Nutrición en Pacientes con Insuficiencia Renal...
33
“ Nutrición en Pacientes con Insuficiencia Renal Crónica ” Dr. Tommasso Bochicchio Fresenius Medical Care, Morelos
Transcript of Nutrición en Pacientes con Insuficiencia Renal...
“Nutrición en Pacientes con
Insuficiencia Renal Crónica”Dr. Tommasso Bochicchio Fresenius Medical Care,
Morelos
100
010203040
9080706050
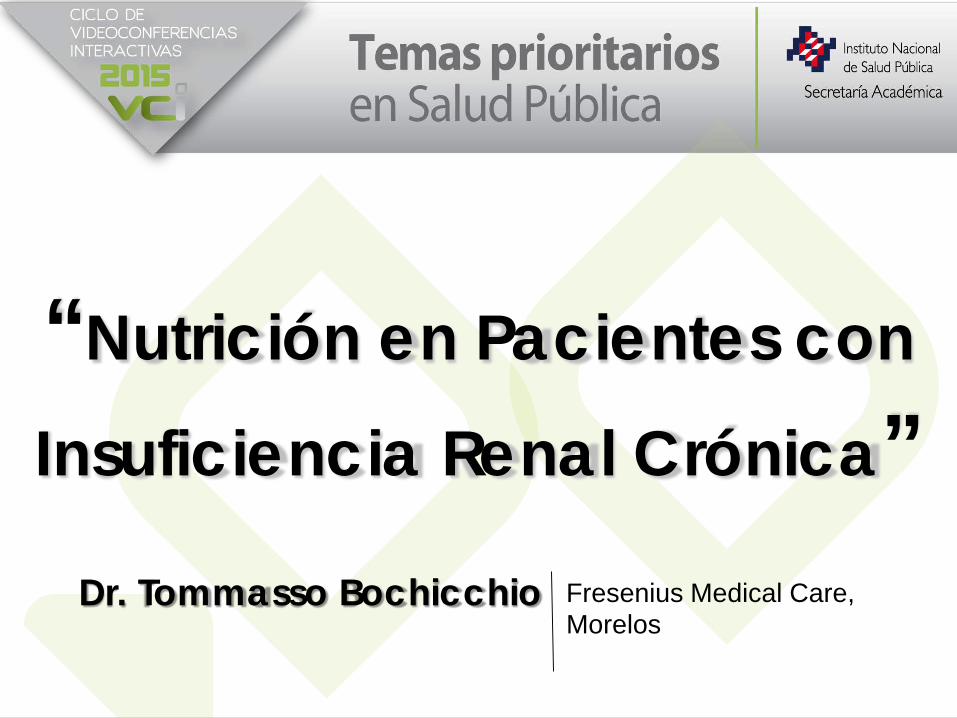
Etapas / FGFGml/min/1.73m2
Etapas de la Insuficiencia Renal Descripción Prevalent *
(pmh)
Etapa 1> 90
Daño renal con FG normal o ↑ 61,653 Escrutinio: reducción de
riesgos para IRC
Acciones
Etapa 260 - 89
Daño renal con ↓ leve de la FG 35,148
Dx y tratamiento de condiciones
comorbilidad, reducción de la progresión y riesgo
cardiovascular
Etapa 330 - 59
Daño renal con ↓ moderada de la FG 24,834 Disminuir la progresión
Etapa 415 - 29
Daño renal con ↓ severa de la FG 1,707 Preparación para terapias
de remplazo
Etapa 5< 15
IR en tratamiento substitutivo 1,233 Terapia de remplazo en
presencia de uremiaAdaptado de Am J Kidney Dis 2002; 39 (2,Suppl. 1): S17-S31
* Insuficiencia Renal Crónica y Atención Mediante Tratamiento de Sustitución. UNAM
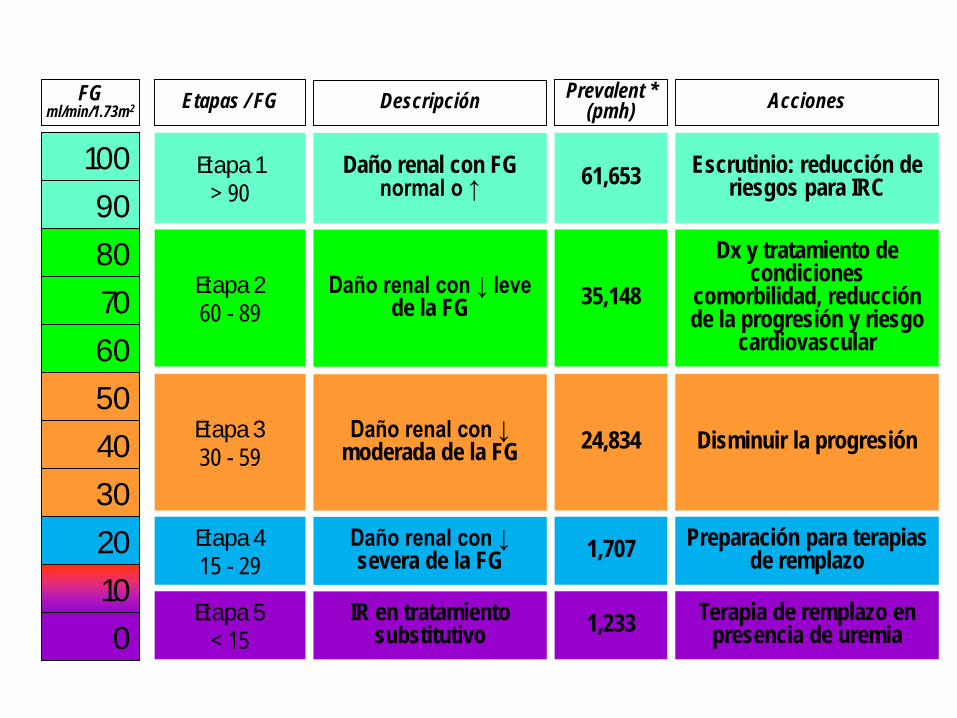
BALANCE DE FACTORES EN LOS RESULTADOSPrimer Foro Bioético sobre la Enfermedad Renal
Tecnología
Políticas de Salud
Epidemiología
Recursos Humanos
AtenciónNefrológica
Final
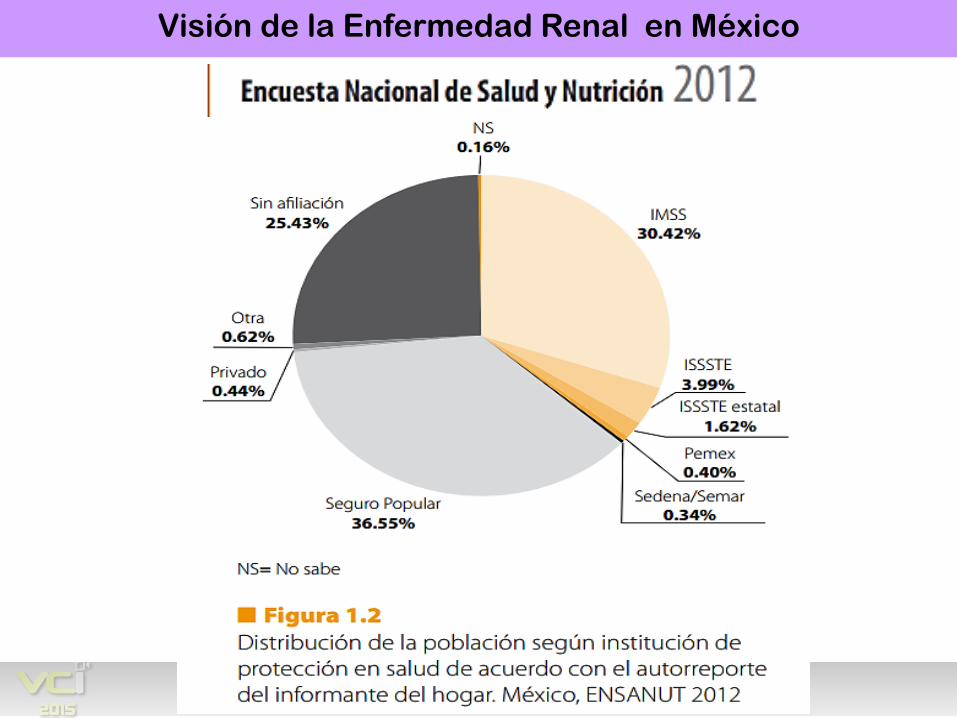
Visión de la Enfermedad Renal en México
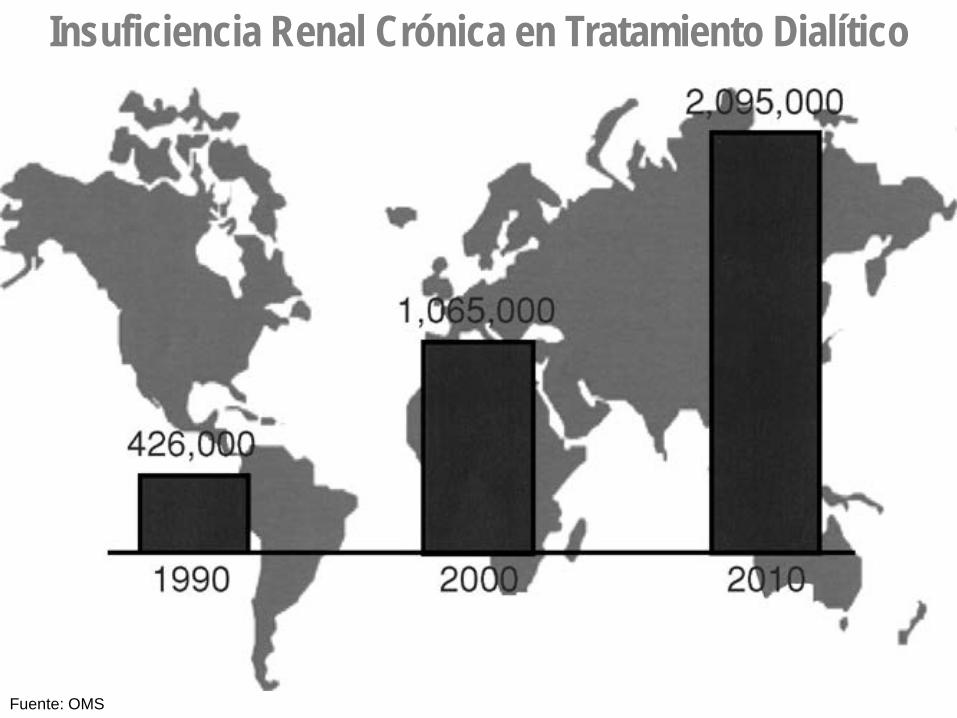
Insuficiencia Renal Crónica en Tratamiento Dialítico
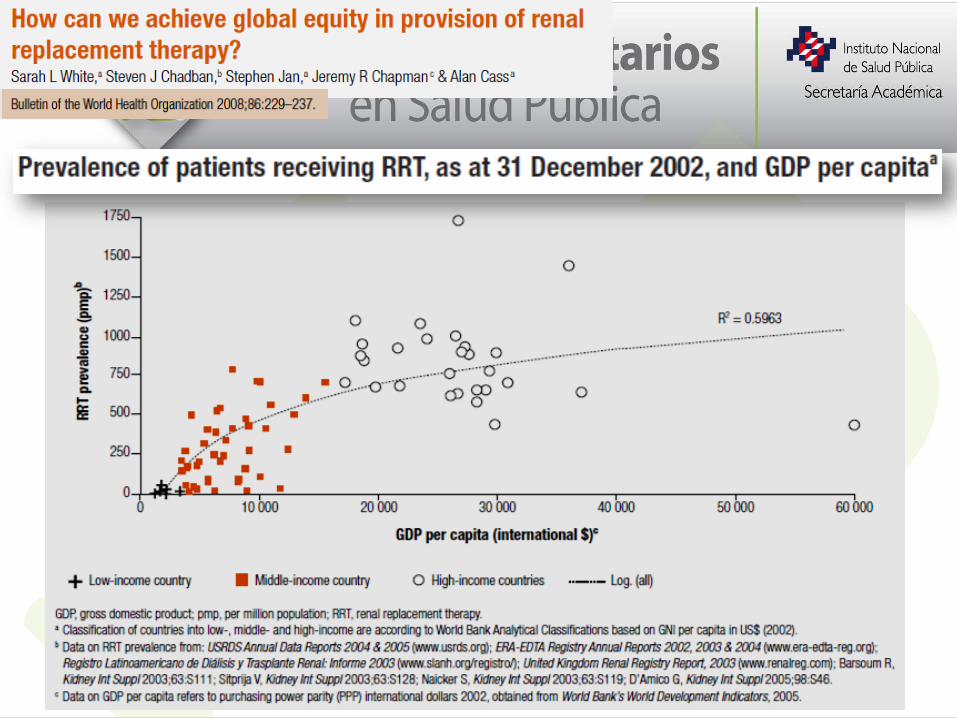
Fuente: OMS
PLANTEAMIENTO
¿ Cuántos pacientes hay y cuantos debería de haber ?
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
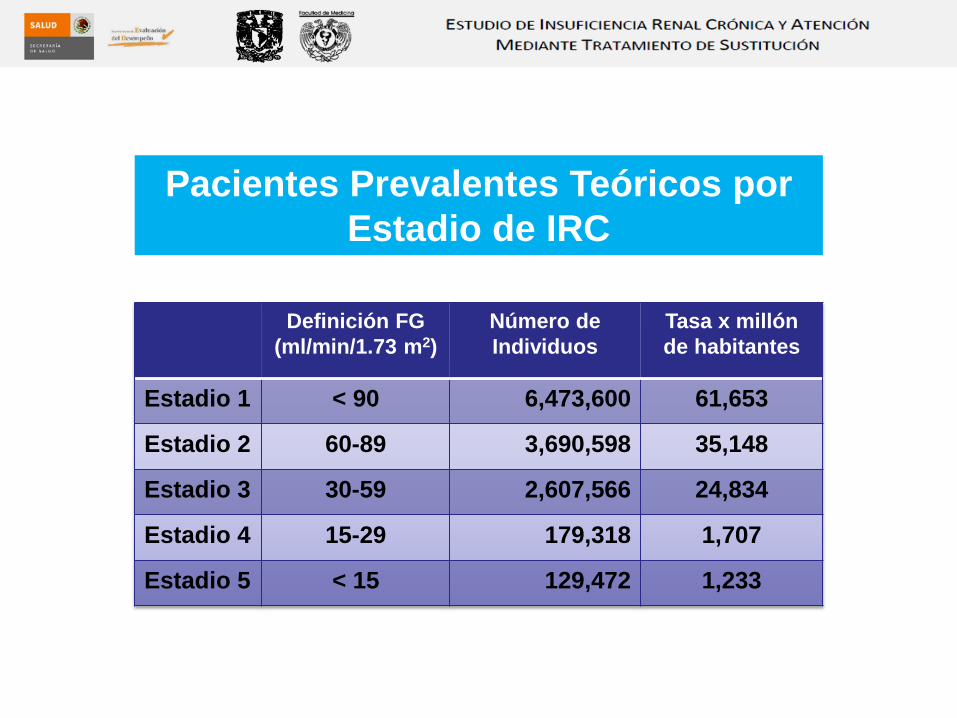
Definición FG (ml/min/1.73 m2)
Número de Individuos
Tasa x millón de habitantes
Estadio 1 < 90 6,473,600 61,653
Estadio 2 60-89 3,690,598 35,148
Estadio 3 30-59 2,607,566 24,834
Estadio 4 15-29 179,318 1,707
Estadio 5 < 15 129,472 1,233
Pacientes Prevalentes Teóricos porEstadio de IRC
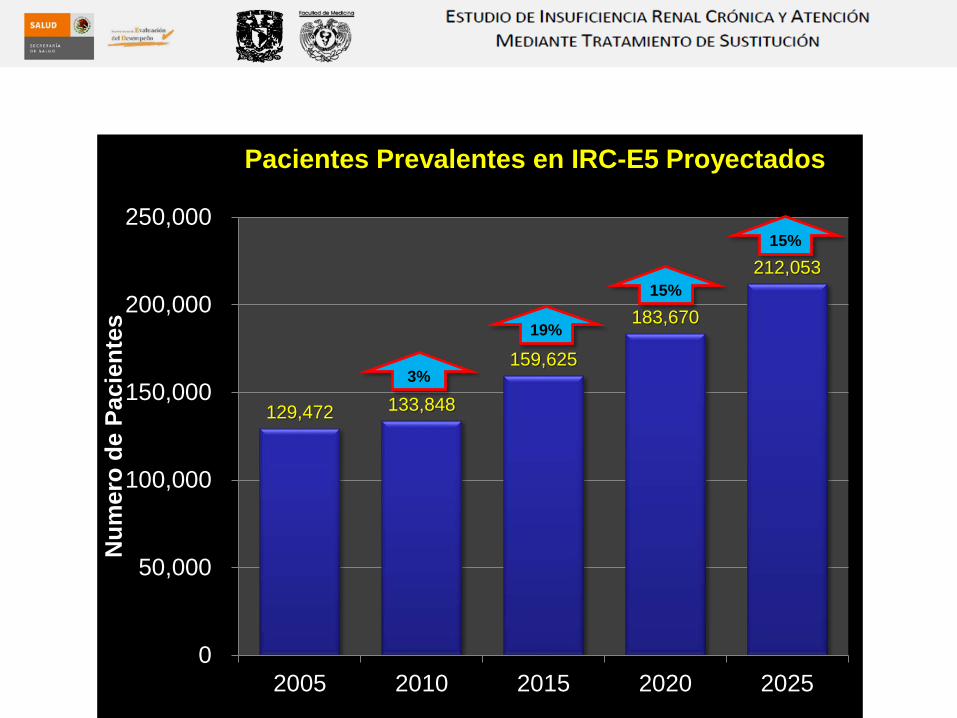
129,472 133,848
159,625
183,670
212,053
0
50,000
100,000
150,000
200,000
250,000
2005 2010 2015 2020 2025
Num
ero
de P
acie
ntes
Pacientes Prevalentes en IRC-E5 Proyectados
3%
15%
19%
15%
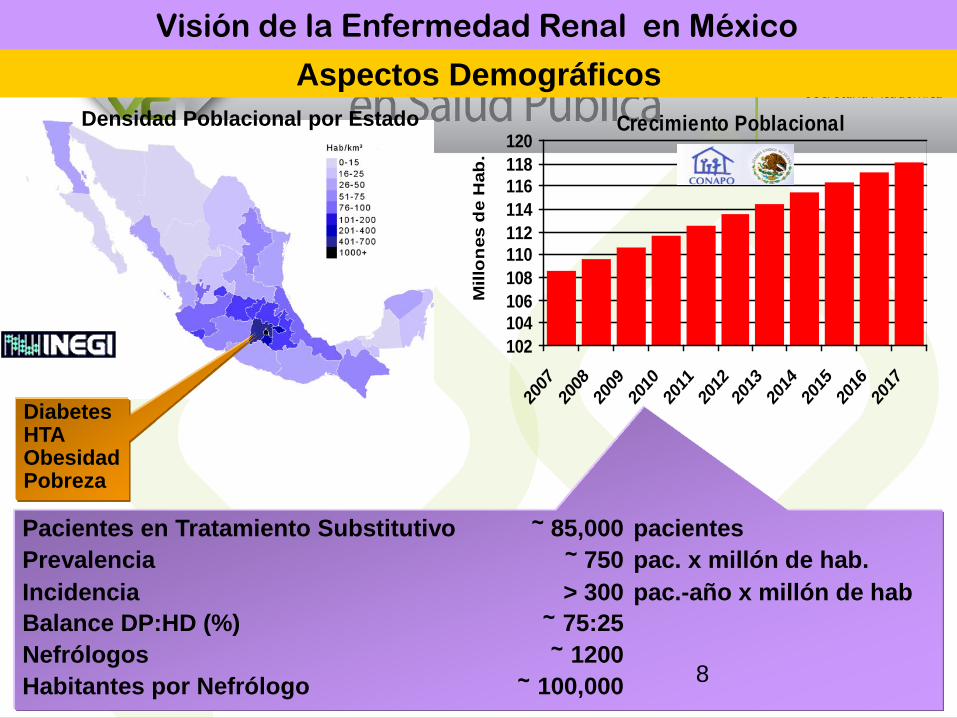
Crecimiento Poblacional
102104106108110112114116118120
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
Mill
on
es d
e H
ab.
Aspectos DemográficosDensidad Poblacional por Estado
Pacientes en Tratamiento Substitutivo ~ 85,000 pacientesPrevalencia ~ 750 pac. x millón de hab.Incidencia > 300 pac.-año x millón de habBalance DP:HD (%) ~ 75:25Nefrólogos ~ 1200Habitantes por Nefrólogo ~ 100,000
DiabetesHTAObesidadPobreza
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
8
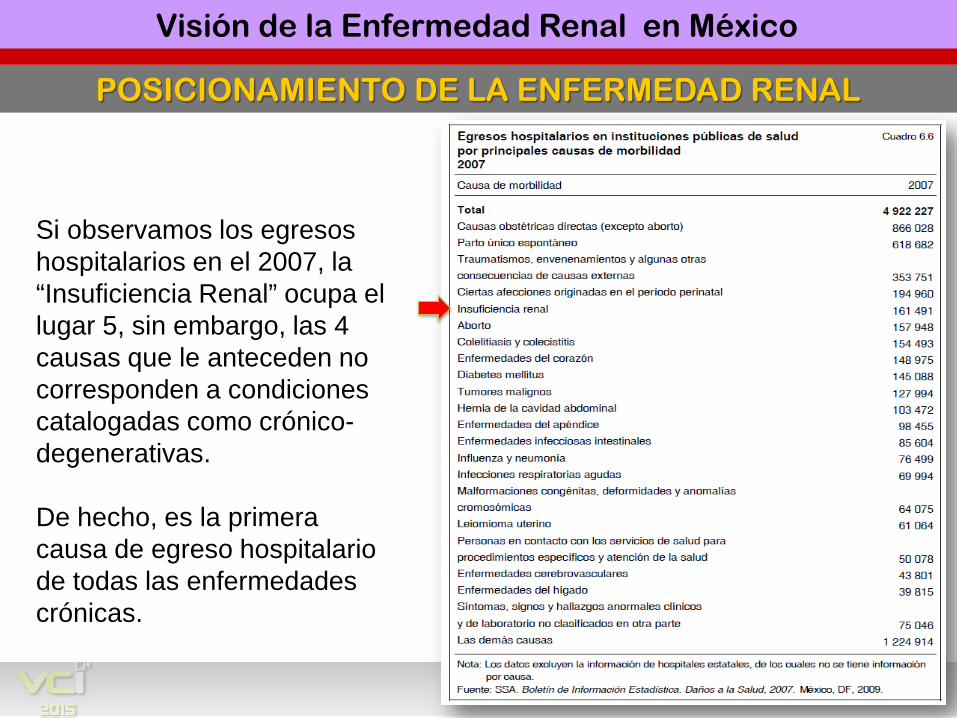
POSICIONAMIENTO DE LA ENFERMEDAD RENAL
Primer Foro Bioético sobre la Enfermedad Renal
Si observamos los egresos hospitalarios en el 2007, la “Insuficiencia Renal” ocupa el lugar 5, sin embargo, las 4 causas que le anteceden no corresponden a condiciones catalogadas como crónico-degenerativas.
De hecho, es la primera causa de egreso hospitalario de todas las enfermedades crónicas.
Visión de la Enfermedad Renal en México
PLANTEAMIENTO
¿ Cuál es la cobertura actual de los pacientes renales ?
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
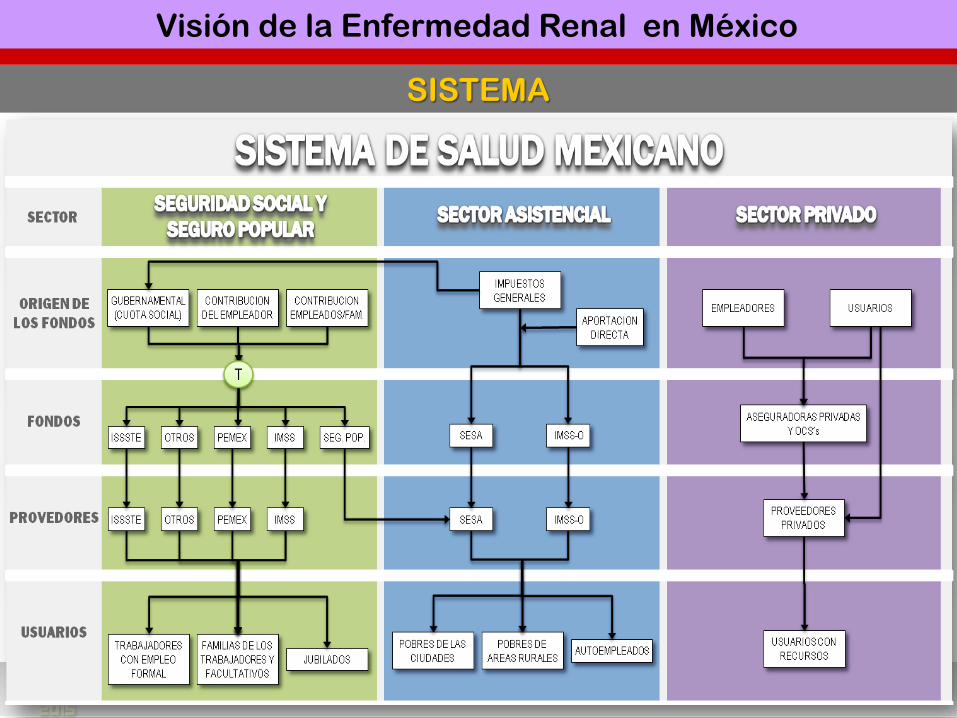
SISTEMA
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
Visión de la Enfermedad Renal en México
PLANTEAMIENTO
¿ Cómo y por qué crecen losPacientes con enfermedad renal ?
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
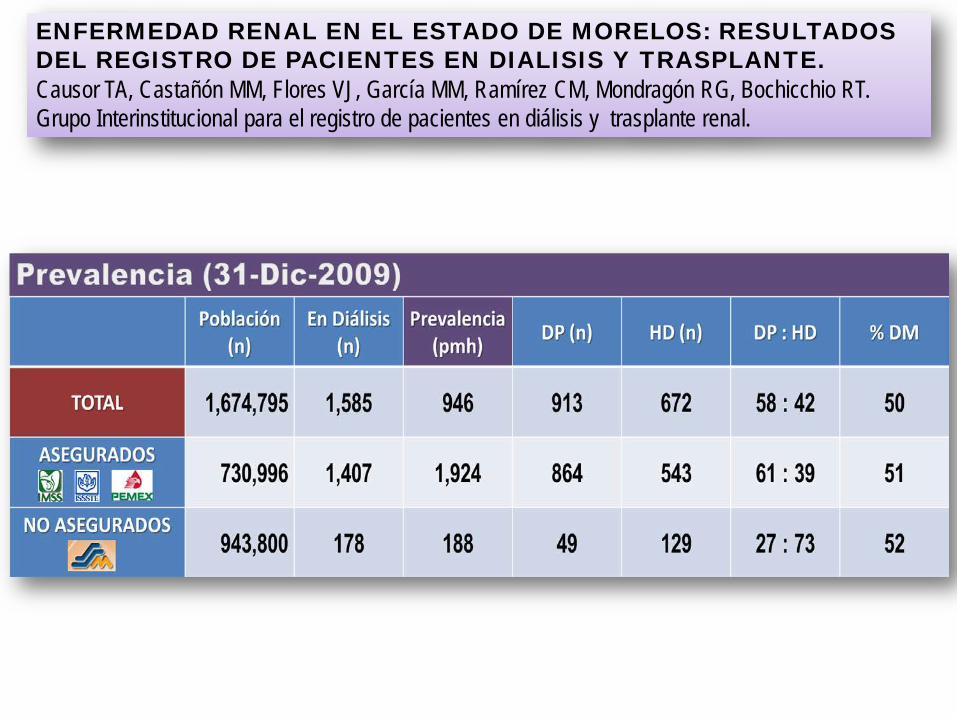
ENFERMEDAD RENAL EN EL ESTADO DE MORELOS: RESULTADOS DEL REGISTRO DE PACIENTES EN DIALISIS Y TRASPLANTE. Causor TA, Castañón MM, Flores VJ, García MM, Ramírez CM, Mondragón RG, Bochicchio RT.Grupo Interinstitucional para el registro de pacientes en diálisis y trasplante renal.
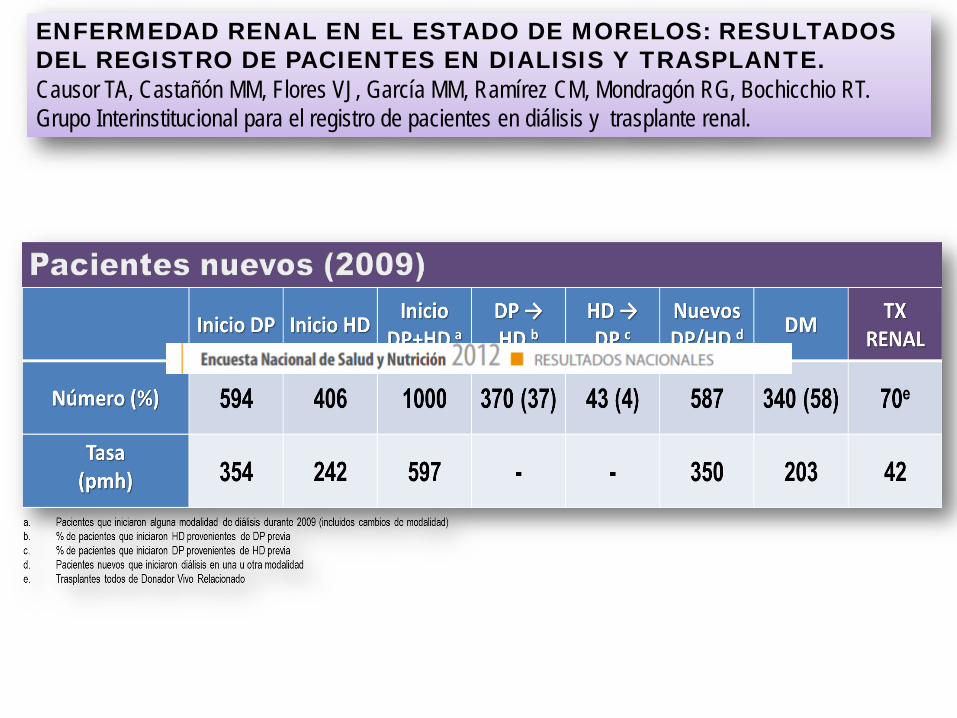
ENFERMEDAD RENAL EN EL ESTADO DE MORELOS: RESULTADOS DEL REGISTRO DE PACIENTES EN DIALISIS Y TRASPLANTE. Causor TA, Castañón MM, Flores VJ, García MM, Ramírez CM, Mondragón RG, Bochicchio RT.Grupo Interinstitucional para el registro de pacientes en diálisis y trasplante renal.
Vol 2, ESRD, Ch 10 16
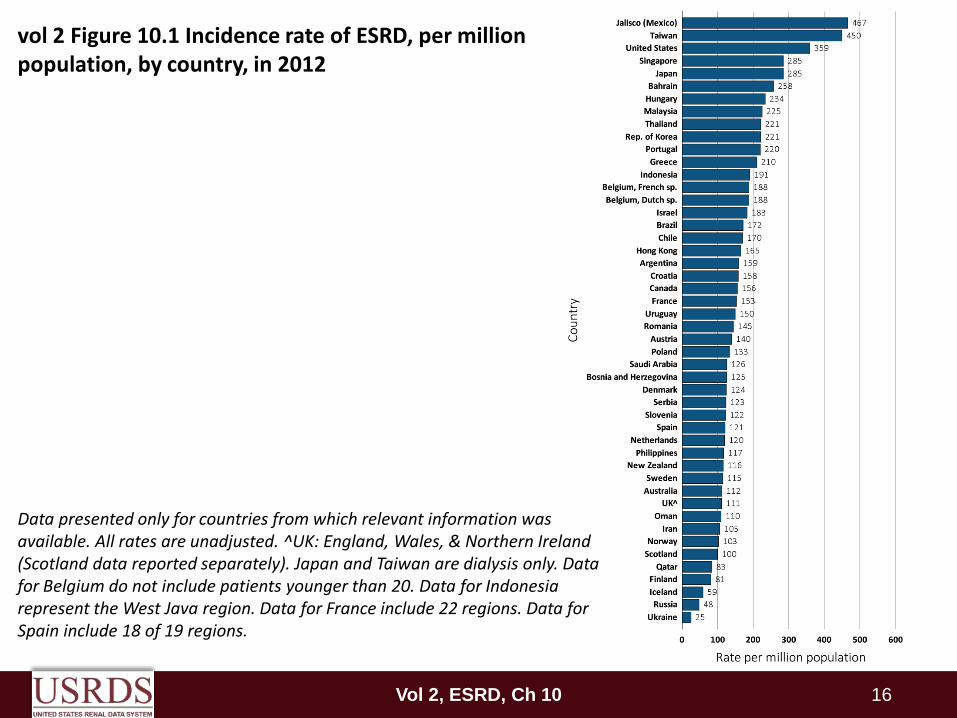
Data presented only for countries from which relevant information was available. All rates are unadjusted. ^UK: England, Wales, & Northern Ireland (Scotland data reported separately). Japan and Taiwan are dialysis only. Data for Belgium do not include patients younger than 20. Data for Indonesia represent the West Java region. Data for France include 22 regions. Data for Spain include 18 of 19 regions.
vol 2 Figure 10.1 Incidence rate of ESRD, per million population, by country, in 2012
Vol 2, ESRD, Ch 10 17
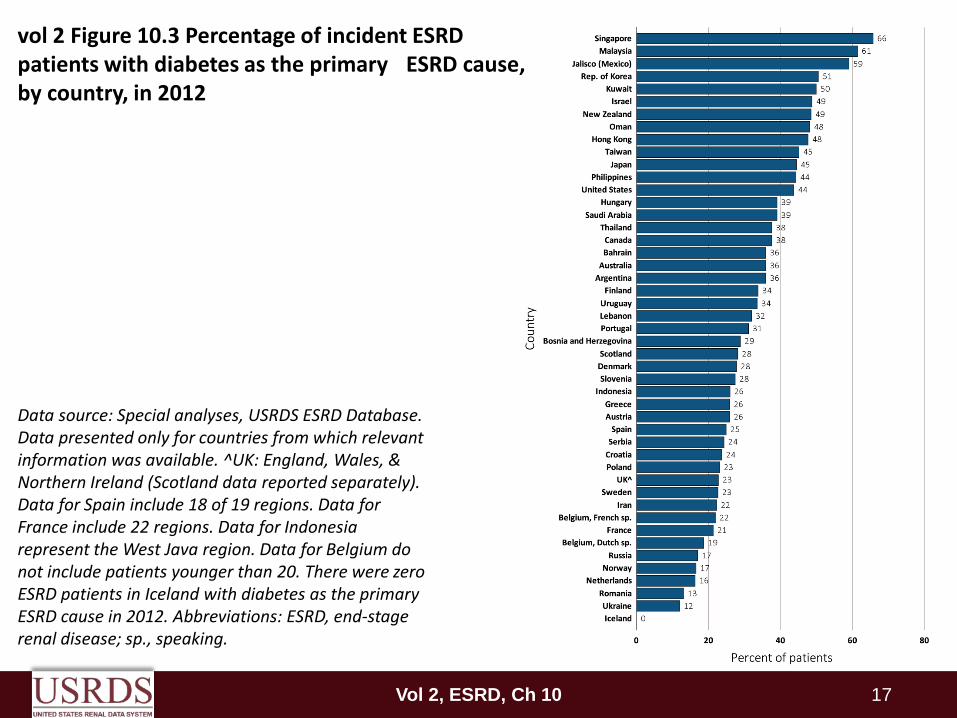
Data source: Special analyses, USRDS ESRD Database. Data presented only for countries from which relevant information was available. ^UK: England, Wales, & Northern Ireland (Scotland data reported separately). Data for Spain include 18 of 19 regions. Data for France include 22 regions. Data for Indonesia represent the West Java region. Data for Belgium do not include patients younger than 20. There were zero ESRD patients in Iceland with diabetes as the primary ESRD cause in 2012. Abbreviations: ESRD, end-stage renal disease; sp., speaking.
vol 2 Figure 10.3 Percentage of incident ESRD patients with diabetes as the primary ESRD cause, by country, in 2012
Vol 2, ESRD, Ch 10 18
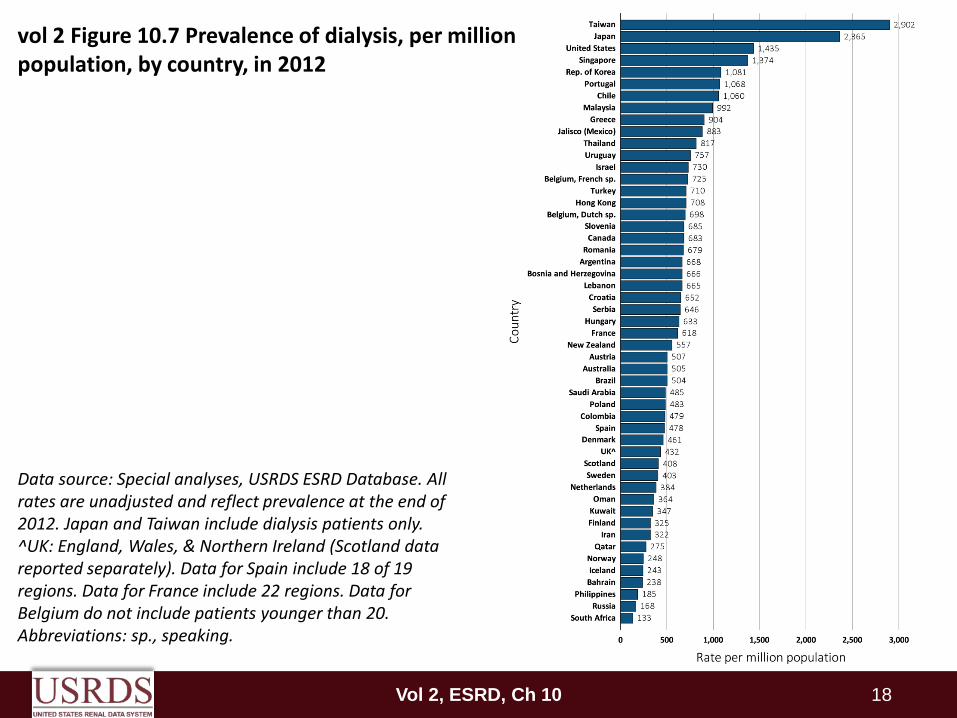
vol 2 Figure 10.7 Prevalence of dialysis, per million population, by country, in 2012
Data source: Special analyses, USRDS ESRD Database. All rates are unadjusted and reflect prevalence at the end of 2012. Japan and Taiwan include dialysis patients only. ^UK: England, Wales, & Northern Ireland (Scotland data reported separately). Data for Spain include 18 of 19 regions. Data for France include 22 regions. Data for Belgium do not include patients younger than 20. Abbreviations: sp., speaking.
Vol 2, ESRD, Ch 10 19
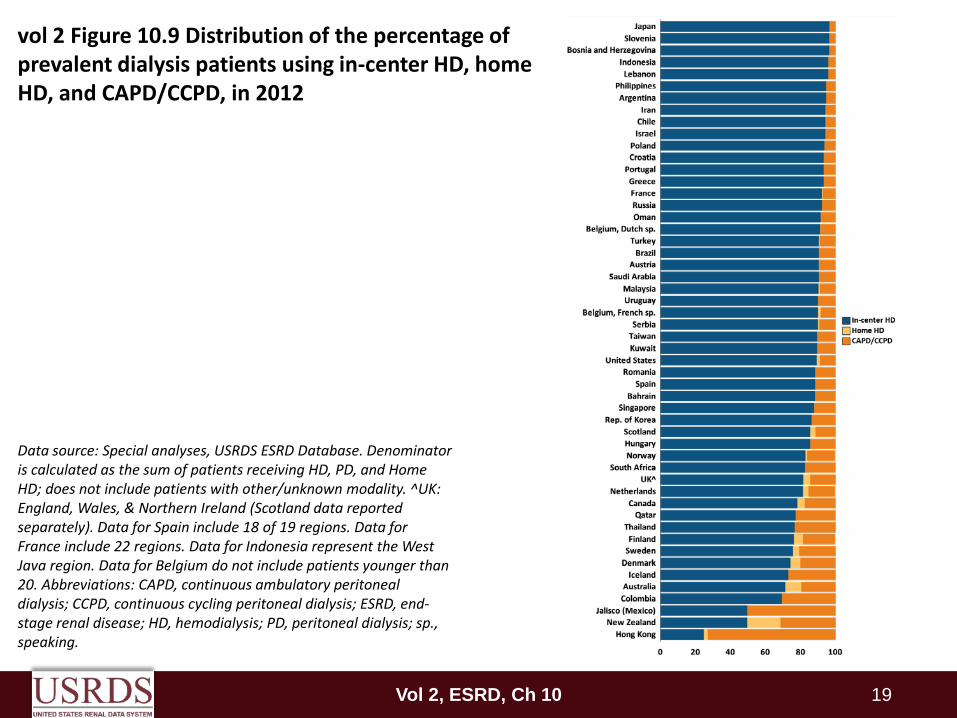
vol 2 Figure 10.9 Distribution of the percentage of prevalent dialysis patients using in-center HD, home HD, and CAPD/CCPD, in 2012
Data source: Special analyses, USRDS ESRD Database. Denominator is calculated as the sum of patients receiving HD, PD, and Home HD; does not include patients with other/unknown modality. ^UK: England, Wales, & Northern Ireland (Scotland data reported separately). Data for Spain include 18 of 19 regions. Data for France include 22 regions. Data for Indonesia represent the West Java region. Data for Belgium do not include patients younger than 20. Abbreviations: CAPD, continuous ambulatory peritoneal dialysis; CCPD, continuous cycling peritoneal dialysis; ESRD, end-stage renal disease; HD, hemodialysis; PD, peritoneal dialysis; sp., speaking.
Vol 2, ESRD, Ch 1 20
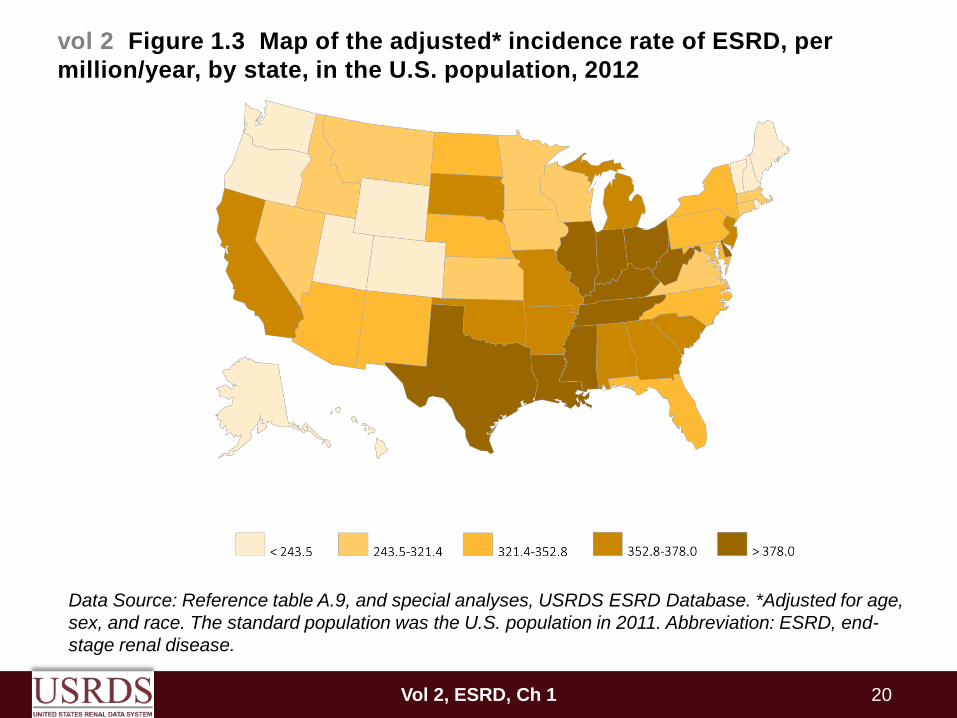
vol 2 Figure 1.3 Map of the adjusted* incidence rate of ESRD, per million/year, by state, in the U.S. population, 2012
Data Source: Reference table A.9, and special analyses, USRDS ESRD Database. *Adjusted for age, sex, and race. The standard population was the U.S. population in 2011. Abbreviation: ESRD, end-stage renal disease.
Vol 2, ESRD, Ch 1 21
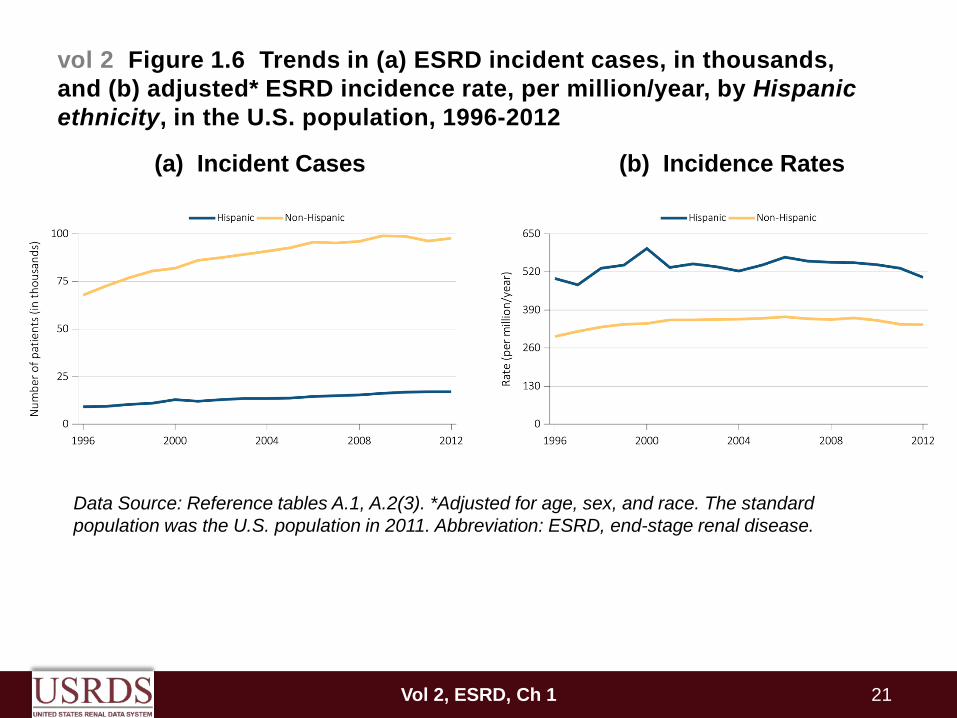
vol 2 Figure 1.6 Trends in (a) ESRD incident cases, in thousands, and (b) adjusted* ESRD incidence rate, per million/year, by Hispanic ethnicity, in the U.S. population, 1996-2012
Data Source: Reference tables A.1, A.2(3). *Adjusted for age, sex, and race. The standard population was the U.S. population in 2011. Abbreviation: ESRD, end-stage renal disease.
(a) Incident Cases (b) Incidence Rates
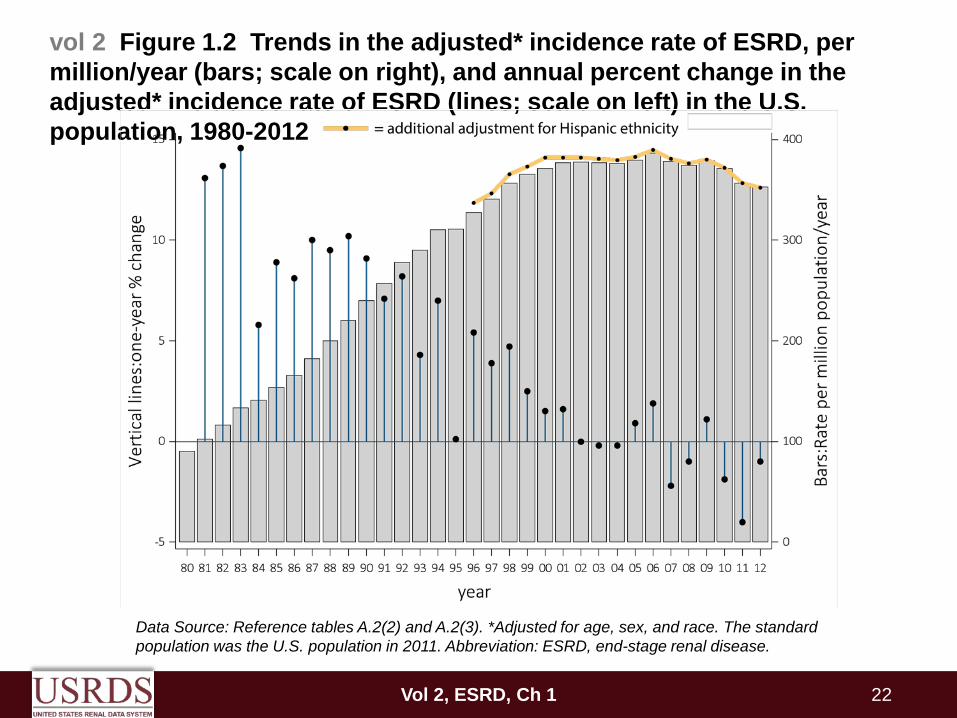
Data Source: Reference tables A.2(2) and A.2(3). *Adjusted for age, sex, and race. The standard population was the U.S. population in 2011. Abbreviation: ESRD, end-stage renal disease.
vol 2 Figure 1.2 Trends in the adjusted* incidence rate of ESRD, per million/year (bars; scale on right), and annual percent change in the adjusted* incidence rate of ESRD (lines; scale on left) in the U.S. population, 1980-2012
Vol 2, ESRD, Ch 1 22
Vol 2, ESRD, Ch 1 23
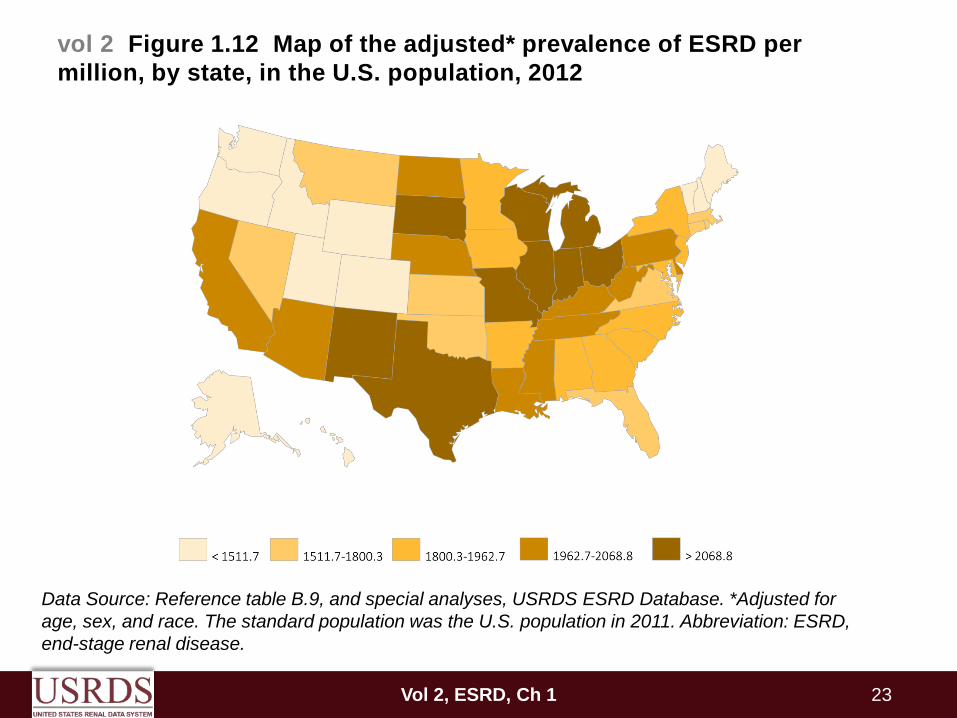
vol 2 Figure 1.12 Map of the adjusted* prevalence of ESRD per million, by state, in the U.S. population, 2012
Data Source: Reference table B.9, and special analyses, USRDS ESRD Database. *Adjusted for age, sex, and race. The standard population was the U.S. population in 2011. Abbreviation: ESRD, end-stage renal disease.
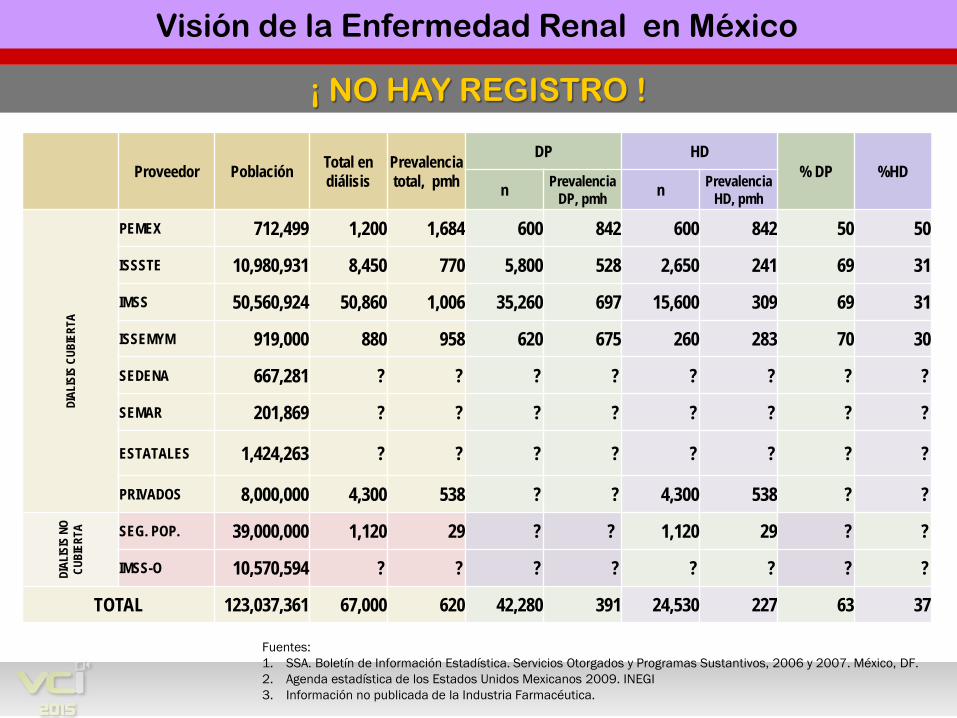
¡ NO HAY REGISTRO !
Primer Foro Bioético sobre la Enfermedad Renal
Fuentes:1. SSA. Boletín de Información Estadística. Servicios Otorgados y Programas Sustantivos, 2006 y 2007. México, DF.2. Agenda estadística de los Estados Unidos Mexicanos 2009. INEGI3. Información no publicada de la Industria Farmacéutica.
Proveedor Población Total en diálisis
Prevalencia total, pmh
DP HD % DP %HD
n Prevalencia DP, pmh n Prevalencia
HD, pmh
DIAL
ISIS
CUB
IERT
A
PEMEX 712,499 1,200 1,684 600 842 600 842 50 50
ISSSTE 10,980,931 8,450 770 5,800 528 2,650 241 69 31
IMSS 50,560,924 50,860 1,006 35,260 697 15,600 309 69 31
ISSEMYM 919,000 880 958 620 675 260 283 70 30
SEDENA 667,281 ? ? ? ? ? ? ? ?
SEMAR 201,869 ? ? ? ? ? ? ? ?
ESTATALES 1,424,263 ? ? ? ? ? ? ? ?
PRIVADOS 8,000,000 4,300 538 ? ? 4,300 538 ? ?
DIAL
ISIS
NO
CUBI
ERTA
SEG. POP. 39,000,000 1,120 29 ? ? 1,120 29 ? ?
IMSS-O 10,570,594 ? ? ? ? ? ? ? ?
TOTAL 123,037,361 67,000 620 42,280 391 24,530 227 63 37
Visión de la Enfermedad Renal en México
21.3
5.1
9.8
7.4
1.9 4.
4
21.7
3.1
2.4
1.7
1.3 2.1 2.6
6 4.9
4.9
13
4.4
36.3
12.2
8.3
33.3
6
2.29
18.4
1
7.65
5.76
4.77
31.8
3
7.39
5.29
2.15
1.72
5.46
2.94
7.92
5.88
10.1
7
26
9.05
52.6
5
18.5
1
13.8
4
0
10
20
30
40
50
60
Arge
ntin
a
Boliv
ia
Bras
il
Chi
le
Col
ombi
a
Cos
ta R
ica
Cub
a
Ecua
dor
El S
alva
dor
Gua
tem
ala
Hon
dura
s
Méx
ico
Nic
arag
ua
Pana
má
Para
guay
Perú
Puer
to R
ico
Rep
Dom
inic
ana
Uru
guay
Vene
zuel
a
tota
l
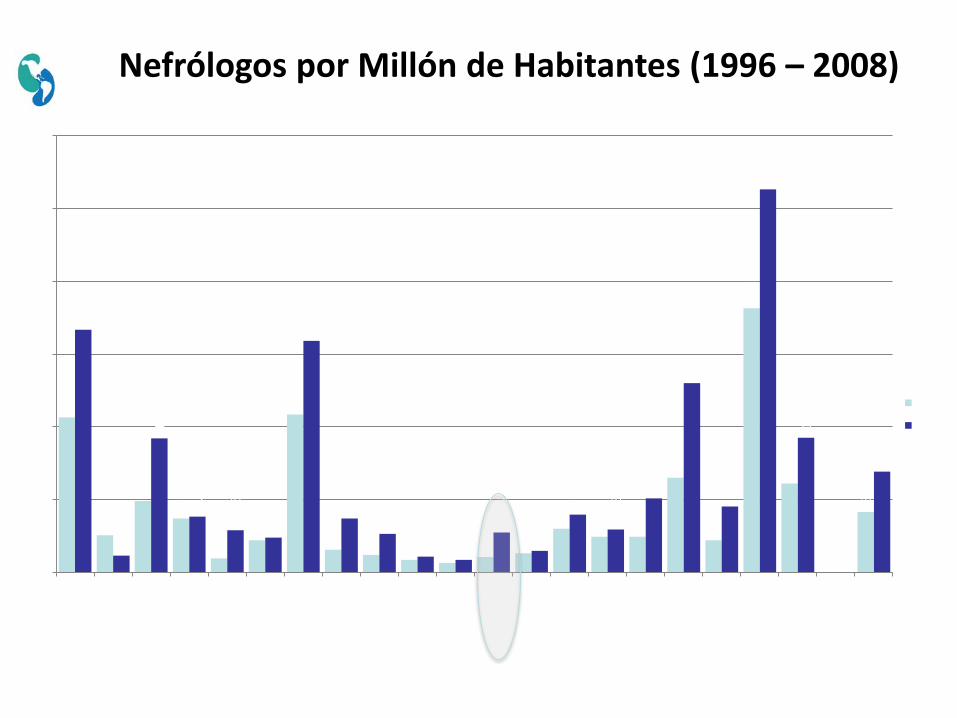
1996
2008
Nefrólogos por Millón de Habitantes (1996 – 2008)
PLANTEAMIENTO
¿ Cuáles son las acciones a tomar?
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
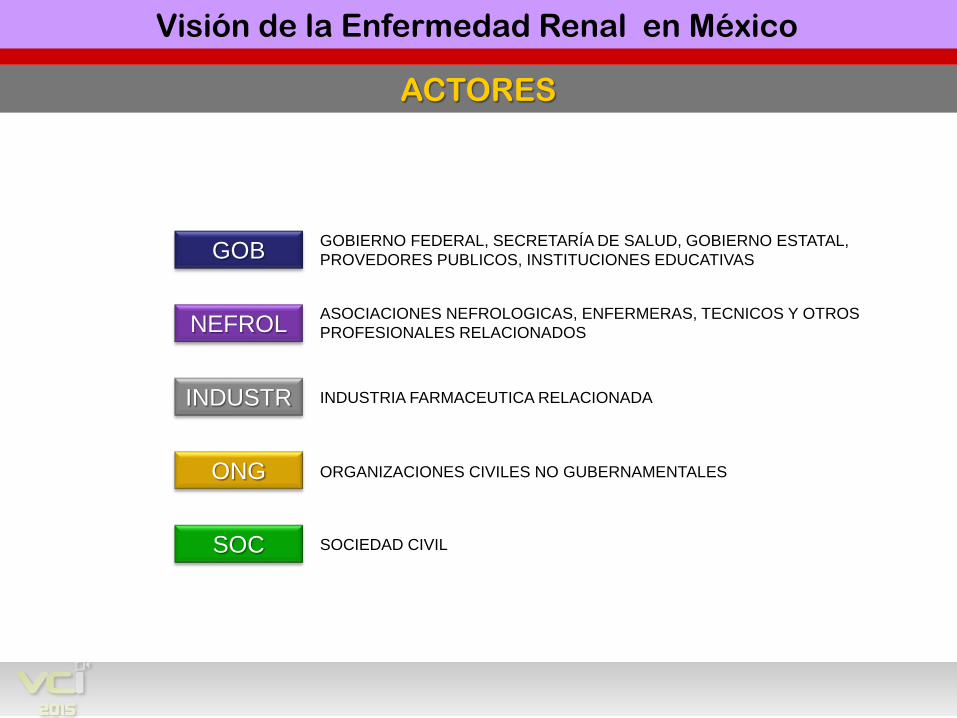
ACTORES
Primer Foro Bioético sobre la Enfermedad Renal
GOB
NEFROL
INDUSTR
ONG
SOC
GOBIERNO FEDERAL, SECRETARÍA DE SALUD, GOBIERNO ESTATAL,PROVEDORES PUBLICOS, INSTITUCIONES EDUCATIVAS
ASOCIACIONES NEFROLOGICAS, ENFERMERAS, TECNICOS Y OTROSPROFESIONALES RELACIONADOS
INDUSTRIA FARMACEUTICA RELACIONADA
ORGANIZACIONES CIVILES NO GUBERNAMENTALES
SOCIEDAD CIVIL
Visión de la Enfermedad Renal en México
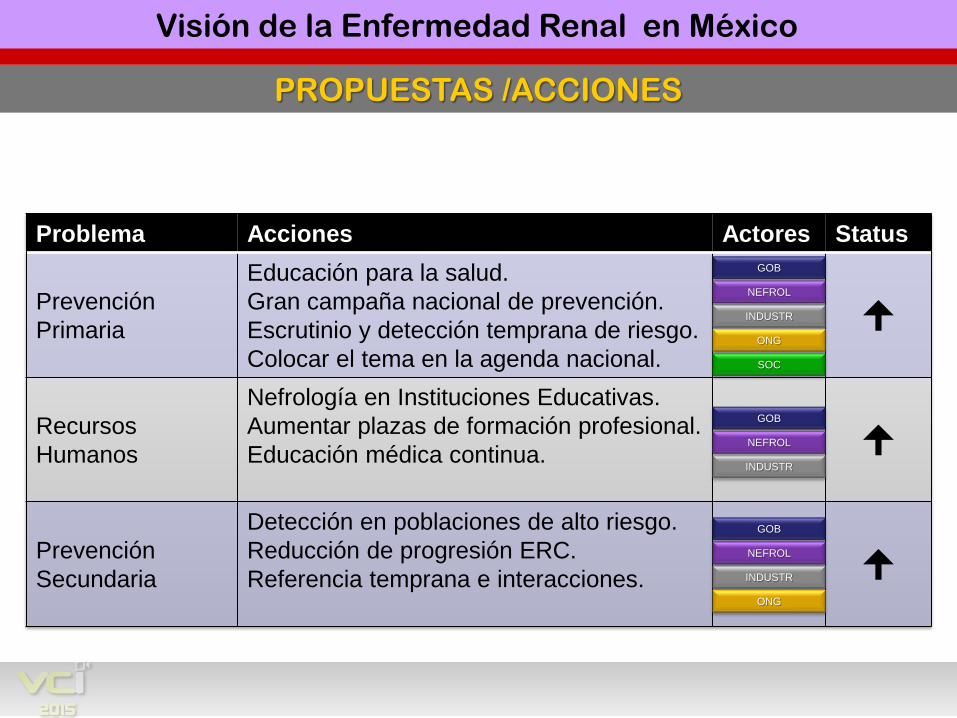
PROPUESTAS /ACCIONES
Problema Acciones Actores Status
PrevenciónPrimaria
Educación para la salud.Gran campaña nacional de prevención.Escrutinio y detección temprana de riesgo.Colocar el tema en la agenda nacional.
Recursos Humanos
Nefrología en Instituciones Educativas.Aumentar plazas de formación profesional.Educación médica continua.
Prevención Secundaria
Detección en poblaciones de alto riesgo.Reducción de progresión ERC.Referencia temprana e interacciones.
Primer Foro Bioético sobre la Enfermedad Renal
GOB
NEFROL
INDUSTR
ONG
SOC
GOB
NEFROL
INDUSTR
GOB
NEFROL
INDUSTR
ONG
Visión de la Enfermedad Renal en México
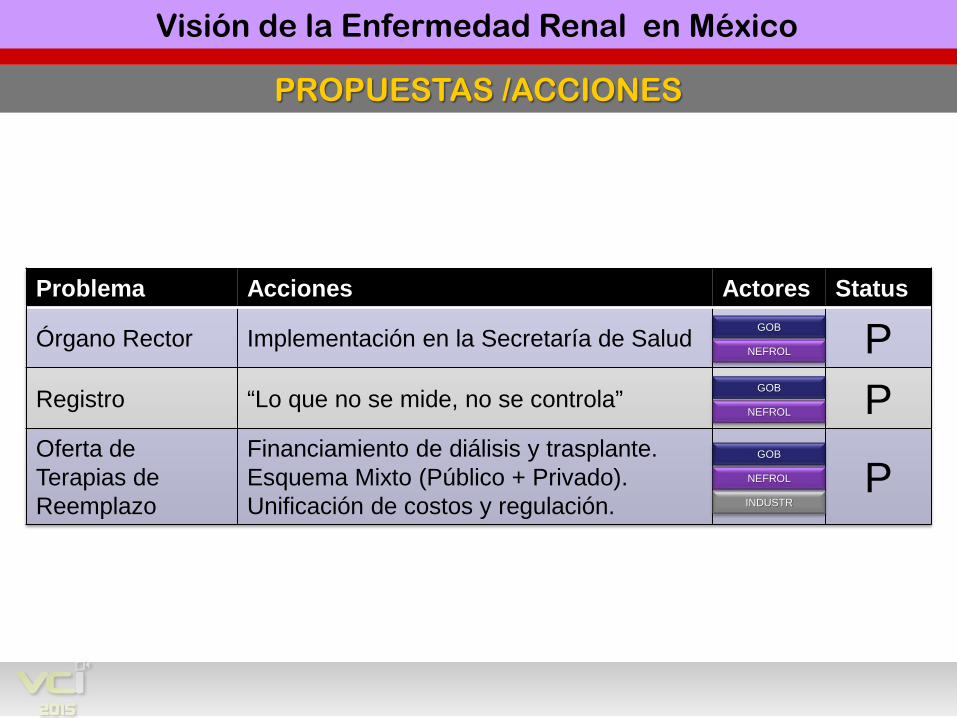
PROPUESTAS /ACCIONES
Problema Acciones Actores Status
Órgano Rector Implementación en la Secretaría de Salud PRegistro “Lo que no se mide, no se controla” POferta de Terapias de Reemplazo
Financiamiento de diálisis y trasplante.Esquema Mixto (Público + Privado).Unificación de costos y regulación.
P
Primer Foro Bioético sobre la Enfermedad Renal
GOB
NEFROL
GOB
NEFROL
INDUSTR
GOB
NEFROL
Visión de la Enfermedad Renal en México
PLANTEAMIENTO
La enfermedad renal es prioritariapara las políticas de salud
Primer Foro Bioético sobre la Enfermedad Renal Visión de la Enfermedad Renal en México
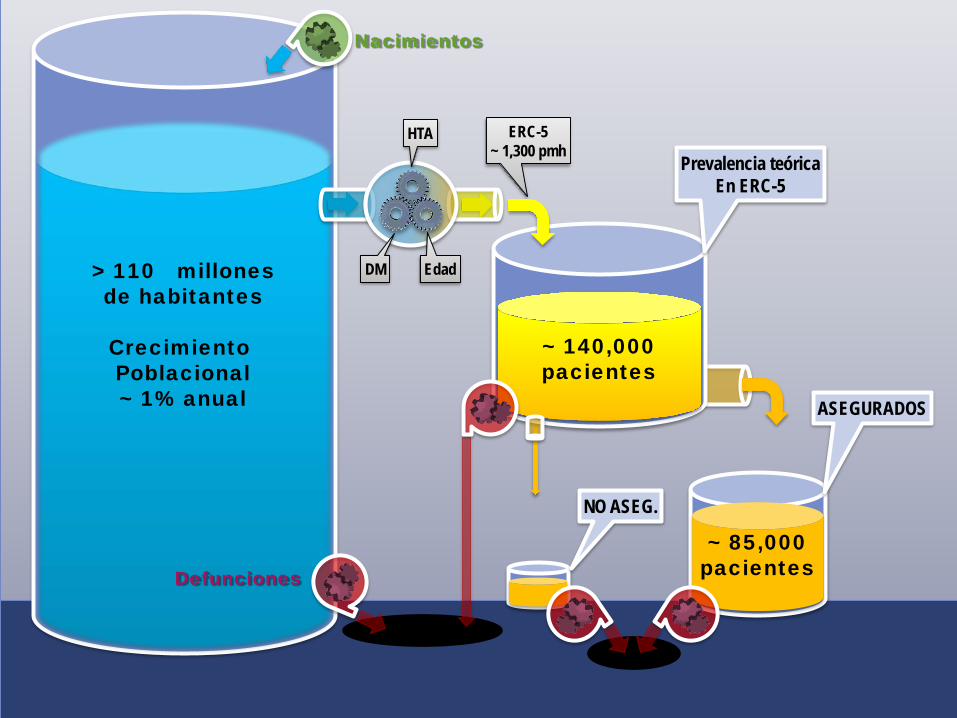
Nacimientos
Defunciones
Edad
HTA
DM
ERC-5~ 1,300 pmh
> 110 millonesde habitantes
Crecimiento Poblacional~ 1% anual
~ 140,000pacientes
Prevalencia teóricaEn ERC-5
NO ASEG.
ASEGURADOS
~ 85,000pacientes

REFLEXION FINAL
Primer Foro Bioético sobre la Enfermedad Renal
“ Si buscas resultados distintos,no hagas siempre lo mismo ”
Albert Einstein.
Visión de la Enfermedad Renal en México