Cáncer Renal; Cara a Cara: Tratamiento de 2a línea/ A ...€¦ · Hospital Universitario Central...
25
Cáncer Renal; Cara a Cara: Tratamiento de 2a línea/ A favor Inmunoncología Hospital Universitario Central de Asturias Servicio de Oncología Médica Emilio Esteban González
Transcript of Cáncer Renal; Cara a Cara: Tratamiento de 2a línea/ A ...€¦ · Hospital Universitario Central...

Cáncer Renal; Cara a Cara: Tratamiento de 2a línea/ A favor Inmunoncología
Hospital Universitario Central de Asturias Servicio de Oncología Médica Emilio Esteban González

Inmunoterapia – Carcinoma Renal
XD Liu et al. Cancer Immunol Res 2015

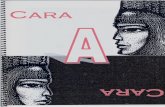
Mecanismos de Acción Agentes en segunda línea de tratamiento
aMitochondrial VEGFR-3 IC50 is 20 nM.
1. Axitinib EPAR assessment report; 2. Sorafenib EPAR; 3. Everolimus EPAR public assessment; 4. Wang C, et al. Cancer Immunol Res 2014; 2:846–
56; 5. Cabozantinib FDA; 6. You W-K, et al. Cancer Res 2011;71:4758–68; 7. Lenvatinib EPAR [All accessed April 2017].
Axitinib1 Sorafenib2 Everolimus3 Nivolumab4 Cabozantinib
5,6 Lenvatinib7
MoA VEGFR-TKI VEGFR-TKI mTOR inhibitor
PD-1 inhibitor
VEGFR-TKI VEGFR-TKI
Selectivity (IC50, <10 nM)
VEGFR-1 VEGFR-2 VEGFR-3 PDGFRα PDGFRβ
KIT
CRAF FKBP-12 PD-L1 PD-L2
VEGFR-2 VEGFR-3
MET RET AXL KIT
TRKB
VEGFR-1 VEGFR-2 VEGFR-3
RET
Potency (IC50, nM) VEGFR-1 VEGFR-2 VEGFR-3 MET AXL FGFR2
0.09–0.12 0.2 ± 0.06 0.1–0.29
– – –
–
90 –a
– – –
– – – – – –
– – – – – –
12.2
0.035 6.0 1.3 7.0 –
4.7 3.0 2.3 – –
27

4

ESTUDIO CheckMate 025 Patients previously treated with anti-angiogenic therapy
Primary endpoints: OS
Secondary endpoints: PFS, ORR, duration of objective response, duration of OS in PD-L1-
positive versus negative subgroups, safety, disease-related symptom progression rate
Eligibility
Advanced or mRCC with clear cell component
Received 1 or 2 prior anti-angiogenic therapy
Progression on or after most recent therapy (within 6 months of study enrolment)
Karnofsky PS ≥70
Nivolumab
3 mg/kg IV every 2 weeks
Everolimus
10 mg po daily
RANDOM I
SA T I ON
N=822
1:1
Treatment until
disease progression
or unacceptable
toxicity
clinicaltrials.gov (NCT01668784)
IV, intravenous; po, per os [oral administration]; PD-L1, programmed death ligand 1; PS, performance status
Study completion: Feb 2016

Motzer RJ et al. N Engl J Med 2015; 373:1803–1813.
Nivolumab (n=410) Everolimus (n=411)
Median age, years (range) 62 (23–88) 62 (18–86)
Male gender 77% 74%
MSKCC risk group
Favorable
Intermediate
Poor
35%
49%
16%
36%
49%
15%
Previous nephrectomy 89% 87%
Previous antiangiogenic regimens for RCC
1
2
72%
28%
72%
28%
Previous systemic therapy for mRCC
Sunitinib
Pazopanib
Axitinib
60%
29%
12%
59%
32%
12%
Patients with quantifiable PD-L1 expression
≥1%
<1%
90%
25%
75%
94%
23%
77%
CARACTERISTICAS PACIENTES

7
SUPERVIVENCIA GLOBAL (SG) Median OS, months (95% CI)
Nivolumab 25.0 (21.8–NE)
Everolimus 19.6 (17.6–23.1)
HR (98.5% CI): 0.73 (0.57–0.93)
P = 0.0018
0 3 6 12 9 15
Months
18 21 24 27 30 33
No. of patients at risk Nivolumab 410 389 359 337 305 275 213 139 73 29 3 0
411 366 324 287 265 241 187 115 61 20 2 0 Everolimus
0.0
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Ove
rall
Surv
ival
(P
rob
abili
ty)
Nivolumab
Everolimus
Minimum follow-up was 14 months.
NE, not estimable.

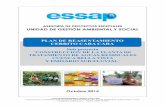
Resultados a dos años (SG)
8
Nivolumab
Ove
rall
Su
rviv
al
(Pro
ba
bil
ity)
0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
6 12 18
Months
24 30 36 42
Everolimus
Median OS,
months (95% CI)
Nivolumab 26.0 (22.2–29.6)
Everolimus 19.7 (17.6–22.3)
HR (95% CI) 0.73 (0.61–0.88)
P = 0.0006
3 9 15 21 27 33 39
No. at risk
Nivolumab
Everolimus 410 359 305 251 204 129 38 0
411 325 268 214 162 103 32 0
390 337 276 225 171 80 5
367 289 247 183 130 61 5
52%
76%
67%
42%
• Minimum follow-up was 26 months at the database lock on May 11, 2016 (Figure 2)
• Median OS benefit was observed with nivolumab versus everolimus in patients with
Memorial Sloan Kettering Cancer Center intermediate risk (21.9 vs 18.4 months, respectively)
and poor risk (15.3 vs 7.9 months) Adapted from poster presented by Plimack ER et al at the 15th International Kidney Cancer Symposium; November 4–5, 2016; Miami, FL, USA.


SG DEPENDIENDO DE LA EXPRESIÓN PD-L1
PD-L1 <1% (n = 76%)
Median OS, months (95% CI)
Nivolumab 21.8 (16.5–28.1)
Everolimus 18.8 (11.9–19.9)
No. of patients at risk
Nivolumab 94 86 79 73 66 58 45 31 18 4 1 0
Everolimus 87 77 68 59 52 47 40 19 9 4 1 0
0.0
0 3 6 12 9 15
Months
18 21 24 27 30 33
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Ove
rall
Surv
ival
(P
rob
abili
ty)
Nivolumab
Everolimus
PD-L1 ≥1% (n = 24%)
10
Median OS, months (95% CI)
Nivolumab 27.4 (21.4–NE)
Everolimus 21.2 (17.7–26.2)
276 265 245 233 210 189 145 94 48 22 2 0
299 267 238 214 200 182 137 92 51 16 1 0
Nivolumab
0 3 6 12 9 15
Months
18 21 24 27 30 33
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0.0
Everolimus
HR (95% CI): 0.79 (0.53–1.17)
HR (95% CI): 0.77 (0.60–0.97)

PD-L1 <5% (n=671) PD-L1 ≥5% (n=85)
Months 0
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
3 6 9 12 15 18 21 24 27 30 33 Months
0 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
3 6 9 12 15 18 21 24 27 30 33 Number of patients at risk
Nivolumab 44 41 38 36 33 28 22 16 9 1 1 0
Everolimus 41 38 31 27 23 21 17 6 3 2 1 0
Number of patients at risk
Nivolumab 326 310 286 270 243 219 168 109 57 25 2 0
Everolimus 345 306 275 246 229 208 160 105 57 18 1 0
Median OS, months (95% CI)
Nivolumab 21.9 (14.0–NE)
Everolimus 18.1 (10.3–NE)
Median OS, months (95% CI)
Nivolumab 24.6 (21.4–NE)
Everolimus 20.0 (17.7–24.7)
Nivolumab
Everolimus
Nivolumab
Everolimus
SG DEPENDIENDO DE LA EXPRESIÓN PD-L1

Líneas de tratamiento Posterior
12
Nivolumab N = 410
Everolimus N = 411
Subsequent systemic therapya, % Everolimus Axitinib Pazopanib Sunitinib Sorafenib Bevacizumab Cabozantinib Nivolumab
61 31 29 11 9 7 6 5 2
67 6
39 16 10 10 6 2 6
Median time from randomization to subsequent therapy, months (95% CI)
12.4 (10.3–13.2)
8.0 (7.0–9.6)
aSubsequent therapy received by ≥5% of patients
Adapted from poster presented by Plimack ER et al at the 15th International Kidney Cancer Symposium; November 4–5, 2016; Miami, FL, USA.

13
RESPUESTAS OBJETIVAS (ORR)
Nivolumab
N = 410
Everolimus
N = 411
Objective response rate, % 25 5
Odds ratio (95% CI)
P value
5.98 (3.68–9.72)
<0.0001
Best overall response, %
Complete response
Partial response
Stable disease
Progressive disease
Not evaluated
1
24
34
35
6
1
5
55
28
12
Median time to response,
months (range) 3.5 (1.4–24.8) 3.7 (1.5–11.2)
Median duration of response,
months (range)* 12.0 (0–27.6) 12.0 (0–22.2)
Ongoing response, n/N (%) 49/103 (48) 10/22 (45)


SUPERVIVENCIA LIBRE DE PROGRESIÓN (PFS)
No. of patients at risk Nivolumab 410 230 145 116 81 66 48 29 11 4 0 Everolimus 411 227 129 97 61 47 25 16 3 0 0
0 3 6 12 9 15
Months
18 21 24 27 30
0.0
0.3
0.1
0.2
0.4
0.5
0.6
0.7
0.8
0.9
1.0 P
rogr
ess
ion
-Fre
e S
urv
ival
(P
rob
abili
ty)
Nivolumab
Everolimus
Median PFS, months (95% CI)
Nivolumab 4.6 (3.7–5.4)
Everolimus 4.4 (3.7–5.5)
HR (95% CI): 0.88 (0.75–1.03)
P = 0.1135
In a post-hoc analysis of patients who had not progressed or died at 6 months, median PFS was 15.6 months for nivolumab vs 11.7 months for everolimus (HR (95% CI): 0.64 (0.47–0.88)) 15

EFECTOS ADVERSOS
16
Treatment-related AEs in >15% of patients in either arm
Adapted from poster presented by Plimack ER et al at the 15th International Kidney Cancer Symposium; November 4–5, 2016; Miami, FL, USA.
AE, % Nivolumab (n = 406)
Everolimus (n = 397)
Any Grade Grade 3/4 Any Grade Grade 3/4
Treatment-related AEs 79 19 88 37
Fatigue 33 2 34 3
Nausea 14 < 1 17 1
Pruritus 14 0 10 0
Diarrhea 12 1 21 1
Decreased appetite 12 < 1 21 1
Rash 10 < 1 20 1
Cough 9 0 19 0
Anemia 8 2 24 8
Dyspnea 7 1 13 < 1
Edema peripheral 4 0 14 < 1
Pneumonitis 4 1 15 3
Mucosal inflammation 3 0 19 3
Dysgeusia 3 0 13 0
Hyperglycemia 2 1 12 4
Stomatitis 2 0 29 4
Hypertriglyceridemia 1 0 16 5
Epistaxis 1 0 10 0

EECTOS ADVERSOS
aTime to resolution is based on the time of onset of the AE (not at the start of treatment). + indicates a censored value
GI = gastrointestinal; NR = not reached
17
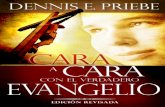
• The median time to onset of treatment-related select AEs with nivolumab was 7.3–17.4 weeks,
depending on AE category (Figure 3)
• The majority of treatment-related select AEs with nivolumab resolved (63%–89%, depending
on AE category), with the exception of endocrine AEs (37%) (Figure 3)
Time to onset and resolution of treatment-related select Aes
0 50 100 150 200
Weeks
Median time to onset (range)
7.3 (2.0–71.1)
Hepatic (n = 45; 11%)
Skin (n = 107; 26%)
GI (n = 56; 14%)
Renal (n = 28; 7%)
Endocrine (n = 41; 10%)
Pulmonary (n = 18; 4%)
8.4 (0.1–100.1)
10.1 (0.1–122.1)
10.6 (4.0–79.1)
16.4 (2.1–112.3)
17.4 (1.9–73.0)
0 5 0 1 0 0 1 5 0 2 0 0
W e e k s
M e d i a n t i m e t o r e s o l u t i o n a ( r a n g e )
H e p a t i c ( n = 3 7 / 4 4 ; 8 4 % )
S k i n ( n = 8 3 / 1 0 6 ; 78 % )
G I ( n = 4 7 / 5 6 ; 8 4 % )
R e na l ( n = 1 7 / 2 7 ; 6 3 % )
E n do c r i n e ( n = 1 5 / 4 1 ; 3 7 % )
P u l mo n a r y ( n = 1 6 / 1 8 ; 8 9 % )
8 . 0 ( 1 . 6 – 1 2 7 . 1 + )
1 6 . 0 ( 0 . 1 – 1 5 6 .6 + )
7 . 8 6 ( 0 . 1 – 1 3 2 . 1 + )
2 6 . 1 4 ( 0 . 6 – 1 0 9 . 1 + )
N R ( 1 . 9 – 1 4 1 . 9 + )
5 . 5 7 ( 1 . 3 – 9 6 . 1 + )
Adapted from poster presented by Plimack ER et al at the 15th International Kidney Cancer Symposium; November 4–5, 2016; Miami, FL, USA.

18
CALIDAD DE VIDA (QoL) CON FKSI-DRS
Questionnaire completion rate: ≥80% during the first year of follow-up.
Mean
Ch
an
ge F
rom
Baselin
e
Nivolumab
Everolimus
4 0 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100 104
W eek
-6
0
-4
-2
2
4
6
No. of patients at risk Nivolumab 362 334 302 267 236 208 186 164 159 144 132 1 19 1 12 97 90 89 81 72 63 59 53 44 43 31 30 26 20 Everolimus 344 316 270 219 191 157 143 122 102 97 87 74 73 63 58 49 44 35 30 28 24 21 15 12 12 9 9
Wo
rse
B
ett
er
▪ Mean change from baseline in the nivolumab group increased over time
and differed significantly from the everolimus group at each assessment
through week 76 (P<0.05)

DROGAS CON DIFERENTE
TOXICIDAD
aOutcomes from different clinical trials
should not be
directly compared because of differences
in trial design and patient populations.
1. Choueiri TK, et al. Lancet Oncol 2016;17:917–27. 2. Escudier B, et al. NEJM
2007;356:125–34. 3. Motzer RJ, et al. J Clin Oncol 2009; 27:3584–90 4. Motzer RJ,
et al. Cancer 2010;116:4256–65. 5. Rini BL, et al. Lancet 2011;378:1931–9. 6.
Motzer R, et al. NEJM 2015;373:1803–13. 7. Sternberg CN, et al. J Clin Oncol 2010;
28:1061–8; 8. Hutson TE, et al. J Clin Oncol 2014;32:760–7; 9. Nivolumab EPAR
[Accessed April 2017].
mTOR
TKI
ANOREXIA MUCOSAL INFLAMMATION
RASH STOMATITIS
VOMITING FATIGUE
DIARRHOEA NAUSEA
WEIGHT LOSS DECREASED APPETITE
CONSTIPATION
COUGH DYSPNOEA
ALOPECIA DRY SKIN
DYSGEUSIA DYSPEPSIA
DYSPHONIA HAIR DISCOLOURATION
HAND–FOOT SYNDROME HYPERTENSION
SKIN DISCOLOURATION HYPOTHYROIDISM
ANAEMIA
ASTHENIA
HYPERTRIGLYCERIDEMIA
INFECTIONS
PERIPHERAL OEDEMA
PRURITIS
PYREXIA
BACK PAIN I
O

Efectos secundarios y seguridad
Data do not constitute substantial evidence because they represent cross-study comparisons of trials conducted using different methodologies. a23 weeks; b141 days. NA, not available.
1. Motzer RJ, et al. Lancet Oncol 2013;14:552–62; 2. Axitinib EPAR;
[Accessed April 2017]; 3. Escudier et al. NEJM 2007;356:125–34; 4. Sorafenib EPAR [Accessed
April 2017]; 5. Motzer RJ, et al. Cancer 2010;116:4256–65; 6. Motzer RJ, et al. NEJM 2015;373:1803–13; 7. Nivolumab EPAR [Accessed April 2017]; 8.
Choueiri TK, et al. NEJM 2015;373:1814–23;
9. Choueiri TK, et al. Lancet Oncol 2016;17:917–27.
AXIS (N=723)1,2
TARGET (N=903)3,4
RECORD-1 (N=416)5
CheckMate-025 (N=821)6,7
METEOR (N=658)8
HOPE 205 (N=153)9
Experimental arm Axitinib Sorafenib Everolimus Nivolumab Cabozantinib Lenvatinib + everolimus
Median treatment duration, months
8.2 5.3a 4.7b 5.5 8.3 7.6
Any dose reduction, %
34 13 7 NA 62 71
Discontinued due to AEs, %
4 10 13 8.6 12 24
All causality AEs Grade 3/4, %
65.7 64.3 NA 53 71 71

Guidelines ESMO 2016
Escudier B, et al. ESMO 2016

Guidelines NCCN 2017 (USA): NCCN v2.2017

AXINIVO study design (Phase II)
Eligibility criteria
• Clear-cell mRCC
• Failure of prior first-line regimen containing an anti-angiogenic
• Measurable disease (RECIST v1.0) and non-measurable lesion that could be followed by the investigator
• ECOG PS ≤1
N=224
Strata: MSKCC risk
criteria
RANDOM I S A T I ON
1:1
Axitinib 5 mg BID
Nivolumab 3 mg/kg IV
every 2 weeks
Nivolumab 3 mg/kg IV
every 2 weeks
Axitinib 5 mg BID
Crossover upon
progression
Final OS
analysis
after the 3-
year follow-
up period

RESULTADOS DEL RAPID CARACTERIZACIÓN MOLECULAR

Nivolumab como representante de inmunoterapia moduladora anti
PD-1 ha demostrado mejorar la SG y QoL en 2 ª y 3ª línea frente a
Everolimus (vía m-TOR)
Nivolumab es una alternativa sólida al tratamiento anti-angiogénico
por su mecanismo de acción y perfil de toxicidad diferente
Precisar el valor de PD-L1 en tumor/células inmunológicas infiltrantes
o perfiles moleculares son imprescindibles para mejorar la estrategia
terapéutica actual
CONCLUSIONES