DIABETES MELLITUS TIPO 2 ENFERMEDAD … · 5.-incretinas sumario . desarrollo y progresiÓn de la...
84
DIABETES MELLITUS TIPO 2 ENFERMEDAD CARDIOVASCULAR Dr. Iñaki Lekuona Sº Cardiología HGU- Osakidetza
Transcript of DIABETES MELLITUS TIPO 2 ENFERMEDAD … · 5.-incretinas sumario . desarrollo y progresiÓn de la...

DIABETES MELLITUS TIPO 2 ENFERMEDAD CARDIOVASCULAR
Dr. Iñaki Lekuona Sº Cardiología HGU- Osakidetza

1.-Introducción
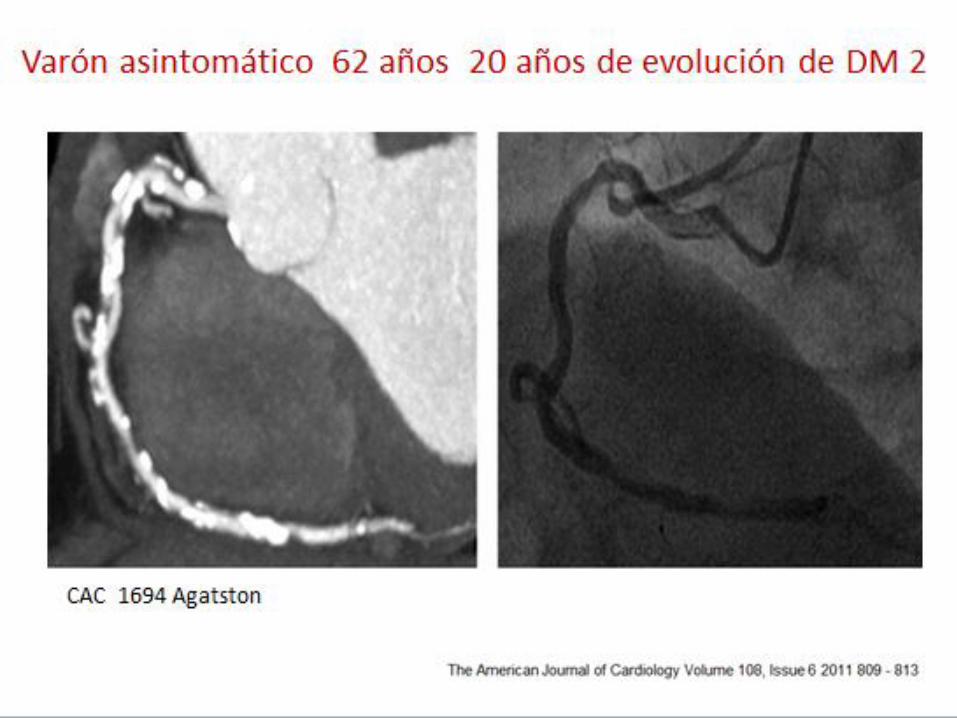
2.-¿Es diferente la aterosclerosis del diabético? IMAGEN
3.-Mecanismos de la afectación vascular en la diabetes
4.-Influencia del tratamiento hipoglucemiante en la afectación vascular
5.-Incretinas
SUMARIO

DESARROLLO Y PROGRESIÓN DE LA DIABETES

RESISTENCIA INSULÍNICA
EDAD
FÁRMACOS OBESIDAD e INACTIVIDAD
ANOMALÍAS GENÉTICAS
HIPERTENSIÓN DISLIPIDEMIA
ATEROSCLEROSIS
PCOS
ENFERMEDADES RARAS
DIABETES TIPO 2
LA RESISTENCIA INSULÍNICA ES LA CLAVE
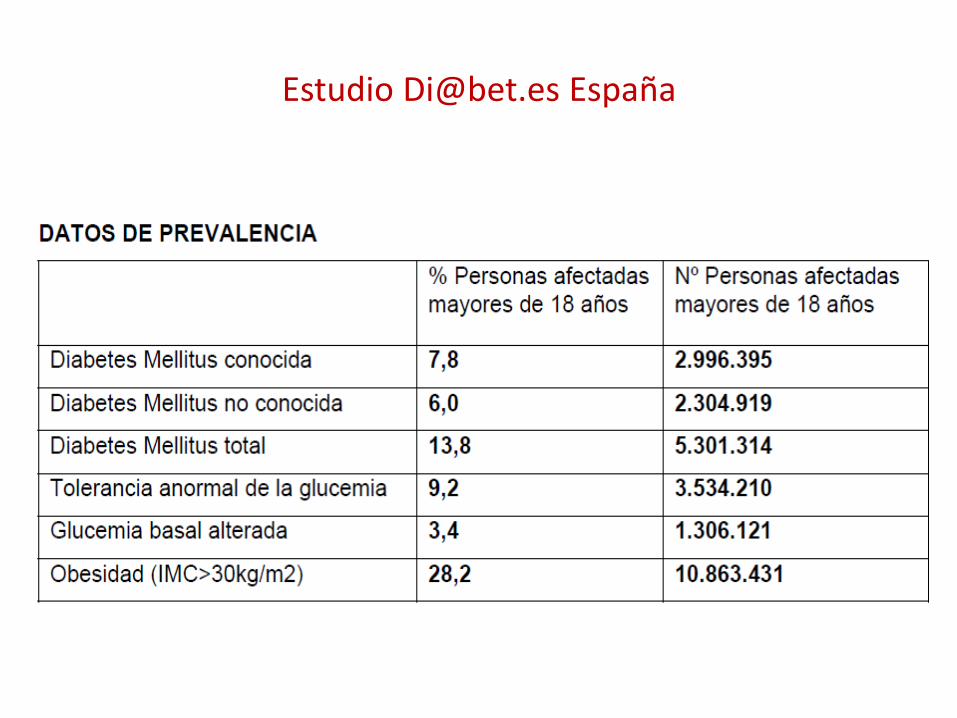
Estudio [email protected] España
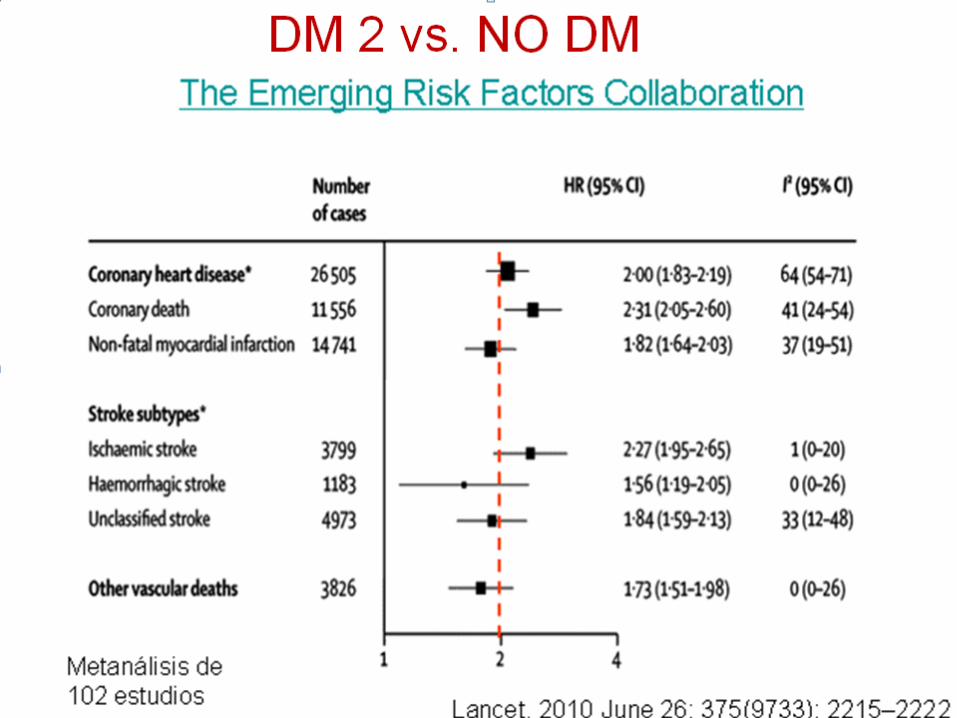




DIABETES ES MUY PREVALENTE EN EL PACIENTE CORONARIO
TRIUMPH registro > 4.000 IAM 29.6% DM2 69% SM JACC 2013
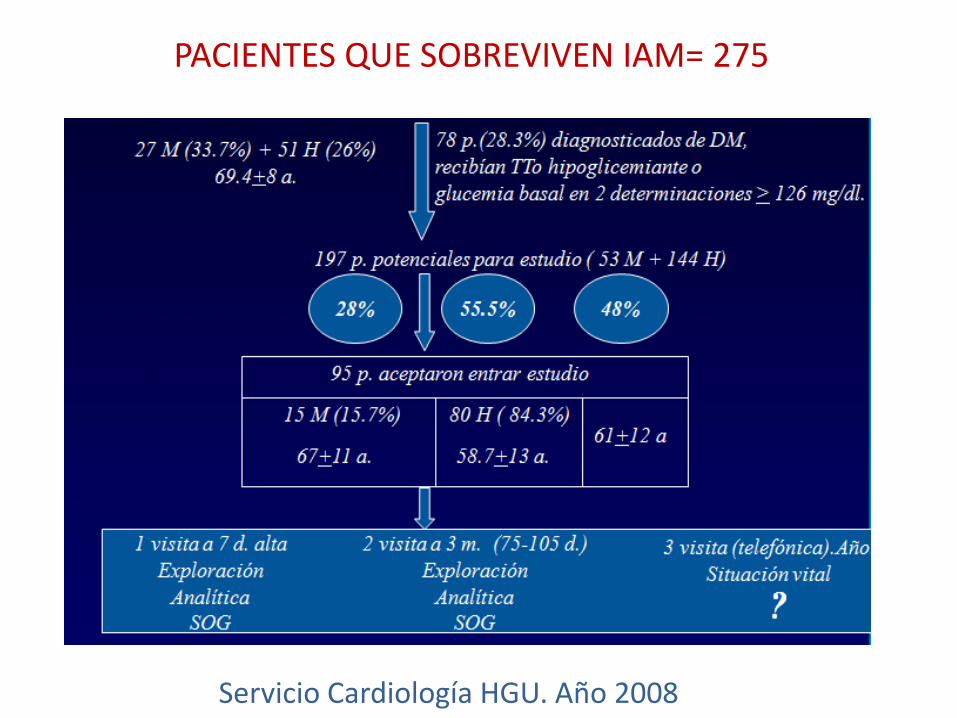
PACIENTES QUE SOBREVIVEN IAM= 275
Servicio Cardiología HGU. Año 2008

ANOMALÍAS METABOLISMO HDC TRAS SOG
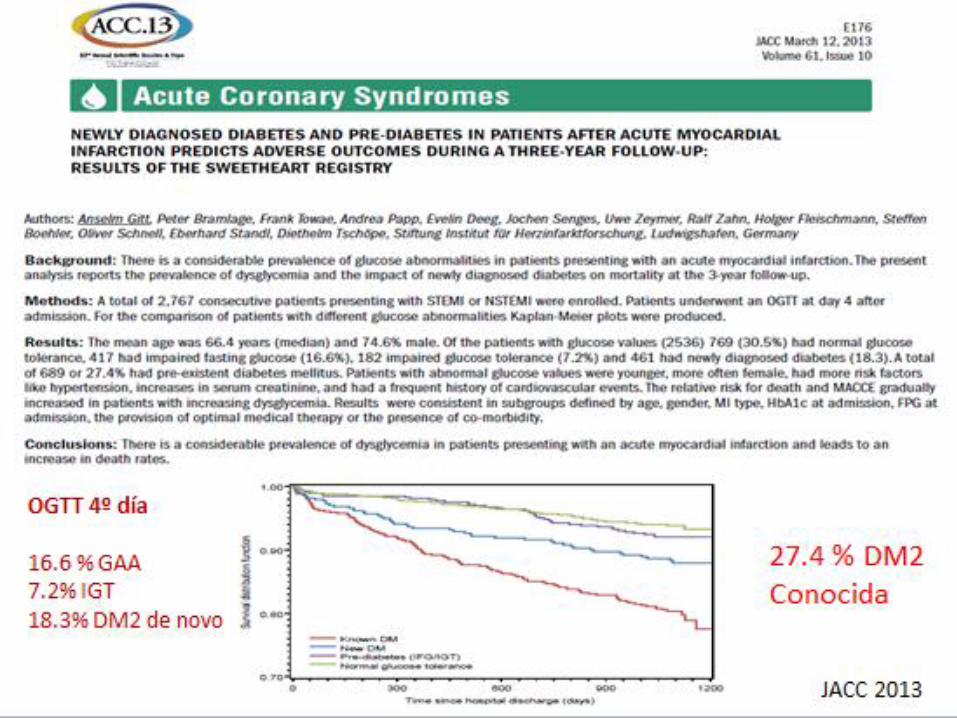
63% DE LA POBLACIÓN IAM 2008 PRESENTAN ANOMALÍAS DEL METABOLISMO HIDROCARBONADO
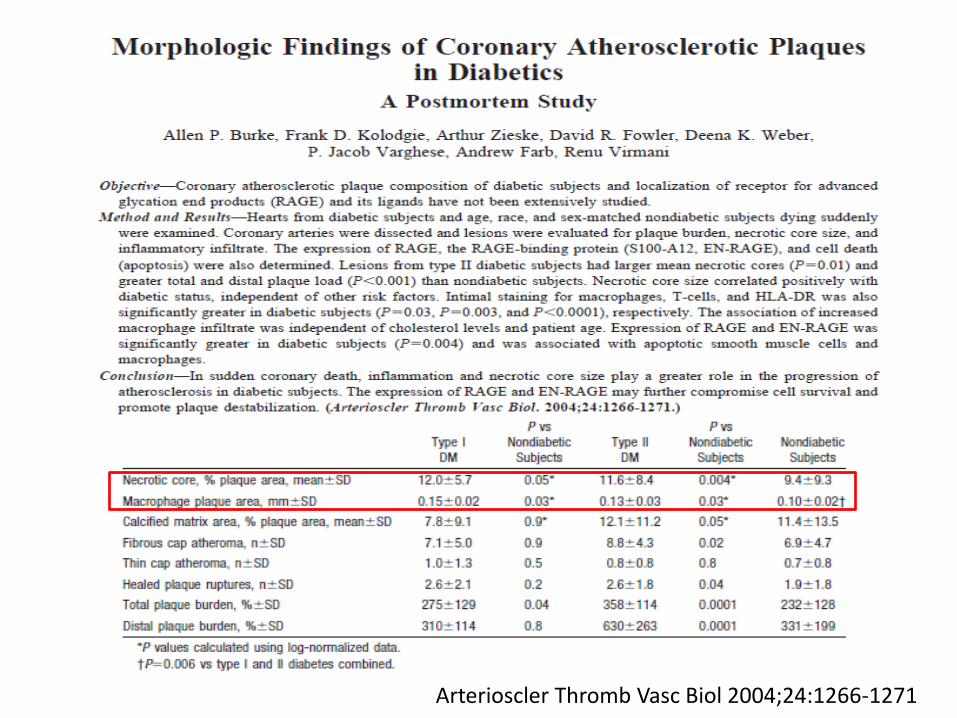
Arterioscler Thromb Vasc Biol 2004;24:1266-1271

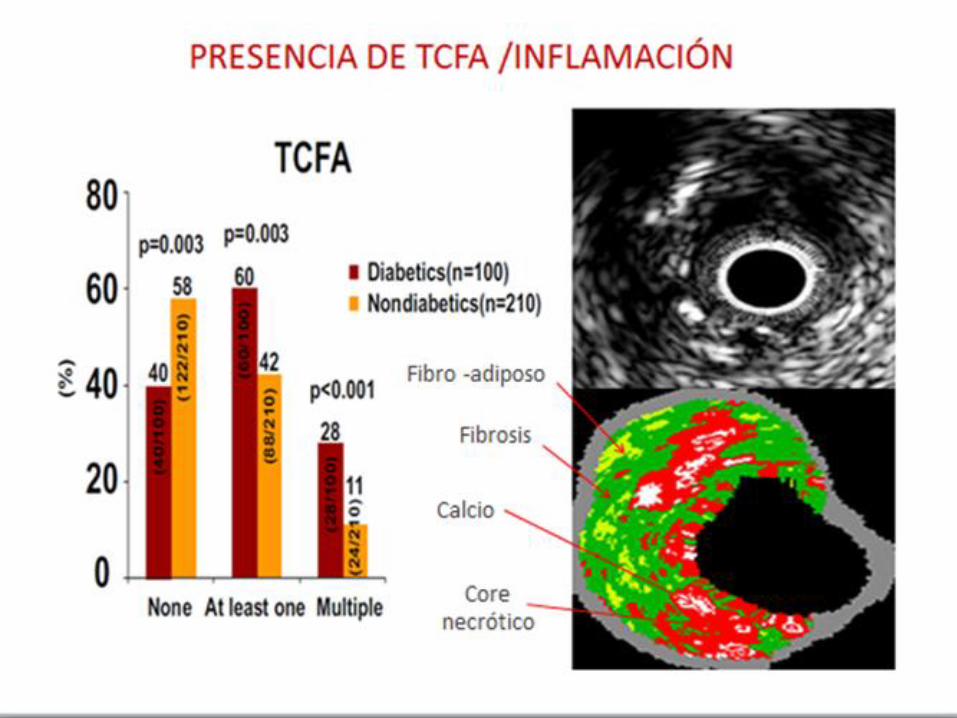
Vascular Medicine 2011;16(2):103-108

IVUS HISTOLOGÍA VIRTUAL
SCA más placas vulnerables con diferente composición y mayor componente inflamatorio en DM
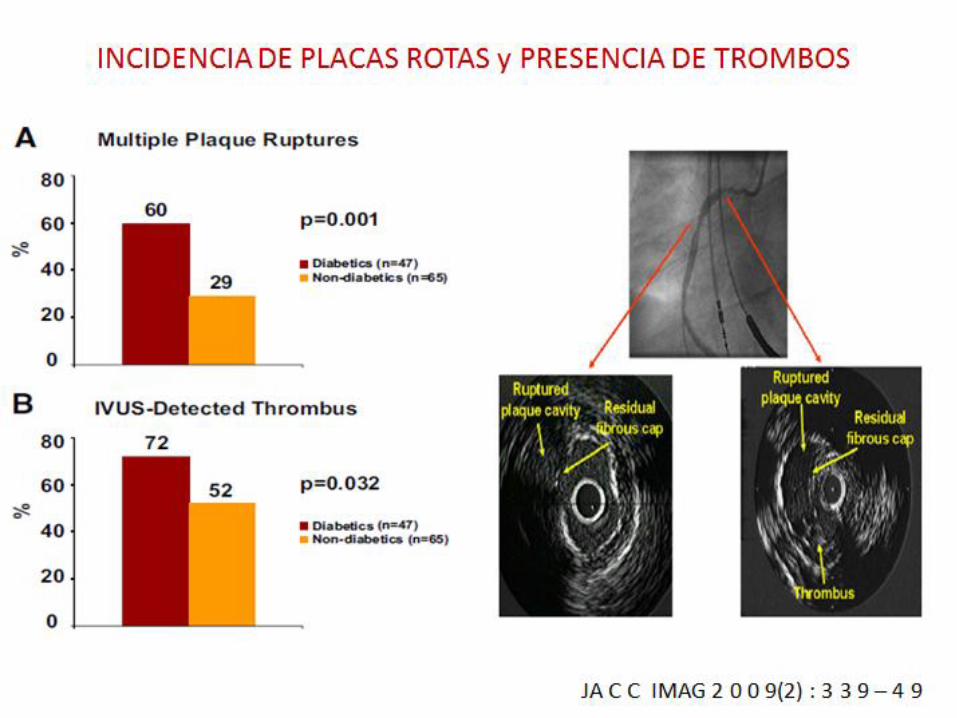


Mas carga de placa, mas calcificada, mas roturas en DM

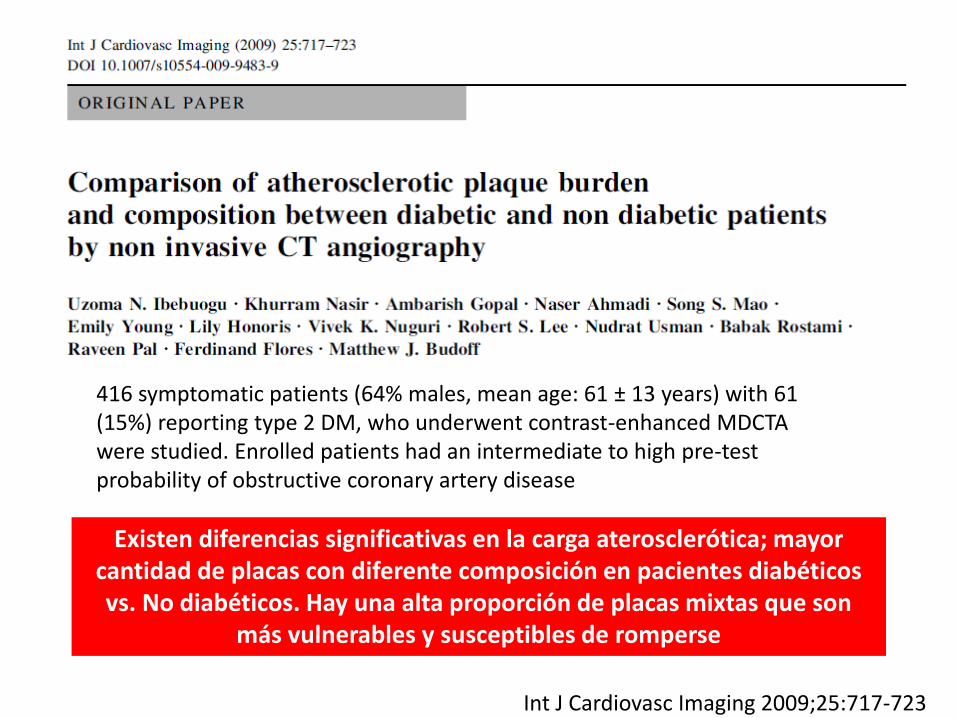
Existen diferencias significativas en la carga aterosclerótica; mayor cantidad de placas con diferente composición en pacientes diabéticos vs. No diabéticos. Hay una alta proporción de placas mixtas que son
más vulnerables y susceptibles de romperse
416 symptomatic patients (64% males, mean age: 61 ± 13 years) with 61 (15%) reporting type 2 DM, who underwent contrast-enhanced MDCTA were studied. Enrolled patients had an intermediate to high pre-test probability of obstructive coronary artery disease
Int J Cardiovasc Imaging 2009;25:717-723

TC MULTICORTE EN DM CON ENFERMEDAD MULTIVASO








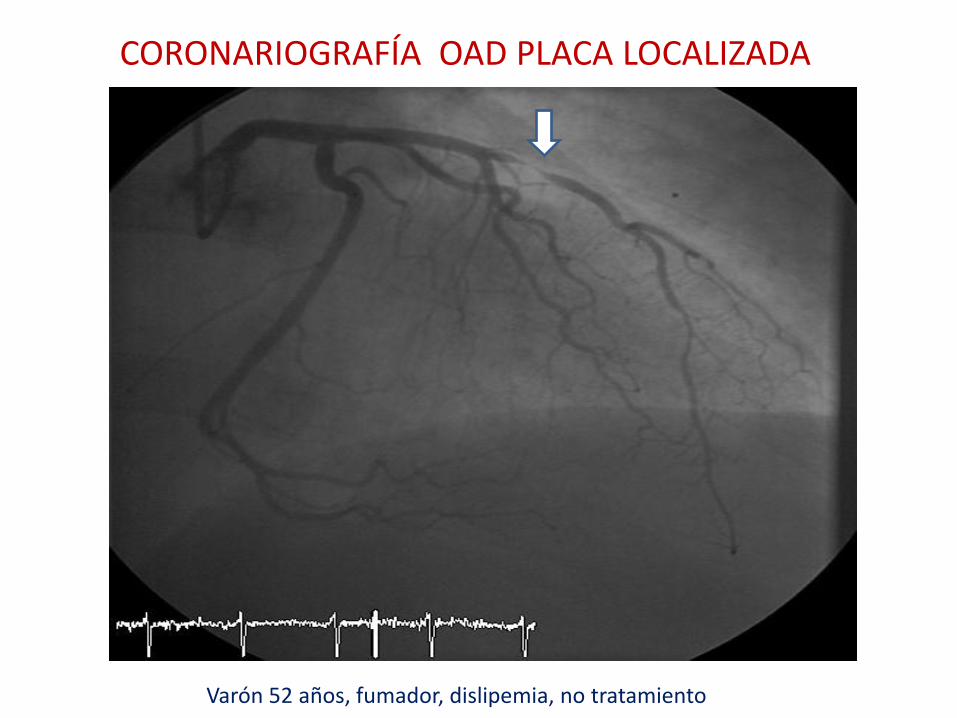
CORONARIOGRAFÍA OAD PLACA LOCALIZADA
Varón 52 años, fumador, dislipemia, no tratamiento
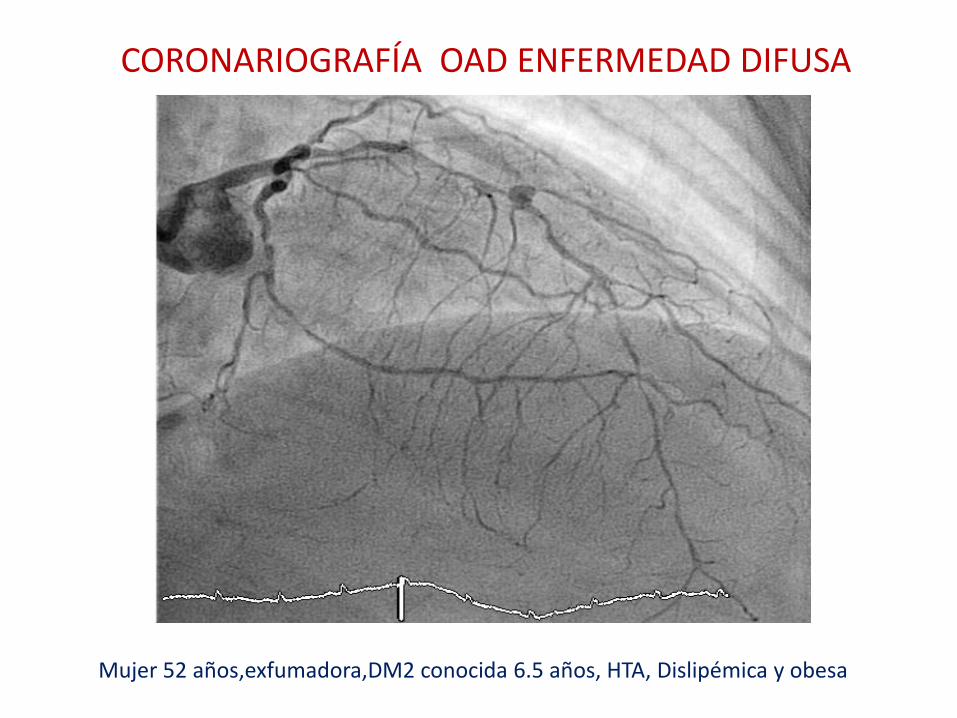
CORONARIOGRAFÍA OAD ENFERMEDAD DIFUSA
Mujer 52 años,exfumadora,DM2 conocida 6.5 años, HTA, Dislipémica y obesa


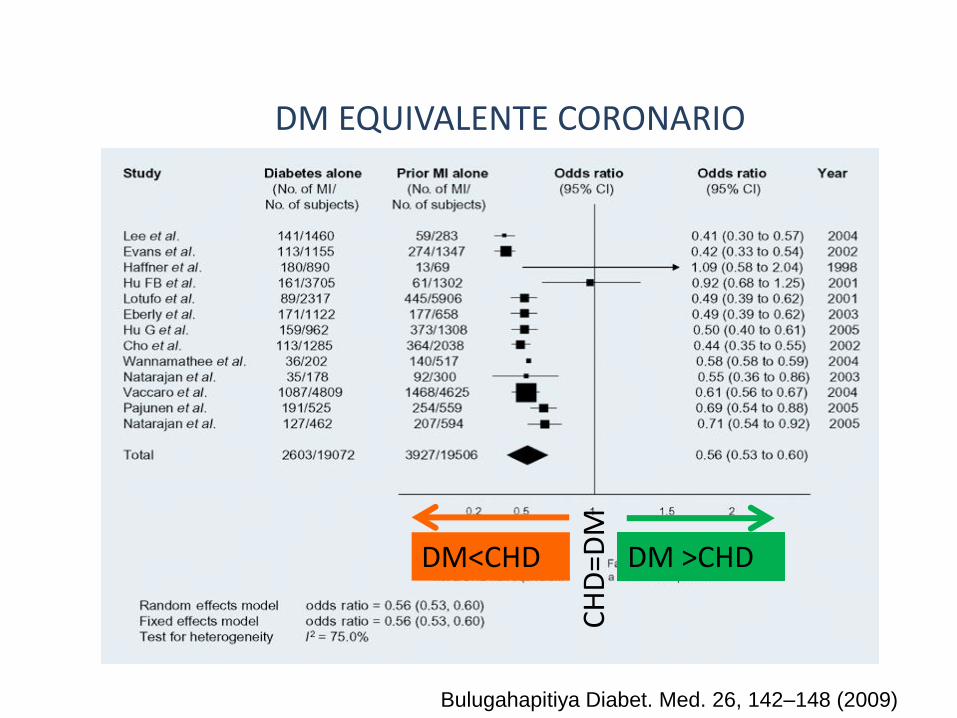
CH
D=D
M
DM >CHD DM<CHD
Bulugahapitiya Diabet. Med. 26, 142–148 (2009)
DM EQUIVALENTE CORONARIO

Bulugahapitiya Diabet. Med. 26, 142–148 (2009)
DM equivalente de riesgo CORONARIO ?

IAM DM+ ERC
ERC DM
PG
Lancet 2012; 380: 807–14
Risk of coronary events in coronary heart disease, chronic kidney disease & diabetes: A population-level cohort study




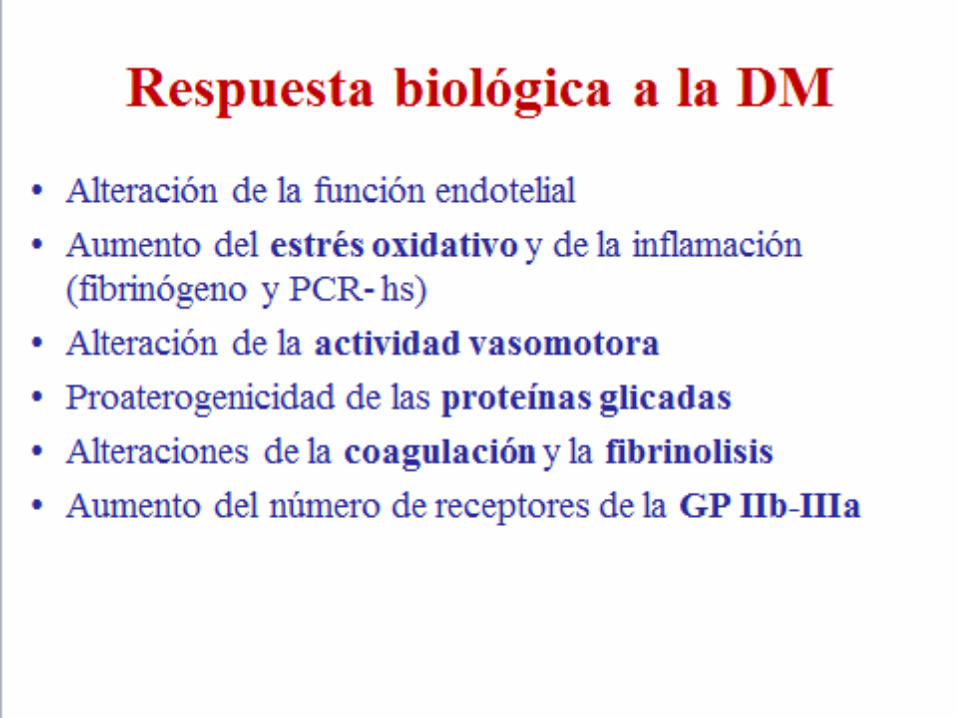
MECANISMOS DE LA AFECTACIÓN VASCULAR EN LA DIABETES
HIPERGLICEMIA DISLIPEMIA DIABÉTICA INFLAMACIÓN HIPERAGREGACIÓN PLAQUETARIA


LEGADO VASCULAR
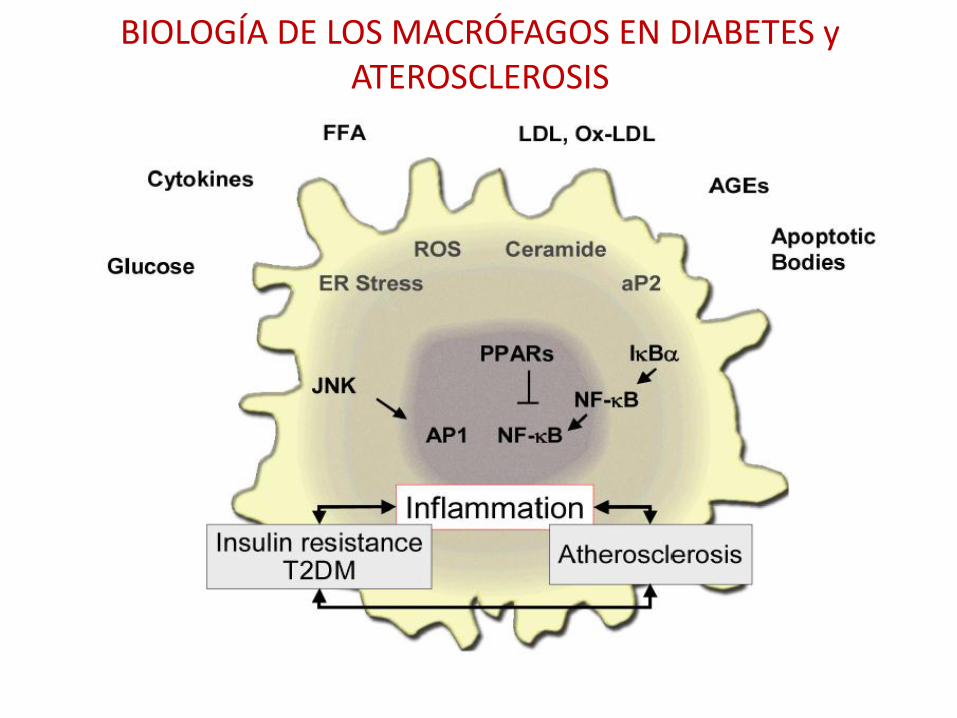
BIOLOGÍA DE LOS MACRÓFAGOS EN DIABETES y ATEROSCLEROSIS

PROLIFERACIÓN DE LOS VASA VASORUM EN DIABÉTICOS

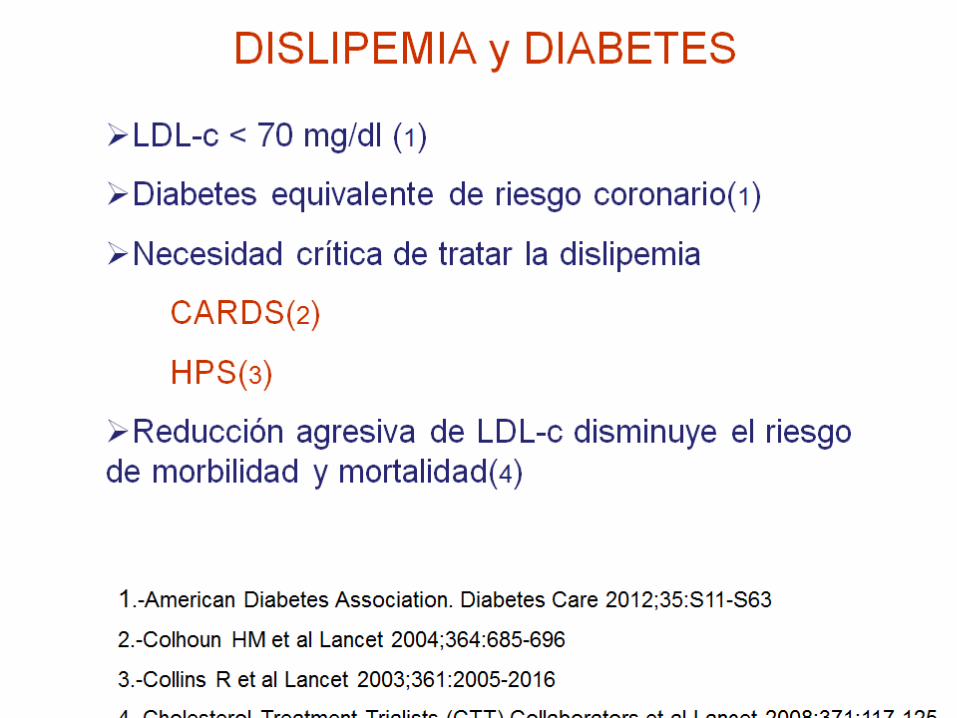
DISLIPIDEMIA DIABÉTICA Y PARED VASCULAR
LDL densas y pequeñas HDL bajo TG altos

INFLAMACIÓN, DIABETES Y ATEROSCLEROSIS














Diabetes: Estudios clínicos esenciales
ACCORD, ADVANCE, VADT

LECCIONES APRENDIDAS DE LOS ENSAYOS CLÍNICOS
1.-Para obtener evidencias se precisan grandes ensayos a muy largo plazo 2.-El control glucémico estricto y precoz es la mejor estrategia para prevenir complicaciones microvasculares. Legado vascular 3.-El control estricto de los FRCV asociados sigue siendo la mejor estrategia para reducir el riesgo macrovascular 4.-La estrategia terapéutica elegida puede ser tan importante como el valor diana de Hb A 1C
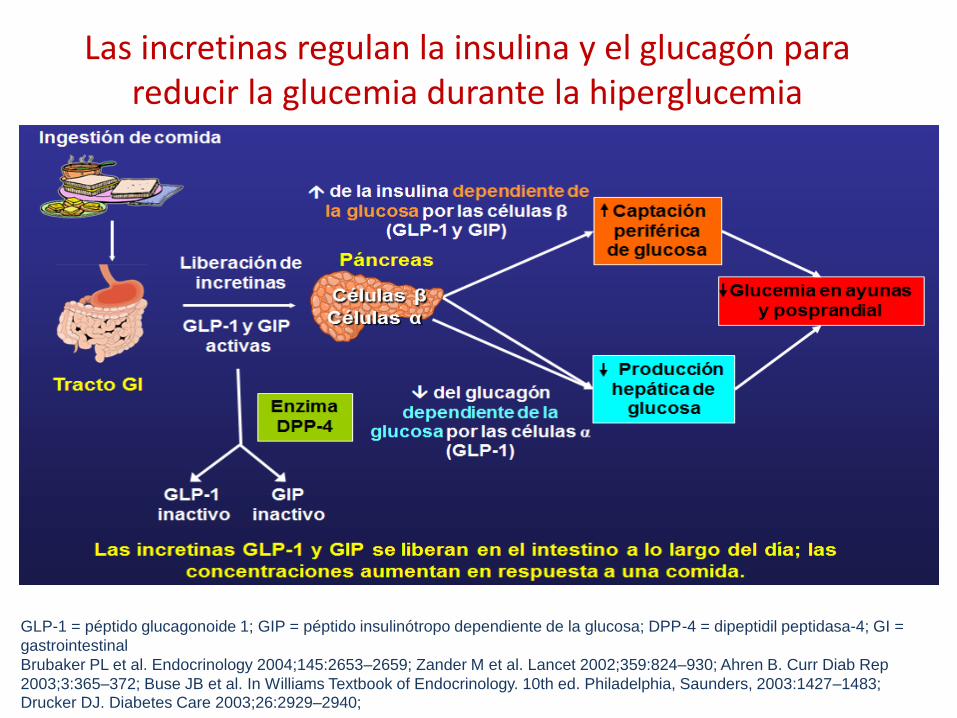
Las incretinas regulan la insulina y el glucagón para reducir la glucemia durante la hiperglucemia
GLP-1 = péptido glucagonoide 1; GIP = péptido insulinótropo dependiente de la glucosa; DPP-4 = dipeptidil peptidasa-4; GI =
gastrointestinal
Brubaker PL et al. Endocrinology 2004;145:2653–2659; Zander M et al. Lancet 2002;359:824–930; Ahren B. Curr Diab Rep
2003;3:365–372; Buse JB et al. In Williams Textbook of Endocrinology. 10th ed. Philadelphia, Saunders, 2003:1427–1483; Drucker DJ. Diabetes Care 2003;26:2929–2940;
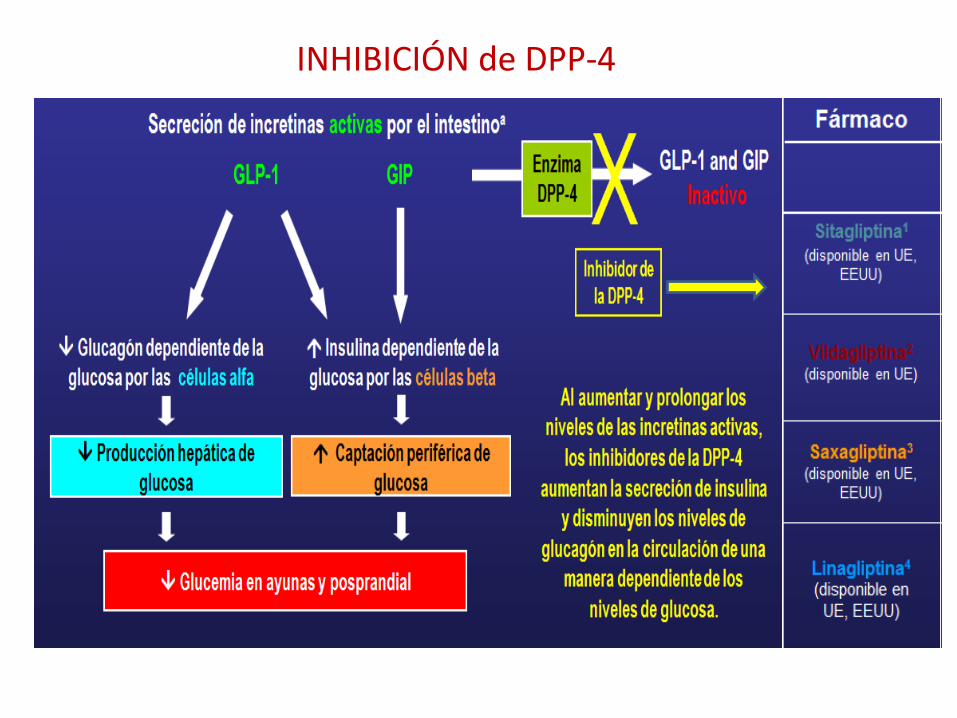
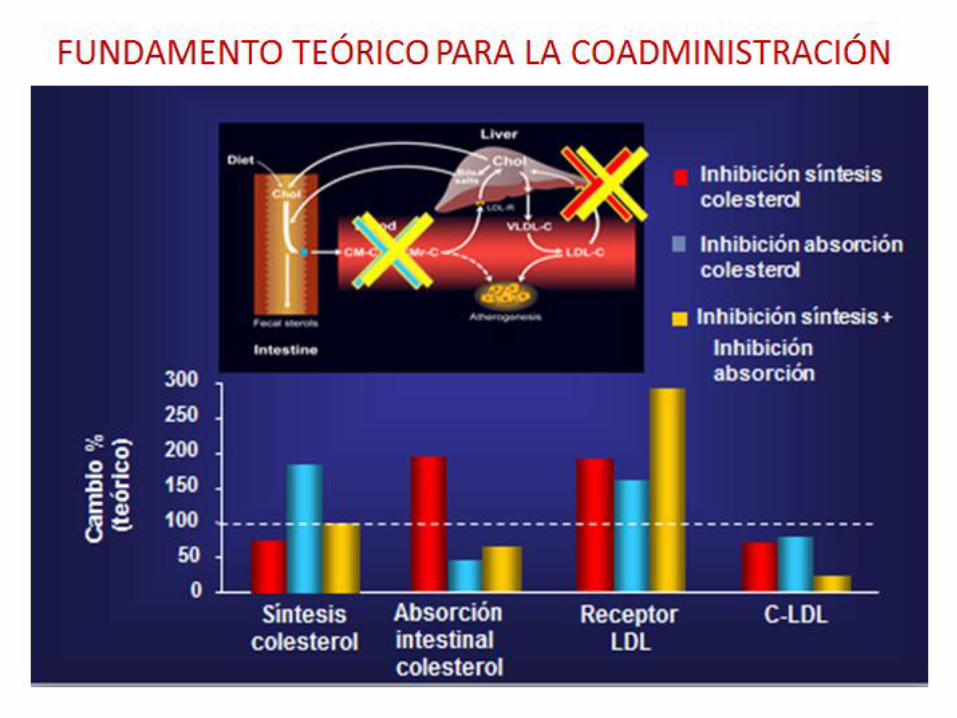
INHIBICIÓN de DPP-4
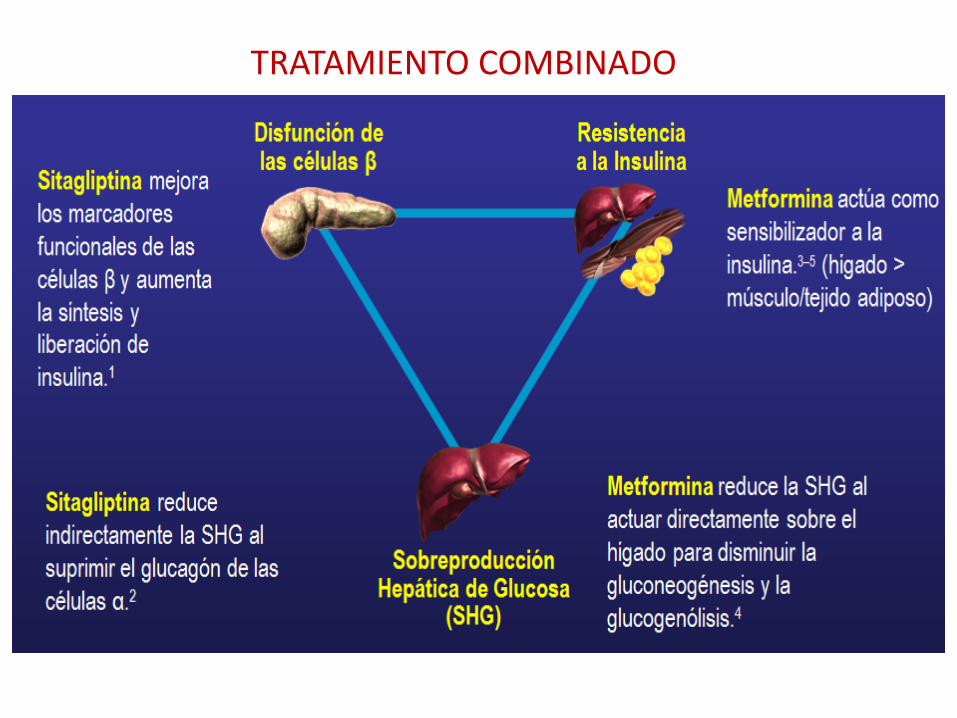
TRATAMIENTO COMBINADO


27 reports of 19 studies including 7136 patients randomized to a DPP-4 inhibitor and 6745 patients randomized to another hypoglycaemic drug
CONCLUSIONS: In patients with type 2 diabetes who do not achieve the glycemic targets with metformin alone, DPP-4 inhibitors can lower HbA1c, in a similar way to sulfonylureas or pioglitazone, with neutral effects on body weight.
CONCLUSIONS: DPP-4 inhibitors were associated with a reduction in A1C with comparable safety profiles compared to placebo, but no significant difference in A1C compared to other hyperglycemics. Differences in efficacy and safety were observed between Japanese and non-Japanese patients.
Ann Pharmacother. 2012 Nov;46(11):1453-69. doi: 10.1345/aph.1R041. Epub 2012 Nov 7

SUSTRATOS DPP-4 Regulan directa ó indirectamente la función cardiovascular
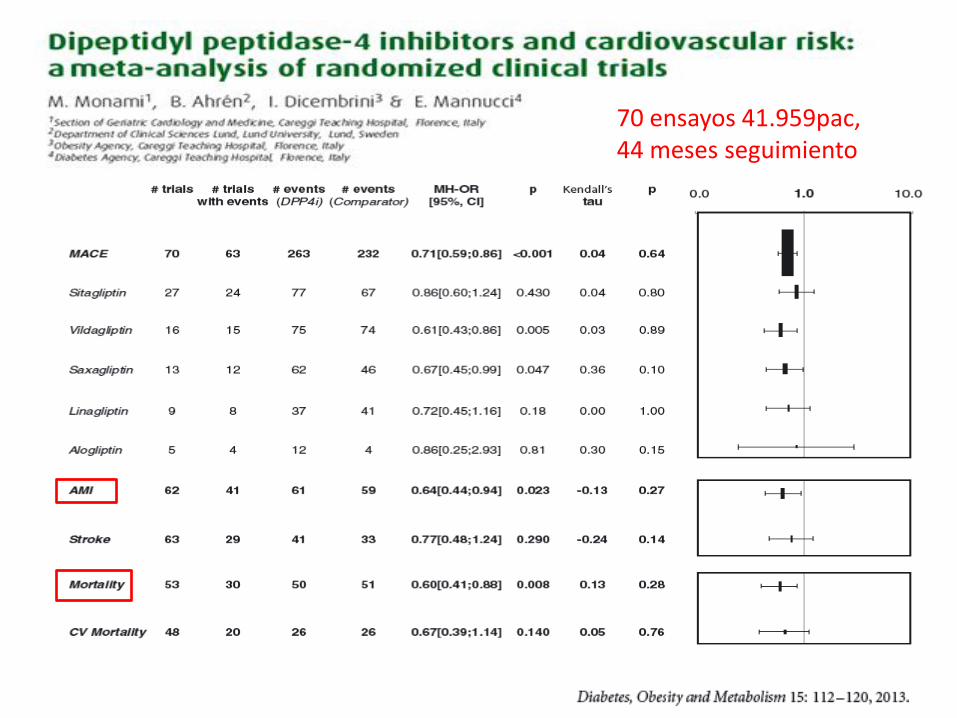
70 ensayos 41.959pac, 44 meses seguimiento
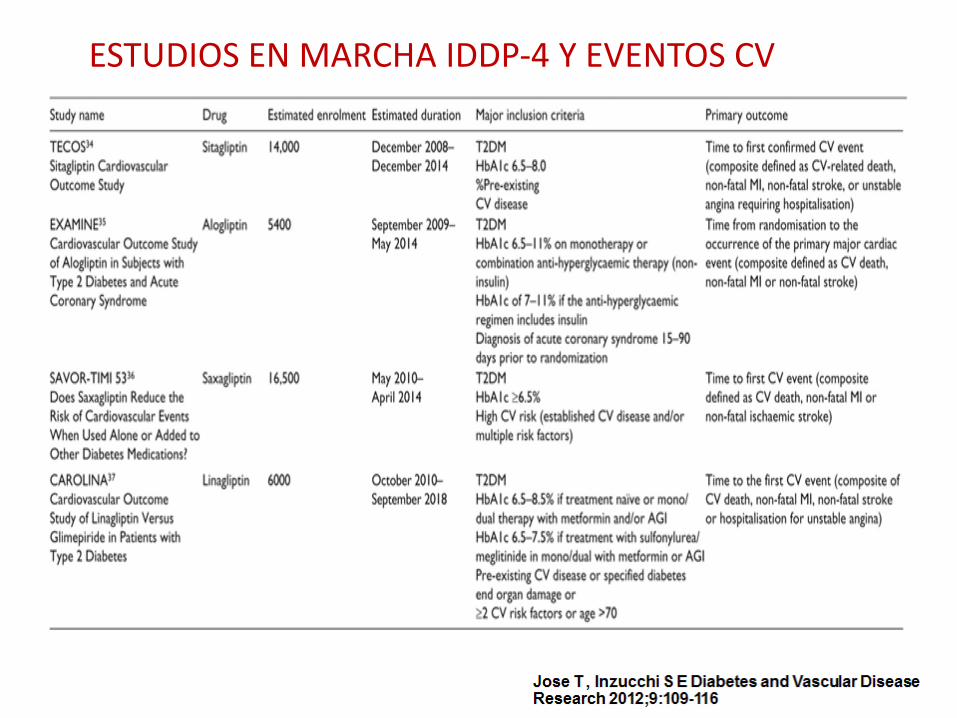
ESTUDIOS EN MARCHA IDDP-4 Y EVENTOS CV