
Adjuvância para o Câncer de Mama HER-2 Positivo de Acordo ...
40
Adjuvância para o Câncer de Mama HER-2 Positivo de Acordo com Risco Dr Antonio C Buzaid Diretor, Centro Oncológico Antonio Ermírio de Moraes, Beneficência Portuguesa de São Paulo Membro do Comitê Gestor, Centro de Oncologia Dayan-Daycoval, Hospital Israelita Albert Einstein
Transcript of Adjuvância para o Câncer de Mama HER-2 Positivo de Acordo ...

Adjuvância para o Câncer de Mama
HER-2 Positivo de Acordo com Risco
Dr Antonio C Buzaid
Diretor, Centro Oncológico Antonio Ermírio de Moraes, Beneficência Portuguesa de São Paulo
Membro do Comitê Gestor, Centro de Oncologia Dayan-Daycoval, Hospital Israelita Albert Einstein

De acordo com a resolução do Conselho Federal de Medicina nº 1595/2000 e Resolução da
Diretoria Colegiada da ANVISA nº 96/2008, eu declaro os seguintes potenciais conflitos de
interesse:
Pesquisa Clínica – Como investigador: Roche, MSD, BMS, Novartis, Pfizer
Apresentações científicas – Como palestrante: Roche, MSD, BMS, Novartis, Pfizer, United
Medical, AstraZeneca, Sanofi
Atividades de Consultoria – Como membro de Advisory Boards: Roche, MSD, BMS, Novartis,
Pfizer, United Medica, AstraZeneca, Sanofi, Blau
Declaro não ter ações em bolsa de valores das empresas supracitadas.
Meus pré-requisitos para participar destas atividades são o intercâmbio científico, a
autonomia do pensamento científico, independência de opinião e liberdade de expressão,
aspectos estes respeitados pela Novartis.
Esta apresentação pode conter informações que não constam nas bulas aprovadas dos
produtos Novartis . Estas informações têm o intuito de fornecer a você os dados científicos
pertinentes para tirar suas próprias conclusões e para tomar suas próprias decisões. A
Novartis não corrobora a promoção de seus produtos de uma forma que não esteja de
acordo com suas bulas aprovadas.
Disclaimer

Estudos de Adjuvância com Trastuzumabe
1. Gianni L, et al. Lancet Oncol 2011; 12:236244;
2. Slamon D, et al. N Engl J Med 2011; 365:12731283;
3. Perez EA, et al. J Clin Oncol 2011; 29:33663373.

DFS and OS Benefits Demonstrated with Addition of Trastuzumab
Study Follow-up (years)
DFS OS
N HR p value HR p value
HERA1–4
CT+/–RTH vs. CT+/–RT
1 3387 0.54 < 0.0001 0.76 0.26
2 3401 0.64 < 0.0001 0.66 0.0115
4 3401 0.76 < 0.0001 0.85 0.1087
8 3401 0.76 < 0.0001 0.76 0.0005
NCCTG N9831/
NSABP B-315–7
ACTHH vs. ACT
2 3351 0.48 < 0.0001 – –
4 4045 0.52 < 0.001 0.61 < 0.001
8.4 4046 0.60 < 0.0001 0.63 < 0.0001
BCIRG 0068
ACTHH vs. ACT5.5 3222
0.64 < 0.001 0.63 < 0.001
TCH vs. ACT 0.75 0.04 0.77 0.04
CT, chemotherapy; DFS, disease-free survival; H, trastuzumab;
HR, hazard ratio; OS, overall survival; RT, radiotherapy; T, taxane.
1. Piccart-Gebhart MJ, et al. N Engl J Med. 2005;353:1659-1672; 2. Smith I, et al. Lancet. 2007;369:29-36;
3. Gianni L, et al. Lancet Oncol. 2011;12:236-244; 4. Goldhirsch A, et al. Lancet. 2013 [Epub ahead of print];
5. Romond EH, et al. N Engl J Med. 2005;353:1673-1684; 6. Perez EA, et al. J Clin Oncol. 2011;29:3366-3373;
7. Romond EH, et al. SABCS 2012 (abstract S5-5; oral presentation); 8. Slamon D, et al. N Engl J Med. 2011;365:1273-1283.

BCIRG 006
Phase III Trial Comparing
AC→T with AC→TH and with TCH
in the Adjuvant Treatment of
HER2-Amplified Early Breast Cancer Patients:
ACT-TH vs TCH
Third Planned Efficacy Analysis
Slamon D, Eiermann W, Robert N, Pienkowski T, Martin M, Rolski J, Chan A, Mackey J, Liu M, , Pinter T, Valero V,
Falkson C, Fornander T, Shiftan T, Olsen S, Buyse V, Falkson C, Fornander T, Shiftan T, Olsen S, Buyse M, Kiskartalyi T,
Landreau V, Wilson V, Press M, Crown J, on behalf of the BCIRG 006 Investigators.
Study sponsored by Sanofi
Support from Genentech
Slamon et al. SABCS abstr S5-04, 2015

BCIRG006: Braço sem antraciclina
Slamon et al. SABCS abstr S5-04, 2015

BCIRG-006 Disease Free Survival Final Analysis (10.3yrs)
1
0.9
0.8
0.7
0.6
0.5
0.40 12 24 36 48 60 72 84 96 108 120 132
Time (months)
% a
live
and
dis
ease
-fre
e
AC-TAC-THTCH
Patients107310741075
Events328269279
HR (95% C.I.)1 (reference)
0.72 (0.61 – 0.85)0.77 (0.65 – 0.90)
P
< 0.00010.0011
67.9%
74.6%
73.0%
Slamon et al. SABCS abstr S5-04, 2015

Diferença em toxicidade
Therapeutic Index – Most Recent 006 Data
AC → TH TCH
DFS Events 269 279
Grade 3 / 4 CHF 21 4
Totals 290 283
RX-Related
Leukemias
7 (8)*
*Only in AC-Rx
patients
0(1)**
**Leukemia developed after
CHOP Rx
Sustained LVEF
Loss > 10%200 97
Slamon et al. SABCS abstr S5-04, 2015

Descalonamento da Adjvância


Paclitaxel semanal e Trastuzumabe (de-escalonando)
Primary tumor
Size
T1mic: ≤ 0.1 cm 9 (2.2)
T1a: > 0.1 to ≤ 0.5 cm 68 (16.7)
T1b: > 0.5 to ≤ 1.0 cm 124 (30.5)
T1c: > 1.0 to ≤ 2.0 cm 169 (41.6)
T2: > 2.0 to ≤ 3.0 cm 36 (8.9)
Nodal status
N0 400 (98.5)
N1mic 6 (1.5)
Tolaney S, N Eng J Med 2015;372:134
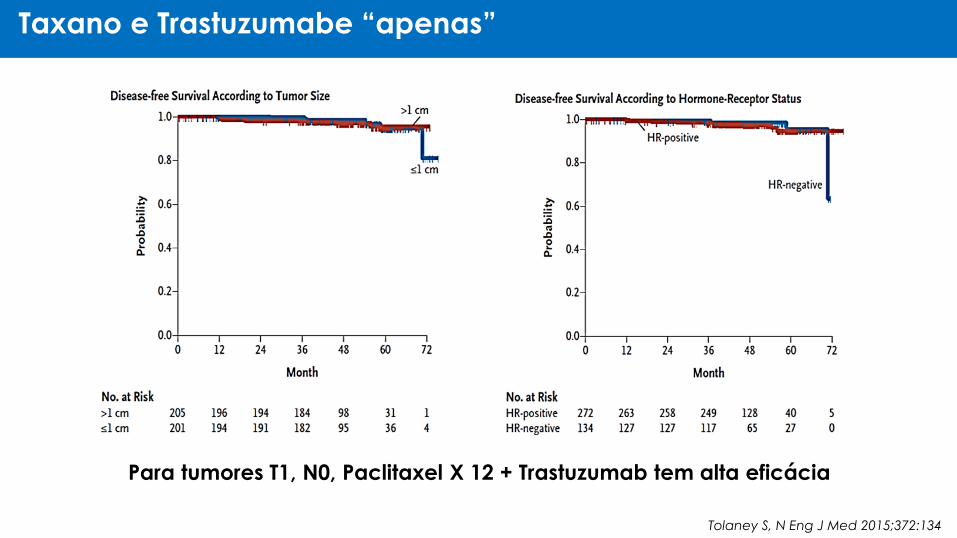
Taxano e Trastuzumabe “apenas”
Tolaney S, N Eng J Med 2015;372:134
Para tumores T1, N0, Paclitaxel X 12 + Trastuzumab tem alta eficácia

Paclitaxel semanal e Trastuzumabe
Ano Estimativa
3 anos 99,2%
5 anos 98,1%
7 anos 97,5%*
ASCO 2017, abstr #511
*1% de recorrência à distância
Intervalo Livre de Recorrência

6 vs 12 meses
(PHARE vs PERSEPHONE)



6 meses foi não inferior a 12 meses




PHARE DFS e OS

Sequential vs Concomitant

Comparison PHARE vs PERSEPHONE
Parameter PHARE PERSEPHONE
4-DFS in control Around 89% 89.8%
DFS HR 1.08 1.07
Margin required to declare NI 1.15 1.32*
Upper limit of 95% CI for DFS HR 1.25 1.24
Authors’ conclusion of NI Negative Positive
*Not prespecified, but computed on the basis of observed 4-year difference in DFSAnalyses performed by Dr Everardo Saad

Comparison of Buzaid vs Pitt

Adição de Pertuzumabe ao Trastuzumabe

The APHINITY Study Adjuvant Pertuzumab and Herceptin in Initial Therapy
BIG 4-11 / BO25126 / TOC4939g
A randomized comparison of chemotherapy plus trastuzumab
plus placebo versus chemotherapy plus trastuzumab plus
pertuzumab as adjuvant therapy in patients with HER2-positive
early breast cancer
G. von Minckwitz, M. procter, E. de Azambuja, D. Zardavas, M. Benyunes, G.
Viale, T. Suter, A. Arahmani, N. Rouchet, E. Clark, A. Knott, I. Lang, C. levy, D.
Yardley, J. Bines, R. Gelber, M. Piccart, J. Baselga
for the APHINITY Steering Committee and Investigators

APHINITY: Trial Design
APHINITY: Trial Design
Chemotherapy* + trastuzumab
+ pertuzumab
Chemotherapy* + trastuzumab
+ placebo
F
O
L
L
O
W
-
UP
10
Y
E
A
R
SRandomisation and treatment
within 8 weeks of surgery
Anti-HER2 therapy for a total of 1 year (52 weeks)
(concurrent with start of taxane)
Radiotherapy and/or endocrine therapy may be
started at the end of adjuvante chemotherapy
*A number of standard anthracycline-taxane-sequences or a non-anthracycline (TCH) regimen were allowed
S
U
R
G
E
R
Y
Central
confirmation
of HER2 status
(n = 4805)
R

APHINITY: Key Eligibility CriteriaAPHINITY: Key Eligibility Criteria
Inclusion criteria
• HER2-positive status confirmed by a central review (IHC 3+ or FISH-/CISH-positive)*
• Node-positive, any tumour size except T0
• Node-negative
• Tumour size > 1 cm
OR
• For tumours > 0.5 and ≤ 1cm, at least 1 of:
• Histological/nuclear grade 3
OR
• ER- and PR-egative
OR
• Age < 35
• Baseline LVEF ≥ 55%
Exclusion criteria
• Prior invasive breast câncer
• Non-operable breast câncer
• Metastatic disease (stage IV)
• Previoues non-reast malignances (except for the following: carcinomain situ of the cervix, carcinomain situ of the colon, melanoma in situ, and basal cell and squamous cell carcinomas of the skin)
• Previous or current anti-cancertherapy or previous radiotherapy for any malignancy
• Cardiac dysfunction or serious medical conditions
*Wolff A et al, J Clin Oncol 2013

APHINITY: Key Eligibility CriteriaAPHINITY: Primary Endpoint: Invasive Disease-Free Survival (IDFS)
Time from randomisation until the date of the first occurrence of one of the following events:
• Ipsilateral invasive breast tumour recurrence
• Ipsilateral local-regional invasive breast câncer recurrence
• Distant recurrence
• Contralateral invasive breast câncer
• Death attributable to any cause including breast câncer, non-breast cancer, or unknown cause
This IDFS definition• Was the FDA’s recommended definition for a trial intended to support a regulatory filing
• Differs from the STEEP definition1 of IDFS since it exclides second primary non-breast
cancers as event
1Hudis CA, J Clin Oncol 2007

APHINITY: Intent-to-Treat Primary Endpoint Analysis Invasive Disease-free Survival
Inv
asi
ve
dis
ea
se-f
ree
su
rviv
al (
%)
100
80
60
40
20
00 6 12 18 24 30 36 42 48
MonthsNo at Risk
Pertuzumab
Placebo2400
2404
2309
2335
2275
2312
2236
2274
2199
2215
2153
2168
2101
2108
1687
1674
879
866
Pertuzumab, 171 events
Placebo, 210 events
Stratified hazard ratio, 0.81 (95% CI, 0.66-1.00)
p = 0.045
Number needed to treat: 112
Expected: 89.2%
98.6% 96.4% 94.1% 92.3%
98.8%95.7%
93.2% 90.6%

Inv
asi
ve
dis
ea
se-f
ree
su
rviv
al (
%)
100
80
60
40
20
00 6 12 18 24 30 36 42 48
MonthsNo at Risk
Pertuzumab
Placebo1503
1502
1444
1453
1419
1439
1387
1408
1358
1359
1327
1319
1283
1264
912
882
423
405
Pertuzumab, 139 events
Placebo, 181 events
Unstratified hazard ratio, 0.77 (95% CI, 0.62-0.96)
p = 0.019
Number needed to treat: 56
98.1%94.9% 92.0% 89.9%
98.2%93.7%
90.2% 86.7%
APHINITY: Node-positive Subgroup

Inv
asi
ve
dis
ea
se-f
ree
su
rviv
al (
%)
100
80
60
40
20
00 6 12 18 24 30 36 42 48
MonthsNo at Risk
Pertuzumab
Placebo897
902
865
882
856
873
849
866
841
856
826
849
818
844
775
792
456
461
Pertuzumab, 32 events
Placebo, 29 events
Unstratified hazard ratio, 1.13 (95% CI, 0.68-1.86)
p = 0.644
99.5% 99.0% 97.5%96.2%
99.7% 99.1% 98.4% 96.7%
APHINITY: Node-negative Subgroup

Inv
asi
ve
dis
ea
se-f
ree
su
rviv
al (
%)
100
80
60
40
20
00 6 12 18 24 30 36 42 48
MonthsNo at Risk
Pertuzumab
Placebo864
858
836
827
821
811
813
793
797
771
774
758
755
730
600
569
314
302
Pertuzumab, 71 events
Placebo, 91 events
Unstratified hazard ratio, 0.76 (95% CI, 0.56-1.04)
p = 0.085
Number needed to treat: 63
98.1% 96.2%92.8%
91.0%97.9%
93.7%91.2% 88.7%
APHINITY: Hormone Receptor-negative Subgroup
Inv
asi
ve
dis
ea
se-f
ree
su
rviv
al (
%)
100
80
60
40
20
00 6 12 18 24 30 36 42 48
MonthsNo at Risk
Pertuzumab
Placebo1536
1546
1473
1508
1454
1501
1423
1481
1402
1444
1379
1410
1346
1378
1087
1105
565
564
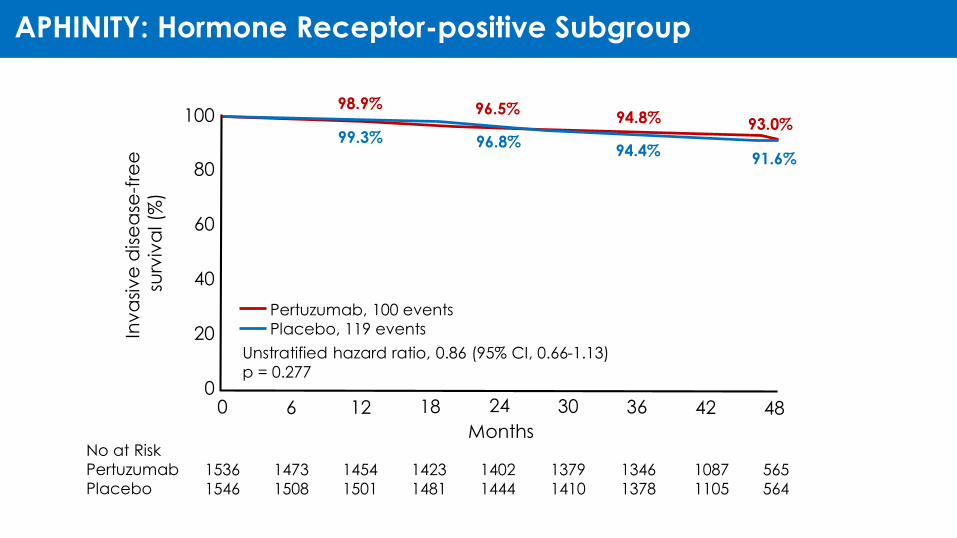
Pertuzumab, 100 events
Placebo, 119 events
Unstratified hazard ratio, 0.86 (95% CI, 0.66-1.13)
p = 0.277
98.9% 96.5%94.8% 93.0%
99.3% 96.8%94.4%
91.6%
APHINITY: Hormone Receptor-positive Subgroup

APHINITY: Conclusions
The APHINITY study met its primary objective
• Pertuzumab reduced the risk of an IDFS event by 19% compared with placebo (HR 0.81; 95% CI 0.66, 1.00; p = 0.045) at a median follow up of 45.4 months (3 years IDFS of 94.1% with pertuzumab and 93.2% with placebo)
Treatment effect was homogenous throughout all subgroups, however the N+ and HR- negative cohorts appeared to derive most benefit at the current point of time
• with a relative risk reduction of 23% and 24%, respectively and
• a 3-year IDFS absolute increase of 1.8% and 1.6% respectively
Cardiac toxicity was low and not diferente between the two arms
The incidence of diarrhea was increased in the pertuzumab arm and occurred predominantly during chemotherapy and with TCH

Redução de Risco de Morte de 20% (HR 0,80)
Linfonodo Positivo com 50% de Risco de Morte
Linfonodo Negativo com 10% de Risco de Morte
Nº de Pacientes % SG aos 5 anos DiferençaAbsoluta %
Adj. Obs. Adj. Obs.
Nº total 500 500 60 50 10
Nº de mortes 200(0,8 x 250)
250 (300 / 500) (250 / 500) (60 – 50)
Nº de Pacientes % SG aos 5 anos DiferençaAbsoluta %Adj. Obs. Adj. Obs.
Nº total 500 500 92 90 2
Nº de mortes 40(0,8 x 50)
50 (460 / 500) (450 / 500) (92-90)
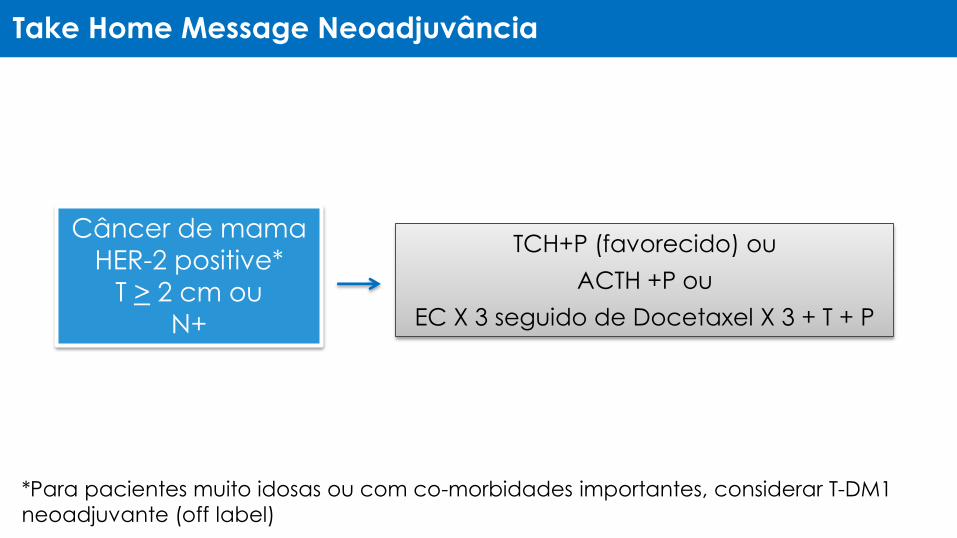
Take Home Message Neoadjuvância
*Para pacientes muito idosas ou com co-morbidades importantes, considerar T-DM1
neoadjuvante (off label)
Câncer de mama
HER-2 positive*
T > 2 cm ou
N+
TCH+P (favorecido) ou
ACTH +P ou
EC X 3 seguido de Docetaxel X 3 + T + P

Take Home Message Adjuvância
T > 2 cm, N0
T 0,6 a ≤ 2 cm e LN -
T ≤ 0,5 cm e LN -
TH
TCH ou ACTH*
Discutir TH
*Em casos selecionados, considerar TH para pacientes muito idosas ou com
co-morbidades importantes.
Câncer de mama
HER-2 positivo
qqT, LN + TCH+P ou ACTH +P

Thank you


















