Presentation ALOV
17
Loss of Vision Opthalmology Presentation : Painful Acute Loss of Vision 1. Acute Closed Angle Glaucoma 2. Optic Neuritis 3.T emporal Arthritis (Giant Cell Arthritis) 4. Anterior Ischaemic Optic Neuropathy 5. T rauma
-
Upload
norzahidah-mohd-khair -
Category
Documents
-
view
222 -
download
0
Transcript of Presentation ALOV

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 1/17
Loss of VisionOpthalmology Presentation :
Painful Acute Loss of Vision1. Acute Closed Angle Glaucoma
2. Optic Neuritis
3.T emporal Arthritis (Giant Cell Arthritis)
4. Anterior Ischaemic Optic Neuropathy
5. T rauma

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 2/17
Acute Closed Angle Glaucoma
- typically pr imary glaucoma
Pathogenesis :- Sudden obstruction of drainage angle by per ipher al ir is- The aqueous flow f r om poster ior to anter ior chamber impaired- There is no dr ainage of aqueous thr ough tr abecular meshwork
R Increase in Intraocular Pressure
- Contact of per ipher al ir is eventually may causes adhesionR Peripheral Anterior Synechiae
Risk factors:- Age : Aver age age 60 year s old- Female : Male = 4 : 1
- More common in South East Asians- Increased r isk in 1st degree relative

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 3/17
Risk factors:- Age : Aver age age 60 year s old- Female : Male = 4 : 1- More common in South East Asians- Increased r isk in 1st degree relative
Anatomical predisposing factors:- Lens size increase thr oughout lif e, gr owth br ings anter ior sur face to the cor nea- Small cor nea diameter usually smaller about 0.25mm comparedto nor mal- Short axial length lens located more anter ior ly

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 4/17
Symptoms- Severe pain- Photophobia- Loss of vision- Coloured haloes- Nausea + Vomiting
- Previous symptoms of attack (subacute)
Signs- Decreased vision- Cloudy cor nea- Oval, non-reactive pupil- Loss of red reflex
- Ciliary injection- Increased Intr aocular pressure

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 5/17
Investigations
- Fundoscopy- Increase Cup : Disc r atio- Thinning of neur oretinal r im- DOES NOT RULE OUT
- Tonometry- Intr aocular Pressure Measurement : Pressure > 20
- Gonioscopy - gain a view of the anatomical angle for med between the eyes cor nea andir is
- help distinguish open and closed angle

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 6/17
Management :
- Reduce the intr aocular pressure- IV Acetazolamide 500mg ; Or al Acetazolamide 500mg 4x/daily
- Rever se pupil block
- Topical Pilocarpine 2% (every 15 minutes for 1 hour followed by every hour for 4 hour)
- Prevent recurrence- Laser ir idotomy

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 7/17
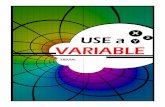
Glaucoma eye

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 8/17
Optic Neuritis
Aetiology Classification:- Demyelinating : Nerve fibres lose their myelin layer, most common
cause. E.g Multiple Sclerosis
- Infectious : Sinus related, Cat-scratch fever, Syphilis (1* or 2*
Stage), Lyme disease(spirochete infection), Cryptococcal Meningitis (in
patient with AIDS)
- Parainfectious : Measles, Mumps- Non-infectious : Sarcoid, Autoimmune
Opthalmoscopic Classification:
- Retrobulbar neuritis : optic disc appearance normal, optic nerve head
not involved. Frequent in Multiple Sclerosis
- Papillitis : Optic nerve head affected primarily or secondarily due to
retinal inflammation.
- Neuroretinitis : Characterized by papillitis in association with
inflammation of retinal nerve fibre layer and macular star figure

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 9/17
Presentation:
- in age between 20 and 50 (mean ar ound 30 y/o)- vision wor sens over sever al days recover ar ound 2-4 weeks
Symptoms :- pain in or ar ound eye, exacerbated on eye movement (especially retr obulbar neur itis)- Acute loss of vision, that lasts a f ew days
- Tiny white or coloured flashes/sparkles- Fr ontal headache- Tender ness of the globe
Signs :- Reduce visual acuity- Reduced colour vision
- Other signs of optic disc dysfunction. E.g Impair ment of contr ast sensitivity, aff erent pupillary def ect.- Swollen disc in papillitis , nor mal in retr obulbar neur itis- Centr al scotoma

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 10/17
Investigation :- MRI Identif y additional plaques of demyelination
Treatment :- IV Methylprednisolone sodium succinate 1g daily for 3 days, followed by or alprednisolone 1mg/kg/day for 11 days

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 11/17
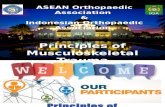
Macular star in Optic neur itis

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 12/17
Anter ior Ischaemic Optic Neur opathy ( AION)
- 2 types : Arter itic and Non Arter itic- Arter itic AION can be caused by Giant Cell Arter itis (GCA)
Pathogenesis :- Degener ative vaso-occlusive or vasculitis disease of the arter iolescauses poster ior cilliary vessels become compr omised.
- Leads to sudden decrease in blood supply to the optic nerve head that result in anter ior ischaemic optic neur opathy
Giant Cell Arteritis:- Autoimmune vasculitis occurr ing in patient aged over 60- Aff ect arter ies with inter nal elastic lamina- Presents with sudden loss of vision, tender scalp, pain on chewing,
shoulder pain, malaise

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 13/17
Symptoms :- Sudden, pr ofound unilater al loss of vision or visual field of ten onwaking up- Per iocular pain preceded by tr ansient flashing of light- Jaw claudication*- Headache of recent onset*- Scalp tender ness*
- Weight loss*
Signs :- Tender ness and loss of pulsation of one or both tempor al arter ies- Swollen Optic Disc with haemorrhage and cotton wool spots- Pale 'Chalky white' Disc- Relative Aff erent Pupil Def ect
Symptoms of GCA

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 14/17
Investigations :- ESR and CRP will be r aised- C-reactive pr otein- Tempor al artery biopsy- gr anulomatous inflammation
Treatment :- IV Methylprednisolone sodium succinate - 1g daily for 3 days and or al prednisolone 80mg daily- Or al dose reduced to 60mg af ter 3 days then 50mg for 1 week each

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 15/17
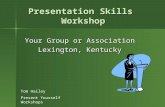
Pale, Oedematous Optic Disc

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 16/17
Non-Arteritic Anterior Ischaemic OpticNeropathy
- presented as sudden painless, monocular visual loss- common in patient ages of 55 to 70 y/o
- predisposing systemic conditions includes diabetes, hypertension, hyper cholester olaemia, antiphospholipid syndr ome- Investigations should be done :- Full blood count Exclude anaemia- Blood pressure check- Blood sugar check- ESR and C-Reactive pr otein to exclude Giant Cell (Tempor al) Arter itis

8/8/2019 Presentation ALOV
http://slidepdf.com/reader/full/presentation-alov 17/17
Trauma
Examples of traumaBlunt and penetrating trauma are both significant causes of visual loss.
1. Blunt trauma more common. E.g eye is struck with a finger, fist,tennis ball,or other solid object.R sudden compression and indentation of the globe that occurs at themoment of impact.Damages- Hyphema : Bleeding may occur in the front of the eye between the clear cornea and colored iris .- Damaged lens may turn cloudy, thus forming a cataract or displaced withinthe eye so that is can no longer focus a clear image.- Retinal damage result reduce of vision. A tear in the retina leads to a largeretinal detachment.- Late effect, becomes evident for months or years after the injury occurs.These late effects, including cataract, retinal detachment, or glaucoma
2. Penetrating trauma i.e eye pierced by a sharp object such as a knife, or by a
high-velocity missile such as BB pellet. Surgery is often needed to repair thedamage.Damages:- Intraocular infection may develop that can rapidly lead to permanent blindness in that eye.