Amanda Brandt, MS, CGC Oncología Ginecológica y … · representa a un hombre y un círculo que...
20
1 PowerPoint Slides English Spanish Translation “Identification of High-risk Patients” Video Transcript “Identificación de pacientes de alto riesgo” Transcripción del video Professional Oncology Education Hereditary Breast and Ovarian Cancer Series Time: 25:25 Educación Oncológica Profesional Serie sobre cáncer hereditario de mama y ovario Duración: 25:25 Amanda Brandt, MS, CGC Certified Genetic Counselor Clinical Cancer Genetics Program Gynecologic Oncology and Reproductive Medicine The University of Texas MD Anderson Cancer Center Amanda Brandt, MS, CGC Asesora Genética Certificada Programa de Genética Clínica del Cáncer Oncología Ginecológica y Medicina Reproductiva MD Anderson Cancer Center de la Universidad de Texas Welcome. My name is Amanda Brandt. I am one of the Cancer Genetic Counselors at the University of Texas MD Anderson Cancer Center. Today, we are going to be discussing how to identify patients at high risk for hereditary breast and ovarian cancer syndrome. Bienvenido. Mi nombre es Amanda Brandt y soy una de las asesoras genéticas de cáncer del MD Anderson Cancer Center de la Universidad de Texas. Hoy hablaremos de cómo identificar a las pacientes con alto riesgo de sufrir síndrome de cáncer hereditario de mama y ovario.
Transcript of Amanda Brandt, MS, CGC Oncología Ginecológica y … · representa a un hombre y un círculo que...

1
PowerPoint Slides English Spanish Translation
“Identification of High-risk Patients” Video Transcript
“Identificación de pacientes de alto riesgo” Transcripción del video
Professional Oncology Education Hereditary Breast and Ovarian Cancer Series Time: 25:25
Educación Oncológica Profesional Serie sobre cáncer hereditario de mama y ovario Duración: 25:25
Amanda Brandt, MS, CGC Certified Genetic Counselor Clinical Cancer Genetics Program Gynecologic Oncology and Reproductive Medicine The University of Texas MD Anderson Cancer Center
Amanda Brandt, MS, CGC Asesora Genética Certificada Programa de Genética Clínica del Cáncer Oncología Ginecológica y Medicina Reproductiva MD Anderson Cancer Center de la Universidad de Texas
Welcome. My name is Amanda Brandt. I am one of the Cancer Genetic Counselors at the University of Texas MD Anderson Cancer Center. Today, we are going to be discussing how to identify patients at high risk for hereditary breast and ovarian cancer syndrome.
Bienvenido. Mi nombre es Amanda Brandt y soy una de las asesoras genéticas de cáncer del MD Anderson Cancer Center de la Universidad de Texas. Hoy hablaremos de cómo identificar a las pacientes con alto riesgo de sufrir síndrome de cáncer hereditario de mama y ovario.

2
Up --- Upon completing this module, you’ll be able to understand the importance of family history; be able to differentiate between hereditary versus sporadic cancer; increase the knowledge of BRCA1 and BRCA2 genes and its associated cancer risks; and how to identify appropriate testing candidates for BRCA1 and BRCA2.
Al finalizar este módulo, usted podrá comprender la importancia de los antecedentes familiares, diferenciar entre el cáncer hereditario y el esporádico, conocer más sobre los genes BRCA1 y BRCA2, y los riesgos de cáncer asociados; e identificar a las candidatas apropiadas para las pruebas de BRCA1 y BRCA2.
First, I want to go over a little bit of a pedigree nomenclature. So a pedigree is what we draw when we meet with a family and it helps us to draw both a maternal and paternal sides of the family and easily identify who’s had cancer, who has not had cancer, and how old people are in their family, or how old they were when they are deceased. So to give you a little idea so you can follow through during this presentation, we wanted to give you a little bit of a key. So when you’re looking at the family histories, you will see a square will represent a male, a circle will represent a female. Anyone who is shaded in will show that they’ve been affected with cancer. Someone who has a line through them are a deceased individual. The person who has the arrow pointing to them is considered the proband: this is the person in the family who presented first for genetic counseling. Someone who’s connected to another individual shows that they are a mating. You can see siblings are attached at the very top of their symbol. Anyone who is adopted will have brackets
Quiero elaborar un poco sobre la nomenclatura genealógica. El árbol genealógico es lo que trazamos cuando conocemos a una familia. Nos ayuda a representar los lados materno y paterno, y a identificar quién ha tenido cáncer, quién no lo ha tenido, cuántos años tienen los familiares o cuántos años tenían cuando fallecieron. Para que pueda seguir esta presentación, le proporcionaremos una clave. Cuando observe los antecedentes familiares, verá un cuadrado que representa a un hombre y un círculo que representa a una mujer. Todo símbolo sombreado indica que esa persona ha sido afectada con cáncer. El símbolo con una línea cruzada indica una persona fallecida. El símbolo al cual apunta una flecha se considera el caso índice: es la persona de la familia que se presentó primero para recibir asesoría genética. Los símbolos conectados entre sí indican una pareja. Los hermanos se representan unidos en la parte superior del símbolo. Un familiar adoptado se representa por

3
around their symbol. If we don’t know the gender, we will just use a diamond, and the dx that we have in the --- in the pedigrees just let us know they’ve been diagnosed. And so that, in following the dx, you will indicate whether it was breast cancer or ovarian cancer so that you are able to follow through the pedigree.
un símbolo entre corchetes. Si no conocemos el sexo, usamos un diamante, y el “dx” en un árbol genealógico solo nos informa que esa persona recibió un diagnóstico. Al seguir el “dx” se indicará si fue cáncer de mama u ovario para que sea posible hacer un seguimiento del árbol genealógico.
We also want to go over a little bit about who is related to everybody. So a first degree relative includes your parents, your siblings, and your children. A second degree relative are your grandparents, your aunts and your uncles, and your nieces and your nephews. Your third degree relatives are your cousins, your great-aunts, your great-uncles, and your great-grandparents. And this will come into play when you’re considering what the risk is for your patient to have hereditary cancer syndrome, depending on what degree of relationship that person in that family might have had cancer.
También queremos referirnos a los parentescos. Los familiares de primer grado son padres, hermanos e hijos. Los familiares de segundo grado son abuelos, tíos y sobrinos. Los familiares de tercer grado son primos, tíos abuelos y bisabuelos. Esto será relevante cuando considere cuál es el riesgo de que su paciente tenga el síndrome de cáncer hereditario, según el grado de parentesco con la persona de esa familia que podría haber tenido cáncer.

4
When you’re recording the family history, what we do for each family member, we’re going to specify their gender, if they’re living, what year are --- were they born or old are they today. If they’re deceased, we will record how old they were when they passed away and what was their cause of death. We’ll ask about any medical problems that that individual might have, particularly pertaining to cancer, and we’ll ask about if there’s been any prophylactic surgery. So did someone undergo a total hysterectomy and bilateral salpingo-oophorectomy? And then, reducing their ovarian cancer risk would be important information to capture. And whenever it is possible, it is ideal to be able to ob --- obtain the medical documentation confirming the cancer diagnoses so that we’re really aware of the cancer that we’re diagnosing in that family and can confirm that with absolute.
Cuando registramos los antecedentes familiares, especificamos para cada miembro de la familia el sexo, si vive, el año en que nació y su edad actual. Si ha fallecido, registramos la edad que tenía cuando falleció y la causa de su muerte. Indagamos sobre cualquier problema médico que esa persona pueda tener, en particular con respecto al cáncer, y verificamos si hubo alguna cirugía profiláctica. ¿Se sometió a una histerectomía total y a una salpingo-ooforectomía bilateral? Reducir el riesgo de cáncer de ovario sería un dato importante. Si es posible, es ideal obtener la documentación médica que confirme el diagnóstico, así estaremos seguros del cáncer que estamos diagnosticando en esa familia y podemos confirmarlo con absoluta certeza.
For each family member with cancer, we are going to ask that you specify what type of cancer the patient was diagnosed with, how old were they when they were diagnosed, did they have more than one cancer? So did someone have breast and ovarian cancer? Or did someone have breast and brain cancer? And when you ask a little bit more questions, you’ll realize that the brain cancer is really a metastasis from the breast cancer, and we want to be able to differentiate that. We’ll also ask about any lifestyle factors. So smoking, obesity, occupational hazards which may be a risk factor for the cancer that that patient might have developed. For example, if someone had lung cancer, were they a smoker and which would have placed them at risk for that cancer?
Para cada familiar con cáncer, se debe especificar qué tipo de cáncer se diagnosticó al paciente, qué edad tenía al momento del diagnóstico y si tuvo más de un cáncer. ¿Tuvo alguien cáncer de mama y ovario? ¿O tuvo alguien cáncer de mama y cerebro? Si se hacen más preguntas, se podrá comprobar que el cáncer de cerebro es realmente una metástasis del cáncer de mama y es preciso diferenciar esa circunstancia. También haremos preguntas acerca de factores de estilo de vida: el tabaquismo, la obesidad, los riesgos laborales que pueden ser un factor de riesgo para el cáncer que el paciente podría haber desarrollado… Por ejemplo, si alguien tenía cáncer de pulmón, ¿era fumador? ¿Qué circunstancia podría haberlo puesto en riesgo de padecer ese cáncer?

5
It is really important to gather an accurate family history, and we really rely on this the most in cancer genetic counseling. It enables the health care provider to accurately perform a risk assessment regarding the likelihood of a hereditary cancer syndrome in the family. You might ident --- identify other cancer risks. So maybe they just have breast cancer in the family at this point but if you identify if they’re at high risk for breast and ovarian cancer. You are going to manage those people much differently. You’re going to recommend appropriate cancer risk management based on what that family history is telling and showing you, and it allows you to accurately interpret the genetic test results and make the best recommendations for the family. So making sure that the family history is accurate and has all the pertinent information in there is really going to help you in this risk assessment.
Es muy importante reunir los antecedentes familiares exactos. Ese es el factor en el cual más nos basamos en la asesoría genética sobre el cáncer. Ello permite al proveedor de cuidado de la salud efectuar con precisión una evaluación de riesgos sobre la probabilidad de un síndrome de cáncer hereditario en la familia. Se podrían identificar riesgos de otros tipos de cáncer. Tal vez en este momento lo único que tienen en la familia es cáncer de mama, pero, si se identifica que hay también un alto riesgo de cáncer de mama y ovario, esas personas serán controladas de manera muy diferente. Se recomendará un adecuado tratamiento del riesgo de cáncer según lo demuestren los antecedentes familiares, se podrán interpretar con precisión los resultados de las pruebas genéticas y se harán las mejores recomendaciones para la familia. Asegurar que los antecedentes familiares sean precisos y que se tenga toda la información pertinente sin duda ayudará a hacer la evaluación de riesgos.
So how much of breast and ovarian cancer is hereditary? A). 5 to 10 percent. B). 20 to 30 percent. C). 50 percent. Or D). 65 to 70 percent.
¿En qué grado el cáncer de mama y ovario es hereditario? A) Del 5% al 10%. B) Del 20% al 30%. C) 50%. O D) Del 65% al 70%.

6
So 5 to 10 percent of breast cancer is inherited. In those family histories we will tend to see particular patterns including early onset breast cancers, usually diagnosed premenopausally. You’ll see individuals diagnosed with more than one type of cancer, and you’ll see multiple generations affected. About 15 to 20 percent of breast cancer is considered familial. In those family histories, you’ll see more than two individuals diagnosed with breast cancer. But they’ll tend to be later ages of onset, more representative of the general population ages of onset. And there won’t be a clear pattern of inheritance. So you might see a great-aunt diagnosed with breast cancer in her seventies, and maybe your patient was diagnosed with breast cancer in her sixties, but there’s nobody else in the family diagnosed. It may just be a familial component leading to the breast cancers that we are seeing. Seventy to 80 percent of breast cancers are not inherited. They’re considered sporadic. Basically, they’re just happening by chance and chance alone. And it really composes the most of the breast cancer that we see diagnosed each year.
Del 5% al 10% del cáncer de mama es hereditario. En esos antecedentes familiares solemos ver patrones particulares, cánceres de mama de aparición temprana, por lo general diagnosticados antes de la menopausia. Habrá mujeres diagnosticadas con más de un tipo de cáncer, con varias generaciones afectadas. De un 15% a un 20% del cáncer de mama se considera familiar. En esos antecedentes familiares habrá más de dos mujeres diagnosticadas con cáncer de mama, pero la edad de aparición será más tardía, más representativa de las edades de la población general. No habrá un patrón hereditario claro. Podría haber una tía abuela diagnosticada con cáncer de mama a los 70 años y tal vez su paciente recibió ese diagnóstico a los 60, pero no hay otra mujer diagnosticada en la familia. Quizás solo se trate de un componente familiar que lleve al cáncer de mama. Del 70% al 80% de los cánceres de mama no son hereditarios; son considerados esporádicos. Básicamente, ocurren de manera exclusiva por casualidad y son la mayoría de los cánceres de mama que vemos diagnosticados cada año.

7
So ovarian cancer, about 10 to 15 percent of ovarian cancer is inherited, particularly if it’s a high-grade serous-type ovarian cancer. You’ll see those same similar patterns in the family history. Otherwise, about 85 to 90 percent of ovarian cancer is considered sporadic, hopening --- happening purely by chance, and happening at the general age of onset in the mid sixties.
En el caso del cáncer de ovario, de un 10% a un 15% es hereditario, sobre todo si se trata del tipo seroso de alto grado. Comprobará esos mismos patrones similares en los antecedentes familiares. Del 85% al 90% de los casos se consideran esporádicos, puramente casuales, y suelen aparecer alrededor de los 65 años.
So to quickly compare a family history that might have a sporadic cancer versus a hereditary cancer pattern, we’re going to talk about this here. So you can see in this sporadic family history, you have a patient who’s been diagnosed with breast cancer at the age of 60, but nobody else in her family, either on her maternal or paternal side of the family have a history of cancer. For this patient, we would tell them she has a sporadic cause to her breast cancer. And her family members would not be at a significantly increased risk to develop this cancer. If we compare that to the hereditary family history that we have, we see that a grandmother was diagnosed with breast cancer at the age of 42 and is now deceased. She had a daughter who was diagnosed with breast cancer at the age of 47. And this individual had a daughter who was diagnosed with ovarian cancer at 50 and a daughter with breast cancer at 45. What we’re tending to see in these families are multiple generations affected. We see the grandparents, parents, and the grandparents --- [speaker intended
Comparemos rápidamente los antecedentes familiares de una persona que podrían tener un patrón de cáncer esporádico con otra que tiene un patrón de cáncer hereditario. En el caso de la familia con cáncer esporádico, hay una paciente diagnosticada con cáncer de mama a los 60 años, pero nadie más en su familia, ya sea por el lado materno o paterno, tiene antecedentes de cáncer. A esta paciente le diríamos que la causa de su cáncer de mama es esporádica y sus familiares no tendrían un riesgo considerablemente mayor de desarrollar este cáncer. Si comparamos este caso con los antecedentes familiares de cáncer hereditario, vemos que a una abuela se le diagnosticó cáncer de mama a los 42 años y falleció. Su hija fue diagnosticada con cáncer de mama a los 47 años y esta mujer tuvo una hija que fue diagnosticada con cáncer de ovario a los 50 años, y otra hija con cáncer de mama a los 45 años. La tendencia verificada en estas familias es que hay múltiples generaciones afectadas. Vemos

8
to say grandchildren] affected. We see early ages of onset, so cancer diagnosed before the age of 50. And all of these patterns make us concerned about family history is due to something inherited from the maternal side of the family.
la enfermedad tanto en abuelas, como en sus hijas y nietas. La aparición es temprana y el cáncer se diagnostica antes de los 50 años. Todos estos patrones nos hacen pensar que los antecedentes familiares se deben a algo heredado del lado materno de la familia.
Some of the red flags for hereditary breast and ovarian cancer when you’re reviewing a patient’s medical and family history include premenopausal or early onset breast cancer, usually diagnosed under the age of 50. If you’re seeing many relatives with breast and/or ovarian cancer on the same side of the family; both breast and ovarian cancer diagnosed in the same person. A woman who has bilateral breast cancer; even men who can diagnose with breast cancer be concerning that it might be hereditary. Is there a known BRCA mutation identified in a family member or is anyone of Ashkenazi Jewish ancestry, particularly pertaining to the central or eastern Euro --- European geography?
Cuando se revisan la historia clínica y los antecedentes familiares de una paciente, la aparición temprana o en etapa premenopáusica del cáncer de mama, por lo general diagnosticado antes de los 50 años, es signo de advertencia. Si se observan muchos familiares con cáncer de mama u ovario en el mismo lado de la familia, ambos tipos de cáncer diagnosticados en la misma persona, una mujer con cáncer de mama bilateral, o incluso hombres diagnosticados con cáncer de mama, podría tratarse de cáncer hereditario. ¿Hay una mutación de BRCA conocida identificada en un familiar, o alguien de ascendencia judía asquenazí, sobre todo de Europa central u oriental?

9
So who are you going to refer and who are we testing? So, there are many professional guidelines out there that’ll help you identify who’s at risk and who’s really the appropriate person to test, given a person’s personal or family history of breast and ovarian cancer. These include, but are not limited to, the National Comprehensive Cancer Network, or the NCCN. We ’ve lis te d the we bs ite he re s o you ca n go and read a little bit more. It’ll also be included in the appendix which we will review at the very end. And these review who should be referred for genetic counseling and risk assessment and who should be tested for hereditary breast and ovarian cancer. You might also check out the American Society of Clinical Oncology, or ASCO, as well as the American Congress of Obstetricians and Gynecologists, or ACOG.
¿A quién se va a referir y a quién haremos pruebas? Muchas pautas profesionales ayudan a identificar quién está en riesgo y a quién corresponde hacer pruebas, dados los antecedentes personales o familiares de cáncer de mama y ovario de una persona, que incluyen, entre otras, las de la Red Nacional Integral del Cáncer, o NCCN. Hemos incluido el sitio web aquí para que pueda leer más. También se incluirá en el apéndice que revisaremos al final. Se analiza así quiénes deben ser referidas para asesoría genética y evaluación de riesgos, y en quién se deben hacer pruebas de cáncer hereditario de mama y ovario. También se puede recurrir a la Sociedad Americana de Oncología Clínica, o A-S-C-O, y al Colegio Americano de Obstetras y Ginecólogos, o ACOG.
So when we’re thinking about hereditary breast and ovarian cancer, the two genes that are most normally associated as a cause are BRCA1 and BRCA2. They really are responsible for the majority of hereditary breast and ovarian cancer that we will see. These are large tumor suppressor genes that are likely revolved --- involved in DNA repair. So we want these genes to be working properly so that the repair of the DNA can be performed. But, if there is a problem or a mutation in either of these genes, they no longer can suppress cancer, which is why we see very high risk of cancers in these families when these mutations are inherited. About one in 500 to one in 800 individuals in the general population are estimated to have a BRCA1 or BRCA2 mutation. Individuals who are Ashkenazi Jewish actually have a higher chance of having a mutation, with that being one in 40 individuals. And they actually have one of three common Jewish mutations that are listed here,
Cuando consideramos el cáncer hereditario de mama y ovario, los dos genes que más normalmente se asocian como causa son los BRCA1 y BRCA2, los responsables de la mayoría de los cánceres hereditarios de mama y ovario que veremos. Son grandes genes supresores de tumores que probablemente participan en la reparación del ADN. Estos genes deben funcionar bien para que se pueda reparar el ADN. Si hay un problema o una mutación en estos genes, no pueden suprimir el cáncer y por eso vemos un riesgo muy alto de cáncer en estas familias si se heredan esas mutaciones. La mutación BRCA1 o BRCA2 en la población general se estima entre 1 de cada 500 y 1 de cada 800 personas. Las personas de origen judío asquenazí tienen una mayor probabilidad de tener una mutación, que es de 1 en 40 personas. Tienen una de tres mutaciones comunes en la población judía listadas aquí, 185delAG, 5382insC y 6174delT. Estas son

10
185delAG, 5382 insertion C, and 6174 deletion T. These are the three common mutations that you will test a Jewish person for, if they have hereditary breast and ovarian cancer.
las tres mutaciones comunes que hay que descartar en una mujer judía, si tiene cáncer hereditario de mama y ovario.
So how are these mutations inherited? So if a parent has a mutation, and this is highlighted here in the small “m” that’s the color red, they have a 50% chance to pass that mutation onto a child and an equal 50 percent chance to pass on the normal copy of the gene, and this one is designated with the capital “M” in black. And it --- it can equally be inherited from either a mother or a father and passed onto a son or to a daughter. So once again, it’s a 50 percent chance that if a parent has the mutation that they have a chance of passing that on to a child.
¿Cómo se heredan estas mutaciones? Si un progenitor tiene una mutación, lo que aquí se indica con la “m” minúscula roja, tiene una probabilidad del 50% de transmitir esa mutación a un hijo y otro 50% de transmitir la copia normal del gen, lo cual se designa con la “M” negra. Es posible heredarla de la madre o el padre y transmitirla a un hijo o una hija. Entonces, si un progenitor tiene la mutación, la probabilidad de transmitirla a un hijo es del 50%.
What is the breast cancer risk associated with a BRCA mutation? A). Up to 25 percent. B). Up to 55 percent. C). Up to 85 percent. Or D). Up to 100 percent. The answer is C) – Up to 85 percent.
¿Cuál es el riesgo de cáncer de mama asociado con la mutación BRCA? A) Hasta del 25%. B) Hasta del 55%. C) Hasta del 85%. O D) Hasta del 100%. La respuesta es: C) Hasta del 85%.

11
Here, I’m going to review the cancer risk and BRCA1 mutation carriers. In the green, we’ll show you the individuals who have a mutation, the risk for primary breast cancer is between 60 and 85 percent chance over that woman’s lifetime, and that’s compared to about a 12 percent risk in the general population. Below that you’ll see that there’s a secondary primary breast cancer risk that a woman might have, and that is up to a 40 to 60 percent chance to develop breast cancer, and that’s compared to about a 5 percent chance in the general population. A woman also has an increased chance to develop ovarian cancer up to 45 percent chance over her lifetime, compared to about a one and a half percent chance in the general population.
Ahora voy a referirme al riesgo de cáncer y a los portadores de la mutación BRCA1. Se indican con verde las personas con una mutación. El riesgo de cáncer de mama primario es de entre 60% y 85% durante toda la vida de esa mujer, lo cual se compara con un riesgo de 12% en la población general. Debajo se indica el riesgo de cáncer de mama primario secundario que una mujer podría tener, una probabilidad del 40% al 60% de desarrollar cáncer de mama, que en la población general es de un 5%. La mujer también tiene una mayor probabilidad de desarrollar cáncer de ovario, de hasta el 45% durante su vida, en comparación con un 1.5% en la población general.
There are some other cancer risks associated with a BRCA mutation. For men, they would have an increased chance for male breast cancer. There’s a slightly increased risk for prostate cancer. And we can see and reported in the literature, a slightly increased risk of pancreatic cancer above that of the general population. But, the associations with BRCA1 are a little bit less clear.
Existen otros riesgos de cáncer de mama asociados con la mutación BRCA. Los hombres tendrían una mayor probabilidad de sufrir cáncer de mama masculino. Hay un ligero aumento del riesgo de cáncer de próstata y, según la literatura, un riesgo de cáncer de páncreas ligeramente mayor que el de la población general. Las asociaciones con el BRCA1 son menos claras.

12
In individuals who carry a BRCA2 mutation, the risk for a primary breast cancer would be similar, about a 60 to 85 percent chance to develop breast cancer, compared to about a 12 percent risk in the general population. They would have between a 40 and 60 percent chance to develop a secondary breast cancer, compared to about a 5 percent risk in the general population. Women who have a BRCA2 mutation actually have a little bit lower risk of ovarian cancer compared to BRCA1, with that risk being up to 27 percent chance in their lifetime, compared to about a one and a half percent chance in the general population. Male breast cancer risk is a little bit more clear here. It’s up to a 6 percent chance. The prostate cancer risk for men would be up to 20 percent, compared to a 16 percent chance in the general population. And we know the pancreas cancer risk is elevated above that of the general population with a little bit more certainty than we knew for BRCA1, and that’s up to about a 7 to 8 percent risk.
En los portadores de una mutación BRCA2, el riesgo de cáncer de mama primario sería similar, de un 60% a un 85%, en comparación con un riesgo del 12% en la población general. Tendrían una probabilidad de entre el 40% y el 60% de desarrollar un cáncer de mama secundario, en comparación con un riesgo del 5% en la población general. Las mujeres que tienen una mutación BRCA2 tienen un riesgo algo más bajo de cáncer de ovario respecto de la BRCA1, con una probabilidad de hasta el 27% en su vida, en comparación con un 1.5% en la población general. El riesgo de cáncer de mama masculino es más claro: la probabilidad es de hasta un 6%. El riesgo de cáncer de próstata sería de hasta un 20%, en comparación con el 16% en la población general. Sabemos que el riesgo de cáncer de páncreas es mayor que el de la población general, con más certeza que para el BRCA1, y es de hasta un 7% a un 8%.
In the literature there have been various other cancers that have been reportedly associated with BRCA1 and BRCA2. These include melanoma, colon cancer, larynx cancer, esophageal cancer, and gastric cancer. However, the clear associations and the accurate risk assessment and the risk number is not very clearly associated with either of these mutations. So we do not screen closely for individuals who have BRCA1 or BRCA2 mutations for these cancers. If there’s a family history, we might recommend different screening based on that alone.
En la literatura se han informado otros tipos de cáncer asociados con los genes BRCA1 y BRCA2 que incluyen melanoma y cáncer de colon, laringe, esofágico y gástrico. Sin embargo, no hay asociaciones claras ni una evaluación precisa del riesgo y su probabilidad en relación con estas mutaciones, por lo cual no hacemos pruebas de diagnóstico de estos tipos de cáncer en las personas con mutaciones BRCA1 o BRCA2. Si hay antecedentes familiares, podríamos recomendar diferentes pruebas en función de esa única circunstancia.

13
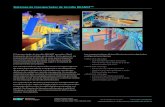
So over time, these risks will gradually increase, and that’s what we show here comparing BRCA1 and BRCA2 mutation carriers. This is a cumulative risk for them to develop breast cancer, which will be the green line, and ovarian cancer, which will be the blue line. So if you can kind of look, in a woman who’s 30 years old, her risk to develop either breast or ovarian cancer is close to about 0 percent. But, you can see over her lifetime that number dramatically increases over her lifetime. And that’s why we start screening at much younger ages so that we’re capturing these cancers at their earliest ages of onset, because we tend to see that they’re diagnosed at young ages.
Con el tiempo, estos riesgos aumentarán gradualmente y lo mostramos al comparar aquí los portadores de mutaciones BRCA1 y BRCA2. Este es un riesgo acumulativo de desarrollar cáncer de mama (la línea verde) y ovario (la línea azul). Observemos que en una mujer de 30 años, el riesgo de desarrollar cáncer de mama u ovario es cercano al 0%; sin embargo, durante su vida ese número aumenta drásticamente. Por eso empezamos las pruebas a menor edad, para detectar estos cánceres en sus etapas más tempranas, pues tendemos a ver que se diagnostican en las personas jóvenes.
So there’re some various discrepancies in terms of the actual risk associated with a BRCA1 and BRCA2 mutation in the literature. And this may be attributed to the ascertainment of the study population. In the initial study, some of these families were picked up based on their very strong family histories of cancers. You know, they might’ve had multiple women in the family with very young breast cancer that it’s hard to ignore there was something hereditary there. So the risks in those studies are probably higher because you are ascertaining families that have a higher chance to develop those cancers with as many people as you’re seeing in those families. Compared to a population-based study where we’re testing all comers who present to the study with breast cancer or ovarian cancer, and testing everybody. That’s going to give you a little bit better and accurate number in terms of the risk. Because you’re testing everyone, whether it’s a more lower penetrant type of mutation and --- in the families where they have a little bit lesser cancer risk potentially, and so, that’s
En la literatura hay varias discrepancias en cuanto al riesgo real asociado con una mutación BRCA1 y BRCA2. Esto puede atribuirse a la comprobación de la población de estudio. En el estudio inicial, ciertas familias se seleccionaron en función de antecedentes familiares de cáncer contundentes. Podrían haber tenido varias mujeres en la familia con cáncer de mama a corta edad, por lo cual es difícil omitir que se trataba de algo hereditario. Los riesgos de esos estudios son tal vez más altos, ya que se están comprobando familias con mayor probabilidad de desarrollar esos tipos de cáncer con todos sus miembros. Comparativamente, en un estudio de base poblacional, hacemos pruebas a toda persona que se presenta en el estudio con cáncer de mama u ovario. Eso arrojará una cifra algo más precisa en términos de riesgo porque se están haciendo pruebas en todos, lo que incluye mutaciones de menor penetración en las familias con menos riesgo de cáncer. Proporcionamos, entonces, un rango del riesgo de cáncer de mama,

14
why we give you a range of breast cancer risk, anywhere from 45 to 85 percent, because it’s depending on which study you’re looking at and what population they were testing. The ovarian cancer risk might range from 30 to 45 percent for a BRCA1 carrier and 10 to 27 percent for BRCA2, depending on which study you’re looking at.
del 45% al 85%, porque depende del estudio que veamos y de qué población se haya sometido a pruebas. El riesgo de cáncer de ovario podría variar del 30% al 45% para un portador de BRCA1 y del 10% al 27% para el de BRCA2, según el estudio observado.
Over time, we’ve really noticed that there’re particular pathology and histology trends of hereditary breast cancer and first, we’ll discuss BRCA1. So these breast cancers tend to be hormone receptor negative. So ER/PR will be negative, and they will also be HER2 negative. So it’s something that we look and evaluate for in the pathology when we’re assessing a family history for hereditary breast and ovarian cancer. And we look closely at the pathology to give us a little bit more information. We tend to see increased frequency of medullary breast carcinomas. These cancers tend to be high grade. And you can also observe ductal carcinoma in situ, or DCIS, as well as ductal and lobular carcinomas that are invasive. And so, making sure that you’re testing the patients even though they have DCIS, is something to be aware of. In BRCA2 carriers, their breast cancers tend to be hormone receptor positive, so ER and PR positive. They are still going to be high grade. And you will also observe ductal carcinoma in situ as well as ductal and lobular invasive carcinomas.
Hemos comprobado que, con el tiempo, hay tendencias particulares de patología e histología del cáncer de mama hereditario. Primero, hablaremos del BRCA1. Estos cánceres de mama tienden a no tener receptores hormonales. No tendrán receptores ER/PR ni HER2. Es algo que buscamos en la patología al evaluar antecedentes familiares de cáncer hereditario de mama y ovario. Observar la patología nos brinda más información. Vemos una mayor frecuencia de carcinoma de mama medular, un tipo de cáncer que suele ser de alto grado. También se puede observar carcinoma ductal in situ, o DCIS, y carcinomas ductales y lobulares invasivos. Entonces, es preciso hacer pruebas incluso en las pacientes que tengan DCIS. En las portadoras de BRCA2, el cáncer de mama tiende a tener los receptores hormonales ER y PR, y también serán de alto grado. Se observarán carcinoma ductal in situ, así como carcinomas ductales y lobulares invasivos.

15
For ovarian cancers that are hereditary associated with BRCA1 and BRCA2, you will most frequently see serous type carcinoma, composing about 63 to 93 percent of patients, followed by endometrioid type ovarian cancer. It’s associated with a high grade and stage. Oftentimes, patients are diagnosed at Stage III or Stage IV of their disease. And overall prognosis may be better for women who have BRCA mutation and ovarian cancer compared to sporadic ovarian cancers. They tend to have longer survival and longer times between recurrences, compared to sporadic carriers with ovarian cancer. Non-epithelial ovarian cancers have no known association with BRCA1 or BRCA2 mutations and should be considered when you’re performing the risk assessment when you have the patient in front of you. If she has a non-epithelial cancer, you can reassure her that she is not at risk for a BRCA mutation. And BRCA1 and BRCA2 mutations are quite rare in borderline or low malignant potential, otherwise called LMP ovarian tumors and mucinous type ovarian cancers, which should also be, you know, considered when you’re reviewing the pathology of your patient with ovarian cancer and considering whether or not to do genetic testing.
En el caso de los cánceres de ovario hereditarios asociados con los genes BRCA1 y BRCA2, a menudo se verá el carcinoma de tipo seroso en cerca del 63% al 93% de las pacientes, seguido del cáncer de ovario de tipo endometrioide, este último asociado con grado y estadio altos. Las pacientes suelen ser diagnosticadas en los estadios III o IV de su enfermedad. El pronóstico general puede ser mejor para las mujeres con mutación BRCA y cáncer de ovario en comparación con los casos de cáncer de ovario esporádico. También tienden a tener una mayor supervivencia y períodos más largos entre recurrencias, en comparación con las portadoras de cáncer de ovario esporádico. Los cánceres de ovario no epiteliales no tienen ninguna asociación conocida con las mutaciones BRCA1 o BRCA2 y esto debe remarcarse al realizar la evaluación de riesgo en presencia de la paciente. Si ella tiene un cáncer no epitelial, es posible asegurarle que no tiene el riesgo de una mutación BRCA. Las mutaciones BRCA1 y BRCA2 son muy raras en los tumores de ovario de bajo potencial maligno (LMP) y de tipo mucinoso, para los cuales también hay que analizar la patología de la paciente con cáncer de ovario y considerar si se deben hacer o no pruebas genéticas.

16
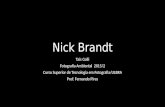
So here we have a pedigree for you. So “who in this family should be tested first?” Your patient with the arrow is 24 years old with no history of cancer. But, she reports that her mother was diagnosed with ovarian cancer at the age of 48. Her grandmother was diagnosed with breast cancer at the age of 49 and is now deceased. Her aunt was diagnosed with breast cancer at the age of 37 and is now deceased. And her cousin was diagnosed with breast cancer at the age of 33. So clearly, this is a family that would be highly concerning for hereditary breast and ovarian cancer. But let’s decide who should we test?
Aquí tenemos un árbol genealógico. ¿Quién de esta familia debe someterse a una prueba primero? La paciente con la flecha tiene 24 años y carece de antecedentes de cáncer. Ella informa que su madre fue diagnosticada con cáncer de ovario a la edad de 48 años. Su abuela fue diagnosticada con cáncer de mama a los 49 años y ya falleció. Su tía fue diagnosticada con cáncer de mama a los 37 años y también falleció ya. Por último, su prima fue diagnosticada con cáncer de mama a los 33 años. Claramente, esta familia plantearía mucha inquietud sobre el cáncer hereditario de mama y ovario. Decidamos a quién practicar pruebas.
Should it be A – your proband, your patient who is 24 years old with no cancer history? Is it B – the mother, 49 years old, diagnosed with ovarian cancer at age 48? Or C – the maternal cousin who is 33 years old, diagnosed with breast cancer age 33?
¿Al caso índice A, la paciente de 24 años, que no tiene antecedentes de cáncer? ¿A la paciente B, la madre de 49 años, diagnosticada con cáncer de ovario a los 48? ¿O a la paciente C, la prima materna de 33 años, diagnosticada con cáncer de mama a esa edad?

17
In this family, the ideal testing candidate would be the mother of your patient diagnosed with ovarian cancer at 48.
En esta familia, la candidata ideal sería la madre de la paciente, diagnosticada con cáncer de ovario a los 48 años.
This is because the most informative person to do genetic testing on is someone who has been diagnosed with cancer themselves, so, either breast or ovarian cancer. In that pedigree the mother is the ideal testing candidate because she’s the most closely related to your patient, the 24-year-old unaffected woman. But, she’s also been diagnosed with ovarian cancer and --- and really particularly at a younger age than we tend to see in the general population. If we test that mother and we find that she has a mutation in BRCA1 and BRCA2, we can clearly see that there is hereditary cancer in the family and it better allows us to test other at-risk family members. If, let’s say, we test the person who has cancer and she is negative, we really are not going to know what to do very much in that family because we’ve tested the ideal --- ideal testing candidate and she does not have a hereditary form of breast and ovarian cancer due to the BRCA1 or BRCA2 genes. And in that scenario, we would not test the unaffected woman because we would
Esto se debe a que la persona más informativa para hacer pruebas genéticas en alguien que haya recibido un diagnóstico de cáncer propio, ya sea de mama u ovario. En este árbol genealógico, la madre es la candidata ideal porque es quien está más íntimamente relacionada con la paciente de 24 años no afectada. También fue diagnosticada con cáncer de ovario y a una edad más joven que la que solemos ver en la población general. Si se comprueba que la madre tiene una mutación en BRCA1 y BRCA2, es claro que hay cáncer hereditario en la familia y podemos hacer pruebas en otros familiares en situación de riesgo. Si hacemos la prueba a la mujer con cáncer y el resultado es negativo, no sabremos muy bien qué hacer en esa familia, ya que hemos seleccionado a la candidata ideal y ella no tiene un cáncer de mama y ovario de tipo hereditario debido a los genes BRCA1 o BRCA2. En ese contexto, no haríamos la prueba en la mujer no afectada, ya que podríamos prever que también será negativa

18
anticipate that her testing would also be negative if her mother’s was negative. So a negative test result in someone without cancer. So if we had tested the 24-year-old woman before testing anybody else, maybe it can offer a false reassurance, and it does not entirely rule out hereditary cancer in the family. You might have just tested the wrong person and so, this is really why it’s key when you’re meeting with families and meeting with patients that you’re testing the most appropriate candidate in the family, and those are going to be the individuals who have cancer themselves.
si ese resultado se comprobó en su madre. Un resultado negativo implica una persona sin cáncer. Si hubiéramos seleccionado a la mujer de 24 años antes que a otra persona, podría haber generado una falsa confianza y no se hubiera descartado por completo el cáncer hereditario en la familia. Tal vez se hubiera analizado a la persona equivocada y por eso es esencial hacer la prueba al candidato más apropiado de la familia, el que tiene cáncer.
So, in summary, the majority of cancer is not inherited. Approximately 10% of breast and ovarian cancers are the result of mutations in BRCA1 and BRCA2. There are various red flags that you can use to help identify individuals and families at risk for hereditary breast and ovarian cancer, and there’re multiple guidelines and recommendations regarding who is appropriate to perform genetic testing.
En resumen, la mayoría de los cánceres no se hereda. Cerca del 10% de los cánceres de mama y ovario son el resultado de mutaciones BRCA1 y BRCA2. Hay varios signos de advertencia que se pueden utilizar para identificar a las personas y familias en situación de riesgo de cáncer hereditario de mama y ovario, y múltiples pautas y recomendaciones sobre quién es adecuado para las pruebas genéticas.

19
The family history is an important tool in the genetic risk assessment and providing accurate risk assessment, risk management strategies, and interpring --- interpreting the genetic test results. Making sure that you’re gathering a family history and always updating it on an annual basis is probably the best strategy because we know that these family histories change over time and you want to make sure that your risk assessment and how you’re screening these family members isn’t going to change over time. You want to make sure you’re appropriately identifying the ideal testing candidate in the family, and it enables you to have a more accurate interpretation of a genetic test result and --- and be able to identify who else in the family might also be at risk for hereditary breast and ovarian cancer.
Los antecedentes familiares son una herramienta importante para evaluar el riesgo genético, aplicar estrategias de administración del riesgo e interpretar los resultados de las pruebas genéticas. Asegurarse de estar recopilando los antecedentes familiares y actualizarlos siempre una vez al año es tal vez la mejor estrategia, porque sabemos que estos antecedentes cambian con el tiempo y es necesario que nuestra evaluación del riesgo y la forma de analizar a estos familiares no se modifiquen. También es importante identificar al candidato ideal para las pruebas, ya que esto nos permitirá interpretar con más precisión el resultado de una prueba genética y verificar quién más en la familia podría estar en riesgo de sufrir cáncer hereditario de mama y ovario.
Here, in the Appendix,… Aquí, en el apéndice…

20
…is the National Comprehensive Cancer Network Referral Guidelines for who s hould be cons ide re d for hereditary breast and ovarian cancer syndrome testing. And I have them here for your reference. So you can take some time now and review those particular individuals who we would at --- identify as someone who might be high risk and should consider genetic counseling and testing.
... están las pautas de referidos de la Red Nacional Integral del Cáncer sobre quién debe considerarse para las pruebas del síndrome de cáncer hereditario de mama y ovario. Las tengo aquí para su referencia. Pueden revisar esos casos particulares que identificaríamos como una persona en alto riesgo, para quién consideraríamos la asesoría y las pruebas genéticas.
And they’re going to continue here on the second page. And so, if any of your patients or your family members of patients fall into any or meet any of these criteria, it might be something that would be appropriate for them to be counseled, perform a risk assessment, and possible genetic testing. So I thank you for listening today to our talk about hereditary breast and ovarian cancer and identifying individuals who are at high risk, and I welcome any of your feedback.
Continúan aquí, en la segunda página. Si alguno de los pacientes o familiares de estos se encuadran en alguno de estos criterios, correspondería asesorarlos, realizar una evaluación de riesgos y, tal vez, hacer pruebas genéticas. Gracias por escuchar hoy nuestra disertación sobre el cáncer hereditario de mama y ovario, y cómo identificar a las personas que están en alto riesgo. Apreciaré sus comentarios.