PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN EL … · 2016-09-14 · leucemia aguda de...
25
LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN PACIENTE PLURIPATOLÓGICO SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA SÍNDROME ANTI-SINTETASA, UN DESAFÍO DIAGNÓSTICO AGOSTO 2016. Volumen 3 PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN EL SEDIMENTO DE ORINA DE UNA LACTANTE
Transcript of PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN EL … · 2016-09-14 · leucemia aguda de...

LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN PACIENTE PLURIPATOLÓGICO
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA SÍNDROME ANTI-SINTETASA, UN DESAFÍO DIAGNÓSTICO
AGOSTO 2016. Volumen 3
PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN EL SEDIMENTO DE ORINA DE UNA LACTANTE

Laboratory Medicine at a glance
Medicina de Laboratorio de un vistazo
VOL.3 ISSN 2444-8699
PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN
EL SEDIMENTO DE ORINA DE UNA LACTANTE
ATYPICAL CLUSTERS OF URIC ACID CRYSTALS IN THE
URINARY SEDIMENT FROM A BREASTFED BABY
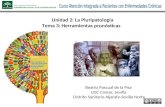
Figura 1. Sedimento de orina de la paciente (microscopía óptica de campo claro, 400x). Se muestran distintas imágenes de maclas atípicas compuestas de cristales de ácido úri-co (romboidales). Figure1. Urinary sediment of the patient (bright-field optical microscopy, 400x). Several images of atypical clusters of rhomboid uric acid crystals are shown.
Autores Iñaki Vallés Díez1
Blanca Acha Santamaría2
Naiara Tirapu Fernández de la
Cuesta1
Centro 1Servicio de Análisis Clínicos,
Hospital San Jorge (Huesca). 2Laboratorio Unificado,
Complejo Hospitalario de
Navarra (Pamplona).
Fecha de publicación 29 agosto 2016
Páginas Páginas 1-6

VOLUMEN 3 PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN
EL SEDIMENTO DE ORINA DE UNA LACTANTE 02
Laboratory Medicine at a glance
Presentamos dos fotografías del sedimento urina-
rio de una niña lactante de dos meses de vida. En la
primera imagen se observan varios cristales forman-
do maclas de morfología atípica (figura 1). La segun-
da imagen nos muestra la intensa birrefringencia que
adquieren dichas maclas cuando se observan en un
microscopio de luz polarizada (figura 2). Este hallaz-
go, junto con otros datos de laboratorio, sugiere que
las maclas están formadas por cristales de ácido úri-
co.
We report two photographs of the urinary sedi-
ment from a 2-month-old breastfed baby. In the first
image several atypical crystal clusters can be ob-
served (figure 1). Second image shows an intense
birefringence in the clusters, when observed in a po-
larized light microscope (figure 2). This finding, to-
gether with other laboratory data, suggests that the
clusters are formed by uric acid crystals.
Figura 2. Maclas atípicas de ácido úrico observadas con luz polarizada (microscopía óptica, 400x). Se de-
tecta una intensa birrefringencia en los cristales. Figure 2. Atypical clusters of uric acid are observed under pola-

VOLUMEN 3 PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN
EL SEDIMENTO DE ORINA DE UNA LACTANTE 03
Laboratory Medicine at a glance
rized light (optical microscopy, 400x). An intense birefringence is detected in the crystals.
La paciente, que no tenía antecedentes previos,
fue derivada desde su centro de salud por presentar
varios episodios febriles, de 22 horas de evolución y
con un pico máximo de 39,5ºC, atenuados parcial-
mente con antipiréticos, y sin otra sintomatología
acompañante. El embarazo y el parto habían trans-
currido sin incidencias y se siguió el calendario vacu-
nal vigente.
En un primer ingreso se realizó sedimento urina-
rio y se observó moderada cantidad de leucocitos y
bacterias. El análisis químico de la orina objetivó un
pH ligeramente ácido, con proteinuria, elevación del
cociente albúmina/creatinina, hiperuricosuria y con-
centraciones bajas de sodio, cloro, calcio, magnesio
y urea. En la analítica sanguínea destacó leucocito-
sis con neutrofilia, trombocitosis y elevación de la
proteína C reactiva. Se aisló Klebsiella pneumoniae
en el urocultivo, se diagnosticó infección del tracto
urinario y se pautó tratamiento antibiótico con trime-
toprim/sulfametoxazol.
Sin embargo, la paciente volvió dos veces más a
Urgencias con un patrón clínico de fiebre similar y
ausencia de otros síntomas. Los datos de laboratorio
nuevamente mostraron una infección del tracto urina-
rio, con bacterias del género Pseudomonas. En el
sedimento urinario, además de piuria, se observaron
las atípicas y birrefringentes maclas de cristales de
ácido úrico descritas en las figuras 1 y 2.
Considerando los datos clínicos y de laboratorio,
y ante la sospecha de una ectasia, se realizó una
ecografía renal que reveló, en ambos riñones, dilata-
ción pielocalicial con afectación incipiente de cálices
y alteración en el diámetro anteroposterior de la pel-
vis. Se observó también ectasia intermitente de am-
bos uréteres distales. Con estos hallazgos se diag-
nosticó un reflujo vesicoureteral bilateral, de grado II
en el riñón derecho y III-IV en el izquierdo, con urete-
The patient, who had not a previous interesting
medical history, was derived from her health center
because of several febrile episodes (lasting 22 hours,
maximum peak: 39,5ºC) partially lessened with anti-
pyretics, and no other symptoms. Pregnancy and
childbirth had passed without incidents and vaccina-
tions were according to the current calendar.
In a first admission, urinary sediment was done
and a moderate amount of leukocytes and bacteria
were observed. Urine chemistry analysis showed a
slightly acidic pH, with proteinuria, a high albu-
min/creatinine ratio, hyperuricosuria and low concen-
trations of sodium, chloride, calcium, magnesium and
urea. Serum clinical chemistry tests revealed leuko-
cytosis with neutrophilia, thrombocytosis and eleva-
tion of C-reactive protein. Klebsiella pneumoniae
was isolated in urine culture, the patient was diag-
nosed with an urinary tract infection and treatment
with trimethropim/sulfamethoxazole was prescribed.
However, the patient returned two more times to
the Emergency Room with a similar clinical pattern of
fever and absence of other symptoms. Laboratory
tests confirmed again an urinary tract infection and
bacteria of the genus Pseudomonas were isolated.
Apart from pyuria, in the urinary sediment the atypical
and birefringent clusters of uric acid crystal described
in figures 1 and 2 were observed.
Considering clinical and laboratory data, and due
to the suspicion of ectasia, a renal ultrasound was
realized, which revealed pyelocalyceal dilatation in
both kidneys with incipient involvement of renal caly-
ces and alteration in the anteroposterior diameter of
the pelvis. Intermittent ectasia of both distal ureters
was also observed. Taking these findings together, a
bilateral vesicoureteral reflux was diagnosed, grade II
in the right kidney and grade III-IV in the left one, with

VOLUMEN 3 PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN
EL SEDIMENTO DE ORINA DE UNA LACTANTE 04
Laboratory Medicine at a glance
rohidronefrosis de grado II en el riñón izquierdo y pa-
rénquima renal conservado. La cistouretrografía mic-
cional seriada realizada después confirmó el reflujo
vesicoureteral bilateral.
Debido a la mala evolución clínica de la paciente
y a la ineficacia del tratamiento antibiótico para resol-
ver el reflujo vesicoureteral, se realizó cirugía pediá-
trica para corregir el mecanismo de válvula antirreflu-
jo, mediante reimplantación del uréter en la vejiga.
Asimismo, se mantuvo el tratamiento profiláctico con
antibióticos.
A los 4 meses se repitieron las pruebas de ima-
gen y se observó la completa normalización de todas
las vías urinarias, con buena diferenciación cortico-
medular y sin dilatación de los sistemas colectores.
Ante la desaparición del reflujo vesicoureteral, au-
sencia de alteraciones en las analíticas de laborato-
rio y de síntomas clínicos, se suspendió la profilaxis
antibiótica y se dio de alta a la paciente.
El reflujo vesicoureteral es el paso retrógrado no
fisiológico de la orina desde la vejiga al uréter, por un
defecto anatómico/funcional de la unión uretero-
vesical. Su importancia clínica en niños viene por su
asociación con infecciones urinarias de repetición,
daño renal crónico y progresión a insuficiencia renal.
Existen diversos grados de reflujo según las estructu-
ras urinarias afectadas y el daño ocasionado1-2.
Las técnicas de imagen más utilizadas para el
diagnóstico de reflujo vesicoureteral son: ecografía
renal, cistografía isotópica y cistouretrografía miccio-
nal seriada. Otros parámetros utilizados para valorar
la nefropatía de reflujo son: presión arterial, albumi-
nuria, pruebas de concentración urinaria y estimación
de la función glomerular3.
El tratamiento inicial consiste en medidas higiéni-
cas generales. La profilaxis antibiótica se pauta a
grupos de riesgo, como la presencia de reflujo vesi-
ureterohydronephrosis (grade II) in the left kidney
and preserved renal parenchyma. A voiding cys-
tourethrogram was done later and it confirmed the
bilateral vesicoureteral reflux.
Due to the poor clinical evolution of the patient
and the inefficiency of the treatment with antibiotics to
spontaneously resolve the vesicoureteral reflux, a
pediatric surgical procedure was done to repair the
mechanism of the anti-reflux valve, by means of ure-
teral reimplantation into the bladder. Moreover, the
prophylactic treatment with antibiotics was main-
tained.
Imaging tests were repeated 4 months later and a
complete normalization of the urinary tract was ob-
served, with a good corticomedullary differentiation
and no expansion of the collecting duct system. Due
to the disappearance of vesicoureteral reflux, the ab-
sence of alterations in laboratory tests or clinical
symptoms, the antibiotic prophylaxis was suspended
and the patient was discharged from the hospital.
Vesicoureteral reflux is defined as the abnormal
retrograde flow of urine from the bladder to the ure-
ter, due to an anatomical/functional defect of
ureterovesical junction. Clinical significance in chil-
dren is due to its association with recurrent urinary
tract infections, chronic renal damage and progres-
sion to renal insufficiency. There are different grades
of reflux, according to the affected urinary structures
and damage caused1-2.
Imaging techniques most commonly used for the
diagnosis of vesicoureteral reflux are: renal ultraso-
nography, isotopic cystography and voiding cys-
tourethrogram. Other parameters used to assess re-
flux nephropathy are: blood pressure, albuminuria,
urine concentration tests and estimated glomerular
filtration rate3.

VOLUMEN 3 PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN
EL SEDIMENTO DE ORINA DE UNA LACTANTE 05
Laboratory Medicine at a glance
coureteral dilatado o infección del tracto urinario con
fiebre recurrente. Con estos abordajes se pretende
que el reflujo remita espontáneamente. Sin embargo,
en el resto de casos se realiza tratamiento quirúrgi-
co/endoscópico para reparar el defecto en la unión
uretero-vesical4-5.
Ante el hallazgo de maclas de ácido úrico en el
sedimento urinario, el especialista de laboratorio de-
be valorar el diagnóstico diferencial entre varias enti-
dades6:
Uricosuria idiopática.
Ingesta elevada de purinas.
Desórdenes tubulares renales.
Reflujo vesicoureteral.
Cardiopatía congénita cianótica.
Enfermedades mieloproliferativas.
Síndrome de Lesh-Nyhan.
Glucogenosis tipo I.
Infecciones del tracto urinario.
Para ello, algunas de las pruebas complementa-
rias en las que se debe apoyar serían7:
Anamnesis y exploración clínica: historia fami-
liar, anomalías estructurales, medicación, to-
ma de temperatura corporal, palpación abdo-
minal.
Urocultivo.
Análisis de orina de 24 horas: volumen, densi-
dad, pH, creatinina, urea, albúmina, iones y
ácido úrico.
Hemograma y determinación en sangre de io-
nes, creatinina, ácido úrico y marcadores de
infección.
Pruebas de imagen: ecografía re-
nal/ureteral/vesical, tomografía computerizada
helicoidal, cistouretrografía miccional seriada.
The initial treatment consists of general hygiene
measures. Antibiotic prophylaxis is recommended for
risk groups, such as the presence of dilating
vesicoureteral reflux or recurrent febrile urinary tract
infections. These approaches expect to get a sponta-
neous resolution of vesicoureteral reflux. However, in
other cases surgical/endoscopic treatments are per-
formed to repair the defect in the ureterovesical junc-
tion4-5.
When uric acid clusters are detected in an urinary
sediment, the laboratory specialist shoud weigh the
differential diagnosis and consider several options6:
Idiopathic uricosuria.
High purine intake.
Renal tubular disorders.
Vesicoureteral reflux.
Cyanotic congenital cardiopathy.
Myeloproliferative diseases.
Lesh-Nyhan syndrome.
Glycogenosis type I.
Urinary tract infections.
With this purpose, some additional tests shoud be
taken into account7:
Anamnesis and clinical exploration: family
medical history, structural abnormalities, medi-
cation, body temperature measurement, ab-
dominal palpation.
Urine culture.
24-hour urine tests: volume, specific gravity,
pH, creatinine, urea, albumin, ions and uric ac-
id.
Hemogram and serum concentrations of ions,
creatinine, uric acid and inflammatory markers.
Imaging tests: renal/ureteral/vesical ultraso-
nography, helical computed tomography, void-
ing cystourethrogram.

VOLUMEN 3 PRESENCIA DE MACLAS ATÍPICAS DE ÁCIDO ÚRICO EN
EL SEDIMENTO DE ORINA DE UNA LACTANTE 06
Laboratory Medicine at a glance
Bibliografía/References:
1. Greenfield SP, Ng M, Wan J. Experience with vesicoureteral reflux in children: clinical characteristics. J
Urol. 1997;158:574-7.
2. LA, Mesrobian HG. Vesicoureteral reflux. Pediatr Clin North Am. 2006;53:413-427.
3. Escribano Subías J, Valenciano Fuentes B. Reflujo vesicoureteral. Protocolos de la Asociación
Española de Pediatría. 2014;1:269-81.
4. Peters CA, Skoog SJ, Arant BS Jr., Copp HL, Elder JS, Hudson RG, et al. Summary of the AUA Gui-
deline on Management of Primary Vesicoureteral Reflux in Children. J Urol. 2010;184:1134-44.
5. Tekgül S, Riedmiller H, Hoebeke P, Copp HL, Elder JS, Hudson RG, et al. EAU guidelines on
vesicoureteral reflux in children. Eur Urol. 2012;62;534-42.
6. Camacho Díaz JA, Vila Cots J. Litiasis renal. Protocolos Diagnóstico Terapéuticos de la AEP: Nefrología
Pediátrica. 2008;1:189-196. https://www.aeped.es/sites/default/files/documentos/17_3.pdf
7. Litiasis en el niño. Urología práctica 2011.
https://seattleclouds.com/myapplications/jpburgues/urologia/Litiasisnino.pdf

Laboratory Medicine at a glance
Medicina de Laboratorio de un vistazo
VOL.3 ISSN 2444-8699
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN
QUÍMICA
SIALOLITHIASIS: ANALYSIS AND CHEMICAL
COMPOSITION
Volumen 3
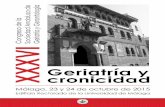
En la Figura 1 se observa el sialolito obtenido de
93 mg por cirugía maxilofacial. Las características
macroscópicas de este cálculo fueron: color miel,
consistencia dura y superficie rugosa, propias de las
descritas en la bibliografía. Este sialolito pertenece a
In Figure 1 the sialolith of 93 mg obtained by max-
illofacial surgery is shown. The macroscopic charac-
teristics of this calculus were the following: honey co-
lour, hard consistency and rough surface, typical fea-
tures described in the literature. This sialolith corres-
Autores
María del Mar Rodríguez Rodríguez Lucía Jiménez Mendiguchía Ana María García Cano
Centro Servicio de Bioquímica Clínica del
Hospital Universitario Ramón y
Cajal de Madrid.
Fecha de publicación 29 Agosto 2016
Páginas Páginas 7-12
Figura 1. Cálculo salival formado por dos fragmentos de color miel. Figure 1. Salivary
calculus made up of two honey-colored fragments.

VOLUMEN 3
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA Pag.08
Laboratory Medicine at a glance
un paciente de 46 años, que acude a la consulta por
episodio de inflamación submaxilar derecha con
supuración por carúncula del conducto de Wharton.
La localización del sialolito suele ser la glándula
salival submaxilar (80-92%) y, con menos frecuencia,
la glándula parótida (6-20%) y la glándula sublingual
(1-2%). Además, la mayoría de los sialolitos son
radiopacos y visibles en radiografías planas
(panorámicas u oclusales) o con TC, lo que permite
localizarlos para su posterior tratamiento quirúrgico.
En este caso, se le realiza un TC de cuello con
contraste intravenoso (CIV), tal y como se muestra
en la Figura 2. En el TC se observan:
Glándulas submaxilares y parótidas de
tamaño normal y captación homogénea.
Discreta dilatación del conducto de Wharton
derecho, que muestra cambios inflamatorios-
infecciosos con captación difusa y
circunferencial de su pared, identificando dos
litiasis en su segmento distal de 6.6 y 4.6 mm,
respectivamente.
Pequeñas adenopatías subcentrimétricas
submandibulares bilaterales.
No se identifican adenopatías de tamaño o
aspecto patológico en el resto de estaciones
gangliolares laterocervicales bilaterales.
Nasofaringe, orofaringe, hipofaringe y cavidad
laríngea sin hallazgos a destacar.
Cambios inflamatorios en senos maxilares,
celdillas etmoidales bilaterales y seno
esfenoidal.
ponds to a 46 years old patient, who presents an epi-
sode of right submandibular inflammation with suppu-
ration by Wharton´s duct caruncula. Sialoliths are
most common within the body of the submandibular
gland or Warton´s duct (80-92%). From 6% to 20% of
sialoliths occur in the parotid gland, and the remain-
ing 1-2% are located within the sublingual or minor
salivary glands. Furthermore, the majority of sialoliths
are radiopaque and they are visible on plain radio-
graphs (panoramic or occlusal radiograph) or CT
scans. It allows locating them for later surgical treat-
ment. In this case, a CT scan with intravenous con-
trast was achieved, as shown in Figure 2. In this CT
scan the following characteristics were observed:
Parotid and submandibular glands of normal
size and homogeneous uptake.
Discrete dilatation of the right Wharton´s duct
which shows infectious- inflammatory
changes with diffuse and circumferential up-
take in its wall, identifying two stones of 6.6
and 4.6 mm, respectively, in the distal seg-
ment.
Small bilateral submandibular subcentrime-
trics adenopathies.
No adenopathies with pathological appear-
ance or size in the other bilateral laterocer-
vical gangliolares stations are identified.
Nasopharynx, oropharynx, hypopharynx and
laryngeal cavity without highlight findings.
Inflammatory changes in maxillary sinus, bila-
teral ethmoid cells and sphenoid sinus are
observed.

VOLUMEN 3
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA Pag.09
Laboratory Medicine at a glance
Así, se localizó en la glándula submaxilar,
concretamente en el conducto de Wharton. El
tratamiento realizado fue la eliminación quirúrgica de
los dos cálculos en el interior del conducto de
Wharton derecho bajo anestesia general.
Clínicamente es importante realizar un
diagnóstico diferencial, ya que sus signos y síntomas
se relacionan con otros agrandamientos glandulares.
Por ejemplo, algunos agrandamientos bilaterales
asintomáticos de la región parotídea incluyen las
lesiones linfoepiteliales (síndrome de Mikulicz),
síndrome de Sjögren, la toma prolongada de
diversos medicamentos (yodo y metales pesados) y
al tumor de Whartin. Los agrandamientos bilaterales
dolorosos pueden originarse tras radioterapia o
pueden ser secundarios a una sialoadenitis vírica
(incluyendo las paperas) cuando se acompañan de
otros síntomas sistémicos. Tanto el diagnóstico como
el tratamiento dependen del tipo de lesión, su
ubicación, composición, tamaño e historia clínica del
Thus, it was located in the submandibular gland,
particularly in Wharton's duct and the performed
treatment was the surgical removal of the two calculi
inside the right Wharton´s duct under general anes-
thesia.
The differential diagnosis is clinically important
because its signs and symptoms are related to other
glandular enlargements. For example, some asymp-
tomatic bilateral enlargements of the parotid region
include lymphoepithelial lesions (Mikulicz syndrome),
Sjögren's syndrome, prolonged intake of various
drugs (iodine and heavy metals) and tumor Warthin.
Painful bilateral enlargements may arise after radio-
therapy or may be secondary to a viral sialadenitis
(including mumps) when they are accompanied by
other systemic symptoms. Both diagnosis and treat-
ment depend on the type of injury, location, composi-
tion, size and medical history of the patient. In this
sense, in Figure 3 the spectrum obtained by IR spec-
troscopy is shown. The characteristic bands corres-
Figura 2. TC de cuello con CIV realizado en el paciente y en el que se ob-
servan las dos litiasis radiopacas en la glándula submandibular. Figure 2. A
CT scan with intravenous contrast revealed two radiopaque stones within
the body of the submandibular gland.

VOLUMEN 3
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA Pag.10
Laboratory Medicine at a glance
paciente. En este sentido, en la Figura 3 se muestra
el espectro obtenido mediante espectroscopía de IR,
en el que se observan las bandas típicas del
fosfocarbonato cálcico que aparecen reflejadas en el
mismo. Para este análisis se realiza una muestra
alícuota del cálculo que se obtiene por un único
raspado longitudinal con bisturí, dado que la
estructura del mismo es homogénea. Posteriormente
se realiza una dispersión y mezcla de la alícuota con
KBr obteniéndose, tras someter a presión, un disco
plano de 1 mm de grosor, sobre el que se realiza la
lectura. Las ventajas de la espectroscopía de IR son
su rapidez, sensibilidad, requiere poca muestra y
analiza compuestos amorfos. Por ello, es de suma
importancia, la labor del laboratorio en la descripción
macroscópica y en la composición del cálculo.
Además, respecto al papel del laboratorio, no se ha
relacionado con ningún trastorno del metabolismo
calcio-fósforo y, en general, el estudio de electrolitos
y de las hormonas paratiroideas en estos pacientes
es normal, hecho que se observó en este caso.
ponding to an IR spectrum of pure calcium phospho-
carbonate are observed. For this analysis, as the
structure of the sialolith calculi is homogeneous, an
aliquot sample is obtained by a single longitudinal
scraping with a scalpel. Subsequently, the aliquot is
scattered and mixed with KBr. After pressurizing, we
obtain a flat disc of 1 mm thick, upon which the read-
ing is performed. The advantages of IR spectroscopy
are its speed, its sensitivity, that it requires little sam-
ple and it analyzes amorphous compounds. Thus, the
work of the laboratory in the macroscopic description
and the determination of the calculus composition is
very important. Furthermore, regarding the role of the
laboratory, sialolithiasis has not been associated with
any disorder of calcium-phosphorus metabolism and,
in general, the study of electrolytes and parathyroid
hormone in these patients provides normal results, a
fact that was observed in this particular case.
Figura 3. Espectro de IR obtenido con una dispersión de la muestra de sialolito con bromuro potásico. En el mismo se
muestran las longitudes de onda de las bandas características obtenidos y, que corresponden, a un espectro de fosfo-
carbonato cálcico puro. Figure 3. IR spectrum obtained with a dispersion sialolith sample with potassium bromide. In
this spectrum the wavelength of the characteristic bands, which correspond to a spectrum of pure calcium phosphocar-
bonate, are shown.

VOLUMEN 3
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA Pag.11
Laboratory Medicine at a glance
La sialolitiasis es la enfermedad no neoplásica
más común de las glándulas salivares y la causa
más común de obstrucción de la glándula salival. Los
cálculos en la glándula salival ocurren en 1% o 2 %
de la población, pero la prevalencia de sialolitiasis
sintomáticas es del 0.45%. Los sialolitos pueden
aparecer a cualquier edad, pero su frecuencia es
mayor entre los 40 y 60 años, con predominio en los
varones.
La sialolitiasis es una afección que se produce
por la obstrucción de una glándula salival o de su
conducto excretor por la formación de concreciones
calcáreas o sialolitos en el parénquima de los
mismos. Su composición química es fosfato cálcico
(70%), carbonato cálcico (10%), sales y sustancias
orgánicas (12%) y agua (3%). La verdadera causa es
desconocida, pero existen teorías que afirman que
los sialolitos en las glándulas y conductos salivales
son originados por la mineralización de varios
componentes como: cuerpos extraños, detritus
celulares y microorganismos, depositándose
inicialmente una matriz orgánica, probablemente de
glucoproteínas, para luego posteriormente
presentarse el depósito de material inorgánico que
inicia su mineralización. Esta patología desencadena
una serie de signos y síntomas, como dolor de
moderado hasta severo antes, durante y después de
las comidas, hasta la obstrucción del conducto que
no permite el paso de la saliva, lo que produce
sintomatología fuertemente dolorosa y tumefacción.
En algunas ocasiones el paciente no presenta
síntomas notables y la única manifestación puede
ser la presencia de una lesión tumoral de
consistencia pétrea, que se palpa en el conducto o
en el interior de la glándula.
Sialolithiasis is the most common non neoplastic
disease of the salivary glands and the most common
cause of salivary gland obstruction. Salivary gland
calculi are estimated to occur in 1% to 2% of the
population. However, the prevalence of symptomatic
sialolithiasis is 0.45%. Sialoliths can appear at any
age, but it is more frequent to appearance in people
between 40 and 60 years old. It is prevalent in males.
Sialolithiasis is a clinical condition produced by a
blockage of the salivary gland or excretory duct by
the formation of calcareous concretions or sialoths in
their parenchyma. Its chemical composition is cal-
cium phosphate (70%), calcium carbonate (10%),
salts and organic substances (12%) and water (3%).
The etiology of sialolithiasis is not clear, but there are
theories that claim that the sialoliths in the salivary
glands and ducts are caused by the mineralization of
various components such as foreign bodies, cellular
debris and microorganisms, originally settled an or-
ganic matrix, probably formed of glycoproteins, and
then subsequently submitted to the General Assem-
bly Hall of inorganic material which began its minera-
lization. This condition triggers a series of signs and
symptoms, as moderate to severe pain before, during
and after meals, to duct obstruction that does not al-
low passage of saliva, which causes swelling and
pain symptoms strongly. Sometimes the patient has
not symptoms and the only manifestation may be the
presence of a tumor lesion of stony consistency,
which is evident in the duct or inside the gland.

VOLUMEN 3
SIALOLITIASIS: ANÁLISIS Y COMPOSICIÓN QUÍMICA Pag.12
Laboratory Medicine at a glance
Bibliografía/References:
1. Wilson KF, Meier JD and Ward PD. Salivary Gland Disorders. Am. Fam. Physician. 2014;89(11):882-
888.
2. Al Chalabi H, Walshe P and Curran A. Submandibular gland stones, a clinical review. Ir. Med. J.
2006;99(10):303-304.
3. Jadu FM and Jan AM. A meta-analysis of the efficacy and safety of managing parotid and submandibu-
lar sialoliths using sialendoscopy assisted surgery. Saudi Med J. 2014;35(10):1188-1194.
4. Omezli MM, Ayranci F, Sadik E and Polat ME. Case Report of giant sialolith (megalith) of the Wharton´s
duct. Niger J. Clin. Pract. 2016;19(3):414-417.

Laboratory Medicine at a glance
Medicina de Laboratorio de un vistazo
VOL.3 ISSN 2444-8699
SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO
ANTISYNTHETASE SYNDROME, A
DIAGNOSTIC CHALLENGE
Volumen 3
La imagen adjunta (Figura 1) corresponde a un
patrón citoplasmático moteado denso fino con
metafases negativas a título 1:640 observado por
inmunofluorescencia indirecta (IFI) en un sustrato de
células Hep-2. Ante la sospecha de la posible
asociación con anticuerpos antisintetasa se realiza
The attached image (Figure 1) corresponds to a
dense fine speckled cytoplasmic pattern with nega-
tive metaphases at 1:640 observed by indirect immu-
nofluorescence (IIF) in Hep-2 cells line. Suspecting
the possible association with antisynthetase antibo-
dies, the presence of antibodies anti PL-7 and anti
Autores Jose Luis García de Veas Silva
1
Rocio Escobar Conesa2
Maria del Señor Lopez Vélez1
Centro 1Complejo Hospitalario
Universitario de Granada 2Hospital de Cabueñes, Gijón
Fecha de publicación 29 Agosto 2016
Páginas Páginas 13-19
Figura 1. Inmunofluorescencia indirecta en células Hep-2. Patrón citoplasmático moteado
denso fino a título 1:640. Figure 1. Indirect immunofluorescent in Hep-2 cells. Cytoplas-
mic dense fine speckled pattern at 1:640.

VOLUMEN 3 SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO Pag.14
Laboratory Medicine at a glance
un inmunoblot específico de miositis donde se
identifica la especificidad antigénica del patrón como
anticuerpos anti PL-7 y anti Ro-52 kD (Figura 2).
La imagen corresponde a una mujer de 45 años
en estudio por presentar artralgias en manos junto a
disnea de moderado esfuerzo de un año de
evolución. En la exploración la paciente refiere
fenómeno de Raynaud y presenta lesiones
descamativas en las manos denominadas “manos de
mecánico”. Según los resultados del laboratorio y
con los datos clínicos se orienta el estudio
diagnóstico hacia un “Síndrome Antisintetasa”
asociado a miopatía autoinmune (dermatomiositis,
polimiositis, etc.). Se realiza un TAC de tórax donde
se observa un patrón intersticial con opacidades en
vidrio deslustrado y un estudio de electromiografía
que informa presencia de una miopatía inflamatoria
Ro-52 kD (Figure 2) were identified by “myositis im-
munoblot”.
The image belongs to a 45-year old woman with
joint pain in the hands and moderate dyspnea during
the last year. The patient reported Raynaud's phe-
nomenon and the physical exploration showed scaly
skin lesions in hands described as "mechanic´s
hands". With the clinical and laboratory findings, the
study of the patient was conducted towards an “Anti-
synthetase Syndrome” associated with an autoim-
mune myopathy. A Thoracic CT scan revealed an
interstitial pattern defined as ground glass opacity
and an lectromyography refers a mild inflammatory
myopathy.
Figura 2. Inmunoblot del paciente positivo para anti PL-7 y anti Ro (52 kD). Figure 2. Immunoblot positive for anti
PL-7 and anti Ro (52 kD).

VOLUMEN 3 SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO Pag.15
Laboratory Medicine at a glance
leve.
El “Síndrome Antisintetasa” es una entidad clínica
heterogénea que presenta seis manifestaciones
clínicas predominantes: enfermedad pulmonar
intersticial, poliartritis inflamatoria, miositis, fenómeno
de Raynaud, “manos de mecánico” y fiebre. Es
imprescindible su asociación a autoanticuerpos
antisintetasas dirigidos contra t-RNA sintetasas;
enzimas citoplasmáticas que catalizan la unión del t-
RNA a su aminoácido correspondiente en la síntesis
de proteínas. Los principales anticuerpos son anti Jo-
1 (histidil-tRNA sintetasa, prevalencia 25-30%), anti
PL-7 (treonil-tRNA sintetasa, 2-5%), anti PL-12
(alanil-tRNA sintetasa, 2-5%), anti EJ (glicil-tRNA
sintetasa, 1%), anti OJ (isoleucil-tRNA sintetasa, 1%)
y anti KS (asparaginil-tRNA sintetasa, 1%)1,2
. Estos
anticuerpos se han descrito en pacientes con
miopatías autoinmunes: 20-40% de adultos con
polimiositis y 5% de adultos con dermatomiositis3.
Con los hallazgos clínicos descritos y el resultado de
las pruebas de autoinmunidad, la paciente fue
diagnosticada de Síndrome Antisintetasa PL-7.
En los pacientes con sospecha de enfermedades
autoinmunes es muy importante la colaboración
entre el clínico y el laboratorio. En este contexto, la
presencia de anticuerpos antisintetasas se debería
estudiar en pacientes con miopatías autoinmunes así
como en aquellos con enfermedad pulmonar
intersticial difusa. El cribado de anticuerpos
antinucleares con técnicas de ELISA puede ser
insuficiente en muchos casos para detectar los
anticuerpos antisintetasas. Por ello, es fundamental
la solicitud del estudio de “sospecha de síndrome
antisintetasa” por el clínico para el estudio de estos
anticuerpos directamente mediante IFI. Si un patrón
citoplasmático es observado, a continuación se debe
The “Antisynthetase Syndrome” is a heterogene-
ous clinical entity characterized by six predominant
clinical manifestations: interstitial lung disease, in-
flammatory polyarthritis, myositis, Raynaud´s phe-
nomenon, “mechanic´s hands” and fever. Importantly,
it is associated with antisynthetase autoantibodies
directed against aminoacyl t-RNA synthetases.
These are cytoplasmic enzymes that attaches the
appropriate amino acid onto its tRNA. The primary
antibodies are anti Jo-1 (histidyl-tRNA synthetase,
prevalence 25-30%), anti PL-7 (threonyl-tRNA, 2-
5%), anti PL-12 (alanyl-tRNA, 2-5%), anti EJ (glycyl-
tRNA, 1%), anti OJ (isoleucyl-tRNA, 1%) and anti KS
(asparaginyl-tRNA, 1%)1,2
. The presence of these an-
tibodies is found in patients with inflammatory muscle
disease: 20-40% of adults with polymyositis and 5%
of adults with dermatomyositis3. With the clinical and
laboratory findings, the patient was diagnosed of An-
tisynthetase Syndrome PL-7.
The collaboration between physician and labora-
tory is very important in patients with suspect of auto-
immune diseases. In this context, tests for antisyn-
thetase antibodies should be obtained in patients with
inflammatory muscle disease, as well as patients with
interstitial lung disease. The screening for antinuclear
antibodies by ELISA techniques may be insufficient
and could not detect the antisynthetase antibodies.
Therefore, it is very important the application of "sus-
pected of antisynthetase syndrome" by the clinician
and the study of these antibodies by IIF. When a cy-
toplasmic pattern is observed, the antibody associ-
ated must be identified by immunoblot to complete
the study. In addition, anti-Ro (52 kD) antibodies co-
exist with antisynthetase antibodies and their pres-
ence is associated with a worse prognosis of the pa-
tients4.

VOLUMEN 3 SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO Pag.16
Laboratory Medicine at a glance
identificar el anticuerpo asociado por inmunoblot para
completar el estudio como en nuestro paciente.
Además, los anticuerpos anti-Ro (52 kD) coexisten
con los anticuerpos antisintetasas y su presencia se
asocia a un peor pronóstico de los pacientes4.
Finalmente, un resumen de los principales
anticuerpos citoplasmáticos detectados por IFI se
muestran en la tabla 1 según las recomendaciones
mas recientes5,6
.
Finally, a brief summary of the main cytoplasmic
autoantibodies detected by IIF are show in Table 1
based on recently recommendations5,6
.
PATRONES CITOPLASMÁTICOS
ANTÍGENO ENFERMEDADES
ASOCIADAS DESCRIPCIÓN
Actina
Hepatitis Autoinmune tipo I
Fibras de actinas estriadas que se ex-tienden por todo el eje de la célula en interfase
FIBRILAR LINEAL
GW182 Su/Ago2
Inespecífico, presente en enfermedades neu-rológicas y autoin-munes.
Tinción en forma de puntos de los cuerpos GW en el citoplasma de las células en interfase
GRANULAR PUNTEADO
Tabla 1. Principales anticuerpos anti-citoplasmáticos detectados por inmunofluorescencia indirecta.Table 1.
Brief summary of the main cytoplasmic autoantibodies detected by indirect immunofluorescence.

VOLUMEN 3 SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO Pag.17
Laboratory Medicine at a glance
PL-7 PL-12 Ribosomal P SRP
Síndrome antisintetasa Polimiositis Dermatomiositis LES juveil LES neuropsiquiátrico
Tinción granular muy fina que se extiende por el citoplasma en interfase
MOTEADO DENSO FINO (HO-MOGÉNEO)
Jo-1 Síndrome antisintetasa Polimiositis Dermatomiositis
Pequeños gránulos que extienden por el citoplasma en inter-fase
MOTEADO FINO
PCD-E2 / M2 BCOADC-E2 OGDC-E2
Cirrosis Biliar Primaria Esclerosis Sistémica
Tinción de filamentos granulares que se extienden por el citop-lasma en interfase
RETICULAR (MITOCONDRIAL M2)
Golgina-245 Giantina
Inespecífico Tinción granular dis-continua perinuclear con distribución polar
GRANULAR POLAR

VOLUMEN 3 SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO Pag.18
Laboratory Medicine at a glance
IMPDH2 Pacientes con VHC en tratamiento con IFN-Ribavirina
Tinción de corpúscu-los en forma de anil-los y bastones en el citoplasma de las células en interfase
BASTONES Y ANILLOS
Bibliografía/References:
1. Chatterjee S. Prayson R, Farver C. Antisynthetase syndrome: Not just an inflammatory myopathy. Cleve
Clin J Med. 2013 Oct 1;80(10):655–66.
http://www.ccjm.org/view-pdf.html?file=uploads/media/media_9d4816d_655
2. Labirua-Iturburu A, Trallero Araguás E, Selva O’Callaghan A. Síndrome por anticuerpos antisintetasa.
Med Clin (Barc). Elsevier; 2011 Jun;137(2):77–83.
http://www.elsevier.es/es-revista-medicina-clinica-2-articulo-sindrome-por-anticuerpos-antisintetasa-
S0025775311003228?redirectNew=true
3. Ghirardello A, Rampudda M, Ekholm L, Bassi N, Tarricone E, Zampieri S, et al. Diagnostic performance
and validation of autoantibody testing in myositis by a commercial line blot assay. Rheumatology (Ox-
ford). Oxford University Press; 2010 Dec;49(12):2370–4.
http://rheumatology.oxfordjournals.org/content/49/12/2370.long
4. Yoshimi R, Ueda A, Ozato K, Ishigatsubo Y, Yoshimi R, Ueda A, et al. Clinical and pathological roles of
Ro/SSA autoantibody system. Clin Dev Immunol. Hindawi Publishing Corporation; 2012;2012:606195.
http://www.hindawi.com/journals/jir/2012/606195/
5. Chan EKL, Damoiseaux J, Carballo OG, Conrad K, de Melo Cruvinel W, Francescantonio PLC, et al.
Report of the First International Consensus on Standardized Nomenclature of Antinuclear Antibody HEp-
2 Cell Patterns 2014–2015. Front Immunol. Frontiers; 2015 Aug 20;6:412.
http://journal.frontiersin.org/article/10.3389/fimmu.2015.00412/full
6. ICAP – International Consensus on ANA patterns.

VOLUMEN 3 SÍNDROME ANTI-SINTETASA, UN DESAFIO
DIAGNOSTICO Pag.19
Laboratory Medicine at a glance
http://www.anapatterns.org/

Laboratory Medicine at a glance
Medicina de Laboratorio de un vistazo
VOL.3 ISSN 2444-8699
LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN
PACIENTE PLURIPATOLÓGICO
ACUTE PLASMA CELL LEUKEMIA IN
PLURIPATHOLOGICAL PATIENT
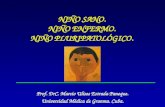
Figura 1. A) Morfología de sangre periférica. B) Estudio morfológico de médula ósea. C-H) Estudio de citometría de flujo del aspirado medular. C) Diagrama de tamaño (FSC) y com-plejidad (SSC) de las poblaciones leucocitarias en médula ósea) D) Diagrama CD45/Complejidad (SSC) de las poblaciones medulares. E) Diagrama CD45/CD38; mues-tra la expresión de CD38 y ausencia de CD45 en la población de células plasmáticas (población rosa). F) y G) Fenotipo de las células plasmáticas. H) Expresión clonal de ca-
Autores Beatriz Moreno González
Rosa María Lillo Rodríguez
Montserrat Alvarellos Outeiro
Centro Complejo Hospitalario de
Navarra
Fecha de publicación 29 agosto 2016
Páginas Páginas 20-25

VOLUMEN 3 LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN
PACIENTE PLURIPATOLÓGICO 21
Laboratory Medicine at a glance
denas ligeras kappa intracitoplasmáticas.
En la imagen A, se muestra la morfología de sangre pe-
riférica de un varón pluripatológico de 79 años que acu-
de al Servicio de Urgencias de nuestro hospital debido a
un empeoramiento del estado general de un mes de
evolución y aparición de un hematoma doloroso a la
palpación en hemitórax izquierdo. En la analítica urgen-
te destaca un aumento de leucocitos (32,9 x 109/L) con
marcada linfocitosis (21,1 x 109/L). En el estudio morfo-
lógico (figura A) se observaron células atípicas, de ma-
yor tamaño respecto a los linfocitos normales, y con
elevada basofilia citoplasmática. A la vista de los resul-
tados, y ante la sospecha de patología hematológica, se
realiza punción de médula ósea y se solicita completar
estudio mediante citometría de flujo, estudio citogenéti-
co y pruebas bioquímicas.
El estudio citológico del aspirado de médula ósea (figu-
ra B) refleja una muestra hipercelular con infiltración
masiva por células plasmáticas (87%) y mínima repre-
sentación de hematopoyesis normal. Las células atípi-
cas son de tamaño pequeño/medio, con núcleo excén-
trico, de cromatina más o menos condensada, con nu-
cleolo visible en algunas células, mostrando el núcleo
con frecuencia lobulaciones, protuberancias o binuclea-
ridad. El citoplasma es basófilo, con mamelones y en la
mayoría se conserva el arcoplasma. Algunas células
son grandes, observando incluso células multinuclea-
das.
En el estudio de citometría de flujo de la médula ósea
(Figuras C a H) se observa una infiltración por una po-
blación de células plasmáticas (75,8%) con expresión
monoclonal de cadena ligera Kappa intracitoplasmática
y un inmunofenotipo característico de mieloma múltiple
(CD38 ++/+++, CD138 +, CD56 parcialmente + (50%),
CD19 -, CD117 -, CD45 -, CD27 -, CD81).
Figure A shows peripheral Blood morphology from a plu-
ripathological male aged 79 who was admitted in our
emergency department due to worsening of the overall
condition and appearance of a painful hematoma in his
left hemithorax. Urgent blood tests showed an increased
leukocyte count (32,9 x 109/L) with marked lymphocyto-
sis (21,1 x 109/L). Morphological analysis showed atypi-
cal cells, bigger than normal lymphocytes, and a highly
basophilic cytoplasm. In view of the results, a hematolo-
gical malignancy was suspected. Thus, a bone marrow
analysis with flow cytometry and cytogenetics analysis
was requested. Biochemical test were also ordered.
Morphological analysis (figure B) showed a hypercellular
bone marrow with a massive infiltration by plasma cells
(87%) and minimal normal hematopoiesis. Atypical cells
were small to medium size, with eccentric nucleus, more
or less condensed chromatin with visible nucleoli in so-
me cells. Frequently cells showed nuclei lobularity or
binuclearity. The cytoplasm was basophilic, with hubs
and the most arcoplasma is preserved. A few cells were
large, even multinuclear cells were seen.
Bone marrow flow cytometry analysis (figures C to H)
showed a monoclonal plasma cell infiltration with a cha-
racteristic multiple myeloma immunophenotype. Patho-
logical cells were CD38 ++/+++, CD138 +, partial CD56
+ (50%), CD19 -, CD117 -, CD45 -, CD27 -, CD81, with
clonal intracytoplasmatic kappa light chain expression.
Cytogenetics was consistent with a normal male kar-
yotype without numerical or structural abnormalities (46,
XY [20]).
Morphological and flow cytometry results are consistent
with a massive bone marrow infiltration by a plasma cell
leukemia with a multiple myeloma associated immunop-

VOLUMEN 3 LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN
PACIENTE PLURIPATOLÓGICO 22
Laboratory Medicine at a glance
En el estudio citogenético realizado se observa cariotipo
masculino normal, sin alteraciones cromosómicas nu-
méricas ni estructurales (46, XY [20]).
Los resultados de la morfología y citometría de flujo son
compatibles con el diagnóstico de una leucemia aguda
de células plasmáticas con infiltración medular masiva
con fenotipo de mieloma múltiple. Llama la atención la
ausencia de pico monoclonal tanto en el proteinograma,
como en la inmunofijación sérica. Debido a la pluripato-
logía existente y la mala evolución del paciente, se de-
cide no realizar ningún tratamiento oncoespecífico y
priorizar su bienestar y confort a través de un buen con-
trol sintomático. A las 24 horas es exitus.
La leucemia de células plasmáticas (LCP) es una gam-
mapatía monoclonal poco frecuente, muy agresiva y de
mal pronóstico que se caracteriza por la presencia de
células plasmáticas circulantes en sangre periférica (1).
En los datos de laboratorio destaca la presencia de cé-
lulas plasmáticas en sangre periférica, cuyo recuento
suele ser superior a 2.000 por microlito, o bien repre-
sentar más del 20% de los leucocitos totales. En oca-
siones las células plasmáticas ofrecen aspectos morfo-
lógicos aberrantes, como incisuras a nivel nuclear, mul-
tilobularidad o ser de aspecto peludo (2), por lo que
pueden ser fácilmente confundibles con células típicas
de distintas patologías hematológicas. Fenotípicamente
las células plasmáticas son parecidas a las del mieloma
múltiple, siendo de especial interés el uso de los mar-
cadores CD38 y CD138 (3). Para completar el diagnós-
tico de laboratorio es necesario cuantificar la β2-
microglobulina y realizar un estudio completo de inmu-
noglobulinas incluyendo proteinograma e inmunofijación
(1).
La LCP sigue siendo una entidad extremadamente
agresiva, con una supervivencia muy corta; siete meses
henotype. Absence of monoclonal component using ca-
pillary electrophoresis and also immunotyping was re-
markable. Given the patient’s pluripathological condition
and his poor outcome, comfort and wellness were priori-
tized over oncological treatment. The patient died with in
24 hour after diagnosis.
Plasma cell leukemia is a very agressive and rare mo-
noclonal gammapathy with a bad prognosis characteri-
zed by the presence of circulating plasma cells in perip-
heral blood (1).
Identification of plasma cells in the patients peripheral
blood is an important laboratory data . Usually plasma
cell count is more than 2000/ L, or their frequency is
bigger than 20% of total leukocytes. Sometimes plasma
cells show cytological abnormalities, such as nuclear
incisures, multiple lobes, or hairy cell morphology. Thus,
they can easily be taken as another hematological ma-
lignancy. Plasma cell leukemia shares immunopheno-
typical characteristics with multiple myeloma cells, being
of special interest is the use of CD38 and CD138 anti-
gens (3). Laboratory diagnosis is completed with
β2microglobulin quantification and a complete immuno-
globulin analysis, including protein electrophoresis and
immunotyping electrophoresis.
Plasma cell leukemia remains an extremely aggressive
disease, with a short survival. Over al survival of pa-
tients receiving chemotherapy is 7 months. There is no
consensus about PCL treatment. The main goal for
these patients is to prolong survival of the patients and
improve their quality of life.
In this case, laboratory workup was essential for an
early diagnosis that enabled appropriate symptomatic
treatment, taking into account the aggressiveness of the
disease and the huge tumoral load in this patient.

VOLUMEN 3 LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN
PACIENTE PLURIPATOLÓGICO 23
Laboratory Medicine at a glance
tras su diagnóstico para los pacientes que reciben tra-
tamiento quimioterápico. El tratamiento de la LCP no
está del todo establecido; va dirigido principalmente a
prolongar la supervivencia de los pacientes y a maximi-
zar su calidad de vida (3).
En el caso expuesto, el papel del laboratorio resultó
fundamental para diagnosticar de forma precoz al pa-
ciente e instaurar el tratamiento sintomático adecuado,
ya que se trata de una patología agresiva y muy avan-
zada en nuestro paciente.
A B C
D E F

VOLUMEN 3 LEUCEMIA AGUDA DE CÉLULAS PLASMÁTICAS EN
PACIENTE PLURIPATOLÓGICO 24
Laboratory Medicine at a glance
Bibliografía/References:
1. Niels W. C. J. van de Donk, Henk M. Lokhorst, Kenneth C. Anderson, and Paul F. Richardson. How I
treat plasma cell leukemia. Blood 2012; 120(12):2376-2389.
2. C Fernández de Larrea, RA Kyle, BGM Durie, H Ludwing, S Usmani, DH Vesole et al. Plasma cell
leukemia: consensus statement on diagnostic requirements, response criteria and treatment
recommendations by the International Myeloma Working Group. Leu 2012; 336:1-12.
3. Beatriz Aguado Bueno, Natalia Acedo Domínguez y Adrián Alegre Amor. Diagnóstico y tratamiento de la
leucemia de células plasmáticas. Cuadernos de Hematología III. 2012; 1-10.
Enlaces de interés:
1. http://www.bloodjournal.org/content/bloodjournal/120/12/2376.full.pdf. Uptodate. Plasma cell leucemia
Plasma cell leucemia. S Vincent Rajkumar, MD.