Actualización en sedación octubre 2014, WHAT´S NEW ON SEDATION IN ICU
44
ACTUALIZACIÓN EN SEDACIÓN Juan Pablo González V. Medicina de Urgencias USACH - HRR CICLO DE FORMACIÓN CONTINUA UNIDAD DE CUIDADOS INTENSIVOS Tutor: Dra. Daniela Soto Medicina Interna UCI HRR
-
Upload
juan-pablo-gonzalez-vallejos -
Category
Healthcare
-
view
114 -
download
0
Transcript of Actualización en sedación octubre 2014, WHAT´S NEW ON SEDATION IN ICU

ACTUALIZACIÓN EN SEDACIÓN
Juan Pablo González V.
Medicina de Urgencias
USACH-HRR
CICLO DE FORMACIÓN CONTINUAUNIDAD DE CUIDADOS INTENSIVOS
Tutor: Dra. Daniela Soto
Medicina Interna
UCI HRR

RINALDO BELLOMO
¿Cual es el futuro de los cuidados intensivos?
“PRIMUN NON NOCERE”

PUNTOS A TRATAR
• CONCEPTOS
• DROGAS MÁS UTILIZADAS
• EVIDENCIA
• OTRA EXPERIENCIA
• NUESTRO PROTOCOLO
• CONCLUSIONES

SEDACIÓN EN CUIDADOS INTENSIVOS
• ANSIEDAD – INCOMODIDAD
• FACILITAR PROCEDIMIENTOS (ASPIRACIÓN - PUNCIONES)
• DISMINUIR CONSUMO DE OXÍGENO
• EVENTOS: EXTUBACIÓN ACCIDENTAL
CONCEPTOS

DELIRIUM
• EL DELIRIUM MATA (A)
• EL DELIRIUM AUMENTA EL DETERIORO COGNITIVO (B)
• EL DELIRIUM AUMENTA LOS DÍAS DE HOSPITALIZACIÓN (A)
• EL DELIRIUM AUMENTA LOS COSTOS
Barr J, Fraser G. Clinical practice guidelines for the management of pain,agitation, and delirium in adult patients in the intensive care unit.Crit Care Med. 2013 Jan;41(1):263-306.
CONCEPTOS

INTERRUPCIÓN DIARIA DE SEDACIÓN
Y PROTOCOLOS
MENOS DÍAS ESTADÍA
MENOS DÍAS VM
Kress JP et al. Daily interruption of sedative infusions in critically ill patients undergoingmechanical ventilation. N Engl J Med 2000, 342:1471-1477.
Brook AD et al. Effect of a nursing implemented sedation protocol on the duration of mechanical ventilation. Crit Care Med 1999, 27:2609-2615
CONCEPTOS

SOBRESEDACIÓN MAYOR MORTALIDAD
Girard TD et al. Efficacy and safety of a paired sedation and ventilator weaning protocolfor mechanically ventilated patients in intensive care (Awakening and BreathingControlled trial: a randomised controlled trial. Lancet 2008;371:126–134.
Shehabi Y, Bellomo R et al. Sedation Practice in Intensive Care Evaluation (SPICE) StudyInvestigators; ANZICS Clinical Trials Group. Early intensive care sedation predicts longterm mortality in ventilated critically ill patients. Am J Respir Crit Care Med2012;186:724–731
Shehabi Y, Chan L et al. Sedation Practice in Intensive Care Evaluation (SPICE) StudyGroup investigators. Sedation depth and long-term mortality in mechanically ventilatedcritically ill adults: a prospective longitudinal multicentre cohort study. Intensive CareMed 2013;39:910–918
CONCEPTOS
MIDAZOLAM
• SINDROME DE DESCONTINUACIÓN
• RECUPERACIÓN RETARDADA POR ACUMULACIÓN (FALLA RENAL)
DROGAS
Hughes MA et al. Context-sensitive half-time in multicompartmentpharmacokinetic models for intravenous anesthetic drugs. Anesthesiology1992;76:334–341

LORAZEPAM – MIDAZOLAM
Factores de riesgo independientes para
DELIRIUM
Pandharipande PP, Pun BT, et al. Effect of sedation with dexmedetomidine vs lorazepamon acute brain dysfunction in mechanically ventilated patients: the MENDS randomizedcontrolled trial. JAMA 2007;298:2644–2653.
Pisani MA, Murphy TE, et al. Benzodiazepine and opioid use and the duration of intensive care unit delirium in an older population. Crit Care Med 2009;37:177–183
Pandharipande P et al. Lorazepam is an independent risk factor for transitioning todelirium in intensive care unit patients. Anesthesiology 2006;104:21–26.
DROGAS

BENZODIACEPINAS
PEORES RESULTADOS :
SOBRESEDACIÓN, DELIRIUM, RETRASO DE EXTUBACIÓN, ESTADÍAS EN UCI PROLONGADAS Y COSTOSAS
Carson SS, et al. A randomized trial of intermittent lorazepam versus propofol with dailyinterruption in mechanically ventilated patients. Crit Care Med 2006; 34:1326–1332.
Pandharipande, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute braindysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA 2007;298:2644–2653.
Breen D, Karabinis A. Decreased duration of mechanical ventilation when comparing analgesia-based sedation using remifentanil with standard hypnotic-based sedation for up to 10 days in intensive care unit patients: a randomised trial. Crit Care 2005.
DROGAS

PROPOFOL
• EFECTOS DOSIS DEPENDIENTES
• RECUPERACIÓN MÁS RAPIDA, SIN ACUMULACIÓN
• HIPERTRIGLICERIDEMIA
• DEPRESIÓN CARDIOVASCULAR
• SD DE INFUSIÓN DE PROPOFOL
• MAYOR COSTO
DROGAS
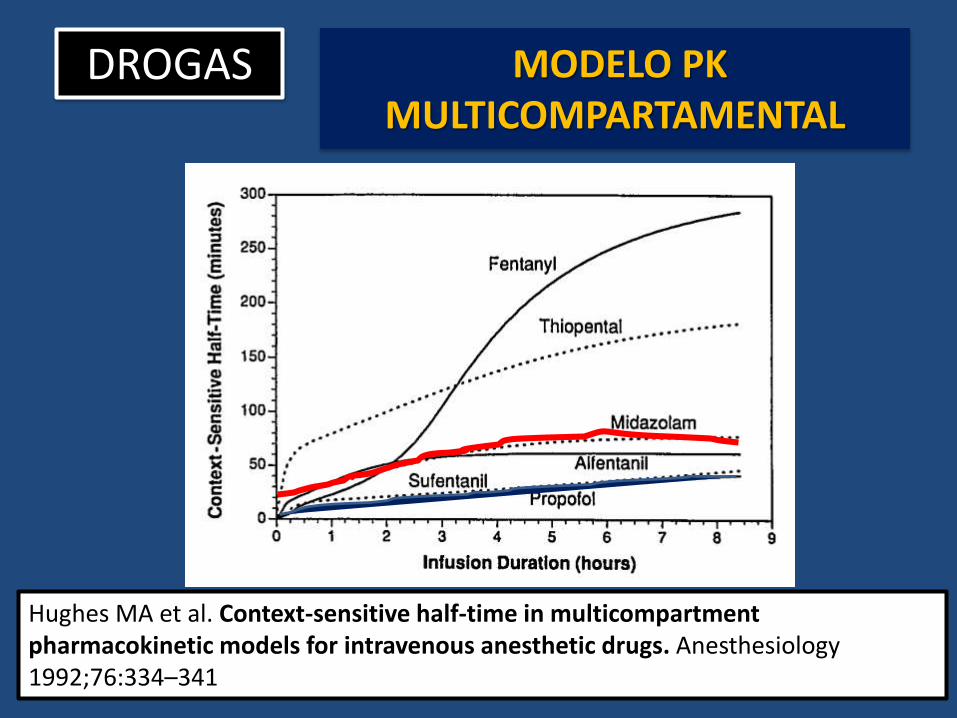
MODELO PK MULTICOMPARTAMENTAL
Hughes MA et al. Context-sensitive half-time in multicompartmentpharmacokinetic models for intravenous anesthetic drugs. Anesthesiology1992;76:334–341
DROGAS

Sanders RD et al. Benzodiazepine augmented g-amino-butyric acid signalingincreases mortality from pneumonia in mice. Crit Care Med 2013;41:1627–1636.
DROGAS

Sanders RD et al. Benzodiazepine augmented g-amino-butyric acid signalingincreases mortality from pneumonia in mice. Crit Care Med 2013;41:1627–1636.
BENZODIACEPINAS
EFECTOS INMUNOMODULADORES
ESTIMULACIÓN rGABA
Producción citokinasFagocitosis bacteriana
Obiora E, Sanders RD et al. The impact of benzodiazepines on occurrence of pneumonia and mortality from pneumonia: a nested case-control and survival analysis in a population based cohort. Thorax 2013;68:163–170.
DROGAS
• α2-AGONISTA
• MECANISMO DE ACCIÓN UNICO
• SEDANTE – ANALGESICO – SIMPATICOLÍTICO
• HIPOTENSIÓN
• BRADICARDIA
Myatra et al. Dexmedetomidine: Toward a paradigm shift in ICU sedation. Indian J Crit Care Med. May 2014; 18(5): 271–272.
DexmedetomedinaDROGAS

PUNTOS CLAVE
• EXISTE UNA ACTIVA DISCUSIÓN SOBRE LA SEDACIÓN EN UCI – TEMA NO ACABADO
• EL DELIRIUM DAÑA A LOS PACIENTES
• HAY EVIDENCIA DE QUE LAS BENZODIACEPINAS POR DIVERSOS MECANISMOS PODRÍAN SER DELETÉREAS

EVIDENCIA American College of Critical Care MedicineCrit Care Med. 2013 Jan;41(1):263-306

EVIDENCIA
“SE SUGIERE PREFERIR NO BENZODIAZEPINICOS PARA SEDACIÓN PARA
MEJORAR RESULTADOS EN PACIENTES ADULTOS EN VENTILACIÓN MECANICA” (2B)
EVIDENCIA

PROYECTO IMPACTEVIDENCIA

EVIDENCIA
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA

• BASE DE DATOS IMPACT
• RETROSPECTIVO, COHORTE
• PAREAMIENTO POR PROPENSIÓN
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit Care Med2014;189: 1383–1394.
EVIDENCIA

• VENTILACIÓN MECANICA
• Analisis pareado 1:1
Infusión contínua sedante único
PROPOFOL VS MIDAZOLAM (2250 c/u)
PROPOFOL VS LORAZEPAM (1054 c/u)
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit Care Med2014;189: 1383–1394.
EVIDENCIA
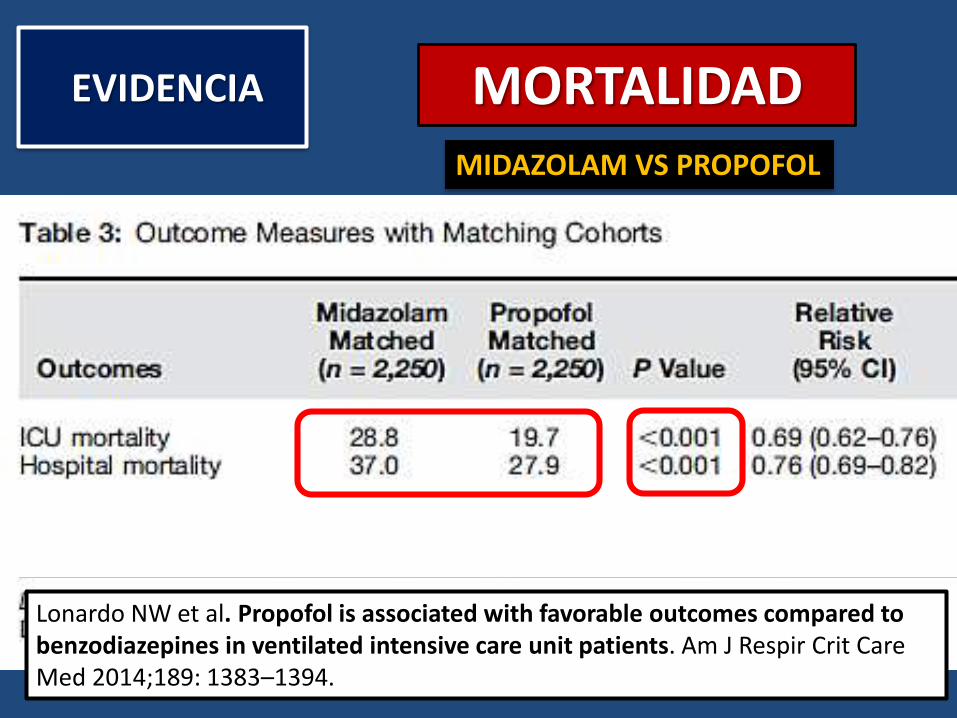
MORTALIDAD
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA
MIDAZOLAM VS PROPOFOL

MORTALIDAD – TRAQUEOSTOMÍA NEUMONIA
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA
LORAZEPAM VS PROPOFOL
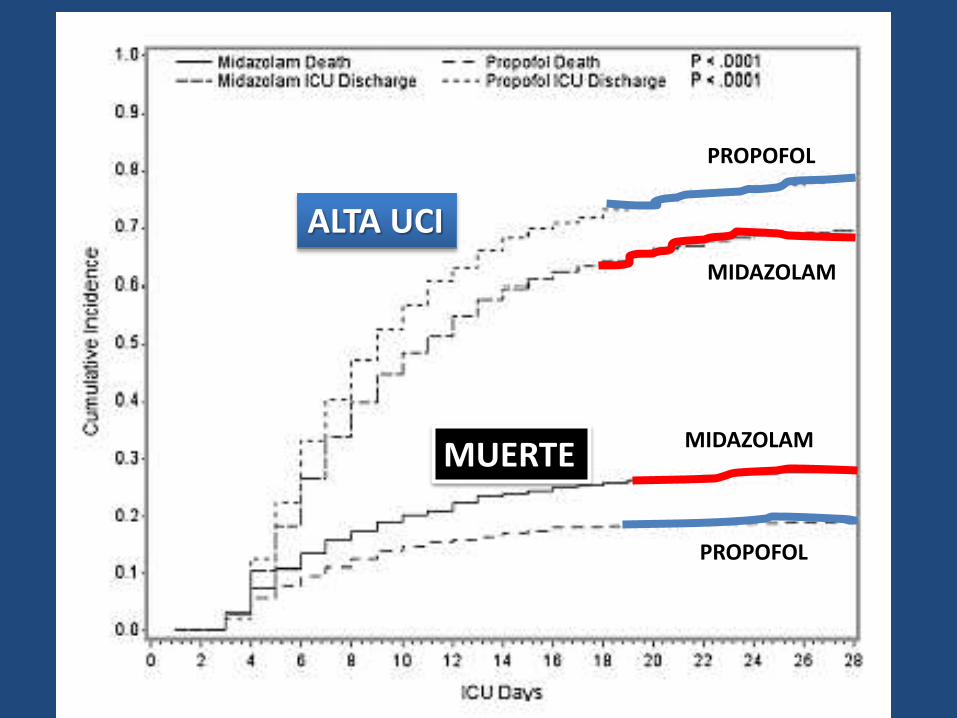
ALTA UCI
MUERTE
PROPOFOL
MIDAZOLAM
PROPOFOL
MIDAZOLAM

ALTA UCI
MUERTE
PROPOFOL
LORAZEPAM
PROPOFOL
LORAZEPAM
ALTA UCI
MUERTE

PROPOFOL MDZ P
WEANING (+)
(DIA 28) 84,4% 75.1% < 0,001
PROPOFOL LRZ P
WEANING (+)
(DIA 28) 84,3% 78,8% < 0,001
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA DEPENDENCIA DE
VENTILACIÓN

PROPOFOL MDZ P
ALTA DE UCI
(DIA 28) 78,9% 69,5% < 0,001
PROPOFOL MDZ P
ALTA DE UCI
(DIA 28) 78,9% 69,5% < 0,001
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA ESTADÍA ICU

NEUMONIA
PROPOFOL LRZP P
NEUMONIA 7,9% 12,7% < 0,001
ASOCIADA VM
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA

PUNTOS CLAVE DEL ESTUDIO
• EL USO DE BENZODIAZEPINAS PARA SEDACIÓN EN UCI PODRÍA GENERAR PEORES RESULTADOSCOMPARADO CON PROPOFOL
• EN MORTALIDAD, TIEMPO DE VM, TIEMPO DE ESTADÍA, NECESIDAD DE TRAUEOSTOMÍA Y NEUMONIA AVM
Lonardo NW et al. Propofol is associated with favorable outcomes compared tobenzodiazepines in ventilated intensive care unit patients. Am J Respir Crit CareMed 2014;189: 1383–1394.
EVIDENCIA

EVIDENCIA

• UN CENTRO, RANDOMIZADO, ABIERTO
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIA
West China Hospital of Sichuan University

TRES GRUPOS
FENTANILO Bolo 1 to 2 μg/kg
BIC 1 to 2 μg/kg/hr
INTERRUPCIONES DIARIAS
TODOS
+
MIDAZOLAM (M)
PROPOFOL (P)
MIDAZOLAM-PROPOFOL(M-P)
EVIDENCIA

1. GRUPO MIDAZOLAM
Bolo 0.03 - 0.30 mg/kg
BIC 0.04 - 0.20 mg/kg/hr
2. GRUPO PROPOFOL
Bolo 0.50 - 3mg/kg
BIC 0.50 - 3 mg/kg/hr
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIA

GRUPO MIDAZOLAM - PROPOFOL
PRIMERO Midazolam LUEGO: Propofol
CRITERIOS DE CAMBIO:Pa O2 > 60 mmHgFiO2 < 50%PEEP < 10ESTABILIDAD HEMODINAMICA: NO ISQUEMIA MIOCARDICA NI HIPOTENSIÓNDobuta < 5 μg/kg/minNorepinefrina ≤2 μg/min
EVIDENCIA
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIA

RESULTADOSEVIDENCIA
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIA

COSTOSEVIDENCIA
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIA

RECUERDOS
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIAEVIDENCIA

PUNTOS CLAVE DEL ESTUDIO
• UN PROTOCOLO COMBINADO DE SEDACIÓN CON MIDAZOLAM – PROPOFOL PODRÍA TENER MEJORES RESULTADOS EN UCI
• EN TIEMPO DE ESTADÍA, TIEMPO DE VENTILACIÓN MECÁNICA, COSTOS Y CANTIDAD DE RECUERDOS TRAUMÁTICOS
Zhou et al. Midazolam and propofol used alone or sequentially for long-term sedation in critically ill, mechanically ventilated patients: a prospective, randomized study. Critical Care 2014, 18:R122
EVIDENCIA

OTRA EXPERIENCIA

NUESTRO PROTOCOLO
ENCUESTA ¿Por qué no usa el protocolo de sedación?
Los residentes no lo indican
Se inicia y después es cambiado por el residente
No se indica por escalón de sedación
Porque no sirve – dosis muy bajas – respuesta inadecuada
Nunca se a discutido ni actualizado
Dosis se calculan por pero estimado y no real
• Escasa adherencia

CONCLUSIONES
• LA MEJOR ESTRATEGIA DE SEDACIÓN EN UCI ES UN TEMA EN DISCUSIÓN
• EXISTE EXTENSA EVIDENCIA EL USO DE BENZODIAZEPINAS PODRÍA SER DELETÉREO, INCLUSO CON EFECTO EN MORTALIDAD
• PROPOFOL PARECE SER UNA BUENA ALTERNATIVA

CONCLUSIONES
• EL USO DE UN PROTOCOLO COMBINADO PODRÍA MINIMIZAR EL RIESGO DE LAS BZD Y GENERAR MEJORES RESUTADOS CLÍNICOS Y ECONÓMICOS
• HAY POCA ADHERENCIA A NUESTRO PROTOCOLO. ¿SERÁ MOMENTO DE ANALIZAR EL TEMA?

• MUCHAS GRACIAS.






![ICU 2003 [Unlocked by Www.freemypdf.com].en.es](https://static.fdocuments.ec/doc/165x107/563dbaf2550346aa9aa8f547/icu-2003-unlocked-by-wwwfreemypdfcomenes.jpg)