Presentasi Dr. Tonny

of 60
-
Upload
muhammad-faried-fahda -
Category
Documents
-
view
220 -
download
0
Transcript of Presentasi Dr. Tonny
-
8/12/2019 Presentasi Dr. Tonny
1/60
AIR WAY DISEASEImaging aspect
Tonny K.Sudarmo
Bag.Radiologi FKUI.
-
8/12/2019 Presentasi Dr. Tonny
2/60
GROUP
1. Air Space Enlargement.
2. Alveolar Filling disorders.
-
8/12/2019 Presentasi Dr. Tonny
3/60
AIR SPACE ENLARGEMENT
Definition:
An increased in air space size as
compared with airspace of normal
lung.
-
8/12/2019 Presentasi Dr. Tonny
4/60
AIR SPACE ENLARGEMENT
Simple air space enlargement.Congenital :
Congenital lobar over inflation
Down Syndrome
Acquired:
Secondary to loss of volume
Associated with aging
-
8/12/2019 Presentasi Dr. Tonny
5/60
Emphysema
Centroacinar
Paraacinar
Distal emphysema
Bullae
Airspace enlargement with fibrosis
Bronchiectasis
Irregular or paracicatrical emphysema
Honey combing ( end-stage) lung
-
8/12/2019 Presentasi Dr. Tonny
6/60
Air space enlargement
Emphysema
Bronchiectasis
Bullae
-
8/12/2019 Presentasi Dr. Tonny
7/60
EMPHYSEMA
Characterized by:
Enlarged of the air space distal to the
terminal bronchiole, with destruction of their
wall, and without obvious fibrosis.
Parenchyma distal to the terminal
bronchioleacinus or primary lobe. Large cystic area or bullae develop ( bullous
emphysema)
-
8/12/2019 Presentasi Dr. Tonny
8/60
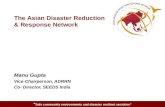
TB = Terminal bronchioles
RB = Respiratory bronchiolesA = Alveoli
-
8/12/2019 Presentasi Dr. Tonny
9/60
A. Acinus
B. Centrilobular
C. Panacinar
D. Paraseptal
E. irregular
AD = Alveolar Duct
AS = Alveolar Sacs
-
8/12/2019 Presentasi Dr. Tonny
10/60
Type.
a. . Centrilobular
- Destruction is limited to the central part of the
lobule.
- Peripheral alveolar ducts and alveoli may
escape unscathed.- Apex upper lobe, spreads down as the disease
progress.
-
8/12/2019 Presentasi Dr. Tonny
11/60
Centrilobular
Early
Advance
-
8/12/2019 Presentasi Dr. Tonny
12/60
Normal acinus Centri acinar
-
8/12/2019 Presentasi Dr. Tonny
13/60
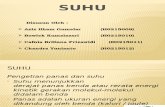
Type
b. Panlobular.
- Show distention and destruction of the whole
lobule.
- No regional preference, or is more common in
the lower lobes.
-
8/12/2019 Presentasi Dr. Tonny
14/60
Normal
Panacinar
Panlobular
-
8/12/2019 Presentasi Dr. Tonny
15/60
-
8/12/2019 Presentasi Dr. Tonny
16/60
Type
c. Distal (paraseptal) emphysema.
- Alveolar duct and sacs are dominantly involved.
- Found deep to pleura and adjacent lobular septa.
- Associated with spontaneous pneumothorax.
-
8/12/2019 Presentasi Dr. Tonny
17/60
-
8/12/2019 Presentasi Dr. Tonny
18/60
Emphysema
CT observation
- Decreased in lung attenuation.
- Decreased in the diameter and number of
pulmonary vessel
-
8/12/2019 Presentasi Dr. Tonny
19/60
Emphysema
Technique :
Using High Resolution CT
- Collimation 1 mm.
- High spatial frequency reconstructionalgorithm.
- Scan interval 10 mm.
-
8/12/2019 Presentasi Dr. Tonny
20/60
Emphysema
The Image
Window level - 600 to - 700 H
Window width 1500 to 1700 H.
-
8/12/2019 Presentasi Dr. Tonny
21/60
Centriacinar Emphysema
CT Findings :
- Focal area of decreased attenuation without
discernable wall.
- Focal arteriole at or near the center of
emphysema ( interior vessel)
-
8/12/2019 Presentasi Dr. Tonny
22/60
Centriacinar
-
8/12/2019 Presentasi Dr. Tonny
23/60
Panacinar Emphysema
CT Findings :
- Large area of decreased attenuation with poorly
defined lateral margin.
- Pulmonary vessel decreased in diameter and
number.
-
8/12/2019 Presentasi Dr. Tonny
24/60
Panlobular emphysema
-
8/12/2019 Presentasi Dr. Tonny
25/60
Panlobular emphysema
-
8/12/2019 Presentasi Dr. Tonny
26/60
-
8/12/2019 Presentasi Dr. Tonny
27/60
Distal Acinar Emphysema
CT Findings :
- Focal area of decreased attenuation in the
sub pleura areas with upper lobe predominance.
- Thin wall and no interior vessel.
-
8/12/2019 Presentasi Dr. Tonny
28/60
Paraseptal
-
8/12/2019 Presentasi Dr. Tonny
29/60
Distal
-
8/12/2019 Presentasi Dr. Tonny
30/60
Paraseptal emphysema
-
8/12/2019 Presentasi Dr. Tonny
31/60
Paraseptal emphysema
-
8/12/2019 Presentasi Dr. Tonny
32/60
Bullae
A bulla is an airspace in the lung more
than 1 cm in diameter in the distended
state.
Cl ifi ti
-
8/12/2019 Presentasi Dr. Tonny
33/60
Classification
Type I :
- Sub pleural and are found in the absence of emphysema.- Multiple and very large.
- Compromise lung function by compression of the
remaining normal lung.
Type II :- Sub pleura but associated with emphysema in the rest of
lung.
Type III :- Located within the lung rather than sub pleural.
- Also associated with emphysema in the rest of the lung.
-
8/12/2019 Presentasi Dr. Tonny
34/60
Bulla emphysema
-
8/12/2019 Presentasi Dr. Tonny
35/60
Bulla emphysema
-
8/12/2019 Presentasi Dr. Tonny
36/60
-
8/12/2019 Presentasi Dr. Tonny
37/60
BRONCHIECTASIS
Defined as permanent abnormal dilatation
of bronchi, but bronchial dilatation also
occur in chronic bronchitis.
Not frequently bronchiectasis and
emphysema occur together
REID CLASSIFICATION
-
8/12/2019 Presentasi Dr. Tonny
38/60
REID CLASSIFICATION
Group 1: Cylindrical bronchiectasisBronchiole minimally dilated
All bronchi and bronchioles are occluded by purulent material.
Branching bronchial tree is within normal limits.
Group 2: Varicose Bronchiectasis
Characterized by localized bulbous areas of bronchial dilatation.Reduced visible bronchial subdivision from the hilum to periphery.
Group 3: Saccular of cystic bronchiectasis
Grossly distorted bronchi with large saccular terminations filled withpurulent secretion.
Number of bronchial division from hilus to periphery is greatly
reduced.
-
8/12/2019 Presentasi Dr. Tonny
39/60
CT DIAGNOSIS OF BRONCHIECTASIS
Primary signIdentification of enlarged internal bronchial diameter
Failure if an airway to taper while progressing toward
periphery.Identification of airway in the extreme lung periphery
Indirect sign
Bronchial wall thickening
Mucus impaction
Focal air trapping
-
8/12/2019 Presentasi Dr. Tonny
40/60
-
8/12/2019 Presentasi Dr. Tonny
41/60
Dilated bronchus run parallelto the plane of
CT Section
Tram track ( Cylindrical Br.)
Beaded appearance ( Varicose Br.)
String of cyst or cluster of cyst ( Cystic Br.)
i i
-
8/12/2019 Presentasi Dr. Tonny
42/60
Dilated bronchus run perpendicular
to the plane of CT section
Signet ring sign :
Ring structure with internal diameter larger
than that of its accompanying pulmonary arterybranches.
-
8/12/2019 Presentasi Dr. Tonny
43/60
-
8/12/2019 Presentasi Dr. Tonny
44/60
-
8/12/2019 Presentasi Dr. Tonny
45/60
Mucus impaction seen as:
Nodular density(in cross section)
Tubular or branching structure
- Beaded, glove finger, Y or V shaped
(in the plane of the section)
Air trappingseen as :Mosaic attenuation
-
8/12/2019 Presentasi Dr. Tonny
46/60
-
8/12/2019 Presentasi Dr. Tonny
47/60
-
8/12/2019 Presentasi Dr. Tonny
48/60
SPECIAL TOPIC
CHRONIC OBSTRUCTIVE LUNG DISEASE.
-
8/12/2019 Presentasi Dr. Tonny
49/60
Common pathophysiologic abnormality
Persistent increase resistance tobronchial air flow
A. Lumen is partly blocked
B. Wall is thickened
C. Abnormality is outside
I d i
-
8/12/2019 Presentasi Dr. Tonny
50/60
Increased resistance
Condition:
1. Inside the lumen
occluded by excessive secretion, edema,
aspiration, foreign bodies
2. In the wall of the airway
Loss of elastic recoil, hipertrophic mucous
gland, inflamation/edema.
3. In the peribronchial regionLoss of radial traction, edema, externalcompression.
-
8/12/2019 Presentasi Dr. Tonny
51/60
Chronic Obstructive Group:
1. Pulmonary Emphysema
2. Chronic Bronchitis
3. Asthma
-
8/12/2019 Presentasi Dr. Tonny
52/60
Cardinal Symptoms :
1. Cough
2. Dysnea
3. Wheeze
Air flow :
1. Forced expiratory volume in
one second ( FEV1)
2. Forced Vital Capacity (FVC)
Lesion associated with chronic airflow obstruction
-
8/12/2019 Presentasi Dr. Tonny
53/60
Lesion associated with chronic airflow obstruction
BronchiMucous gland enlargement
Smooth muscle hyperplasiaCartilage atrophy
Inflamation
BronchiolesUsual chronic airflow obstruction
Inflamation
Bronchiolar narrowing
Bronchiolar obliteration
Fibrosis
Muscle increaseGoblet cell metaplasia
Mucus plugging
Bronchiolar totousity
Loss of alveolar attachment
Pigmentation
-
8/12/2019 Presentasi Dr. Tonny
54/60
Special form of bronchiolitis
-Viral infection, toxic chemical and gasses, rheumatoid arthritis.
- Diffuse pan-bronchiolitis, graft-vs-host disease, heart / lung
- Tranplantation, follicular bronchitis/bronchiolitis, mineral
dust associated bronchiolitis, cryptogenic bronchiolitis
Acinus
- Respiratory bronchiolitis
- Emphysema
- Respiratory airspace enlargement
-
8/12/2019 Presentasi Dr. Tonny
55/60
-
8/12/2019 Presentasi Dr. Tonny
56/60
-
8/12/2019 Presentasi Dr. Tonny
57/60
-
8/12/2019 Presentasi Dr. Tonny
58/60
-
8/12/2019 Presentasi Dr. Tonny
59/60
-
8/12/2019 Presentasi Dr. Tonny
60/60
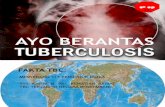
A. Interlobular septal
thickening
B. Intralobular interstitialthickening
C. Hineycombing
D. Centrilobular
E. Interstitial nodules
F. Cavitary nodules
G. Airspace nodules
H. Ground glass opacity
I. Lobular emphysema
J. Panlubular
K. Lung cyst