
Skull Base Tumors Involving the Orbit
54
Skull Base Tumors Involving the Orbit Donald J. Annino, Jr, MD, DMD a a
Transcript of Skull Base Tumors Involving the Orbit
Skull Base Tumors Involving the Orbit
Donald J. Annino, Jr, MD, DMD
a a
Skull Base TumorsSkull Base Tumors
Challenging to treatChallenging to treatRareRareMultiple Multiple histologieshistologiesComplex anatomyComplex anatomy
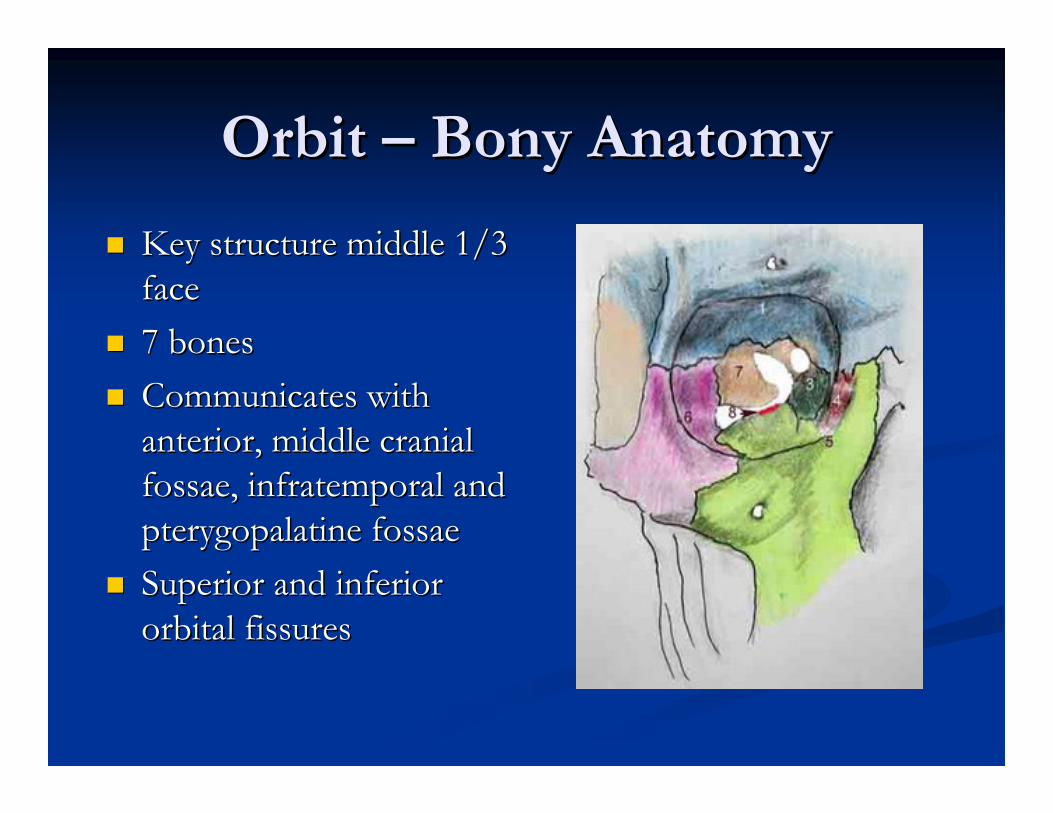
Orbit Orbit –– Bony AnatomyBony Anatomy
Key structure middle 1/3 Key structure middle 1/3 faceface7 bones7 bonesCommunicates with Communicates with anterior, middle cranial anterior, middle cranial fossae, infratemporal and fossae, infratemporal and pterygopalatine fossaepterygopalatine fossaeSuperior and inferior Superior and inferior orbital fissuresorbital fissures
Skull Base Tumors Involving Skull Base Tumors Involving the Orbitthe Orbit
Primary Primary Secondary Secondary MetastaticMetastatic
Primary Orbital TumorsPrimary Orbital Tumors
Benign Benign --InflammatoryInflammatoryVascular Vascular ––Cavernous Cavernous hemangiomashemangiomasNerve sheathNerve sheathBonyBonyLymphangiomaLymphangioma
Primary MalignantPrimary Malignant
Lacrimal glandLacrimal gland50 % malignant50 % malignantACC, malignant ACC, malignant mixedmixed
Lacrimal sacLacrimal sacOsteosarcoma Osteosarcoma –– after after retinoblastomaretinoblastomaRhabdomyosarcomaRhabdomyosarcoma
Secondary Orbital TumorsSecondary Orbital Tumors
Paranasal sinusesParanasal sinusesIntracranialIntracranial
MeningiomasMeningiomas
SkinSkin
Paranasal SinusParanasal Sinus LesionsLesions
BenignBenignOsteomasOsteomasMucoceleMucocelePolypsPolyps
MalignantMalignantCarcinomaCarcinomaSarcomaSarcomaMucosal melanomaMucosal melanoma
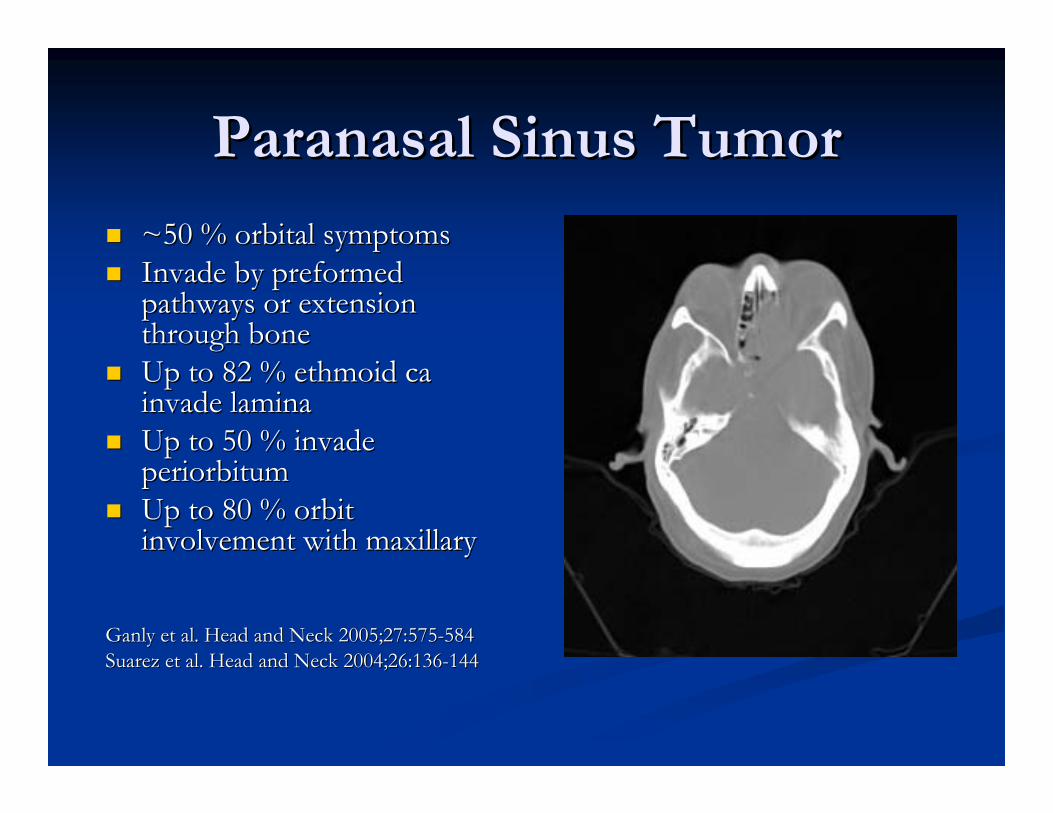
Paranasal Sinus TumorParanasal Sinus Tumor
~50 % orbital symptoms~50 % orbital symptomsInvade by preformed Invade by preformed pathways or extension pathways or extension through bonethrough boneUp to 82 % ethmoid ca Up to 82 % ethmoid ca invade laminainvade laminaUp to 50 % invade Up to 50 % invade periorbitumperiorbitumUp to 80 % orbit Up to 80 % orbit involvement with maxillaryinvolvement with maxillary
Ganly et al. Head and Neck 2005;27:575Ganly et al. Head and Neck 2005;27:575--584584Suarez et al. Head and Neck 2004;26:136Suarez et al. Head and Neck 2004;26:136--144144
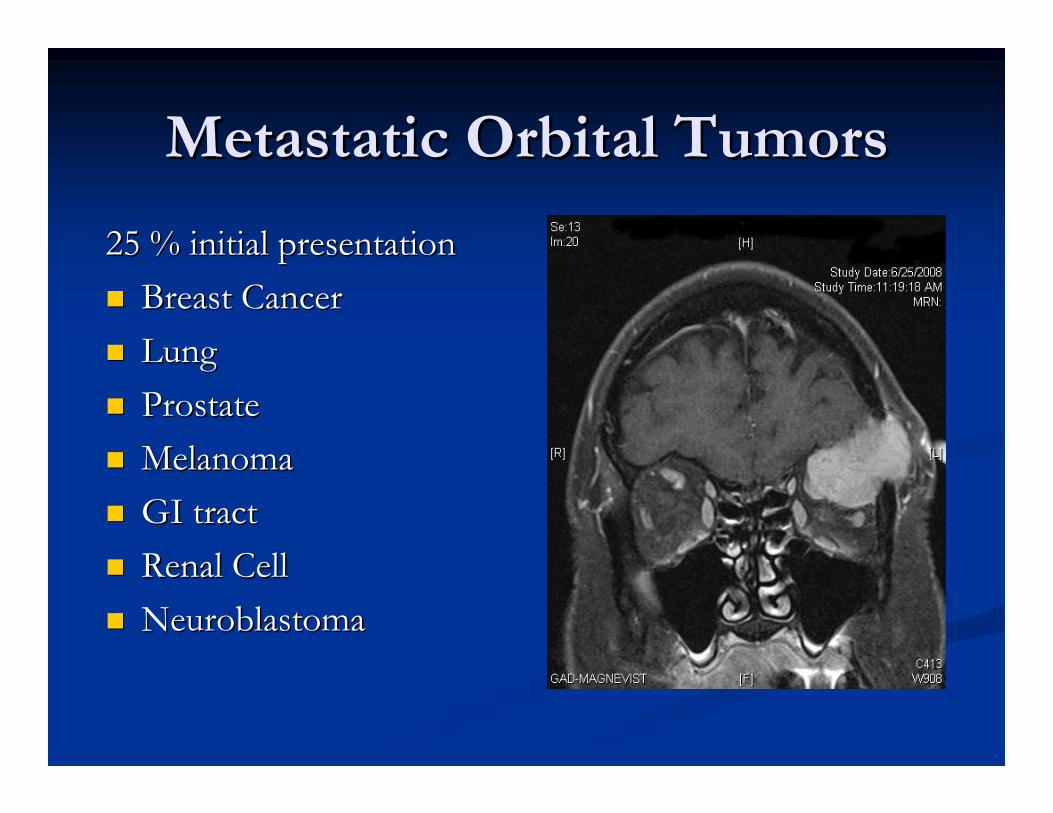
Metastatic Orbital TumorsMetastatic Orbital Tumors
25 % initial presentation25 % initial presentationBreast CancerBreast CancerLungLungProstateProstateMelanomaMelanomaGI tractGI tractRenal CellRenal CellNeuroblastomaNeuroblastoma
WorkWork--upup
CTCTBone detailBone detail
MRIMRISoft tissueSoft tissueIntracranialIntracranial
Ultrasound Ultrasound Ant, middle orbitAnt, middle orbit
MRAMRA

WorkWork--upup
BiopsyBiopsyFNAFNAOpenOpen
Skull Base Tumors TreatmentSkull Base Tumors Treatment
SinonasalSinonasal outcomes improving over 4 outcomes improving over 4 decadesdecadesImproved surgical techniquesImproved surgical techniquesConformal radiation Conformal radiation
Skull Base Tumors TreatmentSkull Base Tumors Treatment
Multimodality therapyMultimodality therapySurgerySurgeryRadiation Radiation ChemotherapyChemotherapy
Minimize morbidity and maximize quality Minimize morbidity and maximize quality of life of life
Orbital TumorsOrbital Tumors
OphthalmologistOphthalmologistHead and Neck SurgeonsHead and Neck SurgeonsNeurosurgeonsNeurosurgeons
Skull Base TumorSkull Base Tumor
Contraindications for surgeryContraindications for surgeryBrain involvementBrain involvementCavernous sinus extensionCavernous sinus extensionInternal carotid involvementInternal carotid involvement
Secondary Orbital TumorsSecondary Orbital Tumors
Survival not changed with invasion limited Survival not changed with invasion limited to periorbitato periorbitaSurvival impacted withSurvival impacted with
Brain Involvement Brain Involvement –– duraldural invasioninvasionHistologyHistologyOrbital soft tissue involvementOrbital soft tissue involvement
Suarez et al. Head Neck 2004:26:136Suarez et al. Head Neck 2004:26:136--144144Ganly et al. Head Neck 2005:27:575Ganly et al. Head Neck 2005:27:575--584584Howard et al. Head Neck 2006:28:867Howard et al. Head Neck 2006:28:867--873873
Periorbitum InvolvementPeriorbitum Involvement
CT & MRI not accurateCT & MRI not accurateDirect observation in OR and frozen Direct observation in OR and frozen sectionsection
Imola, Schramm. Laryngoscope 2002;112:1357Imola, Schramm. Laryngoscope 2002;112:1357--13651365
Indications for ExenterationIndications for Exenteration
Extension through the Extension through the periorbitumperiorbitumPeriorbitum not violated Periorbitum not violated but involved then orbit but involved then orbit contents preservedcontents preservedViolation of bone alone Violation of bone alone not indication for not indication for exenterationexenterationSurvival not improved Survival not improved with orbital with orbital exenterationexenteration/clearance/clearance
Suarez et al. Head and Neck 2008;30:242Suarez et al. Head and Neck 2008;30:242--250250Imola, Schramm. Laryngoscope 2002;112:1357Imola, Schramm. Laryngoscope 2002;112:1357--
13651365
Surgical ApproachesSurgical Approaches
LocationLocationSizeSizeGoal Goal ––
BiopsyBiopsyDebulkingDebulkingTotal excisionTotal excision

Surgical ApproachesSurgical Approaches
Transorbital Transorbital ––OrbitotomyOrbitotomy
Extraorbital Extraorbital ––EndoscopicEndoscopicAnterior Approaches Anterior Approaches ––
Subcranial, frontalSubcranial, frontalLateral Approaches Lateral Approaches ––
Frontotemporal, frontoorbitotemporal craniotomyFrontotemporal, frontoorbitotemporal craniotomyCombinedCombined
Transorbital ApproachesTransorbital Approaches
Anterior lesionsAnterior lesionsNo extension to No extension to the orbital apexthe orbital apexCan be combined Can be combined with extraorbital with extraorbital approachesapproaches
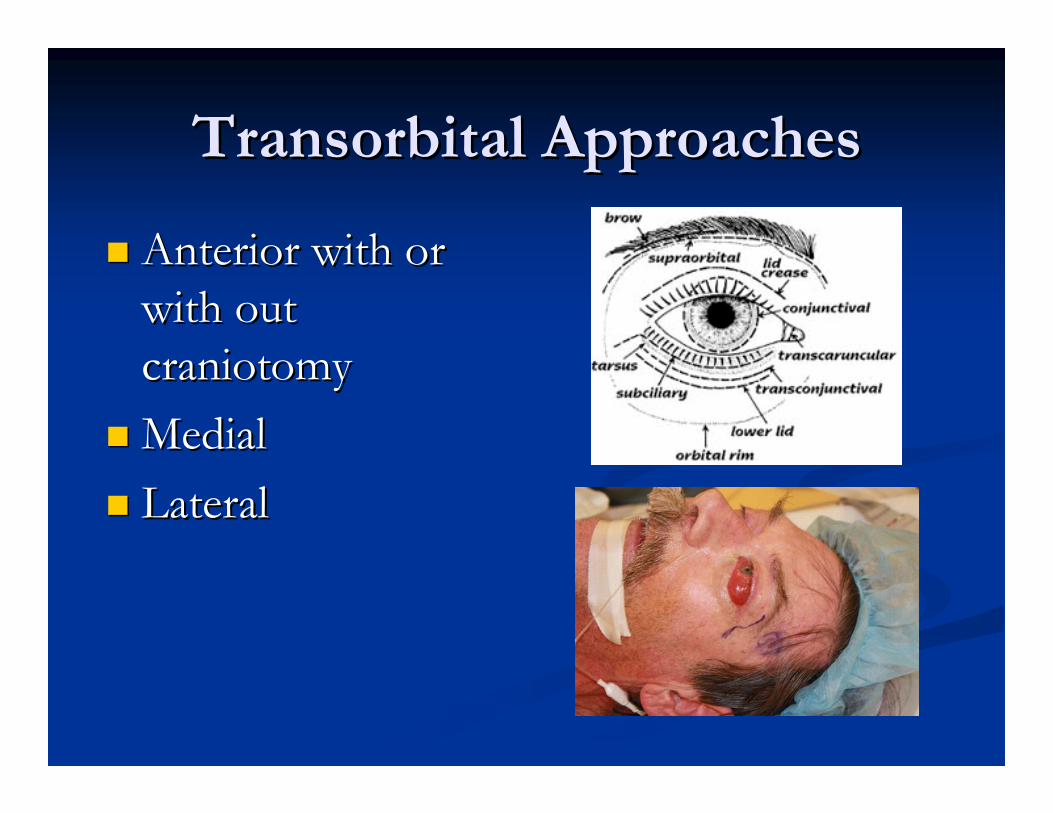
Transorbital ApproachesTransorbital Approaches
Anterior with or Anterior with or with out with out craniotomycraniotomyMedial Medial LateralLateral
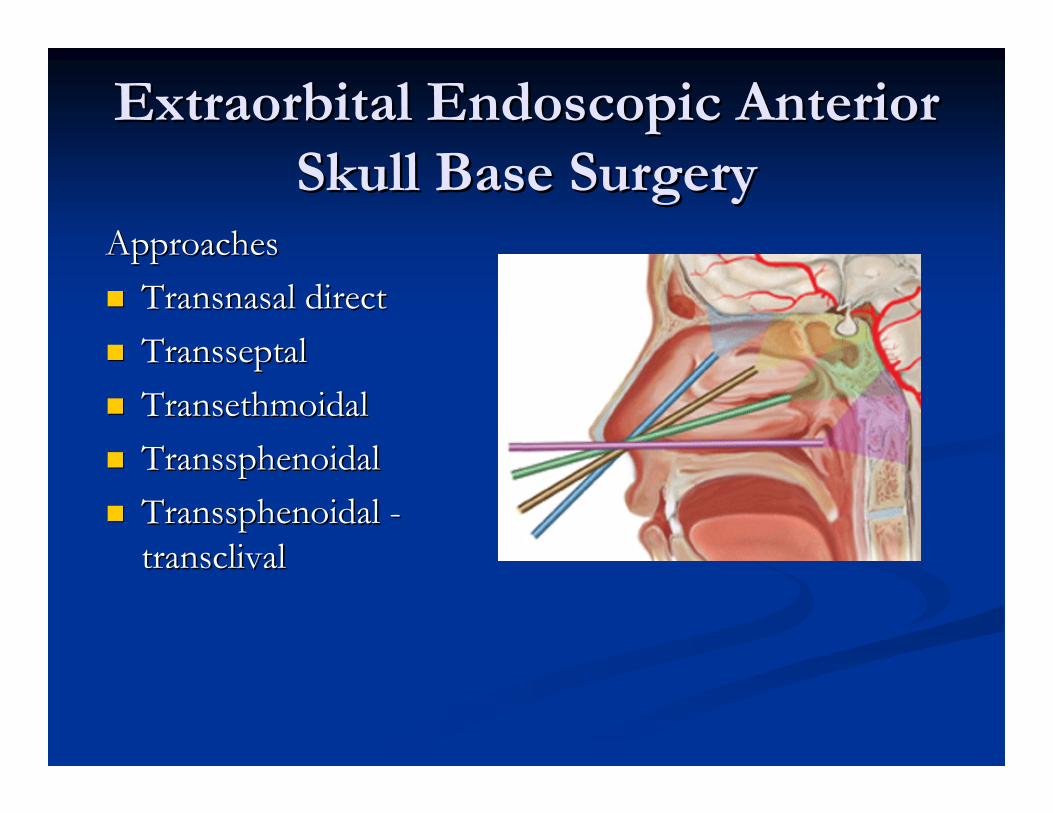
ExtraorbitalExtraorbital Endoscopic Anterior Endoscopic Anterior Skull Base SurgerySkull Base Surgery
ApproachesApproachesTransnasal directTransnasal directTransseptalTransseptalTransethmoidalTransethmoidalTranssphenoidalTranssphenoidalTranssphenoidalTranssphenoidal --transclivaltransclival
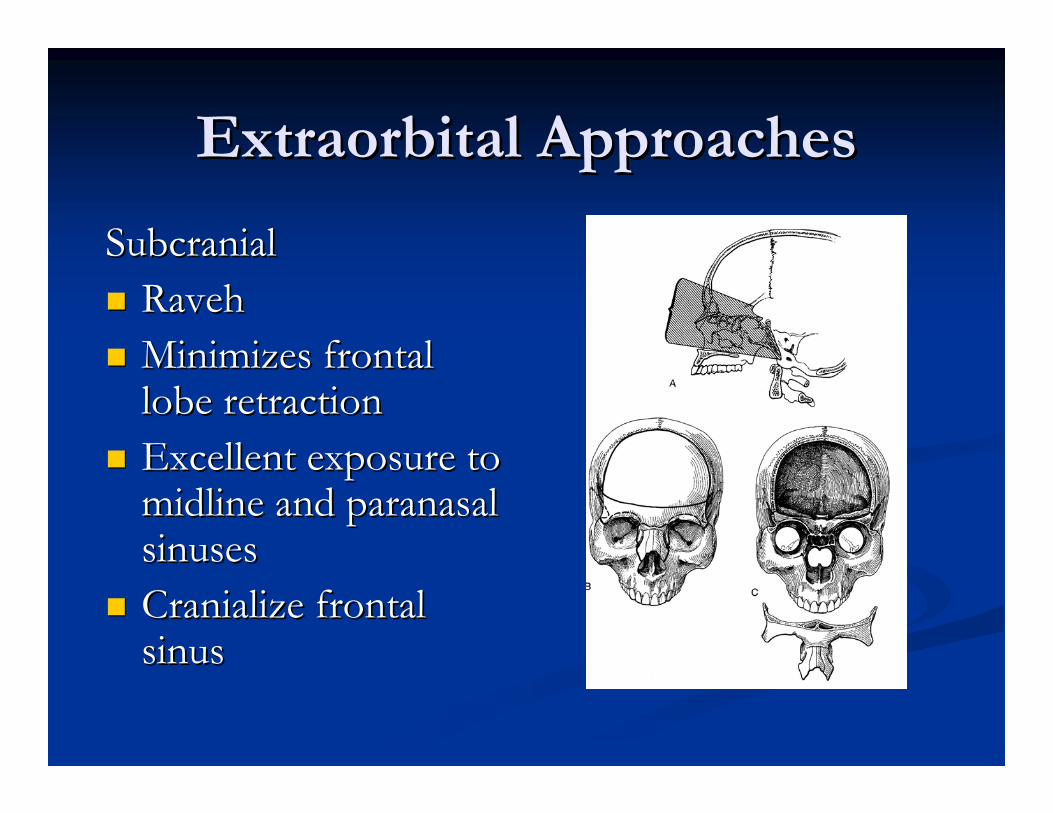
Extraorbital ApproachesExtraorbital Approaches
SubcranialSubcranialRavehRavehMinimizes frontal Minimizes frontal lobe retractionlobe retractionExcellent exposure to Excellent exposure to midline and paranasal midline and paranasal sinusessinusesCranialize frontal Cranialize frontal sinussinus
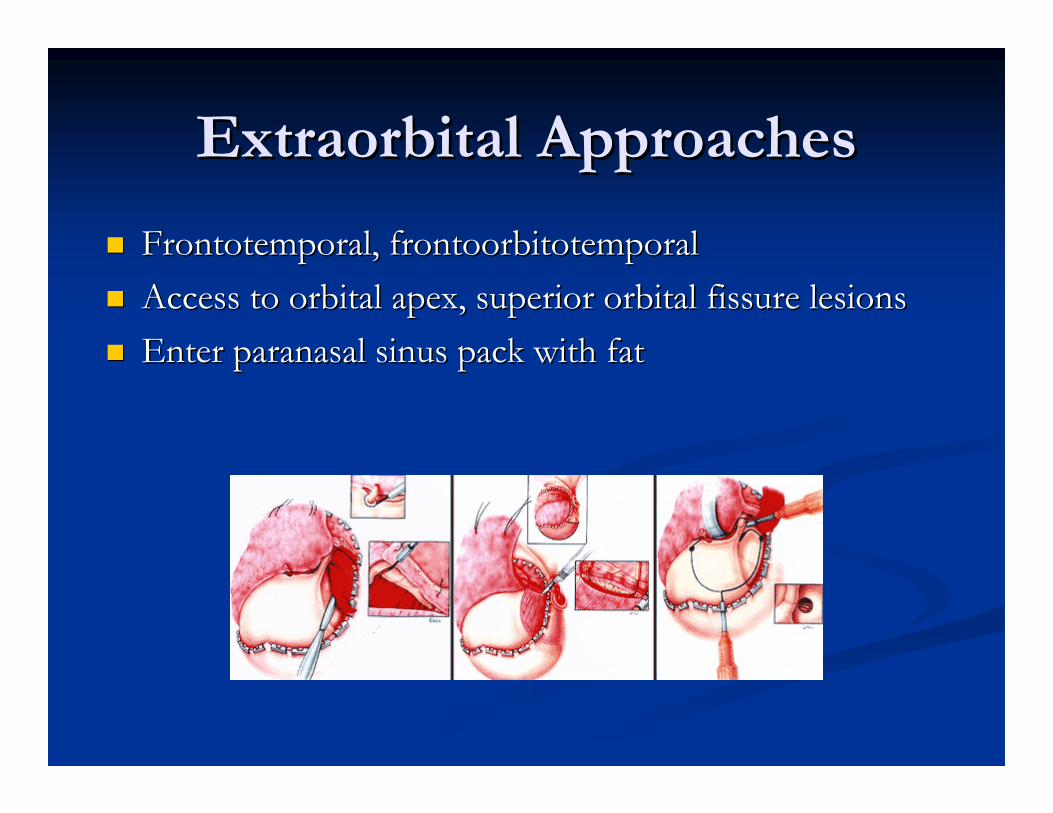
Extraorbital ApproachesExtraorbital Approaches
Frontotemporal, frontoorbitotemporalFrontotemporal, frontoorbitotemporalAccess to orbital apex, superior orbital fissure lesionsAccess to orbital apex, superior orbital fissure lesionsEnter paranasal sinus pack with fatEnter paranasal sinus pack with fat
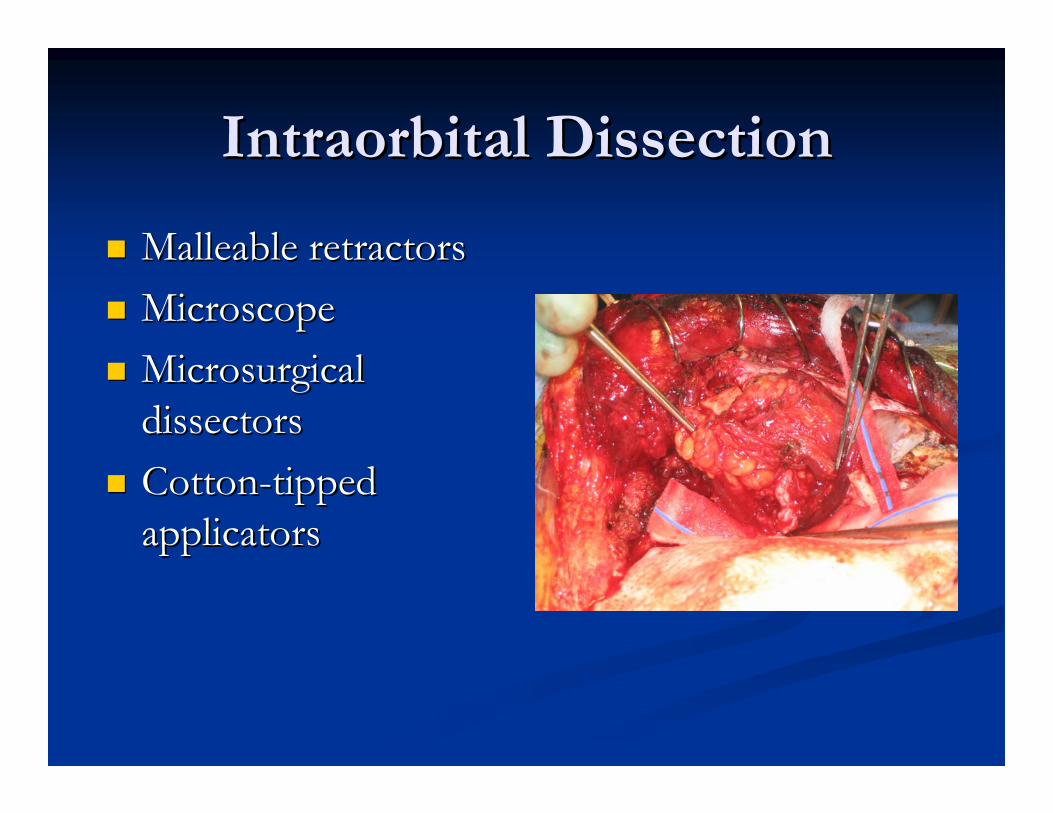
Intraorbital DissectionIntraorbital Dissection
Malleable retractorsMalleable retractorsMicroscopeMicroscopeMicrosurgical Microsurgical dissectorsdissectorsCottonCotton--tipped tipped applicatorsapplicators
Extraorbital ApproachesExtraorbital Approaches
Stereotactic Stereotactic navigationnavigation
ReconstructionReconstruction
Loss of multiple walls Loss of multiple walls –– rigid reconstructionrigid reconstructionLoss floor of floor greater 80%Loss floor of floor greater 80%Periorbita reconstructed with fascia, allodermPeriorbita reconstructed with fascia, allodermOrbital roof no reconstruction if aloneOrbital roof no reconstruction if alone
Pulsations short termPulsations short term
Watertight closure of duraWatertight closure of duraPericranial flapPericranial flap
ReconstructionReconstruction
Epiphora Epiphora -- 36 %36 %Silastic stenting Silastic stenting ––13%13%
Anderson et al. Otolaryngol Head and Anderson et al. Otolaryngol Head and Neck Surg 1996;122:1305Neck Surg 1996;122:1305--13071307
Imola, Schramm. Laryngoscope Imola, Schramm. Laryngoscope 2002;112:13572002;112:1357--13651365
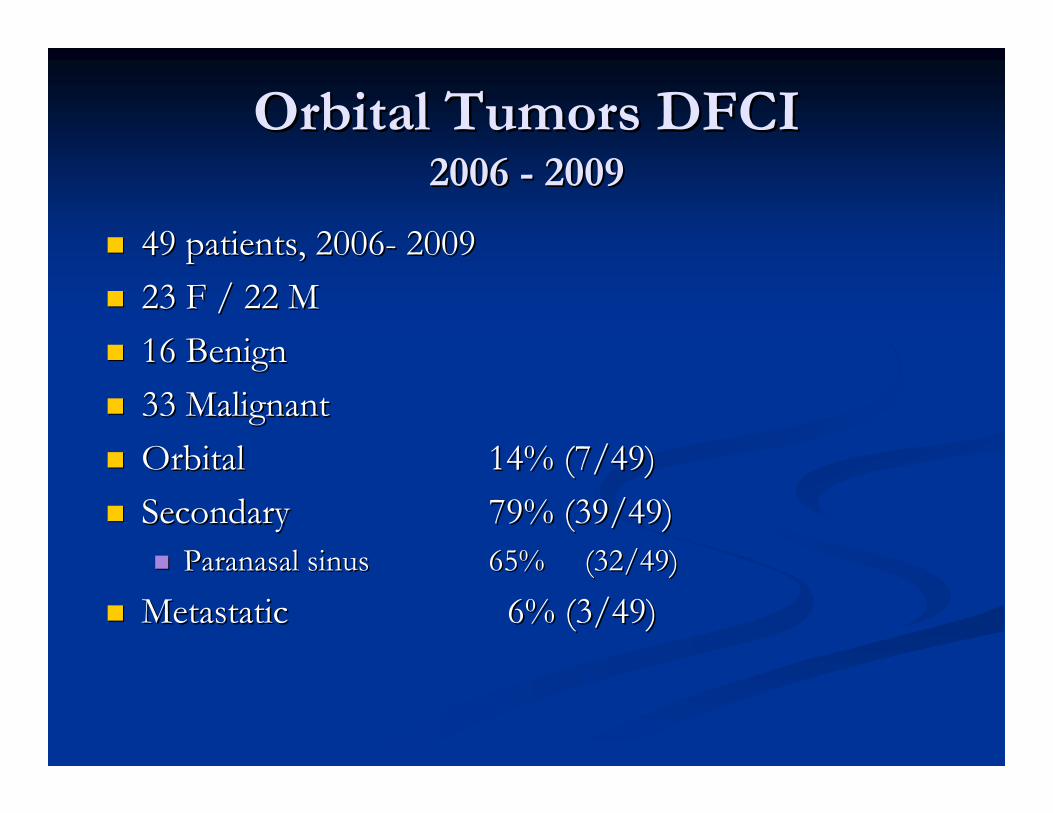
Orbital Tumors DFCIOrbital Tumors DFCI2006 2006 -- 20092009
49 patients, 200649 patients, 2006-- 2009200923 F / 22 M 23 F / 22 M 16 Benign 16 Benign 33 Malignant33 MalignantOrbital Orbital 14% (7/49)14% (7/49)SecondarySecondary 79% (39/49)79% (39/49)
Paranasal sinus Paranasal sinus 65%65% (32/49)(32/49)
MetastaticMetastatic 6% (3/49)6% (3/49)
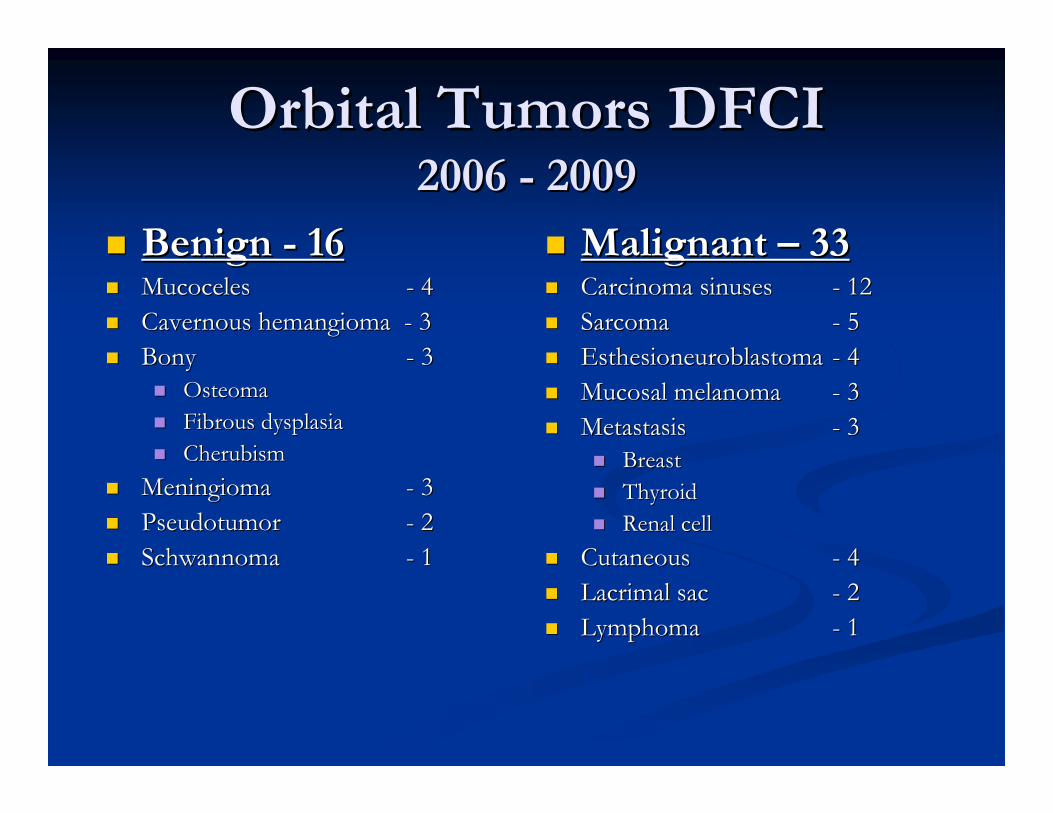
Orbital Tumors DFCIOrbital Tumors DFCI2006 2006 -- 20092009
Benign Benign -- 1616MucocelesMucoceles -- 4 4 Cavernous hemangioma Cavernous hemangioma -- 33BonyBony -- 33
OsteomaOsteomaFibrous dysplasiaFibrous dysplasiaCherubismCherubism
MeningiomaMeningioma -- 33PseudotumorPseudotumor -- 22SchwannomaSchwannoma -- 11
Malignant Malignant –– 33 33 Carcinoma sinusesCarcinoma sinuses -- 12 12 SarcomaSarcoma -- 55EsthesioneuroblastomaEsthesioneuroblastoma -- 44Mucosal melanomaMucosal melanoma -- 3 3 MetastasisMetastasis -- 33
BreastBreastThyroidThyroidRenal cellRenal cell
CutaneousCutaneous -- 44Lacrimal sacLacrimal sac -- 22LymphomaLymphoma -- 11
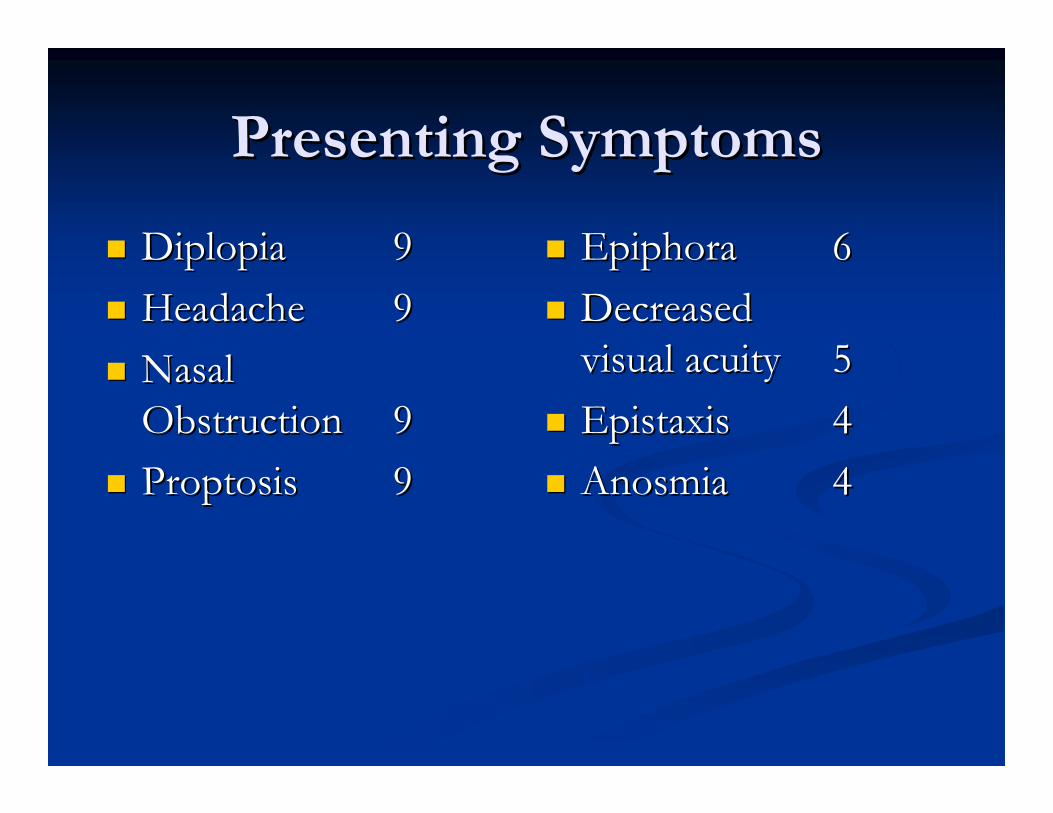
Presenting SymptomsPresenting Symptoms
DiplopiaDiplopia 99HeadacheHeadache 99Nasal Nasal ObstructionObstruction 99ProptosisProptosis 99
EpiphoraEpiphora 66Decreased Decreased visual acuityvisual acuity 55EpistaxisEpistaxis 44AnosmiaAnosmia 44
Initial DiagnosisInitial Diagnosis
47 % (23/49) previous procedures 47 % (23/49) previous procedures SinusitisSinusitis 1919MigraineMigraine 44
Surgical ApproachesSurgical Approaches
TransorbitalTransorbital 66SubcranialSubcranial 1616
w/ exenterationw/ exenteration 22FrontotemporalFrontotemporal 88Maxillectomy Maxillectomy 1111
w/ exenterationw/ exenteration 44EndoscopyEndoscopy 88
Surgical ApproachesSurgical Approaches
Facial incisions avoided except in Facial incisions avoided except in transorbital, maxillectomy w/o intracranial transorbital, maxillectomy w/o intracranial extension and exenterationextension and exenterationEndoscopic assisted Endoscopic assisted
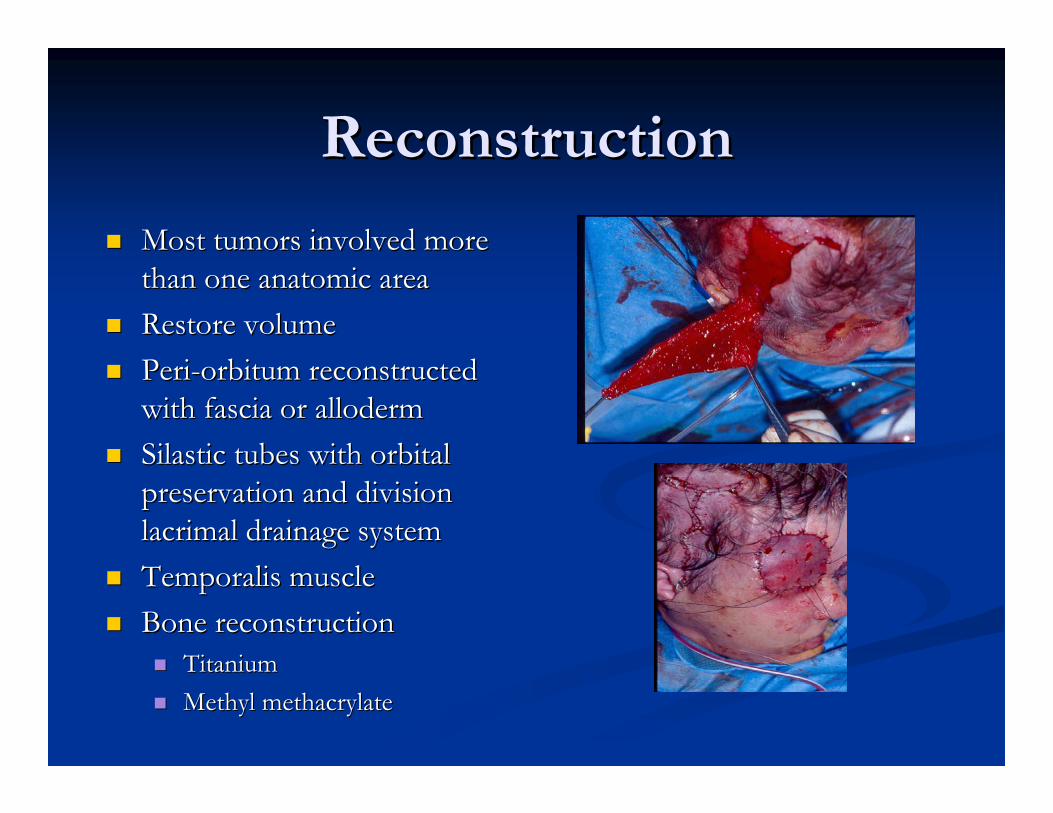
ReconstructionReconstruction
Most tumors involved more Most tumors involved more than one anatomic areathan one anatomic areaRestore volumeRestore volumePeriPeri--orbitum reconstructed orbitum reconstructed with fascia or allodermwith fascia or allodermSilastic tubes with orbital Silastic tubes with orbital preservation and division preservation and division lacrimal drainage systemlacrimal drainage systemTemporalis muscleTemporalis muscleBone reconstruction Bone reconstruction
TitaniumTitaniumMethyl methacrylateMethyl methacrylate
OutcomesOutcomes
6 patients with intraconal dissection6 patients with intraconal dissection2 Patients decreased VA (excludes exenteration)2 Patients decreased VA (excludes exenteration)
Pseudotumor VA 20/100 to NLPPseudotumor VA 20/100 to NLPMeningioma VA hand motion no change but decreased visual Meningioma VA hand motion no change but decreased visual fieldfield
1 Patient improved VA1 Patient improved VASchwannoma 20/300 to 20/70Schwannoma 20/300 to 20/70
Diplopia Diplopia Improved 6 postImproved 6 post--opop2 post2 post--op, 1 short term, 1 persists in upward gazeop, 1 short term, 1 persists in upward gaze
OutcomesOutcomes
EnophthalmosEnophthalmos2 patients2 patients3 walls resected3 walls resected
PtosisPtosis3 patients3 patients
Epiphora Epiphora –– 00Lower lid ectropian Lower lid ectropian –– 00Orbital pulsations selfOrbital pulsations self--limitedlimitedCSF CSF –– 00Cerebritis Cerebritis -- 11
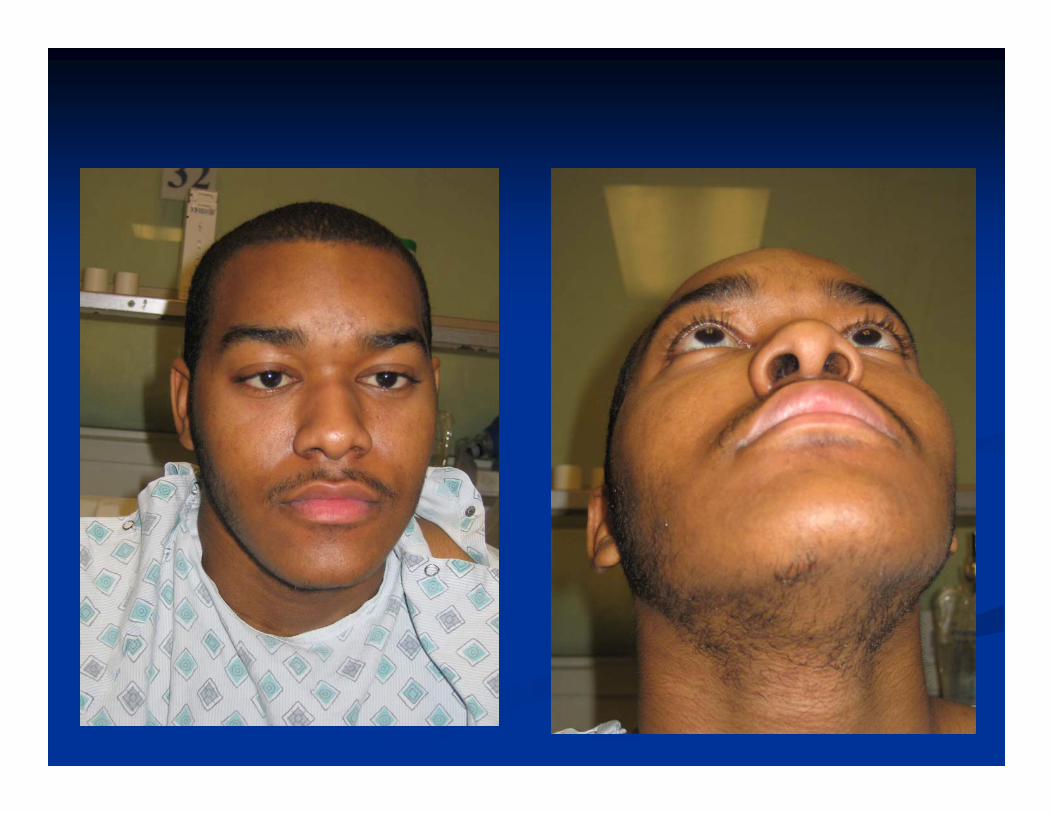
CaseCase
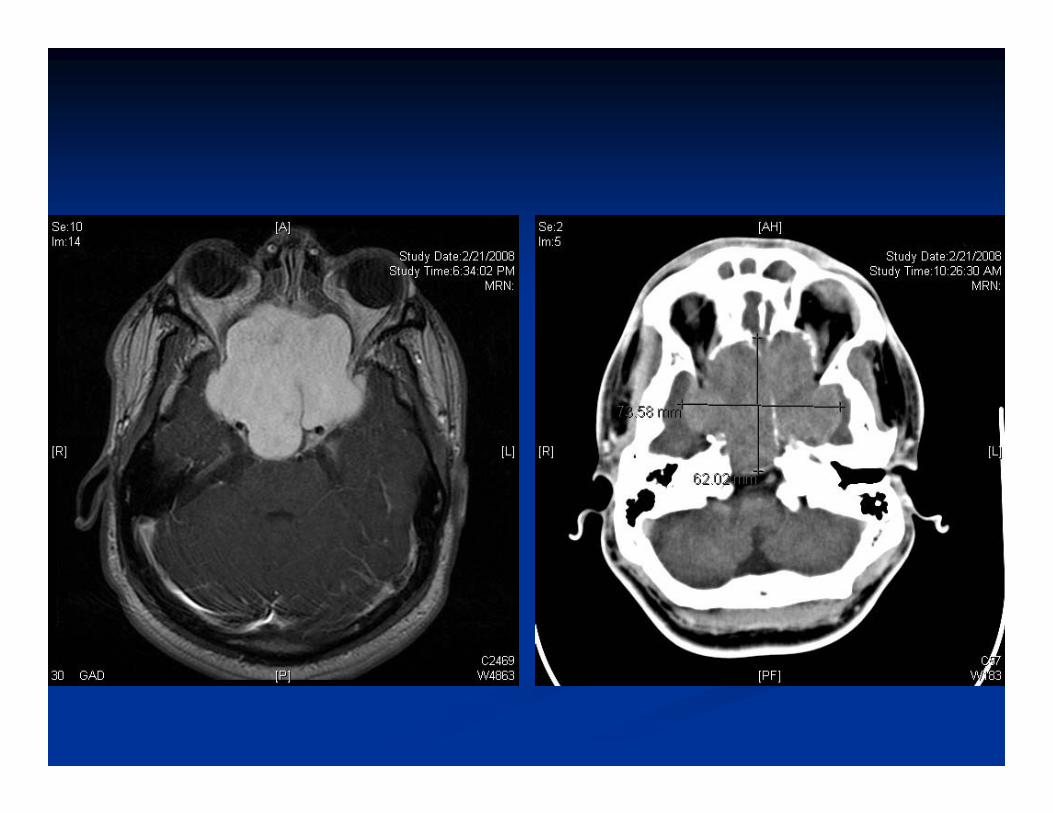
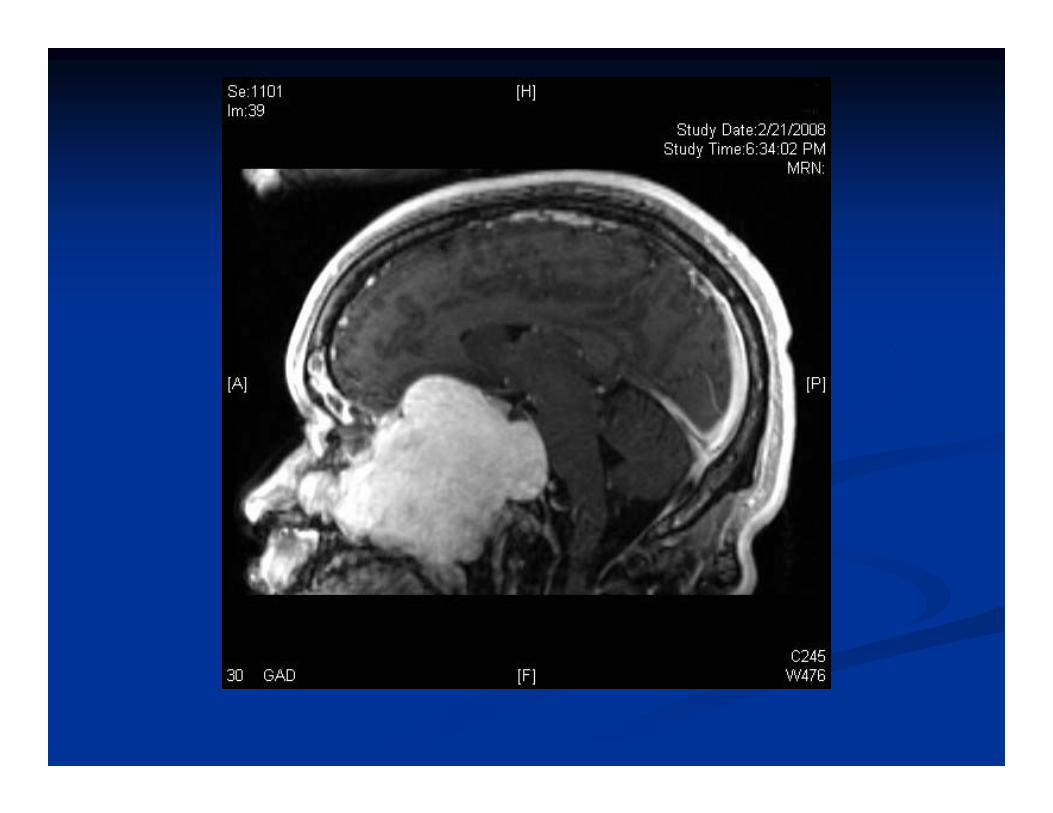
19 yo M19 yo M2 years sx2 years sxSnoring, nasal obstruction, proptosisSnoring, nasal obstruction, proptosisDx Dx –– allergiesallergiesOS OS –– 20/2520/25OD OD –– able to count fingersable to count fingers
CaseCase
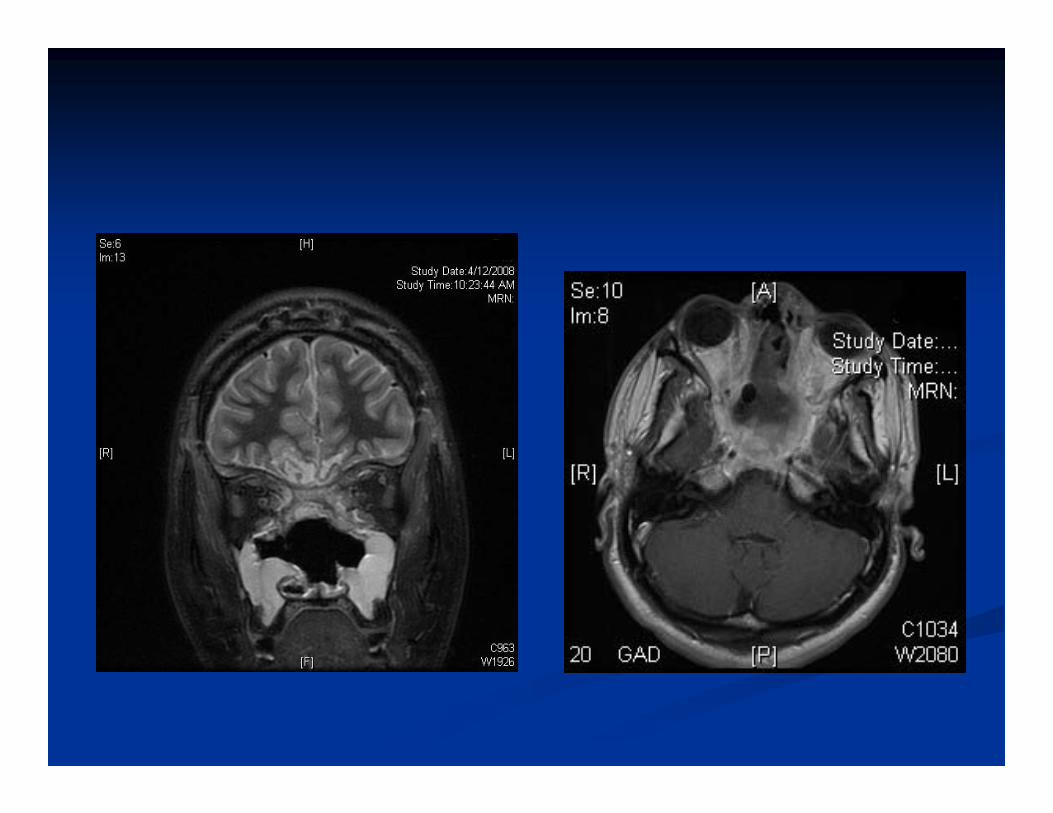
MRI, CT MRI, CT ––Large destructive lesion involving paranasal Large destructive lesion involving paranasal sinuses, bilat orbits, anterior cranial fossa, sinuses, bilat orbits, anterior cranial fossa, middle cranial fossa, extends through clivusmiddle cranial fossa, extends through clivus
CaseCase
Endoscopic biopsyEndoscopic biopsyPath Path –– Intermediate Intermediate chondosarcomachondosarcoma
CaseCase
Subcranial approachSubcranial approachEndoscopic assisted Endoscopic assisted Complete gross removalComplete gross removal

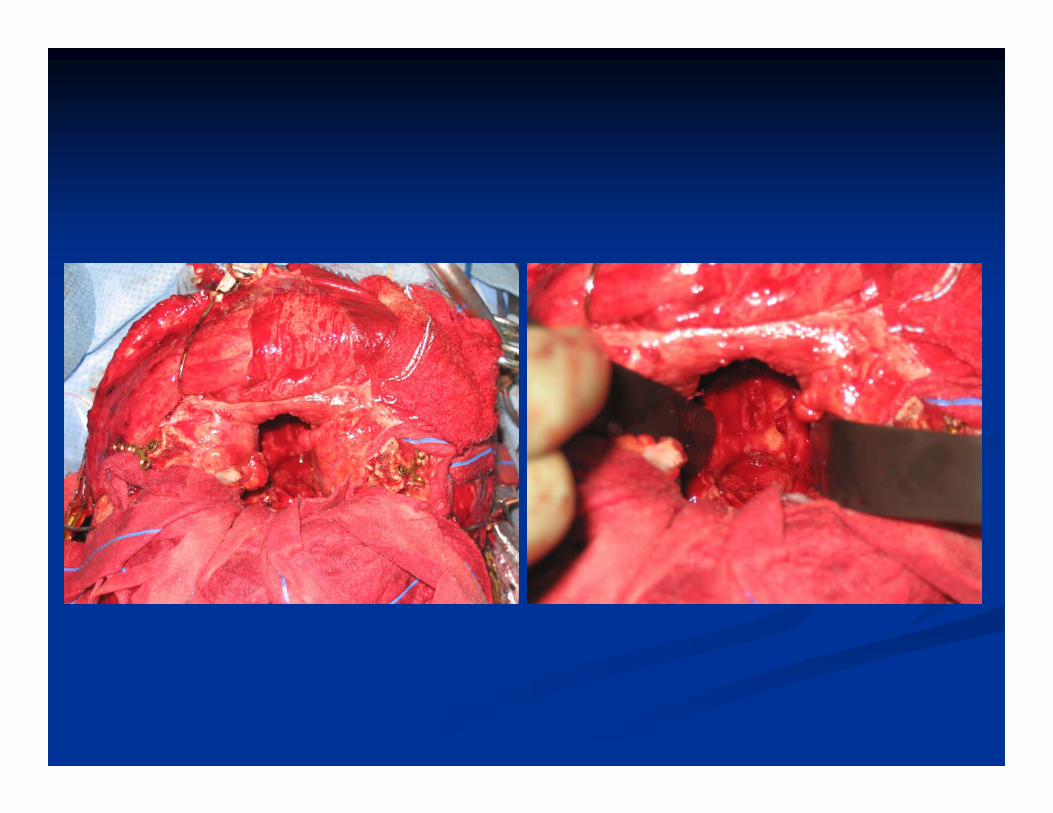
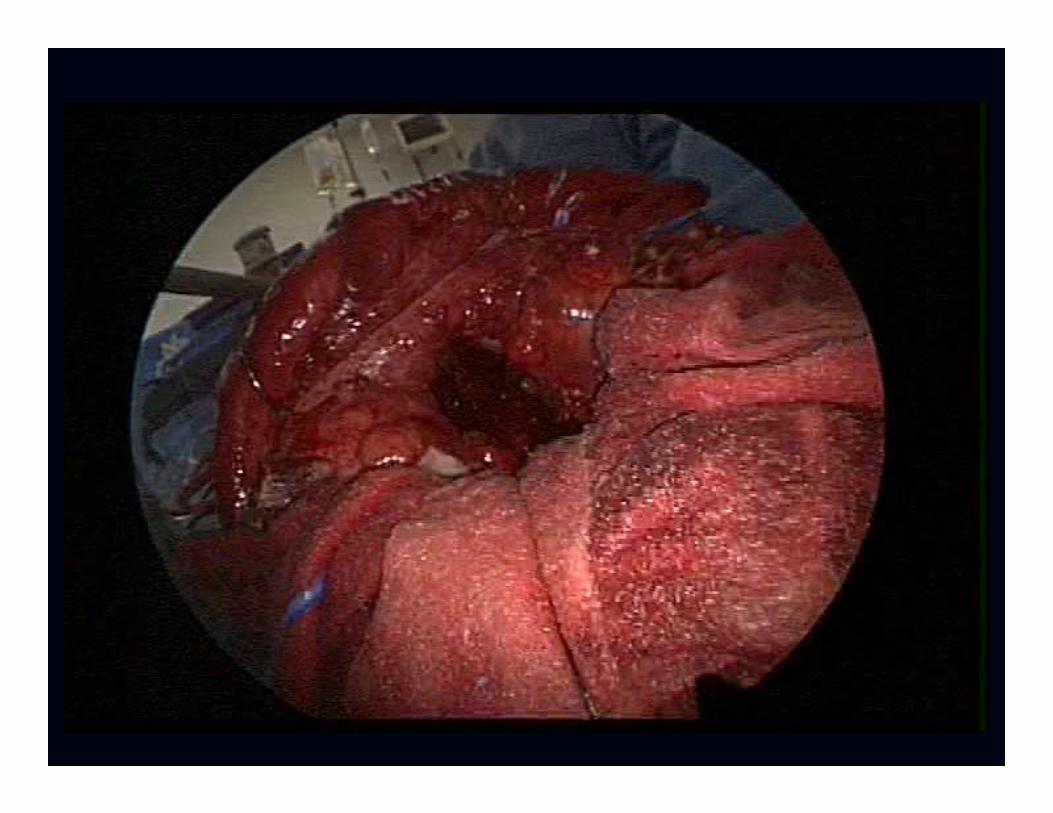
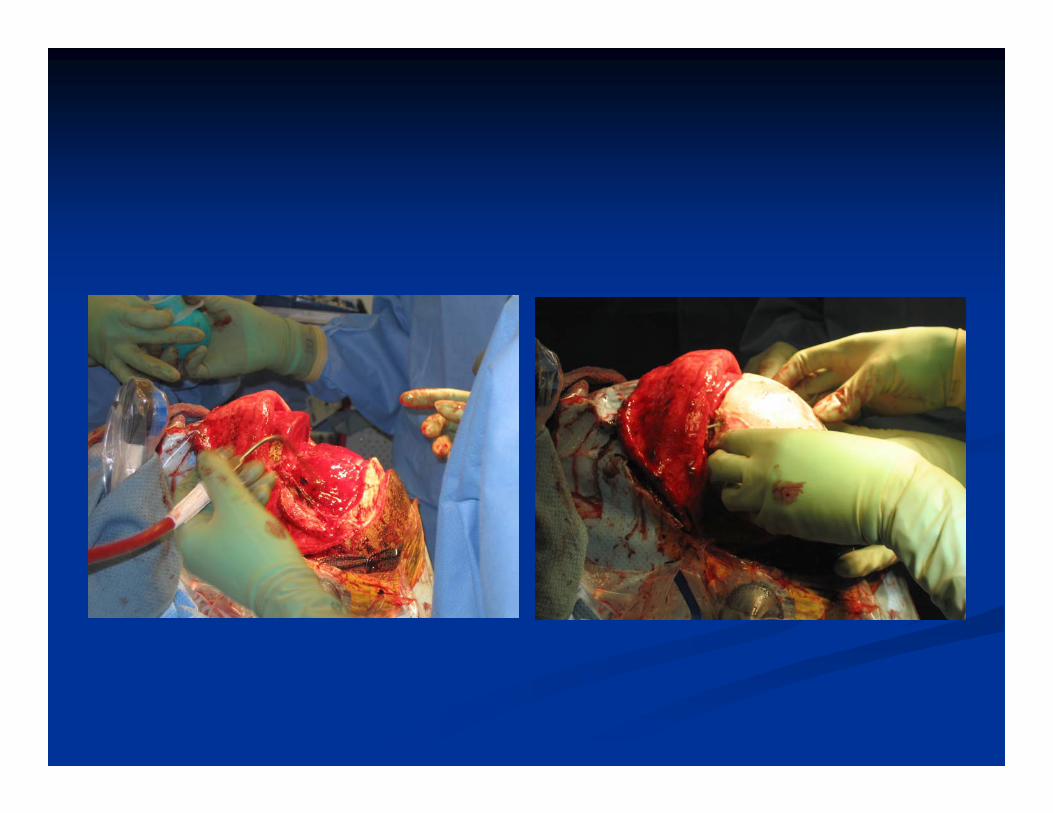
CaseCase
No complicationsNo complicationsVision unchangedVision unchangedPostPost--op proton beamop proton beam

ConclusionConclusion
TumorsTumors involving the orbit require involving the orbit require multidisciplinary approachmultidisciplinary approachVaried histologyVaried histologySafe, good outcomes with proper planning Safe, good outcomes with proper planning and approachand approach


















