Presentación de PowerPoint - asocmi.com · Agentes inotropicos negativos (disopiramida) Volumen...
47
SINCOPE NEUROCARDIOGENICO Dra. Vivien Araya Gómez Cardióloga – Electrofisióloga Centro Cardiológico Integral www.centrocardiologicocr.com
Transcript of Presentación de PowerPoint - asocmi.com · Agentes inotropicos negativos (disopiramida) Volumen...
SINCOPE NEUROCARDIOGENICO
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
www.centrocardiologicocr.com
SÍNCOPE NEUROCORDIOGÉNICO (SNCG)
EPIDEMILOGÍAHasta hace algunos años, en un 30-50% de los casos de síncopes
no se establecía la causa exacta
Lewis: “Vasovagal Syncope and the carotid sinus mechanism”. Br Med J 1932; 1:873-876.
Kenny RA y col, Head-up tilt a useful test for investigation unexplained syncope. Lancet 1986;1:1352-1354.
La mayoría de los síncopes (75%) en pacientes con corazón estructuralmente normal son SNCG.
Aprox. 70% de los pacientes con SNCG son menores de 65 años.
Incidencia mayor en mujeres vs hombres.
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral

Causas de síncope


TRASTORNOS DEL SNA ASOCIADOS A INTOLERANCIA ORTOSTATICA
SNCGCARACTERÍSTICAS CLÍNICAS
La mayoría de los episodios se relacionan con algún factor precipitante:
• Dolor
• Miedo
• Estrés
• Ingesta de alcohol
• Comida copiosa
• Calor
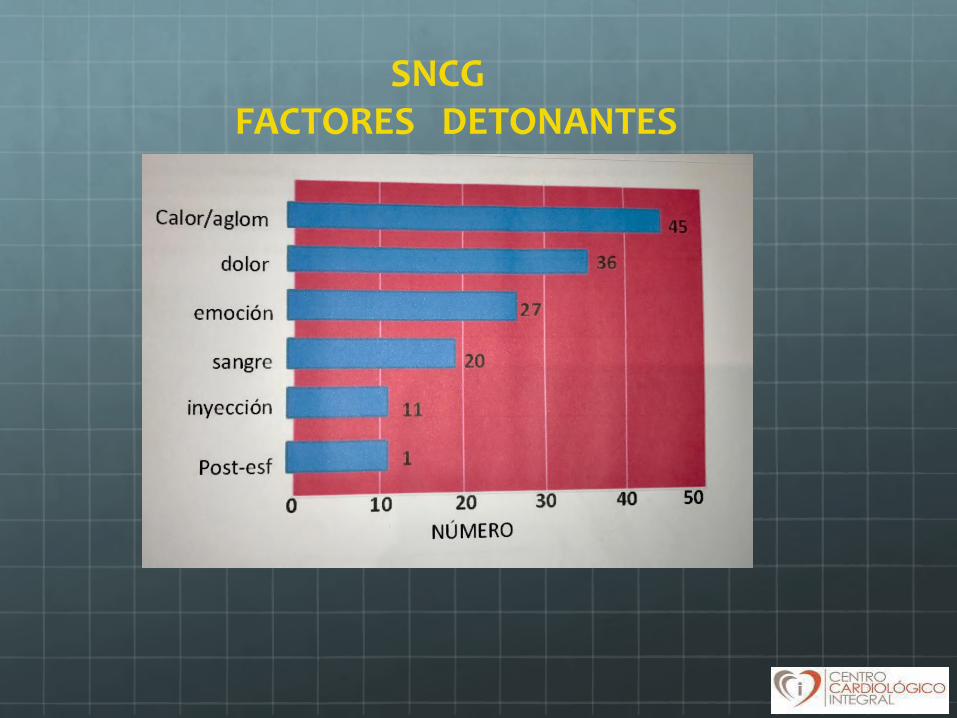
SNCGFACTORES DETONANTES
Puede ocurrir tanto en posición de pie como sentado.
En algunos pacientes hay pródromos tales como:
Bostezos
Malestar epigástrico
Debilidad
Calor
Ansiedad
disminución campo visual
Hiperventilación
Palpitaciones
Palidez
Diaforesis
Náuceas
Mareos
SNCGCARACTERÍSTICAS CLÍNICAS
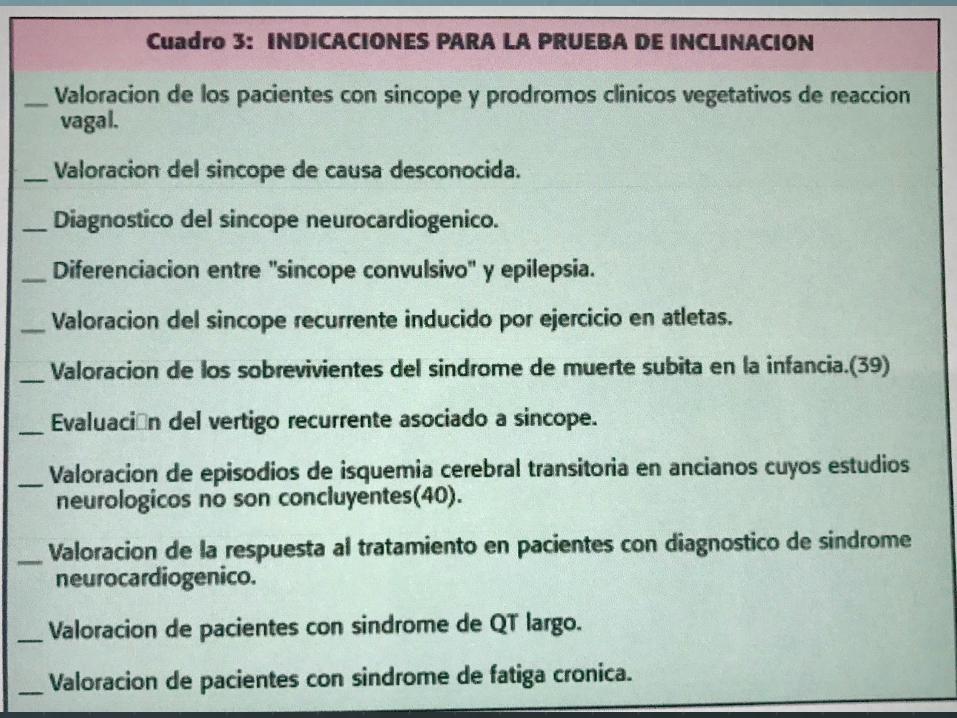
PROTOCOLO PRUEBA DE INCLINACION (“TILT TEST”)
Estudios previos descartando otras causas de síncope.
PREPARACION:
Ayuno de 4 horas
Vía venosa MSI (S. Gluc 5%)
Monitoreo continuo de EKG
Monitoreo de PA
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
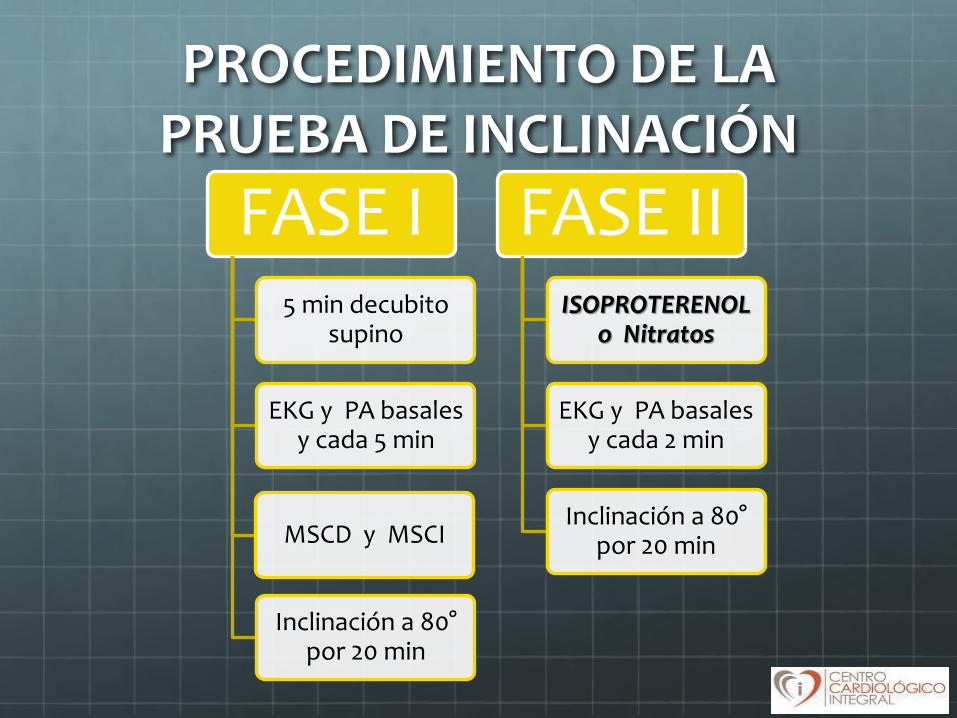
PROCEDIMIENTO DE LA PRUEBA DE INCLINACIÓN
FASE I5 min decubito
supino
EKG y PA basales y cada 5 min
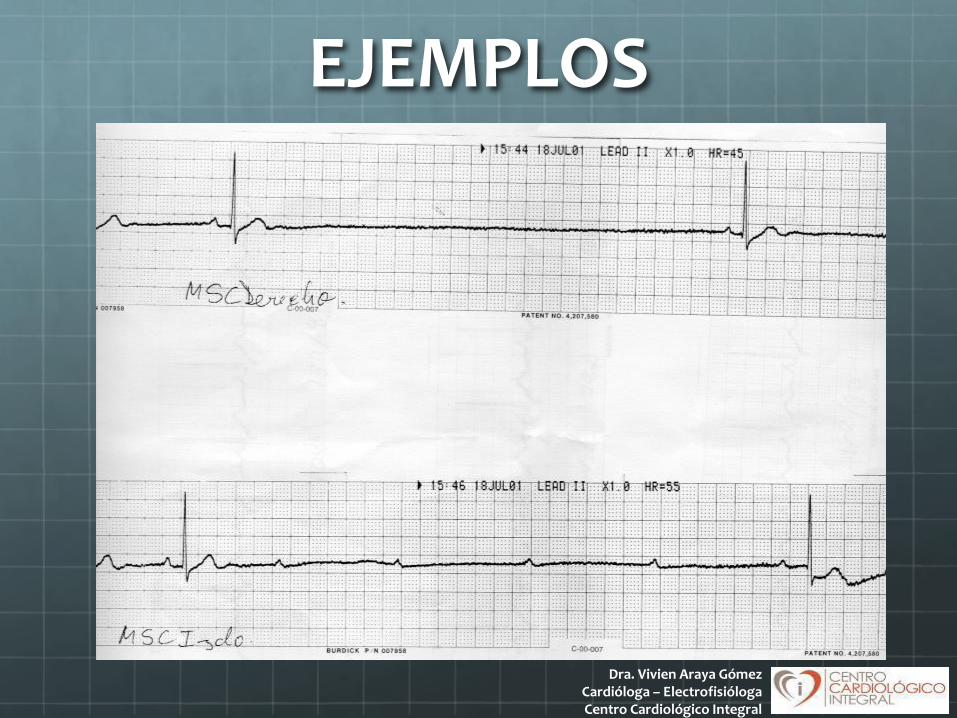
MSCD y MSCI
Inclinación a 80°por 20 min
FASE IIISOPROTERENOL
o Nitratos
EKG y PA basales y cada 2 min
Inclinación a 80°por 20 min

Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral

Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
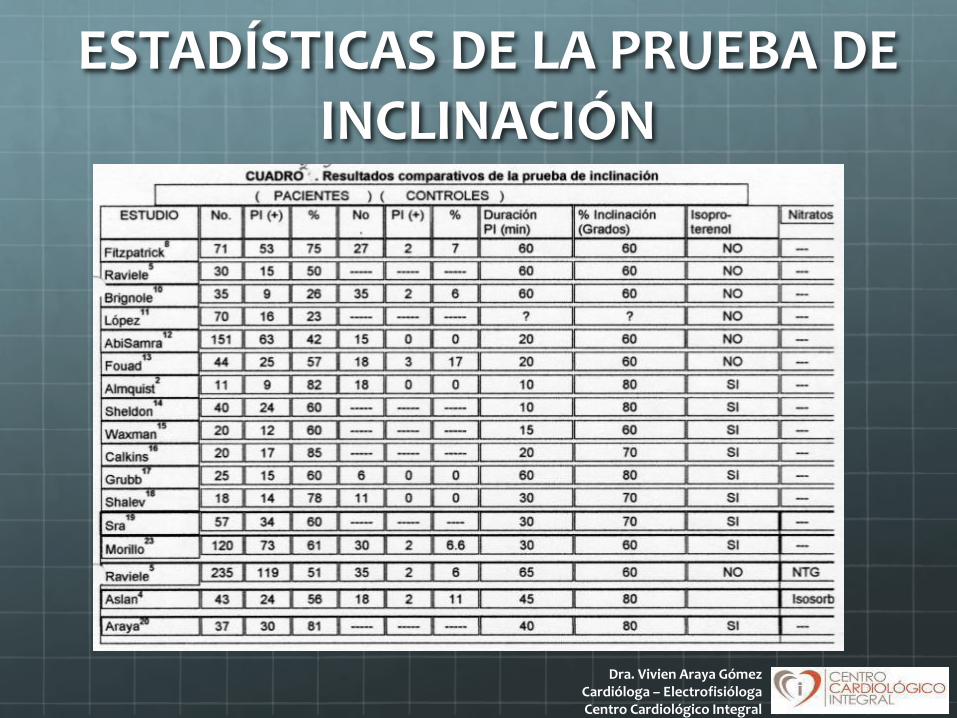
ESTADÍSTICAS DE LA PRUEBA DE INCLINACIÓN
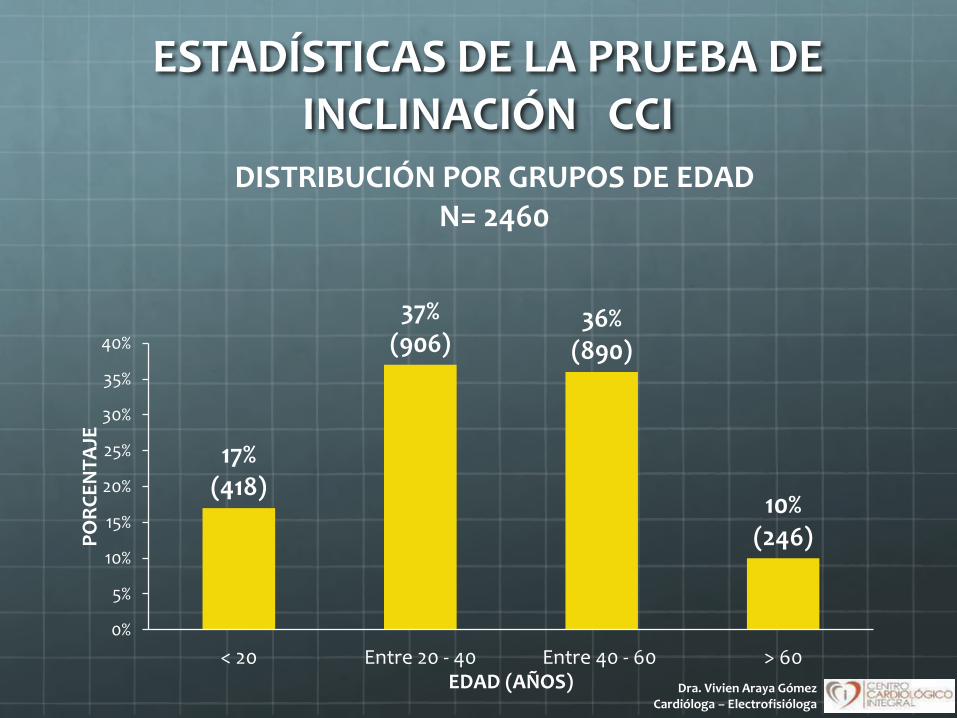
ESTADÍSTICAS DE LA PRUEBA DE INCLINACIÓN CCI
17%(418)
37%(906)
36%(890)
10%(246)
0%
5%
10%
15%
20%
25%
30%
35%
40%
< 20 Entre 20 - 40 Entre 40 - 60 > 60
PO
RC
EN
TA
JE
EDAD (AÑOS)
DISTRIBUCIÓN POR GRUPOS DE EDAD N= 2460
Dra. Vivien Araya GómezCardióloga – Electrofisióloga
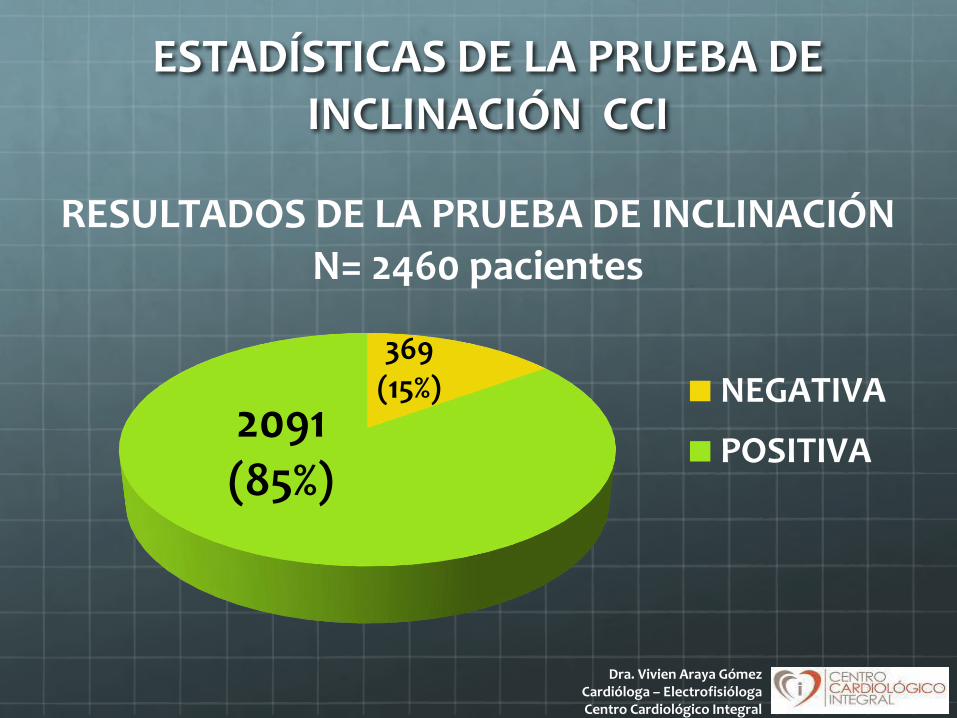
369 (15%)
2091(85%)
RESULTADOS DE LA PRUEBA DE INCLINACIÓN N= 2460 pacientes
NEGATIVA
POSITIVA
ESTADÍSTICAS DE LA PRUEBA DE INCLINACIÓN CCI
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
ESTADÍSTICAS DE LA PRUEBA DE INCLINACIÓN CCI
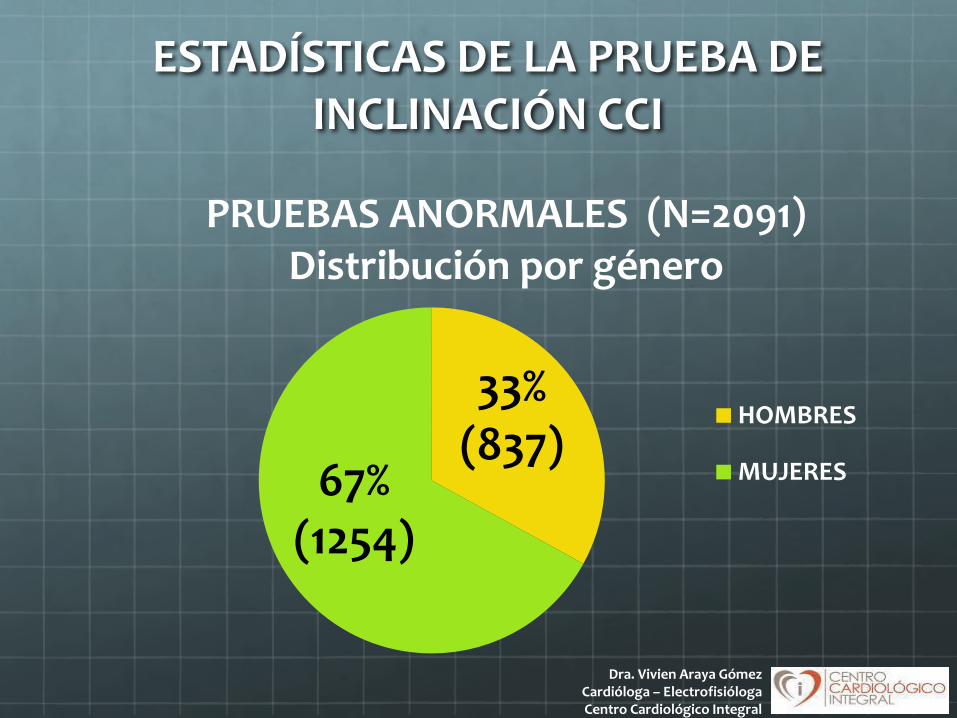
33%(837)
67% (1254)
PRUEBAS ANORMALES (N=2091) Distribución por género
HOMBRES
MUJERES
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral

ESTADÍSTICAS DE LA PRUEBA DE INCLINACIÓN CCI
30%(627)
70%(1464)
PRUEBA DE INCLINACIÓN ANORMAL N= 2091
FASE I
FASE II
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
ESTADÍSTICAS DE LAS PRUEBAS DE INCLINACIÓN ANORMALES - CCI
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
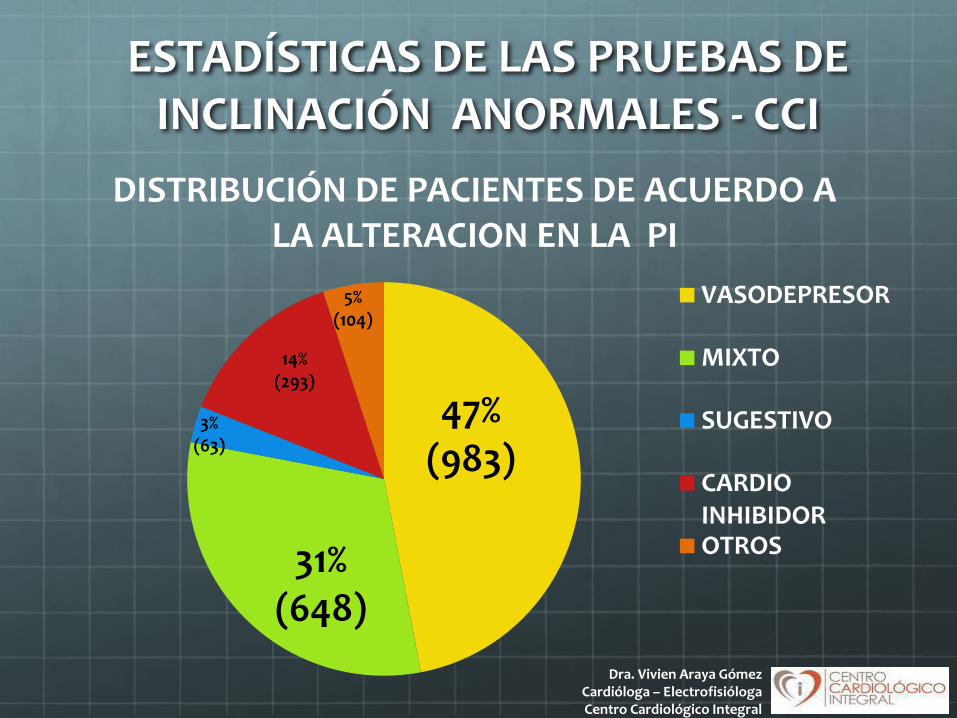
47%(983)
31% (648)
3% (63)
14%(293)
5%(104)
DISTRIBUCIÓN DE PACIENTES DE ACUERDO A LA ALTERACION EN LA PI
VASODEPRESOR
MIXTO
SUGESTIVO
CARDIOINHIBIDOROTROS
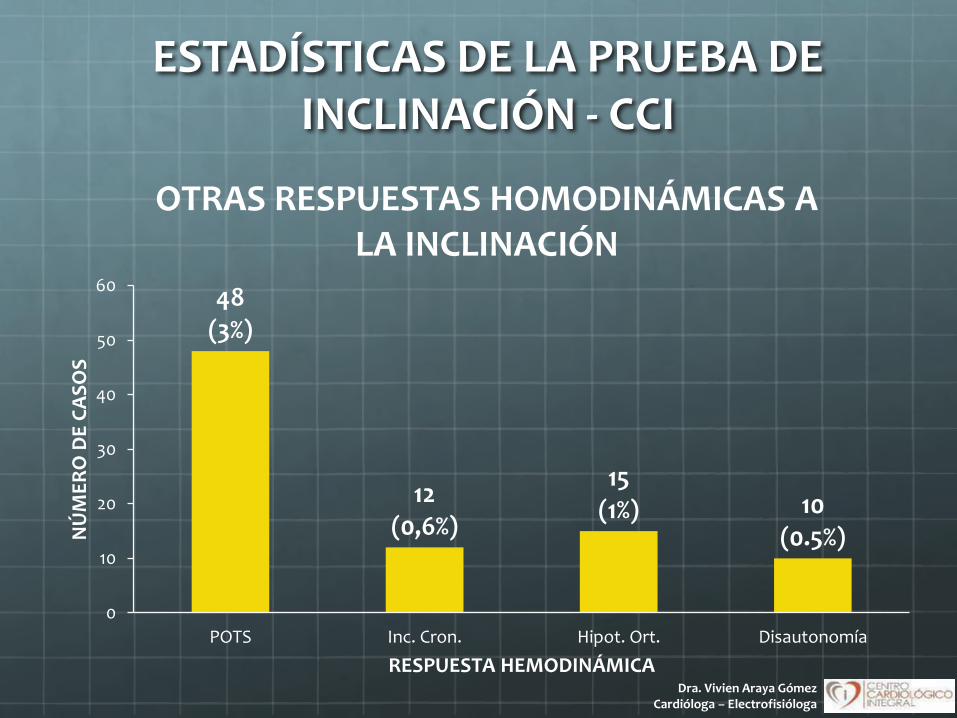
ESTADÍSTICAS DE LA PRUEBA DE INCLINACIÓN - CCI
48 (3%)
12 (0,6%)
15 (1%) 10
(0.5%)
0
10
20
30
40
50
60
POTS Inc. Cron. Hipot. Ort. Disautonomía
NÚ
ME
RO
DE
CA
SO
S
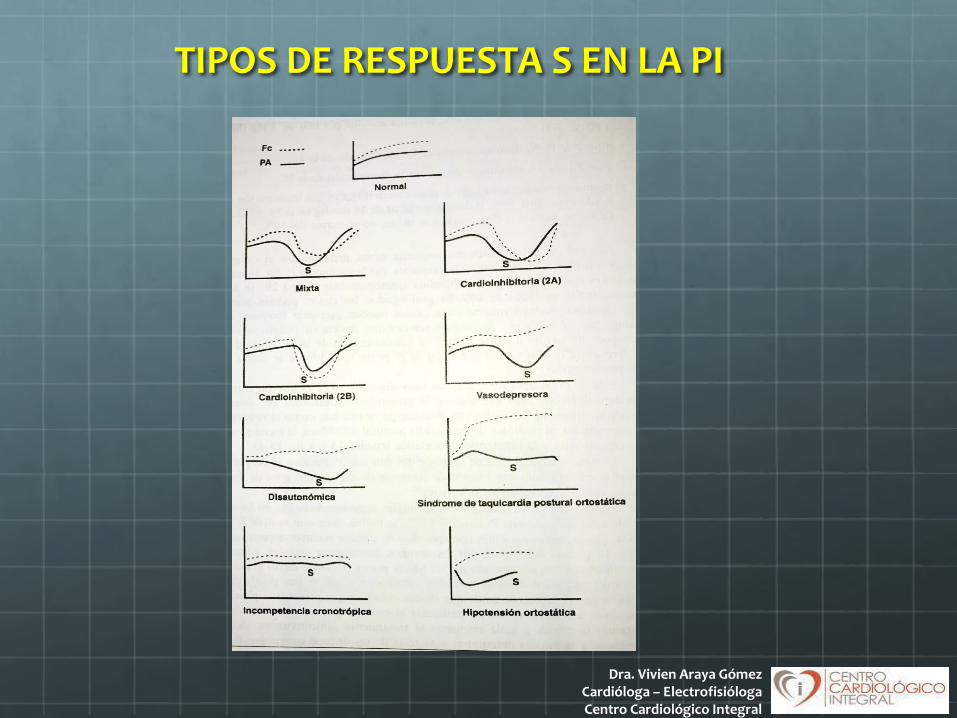
RESPUESTA HEMODINÁMICA
OTRAS RESPUESTAS HOMODINÁMICAS A LA INCLINACIÓN
Dra. Vivien Araya GómezCardióloga – Electrofisióloga
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
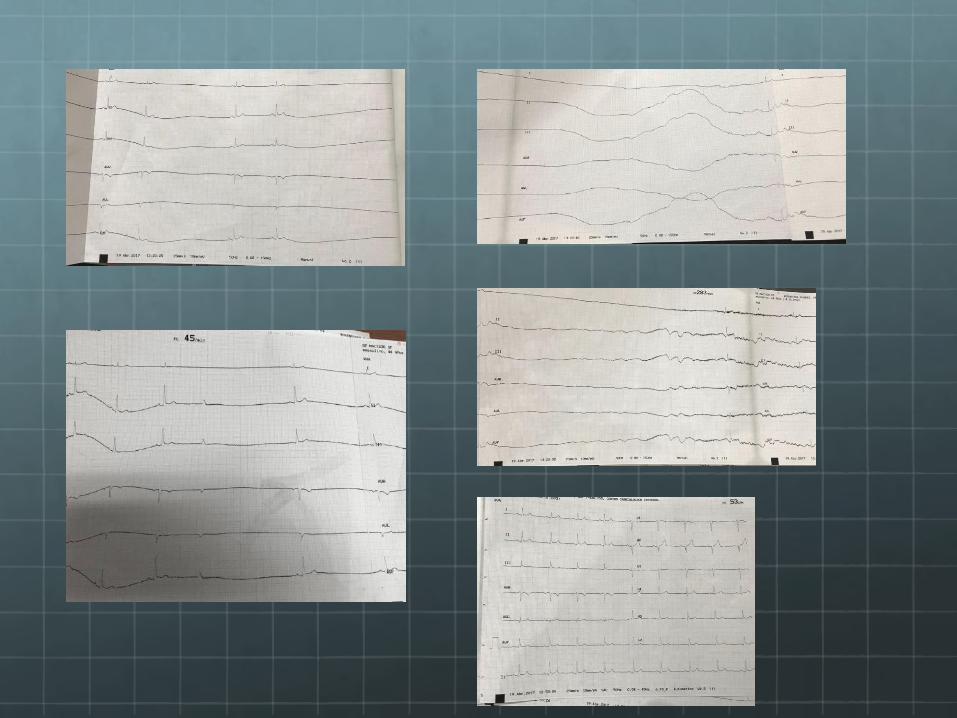
EJEMPLOS
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
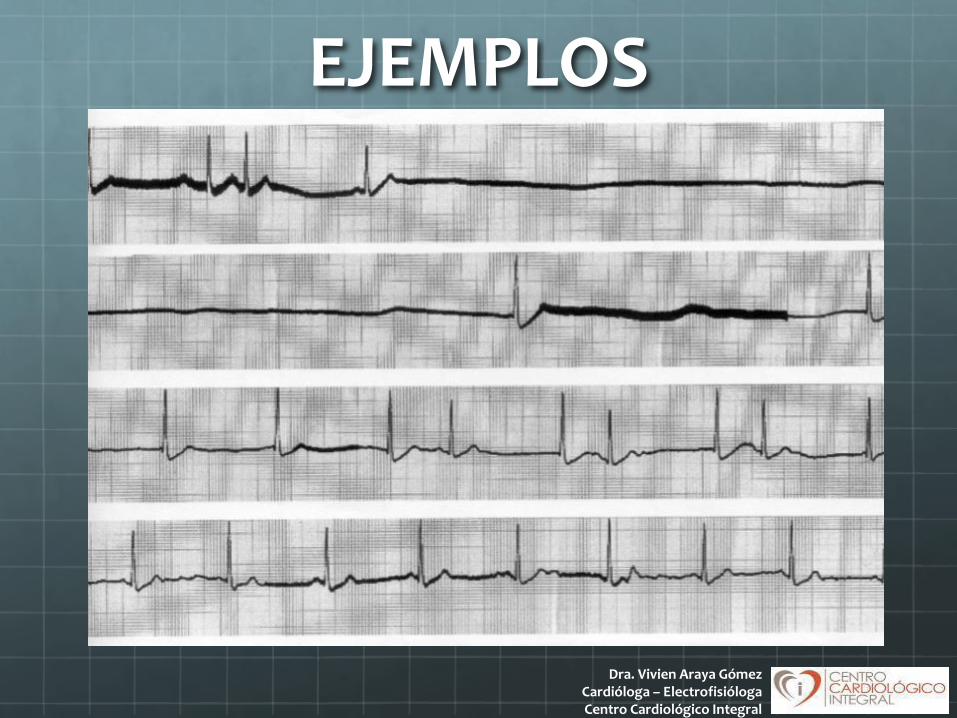
EJEMPLOS

Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
EJEMPLOS
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
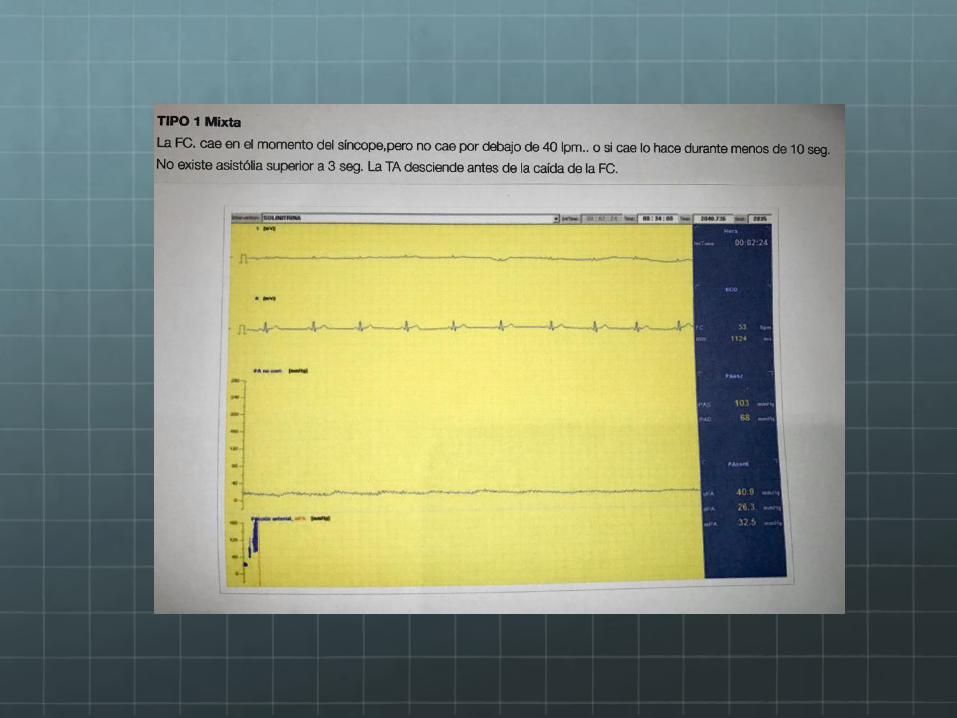
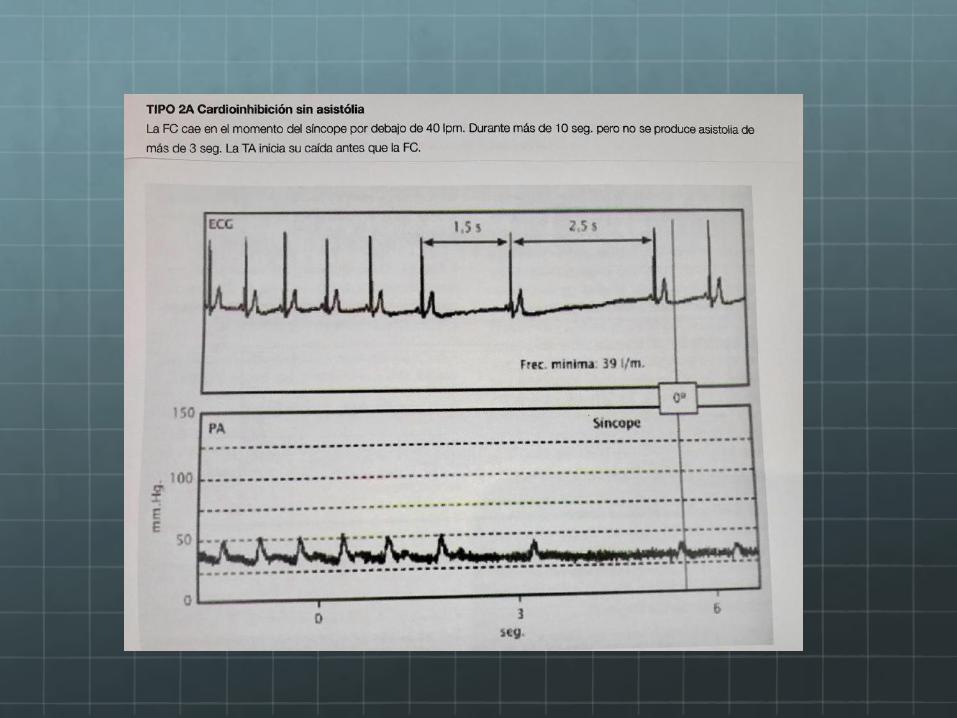
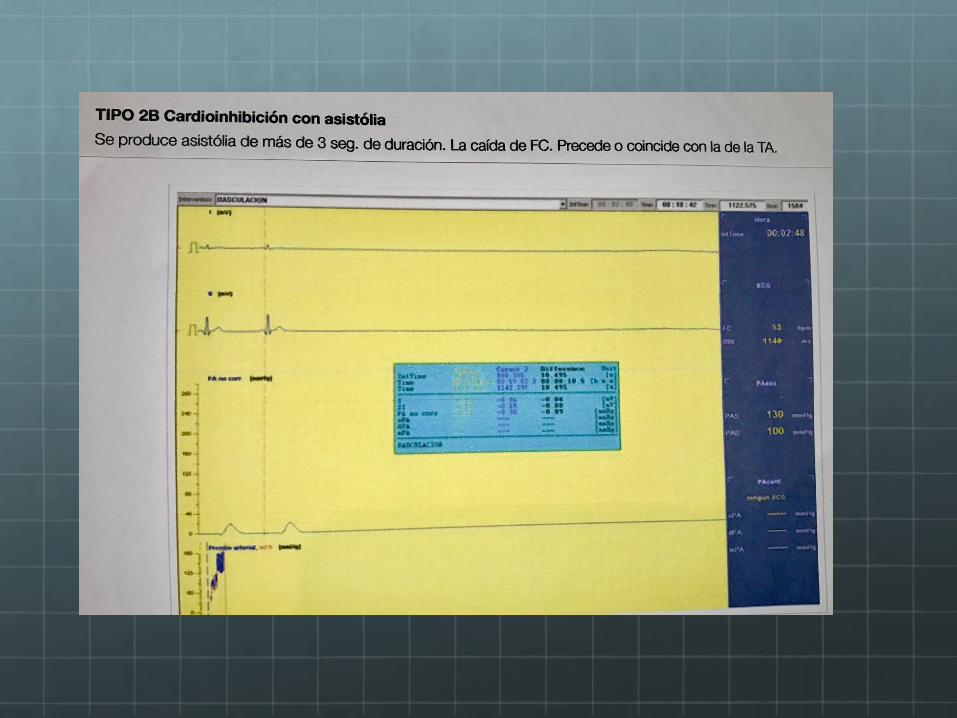
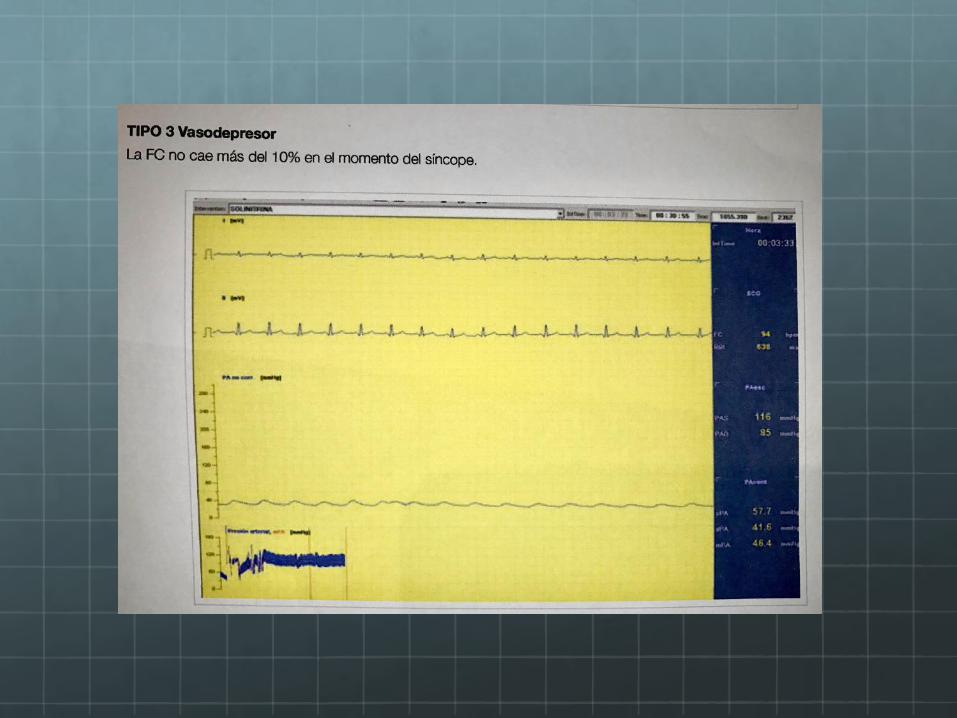
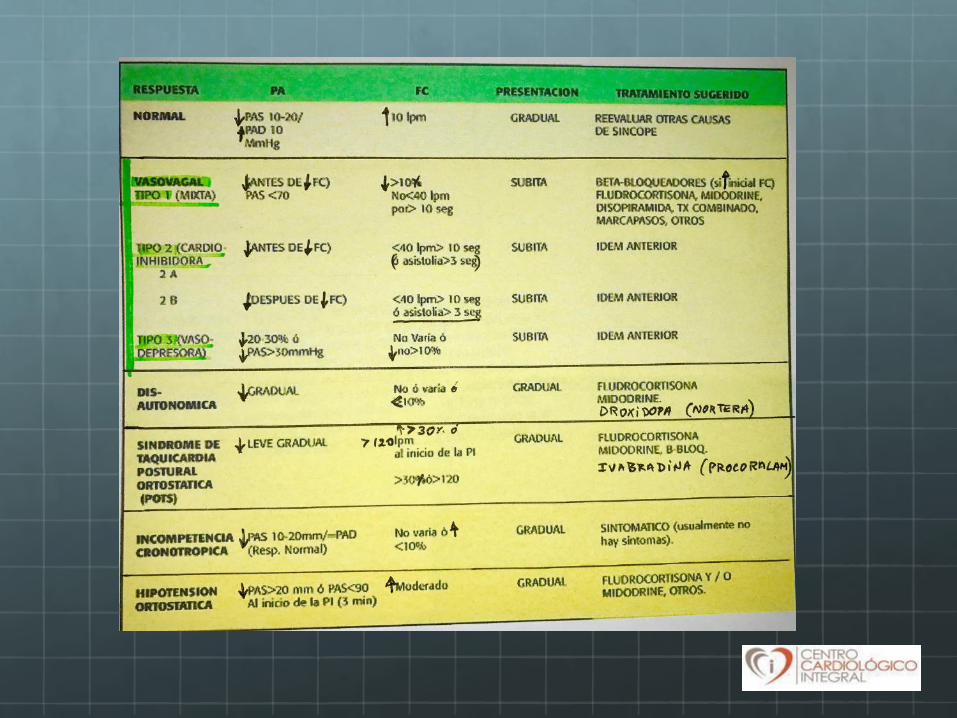
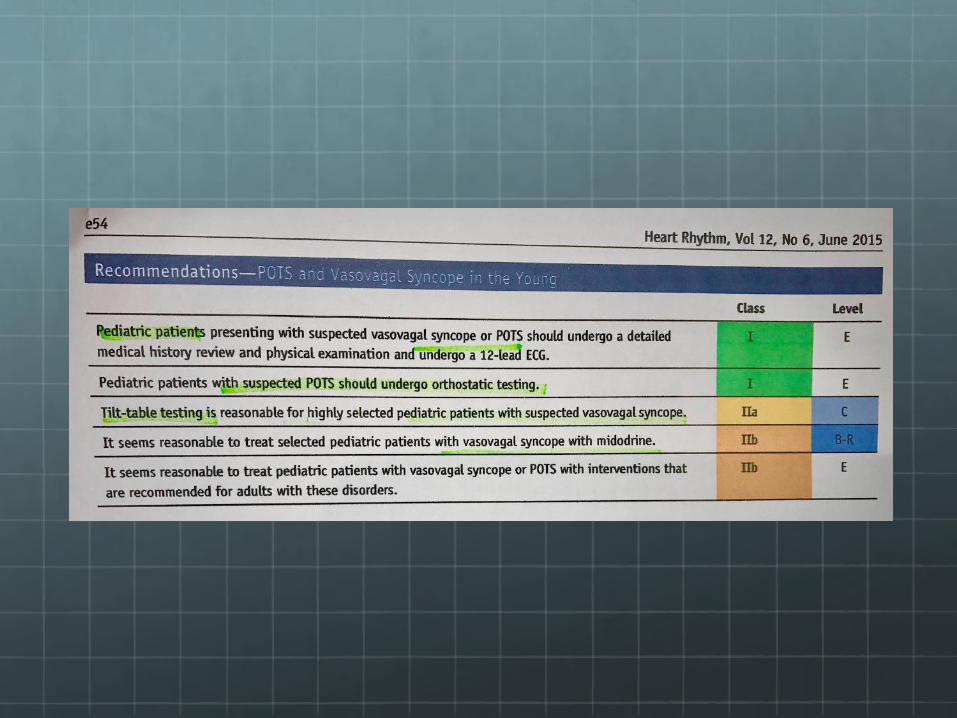
TIPOS DE RESPUESTA S EN LA PI
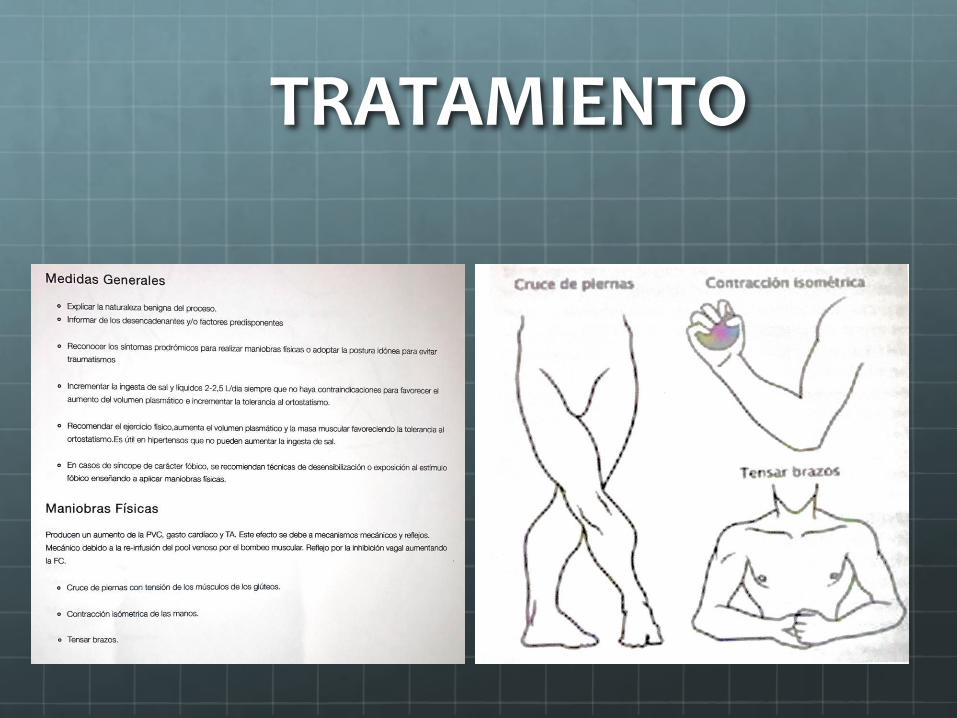
TRATAMIENTO

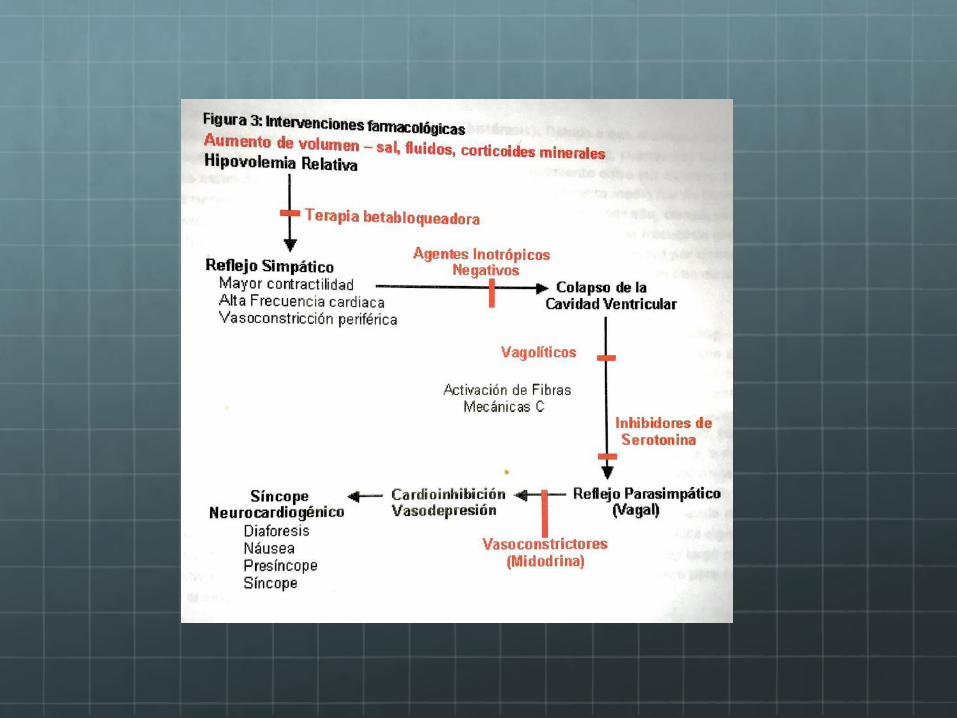
TRATAMIENTO FARMACOLOGICO
A DIFERENTES NIVELES DE LAS VIAS INVOLUCRADAS:
Vía aferente:
Beta bloqueadores (Pindolol, metoprolol, atenolol, propranolol)
Anticolinérgicos
Agentes inotropicos negativos (disopiramida)
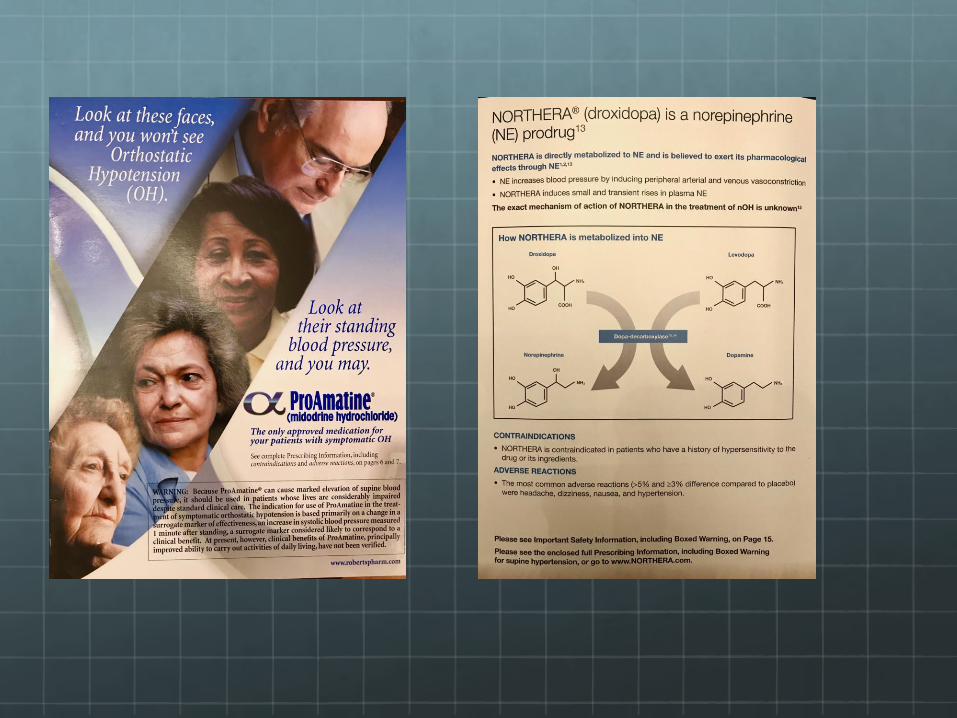
Volumen intravascular : Expansores: florinef (mineralo-corticoides)
Vía eferente:Vagolíticos ( escopolamine or a-agonists- Midodrine))
Dra. Vivien Araya GómezCardióloga – ElectrofisiólogaCentro Cardiológico Integral
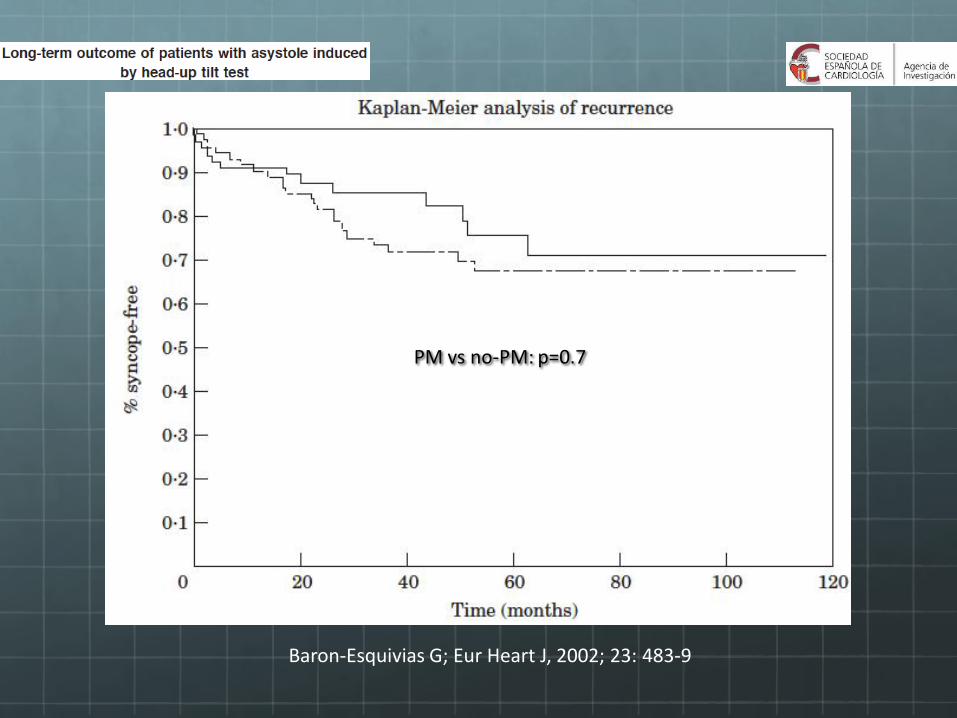
Baron-Esquivias G; Eur Heart J, 2002; 23: 483-9
PM vs no-PM: p=0.7

DDD-CLS vs DDD convencional
Palmisano P et al.
Europace 2012; 14: 1038-43
PM on vs PM off
INVASY
Ochetta E. et al.
Europace 2004; 6: 538-47
DDD-CLS inVVS
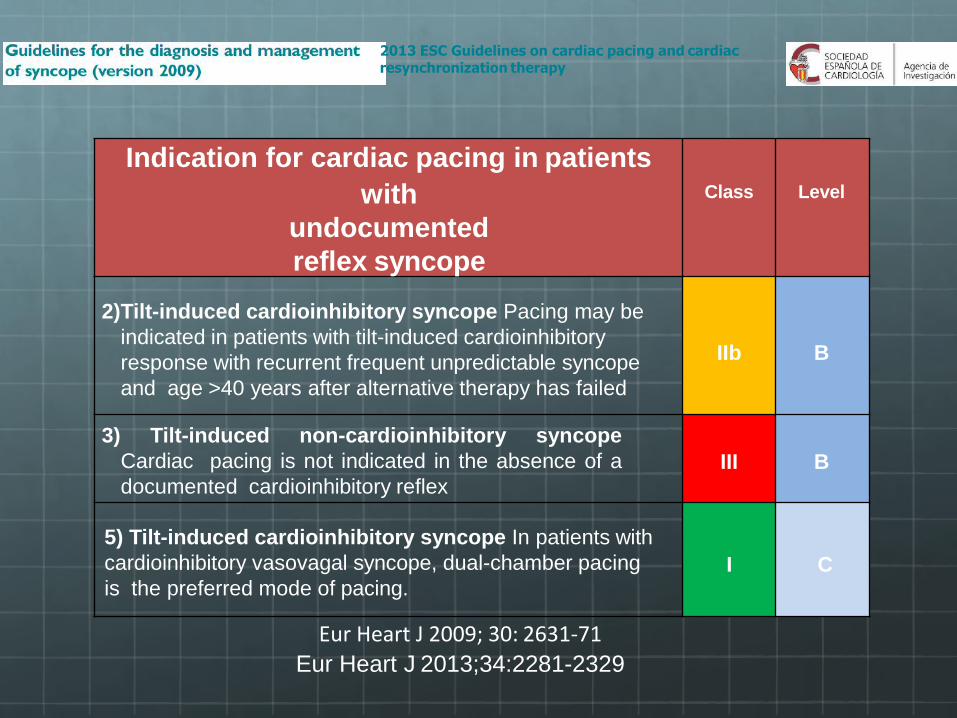
Eur Heart J 2009; 30: 2631-71
Eur Heart J 2013;34:2281-2329
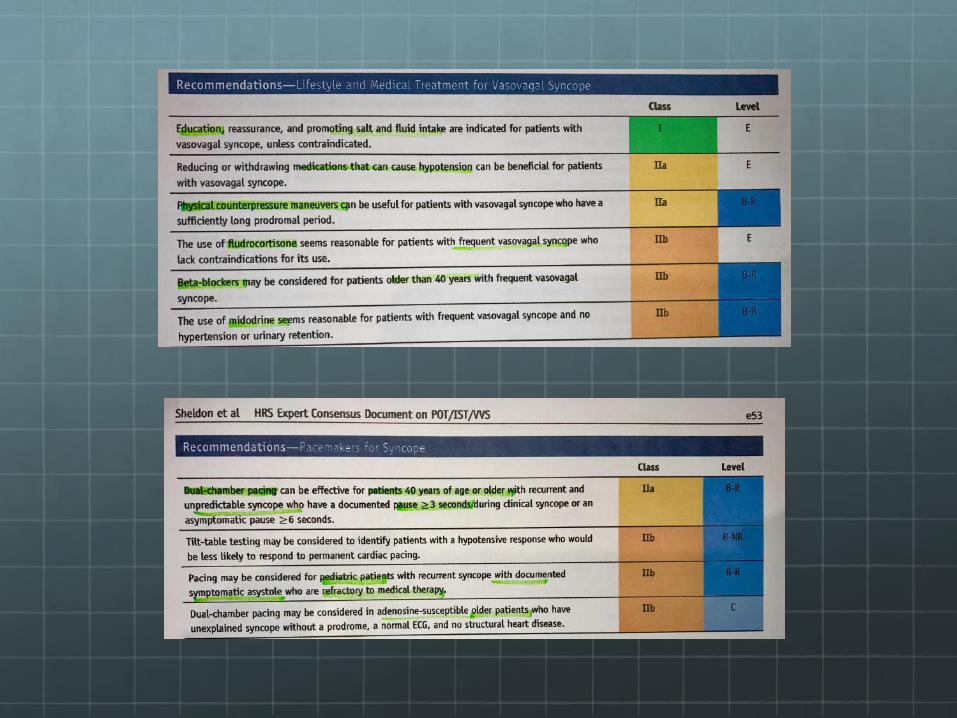
Indication for cardiac pacing in patients
with
undocumented
reflex syncope
Class Level
2)Tilt-induced cardioinhibitory syncope Pacing may be
indicated in patients with tilt-induced cardioinhibitory
response with recurrent frequent unpredictable syncope
and age >40 years after alternative therapy has failed
IIb B
3) Tilt-induced non-cardioinhibitory syncope
Cardiac pacing is not indicated in the absence of a
documented cardioinhibitory reflexIII B
5) Tilt-induced cardioinhibitory syncope In patients with
cardioinhibitory vasovagal syncope, dual-chamber pacing
is the preferred mode of pacing.I C
2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy
Randomized Placebo Controlled Trial of Closed Loop Stimulation in Recurrent Reflex Vasovagal Syncope. SPAIN Study.
Gonzalo Baron-Esquivias MD, PhD, FESC. Carlos A. Morillo,
MD, FRCPC, FACC, FHRS, FESC
Angel Moya-Mitjans MD, PhD, FESC
Jesus Martinez-Alday MD, PhD Ricardo Ruiz-
Granell MD, PhD Javier Lacunza-Ruiz MD.
Roberto Garcia-Civera MD, PhD
Encarnacion Gutierrez-Carretero MD, PhD Rafael Romero-
Rodriguez MD
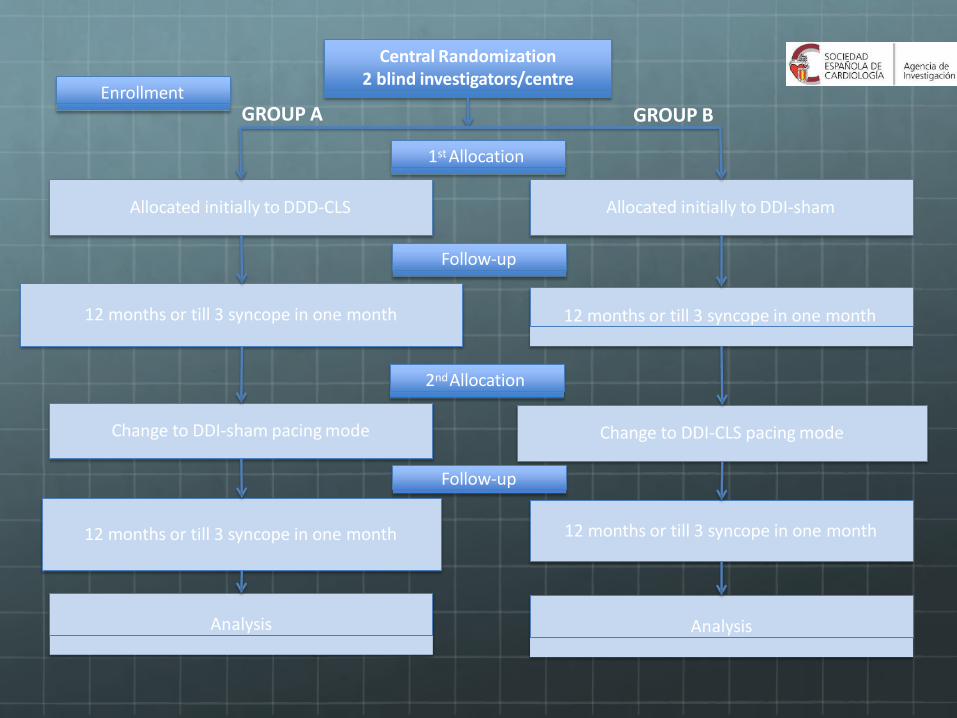
Central Randomization2 blind investigators/centre
Enrollment
Allocated initially to DDD-CLS Allocated initially to DDI-sham
12 months or till 3 syncope in one month 12 months or till 3 syncope in one month
.
Change to DDI-sham pacing mode Change to DDI-CLS pacing mode
1st Allocation
Follow-up
12 months or till 3 syncope in one month 12 months or till 3 syncope in one month
Follow-up
2ndAllocation
Analysis Analysis
GROUP A GROUP B
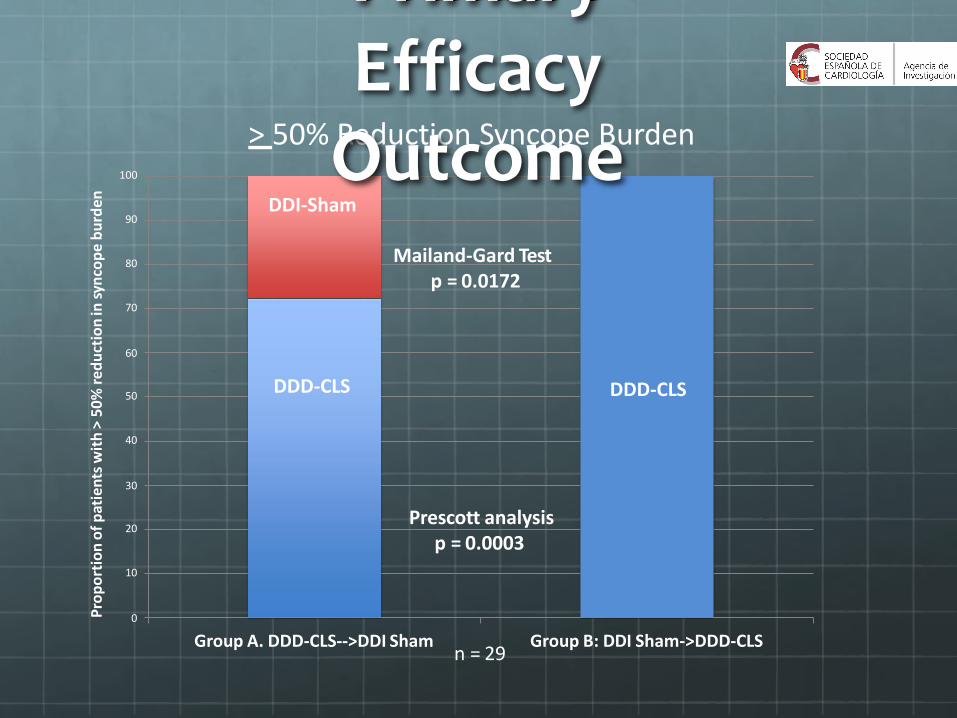
10
0
20
40
30
50
70
60
80
90
100
Group A. DDD-CLS-->DDI Sham Group B: DDI Sham->DDD-CLS
> 50% Reduction Syncope Burden
Pro
po
rtio
no
fp
atie
nts
wit
h>
50
% r
ed
uct
ion
in s
ynco
pe
bu
rde
n
n = 29
DDI-Sham
DDD-CLS DDD-CLS
Primary Efficacy
OutcomeMailand-Gard Test
p = 0.0172
Prescott analysisp = 0.0003
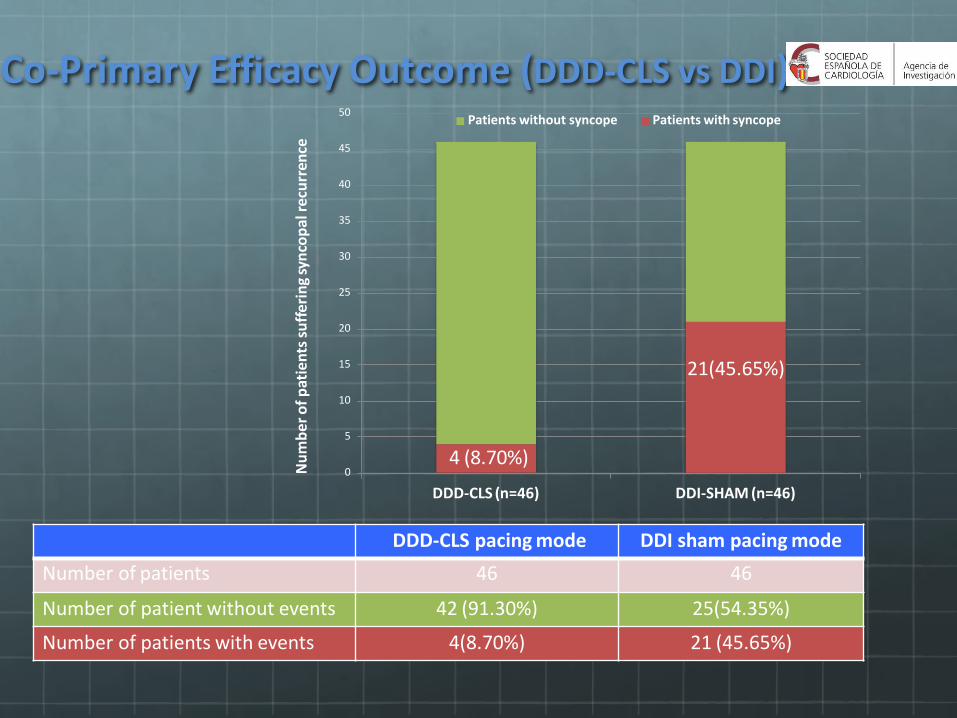
Co-Primary Efficacy Outcome (DDD-CLS vs DDI)
0
5
10
15
20
25
30
35
40
45
50
DDD-CLS (n=46) DDI-SHAM (n=46)
Patients without syncope Patients with syncope
Nu
mb
er
of
pat
ien
tssu
ffer
ing
syn
cop
alre
curr
ence
4 (8.70%)
21(45.65%)
DDD-CLS pacing mode DDI sham pacing mode
Number of patients 46 46
Number of patient without events 42 (91.30%) 25(54.35%)
Number of patients with events 4(8.70%) 21 (45.65%)

CERRO ENA 2017
MUCHAS GRACIAS
www.centrocardiologico.com
[email protected]. Vivien Araya Gómez
Cardióloga – ElectrofisiólogaCentro Cardiológico Integral















![[PPT]INOTROPICOS · Web viewCONTRACCIÓN CARDÍACA Esecalcioliberado del retículosarcoplásmico se uneentonces a la tropinina C lo cual genera un cambioconformacional en el complejoreguladorqueconlleva](https://static.fdocuments.ec/doc/165x107/5bab5ca109d3f2ca018bd6f4/pptinotropicos-web-viewcontraccion-cardiaca-esecalcioliberado-del-reticulosarcoplasmico.jpg)