Periodontiis y Enfermedad Cardiovascular
8
Review Association between periodontal disease and its treatment, ow-mediated dilatation and carotid intima-media thickness: A systematic review and meta-analysis Marco Orlandi a , * , Jeanie Suvan a , Aviva Petrie b , Nikolaos Donos a , Stefano Masi c , Aroon Hingorani d , John Deaneld c , 1 , Francesco D Aiuto a , 1 a Unit of Periodontology, UCL Eastman Dental Institute, 256 Gray ' s Inn Road, London WC1X 8LD, United Kingdom b Biostatistics Unit, UCL Eastman Dental Institute, 256 Gray' s Inn Road, London, United Kingdom c Vascular Physiology Unit, Great Ormond Street Hospital, 34 Great Ormond Street, London, United Kingdom d Faculty of Population Health Sciences, Institute of Cardiovascular Science, UCL, 1e 19 Torrington Place, London, United Kingdom a r t i c l e i n f o Article history: Received 6 April 2014 Received in revised form 27 May 2014 Accepted 4 June 2014 Available online 17 June 2014 Keywords: Cardiov ascular disease Periodontitis Carotid intima-media thickness Flow-mediat ed dilatation Endothelial function a b s t r a c t Objective: T his meta-a nalys is sought to inve stiga te the assoc iati on between carot id intima-med ia thickness (c-IMT), ow-mediat ed dilation (FMD) and peri odont itis (PD) and to assess the effect of periodontal treatment on c-IMT and FMD. Methods: Electronic database searching, hand searching of bibliographic references of included papers, related reviews, and journals in relation to oral, cardiovascular and ultrasound imaging eld was carried out. Random effec ts meta-a naly ses were perfo rmed to inve stiga te the association of co-e xist ence of increased c-IMT, impaired FMD and PD with potential changes in these variables following periodontal intervention. Results: 2009 citations and 101 full text articles were screened, with 35 meeting the review inclusion criteria of which 22 suitable for quantitative analysis. Meta-analysis demonstrated that the diagnosis of PD was associated with a mean increase in c-IMT of 0.08 mm (95% C.I. ¼ 0.07e0.09) and a mean dif- ference in FMD of 5.1% compared to controls (95% C.I. ¼ 2.08e8.11%). A meta-analysis of the effects of periodontal treatment on FMD showed a mean improvement of 6.64% between test and control (95% C.I. ¼ 2.83e10.44%). Conclusions: This review demonstrated an association between increased c-IMT, impaired FMD and PD. Data from intervention studies suggested a bene cial effect of periodontal treatment on FMD indicating an improvement in endothelial function. The ndings support investigation of periodontitis treatment on cardiovascular outcomes. © 2014 Elsevier Ireland Ltd. All rights reserved. Contents 1. Int rod uct ion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2. Met hod s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2.1. Scope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2.2. St udy incl usi on/ exclusion crit eri a . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2.3. Se arc h and scr een ing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 2.4. Qua lit y ass essmen t . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 2.5. Dat a extract ion an d synt hes is . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 3.1. Des cri pti ve re sul ts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 * Corresponding author. Tel.: þ44 20 3456 1276; fax: þ44 20 3456 1137. E-mail address: m.orlandi@ucl.ac.uk (M. Orlandi). 1 These authors equally contributed to the manuscript. Contents lists available at ScienceDirect Atherosclerosis journal homepage: www.elsevier.com/locate/atherosclerosis http://dx.doi.org/10.1016/j.atherosclerosis.2014.06.002 0021-9150/© 2014 Elsevier Ireland Ltd. All rights reserved. Atherosclerosis 236 (2014) 39e46
-
Upload
teresa-mansilla-aguilar -
Category
Documents
-
view
226 -
download
0
Transcript of Periodontiis y Enfermedad Cardiovascular

8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 1/8
Review
Association between periodontal disease and its treatment,ow-mediated dilatation and carotid intima-media thickness: A
systematic review and meta-analysis
Marco Orlandi a , *
, Jeanie Suvan a, Aviva Petrie b, Nikolaos Donos a, Stefano Masi c,Aroon Hingorani d, John Dean eld c , 1, Francesco D ’ Aiuto a , 1
a Unit of Periodontology, UCL Eastman Dental Institute, 256 Gray ' s Inn Road, London WC1X 8LD, United Kingdomb Biostatistics Unit, UCL Eastman Dental Institute, 256 Gray ' s Inn Road, London, United Kingdomc Vascular Physiology Unit, Great Ormond Street Hospital, 34 Great Ormond Street, London, United Kingdomd Faculty of Population Health Sciences, Institute of Cardiovascular Science, UCL, 1 e 19 Torrington Place, London, United Kingdom
a r t i c l e i n f o
Article history:Received 6 April 2014Received in revised form27 May 2014Accepted 4 June 2014Available online 17 June 2014
Keywords:Cardiovascular diseasePeriodontitisCarotid intima-media thickness
Flow-mediated dilatationEndothelial function
a b s t r a c t
Objective: This meta-analysis sought to investigate the association between carotid intima-mediathickness (c-IMT), ow-mediated dilation (FMD) and periodontitis (PD) and to assess the effect of periodontal treatment on c-IMT and FMD.Methods: Electronic database searching, hand searching of bibliographic references of included papers,related reviews, and journals in relation to oral, cardiovascular and ultrasound imaging eld was carriedout. Random effects meta-analyses were performed to investigate the association of co-existence of increased c-IMT, impaired FMD and PD with potential changes in these variables following periodontalintervention.Results: 2009 citations and 101 full text articles were screened, with 35 meeting the review inclusioncriteria of which 22 suitable for quantitative analysis. Meta-analysis demonstrated that the diagnosis of
PD was associated with a mean increase in c-IMT of 0.08 mm (95% C.I. ¼ 0.07 e 0.09) and a mean dif-ference in FMD of 5.1% compared to controls (95% C.I. ¼ 2.08 e 8.11%). A meta-analysis of the effects of periodontal treatment on FMD showed a mean improvement of 6.64% between test and control (95%C.I. ¼ 2.83 e 10.44%).Conclusions: This review demonstrated an association between increased c-IMT, impaired FMD and PD.Data from intervention studies suggested a bene cial effect of periodontal treatment on FMD indicatingan improvement in endothelial function. The ndings support investigation of periodontitis treatment oncardiovascular outcomes.
© 2014 Elsevier Ireland Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.1. Scope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2. Study inclusion/exclusion criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.3. Search and screening . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.4. Quality assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.5. Data extraction and synthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.1. Descriptive results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
* Corresponding author. Tel.: þ 44 20 3456 1276; fax: þ 44 20 3456 1137.E-mail address: [email protected] (M. Orlandi).
1 These authors equally contributed to the manuscript.
Contents lists available at ScienceDirect
Atherosclerosis
j ou rna l homepage : www.e l sev i e r. com/ loca t e / a the rosc le ros i s
http://dx.doi.org/10.1016/j.atherosclerosis.2014.06.002
0021-9150/©
2014 Elsevier Ireland Ltd. All rights reserved.
Atherosclerosis 236 (2014) 39 e 46

8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 2/8
3.1.1. PD and c-IMT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.1.2. PD and FMD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.2. Bias assessment protection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.3. Quantitative results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3.3.1. Mean c-IMT value in individuals with or without PD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43.3.2. Mean FMD values in individuals with or without PD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43.3.3. Effect of periodontal therapy on EDD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6. Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Competing interests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Abbreviation list . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Supplementary data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1. Introduction
Periodontitis (PD) is a chronic oral in ammatory disease initi-ated by the accumulation of a bacterial bio lm on the tooth surfaceand perpetuated by a deregulated local and systemic immune-in ammatory response [1]. Along with dental caries they repre-sent the two major global oral health burdens of our society, withsome forms of PD being detectable in 20% e 50% of the generalpopulation [2] . Inparticular, PD shares a number of risk factors withother non-communicable diseases, including cardiovascular (CV)diseases.
Numerous epidemiological studies have investigated the natureof the association between PD and CV diseases, focusing primarilyon the role of common in ammatory pathways [3] linking the twodiseases, however whether the association is causal is still a matterof debate [4] .
Several studies have reported an association between PD and
increased carotid intima-media thickness (c-IMT), a non-invasivetechnique, which has been shown to correlate with the individualCV risk factor burden as well as the risk of future CV events,including coronary artery disease and stroke [5] . Similarly, severalstudies have reported associations between PD and endothelialdysfunction which occurs at the early stages of atherogenesis asassessed by ow-mediated dilatation (FMD) [6] .
We have undertaken a systematic review and meta-analysisbased on the following question: “ What is the association be-tween PD and vascular function as assessed by c-IMT and FMD andwhat is the impact of PD treatment on these variables in adultsuffering from PD? ”
2. Methods
2.1. Scope
The purpose of the review was to investigate, by means of ameta-analysis: i) whether current data support an association be-tween PD, increased c-IMT and impaired FMD, ii) whether peri-odontal treatment has any effect on these variables and iii) tosummarize the existing evidence of an association between PD (theexposure) and vascular alterations (the outcomes).
PD was de ned to include any measure of disease according toclinical, radiographic and microbiological assessment (includingpocket Probing depth, clinical attachment level, bleeding onprobing, plaque index, gingival index, X-ray and microbiological
results).
Surrogate markers of CV disease eligible for inclusion were: B-ultrasound measurements of c-IMT, expressed as Mean (SD) andFMD as Mean (SD) of the percentage of the brachial artery dilationfollowing the hyperemia induced by 5 min cuff occlusion. Thesample comprised individuals aged 17 years.
2.2. Study inclusion/exclusion criteria
Broad inclusion criteria were set to search for human observa-tional and experimental study designs (cross-sectional, case-control, population surveys, cohort studies, pilot studies,controlled trials and randomized controlled trials).
Comments, letters, editorials, casestudiesand series, newsitems,abstracts not followed by publication and consumer health materialwere excluded, as were studies performed in animals, duplicatedreports, studies providing associations between different markers of CV disease or particular pathogens involved in PD and CV disease,
studies de ning endothelial function with different methodologythan FMD and those providing the IMT in other vascular beds.
2.3. Search and screening
The search strategy was developed using medical subjectheadings (MeSH terms) as well as free text terms and wascustomized as appropriate before application to each database (seeexample in supplemental Table 1).
All publication years through 31st of January 2014 wereincluded. No language or year restrictionswere applied. In addition,bibliographic references of the identi ed papers and previous re-views were hand searched. Online hand searching of issues withinthe past 10 years of some periodontal, CV and imaging journals was
also performed ( supplemental Table 2 ).Two investigators (MO, JS) independently screened titles/ab-
stracts and full text articles were subsequently assessed from thefollowing databases:
F0A7 The Cochrane Oral Health Group 's Trials Register, (wholedatabase to current date)
F0A7 The Cochrane Central Register of Controlled Trials (CENTRAL,whole database at current issue)
F0A7 MEDLINE via OVID, (1946 to present)F0A7 EMBASE via OVID, (1980 to present)F0A7 SCI-EXPANDED via Web of Science, (1900 to present)F0A7 LILACS via VHL, (1982 to present)F0A7 System for Information on Grey Literature in Europe (Open
SIGLE, 1980e
2005)
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 40

8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 3/8
The present article was written according to the PRISMA(Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [7] .
2.4. Quality assessment
Cohort, case-control and cross-sectional studies were assessed
for quality using the validated Newcastlee
Ottawa Quality Assess-ment Scale [8] (Table 1 ).
2.5. Data extraction and synthesis
Data was extracted from all included studies independently andin duplicate (MO, JS). Disagreements were resolved through dis-cussion with a third person (FD).
Data were analyzed using descriptive (evidence tables insupplemental material ) and quantitative (meta-analysis) methods.Statistical analyses were performed using Stata v 11 (StataCorp.2007, TX: StataCorp LP.). Mean differences in both c-IMT and FMDwere used to perform meta-analyses of the difference in individualswith PD compared to controls in observational and intervention
studies. If data were not available in the publications, the missinginformation was obtained directly from the authors. Heterogeneitywas assessed using the c 2-based Q-statistic method and consid-ered signi cant if p < 0.05 and quanti ed with the I-squared sta-tistic [9] . The pooled estimates of the mean differences werecalculated using random effects models to take into account po-tential inter-study heterogeneity and to adopt a more conservativeapproach. The pooled effect was considered signi cant if p < 0.05.Small study bias was examined using a funnel plot and Egger 's test.Sensitivity analyses were performed to understand the in uence of individual studies, by omitting one study each time in a series of meta-analyses to identify in uential studies.
3. Results
2066 hits were obtained from electronic searches and 2 paperswere located from online and hand searching of mentioned jour-nals of interest. Following removal of 59 duplicates, 2009 poten-tially suitable titles and abstracts were screened. After excluding
1906 non-relevant citations, 101 publications were selected andretrieved for full-text review ( Fig. 1).
Among these full text articles and abstracts, 66 were excluded.This resulted in a total of 35 publications eligible to be included inthe systematic review. Of these, 22 papers were included in themeta-analyses. 6 publications did not contain the full informationnecessary for the meta-analyses [10 e 15] , however it was possibleto obtain the required data from the authors. All 35 studies reportedevidence on an association between investigated CV diseasemarkers and PD.
3.1. Descriptive results
3.1.1. PD and c-IMT 26 publications included measures of c-IMT of which 25 were
observational studies ( Supplemental Table 3 ) and 1 interventiontrial ( Supplemental Table 4 ). There was considerable variation interms of de nition of PD, observed population, study sample size,age range, carotid segments studied and de nition of c-IMTamongthe studies. 16 publications were included for further analysis as 10did not provide estimates that were comparable to the other
studies. The de nition of the carotid segments was the majorsource of heterogeneity. Only one uncontrolled longitudinal studyevaluated the impact of periodontal treatment on c-IMT in in-dividuals with mild or moderate PD. After a follow up of 6 and 12months this study showed a reduction of c-IMT compared to theBaseline measurements [16] .
3.1.2. PD and FMDThe relationship between PD and FMD was investigated in 10
articles of which 3 were observational ( Supplemental Table 5 ), and7 intervention studies ( Supplemental Table 6 ). 2 randomizedcontrolled trials were excluded for the meta-analysis as endothelialfunction was assessed using acetylcholine [17,18] and one inter-vention pilot trial had no control group [19] .
Table 1Quality assessment observational studies (Newcastle e Ottawa Scale).
Selection Comparability Exposure Overall
Case-control c-IMT Leivadaros 2005 *** ** *** ********(8/9)Soder 2005 **** *** *******(7/9)Soder 2007 **** *** *******(7/9)Cairo 2008 *** ** *** ********(8/9)Lopez J 2012 *** *** *****(6/9)Zahnd 2012 *** ** *** ******(6/9)Puhar 2012 *** *** ******(6/9)Cross-sectional c-IMT Beck 2001 *** ** *** ********(8/9)Franeck 2006 *** *** ******(6/9)Li X 2009 *** *** ******(6/9)Ylostalo 2010 *** * *** *******(7/9)LI P 2011 *** *** ******(6/9)Vieira 2011 *** * *** *******(7/9)Franek 2012 *** ** *** ********(8/9)Pinho 2013 *** **Hayashida 2013 *** *** ********(8/9)Case-control-FMDAmar 2003 ** ** *** ********(8/9)Ruiz 2013 *** *** ******(6/9)Cross-sectional-FMDLi 2011 *** *** ******(6/9)
Fig. 1. Flow chart of the study selection procedure.
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 41

8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 4/8
3.2. Bias assessment protection
According to the Newcastle e Ottawa Quality Assessment Scale,the majority of the studies were categorized as low or medium riskof bias ( Table 1 ). There was a discrepancy in the periodontal di-agnoses, de nition of controls and not a uniform adjustment forpotential confounders. In case-control studies, individuals includedin control groups were recruited from hospital rather than from thecommunity, introducing a possible selection bias. All cross-sectional studies were considered comparable in quality and thesame was for controlled trials.
3.3. Quantitative results
3.3.1. Mean c-IMT value in individuals with or without PD7 out of 10 case-control studies comparing differences in c-IMT
between individuals with and without PD were included in ameta-analysis [13,15,20 e 24] . 3 publications were excluded; 2papers reported data on the same population analyzed in previ-ous publications [25,26] and 1 study resulted biased in the se-lection of controls [27] . 9 out of 15 cross-sectional studies
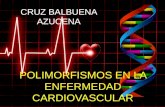
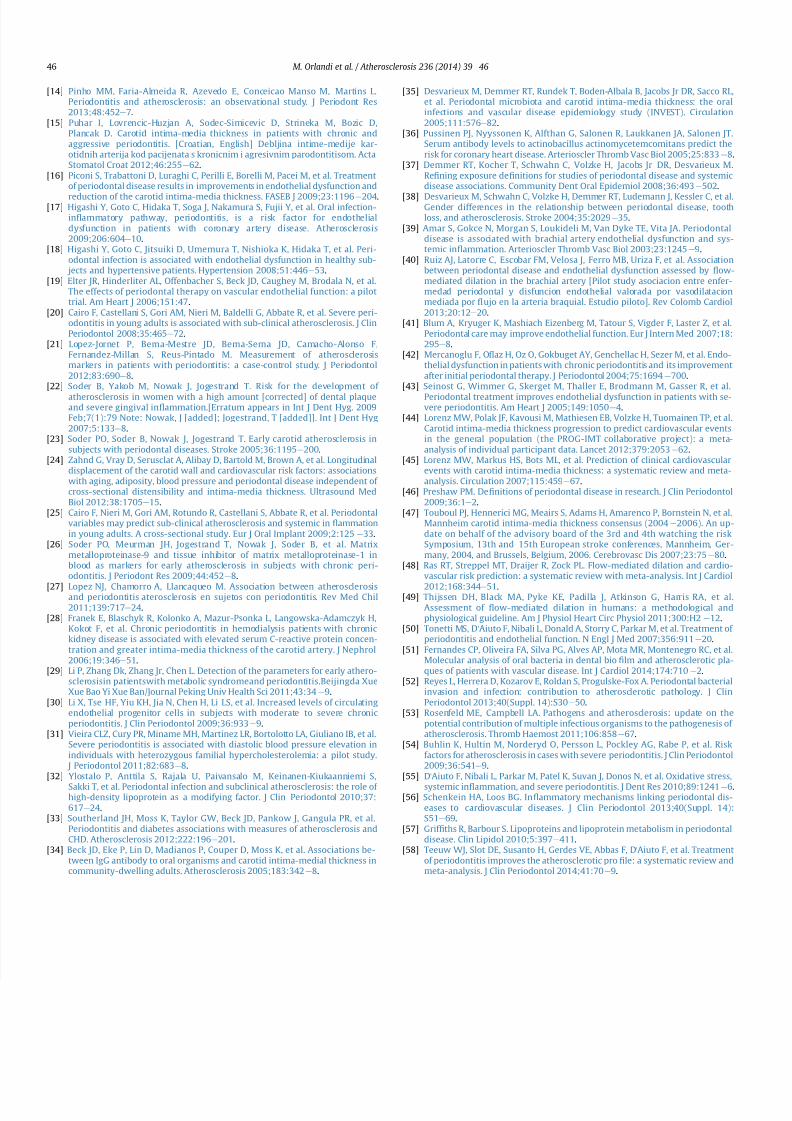
[10 e 12,14,28 e 32] were suitable for a meta-analysis. 6 studieswere excluded for the following reasons: 1 performed analysis onthe same sub-sample of another included study [33] , 3 related c-IMT to antibody levels of periodontal pathogens [34 e 36] , 2calculated c-IMT values across quintiles or tertiles of periodontalde nitions [37,38] . Li P. et al. [29] assessed c-IMT in two differentsamples, individuals with or without metabolic syndrome andwith or without PD. We therefore considered the data as 2separate studies. In some of the included studies, individuals weredivided in different groups according to PD severity. In this case,the severe PD group was chosen for the analysis. The mean dif-ference in c-IMT values in the individual studies ranged from -0.04 mm to 0.19 mm. Adopting a random-effects model ( Fig. 2), ameta-analysis (2021 cases, 3431 controls) indicated a higher c-IMT in individuals with PD (0.08 mm 95% CI [0.07, 0.09], p < 0.0001) compared to controls. A chi-squared test for hetero-geneity and the I-squared index did not show statistically signif-icant heterogeneity ( p ¼ 0.922 and I 2 ¼ 0%). Funnel-plot analysis(Fig. 3A) did not show evidence of bias using the Egger test of symmetry ( p ¼ 0.876) and sensitivity analysis did not suggest thepresence of in uential studies.
3.3.2. Mean FMD values in individuals with or without PDDifferences in FMD (%) between individual with or without
PD, reported by 3 observational studies [29,39,40] and baselinedata from 3 controlled trials [41 e 43] , were included in the meta-analysis. Li P. et al. assessed FMD in two different samples, in-dividuals with or without metabolic syndrome and with or
without PD [29] . We therefore considered the data as 2 separatestudies. Individual studies mean difference in percentage of endothelial dependent dilatation (EDD) ranged from 1.59% to12.48%.
In individuals (155 subjects) with PD, FMD was lower on averageby 5.1% (95% CI 2.08, 8.11], p < 0.001) compared to controls (136subjects) ( Fig. 4). A chi-squared test for heterogeneity and the I-squared index indicated that there was statistically signi cantheterogeneity ( p ¼ 0.000 and I 2 ¼ 80.1%).
Funnel-plot analysis ( Fig. 3B) suggested asymmetry that couldbe evidence of publication bias, although the Egger test ( p ¼ 0.43)did notsupport this, possibly because of lowpower due to the smallnumber of studies. The funnel plot asymmetry may be attributed tothe high heterogeneity among the studies. A sensitivity analysis did
indicate that there were not any in uential studies.
3.3.3. Effect of periodontal therapy on EDDIt was possible to analyze the summary difference in mean
FMD (%) between test and control after periodontal treatment in3 of 6 controlled trials [41e 43] (147 individuals) ( Fig. 5). Meanimprovement in FMD after periodontal intervention ranged fromto 3.7 e 9.3%. The overall summary estimate of the mean increasein FMD based on a random-effects model was 6.64% (95% CI [2.83to 10.44], p < 0.0001). A chi-squared test for heterogeneity andthe I-squared index showed statistically signi cant heterogeneity( p ¼ 0.011 and I 2 ¼ 78%). The Egger test didn 't show a small studyeffect ( p ¼ 0.956) and sensitivity analysis identi ed two in u-ential studies potentially related to the small number of includedtrials.
4. Discussion
Our ndings indicate that PD is associated with greater c-IMTand impaired FMD and that periodontal treatment improvesendothelial function. Despite the number of reports on the topic,this is the rst systematic review and meta-analysis linking PD tospeci c CV surrogate outcomes in the general population. Theseassociations emphasize the importance of oral health as a commonunder-recognized factor increasing CV risk in individuals.
Our analysis relates to c-IMT measurements from 5452 (2021cases, 3431 controls) individuals and demonstrates that those withPD have, on average, a greater c-IMT (0.08 mm) compared withcontrols. Despite the small magnitude of this difference, currentevidence suggests that in the general population the mean esti-mates of c-IMT progression range from 0.001 to 0.030 mm per year[44] . Individuals with PD therefore exhibit greater burden of sub-clinical atherosclerosis compared to controls. Evidence suggeststhat per every 0.1 mm difference in c-IMT, the relative risk of futuremyocardial infarction increases of 1.15 times (95% CI, 1.12 e 1.17) andfor stroke increases of 1.18 times (95% CI, 1.16 e 1.21) [45] . A numberof traditional CV risk factors however are linked to c-IMT pro-gression: age, gender, systolic blood pressure, high-density lipo-
protein cholesterol, smoking, diabetes, hypertension treatment,and total cholesterol. Clearly PD shares most of these risk factorswith atherosclerosis and therefore it is dif cult to discern the po-tential impact of PD alone on the progression of c-IMT. The lack of auniform adjustment for all these confounders in the studiesincluded in our meta-analysis could have also reduced the accuracyof our results.
Despite the low level of statistical heterogeneity detected in ouranalyses (I-squared 0%) the robustness of our ndings could beaffected by differences in the research protocols (i.e. clinical het-erogeneity). The diagnosis of PD and c-IMT assessment criteriavaried considerably throughout the studies included. PD wasassessed using different criteria ranging from validated clinicalmeasures such as clinical attachment level and pockets probing
depth to self-de ned criteria showing the lack of a uniform de -nition of PD [46] . It should be also considered that there is not auniform de nition of severe periodontitis included in the manu-scripts reviewed as well as based on a variety of clinical periodontalparameters with different threshold levels. This could also add ontothe variability of the results presented because the populationcombined could not be relevant to study samples of differentperiodontal severity and extent. In addition, we could not groupindividuals with PD according to disease severity (mild, moderateand severe) as in the majority of the studies such differentiationwas not performed. We therefore followed a conservative approachby comparing healthy versus severe PD individuals. This could haveresulted in an underestimation of the reported associations. As theprevalence of PD is relatively high in the general population, the
identi cation of PD subgroups at increased CV risk would help in
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 42
8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 5/8
reducing possible costs associated with large scale screening pro-grams and further research is needed.
We identi ed multiple sources of clinical heterogeneity for c-
IMT. A recent consensus paper [47] recommends measurement of c-IMT in plaque-free areas and we did not nd explicit statementsabout this methodological aspect in any of the studies. The recentpublication of guidelines for c-IMT measurement is likely toimprove consistency of the technique in future studies.
We identi ed only one longitudinal study evaluating the impactof periodontal treatment on c-IMT in people with mild/moderatePD. 6 and 12 months following periodontal treatment, a statisticallysigni cant reduction in c-IMT compared to baseline measurementswas reported [16] . These ndings could support a potential causalassociation between PD and subclinical atherosclerosis but theabsence of a control group, inclusion of CV disease-free individualsand the lack of multiple measurements of the carotid thickness,
make causal inferences dif cult. Findings will need to be con rmedin larger, controlled trials including a high CV risk population (e.g.greater c-IMT).
The relationship between FMDof the brachial arteryand PD wasalso an objective of the present review. FMD is related to thepathogenesis of atheroma and provides information regarding theearly stage of its evolution. Endothelial function and speci callyFMD can also predict future CV disease outcomes. A recent meta-analysis reported that for every point decrease in FMD, future CV disease risk increases of 10% [48] .
The meta-analysis gathered data from baseline measurementsof 3 controlled trials [41 e 43] and 3 observational studies [29,39,40]showing a mean difference of 5.1% in FMD in individuals with PDcompared to controls and a mean increase of 6.64% followingperiodontal treatment. We included only 3 controlled trials asstudy design and the methodology in assessing FMD differed
Fig. 3. Association between periodontitis, c-IMT (3-A) and FMD (3-B). Funnel plots of observational studies.
Fig. 2. Association between Periodontitis and Carotid Intima-Media Thickness (c-IMT) Difference of c-IMT means between individuals with periodontitis versus controls inobservational studies. Horizontal lines representing 95% CI; lower diamond represents the overall effect size, random effects models. sscase sample size cases, sscontrols sample sizecontrols.
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 43

8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 6/8
considerably among trials examined. Indeed FMD average baselinevalues ranged from 4.1% to 8.4%. Additional sources of variationwere identi ed including underlying health status, different eth-nicities and length of follow-up ranging from 6 weeks to 3 months.Lastly, assessment of endothelial function with FMDis notfree frommethodological, physiological and technical factors that can in u-ence the validity, reproducibility and interpretation of results inclinical research [49] . As con rmation of our cautious interpreta-tion of the evidence, a statistically signi cant high level of het-erogeneity was observed (80.1% for case-control and 78% forintervention trials).
Nevertheless evidence supporting the bene cial role of peri-odontal treatment in improving endothelial function derives from 3RCT [17,18,50] ; two of which were conducted assessing endothelialfunction with a more invasive technique (response of brachialblood ow to acetylcholine injection) and both showed a statisti-cally signi cant improvement after periodontal therapy [17,18] . Thethird one is the only RCT reporting on measure of endothelialfunction with FMD in people with severe PD [50] . Our groupconcluded that 6 months after intensive periodontal therapy(associated with a substantial improvement in the gingival condi-tion) individuals had a 2.0% rise of FMD (95% CI 1.2 to 2.8; p < 0.001)
Fig. 4. Association between Periodontitis and Flow Mediated Dilatation (FMD) Difference of the FMD means between individuals with periodontitis versus controls in observationalstudies. Horizontal lines representing 95% CI; diamond represents the overall effect size, random effects models. sscase sample size cases, sscontrols sample size controls.
Fig. 5. Association between Periodontal Treatment and Flow Mediated Dilatation (FMD) Difference of the FMD means before and after periodontal treatment in controlled clinical
trials. Horizontal lines representing 95% CI; diamond represents the overall effect size, random effects models. sscase sample size cases, sscontrols sample size controls.
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 44

8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 7/8
on average compared to controls. Our interpretation of these re-sults and the meta-analysis collectively supports a causal associa-tion between PD and endothelial dysfunction. Several pathwayshave been proposed to support a potential involvement of peri-odontitis in the development and progression of atherosclerosis.Firstly a direct role of oral bacteria has been hypothesized followingpathogen 's DNA being detected in atheromas [51] . Periodontalbacteria could directly invade endothelial cells and promote avascular in ammatory state [52] . In addition bacterial end-products could trigger an innate [53] or auto-immune response(HSPs auto-antigens) [54] . Secondly, patients suffering from peri-odontitis exhibit higher systemic in ammation than controls [55] .Locally produced in ammatory by-products damped into the sys-temic circulation coupled with a systemic low-grade hepatic acutephase response to periodontitis could result in a state endothelialdysfunction and further promote the atherosclerotic in ammatoryprocess [56] . Lastly, cases with periodontitis tend to show a pro-atherogenic lipid pro le including alterations of lipoprotein func-tion [57] . A recent systematic review and meta-analysis [58]con rmed that periodontal therapy improves individuals ' in am-matory and lipidic pro le, especially in those with other co-morbidities (i.e. diabetes and cardiovascular diseases). Neverthe-less the impact of periodontal therapy on the individual cardio-metabolic pro le is still a matter of debate and should warrantfurther investigation.
5. Conclusion
In conclusion this review suggests that PD is associated withgreater subclinical atherosclerosis as assessed by increased c-IMT,an independent predictor of CV events in high-risk populations.There is evidence of an impaired FMD, which is restored by peri-odontal treatment in individuals suffering from by PD. Robustprospective studies are needed to improve our understanding of the mechanisms underlying these associations. It is encouraged theuse of standardized protocols to measure both c-IMT and FMD aswell as of universally-accepted case de nitions of PD as to facilitatefurther research.
6. Contributors
MO and JS screened the titles and abstracts, assessed trials forinclusion and trial quality, and extracted data. AP performed sta-tistical analyses. MO wrote the draft manuscript. All authorscontributed to writing, reviewing, or revising the paper.
Funding
The study did not receive speci c funding.
Competing interests
All authors declare no con ict of interest, no support from anyorganization for the submitted work; Francesco D 'Aiuto holds aClinical Senior Lectureship Award supported by the UK ClinicalResearch Collaboration. Marco Orlandi holds a UCL Impact Awardpartially supported with a fellowship grant by Johnson and JohnsonConsumer Services EAME Limited. All authors work at UCL, whichreceived a proportion of funding from the Department of Health 'sNational Institute of Health Research (NIHR) Biomedical ResearchCentres funding scheme. Authors declare no relationship with in-dustry; no other relationships or activities that could appear to
have in uenced the submitted work.
Acknowledgments
We are sincerely grateful to Prof Offenbacher (University of North Carolina, Chapel Hill, NC), Prof. Loos (Academic Center forDentistry Amsterdam, Amsterdam, The Netherlands.), Prof. Pussi-nen (University of Helsinki, Finland) and Prof. Franek (CentralClinical Hospital MSWiA, Warsaw, Poland), Dr Pinho (UniversityFernando Pessoa, Porto, Portugal), Prof. Saito (Nagasaki UniversityGraduate School of Biomedical Sciences, Japan) and Dr Puhar(University of Zagreb, Croatia) for generously sharing their datawith us.
Abbreviation list
c-IMT carotid intima media thicknessCV cardiovascularCI con dence intervalEDD endothelial dependent dilatationFMD ow mediated dilatationPD periodontal diseaseRCT randomized controlled trialsSD standard deviationVRFs vascular risk factors
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.atherosclerosis.2014.06.002 .
References
[1] Pihlstrom B, Michalowicz B, Johnson N. Periodontal diseases. Lancet 2005;366:1809 e 20 .
[2] Dye BA. Global periodontal disease epidemiology. Periodontol 2000 2012;58:10 e 25 .
[3] Khader YS, Albashaireh ZS, Alomari MA. Periodontal diseases and the risk of coronary heart and cerebrovascular diseases: a meta-analysis. J Periodontol
2004;75:1046 e 53 .[4] Lockhart PB, Bolger AF, Papapanou PN, Osinbowale O, Trevisan M, Levison ME,
et al. Periodontal disease and atherosclerotic vascular disease: does the evi-dence support an independent association?: a scienti c statement from theAmerican heart association. Circulation 2012;125:2520 e 44 .
[5] Baldassarre D, Hamsten A, Veglia F, de Faire U, Humphries SE, Smit AJ, et al.Measurements of carotid intima-media thickness and of interadventitiacommon carotid diameter improve prediction of cardiovascular events: re-sults of the IMPROVE (Carotid intima media thickness [IMT] and IMT-progression as predictors of vascular events in a high risk european popula-tion) study. J Am Coll Cardiol 2012;60:1489 e 99 .
[6] Charakida M, Masi S, Luscher TF, Kastelein JJ, Dean eld JE. Assessment of atherosclerosis: the role of ow-mediated dilatation. Eur Heart J 2010;31:2854 e 61 .
[7] Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. ThePRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration.BMJ 2009;339:b2700 .
[8] Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessmentof the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol2010;25:603 e 5.
[9] Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. StatMed 2002;21:1539 e 58 .
[10] Beck JD, Elter JR, Heiss G, Couper D, Mauriello SM, Offenbacher S. Relationshipof periodontal disease to carotid artery intima-media wall thickness: theatherosclerosis risk in communities (ARIC) study. Arterioscler Thromb VascBiol 2001;21:1816 e 22 .
[11] Franek E, Januszkiewicz-Caulier J, Blach A, Napora M, Jedynasty K,Budlewski T, et al. Intima-media thickness and other markers of atheroscle-rosis in patients with type 2 diabetes and periodontal disease. Kardiologia Pol2012;70:7 e 13 .
[12] Hayashida H, Saito T, Kawasaki K, Kitamura M, Furugen R, Iwasaki T, et al.Association of periodontitis with carotid artery intima-media thickness andarterial stiffness in community-dwelling people in Japan: The NagasakiIslands study. Atherosclerosis 2013;229:186 e 91 .
[13] Leivadaros E, van der Velden U, Bizzarro S, Ten Heggeler JMAG, Gerdes VEA,Hoek FJ, et al. A pilot study into measurements of markers of atherosclerosis
in periodontitis. J Periodontology 2005;76:121e
8.
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 45
8/20/2019 Periodontiis y Enfermedad Cardiovascular
http://slidepdf.com/reader/full/periodontiis-y-enfermedad-cardiovascular 8/8
[14] Pinho MM, Faria-Almeida R, Azevedo E, Conceicao Manso M, Martins L.Periodontitis and atherosclerosis: an observational study. J Periodont Res2013;48:452 e 7.
[15] Puhar I, Lovrencic-Huzjan A, Sodec-Simicevic D, Strineka M, Bozic D,Plancak D. Carotid intima-media thickness in patients with chronic andaggressive periodontitis. [Croatian, English] Debljina intime-medije kar-otidnih arterija kod pacijenata s kronicnim i agresivnim parodontitisom. ActaStomatol Croat 2012;46:255 e 62 .
[16] Piconi S, Trabattoni D, Luraghi C, Perilli E, Borelli M, Pacei M, et al. Treatmentof periodontal disease results in improvements in endothelial dysfunction and
reduction of the carotid intima-media thickness. FASEB J 2009;23:1196 e 204 .[17] Higashi Y, Goto C, Hidaka T, Soga J, Nakamura S, Fujii Y, et al. Oral infection-
in ammatory pathway, periodontitis, is a risk factor for endothelialdysfunction in patients with coronary artery disease. Atherosclerosis2009;206:604 e 10 .
[18] Higashi Y, Goto C, Jitsuiki D, Umemura T, Nishioka K, Hidaka T, et al. Peri-odontal infection is associated with endothelial dysfunction in healthy sub- jects and hypertensive patients. Hypertension 2008;51:446 e 53 .
[19] Elter JR, Hinderliter AL, Offenbacher S, Beck JD, Caughey M, Brodala N, et al.The effects of periodontal therapy on vascular endothelial function: a pilottrial. Am Heart J 2006;151:47 .
[20] Cairo F, Castellani S, Gori AM, Nieri M, Baldelli G, Abbate R, et al. Severe peri-odontitis in young adults is associated with sub-clinical atherosclerosis. J ClinPeriodontol 2008;35:465 e 72 .
[21] Lopez-Jornet P, Berna-Mestre JD, Berna-Serna JD, Camacho-Alonso F,Fernandez-Millan S, Reus-Pintado M. Measurement of atherosclerosismarkers in patients with periodontitis: a case-control study. J Periodontol2012;83:690 e 8.
[22] Soder B, Yakob M, Nowak J, Jogestrand T. Risk for the development of atherosclerosis in women with a high amount [corrected] of dental plaqueand severe gingival in ammation.[Erratum appears in Int J Dent Hyg. 2009Feb;7(1):79 Note: Nowak, J [added]; Jogestrand, T [added]]. Int J Dent Hyg2007;5:133 e 8.
[23] Soder PO, Soder B, Nowak J, Jogestrand T. Early carotid atherosclerosis insubjects with periodontal diseases. Stroke 2005;36:1195 e 200 .
[24] Zahnd G, Vray D, Serusclat A, Alibay D, Bartold M, Brown A, et al. Longitudinaldisplacement of the carotid wall and cardiovascular risk factors: associationswith aging, adiposity, blood pressure and periodontal disease independent of cross-sectional distensibility and intima-media thickness. Ultrasound MedBiol 2012;38:1705 e 15 .
[25] Cairo F, Nieri M, Gori AM, Rotundo R, Castellani S, Abbate R, et al. Periodontalvariables may predict sub-clinical atherosclerosis and systemic in ammationin young adults. A cross-sectional study. Eur J Oral Implant 2009;2:125 e 33 .
[26] Soder PO, Meurman JH, Jogestrand T, Nowak J, Soder B, et al. Matrixmetalloproteinase-9 and tissue inhibitor of matrix metalloproteinase-1 inblood as markers for early atherosclerosis in subjects with chronic peri-odontitis. J Periodont Res 2009;44:452 e 8.
[27] Lopez NJ, Chamorro A, Llancaqueo M. Association between atherosclerosisand periodontitis aterosclerosis en sujetos con periodontitis. Rev Med Chil2011;139:717 e 24 .
[28] Franek E, Blaschyk R, Kolonko A, Mazur-Psonka L, Langowska-Adamczyk H,Kokot F, et al. Chronic periodontitis in hemodialysis patients with chronickidney disease is associated with elevated serum C-reactive protein concen-tration and greater intima-media thickness of the carotid artery. J Nephrol2006;19:346 e 51 .
[29] Li P, Zhang Dk, Zhang Jr, Chen L. Detection of the parameters for early athero-sclerosisin patientswith metabolic syndromeand periodontitis.Beijingda XueXue Bao Yi Xue Ban/Journal Peking Univ Health Sci 2011;43:34 e 9.
[30] Li X, Tse HF, Yiu KH, Jia N, Chen H, Li LS, et al. Increased levels of circulatingendothelial progenitor cells in subjects with moderate to severe chronicperiodontitis. J Clin Periodontol 2009;36:933 e 9.
[31] Vieira CLZ, Cury PR, Miname MH, Martinez LR, Bortolotto LA, Giuliano IB, et al.Severe periodontitis is associated with diastolic blood pressure elevation inindividuals with heterozygous familial hypercholesterolemia: a pilot study. J Periodontol 2011;82:683 e 8.
[32] Ylostalo P, Anttila S, Rajala U, Paivansalo M, Keinanen-Kiukaanniemi S,Sakki T, et al. Periodontal infection and subclinical atherosclerosis: the role of high-density lipoprotein as a modifying factor. J Clin Periodontol 2010;37:617 e 24 .
[33] Southerland JH, Moss K, Taylor GW, Beck JD, Pankow J, Gangula PR, et al.Periodontitis and diabetes associations with measures of atherosclerosis andCHD. Atherosclerosis 2012;222:196 e 201 .
[34] Beck JD, Eke P, Lin D, Madianos P, Couper D, Moss K, et al. Associations be-tween IgG antibody to oral organisms and carotid intima-medial thickness incommunity-dwelling adults. Atherosclerosis 2005;183:342 e 8.
[35] Desvarieux M, Demmer RT, Rundek T, Boden-Albala B, Jacobs Jr DR, Sacco RL,et al. Periodontal microbiota and carotid intima-media thickness: the oralinfections and vascular disease epidemiology study (INVEST). Circulation2005;111:576 e 82 .
[36] Pussinen PJ, Nyyssonen K, Alfthan G, Salonen R, Laukkanen JA, Salonen JT.Serum antibody levels to actinobacillus actinomycetemcomitans predict therisk for coronary heart disease. Arterioscler Thromb Vasc Biol 2005;25:833 e 8.
[37] Demmer RT, Kocher T, Schwahn C, Volzke H, Jacobs Jr DR, Desvarieux M.Re ning exposure de nitions for studies of periodontal disease and systemicdisease associations. Community Dent Oral Epidemiol 2008;36:493 e 502 .
[38] Desvarieux M, Schwahn C, Volzke H, Demmer RT, Ludemann J, Kessler C, et al.Gender differences in the relationship between periodontal disease, toothloss, and atherosclerosis. Stroke 2004;35:2029 e 35 .
[39] Amar S, Gokce N, Morgan S, Loukideli M, Van Dyke TE, Vita JA. Periodontaldisease is associated with brachial artery endothelial dysfunction and sys-temic in ammation. Arterioscler Thromb Vasc Biol 2003;23:1245 e 9.
[40] Ruiz AJ, Latorre C, Escobar FM, Velosa J, Ferro MB, Uriza F, et al. Associationbetween periodontal disease and endothelial dysfunction assessed by ow-mediated dilation in the brachial artery [Pilot study asociacion entre enfer-medad periodontal y disfuncion endothelial valorada por vasodilatacionmediada por ujo en la arteria braquial. Estudio piloto]. Rev Colomb Cardiol2013;20:12 e 20 .
[41] Blum A, Kryuger K, Mashiach Eizenberg M, Tatour S, Vigder F, Laster Z, et al.Periodontal care may improve endothelial function. Eur J Intern Med 2007;18:295 e 8.
[42] Mercanoglu F, O az H, Oz O, Gokbuget AY, Genchellac H, Sezer M, et al. Endo-thelial dysfunction in patients with chronic periodontitis and its improvementafter initial periodontal therapy. J Periodontol 2004;75:1694 e 700 .
[43] Seinost G, Wimmer G, Skerget M, Thaller E, Brodmann M, Gasser R, et al.Periodontal treatment improves endothelial dysfunction in patients with se-vere periodontitis. Am Heart J 2005;149:1050 e 4.
[44] Lorenz MW, Polak JF, Kavousi M, Mathiesen EB, Volzke H, Tuomainen TP, et al.Carotid intima-media thickness progression to predict cardiovascular eventsin the general population (the PROG-IMT collaborative project): a meta-analysis of individual participant data. Lancet 2012;379:2053 e 62 .
[45] Lorenz MW, Markus HS, Bots ML, et al. Prediction of clinical cardiovascularevents with carotid intima-media thickness: a systematic review and meta-analysis. Circulation 2007;115:459 e 67 .
[46] Preshaw PM. De nitions of periodontal disease in research. J Clin Periodontol2009;36:1 e 2.
[47] Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al.Mannheim carotid intima-media thickness consensus (2004 e 2006). An up-date on behalf of the advisory board of the 3rd and 4th watching the riskSymposium, 13th and 15th European stroke conferences, Mannheim, Ger-many, 2004, and Brussels, Belgium, 2006. Cerebrovasc Dis 2007;23:75 e 80 .
[48] Ras RT, Streppel MT, Draijer R, Zock PL. Flow-mediated dilation and cardio-vascular risk prediction: a systematic review with meta-analysis. Int J Cardiol
2012;168:344 e 51 .[49] Thijssen DH, Black MA, Pyke KE, Padilla J, Atkinson G, Harris RA, et al.Assessment of ow-mediated dilation in humans: a methodological andphysiological guideline. Am J Physiol Heart Circ Physiol 2011;300:H2 e 12 .
[50] Tonetti MS, D 'Aiuto F, Nibali L, Donald A, Storry C, Parkar M, et al. Treatment of periodontitis and endothelial function. N Engl J Med 2007;356:911 e 20 .
[51] Fernandes CP, Oliveira FA, Silva PG, Alves AP, Mota MR, Montenegro RC, et al.Molecular analysis of oral bacteria in dental bio lm and atherosclerotic pla-ques of patients with vascular disease. Int J Cardiol 2014;174:710 e 2.
[52] Reyes L, Herrera D, Kozarov E, Roldan S, Progulske-Fox A. Periodontal bacterialinvasion and infection: contribution to atherosclerotic pathology. J ClinPeriodontol 2013;40(Suppl. 14):S30 e 50 .
[53] Rosenfeld ME, Campbell LA. Pathogens and atherosclerosis: update on thepotential contribution of multiple infectious organisms to the pathogenesis of atherosclerosis. Thromb Haemost 2011;106:858 e 67 .
[54] Buhlin K, Hultin M, Norderyd O, Persson L, Pockley AG, Rabe P, et al. Riskfactors for atherosclerosis in cases with severe periodontitis. J Clin Periodontol2009;36:541 e 9.
[55] D'Aiuto F, Nibali L, Parkar M, Patel K, Suvan J, Donos N, et al. Oxidative stress,systemic in ammation, and severe periodontitis. J Dent Res 2010;89:1241 e 6.
[56] Schenkein HA, Loos BG. In ammatory mechanisms linking periodontal dis-eases to cardiovascular diseases. J Clin Periodontol 2013;40(Suppl. 14):S51 e 69 .
[57] Grif ths R, Barbour S. Lipoproteins and lipoprotein metabolism in periodontaldisease. Clin Lipidol 2010;5:397 e 411 .
[58] Teeuw WJ, Slot DE, Susanto H, Gerdes VE, Abbas F, D 'Aiuto F, et al. Treatmentof periodontitis improves the atherosclerotic pro le: a systematic review andmeta-analysis. J Clin Periodontol 2014;41:70 e 9.
M. Orlandi et al. / Atherosclerosis 236 (2014) 39 e 46 46