
¿Preocupados por el Estreñimiento · Web viewThe term hormone is derived from the Greek word,...
98
¿Preoccupations por el Estreñimiento? Prácticamente todas las personas sufren alguna vez de estreñimiento. Generalmente no es grave. Para evitar la mayoría de los problemas de estreñimiento es necesario conocer sus causas, cómo prevenirlo y cómo tratarlo. El estreñimiento es un síntoma no una enfermedad. Usted puede estar estreñido si hace menos deposiciones de las acostumbradas, con heces largas o duras. Las personas mayores son más propensas al estreñimiento que los jóvenes. Los expertos opinan que las personas mayores con frecuencia se preocupan demasiado si no hacen una deposición diaria, pero no hay un número regular de deposiciones diarias o semanales. La regularidad varía según las personas: para algunas personas puede ser normal hacer dos deposiciones diarias; para otras, solo dos deposiciones por semana es normal. Preguntas para Responderse Algunos médicos sugieren que responda estas preguntas para saber si usted sufre de estreñimiento: ¿Frecuentemente hace usted menos de tres deposiciones semanales? ¿Tiene usted a menudo dificultad para hacer su deposición? ¿Siente dolor? ¿Tiene otros problemas tales como sangrado? Si contestó “sí” a más de una de estas preguntas, usted puede tener un problema de estreñimiento. De lo contrario, usted probablemente no tiene problemas. ¿Cuáles son las Causas del Estreñimiento? 1
Transcript of ¿Preocupados por el Estreñimiento · Web viewThe term hormone is derived from the Greek word,...
¿Preoccupations por el Estreñimiento?
Prácticamente todas las personas sufren alguna vez de estreñimiento. Generalmente no es grave. Para evitar la mayoría de los problemas de estreñimiento es necesario conocer sus causas, cómo prevenirlo y cómo tratarlo.
El estreñimiento es un síntoma no una enfermedad. Usted puede estar estreñido si hace menos deposiciones de las acostumbradas, con heces largas o duras. Las personas mayores son más propensas al estreñimiento que los jóvenes.
Los expertos opinan que las personas mayores con frecuencia se preocupan demasiadosi no hacen una deposición diaria, pero no hay un número regular de deposiciones diarias o semanales. La regularidad varía según las personas: para algunas personas puede ser normal hacer dos deposiciones diarias; para otras, solo dos deposiciones por semana es normal.
Preguntas para Responderse
Algunos médicos sugieren que responda estas preguntas para saber si usted sufre de estreñimiento:
¿Frecuentemente hace usted menos de tres deposiciones semanales? ¿Tiene usted a menudo dificultad para hacer su deposición?
¿Siente dolor?
¿Tiene otros problemas tales como sangrado?
Si contestó “sí” a más de una de estas preguntas, usted puede tener un problema de estreñimiento. De lo contrario, usted probablemente no tiene problemas.
¿Cuáles son las Causas del Estreñimiento?
Los médicos no siempre saben cuales son las causas del estreñimiento. Consumir una dieta inapropiada, no beber suficiente agua o el uso frecuente de laxantes pueden ser las causas. Algunas medicinas también pueden causar estreñimiento, entre las que se encuentran algunos antidepresivos, antiácidos que contienen aluminio o calcio, antihistamínicos, diuréticos y medicinas para el mal de Parkinson.
La importancia de la dieta. Las personas que no consumen alimentos con alto contenido de fibra, como verduras, frutas y granos integrales, pueden sufrir de estreñimiento. Algunas investigaciones demuestran que las dietas con alto contenido de fibra pueden ayudar a prevenir el estreñimiento. Consumir cantidades de carne rica en grasa, productos lácteos y huevos, postres cremosos, grasosos y caramelos muy dulces pueden también producir estreñimiento.
1

Las personas que viven solas a veces pierden el interés en cocinar y comer, y como consecuencia, empiezan a consumir muchos alimentos preparados fuera de casa. Estos alimentos generalmente tienden a ser bajos en fibra y por lo tanto pueden producir estreñimiento. Además, la mala dentadura puede hacer que las personas mayores escojan alimentos blandos, procesados que contienen muy bajas cantidades de fibra.
Algunas veces las personas no toman suficiente líquido. Frecuentemente esto sucede cuando las personas no comen con regularidad. El agua y los líquidos son importantes, porque le dan volumen a la deposición haciéndola más fácil.
Mal uso de laxantes y enemas. Muchas personas piensan que los laxantes son una cura para el estreñimiento. Pero el uso excesivo de laxantes la mayoría de las veces no es necesario y puede crear hábito. Si usted usa laxantes con demasiada frecuencia, su cuerpo puede empezar a depender de ellos para hacer la deposición. (El uso excesivo de laxantes puede también causar diarrea). Con el paso del tiempo su cuerpo olvidará cómo trabajar sin ayuda.
Por esta misma razón, si Usted usa enemas con demasiada frecuencia, su cuerpo puede empezar a depender de ellos. Usar demasiados enemas puede impedirle hacer las deposiciones normales. El uso excesivo de aceite mineral, otro laxante popular, puede disminuir la habilidad de su cuerpo para utilizar vitaminas fundamentales (A, D, E y K). Algunas veces el aceite mineral, si se utiliza con otras drogas que evitan la coagulación de la sangre (anticoagulantes), puede causar efectos secundarios no deseados.
Otras causas del estreñimiento. La falta de ejercicio o las largas permanencias en la cama, como las causadas por accidentes o enfermedades, pueden producir estreñimiento. Algunas veces los médicos prescriben medicinas para las personas que permanecen en la cama y padecen de estreñimiento crónico, pero en la medida de lo posible es mejor tener más actividad.
Algunas personas pueden estreñirse también si hacen caso omiso a su impulso natural parahacer una deposición. Algunos prefieren hacer sus deposiciones en casa solamente, pero contener una deposición puede causar estreñimiento si la espera es demasiado larga.
En algunas personas, los problemas o bloqueos en el intestino pueden causarles estreñimiento. Estos problemas pueden afectar los músculos o los nervios responsables de los movimientos normales del intestino. Un médico puede realizar pruebas para ver si el estreñimiento es producido por un problema de este tipo. Si este es el caso, el problema generalmente puede ser tratado.
Tratamiento
Si usted sufre de estreñimiento, primero consulte con su médico para descartar un problema más serio. Si los resultados no muestran ninguna enfermedad o bloqueo,y si su médico está de acuerdo, ensaye los siguientes remedios:
2
Aumente el consumo de fibra comiendo más frutas y verduras frescas, crudas o cocinadas, y más cereales y panes de granos integrales. Las frutas secas, tales como los albaricoques, las ciruelas y los higos, son especialmente ricos en fibra.
Tome muchos líquidos (1 a 2 litros diariamente), a menos que Usted tenga problemas cardiacos, circulatorios o renales. (Tenga en cuenta que algunas personas pueden estreñirse al tomar grandes cantidades de leche.)
Algunos médicos recomiendan que se agregue pequeñas cantidades de salvado integral a los alimentos horneados, a los cereales y a las frutas. Algunas personas padecen de inflamaciones y gases durante varias semanas después de agregar el salvado a sus dietas. Haga los cambios en su dieta lentamente para permitir que su sistema digestivo se adapte. Recuerde que si su dieta está bien balanceada y contiene suficientes alimentos con alto contenido de fibra natural, no es necesario agregarle el salvado a otros alimentos.
Manténgase activo.
No espere tener deposiciones diarias o cada tercer día. Recuerde, que ser regular es diferente para cada persona. Si sus deposiciones son regulares y sin dolor (puedenser 2 veces por día o 3 veces por semana), usted probablemente no sufre de estreñimiento.
Si usted todavía está preocupado por el estreñimiento, pregúntele a su médico que debe hacer.
Recursos
Usted puede conseguir más información sobre el estreñimiento en:
The National Digestive Diseases Information Clearinghouse(Centro Nacional de Información sobre Enfermedades Digestivas) 2 Information WayBethesda, MD 20892-35701-800-891-5389 301-654-3810Correo Electrónico: [email protected]://www.niddk.nih.gov
Para más información sobre la salud y el envejecimiento, llame o escriba a:
3

The National Institute on Aging Information Center(Centro de Información del Instituto Nacional Sobre el Envejecimiento )P.O. Box 8057Gaithersburg, MD 20898-80571-800-222-22251-800-222-4225 (TTY)Correo Electrónico: [email protected]://www.nia.nih.gov
National Institute on AgingU. S. Department of Health and Human ServicesNational Institutes of HealthEnero 2002
4
Medicamentos: Úselos con Cuidado
Las personas mayores de 65 años de edad usan más medicamentos y más remedios sin receta que las personas de otras edades. Las personas mayores tienden a padecer de más enfermedades crónicas de largo plazo — tales como artritis, diabetes, hipertensióny dolencas cardíacas — que la gente más joven. Es común que las personas mayores tomen diferentes medicamentos a la vez por que tienen más de una enfermedad o incapacidad al mismo tiempo.
Muchos de ellos deben en parte su buena salud a los nuevos y mejores medicamentos y vacunas, pero el uso de los mismos puede ser más arriesgado para ese grupo de personas, especialmente cuando usan varios medicamentos a la vez. Tomar varios medicamentos esno siempre fácil y correcto. Puede ser difícil recordar para qué es cada remedio y como y cuando se debe tomar, sobre todo para las personas con problemas de memoria o demencia.
Los medicamentos pueden actuar de manera diferente en las personas mayores que en la gente más joven. Esto puede ser causado debido a los cambios normales que suceden en elcuerpo con la edad. Por ejemplo, al envejecer, el cuerpo humano va perdiendo agua y tejido magro (principalmente músculos) y agrega más tejido adiposo. Esto puede hacer que sea diferente el lapso de tiempo que tarda el cuerpo en absorber el fármaco.
Los riñones y el hígado son dos órganos importantes que procesan y eliminan la mayoría de las medicinas del cuerpo. Al envejecer, estos órganos pueden no funcionar tan bien como lo hacían y el cuerpo puede demorarse más en eliminar los medicamentos.
Tenga presente que la palabra “drogas” puede significar tanto los fármacos o medicamentos recetados por su médico como los remedios que compra en la farmacia sin receta. Estos últimos pueden incluir las vitaminas, minerales, suplementos de hierbas y dietéticos, laxantes, remedios para el resfrío y antiácidos. Tomar estos remedios sin receta al mismo tiempo que alguno que haya recetado el médico puede provocar serios problemas. Por ejemplo, no se debe tomar aspirina (ácido acetilsalicílico) junto con warfarina (Coumadin). Cerciórese de que su médico sepa qué remedios está tomando usted y que le asegure que no hay riesgo en tomar esas medicinas al mismo tiempo. Pregúntele también si debe tomarse los remedios con las comidas. Por ejemplo, si toma alendronato (Fosamax) con la comida, éste será menos eficaz.
Los suplementos de hierbas también deben tomarse con cuidado. El gingko biloba, por ejemplo, no se debe tomar con aspirina, acetaminofén, warfarina o diuréticos tiazídicos, pues puede causar un aumento de la presión arterial y acarrear el riesgo de una hemorragia.
Usted y su familia deben estar informados sobre las medicinas que toman y sus posibles efectos colaterales. Recuerde que los medicamentos que tienen el suficiente poder para
5

curarle, pueden también ser muy potentes para lesionarlo, si usted no los utiliza correctamente. A continuación le damos algunas sugerencias para ayudarle a evitar riesgos y obtener mejores resultados con sus medicamentos.
En el hogar
Mantenga un registro diario de todas las medicinas que toma. Incluya tanto los fármacos recetados por el médico como los remedios sin receta. Anote el nombre de cada medicamento, del médico que lo recetó, la dosis y el horario en que lo toma. Guarde una copia en su botiquín y otra en su cartera.
Lea y guarde toda la información que venga con la medicina.
Fíjese en la etiqueta del medicamento antes de tomarlo para cerciorarse que es parala persona indicada — usted — con las instrucciones precisas que recetó su médico.
Tome la medicina en la dosis exacta y el horario preciso que su médico le recetó.
Revise en los frascos la fecha de vencimiento de sus medicinas y deseche los medicamentos que estén vencidos.
Llame inmediatamente a su médico si tiene cualquier problema con los medicamentos o si le preocupa que el medicamento pueda estarle causando más mal que bien. El médico puede cambiarle el medicamento por otro que sirva para la misma dolencia y que no le haga daño.
No tome medicinas recetadas para otras personas ni dé sus medicamentos a otras personas.
No interrumpa el tratamiento farmacológico hasta que el médico le diga que puedehacerlo, aunque usted se esté sintiendo mejor.
No tome más ni menos de la cantidad recetada de un medicamento.
No mezcle alcohol y medicamentos, a menos que su médico le diga que puede hacerlo. Algunas medicinas pueden no funcionar o pueden causar alguna enfermedad si se toma alcohol mientras las consume.
En el Consultorio
Estudie su expediente farmacológico con el médico o la enfermera en cada consulta y siempre que el médico le recete nuevos medicamentos. El médico puede tener alguna nueva información sobre sus medicinas que pueden ser importantes para usted.
6

Informe siempre a su médico o a la enfermera sobre todos los problemas que haya tenido con los medicamentos, tales como irritaciones en la piel, indigestión, mareos o falta de apetito.
Pregunte al médico o la enfermera sobre la manera correcta de tomarse los medicamentos antes de comenzar a tomarlos.
Haga todas estas preguntas (y anote las respuestas) antes de salir del consultorio:
– ¿Cuál es el nombre del medicamento y por qué debo tomarlo? – ¿Qué nombre tiene la condición clínica que trata este medicamento? – ¿Cómo funciona este medicamento en mi organismo? – ¿Con qué frecuencia debo tomarlo? – ¿Cuánto tiempo demora en hacer efecto? – ¿Cómo puedo saber si el medicamento está haciendo efecto? – ¿Cómo debo esperar sentirme cuando comience a tomarlo? – ¿Cuándo debo tomarlo? ¿Cuándo lo necesito? ¿Antes, durante o después de las comidas? ¿A la hora de acostarme? – Si se me olvida tomarlo, ¿qué debo hacer? – ¿Qué efectos secundarios puedo esperar? ¿Debo informarle al médico? – ¿Cuánto tiempo debo tomar el medicamento? – ¿Puedo tomar este medicamento con otras medicinas que yo estoy tomando? (Recetadas, sin receta, suplementos dietéticos o de hierbas) – Si yo no tomo medicamentos, ¿hay alguna otra cosa que pueda aliviarme también?
En la Farmacia
Cerciórese que usted puede leer y entender el nombre del medicamento y las instrucciones en el envase. Si es difícil leer las instrucciones, pídale al farmacéutico que use letras más grandes. Comuníquele al farmacéutico si usted tiene dificultad para abrir el frasco de medicamento.
Revise bien, antes de salir de la farmacia, que en la etiqueta de su medicamento diga que es para la persona correcta — Usted — y que tenga las instrucciones correctas que el médico le recetó. En el caso contrario, avise al farmacéutico.
Recursos
U.S. Food and Drug Administration (FDA)(Administración de Drogas y Alimentos – FDA)5600 Fishers LaneHFD - 210Rockville, Maryland 208571-888-INFOFDA(1-888-463-6332)
7

http://www.fda.govEl FDA tiene más información sobre el uso seguro de medicamentos.
Peter Lamy Center for Drug Therapy and Aging(Centro Peter Lamy para la Terapia de Drogas y el Envejecimiento)University of MD School of Pharmacy(Escuela de Parmacia de la Universidad de Maryland)515 West Lombard Street, First FloorBaltimore, Maryland 21201410-706-2434 (en Maryland) o1-877-706-2434 (para llamadas gratis fuera de Maryland)http://www.pharmacy.umaryland.edu/lamyEl Centro tiene folletos e información en inglés sobre el uso de medicamentos para las personas de la tercera edad.
Para recibir el folleto Talking with Your Doctor: A Guide for Older People y más información gratis sobre la salud y el envejecimiento, contacte a:
National Institute on Aging Information Center(Centro de Información del Instituto Nacional Sobre el Envejecimiento)P.O. Box 8057Gaithersburg, Maryland 20898-80571-800-222-22251-800-222-4225 (TTY)http://www.nia.nih.gov
Instituto Nacional Sobre el EnvejecimientoDepartamento de Salud y Servicos Humanos de los Estados UnidosInstitutos Nacionales de SaludJulio de 2003
8

Alzheimer's Disease Medications Fact Sheet
Medications Summary Table
Five prescription drugs currently are approved by the U.S. Food and Drug Administration to treat people who have been diagnosed with Alzheimer's disease (AD). Treating the symptoms of AD can provide patients with comfort, dignity, and independence for a longer period of time and can encourage and assist their caregivers as well. It is important to understand that none of these medications stops the disease itself.
Treatment for Mild to Moderate AD
Four of these medications are called cholinesterase inhibitors. These drugs are prescribed for the treatment of mild to moderate AD. They may help delay or prevent symptoms from becoming worse for a limited time and may help control some behavioral symptoms. The medications are: Reminyl® (galantamine), Exelon® (rivastigmine), Aricept® (donepezil), and Cognex® (tacrine). Scientists do not yet fully understand how cholinesterase inhibitors work to treat AD, but current research indicates that they prevent the breakdown of acetylcholine, a brain chemical believed to be important for memory and thinking. As AD progresses, the brain produces less and less acetylcholine; therefore, cholinesterase inhibitors may eventually lose their effect.
No published study directly compares these drugs. Because all four work in a similar way, it is not expected that switching from one of these drugs to another will produce significantly different results. However, an AD patient may respond better to one drug than another. Cognex® (tacrine) is no longer actively marketed by the manufacturer.
Treatment for Moderate to Severe AD
The fifth approved medication, known as Namenda® (memantine), is an N-methyl D-aspartate (NMDA) antagonist. It is prescribed for the treatment of moderate to severe AD. Studies have shown that the main effect of Namenda® is to delay progression of some of the symptoms of moderate to severe AD. The medication may allow patients to maintain certain daily functions a little longer. For example, Namenda® may help a patient in the later stages of AD maintain his or her ability to go to the bathroom independently for several more months, a benefit for both patients and caregivers.
Namenda® is believed to work by regulating glutamate, another important brain chemical that, when produced in excessive amounts, may lead to brain cell death. Because NMDA antagonists work very differently from cholinesterase inhibitors, the two types of drugs can be prescribed in combination.
Dosage and Side Effects
Doctors usually start patients at low drug doses and gradually increase the dosage based on how well a patient tolerates the drug. There is some evidence that certain patients may
9

benefit from higher doses of the cholinesterase inhibitor medications. However, the higher the dose, the more likely are side effects. The recommended effective dosage of Namenda® is 20 mg/day after the patient has successfully tolerated lower doses. Some additional differences among these medications are summarized in the table on the other side.
Patients may be drug sensitive in other ways, and they should be monitored when a drug is started. Report any unusual symptoms to the prescribing doctor right away. It is important to follow the doctor's instructions when taking any medication, including vitamins and herbal supplements. Also, let the doctor know before adding or changing any medications.
For More Information
To learn about support groups, services, research centers, and publications about AD, contact the following groups:
Alzheimer's Association225 N. Michigan Avenue, Suite 1700 Chicago, IL 606011-800-272-3900Website: www.alz.orgwww.alz.orgThis non-profit association supports families and caregivers of patients with AD. Nationwide chapters provide referrals to local resources.
Alzheimer's Disease Education and Referral (ADEAR) CenterPO Box 8250Silver Spring, MD 20907-82501-800-438-4380Website: www.alzheimers.orgThis service of the National Institute on Aging offers information and publications on diagnosis, treatment, patient care, caregiver needs, long-term care, and research related to AD.
U.S DEPARTMENT OF HEALTH AND HUMAN SERVICESPublic Health ServiceNational Institutes of HealthNational Institute on Aging NIH Publication No. 03-3431January 2004
Table - Medications to Treat Alzheimer's Disease
Note: The brief summary provided below does not include all information important for patient use and should not be used as a substitute for professional medical advice. Consult the prescribing doctor and read the package insert before using these or any other
10

medications or supplements. Drugs are listed in order, as approved by the U.S. Food and Drug Administration, starting with the most recent.
11
DRUG NAME DRUG TYPE
AND TREATMENT
MANUFACTURER’S RECOMMENDED
DOSAGE
COMMON SIDE
EFFECTS
POSSIBLE DRUG
INTERACTIONS
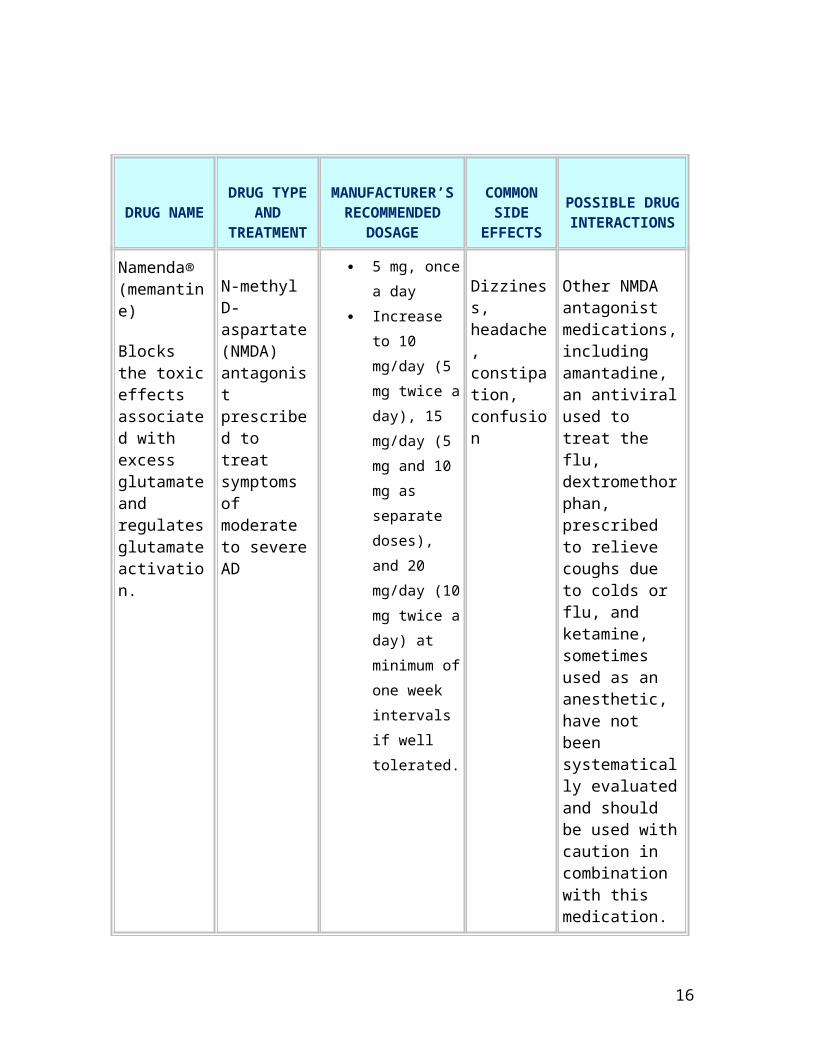
Namenda® (memantine)
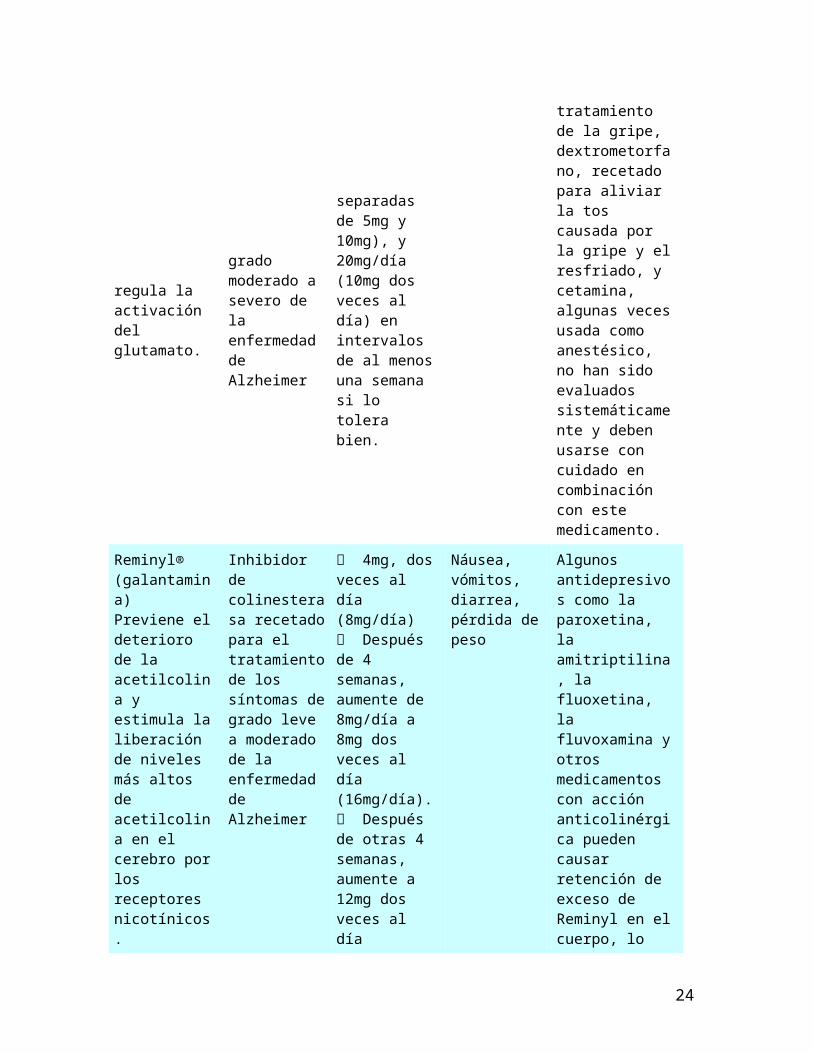
Blocks the toxic effects associated with excess glutamate and regulates glutamate activation.
N-methyl D-aspartate (NMDA) antagonist prescribed to treat symptoms of moderate to severe AD
5 mg, once a day
Increase to 10 mg/day (5 mg twice a day), 15 mg/day (5 mg and 10 mg as separate doses), and 20 mg/day (10 mg twice a day) at minimum of one week intervals if well tolerated.
Dizziness, headache, constipation, confusion
Other NMDA antagonist medications, including amantadine, an antiviral used to treat the flu, dextromethorphan, prescribed to relieve coughs due to colds or flu, and ketamine, sometimes used as an anesthetic, have not been systematically evaluated and should be used with caution in combination with this medication.
Reminyl® (galantamine)
Prevents the breakdown of acetylcholine and stimulates nicotinic receptors to release more acetylcholine in the brain.
Cholinesterase inhibitor prescribed to treat symptoms of mild to moderate AD
4mg, twice a day (8mg/day)
Increase by 8mg/day after 4 weeks to 8mg, twice a day (16mg/day)if well tolerated.
Nausea, vomiting, diarrhea, weight loss
Some antidepressants such as paroxetine, amitriptyline, fluoxetine, fluvoxamine, and other drugs with anticholinergic action may cause retention of excess Reminyl in the
12

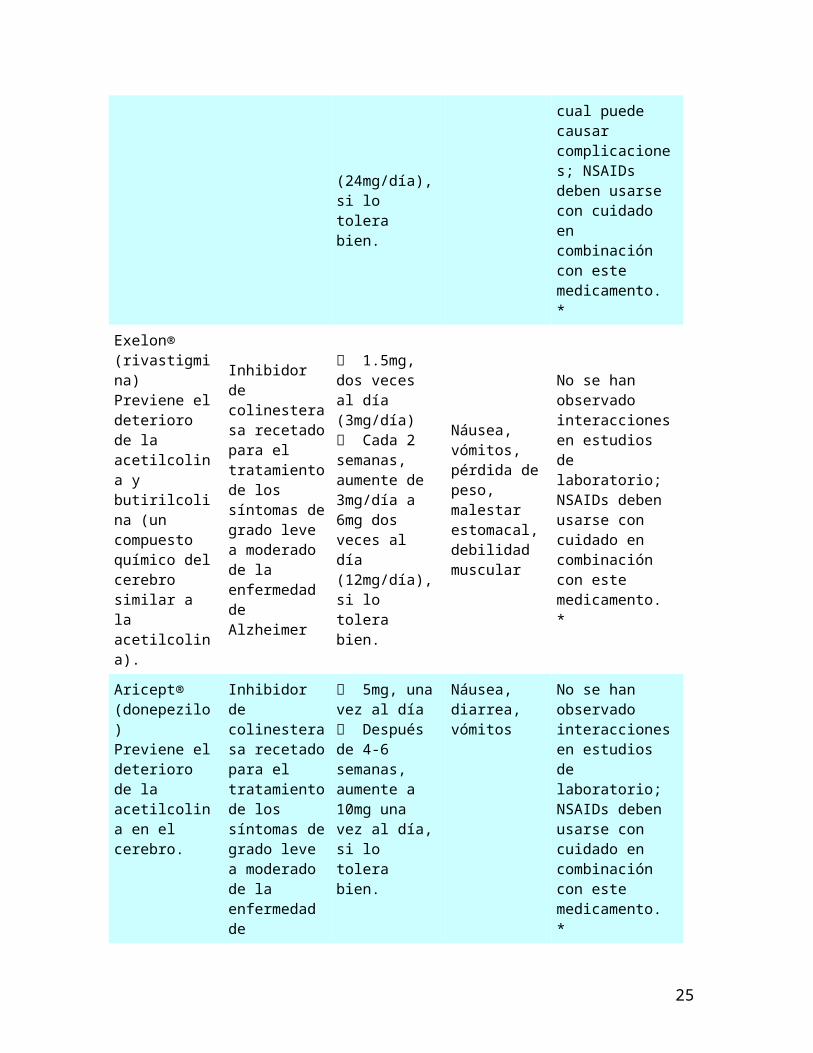
After another 4 weeks, increase to 12mg, twice a day (24mg/day) if well tolerated.
body, leading to complications; NSAIDs should be used with caution in combination with this medication.*
Exelon® (rivastigmine)
Prevents the breakdown of acetylcholine and butyrylcholine (a brain chemical similar to acetylcholine) in the brain.
Cholinesterase inhibitor prescribed to treat symptoms of mild to moderate AD
1.5mg, twice a day (3mg/day)
Increase by 3mg/day every 2 weeks to 6mg, twice a day (12mg/day) if well tolerated.
Nausea, vomiting, weight loss, upset stomach, muscle weakness
None observed in laboratory studies; NSAIDs should be used with caution in combination with this medication.*
Aricept® (donepezil)
Prevents the breakdown of acetylcholine in the brain.
Cholinesterase inhibitor prescribed to treat symptoms of mild to moderate AD
5mg, once a day
Increase after 4-6 weeks to 10mg, once a day if well tolerated.
Nausea, diarrhea, vomiting
None observed in laboratory studies; NSAIDs should be used with caution in combination with this medication.*
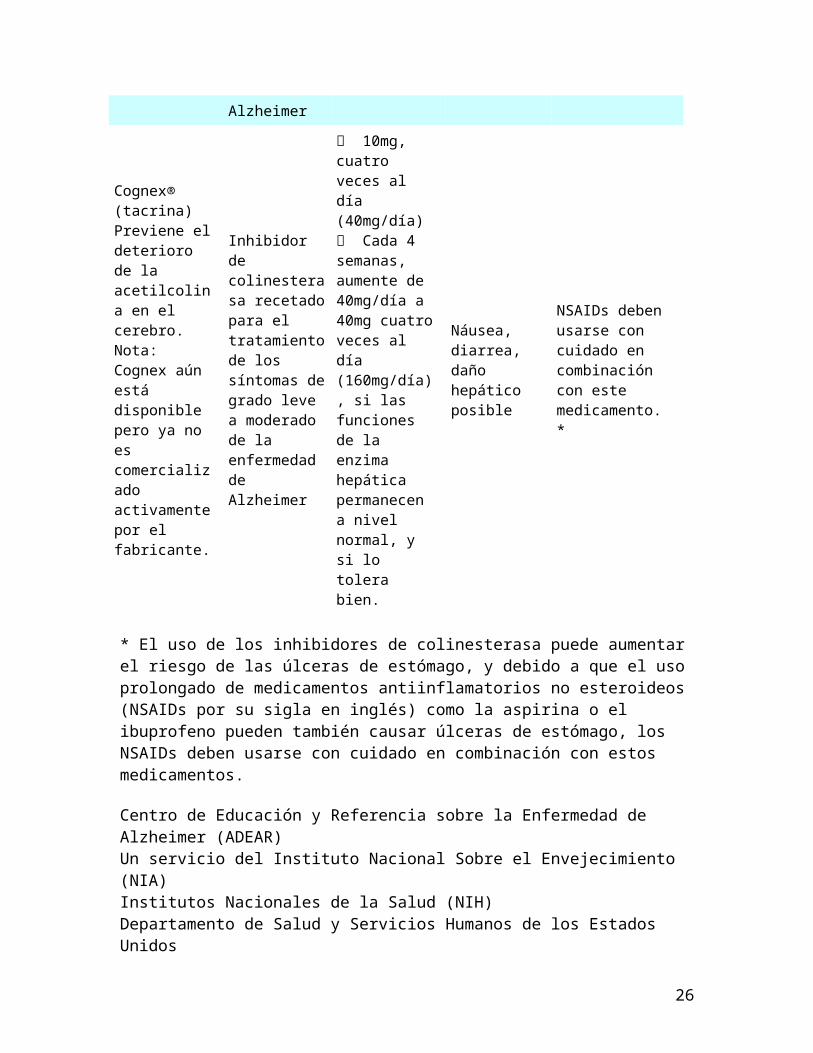
Cognex® (tacrine)
Prevents the breakdown of acetylcholine in the brain.
Cholinesterase inhibitor prescribed to treat symptoms of mild to moderate AD
10mg, four times a day (40mg/day)
Increase by 40mg/day every 4 weeks to
Nausea, diarrhea, possible liver damage
NSAIDs should be used with caution in combination with this medication.*
13
Note: Cognex is still available but no longer actively marketed by the manufacturer.
40mg, four times a day (160mg/day), if liver enzyme functions remain normal and if well tolerated.
* Use of cholinesterase inhibitors can increase risk of stomach ulcers, and because prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs) such as aspirin or ibuprofen can also cause stomach ulcers, NSAIDs should be used with caution in combination with these medications.
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESPublic Health ServiceNational Institutes of HealthNational Institute on Aging
Published in January 2004
14
Medicamentos para la enfermedad de Alzheimer
Tabla de Medicamentos
En la actualidad existen cinco medicamentos de prescripción aprobados por la Administración de Alimentos y Medicamentos de los Estados Unidos (Food and Drug Administration o FDA por su sigla en inglés) para tratar los síntomas de la enfermedad de Alzheimer. El tratamiento de los síntomas de la enfermedad de Alzheimer puede brindar a los pacientes bienestar, dignidad e independencia durante un período más largo y puede alentar y ayudar también a las personas encargadas de atenderlos. Sin embargo, es importante entender que ninguno de estos medicamentos detiene la enfermedad misma.
Tratamiento de los síntomas de grado leve a moderado de la enfermedad de Alzheimer
Cuatro de estos medicamentos se llaman "inhibidores de colines-terasa." Son recetados para el tratamiento de los síntomas de grado leve a moderado de la enfermedad de Alzheimer. Estos medicamentos pueden ayudar a retrasar los síntomas o impedir que empeoren por un tiempo limitado y pueden ayudar a controlar algunos síntomas de comportamiento. Los medicamentos son: Reminyl® (galantamina), Exelon® (rivastig-mina), Aricept® (donepezilo), Cognex® (tacrina). Los científicos todavía no comprenden totalmente cómo funcionan estos medica-mentos para tratar la enfermedad de Alzheimer, pero la investigación actual indica que cada uno actúa para prevenir el deterioro de la acetilcolina, un compuesto químico del cerebro que se cree es impor-tante para los procesos de la memoria y el pensamiento. A medida que la enfermedad progresa, el cerebro produce menos y menos acetilcolina y por lo tanto, con el tiempo, los medicamentos pueden perder su efecto.
No hay ningún estudio publicado que compare directamente estos medicamentos. Dado que los cuatro funcionan de una manera similar, no se espera que el cambio de uno de estos medicamentos a otro produzca resultados significa-tivamente diferentes. Sin embargo, una persona que padezca de la enfermedad de Alzheimer puede responder mejor a un medicamento que a otro. Cognex® (tacrina) ya no es comercializado activamente por el fabricante.
Tratamiento de los síntomas de grado moderado a severo de la enfermedad de Alzheimer
El quinto medicamento aprobado, conocido como Namenda® (memantina), es un antagonista de los receptores del N-metil D-aspartato (NMDA). Es recetado para el tratamiento de los síntomas de grado moderado a severo de la enfermedad de Alzheimer. Algunos estudios han señalado que el efecto principal de Namenda® es retrasar el desarrollo de algunos de los síntomas de grado moderado a severo de la enfermedad. Este medicamento permite a los pacientes mantener algunas de sus capacidades de funcionamiento diario por un periodo más largo. Por ejemplo, Namenda® puede ayudar a un paciente en las etapas avanzadas de la enfermedad a mantener su capacidad de ir al
15
baño por si solo por varios meses, un beneficio tanto para el paciente como para la persona encargada de atenderlo.
Se cree que Namenda® funciona regulando el glutamato, otra importante sustancia química en el cerebro, la cual puede conducir a la muerte de las células del cerebro cuando es producida en cantidades excesivas. Debido a que los antagon-istas del NMDA funcionan de manera distinta a la de los inhibidores de colinesterasa, se pueden recetar ambos tipos de medicamentos combinación.
Dosis y efectos secundarios
Generalmente los doctores comienzan por recetar al paciente una dosis baja y la van aumentando gradualmente en base a cuán bien un paciente tolera el medicamento. Pruebas médicas indican que los medicamentos con dosis elevadas de inhibidores de colinesterasa pueden brindar ventajas a algunos pacientes. Sin embargo, cuanto mayor es la dosis, mayor también es la probabilidad de tener efectos secundarios. La dosis recomendada de Namenda® es 20mg por día luego que el paciente haya tolerado exitosamente dosis más bajas. Otras diferencias entre estos medica-mentos se resumen en el cuadro en el reverso de este folleto.
Algunos pacientes quizá tengan otro tipo de sensibilidad a estos medicamentos y deben ser vigilados cuando comienzan a tomarlos. Notifique de inmediato cualquier síntoma extraño que experimente al doctor que le recetó el medicamento. Es importante seguir las instrucciones del doctor cuando se toma cualquier medicamento, incluidas las vitaminas y los suplementos fabricados a base de hierbas. Además, informe al doctor antes de agregar o cambiar medicamentos.
Para más información
Para obtener información sobre grupos de apoyo, servicios, centros de investigación y publicaciones sobre la enfermedad de Alzheimer, contacte a los siguientes grupos:
Alzheimer's Association(La Asociación de Alzheimer)225 N. Michigan Avenue, Suite 1700Chicago, IL 606011-800-272-3900www.alz.org
Esta asociación sin fines de lucro proporciona apoyo a las personas diagnosticadas con Alzheimer, a sus familias y a aquellos que las cuidan. Las oficinas nacionales proporcionan referencias a los recursos locales de la organización y disponen de personal bilingüe para asistirle.
Alzheimer's Disease Education and Referral Center (ADEAR) (Centro de Educación y Referencia sobre la Enfermedad de Alzheimer -ADEAR)
16

P.O. Box 8250Silver Spring, MD 20907-82501-800-438-4380www.alzheimers.org
Este servicio del Instituto Nacional Sobre el Envejecimiento proporciona publicaciones e información sobre el diagnóstico, tratamiento, cuidado del paciente, necesidades de la persona que cuida a pacientes con la enfermedad de Alzheimer, cuidado a largo plazo e investigación relacionada con la enfermedad de Alzheimer.
Medicamentos para el tratamiento de la enfermedad de Alzheimer
Nota: El breve resumen proporcionado abajo no incluye toda la información importante para que el paciente use un medicamento y no debe usarse como un sustituto para el asesoramiento médico profesional. Consulte al doctor que le haya recetado los medicamentos y lea el prospecto (folleto informativo sobre los medicamentos) antes de usar éstos u otros medicamentos o suplementos. Los medicamentos están enumerados en orden desde el más al menos reciente, según hayan sido aprobados por la Administración de Alimentos y Medicamentos de los Estados Unidos.
Nombre del Medicamento
Tipo de Medicamento
Dosificación Recomendada
por el Fabricante
Efectos Secundarios
Comunes
Interacciones Posibles con
otros Medicamentos
Namenda® (memantina) Bloquea los efectos tóxicos asociados con el exceso de glutamato y regula la activación del glutamato.
Antagonista del N-metil D-aspartato (NMDA) recetado para el tratamiento de los síntomas de grado moderado a severo de la enfermedad de Alzheimer
5mg, una vez al día Aumente a 10mg/día (5mg dos veces al día), 15mg/día (dosis separadas de 5mg y 10mg), y 20mg/día (10mg dos veces al día) en intervalos de al menos una semana si lo tolera bien.
Mareo, dolores de cabeza, estreñimiento, confusión
Otros medicamentos antagonistas del NMDA, incluyendo amantadina, un agente antiviral usado para el tratamiento de la gripe, dextrometorfano, recetado para aliviar la tos causada por la gripe y el resfriado, y cetamina, algunas veces usada como anestésico, no han sido evaluados sistemáticamente y deben usarse con cuidado en
17

combinación con este medicamento.
Reminyl® (galantamina)Previene el deterioro de la acetilcolina y estimula la liberación de niveles más altos de acetilcolina en el cerebro por los receptores nicotínicos.
Inhibidor de colinesterasa recetado para el tratamiento de los síntomas de grado leve a moderado de la enfermedad de Alzheimer
4mg, dos veces al día (8mg/día) Después de 4 semanas, aumente de 8mg/día a 8mg dos veces al día (16mg/día). Después de otras 4 semanas, aumente a 12mg dos veces al día (24mg/día), si lo tolera bien.
Náusea, vómitos, diarrea, pérdida de peso
Algunos antidepresivos como la paroxetina, la amitriptilina, la fluoxetina, la fluvoxamina y otros medicamentos con acción anticolinérgica pueden causar retención de exceso de Reminyl en el cuerpo, lo cual puede causar complicaciones; NSAIDs deben usarse con cuidado en combinación con este medicamento. *
Exelon® (rivastigmina)Previene el deterioro de la acetilcolina y butirilcolina (un compuesto químico del cerebro similar a la acetilcolina).
Inhibidor de colinesterasa recetado para el tratamiento de los síntomas de grado leve a moderado de la enfermedad de Alzheimer
1.5mg, dos veces al día (3mg/día) Cada 2 semanas, aumente de 3mg/día a 6mg dos veces al día (12mg/día), si lo tolera bien.
Náusea, vómitos, pérdida de peso, malestar estomacal, debilidad muscular
No se han observado interacciones en estudios de laboratorio; NSAIDs deben usarse con cuidado en combinación con este medicamento. *
Aricept® (donepezilo)Previene el deterioro de la acetilcolina en el cerebro.
Inhibidor de colinesterasa recetado para el tratamiento de los síntomas de grado leve a moderado de la enfermedad de Alzheimer
5mg, una vez al día Después de 4-6 semanas, aumente a 10mg una vez al día, si lo tolera bien.
Náusea, diarrea, vómitos
No se han observado interacciones en estudios de laboratorio; NSAIDs deben usarse con cuidado en combinación con este
18

medicamento. *
Cognex® (tacrina)Previene el deterioro de la acetilcolina en el cerebro. Nota: Cognex aún está disponible pero ya no es comercializado activamente por el fabricante.
Inhibidor de colinesterasa recetado para el tratamiento de los síntomas de grado leve a moderado de la enfermedad de Alzheimer
10mg, cuatro veces al día (40mg/día) Cada 4 semanas, aumente de 40mg/día a 40mg cuatro veces al día (160mg/día), si las funciones de la enzima hepática permanecen a nivel normal, y si lo tolera bien.
Náusea, diarrea, daño hepático posible
NSAIDs deben usarse con cuidado en combinación con este medicamento. *
* El uso de los inhibidores de colinesterasa puede aumentar el riesgo de las úlceras de estómago, y debido a que el uso prolongado de medicamentos antiinflamatorios no esteroideos (NSAIDs por su sigla en inglés) como la aspirina o el ibuprofeno pueden también causar úlceras de estómago, los NSAIDs deben usarse con cuidado en combinación con estos medicamentos.
Centro de Educación y Referencia sobre la Enfermedad de Alzheimer (ADEAR)Un servicio del Instituto Nacional Sobre el Envejecimiento (NIA)Institutos Nacionales de la Salud (NIH)Departamento de Salud y Servicios Humanos de los Estados Unidos
Publicación de NIH No. 03-3431SMarzo de 2004
19
Arthritis Advice
Arthritis is one of the most common diseases in this country. It affects millions of adults and half of all people age 65 and older.
Arthritis causes pain and loss of movement. It can affect joints in any part of the body. It often is a chronic disease, which means that it can affect you over a long period of time. The more serious forms can cause swelling, warmth, redness, and pain.
There are more than 100 different kinds of arthritis and many different symptoms and treatments. Scientists do not know what causes most forms of arthritis. They understand some better than others.
Common Forms of Arthritis
The three most common kinds of arthritis in older people are osteoarthritis, rheumatoid arthritis, and gout.
Osteoarthritis (OA) is the most common type of arthritis in older people. It mostly affects cartilage—the tissue that cushions the ends of bones within the joint. OA often affects the hands and the large weight-bearing joints of the body, such as knees and hips.
OA occurs when cartilage begins to fray, wear, and decay. In some cases, all of the cartilage may wear away between the bones of the joint, leaving bones that rub against each other. Symptoms can range from stiffness and mild pain that comes and goes, to severe joint pain. OA can cause:
Joint pain, Less joint motion, And sometimes, disability.
Scientists think there may be several causes for OA in different joints. OA in the hands or hips may run in families. OA in the knees is linked with being overweight. Injuries or overuse may cause OA in joints such as knees, hips, or hands.
Treatment. Rest, exercise, a healthy, well-balanced diet, and learning the right way to use your joints are key parts of any arthritis treatment program. Treatment is different for each kind of arthritis.
Right now there are no treatments that cure OA, except surgery to replace joints. But improving the way you use your joints through rest and exercise and keeping your weight down will help you control the pain.
There are some drugs that help people manage OA pain. They are called COX-2 inhibitors and NSAIDs (nonsteroidal anti-inflammatory drugs such as ibuprofen and
20

naproxen). These drugs reduce swelling without use of stronger drugs like cortisone or other steroids. COX-2 inhibitors are a newer type of drug. They work like NSAIDs but may cause fewer side effects.
Another new treatment involves shots of hyaluronic acid (hyaluronic acid viscosupplementation) to the area around the knee joint. The treatment adds fluid to replace natural fluids that the body has lost. It can help people with arthritis keep movement in the knee without pain.
Rheumatoid Arthritis (RA)is an inflammatory disease that causes pain, swelling, stiffness, and loss of function in the joints. People with RA often have a wide range of other symptoms such as feeling tired, running a fever, or generally not feeling well.
RA may occur in a balanced pattern throughout the body. For example, if one knee or hand is involved, the other one is too. The disease often affects wrist and finger joints closest to the hand.
Treatment. RA treatments can help relieve your pain, reduce swelling, slow down or stop joint damage, increase your ability to function, and improve your sense of well being. Treatment may include antirheumatic drugs, called DMARDs (disease-modifying antirheumatic drugs), which can slow the disease. Doctors will sometimes have you take other drugs, called corticosteroids to relieve swelling while you wait for DMARDs to take effect. Other drugs called biologic response modifiers, sometimes work for people with mild-to-moderate RA who have not been helped by other treatment.
Gout is one of the most painful rheumatic diseases. It is caused by deposits of needle-like crystals of uric acid in the connective tissue, joint spaces, or both. These deposits lead to inflammatory arthritis, which causes swelling, redness, heat, pain, and stiffness in the joints.
Gout affects the toes, ankles, elbows, wrists, and hands. Swelling may cause the skin to pull tightly around the joint and make the area red or purple and very tender. Medicines can stop gout attacks and prevent further attacks and joint damage.
Treatment. With the right treatment, most people with gout feel better. Treatment can help ease the pain that comes with acute attacks, prevent future attacks, and keep new uric acid deposits and kidney stones from forming.
The most common treatment for an acute attack of gout uses high doses of NSAIDs and shots of glucocorticoids drugs into the affected joint to lessen swelling. You may start to feel better within a few hours of treatment. The attack usually goes away fully within a few days.
21

Warning Signs
The warning signs of arthritis are:
Swelling in one or more joints, Stiffness around the joints that lasts for at least 1 hour in the early morning, Constant or recurring pain or tenderness in a joint, Difficulty using or moving a joint normally, Warmth and redness in a joint.
If any one of these symptoms lasts longer than 2 weeks, see your regular doctor or a doctor who specializes in arthritis (a rheumatologist). The doctor will ask questions about the history of your symptoms and do a physical exam. The doctor may take x-rays or do lab tests before developing a treatment plan.
What Else Can You Do?
Along with taking the right medicines, exercise is key to managing arthritis symptoms. Daily exercise, such as walking or swimming, helps keep joints moving, reduces pain, and strengthens muscles around the joints. Rest also is important for joints affected by arthritis.
Three types of exercise are best for people with arthritis:
Range-of-motion exercises (for example, dancing) help keep normal joint movement and relieve stiffness. This type of exercise also helps you stay flexible.
Strengthening exercises (for example, weight training) help keep or increase muscle strength. Strong muscles can help support and protect joints affected by arthritis.
Aerobic or endurance exercises (for example, bicycle riding) improve cardiovascular fitness, help control weight, and improve overall function. Some studies show that aerobic exercise also may reduce swelling in some joints.
The National Institute on Aging (NIA) has a 48-minute video showing you how to startand stick with a safe exercise program. The Institute also has an 80-page companionbooklet. Call 1-800-222-2225 (TTY: 1-800-222-4225) for more information. Before beginning any exercise program, talk with your doctor or health care worker.
Along with exercise, some people find other ways to help ease the pain around joints. These include applying heat or cold, soaking in a warm bath, swimming in a heated pool,and controlling or losing weight. Weight control is key for people who have arthritis because extra weight puts extra pressure on many joints. Weight loss can lower stress on joints and help prevent more damage.
22

Your doctor may suggest surgery when damage to the joints becomes disabling or when other treatments fail to reduce pain. Surgeons can repair or replace damaged joints with artificial ones. In the most common operations, doctors replace hips and knees.
Unproven Remedies
Many people with arthritis try remedies that have not been tested. Some of these remedies, such as snake venom, are harmful. Others, such as copper bracelets, are harmless but also useless. The safety of many unproven remedies is unknown.
Some people try taking dietary supplements, such as Glucosamine and Chondroitin, to ease arthritis pain. Scientists are studying these and other alternative treatments to find out if they work and are safe. More information is needed before any recommendations can be made.
Here are some signs that a remedy may be unproven:
The remedy claims that a treatment, like a lotion or cream works, for all types of arthritis and other diseases;
Scientific support comes from only one research study; or The label has no directions for use or warnings about side effects.
More Information
National Institute of Arthritis and Musculoskeletal and Skin DiseasesNIAMS Information Clearinghouse1 AMS CircleBethesda, Maryland 20892–3675301-495-4484877-22-NIAMS (226-4267)TTY: 301-565–2966Fax: 301-718-6366E-mail: [email protected]://www.niams.nih.gov/
American College of Rheumatology/Association of Rheumatology Health Professionals1800 Century PlaceSuite 250Atlanta, GA 30345-4300404-633-3777Fax: 404-633-1870E-mail: [email protected]://www.rheumatology.org
23
Arthritis FoundationP.O. Box 7669Atlanta, GA 30357-06691-800-283-7800, or check the telephone directory for your local chapterFax: 404-872-0457E-mail: [email protected]://www.arthritis.org
For more information on health and aging, contact:National Institute on Aging Information CenterP.O. Box 8057Gaithersburg, MD 20898-80571-800-222-22251-800-222-4225 (TTY)E-mail: [email protected] order publications online:www.niapublications.org
Visit NIHSeniorHealth.gov (www.nihseniorhealth.gov), a senior-friendly website from the National Institute on Aging and the National Library of Medicine. The site, which features popular health topics for older adults, has large type and a "talking" function that reads the text aloud.
National Institute on AgingU. S. Department of Health and Human ServicesNational Institutes of HealthJanuary 2002
24
Consejos Sobre la Artritis
La artritis es una de las enfermedades más comunes en este país. Afecta a millones de adultos y a la mitad de la población mayor de 65 años.
La artritis produce dolor y pérdida de movimientos. Puede afectar las coyunturas en cualquier parte del cuerpo. Frecuentemente es una enfermedad crónica, lo que quiere decir que puede afectarle por un largo período. Los tipos más serios de artritis pueden causar inflamación, calor, enrojecimiento y dolor.
Hay más de 100 tipos diferentes de artritis, muchos síntomas y distintos tratamientos. Los científicos no conocen el origen de la mayoría de los tipos de artritis, pero conocen algunos mejor que otros.
Tipos Comunes de Artritis
Los tres tipos más comunes de artritis en las personas mayores son la artritis ósea, la reumática y la gota.
La artritis ósea (OA por su sigla en Inglés) es el tipo más común de artritis en las personas mayores. Afecta principalmente al cartílago – el tejido que amortigua las terminaciones de los huesos en el interior de las articulaciones. La artritis ósea frecuentemente afecta las manos y las grandes articulaciones que soportan peso en el cuerpo, tales como las rodillas y las caderas.
La artritis ósea se presenta cuando el cartílago comienza a deshacerse, desgastarse y deteriorarse. En algunos casos, todo el cartílago puede desgastarse entre los huesos de la articulación, haciendo que los huesos se rocen entre si. Los síntomas pueden ir desde el entumecimiento y un dolor moderado que se va y regresa, hasta un severo dolor de la articulación. La artritis ósea puede producir:
Dolor en la articulación,
Disminución en el movimiento de la articulación,
Y algunas veces invalidez. Los científicos piensan que la artritis en las diferentes articulaciones puede tener diversas causas. La artritis ósea de las manos o caderas puede tener origen familiar. La artritis ósea de las rodillas se vincula con el sobrepeso. Lesiones o un excesivo uso pueden ser la causa de la artritis ósea en las articulaciones de las rodillas, caderas o manos.
Tratamiento. El descanso, el ejercicio, una dieta saludable y bien balanceada y aprender a usar correctamente las articulaciones son partes importantes de cualquier programa de tratamiento para la artritis. El tratamiento es diferente para cada tipo de artritis.
25
En este momento no hay tratamientos que curen la artritis ósea, excepto la cirugía para reemplazar las articulaciones. Pero mejorar la manera cómo usted utiliza sus articulaciones, por medio del descanso y el ejercicio y mantenerse bien de peso, le ayudarán a controlar el dolor.
Hay algunas medicinas que ayudan a las personas a manejar el dolor de la artritis ósea. Se llaman inhibidores COX-2 y NSAID (drogas anti-inflamatorias sin esteroides tales como el ibuprofeno y el naproxeno). Estas medicinas reducen la inflamación sin utilizar drogas más fuertes como la cortisona y otros esteroides. Los inhibidores COX-2 son un nuevo tipo de medicamento, que funciona como los NSAID pero pueden causar menos efectos secundarios.
En un nuevo tratamiento se inyecta ácido hyalurónico (visco-suplemento de ácido hyalurónico) en el área alrededor de la articulación de la rodilla. En este tratamientose agregan líquidos que reemplazan los fluidos naturales que el cuerpo ha perdido, para ayudar a las personas con artritis a mantener movimiento en la rodilla sin dolor.
La Artritis Reumatoidea (RA por su sigla en Inglés) es una enfermedad inflamatoria que causa dolor, inflamación, rigidez y pérdida de la función de las articulaciones.Las personas que sufren artritis reumatoidea con frecuencia presentan una gama amplia de síntomas tales como cansancio, fiebre o malestar general.
La artritis reumatoidea puede presentarse de forma balanceada en todo el cuerpo, por ejemplo, si una rodilla o mano está afectada, la otra también se afecta. La enfermedad frecuentemente afecta la muñeca y las articulaciones de los dedos más cercanas a la mano.
Tratamiento. Los tratamientos para la artritis reumatoidea pueden aliviar su dolor, reducir la inflamación y disminuir o detener el avance del daño en la articulación, aumentar su habilidad para funcionar y su sensación de bienestar. El tratamiento puede incluir drogas anti-reumáticas llamadas DMARD (medicamentos anti-reumáticos modificadores de la enfermedad) que pueden retardar el avance de la enfermedad. Los médicos a veces le prescribirán otras medicinas llamadas corticoesteroides para aliviar la inflamación mientras usted espera que las DMARD produzcan efecto. Otros medicamentos llamados modificadores de respuesta biológica, a veces pueden servirle a personas con artritis reumatoidea de ligera a moderada, que no hayan recibido alivio con otros tratamientos.
La Gota es una de las enfermedades reumáticas más dolorosas. Es causada por depósitosen los tejidos de cristales de ácido úrico similares a agujas, en los espacios de las articulaciones o en ambos. Estos depósitos producen artritis inflamatoria causando inflamación, enrojecimiento, calor, dolor y rigidez en las articulaciones.
La gota afecta los dedos del pie, los tobillos, los codos, las muñecas y las manos. La inflamación puede causar que la piel se estire alrededor de la articulación y puede enrojecerla, amoratarla y volverla muy sensible. Hay medicinas que pueden detenerlos ataques de gota y prevenir ataques futuros y daños de la articulación.
26
Tratamiento. Con el tratamiento correcto, la mayoría de las personas con gota se sienten mejor. El tratamiento puede aliviar el dolor de los ataques agudos, evitar ataques futuros, y prevenir la formación de nuevos depósitos de ácido úrico y de cálculos renales.
En los tratamientos más comunes para los ataques agudos de gota se utilizan altas dosis de NSAID e inyecciones de medicamentos glucocorticoides en la articulación afectada para disminuir la inflamación. Usted puede empezar a sentirse mejor a las pocas horasde haber iniciado el tratamiento. El ataque generalmente se terminará totalmente en unos pocos días.
Síntomas
Los síntomas de la artritis son:
Inflamación de una o más articulaciones,
Rigidez alrededor de las articulaciones, que dura por lo menos 1 hora temprano en la mañana,
Dolor o sensibilidad constante o frecuente en una articulación,
Dificultad para utilizar o mover una articulación normalmente,
Calor y enrojecimiento en una articulación.
Si cualquiera de estos síntomas le dura más de 2 semanas, consulte con su médico o un especialista en la artritis (reumatólogo). El médico le hará preguntas sobre la historiade sus síntomas y le realizará un examen físico. El médico puede tomar radiografías o hacer pruebas de laboratorio antes de ordenarle un plan de tratamiento.
¿Qué más Puede Usted Hacer?
Además de tomar las medicinas apropiadas el ejercicio es muy importante en el manejo de los síntomas de la artritis. Los ejercicios diarios, tales como caminar o nadar, ayudan a mantener las articulaciones en movimiento, reducen el dolor y fortalecen los músculos alrededor de las articulaciones. El descanso también es importante para las articulaciones afectadas por la artritis.
Hay tres tipos de ejercicios recomendados para las personas con artritis:
Ejercicios de movimientos amplios (por ejemplo, bailar) ayudan a mantener el ovimiento normal de las articulaciones y alivian la rigidez. Este tipo de ejercicios también le ayudan a mantenerse flexible.
27
Ejercicios de fortalecimiento (por ejemplo, entrenamiento con pesas) ayudan a mantener o aumentar la fortaleza de los músculos. Los músculos fuertes pueden ayudar a apoyar y proteger las articulaciones afectadas por la artritis.
Ejercicios aeróbicos o de resistencia (por ejemplo, montar en bicicleta) mejoran el estado cardiovascular, ayudan a controlar el peso y mejoran la funcióngeneral. Algunos estudios muestran que los ejercicios aeróbicos también puedenreducir la inflamación en algunas articulaciones.
El Instituto Nacional Sobre el Envejecimiento (NIA) tiene un video de 48 minutos que le muestra cómo empezar y seguir un programa de ejercicios sin riesgo. El Instituto también tiene un libro de ejercicios de 107 páginas. Llame al 1-800-222-2225 (TTY: 1-800-222-4225) para más información. Antes de empezar cualquier programa de ejercicios hable con su médico o especialista en el cuidado de la salud.
Además del ejercicio, algunas personas han encontrado otras maneras para ayudar a liviar el dolor alrededor de las articulaciones, tales como la aplicación de calor o frío, sumergirse en una tina, nadar en una piscina de agua caliente y controlar o perder el exceso de peso. Controlar el peso es muy importante para las personas que tienen artritis, porque el sobrepeso ejerce presión adicional en muchas articulaciones. La pérdida de peso puede reducir la presión sobre las articulaciones y ayuda a prevenir mayores daños.
Su médico puede aconsejar la cirugía cuando el daño en las articulaciones produce invalidez o cuando otros tratamientos no disminuyen el dolor. Los cirujanos pueden reparar las articulaciones dañadas o reemplazarlas con articulaciones artificiales. En las operaciones más comunes, los cirujanos reemplazan caderas y rodillas.
Remedios de Efectividad no Comprobada
Muchas personas con artritis utilizan remedios cuya efectividad no ha sido probada. Algunos de estos remedios son dañinos, tales como el veneno de serpientes. Otros, como las pulseras de cobre, no producen ningún daño pero también son inútiles. La seguridad de muchos de estos remedios es desconocida.
Algunas personas prueban suplementos dietéticos, tales como la Glucosamina y la Chondroitina, para aliviar el dolor de la artritis. Los científicos están estudiandoéstos y otros tratamientos alternativos para averiguar si son efectivos y si no tienen riesgo. Es necesario tener más información antes de hacer cualquier recomendación.
Las siguientes son algunas indicaciones de que la eficacia de un remedio no ha sido comprobada:
El remedio se anuncia, como una loción o una crema, que sirve para todos los tipos de artritis y otras enfermedades;
El apoyo científico proviene únicamente de una investigación; o
28

La etiqueta no tiene instrucciones sobre su uso o advertencias sobre efectos secundarios.
Para mayor información sobre la artritis contacte a:
National Institute of Arthritis and Musculoskeletal and Skin DiseasesNIAMS Information Clearinghouse(Instituto Nacional de la Artritis y Enfermedades Musculoesqueléticas y de la Piel)(NIAMS Centro de Información) 1 AMS CircleBethesda, MD 20892–3675301-495-4484 1-877-22-NIAMS (226-4267)TTY: 301-565–2966FAX: 301-718-6366 Correo Electrónico: [email protected] http://www.niams.nih.gov
American College of Rheumatology/Association of Rheumatology Health Professionals(Colegio Americano de Reumatología/Asociación Americana de Profesionales de la Salud en Reumatología) 1800 Century Place, Suite 250Atlanta, GA 30345-4300404-633-3777FAX: 404-633-1870 Correo Electrónico: [email protected] http://www.rheumatology.org
Arthritis Foundation (Fundación para la Artritis) P.O. Box 7669 Atlanta, GA 30357-06691-202-537-68001-800-283-7800, o llame a su oficina local (Busque en el directorio telefónico el númerodel capítulo local.)FAX: 404-872-0457 Correo Electrónico: [email protected] http://www.arthritis.org
29

Para más información sobre la salud y el envejecimiento, llame o escriba a: National Institute on Aging Information Center(Centro de Información de Instituto Nacional Sobre el Envejecimiento) P.O. Box 8057 Gaithersburg, MD 20898-8057 1-800-222-2225 1-800-222-4225 (TTY) Correo Electrónico: [email protected] http://www.nia.nih.gov
National Institute on AgingU. S. Department of Health and Human ServicesNational Institutes of HealthJanuary 2002
30
Dietary Supplements:More is Not Always Better
Bill’s retired and lives alone. Often he’s just not hungry or is too tired to fix a whole meal. Does he need a multi-vitamin or one of those dietary supplements he sees in ads everywhere? He wonders if they work—will one help his arthritis, or another give him more energy? And, are they safe?
"Dietary supplements" used to make you think only of vitamins and minerals. But, today this big business makes and sells many different types of dietary supplements that have vitamins, minerals, fiber, amino acids, herbs, or hormones in them. Supplements come in the form of pills, capsules, powders, gel tabs, extracts, or liquids. Sometimes you find them added to drinks or energy bars. They might be used to add nutrients to your diet or to prevent healthproblems. You don’t even need a prescription from your doctor to buy dietary supplements.
Do I Need a Dietary Supplement?
Ads for supplements seem to promise to make you feel better, keep you from getting sick, or even help you live longer. Often there is little, if any, scientific support for these claims. In fact, some supplements can hurt you. Others are a waste of money because they don’tgive you any health benefits.
So, should you take a supplement? You might want to talk to your doctor or a registered dietitian to answer that question. A friend or neighbor, or someone on a commercial shouldn’t be suggesting a supplement for you.
Are These Supplements Safe?
Are you thinking about using dietary supplements? Remember that these "over-the-counter" substances are not like the penicillin or blood pressure medicine your doctor mightprescribe for you. The U.S. Food and Drug Administration (FDA) has to check prescription drugs to make sure they are safe and do what they promise before they are sold. The same is true for "over-the-counter drugs" like cold and pain medicines. It is not the FDA’s job to check dietary supplements in the same way. That means they are not reviewed by the FDA before being sold, but it is the FDA’s job to take action against unsafe products on the market. Only if enough people report problems with a dietary supplement, can the FDA study these possible problems and take action.
Besides the FDA, many federal government agencies and private groups are interested in dietary supplements. The National Institutes of Health (NIH) is the federal focal point for
31

medical research in the United States. NIH supports research studies looking at the safety and helpfulness of some of the ingredients found in many supplements.
Business and consumer groups are also interested in dietary supplements. So are private professional groups such as the National Academy of Sciences (NAS). The NAS develops guidelines saying how much of each vitamin and mineral people need.
What About Vitamins and Minerals?
Vitamins and minerals are nutrients found naturally in food. We need them to stay healthy. The benefits and side effects of many vitamins and minerals have been studied. The best way to get vitamins and minerals is through the food you eat, not any supplements you might take. Try to eat the number of servings of food recommended by the U.S. Department of Agriculture’s Food Guide Pyramid each day (see chart). Pick foods that are lower in fat and added sugars. If you can’t eat enough, then ask your doctor if you should be taking a multivitamin and mineral supplement. And remember:
The supplement doesn’t need to be a "senior" formula.
It shouldn’t have large or "mega-doses" of vitamins and minerals. Generally store or generic brands are fine.
How much should you take? The NAS has developed recommendations for vitamins and minerals. Check the label on your supplement bottle. It shows the level of vitamins and minerals in a serving compared with the suggested daily intake.
How Many Servings Do You Need?
Bread, cereal, rice, and pasta—6 to 11 servings
Vegetables—3 to 5 servings
Fruits—2 to 4 servings
Milk, yogurt, and cheese—2 to 3 servings
Meat, poultry, fish, dry beans, eggs, and nuts—2 to 3 servings
Fats, oils, and sweets—use sparingly
32

For example, a vitamin A intake of 100% DV (Daily Value) means the supplement is giving you the full amount of vitamin A you need each day. This is in addition to what you are getting from your food.
Some people might think that if a little is good, a lot must be better. But, that doesn’t necessarily apply to vitamins and minerals. Depending on the supplement, your age, andyour health, taking more than 100% DV could be harmful to your health. Also, if your body cannot use the entire supplement you take, you’ve wasted money. Finally, large dosesof some vitamins and minerals can also keep your prescription medications from working as they should.
Anything Special For People Over 50?
Even if you eat a good variety of foods, if you are over 50, you might need certain supplements. Talk to your doctor or a registered dietitian. Depending on your needs, he orshe might suggest you get the following amounts from food and, if needed, supplements:
Vitamin B12—2.4 mcg (micrograms) of B12 each day. Some foods, such as cereals, are fortified with this vitamin. But, up to one-third of older people can no longer absorb natural vitamin B12 from their food. They need this vitamin to keep their blood and nerves healthy.
Calcium—1200 mg (milligrams), but not more than 2500 mg a day. As you age, you need more of this and vitamin D to keep bones strong and to keep the bone you have. Bone loss can lead to fractures, mainly of the hip, spine, or wrist, in both older women and men.
Vitamin D—400 IU (international units) for people age 51 to 70 and 600 IU for those over 70, but not more than 2000 IU each day.
Iron—extra iron for women past menopause who are using hormone replacement therapy (men and other postmenopausal women need 8 mg of iron). Iron helps keep red blood cells healthy. Postmenopausal women who use hormone replacement therapy may still experience a monthly period. They need extra iron to make up for that loss of blood.
Vitamin B6—1.7 mg for men and 1.5 mg for women. This vitamin is needed for forming red blood cells and to keep you healthy.
33

What Are Antioxidants?
You may have heard about the possible benefits of antioxidants, natural substances found in food. Right now, there is no proof that large doses of antioxidants will prevent chronic diseases such as heart disease, diabetes, or cataracts. Eating fruits and vegetables (at least five servings a day) rather than taking a supplement is the best way to get antioxidants. Vegetable oil and nuts are also good sources of some antioxidants. Non-dairy calcium sources are especially good for people who cannot use dairy products.
Sources of Calcium
dairy products like milk and cheese and foods made with them,
canned fish with soft bones like salmon and sardines,
dark green leafy vegetables, calcium-fortified products such as orange juice,
and
breads and cereals made with calcium-fortified flour.
What About Herbal Supplements?
You may have heard of ginkgo biloba, ginseng, Echinacea, or black cohosh. These are examples of herbal supplements. They are dietary supplements that come from certain plants. It’s easy to think they are safe because they come from plants. And, although herbal supplements are not approved as drugs, some are being studied as possible treatments for illness. But, it’s still too soon to tell. Remember some strong poisons like hemlock and prescription medicines such as cancer drugs come from plants as well. You need to be careful.
When you use any dietary supplement, including herbals, for a health problem, you are using that supplement as a drug. Because their ingredients may have an effect on your body, they can interfere with medications you may already be taking. Some herbal supplements can also cause serious side effects such as high blood pressure, nausea, diarrhea, constipation, fainting, headaches, seizures, heart attack, or stroke.
34
What’s Best For Me?
If you are thinking about using dietary supplements for any reason, remember:
Talk to your doctor or a registered dietitian. Just because something worked for your neighbor, doesn’t mean the same will be true for you.
Use only the supplement your doctor or dietitian and you decide on—don’t buy combinations that have things you don’t want or need.
If your doctor does not suggest a dietary supplement, but you decide to use one anyway, tell your doctor. Then he or she can keep an eye on your health and adjust your other medications if needed.
Learn as much as you can about the supplement you are thinking about, but be aware of the source of the information. Could the writer or group profit from the sale of a particular supplement?
Buy brands you know from companies you, your doctor, your dietitian, or your pharmacist know are reputable.
Remember that many of the claims made about supplements are not based on enough scientific proof. If you have questions about a supplement, contact the firm and ask if it has information on the safety and/or effectiveness of the ingredients in its product.
What Else Can I Do?
Here’s what one active older person does:
When Pearl was nearing 60, she was concerned about remaining healthy and active as she aged. She began to exercise. Now she takes a long, brisk walk 3 or 4 times a week. In bad weather, she joins the mall walkers at the local shopping mall. In good weather, she also works in her garden. She had long since stopped smoking. Pearl tries to follow a healthy diet. She reads the newspaper everyday. She’s even learninghow to use a computer and keeps in touch with her family by email, as well as phone calls. She always wears a seatbelt when in a car. Last month, she danced at her granddaughter’s wedding. Pearl is now 84 years old.
Try following Pearl’s example—stick to a healthy diet, exercise, keep your mind active, don’t smoke, and see your doctor regularly.
Resources
The following are some resources for information on vitamins, minerals, other dietary supplements, and nutrition.
Center for Food Safety and Applied NutritionFood and Drug Administration
35

5100 Paint Branch ParkwayCollege Park, MD 20740-38351-888-SAFEFOOD (1-888-723-3366)http://www.cfsan.fda.gov
Food and Nutrition Information CenterDepartment of Agriculture10301 Baltimore Ave., Rm. 105Beltsville, MD 20705-2351301-504-5719http://www.nal.usda.gov/fnic
Office of Dietary SupplementsNational Institutes of HealthBldg. 31, Rm. 1B2931 Center Drive, MSC 2086Bethesda, MD 20892-2086301-435-2920http://dietary-supplements.info.nih.gov
The National Institute on Aging (NIA) offers free information on health and aging.
NIA Information CenterPO Box 8057Gaithersburg, MD 20892-80571-800-222-22251-800-222-4225 (TTY)http://www.nia.nih.gov
National Institute on AgingU. S. Department of Health and Human ServicesNational Institutes of HealthAugust 2002.
36

Hormones After Menopause
So this is menopause. You are having hot flashes and trouble sleeping. That leaves you tired all day. You wonder about osteoporosis. Your doctor has suggested that hormones might help. But you have heard stories on the news that make you wonder if they are right for you. You don’t know what to do. How do you decide?
Millions of women take hormones around the time of menopause, called menopausal hormone therapy. Some women should not. It may or may not be the right choice for you.
What Is Menopausal Hormone Therapy?
Menopause is the time around the age of 51 when your body makes much less of the female hormones estrogen and progesterone and you stop having periods. This can cause troublesome symptoms for some women. As early as your forties, you may start having signs like irregular periods or hot flashes (sudden warmth, often followed by sweating).
Doctors sometimes prescribe estrogen to ease these symptoms. This can also protect against the loss of bone after menopause. But there are risks. Estrogen used alone can cause cancer of the lining of the uterus (endometrial cancer). According to the National Cancer Institute, about 5 cases of endometrial cancer may develop in every 10,000 women using this hormone for 10 years. This is about 4 more cases than we would expect in a group of 10,000 women who don’t use estrogen. More importantly estrogen used alone can cause a thickening of the lining of the uterus and irregular bleeding. But, if you have had a total hysterectomy (surgery to remove the uterus and cervix), you can use estrogen alone (estrogen therapy or ET). Several types of estrogen are available. They come in many forms. You can use a pill or tablet, a skin patch, vaginal cream, vaginal ring insert, implant, or shot.
If you still have your uterus and want to take hormones, doctors will prescribe estrogen along with progesterone or one of several progestins, synthetic forms of progesterone. The progestin protects against endometrial cancer. Using estrogen and progesterone or a progestin is called estrogen plus progestin therapy or EPT. Progesterone or progestin is often taken as a pill, sometimes in the same pill as the estrogen. It is also available as a patch, an IUD (intrauterine device), a vaginal gel, suppository, or shot.
The form your doctor suggests may depend on your symptoms. For example, estrogen creams and tablets are used for vaginal dryness. The vaginal ring insert treats vaginal dryness and may help urinary tract symptoms. Pills or patches provide relief from annoying symptoms such as hot flashes, night sweats, sleep problems, and vaginal dryness. They will also prevent bone loss and help delay osteoporosis while you are using them and could improve your cholesterol levels. Some experts think they may help your memory if begun at menopause. But improving cholesterol or helping memory should not be the main reason you take menopausal hormone therapy.
37
Schedules for Taking EPT
If your doctor suggests estrogen plus progestin and you agree, talk to him or her about the schedule that is best for you. The pill form of EPT is taken following one of these two plans:
Cyclic Plan:
Estrogen every day Progesterone or progestin added for 10 to 14 days out of every 4 weeks Often causes monthly bleeding like a light menstrual period
Combined Continuous Plan:
Estrogen and progestin taken every day of the month without a break May stop monthly bleeding after about 6 or more months of treatment Problem spotting may continue longer
Also available as a patch
What Are The Risks of These Hormones?
Both estrogen and progestin can have side effects. You could feel bloating, breast tenderness, cramping, irritability, depression, and sometimes have spotting or a return of monthly periods for a few months or years. By changing the type or amount of these hormones, the way they are taken, or the timing of the doses, your doctor may be able to control these side effects. Or, over time they may go away on their own.
But there could be more serious risks. These include heart disease, blood clots, stroke, and breast cancer in all postmenopausal women, and possibly dementia in women over 65. Many women now live 25, 30, or more years after menopause. Could taking hormone therapy for many of those years be helpful to women? Would it be safe? Women and their doctors need to think about the benefits and risks of using menopausal hormone therapy for just a few years or for longer.
Doctors have known for a while how to reduce the risk of endometrial cancer from using estrogen. But, what about other risks? Studies are now being done to learn more about the risks of using hormones after menopause. An important study of menopausal hormone therapy is included in the Women’s Health Initiative (WHI), funded by the National Institutes of Health (NIH). In 2002 these scientists found that for every 10,000 women taking a pill containing a specific hormone combination of conjugated equine estrogens and a progestin called medroxyprogesterone acetate, each year there would be:
8 more cases of breast cancer than in women not using these hormones,
38

7 more cases of heart disease, 8 more cases of stroke, and 8 more cases of blood clots in the lungs.
But there would also be health benefits:
5 fewer cases of hip fracture, and 6 fewer cases of colorectal cancer.
The WHI hormone study has a substudy called the WHI Memory Study (WHIMS) to look at whether using hormones after age 65 can prevent or delay dementia in older women. In 2003 investigators from WHIMS announced that older women using estrogen plus progestin in their study were at twice the risk for developing dementia. Each year in 10,000 women over age 65 using estrogen plus progestin they found:
23 more cases of dementia than in older women not using these hormones.
The risks found in these two studies may be small for each individual woman, but they need to be taken into account when thinking about menopausal hormone therapy. Other estrogens and progestins that are different from the ones used in these studies are available. They have not been tested for as long or in as many women as the ones used in the WHI studies. Experts think that using these could cause similar effects, but they do not know for sure.
39
Benefits and Risks of Menopausal Hormone Therapy
Here is what scientists can say so far about the advantages and disadvantages of menopausal hormone therapy. ET is estrogen only therapy, and EPT is therapy using estrogen with a progestin.
Benefits
EPT and ET reduce the risk of osteoporosis.EPT and ET relieve hot flashes and night sweats.EPT and ET relieve vaginal dryness.EPT and ET improve cholesterol levels.EPT and ET reduce the risk of cancer of the colon
Risks
ET, without the use of a progestin, increases the risk of cancer of the uterus.EPT and ET modestly increase risk of breast cancer while they are being used; long-term use may pose the greatest risk. EPT increases cardiovascular problems such as heart attack and stroke and is not recommended in women who have these diseases.EPT and ET may increase the risk for blood clots.EPT and ET can have unpleasant side effects, such as bloating and breast tenderness.EPT and ET in pill form can raise level of triglycerides (a type of fat in the blood).
Under study
EPT and ET to improve mood and psychological well-being.ET to prevent the loss of mental abilities with age.EPT to lower risk of developing diabetes.EPT to lower risk of ovarian cancer.
May 2003
Should I Use Menopausal Hormone Therapy?
Right now, experts do not have all the answers to their questions about menopausal hormone therapy. Are other forms of estrogen or progestin safer than the ones used in the WHI studies? How long can a woman safely use menopausal hormone therapy? Is one form of such hormone therapy (pill, patch, or cream, for example) better than another? Which schedule is best? These are just some of the questions that remain.
For now we know that each woman is different, and the answer for each one may also be different. That means this question is best thought about after talking with your doctor
40
(general practitioner, internist, or gynecologist). He or she can help you apply what is known about menopausal hormone therapy to your medical history. For example, you probably should not use these supplements if you have liver disease, high levels of triglycerides (a type of fat in the blood), or a history of blood clots in your veins. However, some experts think that using a patch, rather than a pill, will not make your triglyceride level go higher or increase your chance of gall bladder problems. Women with a family history of breast cancer should check with their doctor about that risk.
The first step is to decide how much you are bothered by menopause symptoms such as hot flashes or vaginal dryness. For many women hot flashes or night sweats will likely go away over time, but vaginal dryness may not. You will also need to think about your medical history, your risk of osteoporosis, heart disease, breast cancer, gall bladder disease, and blood clots, and your family history of these illnesses.
Then talk to your doctor about how best to treat or prevent your symptoms or the diseases for which you are at risk. Ask about your other choices. These too may have risks and benefits. Along with your doctor you can decide whether the benefits of using estrogen plus progestin or estrogen alone are greater than the risks for you.
If you are already using menopausal hormone therapy and decide to stop, ask your health care provider how to do that. Some doctors suggest tapering off.
And remember—any decision about using estrogen plus progestin or estrogen alone is not final. You can start or end the treatment anytime. But, if you stop it, the protection these therapies give you will stop as well. Your decision about menopausal hormone therapy should be reviewed each year with your doctor at your annual checkup. At that time you can ask if there are any new study results.
Research on using hormones during and after menopause is continuing. Almost every study gives women and their doctors another part of the answer to the question: Is menopausal hormone therapy right for me?
Resources
For more information contact:
National Heart, Lung, and Blood InstituteNHLBI Information CenterBox 30105 Bethesda, MD 20824-0105301-592-8573240-629-3255 (TTY)http://www.nhlbi.nih.gov/
National Cancer InstituteNCI Public Inquiries Office
41

Suite 3036A6116 Executive Blvd. MSC8322Bethesda, MD 20892-83221-800-4-CANCER (1-800-422-6237)http://www.cancer.gov/
American College of Obstetricians and Gynecologists (ACOG)409 12th Street, SWBox 96920Washington, DC 20090-6920202-638-5577http://www.acog.org/
North American Menopause SocietyPO Box 94527Cleveland, OH 44101440-442-75501-800-774-5342http://www.menopause.org/
The National Institute on Aging offers free information on menopause and osteoporosis.
National Institute on Aging Information CenterP.O. Box 8057Gaithersburg, MD 20898-80571-800-222-22251-800-222-4225 (TTY)E-mail: [email protected]://www.nia.nih.gov/
National Institute on Aging U.S. Department of Health and Human Services National Institutes of Health May 2003
42
43

Pills, Patches, and Shots:Can Hormones Prevent Aging?
We could not survive without hormones. They are among the most common and vital chemical messengers in the body. From head to toe, each moment of life, they signal cells to perform tasks that range from the ordinary to the extraordinary. Among their many roles, hormones help regulate body temperature, blood pressure, and blood sugar levels. In childhood, they help us “grow up.” In the teen years, they are the driving force behind puberty. But what influence, if any, the natural decline in some hormones has on the aging process in middle and late life is unclear. Although a few proponents are convinced that hormone supplements can favorably alter the aging process and have advocated their widespread use, the scientific evidence supporting this premise is, for the most part, sketchy.
For more than a decade, the National Institute on Aging (NIA), a component of the federal government’s National Institutes of Health, has supported and conducted studies of replenishing hormones and similar substances to find out if they may help reduce frailty and improve function in older people. These studies have focused on hormones known to decline as we grow older:
Dehydroepiandrosterone (DHEA) Growth Hormone Melatonin Testosterone Menopausal hormones, such as estrogen
The results from these NIA-sponsored studies and other research projects likely will improve our understanding of the pros and cons of hormone supplementation. Until the results of these studies are compiled, analyzed, and a consensus among scientists is reached, recommendations to use supplemental hormones and hormone-like molecules to influence the aging process and health problems associated with aging should be viewed with skepticism. It is not yet known, for instance, how much is too much or too little, and when or whether hormone supplements should be taken at all. This fact sheet provides information about what is known so far and what researchers are doing to find out more.
What Is A Hormone?
Hormones are powerful chemicals that help keep our bodies working normally.The term hormone is derived from the Greek word, hormo, which means to set in motion. And that’s precisely what hormones do in the body. They stimulate, regulate, and control the function of various tissues and organs. Made by specialized groups of cells within structures called glands, hormones are involved in almost every biological process including sexual reproduction, growth, metabolism, and immune function. These glands, including the pituitary, thyroid, adrenals, ovaries and testes, release various hormones
44
into the body as needed.
Levels of some hormones like parathyroid hormone, which helps regulate calcium levels in the blood and bone, actually increase as a normal part of aging and may be involved in bone loss leading to osteoporosis. But the levels of a number of other hormones, such as testosterone in men and estrogen in women, tend to decrease over time. In other cases, the body may fail to make enough of a hormone due to diseases and disorders that can develop at any age. When this occurs, hormone supplements—pills, shots, topical (rub-on) gels, and medicated skin patches—may be prescribed.
Unproven claims that taking hormone supplements can make people feel young again or that they can slow or prevent aging have been “hot” news items for several years. The reality is that no one has yet shown that supplements of these hormones prevent frailty or add years to people's lives. And while some supplements provide health benefits for people with genuine deficiencies of certain hormones, they also can cause harmful side effects. In any case, people who have diagnosed hormone deficiencies should take them only under a doctor’s supervision. Remember: More is not necessarily better. The right balance of hormones helps us stay healthy, but the wrong amount might be damaging.
Heed The Warnings
The NIA recognizes that some hormone-like products are available over the counter and can be used without consulting a physician. The Institute discourages individuals from self-medicating with these products for a number of reasons. First, these products are marketed as “dietary supplements”, and therefore are not regulated by the Food and Drug Administration in the same way as drugs. This is an important distinction because the requirements for marketing a dietary supplement are very different from those that apply to hormones marketed as drugs. Unlike drug manufacturers, a firm selling dietary supplements doesn’t need FDA approval of its products and doesn’t need to prove that its products are safe and effective before marketing. Also, there is no specific guarantee that the substance in the container is authentic or that the indicated dosage is accurate. Because of these differing standards, hormone-like substances that are sold as dietary supplements may not be as thoroughly studied as drug products, and, therefore, the potential consequences of their use are not well understood or known. In addition, these over-the-counter products may interfere with other medications you are taking.
Therefore, the NIA does not recommend taking any supplement, including DHEA and melatonin that is touted as an “anti-aging” remedy because no supplement has been proven to serve this purpose. The influence of these supplements on a person’s health is unknown, particularly when taken over a long period of time.
Talk to your doctor if you are interested in any form of hormone supplementation. In fact, you might want to show this fact sheet to your doctor to help explain your concerns.
45

How Hormones Work
Most hormones exist in very low concentrations in the bloodstream. Each hormone molecule travels through the blood until it reaches a cell with a receptor that it matches. Then, the hormone molecule latches onto the receptor and sends a signal into the cell. These signals may instruct the cell to multiply, to make proteins or enzymes, or to perform other vital tasks. Some hormones can even stimulate a cell to release other hormones. However, no single hormone affects all cells in the same way. One hormone, for example, may stimulate a cell to perform one task, while the same hormone can have an entirely different influence over another cell. The response of some cells to hormonal stimulation also may change throughout life.
Hormone supplements, particularly if taken without medical supervision, may adversely affect this complex system. These supplements, for instance, may not behave exactly the same way as our own naturally produced hormones have because the body may process them differently. In addition, natural hormone production isn’t constant, so circulating blood levels may vary significantly over a 24-hour period. Hormone supplements can’t replicate these fluctuations. As a result, high doses of supplements, whether pills, gels, skin patches, or shots, may result in excessive and unhealthy amounts of hormones in the blood. Hormone supplements also may compound any negative effects caused by hormones naturally produced by the body.
Finally, most of the processes in the body are tightly controlled and regulated. Too much stimulation can elicit natural responses to inhibit a hormone’s action. The body’s system of checks and balances is complicated and the notion that hormone supplements can improve function may be an oversimplification.
DHEA
Dehydroepiandrosterone or DHEA is made from cholesterol by the adrenal glands, which sit on top of each kidney. Production of this substance peaks in the mid-20s, and gradually declines with age in most people. What this drop means or how it affects the aging process, if at all, is unclear. In fact, scientists are somewhat mystified by DHEA and have not fully sorted out what it does in the body. However, researchers do know that the body converts DHEA into two hormones that are known to affect us in many ways: estrogen and testosterone (see below).
Supplements of DHEA can be bought without a prescription and are sold as “anti-aging remedies.” Some proponents of these products claim that DHEA supplements improve energy, strength, and immunity. DHEA is also said to increase muscle and decrease fat. Right now there is no consistent evidence that DHEA supplements do any of these things in people, and there is little scientific evidence to support the use of DHEA as a “rejuvenating” hormone. Although the long-term (over one year) effects of DHEA supplements have not been studied, there are early signs that these supplements, even
46
when taken briefly, may have several detrimental effects on the body including liver damage.
In addition, some people's bodies make more estrogen and testosterone from DHEA than others. There is no way to predict who will make more and who will make less. Researchers are concerned that DHEA supplements may cause high levels of estrogen or testosterone in some people. This is important because testosterone may play a role in prostate cancer, and higher levels of estrogen are associated with an increased risk of breast cancer. It is not yet known for certain if supplements of estrogen and testosterone, or supplements of DHEA, also increase the risk of developing these types of cancer. In women, high testosterone levels can cause acne and growth of facial hair.
Overall, the studies that have been done so far do not provide a clear picture of the risks and benefits of DHEA. For example, some studies in older people show that DHEA helps build muscle, but other studies do not. Researchers are working to find more definite answers about DHEA's effects on aging, muscles, and the immune system. In the meantime, people who are thinking about taking supplements of this hormone should understand that its effects are not fully known. Some of these unknown effects might turn out to be harmful.
Growth Hormone
Human growth hormone (hGH) is made by the pituitary gland, a pea-sized structure located at the base of the brain, and is important for normal development and maintenance of tissues and organs. It is especially important for normal growth in children.
Studies have shown that injections of supplemental hGH are helpful to certain people. Sometimes children are unusually short because their bodies do not make enough hGH. When they receive injections of this hormone, their growth improves. Young adults who have no pituitary gland (because of surgery for a pituitary tumor, for example) cannot make the hormone and they become obese. When they are given hGH, they lose weight.
Like some other hormones, blood levels of hGH often decrease as people age, but this may not necessarily be bad. At least one epidemiological study, for instance, suggests that people who have high levels of hGH are more apt to die at younger ages than those with lower levels of the hormone. Studies of animals with genetic disorders that suppress growth hormone production and secretion also suggest that reduced growth hormone secretion may prolong survival in some species.
Although there is no conclusive evidence that hGH can prevent aging, some people spend a great deal of money on supplements. These supplements are claimed, by some, to increase muscle, decrease fat, and to boost an individual’s stamina and sense of well being. Shots—the only proven way of getting the body to make use of supplemental hGH —can cost more than $15,000 a year. They are available only by prescription and should be given by a doctor. In any case, people in search of the "fountain of youth" may have a
47

hard time finding a doctor who will give them shots of hGH because so little is known about the long-term risks and benefits of this controversial treatment. Some dietary supplements, known as human growth hormone releasers, are marketed as a low-cost alternative to hGH shots. But claims that these over-the-counter products retard the aging process are unsubstantiated.
While some studies have shown that supplemental hGH does increase muscle mass, it seems to have little impact on muscle strength or function. Scientists are continuing to study hGH, but they are watching their study participants very carefully because side effects can be serious in older adults. These include diabetes and pooling of fluid in the skin and other tissues, which may lead to high blood pressure and heart failure. Joint pain and carpal tunnel syndrome also may occur. A recent report that treatment of children with human pituitary growth hormone increases the risk of subsequent cancer is a cause for concern. Further studies on this issue are needed. Whether older people treated with hGH for extended periods have an increased risk of cancer is unknown.
For now, there is no convincing evidence hGH supplements will improve the health of those who do not suffer a profound deficiency of this hormone.
Melatonin
This hormone is made by the pineal gland, a structure in the brain. Contrary to the claims of some, secretion of melatonin does not necessarily decrease with age. Instead, a number of factors, including light and many common medications, can affect melatonin secretion in people of any age.
Melatonin supplements can be bought without a prescription. Some people claim that melatonin is an anti-aging remedy, a sleep remedy, and an antioxidant (antioxidants protect against "free radicals," naturally occurring oxygen-related molecules that cause damage to the body). Early test-tube studies suggested that, in large doses, melatonin might be effective against free radicals. However, cells produce antioxidants naturally, and in test-tube experiments, cells reduce the amount they make when they are exposed to additional antioxidants.
Claims that melatonin can slow or reverse aging are very far from proven. Studies of melatonin have been much too limited to support these claims and have focused on animals, not people.
Research on sleep shows that melatonin does play a role in our daily sleep/wake cycle, and that supplements, in amounts ranging from 0.1 to 0.5 milligrams, can improve sleep in some cases. If melatonin is taken at the wrong time, though, it can disrupt the sleep/wake cycle. Other side effects may include confusion, drowsiness, and headache the next morning. Animal studies suggest that melatonin may cause some blood vessels to constrict, a condition that could be dangerous for people with high blood pressure or other cardiovascular problems.
48
These side effects are important to keep in mind since the dose of melatonin usually sold in stores - 3 milligrams - can result in amounts in the blood from 10 to 40 times higher than normal. What long -term effects such high concentrations of melatonin may have on the body are still unknown. Until researchers find out more, caution is advised.
Testosterone
Ask an average man about testosterone, and he might tell you that this hormone helps transform a boy into a man. Or, he might tell that you that it has “something” to do with sex drive. Or, if he has read news stories in recent years, he might mention “male menopause,” a condition supposedly caused by diminishing testosterone levels in aging men. In reality, there is scant evidence that this controversial condition, also known as “andropause” or “viropause,” exists.
Testosterone is indeed a vital sex hormone that plays an important role in puberty. But contrary to what some people believe, testosterone isn’t exclusively a male hormone. Women produce small amounts of it in their bodies as well. In men, testosterone is produced in the testes, the reproductive glands that also produce sperm. The amount of testosterone produced in the testes is regulated by the hypothalamus and the pituitary gland.
As men age, their testes often produce somewhat less testosterone than they did during adolescence and early adulthood, when production of this hormone peaks. But it is important to keep in mind that the range of normal testosterone production is large. So while there are some declines in testosterone production with age, most older men stay well within normal limits, and the likelihood that a man will ever experience a major shut down of hormone production similar to a woman's menopause, is remote.
In fact, many of the changes that take place in older men often are incorrectly blamed on decreasing testosterone levels. Some men who have erectile difficulty (impotence), for instance, may be tempted to blame this problem on lowered testosterone. However, in the vast majority of cases, erectile difficulties are due to circulatory problems, not low testosterone.
Still, a small percentage of men may be helped by testosterone supplements. These supplements are prescribed for men whose bodies make very little or no testosterone—for example, men whose pituitary glands have been destroyed by infections or tumors, or whose testes have been damaged. For these few men who have extreme testosterone deficiencies, supplements in the form of patches, injections, or topical gel may offer substantial benefit. Supplements may help a man with exceptionally low testosterone levels maintain strong muscles and bones, and increase sex drive. However, what effects testosterone replacement may have in healthy older men without these extreme deficiencies requires more research.
The NIA is investigating the role of testosterone supplementation in delaying or preventing frailty. Results from preliminary studies involving small groups of men have
49

been inconclusive, and it remains unclear to what degree supplementation of this hormone can sharpen memory or help men maintain stout muscles, sturdy bones, and robust sexual activity.
Many other questions remain about the use of this hormone in late life. It is unclear, for example, whether men who are at the lower end of the normal range of testosterone production would benefit from supplementation. Some investigators are also concerned about the long-term harmful effects that supplemental testosterone might have on the aging body. It is not yet known, for instance, if testosterone supplements increase the risk of prostate cancer, the second leading cause of cancer death among men. In addition to potentially promoting new prostate cancers, testosterone also may promote the growth of those that have already developed. Studies also suggest that supplementation might trigger excessive red blood cell production in some men. This side effect can thicken blood and increase a man's risk of stroke.
The bottom line: Although some older men who have tried these supplements report feeling "more energetic" or "younger,” testosterone supplementation remains a scientifically unproven method for preventing or relieving any physical and psychological changes that men with normal testosterone levels may experience, as they get older. Until more scientifically rigorous studies are conducted, the question of whether the benefits of testosterone replacement outweigh any of its potential negative effects will remain unanswered.
Menopausal Hormones
Unlike other hormones described in this fact sheet, many large, reliable, long-term studies of estrogen and its effects on the body have been conducted. These studies suggested that estrogen could provide many important benefits. Based on this early research many women were advised to take supplements of estrogen to relieve the symptoms of menopause and to reduce their risk of osteoporosis and heart disease.
But estrogen also is a good example of why it is important to wait until researchers have discovered both the benefits and risks of a hormone supplement before it becomes widely used. While some women are helped by estrogen during and after menopause, others are placed at higher risk for certain diseases if they take it. As research yields new information about this hormone, women and their doctors continue to reevaluate their thinking about who should take estrogen supplements and who should not.
For many women, the helpful effects of estrogen might outweigh the possible harmful effects when taken relatively briefly around the time of menopause. Estrogen supplements decrease hot flashes and vaginal dryness, and lower the risk for osteoporosis, a bone-thinning disease that often disables older people. Estrogen therapy also may improve mood and psychological well-being.
Yet for all of its promise, estrogen supplementation also has raised a number of serious concerns because some harmful effects are more likely to occur in certain women. For
50
example, estrogen is associated with an increased risk of cancer of the uterus among women who have not had a hysterectomy. To counteract this risk, a woman with a uterus is advised to take progestin, a synthetic form of the hormone progesterone, with their estrogen.
Using estrogen alone or with progestin is called menopausal hormone therapy (MHT). Early studies suggested menopausal hormone therapy could lower the risk for heart disease (the number-one killer of women in the U.S.) in postmenopausal women. But subsequent research now suggests that such therapy might actually elevate some women’s chances of developing this disease. Menopausal hormone therapy also increases a woman’s risk of getting blood clots, which can block circulation in arteries and could lead to heart attack or stroke.
In 2002, an important study of menopausal hormone therapy by the Women’s Health Initiative, which is funded by the National Institutes of Health, was stopped after 5.2 years because serious health concerns arose. The investigators found that among every 10,000 women taking a combination of progestin and estrogen, there would be:
8 more cases of breast cancer than in women not using any hormones, which translates into a 26 percent increased risk,
7 more cases of heart disease (a 29 percent increased risk), 8 more cases of stroke (a 41 percent increased risk), and 8 more women who developed blood clots in their lungs, which is twice the rate
occurring among women not taking any hormones.
But there also would be health benefits:
5 fewer cases of hip fracture (a 34 percent reduced risk), and 6 fewer cases of colorectal cancer (a 37 percent reduced risk).
The study was stopped early because the experts believed that by that time the health risks were greater than the health benefits. These risks are still small ones for an individual woman, but it is an important public health issue. The portion of the study looking at hysterectomized women using only estrogen without progestin did not find similar risks, so it will continue.
Some studies suggest that estrogen may protect against Alzheimer's disease, but this has not yet been proven. In fact, in 2003 a related study, the Women’s Health Initiative Memory Study, reported that women age 65 and older taking a combination of estrogen plus progestin were at twice the risk of developing dementia as women not taking any hormones. This means that every year there would be 23 additional cases of dementia in 10,000 women 65 and older taking these hormones compared to 10,000 women the same age not taking any hormones (a 105% increased risk). As with the larger Women’s Health Initiative trial, the estrogen alone portion of this study is continuing.
51

So the decision whether to take estrogen is now far more complex and difficult. Although researchers have studied estrogen for many years, numerous questions about this hormone—once thought answered—are reemerging. Before choosing this treatment, each woman, with the guidance and advice of her doctor, should weigh the pros and cons of menopausal hormone therapy and make an informed choice based on a realistic assessment of her personal risks and benefits.
Keep in mind that even after years of intense study, researchers continue to discover information about the benefits and risks of these menopausal hormones. As these new findings emerge, women and their doctors may have to frequently reassess their decisions about these supplements.
Many Questions, Few Answers
The NIA sponsors many research projects that will reveal more about the risks and benefits of hormone supplements. One goal is to determine whether DHEA, melatonin, and other hormonal supplements improve the health of older people, have no effect, or are actually harmful.
It is important to remember that these studies may not give immediate or final answers, especially in the cases of DHEA, melatonin, and hGH, since research on these supplements is fairly new. For example, some of the studies may simply give researchers more information about what kinds of questions they should ask in their next studies. Research is a step-by-step process, and larger studies may be needed to give more definitive answers.
Until more is known about DHEA, melatonin, and hGH, consumers should view them with a good deal of caution - and doubt. Despite what advertisements or stories in the media may claim, hormone supplements have not been proven to prevent aging. Some harmful side effects already have been discovered, and further research may uncover others.
More is known about estrogen and testosterone, and people who are concerned about genuine deficiencies of these hormones should consult with their doctors about supplements. Meanwhile, people who choose to take any hormone supplement without a doctor's supervision should be aware that these supplements appear to have few clear-cut benefits for healthy individuals, and no proven influence on the aging process.
National Institute on AgingU. S. Department of Health and Human ServicesPublic Health ServiceNational Institutes of HealthAugust 2003
52
Consejos para Dormir Bien
Todos queremos dormir bien. El dormir suficiente y bien nos ayuda a permanecer sanos. Muchas personas de la tercera edad no logran dormir bien todas las noches, sienten dificultad en conciliar el sueño o en permanecer dormidas. Los patrones del sueño cambiancon la edad, pero dormir mal y despertarse cansado todos los días no forma parte del envejecimiento normal. De hecho, la dificultad para dormir puede ser un síntoma de algún trastorno emocional o físico y es algo que se debe comentar con el médico o un especialista del sueño.
El Sueño Y La Tercera Edad
Existen dos períodos de sueño en un ciclo normal de sueño — el sueño agitado (REM, por las siglas en inglés de “rapid eye movement” o movimiento ocular rápido) y el sueño sosegado No-REM (Non-REM, por sus siglas en inglés). Las personas tienen cerca de cuatro o cinco ciclos de REM y No-REM en la noche. En las personas de la tercera edad, el tiempo que pasan en las etapas más profundas del sueño No-REM disminuye. Esto puede explicar por qué se dice que las personas de la tercera edad tienen el sueño ligero.
Aunque la cantidad de horas de sueño que necesitan las personas varía enormemente, el promedio es entre 7 y 8 horas por noche. Al avanzar la edad, la cantidad total de sueño tiende a disminuir. A los 75 años, por muchas razones, algunas personas empiezan a despertarse varias veces por noche. Pero independientemente de la edad, consulte conel médico si sus patrones de sueño cambian.
Problemas Comunes del Sueño
A cualquier edad, la queja más común sobre el sueño es el insomnio. El insomniose caracteriza por:
Dificultad en conciliar el sueño (más de 30 a 45 minutos) Despertarse muchas veces en la noche
Despertarse temprano y no poder conciliar nuevamente el sueño
Despertarse cansado
Salvo raras excepciones, el insomnio es síntoma de un problema, no el problema en sí.
El insomnio puede estar vinculado con otros trastornos del sueño tales como la apnea, que es un problema común en el cual hay un cese de la respiración por períodos de hasta 2 minutos varias veces en la noche. Hay dos tipos de apnea:
53
Apnea obstructiva, que es una pausa involuntaria en la respiración — el aire no puede entrar ni salir por la boca o por la nariz de la persona;
Apnea central, que es menos común y sucede cuando el cerebro no envía las señales indicadas para estimular los músculos de la respiración.
En ambos casos, la persona desconoce completamente su dificultad para respirar. La somnolencia durante el día, además de los fuertes ronquidos durante la noche, son indicaciones de posible apnea. Un médico especializado en trastornos del sueño puede hacer el diagnóstico y recomendar un tratamiento.
Los tratamientos incluyen aprender a dormir en una posición correcta, dispositivos que ayudan a mantener las vías respiratorias abiertas, medicamentos o cirugía.
Sugerencias Para Dormir Bien
El dormir bien por la noche afecta enormemente cómo la persona se siente. Aquí encontrará algunas sugerencias:
Mantenga un horario regular, acuéstese y levántese a la misma hora cada día. Trate de no dormir mucho durante el día, puede sentir menos sueño por la noche.
Trate de hacer ejercicio en un horario regular todos los días.
Trate de aprovechar la luz natural en las tardes todos los días.
Tenga cuidado con lo que come. No tome bebidas con cafeína después de una cierta hora. La cafeína es un estimulante y puede mantenerlo despierto. Además, si le apetece un bocado antes de ir a dormir, una bebida caliente y algunas galletas pueden servirle.
No beba alcohol ni fume para poder dormir mejor. Aún una cantidad pequeña de alcohol puede hacer que sea difícil permanecer dormido. Fumar es peligroso pormuchas razones, incluso por el peligro de quedarse dormido con un cigarrillo encendido. La nicotina también es un estimulante.
Haga que el lugar donde duerme sea seguro y cómodo. Cerciórese que todas las puertas estén cerradas con llave y que todos los pisos tengan alarma contra incendios. Puede ser útil tener una lámpara que sea fácil de encender y un teléfono asu cabecera. El dormitorio debe ser oscuro y bien ventilado y lo más silencioso posible.
Establezca una rutina a la hora de acostarse. Haga las mismas cosas todas las noches para comunicarle al cuerpo que es hora de tranquilizarse. Algunas personas ven algún noticiero, leen un libro o se dan un baño de tina.
54

Use el dormitorio solamente para dormir. Después de apagar la luz, dese cerca de 15 minutos para conciliar el sueño. Si sigue despierto y no está somnoliento, salgade la cama. Cuando le dé sueño nuevamente, vuelva a la cama.
Trate de no preocuparse por dormir. A algunas personas les ayuda jugar algún juegomental. Por ejemplo, piense en algo negro — un gato negro en una almohadilla de terciopelo negro en un sofá de pana negra etc.; o haga de cuenta que tiene que levantarse en 5 minutos y que sólo está tratando de dormir cinco minutitos más.
Si está tan cansado(a) durante el día que no puede actuar normalmente, y si esto dura más de 2 o 3 semanas, debe consultar con su médico o con un especialista de trastornos del sueño.
Fuentes de Información Adicionales
Para recibir información general sobre el sueño, puede comunicarse conlas siguientes organizaciones:
American Sleep Apnea Association(Asociación Estadounidense de la Apnea del Sueño)1424 K Street NWSuite 302Washington, D.C. 20005202- 293-3650http://www.sleepapnea.org
Better Sleep Council(Concilio para el Buen Dormir)501 Wythe StreetAlexandria, Virginia 22314703-683-8371http://www.bettersleep.org
Narcolepsy Network(Red de la Narcolepsia)10921 Reed Hartman HighwaySuite 119Cincinnati, Ohio 45242513- 891-3522http://www.narcolepsynetwork.org
National Center for Sleep Disorders Research(Centro Nacional de Investigación de Trastornos del Sueño)One Rockledge Center, Suite 60226705 Rockledge Drive
55
Bethesda, Maryland 20892-7993301-435-0199http://www.nhlbi.nih.gov/health/public/sleep
National Sleep Foundation(Fundación Nacional del Sueño)1522 K Street, NWSuite 500Washington, D.C. 20005-1253202-347-3471http://www.sleepfoundation.org
56
Restless Legs Syndrome Foundation(Fundación del Síndrome de Piernas In819 Second Street, SWRochester, Minnesota 559002507-287-6465http://www.rls.org
Para más información gratis sobre la salud y envejecimiento, contacte a:
National Institute on Aging Information Center(Centro de Información del Instituto Nacional Sobre el Envejecimiento)P.O. Box 8057Gaithersburg, Maryland 20898-80571-800-222-22251-800-222-4225 (TTY)http://www.nih.gov/nia
Instituto Nacional Sobre el EnvejecimientoDepartamento de Salud y Servicos Humanos de los Estados UnidosInstitutos Nacionales de SaludJulio de 2003
57
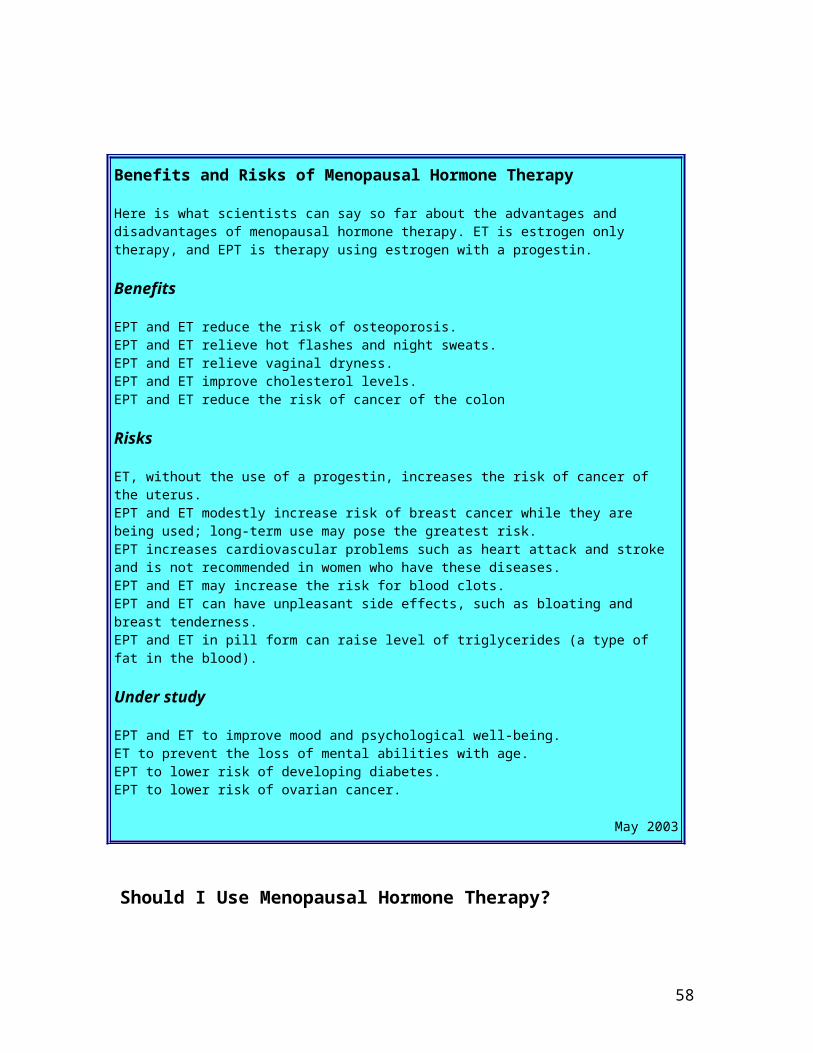
A Good Night's Sleep
We all look forward to a good night's sleep. Getting enough sleep and sleeping well help us stay healthy. Many older people do not enjoy a good night's sleep on a regular basis. They have trouble falling or staying asleep. Sleep patterns change as we age, but disturbed sleep and waking up tired every day is not part of normal aging. In fact, troubled sleep may be a sign of emotional or physical disorders and something you should talk about with a doctor or sleep specialist.
Sleep and Aging
There are two kinds of sleep in a normal sleep cycle - rapid eye movement or dreaming sleep (REM) and quiet sleep (non-REM). Everyone has about four or five cycles of REM and non-REM sleep a night. For older people, the amount of time spent in the deepest stages of non-REM sleep decreases. This may explain why older people are thought of as light sleepers. Although the amount of sleep each person needs varies widely, the average range is between 7 and 8 hours a night. As we age, the amount of sleep we can expect to get at any one time drops off. By age 75, for many reasons, some people may find they are waking up several times each night. But, no matter what your age, talk to a doctor if your sleep patterns change.
Common Sleep Problems
At any age, insomnia is the most common sleep complaint. Insomnia means:
Taking a long time to fall asleep (more than 30 to 45 minutes) Waking up many times each night Waking up early and being unable to get back to sleep Waking up feeling tired
With rare exceptions, insomnia is a symptom of a problem, not the problem itself.Insomnia can be linked with other sleep disorders such as sleep apnea, a common problem that causes breathing to stop for periods of up to 2 minutes, many times each night.
There are two kinds of sleep apnea: Obstructive sleep apnea is an involuntary pause in breathing - air cannot flow in or out of the person's nose or mouth. Central sleep apnea is less common and occurs when the brain doesn't send the right signals to start the breathing muscles.
In either case, the sleeper is totally unaware of his or her struggle to breathe. Daytime sleepiness coupled with loud snoring at night are clues that you may have sleep apnea. A doctor specializing in sleep disorders can make a diagnosis and recommend treatment. Treatments include learning to sleep in the correct position, devices that help keep your airways open, medication, and surgery.
58

Suggestions for a Good Night's Sleep
A good night's sleep can make a big difference in how you feel. Here are some suggestions to help you:
Follow a regular schedule - go to sleep and get up at the same time. Try not to nap too much during the day - you might be less sleepy at night. Try to exercise at regular times each day. Try to get some natural light in the afternoon each day. Be careful about what you eat. Don't drink beverages with caffeine late in the day. Caffeine is a stimulant and can keep you awake. Also, if you like a snack before bed, a warm beverage and a few crackers may help. Don't drink alcohol or smoke cigarettes to help you sleep. Even small amounts of alcohol can make it harder to stay asleep. Smoking is dangerous for many reasons including the hazard of falling asleep with a lit cigarette. The nicotine in cigarettes is also a stimulant. Create a safe and comfortable place to sleep. Make sure there are locks on all doors and smoke alarms on each floor. A lamp that's easy to turn on and a phone by your bed may be helpful. The room should be dark, well ventilated, and as quiet as possible. Develop a bedtime routine. Do the same things each night to tell your body that it's time to wind down. Some people watch the evening news, read a book, or soak in a warm bath. Use your bedroom only for sleeping. After turning off the light, give yourself about 15 minutes to fall asleep. If you are still awake and not drowsy, get out of bed. When you get sleepy, go back to bed. Try not to worry about your sleep. Some people find that playing mental games is helpful. For example, think black - a black cat on a black velvet pillow on a black corduroy sofa, etc.; or tell yourself it's 5 minutes before you have to get up and you're just trying to get a few extra winks.
If you are so tired during the day that you cannot function normally and if this lasts for more than 2 to 3 weeks, you should see your family doctor or a sleep disorders specialist.
Additional Information Sources
For general information about sleep, contact the following organizations:
American Sleep Apnea Association1424 K Street NW,Suite 302Washington, D.C. 20005202-293-3650http://[email protected]
59

Better Sleep Council501 Wythe StreetAlexandria, Virginia 22314 703-683-8371http://www.bettersleep.org
Narcolepsy Network10921 Reed Hartman HighwaySuite 119Cincinnati, Ohio 45242513-891-3522http://www.narcolepsynetwork.org
National Center for Sleep Disorders ResearchTwo Rockledge Center, Suite 100386701 Rockledge Drive, MSC 7920Bethesda, Maryland 20892-7920301-435-0199http://www.nhlbi.nih.gov/health/public/sleep
National Sleep Foundation1522 K Street, NWSuite 500Washington, D.C. 20005-1253202-347-3471http://www.sleepfoundation.org
Restless Legs Syndrome Foundation819 Second Street SWRochester, Minnesota 559002507-287-6465http://[email protected]
Sleep Disorders Dental Society11676 Perry HighwayBldg. 1, Suite 1204Wexford, Pennsylvania 15090724-935-0836http://www.thesdds.org
The National Institute on Aging offers a variety of information about health and aging. For a list of publications, contact:
The National Institute on Aging Information Center P.O. Box 8057
60

Gaithersburg, Maryland 20898-80571-800-222-22251-800-222-4225 (TTY)http://www.nih.gov/nia
National Institute on AgingU. S. Department of Health and Human ServicesPublic Health ServiceNational Institutes of HealthMay 2000
61

Constipation
Nearly everyone becomes constipated at one time or another. Usually, it is not serious. To avoid most constipation problems, it helps to know what causes it, how to prevent it, and how to treat it.
Constipation is a symptom, not a disease. You may be constipated if you are having fewer bowel movements than usual, with a long or hard passing of stools. Older people are more likely than younger people to become constipated.
Experts agree that older people often worry too much about having a bowel movement every day. There is no right number of daily or weekly bowel movements. Being regular is different for each person. For some people, it can mean bowel movements twice a day. For others, movements just twice a week are normal.
Questions to Ask
Some doctors suggest asking these questions to decide if you are constipated:
Do you often have fewer than three bowel movements each week?
Do you often have a hard time passing stools?
Is there pain?
Are there other problems such as bleeding?
Did you answer “yes” to more than one of these questions? If so, you may have a constipation problem. Otherwise, you probably do not.
What Causes Constipation?
Doctors do not always know what causes constipation. Eating a poor diet, not drinking enough water, or using laxatives too often can be causes. Also, some medicines can lead to constipation. These include some antidepressants, antacids containing aluminum or calcium, antihistamines, diuretics, and antiparkinsonism drugs.
The role of diet. People may become constipated if they do not eat enough high-fiber foods like vegetables, fruits, and whole grains. Some research shows that high-fiber diets can help prevent constipation. Eating a lot of high-fat meats, dairy products and eggs, or rich desserts and sugary sweets also may cause constipation.
People who live alone sometimes lose interest in cooking and eating. As a result, they start using a lot of prepared foods. These foods tend to be low in fiber, and so may lead to
62
constipation. In addition, bad teeth can cause older people to choose soft, processed foods that contain small amounts of fiber.
People sometimes do not drink enough fluids. This often is true when people are not eating regular meals. But water and other liquids are important. They add bulk to stools, which helps make bowel movements easier.
Misuse of laxatives and enemas. Many people think of laxatives as a cure for constipation. But heavy use of laxatives often is not needed, and laxatives can become habit forming. If you use laxatives too often, your body can begin to rely on them to bring on bowel movements. (Using laxatives too often also can cause diarrhea.) Over time, your body will forget how to work on its own.
For the same reason, if you use enemas too often, your body may begin to depend on them. Too many enemas may stop you from having normal bowel movements. Too much mineral oil, another popular laxative, can lower your body’s ability to use key vitamins (A, D, E, and K). Sometimes mineral oil, if taken along with other drugs that stop blood clots (anticoagulants), can cause unwanted side effects.
Other causes of constipation. Lack of exercise or long periods in bed, such as after an accident or illness, may cause constipation. Doctors sometimes suggest medicine for people who stay in bed and suffer from chronic constipation. But being more active, when possible, is best.
People also can become constipated if they ignore their natural urge to have a bowel movement. Some people prefer to have bowel movements only at home. But holding in a bowel movement can cause constipation if the delay is too long. In some people, disorders or a blockage of the intestines may cause constipation. These disorders may affect the muscles or nerves responsible for normal bowel movements. A doctor can perform tests to see if a problem like this is the cause of constipation. If so, the problem often can be treated.
Treatment
If you become constipated, first see your doctor to rule out a more serious problem. If test results show no disease or blockage, and if your doctor approves, try these remedies:
Increase fiber by eating more fresh fruits and vegetables, either cooked or raw, and more whole-grain cereals and breads. Dried fruit such as apricots, prunes, and figs are especially high in fiber.
Drink plenty of liquids (1 to 2 quarts daily), unless you have heart, blood vessel, or kidney problems. (But keep in mind that some people can become constipated from drinking large amounts of milk.)
63
Some doctors suggest adding small amounts of unprocessed bran (“miller’s bran”) to baked goods, cereals, and fruit. Some people suffer from bloating and gas for several weeks after adding bran to their diets. Make diet changes slowly to allow your digestive system to adapt. Remember, if your diet is well balanced and contains a variety of foods high in natural fiber, it may not be necessary to add bran to other foods.
Stay active.
Do not expect to have a bowel movement every day or even every other day. Remember, being regular is different for each person. If your bowel movements are usually painless and occur regularly (whether 2 times a day or 3 times a week), you are probably not constipated.
If you still have concerns about constipation, check with your doctor to find out what youshould do.
Resources
You can get more information about constipation from:
The National Digestive Diseases Information Clearinghouse 2 Information Way Bethesda, MD 20892-3570 1-800-891-5389 301-654-3810 E-mail: [email protected] http://www.niddk.nih.gov
For more information about health and aging, call or write:
National Institute on AgingInformation Center P.O. Box 8057 Gaithersburg, MD 20898-8057 1-800-222-2225 1-800-222-4225 (TTY) E-mail: [email protected] http://www.nia.nih.gov
National Institute on Aging U.S. Department of Health and Human Services National Institutes of Health January 2002
64

Medicines: Use Them Safely
People age 65 and older consume more prescription and over-the-counter (OTC) medicines than any other age group. Older people tend to have more long-term, chronic illnesses — such as arthritis, diabetes, high blood pressure and heart disease — than do younger people. Because they may have a number of diseases or disabilities at the same time, it is common for older people to take many different drugs.
Many older people owe their health in part to new and improved medicines and vaccines. But using medicines may be riskier for older adults, especially when several medicines are used at one time. Taking different medicines is not always easy to do right. It may be hard to remember what each medicine is for, how you should take it and when you should take it. This is especially true of people with memory problems or dementia.
The kidneys and liver are two important organs that process and remove most drugs from the body. As we age, these organs may not work as well as they used to and drugs may leave more slowly.
Medicines may act differently in older people than in younger people. This may be because of normal changes in the body that happen with age. For instance, as we get older, we lose water and lean tissue (mainly muscle) and we gain more fat tissue. This can make a difference in how long a drug stays in the body.
Keep in mind that “drugs” can mean both medicines prescribed by your doctor and over-the-counter (OTC) medicines, which you buy without a doctor’s prescription. OTC’s can include vitamins and minerals, herbal and dietary supplements, laxatives, cold medicines, and antacids. Taking some OTC’s together with prescription medicines can cause serious problems. For example, aspirin should not be taken with warfarin (Coumadin). Be sure your doctor knows what medicines you are taking and assures you that it is safe for you to take your medicines together. Also ask about taking your medicines with food. If you take alendronate (Fosamax) with food, for example, the drug will be less effective. Herbal supplements also should be taken with care. Gingko biloba, for instance, should not be taken with aspirin, acetaminophen, warfarin, or thiazide diuretics because it may increase blood pressure and the risk of bleeding problems.
You and your family should learn about the medicines that you take and their possible side effects. Remember, medicines that are strong enough to cure you can also be strong enough to hurt you if they aren’t used correctly. Here are some hints to help avoid risks and get the best results from your medicines:
At Home
DO keep a daily checklist of all the medicines you take. Include both prescription and OTC medicines. Note the name of each medicine, the doctor who prescribed it, the
65

amount you take, and the times of day you take it. Keep a copy in your medicine cabinet and one in your wallet or pocketbook. DO read and save any written information that comes with the medicine. DO check the label on your medicine before taking it to make sure that it is for the correct person — you — with the correct directions prescribed for you by your doctor. DO take medicine in the exact amount and precise schedule your doctor prescribes. DO check the expiration dates on your medicine bottles and throw away medicine that has expired. DO call your doctor right away if you have any problems with your medicines or if you are worried that the medicine might be doing more harm than good. He or she may be able to change your medicine to another one that will work just as well. DO NOT take medicines prescribed for another person or give yours to someone else. DO NOT stop taking a prescription drug unless your doctor says it’s okay — even if you are feeling better. DO NOT take more or less than the prescribed amount of any medicine. DO NOT mix alcohol and medicine unless your doctor says it’s okay. Some medicines may not work well or may make you sick if taken with alcohol.
At Your Doctor's Office
DO review your medicine record with the doctor or nurse at every visit and whenever your doctor prescribes new medicine. Your doctor may have new information about your medicines that might be important to you. DO always tell your doctor or nurse about past problems you have had with medicines, such as rashes, indigestion, dizziness or not feeling hungry. DO always ask your doctor or nurse about the right way to take any medicine before you start to use it. DO ask these questions (and write down the answers) before leaving your doctor’s office:
– What is the name of the medicine and why am I taking it?– What is the name of the condition this medicine will treat?– How does this medicine work?– How often should I take it?– How long will it take to work?– How will I know if this medicine is working?– How can I expect to feel once I start taking this medicine?– When should I take it? As needed? Before, with or between meals? At bedtime?– If I forget to take it, what should I do?– What side effects might I expect? Should I report them?– How long will I have to take it?– Can this medicine interact with other medicines (prescription and OTC’s including herbal and dietary supplements) that I am taking now?– If I don’t take medicine, is there anything else that would work as well?
At the Pharmacy
66
DO make sure you can read and understand the medicine name and the directions on the container. If the label is hard to read, ask your pharmacist to use larger type. Let your pharmacist know if you have trouble opening the medicine bottle. DO check the label on your medicine before leaving the pharmacy to make sure that it is for the correct person — you — and with the correct directions prescribed for you by your doctor. If not, tell the pharmacist.
Resources
The U.S. Food and Drug Administration (FDA), Consumer Affairs Office has more information about safe use of medicines. Contact:FDA5600 Fishers LaneHFD - 210Rockville, Maryland 20857Telephone: 1-888-INFOFDA(1-888-463-6332)
The Peter Lamy Center for Drug Therapy and Aging has brochures and information about medication use in the elderly. Contact:University of MD School of Pharmacy5506 West Fayette Street, Suite 101Baltimore, Maryland 21201Telephone: 410-706-3011 (within Maryland) or 1-877-706-2434 (toll free outside Maryland)Fax: [email protected]
The National Institute on Aging (NIA) distributes a free booklet, Talking with Your Doctor: A Guide for Older People. To order this booklet or other free materials on health and aging, contact:The National Institute on Aging Information CenterP.O. Box 8057Gaithersburg, Maryland 20898-8057Telephone: 1-800-222-2225TTY: 1-800-222-4225http://www.nia.nih.gov
National Institute on AgingU. S. Department of Health and Human ServicesPublic Health ServiceNational Institutes of Health2000
67






![CAS ACADÈMIA3.ppt [Modo de compatibilidad] · HORMONES BASALS HIPOFISÀRIES TSH 0.06 µU/ml T4L 0.66 ng/dL FSH 0.89 mUI/mL LH < 0.8 mUI/mL Test tot < 0.1 ng/dL Test lliure < 0.5](https://static.fdocuments.ec/doc/165x107/5f18aa5a3044fd59f1343678/cas-acadmia3ppt-modo-de-compatibilidad-hormones-basals-hipofisries-tsh-006.jpg)










