Dr A. Artal Hospital Universitario Miguel Servet Zaragoza · Innovación terapéutica en cáncer de...
43
Innovación terapéutica en cáncer de pulmón Dr A. Artal Hospital Universitario Miguel Servet Zaragoza
-
Upload
duongthuan -
Category
Documents
-
view
218 -
download
0
Transcript of Dr A. Artal Hospital Universitario Miguel Servet Zaragoza · Innovación terapéutica en cáncer de...
Innovación terapéutica en cáncer de pulmón
Dr A. Artal
Hospital Universitario Miguel Servet
Zaragoza

INMUNOTERAPIA
NINTEDANIB

INMUNOTERAPIA
NINTEDANIB

Study Intervention Target PFS, months OS, months Primary
endpoint
ESCAPE1
(n=926)
CB/PTX/placebo CB/PTX/sorafenib
VEGFR-2, -3, PDGFR-ß, Flt-3,
b-RAF, c-kit
5.4 4.6
HR: 0.99 (0.84–1.16)
10.6 10.7
HR: 1.15 (0.94–1.41) OS
NExUS2
(n=772)
CIS/GEM/placebo CIS/GEM/sorafenib
5.5 6.0
HR: 0.83 (0.71–0.97)
12.5 12.4
HR: 0.98 (0.83–1.16) OS
ZEAL3
(n=534)
Pemetrexed/placebo Pemetrexed/vandetanib
VEGFR, EGFR, RET
2.8 4.1
HR: 0.86 (0.69–1.06)
9.2 10.5
HR: 0.86 (0.65–1.13) PFS
ZODIAC4
(n=1391)
Docetaxel/placebo Docetaxel/vandetanib
3.2 4.0
HR: 0.79 (0.70–0.90)
10.0 10.6
HR: 0.91 (0.78–1.07) PFS
SUN10875
(n=960)*
Erlotinib/placebo Erlotinib/sunitinib
VEGFR-1, -2, -3, PDGFR-ɑ, -ß,
Flt-3, c-kit
2.0 3.6
HR: 0.81 (0.70–0.94)
8.5 9.0
HR: 0.92 (0.80–1.07) OS
VITAL6 (n=913)
Docetaxel/placebo Docetaxel/aflibercept
VEGF-A, -B, PIGF
4.1 5.2
HR: 0.82 (0.72–0.94)
10.4 10.1
HR: 1.01 (0.87–1.17) OS
BETA7 (n=636)
Erlotinib/placebo Erlotinib/bevacizumab
VEGF-A 1.7 3.4
HR: 0.62 (0.52–0.75)
9.2 9.3
HR: 0.97 (0.80–1.18) OS
Fir
st
lin
e
Seco
nd
lin
e
*280 patients received >1 prior treatment lines. CB = carboplatin; PTX = paclitaxel; CIS = cisplatin; GEM = gemcitabine; OS = overall survival; PFS = progression-free survival; HR = hazard ratio;
VEGF = vascular endothelial growth factor receptor; PDGFR = platelet-derived growth factor receptor; RAF = rapidly accelerated fibrosarcoma; PIGF = placental growth factor receptor.
1. Scagliotti G, et al. J Clin Oncol 2010;28:1835–42; 2. Paz-Ares LG, et al. J Clin Oncol 2012;30:3084–92; 3. de Boer R, et al. J Clin Oncol 2011;29:1067–74; 4. Herbst R, et al. Lancet Oncol
2010;11:619–26; 5. Scagliotti GV, et al. J Clin Oncol 2012;30:2070–8; 6. Ramlau R, et al. J Clin Oncol 2012;30:3640–7; 7. Herbst R, et al. Lancet Oncol 2011;377:1846–54.

Nintedanib (BIBF 1120)* – a triple angiokinase inhibitor
• Oral triple angiokinase inhibitor targeting:1,2
– VEGFR 1–3
– FGFR 1–3
– PDGFR α/β
– RET, Src, FLT3
• Preclinical activity:
• Manageable safety profile in combination with:
– Docetaxel3
– Pemetrexed4
– Paclitaxel/carboplatin5
– Gemcitabine/cisplatin6
– Afatinib7
IC50
(nmol/L)
VEGFR
1 / 2 / 3
34/ 21/ 13
PDGFR
α / β
59/ 65
FGFR
1 / 2 / 3
69/ 37/ 108
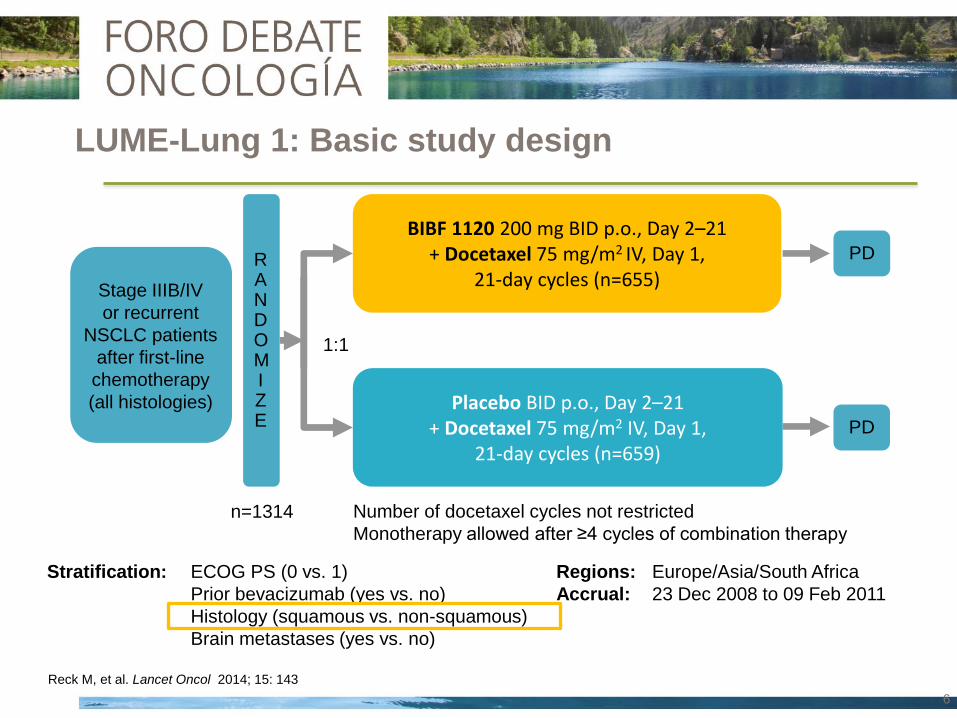
LUME-Lung 1: Basic study design
BIBF 1120 200 mg BID p.o., Day 2–21 + Docetaxel 75 mg/m2 IV, Day 1,
21-day cycles (n=655)
Placebo BID p.o., Day 2–21 + Docetaxel 75 mg/m2 IV, Day 1,
21-day cycles (n=659)
n=1314
RANDOMIZE
Stratification: ECOG PS (0 vs. 1)
Prior bevacizumab (yes vs. no)
Histology (squamous vs. non-squamous)
Brain metastases (yes vs. no)
Stage IIIB/IV
or recurrent
NSCLC patients
after first-line
chemotherapy
(all histologies)
1:1
PD
PD
Number of docetaxel cycles not restricted
Monotherapy allowed after ≥4 cycles of combination therapy
Regions: Europe/Asia/South Africa
Accrual: 23 Dec 2008 to 09 Feb 2011
Reck M, et al. Lancet Oncol 2014; 15: 143
6

Key Inclusion
• Histologically or cytologically confirmed, locally advanced and/or metastatic, stage
IIIB–IV or recurrent NSCLC
• All NSCLC histologies
• Failure after first-line chemotherapy (adjuvant /neoadjuvant allowed)
• ECOG PS 0 or 1
Key Exclusion
• Prior docetaxel or VEGF/VEGFR inhibitors (other than bevacizumab)
• Active brain metastases or leptomeningeal disease
• Centrally located tumours with radiographic evidence (CT or MRI) of local invasion
of major blood vessels or radiographic evidence of cavitary or necrotic tumours
• History of clinically significant hemoptysis within the past 3 months (greater than
one teaspoon of fresh blood per day)
Major Eligibility Criteria
LUME-Lung 1: Statistical design
Primary objective: PFS (centrally reviewed)
Secondary objectives: OS
PFS (investigator assessment)
Response rate
Safety analysis
PFS: 713 events HR 0.78, power 90%): 1300 patients (10% attrition)
Futility analysis with 50% of events
OS: 1151 deaths (HR 0.85, power 80%)

*Stratified for baseline ECOG PS , tumour histology, brain metastases and prior treatment with Bevacizumab.
LUME Lung 2 was stopped on 18 June 2011 at the recommendation of the DMC
based on a futility analysis using investigator assessed PFS.
LUME Lung 2: DMC futility analysis: investigator based PFS

Baseline variables investigated for LUME Lung 1 + 2
Baseline variables
Race (Asian yes / no)*
Gender* (male / female)
Stage at diagnosis* (<IIIB/IV vs. IIIB vs. IV)
Age (<65 / ≥65 years)*
Smoking history* (ever smoked vs. never smoked)
Adrenal metastasis** (yes / no)
Liver metastasis* (yes / no)
Number of metastatic organs**
Therapy with bisphosphonates* (yes / no)
LDH level** (≤1 vs >1)
Best response to 1st line* (CR,PR,SD vs. PD vs. UNK )
Time since start of 1st line treatment * (continuous variable)
Stratification factors
ECOG performance score
Bevacizumab pre-treatment
Brain metastases at baseline
Tumour histology
* Pre-specified in the protocol or identified from
literature** as potential prognostic or predictive variable.
Kaiser R, et al. Eur J Cancer 2013; 49: 3479

OS Adenocarcinoma
T<9mo
Key secondary endpoint: OS • Stepwise testing
time since start of 1st line therapy (T) <9 months all adenocarcinoma all histologies
• 80% power*, HR 0.80
• Two sided stratified log-rank test, α=0.0494**
• Two-sided stratified log-rank test, α=0.05
Primary endpoint: Independently assessed PFS • All histologies
• 90% power after 713 PFS events, HR 0.78
Statistical Design
p<0.0494 p<0.0494 p<0.0494
1
2
Next analysis step only allowed if PFS confirmed
with all PFS events at time point of OS analysis
OS
OS
*Fixed-sequence order testing implemented prior to database lock to validate biomarker findings from independent study
LUME-Lung 2 (Hanna N, et al. ASCO 2013. Abstract #8034; Hanna N, et al. ESMO 2013. Abstract #3418;
Kaiser R, et al. ESMO 2013 Abstract #3479); Reck M, et al. Lancet Oncol 2014; 15: 143**Overall α=0.05
All adenocarcinoma All histologies

Patient characteristics
Nintedanib Placebo
Age 60 (53-67) 60 (54-66)
Gender (Male) % 72.7 72.7
PS 0/ 1 % 28.5/ 71.3 28.7/ 71.3
Never smoker % 25.2 24.4
Brain met. % 5.8 5.8
Squamous/ Adenoca % 42.1/ 49.2 42.3/ 51.0
Months 1st diagnosis 8.8 (5.4-13.6) 8.6 (5.4-13.6)
Prior platinum % 97.2 97.7
Prior bevacizumab % 4.1 3.5
Best response (CR/ PR/ SD) % 2.0/ 33.1/ 38.5 2.9/ 27.2/ 38.2
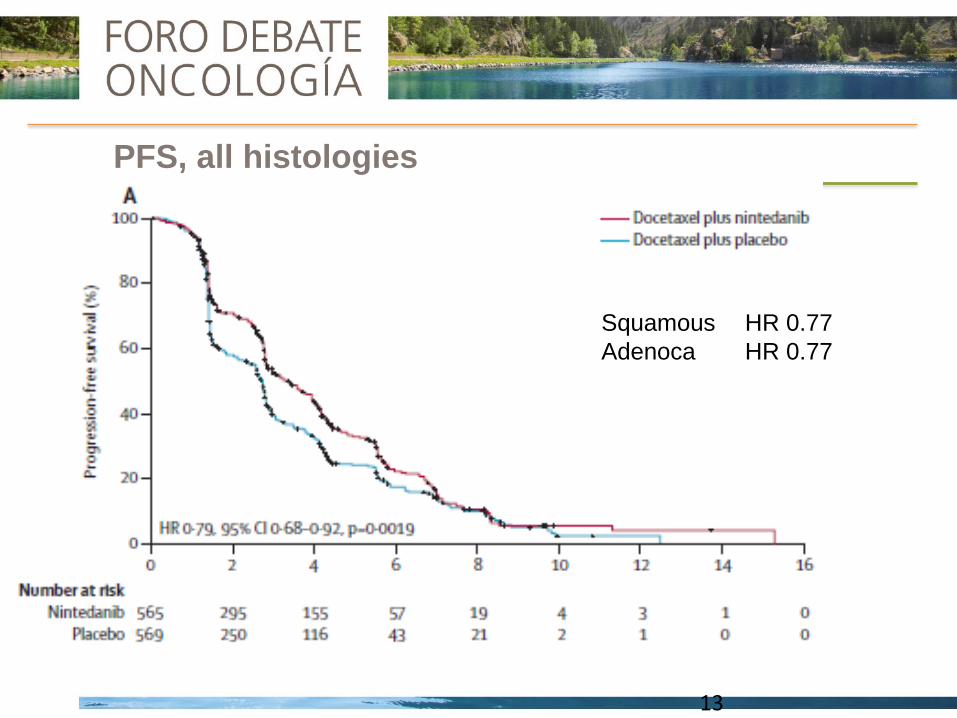
PFS, all histologies
13
Squamous HR 0.77
Adenoca HR 0.77
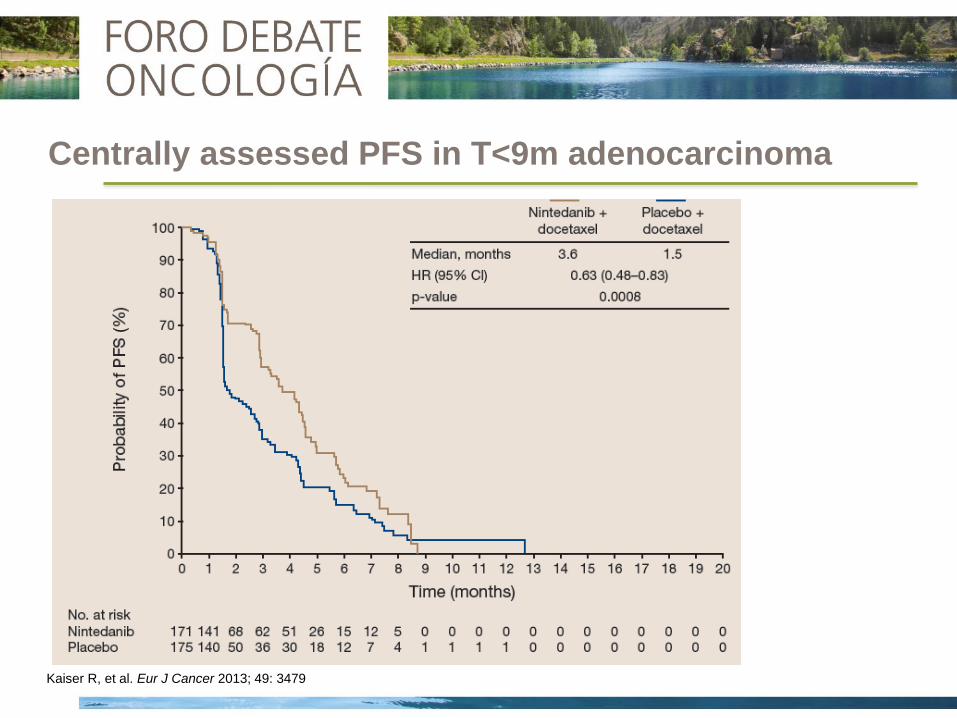
Centrally assessed PFS in T<9m adenocarcinoma
OS
Kaiser R, et al. Eur J Cancer 2013; 49: 3479

Overall Survival: Adenocarcinoma < 9m Since Start of 1st Line
All : 10.1 vs 9.9 m
HR 0.94, p= 0.27
Adenoca: 12.6 vs 10.3 m
HR 0.83, p= 0.03
PD to 1st L 9.8 vs 6.3m
117p HR 0.62, p=0.02
10.9
7.9 m
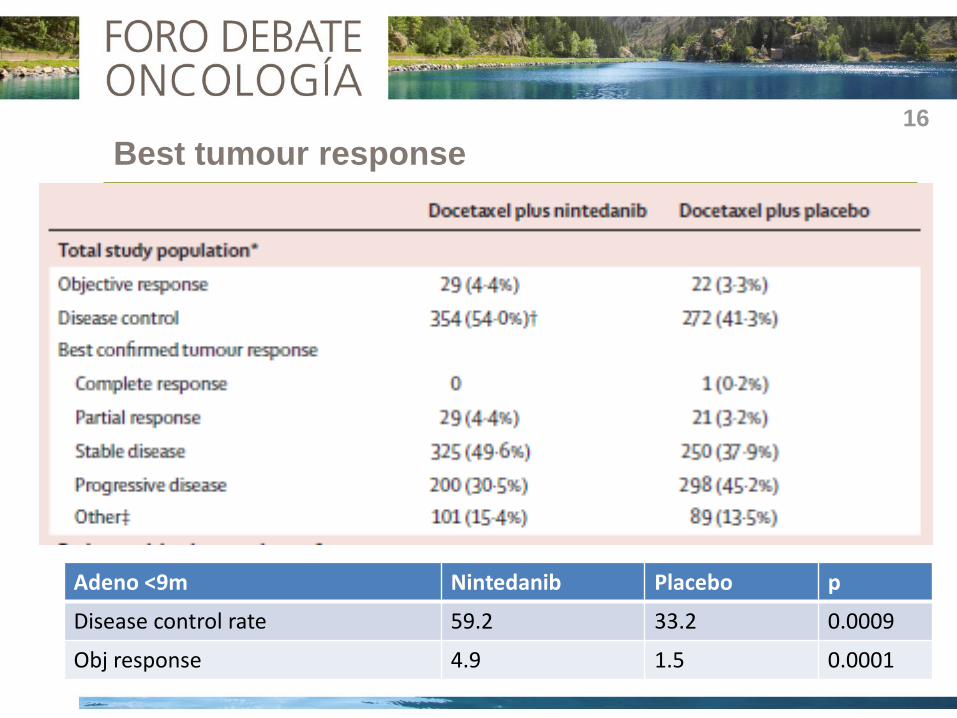
Best tumour response
Adenocarcinoma, T<9 months (n=405) 16
Adeno <9m Nintedanib Placebo p
Disease control rate 59.2 33.2 0.0009
Obj response 4.9 1.5 0.0001

Overall Survival: Adenocarcinoma Histology

Safety in All Treated Patients
45
40
35
30
25
20
15
10 5
0
Pati
en
ts (
%)
All CTCAE grades ≥15% incidence
CTCAE grades ≥3 ≥1% incidence
Nintedanib + docetaxel
Placebo + docetaxel
50
45
40
35
30
25
20
15
10 5
0
50
HBP, bleeding, intestinal perforation: No differences

First positive trial of a targeted agent in second line therapy of NSCLC
along with standard chemotherapy
LUME-Lung1 met its primary endpoint: PFS (HR 0.79, p=0.0019) in all
histologies
Nintedanib + Docetaxel significantly improved OS in adenocarcinoma
histology (HR 0.83, p=0.0359, median OS 10.3 to 12.6 m)
Patients with a poor prognosis (time since start of 1st line therapy <9
months) also experienced significant OS improvement
AEs with Nintedanib + Docetaxel were generally manageable with dose
reductions and symptomatic treatment
Summary
Absolute benefit was small, increased toxicity in a palliative setting,
absence of biomarkers

INMUNOTERAPIA
NINTEDANIB

Reconocimiento
Presentación de antígenos
Activación de linfocitos T
Destrucción celular



Anti- N RO (%) IrRO(%)
Nivolumab PD1 129 17.1 21.7
MK3475 PD1 221 15 21
MPDL3280A PD-L1 85 23 -
BMS936559 PD-L1 207 10 -
MEDI4736 PD-L1 26 15 -
Eficacia

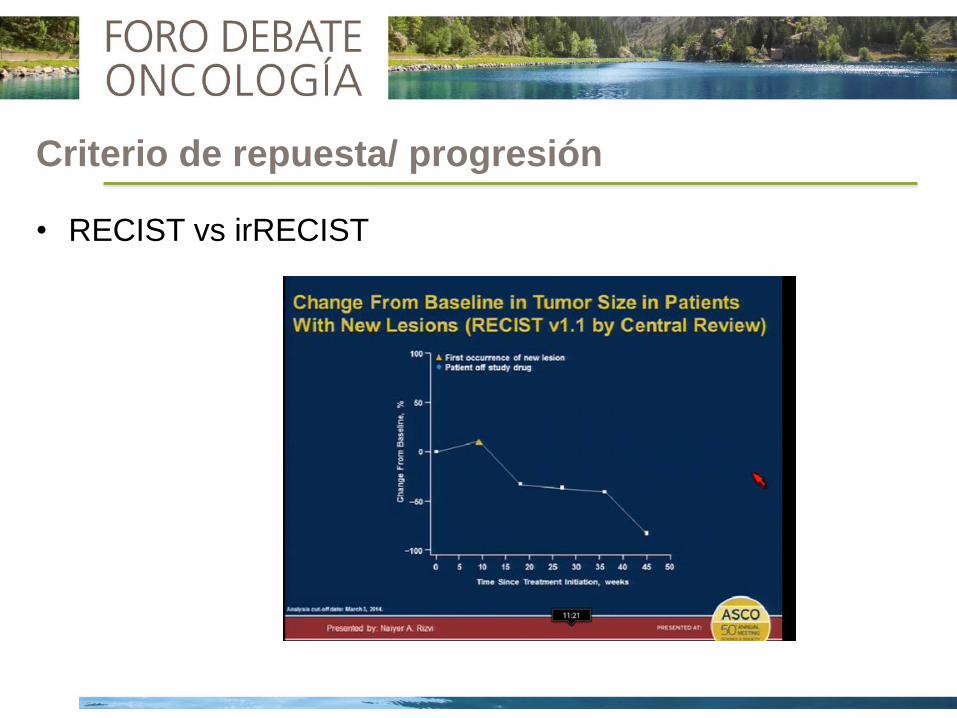
Criterio de repuesta/ progresión
• RECIST vs irRECIST



• Dificultad recuperación en FFPE
• Heterogeneidad tumoral
• Prevalencia
• Influencia de tratamientos previos
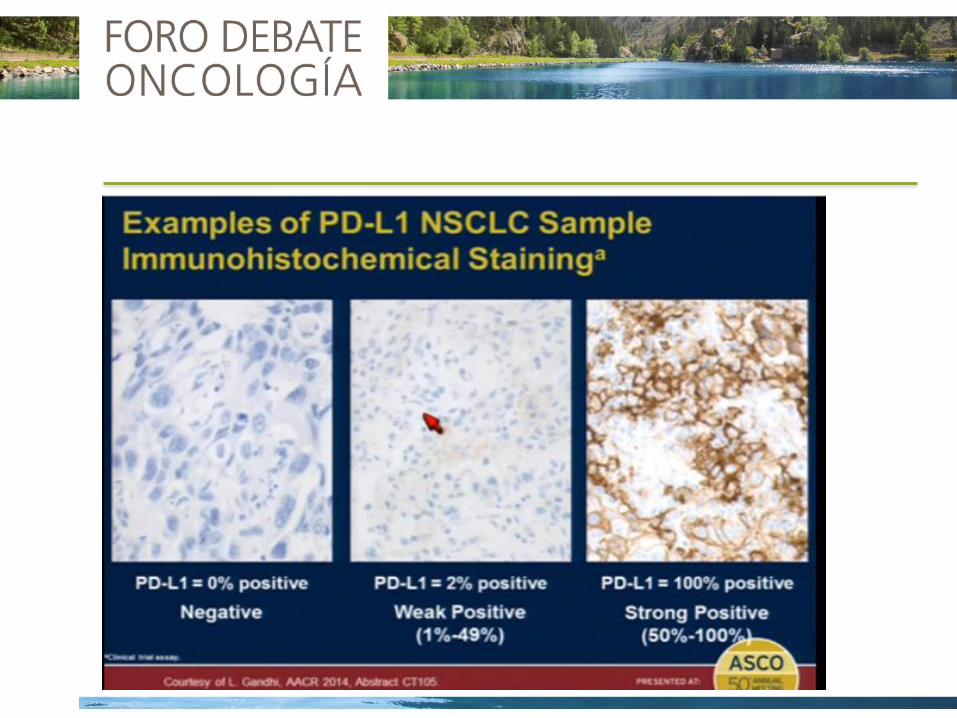
• Criterio de positividad (1/ 5/ 10/ 50%?)
• Positividad en céls. tumorales o linfocitos
• Diferentes pruebas (problemas metodológicos + intereses
comerciales)
Concordancia?
Respuestas en tumores PD-L1 negativo (8-15%)
PD-L1como biomarcador


Toxicidad
Anti- N AE (%) G3-4 (%) Neumonitis (%)-G34-G5
Nivolumab PD1 129 53 5 6-2-2p
MK3475 PD1 221 48 6 1-1-0
MPDL3280A PD-L1 85 66 11 ?-0-0
BMS936559 PD-L1 207 61 9 0-0-0
MEDI4736 PD-L1 26 34 0 0-0-0
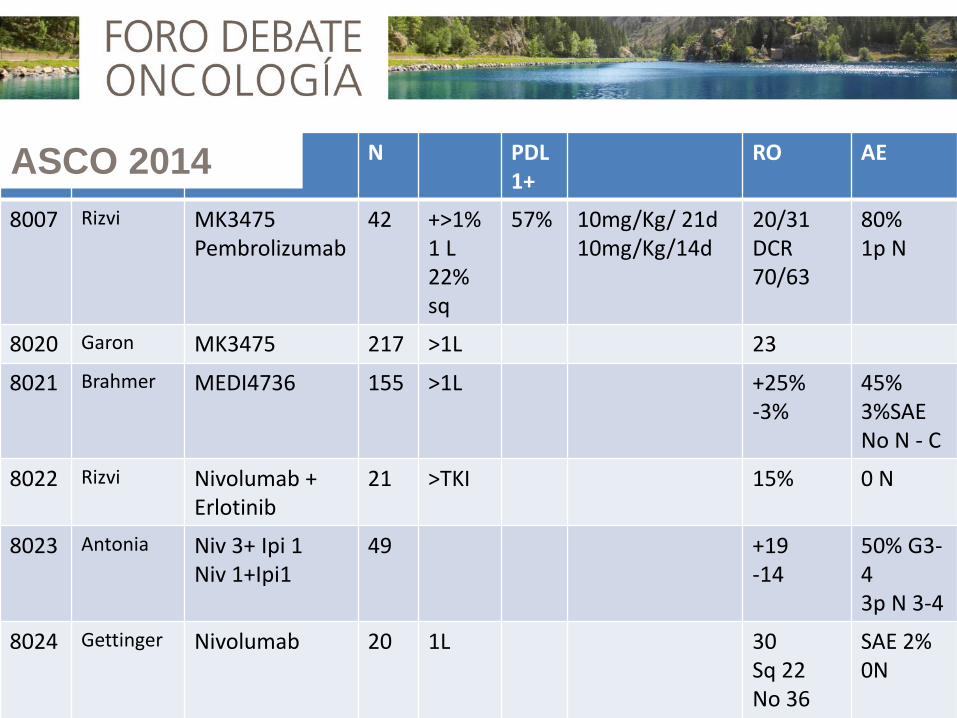
N PDL1+
RO AE
8007 Rizvi MK3475 Pembrolizumab
42 +>1% 1 L 22% sq
57% 10mg/Kg/ 21d 10mg/Kg/14d
20/31 DCR 70/63
80% 1p N
8020 Garon MK3475 217 >1L 23
8021 Brahmer MEDI4736 155 >1L +25% -3%
45% 3%SAE No N - C
8022 Rizvi Nivolumab + Erlotinib
21 >TKI 15% 0 N
8023 Antonia Niv 3+ Ipi 1 Niv 1+Ipi1
49 +19 -14
50% G3-4 3p N 3-4
8024 Gettinger Nivolumab 20 1L 30 Sq 22 No 36 +50, -0%
SAE 2% 0N
ASCO 2014

Ensayos en combinación
Línea
QT Nivolumab 1ª CDDP-Gem CDDP-Pem CBDCA-Tax
MK-3475 1ª CDDP-Pem CBDCA-Tax±Bev
MPDL3280A T. sólidos CBDCA-Tax±Bev Nab-paclitaxel Pem±Bev FOLFOX
T. dirigidas Nivolumab Erlotinib
MK-3475 Erlotinib Gefitinib
MPDL3280A Erlotinib Cobimetinib (Mek)

Línea
Inmunoterapia Nivolumab 1ª Ipilimumab
MK-3476 2ª Tremelimumab
MEDI0680 T. sólidos MEDI4376
Nivolumab T. sólidos Il-21
Nivolumab Anti-CD137 Anti-KIR

Cuestiones pendientes
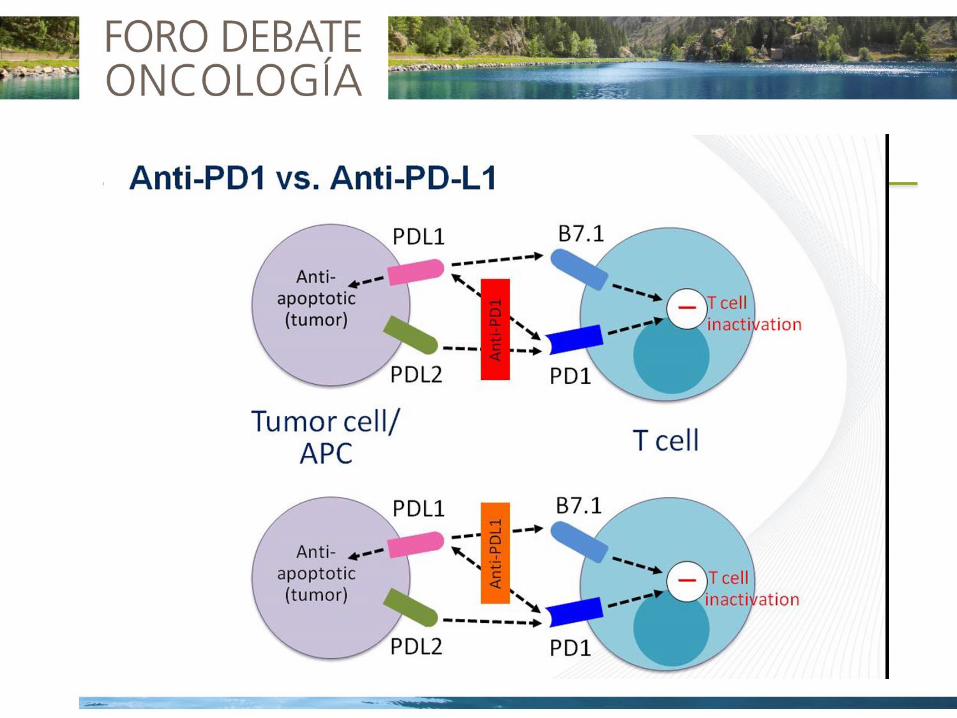
Anti PD-1 o anti PD-L1 Actividad parece semejante
Duración del tratamiento Indefinido vs 1-2 daños
Respuestas en re-tto y post-tto
Combinación QT (dosis y esquema, inmuno-
supresión vs antígenos, MHC,…)
Valor del “priming” (agentes
hipometilantes y HDACi)?
Inmunoterapia (vacunas, citoquinas,
céls. dendríticas)
Bevacizumab (inmunosupresor,
infiltración LT)
RT
Mecanismos de resistencia, activación LT,…