
Carcinoma escamocelular del canal anal metastásico en un ...
Upload
mauricio-lemaCategory
view
327download
5
Tratamiento del cáncer colorectal metastásico: de las guías de práctica clínica, pasando por la genómica y la realidad
Mauricio Lema Medina MDClínica de Oncología Astorga / Clínica SOMA, Medellín, Colombia
Cartagena, Colombia09.07.2014

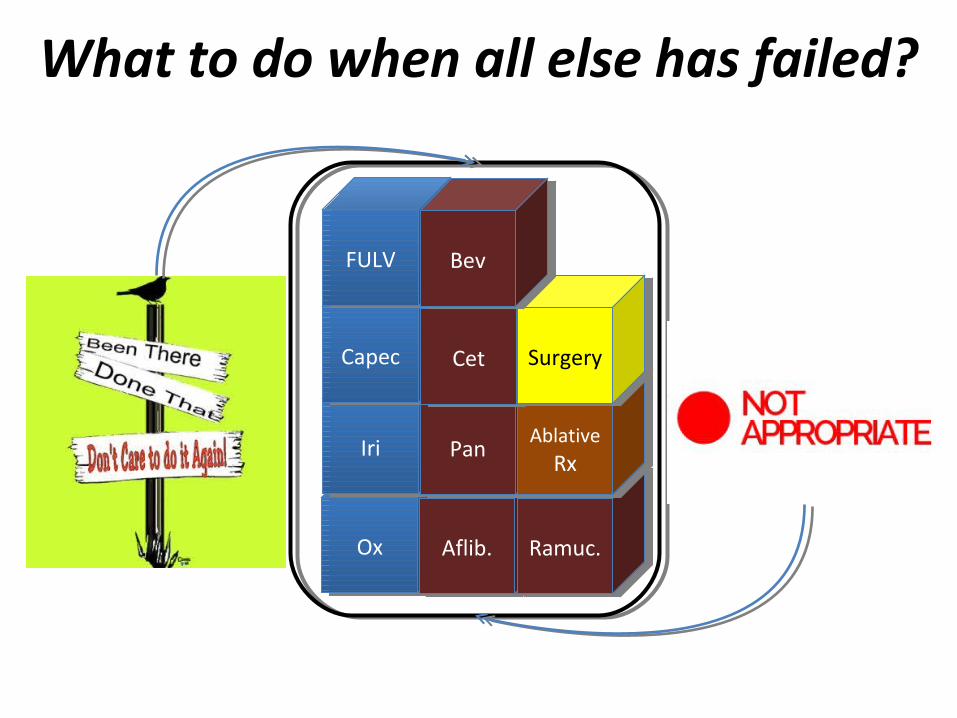
FULVFULV
CapecCapec
IriIri
BevBev
CetCet
PanPan
Regor.Regor.
SurgerySurgery
Ablative Rx
Ablative Rx
OxOx Aflib.Aflib. Ramuc.Ramuc.
FULVFULV BevBevCapecCapec BevBev
FULVFULVCapecCapec
FULVFULV OxOx IriIri
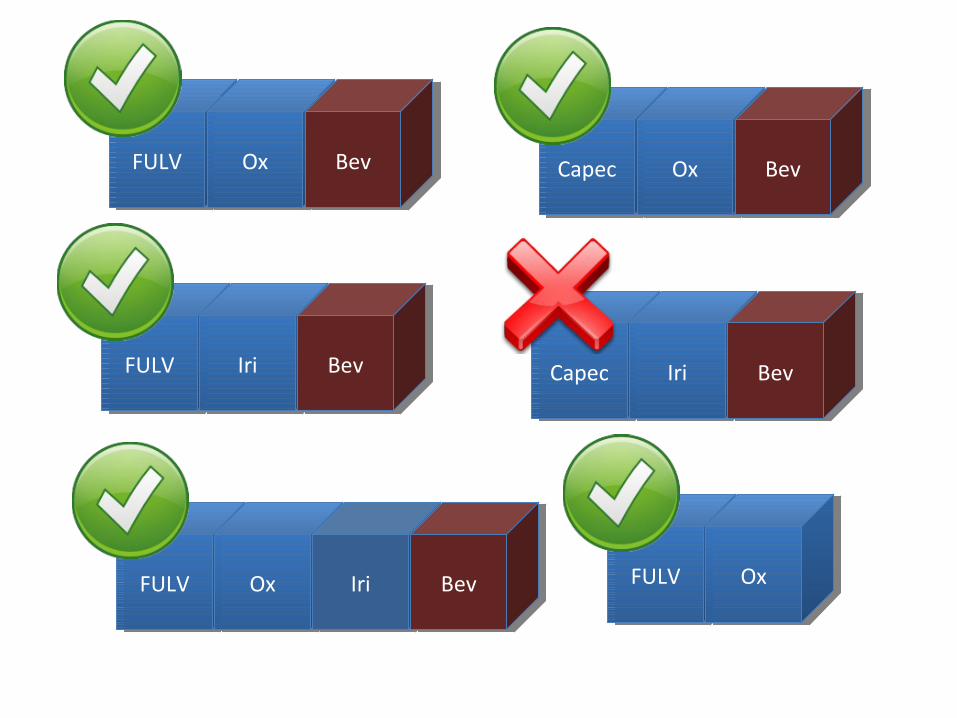
FULVFULV OxOx BevBev CapecCapec OxOx BevBev
FULVFULV OxOx IriIri BevBev FULVFULV OxOx
FULVFULV IriIri BevBev CapecCapec IriIri BevBev
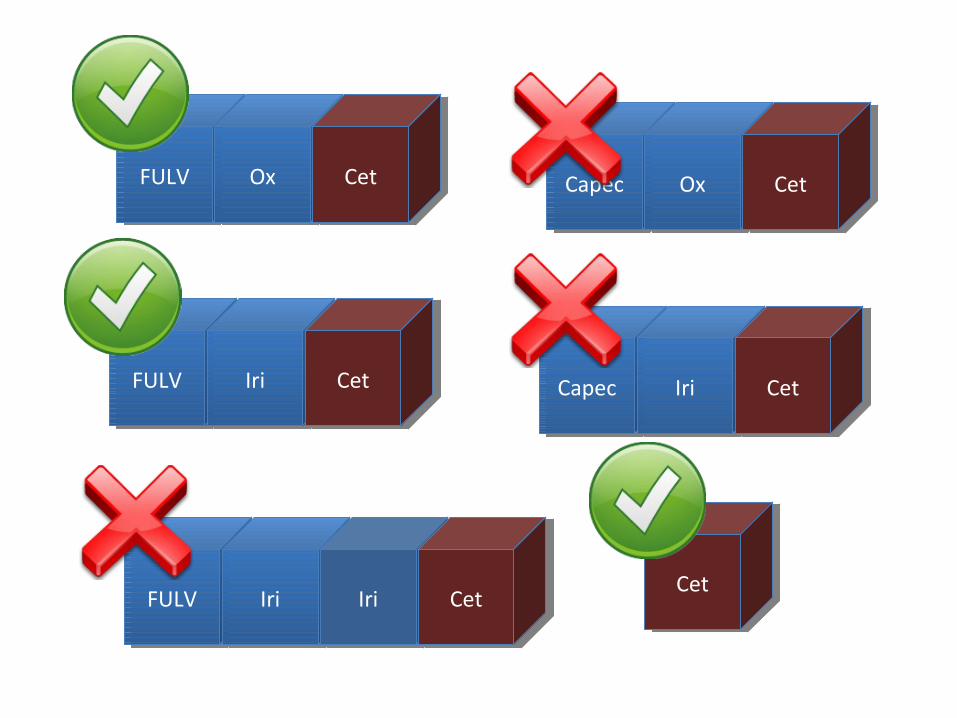
FULVFULV OxOx CetCet CapecCapec OxOx CetCet
FULVFULV IriIri IriIri CetCet
FULVFULV IriIri CetCet CapecCapec IriIri CetCet
CetCet
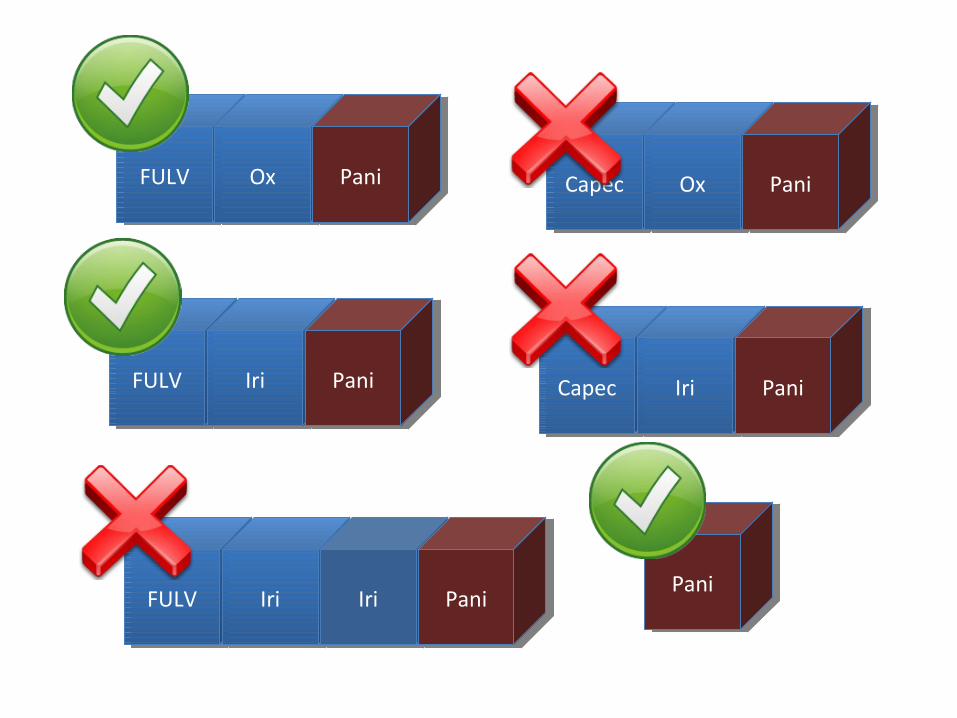
FULVFULV OxOx PaniPani CapecCapec OxOx PaniPani
FULVFULV IriIri IriIri PaniPani
FULVFULV IriIri PaniPani CapecCapec IriIri PaniPani
PaniPani
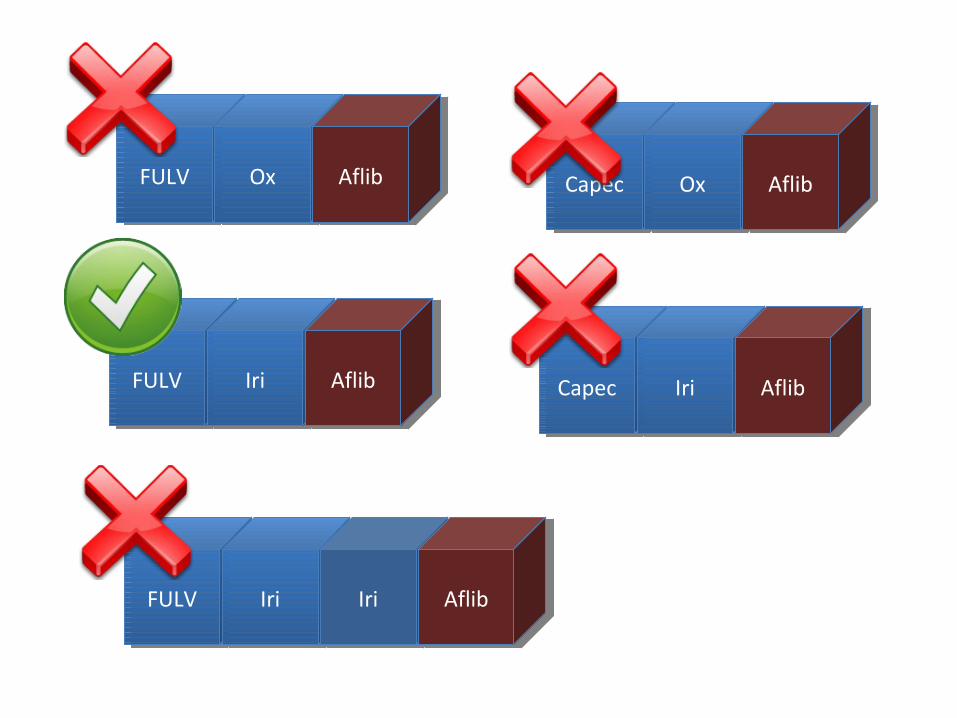
FULVFULV OxOx AflibAflib CapecCapec OxOx AflibAflib
FULVFULV IriIri IriIri AflibAflib
FULVFULV IriIri AflibAflib CapecCapec IriIri AflibAflib
“Thou shall not use anti-EGFR agents in mutated RAS CRC patients”
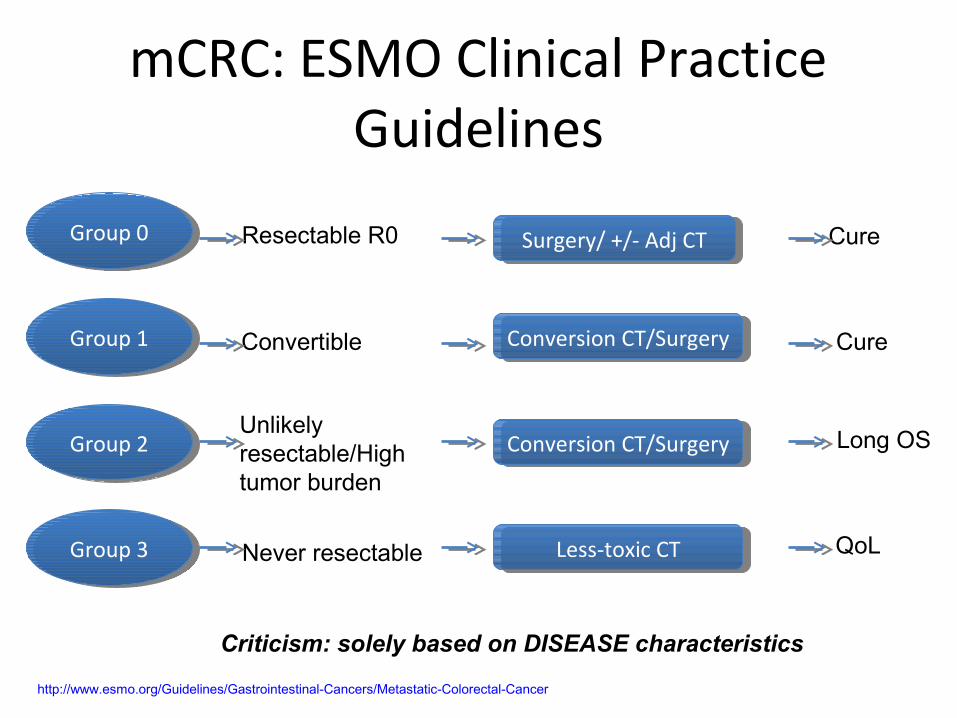
mCRC: ESMO Clinical Practice Guidelines
http://www.esmo.org/Guidelines/Gastrointestinal-Cancers/Metastatic-Colorectal-Cancer
Group 0Group 0
Group 1Group 1
Group 2Group 2
Group 3Group 3
Resectable R0
Convertible
Unlikely resectable/High tumor burden
Never resectable
Surgery/ +/- Adj CTSurgery/ +/- Adj CT
Conversion CT/SurgeryConversion CT/Surgery
Conversion CT/SurgeryConversion CT/Surgery
Less-toxic CTLess-toxic CT
Cure
Cure
Long OS
QoL
Criticism: solely based on DISEASE characteristics
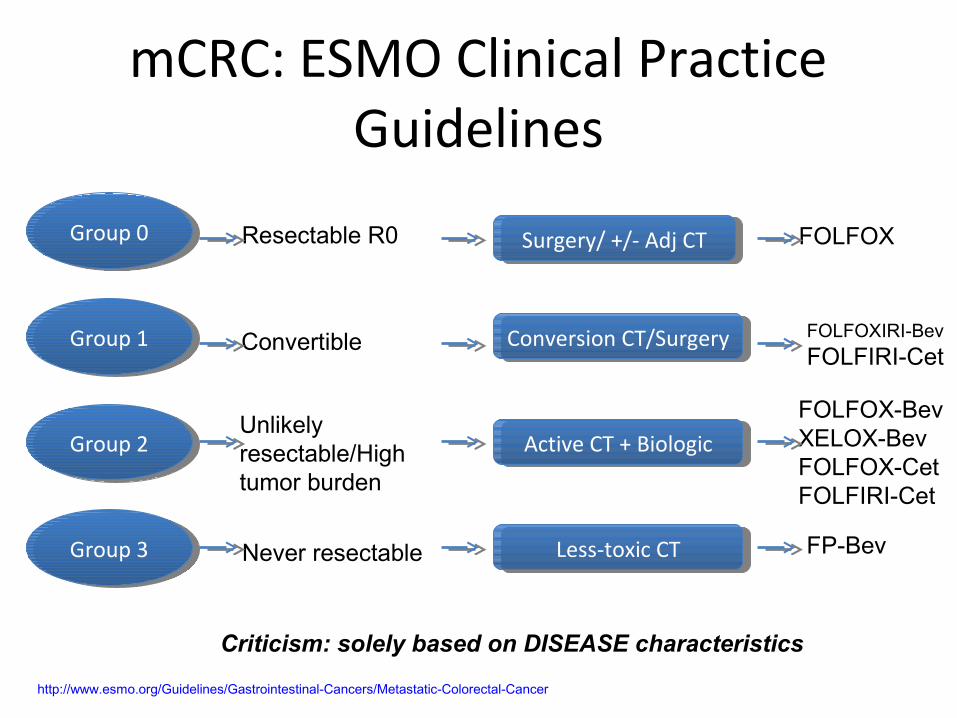
mCRC: ESMO Clinical Practice Guidelines
http://www.esmo.org/Guidelines/Gastrointestinal-Cancers/Metastatic-Colorectal-Cancer
Group 0Group 0
Group 1Group 1
Group 2Group 2
Group 3Group 3
Resectable R0
Convertible
Unlikely resectable/High tumor burden
Never resectable
Surgery/ +/- Adj CTSurgery/ +/- Adj CT
Conversion CT/SurgeryConversion CT/Surgery
Active CT + BiologicActive CT + Biologic
Less-toxic CTLess-toxic CT
FOLFOX
FOLFOXIRI-Bev
FOLFIRI-Cet
FOLFOX-BevXELOX-BevFOLFOX-CetFOLFIRI-Cet
FP-Bev
Criticism: solely based on DISEASE characteristics
Do THESE guidelines, guide?
Let’s start with curative intent
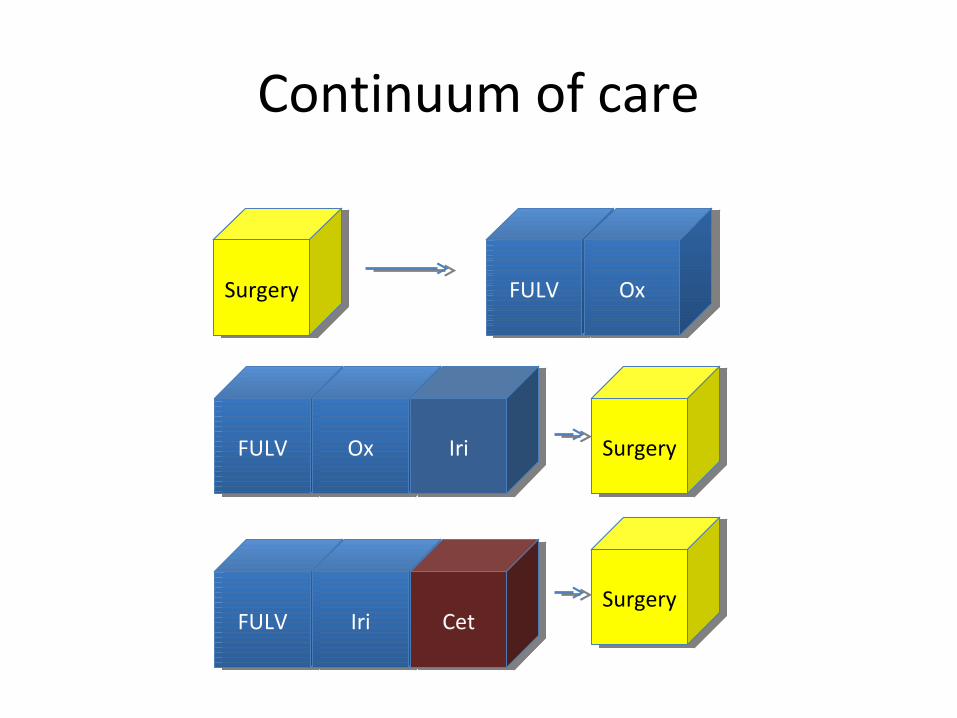
Continuum of care
SurgerySurgery FULVFULV OxOx
FULVFULV OxOx IriIri SurgerySurgery
FULVFULV IriIri CetCetSurgerySurgery
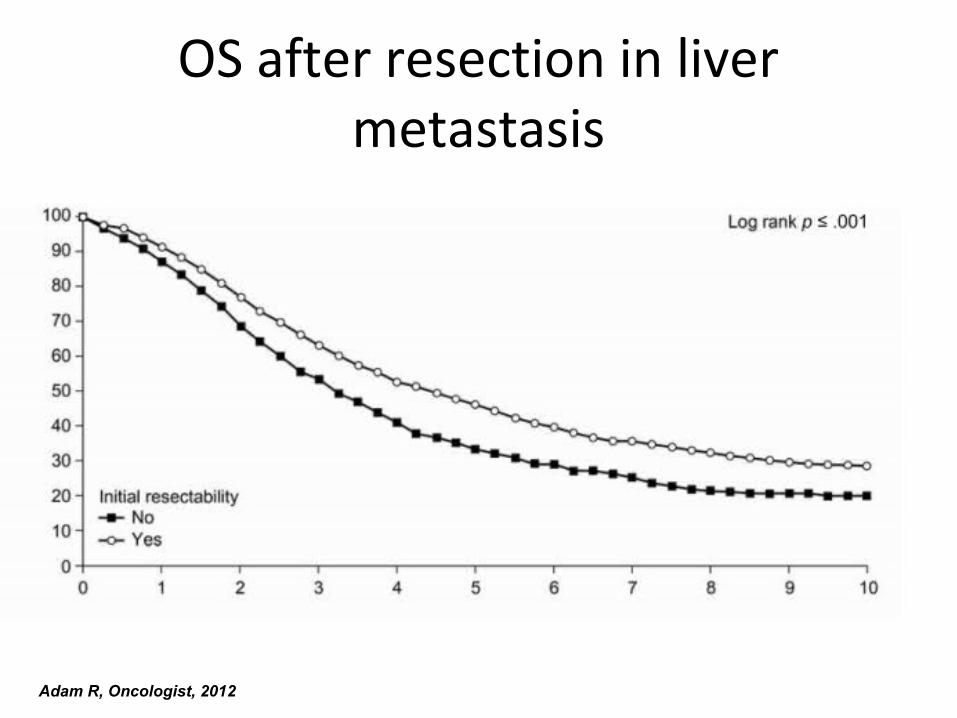
OS after resection in liver metastasis
Adam R, Oncologist, 2012

OS after resection in liver metastasis
Adam R, Oncologist, 2012
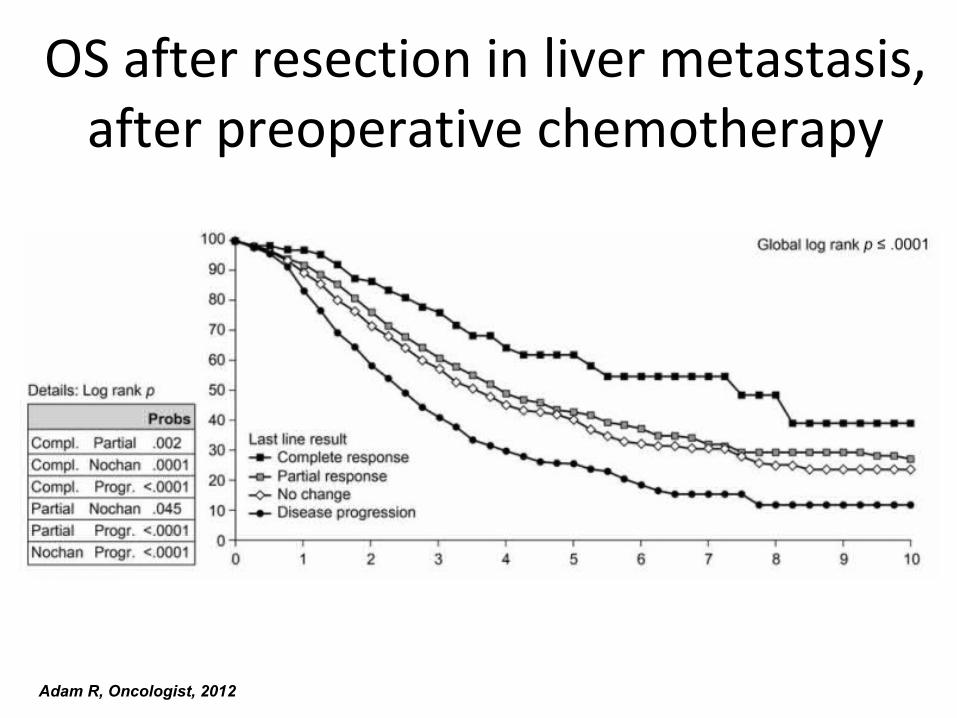
OS after resection in liver metastasis, after preoperative chemotherapy
Adam R, Oncologist, 2012
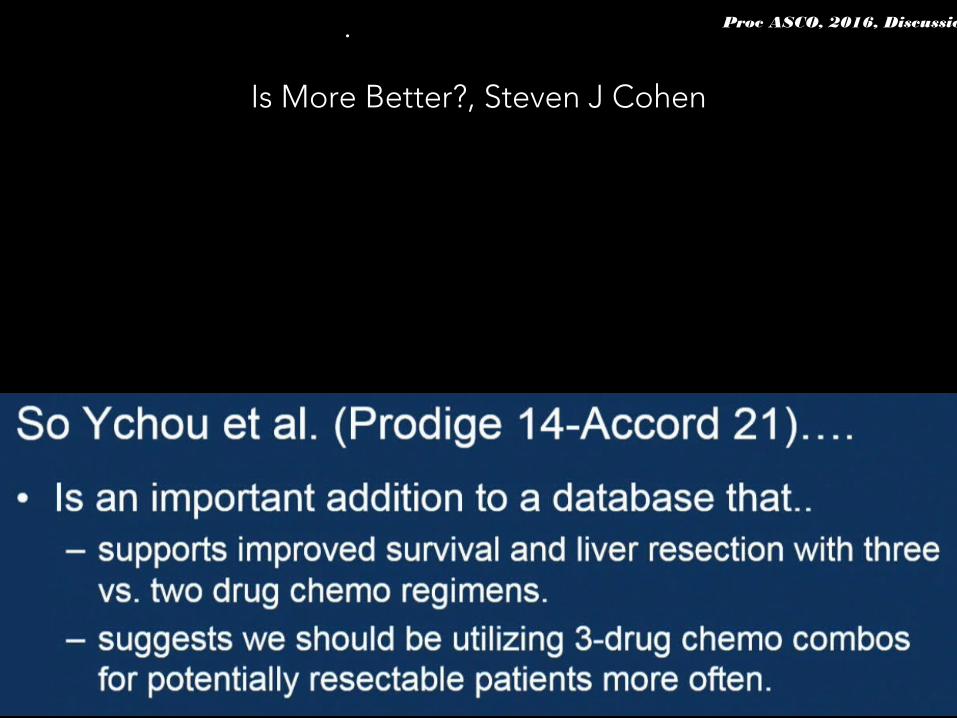
FOLFIRINOX combined to targeted therapy according RAS status for colorectal cancer patients with liver
metastases initially non-resectable: A phase II randomized Study—Prodige 14 – accord 21 (METHEP-2), a unicancer
GI trial. Mark Ychou. Proc ASCO, 2016, Abstract 3512
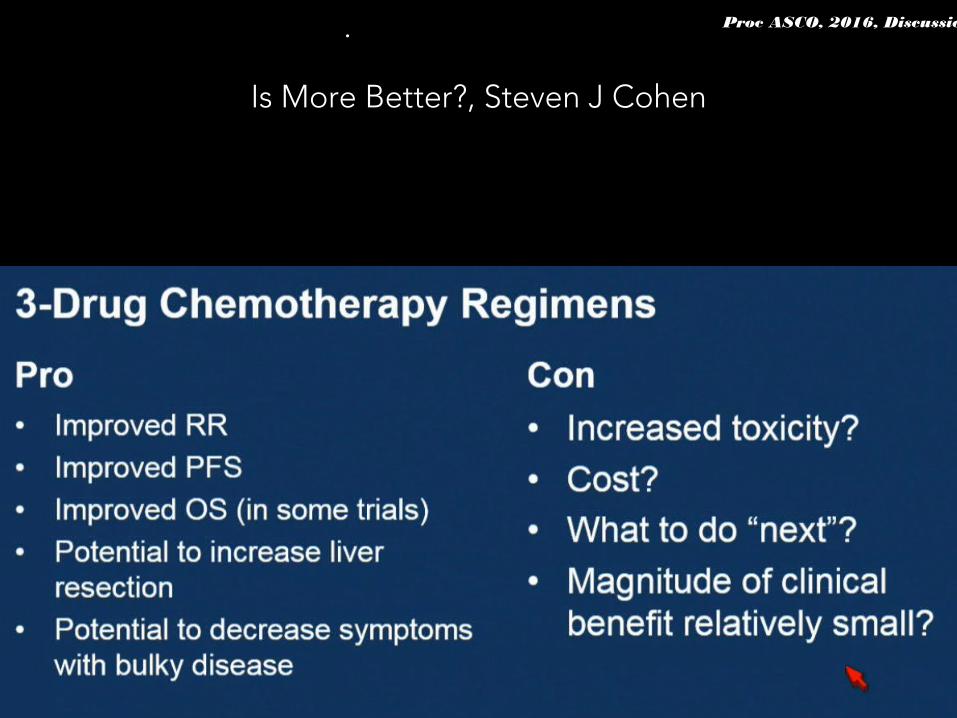
Proc ASCO, 2016, Discussion.
FOLFIRINOX as induction treatment in rectal cancer patients with synchronous metastases (RCSM): Results of
the FFCD 1102 phase II trial. JB Bachet. Proc ASCO, 2016, Abstract 3513
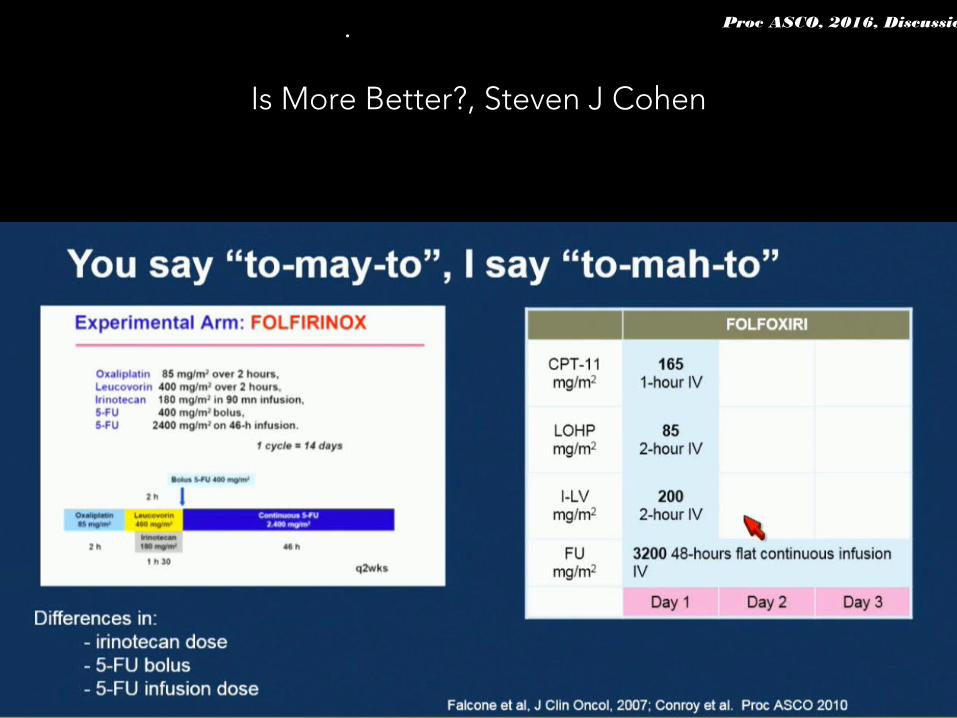
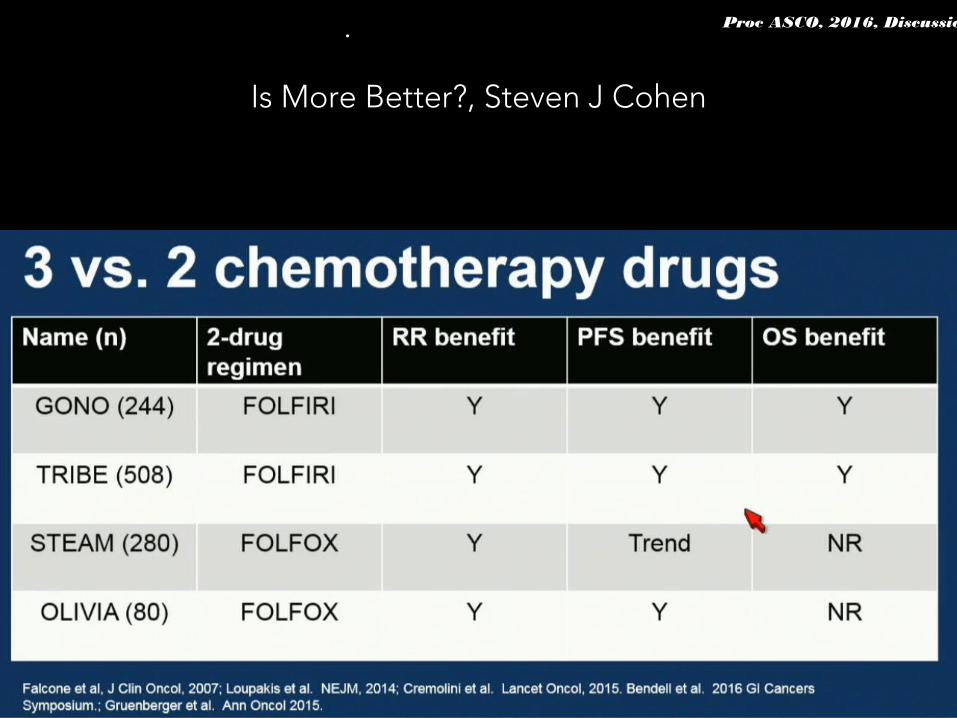
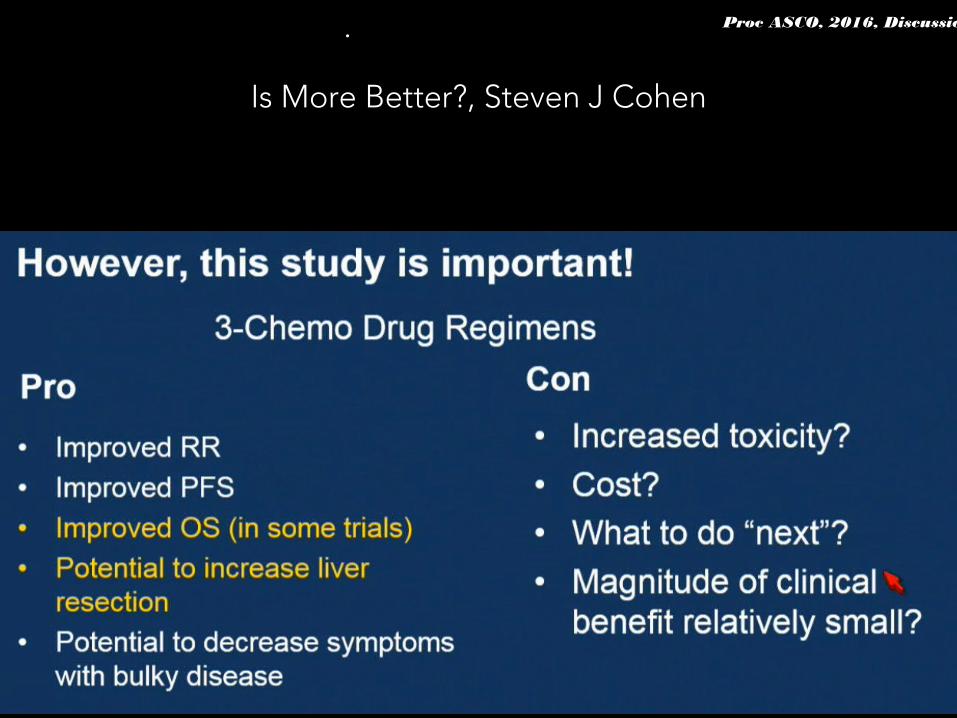
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
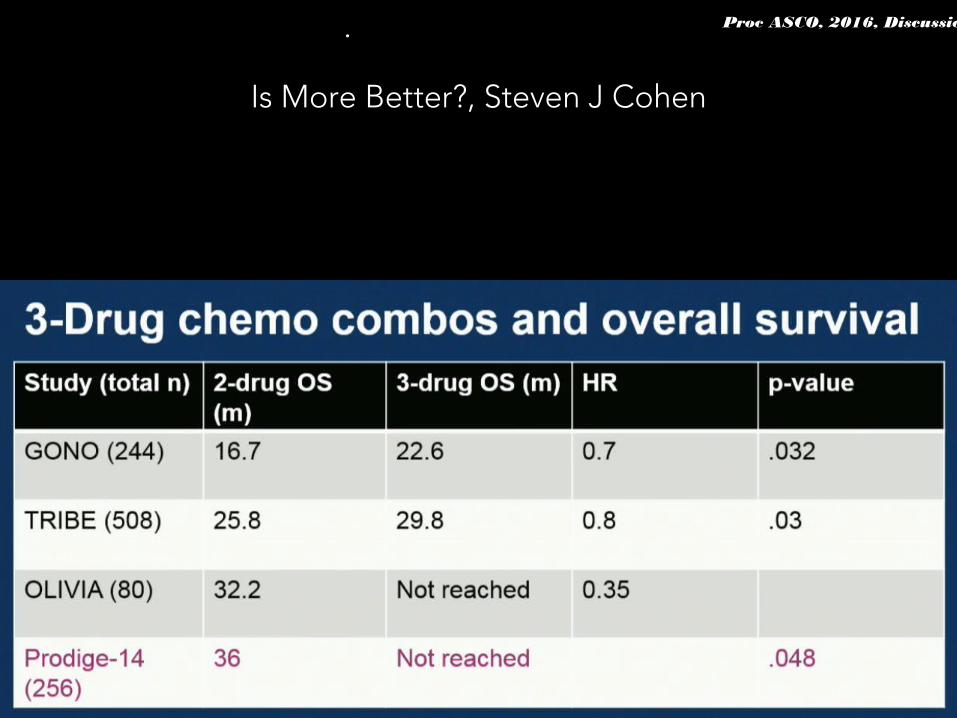
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
Is More Better?, Steven J Cohen
Proc ASCO, 2016, Discussion.
THAT was easy, what about the rest?
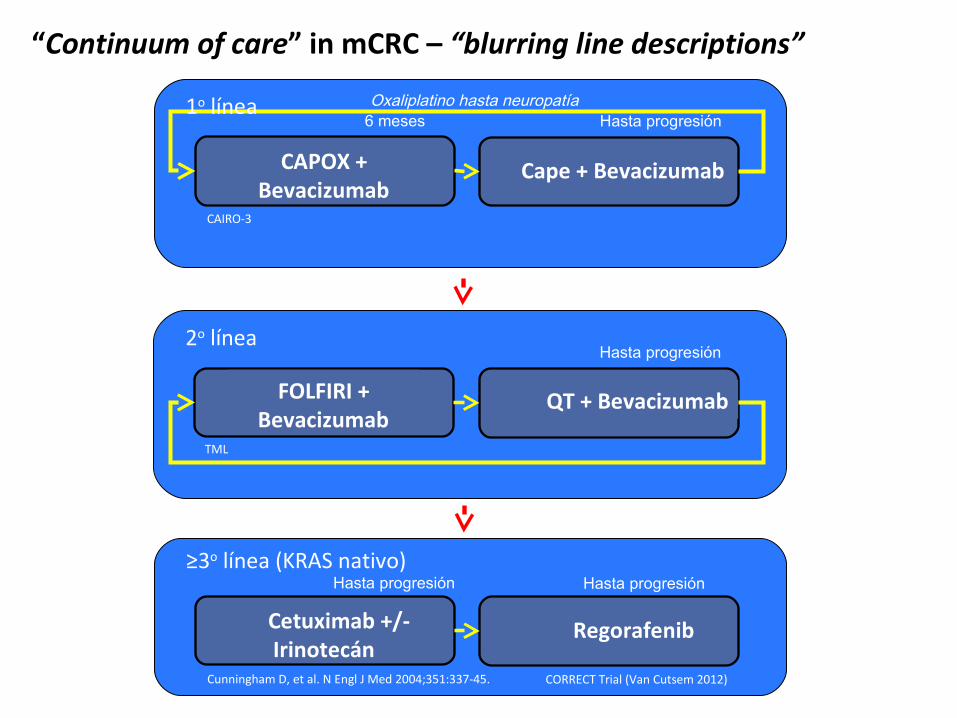
CAPOX + Bevacizumab
6 meses
“Continuum of care” in mCRC – “blurring line descriptions”
Cape + Bevacizumab
Hasta progresión1o línea
FOLFIRI + Bevacizumab
Oxaliplatino hasta neuropatía
QT + Bevacizumab
Hasta progresión2o línea
Cetuximab +/- Irinotecán
Regorafenib
Hasta progresión≥3o línea (KRAS nativo)
Hasta progresión
CAIRO-3
TML
Cunningham D, et al. N Engl J Med 2004;351:337-45. CORRECT Trial (Van Cutsem 2012)
In the RAS wt, which first-line agent?
clinicaloptions.com/oncologyOptimizing Treatment of Metastatic Colorectal Cancer
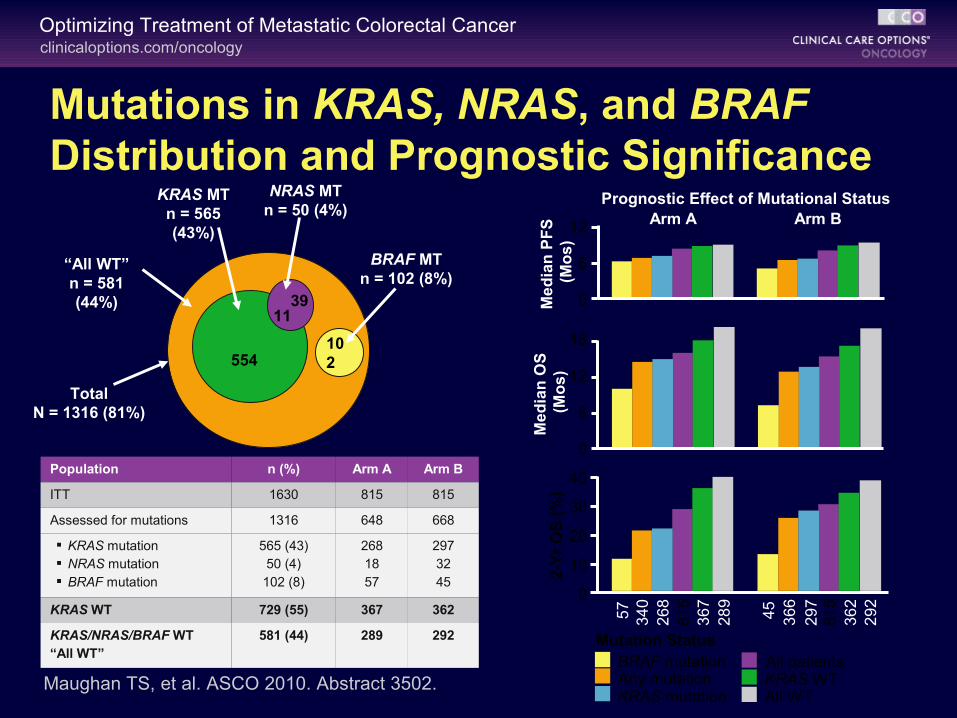
Mutations in KRAS, NRAS, and BRAF Distribution and Prognostic Significance
BRAF mutation All patientsAny mutationKRAS mutation
KRAS WTAll WT
Mutation Status
0
6
12
Me
dia
n P
FS
(M
os
)
Arm A Arm B
0
6
12
18
Me
dia
n O
S
(Mo
s)
57
34
02
68
81
53
67
28
9
45
36
62
97
81
53
62
29
20
10
20
30
40
2-Y
r O
S (
%)
Prognostic Effect of Mutational Status
“All WT”n = 581 (44%)
KRAS MTn = 565 (43%)
NRAS MTn = 50 (4%)
BRAF MTn = 102 (8%)
TotalN = 1316 (81%)
554
1139
102
Population n (%) Arm A Arm B
ITT 1630 815 815
Assessed for mutations 1316 648 668
KRAS mutation NRAS mutation BRAF mutation
565 (43)50 (4)
102 (8)
2681857
2973245
KRAS WT 729 (55) 367 362
KRAS/NRAS/BRAF WT“All WT”
581 (44) 289 292
Maughan TS, et al. ASCO 2010. Abstract 3502.
clinicaloptions.com/oncologyOptimizing Treatment of Metastatic Colorectal Cancer
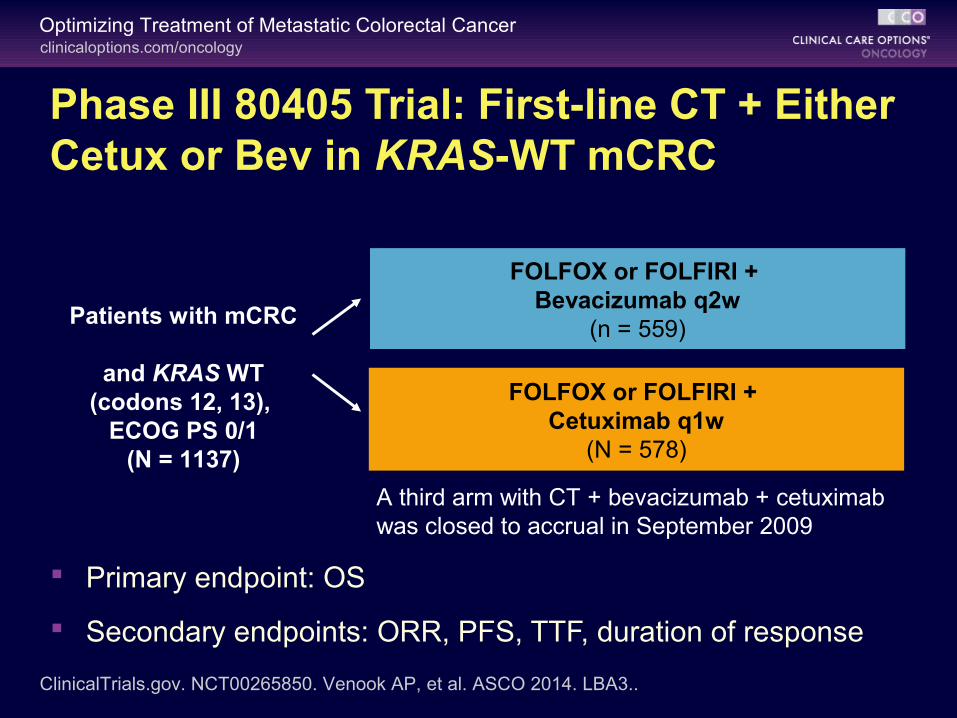
Phase III 80405 Trial: First-line CT + Either Cetux or Bev in KRAS-WT mCRC
Primary endpoint: OS
Secondary endpoints: ORR, PFS, TTF, duration of response
Patients with mCRC
and KRAS WT (codons 12, 13),
ECOG PS 0/1(N = 1137)
FOLFOX or FOLFIRI + Bevacizumab q2w
(n = 559)
ClinicalTrials.gov. NCT00265850. Venook AP, et al. ASCO 2014. LBA3..
FOLFOX or FOLFIRI + Cetuximab q1w
(N = 578)
A third arm with CT + bevacizumab + cetuximab was closed to accrual in September 2009
clinicaloptions.com/oncologyOptimizing Treatment of Metastatic Colorectal Cancer
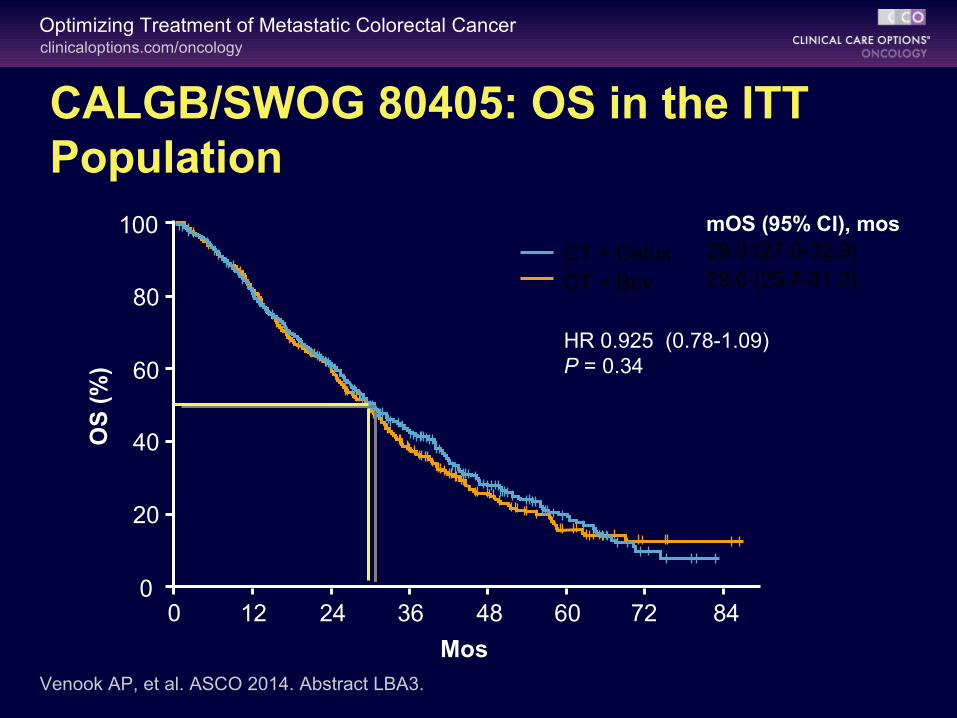
CALGB/SWOG 80405: OS in the ITT Population
mOS (95% CI), mosCT + Cetux 29.9 (27.0-32.9)
CT + Bev 29.0 (25.7-31.2)
HR 0.925 (0.78-1.09)P = 0.34
Venook AP, et al. ASCO 2014. Abstract LBA3.
012 24 36 48 60 72
Mos
80
100
60
40
0
OS
(%
)
20
84
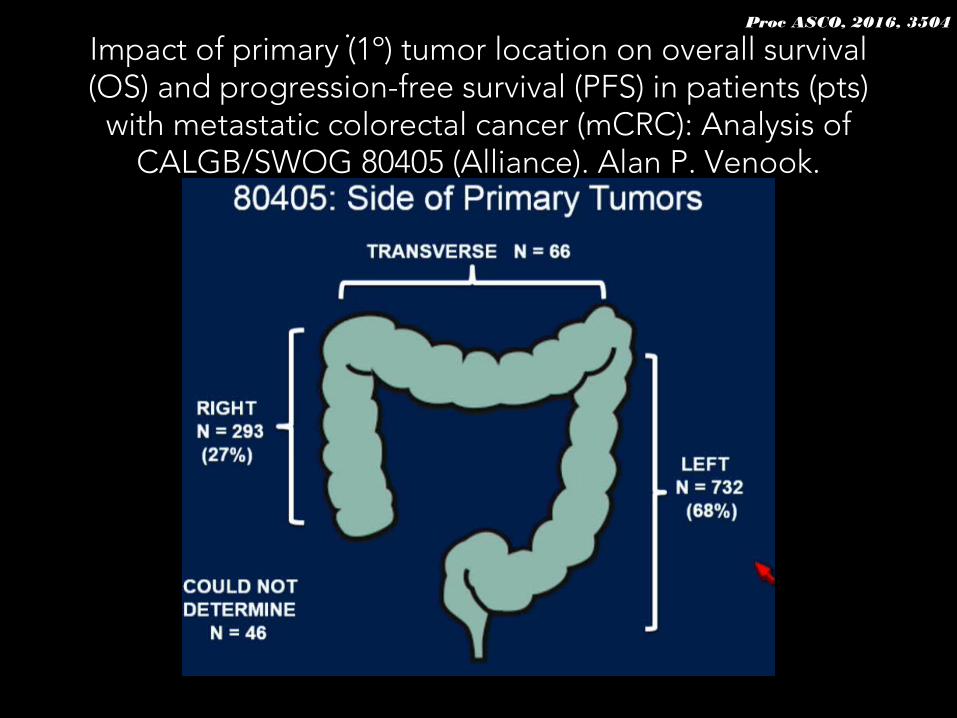
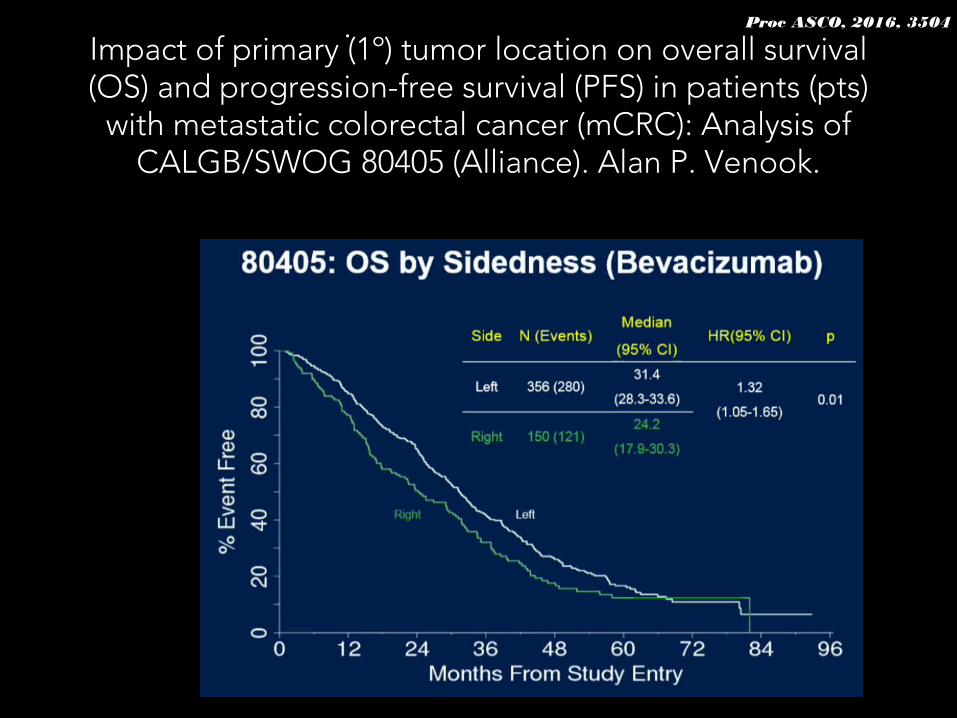
Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts)
with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Alan P. Venook.
Proc ASCO, 2016, 3504.
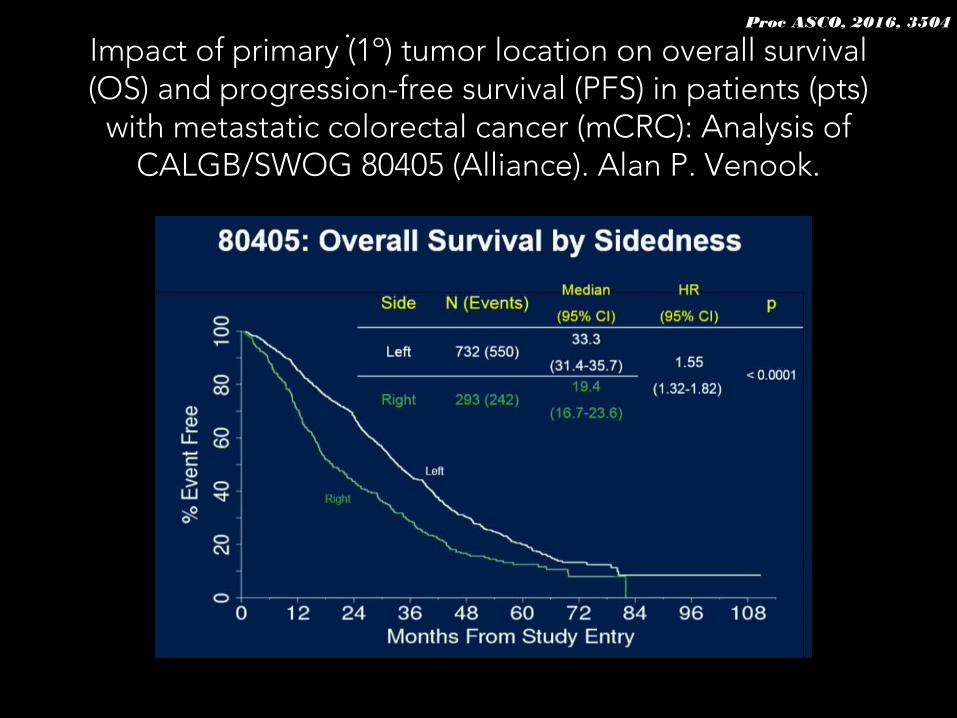
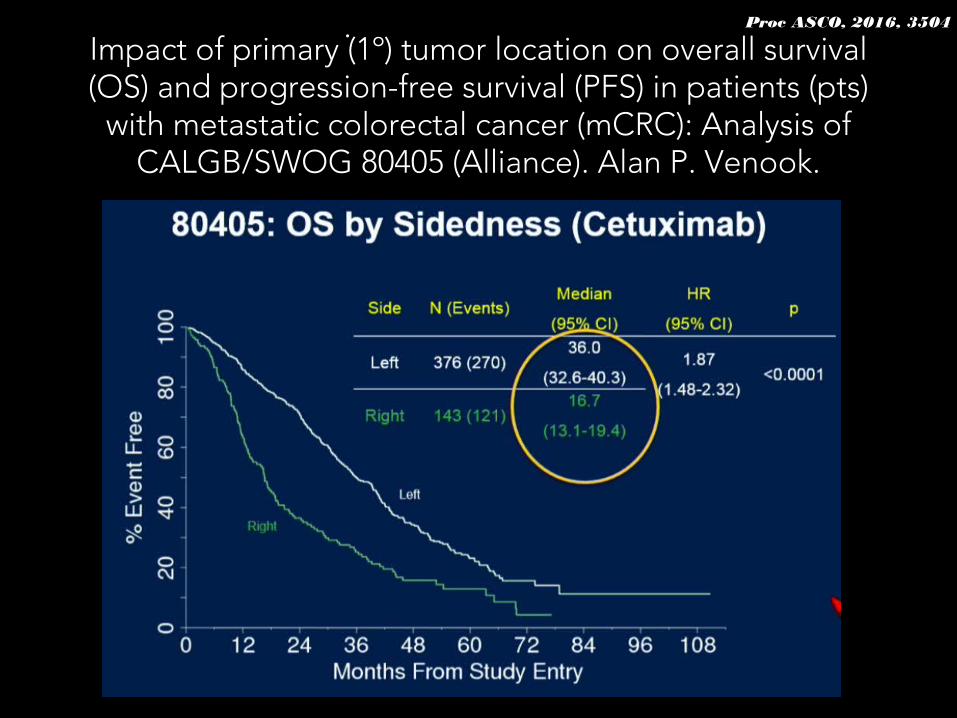
Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts)
with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Alan P. Venook.
Proc ASCO, 2016, 3504.
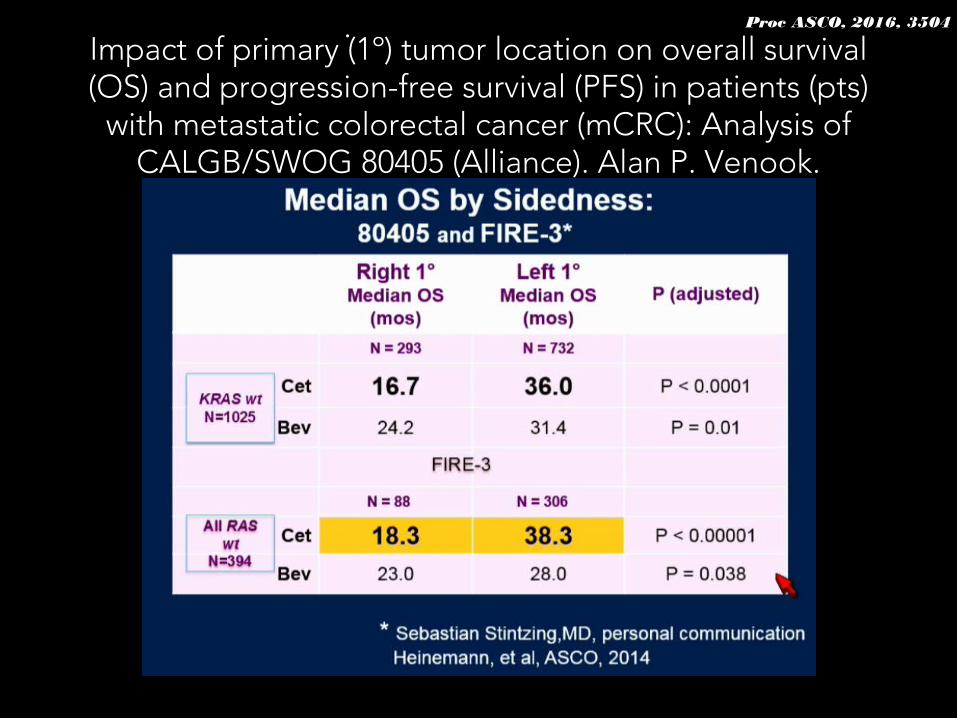
Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts)
with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Alan P. Venook.
Proc ASCO, 2016, 3504.
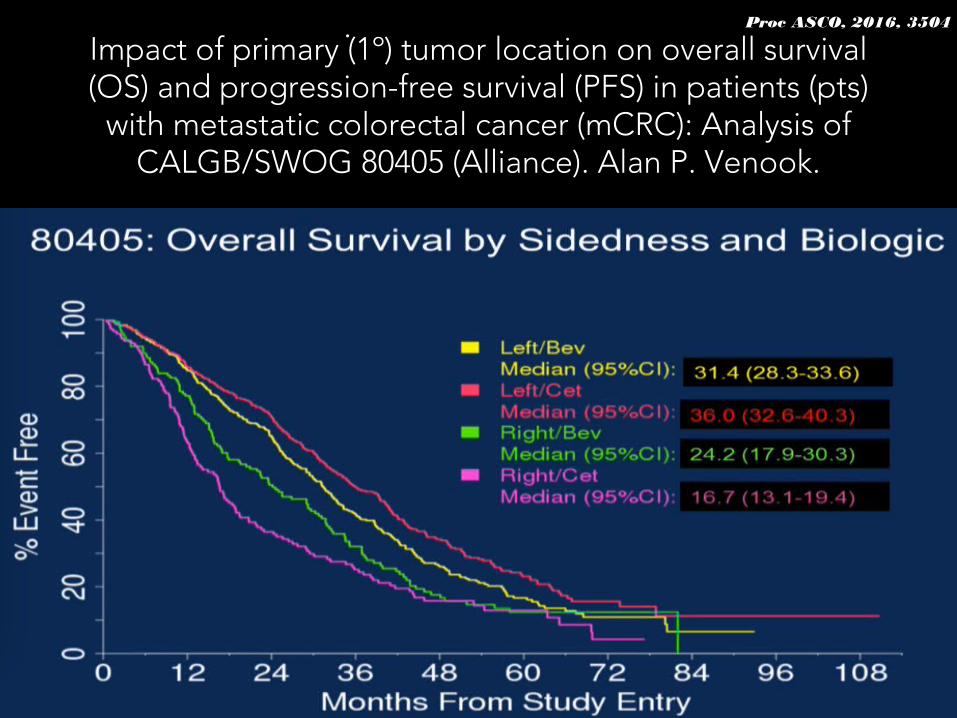
Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts)
with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Alan P. Venook.
Proc ASCO, 2016, 3504.
Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts)
with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Alan P. Venook.
Proc ASCO, 2016, 3504.
Impact of primary (1º) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts)
with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). Alan P. Venook.
Proc ASCO, 2016, 3504.
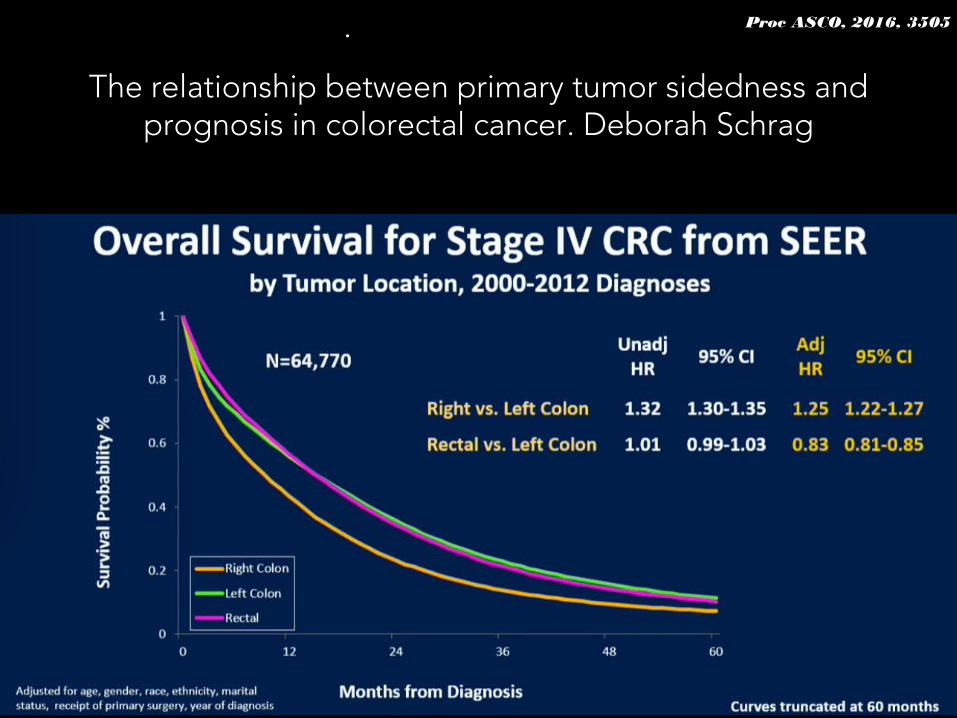
The relationship between primary tumor sidedness and prognosis in colorectal cancer. Deborah Schrag
Proc ASCO, 2016, 3505.
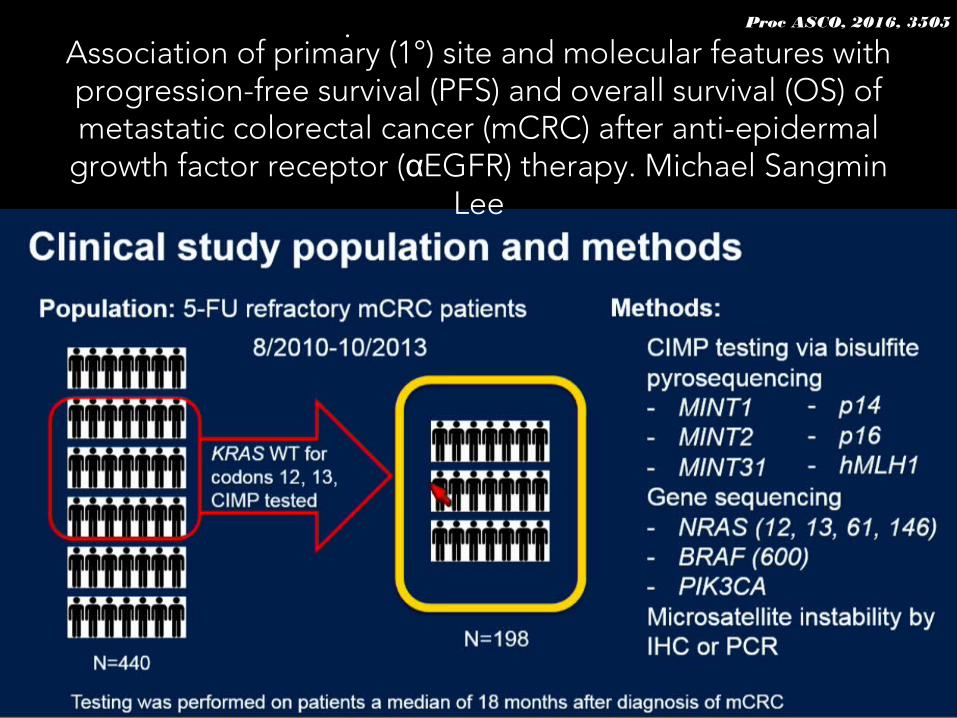
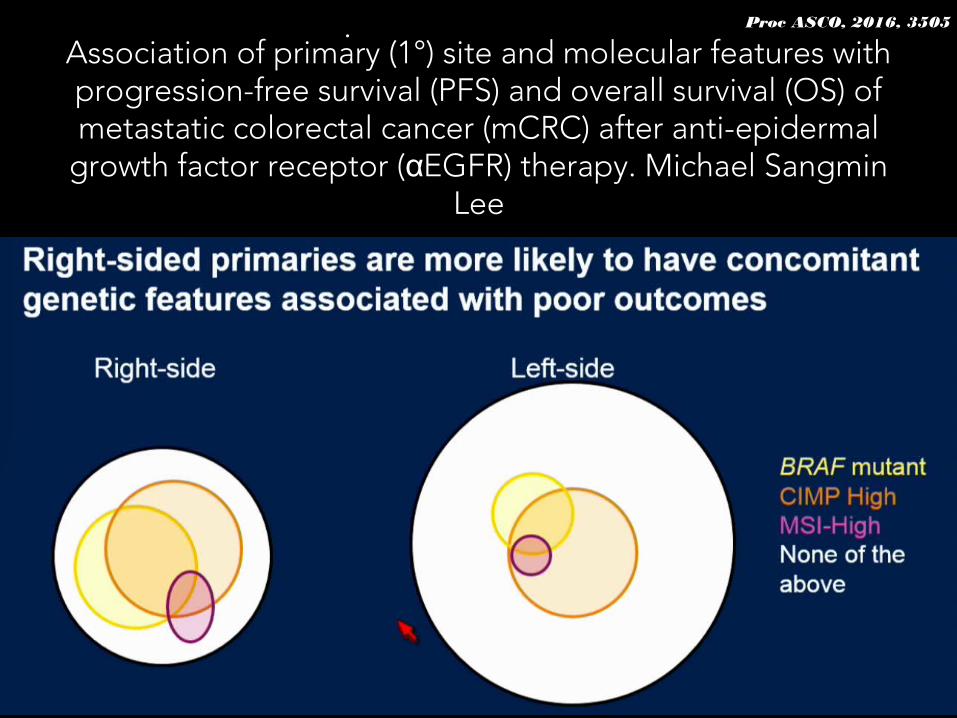
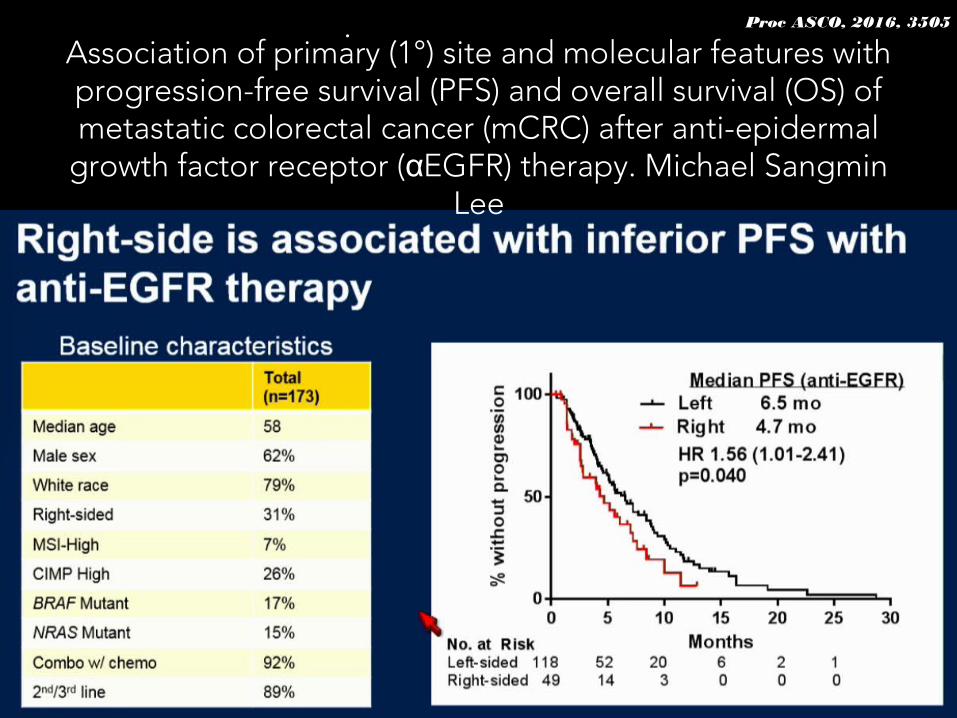
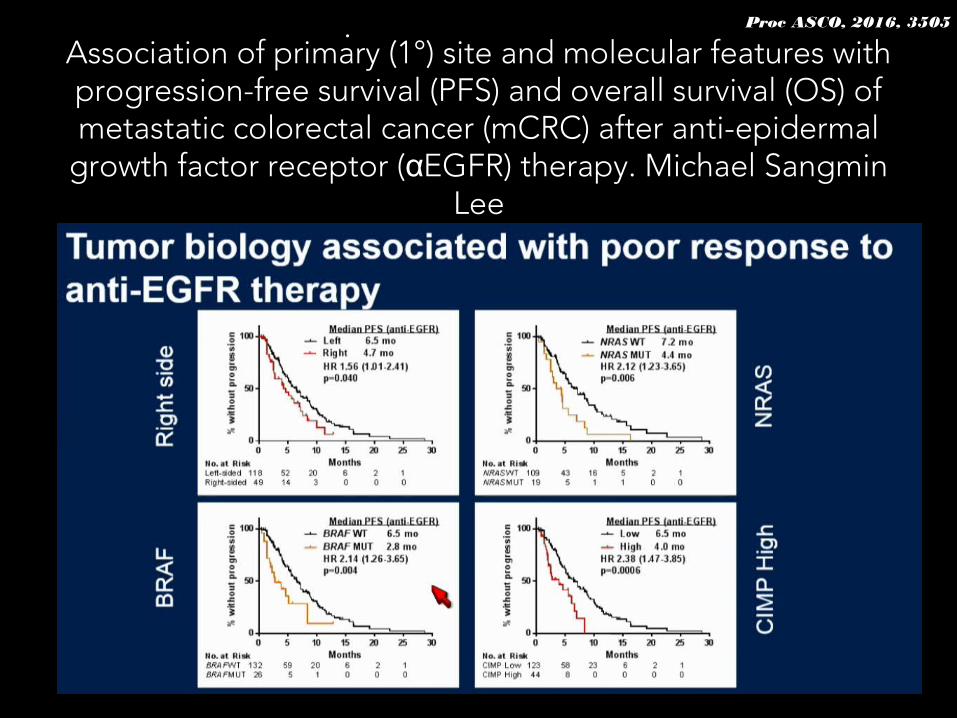
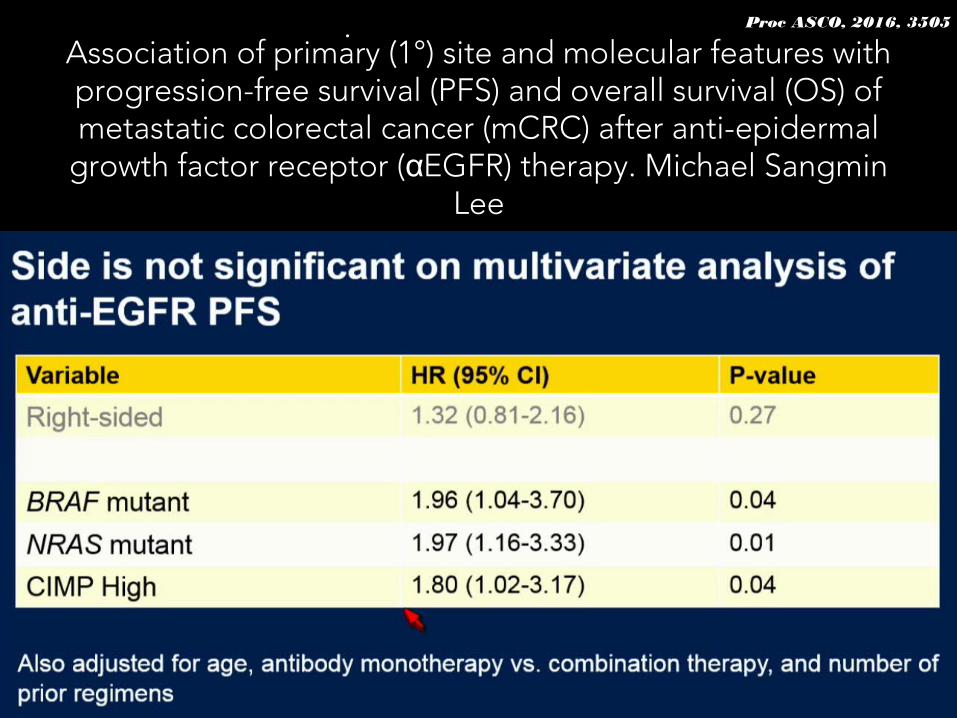
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
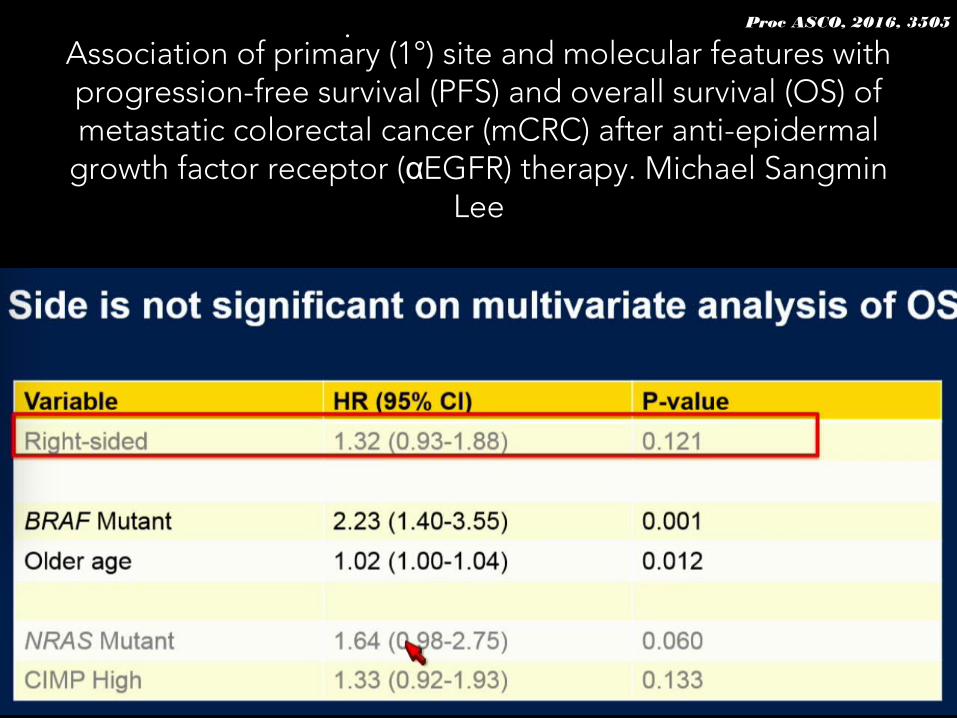
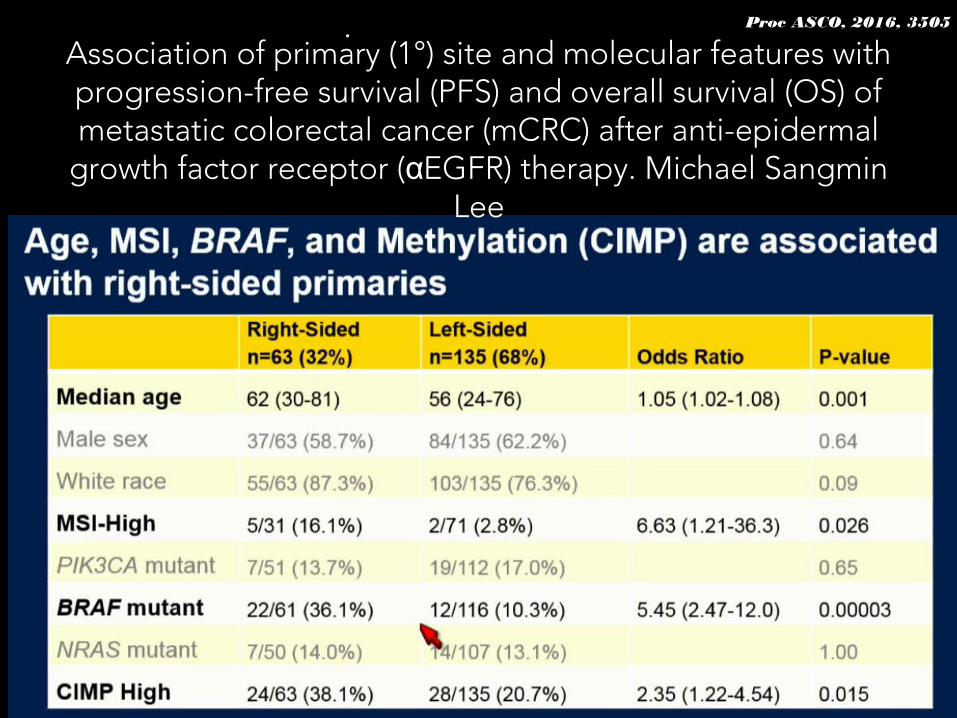
Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Proc ASCO, 2016, 3505.Association of primary (1°) site and molecular features with progression-free survival (PFS) and overall survival (OS) of metastatic colorectal cancer (mCRC) after anti-epidermal
growth factor receptor ( EGFR) therapy. Michael Sangmin αLee
Side Matters. Kimmie Ng
Proc ASCO, 2016, Dicussion..
What should we do with BRAF mutated mCRC?
FULVFULV OxOx IriIri BevBev
What about mBRAF mCRC?
• Not very clear• TRIBE study suggests FOLFOXIRI-Bev(1)
• Further studies of anti-BRAF coupled with other agents are expected (ie, Cetuximab).
1. Loupakis F, NEJM, 2014
Continuum of care in mCRC
Continuum of care
FULVFULV OxOx BevBev
What to do in second line?
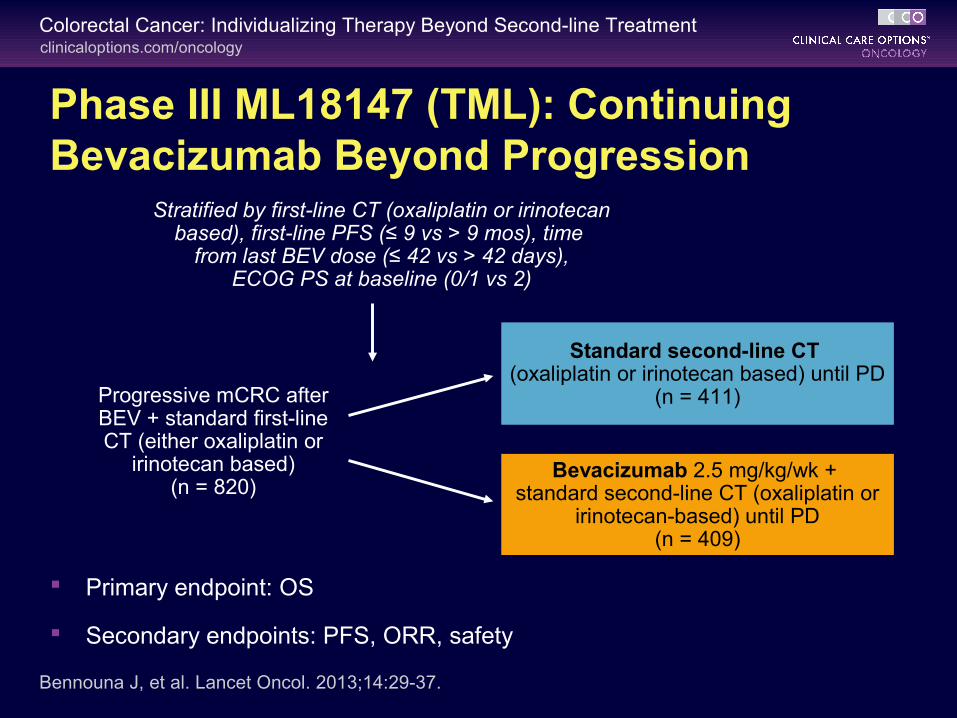
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
Phase III ML18147 (TML): Continuing Bevacizumab Beyond Progression
Standard second-line CT (oxaliplatin or irinotecan based) until PD
(n = 411)
Bevacizumab 2.5 mg/kg/wk + standard second-line CT (oxaliplatin or
irinotecan-based) until PD(n = 409)
Progressive mCRC after BEV + standard first-line CT (either oxaliplatin or
irinotecan based)(n = 820)
Bennouna J, et al. Lancet Oncol. 2013;14:29-37.
Stratified by first-line CT (oxaliplatin or irinotecan based), first-line PFS (≤ 9 vs > 9 mos), time
from last BEV dose (≤ 42 vs > 42 days),ECOG PS at baseline (0/1 vs 2)
Primary endpoint: OS
Secondary endpoints: PFS, ORR, safety
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
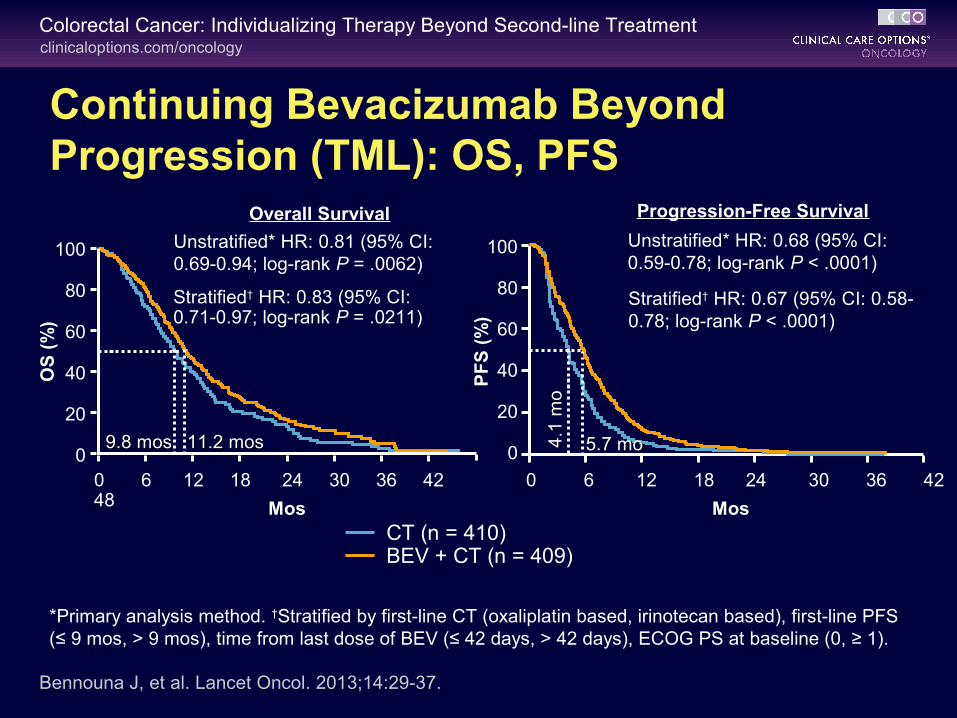
Continuing Bevacizumab Beyond Progression (TML): OS, PFS
OS
(%
)
MosCT (n = 410)BEV + CT (n = 409)
100
80
60
40
20
00 6 12 18 24 30 36 42 48
9.8 mos9.8 mos 11.2 mos11.2 mos
Unstratified* HR: 0.81 (95% CI: 0.69-0.94; log-rank P = .0062)
Stratified† HR: 0.83 (95% CI: 0.71-0.97; log-rank P = .0211)
*Primary analysis method. †Stratified by first-line CT (oxaliplatin based, irinotecan based), first-line PFS (≤ 9 mos, > 9 mos), time from last dose of BEV (≤ 42 days, > 42 days), ECOG PS at baseline (0, ≥ 1).
Bennouna J, et al. Lancet Oncol. 2013;14:29-37.
100
80
60
40
20
0
PF
S (
%)
0 6 12 18 24 30 36 42
Mos
Unstratified* HR: 0.68 (95% CI: 0.59-0.78; log-rank P < .0001)
Stratified† HR: 0.67 (95% CI: 0.58-0.78; log-rank P < .0001)
4.1
mo
4.1
mo
5.7 mo5.7 mo
Overall Survival Progression-Free Survival
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
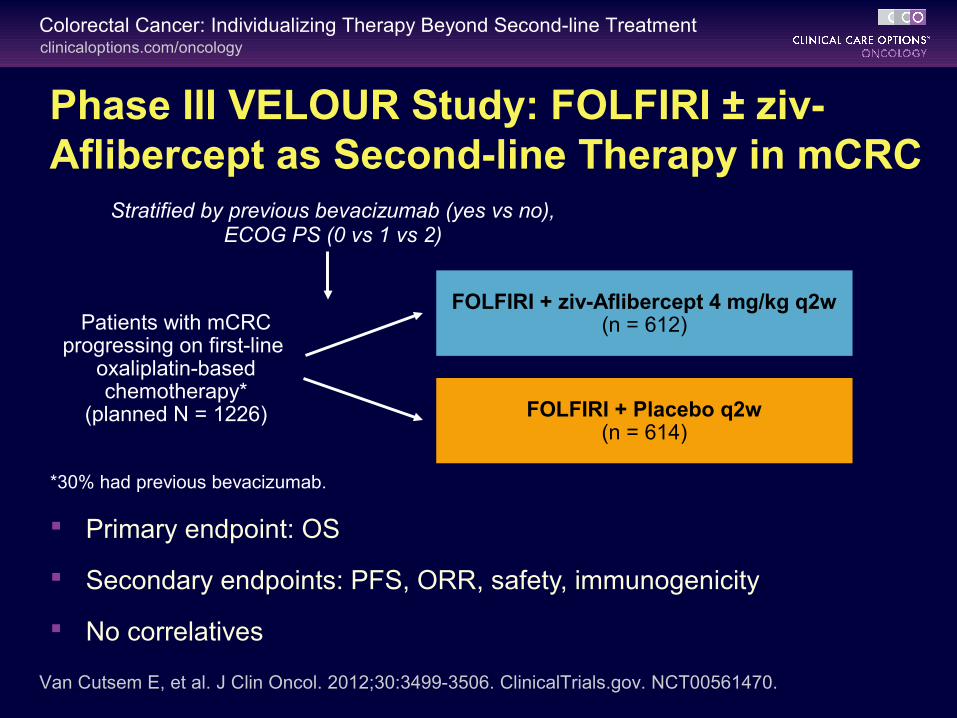
Phase III VELOUR Study: FOLFIRI ± ziv-Aflibercept as Second-line Therapy in mCRC
Primary endpoint: OS
Secondary endpoints: PFS, ORR, safety, immunogenicity
No correlatives
Patients with mCRC progressing on first-line
oxaliplatin-based chemotherapy*
(planned N = 1226)
FOLFIRI + ziv-Aflibercept 4 mg/kg q2w(n = 612)
FOLFIRI + Placebo q2w(n = 614)
*30% had previous bevacizumab.
Stratified by previous bevacizumab (yes vs no),ECOG PS (0 vs 1 vs 2)
Van Cutsem E, et al. J Clin Oncol. 2012;30:3499-3506. ClinicalTrials.gov. NCT00561470.
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
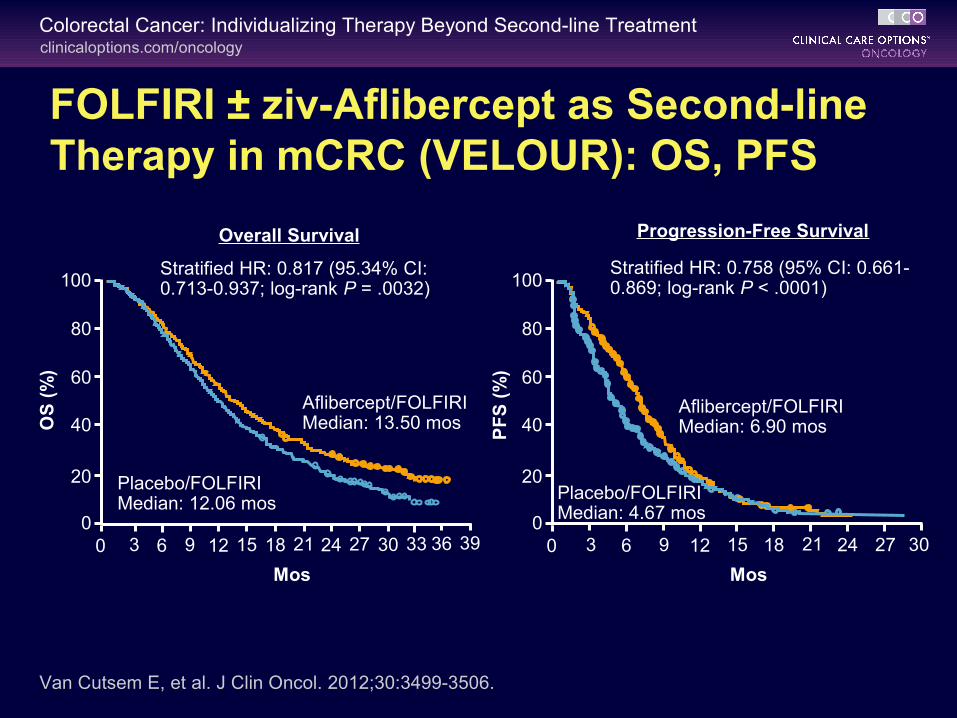
FOLFIRI ± ziv-Aflibercept as Second-line Therapy in mCRC (VELOUR): OS, PFS
Van Cutsem E, et al. J Clin Oncol. 2012;30:3499-3506.
Stratified HR: 0.817 (95.34% CI: 0.713-0.937; log-rank P = .0032)
Placebo/FOLFIRIMedian: 12.06 mos
Aflibercept/FOLFIRIMedian: 13.50 mos
PF
S (
%)
100
80
60
40
20
0
Mos
0 3 6 9 12 15 18 21 24 27 30
Stratified HR: 0.758 (95% CI: 0.661-0.869; log-rank P < .0001)
Placebo/FOLFIRIMedian: 4.67 mos
Aflibercept/FOLFIRIMedian: 6.90 mos
Overall Survival Progression-Free Survival
OS
(%
)
100
80
60
40
20
0
Mos
0 3 6 9 12 15 18 21 24 27 30 33 36 39
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
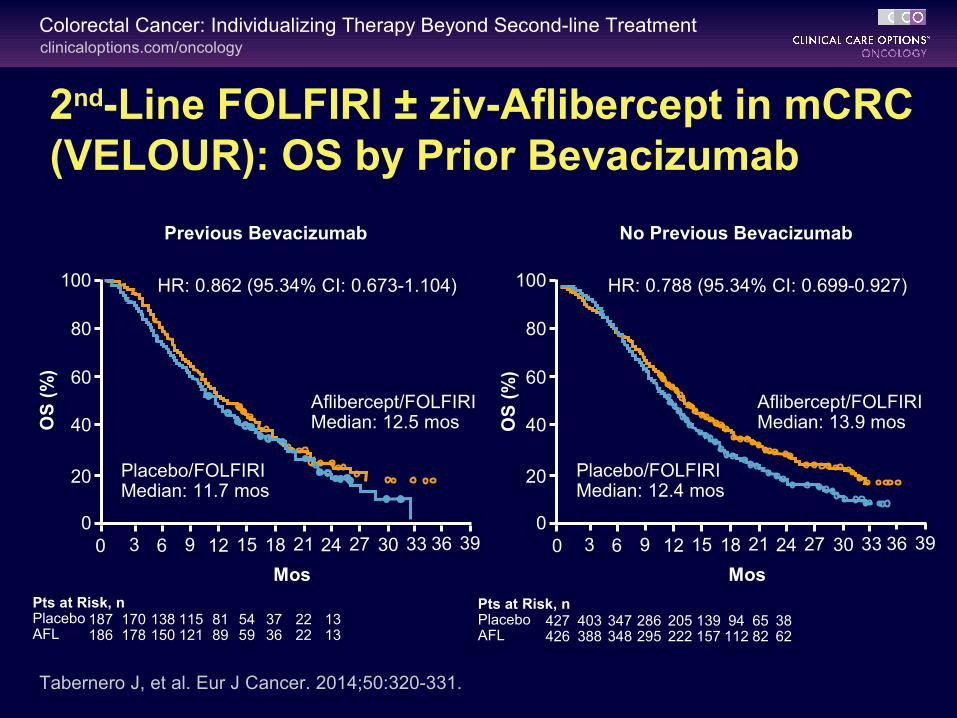
Tabernero J, et al. Eur J Cancer. 2014;50:320-331.
OS
(%
)
100
80
60
40
20
0
Mos
0 3 6 9 12 15 18 21 24 27 30 33 36 39
HR: 0.862 (95.34% CI: 0.673-1.104)
Placebo/FOLFIRIMedian: 11.7 mos
Aflibercept/FOLFIRIMedian: 12.5 mos
Pts at Risk, n PlaceboAFL
187186
170178
138150
115121
8189
5459
3736
2222
1313
Previous Bevacizumab
OS
(%
)
100
80
60
40
20
0
Mos
0 3 6 9 12 15 18 21 24 27 30 33 36 39
HR: 0.788 (95.34% CI: 0.699-0.927)
Placebo/FOLFIRIMedian: 12.4 mos
Aflibercept/FOLFIRIMedian: 13.9 mos
Pts at Risk, n PlaceboAFL
427426
403388
347348
286295
205222
139157
94112
6582
3862
No Previous Bevacizumab
2nd-Line FOLFIRI ± ziv-Aflibercept in mCRC (VELOUR): OS by Prior Bevacizumab
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
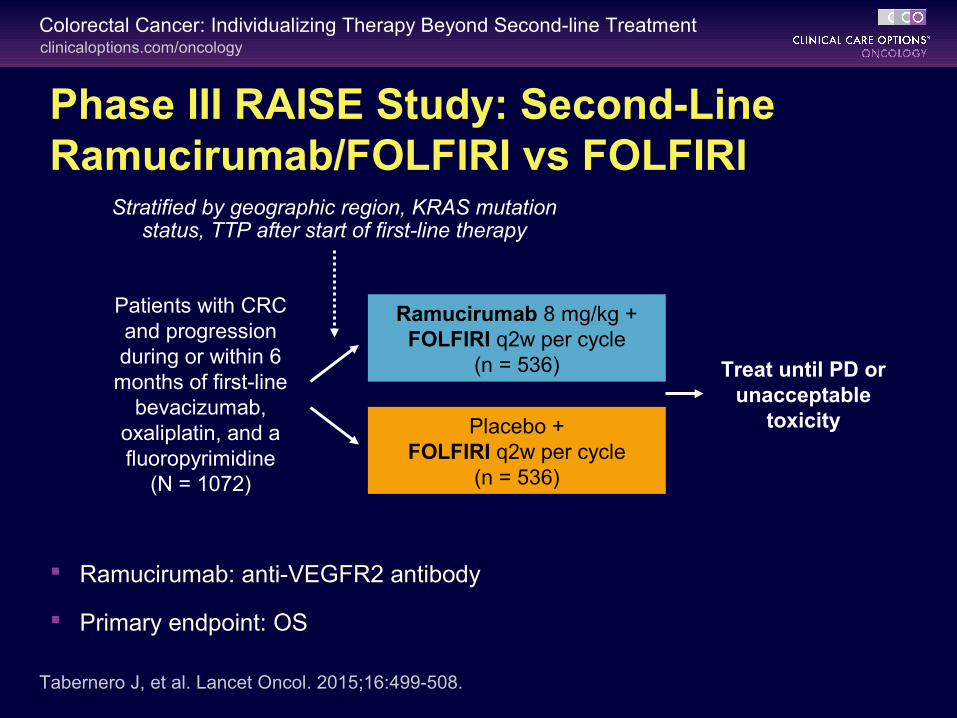
Phase III RAISE Study: Second-Line Ramucirumab/FOLFIRI vs FOLFIRI
Patients with CRC and progression during or within 6
months of first-line bevacizumab,
oxaliplatin, and a fluoropyrimidine
(N = 1072)
Treat until PD or unacceptable
toxicity
Ramucirumab 8 mg/kg +FOLFIRI q2w per cycle
(n = 536)
Placebo +FOLFIRI q2w per cycle
(n = 536)
Stratified by geographic region, KRAS mutation status, TTP after start of first-line therapy
Ramucirumab: anti-VEGFR2 antibody
Primary endpoint: OS
Tabernero J, et al. Lancet Oncol. 2015;16:499-508.

clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
Ramucirumab + FOLFIRI
Placebo + FOLFIRI
Median OS, mo(95% CI)
13.3(12.4-14.5)
11.7(10.8-12.7)
HR (95% CI) 0.844 (0.73-0.976) (stratified)P Value (log-rank) .0219 (stratified)
Second-Line Ramucirumab/FOLFIRI vs FOLFIRI (RAISE): Overall Survival
Tabernero J, et al. Lancet Oncol. 2015;16:499-508.
497 345 195 78 34 12 0536 421 269 114 53 422 0
486 329 166 66 22 2 1536 400 228 108 44 210 0
Pts at Risk, n
Placebo +
FOLFIRI
Ram + FOLFIRI
Ramucirumab + FOLFIRI Placebo + FOLFIRI
Overall S
urvival
0.2
0.4
0.6
0.8
1.0
00 6 12 18 24 30 3633 399 15 21 273 42
Mos
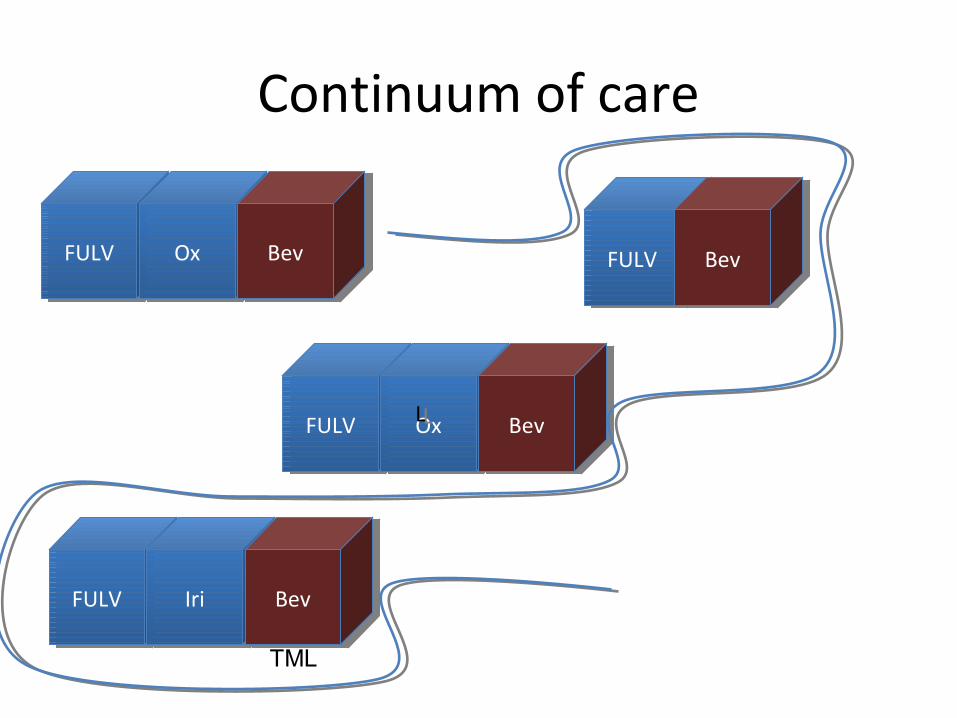
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev
LL
TML
OxOx Aflib.Aflib. Ramuc.Ramuc.
IriIri PanPan Ablative Rx
Ablative Rx
What to do when all else has failed?
CapecCapec CetCet SurgerySurgery
FULVFULV BevBev
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
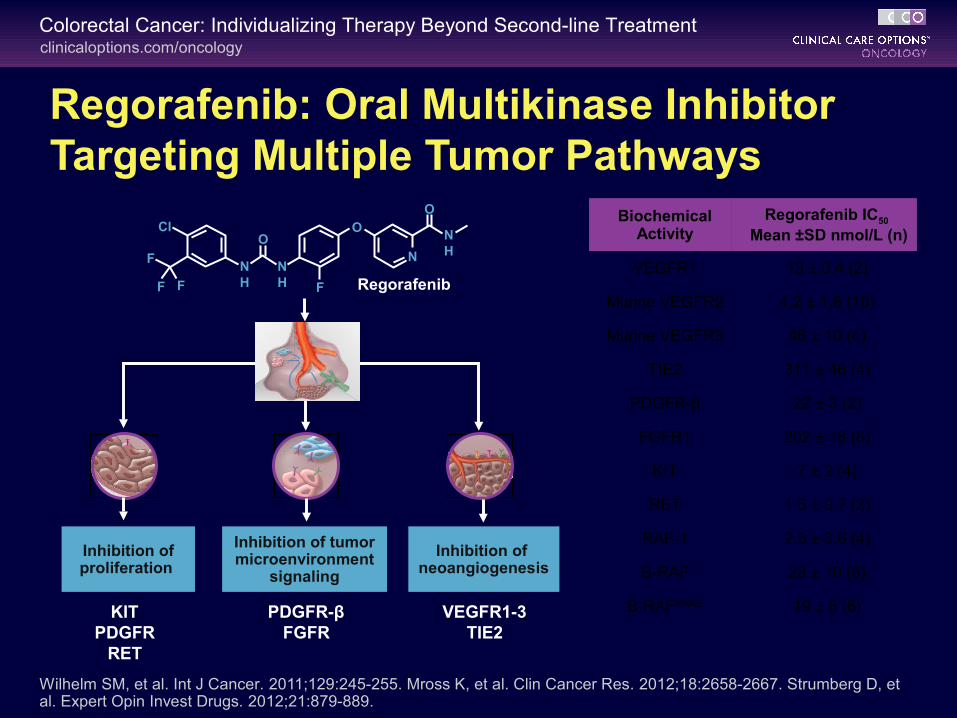
Inhibition of neoangiogenesis
Inhibition of tumor microenvironment
signaling
Inhibition of proliferation
Regorafenib: Oral Multikinase Inhibitor Targeting Multiple Tumor Pathways
Wilhelm SM, et al. Int J Cancer. 2011;129:245-255. Mross K, et al. Clin Cancer Res. 2012;18:2658-2667. Strumberg D, et al. Expert Opin Invest Drugs. 2012;21:879-889.
KITPDGFR
RET
PDGFR-βFGFR
VEGFR1-3TIE2
RegorafenibF
Cl
F
F F
OO
O
NH
NH
NH
N
BiochemicalActivity
Regorafenib IC50 Mean ±SD nmol/L (n)
VEGFR1 13 ± 0.4 (2)
Murine VEGFR2 4.2 ± 1.6 (10)
Murine VEGFR3 46 ± 10 (4)
TIE2 311 ± 46 (4)
PDGFR-β 22 ± 3 (2)
FGFR1 202 ± 18 (6)
KIT 7 ± 2 (4)
RET 1.5 ± 0.7 (2)
RAF-1 2.5 ± 0.6 (4)
B-RAF 28 ± 10 (6)
B-RAFV600E 19 ± 6 (6)
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
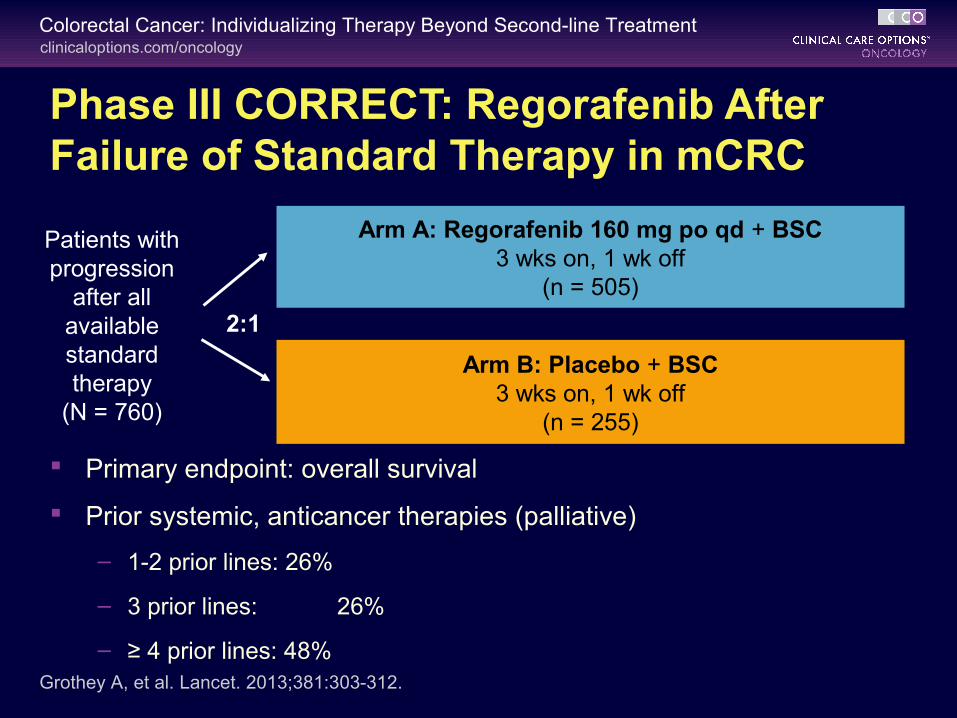
Phase III CORRECT: Regorafenib After Failure of Standard Therapy in mCRC
Primary endpoint: overall survival
Prior systemic, anticancer therapies (palliative)
– 1-2 prior lines: 26%
– 3 prior lines: 26%
– ≥ 4 prior lines: 48%
Patients with progression
after all available standard therapy
(N = 760)
Arm A: Regorafenib 160 mg po qd + BSC3 wks on, 1 wk off
(n = 505)
Arm B: Placebo + BSC3 wks on, 1 wk off
(n = 255)
Grothey A, et al. Lancet. 2013;381:303-312.
2:1
clinicaloptions.com/oncologyColorectal Cancer: Individualizing Therapy Beyond Second-line Treatment
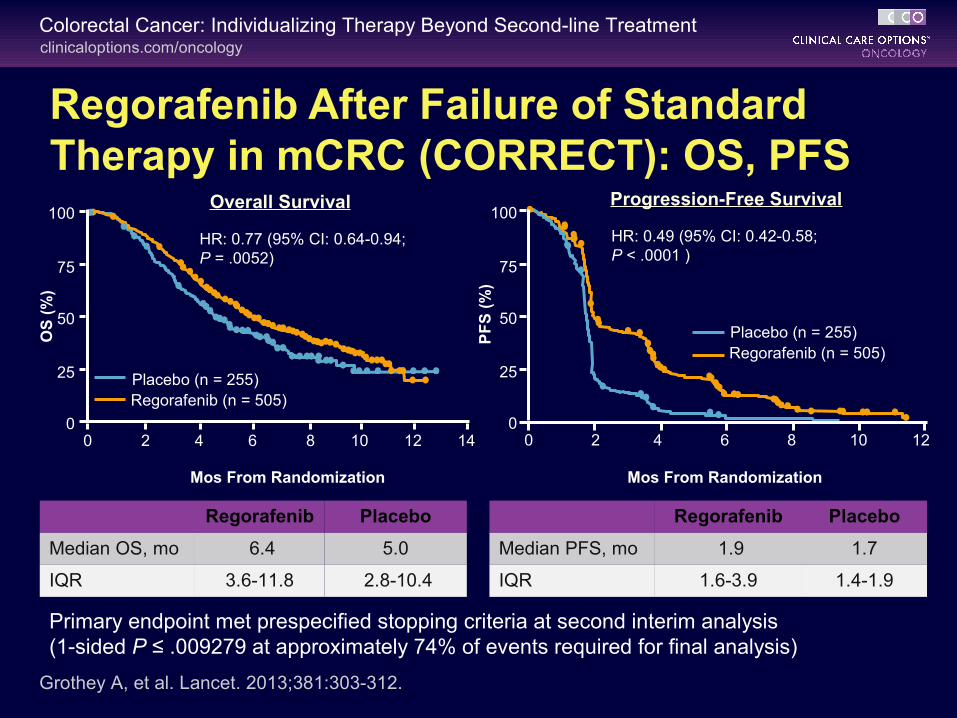
Regorafenib After Failure of Standard Therapy in mCRC (CORRECT): OS, PFS
Primary endpoint met prespecified stopping criteria at second interim analysis (1-sided P ≤ .009279 at approximately 74% of events required for final analysis)
100
50
25
0
75
Mos From Randomization
OS
(%
)
HR: 0.77 (95% CI: 0.64-0.94;P = .0052)
Regorafenib Placebo
Median OS, mo 6.4 5.0
IQR 3.6-11.8 2.8-10.4
Placebo (n = 255)Regorafenib (n = 505)
Grothey A, et al. Lancet. 2013;381:303-312.
0 2 4 6 8 10 12 14
Regorafenib Placebo
Median PFS, mo 1.9 1.7
IQR 1.6-3.9 1.4-1.9
0 2 4 6 8 10 12
Mos From Randomization
100
50
25
0
75
PF
S (
%)
Placebo (n = 255)Regorafenib (n = 505)
HR: 0.49 (95% CI: 0.42-0.58; P < .0001 )
Overall Survival Progression-Free Survival
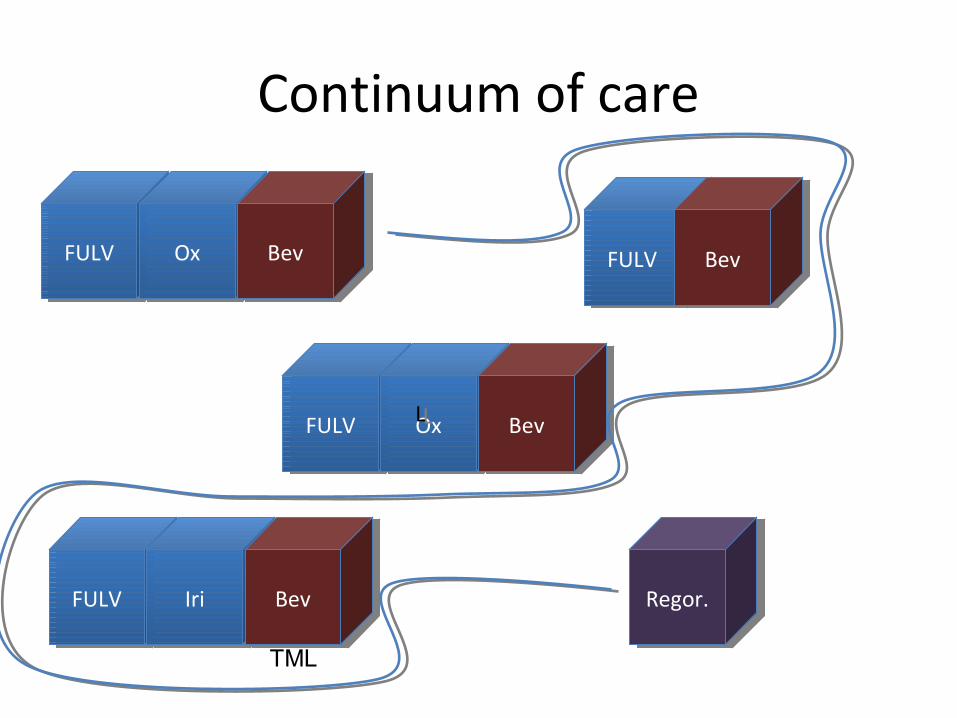
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev Regor.Regor.
LL
TML
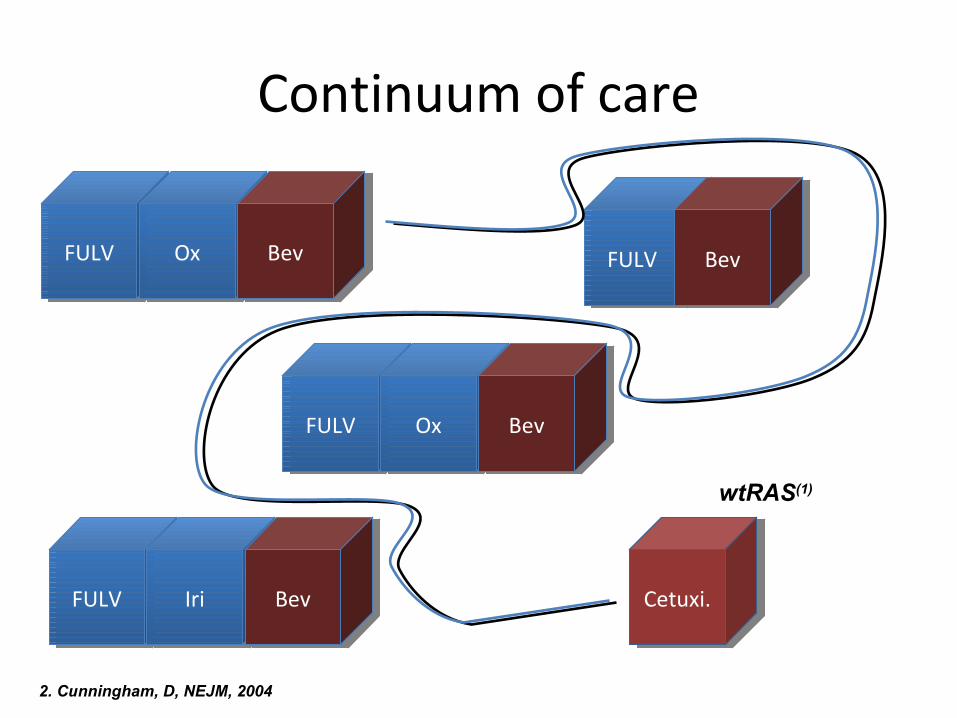
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev Cetuxi.Cetuxi.
wtRAS(1)
2. Cunningham, D, NEJM, 2004
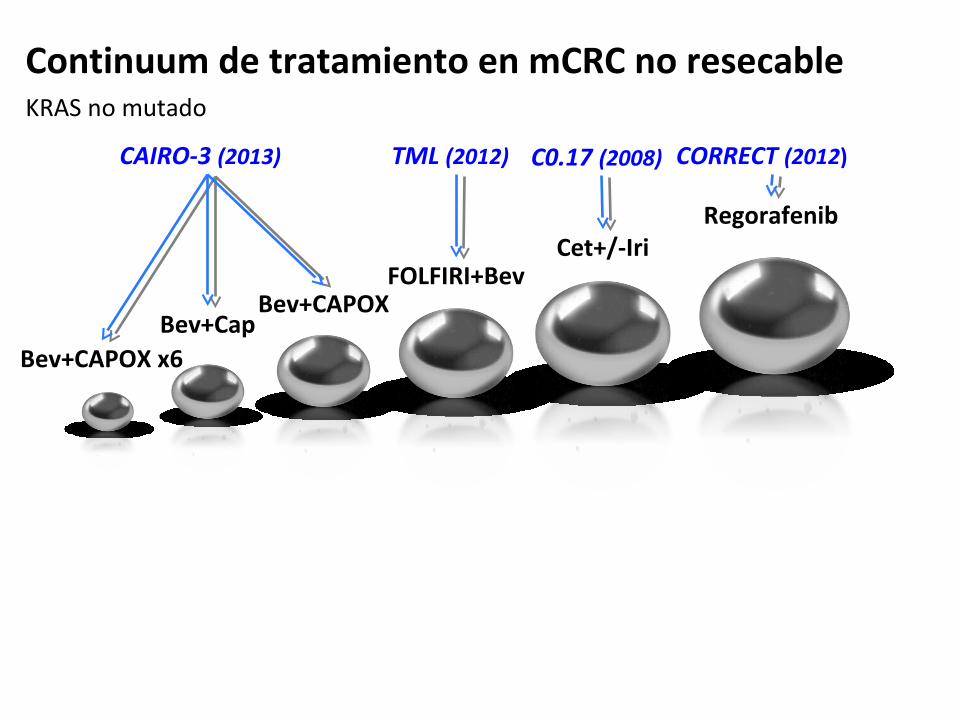
Continuum de tratamiento en mCRC no resecableKRAS no mutado
Bev+CAPOX x6Bev+Cap
Bev+CAPOXFOLFIRI+Bev
Cet+/-IriRegorafenib
CAIRO-3 (2013) TML (2012) C0.17 (2008) CORRECT (2012)
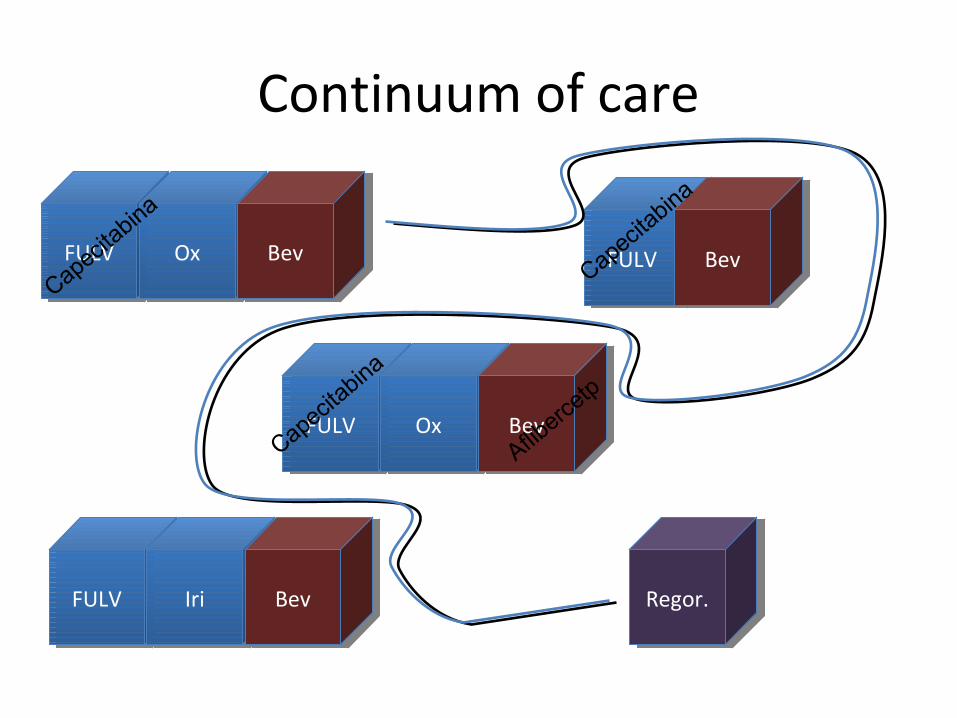
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev Regor.Regor.
Capecitabina
Capecitabina
Capecitabina
Afliberce
tp

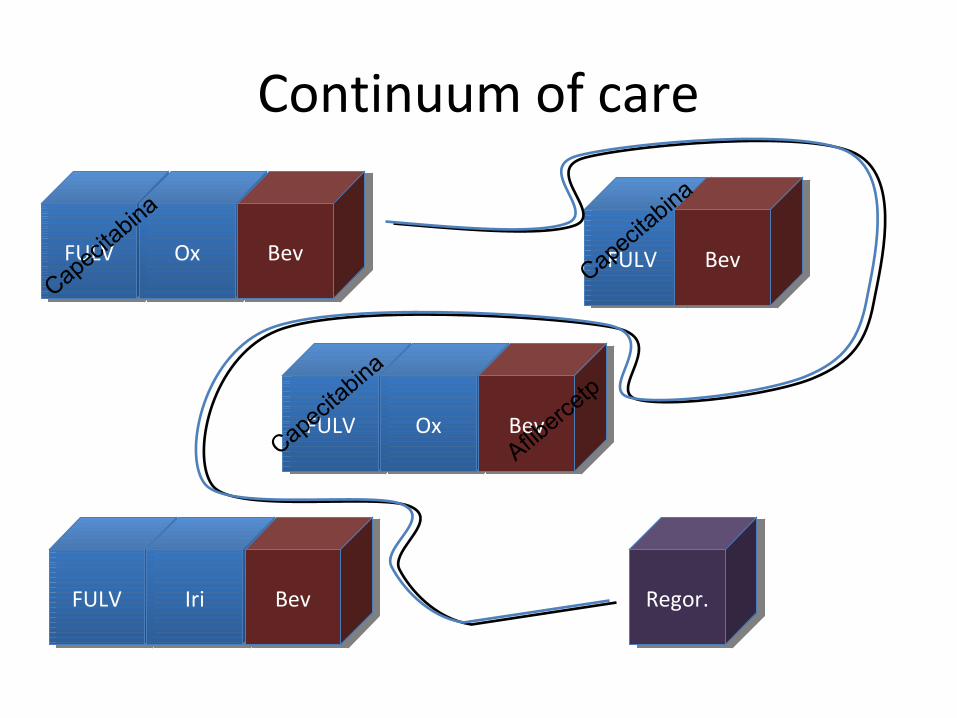
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev Regor.Regor.
Capecitabina
Capecitabina
Capecitabina
Afliberce
tp
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev Regor.Regor.
Capecitabina
Capecitabina
Capecitabina
Afliberce
tp
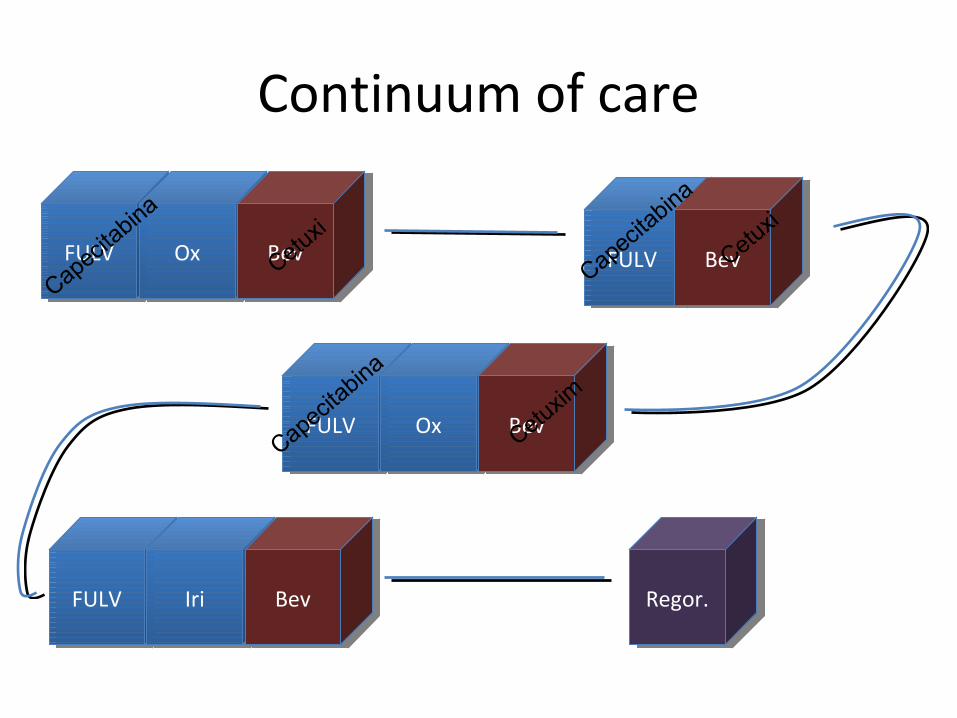
Continuum of care
FULVFULV OxOx BevBev
FULVFULV OxOx BevBev
FULVFULV BevBev
FULVFULV IriIri BevBev Regor.Regor.
Capecitabina
Capecitabina
Capecitabina
CetuxiCetuxi
Cetuxim
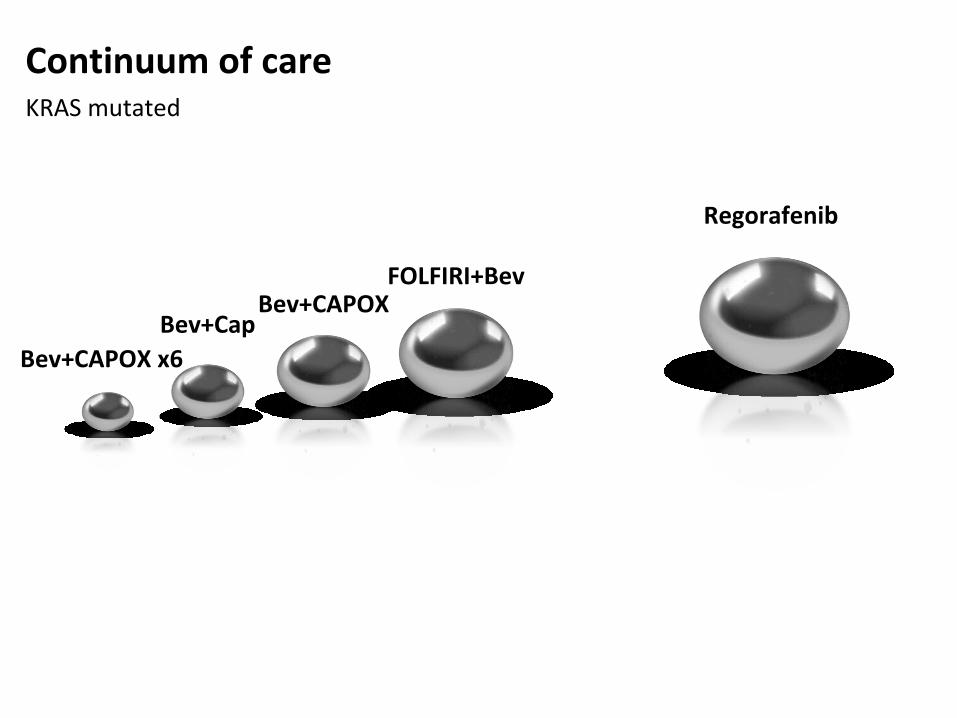
Continuum of careKRAS mutated
Bev+CAPOX x6Bev+Cap
Bev+CAPOXFOLFIRI+Bev
Regorafenib
What about patient related issues?
What to do with a patient only able to tolerate some chemo.
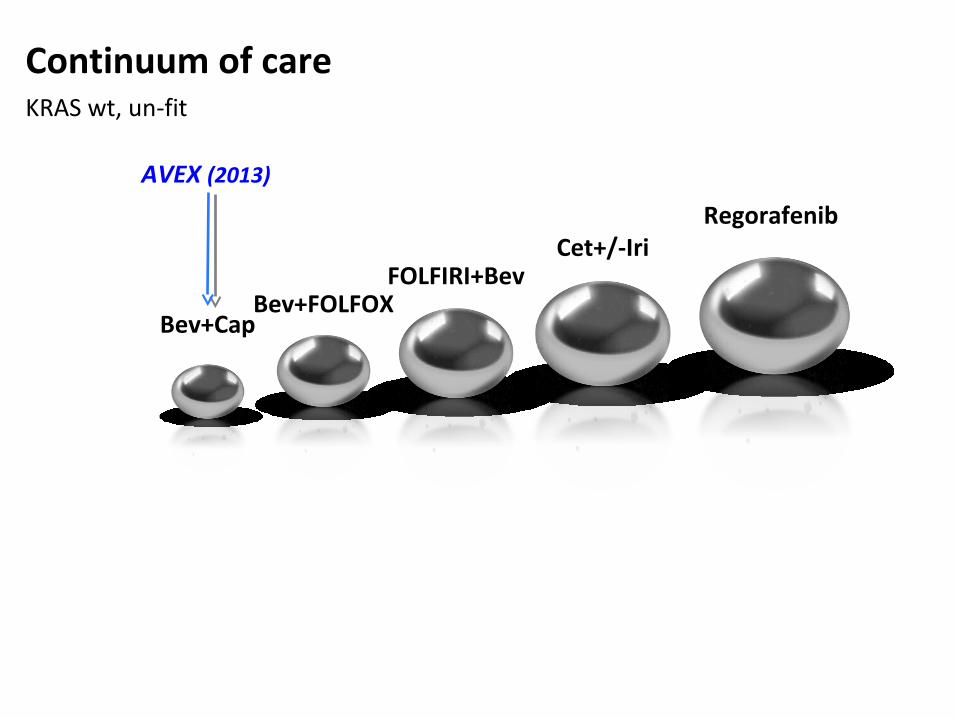
Continuum of careKRAS wt, un-fit
Bev+CapBev+FOLFOX
FOLFIRI+BevCet+/-Iri
Regorafenib
AVEX (2013)
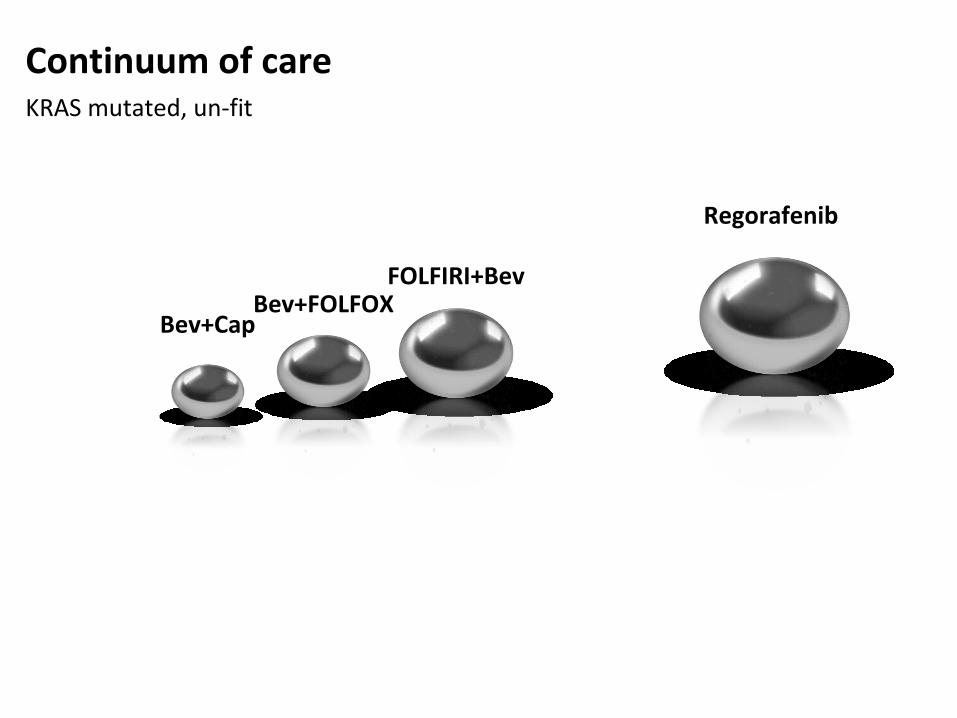
Continuum of careKRAS mutated, un-fit
Bev+CapBev+FOLFOX
FOLFIRI+Bev
Regorafenib
Do THESE guidelines, guide?
Maybe, but a more comprehensive strategy NEEDS to be thought –out
BEFORE therapy initiation.
Conclusions
Clinical presentation
Treatment toolkit
Rules of engagement
What WE desire
Patient preference
Tumor biology
Cost
Patient access
As of today, clinical practice guidelines for mCRC are but a
repository of treatment options filled with soft statements aimed more to convince insurers rather
than to truly guide clinicians.



















