Cáncer de cervix mbe2
38
DIAGNÓSTICO DEL DIAGNÓSTICO DEL CÁNCER DE CÁNCER DE CÉRVIX CÉRVIX SESIÓN MBE SESIÓN MBE Amelia Jiménez Amelia Jiménez Raquel Garófano Raquel Garófano
-
Upload
daniel-alejandro -
Category
Documents
-
view
102 -
download
2
Transcript of Cáncer de cervix mbe2

DIAGNÓSTICO DIAGNÓSTICO DEL CÁNCER DE DEL CÁNCER DE
CÉRVIXCÉRVIXSESIÓN MBE SESIÓN MBE
Amelia JiménezAmelia Jiménez
Raquel GarófanoRaquel Garófano

1.- JUSTIFICACIÓN DEL CASO1.- JUSTIFICACIÓN DEL CASO
Programa de diagnóstico precoz: ha demostrado más eficacia ⇛ permitiendo el diagnóstico y tratamiento de LESIONES PRECANCEROSAS.
Se evita la progresión a CARCINOMAS INVASIVOS.
Herramienta básica y esencial para el médico de atención primaria.
2º Cáncer más común en las mujeres a nivel mundial.
2.- GENERALIDADES2.- GENERALIDADES
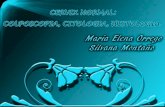
1. ANATOMÍA DEL CUELLO: Endocérvix: cilíndrico monoestratificado. Exocérvix: escamoso poliestratificado. Unión escamo-columnar.2. CA. IN SITU: Lesión en la que parte del grosor del
epitelio células atípicas, sin que sobrepase la ⇒membrana basal.
3. EPIDEMIOLOGÍA: Máxima incidencia entre los 45-55años.

3.- ETIOLOGÍA3.- ETIOLOGÍA• INFECCIÓN POR VPH: causa necesaria pero no
suficiente. Hay 25 serotipos pero los oncogénicos son: 16 y 18 16 y 18 ( 70% de los tumores), 53, 31, 33 y 35.
• COFACTORES DE ADQUISICIÓN: inicio temprano de relaciones y promiscuidadpromiscuidad.
• COFACTORES DE PERSISTENCIA-PROGRESIÓN: Virales (VPH:16-18), genéticos, medioambientales (paridad, ACOs, tabaco, ID, infecciones asociadas (VHS-2, C. trachomatis).
• COFACTORES DE INVASIÓN: F. angiogénicos.
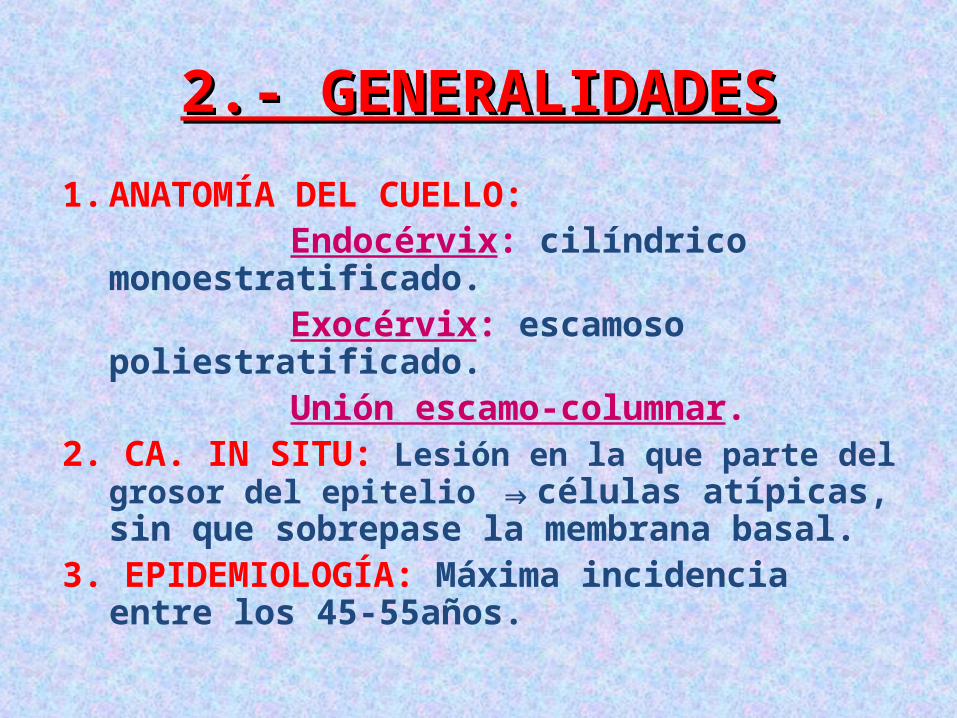
4.- ANATOMÍA PATOLÓGICA4.- ANATOMÍA PATOLÓGICA
EPITELIO NORMAL
INFECCIÓN POR EL VPH
LSIL CIN1
HSIL CIN 2-3
CARCINOMA MICROINVASIVO
CARCINOMA INVASIVO
Co. Adquisición
Co. Invasión
Co. Progresión

5.- DIAGNÓSTICO5.- DIAGNÓSTICO
•TÉCNICAS DE CRIBADOTÉCNICAS DE CRIBADO•PAUTAS DE DIAGNÓSTICOPAUTAS DE DIAGNÓSTICO

• TÉCNICAS DE CRIBADO:TÉCNICAS DE CRIBADO: 1.Citología cevico-vaginal: método de selección para
una confirmación posterior: colposcopia y anatomía patológica. +: ↑ tamaño (x3) e irregularidad nuclear. Baja sensibilidad para las atipias de bajo grado.
2.Colposcopia: junto a citología. Test de Schiller (lugol).
Cribado o para dirigir la bx. Imágenes atípicas: punteado, mosaico, acetoblanco, yodo-negativo, vasos atipicos.
3.Test de VPH-DNA: Captura híbrida o RCP. Útiles en:
mujeres con ASCUS, postmenopáusicas con L-SIL, seguimiento de los CIN tras tratamiento, test de cribado.

1ªCITOLOGÍA 3años despues del 1 coito, o
a los 25 años
Citología anual por 2 añosRepetir cada
3 años
Ambas normales>35 años
Fin del cribado 65 años
Ambos negativos
Citología –VPH + Citología +
Citología y VPH al año
Protocolo de citología anormal
Citología y ADN-VPH
Citología y VPH/5 años

CitologíaRepetir al año
ASC-USLSIL
<25añosLSIL >25 años, ASC-H,
HSIL, AGC, AIS, Ca.
>25años ADN-VPH
Citología a 6 y 12m
Citología a 6 y 12m
Negativo Positivo Cualquiera positiva
Ambas negativas
Cualquiera positiva
Colposcopia Cribado Colposcopia
Colposcopia

PAUTAS DE DIAGNÓSTICO:PAUTAS DE DIAGNÓSTICO:1. Bx dirigida: lesiones atípicas visibles mediante colposcopia.2. Legrado endocervical: -Sospecha de lesión endocervical. -Zona de transformación atípica no es totalmente visible. -Citología anormal y colposcopia no valorable (UEC
intracervical). -Citología anormal y colposcopia normal.3. Colpomicrohisteroscopia con biopsia: -Atipia de células cilíndricas. -Sospecha de adenocarcinoma. -Colposcopia no valorable.4. Conización: diagnóstico definitivo y muchas veces tto. -CIN en citología y colposcopia normal. -Diagnóstico de CIN 3 en biopsia. -Legrado endocervical positivo para CIN.
6.- CLASIFICACIONES6.- CLASIFICACIONES
A.A. CITOLÓGICA (BETHESDA 2001)CITOLÓGICA (BETHESDA 2001)B.B. ANÁTOMO-PATOLÓGICA ANÁTOMO-PATOLÓGICA
MEDIANTE BIOPSIA (RICHART)MEDIANTE BIOPSIA (RICHART)

A.A. CITOLÓGICA (BETHESDA 2001):CITOLÓGICA (BETHESDA 2001):
1.1. --Citología normal
2. -2. -Citología inflamatoria, ASC-US y AGSASC-US y AGS: : repetir citología, colposcopia, detección ADN-VPH, en postmenopáusicas→tto estrogénico previotto estrogénico previo.
ASC-USASC-US: Células Atípicas escamosas de significado incierto. AGS:AGS: Células Atípicas glandulares de significado incierto.
3. 3. -Lesión intraepitelial escamosa de bajo grado bajo grado o L-SILL-SIL ≈ CIN 1 y HPV sin CIN. (1/3 inf).
4. -4. -De alto grado alto grado o H-SIH-SIL≈ CIN 2 y 3: se deben biopsiar biopsiar todas y tratar tras la confirmación histológica.
5.5. -AIGAIG(Lesión glandular intraepitelial).
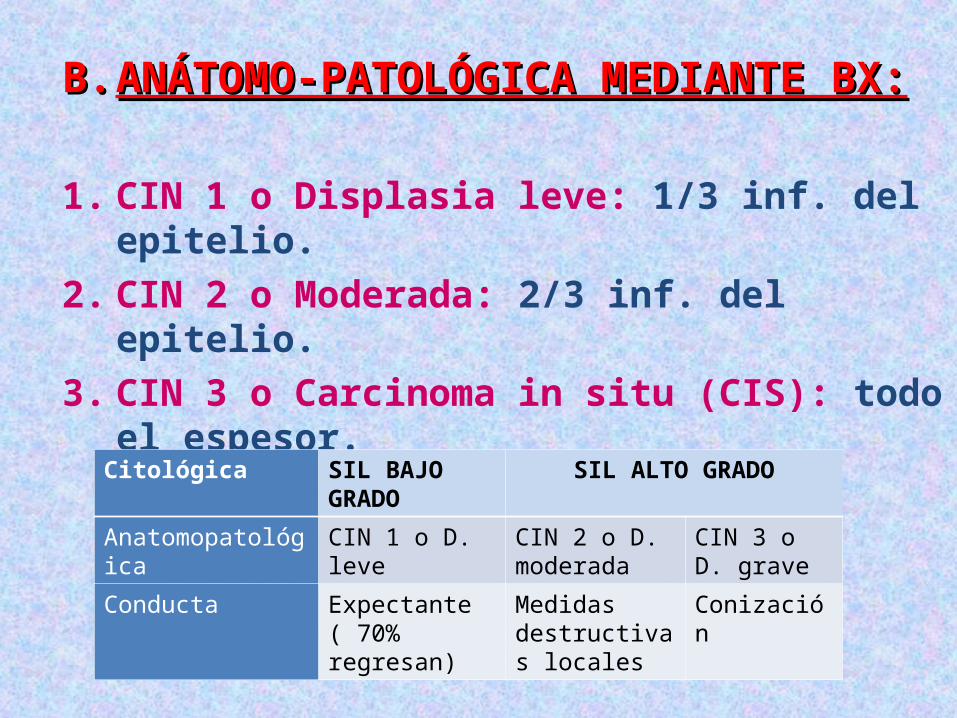
B.B. ANÁTOMO-PATOLÓGICA MEDIANTE BX:ANÁTOMO-PATOLÓGICA MEDIANTE BX:
1. CIN 1 o Displasia leve: 1/3 inf. del epitelio.2. CIN 2 o Moderada: 2/3 inf. del epitelio.3. CIN 3 o Carcinoma in situ (CIS): todo el espesor.
Citológica SIL BAJO GRADO SIL ALTO GRADO
Anatomopatológica CIN 1 o D. leve CIN 2 o D. moderada
CIN 3 o D. grave
Conducta Expectante ( 70% regresan)
Medidas destructivas locales
Conización

7.- TRATAMIENTO7.- TRATAMIENTOa.a. Destructivo local:Destructivo local: - Condiciones: - Condiciones: lesión visible en colposcopia, UEC visible y
legrado cervical normal. - Tipos: - Tipos: electrocoagulación, crioterapia ó vaporización vaporización
con láser.con láser. -Indicaciones: -Indicaciones: condiloma cervical y CIN 1-2.
b.b. Quirúrgico o escisional:Quirúrgico o escisional: - Conización:- Conización: bisturí frío (glandular), láser o asa de
diatermia (escamosa). Fertilidad. - Histerectomía: - Histerectomía: conizaciónconización con bordes no libres,
extensión de la lesión a bóveda vaginal, edad avanzada o problemas ginecológicos asociados. Es el tratamientotratamiento más definitivo del CIN.

8.- SEGUIMIENTO8.- SEGUIMIENTO
• CIN 2-3: CIN 2-3: 5-10%5-10% presentan enfermedad residual tras la conización.
• Citológicos: Citológicos: - - Mínimo 24 meses24 meses - Trimestrales el primer año - Semestrales el 2º año• VIH +: VIH +: incidencia global del CIN 10-25%.10-25%.• Gestantes: Gestantes: - - Confirmar CIN con Biopsia.Biopsia. - - Trimestral: citología y colposcopia. - - CIN no invasivo: tratamiento posparto.

9.- CA. DE CÉRVIX9.- CA. DE CÉRVIX• Síntomas: Síntomas: Hemorragia genitalHemorragia genital: el más frecuente. Sangrado postcoital, leucorrea sucia y tardíamente dolor. El dolor: síntoma frecuente en ca. cérvix avanzado.• Diagnóstico: Diagnóstico: DeDe certezacerteza: biopsia biopsia de zonas sospechosas. De extensión: De extensión: urografía endovenosa, TAC, enema opaco y Rx
tórax. Cito-rectoscopia. Opcionales:Opcionales: RMN (parametrios, vol. tumoral), TAC o PET
(ganglios linfáticos), marcadores tumorales (SCC,CEA y Ca125), laparoscopia.
• Estadiaje:Estadiaje: basado en EF y pruebas radiológicas. Estadío I: confinado a cérvix. Estadío II: más allá del cérvix. Estadío III Estadío IV: extensión más allá de pelvis.

ESTADÍO TRATAMIENTO DE ELECCIÓN
IA1: sin inflitración linfovascular - Conización (mujer joven + deseo genésico).- Histerectomía extrafascial simple o RT intracavitaria aislada.
IA2, IB, IIA, IA1 con infliltración linfovascular
- Histerectomía radical (Wertheim o Schauta).- Con RT posterior cirugía incompleta, 2 ganglios +, tumor > 4cm o recurrencia.- QT o RT neoadyuvante.
IIB - RT radical + QT
III y IVA - RT radical
IVB - Paliativo: QT+/-RT

10.- VACUNA VPH10.- VACUNA VPH1.- 1.- Características:Características: Las vacunas van dirigidas contra
los genotipos: Genotipos 6,11: Genotipos 6,11: verrugas anogenitales. Genotipos 16 y 18: Genotipos 16 y 18: lesiones cervicales
premalignas y cáncer de cérvix.
2.- 2.- Indicaciones:Indicaciones: Gardasil:Gardasil: profilaxis 1ª de la ITS producida por VPH VPH
6,11,16 y 18.6,11,16 y 18. Cervarix:Cervarix: prevención de las lesiones cervicales
premalignas y cáncer de cérvix relacionados causalmente con VPH 16 y 18VPH 16 y 18.
3.- 3.- Recomendaciones de las Sociedades:Recomendaciones de las Sociedades: -Documento de Consenso 2008 de las SCE:-Documento de Consenso 2008 de las SCE: 1.-Niñas de 9-14 años: máxima prioridad. 2.-Mujeres hasta 25/26 años: alta prioridadalta prioridad. 3.-Mujeres mayores de 26 años: indicación debe
individualizarse. 4.-Varones: sin indicación. -Ministerio de Sanidad y consumo: -Ministerio de Sanidad y consumo: vacunación sistemática de las
niñas en una única cohorte, entre los 11 y 14 años de edadentre los 11 y 14 años de edad.
4.- 4.- Contraindicaciones y precauciones: Contraindicaciones y precauciones: hipersensibilidad, <10años y embarazadas. No se ha demostrado la interacción con ACOs. Enfermedad aguda grave: posponer la vacuna.
Precio de venta en España: Gardasil: Gardasil: P.V.P: 464€ / tres dosis. Cervarix: Cervarix: P.V.P: 449 € / tres dosis.
CLINICAL CASECLINICAL CASESetting: Woman Clinic at Primary Care.History of the presenting complaint: 35 years
old woman who asks for a gynaecological check up.
Past history: She has never been followed up at the woman clinic. She has a permanent partner and no history of previous illnesses. She hasn´t got any children and has never been pregnant. She started sexual relations 7 years ago.
Family history: None. Clinical examination: Nothing to report.
CLINICAL QUESTIONCLINICAL QUESTION
• Which screening test is better for Which screening test is better for cervical cancer diagnose in adult cervical cancer diagnose in adult women?women?
P I C O
ADULT WOMEN
HPV TEST PAP MORE ACCURATE DIAGNOSE

WHY THIS QUESTION?WHY THIS QUESTION?Cervical cancer is the second most
common cancer in women.HPV is being used in clinical
practice to triage for colposcopy those women wih a PAP with ASCUS ( atypical squamous cell of undetermined significance).
Cotesting increases cost. Previous data from cross sectional
studies.

BIBLIOGRAPHY SEARCHBIBLIOGRAPHY SEARCH
• “Cervical intraepithelial neoplasia” AND “Diagnose” in (MESH) with the limits: published in the last 3 years, free full text, humans, randomized controlled trial.
• 7 articles. “Human papillomavirus DNA versus Human papillomavirus DNA versus
Papanicolaou screening tests for cervical Papanicolaou screening tests for cervical cancer”cancer”
New England Journal of Medicine,October 2007New England Journal of Medicine,October 2007
SUMMARY Goal: Determine wether HPV test is superior to Pap test for cervical cancer screening.
10154 randomized from Montreal and St John´s in Canada.
2 groups: First test: Index text:• Focus in Pap. • Focus in HPV. End point: High grade (2 or
higher) cervical intraepithelial neoplasia.

INTERNAL VALIDITYINTERNAL VALIDITYPrimary CriteriaPrimary Criteria
BLIND AND INDEPENDENT COMPARISON WITH THE GOLD STANDARD?
Gold standard: Biopsy. Assignment of the test done at the coordination center by a computer-assisted block randomization. The Pap test were read at the participating sites by citotechnologists and cytopathologists without knowledge of the patient´s status as a participant or her HPV test result. The colposcopist and pathologist evaluating the biopsy were unaware of the screening-test results.

INTERNAL VALIDITYINTERNAL VALIDITYPrimary CriteriaPrimary Criteria
ADEQUATE SAMPLE?10154 from two clinics in Canada.30-69 years. Excluded: cervical lesion, lacked a cervix, pregnant, history of cervical cancer, undergone Pap testing in the previous year, unable to provide consent.

INTERNAL VALIDITYINTERNAL VALIDITYSecondary CriteriaSecondary Criteria
DOES THE NEW TEST RESULTS NEED CONFIRMATION WITH THE GOLD STANDARD?
The confirmation in both of them has been made with colposcopy which its the procedure needed to get to the end point.
Estimates corrected for verification bias.

INTERNAL VALIDITYINTERNAL VALIDITYSecondary CriteriaSecondary Criteria
HAS THE NEW TEST BEEN EXPLAINED IN DETAIL?DNA HPV test : The Hybrid Capture 2 test(HC2 probe B, Digene). The manufacter has no role in the study. Supplies purchased at the regular cost.Specimens were considered positive if the ratio of relative light units (RLUs) of the specimen to the mean RLU of positive control triplicates
was at least 1.

RESULTSRESULTSFOCUS ON HPV TESTING:
CONTINGENCY TABLE
CIN2 POSITIVE CIN2 NEGATIVE
HPV POSITIVE
19 (TP) 294 (FP)
HPV NEGATIVE
1 (FN) 746 (TN)

FOCUS ON HPV:FOCUS ON HPV:
SEN= TP / TP + FN = 19/19+1= 0.95 95% of women with CIN have a positive HPV
test.
SPEC= TN / TN + FP = 746/746+294= 0.71 71% of women without CIN have a negative
HPV test.
PPV= TP / TP + FP = 19/19+294= 0.06 6% of women with a positive HPV test suffer
of CIN.
NPV= TN/ TN + FN = 746/746+1= 0.99 99% of women with a negative HPV test dont
suffer of CIN.

LIKELIHOOD RATIOLIKELIHOOD RATIOPPRT= SEN / 1-SPEC = 0.95/1-0.71= 3.2 (>1)
In the group of women with a diagnose of CIN in the biopsy, the chance of having a positive HPV test is 3.2 times more likely than in women without a CIN diagnose in the biopsy.
NPRT = 1-SPEC / SEN = 1-0.71 / 0.95= 0.30 (<1)
Easier interpretation: 1/0.30= 3.3 In the group of women without CIN in the biopsy, the
chance of finding a negative HPV test is 3.3 times more likely than in women with CIN in the biopsy.
.

FOCUS ON PAP:
CONTINGENCY TABLE
CIN2 POSITIVE CIN2 NEGATIVE
PAPPOSITIVE
12 (TP) 139 (FP)
PAPNEGATIVE
9 (FN) 522 (TN)

FOCUS ON PAP:FOCUS ON PAP:
SEN= TP / TP + FN = 12/12+9= 0.57 57% of women with CIN have a positive PAP
test.
SPEC= TN / TN + FP = 522/522+139= 0.78 75% of women withouth CIN have a negative
PAP test.
PPV= TP / TP+VN = 12/139+12= 0.079 7.9% of women with a positive PAP test suffer of
CIN.
NPV= TN / TN+FN = 522/522+9= 0.98 98% of women with a negative PAP test don’t
suffer of CIN.

LIKELIHOOD RATIOLIKELIHOOD RATIOLRPT= SEN / 1-SPEC = 0.57/1-0.78= 2.5 (>1)
In the group of women with a diagnose of CIN in the biopsy, the chance of having a positive PAP test is 2.5 times more likely than in women without a CIN diagnose in the biopsy.
LRNT = 1-SPEC / SEN = 1-0.78 / 0.57= 0.38 (<1)
Easier interpretation: 1/0.38= 2.6 In the group of women without CIN in the biopsy, the
chance of finding a negative HPV test is 2.6 times more likely than in women with CIN in the biopsy.
.

COMPARISONCOMPARISON• SENSITIVITY:SENSITIVITY:
95% of HPV against 57% of PAP 95% of HPV against 57% of PAP o SPECIFICITY:SPECIFICITY:
78% of PAP against 71% of HPV.78% of PAP against 71% of HPV.o POSITIVE PREDICTIVE VALUE:POSITIVE PREDICTIVE VALUE:
7.9% OF PAP against 6% of HPV.7.9% OF PAP against 6% of HPV.o NEGATIVE PREDICTIVE VALUE:NEGATIVE PREDICTIVE VALUE:
99% of HPV against 98% of PAP.99% of HPV against 98% of PAP.o LRPT:LRPT:
3.2 in HPV against 2.5 in PAP.3.2 in HPV against 2.5 in PAP.o LRNT:LRNT:
3.3 in HPV against 2.6 in PAP.3.3 in HPV against 2.6 in PAP.

¿ME AYUDARÁN LOS RESULTADOS EN LA ¿ME AYUDARÁN LOS RESULTADOS EN LA ASISTENCIA DE MIS PACIENTES?ASISTENCIA DE MIS PACIENTES?
1.1. ¿Serán tanto la reproducibilidad del resultado del examen como su ¿Serán tanto la reproducibilidad del resultado del examen como su interpretación satisfactorias en mi ámbito?interpretación satisfactorias en mi ámbito?
Sí, puesto que en el apartado SCREENING TEST especifica que los resultados del Pap test son informados y clasificados Pap test son informados y clasificados de acuerdo a la clasificación de Bethesda 2.001Bethesda 2.001, , sistema que usamos en nuestro medio. Así como para detectar VPH detectar VPH utilizando para ello la PCRPCR. .
Tener en cuenta que la interpretacion dependerá de la preparaciónpreparación que presenten los anatomopatólogos.
2.2. ¿Son aplicables los resultados a mi paciente?¿Son aplicables los resultados a mi paciente? Sí, Sí, puesto que la paciente del caso clínico cumple los criterios de cumple los criterios de
inclusióninclusión no violando ninguno de los de exclusión exclusión (lesión cervical, ausencia de cuello uterino, embarazo, hª previa de Cáncer de Cérvix, no Pap test en años anteriores, no querían firmar consentimiento informado).

PLEASE DONT HIDE!PLEASE DONT HIDE!WE WOULD LIKE TO HEAR YOUR OPINIONSWE WOULD LIKE TO HEAR YOUR OPINIONS
11.- BIBLIOGRAFÍA11.- BIBLIOGRAFÍA• http://www.fisterra.com/guias2/actividades.asp• http://www.fisterra.com/Vacunas/papilomavirus.asp• Shepherd J, Weston R, Peersman G, Napuli IZ. Intervenciones para la
prevención del cáncer cervical mediante modificaciones de la conducta y estilos de vida sexuales (Revisión Cochrane traducida). En: En: La Biblioteca Cochrane Plus, númeroLa Biblioteca Cochrane Plus, número 3, 2008. Oxford 3, 2008. Oxford, Update Software Ltd. Disponible en: http://www.update-software.com.
• Martín Zurro A., Cano Pérez J.F. Patología obstétrica. En: Martín Zurro A., Cano Pérez J.F. Atención Primaria: conceptos, organización y práctica clínica. Vol.2. 6ª edición. Madrid: Elsevier; 2008. P. 1.118-1.128.
• Acién Álvarez P. VI Cánceres genitales y extragenitales en el embarazo. En: Acién Álvarez P. Tratado de obstetricia y ginecología: obstetricia. 2ª edición. Alicante: Molloy; 2001.
P: 547-550• Proceso de cáncer de cervix. Sistema Andaluz de Salud.