Early diagnosis of pancreatic...
82
Early Diagnosis of Pancreatic Cancer Dr. Yuk Tong LEE MBChB, MD(CUHK), FRCP (Edin), FRCP(Lond), FHKCP, FHKAM Specialist in Gastroenterology and Hepatology
Transcript of Early diagnosis of pancreatic...
Early Diagnosis of Pancreatic Cancer
Dr. Yuk Tong LEEMBChB, MD(CUHK), FRCP (Edin), FRCP(Lond), FHKCP, FHKAMSpecialist in Gastroenterology and Hepatology
Pancreatic cancer
� Pancreatic cancer– Primary tumour – adenocarcinoma, cystic neoplasm,
neuroendocrine tumour– Metastasis

Pancreatic cancer
§ In US, estimated 45220 new cases and 38460 deaths in 2013.
§ Developed country 3x> developing country
§ Very low 5-year survival for those confirmed adenoCA,
§ 10 adenoCA in 4922 PC in Finnish Cancer registry
§ Improved to 6% (2003 - 2009) in SEER statistics§ Up to 20% of patients are eligible for initial resection.§ After potential curative resection, 5-year survival of is only up
to 25%.
Carpelan-HolmstrÖm M, Gut 2005; International Agency for Research on Cancer, WHO, 2008. Surveillance, Epidemiology, and End Result Program, National Cancer Institute;
Siegel R, CA Cancer J Clin 2014; Gillen S, PLoS Med 2010; 7: e1000267
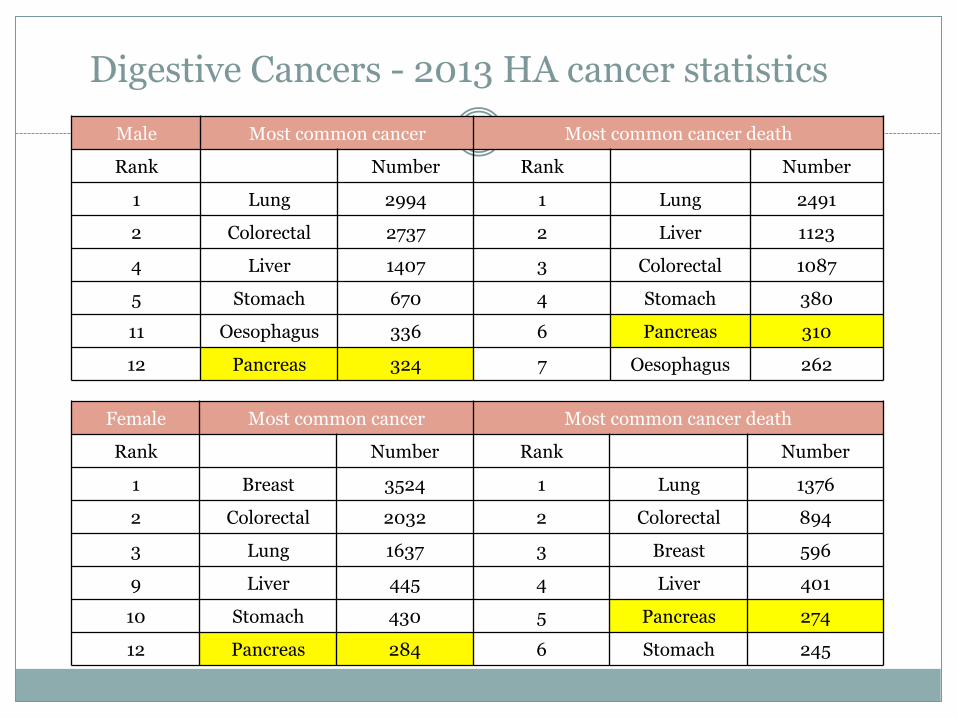
Male Most common cancer Most common cancer death
Rank Number Rank Number
1 Lung 2994 1 Lung 2491
2 Colorectal 2737 2 Liver 1123
4 Liver 1407 3 Colorectal 1087
5 Stomach 670 4 Stomach 380
11 Oesophagus 336 6 Pancreas 310
12 Pancreas 324 7 Oesophagus 262
Digestive Cancers - 2013 HA cancer statistics
Female Most common cancer Most common cancer death
Rank Number Rank Number
1 Breast 3524 1 Lung 1376
2 Colorectal 2032 2 Colorectal 894
3 Lung 1637 3 Breast 596
9 Liver 445 4 Liver 401
10 Stomach 430 5 Pancreas 274
12 Pancreas 284 6 Stomach 245
Symptoms and signs
� Symptom– Nil– Epigastric pain, radiation to back, weight loss– Acute pancreatitis– Vomiting if obstruction– Jaundice if CBD compression– Abdominal distension if peritoneal metastases– Bone pain if metastases
� Sign – Nil– Distended gallbladder (Courvoisier’s sign)– Epigastric mass– Ascites

Risk factors� Age – increasing age� Gender - male� Family history� Genetic diseases� Smoking – increased with year of smoking� Dietary factors – high calorie, high-fat� History of pancreatitis� Chronic pancreatitis� DM, recent onset of DM� Pancreatic cystic lesions
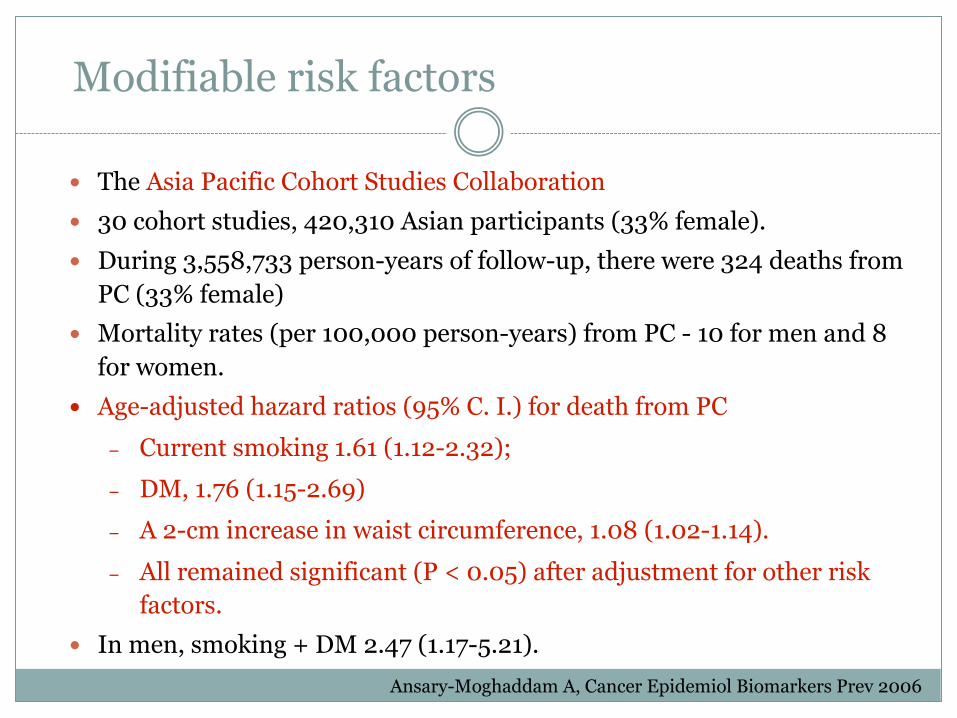
Modifiable risk factors
� The Asia Pacific Cohort Studies Collaboration� 30 cohort studies, 420,310 Asian participants (33% female).� During 3,558,733 person-years of follow-up, there were 324 deaths from
PC (33% female)� Mortality rates (per 100,000 person-years) from PC - 10 for men and 8
for women. � Age-adjusted hazard ratios (95% C. I.) for death from PC
– Current smoking 1.61 (1.12-2.32); – DM, 1.76 (1.15-2.69)– A 2-cm increase in waist circumference, 1.08 (1.02-1.14). – All remained significant (P < 0.05) after adjustment for other risk
factors. � In men, smoking + DM 2.47 (1.17-5.21).
Ansary-Moghaddam A, Cancer Epidemiol Biomarkers Prev 2006

Obesity and Pancreatic CA
� The Pancreatic Cancer Cohort Consortium (PanScan)� A nested case-control study design � 2170 cases and 2209 control subjects � BMI classified to: underweight <18.5; normal weight ≥18.5 - 24.9;
overweight, ≥25.0 - 29.9; obese ≥ 30.0-34.9; and severely obese ≥ 35.0. � Increased BMI – increased PC risk
– adjusted OR for the highest vs lowest BMI quartile, 1.33; 95% CI, 1.12-1.58; P trend <0.001).
– In men, OR 1.33 (95% CI, 1.04-1.69; P trend < 0.03)– in women, OR 1.34 (95% CI, 1.05-1.70; P trend = 0.01)
� Increased waist / hip ratio - increased PC risk– in women OR 1.87(95% CI, 1.31-2.69; P trend = 0.003) but less so in
men.Arslan AA, Arch Intern Med. 2010
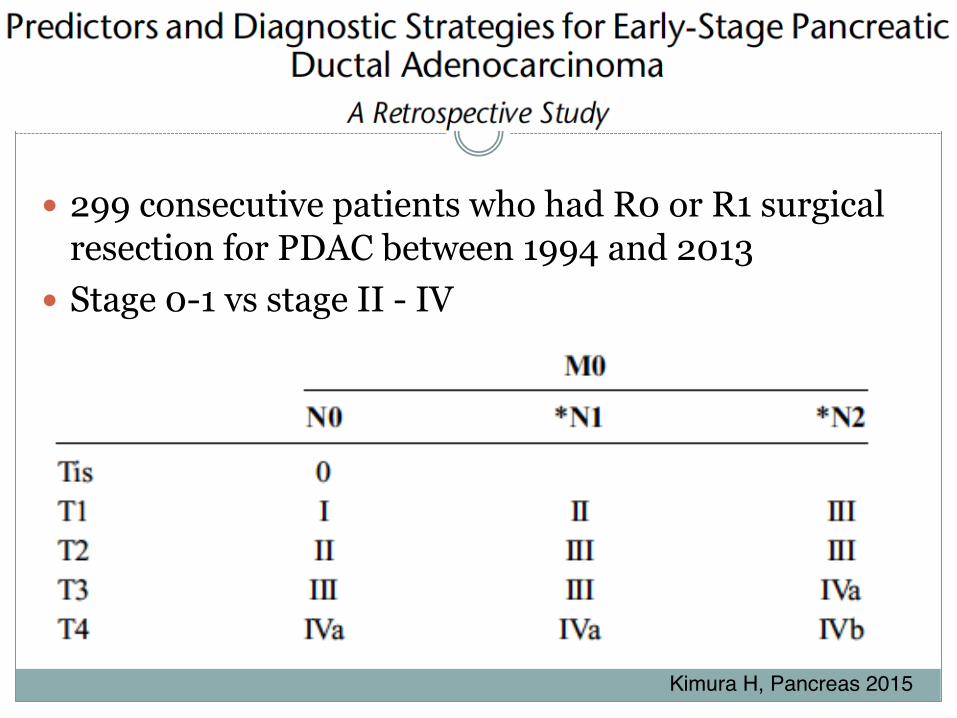
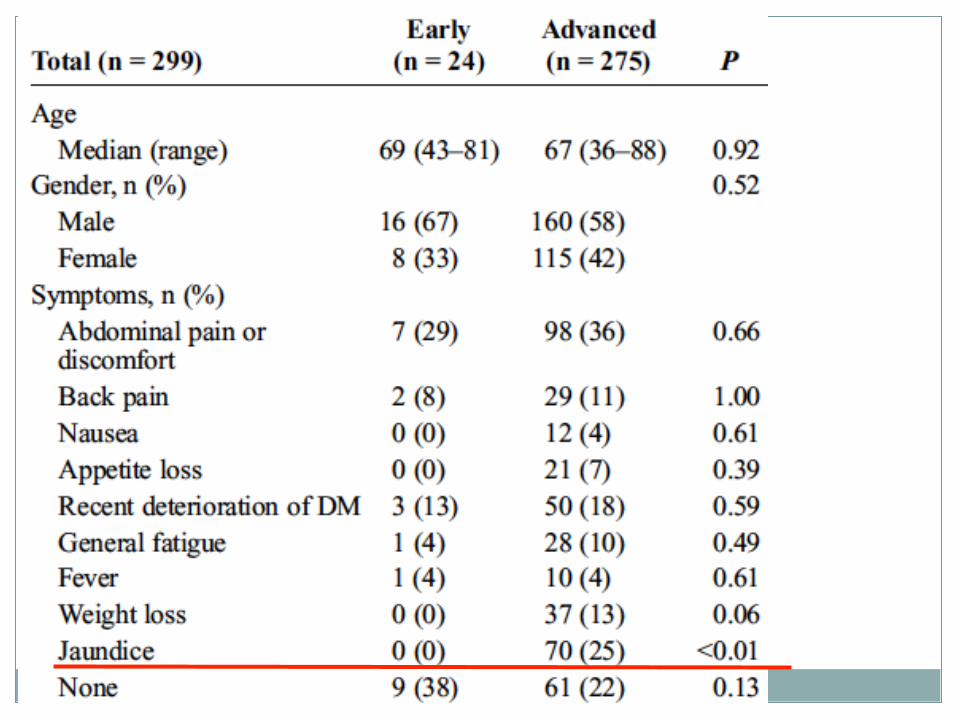
� 299 consecutive patients who had R0 or R1 surgical resection for PDAC between 1994 and 2013
� Stage 0-1 vs stage II - IV
Kimura H, Pancreas 2015

� 13131 patients with PC in National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) database
� Multiple linear regression models for age were generated, adjusting for patient ethnicity, gender, tumour location and neoplastic grades.
� Stage I vs stage IV cancers - on average 1.3 adjusted years younger ( p=0.001).
� Among patients without distant metastases, T1 stage vs T3 or T4 cancers - on average 1.06 and 1.19 adjusted years younger, respectively, (p=0.03 for both)
� Early detection is the keyYu J, Gut 2015
Early detection is important for curative treatment
� Detection methods - how to screen
� Screening of at risk groups
– Who to screen
– When to screen
Early detection is important for curative treatment
� Detection methods - how to screen
� Screening of at risk groups
– Who to screen
– When to screen
CA 19-9 (> 37U/ml)� Systemic review of 22 studies, 2283 patients with proven PC, the median
sensitivity 79 (70 - 90%), specificity is 82 (68 - 91%). PPV 72 (41 - 95) and
NPV 81 (65 – 98).
� Elevated in upper GI tract cancer, ovarian cancer, HCC, and in colorectal
cancer; in inflammatory conditions of the hepatobiliary system, and in
many benign conditions (eg, thyroid disease).
� 2006 American Society of Clinical Oncology (ASCO) and Pancreatic
Cancer Action Network did not recommend for screening of PC.
� Used for monitoring the effectiveness of therapy and recurrence.
Locker GY, J Clin Oncol 2006; Goonetilleke KS, Eur J Surg Oncol 2007
Raised CA 19-9 level
� 62,976 patients for health check, 501 (0.8%) elevated CA 19-9 level.
� 353 (70.5%) followed up for ≥6 months. � 10 (2.8%) were diagnosed with malignancies – Pancreas
(4), thyroid (4), Colon (1), Duodeum (1) � 97 patients (27.5%) with benign diseases and 246 patients
(69.7%) were deemed non-specific.� Conclusions: CA 19-9 should not be used as a screening
tool.
Kim BJ, Dig Liver Dis 2009
CA 19-9, CEA, CA 125
� CA 19-9: At 95% specificity, a sensitivity of 68% up to
1 year, and 53% up to 2 yrs before diagnosis of PC.
� CA 19-9 + CEA: Sensitivity 37%, Specificity 84%
� CA19-9 + CA125 improved sensitivity as CA125 was
elevated (>30 U/mL) in ~20% of CA19-9-negative
cases.
Chan A, Clin Cancer Res 2014; O’Brien DP, Clin Cancer Res 2015

Grote T, Curr Opin Gastroenterol 2007
Biomarkers and molecular diagnosis
Pancreatic imaging
Non-invasive tests� Ultrasound� Contrast CT scan� Contrast MRI / MRCP � PET scan � EUS - contrast study, elastographyInvasive tests � EUS guided fine needle aspiration (FNA), confocal
microendoscopy� ERCP + biopsy� Direct pancreatoscopy + biopsy
Ultrasound (US)
Pros� Simple and readily available� Look for mass lesion, biliary or pancreatic ductal
dilatation
Cons� Sensitivity: 75% to 89%, specificity 90% to 99%. � Accuracy 50-70%� Not sensitive nor accurate esp. small lesion or lesion at
the tail
Rickes S, Scand J Gastroenterol 2002; Conrad C, J Surg Oncol 2013
CT
Pros� Non-invasive� Sensitive and accurate
Cons� Contrast needed� Radiation exposure – not suitable for repeated
examination (screening)� Limited accuracy in small lesion� Could not differentiate mass-forming inflammation from
cancer
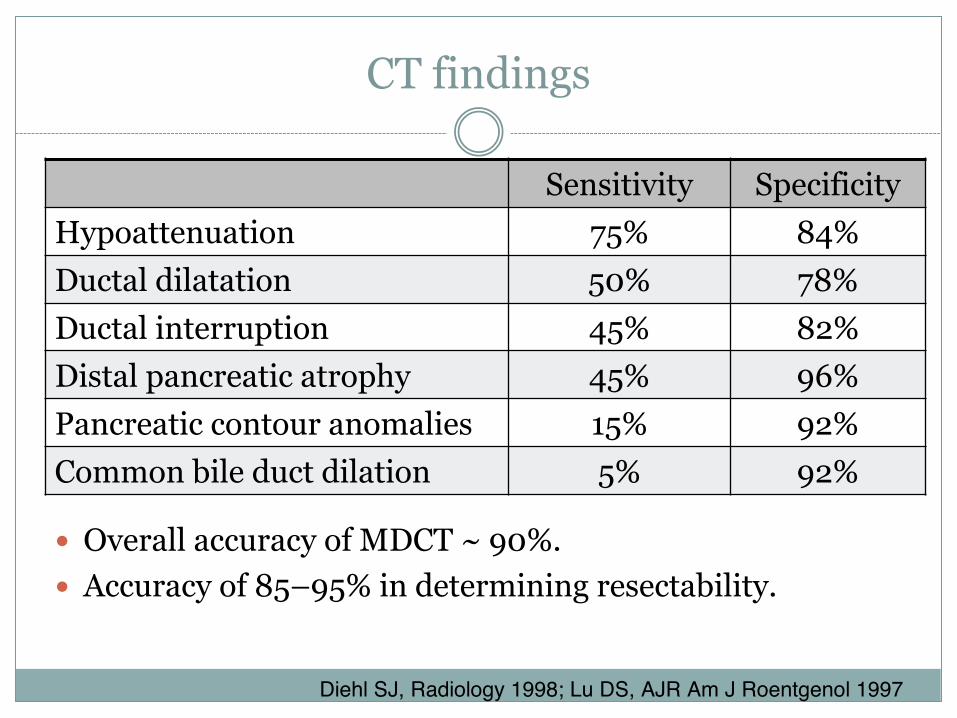
CT findings
� Overall accuracy of MDCT ~ 90%.� Accuracy of 85–95% in determining resectability.
Sensitivity SpecificityHypoattenuation 75% 84%Ductal dilatation 50% 78%Ductal interruption 45% 82%Distal pancreatic atrophy 45% 96%Pancreatic contour anomalies 15% 92%Common bile duct dilation 5% 92%
Diehl SJ, Radiology 1998; Lu DS, AJR Am J Roentgenol 1997

MRI
Pros� Non-invasive� No radiation exposure – suitable for repeated examination
(screening)� High sensitivity
Cons� Reduced accuracy in small lesion� Could not differentiate mass forming inflammation� T1-weighted images and use of dynamic gadolinium
enhancement (rarely renal toxicity)� Claustrophobia, metallic implant, cost
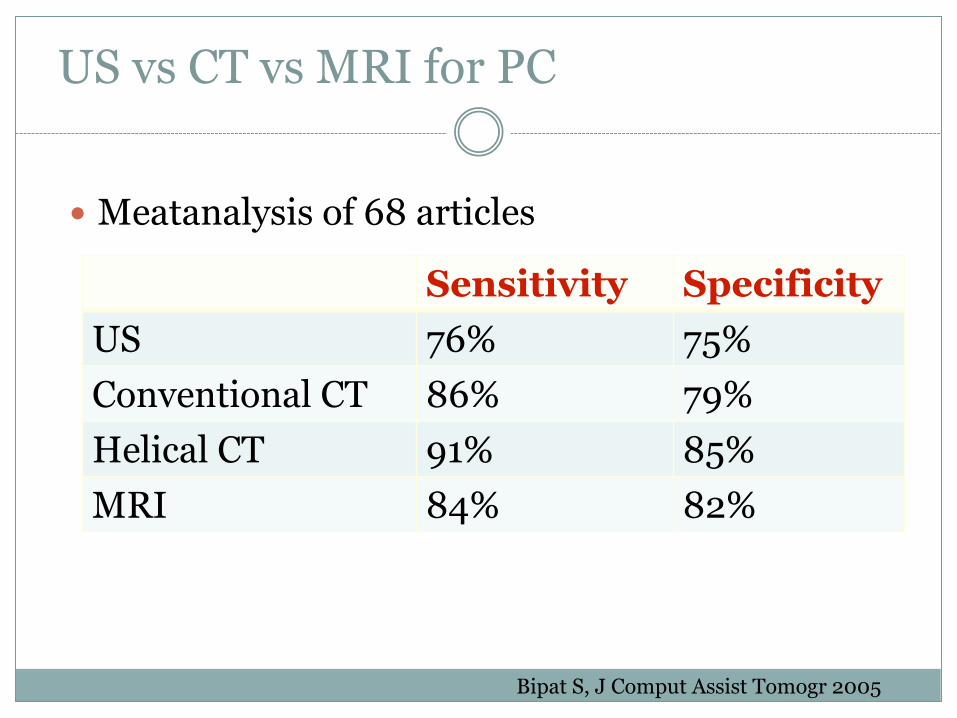
US vs CT vs MRI for PC
� Meatanalysis of 68 articles
Bipat S, J Comput Assist Tomogr 2005
Sensitivity SpecificityUS 76% 75%Conventional CT 86% 79%Helical CT 91% 85%MRI 84% 82%
PET
Pros� Differentiate between benign (chronic pancreatitis) and
malignant mass (carcinoma)� The sensitivity less dependent on lesion size.� In 387 studies, for detection of PC
– sensitivity and specificity for PET 94% and 90%,– sensitivity and specificity for CT 82% and 75%
� In 12 studies, differentiate benign from malignant: Sensitivity 85% - 100%, specificity 67% - 99%, accuracy 85% - 93%
Cons� Radiation exposure, cost
Delbeke D, J Hepatobiliary Pancreat Surg 2004
Gambhir SS, J Nucl Med 2001
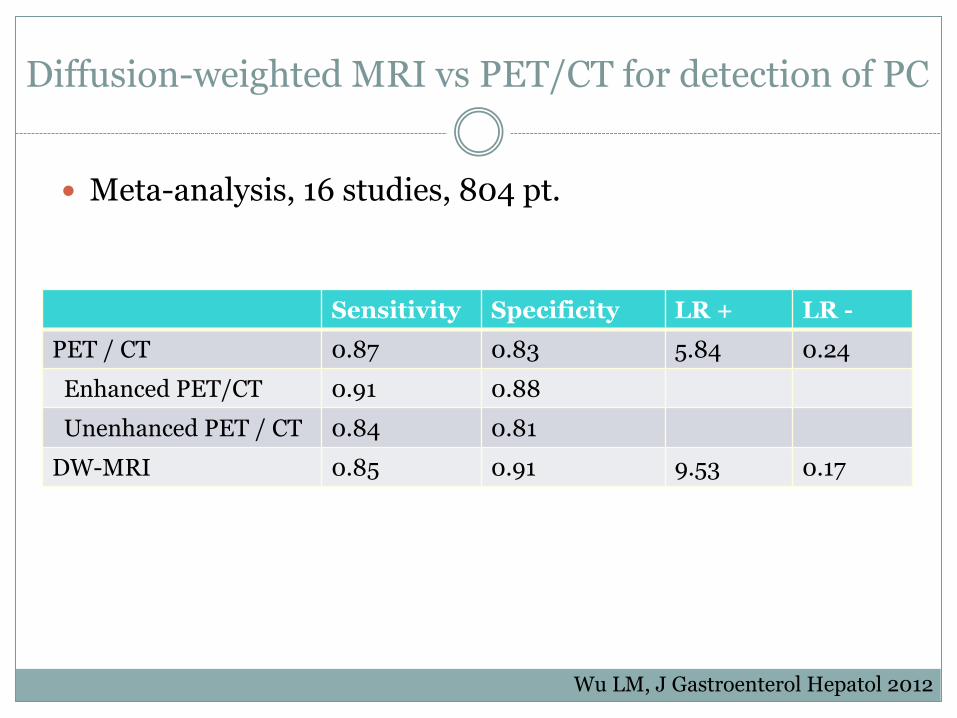
Diffusion-weighted MRI vs PET/CT for detection of PC
� Meta-analysis, 16 studies, 804 pt.
Sensitivity Specificity LR + LR -PET / CT 0.87 0.83 5.84 0.24
Enhanced PET/CT 0.91 0.88Unenhanced PET / CT 0.84 0.81
DW-MRI 0.85 0.91 9.53 0.17
Wu LM, J Gastroenterol Hepatol 2012
� Retrospective review� N=184, in which 60 PET/CT were -ve.� 56 had EUS-FNA or surgical pathology� Benign (18), Pre-malignant (24) and malignant (14)� PET/CT NPV 75% � Conclusion: A negative PET/CT does not exclude PC.
Pancreas 2011

ERCP
� Accuracy ~ 90%� Could obtain cytological diagnosis
� Invasive, radiation exposure, failure rate up to 10%
� Morbidity or mortality related to the procedure (8% and <1%)
� Not suitable for screening
Endoscopic ultrasound (EUS)
� Combined endoscopic and (internal) ultrasound examination in one
� Probe are close to internal organs
� Using higher frequency ultrasound probe - higher resolution
� More accurate in diagnosing pathologies that are close to GI tract - such as pancreas.
� Could obtain fine needle aspiration (FNA) and guided therapy
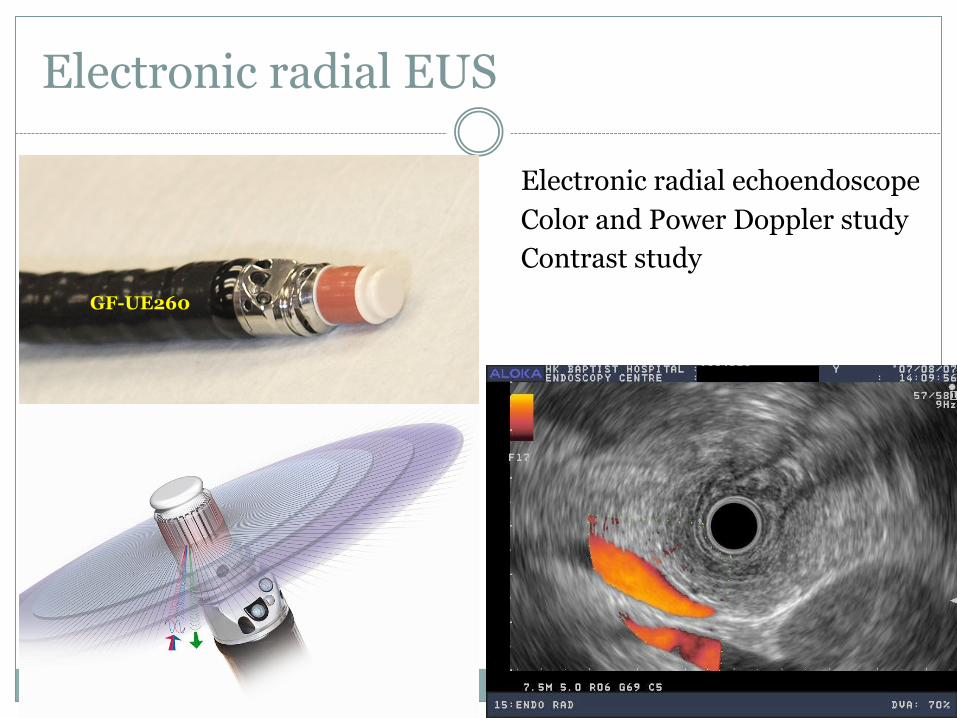
Electronic radial EUS
GF-UE260
Electronic radial echoendoscopeColor and Power Doppler studyContrast study
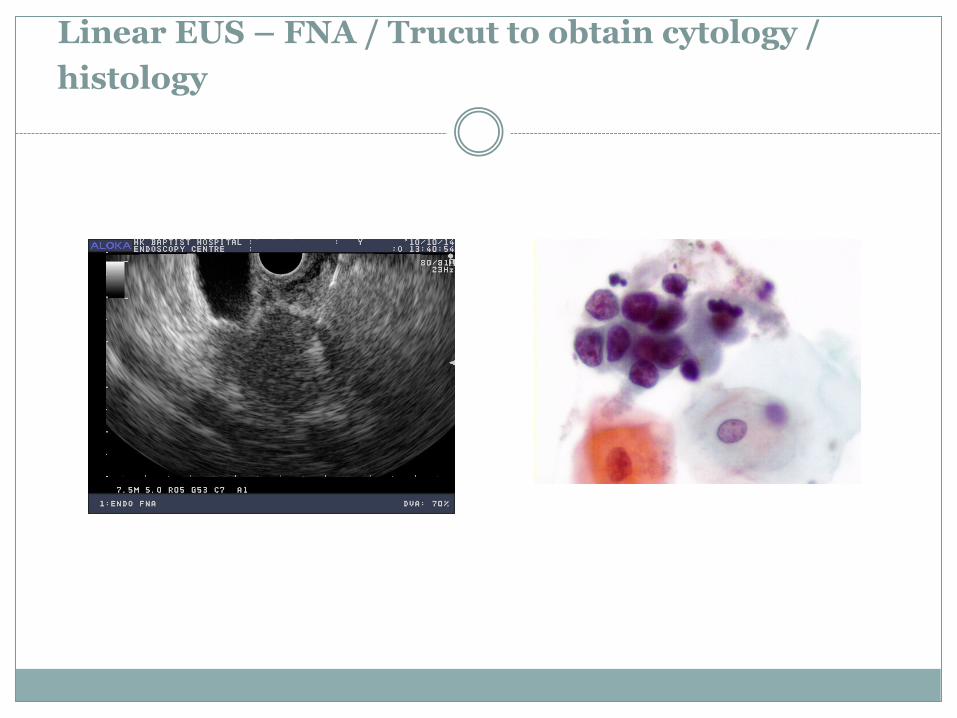
Linear EUS – FNA / Trucut to obtain cytology / histology

Detection of pancreatic tumour
Sensitivity compared with EUS� Tumour > 15mm, CT 100%, EUS 100%� Tumour ≤ 15mm, CT 67%, EUS 100%
� CT for tumour ≤ 2 cm, sensitivity 77%.
Legmann P, AJR Am J Roentgenol 1998
Bronstein YL, AJR Am J Roentgenol 2004
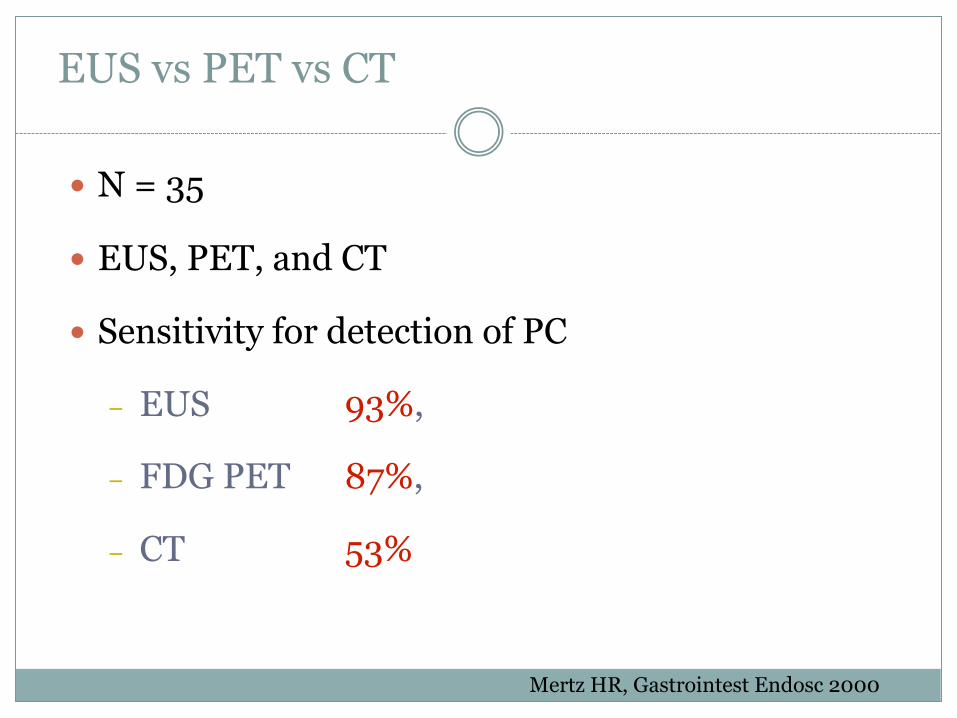
EUS vs PET vs CT
� N = 35
� EUS, PET, and CT
� Sensitivity for detection of PC
– EUS 93%,
– FDG PET 87%,
– CT 53%
Mertz HR, Gastrointest Endosc 2000
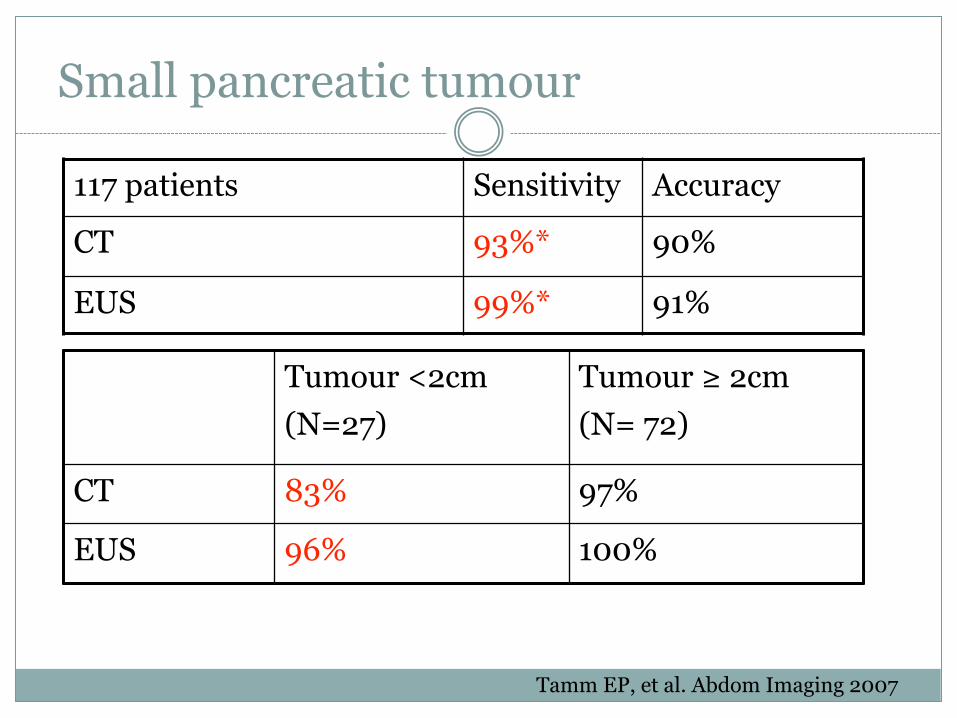
Small pancreatic tumour
117 patients Sensitivity Accuracy
CT 93%* 90%
EUS 99%* 91%
Tumour <2cm(N=27)
Tumour ≥ 2cm(N= 72)
CT 83% 97%
EUS 96% 100%
Tamm EP, et al. Abdom Imaging 2007

Normal EUS rule out pancreatic cancer
� Retrospective study� Clinical suspicion of pancreatic cancer but indeterminate noninvasive diagnostic
tests� 80 patients
– Elevated CA 19-9 without other definitive evidence of pancreatic cancer– Subtle abnormalities on CT of the pancreas– Unexplained abdominal pain and/or weight loss.
� FU >6 months 76 (95%) patients (mean FU 23.9 months).
Catazaro A, Gastrointest Endosc 2003
EUS +/- FNA in patient with enlarged pancreatic head in CT/MRI
� Retrospective analysis of a prospective database.� Patients (N=110):
– Incidental finding of enlarged head of pancreas (n=67)
– Dilated PD +/- dilated CBD (n=43). No obstructive jaundice. � Final diagnosis:
– Adenocarcinoma (n=7), IPMT (n=1), NET (n=1), tumor metastasis (n=1),
– benign cyst (n=3), chronic pancreatitis (n=32), normal (n=65) � EUS and EUS-FNA accuracy (99.1%), Sensitivity (88.8%),
specificity (100%), NPV (99%), PPV (100%).
Agarwal B, Gastrointest Endosc 2008
� Retrospective study of 213 pt, median follow up 19 months. � EUS identified 173 lesions� Final diangosis: adenocarcinoma (89), NET (14), mucinous
cystadenocarcinoma (1), solid pseudopapillary tumor (2), metastases (4), benign cyst (19), pseudocyst (9), abscess (4), chronic pancreatitis (32), and normal pancreas (39).
� EUS - FNA: accuracy 97.6%, sensitivity 96.6%, specificity 99.0%, NPV 96.2%, PPV 99.1%.
Pancreas 2009
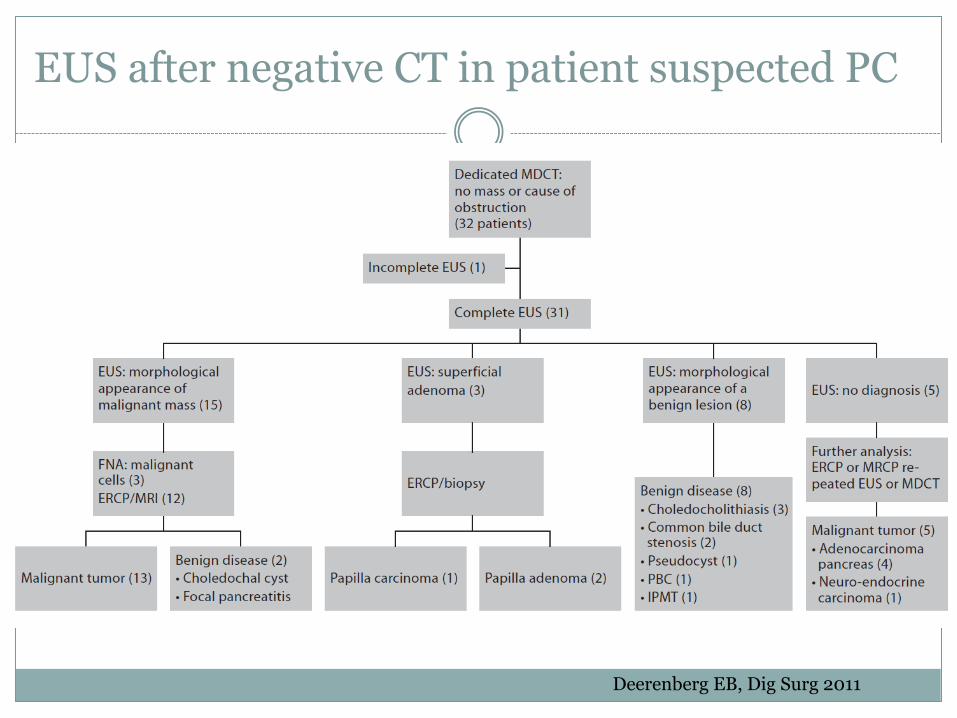
EUS after negative CT in patient suspected PC
Deerenberg EB, Dig Surg 2011
EUS after negative CT
� EUS sensitivity 74%, PPV 86%, NPV 63%
� 5 false -ve cases due to the presence of chronic pancreatitis and endoprosthesis.
Deerenberg EB, Dig Surg 2011
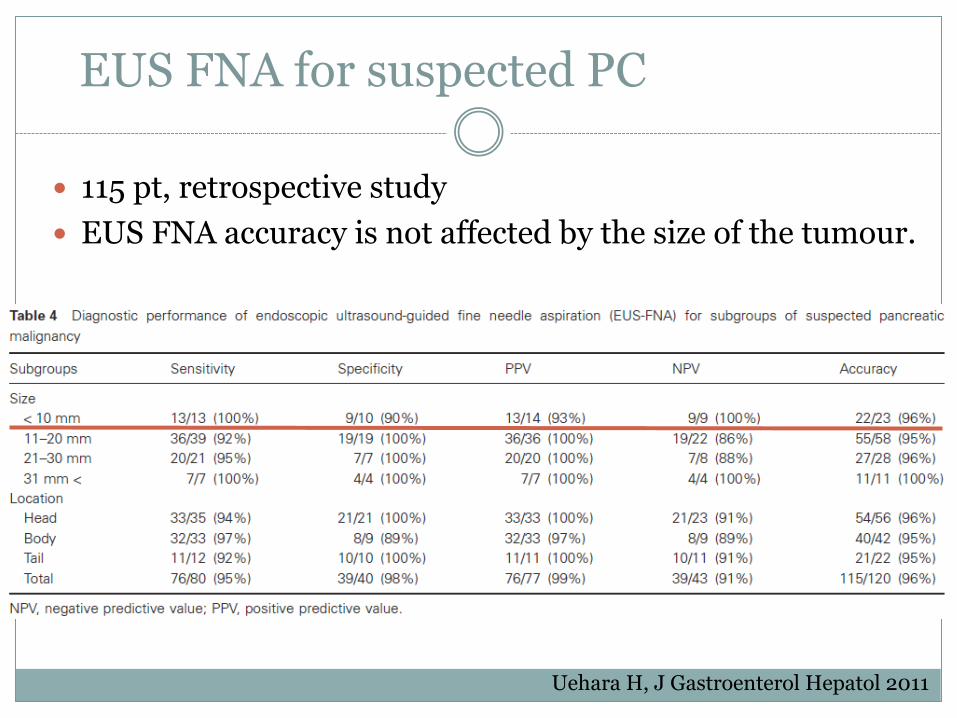
EUS FNA for suspected PC
� 115 pt, retrospective study� EUS FNA accuracy is not affected by the size of the tumour.
Uehara H, J Gastroenterol Hepatol 2011

Krishna NB, Pancreas 2011

EUS-FNA genetic and biomarker analysis
� FNA specimen for p53, k-ras, heat shock protein
27, DNA microsatellite loss, ribonucleotide
reductase M2 mRNA expression, deoxycytidine
kinase markers …
CT vs EUS in PNET
� Johns Hopkins review of pancreatic neuro-endocrine tumour (PNET) diagnosis.
� 217 patients (with 231 PNETs) studied, CT detected 84% of tumors (54.3% of insulinomas).
� Improved sensitivity with latest CT technology (P = 0.02).� CT was more likely to miss lesions <2 cm (P =0.005) and
insulinomas (P <0.0001).� In 56 patients who had both CT and EUS,
Sensitivity EUS vs CT (91.7% vs 63.3%; P =0.0002), For insulinomas (84.2% vs 31.6%; P = 0.001).
� EUS detected 20 of 22 CT-negative tumors (91%).
Khashab MA, Gastrointest Endosc 2011
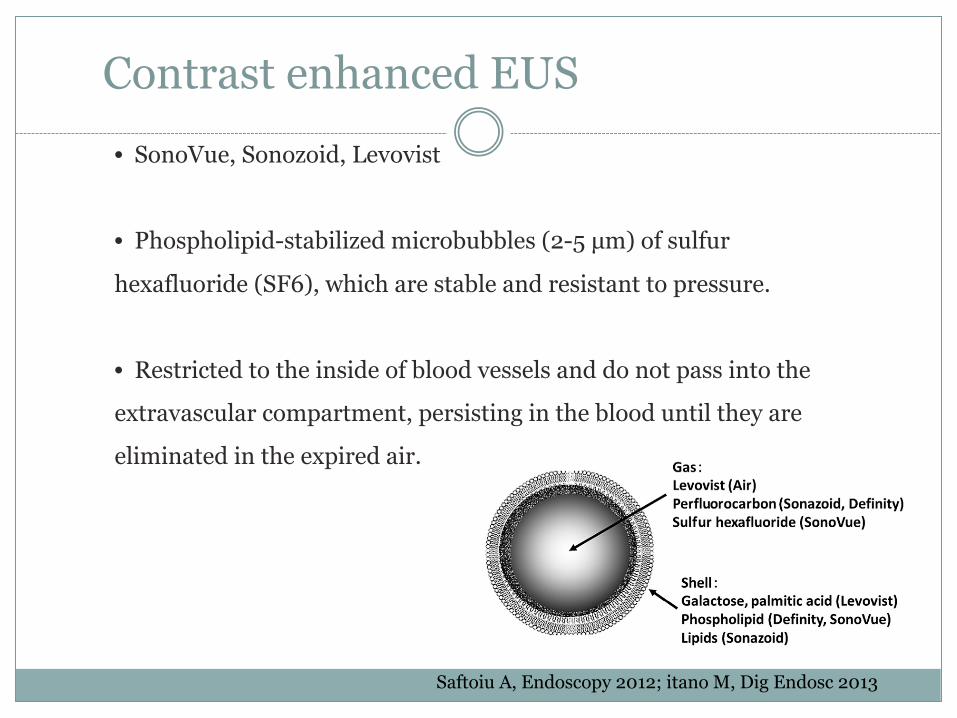
Contrast enhanced EUS
Saftoiu A, Endoscopy 2012; itano M, Dig Endosc 2013
• SonoVue, Sonozoid, Levovist
• Phospholipid-stabilized microbubbles (2-5 µm) of sulfur
hexafluoride (SF6), which are stable and resistant to pressure.
• Restricted to the inside of blood vessels and do not pass into the
extravascular compartment, persisting in the blood until they are
eliminated in the expired air.
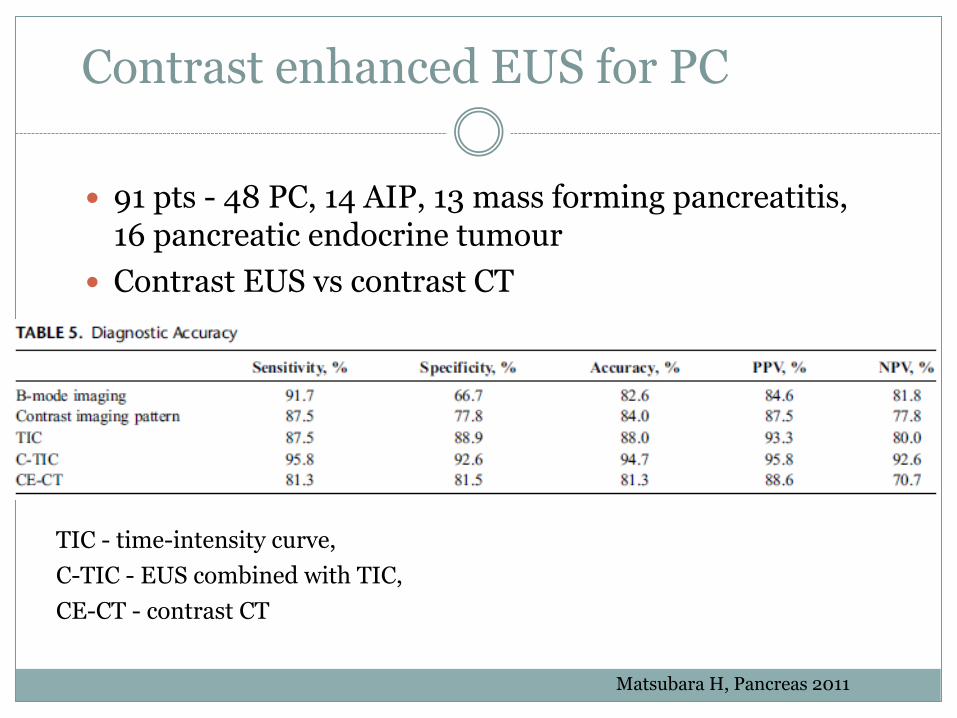
Contrast enhanced EUS for PC
� 91 pts - 48 PC, 14 AIP, 13 mass forming pancreatitis, 16 pancreatic endocrine tumour
� Contrast EUS vs contrast CT
TIC - time-intensity curve, C-TIC - EUS combined with TIC, CE-CT - contrast CT
Matsubara H, Pancreas 2011
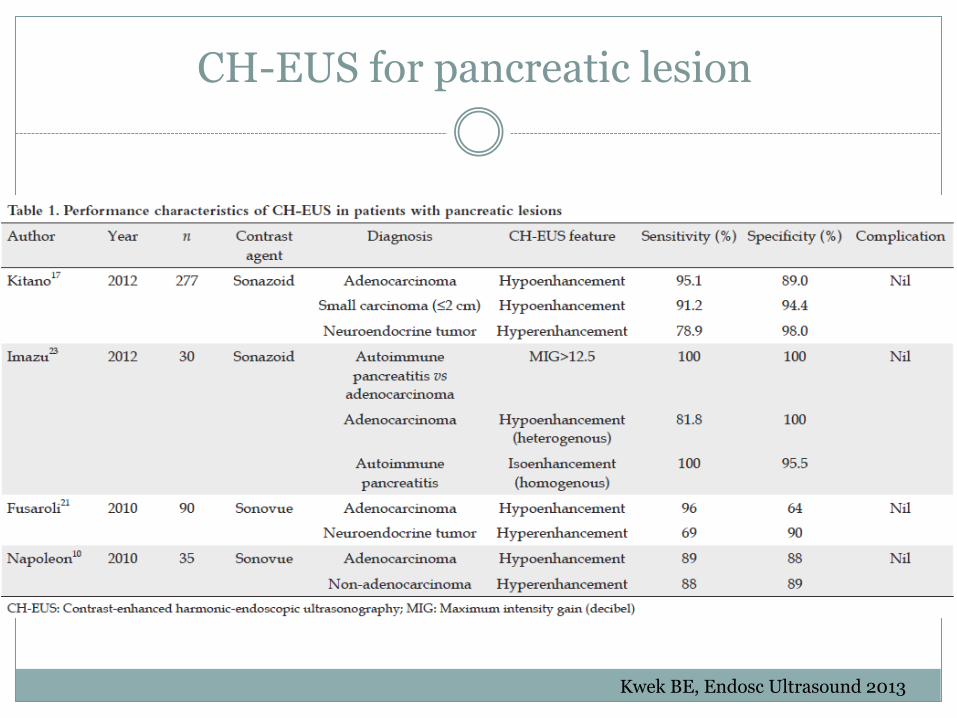
CH-EUS for pancreatic lesion
Kwek BE, Endosc Ultrasound 2013
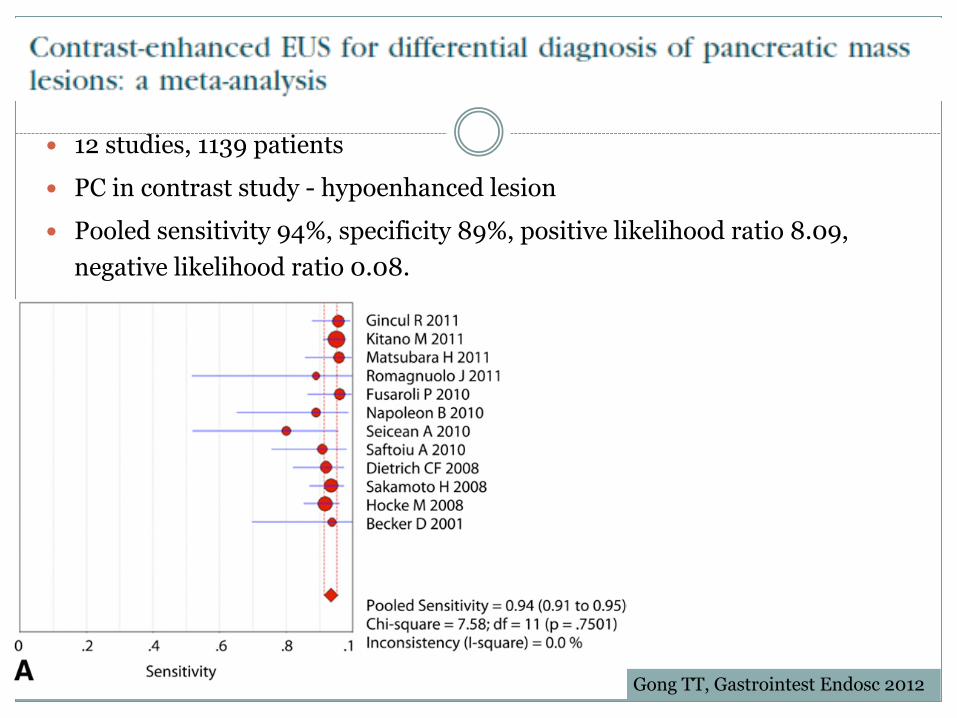
� 12 studies, 1139 patients� PC in contrast study - hypoenhanced lesion � Pooled sensitivity 94%, specificity 89%, positive likelihood ratio 8.09,
negative likelihood ratio 0.08.
Gong TT, Gastrointest Endosc 2012
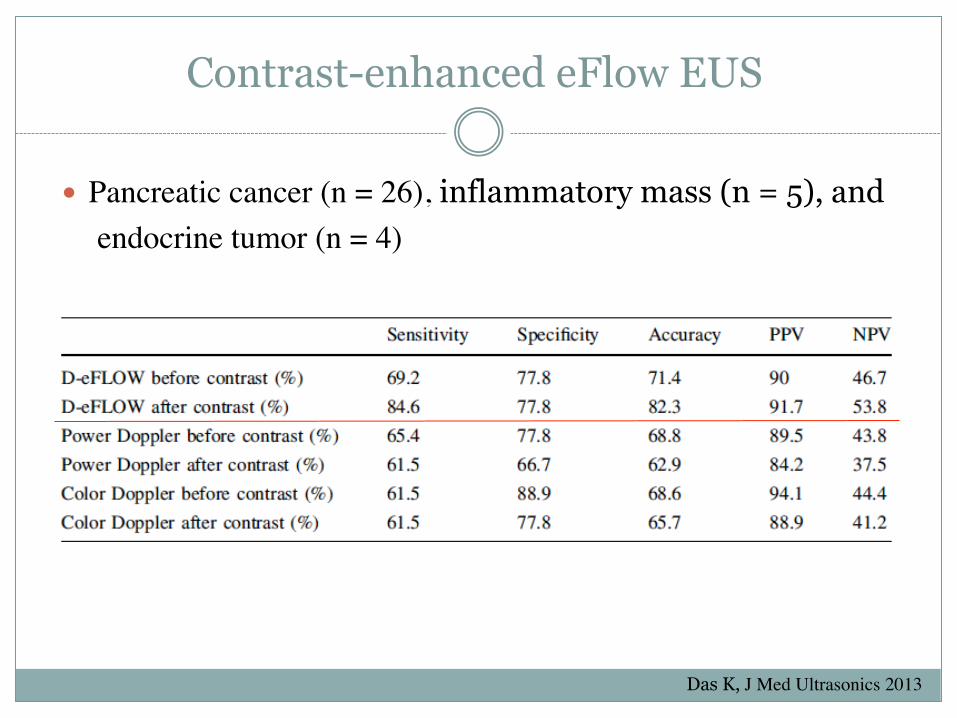
Contrast-enhanced eFlow EUS
� Pancreatic cancer (n = 26), inflammatory mass (n = 5), andendocrine tumor (n = 4)
Das K, J Med Ultrasonics 2013
Contrast-enhanced harmonic EUS
� The second harmonic component from microbubbles is much higher than that from the tissue
� CE-hEUS selectively depicts the second harmonic component, which results in selective visualization of microbubbles and can visualize fine vessels with slow flow as well as parenchymal perfusion.
� Measuring the time-course of echogenicity intensity (time–intensity curve, peak intensity, maximal intensity gain), vascularity can be quantitatively analyzed.
Kitano M, Dig Endosc 2013
Early detection is important for curative treatment
� Detection methods - how to screen
� Screening of at risk groups
– Who to screen
– When to screen

Who to screen
No role for population screening

Family history and PC
Shirts BH, Clin Gastroenterol Hepatol 2010
Review of Utah Cancer Registry and Population Database
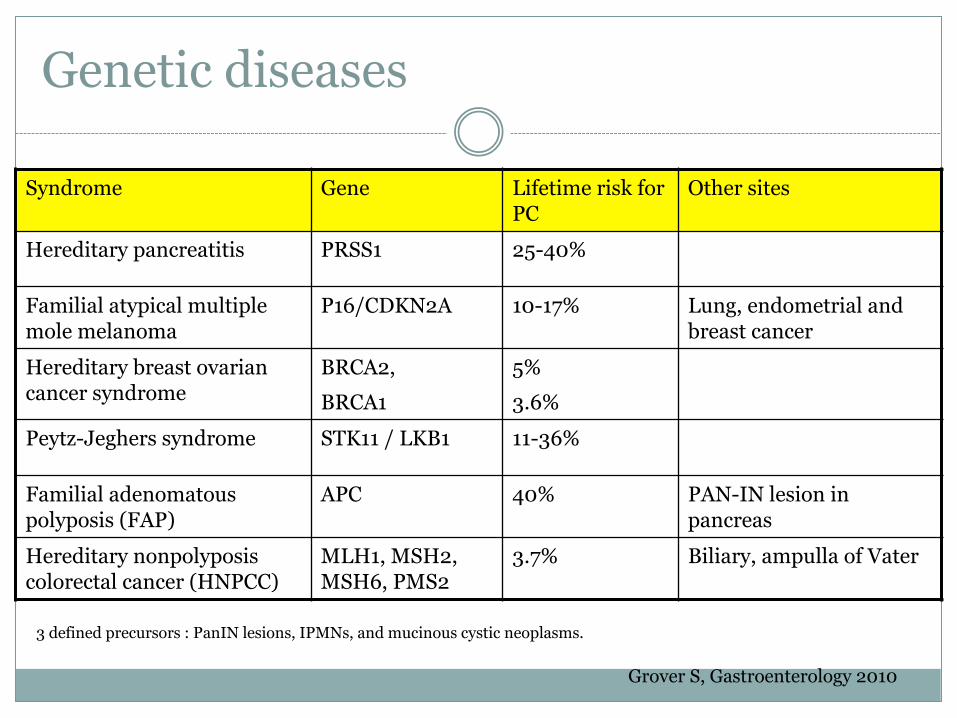
Genetic diseases
Grover S, Gastroenterology 2010
Syndrome Gene Lifetime risk for PC
Other sites
Hereditary pancreatitis PRSS1 25-40%
Familial atypical multiple mole melanoma
P16/CDKN2A 10-17% Lung, endometrial and breast cancer
Hereditary breast ovarian cancer syndrome
BRCA2, BRCA1
5%3.6%
Peytz-Jeghers syndrome STK11 / LKB1 11-36%
Familial adenomatous polyposis (FAP)
APC 40% PAN-IN lesion in pancreas
Hereditary nonpolyposis colorectal cancer (HNPCC)
MLH1, MSH2, MSH6, PMS2
3.7% Biliary, ampulla of Vater
3 defined precursors : PanIN lesions, IPMNs, and mucinous cystic neoplasms.
Brand RE, GUT 2007

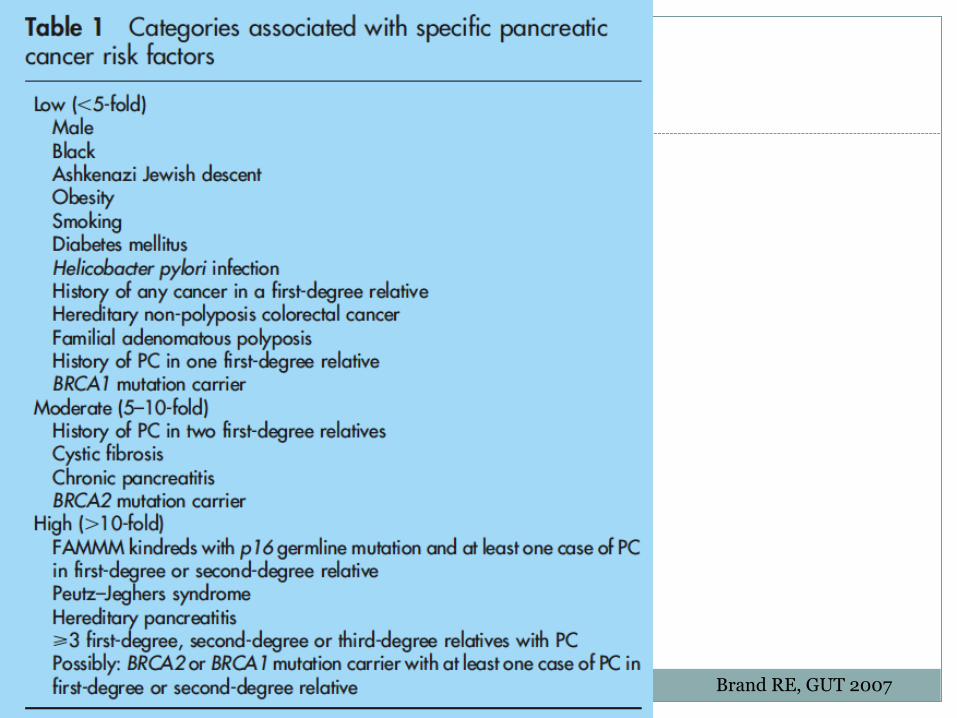
Screening
Brand RE, GUT 2007

Screening
Grover S, Gastroenterology 2010; Langer P, Gut 2009
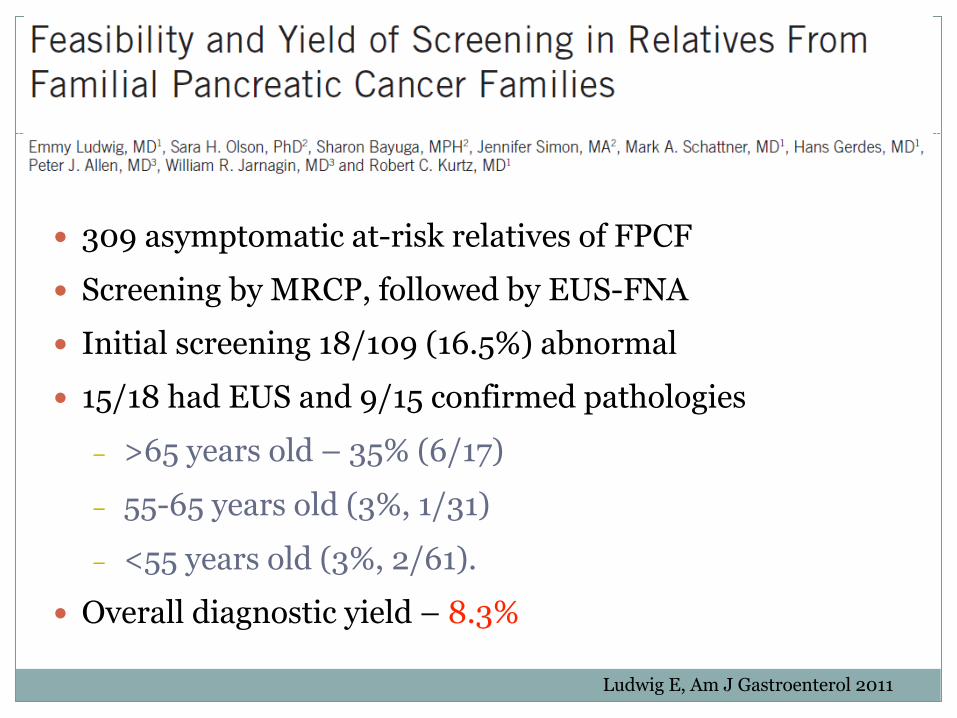
� 309 asymptomatic at-risk relatives of FPCF� Screening by MRCP, followed by EUS-FNA� Initial screening 18/109 (16.5%) abnormal� 15/18 had EUS and 9/15 confirmed pathologies
– >65 years old – 35% (6/17)– 55-65 years old (3%, 1/31)– <55 years old (3%, 2/61).
� Overall diagnostic yield – 8.3%
Ludwig E, Am J Gastroenterol 2011

� Multicentre prospective study. � N = 139 asymptomatic HRI (>10-fold increased risk)� Screening by EUS and MRI. � Clinically relevant lesions - solid lesions, main duct
intraductal papillary mucinous neoplasms (IPMN) and cysts ≥10 mm.
Harinck F, Gut 2015
Screening for high risk individuals
� 2 solid lesions (mean size 9 mm) and 9 cysts ≥10 mm (mean size 17 mm) were detected in 9 HRI (6%).
� Both solid lesions were detected by EUS only -stage I PC and a multifocal pancreatic intraepithelial neoplasia 2.
� 9 cysts ≥10 mm, 6 were detected by both EUS AND MRI, 3 by MRI only.
� Agreement between two methods – 55%
Harinck F, Gut 2015
DM and PC
� T2DM is associated with obesity, insulin resistance,
hyperinsulinemia, oxidative stress, and proinflammatory
signaling, all of which may contribute to the development of
PC.
� Pancreatic steatosis, a condition associated with obesity and
metabolic syndrome and characterized by fatty infiltration of
the pancreas, can cause lipotoxicity to the pancreas and plays
an important role in the development of T2DM, pancreatic
exocrine dysfunction, acute pancreatitis, and PC
Giovannucci E, Gastroenterology 2007, Greer JB, Curr Opin Pharmacol 2009, Smits MM, Nat Rev Gastroenterol Hepatol 2011, Giacca A, Am J Physiol Endocrinol Metab 2011.
DM before diagnosis of PC
� Retrospective review of PC case with CT result and DM state.
� N = 30 patients.
� CT scans done ≥ 6 months showed either a normal pancreas (N = 20) or a resectable mass (N = 6).
� Mean interval between onset of DM and diagnosis of PC – 10 (5–29) months
� At onset of diabetes, pancreatic cancers are generally resectable.
� Pancreatic cancer is frequently undetectable or resectable on CT scans done ≥ 6 months prior to clinical diagnosis.
Pelaez-Luna M, Am J Gastroenterol 2007
DM and PC
� PC (N=736) vs control (N=1875).
� 60 months before the diagnosis of PC, more PC cases had DM vs control. (40.2% vs 19.2%, P < 0.0001).
� Proportion of DM: month 60 to 48 (P = 0.76); 48 to 36 (P = 0.06), 36 to 24 (P = 0.04), 24 to 12 (P < 0.001), and 12 to 0 (P < 0.001)
� New onset of DM vs controls (52.3% vs 23.6%, P < 0.0001).
� Conclusions: Diabetes has a high (40%) prevalence in pancreatic cancer and frequently is new onset.
Chari ST, Gastroenterology 2008
PC with early onset of DM
� 512 newly diagnosed PC and 933 controls
� DM was more prevalent (47% vs 7%; P < 0.001) and
predominantly of new onset (<2-year duration) (74% vs
53%; P = 0.002) in PC patients.
� After Whipple’s OT, DM resolved in 17 of 30 patients
(57%) with new onset DM; unchanged in patients with
long-standing DM (n = 11) (P = 0.009).
Pannala R, Gastroenterology 2008
DM and PC
� Population-based cohort study using Taiwan National Health insurance Database
� 49803 DM patients aged ≥20 years vs 199212 control� Risk of PC
– DM (<2y) - 27.81 vs 6.96 /10000 person-yrs – Age 40-64, HR 5.22; ≥65, HR 7.59– Chronic pancreatitis, HR 19.40, – GS, HR 2.56,– HCV infection, HR 3.08– DM + Chronic pancreatitis, HR 33.52.– Duration of DM, anti-DM drug - not significant
Liao KF, J Gastroenterol Hepatol 2012
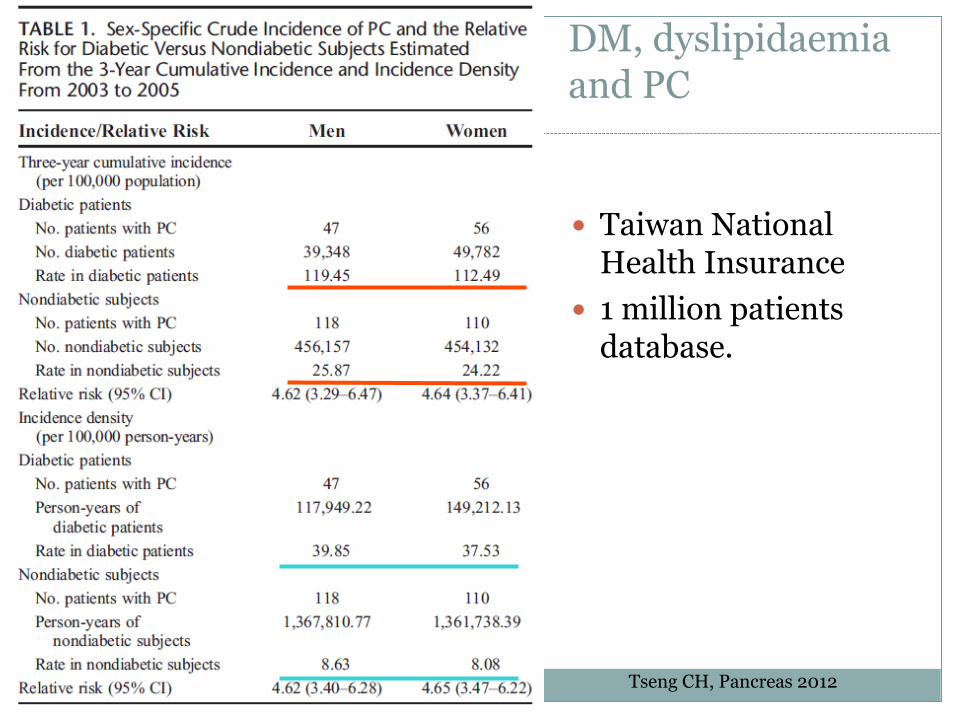
DM, dyslipidaemia and PC
� Taiwan National Health Insurance
� 1 million patients database.
Tseng CH, Pancreas 2012
DM, dyslipidaemia and PC
� Taiwan study - 0.2% of patients with new-onset DM and dyslipidaemia developed PC during 3 years period.
� Rochester study - 1% of DM patients > 50 years old developed PC within 3 years
Larsson SC, Am J Clin Nutr 2006; Tseng CH, Pancreas 2012
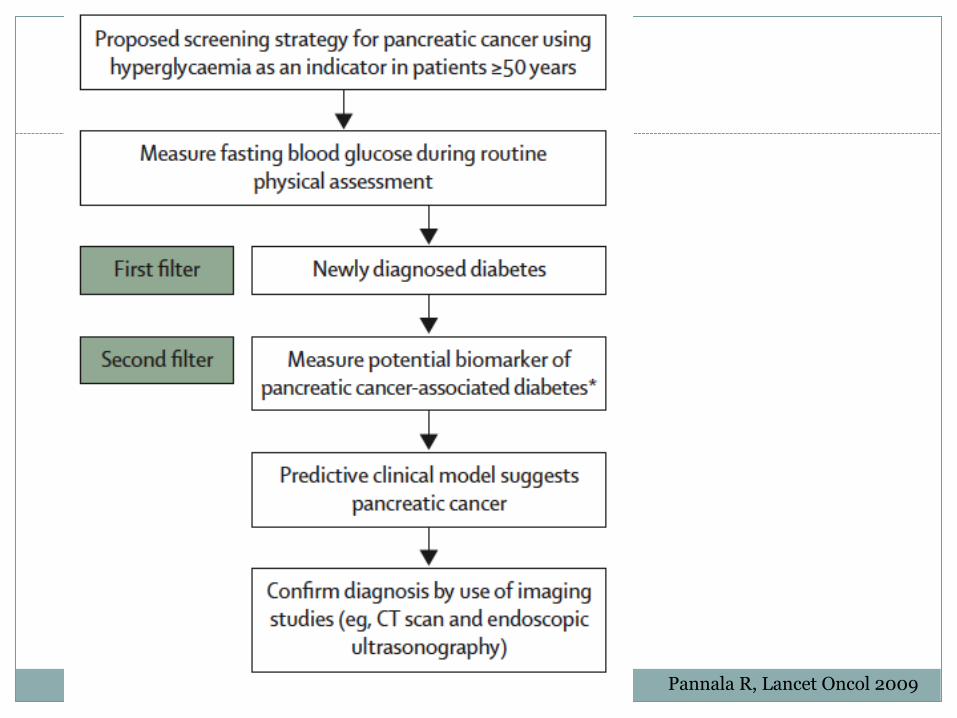
Pannala R, Lancet Oncol 2009
Screening of PC in new onset DM patient?
� Retrospective review� 151 case (New-onset of DM + PC) vs 302 control (New-onset of
DM without PC)� PC group:
– older (≥65), – weight loss (>2kg), – lower BMI (<25), – family history of PC (3.3% vs 0.7%, p=0.044), – less family history of DM (13.9% vs 37.4%, p,0.001)
� 5 features together - sen 80.8%, spec 67.6%, PPV 2.5%, NPV 99.7% of PC.
Lee JH, J Clin Gastroenterol 2012
� N = 115 T2DM, screening with CA 19-9 and US abdomen, if suspicious, also CT
� CA 19-9 elevation in 10 patients but none had PC.� 3 PC was found. USG detected 2 and CT detected all 3. � The value of the Standardized Incidence Ratio for
pancreatic cancer in new-onset type-2 diabetic patients was 198.6 (95% CI . 6.25e46.9).
Illes D, Pancreatology 2016
Incidental pancreatic cystic lesions (IPCL)
� Pancreatic cystic incidentalomas
� defined as asymptomatic cystic pancreatic
lesions that are diagnosed on abdominal
imaging performed for other indications.
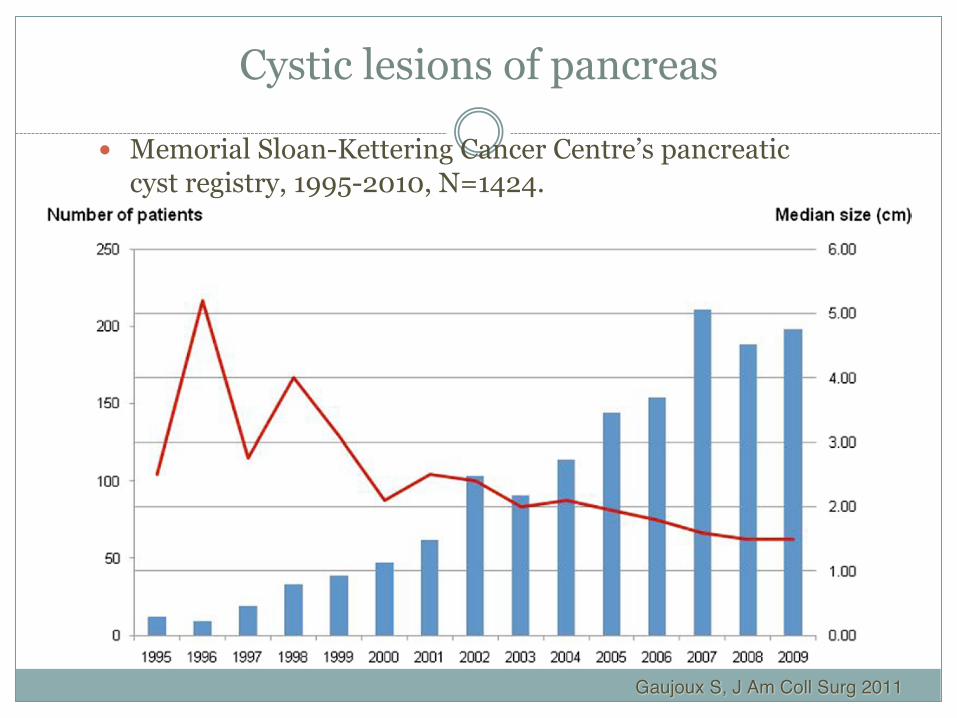
Cystic lesions of pancreas
� Memorial Sloan-Kettering Cancer Centre’s pancreatic cyst registry, 1995-2010, N=1424.
Gaujoux S, J Am Coll Surg 2011
Pancreatic cystic lesions
ªA Japanese autopsy study, up to 24.3% had pancreatic cystic lesion (186 cysts in 73 of 300 cases),
ªNormal epithelium (47.5%), papillary hyperplasia without atypia (32.8%), atypical hyperplasia (16.4%), carcinoma in situ (3.4%), invasive carcinoma (0%).
Kimura W, Int J Pancreatol 1995
ªFor patient with a pancreatic cyst, the chance of having a pancreatic cancer is 22.5 x higher that general population.
Tada M, Clin Gastro and Hepatol 2006
IPCL and pancreatic cancer (PC)
� Retrospective review of 10 years CT and MRI findings - cyst and no-cyst cohorts.
� Cyst cohort vs three-to-one matched no-cyst cohort by age decade, imaging modality, and year of initial study.
� Cyst cohort (n=2034) and no-cyst cohort (n=6018), Mean ages were 69.9 and 69.3 years (P =NS).
� Patients with pancreatic cancer diagnosed within 5 years before initial CT or MR were excluded.
� Adenocarcinomas diagnosed 6 months or longer after initial CT or MR examination were considered incident.
Chernyak V, Radiology 2015
� 38 (1.9%) in cyst cohort and 34 (0.6%) in no-cyst cohort developed pancreatic neoplasm (P<.0001). Incident adenocarcinoma was diagnosed in 12 (0.6%) in cyst cohort and in 11 (0.2%) in no-cyst cohort (P = .003).
� Ten year cumulative incidences of ductal adenocarcinoma were 1.5% in cyst cohort and and 0.6% in non-cyst cohort.
� The incidence rates of ductal adenocarcinoma were 1.8 and 0.6 per 1000 person-years in the cyst and no-cyst cohorts (P = .004).
� IPCL had a hazard ratio of 3.0 for adenocarcinoma, adjusted for age, sex, and race.
IPCL and pancreatic cancer (PC)
Chernyak V, Radiology 2015
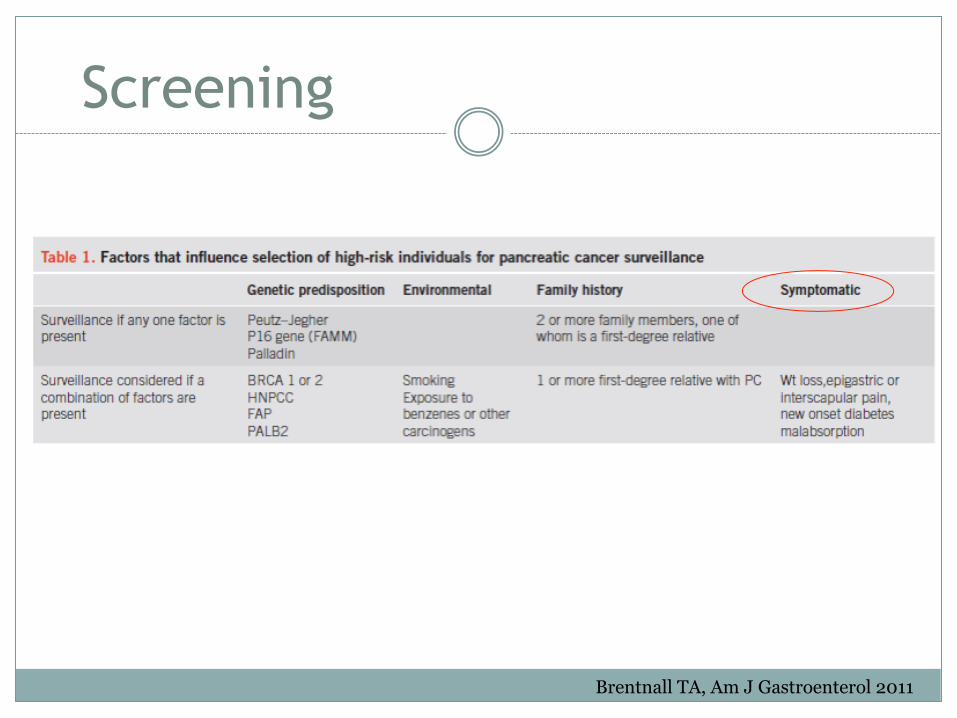
Brentnall TA, Am J Gastroenterol 2011
Screening
Early detection is important for curative treatment
� Detection methods - how to screen
� Screening of at risk groups
– Who to screen
– When to screen
When to screen
� Reaching adulthood in high risk genetically predisposed patients
� Early onset of DM, pancreatic cyst
� Patients with persistent, unresolved upper GI symptoms – opportunistic screening
Screening schedule
� 253 individual at risk (IAR) from familial pancreatic cancer (FPC)
� Significant lesions - PDAC, pancreatic intraepithelial neoplasia (PanIN) 3 lesions, high-grade IPMN
� Result: rarely found significant and potentially relevant pancreatic lesions < 50 years.
� MRI-based screening supplemented by EUS at baseline and every 3rd year or when changes in MRI occur
� Screening intervals of 24 months for an unremarkable pancreas at baseline imaging.
Bartsch DK, Gut 2016
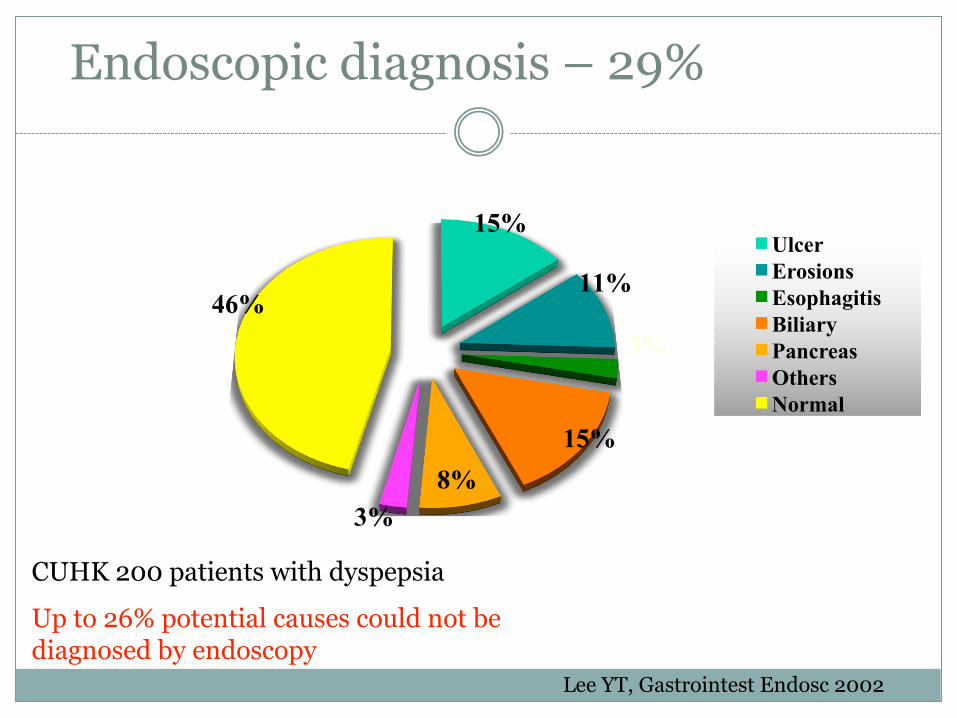
UlcerErosionsEsophagitisBiliaryPancreasOthersNormal
15%
11%
3%
15%8%
3%
46%
Endoscopic diagnosis – 29%
CUHK 200 patients with dyspepsia
Up to 26% potential causes could not be diagnosed by endoscopy
Lee YT, Gastrointest Endosc 2002
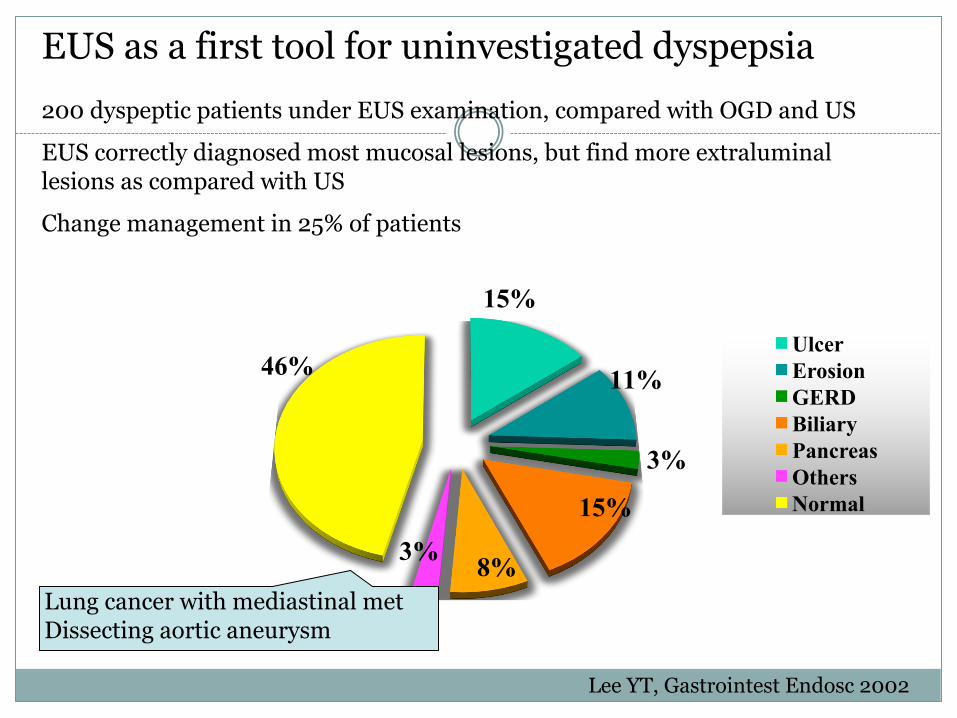
UlcerErosionGERDBiliaryPancreasOthersNormal
15%
11%
3%
15%
8%3%
46%
EUS as a first tool for uninvestigated dyspepsia200 dyspeptic patients under EUS examination, compared with OGD and US
EUS correctly diagnosed most mucosal lesions, but find more extraluminal lesions as compared with US
Change management in 25% of patients
Lung cancer with mediastinal metDissecting aortic aneurysm
Lee YT, Gastrointest Endosc 2002
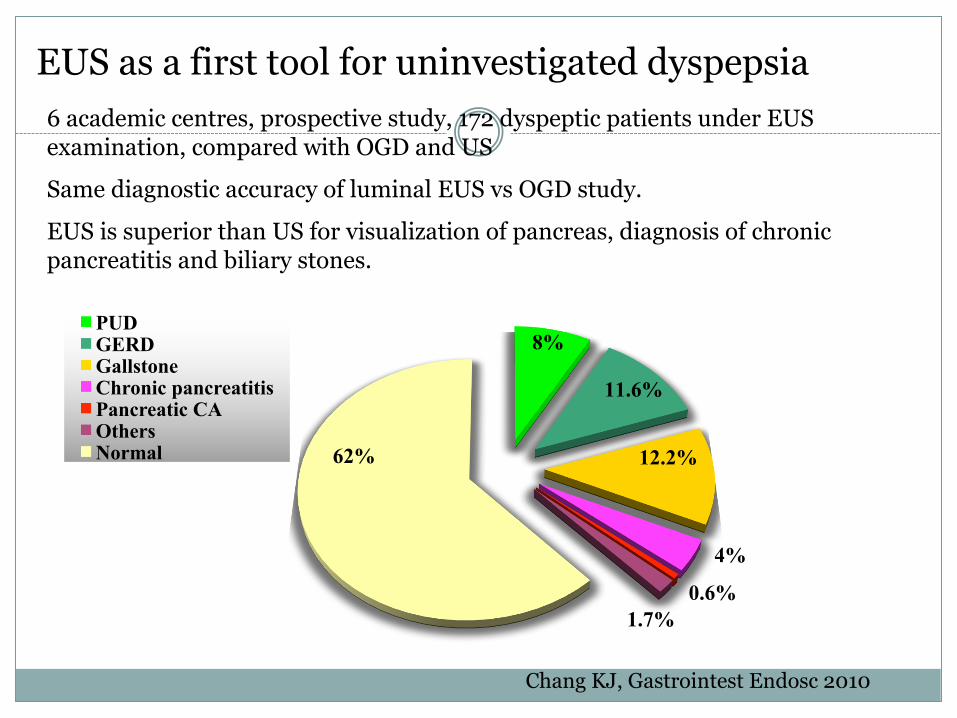
PUDGERDGallstoneChronic pancreatitisPancreatic CAOthersNormal
8%
11.6%
12.2%
4%
1.7%
62%
EUS as a first tool for uninvestigated dyspepsia6 academic centres, prospective study, 172 dyspeptic patients under EUS examination, compared with OGD and US
Same diagnostic accuracy of luminal EUS vs OGD study.
EUS is superior than US for visualization of pancreas, diagnosis of chronic pancreatitis and biliary stones.
Chang KJ, Gastrointest Endosc 2010
0.6%
Conclusion
� Pancreatic cancer carries high mortality
� Screening for at risk groups may detect early cancer
and improve survival.
� Careful selection of screening tools is important