Craneofaringeomas Resultados de Tratamiento Feb 2012

of 12
-
Upload
lilian-maldonado -
Category
Documents
-
view
217 -
download
0
Transcript of Craneofaringeomas Resultados de Tratamiento Feb 2012
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
1/12
J Neurosurg / Volume 116 / February 2012
J Neurosurg 116:373384, 2012
373
C
RANIOPHARYNGIOMA treatment remains a challeng-ing problem in neurosurgery. Due to involvement
of the hypothalamus and ophthalmological andendocrine systems, resection of these lesions is associ-ated with either higher rates of mortality3,5,15,19,34,40,52andrecurrence3,6,15,18,21or a low rate of GTR.1,14,15,21,24,29,31,50,51Obviously, this results in a debate about the optimal treat-ment strategy.21,39A more conservative treatment strate-gy2,9consisting of cyst puncture and insertion of a cysto-ventricular shunt was introduced to avoid damage to thepituitary stalk and the hypothalamus. While this strategyled to improvement in clinical symptoms,9,12,20additionaltreatment, such as radiotherapy,13,39,41,43became necessary
to avoid further tumor growth. Recently, intracavitary ir-radiation (in cystic lesions)16,22,23,53and radiosurgery8,27,36,46
have each been used as sole treatments. Some surgeons,however, believe that radical tumor removal, if possi-ble, is essential for avoidance of tumor regrowth, whichwould cause new and more severe endocrine, ophthal-mological, and neuropsychological decits. Until nowthe rate of GTR could be improved, but some of the re-sults remained unsatisfactory, especially in respect to thetranscranial approaches.33,40,44,45,48,50Moreover, in patientstreated with GTR, the rates of postoperative endocrinedecits5,15,19,24,40,44,47,50,54increased, as important structureslike the pituitary stalk had to be deliberately sacriced.
In 1999, the senior author published his results ofcraniopharyngioma surgery in a rst study, including all
patients treated between 1983 and 1997.
12,19
During that
Results after treatment of craniopharyngiomas: further
experiences with 73 patients since 1997
Clinical article
BERNDM. HOFMANN,M.D.,1,2ANKEHLLIG,M.D.,1CHRISTIANSTRAUSS,M.D., PH.D.,2ROLFBUSLEI,M.D., PH.D.,3MICHAELBUCHFELDER,M.D., PH.D.,1ANDRUDOLFFAHLBUSCH,M.D., PH.D.1,4
Departments of 1Neurosurgery and 3Neuropathology, University of Erlangen-Nuremberg, Erlangen;2Department of Neurosurgery, University of Halle; and 4International Neuroscience Institute,
Hannover, Germany
Object.The authors report surgical and endocrinological results of a series of 73 cases of craniopharyngiomathat they treated surgically since 1997 to demonstrate their change in treatment strategy and its effect on outcomecompared with a previous series and results reported in the literature.
Methods.A total of 73 patients underwent surgery for craniopharyngiomas between May 1997 and January2005. In patients with poor clinical or neuropsychological condition, even following pretreatment, only stereotacticcyst aspiration took place (8 cases). In the remaining patients, gross-total resection (GTR) was intended and appearedto be possible. The most frequent approaches were subfrontal (27 cases) and transsphenoidal (26 cases); in somecases, a multistep approach was used. The rate of GTR, complications, and functional outcome (comparing pre- andpostoperative endocrine and neuropsychological testing) were evaluated. The mean duration of follow-up was 25.2months.
Results.Gross-total resection was achieved in 88.5% of cases in which a transsphenoidal approach was used and79.5% of those in which a transcranial approach was used (85.2% of those in which a subfrontal approach was usedand 72.7% of those in which a frontolateral approach was used). In the total series, GTR was achieved in 83.1% ofcases (vs 49.3% in the authors former series). The complication rate was 13.8% without any mortality. New endo-crine decits were observed more frequently in patients treated with transcranial approaches over the years (16.3%66.7% vs 2.6%50.0%) but were less frequent after transsphenoidal approaches (5.2%19.2% vs 2.9%45.7%).
Conclusions.Open surgery with intended total resection remains the treatment of choice in most patients. Initialstereotactic cyst aspiration or medical pretreatment to improve the patients condition and adequate choice of surgicalapproach(es) are essential to achieve that goal. Nevertheless, a moderate increase in endocrinological decits has tobe accepted. The authors recommend using radiotherapy only in cases in which there are tumor remnants or diseaseprogression after surgery. (DOI: 10.3171/2011.6.JNS081451)
KEYWORDS craniopharyngioma transsphenoidal surgery transcranial surgery endocrinological outcome
neuropsychological outcome oncology
373
Abbreviation used in this paper:GTR = gross-total resection.
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
2/12
B. M. Hofmann et al.
374 J Neurosurg / Volume 116 / February 2012
period, MR imaging became the standard method for di-agnosis, leading to a more precise assessment of tumorextension and facilitating the choice of surgical approach.Furthermore, improvement of surgical dissection tech-niques and technical advances, such as endoscopy, neu-ronavigation, and intraoperative MR imaging, can help toavoid leaving residual tumor and offer new tools for con-trol of tumor removal. As a result of experience with ear-lier cases and changes in technology, our surgical strategyhas changed. Our current strategy is to undertake surgerywith the goal of totally removing the tumor and avoid-ing recurrence; we choose the surgical approach with thisgoal in mind, independent of the risk of subsequent en-docrine decits because adequate substitution therapy isrelatively easy nowadays. Nevertheless, care is taken notto cause any new ophthalmological or neuropsychologi-cal decits, and optimizing the patients condition prior tosurgery is essential for this kind of treatment.
The aim of this study is to demonstrate our short-term results of craniopharyngioma surgery following our
modied treatment protocol and to compare them withour previous results and with the literature.
Methods
Patient Population
From May 1997 to January 2005, 73 patients suf-fering from a newly diagnosed craniopharyngioma weretreated at the University of Erlangen-Nuremberg. Someof the patients were referred to the study hospital becausethey were considered to be difcult to treat in their lo-cal neurosurgical department. Total tumor removal wasintended in 65 cases. The patient group consisted of 42males and 31 females (male to female ratio 1.35:1). Theage of the patients at the time of the initial operationranged from 3 to 80.2 years (mean 35.1 years).
Open surgery was performed at the Department ofNeurosurgery; stereotactic cyst aspirations were eitherperformed by the Department of Neuroradiology underCT guidance or by using neuronavigation and intraopera-tive MR imaging to localize the position of the catheter.None of the patients had undergone previous radiothera-py, and only 1 patient underwent stereotactic cyst aspira-tion at another hospital before major surgery. In 23 pa-tients, a multistep approach consisting of a combinationof different surgical approaches was performed, mainly
by the senior author (R.F.).Neuroradiological Workup
In all patients, preoperative plain skull radiographswere obtained, either for intraoperative orientation duringtranssphenoidal surgery or for surgical planning with re-gard to the frontal sinuses. In all patients, an MR imagingscan (Siemens Magnetom GBS2 and Magnetom Sonata1.5 T, Siemens AG) was routinely used for imaging of thetumor size and location. Coronal and sagittal thin-slice(1- to 2-mm) T1-weighted (TR 600 msec, TE 20 msec,256 512 pixels, FOV 22 22 cm) contrast-enhanced andunenhanced images and T2-weighted (TR 3850 msec, TE111 msec, 256 512 pixels, FOV 22 22 cm) images were
obtained. The largest diameter of the tumor was deter-mined and used for classication. To detect calcications,in most patients, thin-slice CT scans (Siemens SomatomDRH and Somatom Plus4, Siemens AG) with bone win-dows (120 kV, 300 mAs, kernel H70s) were performed inaxial planes, and a coronal reconstruction was calculated.
In 32 cases, intraoperative MR images were obtained(using a 0.2-T Siemens Magnetom open unit in 15 casesand a 1.5-T Siemens Magnetom Sonata in 17) to deter-mine the extent of tumor removal. If a tumor remnant wasidentied, further resection followed.37
Ophthalmological Evaluation
The visual acuity was determined and perimetry andfundoscopic examinations were performed by the De-partment of Ophthalmology of the University of Erlan-gen-Nuremberg preoperatively, about 1 week postopera-tively, 3 months postoperatively, and annually thereafter.
Endocrinological Evaluation
All patients underwent a standardized endocrinologi-cal evaluation. Routinely, a stimulation test of the pituitaryadrenal axis was performed by administering ACTH anddetermining the serum cortisol levels. The basal serumlevels of the remaining pituitary hormones (prolactin,growth hormone, thyroid-stimulating hormone, luteiniz-ing hormone, and follicle-stimulating hormone), as wellas the serum levels of thyronine and thyroxin, testoster-one, and estradiol were determined preoperatively. Inaddition, in 34 patients, hypoglycemia was induced byinsulin administration, and cortisol and growth hormoneserum levels were measured to evaluate somatotroph andcorticotroph function. Posterior pituitary function was
evaluated by measurement of uid intake and output be-fore and after surgery and by determination of the specif-ic gravity of the urine. In some cases, an additional waterdeprivation test was performed. During the rst 10 post-operative days, serum electrolyte balance and osmolaritywere determined. If there was any sign of deciency, thepatient was treated with replacement therapy. Gonado-tropin levels were not determined preoperatively in 8 orpostoperatively in 9 children because of the young age ofthese patients. The somatotropic axis was not evaluatedin 19 patients preoperatively and in 17 patients postopera-tively either because testing was not possible due to thepatients clinical condition or because of older age.
Details regarding the endocrine function tests aregiven elsewhere.10
Neuropsychological Workup
Neuropsychological testing included a cognitive per-formance test for memory, a memory span test similar tothe WAIS-R subtest,49 a verbal intelligence test (Mehr-fach-Wortschatz-Intelligenztest),32and, in some cases, theTrail Making Test.42
Treatment Strategy
A graduated treatment strategy was applied. First,hormone replacement therapy was initiated if required,and external ventricular drainage or a ventriculoperito-
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
3/12
J Neurosurg / Volume 116 / February 2012
Results of craniopharyngioma surgery
375
neal shunting was performed in patients exhibiting hy-drocephalus. After that, special attention was paid tothe clinical and the neuropsychological condition of thepatient. Patients with a large cystic tumor and poor gen-eral clinical condition, especially with hypothalamicsymptoms like a disturbed sleep-wake rhythm or severeshort-term memory disturbances, were not consideredto be suitable candidates for extended transcranial sur-gery. A severe paratumorous edema with hypothalamicdamage was also considered a contraindication for ma-jor surgery. In the latter situation, medical pretreatmentwith corticosteroids was immediately started. In patientswith large cystic tumors, stereotactic cyst aspiration andcystoventricular shunting were performed as the primarytreatment. In these cases, neuropsychological testing wasused to document the patients course, and surgery wasonly considered if conditions such as sleep-wake rhythmdisturbances and hyperphagia resolved and others, suchas memory disturbances, improved. If the patients condi-tion did not improve, a more conservative treatment con-
sisting of radiotherapy was applied.Depending on the tumor size and location, a trans-sphenoidal, frontolateral, or subfrontal approach wasused (described below). As we found that the subfrontalapproach provides a better overview of the surgical eld,we preferred this approach. If the tumor could not be re-moved in 1 session, another surgical approach was car-ried out in a separate operation.
Radiotherapy was applied following successful ste-reotactic cyst evacuation in older patients or those withnonresolving hypothalamic decits. Fractional conformalor stereotactic fractionated radiotherapy was only appliedwhen there were tumor remnants with evident growth andrepeat surgery was not applicable. The same is true for
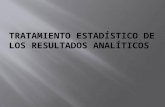
radiosurgery and capsule remnants.The detailed treatment strategy is depicted in Fig. 1.
Surgical Procedures
Pure stereotactic cyst aspiration was performed in 8patients due to nonresolving hypothalamic decienciesand/or patient age.
A transsphenoidal approach was chosen in 23 pa-tients harboring a subdiaphragmatic tumor arising fromthe pituitary fossa in whom there was intrasellar or su-prasellar invasion related to a large sellar entrance. Anextended transsphenoidal approach with removal of thetuberculum sellae and section of the intercavernous si-
nus26,30was carried out in 3 patients in whom a small partof the tumor extended above the planum sphenoidale. In2 of these 26 patients, stereotactic cyst aspiration was per-formed before the transsphenoidal surgery.
Major suprasellar calcications were considered con-traindications for transsphenoidal surgery.20In the eventof perforation of the sellar diaphragm, perioperative lum-bar drainage was placed, and the sellar oor was packedwith fascia lata and fat and nally sealed with brin glue.The latter was especially important in case of a 2-stepstrategy.
A frontolateral approach was used in 11 patientssuffering from a small suprasellar tumor. In 3 of thesepatients, stereotactic cyst aspiration was performed prior
to surgery; in 2 who were suffering from an intra- andsuprasellar tumor, a combination frontolateral and trans-sphenoidal approach was performed. A limitation of thefrontolateral approach is that larger retrosellar and intra-ventricular parts of the tumor may not be adequately vi-sualized.
The subfrontal interhemispheric midline approachwas used in 27 patients. Stereotactic cyst aspiration wasperformed preoperatively in 15 of these cases. In 1 case,this approach was combined with a transsphenoidal onebecause the tumor had invaded the sella. As an advantageof this approach, the lamina terminalis may be opened incase of tumor invasion into the third ventricle. The tumoris easily debulked and its capsule removed.
In the remaining patient, a transventricular approachwas performed following stereotactic cyst aspiration. Inthis case, the tumor had developed within the third andthe lateral ventricles, and the foramen of Monro was en-larged but blocked.
In cases in which multistep approaches were per-
formed, the intervals between the procedures rangedfrom a few days to months depending on the patientscondition. We never performed a combination of the pro-cedures on a single day. In most cases in which stereo-tactic cyst aspiration was performed, a cystoventricularshunt was placed, and this had to be removed during themajor procedure.
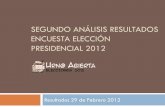
Additional details about the surgical procedures aredescribed elsewhere.11The tumor extensions and the dif-ferent approaches chosen are outlined in Fig. 2.
Denition of Surgical Outcome
Gross-total resection was achieved if tumor or cap-sule remnants were not visible during inspection of thesurgical eld or during imaging performed intraopera-tively or 3 months following surgery.
Histological Evaluation
Histological evaluation was performed by the De-partment of Neuropathology (R.B.), University of Erlan-gen-Nuremberg, to conrm the diagnosis of craniopha-ryngioma in all patients. A clear differentiation betweenadamantinomatous or papillary type was made in all but7 cases.
Follow-Up Examination
Routine postoperative follow-up examinations were
performed 3 months, 1 year, and then every 2nd year (bi-ennially) at our department. These examinations includeMR imaging and determination of the basal serum levelsof the pituitary hormones after an overnight fast. Oph-thalmological examinations were performed at outsideinstitutions, usually annually. The mean follow-up periodin all patients was 25.2 months (range 383 months), 4patients were lost to follow-up immediately followingsurgery, and 1 patient was lost to follow-up 3 months af-ter surgery. Even if this period is very short to evaluaterecurrence rates, it is sufcient for evaluation of endo-crine decits because they occur immediately followingsurgery and normally do not improve after 3 months post-operatively.
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
4/12
B. M. Hofmann et al.
376 J Neurosurg / Volume 116 / February 2012
Results
Presenting Symptoms
The most frequent presenting symptoms were oph-thalmological decits, which occurred in 39 patients(53.4%), and endocrine decits, which occurred in 26(35.6%). Another major complaint was headache (occur-ring in 14 patients [19.2%]); less frequent were neuropsy-chiatric decits (in 11 patients [15.1%]), hydrocephalus(in 5 [6.8%]), and neurological decits (in 2 [2.7%]). Fur-thermore, seizures, meningitis, and coincidental ndingswere observed in 1 patient each (1.4%).
On the basis of neuroradiological examination, thetumors were classied into 4 size categories: Group A,patients with tumors smaller than 2 cm in maximum di-ameter; Group B, those with tumors 23 cm; Group C,those with tumors 34 cm; and Group D, those whose tu-
mors had a maximum diameter greater than 4 cm. Patientdistribution among these groups was as follows: Group A,31 patients (42.5%); Group B, 21 patients (28.8%); Group
C, 11 patients (15.0%); and Group D, 10 patients (13.7%).In the overall study population (73 patients), the tumorsize ranged between 13 and 70 mm (mean 27.3 mm). Inpatients operated on via a subfrontal route, it ranged be-tween 15 and 70 mm (mean 33.0 mm), and in patientsoperated on via a frontolateral approach, between 16 and55 mm (mean 25.2 mm); this difference was only slightlysignicant (p = 0.049, Student t-test). Twenty-eight pa-tients (38.4%) harbored a predominantly cystic tumor,1 patient (1.3%) a mainly solid tumor, and 44 patients(60.3%) a mixed-type tumor. The size of predominantlycystic tumors ranged from 32 to 70 mm (mean 26.3 mm)and that of mixed-type tumors from 15 to 60 mm (mean28.2 mm); this difference was not statistically signicant
FIG. 1. Surgical strategy and decision-making algorithm for the treatment of craniopharyngiomas.
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
5/12
J Neurosurg / Volume 116 / February 2012
Results of craniopharyngioma surgery
377
(p = 0.27). Calcication of the tumor was found in 31 pa-tients (42.5%).
In 1 patient, the tumor was purely intrasellar, in 26patients it was intra- and suprasellar, in 7 it was suprasel-lar with depression of the diaphragm into the sella, and in31 it was purely supradiaphragmatic. The tumor locationwas purely extraventricular in 44 patients and both intra-and extraventricular in 23 patients.
Surgical Results
Detailed surgical results are given in Table 1.Transsphenoidal surgery resulted in GTR in 23
(88.5%) of 26 patients, including 3 patients who under-went an extended approach. Capsule remnants xed tothe optic chiasm had to be left behind in 3 patients. Re-currence has been observed in 1 case as of this writing.
A frontolateral approach resulted in GTR in 8 (72.7%)of 11 patients. Capsule remnants had to be left behind in2 cases. In 1 other case, due to the patients preoperativecondition, only fenestration of the cystic tumor was pos-sible. As of this writing, a recurrence has been observedin 1 patient treated with a frontolateral approach.
A subfrontal approach resulted in GTR in 23 (85.2%)of 27 patients. In 1 patient, only incomplete resection waspossible via a subfrontal approach, and further transven-tricular surgery was scheduled; the transventricular sur-
gery was not performed, however, due to deterioration ofthe patients neuropsychological status. In another 2 pa-tients, capsule remnants were left behind, and in 1 patient,a tumor remnant was misinterpreted as a blood clot on theintraoperative images and was left behind. Recurrencehas been observed in 3 patients treated with a subfrontalapproach.
A transventricular approach was applied in 1 patient.He was scheduled for further surgery, but it was not car-ried out within the study period. (During the followingsubfrontal interhemispheric midline approach, the tumorwas removed completely.)
In summary, following transcranial surgery, GTRwas achieved in 31 (79.5%) of 39 patients.
Applying our modied treatment strategy, in 54(83.1%) of 65 patients suitable for open surgery, GTR wasachieved. A combination of 2 open surgical approacheswas applied in 3 cases leading to GTR. In 75% of thecases (15 of 20), GTR was achieved by combining stereo-tactic cyst aspiration and open surgery.
Gross-total resection was possible in 81.5% (22 of27) of the cystic and 83.8% (31 of 37) of the solid tumors.
In the total series, complications were observed in9 cases (complication rate 13.8%). Four patients suffer-ing from CSF leakage (6.2%) required further surgicaltreatment; severe sinusitis, wound healing problems, and
meningitis each occurred in 1 patient (1.5%). Two patients(3.1%) experienced a deterioration of visual function.Stratied by type of surgery,the complication rates
were 11.5% (3 of 26 cases) for transsphenoidal surgeryand 15.4% (6 of 39 cases). In the 26 patients treated withtranssphenoidal surgery alone, there were 2 cases of CSFleakage (7.7%) and 1 case of meningitis (3.8%). Followingtranscranial surgery, CSF leakage was observed in 2 cases(5.1%), in one of them following a combined transcranialand transsphenoidal approach. Furthermore, sinusitis andwound healing problems were each observed in 1 patient(2.6%). The sinusitis was observed after a combined sub-frontal and transsphenoidal approach. In 1 patient treatedvia a subfrontal interhemispheric approach, vision in theright eye deteriorated from normal preoperatively to per-ception of light postoperatively, whereas the vision in theother eye improved from 0.6 to 1.0. Another patient, whowas treated via a combined subfrontal and transsphenoi-dal approach, experienced bitemporal hemianopsia anddeterioration of vision in 1 eye from 0.8 to 0.5.
Treatment of Recurrent and Residual Tumors
Three patients were lost to follow-up either after re-operation due to recurrence or after the diagnosis of arecurrent tumor or a capsule remnant was made. Con-ventional radiation therapy was performed in 1 patientfollowing tumor recurrence and in 3 patients following
FIG. 2. Criteria for choice of adequate approach, showing tumor extension according to MR imaging (upper row)and thecorresponding approaches (lower rows).
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
6/12
B. M. Hofmann et al.
378 J Neurosurg / Volume 116 / February 2012
stereotactic cyst aspiration as sole treatment. Shaped-beam radiosurgery was applied in 5 patients, in 3 of themfollowing incomplete tumor removal, in 1 case after re-currence, and in another following stereotactic cyst as-piration. Remarkably, shaped-beam radiosurgery led to adecrease in tumor size in 1 patient who underwent incom-plete resection.
Endocrinological Outcome
Reviewing the pre- and postoperative endocrinedecits, a deterioration of pituitary function could beobserved following transcranial and transsphenoidal sur-gery (Figs. 3 and 4).
Following surgery, either no new decit or an im-provement of a separate pituitary axis was observed in33.4% of the patients suffering from a cystic tumor andin 32.5% of patients harboring a mixed-type tumor. In-terestingly, in 51.7% of the patients with the smallest tu-mors (Group A), no new decits were seen; some of thesepatients even experienced an improvement in endocrinefunction. The second-best result was achieved in Group
D (44.4% experienced either improvement or no change).In Group B, 15.8% of the patients exhibited no changeof their preexisting endocrine decits, and all patients inGroup C developed at least 1 new decit. There was nocorrelation regarding the rates of preoperative decits be-tween the different tumor groups (no decit: A 29.0%,B 28.6%, C 27.3%, D 30.0%). Of patients with suprasel-lar tumor origin, only 23.7% exhibited no new endocrinedecit following surgery, whereas 48.1% of the patientsin whom the tumor origin was intrasellar experienced nonew endocrine decit.
Following transsphenoidal surgery, a signicant de-terioration of the preoperative function was found in allaxes (p
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
7/12
J Neurosurg / Volume 116 / February 2012
Results of craniopharyngioma surgery
379
of patients after transcranial surgery. New insufciency of
adrenal function was observed in 56.5% of the cases, newthyroid insufciency in 30.8%, new gonadal insufciencyin 24.3%, and new insufciency of the somatotrophaxisin 16.3% of all cases operated on via a transcranial route.New hyperprolactinemia occurred in 5.2% of cases (Fig.4). All of the above-described functions deteriorated sig-nicantly following surgery (p
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
8/12
B. M. Hofmann et al.
380 J Neurosurg / Volume 116 / February 2012
troph function (p = 0.026, chi-square test). Surprisingly,
there was no signicant difference with respect to thyroidfunction (p = 0.300, chi-square test) or somatotroph func-tion (p = 0.267, chi-square test).
Ophthalmological Outcome
In 57.7% of the patients who underwent transsphe-noidal surgery, there was a preexisting ophthalmologicaldecit. In those patients, total recovery following surgerywas observed in 40.0%, an improvement was found in33.3%, and no change was found in 26.7%. An ophthal-mological decit was preexisting in 89.7% of the patientswho underwent transcranial surgery. In those patients,total recovery following surgery was observed in 34.3%,
improvement of vision or visual eld was seen in 54.3%,and no change was observed in 5.7%. In 2 patients (5.7%),unfortunately, deterioration was observed.
Neuropsychological Outcome
Not surprisingly, neuropsychological decits weremore frequent in patients with larger tumors (Group A3.2%, Group B 14.3%, Group C 28.2%, and Group D90.0%). Neuropsychological decits were more frequentin patients with cystic tumors than in those with mixed-type tumors (21.4% vs 18.2%).
Neuropsychological decits were observed in 9 pa-tients (23.1%) who underwent transcranial surgery but in
none who underwent transsphenoidal surgery. As neu-ropsychological decits appeared mostly in associationwith giant craniopharyngiomas, the outcome is describedelsewhere.11
Discussion
This large series reects our experience gained dur-ing the last 10 years, using a modied strategy in which thesurgical approach was chosen on the basis of MR imag-ing ndings, and the patients clinical condition was opti-mized before surgery. Open surgery is avoided in patientssuffering from hypothalamic decits or hydrocephalus. Ifthose conditions are resolved, surgery is undertaken with
the intention of total tumor removal. During this surgery,
it is important to avoid extensive maneuvers leading toadditional ophthalmological or cognitive and neuropsy-chological decits, although new endocrine disturbancesare accepted to achieve GTR. Six authors5,9,12,24,29,47haverecently reported larger series, but some of these spanneda very long period. As conditions in surgery have changedover the years, these series, as well as the older ones,30,43,52cannot be compared in detail.
In this series, surgical results for GTR improved incomparison with our earlier series; however, endocrineresults deteriorated, an experience that should be evalu-ated critically in the context of results reported in the lit-erature.
Rate of GTR
In the presented study, the rate of GTR was 83.1%(54/65). As expected, the GTR rate was lower in predomi-nantly cystic tumors because the thin capsule is difcultto remove radically. If the rates of GTR following trans-sphenoidal, frontolateral, and subfrontal approaches arecompared, the best rate is achieved by transsphenoidalsurgery (88.5%); however, the tumors removed via thisapproach were the smallest ones and were less adher-ent to important intradural structures. Among the morecommon suprasellar tumors, the subfrontal approach isassociated with a higher success rate, with GTR achieved
in 85.2% of the cases, whereas the frontolateral approachled to a GTR in 72.7%. The former approach should bepreferred for that reason.
The rates achieved with transsphenoidal surgery arecomparable to those reported in the literature, which varybetween 25%38 and 90%;5 in the current literature, therates vary between 63.2% and 90.0%.5,12,24,33,54The lowerrates are mainly caused by an effort of the surgeon to pre-serve pituitary function, as reported by Abe and Ldecke,1who achieved GTR in only 27.3% of patients in their caseseries, accepting a higher risk of tumor regrowth.
For transcranial surgery, a rate of GTR as low as15%24 has been reported, but in general, the rates varybetween 50%3 and 90%17 and are fairly comparable to
FIG. 5. Endocrine function in patients treated via different transcranial approaches. Left:Comparison of pre- and postopera-tive endocrine deficiencies in patients treated via subfrontal and frontolateral approaches. Right: Incidence of new endocrinedeficiencies stratified by approach. DI = diabetes insipidus; COR = cortisol; TSH = thyroid stimulating hormone; GON = gonado-tropins; PRL = prolactin; GH = growth hormone.
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
9/12
J Neurosurg / Volume 116 / February 2012
Results of craniopharyngioma surgery
381
the one (79.5%) reported in this series. Regarding fronto-lateral approaches, GTR rates of 31.2%15and 83%34havebeen reported; regarding the subfrontal approach, ratesof 58.8%12and 71.0%44have been reported. As the GTRrate of 85% that we achieved with a subfrontal interhemi-spheric approach is comparable to rates reported in theliterature, this approach should be favored.
In summary, the results achieved in this series arecomparable to or better than those reported in the mostrecent papers (GTR rates between 82% and 92%).2,39,40,47Our results improved from 49.3%12in our earlier series to83.1% in the current series, an improvement that supportsour latest treatment strategy.
Complications
Our strategy of pretreating patients either by stereo-tactic cyst aspiration or with dexamethasone therapy toimprove their clinical condition has been associated withno patient deaths thus far.
The complication rate for our total series (13.8%) isat the lower range compared with all complication ratesgiven in the literature5,6,9,15,21,29,33,39,40,47 (range 8.3%48 to33.3%40). One typical complication is CSF leakage, whichis reported in up to 19.4% of these cases.7We observedthis phenomenon in 5.1% of cases after transcranial sur-gery and in 7.7% of cases after transsphenoidal surgery,and it was the most common complication in our series.Interestingly, in most series reporting higher rates ofGTR, morbidity and mortality rates are higher as well.
Endocrine Outcome
Because the percentage of patients without any pre-operative decit is not dependent on tumor size, it is sur-
prising that the best results with respect to avoidance ofnew endocrine decits are observed in very small but alsoin very large tumors. The cystic or solid behavior of thetumor does not inuence the endocrine outcome, but thetumor origin does. The higher rate of new decits may beattributed to the (partial) resection of the pituitary stalkin larger tumors and in tumors with a suprasellar origin.
The overall number of patients who experienced adecit following transsphenoidal surgery was lower thanin our former series,12possibly due to the lower numberof preexisting decits (Fig. 3). In contrast, the rate of sur-gery-related deterioration of anterior lobe function washigher than reported in the earlier publication. A reason
for the worse results might be our more aggressive treat-ment strategy of resecting the capsule remnants from theanterior pituitary body.
After transcranial surgery, the results of endocrinefunction were moderately worse than in our former series(Fig. 4). Undertaking surgery with the intention of achiev-ing total tumor removal results in a more aggressive resec-tion of tumor parts adherent to the pituitary stalk, whichwould explain the worse results with respect to endocrinefunction. The slightly higher number of new decits inthe group of patients treated via a subfrontal approach incomparison with the ones treated via a frontolateral ap-proach might be explained by the slightly larger diameterof the tumor in the former group. As manipulation of im-
portant structures, especially the hypothalamus and thepituitary stalk, results in a higher number of endocrinedecits, especially diabetes insipidus (Fig. 5), it is not sur-prising that the rate of new endocrine decits is highestin patients with a suprasellar tumor origin. In contrast,amelioration of hyperprolactinemia will be observed inpatients with smaller tumors following decompression ofthe pituitary stalk. Fingerlike tumor growth toward thebrain parenchyma or the hypothalamus will make com-plete removal more difcult as well.35
Reviewing the literature, our results regarding newendocrine deciencies are comparable to or better thanthose previously published.46,15,24,25,29,39,44,47,48 Further-more, 1 study48reported that there was no difference inpituitary deciency whether complete tumor removal wasachieved or not. Compared with adenoma surgery, it hasto be emphasized that there is a difference regarding theendocrine outcome in craniopharyngiomas. As the softadenomatous tissue can easily be removed, ameliorationof endocrine function is observed more often in patients
who undergo surgery for treatment of ademomas.Neuropsychological Results
Our policy of only performing open surgery in pa-tients without neuropsychological decits is supportedby the literature.9,29,39,40,48 The reported rates of newlydiagnosed neuropsychological decits range from 11.7%to 50%. This depicts worse results than reported in ourseries. As neuropsychological deciencies occur mainlyin patients with giant craniopharyngioma, the results arediscussed elsewhere.11
Value of the Multistep Procedure
Because we did not observe any severe and long-last-ing deterioration of neuropsychological decits followingopen surgery, in our opinion, it is necessary to pretreatpatients with those decits, and open surgery should beperformed only if those decits resolve. As we did notobserve a signicantly higher rate of new ophthalmologi-cal deciencies, we propose to perform GTR wheneverpossible.
Choice of Approach
In our current protocol, the decision to perform opensurgery depends on the clinical condition of the patient.This is based on our earlier experience of unfavorable
outcomes in patients with a preexisting hypothalamicdisturbance. If a patients clinical condition is poor orthere are any preoperative symptoms of a hypothalamicdisturbance, cyst evacuation, medical pretreatment, orCSF shunting is performed rather than open surgery withintention of total tumor removal. If open surgery is to beperformed, collapse of the cyst following aspiration al-lows less dangerous manipulation at the optic system andimprovement of neuropsychological decits as the tensionat those important structures is decreased.
Although in the former series of the senior author,12the frontolateral approach was most frequently used(39.2%) followed by the transsphenoidal one (23.6%), wehave now changed our strategy, as the results with respect
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
10/12
B. M. Hofmann et al.
382 J Neurosurg / Volume 116 / February 2012
to GTR seemed to be better following a subfrontal ap-proach. As a consequence, in this series, the subfrontal ap-proach was the one most used (in 37.0% of cases [27/73]),followed by the transsphenoidal approach (35.6%), where-as the frontolateral approach (15.1%) played a minor role.
In contrast to the literature,47in which about 10% ofall craniopharyngiomas are described as being treatedvia a transsphenoidal route, we performed transsphenoi-dal surgery in 35.6% of all our patients, as even a smallsella allows an (extended) transsphenoidal approach inselected cases. This strategy results in a higher rate ofGTR and a lower risk of new endocrine decits, which isin contrast to the results of our earlier series,19 in whichwe found that diabetes insipidus was observed in a com-parable number of cases whether a transsphenoidal or atranscranial approach was applied.
The increase in the rate of endocrine decits asso-ciated with a transcranial approach was accepted as therate of GTR increased. However, sufcient replacementtherapy has to be ascertained.
Comparison with Gamma Knife Surgery, ConventionalRadiotherapy, and Intracavitary Radiation Therapy
Comparison between surgical treatment and radio-therapy remains difcult as the literature to date includesdifferent types of pituitary tumors and is not focused oncraniopharyngiomas.
The overall rate of GTR reported in this study (83.1%)favors surgical treatment over radiotherapy. FollowingGamma Knife surgery, lfarsson et al.46observed a de-crease in tumor size in 22.7% of cases and an increasein 63.3%. Chung et al.8found a response to radiosurgeryin 64.6% and an increase of tumor size in 12.9% of allexamined cases. Kobayashi and colleagues reported thebest results following stereotactic Gamma Knife Surgeryin craniopharyngiomas. In 1 series,28they report a tumorshrinkage of 70%, whereas in another series,27they reporta complete or partial response of the tumor to radiosur-gery in 63% of cases but also a progression in 23% ofcases.
In the present study, the endocrine outcome did notimprove following open surgery, and the rate of patientssuffering from a deterioration was higher than reported inthe literature for radiotherapy. Depending on the differenthormones, the rate of new endocrine decits reported inthis study ranges between 19.2% and 66.7%. In an Ameri-can survey of pediatric neurosurgeons,43the rates of en-
docrine decits following radical surgery and decompres-sive surgery followed by radiotherapy were comparable(95% vs 94%) but even higher than reported in this series,indicating that less aggressive surgery does not lead tobetter results. Following radiosurgery, in 1 study,8an im-provement of diabetes insipidus was found in 36.4% ofthe cases. In another series, an improvement of endocrinefunction was observed in 18.7% and a deterioration in16.5%.27,28
Compared with results following intracavitary ra-diation, endocrine results following surgery are worse(66.7% vs 29.0%).16However, in the latest literature, tu-mor progression was reported in 70% of cases,54and in-tracavitary radiation therapy does not seem to have any
signicant benet to solid tumors.23Furthermore, we didnot observe any hypothalamic decit following surgerycompared with 3.2% following intracavitary radiation.22This has to be considered as an advantage of surgicaltreatment and justies acceptance of a higher rate of newendocrine decits.
In summary, the rate of new endocrine decits is low-er following radiation therapy, but the observation timereported in the literature is very short. It remains unclearwhether the rate of new decits will increase with a lon -ger follow-up period once the full effect of radiation be-comes apparent. Given that adequate replacement therapyfor endocrine deciencies is available, improvement of vi-sion and neuropsychological decits is more important.For that reason, we support considering surgery as therst treatment option and believe that radiotherapy shouldbe performed only if patients are not suitable candidatesfor extended surgery.
ConclusionsThis study conrms that surgery with intent of total
tumor removal performed as a multistep treatment re-mains the rst choice in the treatment of craniopharyn-giomas. However, selection of patients for primary opensurgerykeeping in mind the contraindicationsandpresurgical symptomatic treatment determine not onlythe rate of GTR but also functional results and qualityof life. Hypothalamic deciencies are a key issue in thetreatment of craniopharyngiomas. In patients with pre-existing hypothalamic deciencies, pretreatment (medi-cal treatment or stereotactic cyst aspiration) is performedprior to open surgery because preexisting deciencies
are associated with an increased risk for deteriorationof these functions. Only if a patient does not suffer fromsuch decits, or if they are resolving, is or she considereda suitable candidate for open surgery.
The kind of surgical approach should be consideredseriously. In intra- and suprasellar, as well as certainpurely suprasellar, tumors, the (extended) transsphenoi-dal approach is suitable because it is associated with ahigher rate of good functional outcome. In large supra-sellar tumors, the subfrontal approach is superior to thefrontolateral one with regard to achieving GTR, but it isassociated with a higher rate of new endocrine decits.These decits should be accepted, however, because suf-cient replacement therapy is available and GTR is not
associated with a signicant increase in ophthalmologi-cal or neuropsychological decits. In difcult cases, acombination of several approaches appeared to be useful.Radiosurgery and intracavitary irradiation should not beconsidered as an alternative to surgery even if new endo-crine decits are observed less frequently. This opinion issupported by the fact that improvements of neuropsycho-logical and ophthalmological decits are observed lessfrequently following radiation therapy than after resec-tion, and progression of tumor growth is reported in a sig-nicantly higher number of patients following radiationtherapy. Radiosurgery is used, however, for patients withpostoperative tumor remnants and following stereotacticcyst aspiration if hypothalamic decits do not improve.
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
11/12
J Neurosurg / Volume 116 / February 2012
Results of craniopharyngioma surgery
383
Addendum
In the last 4 years, the senior author (R.F.) has tried success-fully to resect the majority of suprasellar craniopharyngiomas via afrontolateral approach.
Acknowledgments
The authors wish to thank Prof. Naumann, Department of Oph-thalmology, University of Erlangen-Nuremberg, for providing oph-thalmologic examinations; Prof. Saeger, neuropathologist, Marien-hospital Hamburg; Prof. Plate, Prof. Paulus, and Prof. Blmcke,Department of Neuropathology, University of Erlangen-Nuremberg,for histopathological workup; and Prof. Huk and Prof. A. Doerfler,Department of Neuroradiology, University of Erlangen-Nuremberg,for providing MR imaging scans and performing stereotactic cystaspiration. Furthermore, we are indebted to Mr. F. Bittner for provid-ing the illustrations.
Disclosure
Dr. Hofmann has been an employee of Siemens Healthcaresince September 2006 and is currently also acting as a visiting physi-
cian at the Department of Neurosurgery, Klinikum Nrnberg. Thiswork was conducted in conjunction with Dr. Hofmanns universityappointment, however, and Siemens provided no financial supportfor the study nor does the company have any business interest in theresults or topic. (The imaging in this study was routine.) The otherauthors state that they have no conflicts of interest.
Author contributions to the study and manuscript prepara-tion include the following. Conception and design: Hofmann.Acquisition of data: all authors. Analysis and interpretation of data:Hofmann. Drafting the article: Hofmann. Critically revising the arti-cle: Fahlbusch, Strauss, Buchfelder. Statistical analysis: Hofmann.Administrative/technical/material support: Hofmann, Buslei.
References
1. Abe T, Ldecke DK: Transnasal surgery for infradiaphrag-matic craniopharyngiomas in pediatric patients. Neurosur-gery44:957966, 1999
2. Baskin DS, Wilson CB: Surgical management of craniopha-ryngiomas. A review of 74 cases. J Neurosurg 65:2227,1986
3. Blow B, Attewell R, Hagmar L, Malmstrm P, NordstrmCH, Erfurth EM: Postoperative prognosis in craniopharyn-gioma with respect to cardiovascular mortality, survival, andtumor recurrence. J Clin Endocrinol Metab83:38973904,1998
4. Caldarell i M, Massimi L, Tamburrini G, Cappa M, Di RoccoC: Long-term results of the surgical treatment of craniopha-ryngioma: the experience at the Policlinico Gemelli, CatholicUniversity, Rome. Childs Nerv Syst21:747757, 2005
5. Chakrabarti I, Amar AP, Couldwell W, Weiss MH: Long-termneurological, visual, and endocrine outcomes following trans-nasal resection of craniopharyngioma. J Neurosurg 102:650657, 2005
6. Chen C, Okera S, Davies PE, Selva D, Crompton JL: Cranio-pharyngioma: a review of long-term visual outcome. Clin Ex-periment Ophthalmol31:220228, 2003
7. Chen CJ: Suprasellar and infrasellar craniopharyngioma witha persistent craniopharyngeal canal: case report and review ofthe literature. Neuroradiology43:760762, 2001
8. Chung WY, Pan DH, Shiau CY, Guo WY, Wang LW: Gammaknife radiosurgery for craniopharyngiomas. J Neurosurg93(Suppl 3):4756, 2000
9. Duff JM, Meyer FB, Ilstrup DM, Laws ER Jr, Schleck CD,Scheithauer BW: Long-term outcomes for surgically resectedcraniopharyngiomas. Neurosurgery46:291305, 2000
10. Fahlbusch R, Buchfelder M: Tests of endocrine function forneurosurgical patients, in Crockard A, Hayward R, Hoff JT(eds): Neurosurgery: The Scientic Basis of Clinical Prac-tice, ed 3.Malden, MA: Blackwell Science, 2000, Vol 1, pp936945
11. Fahlbusch R, Hofmann BM: Surgical management of giantcraniopharyngiomas. Acta Neurochir (Wien) 150:12131226, 2008
12. Fahlbusch R, Honegger J, Paulus W, Huk WJ, Buchfelder M:Surgical treatment of craniopharyngiomas: experience with168 patients. J Neurosurg90:237250, 1999
13. Fischer EG, Welch K, Shillito J Jr, Winston KR, Tarbell NJ:Craniopharyngiomas in children. Long-term effects of con-servative surgical procedures combined with radiation thera-py. J Neurosurg73:534540, 1990
14. Fisher PG, Jenab J, Gopldthwaite PT, Tihan T, Wharam MD,Foer DR, et al: Outcomes and failure patterns in childhoodcraniopharyngiomas. Childs Nerv Syst14:558563, 1998
15. Gonc EN, Yordam N, Ozon A, Alikasifoglu A, Kandemir N:Endocrinological outcome of different treatment options inchildren with craniopharyngioma: a retrospective analysis of66 cases. Pediatr Neurosurg40:112119, 2004
16. Hasegawa T, Kondziolka D, Hadjipanayis CG, Lunsford LD:
Management of cystic craniopharyngiomas with phospho-rus-32 intracavitary irradiation. Neurosurgery54:813822,2004
17. Hoffman HJ: Surgical management of craniopharyngioma.Pediatr Neurosurg21 (Suppl 1):4449, 1994
18. Hoffman HJ, De Silva M, Humphreys RP, Drake JM, SmithML, Blaser SI: Aggressive surgical management of cranio-pharyngiomas in children. J Neurosurg76:4752, 1992
19. Honegger J, Buchfelder M, Fahlbusch R: Surgical treatment ofcraniopharyngiomas: endocrinological results. J Neurosurg90:251257, 1999
20. Honegger J, Buchfelder M, Fahlbusch R, Dubler B, Drr HG:Transsphenoidal microsurgery for craniopharyngioma. SurgNeurol37:189196, 1992
21. Isaac MA, Hahn SS, Kim JA, Bogart JA, Chung CT: Manage-
ment of craniopharyngioma. Cancer J7:516520, 200122. Julow J, Backlund EO, Lnyi F, Hajda M, Blint K, Nyry I,et al: Long-term results and late complications after intracavi-tary yttrium-90 colloid irradiation of recurrent cystic cranio-pharyngiomas. Neurosurgery61:288296, 2007
23. Julow J, Lnyi F, Hajda M, Szeifert GT, Viola A, Blint K,et al: Stereotactic intracavitary irradiation of cystic cranio-pharyngiomas with yttrium-90 isotope. Prog Neurol Surg20:289296, 2007
24. Karavitaki N, Brufani C, Warner JT, Adams CB, Richards P,Ansorge O, et al: Craniopharyngiomas in children and adults:systematic analysis of 121 cases with long-term follow-up.Clin Endocrinol (Oxf)62:397409, 2005
25. Karavitaki N, Cudlip S, Adams CB, Wass JA: Craniopharyn-giomas. Endocr Rev27:371397, 2006
26. Kato T, Sawamura Y, Abe H, Nagashima M: Transsphenoidal-transtuberculum sellae approach for supradiaphragmatic tu-mours: technical note. Acta Neurochir (Wien)140:715719,1998
27. Kobayashi T, Kida Y, Hasegawa T: Long-term results of gam-ma knife surgery for craniopharyngioma. Neurosurg Focus14(5):e13, 2003
28. Kobayashi T, Tanaka T, Kida Y: Stereotactic gamma radiosur-gery of craniopharyngiomas. Pediatr Neurosurg21 (Suppl1):6974, 1994
29. Larijani B, Bastanhagh MH, Pajouhi M, Kargar Shadab F, Va-sigh A, Aghakhani S: Presentation and outcome of 93 casesof craniopharyngioma. Eur J Cancer Care (Engl)13:1115,2004
30. Laws ER Jr: Transsphenoidal microsurgery in the manage-ment of craniopharyngioma. J Neurosurg52:661666, 1980
-
7/27/2019 Craneofaringeomas Resultados de Tratamiento Feb 2012
12/12
B. M. Hofmann et al.
384 J Neurosurg / Volume 116 / February 2012
31. Laws ER Jr: Transsphenoidal removal of craniopharyngioma.Pediatr Neurosurg21 (Suppl 1):5763, 1994
32. Lehrl S: Mehrfachwahl-Wortschatz-Intell igenztest (MWT-B).Balingen: Perimed-spitta, 1995
33. Maira G, Anile C, Albanese A, Cabezas D, Pardi F, Vignati A:The role of transsphenoidal surgery in the treatment of cranio-pharyngiomas. J Neurosurg100:445451, 2004
34. Maira G, Anile C, Rossi GF, Colosimo C: Surgical treatmentof craniopharyngiomas: an evaluation of the transsphenoidaland pterional approaches. Neurosurgery36:715724, 1995
35. Miller DC: Pathology of craniopharyngiomas: clinical im-port of pathological ndings. Pediatr Neurosurg21 (Suppl1):1117, 1994
36. Mokry M: Craniopharyngiomas: a six year experience withGamma Knife radiosurgery. Stereotact Funct Neurosurg72(Suppl 1):140149, 1999
37. Nimsky C, Ganslandt O, Hofmann B, Fahlbusch R: Limitedbenet of intraoperative low-eld magnetic resonance imag-ing in craniopharyngioma surgery. Neurosurgery53:7281,2003
38. Norris JS, Pavaresh M, Afshar F: Primary transsphenoidalmicrosurgery in the treatment of craniopharyngiomas. Br JNeurosurg12:305312, 1998
39. Pereira AM, Schmid EM, Schutte PJ, Voormolen JH, Bier-masz NR, van Thiel SW, et al: High prevalence of long-termcardiovascular, neurological and psychosocial morbidity af-ter treatment for craniopharyngioma. Clin Endocrinol (Oxf)62:197204, 2005
40. Poretti A, Grotzer MA, Ribi K, Schnle E, Boltshauser E: Out-come of craniopharyngioma in children: long-term complica-tions and quality of life. Dev Med Child Neurol46:220229,2004
41. Regine WF, Mohiuddin M, Kramer S: Long-term results of pe-diatric and adult craniopharyngiomas treated with combinedsurgery and radiation. Radiother Oncol27:1321, 1993
42. Reitan RM, Herring S: A short screening device for identica-tion of cerebral dysfunction in children. J Clin Psychol41:643650, 1985
43. Sanford RA: Craniopharyngioma: results of survey of theAmerican Society of Pediatric Neurosurgery. Pediatr Neuro-surg21 (Suppl 1):3943, 1994
44. Shirane R, Ching-Chan S, Kusaka Y, Jokura H, YoshimotoT: Surgical outcomes in 31 patients with craniopharyngiomasextending outside the suprasellar cistern: an evaluation ofthe frontobasal interhemispheric approach. J Neurosurg96:704712, 2002
45. Steno J, Malcek M, Bzik I: Tumor-third ventricular relation-ships in supradiaphragmatic craniopharyngiomas: correlationof morphological, magnetic resonance imaging, and operativendings. Neurosurgery54:10511060, 2004
46. lfarsson E, Lindquist C, Roberts M, Rhn T, Lindquist M,Thorn M, et al: Gamma knife radiosurgery for craniopha-ryngiomas: long-term results in the rst Swedish patients. JNeurosurg97 (5Suppl):613622, 2002
47. Van Effenterre R, Boch AL: Craniopharyngioma in adults andchildren: a study of 122 surgical cases. J Neurosurg97:311,2002
48. Villani RM, Tomei G, Bello L, Sganzerla E, Ambrosi B, Re T,et al: Long-term results of treatment for craniopharyngiomain children. Childs Nerv Syst13:397405, 1997
49. Wechsler D: Manual for the Wechsler Adult IntelligenceScale-Revised (WAIS-R).San Antonio: Psychological Cor-poration, 1981
50. Weiner HL, Wisoff JH, Rosenberg ME, Kupersmith MJ, Co-hen H, Zagzag D, et al: Craniopharyngiomas: a clinicopatho-logical analysis of factors predictive of recurrence and func-tional outcome. Neurosurgery35:10011011, 1994
51. Xu X, Shigemori M: Microsurgical management of cranio-pharyngiomasoutcomes in 56 patients. Kurume Med J45:5357, 1998
52. Yaargil MG, Curcic M, Kis M, Siegenthaler G, Teddy PJ,Roth P: Total removal of craniopharyngiomas. Approachesand long-term results in 144 patients. J Neurosurg73:311,1990
53. Zhao R, Deng J, Liang X, Zeng J, Chen X, Wang J: Treatmentof cystic craniopharyngiomas with phosphorus-32 intracavi-tary irradiation. Childs Nerv Syst 26:669674, 2010
54. Zhou ZQ, Shi XE: Changes of hypothalamus-pituitary hor-mones in patients after total removal of craniopharyngiomas.Chin Med J (Engl)117:357360, 2004
Manuscript submitted November 7, 2008.Accepted June 1, 2011.Please include this information when citing this paper: published
online September 23, 2011; DOI: 10.3171/2011.6.JNS081451.Address correspondence to: Rudolf Fahlbusch, M.D., Interna-
tional Neuroscience Institute, Rudolf Pichlmayrstrasse 4, 30625Hannover, Germany. email: [email protected].