Efecto de una fórmula de suero de leche con predominio de arranque que contiene LCPUFAs y...

of 9
-
Upload
brendaf-caro -
Category
Documents
-
view
217 -
download
0
Transcript of Efecto de una fórmula de suero de leche con predominio de arranque que contiene LCPUFAs y...
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
1/9
Asia Pac J Clin Nutr 2010; 19 (4):473-480Original ArticleEffect of a whey-predominant starter formula containingLCPUFAs and oligosaccharides (FOS/GOS) ongastrointestinal comfort in infantsBoosba Vivatvakin M D ' , Atchara M ahayosnond MD^, Apiradee T heam boonlers BSc',Philippe G Steenhout M D '', Nelly J Conus ^'Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Ba ngkok, Thailand^Department of Radiology, Faculty of Medicine, C hulalongkorn U niversity, Bangkok, Thailand^Nestec Ltd, Nestl Nutrition, Vevey, Switzerland
D evelopment of new infant formulas aims to replicate the benefits of breast milk. One benefit of breast milkover infant formulas is greater gastrointestinal comfort. We compared indicators of gastrointestinal comfort ininfants fed a whey-predominant formula containing long-chain polyunsaturated fatty acids, galacto-oligo-saccharides and fructo-oligosaccharides, and infants fed a control casein-predominant formula without additionalingredients. The single-centre, prospective, double-blind, controlled trial randomly assigned healthy, full-terminfants (n=I44) to receive exclusively either experimental or control formula from 30 days to 4 months of age. Agroup of exclusively breast-fed infants served as reference (n=80). At 1,2, 3, and 4 months, infants' growth pa-rameters were measured and their health assessed. Parents recorded frequency and physical characteristics of in-fants' stool, frequency of rgurgitation, vomiting, crying and colic. At 2-months, gastric emptying (ultrasound)and intestinal transit time (H2 breath test) were measured, and stool samples collected for bacterial analysis.Compared to the control (n=69), fewer of the experimental group (n=67) had hard stools (0.7 vs 7.5%, p
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
2/9
474 B Vivatvakin, A Mahayosnond, A Theamboonlers, PG Steenhout and NJ Conus
the effects of human milk. LCPUFAs such as docosahex-aenoic acid (DHA) and arachidonic acid (AA) have im-portant functions as precursors of eicosanoids and othercyclo-oxygenase products, as well as structural compo-nents of cell membranes. Although studies on the specifichealth benefits of LCPUFAs in infants are inconsistent, itappears that dietary LCPUFAs play a role in improvingthe visual and cognitive functions of preterm infants .'*'"The aim of the current study was to determine whetherinfants fed a whey-predominant formula containingLCPUFA and FOS/GOS exhibit better measurements ofGI comfort than infants fed a standard starter casein-predominant formula with no additional constituents.MATERIALS AND METHODSSubjectsSubjects were healthy infants not older than 30 days ofage at the time of enrolment, whose mothers had chosento feed them exclusively with formula from 30 days to 4months of age (formula-fed groups) or had chosen to ex-clusively breast-feed from birth until they were 4 monthsold (breast-fed group). Infants in the formula-fed groupscould have been partially breast-fed prior to being 30days old. To be included in the study, infants had to behealthy, ill-term (gestational age >37 wk), and weighbetween 2500 and 4500 g at birth. Infants were excludedfrom the study if they had congenital illnesses or malfor-mation, had significant pre-or post-natal diseases, hadrequired hospitalisation for >2 days, received antibiotictreatment, were known to have cow's milk allergy, hadparents who were expected to have difficulty complyingwith the feeding regimen, or if they were participating inanother clinical study.
This study was conducted between June 2006 andJanuary 2008, during which time 224 infants were re-cruited. It was run in accordance with the principles andrules of the Declaration of Helsinki and adhered to GoodClinical Practice guidelines of the International Confer-ence on Harmonization. It was approved by the EthicalReview Committee for Research in Human Subjects,Ministry of Public Health and the Faculty of Medicine,Chulalongkom University, Thailand. Informed consentwas obtained from the infants' legal representatives.Trial designThe current study was a single-centre, prospective, ran-domised, double-blinded, controlled parallel-group trialwith an unblinded reference (breast-fed) group. It wasconducted at the Paediatric Gastroenterology Unit of theChulalongkom University Hospital in Bangkok, Thailand.Blinding was performed by labeling each tin of productwith the same product code and protocol number, theonly distinguishable feature being the colour of the label(yellow or blue). The identity of the specific product isblind to subjects, support staff, investigators and spon-sor/manufacturers. Envelopes were used for randomiza-tion. Each envelope is identified by trial no., site ID, gen-
The study lasted approximately 18 months and infants(in formula groups) were fed exclusively with one of thetwo fonnulas until 4 months of age.Upon enrolment, infants were randomly assigned toone of the two formula groups, stratified by sex. Infantsreceived their assigned formula, a whey-predominantformula containing LCPUFAs and the prebiotics FOS/
GOS (experimental formula group), or a standard casein-predominant formula lacking LCPUFAs and prebiotics(control formula group), starting at enrolment. Parentsreceived instructions on preparation and feeding of theformulas.Baseline measurements were taken at enrolment. In-fants were fed ad libitum exclusively with their allocatedformula from 30 days of age through 4 months of age.Follow-up visits took place when infants reached the ageof 303 days, 603 days, 903 days, and 1203 days.Parents kept 3-day diaries prior to each visit, wherethey recorded the volume of the infants' formula, stoolcharacteristics (frequency, consistency colour, and odour),digestive tolerance (occurrence of colic, crying, spitting,and vomiting), and general acceptance of the formulabased on visual analogue scale (VAS). The study stafffilled out case report forms at each visit and recorded thenumber of cans of formula distributed to each infant andthe number that remained unused, any medication ortreatment administered, and any concomitant intake ofliquid, semi-solid, or solid food. At each visit, investiga-tors took anthropomtrie measurements, reviewed the 3-day diary, and assessed any incidents of morbidity. Addi-tionally, at the 2-month visit, GE time was measured byultrasound and intestinal transit by H2 breath analysis.Stool bacterial analysis w as also performed at 2 months ina subset of 30 infants from each group.
FormulasFormulas were isocaloric powdered "starter" fonnulasintended for full nutritional support of infants from birthto 6 months of age (Table 1). The experimental formulacontained whey as the main source of protein, LCPUFAsand a prebiotic mixture of 90% GOS and 10% FOS (4 g/Lof reconstituted formula). Both formulas were identical intaste and texture and were manufactured according to GoodManufacturing Practices and packaged by the sponsor.MeasurementsGE rate was initially selected as the primary outcome butGE time at 2 months of age was taken as the surrogateprimary outcome and was calculated by modification ofthe method described by Darwiche and colleagues.^" GEtime was measured by ultrasound using the ACOUSONmodel Sequeoia 512 (Siemens, Germany) with an 8C4transducer (4-8 mHz broadband) and the infant was laidin the seat designed to maintain a semi-reclining positionthat corresponds to the position of being held by themother during breast feeding. The gastric antrum wasidentified by sagittal ultrasound scan at the level of the
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
3/9
Effect of an infant formula on gastric emptying 475
Table L Formula nutrient compositions
EnergyProteinWhey/Casein ratioFatArachidonic AcidDHA^CarbohydrateLactosc/Maltodextrin ratioGOS^ + FOS^ (GOS/FOS ratio)
unitskcal/lOOmLg/100 kcal-g/100 kcal% of total fat% of total fatg/100 kcal-g/100 kcal
Experimental Formula66.82.1160/405.220.160.1611.1670/300.6(90/10)
Control Formula67.92.4723/775.130010.9870/300
^ DHA = doeosahexaenoic acid, GOS = galacto-oligosaceharides, FOS = fructo-oligosaccharides.
a pause in the semi-reclining position. The ACSA wasmeasured at 10 minute intervals for 1 hour, and thereafter,at 20 minute intervals until the ACSA returned to thebaseline value. The time it took for the ACSA to increaseand retum to the baseline value was taken as the total GEtime.
The secondary outcomes were intestinal transit time,digestive tolerance (stool characteristics and infant's be-haviour), anthropomtrie measurements (weight, recum-bent length, and head circumference), and the occurrenceof any adverse events (AEs).Intestinal transit time was measured at 2 months of ageusing the H2 breath-test. Prior to the test, infants werefasted for 4 h. Exhaled Alveolar air sample was collectedand baseline H2 and CH4 were measured using MicrolyzerSC (Quintron, USA) and CO2 as a standard. Fasting base-
line values of
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
4/9
476 B Vivatvakin, A M ahayosnond, A T heamboonlers, PG Steenhout and NJ Conus
boundary of the 90% confidence interval (CI) for thetreatment difference must lie above A^3.0 g/day. Otheranthropomtrie measures were tested for non-equivalencehypotheses.
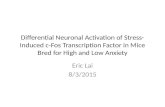
For the analysis of stool microbiota, bacterial countswere log transformed and counts reported per g of stool.Bacteria counts below the detection limit were set to thevalue ofthe detection limit (1x10^ colony forming units/g).Any differences between the experimental and controlgroups were assessed using Wilcoxon rank sum test ad-justing for multiplicity according to the Hommel method.R E S U L T SStudy populationTwo hundred and twenty-four infants were enrolled inthis study and 169 of these infants completed the study.Drop-out rate was slightly higher in the experimentalgroup compared with the control group (25% vs 19%) butthis was not statistically significant (Figure 1). Baseline
characteristics were similar between the groups (Table 2).Gastric emptyingAlthough a small treatment effect of 1.75 mins was de-tected between the two formulation groups, suggesting aslightly shorter mean GE time for the experimental group,no statistically significant differences were detected com-pared with the control group (Table 3). A similarly smalldifference was detected between the two formulationgroups for intestinal transit time (data not shown) thatwas not statistically significant.Formula acceptability and toleranceThe acceptability of the formula based on mean VASscores was similar in the experimental formula group(8.32.1) and the control formula group (8.11.8). Theprofile ofthe behaviour characteristics is fairly similar forthe experimental and control groups.
Enrolment and randomisationn = 224(ITT-population)
f
Experimental formulan = 71
r
Control formula jn = 7 3 J
f
f
Breast-fedn = 80
r
Comple tedn = 53
Withdrawnn = 18AE (2 )
Consent withdrawn (1)Lost in follow-up (15) ^/
' Completed >n = 59
Withdrawnn = 14
Consent withdrawn (1)
' Completed >n = 57
Withdrawnn = 23
Consent withdrawn (3)\^ Lost in follow-up (13) ^ \^ Lost in follow-up (20) ^
Figure 1. Disposition of recruited patients (ITT = intention-to-treat).Table 2. Baseline ch aracteristics (mean SD) of infants (intention-to-treat group)
Treatment GroupsGirls (n)Age (days)
Weight (kg)Height (cm)Head circumference (cm)
Experimental3816.7 5.2
3.4 0.551 .42 .035.0 1.5
Control3816.0 5.6
3.4 0.551.1 2.634.9 I.I
Breastfed3516.8 6. 0
3.5 0.35 I . 9 2 . 13 5 . 0 l . l
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
5/9
Effect of an infant formula on gastric emptying 477
Stool characteristicsThe diary recordings of stool characteristics revealed thatthere was a statistically significant difference between theexperimental and control groups with regard to stool con-sistancy with less hard stools (p
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
6/9
47 8 B Vivatvakin, A Mahayosnond, A Theamboonlers, PG Steenhout and NJ Conus
between the experimental and control groups for bodylength and head circumference.Stool microbiotaTotal bacterial count was similar in all groups. Bifidobac-teria, the most predominant species identified in all groups,were found in higher percentages in the experimental(78.1%) and breast-fed (74.3%) groups compared withthe control group (63.7%). Despite the low level of sam-ples analysed, the stool microbiota of the experimentalgroup appe ared to resemble that of the breast-fed infantsbetter, (with higher Bifidobacteria and lower Clostridiaand Enterobacteriacae counts) (Table 5) than did the mi-crobiota of the control group.Adverse eventsTwo hundred and twenty-eight AEs were reported in 123infants. AE s occurred in 49% , 56%, and 59% of infants inthe experimental, control and breast-fed groups, respec-tively. The most frequently occurring AEs were upperrespiratory tract infections. GI problems (diarrhoea, vom-iting, and constipation) were reported in infants at a rateof 11 % in the experimental formula g roup, 15% in thecontrol formula group, and 9% in the breast-fed group.There were no significant differences in occurrence of thedifferent AEs between grou ps.
Three AEs were identified as serious by the investiga-tor (one in each treatment group).DISCUSSIONWe hypothesised that an experimental formula containingwhey as the main source of protein and oligosaccharideswould improve gastrointestinal comfort since these ingre-dients have been previously implicated as promoting goodgastrointestinal health.""'''''' The current study providedevidence that the GI comfort of infants fed the experi-mental whey-predominant prebiotic containing formulawas superior to that of infants fed the standard casein-predominant control formula. Infants in the experimentalgroup had significantly less hard and more, soft stoolsthan the control group. Although not reaching statisticalsignificance, the experimental group also tended to have aslightly faster mean GE time (1.75 min; p=0 .88) andhigher stool frequency (p=0.28) than the control group.Also, the experimental group appeared to have higherBifidobacteria and lower Clostridia and Enterobacteriacaethan the control group and was closer to the breastfeedinggroup. Taken together, the results obtained with thewhey-predominant FOS/GOS-containing formula supportthe view of improved gut comfort in terms of stool con-sistency, GE time, GI symptoms and stool microbiotacompared with a standard casein-predominant controlformula without prebiotics.
Oligosaccharides have a bulking effect in the colon,increasing colonie motility and reducing intestinal tran-sit.'^ Also, previous studies have shown that infants fed awhey hydrolysate formula have higher GE compared with
cient to detect differences. Specifically, in the currentstudy, sample size calculation was based on a previousstudy that compared the GE rate in healthy subjects withthat of diabetic subjects.^" Because up to 50% of diabeticpatients have been reported to suffer from gastroparesis,the number of subjects required to observe a treatmenteffect between these two populations may be smaller thancomparison of two healthy populations.^' Our study com-pared the effect of different formulas in healthy infants, inwhom an effect may not be readily detectable. Indeed, incontrast to previous studies that had shown that breast-fedinfants have faster GE than formula-fed infants, we didnot observe statistically significant differences in GE be-tween the formula-fed infants and the breast-fed infants.'Nevertheless, our results indicated a tendency for the ex-perimental formula, as compared to the control formula,to increase gastric and intestinal transit and showed thatthe experimental formula was safe and well-tolerated.
The lower boundary of the 90% CI for difference inmean weight gain in the two formula groups was higherthan -3.0 g/day indicating that the experimental formula isnot inferior to the control formula based on the pre-defined criteria of non-inferiority. Thus, it was estab-lished that the feed formulas did not effect normal growth.A study with a larger number of infants is probably re-quired to establish whether GE in infants is significantlyaffected by the experimental formula used in this study.The results presented here indicate, however, the safety ofthe whey-predominant prebiotic-containing formula. It alsoshowed improved gut comfort in terms of stool consis-tency, GE time and GI symptoms; in addition, the micro-biota composition of infants fed the experimental formulaappeared to resemble that of the breast-fed formula. Addi-tional studies with whey predominant and prebiotic-containing formulas will be required to further supportthese findings.ACKNOWLEDGEMENTSThis study was funded by Nestec Ltd. We thank Dr GerardMcGregor, OmniScience SA, who provided medical writingservices on behalf of Nestl Nutrition. The authors were fullyresponsible for contents and editorial decisions for this manu-script.AUTHOR DISCLOSURESDr Boosba Vivavakin, received grant from Thai Red Cross So-ciety, Chulalongkom University and a non-profitable fund fromPacific Healthcare (Thailand), Dr Atchara Mahayosnond, Na-tional research Council of Thailand, received grant from Chu-lalongkorn University, Apiradee Theamboonlers, received grantfrom Nationa l Research Council of Thailand , Dr Nelly Con usand Dr Philippe Steenhout are Nestl em ployees.REFERENCES1. Hunt JN. A possible relation betwee n the regulation of gas-
tric emptying and food intake. Am J Physiol GastrointestLiver Physiol. 1980;239:Gl-G4.2. Siegel M, Lebenthal E, Krantz B. Effect of caloric density
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
7/9
Effect of an infant formula on gastric emptying 47 9
4. Nyman M. Fermentation and bulking capacity of indigesti-ble carbohydrates: the case of inulin and oligofructose. Br JNutr.2002;87;S 163-8.
5. Siegel M, Krantz B, Lebenthal E. Effect of fat and carbohy-drate composition on the gastric emptying of isocaloricfeedings in premature infants. Gastroenterology. 1985;89:785-90.
6. Pascale JA, Mims LC, Greenberg MG, Alexander JB. Gas-tric response in low birth weight infants fed various formu-las. Biol Neonate. 1978;34:150-4.
7. Van Den Driessche M, Peeters K, Marien P, Ghoos Y, Dev-lieger H, Veereman-Wauters G. Gastric emptying in for-mula-fed and breast-fed infants measured with the 13C-octanoic acid breath test. J Pediatr Gastroenterol Nutr. 1999;29:46-51.
8. Langhen dries JP, Detry J, Van Hees J, Lamboray JM, Dari-mont J, Mozin MJ Sec retin MC , Senterre J. Effect of a fer-mented infant formula containing viable bifidobacteria onthe fecal flora composition and pH of healthy full-term in-fants. J Pediatr Gastroenterol Nutr. 1995;21:177-8I.
9. Rochat F, Cherbut C, Barclay D, Puccio G, Fazzolari-NesciA, Grathwohl D, Hasche F. A whey-predominant formulainduces fecal microbiota similar to that found in breast-fedinfants. Nutr Res. 2007;27:735-40.
10. Petschow BW, Talbott RD. Growth promotion of Bifidobac-terium species by whey and casein fractions from humanand bovine milk. J Clin Microbiol. l990;28:287-92.
11. Billeaud C, Guillet J, Sandier B. Gastric emptying in infantswith or without gastro-oesophageal reflux according to thetype of milk. EurJ Clin Nutr. 1990;44:577-83.
12. Fried MD, Khoshoo V, Seeker DJ, Gilday DL, Ash JM,Pencharz PB. Decrease in gastric emptying time and epi-
sodes of rgurgitation in children with spastic quadriplegiafed a whey-based formula. J Pediatr. 1992; 120:569-72.
13. Tolia V, Lin CH, Kuhns LR. Gastric emptying using threedifferent formulas in infants with gastroesophageal reflux. JPediatr Gastroenterol Nutr. 1992;15:297-301.
14. Thorkelsson T, Mimouni F, Namg ung R, Fernandez-UlloaM, Krug-Wispe S, Tsang RC. Similar gastric emptying ratesfor casein- and whey-predominant formulas in preterm in-fants. Pediatr Res. 1994;36:329-33.
15. Cherbut C. Inulin and oligofructose in the dietary fibre con-cept. Br J Nutr. 2002;87:S 159-62.
16. Gibson GR, Beatty ER, Wang X, Cummings JH. Selectivestimulation of bifidobacteria in the human colon by oli-gofructose and inulin. Gastroenterology. 1995; 108:975-82.
17. Kleessen B, Sykura B, Zunft HJ, Blaut M. Effects of inulinand lactose on fecal microflora, microbial activity, andbowel habit in elderly constipated persons. Am J Clin Nutr.1997;65:1397-402.
18. Carlson SE, Werkman SH, Rhodes PG, Tolley EA. Visual-acuity development in healthy preterm infants: effect of ma-rine-oil supplementation. Am J Clin Nutr. 1993;58:35-42.19. O'Connor DL, Hall R, Adamkin D, Auestad N, Castillo M,Connor WE et al. Growth and development in preterm in-fants fed long-chain polyunsaturated fatty acids: a prospec-tive, randomized controlled trial. Pediatrics. 200l;l08:359-7I.
20 . Darwiche G, Almer LO, Bjorgell O, Cederholm C, NilssonP. Measurement of gastric emptying by standardized real-time ultrasonography in healthy subjects and diabetic pa-tients. J Ultrasound Med. 1999; 18:673-82.
21 . De Block CE, De Leeuw IH, Pelckmans PA, Van Gaal LF.Current concepts in gastric motility in diabetes mellitus.Curr Diabetes Rev. 2006;2:l 13-30.
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
8/9
480 B Vivatvakin, A Mahayosnond, A Theamboonlers, PG Steenhout and NJ Conus
Original ArticleEffect of a whey-predominant starter formula containingL C P U F A s and oligosaccharides (FOS/GOS) ongastrointestinal comfort in infantsBoosba Vivatvakin MD' , Atchara Mahayosnond MD^, Apiradee Theamboonlers BSc',Philippe G Steenhout MD^ Nelly J Conus ^'Department of Pediatrics, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand^Department of Radiology, Faculty of Medicine, C hulalongkorn University, Bangkok, Thailand^Nestec Ltd, Nestl Nutrition, Vevey, Switzerland
^ 80 ^ t is. % 1^ 2 o o 4
t # l ^ ( tb 7.5%.8 bb 8 2 . 3 % ' p < 0 . 0 5 ) ^ . ^ j t i t ^ ^ ^ ^ ^ ^ - B - i K ^IJ-^ 78.1% ^ # a s j j . ^ 63.7% ^ # | L . ^ ^ 74.3%l; 59.6 ^^# ^ f i a s a ^ 61.4 ^^# ^ #ILa . 55.9
4!-Ase.;r:fej
-
8/4/2019 Efecto de una frmula de suero de leche con predominio de arranque que contiene LCPUFAs y oligosacridos (FOS
9/9
Copyright of Asia Pacific Journal of Clinical Nutrition is the property of Asia Pacific Journal of Clinical
Nutrition and its content may not be copied or emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission. However, users may print, download, or email articles for
individual use.