







Idiomas
Páginas
Jurídico

Dilema éticoHasta cuándo continuar tratamiento oncológico
V JORNADAS ONCOLOGICAS HOSPITALARIAS.
CCR.FOPA 2015
DR. HUGO FORNELLS. CUIDADOS PALIATIVOS. ROSARIO
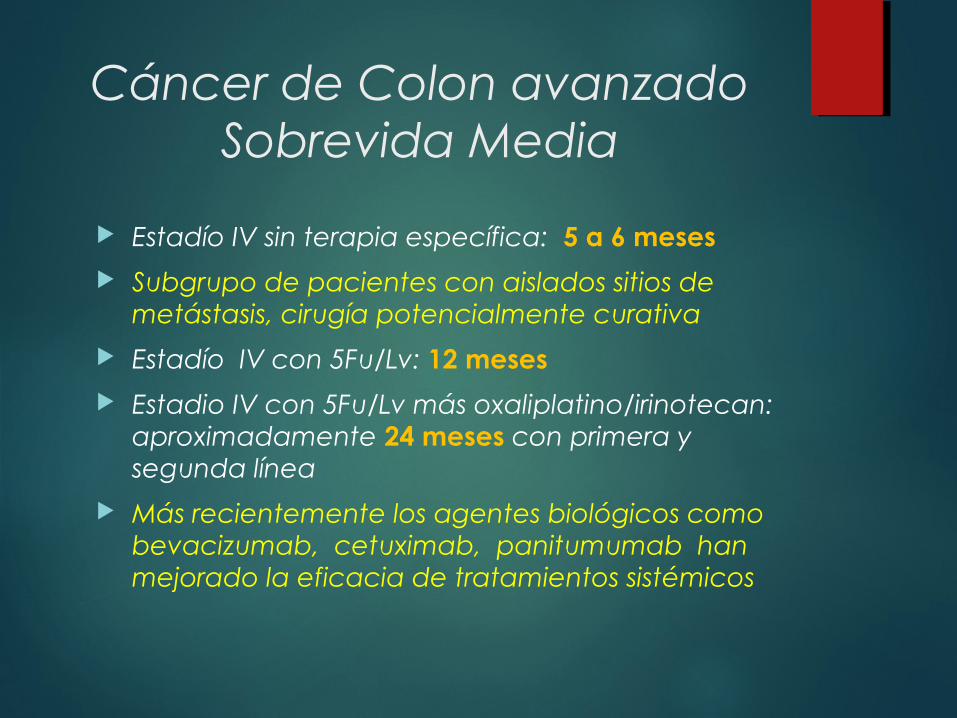
Cáncer de Colon avanzadoSobrevida Media
Estadío IV sin terapia específica: 5 a 6 meses
Subgrupo de pacientes con aislados sitios de metástasis, cirugía potencialmente curativa
Estadío IV con 5Fu/Lv: 12 meses
Estadio IV con 5Fu/Lv más oxaliplatino/irinotecan: aproximadamente 24 meses con primera y segunda línea
Más recientemente los agentes biológicos como bevacizumab, cetuximab, panitumumab han mejorado la eficacia de tratamientos sistémicos

Objetivos en Medicina
Los dos grandes objetivos de la medicina: Curar la enfermedad Aliviar el sufrimiento
Dentro de estos dos objetivos globales, múltiples objetivos: curación completa prolongar la sobrevida mejorar la calidad de vida alivio de múltiples sufrimientos apoyo a la familia y seres queridos buena muerte

Objetivos en Medicina cuando la curación no es posible
Los dos grandes objetivos de la medicina: Curar la enfermedad Aliviar el sufrimiento
Dentro de estos dos objetivos globales, múltiples objetivos: curación completa prolongar la sobrevida mejorar la calidad de vida alivio de múltiples sufrimientos apoyo a la familia y seres queridos buena muerte

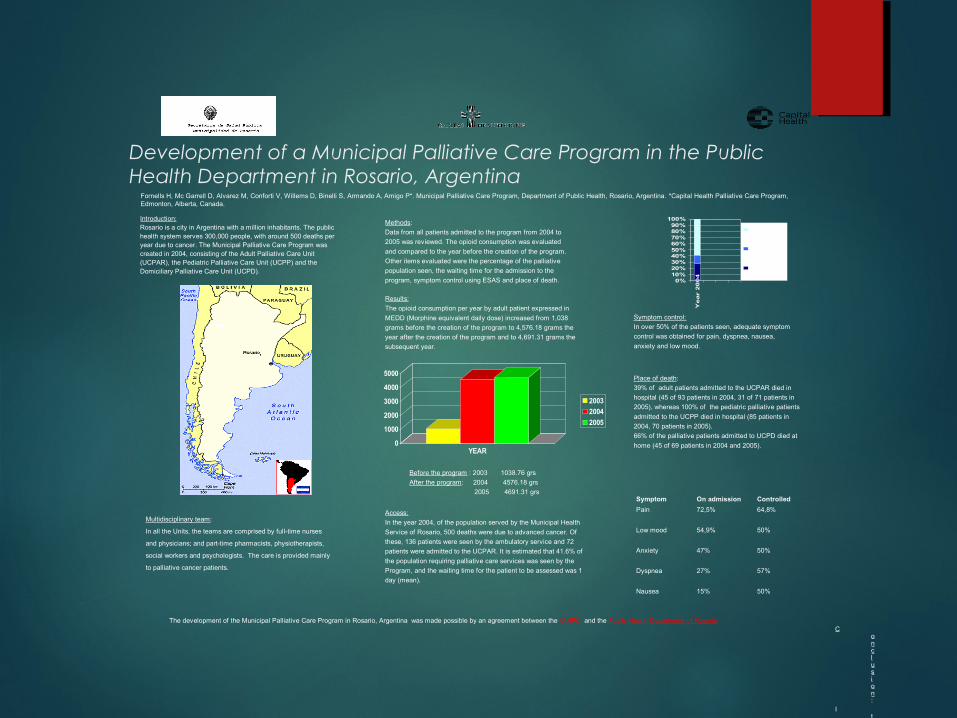
Development of a Municipal Palliative Care Program in the Public Health Department in Rosario, Argentina
Fornells H, Mc Garrell D, Alvarez M, Conforti V, Willems D, Binelli S, Armando A, Amigo P*. Municipal Palliative Care Program, Department of Public Health, Rosario, Argentina. *Capital Health Palliative Care Program, Edmonton, Alberta, Canada.
Introduction:Rosario is a city in Argentina with a million inhabitants. The public health system serves 300,000 people, with around 500 deaths peryear due to cancer. The Municipal Palliative Care Program wascreated in 2004, consisting of the Adult Palliative Care Unit(UCPAR), the Pediatric Palliative Care Unit (UCPP) and theDomiciliary Palliative Care Unit (UCPD).
Methods:
Data from all patients admitted to the program from 2004 to
2005 was reviewed. The opioid consumption was evaluated
and compared to the year before the creation of the program.
Other items evaluated were the percentage of the palliative
population seen, the waiting time for the admission to the
program, symptom control using ESAS and place of death.
Results:
The opioid consumption per year by adult patient expressed in
MEDD (Morphine equivalent daily dose) increased from 1,038
grams before the creation of the program to 4,576.18 grams the
year after the creation of the program and to 4,691.31 grams the
subsequent year.
0
1000
2000
3000
4000
5000
YEAR
2003
2004
2005
Before the program : 2003 1038.76 grs
After the program: 2004 4576.18 grs
2005 4691.31 grs
0%10%20%30%40%50%60%70%80%90%
100%
Year
20
04
not seen
UCPARinpatient
UCPARambulatory
Access:
In the year 2004, of the population served by the Municipal Health
Service of Rosario, 500 deaths were due to advanced cancer. Of
these, 136 patients were seen by the ambulatory service and 72
patients were admitted to the UCPAR. It is estimated that 41.6% of
the population requiring palliative care services was seen by the
Program, and the waiting time for the patient to be assessed was 1
day (mean).
Symptom On admission Controlled
Pain 72,5% 64,8%
Low mood 54,9% 50%
Anxiety 47% 50%
Dyspnea 27% 57%
Nausea 15% 50%
Symptom control:
In over 50% of the patients seen, adequate symptom
control was obtained for pain, dyspnea, nausea,
anxiety and low mood.
Place of death:
39% of adult patients admitted to the UCPAR died in
hospital (45 of 93 patients in 2004, 31 of 71 patients in
2005), whereas 100% of the pediatric palliative patients
admitted to the UCPP died in hospital (85 patients in
2004, 70 patients in 2005).
66% of the palliative patients admitted to UCPD died at
home (45 of 69 patients in 2004 and 2005).
Conclusion:
It was possible to provide good interdisciplinary palliative
care services with little waiting time and good symptom
control, increasing the opioid consumption and providing
adequate support for those who chose to die at home and
their families.
Future goal: to increase access to the service and to
extend this care to non-cancer patients.
The development of the Municipal Palliative Care Program in Rosario, Argentina was made possible by an agreement between the IAHPC and the Public Health Department of Rosario
Multidisciplinary team:
In all the Units, the teams are comprised by full-time nurses
and physicians; and part-time pharmacists, physiotherapists,
social workers and psychologists. The care is provided mainly
to palliative cancer patients.
Es difícil decirle a un paciente: “Sí es cáncer” o “Sí, parece que la enfermedad está ganando”. Y especialmente difícil cuando el paciente tiene 16 ó 26 años. Incluso a los 76 u 86 no es fácil. De hecho si alguna vez parece fácil el médico puede estar seguro de que ya no está siendo de mucha utilidad para sus pacientes.
Robert Twycross. Acta Bioethica. OPS/OMS
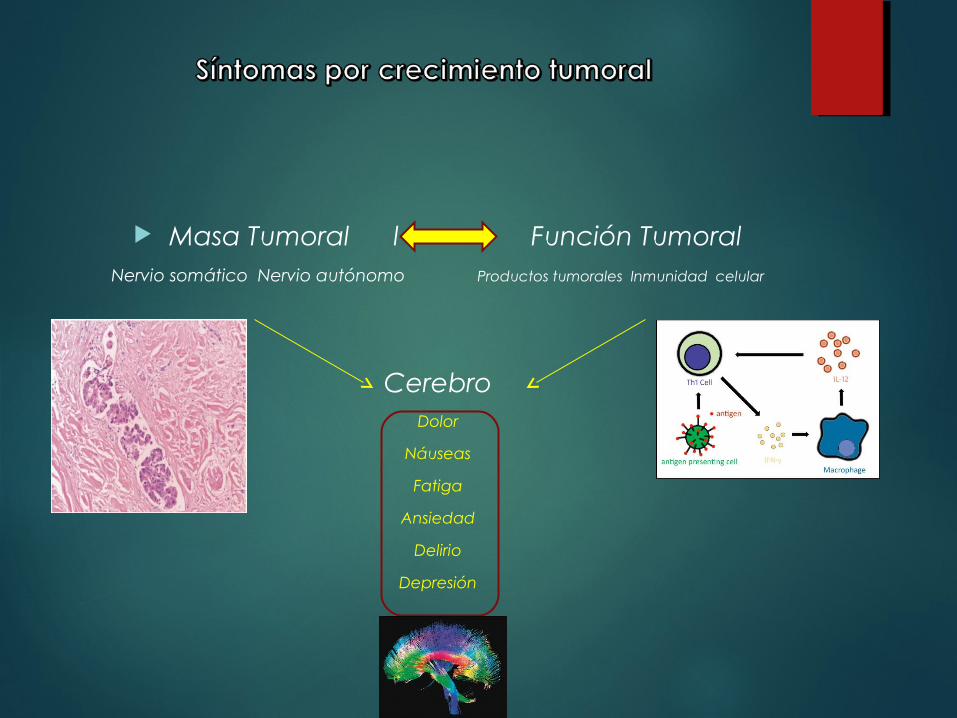
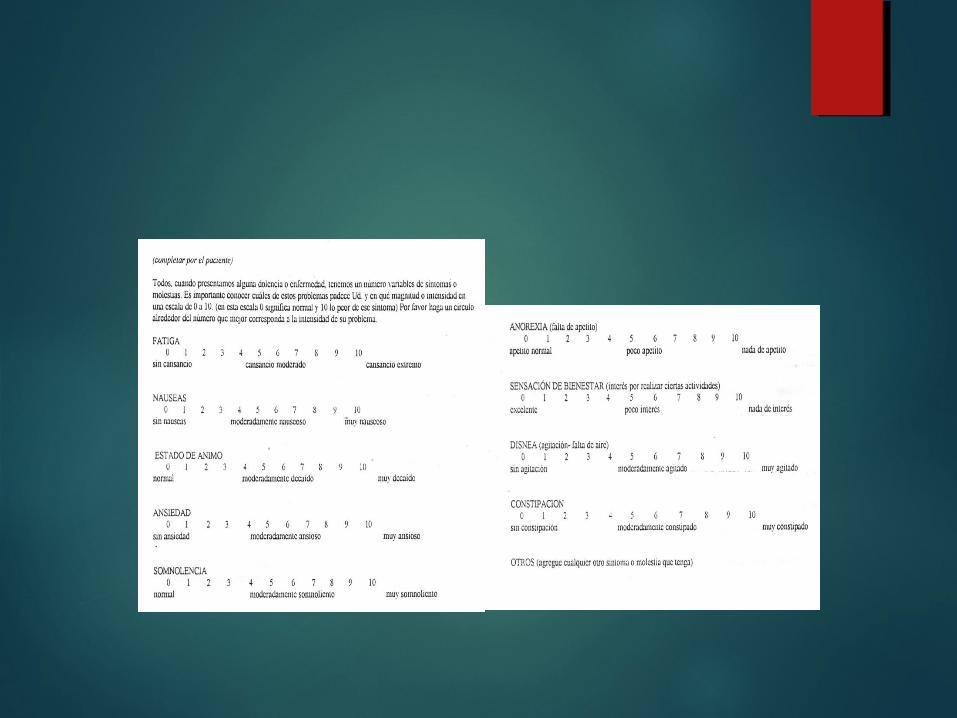
Masa Tumoral l Función TumoralNervio somático Nervio autónomo Productos tumorales Inmunidad celular
CerebroDolor
Náuseas
Fatiga
Ansiedad
Delirio
Depresión

Obstrucción Intestinal
Obstrucción Intestinal
Cáncer ginecológico avanzado
Cáncer gastrointestinal avanzado
Complica 5 a 51% de cáncer de ovario
Complica 10 a 28% de cáncer de colon
Cáncer de pulmón, de mama y melanoma son los más frecuentes extra-abdominales

Obstrucción Intestinal
FISIOPATOLOGÍA: Obstrucción ------ Secreciones
proximales no absorbidas ------- Distensión Abdominal y Cólico Intestinal
Peristalsis inefectiva Hipertensión endoluminal --- Daña
epitelio ----- Respuesta inflamatoria ----- Cicloxigenasas-----Prostaglandinas---- Aumento de secreción intestinal ----- Aumenta presión endoluminal----- Bloquea drenaje venoso ----- Interfiere con consumo de O2 ----- Gangrena o Perforación

Obstrucción Intestinal
Fisiopatología: Hipoxia---- aumenta secreción de
VIP----- VIP en circulación portal y circulación periférica------VIP produce hiperemia y edema pared intestinal y mayor secreción endoluminal, vasodilatación esplácnica e hipotensión-----Falla sistémica multiorgánica
Sobrecrecimiento bacteriano + Isquemia----Sepsis

Obstrucción Intestinal
Cuándo ocurre? Cómo estaba el paciente previo a la
obstrucción?
Qué rol ya presentaban los productos tumorales: citokinas, TNF, inmunidad celular en el estado previo del paciente?
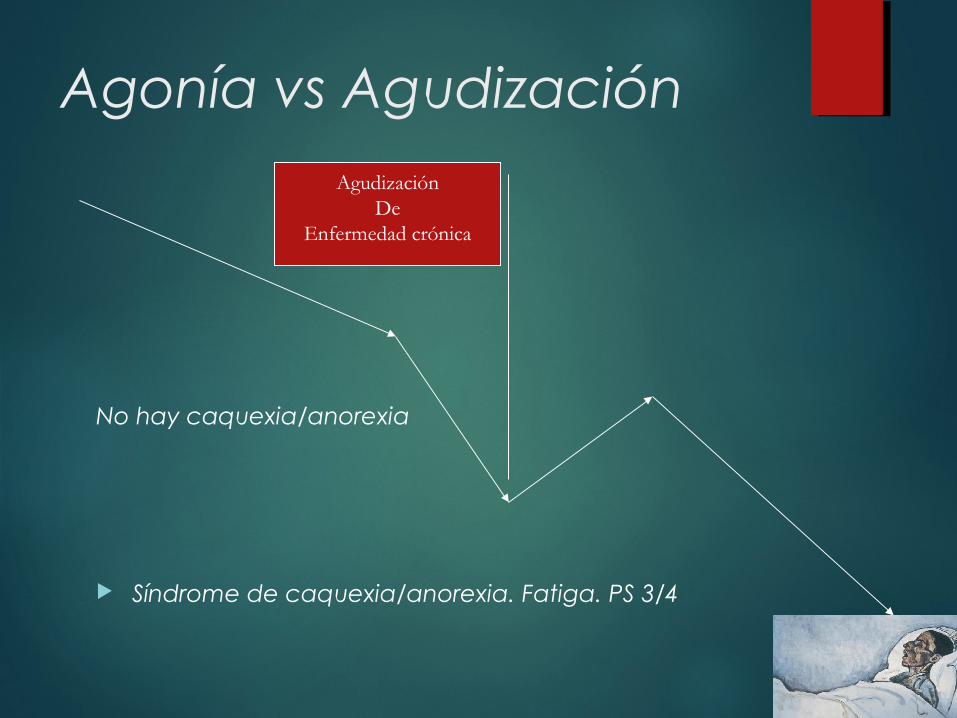
Agonía vs Agudización
No hay caquexia/anorexia
Síndrome de caquexia/anorexia. Fatiga. PS 3/4
AgudizaciónDe
Enfermedad crónica

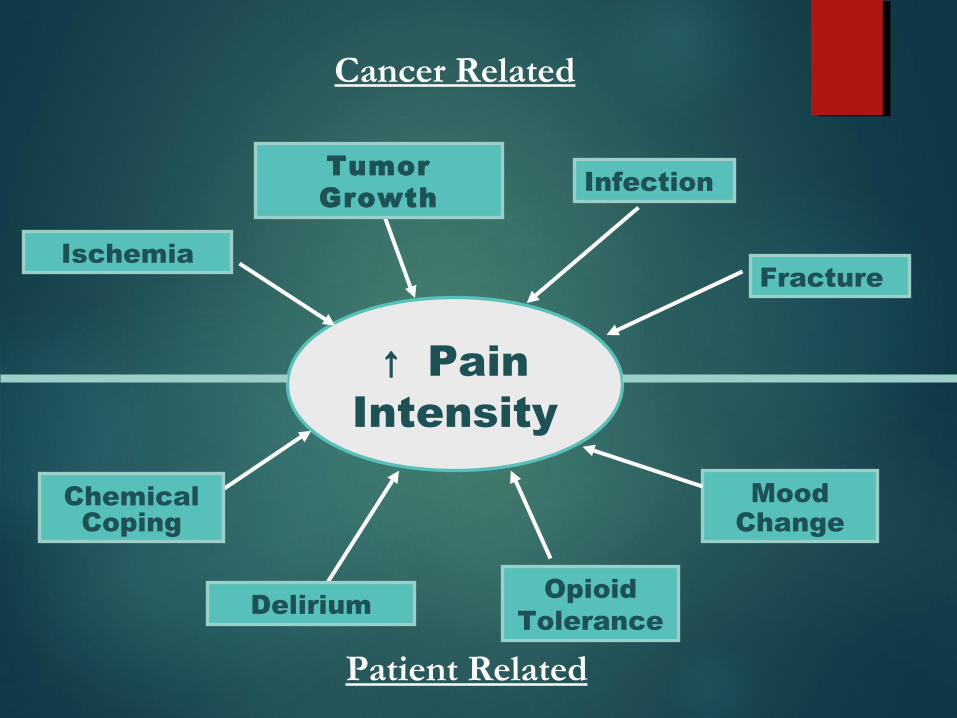
↑ PainIntensity
ChemicalCoping
Ischemia
Tumor Growth Infection
Opioid ToleranceDelirium
Fracture
MoodChange
Cancer Related
Patient Related
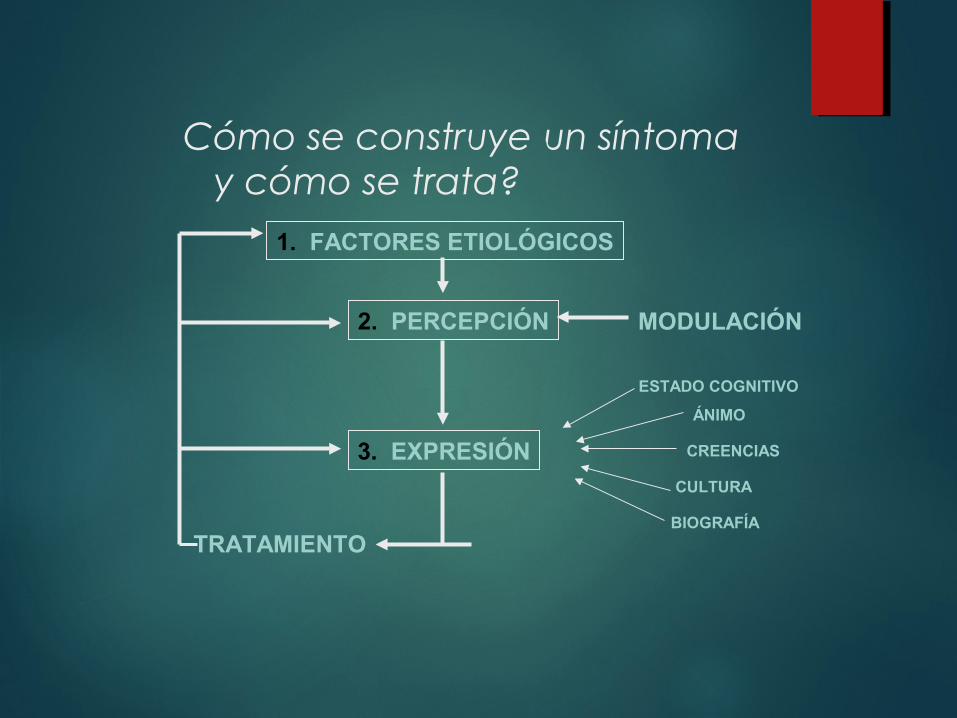
Cómo se construye un síntoma y cómo se trata?
1. FACTORES ETIOLÓGICOS
2. PERCEPCIÓN
3. EXPRESIÓN
MODULACIÓN
ESTADO COGNITIVO
ÁNIMO
CREENCIAS
CULTURA
BIOGRAFÍA
TRATAMIENTO

Cómo se construye un síntoma y cómo se trata?
1. FACTORES ETIOLÓGICOS
2. PERCEPCIÓN
3. EXPRESIÓN
MODULACIÓN
ESTADO COGNITIVO
ÁNIMO
CREENCIAS
CULTURA
BIOGRAFÍA
TRATAMIENTO
Sobrevida es el resultado más importante esperado
Mejoría en sobrevida libre de enfermedad es un requisito para indicar adyuvancia
En enfermedad avanzada los resultados referidos al paciente son más importantes que los resultados referidos al tumor

Qué es más importante?
1. El manejo de los síntomas físicos
2. El control de los síntomas psicológicos
3. La contención social
4. La calidad de vida
5. El trato digno
6. Evitar sufrimientos innecesarios
El sufrimiento es experimentado por personas, no por cuerpos, por lo tanto es físico, psicológico, social.
Es un estado de distrés severo que es personal, individual y subjetivo
Es la percepción de que hay algo que amenaza la integridad de uno mismo
Hay más sufrimiento en sus pacientes que lo que Ud. sospecha. Eric Cassell
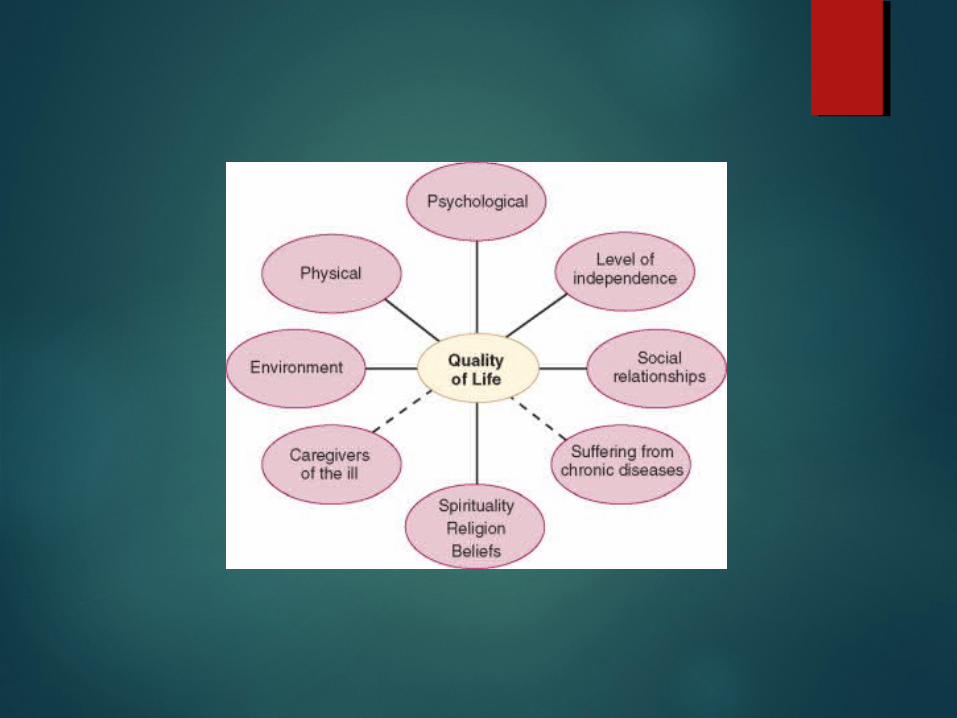
Calidad de Vida
deseos esperanzas ambiciones
estado funcional actual

QUIMIOTERAPIA PALIATIVA?
El Enfoque Inclusivo con tratamiento del tumor y con
cuidados paliativos debería ser el standard de alta calidad en
todo Departamento de Oncología


Estudio prospectivo multicéntrico de cohorte: 386 adultos con cáncer metastásico progresados al menos a un plan de QT
216 (56%) recibían quimioterapia paliativa con una media de 4 meses antes de la muerte
14% del grupo QT : ARM o RCP o ambas en semana previa a la muerte comparado con 2% del grupo no QT
34% del grupo QT tardía derivación a hospice vs 47% no QT
11% del grupo QT tardía murieron en UTI vs 2% del grupo no QT
47% del grupo QT murieron en casa vs 66% del grupo noQT
Sobrevida Global igual en ambos grupos Prigerson H. BMJ 2014; 348:g1904

Datos comparativos:Hospital público municipal c/ UCPSanatorio Privado s/ UCP
Sanatorio Privado (datos Sanatorio Privado (datos setptiembre 2009)setptiembre 2009)
UCPAR (datos septiembre UCPAR (datos septiembre 2008)2008)
Muertes por cáncer en un Muertes por cáncer en un mes: 20mes: 20
Muertes por cáncer en un Muertes por cáncer en un mes: 15mes: 15
Muertes internados: 18 Muertes internados: 18 90%90% (domicilio 10%) (domicilio 10%)
Muertes internados: 6 Muertes internados: 6 39%39% (domicilio 61%)(domicilio 61%)
Quimioterapias último mes de vidaQuimioterapias último mes de vida
35%35%Quimioterapias último mes de vidaQuimioterapias último mes de vida
0%0%
Control síntomas distresantesControl síntomas distresantes
No hay registrosNo hay registrosControl síntomas distresantes Control síntomas distresantes > > 50%50%

The NEW ENGLAND JOURNAL of MEDICINE
ORIGINAL ARTICLE
PARA TOMA DE DECISIONES COMPARTIDAS

. . .. . . Escala de Karnofsky como Escala de Karnofsky como predictor de supervivenciapredictor de supervivencia
. . .. . . Escala de Karnofsky como Escala de Karnofsky como predictor de supervivenciapredictor de supervivencia
KPSKPS Supervivencia en díasSupervivencia en días
≥≥ 5050 86.186.1
30-4030-40 49.849.8
10-2010-20 16.816.8
Reuben DB, Mor V, Hiris J. Arch Intern Med. 1988.

Impacto de PronósticoImpacto de PronósticoImpacto de PronósticoImpacto de Pronóstico
ÍndiceÍndice Supervivencia promedio Supervivencia promedio (Meses)(Meses)
HipercalcemiaHipercalcemia 1 - 4.51 - 4.5
Metástasis cerebral Metástasis cerebral más cirugíamás cirugía 9.59.5
Metástasis cerebral sin Metástasis cerebral sin cirugíacirugía 44
Efusión pleuralEfusión pleural 33

Dar información directamente sobre pronóstico y tratamiento es deseada y útil. Leighel. J Clin Oncol 2007
No hay trabajo que demuestren que dar información cuidadosa a los pacientes aumente el daño. Tobias J.S. BMJ 1993. Fallowfield L. BMJ 2001
98% de 126 pacientes terminalmente enfermos dijeron que querían que su oncólogo fuera realista, sincero, compasivo y siga tratándolo durante su enfermedad. Hagerty R.G. J Clin Oncol 2005. Canadian and Australian Qualitative Study. BMJ 2004

CONCEPTO DE INTEGRACIÓN DE TRATAMIENTO DEL PACIENTE CON CÁNCER Y SU FAMILIA
Dr. Hugo Fornells Congreso de Cancerología Cali, Colombia 2008
PS 0 PS 1 PS 2 PS3 PS 4 Control Psicosocial y Espiritual
Dimensión
Control de Síntomas Fisicos
Duelo
C U I D A D O S P A L I A T I V O S : Equipo – Paciente Familia
Inicio de Enfermedad Muerte
TratamientoOncológico
Terapia de Soporte

DILEMA ÉTICO
DILEMA ÉTICO
DILEMA ÉTICO
Top Related