





Idiomas
Páginas
Jurídico


Anticuerpos Monoclonales Anticuerpos Monoclonales contra el EFGRcontra el EFGR
Dra. María Verónica Pereira Díaz, R4Dra. María Verónica Pereira Díaz, R4
Tutora: Dra. Laura VidalTutora: Dra. Laura Vidal
Servicio de Oncología MédicaServicio de Oncología Médica
Hospital Clínic de BarcelonaHospital Clínic de Barcelona
22 Enero 201222 Enero 2012
V Jornada Growing UpTratamiento dirigido a diana:
eficacia y toxicidad

OutlineOutline
• EGFR signalling pathway• Monoclonal antibodies
– Cetuximab– Panitumumab
• Indicaciones clínicas– EFGR mAB in colorectal cancer– EGFR mAB in head and neck cancer
• Toxicidades y su manejo


EGF TGF
Amfiregulina HB-EGF
-celulina Heregulinas
Heregulinas-celulinaNRG2NRG3
EGFR HER2 HER3 HER4
Membrana
Dominio extracelular
DominioTirosín-kinasa
Ligandos

100% Mouse Protein
Mouse
The Development of Monoclonal Antibodies
~10% Mouse Protein
Humanized
~34% Mouse Protein
Chimeric Fully Human
100% Human Protein
cetuximab panitumumab
Yang XD, et al. Crit Rev Oncol Hematol 2001;38:17-23.
(IgG1) (IgG2)

Panitumumab
Panitumumab Inhibits Ligand Binding to EGFR and Dimerization
• A fully human lgG2 monoclonal antibody to EGFR
• High affinity, KD = 5 x 10-11 M• Inhibits ligand-induced EGFR
tyrosine phosphorylation
Inhibition of EGF binding to EGFR
This may lead to: Cell proliferation Cell survival Angiogenesis Metastatic spread
EGF, TGFα or other ligands binding to EGFR
1. Yang XD, et al. Crit Rev Oncol Hematol. 2001;38(1):17-23. 2. Foon KA, et al. Int J Radiat Oncol Biol Phys. 2004;58(3):984-990.





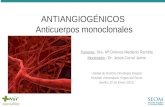
Potential relationship between KRAS status and response to epidermal growth factor receptor (EGFR) monoclonal antibodies, alone or in combination with irinotecan, in
chemotherapy-refractive patients.
Wong R , Cunningham D JCO 2008;26:5668-5670
©2008 by American Society of Clinical Oncology


• EXTREME study: Erbitux + platinum/5-FU in first line recurrent and/or metastatic SCCHN– Primary endpoint (OS) was met– Significant improvements in OS, PFS and response rate– Addition of Erbitux did not adversely influence QoL
Breakthrough advances
Erbitux + platinum/5-FU is the first systemic treatment to show an overall
benefit over platinum/5-FU alone in recurrent and/or metastatic SCCHN
Recent developments with Erbitux: Recurrent and/or metastatic SCCHN

EGFR EGFR is a potent mediator of is a potent mediator of radioresistanceradioresistance
• Posibles mecanismos1-3:
– Upregulation of Bcl-2 (down-regulation of apoptotic response induced by RT [or CT])
– Upregulation of DNA repair mechanisms (repair of potential lethal damage RT [or CT] induced)
– Upregulation of cyclin D activating cell proliferation (enlarging proportion of cells in radioresistant phase of cell cycle)
1 Ke Liang MS, et al. Int J Radiat Oncol Biol Phys 2003;57:246–254;2 Mendelshon J. J Clin Oncol 2002;20:1s–13s; 3 Ochs J. Int J Radiat Oncol Biol Phys 2004;58:941–949
CT, chemotherapy
• Blockade of EGFR signal transduction increases RT activity4 and enhances apoptotic response5
4 Huang S-M, et al. Clin Cancer Res 2000;6:2166–2174; 5 Harari P, et al. Int J Rad Oncol 2001:49;427–433

Stage III and IV non-metastatic
SCCHN(n=424)
RT (n=213)
Erbitux + RT (n=211)Erbitux initial dose (400 mg/m2)1 week before RTErbitux (250 mg/m2) + RT (weeks 2–8)b
Erbitux + RT in locally advanced SCCHN: Phase III study design
Bonner J, et al. N Engl J Med 2006;354:567–578
aInvestigators’ choice; bUAB regimen: Robert F. J Clin Oncol (2001)
R
Primary endpoint: Duration of locoregional control
Secondary endpoints: OS, PFS, RR, and safety
Stratified by
• KPS
• Nodal involvement
• Tumor stage
• RT regimena

Erbitux in locoregionally advanced SCCHN: Efficacy summary
• Erbitux + RT demonstrated significant efficacy benefits over
RT alone
– 20-month increase in median survival
– 26% reduction in risk of death
– 10-month increase in median locoregional control
– 32% reduction in locoregional relapse
Bonner J, et al. N Engl J Med 2006;354:567–578

Frecuencia
Efecto adverso
>10% - Hipomagnesemia- Aumento en los niveles de enzimas hepáticas- Reacciones cutáneas - Reacciones leves o moderadas en la perfusión
1-10% - Deshidratación- Hipocalcemia- Cefalea- Conjuntivitis- Diarrea, náuseas, vómitos, anorexia.- Reacciones graves relacionadas con la perfusión. - Cansancio
<1% - Blefaritis, queratitis. - TVP, TEP.
Toxicidad por anti EGFR Toxicidad por anti EGFR monoclonal antibodiesmonoclonal antibodies

Grado Lesión Extensión
Síntomas AVD Infección
Grado 1 pápulas / pústulas
<10% +/- prurito / hiperestesia
Grado 2 pápulas / pústulas
10-30% +/- prurito / hiperestesia
Dificulta instrumentale
s
Grado 3 pápulas / pústulas
>30% +/- prurito / hiperestesia
Dificulta básicas
Local: atb tópicos
Grado 4 pápulas / pústulas
cualquiera
+/- prurito / hiperestesia
Extendida: atb iv

2
3
1
ERUPCIÓN CUTÁNEA ACNEIFORME

• Desde una semana antes y durante el tto:
– Lavado diario con agua tibia (no caliente).– Evitar irritantes: NO jabones, perfumes, desodorantes,
lociones con alcohol.– SÍ: geles de ducha basados en aceites / avena.– Uso diario de cremas hidratantes (prevención
sequedad). NO aloe vera.– Evitar:
• Exposiciones al sol (hasta 3 meses después del tto).• Afeitado con navaja (maquinilla eléctrica).• Tintes de cabello con amoniaco.



CONCLUSIONES I
• EGFR juega un papel importante en la regulación de múltiples mecanismos de subsistencia tumoral y su expresión esta asociada con un peor pronóstico.
• En CCR avanzado se ha demostrado el beneficio de los anticuerpos monoclonales Cetuximab y Panitumumab en pacientes KRAS wt ( factor predictivo).
• Es de practica clínica habitual la determinación del estado de KRAS en pacientes con CCR avanzado.

CONCLUSIONES II
• En carcinoma de cabeza y cuello avanzado se ha demostrado la eficacia del Cetuximab en regímes basados en platino. No existe marcador predictivo de respuesta.
• El rush acneiforme es una toxicidad característica de estoa agentes y en CCR avanzado se asocia a mayor beneficio clínico.
• Un manejo adecuado de las toxicidades permite menos interrupciones en el tratamiento.

MUCHAS GRACIAS!
Top Related