recurrió a una herra-
mienta terapéutica, la terapia electro convulsiva a fin de incrementar el flujo sanguíneo en
su cerebro. Después de 6 sesiones, los delirios comenzaron a controlarse hasta llegar a
desaparecer.

SECCION:
LO QUE NUNCA ME ENSEÑARON LA CIRUGIA ES COMO LA MUSICA
SECCION: CIRUGIA BASADA EN EVIDENCIAS: Efectividad de la Cirugía Laparoscópica para Colecistolitiasis y Coledocolitiasis: Revisión Global de la Evidencia. Dra. Mónica Uribe León
Página 6
Volumen 1 Numero 8
Para participar envienos sus aportes personales que le impactaron al siguiente correo: boletí[email protected]
En los Archivos Adjuntos, podrá leer el articulo completo con el título: 01 CIRUGIA DE EVIDENCIA VIA BILIAR
Les invitamos a enviar su opinión , comentarios o las críticas al Email :[email protected]
Cuando era residente de cirugía uno de los aspectos que privilegiábamos en nuestro aná-
lisis era el factor rapidez. Clasificábamos a nuestros maestros y colegas por su velocidad
quirúrgica. Mientras más rápido terminaba una cirugía asumíamos que era mejor. Algu-
nos justificaban su lentitud en función de mejores resultados. Otros justificaban que la
rapidez era sinónimo de conocimiento y por consiguiente la lentitud era ignorancia. Pasó un buen tiempo para darme cuenta que habían algunos cirujanos que no eran velo-
ces pero que terminaban rápido sus cirugías. Habían otros factores que recién aprendí:
conocimiento de la anatomía, conocimiento de la patología, buena exposición, buena
ayudantía, buena iluminación y otros muchos más.
A todos estos factores los clasifiqué como RITMO.
El buen cirujano tiene que tener ritmo, como el tango.
Dr. José De Vinatea De Cárdenas
El objetivo del presente estudio fue evaluar la evidencia disponible respecto de la efectividad de la cirugía laparoscó-pica en el tratamiento de la colelitiasis y la litiasis de la vía biliar (LVBP). Se realizo una revisión global de la evidencia disponible. Se realizaron búsquedas en las bases de datos MEDLINE, EMBASE y the Cochrane Library (1998-2008). Se incluyeron guías de práctica clínica (GPC), revisiones sistemáticas (RS), ensayos clínicos con asignación aleato-ria (EC) y estudios observacionales. Los datos disponibles y la evidencia generada se clasificaron en base a la propuesta del Centro de Oxford de Medici-na Basada en la Evidencia. Se incluyeron 87 estudios (3 GPC, 12 RS, 23 EC, 13 estudios de cohortes, 3 estudios transversales, 2 estudios de casos y de controles y 31 series de casos). En comparación con la colecistectomía abierta, la colecistectomía laparoscópica (CL) se asocia con menor tiempo operatorio y estancia hospitalaria y mejor calidad de vida (evidencia de alta calidad). El uso de profilaxis antibiótica no parece reducir la tasa de infección en pacientes de bajo riesgo (evidencia de alta calidad). Aunque se han descrito numerosas técnicas para realizar una CL, su eficacia no es aun concluyente (evidencia de baja calidad). La cirugía en dos etapas es la estrategia más adecuada para los pacientes de alto riesgo con LVBP (evidencia de alta calidad). La mortalidad del tratamiento laparoscópico de la LVBP es similar a la de la cirugía abierta; y como su eficacia es similar a la del tratamiento endoscópico (evidencia de alta calidad). Se puede concluir señalando que la evidencia disponible respecto de la efectividad de la cirugía laparoscópica para el tratamiento de la colelitiasis y la LVBP es es-casa y de baja calidad metodológica; y que se requieren estudios de mejor calidad para valorar de forma más apro-piada estas técnicas. Material, C.; Pineda, V.; Tort, M.; Targagona, E.; Villegas, P. R. & Alonso, P. Effectiveness of laparoscopic surgery for gallstones and common bile duct lithiasis: a systematic overview. Int. J. Morphol., 28(3):729-742, 2010.

SECCION: ANALISIS CRITICO: EL ROL DEL ESTADIAJE LAPAROSCÓPICO EN CÁNCERES INTRA-ABDOMINALES
Página 7
Volumen 1 Numero 8
Uno de los aspectos más importantes en oncología es la necesidad de una exacta determinación del estadío de la enfermedad al
momento del diagnóstico. Este paso permite diseñar la estrategia terapéutica y definir el pronóstico del paciente. Antes de los
grandes avances tecnológicos actuales en la mayoría de pacientes, la determinación del estadío de enfermedad se realizaba en el
quirófano durante una laparotomía exploratoria. Por supuesto, este es un método bastante agresivo para hacer un diagnóstico,
pero que sin embargo, aún se sigue empleando pero ahora en cada vez menor número de pacientes.
Los métodos de estadiaje oncológico preoperatorio han mejorado notablemente en sensibilidad, especificidad, valor predictivo
positivo y negativo, y sus niveles de exactitud diagnóstica son cada vez mayores. No cabe duda que la tomografía es el mejor
método actualmente para la determinación del nivel de avance de la enfermedad a nivel local y regional como del compromiso
metastásico a distancia. Sin embargo, es importante aclarar que las tomografías de hace 20 años no son las mismas que las que
vemos ahora. La tomografía espiral multicortes (TEM) (multidetector computed tomography MDCT ) ha permitido alcanzar una
precisión diagnóstica mayor del 90% en la mayoría de cánceres. Por ejemplo, en cáncer de páncreas el porcentaje de la TAC
(tomografía axial computarizada) para definir resecabilidad (estadiaje locorregional) era del 70% y gran parte de estos pacientes
debían ser explorados quirúrgicamente. Actualmente con el TEM la resecabilidad se determina hasta en un 90% de casos con
suma precisión.
En la época de la década del 90 no se contaba aún con esta tecnología por lo que muchos pacientes se perjudicaban al ser someti-
dos a una laparotomía innecesaria, en la que lo único que se hacía era el famoso “open/close”. Con esta cirugía se expone al pa-
ciente a riesgos como complicaciones de la herida operatoria, dolor, estancia hospitalaria de varios días y al riesgo bajo pero exis-
tente de la anestesia general sin mayor beneficio.
La cirugía mínimamente invasiva aparece como una excelente alternativa complementaria para realizar un estadiaje mucho más
preciso detectando principalmente depósitos metastásicos de poca magnitud no detectables por TAC, como pequeños implantes
peritoneales o metástasis hepáticas menores de 10 mm. Además útil en evitar los efectos negativos mencionados de la laparoto-mía innecesaria.
Así la laparoscopía encontró su rol en el estadiaje primordialmente en los cánceres del aparato digestivo los cuales por su ubica-
ción intra-abdominal tienen la proclividad a diseminarse principalmente al peritoneo y al hígado. Por lo tanto, el principal lugar
de metástasis de estas neoplasias es el abdomen. Sin embargo, los patrones de diseminación dependen del comportamiento bioló-
gico de cada cáncer y esto determina la mayor o menor utilidad de la laparoscopía de estadiaje. Por ejemplo, el cáncer gástrico
tiene una gran predilección en sus estadíos avanzados a producir carcinomatosis peritoneal antes que metástasis hepáticas. Lo
contrario ocurre con la mayoría de cánceres colorrectales en los que predomina su propensión a las metástasis hepáticas antes que
las peritoneales. Así mismo, el cáncer de cabeza de páncreas tiene mayor propensión a la invasión locorregional y a las metástasis
hepática, mientras que el cáncer de cola de páncreas tiene una gran tendencia a la carcinomatosis peritoneal desde el momento en
que se hace el diagnóstico. Por ende, la importancia de la laparoscopía variará de acuerdo al cáncer que estemos enfrentando. In-
cluso dependerá del estadío tomográfico que estemos presuponiendo y del tipo histológico obtenido en la biopsia. Por ejemplo, un
carcinoma de células en anillo de sello del estómago o un adenocarcinoma mucinoso pobremente diferenciado del colon con sos-
pecha de compromiso tumoral transmural seguramente será candidato para una laparoscopía preopratoria, a diferencia de un cán-
cer de estómago submucoso menor de 2cm tubular bien diferenciado en el que la chance de metástasis a distancia es mínimo.
En algún momento se planteó que todos los pacientes con cáncer abdominal fueran sometidos a una laparoscopía preoperatoria de
estadiaje, sobretodo para cáncer gástrico y páncreas. Actualmente, por lo dicho anteriormente, este método debe ser selectivo.
Debería aplicarse en forma individualizada sólo a pacientes con riesgo de metástasis peritoneal y/o hepática en los que no se han
detectado éstas en un estudio TEM con cortes de mínimo 5 mm. Puede aplicarse necesariamente también en pacientes que aún
teniendo bajo riesgo de metástasis tengan lesiones dudosas en el estudio TEM.

SECCION: ANALISIS CRITICO: EL ROL DEL ESTADIAJE LAPAROSCÓPICO EN CÁNCERES INTRA-ABDOMINALES
Página 8
Volumen 1 Numero 8
.
Es importante también mencionar que la ultrasonografía laparoscópica (USL) agrega mayor sensibilidad al estadiaje sobretodo
para las metástasis hepáticas. También se viene usando para definir el grado de infiltración local vascular principalmente en
cáncer de páncreas, sin embargo, la ultrasonografía endoscópica ha ganado terreno en esta área desplazando el rol de la USL
para este fin. Así mismo el PET-CT se viene probando como método preoperatorio para la detección de metástasis no detecta-das por el TEM, y estamos a la espera que se defina su exacto rol en el estadiaje de los cánceres abdominales.
En conclusión, el rol de la laparoscopía de estadiaje para los cánceres del aparato digestivo, evoluciona constantemente, y su
utilidad se va reduciendo a un selecto grupo de pacientes debido al avance de la tecnología en radiología, y que seguro en el
futuro tal vez eviten llevar a sala de operaciones incluso para una laparoscopía a pacientes con enfermedad metástasica inope-
rable.
El estudio de Chang y cols (Chang L, Stefanidis D, Richardson WS, Earle DB, Fanelli RD. The role of staging laparoscopy for
intraabdominal cancers: an evidence-based review. Surg Endosc (2009) 23:231-241) es una revisión basada en evidencias al
respecto de este tema. Será de mucha utilidad contrastar la opinión crítica vertida, con las evidencias plasmadas en este artícu-
lo, sin embargo deben tomar en cuenta que la revisión se hizo hasta el 2006 y en estos 5 años han seguido habiendo muchos
cambios.
DR. GUSTAVO REAÑO PAREDES
SERV. CIRUGÍA DE PÁNCREAS, BAZO Y RETROPERITONEO
HOSPITAL NAC. G. ALMENARA I. ESSALUD
Podrá ver el articulo completo en los Archivos Adjuntos con el titulo: 02 ANALISIS CRITICO: THE ROLE OF STAGING LAPAROSCOPY FOR INTRAABDOMINAL CANCERS

rocaudal laparoscópica
por Nesidioblastosis
El otro modo de acceder es
colocar el título del video en el
BUSCADOR DE YOUTUBE
Si Ud. está interesado en com-
partir su video, cuélguelo en
YOUTUBE y envíenos el
LINK a:
Acompañe el título del video,
Estimados lectores, en esta sec-ción podrán ver los videos a tra-
vés de los Archivos Adjuntos.
Encontrará un archivo en Word
donde estarán los links de los
videos colgados en la cuenta de
ALACE en YOUTUBE. Deberá
utilizar las teclas:
CONTROL+CLICK SOBRE EL LINK.
EN ARCHIVOS ADJUNTOS: 03 VIDEO
El título del video de este número
es: Pancreatectomía corpo-
SECCION:
LOS VIDEOS DEL BOLETIN ALACE Dr. Edgar González Valdivia
Página 9
Volumen 1 Numero 8
SECCION:
IRREVERENTE
Si desea colaborar: envií tu artículo a: boletí[email protected]
CONOCE SU HISTORIA: IR A ARCHIVOS ADJUNTOS
TITULO: 04 LA TIA AMPARO

GALERIA FOTOGRAFIAS MEDICAS: Dr. José de Vinatea De Cárdenas
Servicio de Cirugía de Páncreas Bazo y retroperitoneo Hospital Guillermo almenara Irigoyen Essalud Lima Perú
Volumen Numero
SI DESEA COMPARTIR SUS FOTOGRAFIAS, ENVIARLAS AL CORREO:
boletí[email protected]
DEBE INCLUIR TITULO DE LA SERIE, BREVE RESEÑA DEL CASO, NOMBRE DEL AUTOR, NACIONALIDAD
APENDICOCECOSTOMIA POR INCONTINENCIA FECAL
APLICACIONES: DISMOTILIDAD COLÓNICA NEUROGÉNICA con estreñimiento pertinaz. VEJIGA NEUROGÉNICA.
ESPLENECTOMIA MASIVA
PACIENTE CON DIAGNOSTICO DE MIELODISPLASIA, ESPLENECTOMIA LAPAROSCOPICA CON SISTEMA DE MANO ASISTIDA (HALS)

Volumen Numero
GALERIA FOTOGRAFIAS NO MEDICAS
LA MODA NO INCOMODA
SI DESEA COMPARTIR SUS FOTOGRAFIAS, ENVIARLAS AL CORREO:
boletí[email protected]
DEBE INCLUIR TITULO DE LA SERIE, NOMBRE DEL AUTOR Y NACIONALIDAD
Dr Carlos Benavides Zúñiga

Volumen Numero
COMENTARIOS, CASOS, OPINIONES Y CRITICAS
CURSOS Y CONGRESOS
SI DESEA COMPARTIR SUS FOTOGRAFIAS, ENVIARLAS AL CORREO:
boletí[email protected]
DEBE INCLUIR TITULO DE LA SERIE, NOMBRE DEL AUTOR Y NACIONALIDAD
Se invita a participar en el
5 TH INTERNATIONAL HERNIA CONGRESS.
Se celebrará entre el 28 y 31 marzo 2012
Nueva York Estados Unidos
Ver la convocatoria en ARCHIVOS ADJUNTOS: denominado: 07 5| congreso
En PUERTO VALLARTA MEXICO, se desarrollara el XIII WORLD CONGRESS OF ENDOSCOPIC
SURGERY, XXI INTERNATIONAL CONGRESS MEXICAL ASSOCIATION OF ENDOSCOPIC
SURGERY,X LATIN AMERICAN CONGRESS OF ENDOSCOPIC SURGERY en el mes de abril
2012 entre el 24 y 28.
Extendemos la invitación a participar de él. Ver afiche del Congreso en el ARCHIVO ADJUNTO denominado: 05 “XIII CONGRESS……”
En BUENOS AIRES –ARGENTINA se invita a participar en el 82
CONGRESO ARGENTINO DE CIRUGÍA entre los días 14 al 17 de
NOVIEMBRE del 2011
Ver invitación y afiches del congreso en ARCHIVOS ADJUNTOS DE-
NOMINADO: 06—82°CONGRESO ARGENTINO

729
Int. J. Morphol.,28(3):729-742, 2010.
Effectiveness of Laparoscopic Surgery for Gallstones andCommon Bile Duct Lithiasis: a Systematic Overview
Efectividad de la Cirugía Laparoscópica para Colecistolitiasis y Coledocolitiasis:Revisión Global de la Evidencia
*Carlos Manterola; **Viviana Pineda; ***Montserrat Tort;****Eduardo Targarona; *****Román Villegas Portero & ******Pablo Alonso
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopicsurgery for gallstones and and common bile duct lithiasis: a systematic overview. Int. J. Morphol., 28(3):729-742, 2010.
SUMMARY: The aim of the present study was to evaluate the available evidence on the effectiveness of laparoscopic surgeryfor treating gallstones and common bile duct lithiasis (CBDL). A systematic overview was performed. Medline, EMBASE and TheCochrane Library were searched (1998-2008). Systematic reviews (SR), clinical practice guidelines (CPG), randomised clinical trials(RCT) and observational studies were included. Internal validity and overall quality of the evidence were assessed. The available evidencewas classified according to the Oxford Centre for Evidence Based Medicine proposal. 87 studies were included in this review (12 SR, 23RCT, 3 CPG, 13 cohort studies, 3 cross-sectional studies, 2 case and control studies and 31 case series). Compared with opencholecystectomy, laparoscopic cholecystectomy (LC) is associated with shorter operating time, shorter hospital stay and better quality oflife (high quality evidence). The use of antibiotic prophylaxis does not appear to reduce the infection rate in low-risk patients (highquality evidence). Although many techniques have been advocated to perform LC their effectiveness is as yet inconclusive (low-qualityevidence). Two-stage surgery is the most appropriate strategy for high-risk patients with CBDL (high-quality evidence). Mortality issimilar to open surgery, as the effectiveness is similar to that of endoscopic treatment (high-quality evidence). As a conclusion we canstate that the evidence concerning the effectiveness of laparoscopic surgery for gallstones and CBDL is scarce and of low methodologicalquality and that better quality studies are warranted to assess these techniques more adequately.
KEY WORDS: Cholecystolithiasis; Choledocholithiasis; Cholelithiasis; Gallstones; Laparoscopy; Cholecystectomy;Laparoscopic; Technology Assessment; Biomedical.
INTRODUCTION
The use of laparoscopic procedures for treatinghepato-biliary diseases started in the late eighties whenMouret, Doubois and Perissat performed the first laparoscopiccholecystectomies (LC) in-patients with cholecystolithiasis(Perissat, 1989; Litynski, 1999; Vecchio, 2000; Reynolds,2001; Jaffray, 2005). LC quickly became the first-linetreatment for uncomplicated cholecystolithiasis (Weil, 1992),
promoting research on the application of laparoscopicprocedures in various surgical contexts. Many approacheswere quickly developed and the field has undergonerevolutionary changes (Matthews, 1999; Young-Fadok, 2000).Evidence in favour of LC, however, is scarce. Furthermore,the advantages of laparoscopic techniques do not appear tooutweigh those of open approaches yet (Troidl, 1999).
* Full Professor, Hepatobiliary Surgery Unit, Department of Surgery, Faculty of Medicine, Universidad de La Frontera, Temuco, Chile.** Assistant Professor, Mastology Unit, Department of Surgery, Faculty of Medicine, Universidad de La Frontera, Temuco, Chile.*** Iberoamerican Cochrane Centre, Spain. Epidemiology and Public Health Department, Universidad Autónoma de Barcelona, Hospital de Sant Pau,
Barcelona, Spain.**** Full Professor, Department of Surgery, Hospital de Sant Pau, Universitat Autonoma de Barcelona, Barcelona, Spain.***** Andalusian Agency for Health Technology Assessment, Sevilla, Spain.****** Iberoamerican Cochrane Centre, Spain. Epidemiology and Public Health Department, Universidad Autónoma de Barcelona, Hospital de Sant Pau,
Barcelona, Spain. Sources of financial support: Andalusian Agency for Health Technology Assessment and DID-UFRO Project DI09-0060 of the Universidad de La
Frontera Research Direction.

730
The aim of this study was to systematically reviewthe available evidence on the effectiveness of laparoscopicsurgery for treating gallstones and common bile duct lithiasis(CBDL).
MATERIAL AND METHOD
The following databases were searched: CochraneLibrary, Medline and EMBASE. The TRIP Database engineand several international technology assessment agencieswere also searched. All studies evaluating the effectivenessof laparoscopic treatment in patients with cholecystolithiasisor CBDL, published between 1988 and 2007 in English,French or Spanish were considered. Firstly, systematicreviews (SR), clinical practice guidelines (CPG) andrandomised clinical trials (RCTs) were retrieved. The internalvalidity of studies was assessed and synthesised in evidencetables (SIGN, 2004). If this type of design was not availableobservational studies were included. The available evidencewas classified according to the system proposed by theOxford Centre for Evidence Based Medicine (OCEBM,2006) and the overall quality of the evidence for eachintervention was rated as high, moderate or low quality in amodified approach of the GRADE system (Guyatt, 2006).This approach considers not just the study design but otherissues like internal validity, consistency, precision of results,and whether evidence assessment was direct or indirect.
We did not formulate recommendations in this reportbecause these are specific to each setting. Besides the overallquality of the evidence and the balance between risks andbenefits, recommendations need to take into account localfactors, values and preferences, the baseline risk of thepopulation of interest, and costs (Guyatt, 2006).
RESULTS
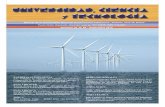
1951 records were retrieved and 87 studies meetingthe selection criteria were finally included (Fig. I).
Effectiveness of laparoscopic cholecystectomy
Laparoscopic versus open cholecystectomy. Four SRs(ANDEM, 1994; Downs, 1996; Korolija, 2004; Keus, 2006a;Keus, 2006b), two RCTs (Mimica, 2000; Ros, 2001), threecohort studies (Devereaux, 2005; Elder, 1996; Finan, 2006),one CPG (Zacks, 2002), one cross-sectional study (Collet,1997) and one case series (Ibrahim, 2006) were included.One SR concluded that laparoscopic techniques take longer
than conventional techniques. LC implied a shorter hospitalstay and greater comfort for the patient compared with opensurgery. However, expertise played a key role in the resultsas both duration and complications were reduced when thetreatment was performed by more experienced surgeons(ANDEM, 1994), (Treatment studies 2a).
Two SR evaluated the effectiveness, safety andpostoperative recovery of LC compared with open andminilaparotomic cholecystectomy no difference wasobserved in postoperative symptomatic relief. The incidenceof postoperative pain, morbidity and mortality were lowerin patients who underwent LC than in those who underwentconventional open surgery. Postoperative ventilatoryfunction was better in LC patients. No differences wereobserved with minilaparotomic cholecystectomy. Thefrequency of biliary complications was higher in LC thanin both conventional and minilaparotomic procedures. Thesurgeons' training and expertise played a significant role interms of surgical morbidity. Length of hospital stay wassimilar for both LC and minilaparotomic cholecystectomybut recovery time was slightly shorter for LC (Downs, 1996;Keus, 2006a). Other SR concluded that there are notdifferences between open and laparoscopic groups in termsof morbilidity, mortality and frequency of biliarycomplications, but hospital stay was lower in laparoscopicgroup (Keus, 2006b), (Treatment studies 1a).
A multicenter RCT comparing LC withminilaparotomic cholecystectomy concluded that LC entailslonger operating time and a slightly shorter hospital stay(Elder, 1996). LC was associated only with shortertemporary disability (12.7 vs. 16.0 days, p<0,001). Of noteis the fact that the study may have been biased by differencesin surgical experience using the two techniques since therewere more experienced surgeons in the LC group (Elder,1996), (Treatment studies 1b). Another RCT examiningrespiratory function in patients that had undergonelaparoscopic or open cholecystectomy showed thatventilatory parameters were similar in both groups, beingon average 40% worse than at baseline (Keus, 2006a),(Treatment studies 2b).
A cohort study that aimed to compare the resultsbetween expert surgeons and surgical trainees found nosignificant differences in either the conversion rate or theoperating time (Elder, 1996). A similar study noted thatmortality risk was lower with LC than with the openprocedure (Zacks, 2002). A population-based studyperformed by the French Society of Endoscopic andOperative Radiology Surgery (SFERO) indicated aconversion rate of 6.9%, a morbidity rate of 4.9% and amortality rate of 0.2% (Collet, 1997), (Treatment studies 4).
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

731
Fig. 1. Flow diagram of studies.
Following a SR of the evidence one clinical practiceguideline (CPG) showed that LC improves quality of lifesooner than open cholecystectomy. Nevertheless, long-termLC results were similar to the open procedure (Korolija,2004), (Treatment studies 1a); and a prospective cohortsupports the utility of LC by showing not only a significantreduction of GI postoperative symptoms but also markedimprovement in patients' general QOL (Finan, 2006).(Treatment studies 2b).
Related with eventual risk factors for conversion toopen surgery in patients undergoing laparoscopiccholecystectomy, a large prospective case series concludedthat male gender, advanced age (over 60 years), higher bodyweight > 65 kg, acute cholecystitis, previous upper abdomi-nal surgery, junior surgeons, and diabetes associated withHba1c > 6. are variables to consider as potential associatedfactor (Ibrahim, 2006), (Treatment studies 4).
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

732
Special groups of patients. Two SR, 3 RCTs, 3 cohortstudies, 1 case-control study and 10 case series were found.The SR concluded that LC resulted in less postoperative pain,shorter hospital stay and fewer complications compared withthe open approach in patients aged 65 or older (Weber, 2003),(Treatment studies 3a). Furthermore, a cohort studyexamining mortality rate for LC versus opencholecystectomy noted that the mortality rate wassignificantly reduced for LC in the subgroup of patients aged70 to 79 (Feldman, 1994). In addition, a retrospective caseseries with patients aged 70 or over who underwent LC notedfound a shorter hospital stay, lower morbidity and mortalityrates, and better postoperative recovery compared with theopen technique (Perez Lara, 2006), (Treatment studies 4).
Assessment of two prospective case series includingpregnant women with symptomatic and complicatedcholecystolithiasis who underwent LC revealed noconversion or morbidity, faster recovery, and nocomplications among the infants. According to the authors,special care should be taken with the trocar position inwomen after their 32nd week of pregnancy, a maximumpneumoperitoneum level of 10 mmHg should be used andthe routine intraoperative cholangiography (RIOC) shouldbe avoided (Sungler, 2000; Daradkeh, 1999), (Treatmentstudies 4).
In patients with cirrhosis and portal hypertensionChild A and B, one RCT found lower blood loss (75.5 vs.112.5 mL, p<0,001), lower morbidity (13,2% vs. 30%, p <0,001) and shorter time to resume eating (18.3 vs. 44.2 hours,p<0,05) in the LC group compared with open surgery (Ji,2005), (Treatment studies 2b). A case control study showedthe conversion and morbidity rate was higher in the cirrhosisgroup than in the control group (Fernandes, 2000),(Treatment studies 3b); and two case series shows similarresults than the previous RCT reported in patients withcirrhosis and portal hypertension Child A and B (Palanivelu,2006; da Silveira, 2006).
A SR based on 5 RCT concluded that earlylaparoscopic cholecystectomy during acute cholecystitis issafe and provide shorter hospital stay (Gurusamy, 2006),(Treatment studies 1a). One RCT on acute cholecystitis (AC)compared safety and cost-effectiveness of urgent versuselective LC (use of percutaneous decompression prior to LC).Elective surgery did not show any advantages in terms ofoperating time, complication rate, blood loss, and conversionrate or hospital stay as compared with urgent LC (Sungler,2000). Another low quality RCT comparing safety and resultsof LC vs. open surgery in patients with gangrenous AC founda similar operating duration and hospital stay but time toreturn to work was longer in the open group (Kiviluoto,
1998), (Treatment studies 2b). A retrospective cohortexamining patients with AC who underwent open andlaparoscopic procedures noted that LC was superior, withlower analgesic use, shorter hospital stay and less temporaldisability (Glavic, 2001). A case series examining patientswith AC, gallbladder gangrene, hydrops and gallbladderempyema observed a conversion rate of 20.5% and amorbidity of 17% (Eldar, 1998). A retrospective case seriesof LC for AC found similar results to those described forcholecystolithiasis, except in operating time and conversionrate which were significantly higher (Lujan, 1995), andanother larger case series described statistical diferences ofconversion rate between patients with AC vs. Chroniccholecystitis (20.6% vs 4.2%) (Tan, 2006), (Treatmentstudies 4).
Several studies on the effectiveness of LC in chronicinflammation conditions, including Mirizzi syndrome, werealso found. One cohort study comparing simple cholelithiasisand complicated cholelithiasis (Mirizzi syndrome andfistulae) groups found similar results in conversion rate andmorbidity, and a longer operating time in the complicatedcholelithiasis group (Perez-Morales, 2005). Case seriesshowed widely variable results, with conversion rates rangingfrom 22.2% to 74% in patients with Mirizzi syndrome(Bagia, 2001; Schafer, 2003). One series reported a morbidityrate of 10.3%44 (Treatment studies 4).
Antibiotic prophylaxis. One SR, 2 RCTs and 1 CPG werefound. One SR that included a meta-analysis concluded thatthe use of antibiotic prophylaxis for LC in low-risk patientsdid not reduce surgical wound infection or remote infectionrates (Al-Ghnaniem, 2006), (Treatment studies 1a). One RCTshowed similar results (Koc, 2003). Another low quality RCTcomparing the use of antibiotic prophylaxis with mechanicalprophylaxis (gallbladder removal with a polyethylene bag)observed a similar postoperative infection rate in both groups(Harling, 2000), (Treatment studies 2b). One CPG, currentlyunder revision, evaluated the requirement of antibioticprophylaxis in different types of surgery; it concluded thatnot only was prophylaxis not proven effective for thispurpose but that its use may potentially increase hospitalantibiotic use with little clinical benefit (SIGN, 2004).
Routine intraoperative cholangiography. Sevenobservational studies were found (one cohort study and 5case series). One cohort study compared routineintraoperative cholangiography (RIOC) with selectivecholangiography (in cases of suspected CBDL or unclearanatomy). RIOC did not improve the identification of hiddencommon bile duct (CBD) or reduce the number of bile ductinjuries, and it lengthened operating time and increasedassociated costs (Ladocsi, 1997), (Diagnostic studies 3b).
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

733
Retrospective case series observed an average time for RIOCof 12±9 minutes, a conversion rate of 6.9%, morbidity rateof 1.2%, and retained CBD of 4% (Millat, 1997); but a largerecently published case series observed 27,2% of abnormalcholangiograms in elective LC and 94.1% of abnormalcholangiograms in patients admitted with biliaryemergencies, concluding that in their experience 10% ofabnormal cholangiograms occurred in patients withoutpreoperative risk factors for bile duct stones (Hamouda,2007), (Diagnostic studies 3b). Another retrospective caseseries evaluated LC without RIOC but including selectivepreoperative endoscopic cholangiography, and observed thatonly 0.5% of all patients had retained stones (Thornton,2002); another one suggest that selective intraoperativecholangiography would miss a proportion of patients withcholedocholithiasis (Tan, 2006). Finally another case seriesrecommended the use of routine laparoscopic ultrasound toreduce the need for intraoperative cholangiography duringcholecystectomy, due to a 95% sensitivity, 100% specificity,100% positive predictive value and 99.4% negativepredictive value (Machi, 2007), (Diagnostic studies 3b).
Laparoscopic cholecystectomy related bile duct injuries.Cystic and hepatic duct lesions are among the most frequentcomplications of laparoscopic cholecystectomy (LC) (Kwon,2001; Regoly-Merei, 1998; Targarona, 1998; Nuzzo, 2005),with values varying from 11.9% to 43% for morbidity and1.7% to 12% for mortality (Regoly-Merei, 1998; Targarona,1998; Sarmiento, 2004; Sicklick, 2005). Their incidence isapproximately 0.31 to 1.34 per 1,000 cases. A survey wasconducted among 1661 American surgeons to investigatethe frequency of major bile duct injuries during LC. With a45% response rate the prevalence of bile duct injuries wasestimated to be around a third of procedures (34.1%). Mostcomplications occurred during the first 50 procedures which,despite the limitations of the report, suggest that most lesionsare associated with inadequate expertise. Nevertheless, atleast a third of those lesions might be associated with otherfactors such as those derived from inappropriate surgicalmaneuvers (Archer, 2001). A similar study with a 58%response rate observed 75.7% of major lesions, with nodifferences between the type of technique used or the use ofRIOC (Nuzzo, 2005), (Treatment studies 4).
Regarding the repair of these lesions, two low qualityRCT suggest that biliary stenting alone is as effective asbiliary stenting with sphincterotomy in the treatment ofuncomplicated post-laparoscopic cholecystectomy bile leaks(Mavrogiannis, 2006; Carr-Locke 2006), (Treatment studies2b). A prospective case series described the results of anumber of major lesions requiring complex reconstructionsuch as hepaticojejunostomy. These lesions required a me-dian of 9 days’ hospital stay, and morbidity and mortality
rates of 42.9% and 1.7% respectively were reported(Sicklick, 2005). One small case series that assessedlaparoscopic repair of minor lesions reported that most ofthese only involved simple sutures associated with theendoscopic drainage (Kwon, 2001), (Treatment studies 4).One retrospective case series applied a quality-of-lifequestionnaire in 59 patients who had undergone surgicalreconstruction after a bile duct lesion during LC and nodifferences between the patient and control groups wereobserved in any of the assessed domains (Sarmiento, 2004).Finally, a case control study comparing costs in a group ofpatients undergoing LC, with bile duct injuries, vs. a groupof patients that had undergone cholecystectomy withoutlesions, did not find any significant differences in costsassociated with bile duct injuries (Woods, 1996), (Treatmentstudies 3b).
Technological variants. Twenty one studies were found.13 RCT, two cohort studies and 6 case series (four of themretrospective and two prospective). Routine intraoperativeaspiration of gallbladder during laparoscopiccholecystectomy seems to be associated to less postoperativemorbidity proportion respect to traditional LC (Calik, 2007).Undertaking LC without pneumoperitoneum is one of themultiple variants described for LC and is supported by twolow quality RCTs (Kitano, 1993; Barczynski, 2004) and alsoby a retrospective case series (Nande, 2002). The reductionin the number of access ports (Trichak, 2003) and the use of'mini-laparoscopy' and 'mini-instruments' is upheld bymedium-quality RCTs and by a prospective case series(Nuzzo, 2005; Novitsky, 2005; Lai, 2003). The use of roboticsystems is supported by a low quality RCT (Zhou, 2006).The use of neodynium YAG laser, which did not show anysignificant benefit over electrosurgery, is backed by two low-quality RCTs (Corbitt, 1991; Bordelon, 1993) and two caseseries (Lane, 1993; Mohiuddin, 2006). Ultrasound dissection,which might imply benefits over conventional electroscalpeldissection, is supported by two medium-quality RCTs(Janssen, 2003; Cengiz, 2005). Gallbladder dissection withbipolar cautery scissors, a variant that was not superior tomonopolar scissors, is supported by a low-quality RCT(Edelman, 1995). In two low-quality RCT assistance with awater irrigation system and a hydrodissection withadrenaline-lidocaine-saline solution, as an alternative todissection, showed clinically modest results (Shekarriz,2003) and no differences respect to traditional dissectionsystem (Caliskan, 2006). The use of various types of ligatureand suture as an alternative to conventional stapling issupported by a retrospective cohort81 and two retrospectivecase series (Yano, 2003; Yeh, 2004). Finally, the use of 0.5%bupivacaine-soaked Surgicel in the gallbladder proved in acohort study, appear to be effective for control visceral painafter laparoscopic cholecystectomy, but port-site infiltration
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

734
alone would be ineffective (Verma, 2006), (Treatment studies2b and 4).
Laparoscopic cholecystectomy as short-stay majorsurgery. In the 90s, LC was regarded as a way to reducehospital stay in patients undergoing cholecystectomy (Verma,2006). However, this potential benefit of LC with earlydischarge versus the standard protocol is supported only byobservational studies with non-conclusive results (Grace,1991; Martinez Vieira, 2004; Lau, 2002; Pattillo, 2004; Bue-no Lledo, 2006), (Treatment studies 4).
Effectiveness of laparoscopic treatment for common bileduct lithiasis.
The ideal treatment for CBDL remains controversial.Options vary from endoscopic papillotomy to laparotomicor laparoscopic choledochotomy, including bile ductexploration via the cystic duct (Paganini, 2007). CBDLtreatment has mainly been undertaken by endoscopy priorto LC. This strategy appears to resolve CBDL in most casesbut is likely to find no evidence of the presence of a stone in20-60% of patients and is associated with a considerablemorbidity risk (Paganini, 2007; Smith, 1997; Joyce, 1991;Prat, 1996; Costi, 2007; Trondsen, 1998).
There are also reports on primary choledochorraphyversus choledochorraphy with a Kehr tube or modifiedbiliary endoprosthesis. It is generally accepted that two-stagesurgery (endoscopic papillotomy followed by LC) is the mostappropriate strategy for high-risk patients, such as those withcholangitis and pancreatitis (Liu, 2001). However, for lowrisk patients, a one-step strategy has progressively beenadopted in clinical practice, this involves LC andlaparoscopic bile duct exploration (transcystic or viacholedochotomy). There is yet no specified algorithm forthe laparoscopic treatment of CBDL (Cuschieri, 1999; Wei,2003), and this uncertainty become evident in the findingsof the 5 available SRs (Martin, 2006; Pichon Riviere, 2005;Tranter, 2002; Vial, 2005; Clayton, 2006).
The Institute for Health and Clinical Effectivenessreport concludes that effectiveness of bile duct laparoscopicexploration is very high (90% in most studies) and similarto that of endoscopic treatment. Endoscopic morbidity isabout 8% and is related to the procedure (pancreatitis,perforation and bleeding). Morbidity of bile ductlaparoscopic exploration includes the risk of incompletestone (5%) or stricture removal (3%), and the need forconversion to open surgery (4%). Disadvantages of thelaparoscopic method include the need for highly trainedsurgeons and specific equipment (Pichon Riviere, 2005),(Treatment studies 1a).
Three SRs comparing endoscopic treatment withsurgical treatment of CBDL (open and laparoscopic) haverecently been published (Martin, 2006; Pichon Riviere, 2005;Tranter, 2002; Vial, 2005). These reviews conclude that bileduct laparotomic exploration is more effective thanendoscopic treatment for bile duct cleaning. Endoscopictreatment requires a higher number of procedures per patientand a longer hospital stay and is at least as safe and effective.Nevertheless, no clear advantages, in terms of lack ofresponse to treatment, morbidity or mortality have beenobserved (Martin, 2006; Pichon Riviere, 2005; Tranter, 2002;Vial, 2005), (Treatment studies 1a).
Another SR comparing endoscopic and surgery vs.surgery alone for CBDL treatment with the gallbladder insitu, verified that there was no significant difference insuccessful duct clearance, mortality, morbidity betweenthe endoscopic and surgical groups. There was also nosignificant difference between the endoscopic andlaparoscopic surgery groups. So authors concluded thatboth approaches have similar outcomes, and treatmentshould be determined by local resources and expertise(Clayton, 2006), (Treatment studies 1a).
On the other hand, a recently published low-qualityRCT compare success rate, length of hospital stay, clinicalresults, and costs of sequential treatment (ERCP followedby LC) vs. the laparoendoscopic rendezvous in patientswith CBDL and verified that laparoendoscopic rendezvoustechnique allows a higher rate of CBDL clearance, shorterhospital stay and cost reduction respect the ERCP followedby LC group (Morino, 2006), (Treatment studies 2b).
Another aspect to consider is bile duct drainagevia choledochotomy plus ulterior choledochorraphy witha Kehr tube. One recent published SR tried to assess thebenefits and harms of routine primary closure versus T-tube drainage following laparoscopic common bile ductstone exploration and concluded that there is insufficientevidence to recommend T-tube drainage or primaryclosure after laparoscopic common bile duct stoneexploration (Gurusamy, 2007), (Treatment studies 1a).Other studies available to date on this subject areobservational [three cohort studies (Griniatsos, 2005;KimK, 2004; Lien, 2005) and two case series (Decker,2003; Fanelli, 2001)] and their results support the use ofbiliary endoprosthesis after bile duct laparoscopicexploration as a safe, quick and effective alternative.Biliary endoprosthesis is a minimally invasive therapythat implies a shorter hospital stay and seems to reducemorbidity after the insertion of a Kehr tube (Griniatsos,2005; KimK, 2004; Lien, 2005; Decker, 2003; Fanelli,2001), (Treatment studies 4).
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

735
DISCUSSION
Following the great technological advances that haveoccurred in recent years laparoscopic treatment is generallyconsidered a quick and safe procedure. A high level oftraining in the procedure is required, however, and thenumber of complications appears to decrease as experienceincreases. In this overview, LC for patients withcholecystolithiasis and acute cholecystitis is associated witha longer operating time, a shorter hospital stay and a better
postoperative quality of life in comparison with open surgery.Although it is a relatively safe procedure, there is a higherrisk of bile duct injuries and complex repair surgery is oftenrequired. (High quality evidence). LC seems a relatively safeprocedure for special groups of patients such as the elderly,pregnant women or patients with cirrhosis and portalhypertension Child A y B (Low quality evidence) (ANDEM,1994; Downs, 1996; Korolija, 2004; Mimica, 2000; Ros,
Clinical question Number of studies Quality of theevidence
Summary of findings
High LC is associated with longer operating time, a shorterhospital stay and a better postoperative course for patientswith cholecystolithiasis.
LC vs. open cholecystectomy. 4 SRs2 RCTs3 Cohort studies1 CPG1 C ross-sectionalstudy1 case series
Low LC can be a safe procedure for special groups of patientssuch as the elderly, pregnant women and patients withcirrhosis and portal hypertension Child A y B.
Moderate LC results in less postoperative pain, shorter hospital stayand fewer complications compared with open approach inpatients aged 65 and older.
Moderate LC is a safe procedure in patients with acutecholecystitis.
LC in special groups ofpatients.
2 SR3 RCTs3 Cohort studies1 C ase controlstudies10 case series Low It has shown to be a safe procedure for special groups of
patients such as the elderly, pregnant women and patientswith cirrhosis and portal hypertension Child A y B.
Use of antibiotic prophylaxisfor LC.
1 SR2 RCTs1 CPG
High Use of antibiotic prophylaxis in low-risk patientsundergoing a LC does not offer any additional benefits interms of reduction of postoperative infection rates.
Use of routine intra operativecholangiography during LC.
1 Cohort studies5 case series
Low There is scarce evidence about the need of RIOC duringLC and results do not support its use.
LC-related bile duct injuries. 1 C ase controlstudies2 C ross-sectionalstudies3 case series
Moderate Higher risk of bile duct injuries mainly associated withexperience, which often requires more complex repairsurgeries.
Technological variants forLC.
13 RCTs2 Cohort studies6 case series
Low Multiple variants for LC have been described; however,there is little evidence for their effectiveness.
LC as short-stay majorsurgery.
1 Cohort studies4 case series
Low No evidence of major complications of outpatient LC.
High Two-stage surgery is the most appropriate strategy forhigh-risk patients.
Effectiveness of laparoscopictreatment for common bileduct lithiasis.
5 SR1 RCT1 CPG3 Cohort studies3 case series
Low One-time laparoscopic treatment has been incorporatedfor low-risk patients. Use of biliary endoprosthesis afterbile duct laparoscopic exploration may be a s afe,effective alternative as compared with the implantation ofa Kehr drainage.
LC: laparoscopic cholecystectomy; SR: systematic reviews; RCT: randomised clinical trial; CPG: clinical practice guideline; RIOC: routine intraoperativecholangiography.High quality: it is very unlikely that future studies change our confidence in the estimate of effect and therefore our confidence is high. Moderate quality:it is likely that future studies change our confidence in the estimate of effect. Low quality: it very likely that future studies change our confidence in theestimate of effect, therefore our confidence is low.
Table I. Evidence Table.
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

736
2001; Elder, 1996; Finan, 2006; Zacks, 2002; Collet, 1997;Ibrahim, 2006; Weber, 2003; Feldman, 1994; Perez Lara,2006; Sungler, 2000; Daradkeh, 1999; Ji, 2005; Fernandes,2000; Palanivelu, 2006; da Silveira, 2006; Gurusamy, 2006;Chandler, 2000; Kiviluoto, 1998; Glavic, 2001; Eldar, 1998;Lujan, 1995; Tan, 2006; Perez-Morales, 2005; Bagia, 2001;Schafer, 2003; Kwon, 2001; Woods, 1996).
Antibiotic prophylaxis in low-risk patientsundergoing LC does not offer any additional benefits interms of reduction of postoperative infection rates (Highquality evidence). There is little available evidence on theneed for routine intraoperative cholangiography during LCand results so far do not support its use (Low qualityevidence). Several variants of LC have been described, butevidence about their effectiveness is scarce (Low qualityevidence). On the other hand, there is no evidence of majorcomplications with outpatient LC (Low quality evidence)(Al-Ghnaniem, 2003; Koc, 2003; Harling, 2000; SIGN,2004; Ladocsi, 1997; Millat, 1997; Thornton, 2002; Kitano,1993; Barczynski, 2004; Nande, 2002; Trichak, 2003;Novitsky, 2005; Lai, 2003; Zhou, 2006; Corbitt, 1991;Bordelon, 1993; Lane GE, 1993; Janssen, 2003; Cengiz,2005; Edelman, 1995; Shekarriz, 2003; Bencini, 2003;Yano, 2003; Verma, 2006; Grace, 1991; Martinez Vieira,2004; Lau, 2002; Pattillo, 2004; Bueno Lledo, 2006).
Regarding laparoscopic treatment for CBDL theavailable evidence suggests that two-stage surgery is themost appropriate strategy for high-risk patients (Highquality evidence). For low-risk patients the one-steplaparoscopic treatment has progressively been incorporatedinto clinical practice. Furthermore, the use of biliaryendoprosthesis after bile duct laparoscopic exploration maybe a safe and effective alternative as compared with theimplantation of a Kehr tube (Low quality evidence) (Smith,1997; Joyce, 1991; Prat, 1996; Costi, 2007; Trondsen, 1998;Liu, 2001; Cuschieri, 1999; Wei, 2003; Gurusamy, 2007;Griniatsos, 2005; KimK, 2004; Lien, 2005; Decker, 2003;Fanelli, 2001).
From the present overview we can conclude thatstudies with a better methodological quality are warrantedto assess the issues reported here. In the LC context, theeffectiveness and safety of laparoscopic therapy versusconventional surgery should be assessed in low-riskpatients. Other issues yet to be clarified are the need or notfor antibiotic prophylaxis in high-risk patients and the cost-effectiveness of LC and its different technological variants.For CBDL, the effectiveness and safety of laparoscopictreatment versus conventional surgery in low-risk patientsshould be established. Finally, the effectiveness and safetyof one-time laparoscopic treatment versus two-stage surgery
in low-risk patients and also the effectiveness ofcholedochorraphy without endoprosthesis should bedetermined (Table I).
Despite the wide implementation of laparoscopicprocedures the available evidence for their effectivenessin the treatment of gallstones and CBDL is scarce and oflow methodological quality. Adequately powered head-to-head studies are warranted in order to clarify these issues.These trials should have a rigorous design with participantsbeing randomised to clinicians who will only undertakethe intervention they are expert in (Howes, 1997).
ACKNOWLEDGEMENTS
This overview was conducted under the direction ofthe Andalusian Agency for Health Technology Assessmentwithin the collaboration framework established in theNational Health System Quality Plan, thanks to theagreement between the Carlos III Institute (Ministry ofHealth) and the Foundation Progress and Health.
We would like to express our gratitude to CarolynNewey for her help reviewing and editing of this overview.
MANTEROLA, C.; PINEDA, V.; TORT, M.;TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P.Efectividad de la cirugía laparoscópica para colecistolitiasisy coledocolitiasis: Revisión global de la evidencia. Int. J.Morphol., 28(3):729-742, 2010.
RESUMEN: El objetivo del presente estudio fue evaluarla evidencia disponible respecto de la efectividad de la cirugíalaparoscópica en el tratamiento de la colelitiasis y la litiasis de lavía biliar (LVBP). Para ello, se realizó una revisión global de laevidencia disponible. Se realizaron búsquedas en las bases de da-tos MEDLINE, EMBASE y The Cochrane Library (1998-2008).Se incluyeron guías de práctica clínica (GPC), revisiones sistemá-ticas (RS), ensayos clínicos con asignación aleatoria (EC) y estu-dios observacionales. Se valoró la validez interna y la calidad glo-bal de los estudios. Los datos disponibles y la evidencia generadase clasificaron en base a la propuesta del Centro de Oxford de Me-dicina Basada en la Evidencia. 87 estudios fueron incluidos en estarevisión (3 GPC, 12 RS, 23 EC, 13 estudios de cohortes, 3 estu-dios transversales, 2 estudios de casos y de controles y 31 series decasos). En comparación con la colecistectomía abierta, lacolecistectomía laparoscópica (CL) se asocia con menor tiempooperatorio y estancia hospitalaria y mejor calidad de vida (eviden-cia de alta calidad). El uso de profilaxis antibiótica no parece redu-cir la tasa de infección en pacientes de bajo riesgo (evidencia dealta calidad). Aunque se han descrito numerosas técnicas para rea-lizar una CL, su eficacia no es aún concluyente (evidencia de baja
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

737
calidad). La cirugía en dos etapas es la estrategia más adecuadapara los pacientes de alto riesgo con LVBP (evidencia de alta cali-dad). La mortalidad del tratamiento laparoscópico de la LVBP essimilar a la de la cirugía abierta; y como su eficacia es similar a ladel tratamiento endoscópico (evidencia de alta calidad). Se puedeconcluir señalando que la evidencia disponible respecto de la efec-tividad de la cirugía laparoscópica para el tratamiento de lacolelitiasis y la LVBP es escasa y de baja calidad metodológica; yque se requieren estudios de mejor calidad para valorar de formamás apropiada estas técnicas.
PALABRAS CLAVE: Colelitiasis; Colecistolitiasis;Coledocolitiasis; Cálculos biliares; Laparoscopia;Colecistectomía laparoscópica; Evaluación de tecnología sani-taria.
REFERENCES
Al-Ghnaniem, R.; Benjamin, I.S. & Patel A.G. Meta-analysissuggests antibiotic prophylaxis is not warranted in low-risk patients undergoing laparoscopic cholecystectomy.Br. J. Surg., 90:365-66, 2003.
A.N.D.E.M. Agence Nationale pour le Développement del’Évaluation Médicale. Evaluation des methodescoelioscopiques en chirurgie digestive, 1994.
Archer, S. B.; Brown, D. W.; Smith, C. D.; Branum, G. D.& Hunter, J. G. Bile duct injury during laparoscopiccholecystectomy: results of anational survey. Ann. Surg.,234:549-58, 2001.
Bagia, J. S.; North, L. & Hunt, D. R. Mirizzi syndrome: anextra hazard for laparoscopic surgery. ANZ J. Surg.,71:394-97, 2001.
Barczynski, M. & Herman, R. M. Low-pressurepneumoperitoneum combined with intraperitoneal salinewashout for reduction of pain after laparoscopiccholecystectomy: A prospective randomized study. Surg.Endosc., 18:1368-73, 2004.
Bencini, L.; Boffi, B.; Farsi, M.; Sanchez, L. J.; Scatizzi;M. & Moretti R. Laparoscopic cholecystectomy:retrospective comparative evaluation of titanium versusabsorbable clips. J. Laparoendosc. Adv. Surg. Tech. A,13:93-8, 2003.
Bordelon, B. M.; Hobday, K. A. & Hunter, J. G. Laser vselectrosurgery in laparoscopic cholecystectomy. Aprospective randomized trial. Arch. Surg., 128:233-6,1993.
Bueno Lledo, J.; Planells Roig, M.; Arnau Bertomeu, C.;Sanahuja Santafe, A.; Oviedo Bravo, M.; Garcia Espi-nosa, R.; Marti Obiol, R. & Espi Salinas, A. Outpatientlaparoscopic cholecystectomy: a new gold standard forcholecystectomy. Rev. Esp. Enferm. Dig., 98:14-24,2006.
Calik, A.; Topaloglu, S.; Topcu, S.; Turkyilmaz, S.;Kucuktulu, U. & Piskin B. Routine intraoperativeaspiration of gallbladder during laparoscopiccholecystectomy. Surg. Endosc., 21:1578-81, 2007.
Caliskan, K.; Nursal, T. Z. & Yildirim, S. Hydrodissectionwith adrenaline-lidocaine-saline solution in laparoscopiccholecystectomy. Langenbecks Arch. Surg., 391:359-63,2006.
Carr-Locke, A. D. 'Biliary stenting alone versus biliarystenting plus sphincterotomy for the treatment of post-laparoscopic cholecystectomy bile leaks'. Eur. J.Gastroenterol. Hepatol., 18:1053-5, 2006.
Cengiz, Y.; Janes, A.; Grehn, A. & Israelsson, L. A.Randomized trial of traditional dissection withelectrocautery versus ultrasonic fundus-first dissectionin patients undergoing laparoscopic cholecystectomy. Br.J. Surg., 92:810-3, 2005.
Chandler, C. F.; Lane, J. S.; Ferguson, P.; Thompson, J. E.& Ashley, S. W. Prospective evaluation of early versusdelayed laparoscopic cholecystectomy for treatment ofacute cholecystitis. Am. Surg., 66:896-900, 2000.
Clayton, E. S.; Connor, S.; Alexakis, N. & Leandros, E. Meta-analysis of endoscopy and surgery versus surgery alonefor common bile duct stones with the gallbladder in situ.Br. J. Surg., 93:1185-91, 2006.
Collet, D. Laparoscopic cholecystectomy in 1994. Resultsof a prospective survey conducted by SFCERO on 4,624cases. Societe Francaise de Chirurgie Endoscopique etRadiologie Operatoire. Surg. Endosc., 11:56-63, 1997.
Corbitt J. D. Jr. Laparoscopic cholecystectomy: laser versuselectrosurgery. Surg. Laparosc. Endosc., 1:85-8, 1991.
Costi, R.; DiMauro, D. & Mazzeo, A. Routine laparoscopiccholecystectomy after endoscopic sphincterotomy forcholedocholithiasis in octogenarians: is it worth the risk?Surg. Endosc., 21:41-7, 2007.
Cuschieri, A.; Lezoche, E.; Morino, M.; Croce, E.; Lacy, A.& Toouli, J. E.A.E.S. multicenter prospective
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

738
randomized trial comparing two-stage vs single-stagemanagement of patients with gallstone disease and ductalcalculi. Surg. Endosc., 13:952-7, 1999.
Daradkeh, S.; Sumrein, I.; Daoud, F.; Zaidin, K. & Abu-Khalaf, M. Management of gallbladder stones duringpregnancy: conservative treatment or laparoscopiccholecystectomy? Hepatogastroenterology, 46:3074-6, 1999.
da Silveira, E. B. Outcome of cirrhotic patients undergoingcholecystectomy: applying Bayesian analysis ingastroenterology. J. Gastroenterol. Hepatol., 21:958-62, 2006.
Decker, G.; Borie, F.; Millat, B.; Berthou, J. C.; Deleuze,A. & Drouard, F. One hundred laparoscopiccholedochotomies with primary closure of thecommon bile duct. Surg. Endosc., 17:12-8, 2003.
Devereaux, P. J.; Bhandari, M.; Clarke, M.; Montori, V.M.; Cook, D. J. & Yusuf, S. Need for expertise-basedrandomised controlled trials. BMJ, 330(7482):88,2005.
Downs, S. H. Systematic review of the effectiveness andsafety of laparoscopic cholecystectomy. Ann. R. Coll.Surg. Engl., 78(3 Part 2):241-323, 1996.
Edelman, D. S. & Unger, S. W. Bipolar versus monopolarcautery scissors for laparoscopic cholecystectomy: arandomized, prospective study. Surg. Laparosc.Endosc., 5:459-62, 1995.
Elder, S.; Kunin, J.; Chouri, H.; Sabo, E.; Matter, I.; Nash,E. & Schein, M. Safety of laparoscopiccholecystectomy on a teaching service: a prospectivetrial. Surg. Laparosc. Endosc., 6:218-20, 1996.
Elder, S.; Sabo, E.; Nash, E.; Abrahamson, J. & Matter, I.Laparoscopic cholecystectomy for the various typesof gallbladder inflammation: a prospective trial. Surg.Laparosc. Endosc., 8:200-7, 1998.
Fanelli, R. D. & Gersin, K. S. Laparoscopic endobiliarystenting: a simplified approach to the management ofoccult common bile duct stones. J. Gastrointest. Surg.,5:74-80, 2001.
Feldman, M. G.; Russell, J. C.; Lynch, J. T. & Mattie, A.Comparison of mortality rates for open and closedcholecystectomy in the elderly: Connecticut statewidesurvey. J. Laparoendosc. Surg., 4:165-72, 1994.
Fernandes, N. F.; Schwesinger, W. H. & Hilsenbeck, S. G.Laparoscopic cholecystectomy and cirrhosis: a case-con-trol study of outcomes. Liver Transpl., 6:340-4, 2000.
Finan, K. R.; Leeth, R. R.; Whitley, B. M.; Klapow, J. C. &Hawn, M. T. Improvement in gastrointestinal symptomsand quality of life after cholecystectomy. Am. J. Surg.,192:196-202, 2006.
Glavic, Z.; Begic, L.; Simlesa, D. & Rukavina, A. Treatmentof acute cholecystitis. A comparison of open vslaparoscopic cholecystectomy. Surg. Endosc., 15:398-401, 2001.
Grace, P. A.; Quereshi, A.; Coleman, J.; Keane, R.; McEntee,G. & Broe, P. Reduced postoperative hospitalization afterlaparoscopic cholecystectomy. Br. J. Surg., 78:160-2,1991.
Griniatsos, J.; Karvounis, E.; Arbuckle, J. & Isla, A. M. Cost-effective method for laparoscopic choledochotomy. ANZJ. Surg., 75:35-8, 2005.
Gurusamy, K. S. & Samraj, K. Early versus delayedlaparoscopic cholecystectomy for acute cholecystitis.Cochrane Database Syst. Rev., (4):CD005440, 2006.
Gurusamy, K. & Samraj, K. Primary closure versus T-tubedrainage after laparoscopic common bile duct stoneexploration. Cochrane Database Syst. Rev.,(1):CD005641, 2007.
Guyatt, G.; Gutterman, D.; Baumann, M. H.; Addrizzo-Harris, D.; Hylek, E. M. & Phillips, B. Grading strengthof recommendations and quality of evidence in clinicalguidelines: report from an american college of chestphysicians task force. Chest, 129:174-81, 2006.
Hamouda, A. H.; Goh, W.; Mahmud, S.; Khan, M. & Nassar,A. H. Intraoperative cholangiography facilitates simpletranscystic clearance of ductal stones in units withoutexpertise for laparoscopic bile duct surgery. Surg.Endosc., 21:955-99, 2007.
Harling, R.; Moorjani, N.; Perry, C.; MacGowan, A. P. &Thompson, M. H. A prospective, randomised trial ofprophylactic antibiotics versus bag extraction in theprophylaxis of wound infection in laparoscopiccholecystectomy. Ann. R. Coll. Surg. Engl., 82:408-10,2000.
Howes, N.; Chagla, L.; Thorpe, M. & McCulloch, P. Surgicalpractice is evidence based. Br. J. Surg., 84:1220-3, 1997.
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

739
Ibrahim, S.; Hean, T. K.; Ho, L. S.; Ravintharan, T.; Chye,T. N. & Chee, C. H. Risk factors for conversion to opensurgery in patients undergoing laparoscopiccholecystectomy. World J. Surg., 30:1698-704, 2006.
Janssen, I. M.; Swank, D. J.; Boonstra, O.; Knipscheer, B.C.; Klinkenbijl, J. H. & van Goor, H. Randomizedclinical trial of ultrasonic versus electrocautery dissectionof the gallbladder in laparoscopic cholecystectomy. Br.J. Surg., 90:799-803, 2003.
Jaffray, B. Minimally invasive surgery. Arch. Dis. Child,90:537-42, 2005.
Ji, W.; Li, L. T.; Wang, Z. M.; Quan, Z. F.; Chen, X. R. & Li,J. S. A randomized controlled trial of laparoscopic ver-sus open cholecystectomy in patients with cirrhotic por-tal hypertension. World J. Gastroenterol., 11:2513-17,2005.
Joyce, W. P.; Keane, R.; Burke, G. J.; Daly, M.; Drumm, J.;Egan, T. J. 6 Delaney, P. V. Identification of bile ductstones in patients undergoing laparoscopiccholecystectomy. Br. J. Surg., 78:1174-6, 1991.
Keus, F.; de Jong, J. A.; Gooszen, H. G. & van Laarhoven,C. J. Laparoscopic versus open cholecystectomy forpatients with symptomatic cholecystolithiasis. CochraneDatabase Syst. Rev., (4):CD006231, 2006.
Keus, F.; de Jong, J. A.; Gooszen, H. G. & van Laarhoven,C. J. Laparoscopic versus small-incisioncholecystectomy for patients with symptomaticcholecystolithiasis. Cochrane Database Syst. Rev.,(4):CD006229, 2006.
Korolija, D.; Sauerland, S.; Wood-Dauphinee, S.; Abbou,C. C.; Eypasch, E. & Caballero, M. G. Evaluation ofquality of life after laparoscopic surgery: evidence-basedguidelines of the European Association for EndoscopicSurgery. Surg. Endosc., 18:879-97, 2004.
Kim, E. K. & Lee, S. K. Laparoscopic treatment ofcholedocholithiasis using modified biliary stents. Surg.Endosc., 18:303-6, 2004.
Kitano, S.; Iso, Y.; Tomikawa, M.; Moriyama, M. &Sugimachi, K. A prospective randomized trial comparingpneumoperitoneum and U-shaped retractor elevation forlaparoscopic cholecystectomy. Surg. Endosc., 7:311-4,1993.
Kiviluoto, T.; Siren, J.; Luukkonen, P. & Kivilaakso, E.
Randomised trial of laparoscopic versus opencholecystectomy for acute and gangrenous cholecystitis.Lancet, 1(9099):321-5, 1998.
Koc, M.; Zulfikaroglu, B.; Kece, C. & Ozalp, N. Aprospective randomized study of prophylactic antibioticsin elective laparoscopic cholecystectomy. Surg. Endosc.,17:1716-8, 2003.
Kwon, A. H.; Inui, H. & Kamiyama, Y. Laparoscopicmanagement of bile duct and bowel injury duringlaparoscopic cholecystectomy. World J. Surg., 25:856-61, 2001.
Ladocsi, L. T.; Benitez, L. D.; Filippone, D. R. & Nance, F.C. Intraoperative cholangiography in laparoscopiccholecystectomy: a review of 734 consecutive cases. Am.Surg., 63:150-6, 1997.
Lai, E. C.; Fok, M. & Chan, A. S. Needlescopiccholecystectomy: prospective study of 150 patients.Hong Kong Med. J., 9:238-42, 2003.
Lane, G. E. & Lathrop, J. C. Comparison of results of KTP/532 laser versus monopolar electrosurgical dissectionin laparoscopic cholecystectomy. J. Laparoendosc. Surg.,3:209-14, 1993.
Lau, H. & Brooks, D. C. Transitions in laparoscopiccholecystectomy: the impact of ambulatory surgery.Surg. Endosc., 16:323-6, 2002.
Lien, H. H.; Huang, C. C.; Huang, C. S.; Shi, M. Y.; Chen,D. F.; Wang, N. Y. & Tai, F. C. Laparoscopic commonbile duct exploration with T-tube choledochotomy forthe management of choledocholithiasis. J.Laparoendosc. Adv. Surg. Tech. A, 15:298-302, 2005.
Litynski, G. S. Profiles in laparoscopy: Mouret, Dubois, andPerissat: the laparoscopic breakthrough in Europe (1987-1988). JSLS, 3:163-7, 1999.
Liu, T. H.; Consorti, E. T.; Kawashima, A.; Tamm, E. P.;Kwong, K. L. & Gill, B. S. Patient evaluation andmanagement with selective use of magnetic resonancecholangiography and endoscopic retrogradecholangiopancreatography before laparoscopiccholecystectomy. Ann. Surg., 234:33-40, 2001.
Lujan, J. A.; Parrilla, P.; Robles, R.; Torralba, J. A.; GarciaAyllon, J.; Liron, R. & Sanchez-Bueno, F. Laparoscopiccholecystectomy in the treatment of acute cholecystitis.J. Am. Coll. Surg., 181:75-7, 1995.
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

740
Machi, J.; Oishi, A. J.; Tajiri, T.; Murayama, K. M.;Furumoto, N. L. & Oishi, R. H. Routine laparoscopicultrasound can significantly reduce the need for selectiveintraoperative cholangiography during cholecystectomy.Surg. Endosc., 21:270-4, 2007.
Martin, D. J.; Vernon, D. R. & Toouli, J. Surgical versusendoscopic treatment of bile duct stones. CochraneDatabase Syst. Rev., (2):CD003327, 2006.
Martinez Vieira, A.; Docobo Durantez, F.; Mena Robles, J.;Duran Ferreras, I.; Vazquez Monchul, J.; Lopez Bernal,F. & Romero Vargas, E.Laparoscopic cholecystectomyin the treatment of biliary lithiasis: outpatient surgery orshort stay unit? Rev. Esp. Enferm. Dig., 96:452-5, 456-9, 2004.
Mavrogiannis, C.; Liatsos, C.; Papanikolaou, I. S.;Karagiannis, S.; Galanis, P. & Romanos, A. Biliarystenting alone versus biliary stenting plus sphincterotomyfor the treatment of post-laparoscopic cholecystectomybiliary leaks: a prospective randomized study. Eur. J.Gastroenterol. Hepatol., 18:405-9, 2006.
Matthews, J. B. Minimally invasive surgery: how goes therevolution? Gastroenterology, 116:513, 1999.
Millat, B.; Deleuze, A.; de Saxce, B.; de Seguin, C. &Fingerhut, A. Routine intraoperative cholangiographyis feasible and efficient during laparoscopiccholecystectomy. Hepatogastroenterology, 44:22-7,1997.
Mimica, Z.; Biocic, M.; Bacic, A.; Banovic, I.; Tocilj, J. &Radonic, V. Laparoscopic and laparotomiccholecystectomy: a randomized trial comparingpostoperative respiratory function. Respiration,67:153-8, 2000.
Mohiuddin, K.; Nizami, S.; Fitzgibbons, R. J. Jr; Watson,P.; Memon B. & Memon, M. A. Predicting iatrogenicgall bladder perforation during laparoscopiccholecystectomy: a multivariate logistic regressionanalysis of risk factors. ANZ J. Surg., 76:130-2, 2006.
Morino, M.; Baracchi, F.; Miglietta, C.; Furlan, N.; Ragona,R. & Garbarini, A. Preoperative endoscopicsphincterotomy versus laparoendoscopic rendezvousin patients with gallbladder and bile duct stones. Ann.Surg., 244:889-93, 2006.
Nande, A. G.; Shrikhande, S. V.; Rathod, V.; Adyanthaya,K. & Shrikhande, V. N. Modified technique of gasless
laparoscopic cholecystectomy in a developing country:a 5-year experience. Dig. Surg., 19:366-71, 2002.
Novitsky, Y. W.; Kercher, K. W. & Czerniach, D.Advantages of mini-laparoscopic vs conventionallaparoscopic cholecystectomy: results of a prospectiverandomized trial. Arch. Surg., 140:1178-83, 2005.
Nuzzo, G.; Giuliante, F. & Giovannini, I. Bile duct injuryduring laparoscopic cholecystectomy: results of anItalian national survey on 56 591 cholecystectomies.Arch. Surg., 140:986-992, 2005.
O.C.E.B.M. Centre for Evidence-Based Medicine.Available from: http://cebm.jr2.ox.ac.uk access on 6June 2006.
Paganini, A. M.; Guerrieri, M. & Sarnari, J. Thirteen years'experience with laparoscopic transcystic common bileduct exploration for stones. Effectiveness and long-term results. Surg. Endosc., 21:34-40, 2007.
Palanivelu, C.; Rajan, P. S. & Jani, K. Laparoscopiccholecystectomy in cirrhotic patients: the role ofsubtotal cholecystectomy and its variants. J. Am. Coll.Surg., 203:145-51, 2006.
Pattillo, J. C.; Kusanovic, R.; Salas, P.; Reyes, J.; Garcia-Huidobro, I. & Sanhueza, M. Outpatient laparoscopiccholecystectomy. Experience in 357 patients. Rev. Med.Chil., 132:429-36, 2004.
Perez Lara, F. J.; de Luna Diaz, R.; Moreno Ruiz, J.;Suescun Garcia, R.; del Rey Moreno, A.; HernandezCarmona, J. & Oliva Munoz, H. Laparoscopiccholecystectomy in patients over 70 years of age: reviewof 176 cases. Rev. Esp. Enferm. Dig., 98:42-8, 2006.
Perez-Morales, A.; Roesch-Dietlen, F.; Diaz-Blanco, F. &Martinez-Fernandez, S. Safety of laparoscopiccholecystectomy in complicated vesicular disease. Cir.Cir., 73:15-8, 2005.
Perissat, J.; Collet, D. R. & Belliard, R. Gallstones:laparoscopic treatment, intracorporeal lithotripsyfollowed by cholecystostomy or cholecystectomy--apersonal technique. Endoscopy, 21(1):373-4, 1989.
Pichon Riviere, A.; Augustovski, F.; Bardach, A.; GarciaMarti, S.; Lopez, A. & Glujovsky, D. Laparoscopyusefulness in the management of biliary tract stones.Buenos Aires, Institute for Clinical Effectiveness andHealth Policy (IECS), 2005.
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

741
Prat, F.; Amouyal, G.; Amouyal, P.; Pelletier, G.; Fritsch, J.& Choury, A. D. Prospective controlled study ofendoscopic ultrasonography and endoscopic retrogradecholangiography in patients with suspected common bileduct lithiasis. Lancet, 347:75-9, 1996.
Regoly-Merei, J.; Ihasz, M.; Szeberin, Z.; Sandor, J. & Mate,M. Biliary tract complications in laparoscopiccholecystectomy. A multicenter study of 148 biliary tractinjuries in 26, 440 operations. Surg. Endosc., 12:294-300,1998.
Reynolds, W. Jr. The first laparoscopic cholecystectomy. JSLS,5:89-94, 2001.
Ros, A.; Gustafsson, L.; Krook, H.; Nordgren, C.E.; Thorell,A.; Wallin, G. & Nilsson, E. Laparoscopiccholecystectomy versus mini-laparotomycholecystectomy: a prospective, randomized, single-blindstudy. Ann. Surg., 234:741-9, 2001.
Sarmiento, J. M.; Farnell, M. B.; Nagorney, D. M.; Hodge,D. O. & Harrington, J. R. Quality-of-life assessment ofsurgical reconstruction after laparoscopiccholecystectomy-induced bile duct injuries: what happensat 5 years and beyond? Arch. Surg., 139:483-8, 2004.
Schafer, M.; Schneiter, R. & Krahenbuhl, L. Incidence andmanagement of Mirizzi syndrome during laparoscopiccholecystectomy. Surg. Endosc., 17:1186-90, 2003.
Shekarriz, H.; Shekarriz, B. & Kujath, P. Hydro-Jet-assistedlaparoscopic cholecystectomy: a prospective randomizedclinical study. Surgery, 133:635-40, 2003.
Sicklick, J. K.; Camp, M. S.; Lillemoe, K. D.; Melton, G. B.;Yeo, C. J.; Campbell, K. A; Talamini, M. A.; Pitt H. A.;Coleman, J.; Sauter, P. A.& Cameron, J. L. Surgicalmanagement of bile duct injuries sustained duringlaparoscopic cholecystectomy: perioperative results in200 patients. Ann. Surg., 241:786-92, 2005.
S.I.G.N. Scottish Intercollegiate Guidelines Network. SIGN50: a guidelines developers’ handbook. Edinburgh, SIGN,2004.
Smith, M. 2nd; Wheeler, W. & Ulmer, M. B. Comparison ofoutpatient laparoscopic cholecystectomy in a privatenonteaching hospital versus a private teaching communityhospital. JSLS, 1:51-3, 1997.
Sungler, P.; Heinerman, P. M. & Steiner, H. Laparoscopiccholecystectomy and interventional endoscopy for
gallstone complications during pregnancy. Surg.Endosc., 14:267-71, 2000.
Tan, J. T.; Suyapto, D. R.; Neo, E. L. & Leong, P. S.Prospective audit of laparoscopic cholecystectomyexperience at a secondary referral centre in South Aus-tralia. ANZ J. Surg., 76:335-8, 2006.
Targarona, E. M.; Marco, C.; Balague, C.; Rodriguez, J.;Cugat; E.; Hoyuela, C.; Veloso, E. & Trias, M. How,when, and why bile duct injury occurs. A comparisonbetween open and laparoscopic cholecystectomy. Surg.Endosc., 12:322-6, 1998.
Thornton, D. J.; Robertson, A. & Alexander, D. J.Laparoscopic cholecystectomy without routine operativecholangiography does not result in significant problemsrelated to retained stones. Surg. Endosc., 16:592-5, 2002.
Tranter, S. E. & Thompson, M. H. Comparison of endoscopicsphincterotomy and laparoscopic exploration of thecommon bile duct. Br. J. Surg., 89:1495-504, 2002.
Trichak, S. Three-port vs standard four-port laparoscopiccholecystectomy. Surg. Endosc., 17:1434-6, 2003.
Troidl, H. Disasters of endoscopic surgery and how to avoidthem: error analysis. World J. Surg., 23:846-55, 1999.
Trondsen, E.; Edwin, B.; Reiertsen, O.; Faerden, A. E.;Fagertun, H. & Rosseland, A. R. Prediction of commonbile duct stones prior to cholecystectomy. Arch. Surg.,133:162-6, 1998.
Vecchio, R.; MacFayden, B. V. & Palazzo, F. History oflaparoscopic surgery. Panminerva Med., 42:87-90, 2000.
Verma, G. R.; Lyngdoh, T. S.; Kaman, L. & Bala, I.Placement of 0.5% bupivacaine-soaked Surgicel in thegallbladder bed is effective for pain after laparoscopiccholecystectomy. Surg. Endosc., 20:1560-4, 2006.
Vial, M.; Manterola, C.; Pineda, V. & Losada, H.Coledocolitiasis. Elección de una terapia basada en laevidencia. Revisión sistemática de la literatura. Rev. Chil.Cir., 57:404-11, 2005.
Weber, D. M. Laparoscopic surgery: an excellent approachin elderly patients. Arch. Surg., 138:1083-8, 2003.
Wei, Q.; Wang, J. G.; Li, L. B. & Li, J. D. Management ofcholedocholithiasis: comparison between laparoscopiccommon bile duct exploration and intraoperative
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

742
endoscopic sphincterotomy. World J. Gastroenterol.,9:2856-8, 2003.
Weil, B. Cholelithiasis: therapeutic strategy. Report froman European concensus conference. Gastroenterol. Clin.Biol., 16:251-4, 1992.
Woods, M. S. Estimated costs of biliary tract complicationsin laparoscopic cholecystectomy based upon Medicarecost/charge ratios. A case-control study. Surg. Endosc.,10:1004-7, 1996.
Yano, H.; Okada, K.; Kinuta, M.; Nakano, Y.; Tono, T.;Matsui, S.; Iwazawa, T.; Kanoh, T. & Monden, T.Efficacy of absorbable clips compared with metal clipsfor cystic duct ligation in laparoscopic cholecystectomy.Surg. Today, 33:18-23, 2003.
Yeh, C. N.; Jan, Y. Y.; Liu, N. J.; Yeh, T. S. & Chen, M. F.Endo-GIA for ligation of dilated cystic duct duringlaparoscopic cholecystectomy: an alternative, novel, andeasy method. J. Laparoendosc. Adv. Surg. Tech. A,14:153-7, 2004.
Young-Fadok, T. M.; Smith, C. D. & Sarr, M. G.Laparoscopic minimal-access surgery: where are wenow? Where are we going? Gastroenterology, 118:S148-65, 2000.
Zacks, S. L.; Sandler, S. R.; Rutledge, R. & Brown, S. R. Jr.A population-based cohort study comparing laparoscopiccholecystectomy and open cholecystectomy. Am. J.Gastroenterol., 97:334-40, 2002.
Zhou, H. X.; Guo, Y. H.; Yu, X. F.; Bao, S. Y.; Liu, J. L.;Zhang, Y. & Ren, Y. G. Zeus robot-assisted laparoscopiccholecystectomy in comparison with conventionallaparoscopic cholecystectomy. Hepatobiliary Pancreat.Dis. Int., 5:115-8, 2006.
Correspondence to:
Dr. Carlos Manterola
Department of Surgery
Universidad de La Frontera.
Casilla 54-D, Temuco
CHILE
Phone: 56-45-325760
Fax: 56-45-325761
Email: [email protected]
Received: 19-03-2010
Accepted: 25-05-2010
MANTEROLA, C.; PINEDA, V.; TORT, M.; TARGARONA, E.; VILLEGAS, P. R. & ALONSO, P. Effectiveness of laparoscopic surgery for gallstones and and common bile duct lithiasis: asystematic overview. Int. J. Morphol., 28(3):729-742, 2010.

REVIEW
The role of staging laparoscopy for intraabdominal cancers:an evidence-based review
L. Chang Æ D. Stefanidis Æ W. S. Richardson ÆD. B. Earle Æ R. D. Fanelli
Received: 6 May 2008 / Accepted: 8 July 2008 / Published online: 24 September 2008
� Springer Science+Business Media, LLC 2008
Abstract Diagnostic laparoscopy is minimally invasive
surgery for the diagnosis of intraabdominal diseases. The
aim of this review is a critical examination of the available
literature on the role of laparoscopy for the staging of
intraabdominal cancers. A systematic literature search of
English-language articles on MEDLINE, the Cochrane
database of evidence-based reviews, and the Database of
Abstracts of Reviews of Effects was performed for the
period 1995–2006. The level of evidence in the identified
articles was graded. The search identified and reviewed
seven main categories that have received attention in the
literature: esophageal cancer, gastric cancer, pancreatic
cancer, hepatocellular carcinoma, biliary tract cancer,
colorectal cancer, and lymphoma. The indications, con-
traindications, risks, benefits, diagnostic accuracy of the
procedure, and its associated morbidity are discussed. The
limitations of the available literature are highlighted, and
evidence-based recommendations for the use of laparos-
copy to stage intraabdominal cancers are provided.
Keywords Diagnostic laparoscopy �Intraabdominal cancer � Staging laparoscopy
Diagnostic laparoscopy is minimally invasive surgery for
the diagnosis of intraabdominal diseases. The procedure
enables direct inspection of large surface areas of intraab-
dominal organs; facilitates obtaining biopsy specimens,
cultures and aspirates; allows the use of laparoscopic
ultrasound; and makes therapeutic intervention possible.
Diagnostic laparoscopy has been applied to many clin-
ical situations with variable success. Its application for the
staging of intraabdominal cancers is known as staging
laparoscopy (SL). This article aims to review and grade the
available evidence (Table 1) on the role of SL for a variety
of intraabdominal cancers.
To achieve our objective, a systematic literature search
of English-language articles on MEDLINE, the Cochrane
database of evidence-based reviews, and the Database of
Abstracts of Reviews of Effects (DARE) was performed
for the period 1995–2006. A detailed description of this
method has been published previously [1]. This review
addresses seven main categories identified and reviewed in
the literature: esophageal cancer, gastric cancer, pancreatic
cancer, hepatocellular carcinoma, biliary tract cancer,
colorectal cancer, and lymphoma.
Staging laparoscopy for esophageal cancer
Patients with esophageal cancer often present with an
advanced stage with lymph-node or even distant
L. Chang (&)
Department of General Surgery, Virginia Mason Medical Center,
1100 Ninth Avenue, Seattle, WA 98101, USA
e-mail: [email protected]; [email protected]
D. Stefanidis
Department of General Surgery, Carolinas Medical Center,
Charlotte, NC, USA
W. S. Richardson
Department of Surgery, Ochsner Clinic, New Orleans, LA, USA
D. B. Earle
Department of Surgery, Baystate Medical Center, Springfield,
MA, USA
R. D. Fanelli
Department of Surgery, Surgical Specialists of Western New
England, PC and Berkshire Medical Center, Pittsfield, MA,
USA
123
Surg Endosc (2009) 23:231–241
DOI 10.1007/s00464-008-0099-2

metastases. For this reason, the overall prognosis for
patients with esophageal cancer is poor.
Patients with advanced cancer commonly undergo pre-
operative chemotherapy and radiation in an attempt to
improve survival. Thus, the value of precise staging is
important to separate patients with an early-stage tumor
who are candidates for immediate curative resection from
those who need neoadjuvant therapy. The most common
radiologic tests used to confirm the stage of the tumor are
computed tomography (CT) scan, endoscopic ultrasound,
and positron emission tomography (PET) scan. Staging
laparoscopy may aid in more accurate staging of esopha-
geal cancers to guide the most appropriate treatment and
avoid nontherapeutic laparotomy.
Staging laparoscopy is most commonly performed with
the patient under general anesthesia in supine position.
After pneumoperitoneum has been safely established, an
angled laparoscope placed through an umbilical port site is
recommended for optimal visualization. Additional ports in
the left upper quadrant and epigastric area can be placed as
needed for tissue manipulation.
Full inspection of the peritoneal cavity is performed to
evaluate for peritoneal or liver metastases. If no distant
disease is discovered initially, then the left lateral lobe of
the liver is elevated to expose the gastroesophageal junc-
tion with the patient placed in steep reverse Trendelenburg
position. The tumor is inspected for extension into the
surrounding area. Biopsies can be performed for lymph
nodes in the gastrohepatic ligament or celiac axis suspected
to be malignant. An optional laparoscopic feeding jeju-
nostomy may be placed if neoadjuvant therapy is planned.
In addition, combined thoracoscopic/laparoscopic stag-
ing has been described to improve staging for esophageal
cancer by increasing the number of positive lymph nodes
identified compared with conventional staging [2]. Spe-
cifically for the thoracoscopic evaluation, the patient is in
full, left lateral decubitus position with single-lung venti-
lation. Two to three thoracic trocars are placed, and the
mediastinal pleura overlying the esophagus is incised to
identify lymph nodes and to perform biopsies for them as
needed.
Staging laparoscopy should be used for patients with
esophageal cancer who are potential candidates for curative
surgical resection based on preoperative staging showing
no evidence of lymph node or distant metastases. Fur-
thermore, the procedure can be used to place enteral
feeding access for patients who are candidates for neoad-
juvant therapy, particularly if percutaneous endoscopic
gastrostomy is not feasible. In contrast, SL is contraindi-
cated for patients with known metastatic disease. In
addition, dense intraabdominal adhesions from prior sur-
gery, particularly in the upper abdomen, may preclude
successful laparoscopy.
Because patients with distant or lymph node metastasis
are best treated with chemotherapy and radiation as neo-
adjuvant therapy or even palliation, SL can potentially
decrease the time to this adjuvant treatment. The average
length of hospital stay after SL typically is only 1–3 days,
which compares favorably with that for open exploration.
Subsequently, this faster postoperative recovery may lead
to a shortened interval to the appropriate therapy. However,
this assumed benefit of earlier adjuvant therapy for patients
with metastatic disease has not been measured specifically
in the literature.
Complications after SL for esophageal cancer are low,
and no mortality has been reported. Potential complications
include bleeding, infection, esophageal injury during
inspection, and the general risks associated with anesthesia.
One report documented perforation at the feeding jeju-
nostomy tube site as well as pulmonary edema due to
unexpected aortic valve stenosis [3]. False-negative diag-
nostic laparoscopy can potentially lead to unnecessary
laparotomy. No adverse oncologic effects of SL for
esophageal cancer have been reported.
When all preoperative imaging indicates no metastatic
disease, SL with or without laparoscopic ultrasound has a
sensitivity of 71% for finding peritoneal metastases, 78%
for finding nodal metastases, and 86% for finding liver
metastases (level 2 evidence) [4]. This compares with
respective ultrasound sensitivities of 14, 11, and 86% and
CT scan sensitivities of 14, 55, and 71% (level 2 evidence)
[4]. The accuracy is reported to be 75–80% (level 3 evi-
dence) [3]. However, several reports indicate that only
0.08–10% of patients actually had a change in their man-
agement based on the results of laparoscopy (levels 2 and 3
evidence) [4, 5].
In the hands of a skilled thoracic surgeon, combined
thoracoscopic and laparoscopic staging can be performed
more than 70% of the time [2]. Compared with final
pathologic staging, thoracoscopic and laparoscopic staging
has a sensitivity of 64%, a specificity of 60%, and an
accuracy of 60% (level 2 evidence) [6].
The available literature has limitations with regard to SL
for esophageal cancer, and no level 1 evidence exists. A
small number of reports have been published by highly
specialized centers, which may make the reproducibility of
their results difficult. In addition, studies differ in their
Table 1 Levels of evidence
Level 1 Evidence from properly conducted randomized,
controlled trials
Level 2 Evidence from controlled trials without randomization
Cohort or case-control studies
Multiple time series dramatic uncontrolled experiments
Level 3 Descriptive case series, opinions of expert panels
232 Surg Endosc (2009) 23:231–241
123

technique and intended hypotheses. The impact of the
surgeon’s expertise on the diagnostic accuracy of the pro-
cedure is unknown. Thus, the overall analysis of SL for
esophageal cancer is difficult given the inconsistency of the
reported data.
Summary of SL for esophageal cancer
Based upon our review of the literature, diagnostic lapa-
roscopy for staging can be performed safely for patients
with esophageal cancer. Patients considered to be candi-
dates for curative resection (with early-stage esophageal
cancer and no evidence for distant or lymph node metas-
tases on high-quality preoperative imaging) may benefit
from SL. Laparoscopy also provides the opportunity for
enteral feeding tube placement without the need for lapa-
rotomy. The procedure also may facilitate a shorter time to
adjuvant therapy initiation than laparotomy, but data are
limited, and additional research is needed to elucidate the
true value of diagnostic laparoscopy in this setting.
Staging laparoscopy for gastric cancer
Because many patients with gastric cancer present with
locally advanced or metastatic disease, accurate staging of
gastric cancer aids in the appropriate treatment selection
for both cure and palliation. Palliative resection may be
indicated for gastric cancer causing obstruction, hemor-
rhage, or perforation. However, surgical resection alone for
patients with advanced disease has not been shown to
improve survival.
Studies investigating neoadjuvant protocols for locally
advanced gastric cancers are ongoing, which makes accu-
rate staging imperative. Moreover, even after many
preoperative radiologic tests (CT scan, endoscopic and
transabdominal ultrasound, and PET scan) for staging of
gastric tumors, a proportion of patients are found at
exploration to have unsuspected, unresectable disease.
Thus, SL may aid in more accurate staging of gastric
cancers and guide appropriate treatment without the mor-
bidity associated with exploratory laparotomy.
The SL procedure is most commonly performed with the
patient under general anesthesia in the supine position.
After safe establishment of pneumoperitoneum, an angled
laparoscope typically is inserted through an umbilical port
site. If present, ascites can be aspirated and sent for
cytology. In the absence of ascites, 200 ml of normal saline
can be instilled into the peritoneal cavity and aspirated
from the pelvis and bilateral subdiaphragmatic spaces for
cytologic examination [7]. Full inspection of the peritoneal
cavity is performed to evaluate for peritoneal or liver
metastases. Laparoscopic ultrasound may aid in the
detection of deep hepatic lesions.
If no metastatic disease is discovered, then the left lat-
eral lobe of the liver is elevated to expose the entire
stomach. The perigastric nodes along the greater and lesser
curvature are inspected, and biopsies are performed if
necessary. In addition, the porta hepatis and gastrohepatic
ligaments are inspected carefully. Next, the gastric tumor
itself is inspected for extraserosal invasion and infiltration
into surrounding structures. If the tumor is posterior, then
the lesser sac must be accessed to gain appropriate
visualization.
Staging laparoscopy is indicated for patients who have
T3 or T4 gastric cancer without evidence of lymph node or
distant metastases on high-quality preoperative imaging.
Accurate preoperative staging determines the most appro-
priate therapy for gastric cancer. Staging laparoscopy can
identify patients with locally advanced disease and
metastasis that may be treated best with neoadjuvant or
palliative chemotherapy rather than surgical resection.
These patients may potentially be spared the risks and
complications of a nontherapeutic laparotomy and may
have a shorter convalescence period with an earlier start of
chemotherapy.
Staging laparoscopy should not be undertaken for
patients with gastric cancer complicated by obstruction,
hemorrhage, or perforation in need of palliative surgery. In
addition, patients with early-stage gastric cancer (T1 or T2)
should proceed directly to surgical resection without SL.
Complications of SL with gastric cancer tend to be rare
and include bleeding, infection, and visceral injury. No
mortality has been reported. Although no direct compari-
sons have been made between SL and exploratory
laparotomy for gastric cancer staging, the average length of
hospital stay after SL is reported to be 1 to 2 days, which
compares favorably with stays after exploratory laparot-
omy for other indications [8, 9]. No adverse oncologic
effects of SL for gastric cancer have been reported.
Staging laparoscopy can identify unsuspected metastatic
disease in 13% to 57% of patients despite negative pre-
operative imaging studies (levels 2 and 3 evidence) [7, 10–
14]. Accuracy is reported to range from 89% to 100% in
different series (levels 2 and 3 evidence) [7, 11–15]. In
addition, exploratory laparotomy has been avoided in 17–
40% of cases (levels 2 and 3 evidence) [7, 8, 13–15]. The
SL procedure is more sensitive (96%) for detecting hepatic
metastasis than either CT (52%) or ultrasound (37%) (level
3 evidence) [15]. Similarly, SL sensitivity also is better for
detecting peritoneal metastasis (laparoscopy, 69%; ultra-
sound, 23%; CT, 8%) (level 3 evidence) [15].
The additional value of laparoscopic ultrasound has not
yet been determined. Peritoneal washings positive for
cancer cells have been demonstrated to correlate with the
extent of disease (T1/T2, 0%; T3/T4, 10%; and M?, 59%)
(level 3 evidence) [16].
Surg Endosc (2009) 23:231–241 233
123

The quality of the available literature on SL for gastric
cancer is limited because no level 1 evidence exists. In
addition, studies differ in their technique and use of lapa-
roscopic ultrasound and peritoneal washings. Many reports
do not clearly state preoperative imaging or postoperative
pathology. The impact of the surgeon’s expertise on the
diagnostic accuracy of the procedure also is unknown. The
reported data are not consistent across studies, making their
analysis difficult.
Summary of SL for gastric cancer
Based on our review of the literature, SL can be performed
safely for patients with gastric cancer. The procedure
should be considered for patients with T3 or T4 tumors
who are thought to have localized or locally advanced
disease according to high-quality preoperative imaging. In
contrast, the procedure has a very low yield for patients
with early-stage disease (T1 or T2) and therefore is not
necessary for this patient population.
Staging laparoscopy for pancreatic cancer
Pancreatic cancer has a dismal overall 5-year survival rate
(\5%), and most patients have inoperable disease at
diagnosis. Even after aggressive preoperative imaging,
many patients are found to have unresectable disease dur-
ing laparotomy. Staging laparoscopy may benefit patients
with pancreatic adenocarcinoma by sparing those with
imaging-occult incurable disease the morbidity, inconve-
nience, and expense of a nontherapeutic operation. In
addition, it may lead to better selection of palliative
treatments for patients with locally advanced disease.
The procedure is performed with the patient under
general anesthesia using initial access near the umbilicus.
Additional ports are placed as necessary to complete a
thorough evaluation of peritoneal surfaces including the
suprahepatic and infrahepatic spaces, surface of the bowel,
lesser sac, root of the transverse mesocolon and small
bowel mesentery, ligament of Treitz, paracolic gutters, and
pelvis. Often, frequent bed position changes are necessary
for full visualization of the aforementioned areas.
In addition to visual inspection, peritoneal washings can
be performed, ascitic fluid can be sent for cytology, and
biopsies of suspicious lesions can be obtained. When no
metastatic disease is identified with inspection, a detailed
laparoscopic ultrasound examination may be used to
evaluate the deep hepatic parenchyma, portal vein, mes-
enteric vessels, celiac trunk, hepatic artery, entire pancreas,
and even periportal and paraaortic lymph nodes. The
addition of color flow Doppler can further assist in the
assessment of vascular patency.
The extent of inspection during SL for pancreatic ade-
nocarcinoma has been controversial. Advocates of a short-
duration procedure based only on inspection of abdominal
organ surfaces argue that the procedure can be performed
quickly (usually within 10–20 min), requires only one port,
does not require significant expertise, minimizes the risk of
potential complications from dissection near vascular
structures, and has good diagnostic accuracy [17, 18].
Conversely, advocates of a more extensive procedure
that includes opening of the lesser sac and assessment of
the vessels argue that the diagnostic accuracy of the pro-
cedure can be enhanced by detection of metastatic lesions
in the lesser sac, vascular invasion by the tumor, or deep
hepatic metastasis, which often are missed by visual
inspection alone. They further insist that it can be per-
formed safely without a significant increase in morbidity
and within a reasonable time [19–21]. It is very important,
therefore, to consider these differences in technique during
evaluation of reports on the diagnostic yield of SL for
patients with pancreatic adenocarcinoma.
The primary indication for SL is imaging-occult meta-
static pancreatic adenocarcinoma or unsuspected locally
advanced disease detected in patients with resectable dis-
ease based on preoperative imaging. Other indications
include assessment of disease extent before administration
of neoadjuvant chemoradiation as well as selection of
palliative treatments for patients with locally advanced
disease. However, SL should not be performed for patients
with known metastatic disease. Dense adhesions that
impair visual inspection may compromise the diagnostic
yield of the procedure.
Procedure-related morbidity is reported to range from
0% to 4% [17–46]. Most complications are minor and
include wound infections, port-site bleeding, or subcuta-
neous emphysema. Nevertheless, major complications such
as myocardial infarction, pulmonary embolism, and intes-
tinal or vascular injury have been described. The majority
of the literature reports mortality rates of 0% [17–46].
However, at least one death has been reported due to a
missed colonic injury during the procedure.
Conversions to open surgery are uncommon and in one
large series were reported to occur for less than 2% of the
patients [21]. The hospital length of stay after SL is
reported to range from 1 to 4 days [39]. Evidence suggests
that the hospital stay is shorter after laparoscopic staging
than after open staging for pancreatic cancer patients [26].
For patients with locally advanced disease, SL is reportedly
superior to exploratory laparotomy because it decreases
length of hospital stay, increases the number of patients
who receive chemotherapy, and shortens the time to initi-
ation of such treatment [34, 47].
With regard to oncologic safety, initial concerns for
port-site recurrence after laparoscopic procedures for
234 Surg Endosc (2009) 23:231–241
123

cancer patients have not been substantiated. Multiple
studies report a 0–2% incidence of port-site recurrences
after SL, which is similar to that after open explorations for
cancer patients [24, 39, 47]. In one study of 235 patients
comparing exploratory laparotomy with SL, laparoscopy
was not associated with increased port-site recurrences or
peritoneal disease progression [47]. Furthermore, evidence
from the Surveillance Epidemiology and End Results
(SEER) database suggests no survival differences between
pancreatic cancer patients who underwent a laparoscopic
procedure and those who had open surgery [48].
For detecting imaging-occult unresectable pancreatic
adenocarcinoma, the literature reports that SL has a median
sensitivity of 94% (range, 93–100%), a median specificity
of 88% (range, 80–100%), and a median accuracy of 89%
(range, 87–98%) (levels 2 and 3 evidence) [18–39].
However, the procedure misses 6% (range, 5–25%) of
patients whose disease is identified as unresectable during
an ensuing laparotomy (levels 2 and 3 evidence) [18–39].
Overall, 4% to 36% of patients can potentially avoid a
nontherapeutic laparotomy (levels 2 and 3 evidence) [18–
39]. A number of studies also have evaluated the added
benefit of laparoscopic ultrasound at the time of laparo-
scopic staging. These studies indicate that the diagnostic
accuracy of the procedure can be improved by 12–14%
(levels 2 and 3 evidence) [19–24, 35–38].
Peritoneal washings are reported to augment the yield of
the procedure. Reports on the sensitivity of peritoneal
washings have ranged widely from 25% to 100%) [18, 33,
40–42]. The highest sensitivity for peritoneal cytology is
reported for patients with a disrupted ventral pancreatic
margin, in which case, peripancreatic fatty tissue cannot be
differentiated from the tumor by helical CT scan (level 3
evidence) [42].
In addition, locally advanced pancreatic cancers have a
higher incidence of positive cytology (level 3 evidence)
[28, 33, 43]. Furthermore, studies have shown a 7–14%
incidence of positive peritoneal washings if no other met-
astatic disease is found during preoperative imaging and
SL (level 3 evidence) [18, 33]. This incidence seems to be
lower in studies that include a variety of periampullary
tumors (level 2 evidence) [30].
The diagnostic yield of the procedure also depends on
the histology, stage of disease, tumor size, and location.
There is convincing evidence that the yield of SL is sig-
nificantly higher for patients with pancreatic cancer than
for those with types of periampullary tumors (level 3 evi-
dence) [27, 28, 32, 39]. Furthermore, SL also appears to
have a higher yield for patients with locally advanced
cancer than for patients with localized disease. Identifica-
tion of metastatic disease by SL for patients with locally
advanced disease detected by high-quality imaging studies
is reported in 34–37% of cases, which compares favorably
with the identification rates for metastatic disease among
patients with localized disease (level 3 evidence) [17, 43,
44].
Tumors of the pancreas body and tail are associated with
a higher likelihood for unsuspected metastasis found at
laparoscopy (level 3 evidence) [18, 33]. Larger tumors
appear to be associated with a higher incidence of imaging-
occult metastatic disease (level 3 evidence) [28, 39, 45,
46]. Although the tumor size at which the risk of occult M1
disease justifies the added time and cost of laparoscopy is
currently unknown, some studies suggest that tumors larger
than 3 cm are more likely to be associated with metastatic
disease at exploration (level 3 evidence) [45, 46]. More-
over, a CA 19–9 level lower than 150 has been associated
with a lower likelihood for metastatic disease and conse-
quently a lower yield for SL (level 3 evidence) [49].
Although high-quality evidence on the cost effective-
ness of SL is lacking, the literature suggests that SL is more
cost effective than open exploration when it is the only
procedure required (i.e., for patients with unsuspected
metastatic disease identified during SL) (level 2 evidence)
[50]. This is a consequence of decreased patient length of
hospital stay. On the other hand, the cost effectiveness of
SL when applied in the diagnostic algorithm of all pan-
creatic cancer patients appears linked directly to the yield
of the procedure in identifying patients with imaging-
occult disease. In a cost utility analysis of the most effec-
tive management strategy for pancreatic cancer patients, at
least a 30% yield was needed for SL to be more cost
effective than open exploration (level 3 evidence) [51].
The quality of the available studies on SL for patients
with pancreas cancer is limited. No level 1 evidence exists.
Furthermore, population-based data are very limited
because the majority of studies are single-institution
reports from highly specialized centers, making general-
izations difficult and allowing institutional and personal
biases to be introduced into the results. In addition,
reported data are not uniform across studies, making their
analysis difficult. A number of studies assess the role of
laparoscopy indirectly without performance of a single
laparoscopic staging procedure (referred to as ‘‘phantom’’
studies by some authors). These studies assume that only
visible metastatic disease would have been detected at the
time of laparoscopy, ignoring the value of laparoscopic
ultrasound and cytology.
Other studies do not clearly report the quality of pre-
operative imaging, the criteria used to define resectability,
or the number of R0 resections. Furthermore, studies often
evaluate nonhomogeneous patient samples, including
patients with localized and locally advanced pancreatic
cancers as well as patients with periampullary and other
nonpancreatic cancers or even benign disease and do not
report results separately.
Surg Endosc (2009) 23:231–241 235
123

Summary of SL for pancreatic cancer
Based on our review of the literature, SL can be performed
safely and effectively for patients with pancreatic adeno-
carcinoma. The procedure should be considered after high-
quality imaging studies have excluded metastatic disease
for appropriately selected patients with either localized or
locally advanced pancreatic adenocarcinoma. The use of
laparoscopic ultrasound and peritoneal washings is
encouraged because they may improve the diagnostic
accuracy of the procedure. Based on the available evi-
dence, selective rather than routine use of the procedure
may be better justified and more cost effective for those
with larger tumors; tumors involving the pancreatic neck,
body, or tail; and patients with clinical, laboratory, or
imaging findings suggestive of more advanced disease.
Nevertheless, the effectiveness of such selection criteria
needs to be verified by additional prospective studies.
Staging laparoscopy for hepatocellular carcinoma
The prognosis of patients with hepatocellular carcinoma
may be improved with the appropriate selection of treat-
ment based on extent of disease. Subsequently, accurate
identification of all hepatic lesions including size, number,
and location is critical to therapy. Because peritoneal dis-
ease is uncommon with hepatocellular carcinoma,
inspection of peritoneal surfaces with diagnostic laparos-
copy alone tends to be less valuable than SL with
laparoscopic ultrasound. The appropriate identification of
patients who have unresectable disease using SL with
laparoscopic ultrasound not only will spare these patients a
nontherapeutic laparotomy with its associated morbidity,
but also may alter treatment plans. Additional benefits
include decreased patient morbidity, hospital stay, and
costs, as well as earlier adjuvant treatment. A 60% drop in
hospital charges for patients undergoing SL compared with
open laparotomy patients has been described for this pop-
ulation [52].
Staging laparoscopy generally is performed with the
patient under general anesthesia in the supine position.
After establishment of pneumoperitoneum, an angled
laparoscope through an umbilical port is recommended
for optimal visualization of the entire liver. Additional
ports can be placed in the right anterior axillary line and
epigastric area as needed. A standard laparoscopic ultra-
sound probe is used for systematic examination of the
entire liver to identify all lesions suspected to be malig-
nant. Ultrasound-guided core biopsy should be used for
suspicious lesions that are unresectable or preclude
curative resection. Biopsy of resectable lesions need not
be performed.
Patients with primary hepatic tumors whose proposed
curative resection is based on preoperative identification of
disease size and location with adequate hepatic reserve are
the best candidates for SL. Conversely, known unresectable
hepatic disease such as major vessel or organ invasion
would be a contraindication for SL. In addition, patients
with dense intraabdominal adhesions, particularly sur-
rounding the liver, from prior surgery may not be ideal
candidates for SL and laparoscopic ultrasound.
Procedure-related complications are uncommon, and no
mortality has been reported. Bleeding, infection, bowel
injury, bile leak, and anesthesia-related complications may
occur. Compared with open exploration, patients under-
going SL with laparoscopic ultrasound are reported to have
a shorter hospital stay (9 vs. 2.2–5 days, respectively) and
earlier adjuvant therapy (within 23 vs. 6 days, respectively)
(levels 2 and 3 evidence) [52, 53]. No adverse oncologic
effects of the procedure have been described.
For identifying hepatic tumors using, triphasic CT scan
is less sensitive than laparoscopic ultrasound in correlation
studies and highly dependent on tumor size, with detection
rates of 71% for tumors size 0–1 cm, 84% for tumors size
1–2 cm, 96% for tumors size 2–3 cm, and 100% for tumors
larger than 3 cm (100%) (level 2 evidence) [54]. Laparo-
scopic ultrasound can detect 9.5% more tumors (most
smaller in size than 1 cm) than CT alone (level 2 evidence)
[54]. Staging laparoscopy correctly identifies 63% to 67%
of patients with unresectable disease (levels 2 and 3 evi-
dence) [52, 53]. Unresectable disease was most commonly
missed by SL because of vascular invasion, lymph node
metastases, and adjacent organ invasion. With the combi-
nation of SL and laparoscopic ultrasound, 16% to 25% of
patients may avoid open laparotomy (levels 2 and 3 evi-
dence) [52, 53].
The quality and amount of the available literature on SL
for primary hepatic tumors are limited, and no level 1
evidence exists. The designs of these studies differ. Some
compare combined SL and laparoscopic ultrasound with
preoperative imaging, whereas others compare it with
exploratory laparotomy. There also is inconsistency in the
type of preoperative imaging and the specific CT scan
techniques used. In addition, the impact of each surgeon’s
expertise with laparoscopic ultrasound on the diagnostic
accuracy of the procedure remains unknown. These limi-
tations make firm recommendations difficult.
Summary of SL for hepatocellular carcinoma
Based on our review of the literature, SL with laparoscopic
ultrasound can be performed safely for patients with pri-
mary hepatic tumors or hepatocellular carcinoma. Patients
with primary hepatic cancers that appear resectable on
preoperative imaging may benefit from SL with
236 Surg Endosc (2009) 23:231–241
123

laparoscopic ultrasound used to evaluate extent, location,
and size of disease. Results of SL have the potential to alter
treatment appropriate to the extent of disease. Selection
criteria that may increase the yield and cost effectiveness
of the procedure still need to be determined, and further
studies are needed.
Staging laparoscopy for biliary tract tumors
Biliary tract tumors can be divided into two main categories:
gallbladder cancers and cholangiocarcinomas. The two
groups differ in their patterns of spread and their prognoses.
Gallbladder cancer tends grow more rapidly, with earlier
dissemination, which makes SL a more useful tool in this
setting. In contrast, cholangiocarcinomas tend to be more
locally invasive, decreasing the yield of SL. Preoperative
imaging to determine resectability of all biliary tract cancers
often includes ultrasound, CT scan, direct cholangiography
(percutaneous transhepatic cholangiography or endoscopic
retrograde cholangiopancreatography), and/or magnetic
resonance cholangiopancreatography. These radiologic
preoperative studies are used to evaluate the extent of tumor
within the biliary tree, vascular invasion, hepatic lobar
atrophy, and metastatic disease. The goal of SL would be to
spare patients from a laparotomy for incurable disease and to
offer the associated benefits of decreased morbidity and
pain, faster recovery, and earlier adjuvant treatment. Nota-
bly, however, many gallbladder cancers are incidental
findings during or after laparoscopic cholecystectomy. Thus,
for patients with gallbladder cancers found after cholecys-
tectomy, liver resection is indicated as a secondary
procedure, thereby obviating the need for SL.
Typically, SL is performed with the patient under gen-
eral anesthesia in the supine position. After establishment
of pneumoperitoneum, an angled laparoscope through an
umbilical port is recommended for optimal visualization of
the entire abdominal cavity. Additional ports can be placed
in the right anterior axillary line and epigastric area as
needed. Careful and thorough inspection of the peritoneum,
pelvis, liver surfaces, porta hepatis, gastrohepatic ligament,
and omentum should be performed. A standard laparo-
scopic ultrasound probe may improve the yield of lesions
found in the liver as well as lymph node metastasis found
in the porta hepatis and celiac nodal areas. Biopsy speci-
mens of peritoneal metastases, nodes suspected to be
malignant, and hepatic lesions should be obtained to
determine the extent of disease.
The indications for the use of SL to detect biliary tract
tumors differ slightly depending on the origin of the cancer.
For gallbladder cancer, SL generally is indicated for
patients with known or suspected gallbladder cancer but no
evidence of unresectable or metastatic disease unless noted
as an incidental finding after cholecystectomy. With cho-
langiocarcinomas, SL is indicated for stage T2 or T3 hilar
cholangiocarcinoma without evidence of unresectable or
metastatic disease determined by preoperative imaging.
Alternatively, SL is contraindicated for known metastatic or
unresectable disease and known stage T1 disease found
incidentally for gallbladder cancer. Dense intraabdominal
adhesions from prior surgery, particularly surrounding the
porta hepatis, may be considered a relative contraindication.
The reported incidence of complications is low, with no
mortality. Potential risks include bleeding, infection, and
bile leak, particularly if liver biopsy is performed. Addi-
tional risks include those associated with surgical
laparoscopy in general and those associated with anesthe-
sia. The assumed benefit of earlier adjuvant therapy for
patients with metastatic disease has not been addressed in
the literature. However, the average length of hospital stay
after SL is 2 to 3 days, which compares favorably with
laparotomy (level 2 evidence) [55, 56]. There have been no
reported adverse oncologic effects of SL for biliary cancer.
Staging laparoscopy can add further information to
standard preoperative imaging by identifying peritoneal or
superficial liver metastases (23%), which often are not
detected with radiology (level 3 evidence) [57]. For gall-
bladder cancer, the overall yield for unresectable disease
found with SL is reported to be 48%, with a diagnostic
accuracy of 58% (level 2 evidence) [55]. For cholangio-
carcinoma, as many as 9–42% [56–58] of patients may
avoid laparotomy with an accuracy of 42–53% (levels 2
and 3 evidence) [58]. For detecting unresectable disease,
SL has a reported sensitivity of 60% and a negative pre-
dictive value of 52% (level 2 evidence) [56].
The yield of SL for gallbladder cancer is slightly higher
than for cancers of the biliary tree due to the higher inci-
dence of peritoneal and liver metastases associated with
gallbladder cancer. One study suggests that the yield for
cholangiocarcinoma may be improved if SL is limited to
patients with higher-stage primary tumors on preoperative
imaging (T2 and T3) because few patients with stage T1
disease are deemed unresectable by laparoscopy (9%) [55].
The added benefit that laparoscopic ultrasound improves
the diagnostic yield of the procedure has been inconsistent
in the literature (0–41%) (levels 2 and 3 evidence) [57, 58].
The reported literature on SL used for biliary tract
cancer patients is limited, and no level 1 evidence exists. A
small number of reports describe highly specialized centers
with variations in technique. In addition, some studies span
a period of 7–10 years, which likely affects the quality of
preoperative imaging and laparoscopic technique at the
beginning and end of the study. The impact of the sur-
geon’s expertise on the diagnostic accuracy of the
procedure is unknown. These shortcomings of the literature
limit our ability to provide strong recommendations.
Surg Endosc (2009) 23:231–241 237
123

Summary of SL for biliary tract cancers
Based upon our review of the literature, SL can be per-
formed safely for patients with cancers of the biliary tract
and gallbladder. Staging laparoscopy may be used for
suspected gallbladder cancers believed to be resectable by
preoperative, high-quality imaging studies. However, SL
generally is not used for patients in whom an incidental
gallbladder cancer was identified after cholecystectomy.
Patients with biliary tract cancers or cholangiocarcinomas
also may benefit from SL through the identification of
imaging-occult disease in the peritoneum, the lymph nodes,
or the liver itself. The benefit of the procedure may be
maximized for patients with locally advanced cholangio-
carcinoma (stage T2 and T3) because the yield of the
procedure with this patient population is higher. Laparo-
scopic ultrasound may improve the yield of the procedure.
However, additional data are needed.
Staging laparoscopy for colorectal cancer
In the primary treatment of colorectal cancer, SL seldom
is used because surgical resection and palliation typically
are indicated to prevent bleeding, obstruction, and perfo-
ration even in patients with advanced disease. However,
patients who have liver metastases from a primary colo-
rectal cancer may be candidates for curative resection
when no other extrahepatic disease exists and when all the
disease in the liver is resectable. Thus, for these patients,
SL can provide more accurate identification of all hepatic
lesions than noninvasive imaging including size, number,
and location.
Similar to SL for primary hepatic tumors, SL and lap-
aroscopic ultrasound can identify patients with unsuspected
extrahepatic metastatic disease. The identification of these
patients may spare them the morbidity of a nontherapeutic
open laparotomy and may alter treatment plans. As with
other intraabdominal cancers, SL may lead to lower hos-
pital costs, shorter length of stay, and earlier adjuvant
therapy than open exploration without resection.
The technique is similar to SL in other settings. The
patient is placed in the supine position, and pneumoperi-
toneum is established. An angled laparoscope through an
umbilical port is recommended for optimal visualization of
the entire abdominal cavity. Additional ports can be placed
as needed. A standard laparoscopic ultrasound probe often
is used for systematic examination of the entire liver to
identify all lesions suspected to be malignant. The ultra-
sound examination also should include the porta hepatis
and celiac lymph nodes. Ultrasound-guided biopsy of
peritoneal, lymph node, and unsuspected liver lesions
should be obtained.
The primary indication of SL in this population is
resectable liver metastases from colorectal cancer without
concomitant evidence of extrahepatic metastatic disease on
noninvasive imaging. Conversely, patients with known
extrahepatic metastatic disease or unresectable hepatic
disease should not undergo SL. Dense intraabdominal
adhesions from prior surgery, particularly surrounding the
liver, may preclude adequate examination and thorough
SL.
In general, the morbidity and mortality for SL in these
patients are low, and the complications include bleeding,
infection, bowel injury, bile leak, and other complications
associated with laparoscopy. However, complications are
reported to be as high as 28%, including pneumonia and
myocardial infarction [59]. The hospital length of stay is
demonstrated to be significantly shorter for SL (1.2 days)
than for open laparotomy (5.8 days) [60]. A 55% reduction
in total hospital charges, with the greatest savings in room
and board charges, has been reported with SL compared
with open exploration (level 2 evidence) [60]. No adverse
oncologic effects have been described.
Studies comparing open intraoperative ultrasound with
laparoscopic ultrasound and preoperative CT scanning for
colorectal metastases have shown that the yield is best with
open intraoperative ultrasound, followed by laparoscopic
ultrasound (98% yield; one detected lesion less than with
open intraoperative ultrasound) and CT scan (78% yield)
[61]. Furthermore, SL and laparoscopic ultrasound have
better sensitivity than noninvasive imaging studies for the
detection of nodal metastases (94% for laparoscopic
ultrasound vs 18% for preoperative imaging) [62]. The
combination of SL and laparoscopic ultrasound is reported
to detect unresectable disease in 25–42% of patients for
whom preoperative radiologic testing showed potentially
curable disease [59, 60]. The use of laparoscopic ultra-
sound can further identify unresectable disease, which may
not be seen with laparoscopic inspection alone [60]. In
addition, the findings of the procedure have altered the
management for 33% to 48% of patients [59, 62, 63].
The Clinical Risk Score (CRS) system was developed to
predict which patients will most likely benefit from SL.
This system uses five preoperative criteria, which are
independent factors of prognosis: (1) lymph node-positive
colon cancer, (2) disease-free interval shorter than
12 months (time from discovery of primary colon cancer to
discovery of liver metastases), (3) more than one hepatic
tumor, (4) carcinoembryonic antigen greater than 200 ng/
ml within 1 month after surgery, and (5) size of largest
hepatic tumor greater than 5 cm. Each factor is assigned
one point. If the CRS is greater than 2, then the yield of SL
is higher [60].
The quality and amount of the available literature on SL
for colorectal cancer liver metastasis is limited because no
238 Surg Endosc (2009) 23:231–241
123

level 1 evidence exists. Although most studies use lapa-
roscopic ultrasound to establish resectability, institutions
differ in their technique and expertise. The impact of the
surgeon’s expertise on the diagnostic accuracy of the pro-
cedure is unknown. The limited available evidence impairs
our ability to provide firm recommendations.
Summary of SL for colorectal cancers
Based upon our review of the literature, SL can be per-
formed safely for patients with hepatic metastasis of
colorectal cancer. Patients with isolated colorectal hepatic
metastases who are candidates for liver resection may
benefit from SL with laparoscopic ultrasound. The patients
most likely to benefit from this procedure are those who
have more than two poor outcome factors as described by
the CRS.
Staging laparoscopy for lymphoma
Hodgkin’s lymphoma originates in one nodal group and
spreads in a stepwise manner to contiguous nodal groups.
Staging laparoscopy may be useful in determining the stage
and location of the disease, and this may affect decisions
regarding treatment, particularly the administration of che-
motherapy. In contrast, for non-Hodgkin’s lymphoma, the
exact extent of the disease has less impact on the treatment
course, so SL is less frequently performed in cases of non-
Hodgkin’s lymphoma. Staging laparoscopy may spare
patients the morbidity of a laparotomy and provide tissue to
confirm the diagnosis of non-Hodgkin’s lymphoma or allow
the surgical staging of Hodgkin’s lymphoma. Staging lap-
aroscopy also can be used for patients who need
laparoscopic splenectomy as treatment and may lead to less
pain, faster recovery, and earlier definitive treatment.
The technique of SL for lymphoma tends to be more
involved than SL for simple inspection of the peritoneal
surfaces with other cancers. Patients are commonly placed at
a 45� angle in the left decubitus position. A laparoscopic
hand-assisted technique may be used, especially when
splenectomy is planned. The steps of SL are similar to those
used in the traditional open procedure including inspection
for gross abnormalities; core liver biopsy of each hepatic
lobe and wedge biopsy of left lateral liver segment; laparo-
scopic ultrasound to search for hepatic lesions; splenectomy
with removal of the organ intact; lymph node sampling of the
iliac, celiac, portal, mesenteric, and periaortic areas; lymph
node excision of abnormal nodes identified at preoperative
testing with application of clips in those excision areas; and
oophoropexy posterior to the uterus.
The primary indication for SL in non-Hodgkin’s lym-
phoma is a tissue diagnosis through biopsy of
intraabdominal lymph nodes in the absence of peripheral
lymphadenopathy, particularly when percutaneous core
needle biopsy has been nondiagnostic. In addition, SL can
be used for accurate staging of Hodgkin’s lymphoma when
staging affects decisions for appropriate treatment or
prognosis. Staging laparoscopy also may be indicated for
restaging after treatment or when recurrence is suspected.
Published morbidity rates range widely (1–20%) and
include complications such as small bowel perforation,
abscess, pancreatitis, bleeding, and pneumonia [64–66].
Conversion to laparotomy is reported to occur in 5–17% of
the cases. No mortality has been reported [64–66]. The
presumed benefit of earlier adjuvant therapy has not been
addressed in the literature, but length of hospital stay after
diagnostic laparoscopy is reported to vary from 1 to 4 days
[64, 65]. No adverse oncologic effects from the procedure
have been reported.
Data on the accuracy of the procedure come mainly
from feasibility studies and are sparse. Compared with
percutaneous biopsy, laparoscopic biopsy is demonstrated
to have superior sensitivity (87% vs. 100%), specificity
(93% vs. 100%), and accuracy (33% vs. 83%) (level 3
evidence) [64].
The quality of the available literature on SL for lym-
phoma is primarily limited to retrospective reviews. In
addition, the number of available studies is quite small.
Furthermore, some studies compare the accuracy of the
procedure with that of historical controls for open surgery,
which increases the bias of the results. Surgical technique
differs according to institution and surgeon experience,
making generalizations difficult and strong recommenda-
tions impossible.
Summary of SL for lymphomas
Based on our review of the literature, SL for lymphopro-
liferative disorders is safe and effective. The best
indication for SL in lymphoproliferative disorders may be a
tissue diagnosis of non-Hodgkin’s lymphoma when core
needle biopsy is nondiagnostic. In addition, SL is indicated
for primary staging or even restaging of Hodgkin’s lym-
phoma when accurate staging affects decisions for
appropriate treatment and prognosis. Furthermore, lapa-
roscopy may be performed when splenectomy is required
in this patient population.
References
1. Guidelines for diagnostic laparoscopy. Retrieved March 25, 2008
at http://www.sages.org/sagespublication.php?doc=12
2. Krasna MJ, Reed CE, Nedzwiecki D, Hollis DR, Luketich JD,
DeCamp MM, Mayer RJ, Sugarbaker DJ CALGB, Surgeons
Surg Endosc (2009) 23:231–241 239
123

Thoracic (2001) CALGB 9380: a prospective trial of the feasi-
bility of thoracoscopy/laparoscopy in staging esophageal cancer.
Ann Thorac Surg 71:1073–1079
3. Heath EI, Kaufman HS, Talamini MA, Wu TT, Wheeler J,
Heitmiller RF, Kleinberg L, Yang SC, Olukayode K, Forastiere
AA (2000) The role of laparoscopy in preoperative staging of
esophageal cancer. Surg Endosc 14:495–499
4. Bonavina L, Incarvone R, Lattuada E, Segalin A, Cesana B,
Peracchia A (1997) Preoperative laparoscopy in management of
patients with carcinoma of the esophagus and of the esophag-
ogastric junction. J Surg Oncol 65:171–174
5. Romijn MG, van Overhagen H, Spillenaar Bilgen EJ, Ijzermans
JN, Tilanus HW, Lameris JS (1998) Laparoscopy and laparo-
scopic ultrasonography in the staging of oesophageal and cardial
carcinoma. Br J Surg 85:1010–1012
6. Krasna MJ, Jiao X, Mao YS, Sonett J, Gamliel Z, Kwong K,
Burrows W, Flowers JL, Greenwald B, White C (2002) Thora-
cosopy/laparoscopy in the staging of esophageal cancer. Surg
Laparosc Endosc Percutan Tech 12:213–218
7. D’Ugo DM, Pende V, Persiani R, Rausei S, Picciocchi A (2003)
Laparoscopic staging of gastric cancer: an overview. J Am Coll
Surg 196:965–974
8. Asencio F, Aguilo J, Salvador JL, Villar A, De la Morena E,
Ahamad M, Escrig J, Puche J, Viciano V, Sanmiguel G, Ruiz J
(1997) Video-laparoscopic staging of gastric cancer. Surg Endosc
11:1153–1158
9. Hulscher JBF, Nieveen van Dijkum EJ, de Wit LT, van Delden
OM, van Lanschot JJ, Obertop H, Gouma DJ (2000) Laparoscopy
and laparoscopic ultrasonography in staging carcinoma of the
gastric cardia. Eur J Surg 166:862–865
10. Gross E, Bancewicz J, Ingram G (1984) Assessment of gastric
cancer by laparoscopy. Br Med J 288:1577
11. Possik RA, Franco EL, Pires DR, Wohnrath DR, Ferreira EB
(1986) Sensitivity, specificity, and predictive value of laparos-
copy for the staging of gastric cancer and for the detection of liver
metastases. Cancer 58:1–6
12. Kriplani AK, Kapur BML (1991) Laparoscopy for the preoper-
ative staging and assessment of operability in gastric carcinoma.
Gastrointest Endosc 37:441–443
13. Lowy AM, Mansfield PF, Leach SD, Ajani J (1996) Laparoscopic
staging for gastric cancer. Surgery 119:611–614
14. Burke EC, Karpeh MS, Conlon KC, Brennan MF (1997) Lapa-
roscopy in the management of gastric adenocarcinoma. Ann Surg
225:262–267
15. Stell DA, Carter CR, Stewart I, Anderson JR (1996) Prospective
comparison of laparoscopy, ultrasonography, and computed
tomography in the staging of gastric cancer. Br J Surg 86:1260–
1262
16. Conlon KC (2001) Staging laparoscopy for gastric cancer. Ann
Ital Chir 72:33–37
17. Luque-de Leon E, Tsiotos GG, Balsiger B, Barnwell J, Burgart
LJ, Sarr MG (1999) Staging laparoscopy for pancreatic cancer
should be used to select the best means of palliation and not
only to maximize the resectability rate. J Gastrointest Surg
3:111–117
18. Jimenez RE, Warshaw AL, Rattner DW, Willett CG, McGrath D,
Fernandez-Del Castillo C (2000) Impact of laparoscopic staging
in the treatment of pancreatic cancer. Arch Surg 135:409–414
19. Schachter PP, Avni Y, Shimonov M, Gvirtz G, Rosen A, Czer-
niak A (2000) The impact of laparoscopy and laparoscopic
ultrasonography on the management of pancreatic cancer. Arch
Surg 135:1303–1307
20. Minnard EA, Conlon KC, Hoos A, Dougherty EC, Hann LE,
Brennan MF (1998) Laparoscopic ultrasound enhances standard
laparoscopy in the staging of pancreatic cancer. Ann Surg
228:182–187
21. Hunerbein M, Rau B, Hohenberger P, Schlag PM (1998) The role
of staging laparoscopy for multimodal therapy of gastrointestinal
cancer. Surg Endosc 12:921–925
22. Durup Scheel-Hincke J, Mortensen MB, Qvist N, Hovendal CP
(1999) TNM staging and assessment of resectability of pancreatic
cancer by laparoscopic ultrasonography. Surg Endosc 13:967–
971
23. Doran HE, Bosonnet L, Connor S, Jones L, Garvey C, Hughes M,
Campbell F, Hartley M, Ghaneh P, Neoptolemos JP, Sutton R
(2004) Laparoscopy and laparoscopic ultrasound in the evalua-
tion of pancreatic and periampullary tumours. Dig Surg 21:305–
313
24. Pietrabissa A, Caramella D, Di Candio G, Carobbi A, Boggi U,
Rossi G, Mosca F (1999) Laparoscopy and laparoscopic ultra-
sonography for staging pancreatic cancer: critical appraisal.
World J Surg 23:998–1002
25. Awad SS, Colletti L, Mulholland M, Knol J, Rothman ED,
Scheiman J, Eckhauser FE (1997) Multimodality staging opti-
mizes resectability in patients with pancreatic and ampullary
cancer. Am Surg 63:634–638
26. Conlon KC, Dougherty E, Klimstra DS, Coit DG, Turnbull AD,
Brennan MF (1996) The value of minimal access surgery in the
staging of patients with potentially resectable peripancreatic
malignancy. Ann Surg 223:134–140
27. Vollmer CM, Drebin JA, Middleton WD, Teefey SA, Linehan
DC, Soper NJ, Eagon CJ, Strasberg SM (2002) Utility of staging
laparoscopy in subsets of peripancreatic and biliary malignancies.
Ann Surg 235:1–7
28. Pisters PW, Lee JE, Vauthey JN, Charnsangavej C, Evans DB
(2001) Laparoscopy in the staging of pancreatic cancer (review,
45 references). Br J Surg 88:325–337
29. Kwon AH, Inui H, Kamiyama Y (2002) Preoperative laparo-
scopic examination using surgical manipulation and
ultrasonography for pancreatic lesions. Endoscopy 34:464–468
30. Nieveen van Dijkum EJ, Romijn MG, Terwee CB, de Wit LT,
van der Meulen JH, Lameris HS, Rauws EA, Obertop H, van
Eyck CH, Bossuyt PM, Gouma DJ (2003) Laparoscopic staging
and subsequent palliation in patients with peripancreatic carci-
noma. Ann Surg 237:66–73
31. Friess H, Kleeff J, Silva JC, Sadowski C, Baer HU, Buchler MW
(1998) The role of diagnostic laparoscopy in pancreatic and pe-
riampullary malignancies. J Am Coll Surg 186:675–682
32. Barreiro CJ, Lillemoe KD, Koniaris LG, Sohn TA, Yeo CJ,
Coleman J, Fishman EK, Cameron JL (2002) Diagnostic lapa-
roscopy for periampullary and pancreatic cancer: what is the true
benefit? J Gastrointest Surg 6:75–81
33. Liu RC, Traverso LW (2005) Diagnostic laparoscopy improves
staging of pancreatic cancer deemed locally unresectable by
computed tomography. Surg Endosc 19:638–642
34. Holzman MD, Reintgen KL, Tyler DS, Pappas TN (1997) The
role of laparoscopy in the management of suspected pancreatic
and periampullary malignancies. J Gastrointest Surg 1:236–243
35. Tilleman EH, de Castro SM, Busch OR, Bemelman WA, van
Gulik TM, Obertop H, Gouma DJ (2002) Diagnostic laparoscopy
and laparoscopic ultrasound for staging of patients with malignant
proximal bile duct obstruction. J Gastrointest Surg 6:426–430
36. John TG, Wright A, Allan PL, Redhead DN, Paterson-Brown S,
Carter DC, Garden OJ (1999) Laparoscopy with laparoscopic
ultrasonography in the TNM staging of pancreatic carcinoma.
World J Surg 23:870–881
37. Callery MP, Strasberg SM, Doherty GM, Soper NJ, Norton JA
(1997) Staging laparoscopy with laparoscopic ultrasonography:
optimizing resectability in hepatobiliary and pancreatic malig-
nancy. J Am Coll Surg 185:33–39
38. Bemelman WA, de Wit LT, van Delden OM, Smits NJ, Obertop
H, Rauws EJ, Gouma DJ (1995) Diagnostic laparoscopy
240 Surg Endosc (2009) 23:231–241
123

combined with laparoscopic ultrasonography in staging of cancer
of the pancreatic head region (see comment). Br J Surg 82:820–
824
39. Stefanidis D, Grove KD, Schwesinger WH, Thomas CR Jr (2006)
The current role of staging laparoscopy for adenocarcinoma of
the pancreas: a review. Ann Oncol 17:189–199
40. Fernandez-del Castillo CL, Warshaw AL (1998) Pancreatic
cancer. laparoscopic staging and peritoneal cytology. Surg Oncol
Clin North Am 7:135–142
41. Fernandez-Del Castillo C, Rattner DW, Warshaw AL (1995)
Further experience with laparoscopy and peritoneal cytology in
the staging of pancreatic cancer. Br J Surg 82:1127–1129
42. Schmidt J, Fraunhofer S, Fleisch M, Zirngibl H (2004) Is peri-
toneal cytology a predictor of unresectability in pancreatic
carcinoma? Hepatogastroenterology 51:1827–1831
43. Liu RC, Traverso LW (2004) Laparoscopic staging should be
used routinely for locally extensive cancer of the pancreatic head.
J Gastrointest Surg 8:923–924
44. Shoup M, Winston C, Brennan MF, Bassman D, Conlon KC
(2004) Is there a role for staging laparoscopy in patients with
locally advanced, unresectable pancreatic adenocarcinoma? J
Gastrointest Surg 8:1068–1071
45. Yoshida T, Matsumoto T, Morii Y, Ishio T, Kitano S, Yamada Y,
Mori H (2002) Staging with helical computed tomography and
laparoscopy in pancreatic head cancer. Hepatogastroenterology
49:1428–1431
46. Morganti AG, Brizi MG, Macchia G, Sallustio G, Costamagna G,
Alfieri S, Mattiucci GC, Valentini V, Natale L, Deodato F, Mu-
tignani M, Doglietto GB, Cellini N (2005) The prognostic effect
of clinical staging in pancreatic adenocarcinoma. Ann Surg Oncol
12:145–151
47. Velanovich V (2004) The effects of staging laparoscopy on trocar
site and peritoneal recurrence of pancreatic cancer. Surg Endosc
18:310–313
48. Urbach DR, Swanstrom LL, Hansen PD (2002) The effect of
laparoscopy on survival in pancreatic cancer. Arch Surg
137:191–199
49. Connor S, Bosonnet L, Alexakis N, Raraty M, Ghaneh P, Sutton
R, Neoptolemos JP (2005) Serum CA19-9 measurement increases
the effectiveness of staging laparoscopy in patients with sus-
pected pancreatic malignancy. Dig Surg 22:80–85
50. Andren-Sandberg A, Lindberg CG, Lundstedt C, Ihse I (1998)
Computed tomography and laparoscopy in the assessment of the
patient with pancreatic cancer. J Am Coll Surg 186:35–40
51. Obertop H, Gouma DJ (1999) Essentials in biliopancreatic stag-
ing: a decision analysis. Ann Oncol 10(Suppl 4):150–152
52. Jarnagin WR, Bodniewicz J, Dougherty E, Conlon K, Blumgart
LH, Fong Y (2000) A prospective analysis of staging laparoscopy
in patients with primary and secondary hepatobiliary malignan-
cies. J Gastrointest Surg 4:34–43
53. Lo CM, Lai EC, Liu CL, Fan ST, Wong J (1998) Laparoscopy
and laparoscopic ultrasonography avoid exploratory laparotomy
in patients with hepatocellular carcinoma. Ann Surg 227:527–532
54. Foroutani A, Garland AM, Berber E, String A, Engle K, Ryan
TL, Pearl JM, Siperstein AE (2000) Laparoscopic ultrasound vs.
triphasic computed tomography for detecting liver tumors. Arch
Surg 135:933–938
55. Weber SM, DeMatteo RP, Fong Y, Blumgart LH, Jarnagin WR
(2002) Staging laparoscopy in patients with extrahepatic biliary
carcinoma. Ann Surg 235:392–399
56. Tilleman EH, de Castro SM, Busch OR, Bemelman WA, van
Gulik TM, Obertop H, Gouma DJ (2002) Diagnostic laparoscopy
and laparoscopic ultrasound for staging of patients with malig-
nant proximal bile duct obstruction. J Gastroint Surg 6:426–430
57. van Delden OM, de Wit LT, Nieveen van Dijkum EJM, Smits NJ,
Gouma DJ, Reeders JW (1997) Value of laparoscopic ultraso-
nography in staging of proximal bile duct tumors. J Ultrasound
Med 16:7–12
58. Connor S, Barron E, Wigmore SJ, Madhavan KK, Parks RW,
Garden OJ (2005) The utility of laparoscopic assessment in the
preoperative staging of suspected hilar cholangiocarcinoma. J
Gastrointest Surg 9:476–480
59. Thaler K, Kanneganti S, Khajanchee Y, Wilson C, Swanstrom L,
Hansen PD (2005) The evolving role of staging laparoscopy in
the treatment of colorectal hepatic metastasis. Arch Surg
140:727–734
60. Jarnagin WR, Conlon K, Bodniewicz J, Dougherty E, Dematteo
RP, Blumgart LH, Fong Y (2001) A clinical scoring system
predicts the yield of diagnostic laparoscopy in patients with
potentially resectable hepatic colorectal metastases. Cancer
91:1121–1128
61. Milsom JW, Jerby BL, Kessler H, Hale JC, Herts BR, O’Malley
CM (2000) Prospective, blinded comparison of laparoscopic
ultrasonography vs contrast-enhanced computerized tomography
for liver assessment in patients undergoing colorectal carcinoma
surgery. Dis Colon Rectum 43:44–49
62. Goletti O, Celon G, Galatioto C, Viaggi B, Lippolis PV, Pieri L,
Cavina E (1998) Is laparoscopic sonography a reliable and sen-
sitive procedure for staging colorectal cancer? Surg Endosc
12:1236–1241
63. Rahusen FD, Cuesta MA, Borgstein PJ, Bleichrodt RP, Barkhof
F, Doesburg T, Meijer S (1999) Selection of patients for resection
of colorectal metastases to the liver using diagnostic laparoscopy
and laparoscopic ultrasonography. Ann Surg 230:31–37
64. Asoglu O, Porter L, Donohue JH, Cha SS (2005) Laparoscopy for
the definitive diagnosis of intraabdominal lymphoma. Mayo Clin
Proc 80:625–631
65. Baccarani U, Carroll BJ, Hiatt JR, Donini A, Terrosu G, Decker
R, Chandra M, Bresadola F, Phillips EH (1998) Comparison of
laparoscopic and open staging in Hodgkin’s disease. Arch Surg
133:517–522
66. Silecchia G, Raparelli L, Perrotta N, Fantini A, Fabiano P,
Monarca B, Basso N (2003) Accuracy of laparoscopy in the
diagnosis and staging of lymphoproliferative diseases. World J
Surg 27:653–658
Surg Endosc (2009) 23:231–241 241
123