La histopatologia del rechazo humoral.
57
La histopatologia del rechazo humoral (RH) Cinthia Beskow Drachenberg Profesora de Patologia Universidad de Maryland
-
Upload
webee-by-formar -
Category
Education
-
view
73 -
download
3
Transcript of La histopatologia del rechazo humoral.

La histopatologia del rechazo
humoral (RH)
Cinthia Beskow Drachenberg
Profesora de Patologia
Universidad de Maryland
La histopatologia del rechazo humoral renalBosquejo de la conferencia
1 Describir los componentes histologicos
principales
2 Describir la clasificacion de Banff para RH
3 Presentar ejemplos clinicos
4 Discutir brevemente RH en otros organos
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos-contra donante
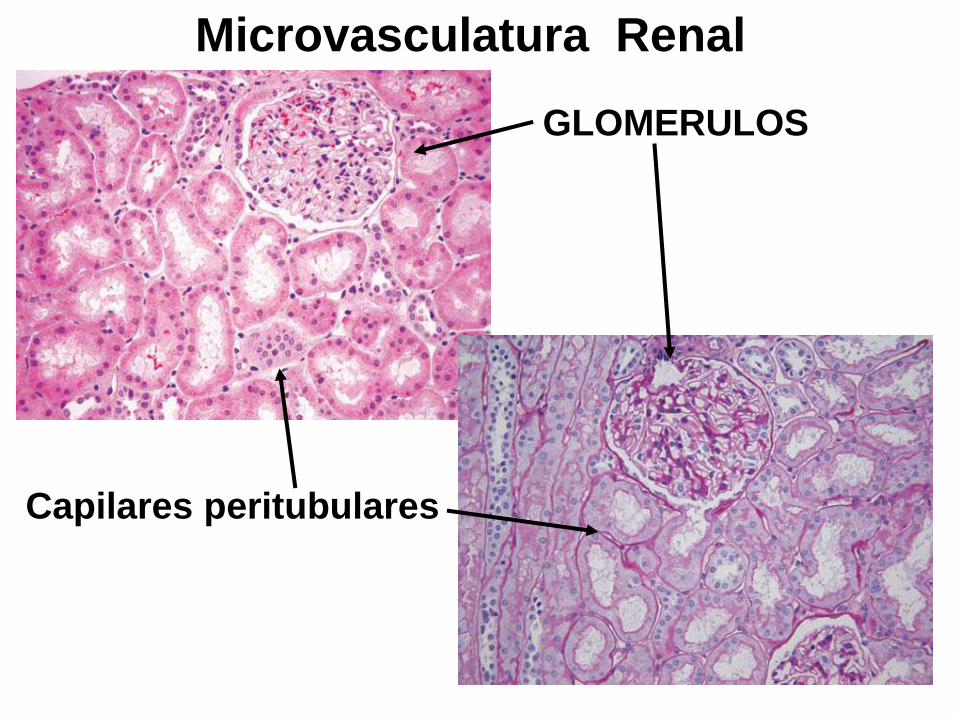
GLOMERULOS
Capilares peritubulares
Microvasculatura Renal
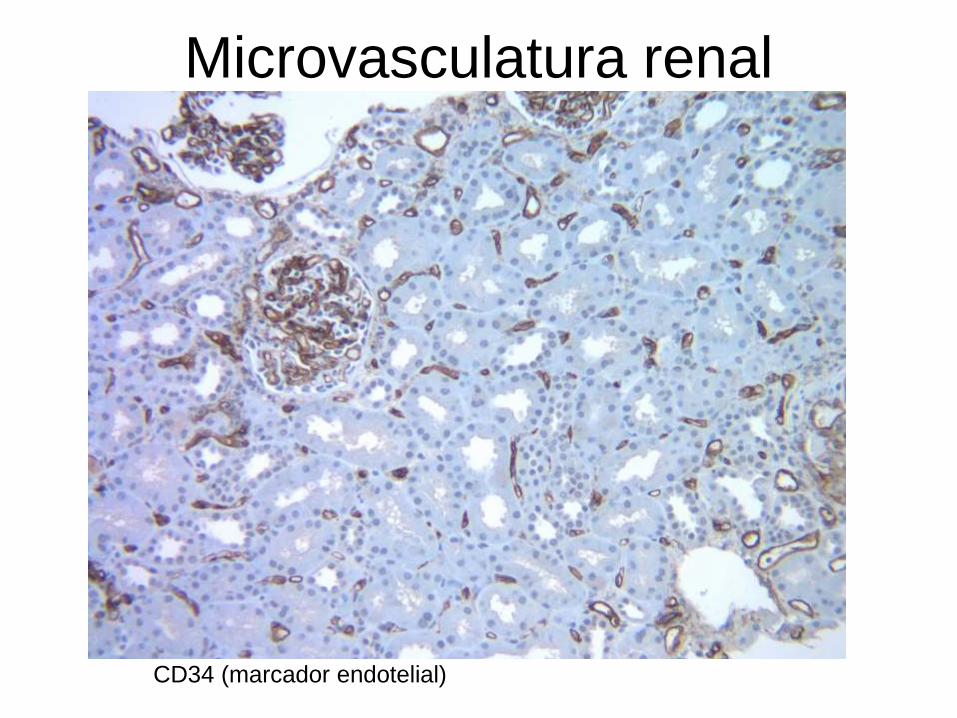
Microvasculatura renal
CD34 (marcador endotelial)
Luz de capilar peritubular normal
Base de un tubulo renal
Base de un tubulo renal
Membrana basa simple
CD34 (marcador endotelial)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
La histopatologia del rechazo humoral renalBosquejo de la conferencia
1 Describir los componentes histologicos
principales
2 Describir la clasificacion de Banff para RH
3 Presentar ejemplos clinicos
4 Discutir brevemente RH en otros organos
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos-contra donante
GLOMERULOS
Capilares peritubulares
Microvasculatura Renal
Microvasculatura renal
CD34 (marcador endotelial)
Luz de capilar peritubular normal
Base de un tubulo renal
Base de un tubulo renal
Membrana basa simple
CD34 (marcador endotelial)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos-contra donante
GLOMERULOS
Capilares peritubulares
Microvasculatura Renal
Microvasculatura renal
CD34 (marcador endotelial)
Luz de capilar peritubular normal
Base de un tubulo renal
Base de un tubulo renal
Membrana basa simple
CD34 (marcador endotelial)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
GLOMERULOS
Capilares peritubulares
Microvasculatura Renal
Microvasculatura renal
CD34 (marcador endotelial)
Luz de capilar peritubular normal
Base de un tubulo renal
Base de un tubulo renal
Membrana basa simple
CD34 (marcador endotelial)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Microvasculatura renal
CD34 (marcador endotelial)
Luz de capilar peritubular normal
Base de un tubulo renal
Base de un tubulo renal
Membrana basa simple
CD34 (marcador endotelial)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
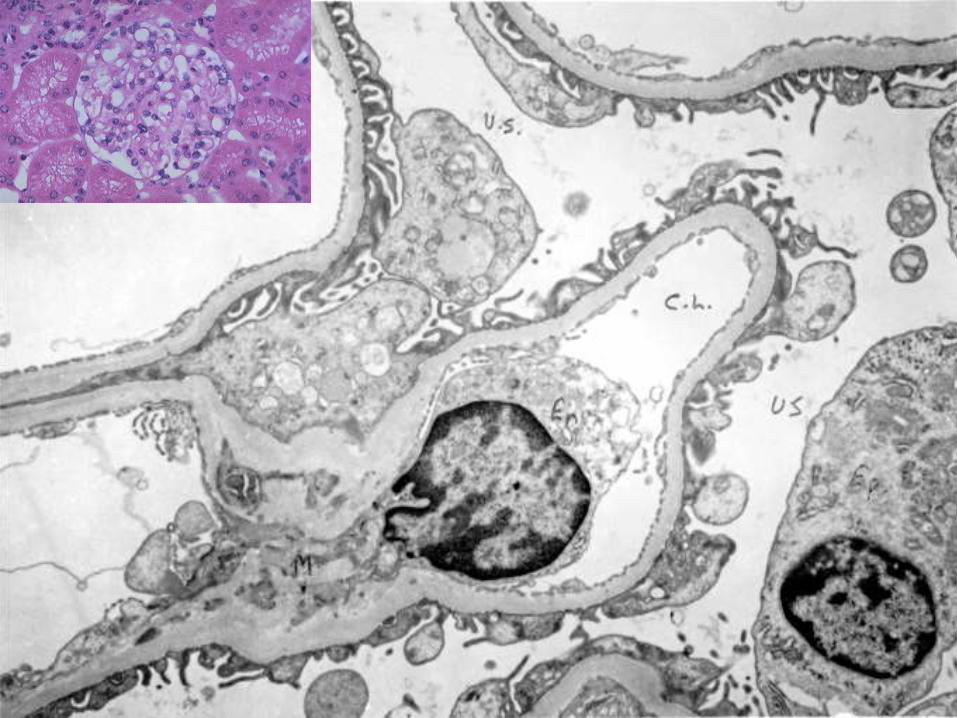
Luz de capilar peritubular normal
Base de un tubulo renal
Base de un tubulo renal
Membrana basa simple
CD34 (marcador endotelial)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
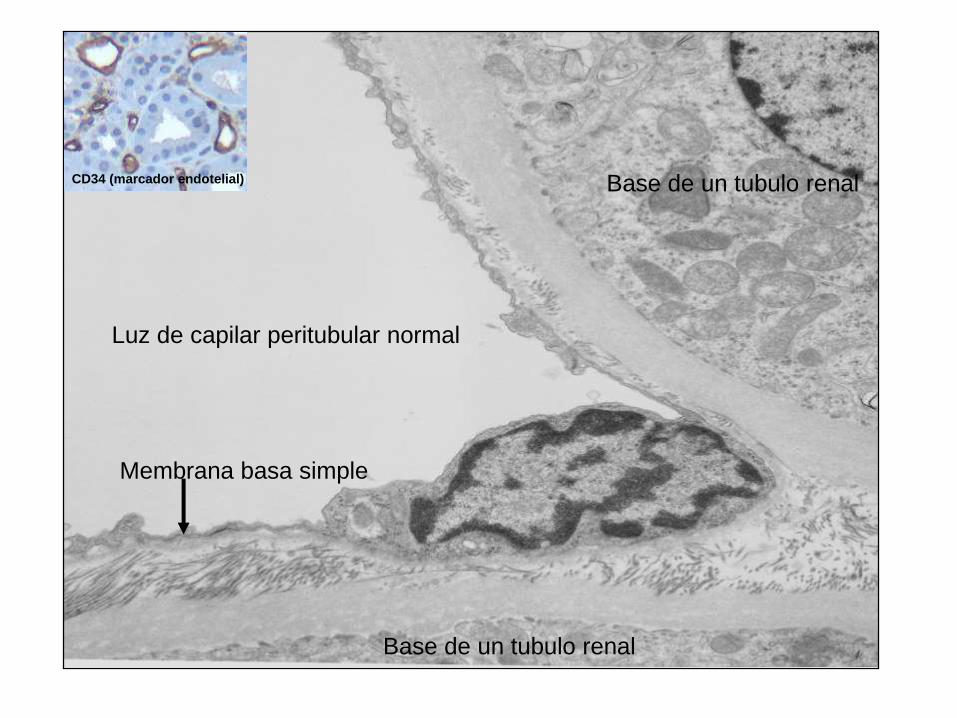
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Rechazo humoral agudo
Capilar glomerular normal
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
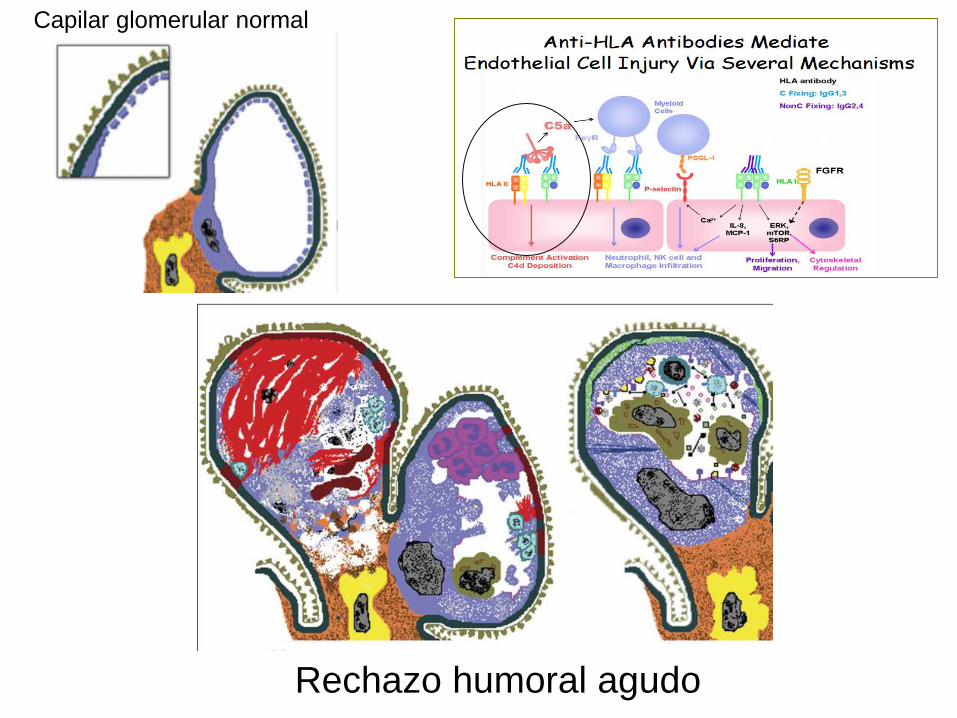
Rechazo humoral agudo leve trombosis glomerular focal y necrosis tubular aguda
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
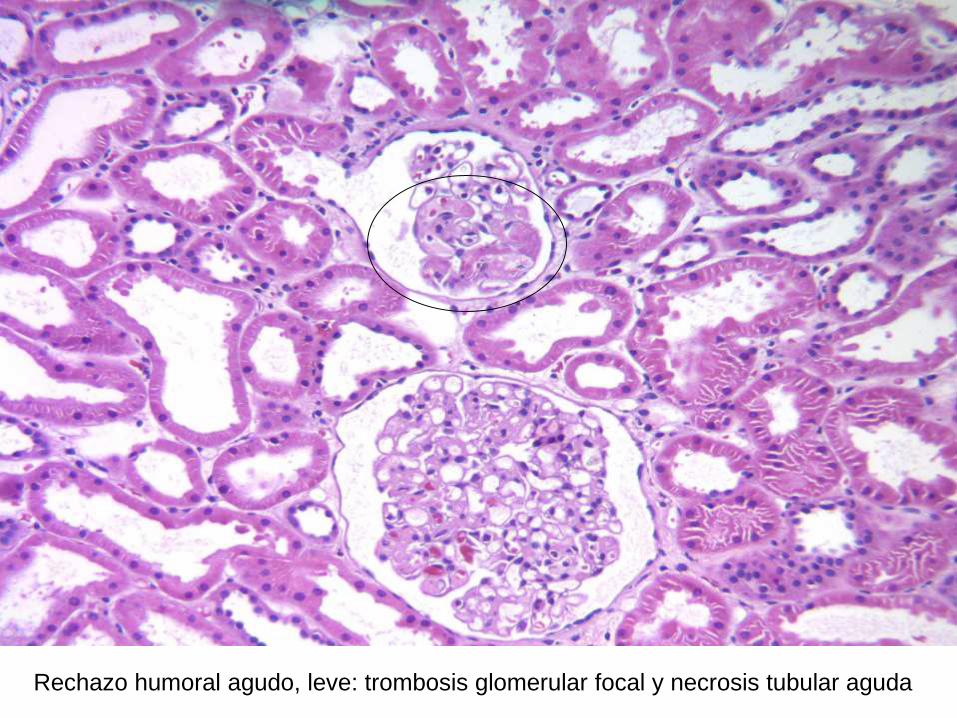
Tipica lesion endotelial aguda litica
( necrosis endotelial microthrombosis)
Rechazo humoral severo con necrosistrombosis glomerular
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
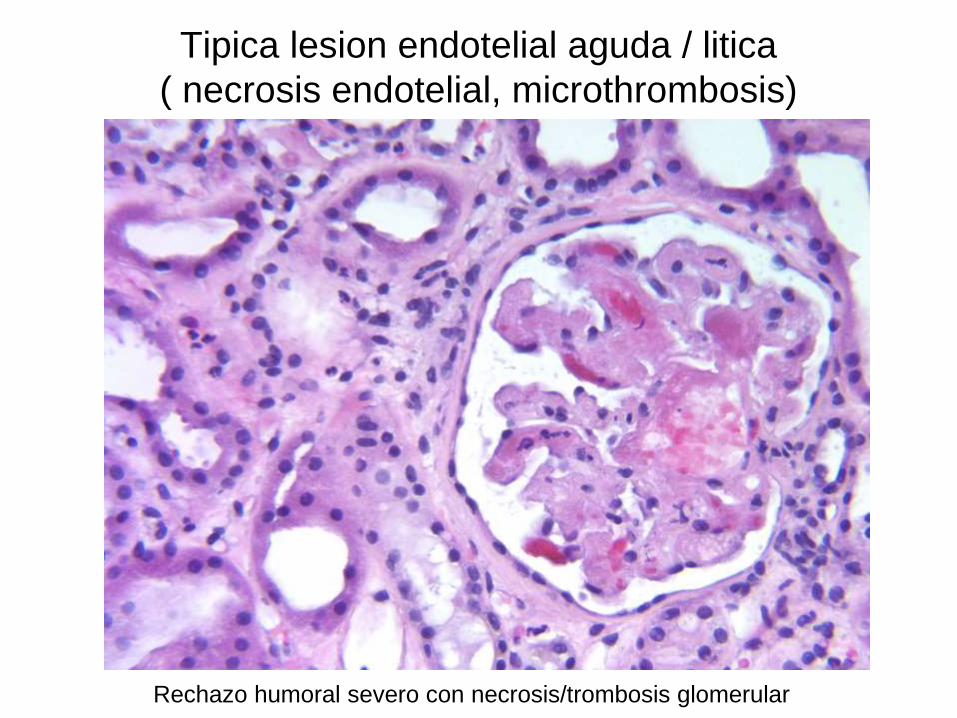
Oclusion de glomerulos capilares en RH Necrosis endotelial thrombosis inflamacion
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
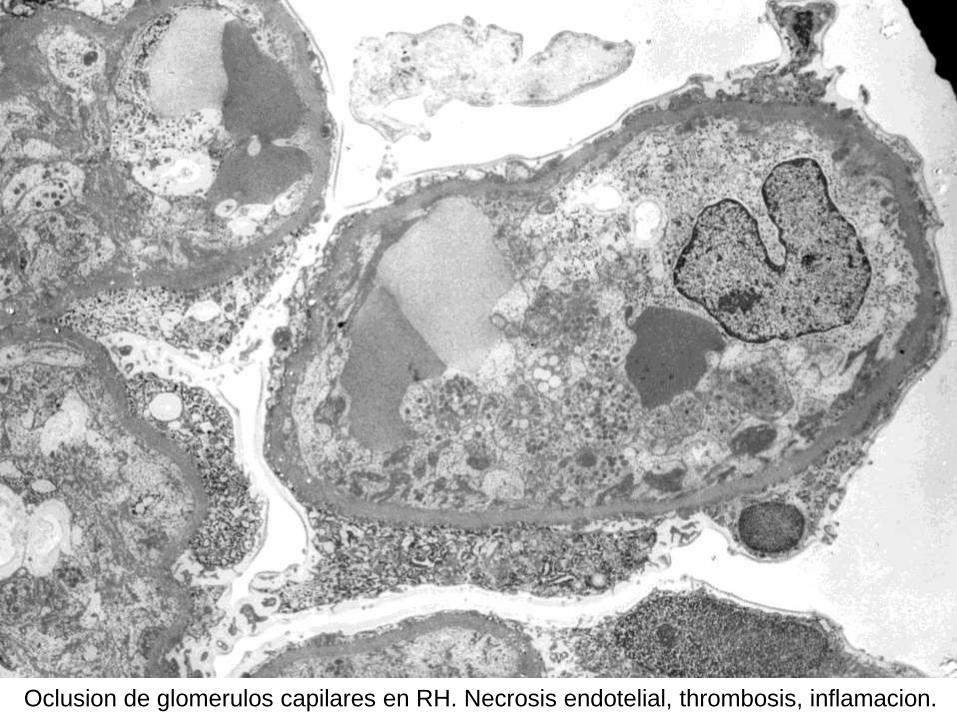
C4d
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
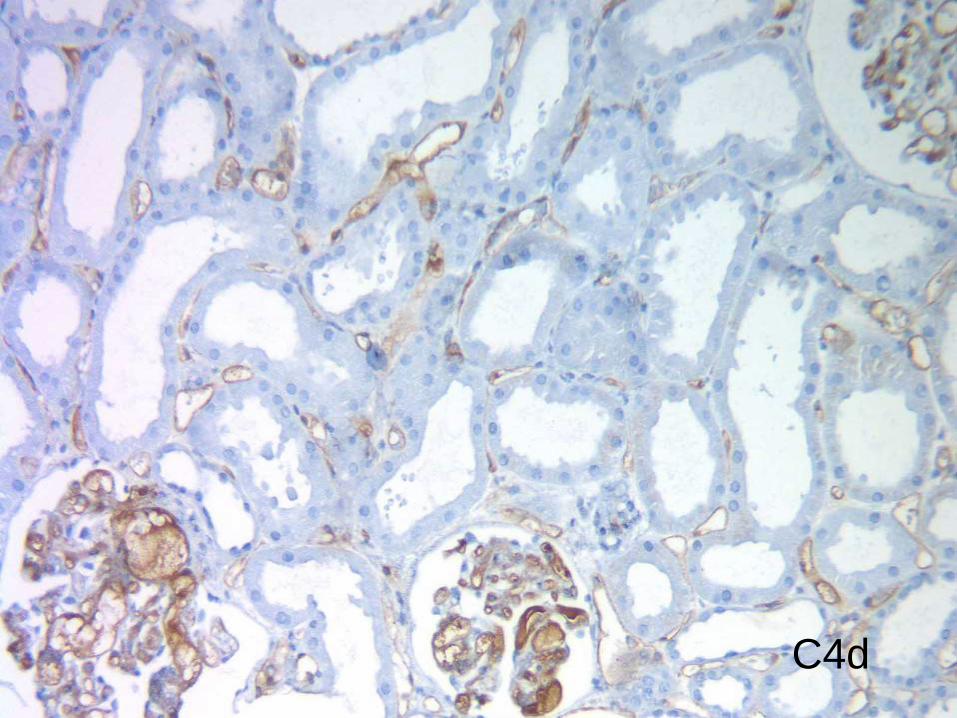
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
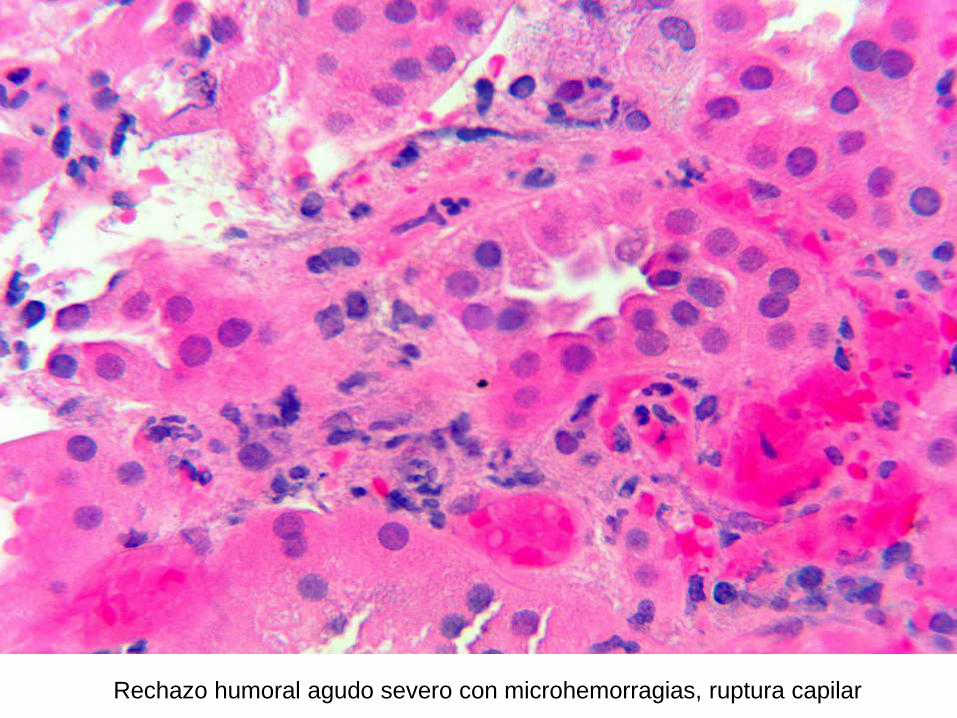
Rechazo humoral agudo severo con microhemorragias ruptura capilar
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
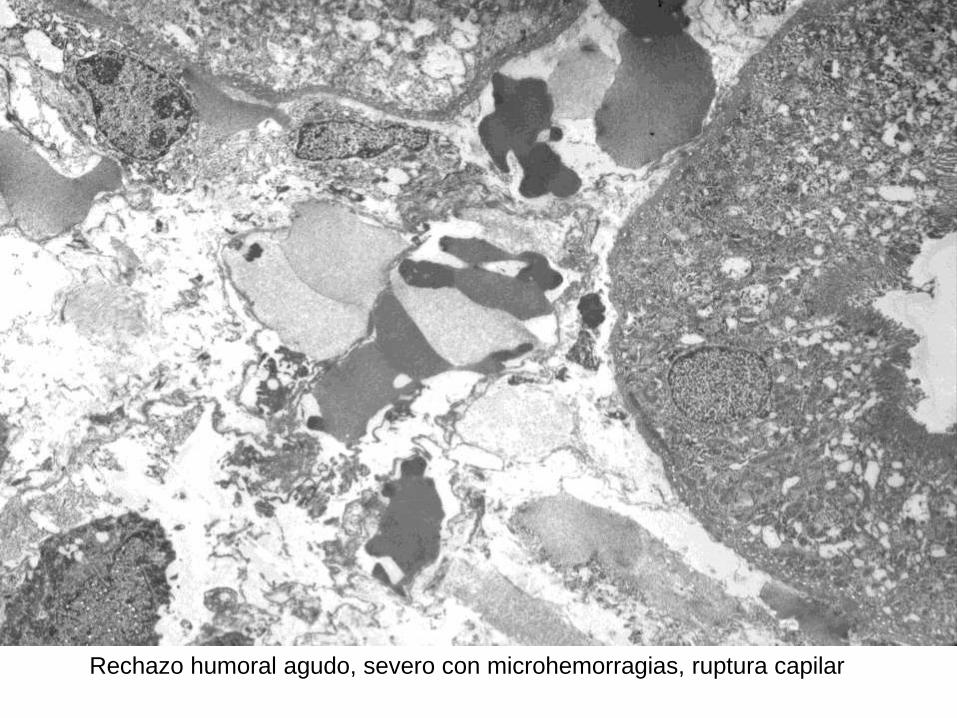
Rechazo humoral agudo
Capilar glomerular normal
Cascada del complemento
Necrosis
Cascada de la coagulacion
Thrombosis
Reclutamiento de celulas inflamatorias
Glomerulitis - capilaritis
Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival

Glomerulitis
Capillaritis
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
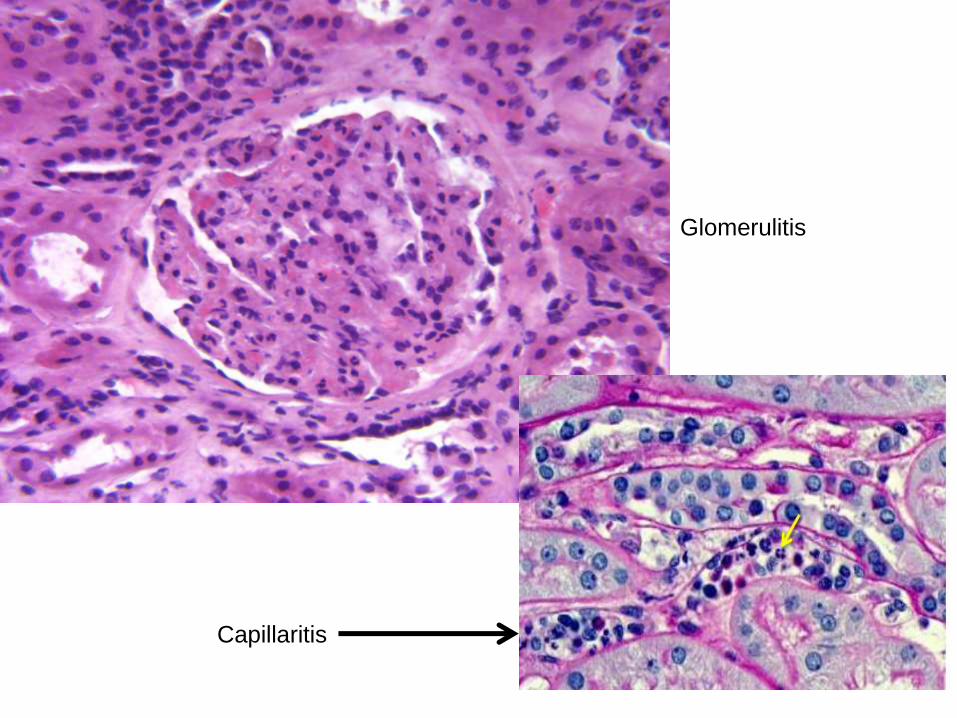
Glomerulitis hinchazon de las celulas endoteliales microtrombos (flechas)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
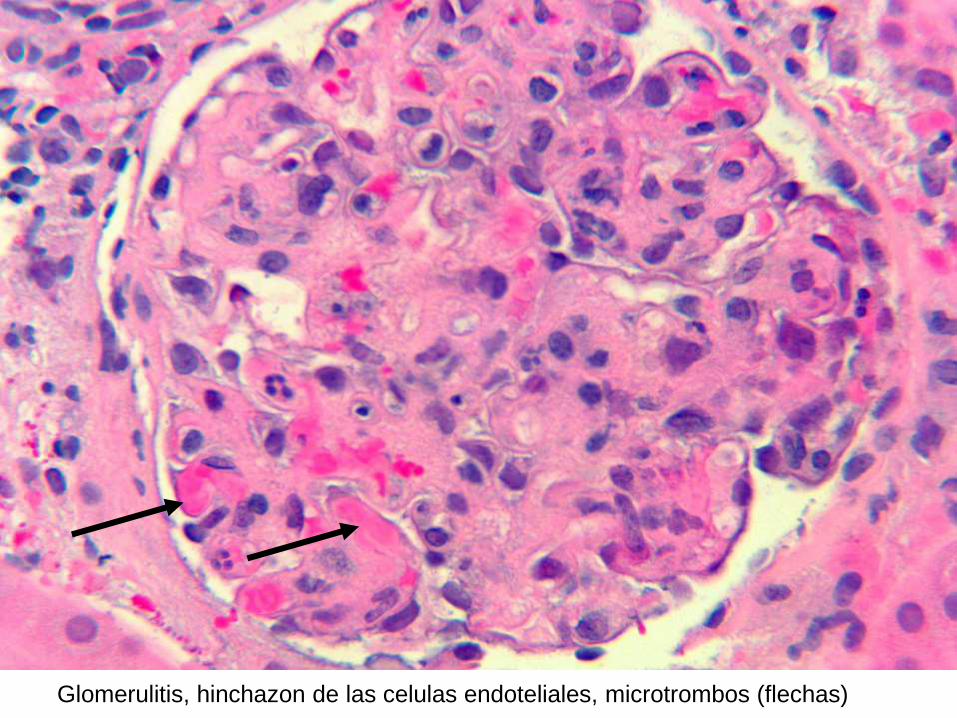
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Lesiones microvasculares cronicas
bull Duplicacion de la membrana basal
glomerular
ndash Glomerulopatia del trasplante
bull Multilaminacioacuten de la membrana basal
peritubular
ndash Capilaropatia del trasplante (ME)
bull Acumulacion de celulas inflamatorias
ndash Glomerulitis capilaritis
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Hinchazon de la celula endotelial con
perdida de las fenestraciones normales
El RH esta uniformemente caracterizado por la hinchazon (activacion) de las celulas
endoteliales resultando en acumulacion de celulas inflamatorias y remodelamiento de
la membrana basal
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
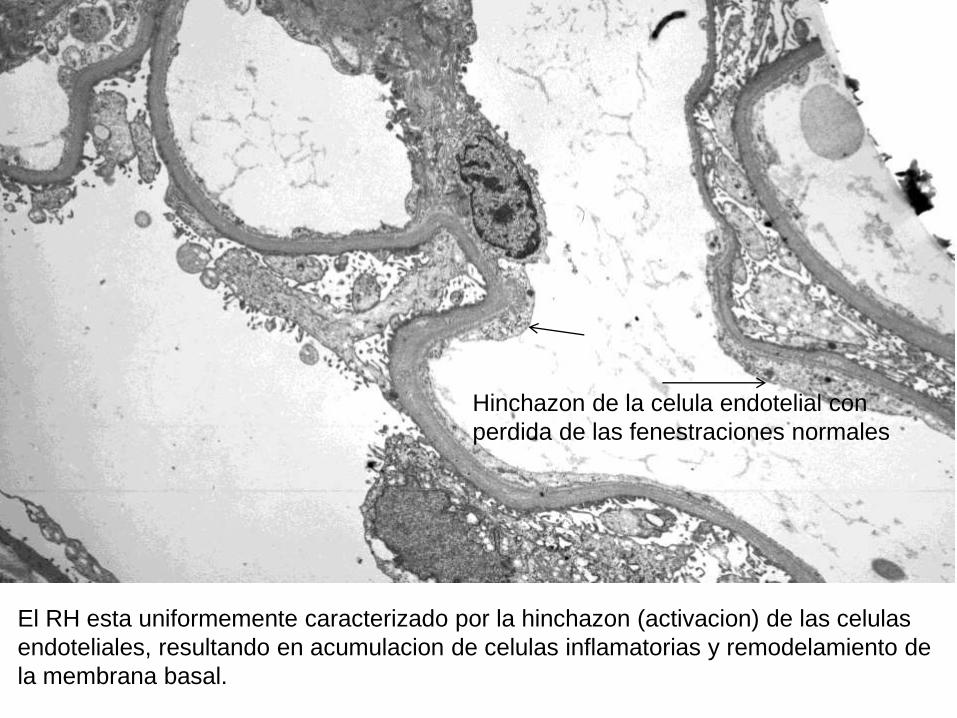
Remodelamiento de la membrana basal glomerular con duplicacion incipiente
(glomerupatia del tx temprana)
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
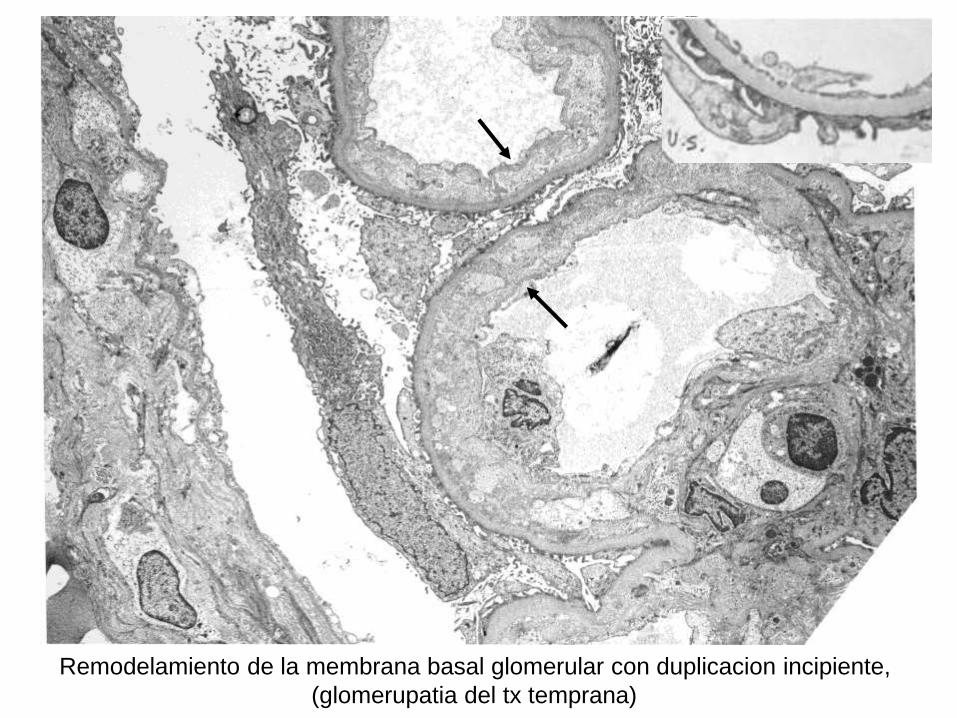
Progresion en el remodelamiento glomerular en el RH cronico en los estadios
tempranos hay solamente expansion del espacio subendotelial (imagen B)
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
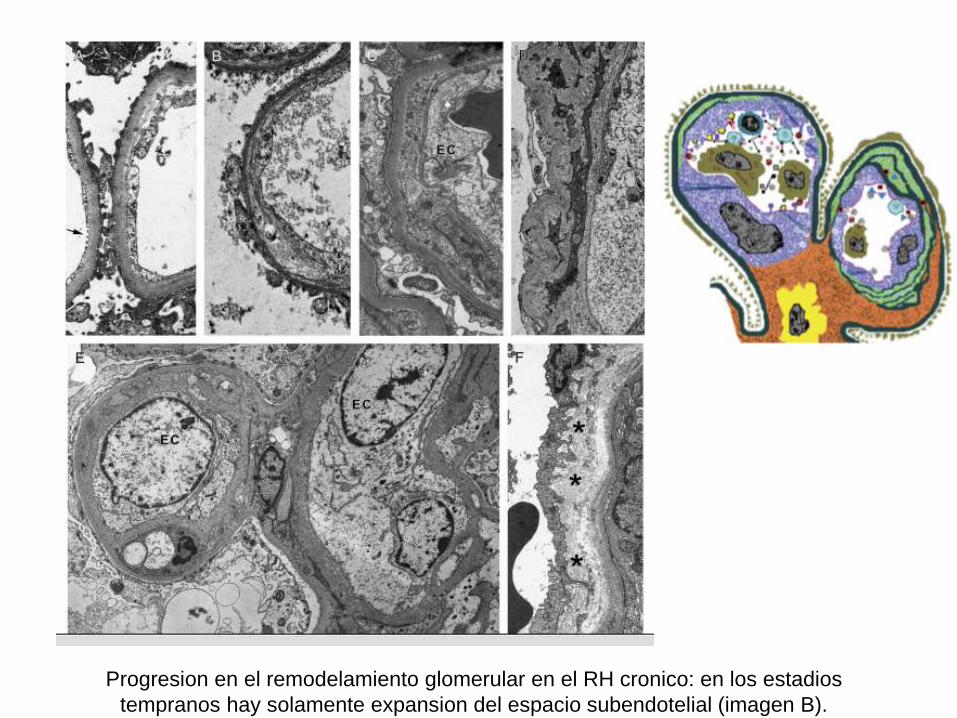
Duplicacion de la membrana basal glomerular Glomerulopatia del trasplante
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
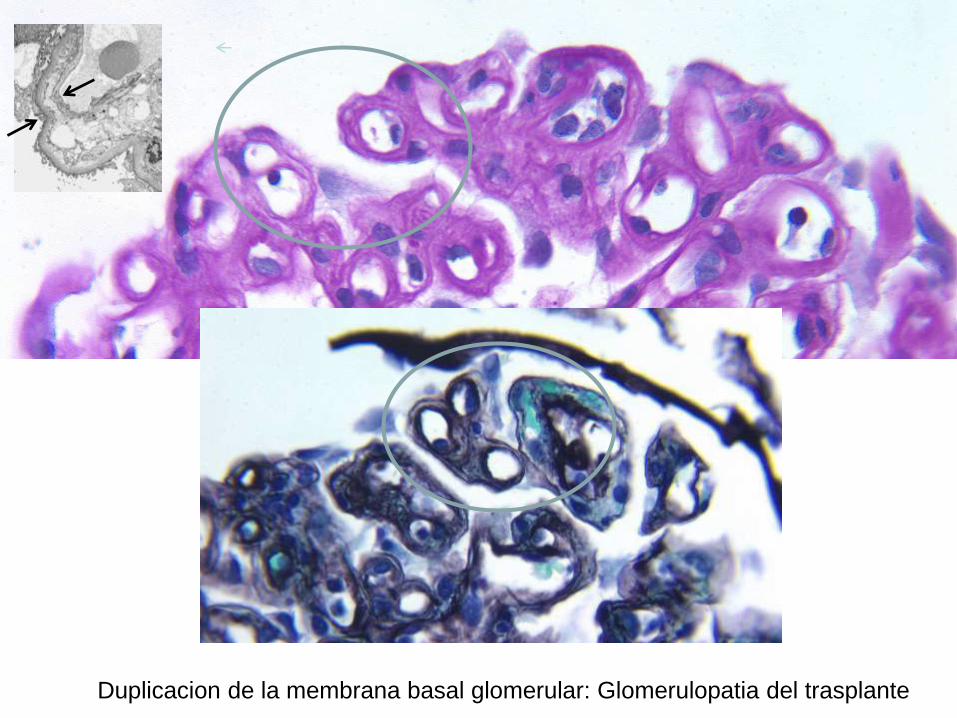
Capilar peritubular
normal La
membrana basal
es simple
Capilar peritubular en RH con multi-
lamelacion de la membrana basal
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
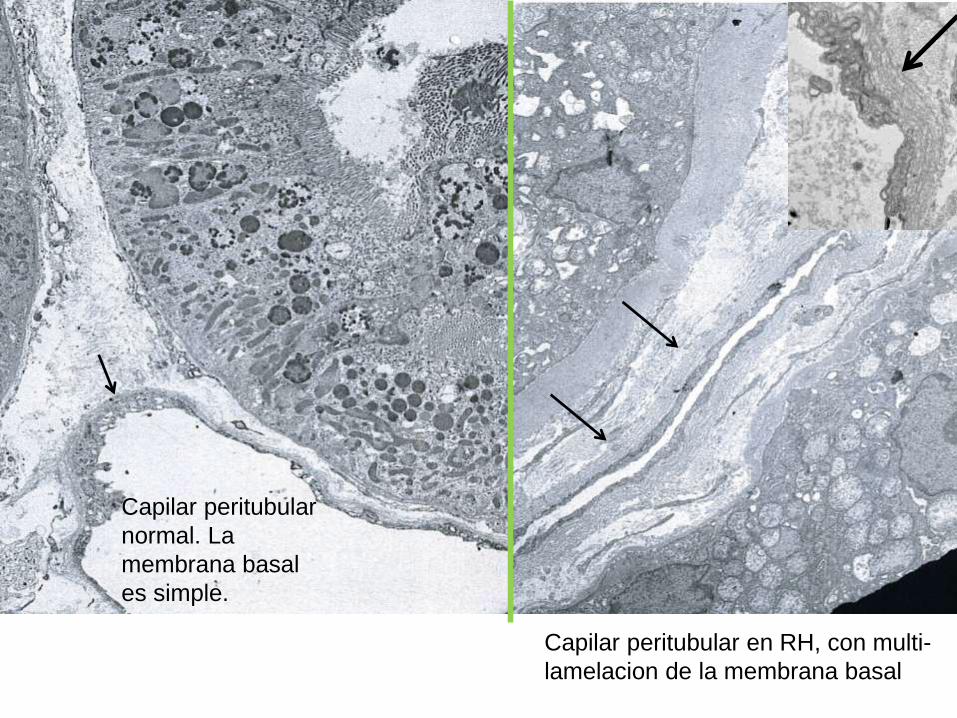
CD68 (tincion para macrofagos)
Acumulacion de celulas inflamatorias
(manifestacion aguda y cronica)
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
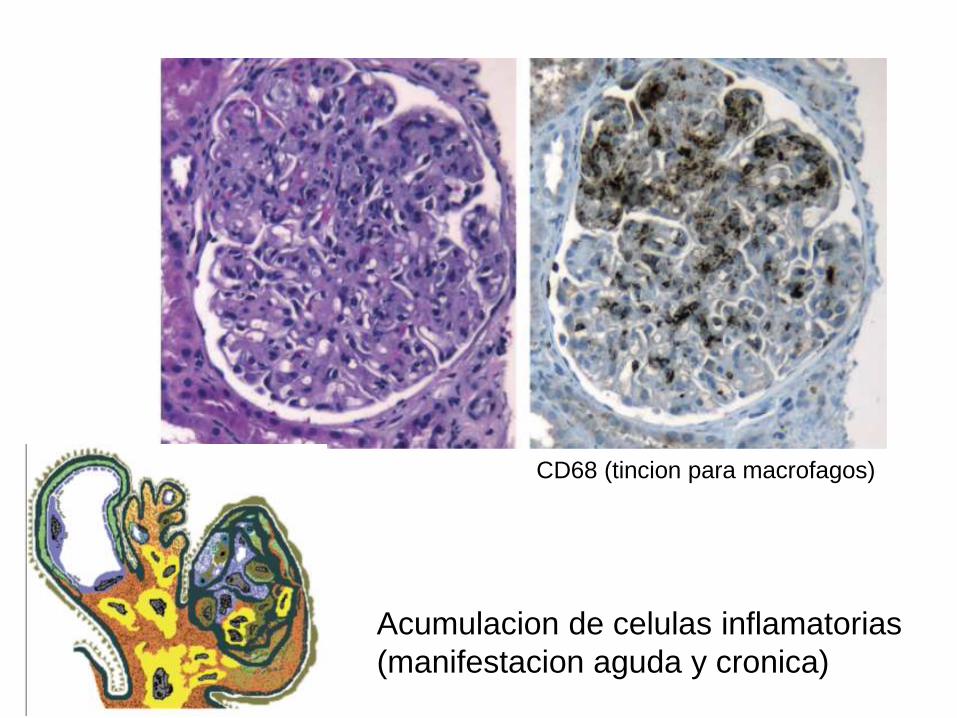
Acumulacion de celulas inflamatorias que se adhieren al endotelio y causan
estrechamiento de la luz capilar tambien participan en el remodelamiento
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
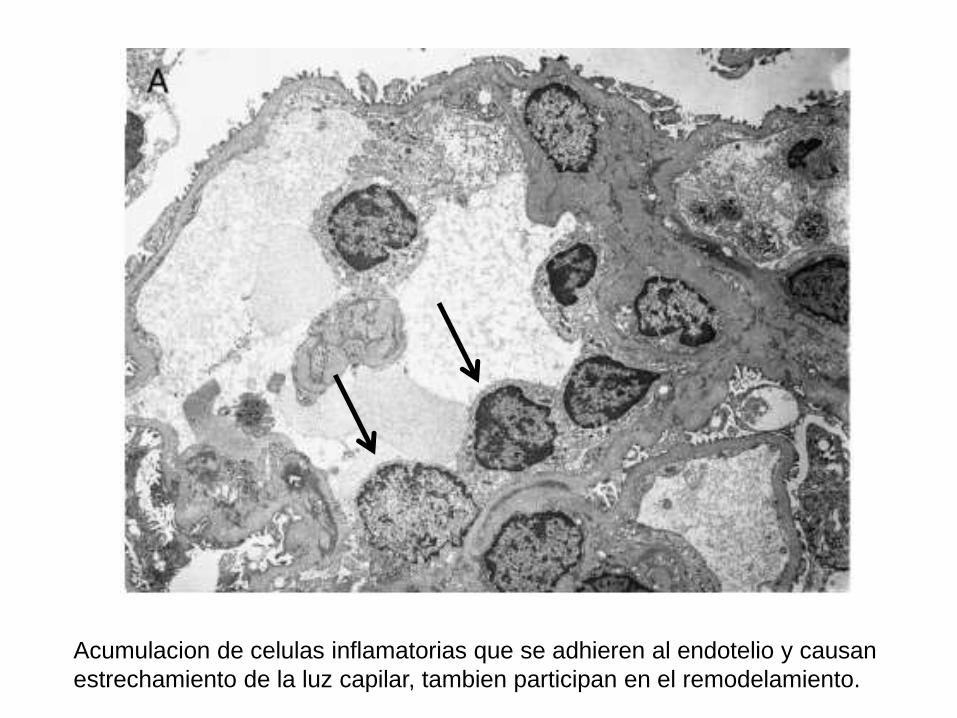
Dantildeo endotelial en arterias de mayor calibre
(una lesion recientemente reconocida en el RH)
Arteria normal
Arteritis intimal (Hematoxilina-Eosina y CD3 (marcador de linfocitos T)
(En forma similar la necrosis arterial es una manifestacion de RH agudo severe)
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
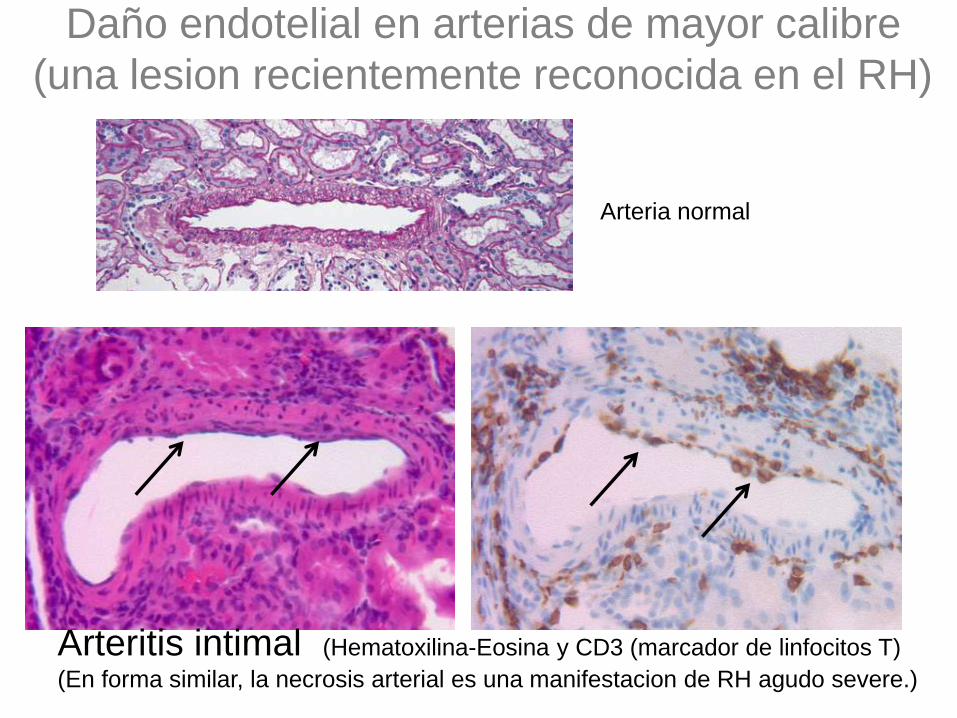
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
Dantildeo tubular secundario a isquemia
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos contra el donante
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
C4d
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
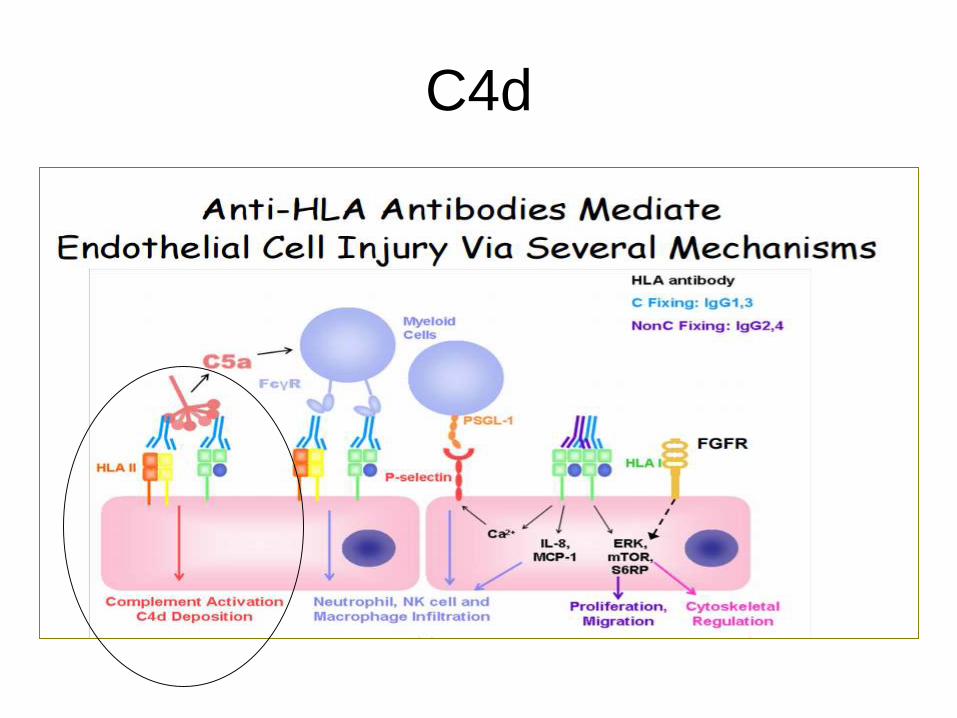
Metodo inmunohistoquimico (IHC) tejido fijado en formalina y en parafina
Metodo por immunoflorescencia (IF) tejido fresco congelado
Este metodo es mas sensible
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
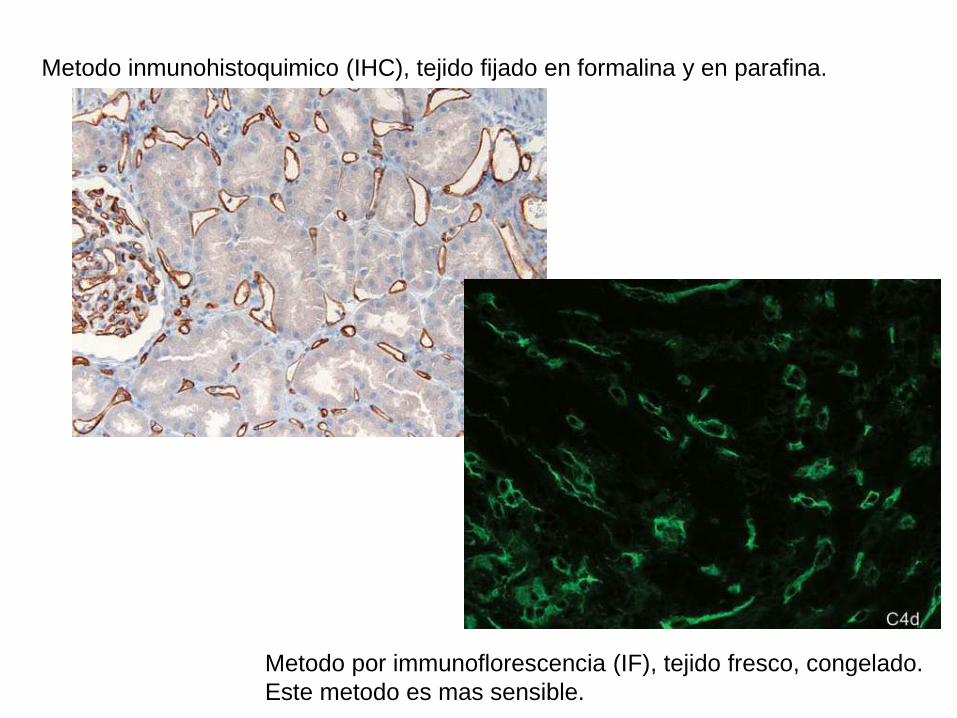
Lesion endotelial aguda litica
Ejemplo tipico Rechazo humoral agudo en pacientes
hiper immunizados
bull Reclutamiento de Complemento y
formacion del complejo de ataque a
membrana
bull C4d+
bull Esta etapa bloqueada por anti C5
eculizumab)
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
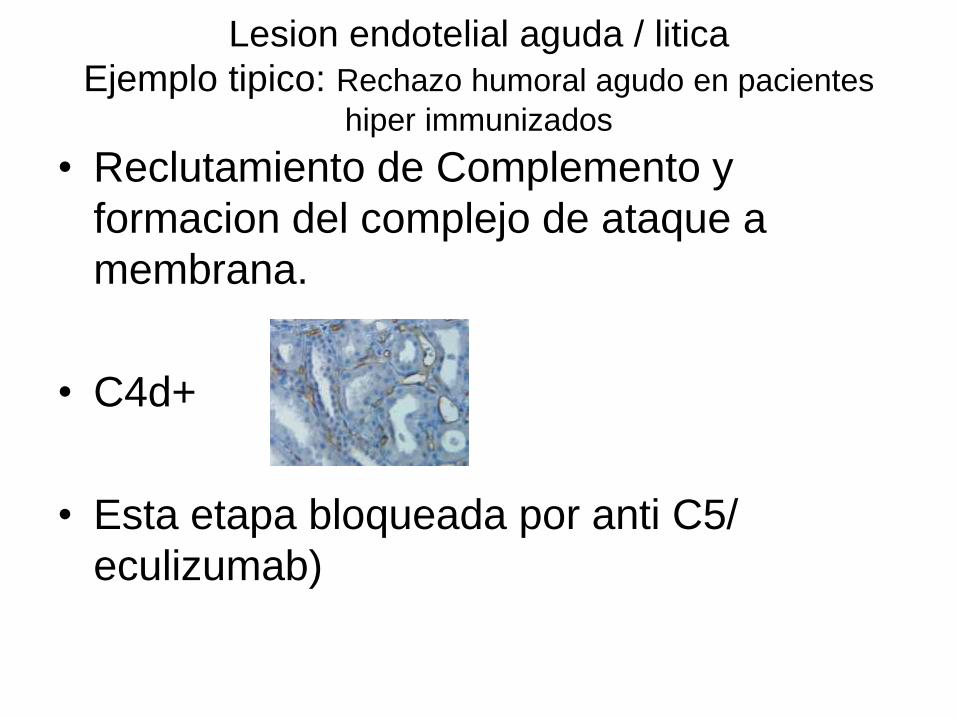
RH con C4d negativo
bull La entidad de RH con C4d negativo se
acepta universalmente
bull Es por lo tanto muy importante reconocer
las lesiones endoteliales caracteristicas
del RH (glomerulitis capilaritis
microtrombosis etc) Alguna de estas
lesiones estara presente aun cuando el
C4d sea negativo
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Microvasculatura del trasplanteProceso agudo activo
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Lesion litica Activacion de la cascada de la coagulacion
Reclutamiento de cellulas inflamatorias
(Dantildeo tubular secundario a isquemia)
Proceso cronico (plusmn proceso activo)
Dantildeo a las cellulas endoteliales (glomerulos capilares arterias)
Activacion endotelial cronica remodelamiento de los capilares
glomerulares y peritubulares
Reclutamiento de celulas inflamatorias
Fibrosis interstitial atrofia tubular esclerosis glomerular
C4d
Anticuerpos especificos contra donante
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Anticuerpos especificos contra-donante
La magnitud del problema
Incidencia
bull Pacientes hiper inmunizados
asymp 30 desarrollan RHA necesitando
tratamiento agresivo
asymp 45 desarrollan RH cronico en 1 aňo (GT)
asymp 30 pierden el riňon en 5 aňos
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
RH La magnitud del problema
Incidencia
bull Transplantes convencionales
asymp 20 desarrollan DSA en 3-4 aňos
asymp 15 desarrollan GT y el riesgo aumenta con
cada aňo que pasa
asymp 25-80 con GT perderan el riňon a
causa de eso
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Development of DSA after kidney Tx
bull Chaudhury 124 6 (2 yearspediatric)
bull Cooper 244 27
bull Wiebe 315 15 in 5-years
bull Everly 189 20 in 5-years
bull Loupy 1016 31 in 5-years
bull Freitas 284 19 in 1-year
(Pancreas Tx
bull Cantarovich 167 155 in 1-year
Author Number of patients
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
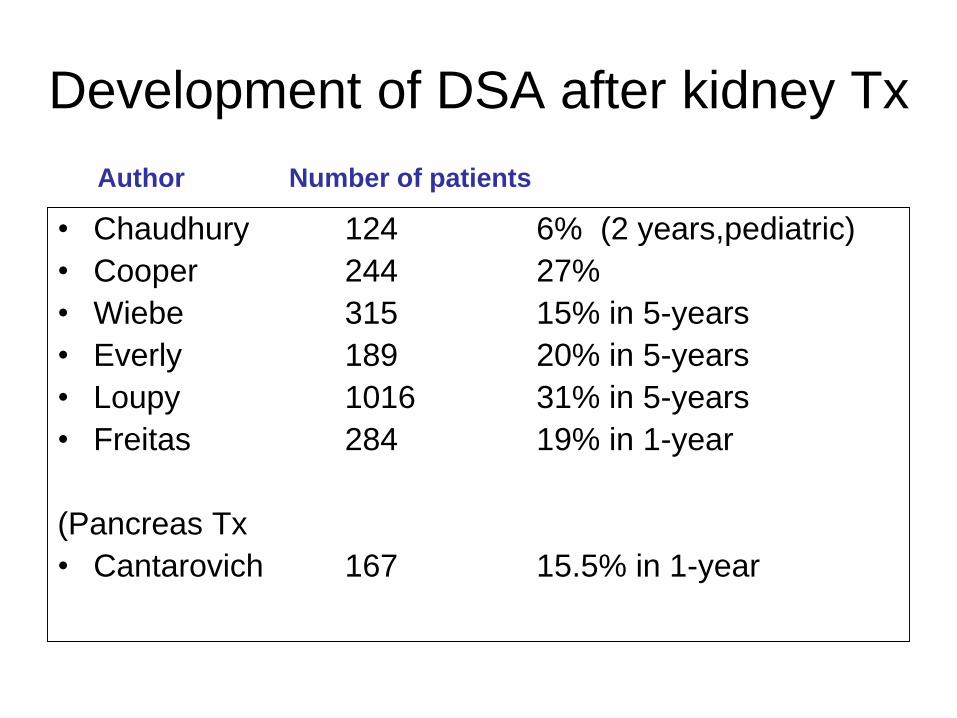
Factores de riesgo
bull DSA pre-trasplante - retrasplantados
bull Nivel de DSA
bull Historia de RH agudo
bull Edad (mas en jovenes)
bull Mala adherencia al tratamiento
bull Etc
ndash Hay relacion entre la severidad cronica y el nivel de DSA y anticuerpos HLA Tipo II) pero la relacion no es absoluta y la presentacion clinica varia mucho de paciente a paciente
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Anticuerpos especificos contra donante
bull Anti HLA antibodies (Class I Class II)
ndash MHC class I (HLA A B C)
ndash MHC class II (HLA DR DP DQ)
bull ABO blood group antigens
bull Non HLA antigens
ndash Angiotensin II type I receptor (AT1R)
ndash MHC Class I related chain A (MICA)
ndash Various other antiendotelial antibodies
More likely to
be C4d
negative
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Clasificacion de Banff RH
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
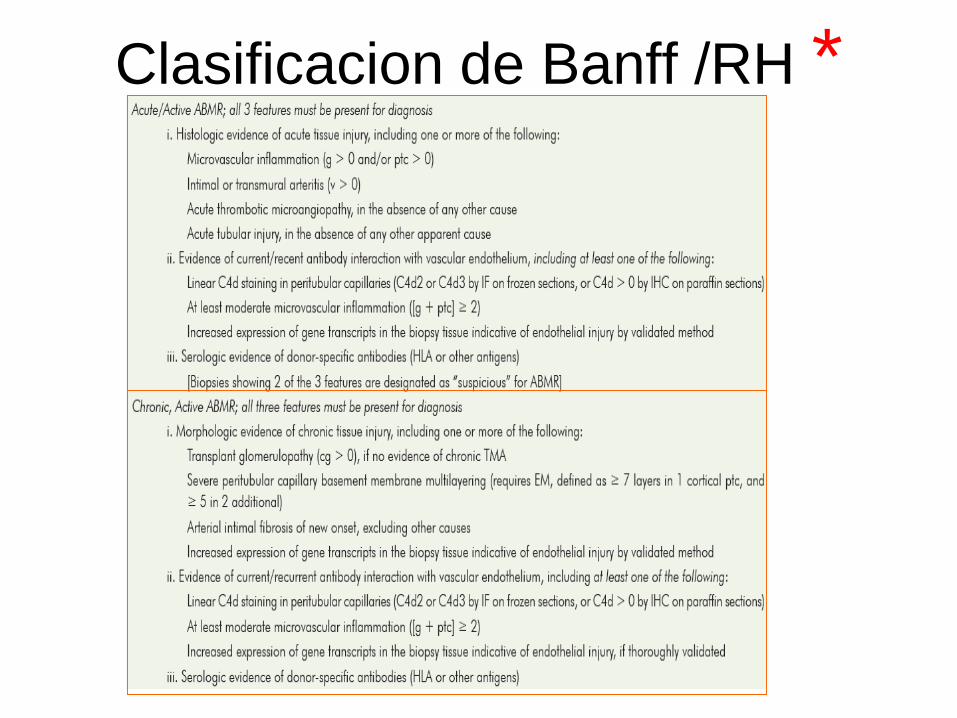
Clasificacion de Banff para el RH Agudo
RH agudoactivodefinido por la ausencia de remodelamiento Puede ser agudo (temporalmente)
Puede ocurrir en cualquier momento post-trasplante
Es tipicamente ldquoactivordquo tiene dantildeo microvascular obvio como
microtrombosis asi como inflamacion (glomerulitis capilaritis)
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
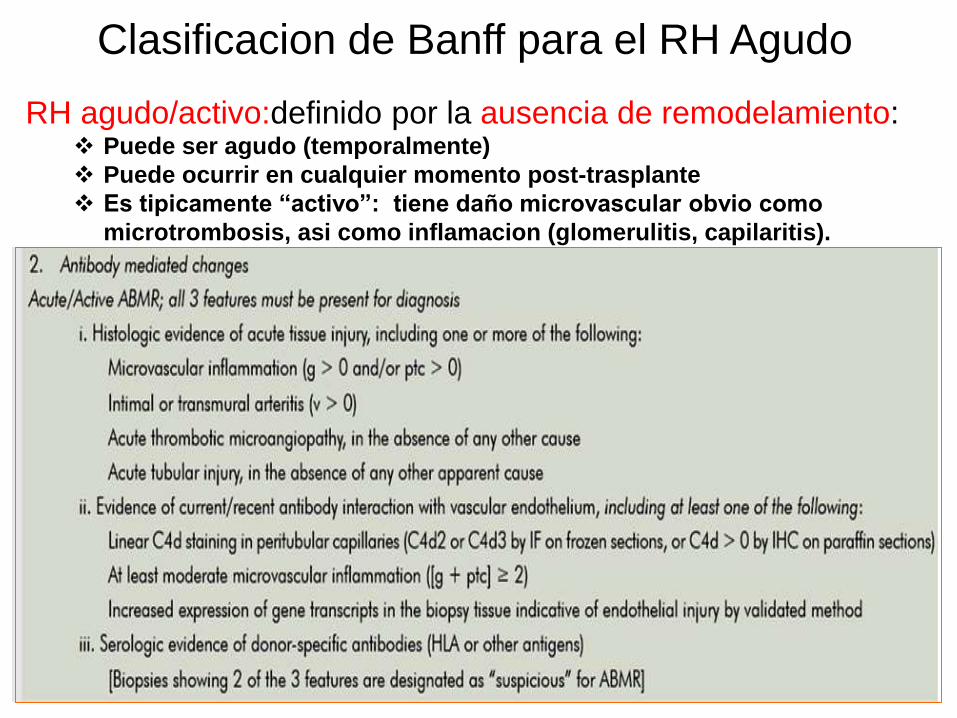
Clasificacion de Banff para el RH cronico
RH chronico definido por remodelamiento
bull Duplicacion de la membrana basal (glomerulopatia del trasplante)
bull Multilamelacion de la membrana basal de los capilares peritubulares
El RH cronico puede ser inactivo (el RH ocurrio en el pasado y se resolvio dejando la
sequela del remodelamiento)
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
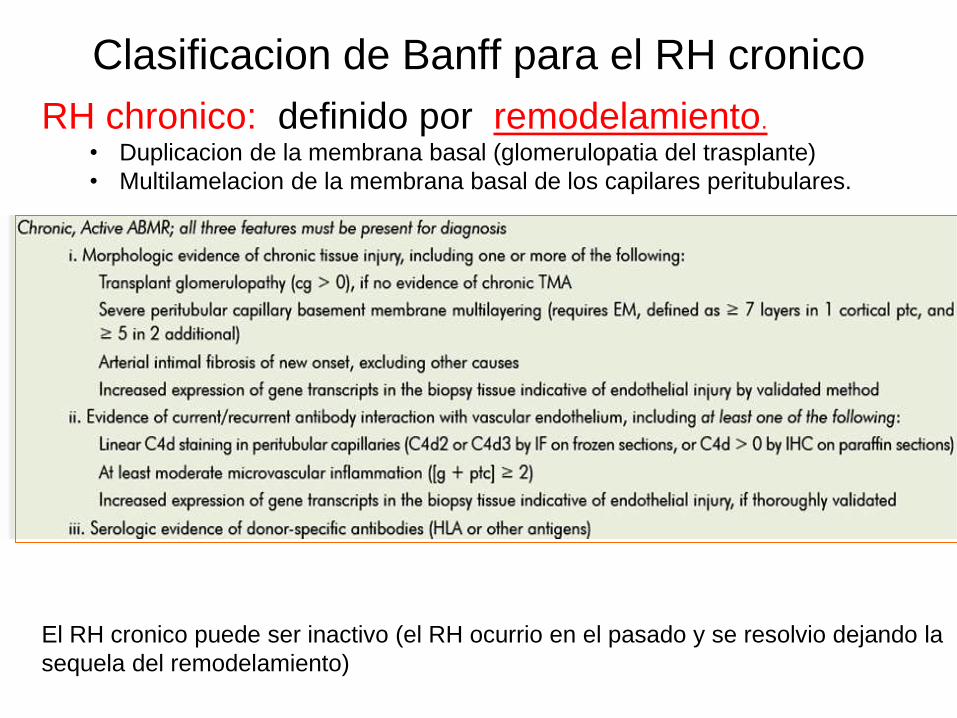
Inflamacion y remodelamiento en el RH
lleva a la perdida prematura del Tx (fibrosis)
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
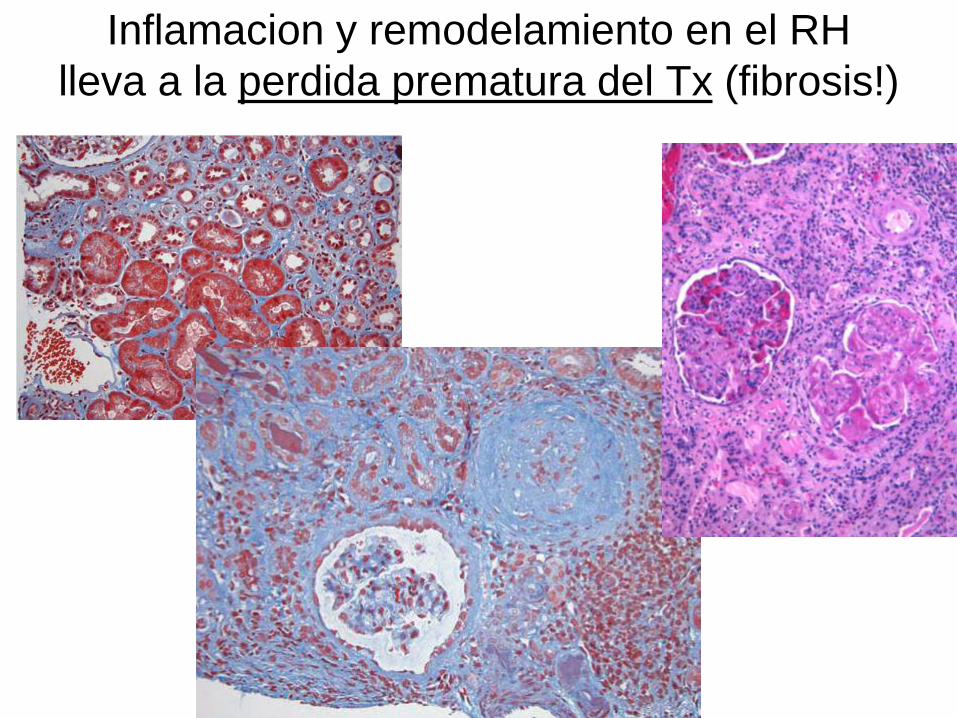
Diagnostic de RH en biopsias
renales
Evidencia histologica de RH se puede
encontrar en pacientes con
ndash Disfuncion aguda
ndash Disfuncion cronica
ndash Funcion estable (lesiones subclinicas)
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Elementos principales
Inflamacion dantildeo microvascular -Agudo glomerulitis (g) capilaritis (ptc) trombosis arteritis necrosis
tubular aguda sin causa aparente
-Cronico duplicacion de la membrana basal glomerular (yo en
capilares peritubulares
-(Estudios moleculares)
C4d (+ en anti-HLA agudo o ndash en otros casos)
Anticuerpo especifico-contra donante- anti-HLA negativo (otro tipo de anticuerpo)
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
61 year-old man with history of HTN status post LURT
History of pre transplant DSA to A24 (niveles bajos)
3 months protocol biopsy
Creatinine from 14 mgdl
No significant proteinuria
Current immunosuppression
FK Goal 8
MMF2g 24hr
Prednisone 5mgday
+ DSA against A24 MFI 6249
B7 MFI 4454
B8 MFI 4032
DR15 MFI 1314
DP4 MFI 2429
CASE 3
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
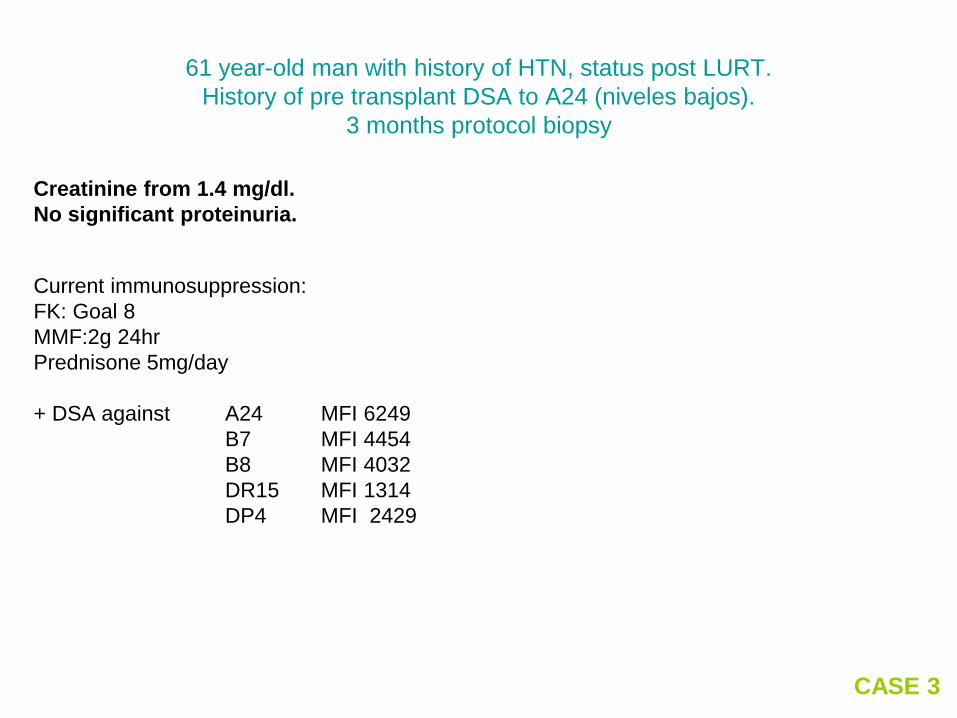
Rechazo agudo (activo)
Perdida de
fenestraciones
en las celulas
endotheliales
Capilaritis
Glomerulitis
C4d
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
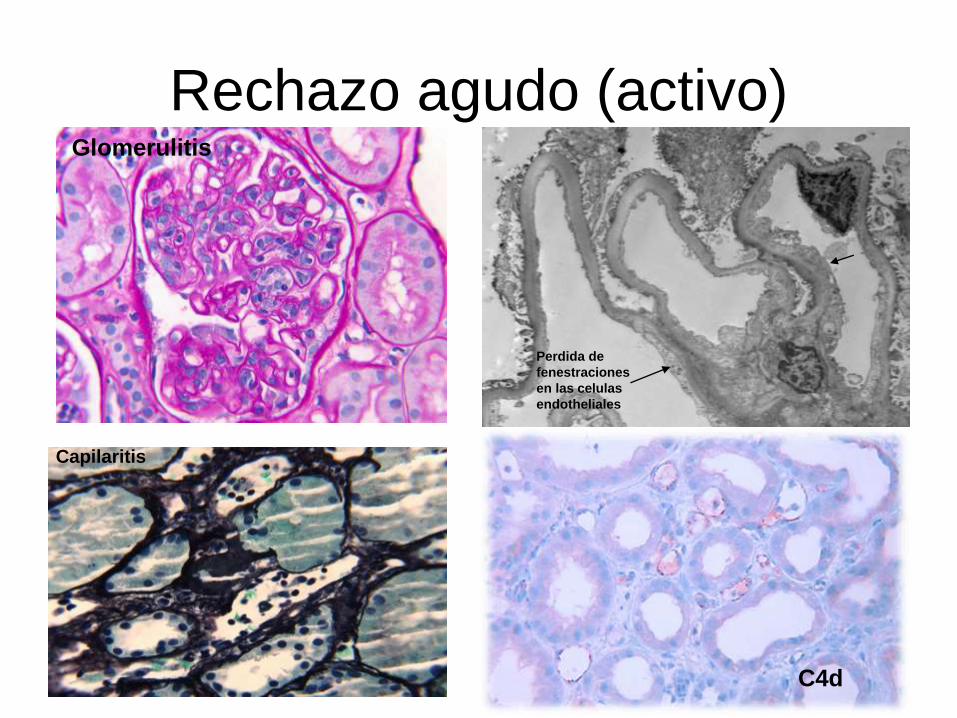
54 year-old woman with history of DM status post cadaveric Tx 12 years ago
Presents with stable creatinine Increasing proteinuria (2gm24h)
Creatinine 21 mgdl
Current immunosuppression
FK Goal 6
MMF1g 24hr
+ DSA against DRw53 MFI 6700
DR15 MFI 2314
CASE 3
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
RH cronico activo
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
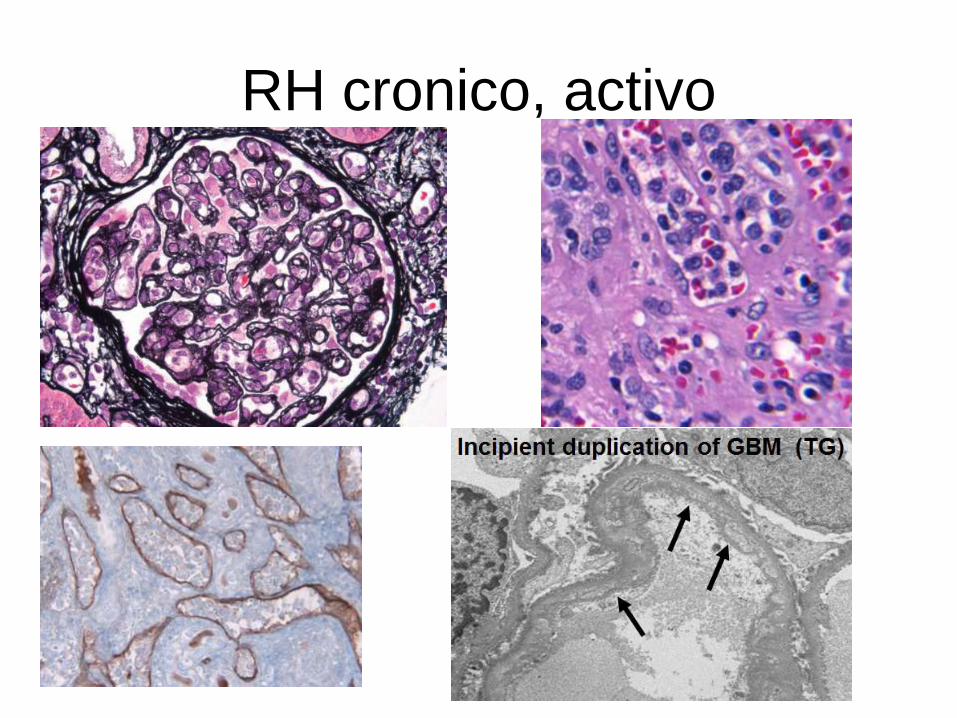
31 year old female with ESRD secondary to acute interstitial nephritis
Presents for protocol biopsy 6 months post LURT
Serum Creatinine stable between 14 and 16 mgdl
No significant proteinuria
Immunosuppression
FK Goal 7-8
MMF 750 mg 2 times daily
Negative DSA studies Negative C4d
CASE 2
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
Multifocal capillaritisIncipient duplication of
basal lamina of PTC
Mild glomerulitis
ldquoSuspiciousrdquo for chronic active antibody mediated allograft rejection
(only 2 of the Banff components present as C4d stain is negative)
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
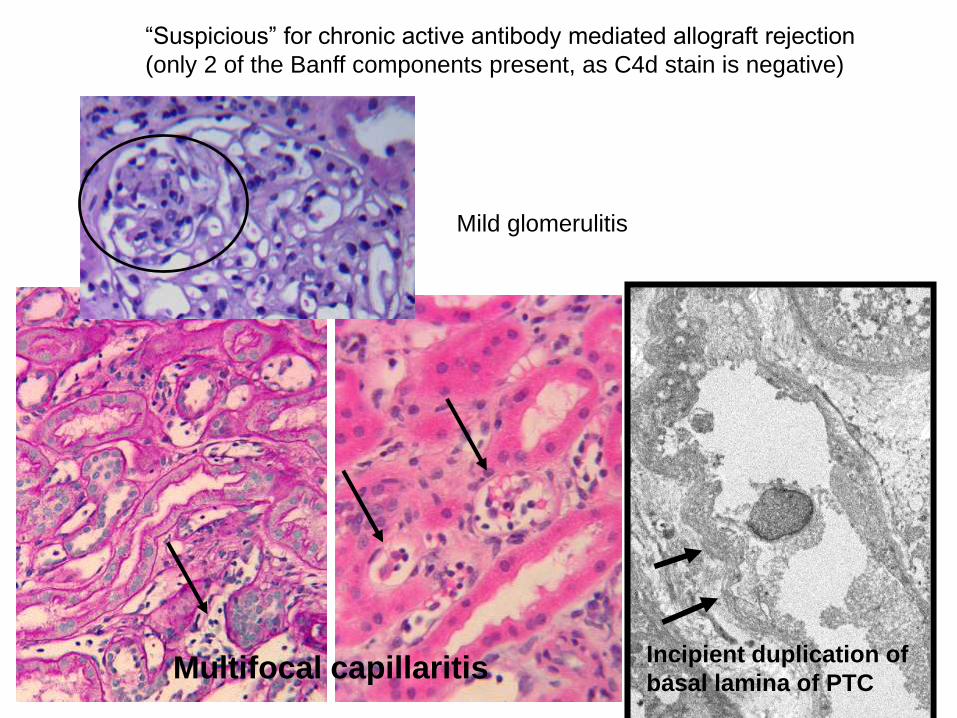
Inflamacion y dantildeo microvascular
caracterizan el RH en otros organosTrasplante de pancreas Trasplante cardiaco
Capilaritis microhemorragias Inflamacion en la microvasculatura
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
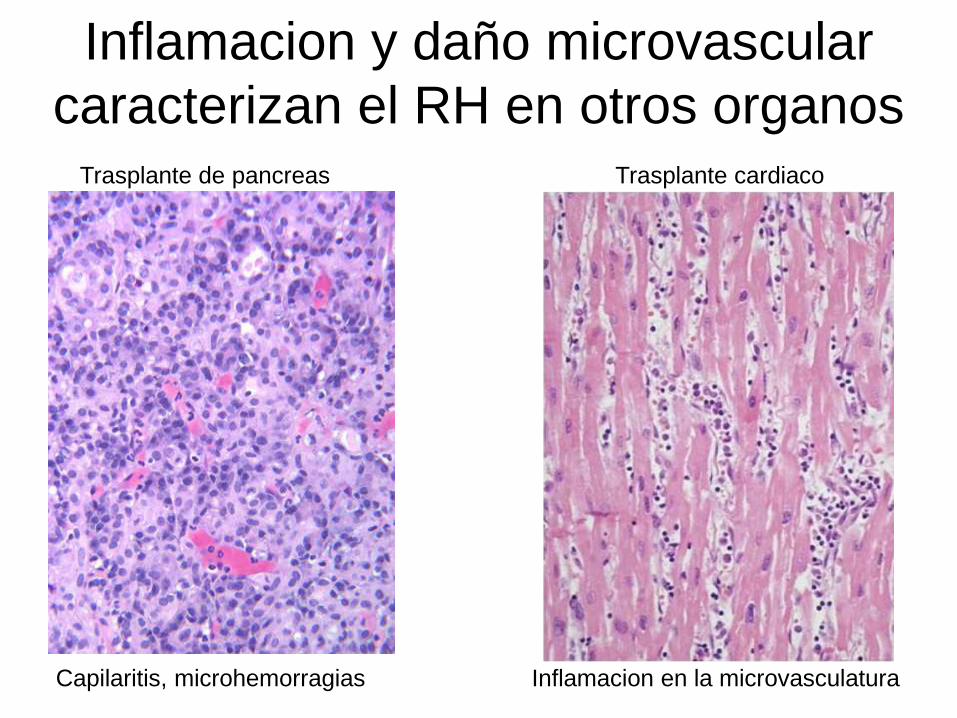
FIN
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
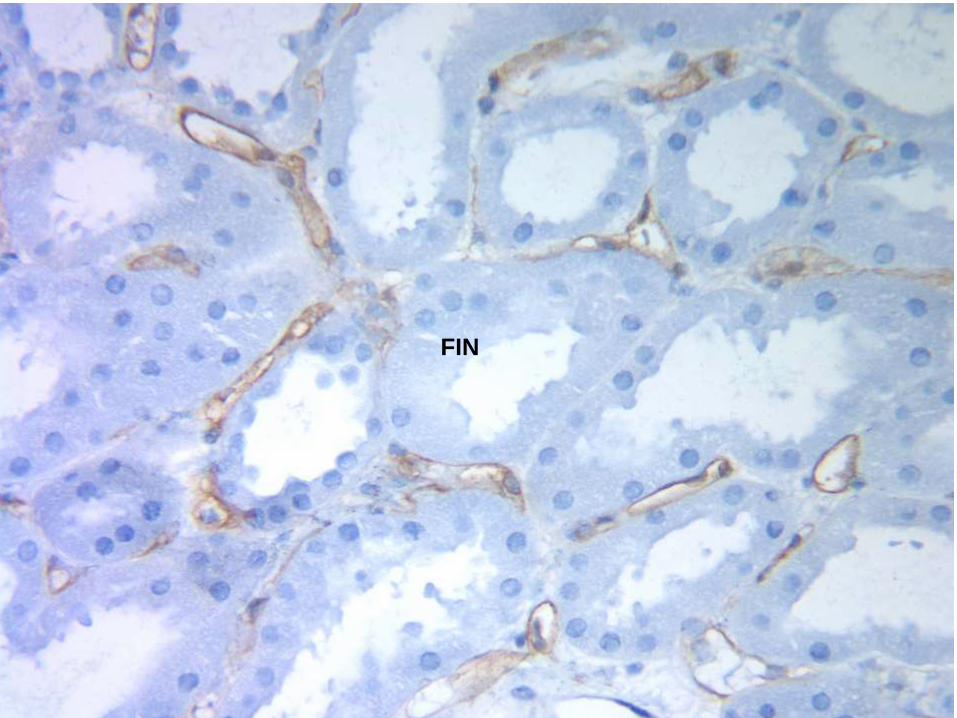
bull Kidney Int 2015 Mar 4 doi 101038ki201564 [Epub ahead of print]
bull The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
bull Kozakowski N1 Herkner H2 Boumlhmig GA3 Regele H1 Kornauth C1 Bond G3 Kikić Ž3
bull Author information
bull Abstract
bull By the Banff classification the score of peritubular capillaritis its extent and its cellular composition should normally be reported in renal allograft pathology While the score represents an important diagnostic and prognostic variable the clinical value of capillaritis extent or composition has yet to be resolved In a retrospective study of 749 renal transplant recipients subjected to 1322 indication biopsies we found that prevalence scores of 1 2 or 3 in the biopsy specimens were 107 116 and 26 respectively Focal and diffuse peritubular capillaritis (inflammation over 50 of cortical peritubular capillaries) was diagnosed in 105 or 144 of cases respectively Mononuclear granulocytic and mixed peritubular capillaritis was present in 131 33 and 85 respectively While peritubular capillaritis without further subclassification was not related to higher allograft loss rates a score of 3 (hazard ratio 257 (CI 125-528)) and diffuse peritubular capillaritis (167 (11-254)) were significant impartial risk factors for allograft loss Diffuse peritubular capillaritis was independently associated with features of chronic antibody-mediated rejection and greater eGFR decline after 3 years In contrast detailed report of leukocytic composition in peritubular capillaritis did not confer additional prognostic information Thus in contrast to typing the infiltrating inflammatory cells the score and extent of peritubular capillaritis in kidney allograft pathology is essential to assess transplant prognosisKidney International advance online publication 4 March 2015 doi101038ki201564
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
bull Nephrology (Carlton) 2015 Feb 26 doi 101111nep12441 [Epub ahead of print]
bull C4d Negative Antibody Mediated Rejection With High Anti-Angiotensin II Type I Receptor Antibodies In Absence Of Donor Specific Antibodies
bull Fuss A1 Hope CM Deayton S Bennett GD Holdsworth R Carroll RP Coates PT
bull Author information
bull Abstract
bull AIMS
bull Acute antibody mediated rejection can occur in absence of circulating donor specific antibodies Agonistic antibodies targeting the anti-angiotensin II type 1 receptor are emerging as important non-HLA antibodies Elevated levels of anti-angiotensin II receptor antibodies were first observed in kidney transplant recipients with malignant hypertension and allograft rejection They have now been studied in three separate kidneytransplant populations and associate to frequency of rejection severity of rejection and graft failure
bull METHODS
bull We report eleven cases of biopsy proven C4d negative acute rejection occurring without circulating donor specific anti-human leukocyte antigen antibodies In eight cases anti angiotensin receptor antibodies were retrospectively examined The remaining three subjects were identified from our centres newly instituted routine anti angiotensin receptor antibody screening
bull RESULTS
bull All subjects fulfilled Banff 2013 criteria for antibody mediated rejection and all responded to anti-rejection therapy which included plasma exchange and angiotensin receptor blocker therapy
bull CONCLUSIONS
bull These cases support the routine assessment of anti-AT1R antibodies in Kidney transplant recipients to identify subjects at risk Further studies will need to determine optimal assessment protocol and the effectiveness of pre-emptive treatment with angiotensin receptor blockers
bull This article is protected by copyright All rights reserved
bull KEYWORDS
bull AT1R Angiotensin receptor blocker angiotensin II type 1 receptor antibody antibody mediated rejection atypical hla antibody
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival
bull J Am Soc Nephrol 2015 May26(5)1161-71 doi 101681ASN2013121277 Epub 2014 Nov 7
bull Endothelial cell antibodies associated with novel targets and increased rejection
bull Jackson AM1 Sigdel TK2 Delville M3 Hsieh SC2 Dai H2 Bagnasco S4 Montgomery RA5 Sarwal MM6
bull Author information
bull Abstract
bull The initial contact point between a recipients immune system and a transplanted graft is the vascular endothelium Clinical studies suggest a pathogenic role for non-HLA antiendothelial cell antibodies (AECAs) in allograft rejection however evidence linking AECAs of known specificity to in vivo vascular injury is lacking Here we used high-density protein arrays to identify target antigens for AECAs isolated from the sera of recipients of kidney transplants experiencing antibody-mediated rejection in the absence of donor-specific HLA antibodies Four antigenic targets expressed on endothelial cells were identified endoglin Fms-like tyrosine kinase-3 ligand EGF-like repeats and discoidin I-like domains 3 and intercellular adhesion molecule 4 the first three have been implicated in endothelial cell activation and leukocyte extravasation To validate these findings ELISAs were constructed and sera from an additional 150 renal recipients were tested All four AECAs were detected in 24 of pretransplant sera and they were associated with post-transplant donor-specific HLA antibodies antibody-mediated rejection and early transplant glomerulopathy AECA stimulation of endothelial cell cultures increased adhesion molecule expression and production of inflammatory cytokines regulated on activation normal T cell expressed and secreted PDGF and RESISTIN These correlations between in vitro experiments and in vivo histopathology suggest that AECAs activate the vascular endothelium amplifying the alloimmune response and increasing microvascular damage Given the growing number of transplant candidates a better understanding of the antigenic targets beyond HLA and mechanisms of immune injury will be essential for improving long-term allograft survival