
Neoadyuvancia en Cáncer de - Doctaforum · •Inicio precoz del tto sistémico •Downstaging...
72
Transcript of Neoadyuvancia en Cáncer de - Doctaforum · •Inicio precoz del tto sistémico •Downstaging...

Neoadyuvancia en Cáncer de Mama
E. Ciruelos
Servicio de Oncología Médica
Hospital 12 de Octubre
- Excelentes tasas de respuestas en CM localmente avanzado
e inflamatorio (tratamiento estándar) Chia S, JCO 2008; 26: 786
Tasa alta de respuesta clínica (60-70%)
Tasa baja de respuesta patológica (20%)
- Mayor tasa de cirugía conservadora (resultado estético)
- Supervivencia equivalente a la quimioterapia
adyuvante (SLE, SG)
Justificación
Tratamiento neoadyuvante
del cáncer de mama
VENTAJAS
• Inicio precoz del tto sistémico
• Downstaging (operabilidad, qx conservadora)
• Test in vivo del efecto antitumoral
• Valor pronóstico de pCR*
• Oportunidad de marcadores surrogados
• Desarrollo nuevos fármacos
Tratamiento neoadyuvante
del cáncer de mama
DESVENTAJAS
• Diagnóstico inicial según biopsia/cilindro
(no refleja heterogeneidad del tumor)
• No estadiaje histopatológico
• Riesgo de enfermedad multifocal residual
• Requiere Unidad Multidisciplinar
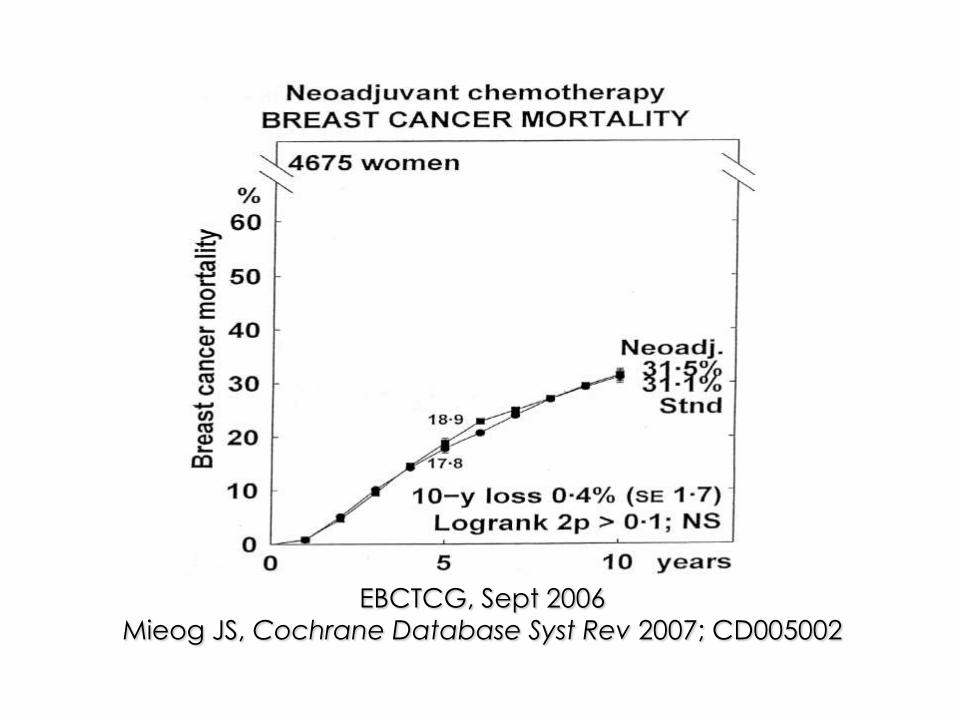
EBCTCG, Sept 2006
Mieog JS, Cochrane Database Syst Rev 2007; CD005002
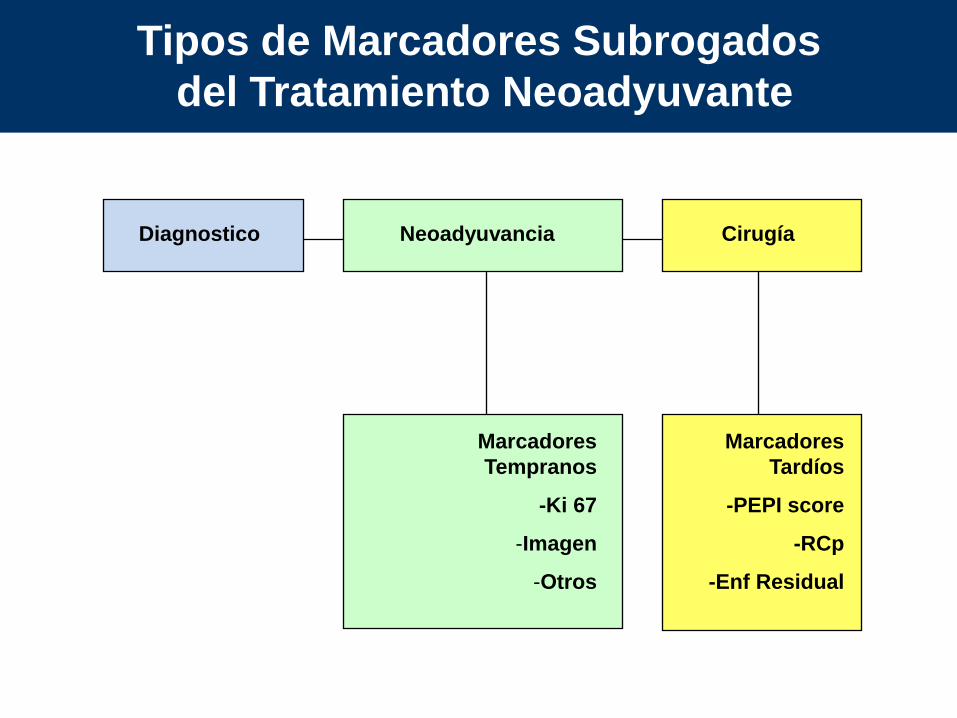
Tipos de Marcadores Subrogados
del Tratamiento Neoadyuvante
Diagnostico Neoadyuvancia Cirugía
Marcadores
Tempranos
-Ki 67
-Imagen
-Otros
Marcadores
Tardíos
-PEPI score
-RCp
-Enf Residual
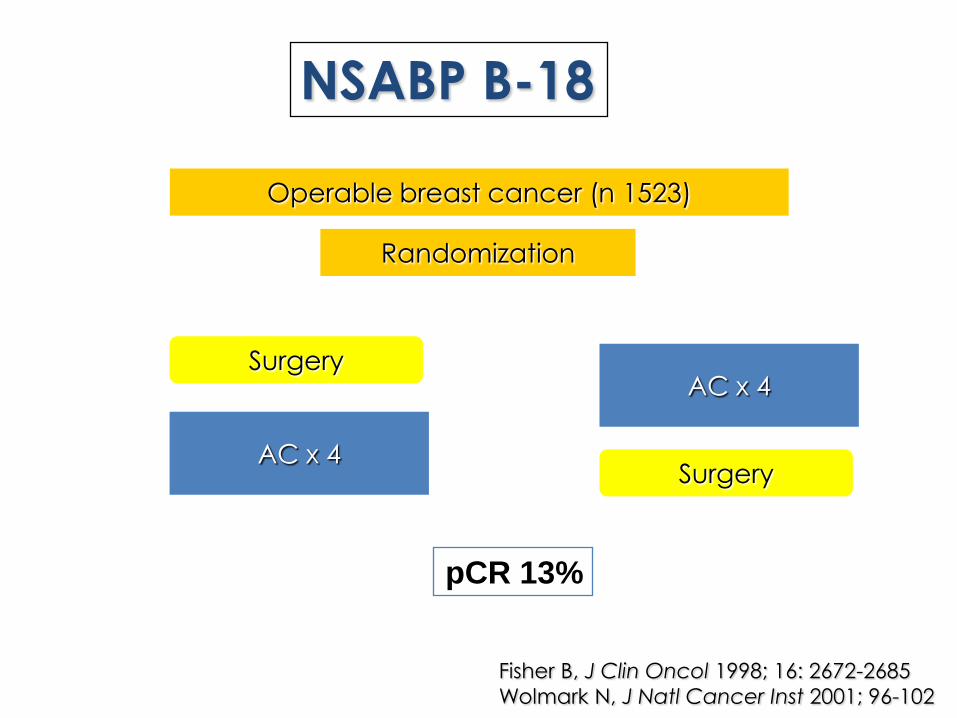
NSABP B-18
Operable breast cancer (n 1523)
Randomization
AC x 4 Surgery
SurgeryAC x 4
Fisher B, J Clin Oncol 1998; 16: 2672-2685
Wolmark N, J Natl Cancer Inst 2001; 96-102
pCR 13%
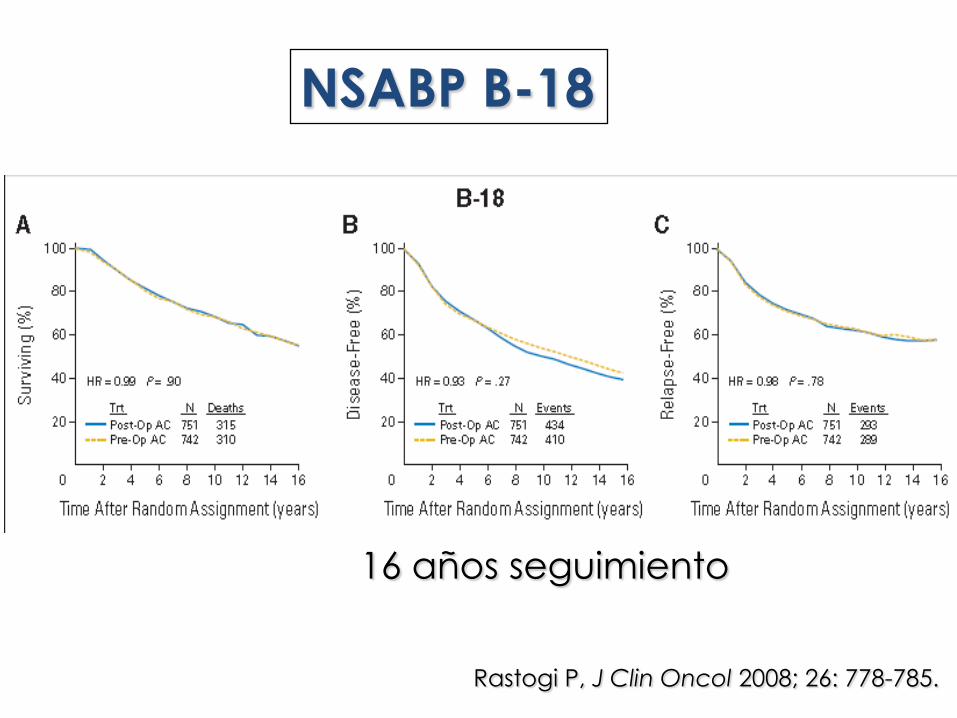
NSABP B-18
Rastogi P, J Clin Oncol 2008; 26: 778-785.
16 años seguimiento

NSABP B-18
Rastogi P, J Clin Oncol 2008; 26: 778-785.
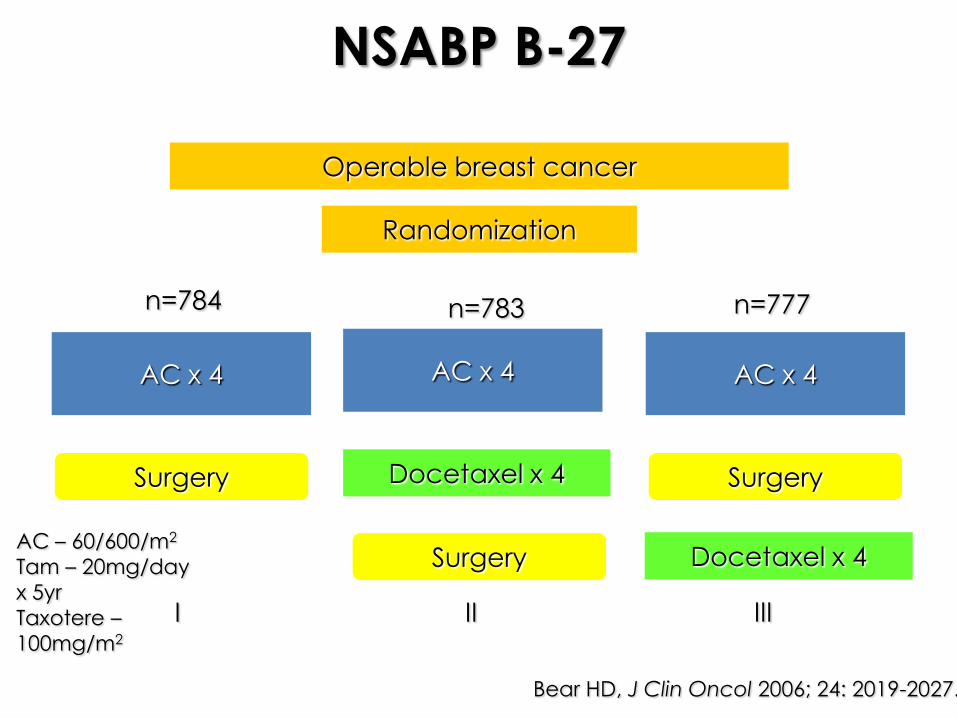
NSABP B-27
Operable breast cancer
Randomization
I II III
AC x 4 AC x 4 AC x 4
Surgery Docetaxel x 4 Surgery
Surgery Docetaxel x 4
n=784 n=777n=783
AC – 60/600/m2
Tam – 20mg/day
x 5yr
Taxotere –
100mg/m2
Bear HD, J Clin Oncol 2006; 24: 2019-2027.
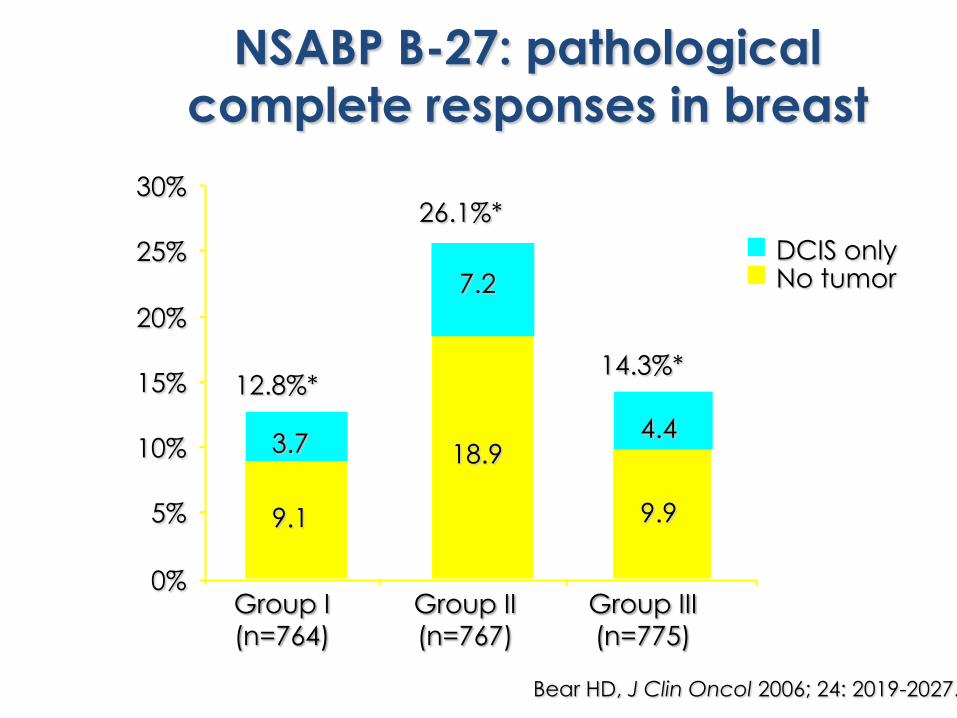
NSABP B-27: pathological
complete responses in breast
12.8%*
26.1%*
14.3%*
9.1
3.7 18.9
7.2
9.9
4.4
0%
5%
10%
15%
20%
25%
30%
Group I
(n=764)Group II
(n=767)Group III
(n=775)
DCIS onlyNo tumor
Bear HD, J Clin Oncol 2006; 24: 2019-2027.
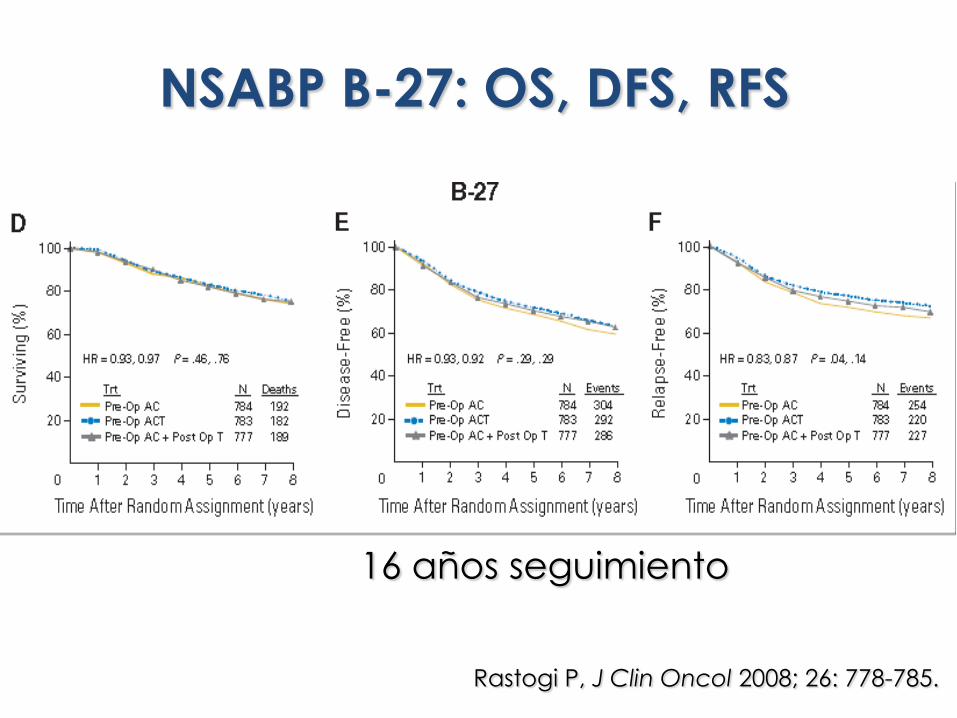
NSABP B-27: OS, DFS, RFS
Rastogi P, J Clin Oncol 2008; 26: 778-785.
16 años seguimiento
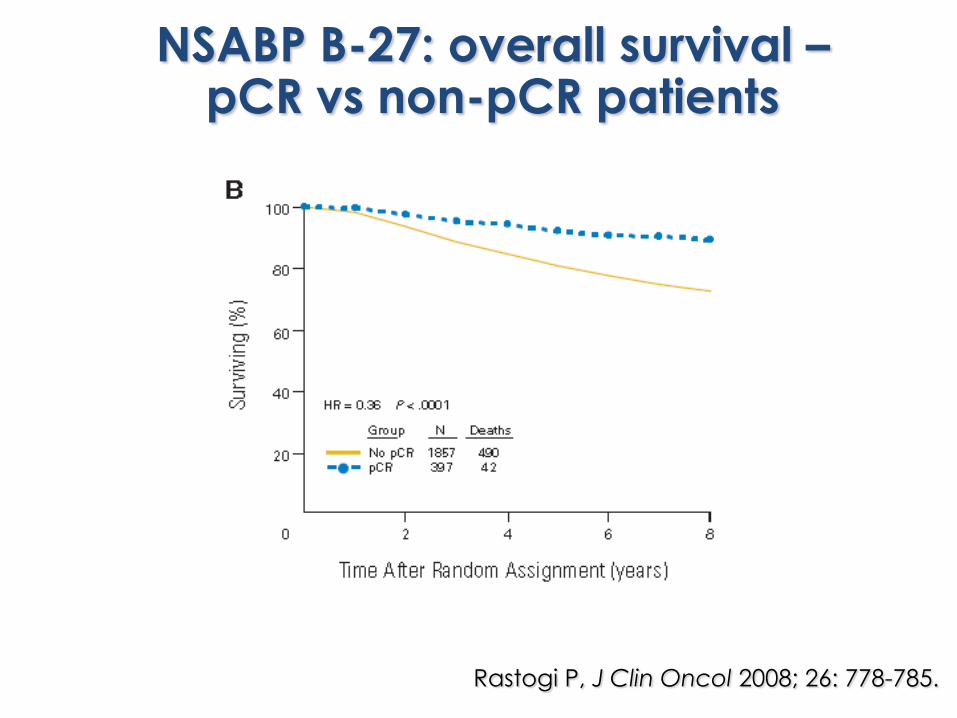
Rastogi P, J Clin Oncol 2008; 26: 778-785.
NSABP B-27: overall survival –pCR vs non-pCR patients
Definiciones de pCR
• Ausencia de tumor invasivo en mama (NSABP)• Ausencia de tumor invasivo en mama y axila (MDA)• Ausencia de tumor invasivo y no invasivo
en mama y axila (GBG)• Symmans (MDA; GEICAM)
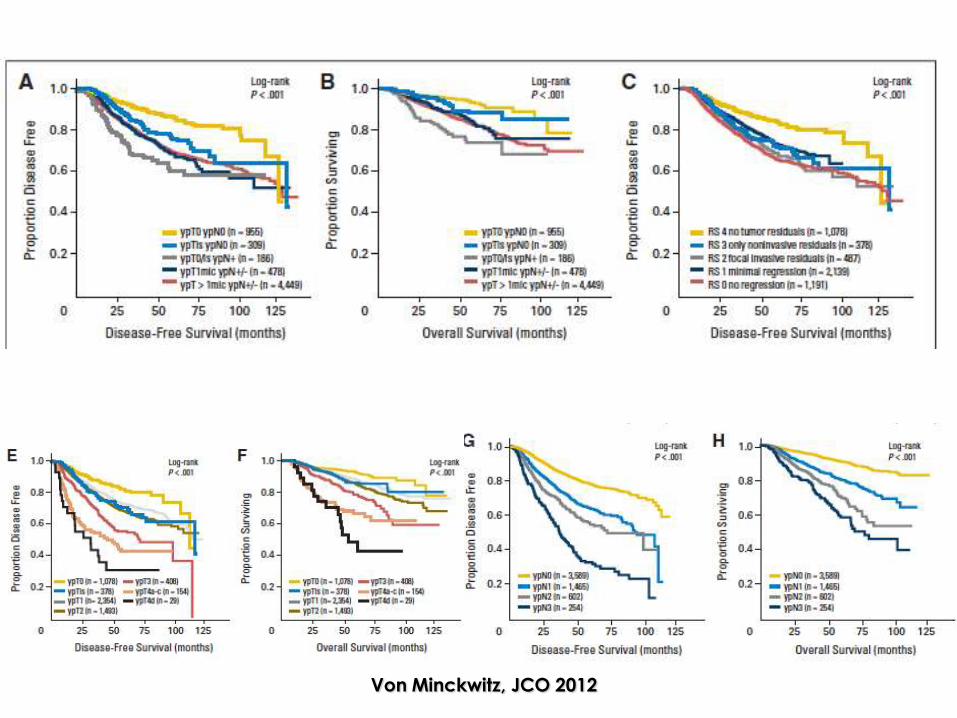
Von Minckwitz, JCO 2012
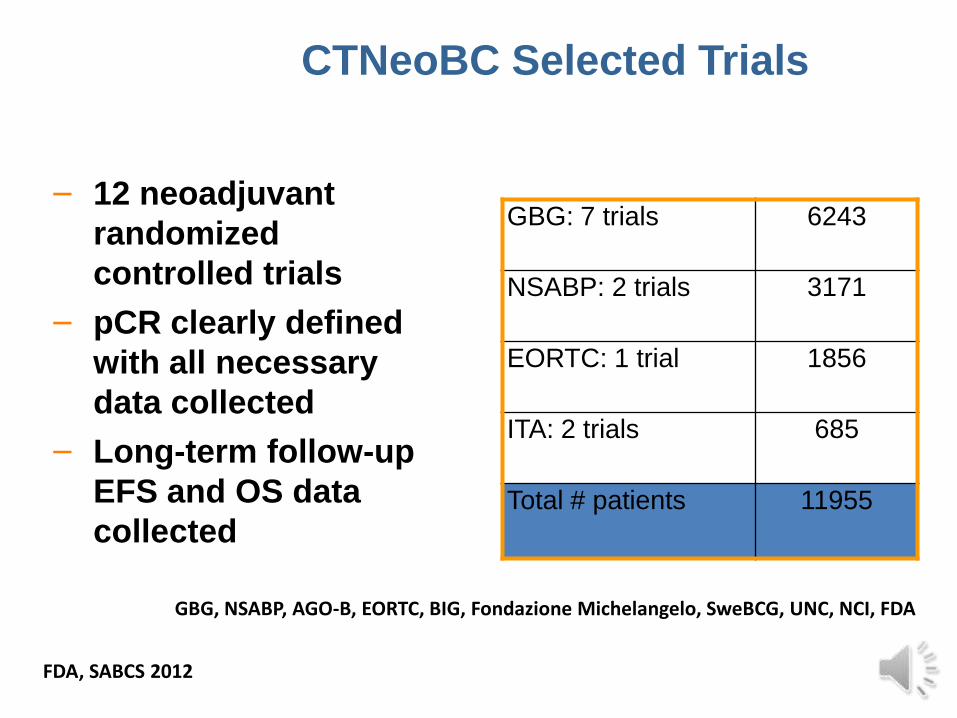
CTNeoBC Selected Trials
– 12 neoadjuvant
randomized
controlled trials
– pCR clearly defined
with all necessary
data collected
– Long-term follow-up
EFS and OS data
collected
GBG: 7 trials 6243
NSABP: 2 trials 3171
EORTC: 1 trial 1856
ITA: 2 trials 685
Total # patients 11955
GBG, NSABP, AGO-B, EORTC, BIG, Fondazione Michelangelo, SweBCG, UNC, NCI, FDA
CTNeoBCFDA, SABCS 2012
Considerations FDA For Future
Trials:
pCR Definition
A pCR definition that includes the
assessment of the axillary nodes
(ypT0ypN0 or ypT0/isypN0) should be
used in future trials.
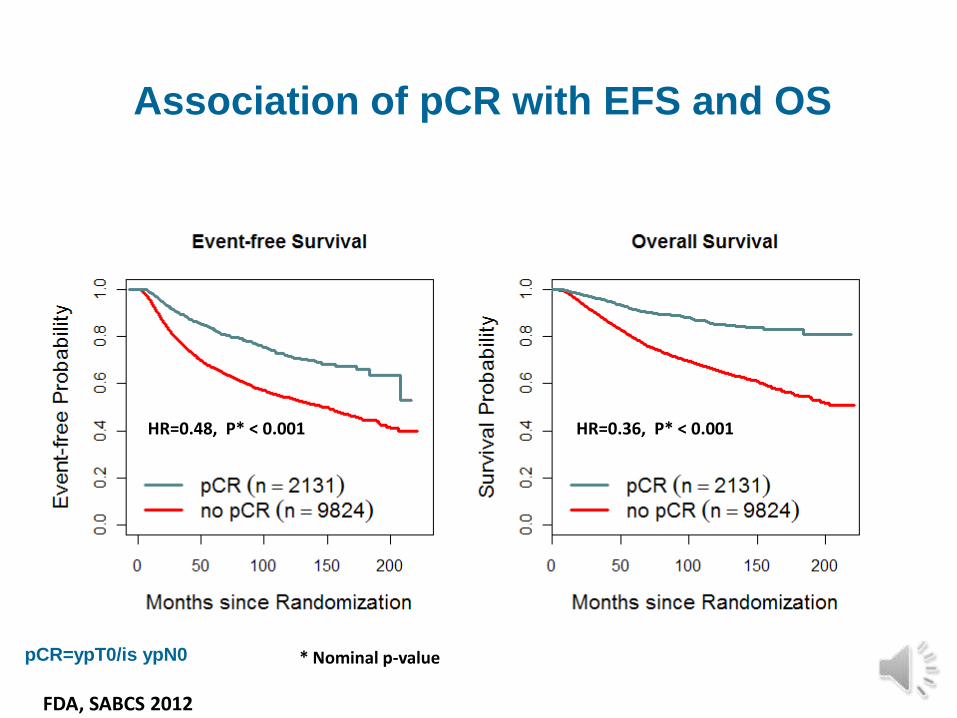
pCR=ypT0/is ypN0
HR=0.48, P* < 0.001 HR=0.36, P* < 0.001
* Nominal p-value
Association of pCR with EFS and OS
CTNeoFDA, SABCS 2012
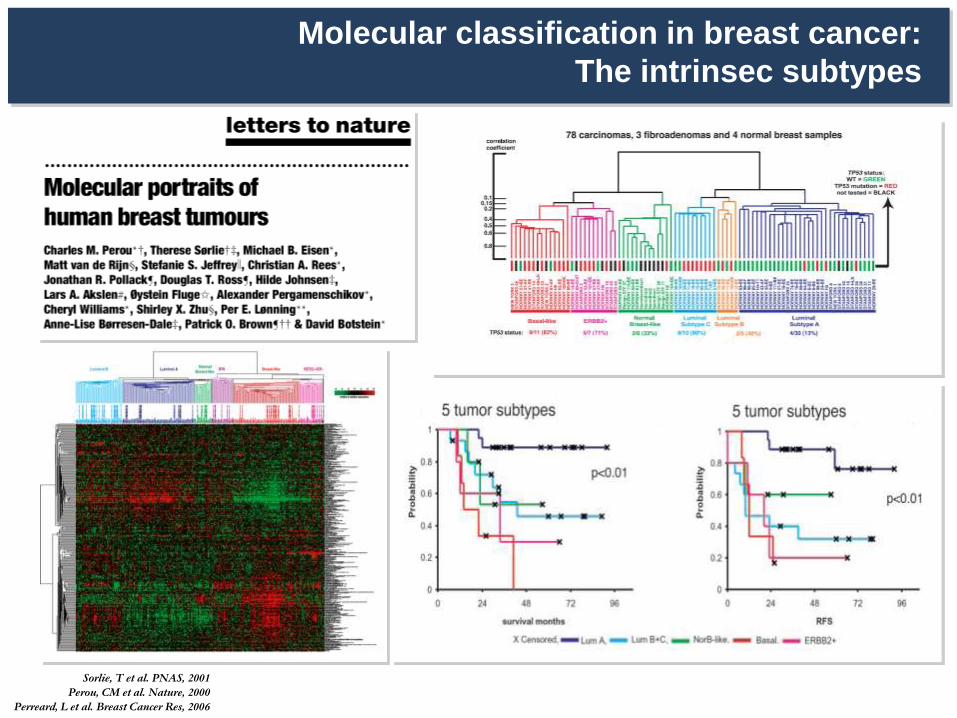
Molecular classification in breast cancer:
The intrinsec subtypes
Sorlie, T et al. PNAS, 2001
Perou, CM et al. Nature, 2000
Perreard, L et al. Breast Cancer Res, 2006
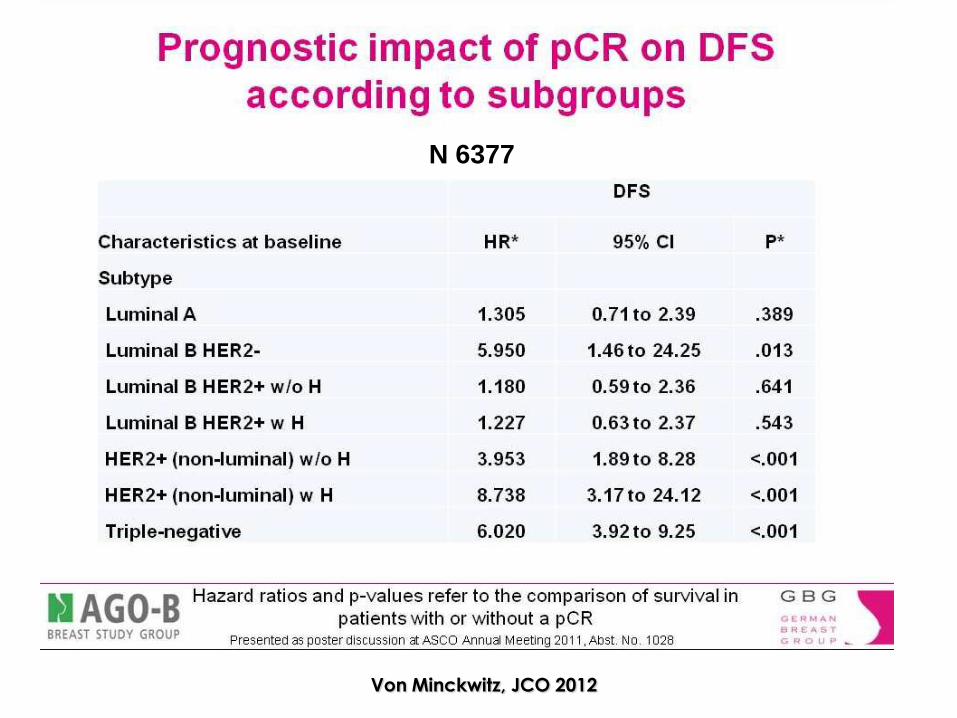
Von Minckwitz, JCO 2012
N 6377
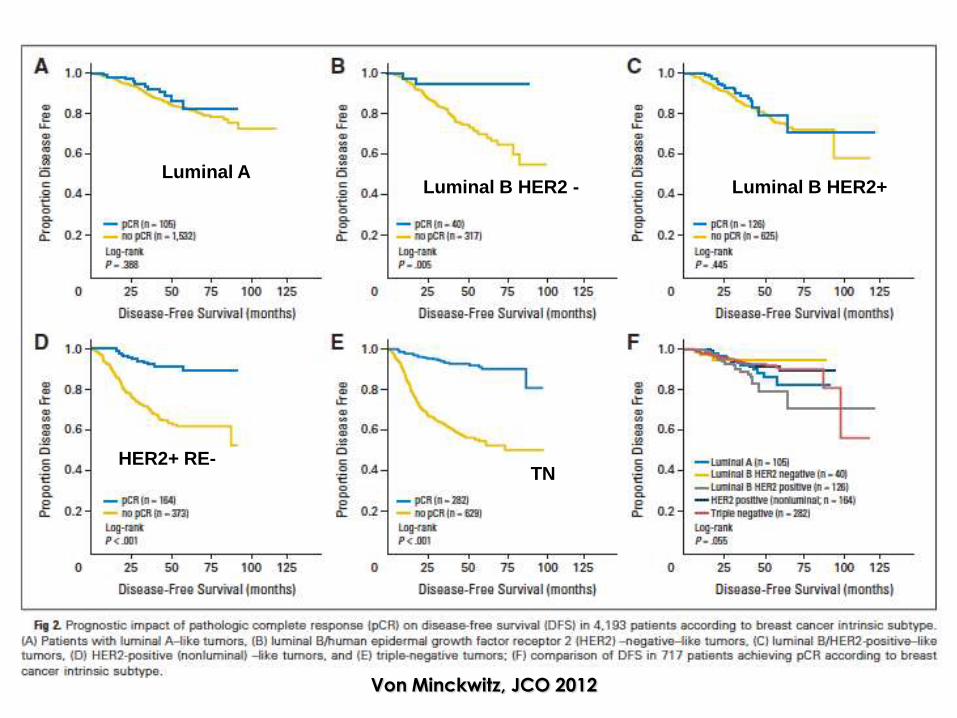
Von Minckwitz, JCO 2012
Luminal ALuminal B HER2 - Luminal B HER2+
HER2+ RE-TN
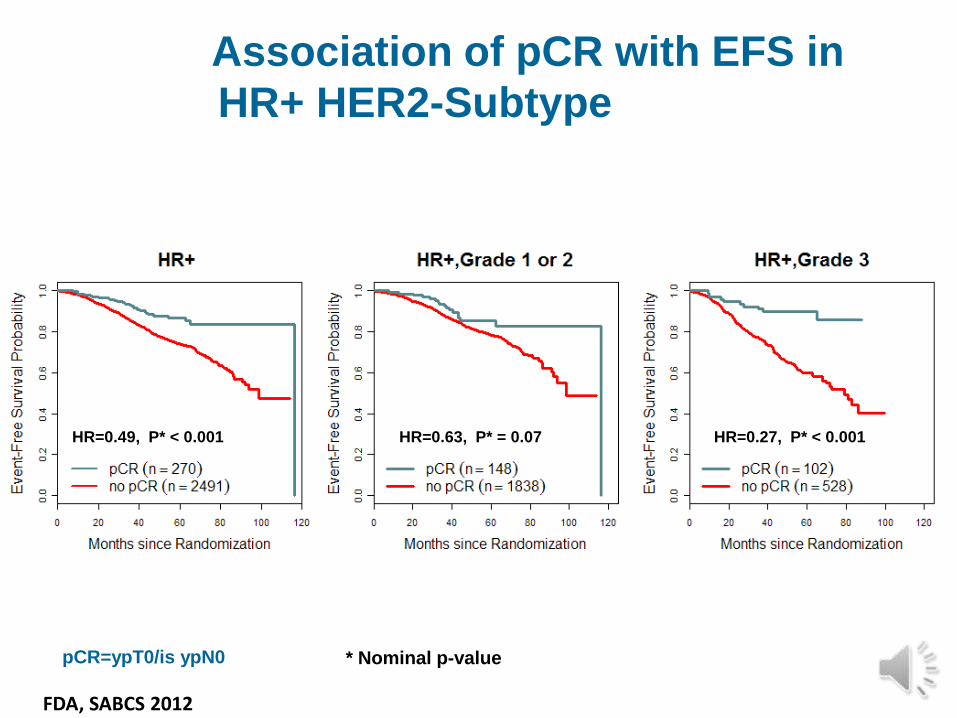
pCR=ypT0/is ypN0
HR=0.49, P* < 0.001 HR=0.63, P* = 0.07 HR=0.27, P* < 0.001
* Nominal p-value
Association of pCR with EFS in
HR+ HER2-SubtypeHR+ HER2-
Subtype
FDA, SABCS 2012
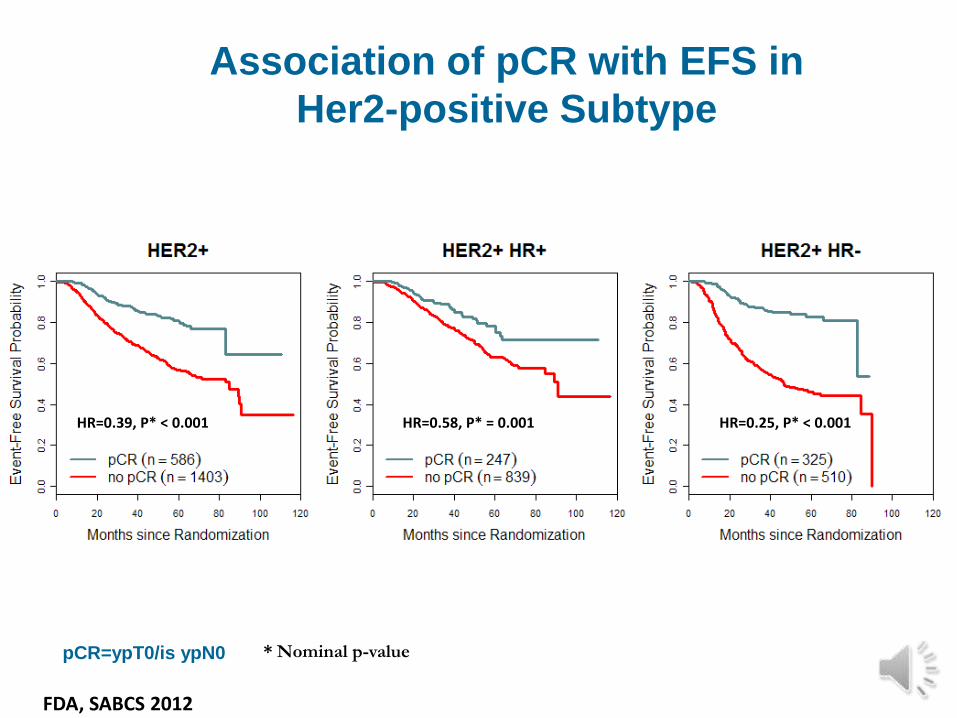
Association of pCR with EFS in
Her2-positive Subtype
pCR=ypT0/is ypN0
HR=0.39, P* < 0.001 HR=0.58, P* = 0.001 HR=0.25, P* < 0.001
* Nominal p-value
CTNeoFDA, SABCS 2012
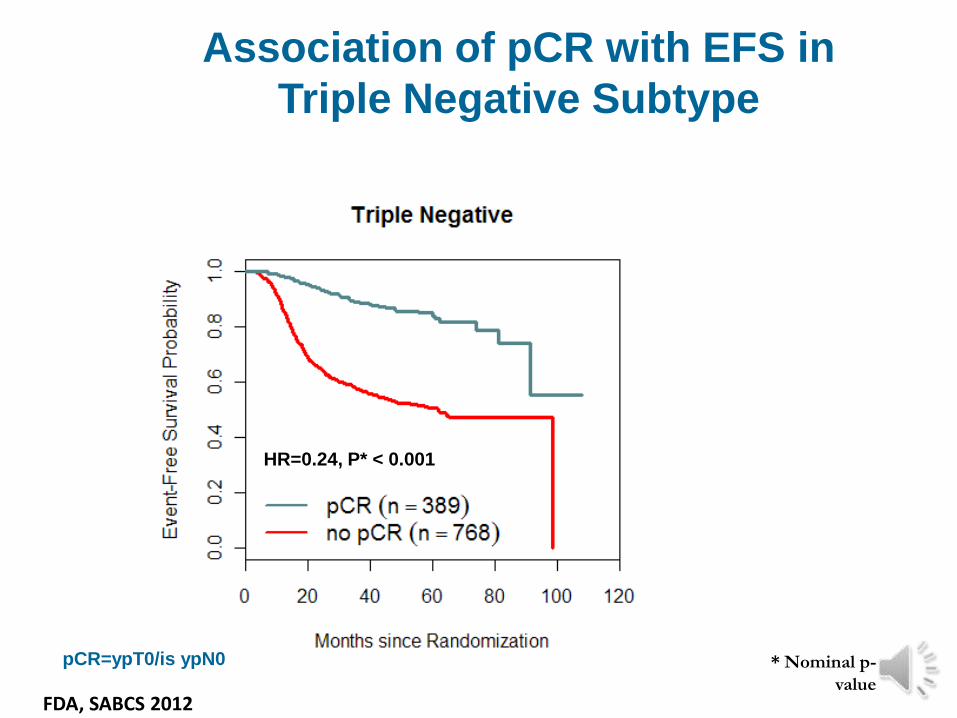
HR=0.24, P* < 0.001
pCR=ypT0/is ypN0 * Nominal p-
value
Association of pCR with EFS in
Triple Negative Subtype
FDA, SABCS 2012
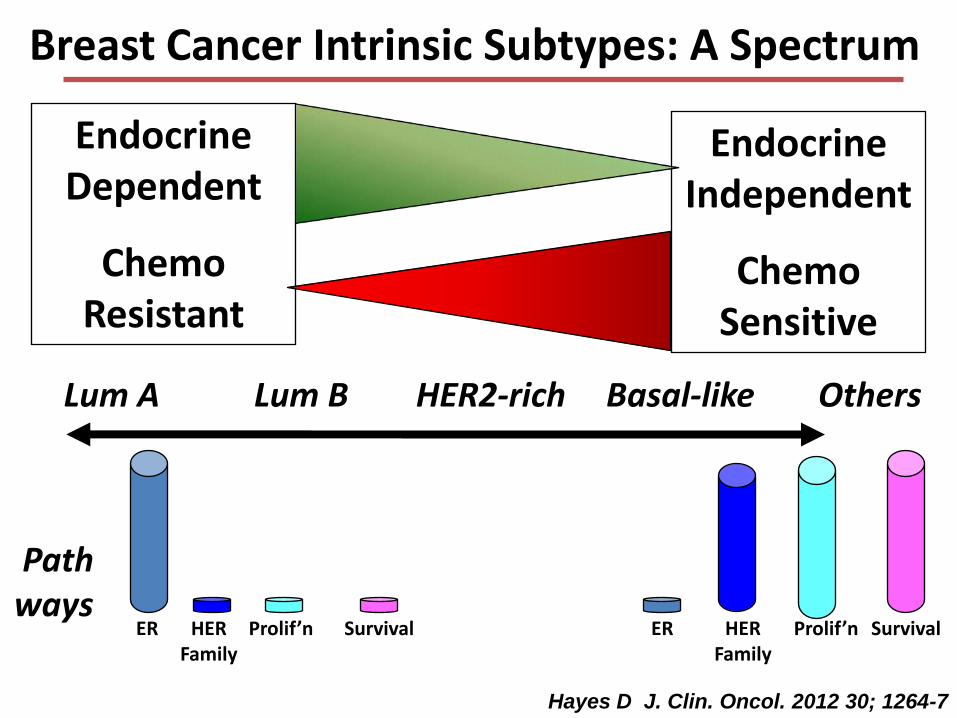
Breast Cancer Intrinsic Subtypes: A Spectrum
Endocrine Dependent
Chemo Resistant
Endocrine Independent
Chemo Sensitive
Pathways
ER HER Family
SurvivalProlif’n ER SurvivalProlif’nHER Family
Lum A Lum B HER2-rich Basal-like Others
Hayes D J. Clin. Oncol. 2012 30; 1264-7
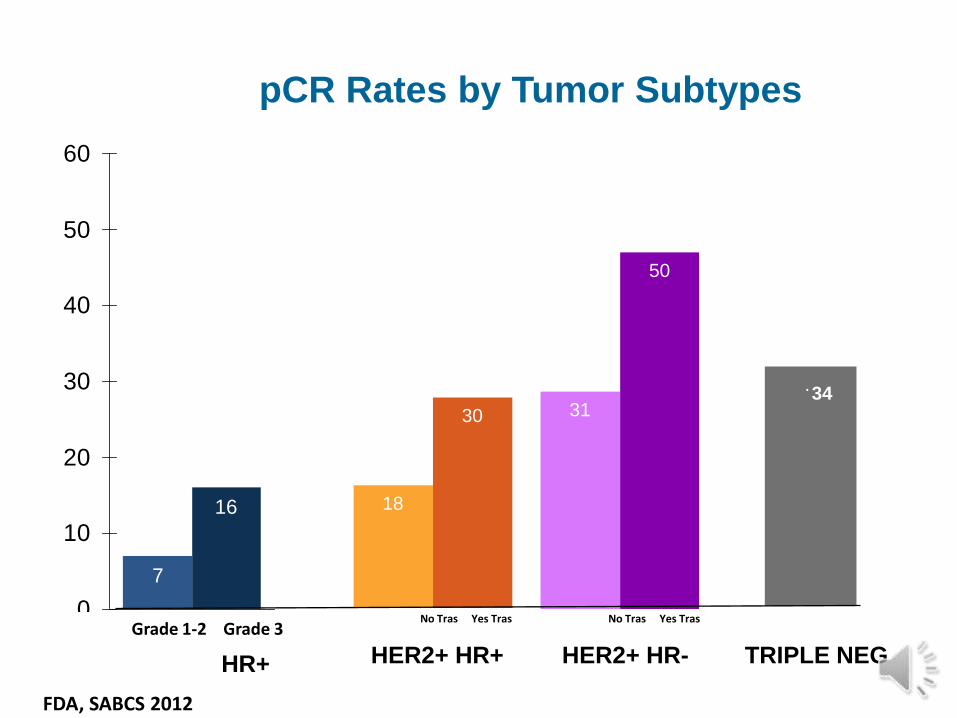
7
16
0
10
20
30
40
50
60
18
30 31
50
.
Grade 1-2 Grade 3
HR+
No Tras Yes Tras
HER2+ HR+
No Tras Yes Tras
HER2+ HR- TRIPLE NEG
34
pCR Rates by Tumor Subtypes
FDA, SABCS 2012
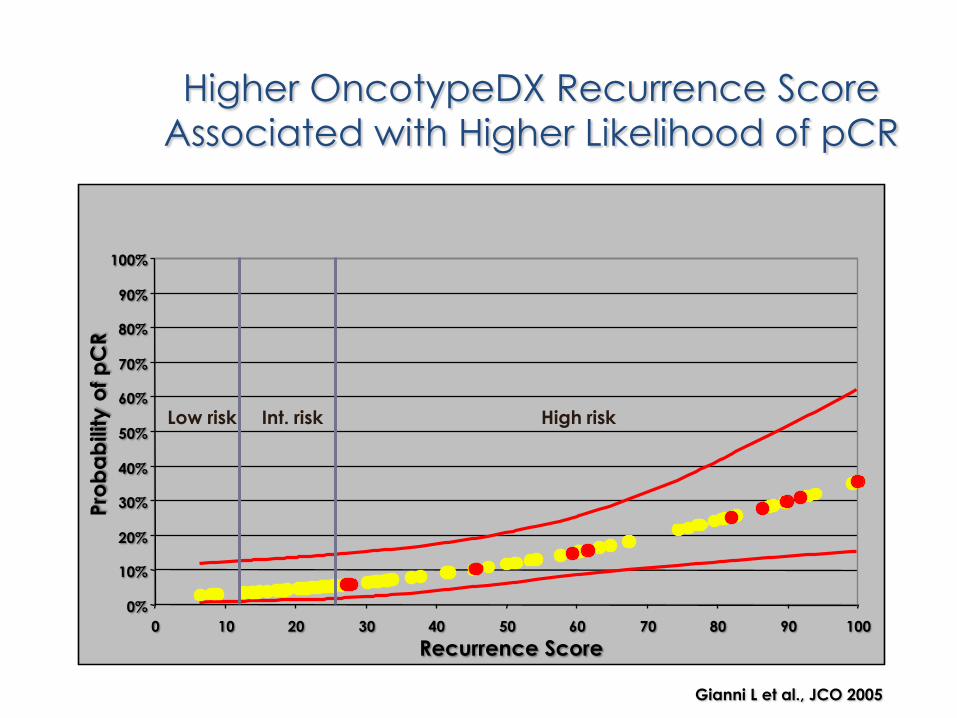
Higher OncotypeDX Recurrence Score
Associated with Higher Likelihood of pCR
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 10 20 30 40 50 60 70 80 90 100
Recurrence Score
Pro
ba
bility
of
pC
R
Low risk Int. risk High risk
Gianni L et al., JCO 2005
HER2+
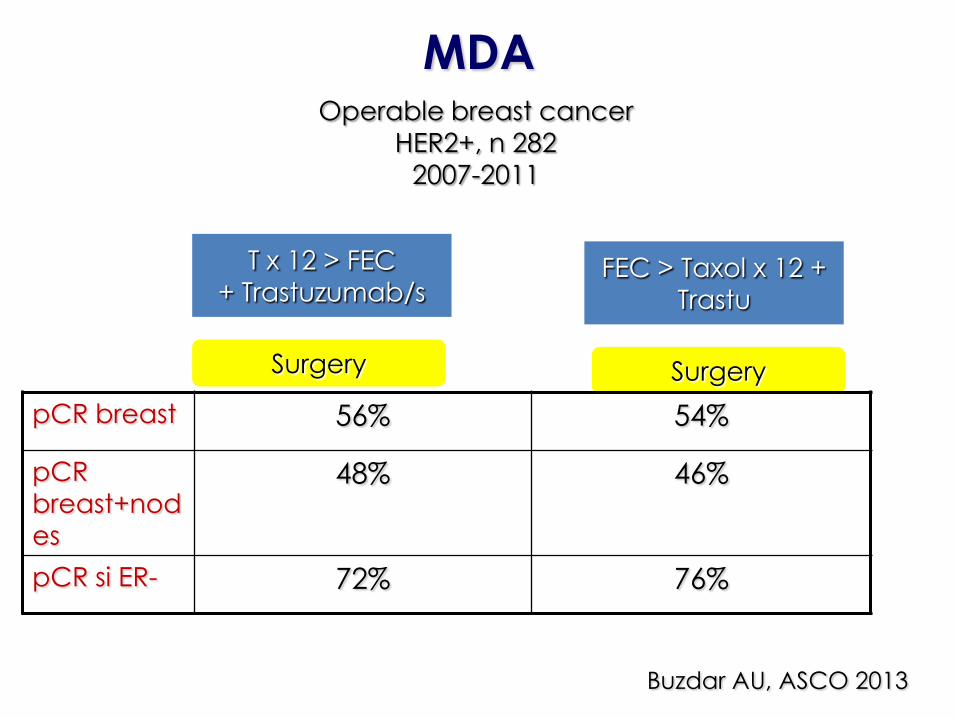
MDAOperable breast cancer
HER2+, n 282
2007-2011
T x 12 > FEC
+ Trastuzumab/s
SurgerySurgery
FEC > Taxol x 12 +
Trastu
pCR breast 56% 54%
pCR
breast+nod
es
48% 46%
pCR si ER- 72% 76%
Buzdar AU, ASCO 2013
CMFq4w x 3 cycles
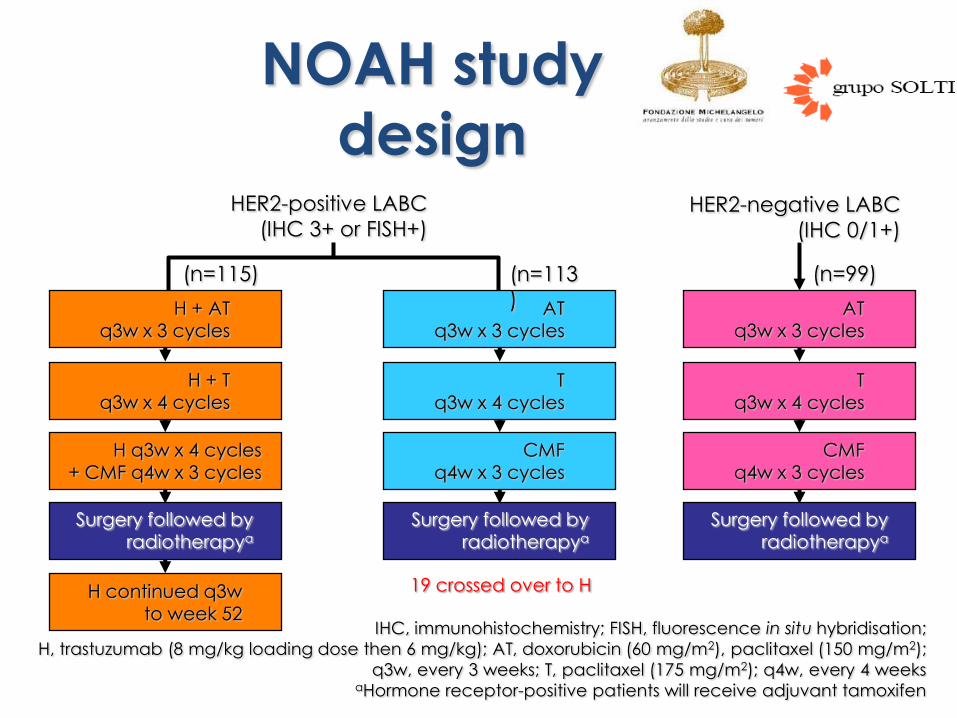
NOAH study
design
IHC, immunohistochemistry; FISH, fluorescence in situ hybridisation;
H, trastuzumab (8 mg/kg loading dose then 6 mg/kg); AT, doxorubicin (60 mg/m2), paclitaxel (150 mg/m2);
q3w, every 3 weeks; T, paclitaxel (175 mg/m2); q4w, every 4 weeksaHormone receptor-positive patients will receive adjuvant tamoxifen
HER2-positive LABC
(IHC 3+ or FISH+)
ATq3w x 3 cycles
Tq3w x 4 cycles
H + ATq3w x 3 cycles
H + T
q3w x 4 cycles
H q3w x 4 cycles+ CMF q4w x 3 cycles
H continued q3wto week 52
(n=115) (n=113
) ATq3w x 3 cycles
Tq3w x 4 cycles
CMFq4w x 3 cycles
HER2-negative LABC
(IHC 0/1+)
Surgery followed byradiotherapya
(n=99)
Surgery followed byradiotherapya
Surgery followed byradiotherapya
19 crossed over to H
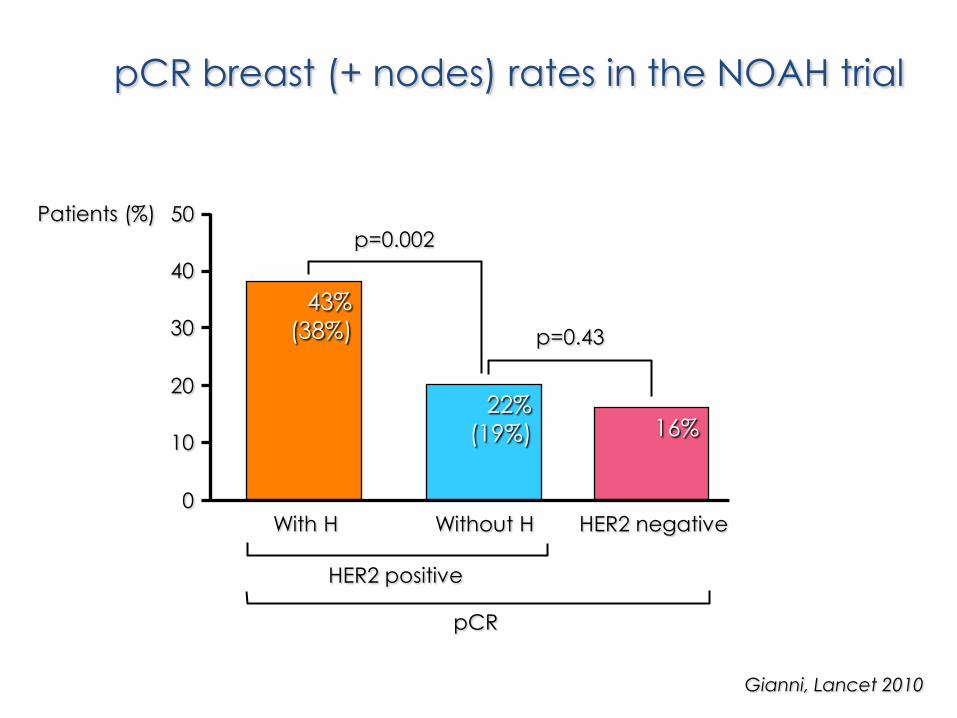
Patients (%)
43%
(38%)
22%
(19%) 16%
0
10
20
30
40
50
With H Without H HER2 negative
HER2 positive
pCR
p=0.002
p=0.43
pCR breast (+ nodes) rates in the NOAH trial
Gianni, Lancet 2010
DFS and OS: HER2-positive population
Median follow-up is 5,4 years
Gianni, ASCO 2013
• DFS - HR 0,64 (p 0,01) a favor de trastuzumab• OS - HR 0,66 (p 0,05) a favor de trastuzumab
• DFS en pCR: HR 0,29• DFS en no pCR: HR 0.92
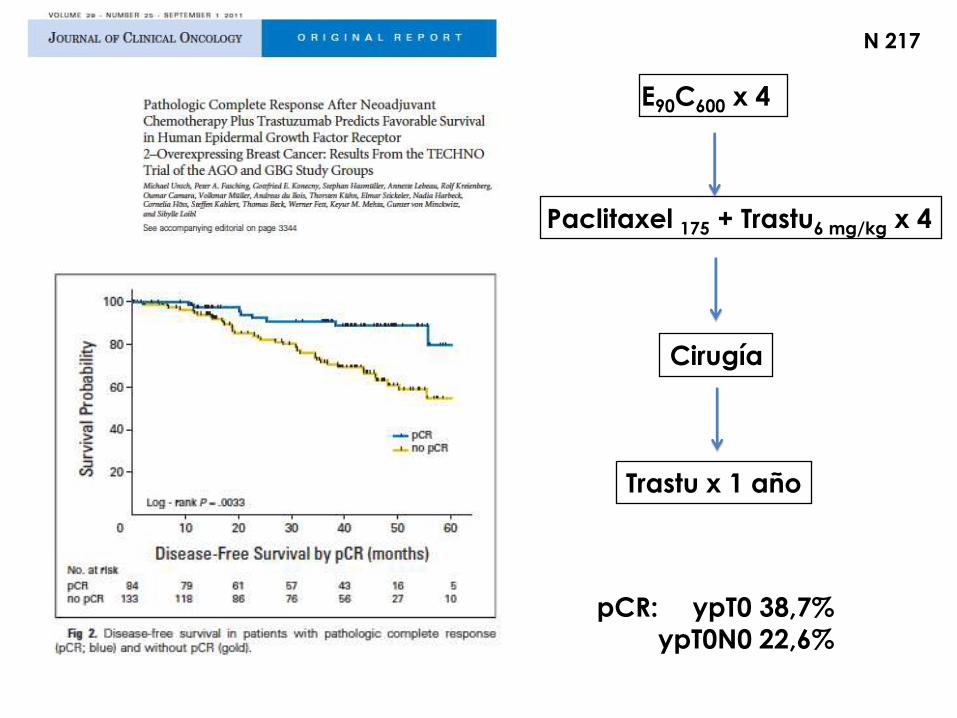
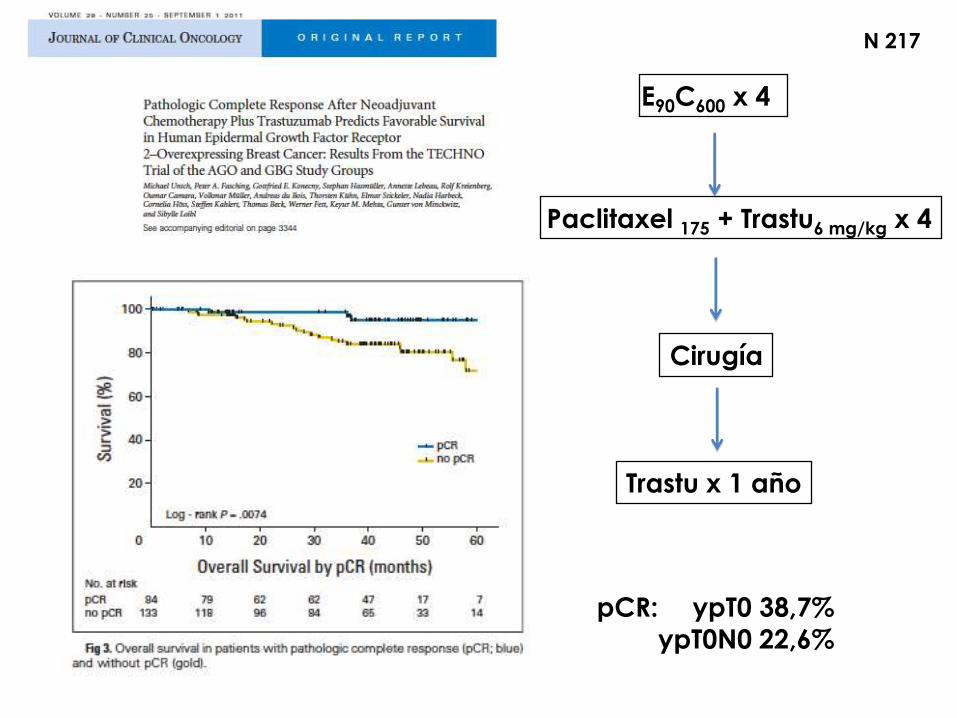
E90C600 x 4
Paclitaxel 175 + Trastu6 mg/kg x 4
Cirugía
Trastu x 1 año
N 217
pCR: ypT0 38,7%
ypT0N0 22,6%
E90C600 x 4
Paclitaxel 175 + Trastu6 mg/kg x 4
Cirugía
Trastu x 1 año
N 217
pCR: ypT0 38,7%
ypT0N0 22,6%
HER2+: Doble bloqueo
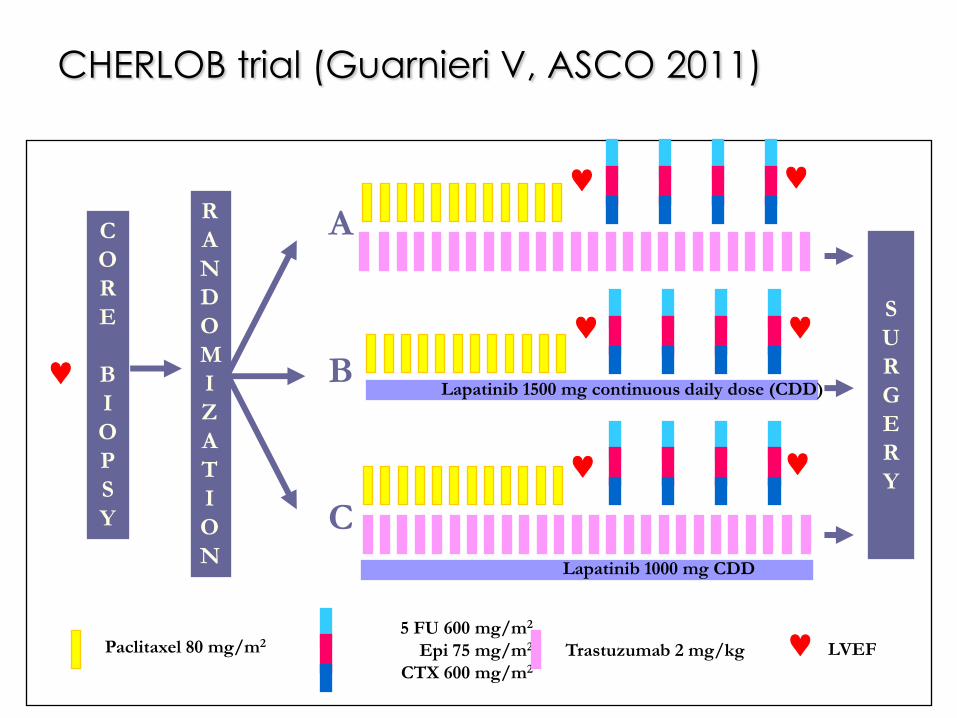
5 FU 600 mg/m2
Epi 75 mg/m2
CTX 600 mg/m2
Paclitaxel 80 mg/m2Trastuzumab 2 mg/kg
R
A
N
D
O
M
I
Z
A
T
I
O
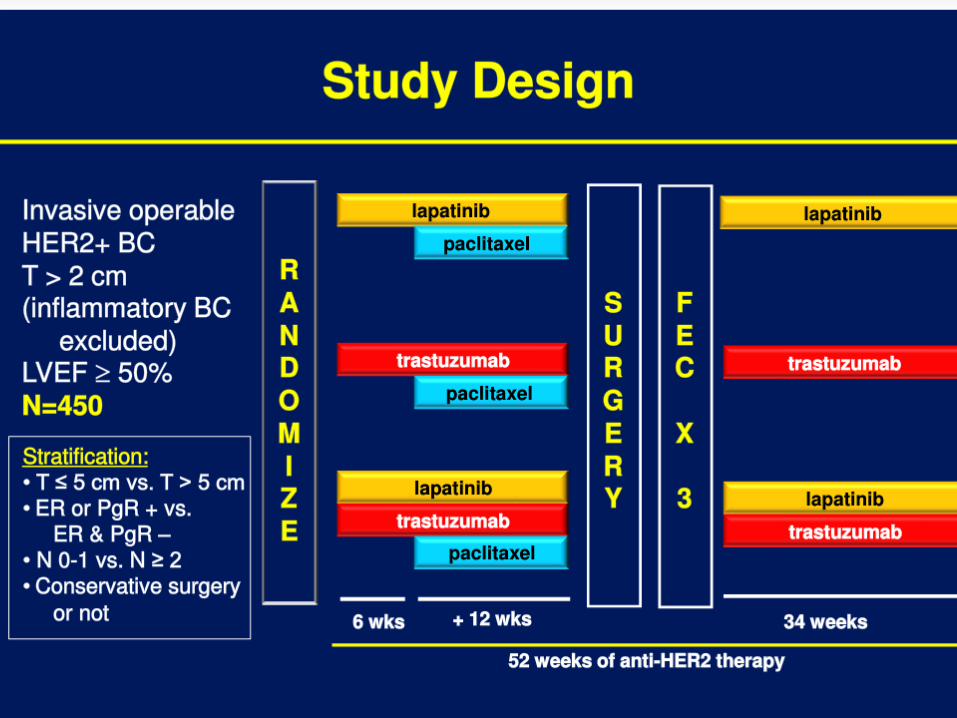
NLapatinib 1000 mg CDD
Lapatinib 1500 mg continuous daily dose (CDD)
C
O
R
E
B
I
O
P
S
Y
S
U
R
G
E
R
Y
A
B
C
LVEF
CHERLOB trial (Guarnieri V, ASCO 2011)

NeoSphere: study design
THP (n=107)docetaxel +
trastuzumab +pertuzumab
HP (n=107)trastuzumab +
pertuzumab
TP (n=96)docetaxel + pertuzumab
S
U
R
G
R
Y
docetaxel q3w x 4→FEC q3w x 3
trastuzumab q3w cycles 5–17
FEC q3w x 3trastuzumab q3w cycles 5–17
FEC q3w x 3trastuzumab q3w cycles 5–17
FEC q3w x 3trastuzumab q3w cycles 5–21
Study dosing: q3w x 4
TH (n=107)docetaxel + trastuzumab
Patients with
operable or
locally
advanced
/inflammatory*
HER2-positive BC
Chemo-naïve &
primary tumors
>2cm (N=417)
BC, breast cancer; FEC, 5-fluorouracil, epirubicin and cyclophosphamide
*Locally advanced=T2–3, N2–3, M0 or T4a–c, any N, M0; operable=T2–3, N0–1, M0; inflammatory = T4d, any N, M0
H, trastuzumab; P, pertuzumab; T, docetaxel3
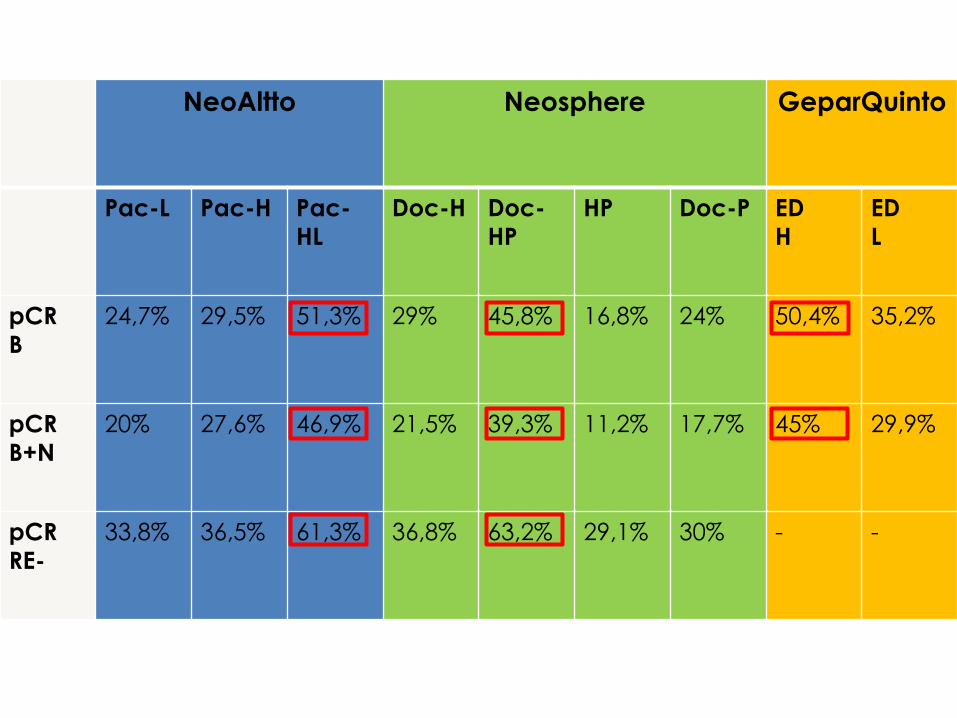
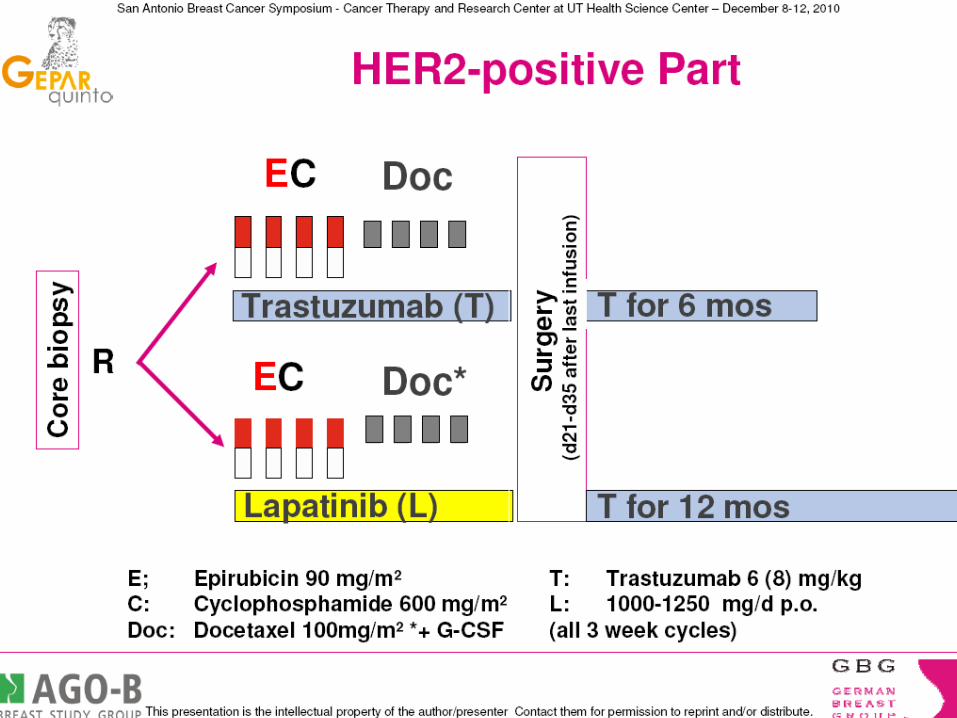
NeoAltto Neosphere GeparQuinto
Pac-L Pac-H Pac-
HL
Doc-H Doc-
HP
HP Doc-P ED
H
ED
L
pCR
B
24,7% 29,5% 51,3% 29% 45,8% 16,8% 24% 50,4% 35,2%
pCR
B+N
20% 27,6% 46,9% 21,5% 39,3% 11,2% 17,7% 45% 29,9%
pCR
RE-
33,8% 36,5% 61,3% 36,8% 63,2% 29,1% 30% - -
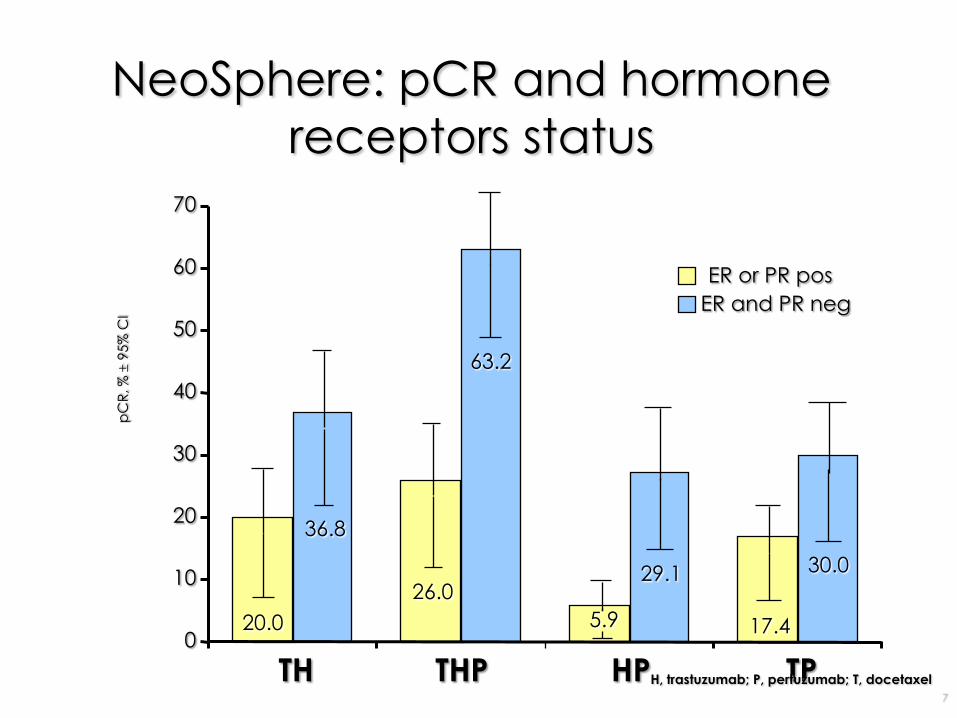
0
10
20
30
40
50
60
70
TH THP HP TP
ER or PR pos
ER and PR neg
NeoSphere: pCR and hormone
receptors status
20.0
26.0
17.4
36.8
29.1 30.0
63.2
5.9
pC
R, %
9
5%
CI
H, trastuzumab; P, pertuzumab; T, docetaxel
7
HER2+: Doble bloqueo Opción sin antraciclinas
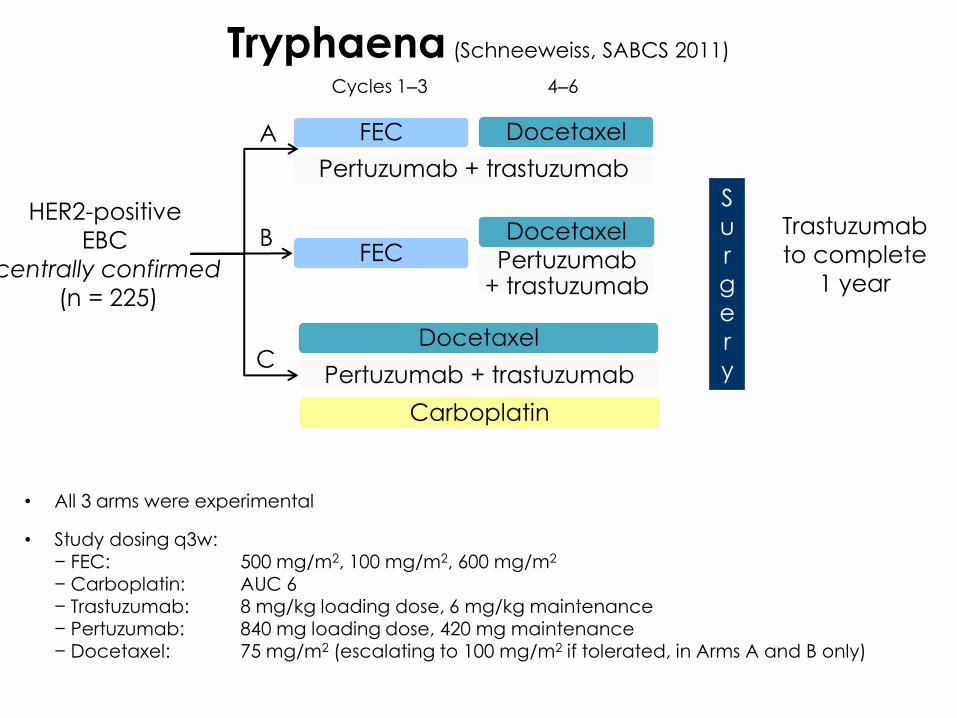
Tryphaena (Schneeweiss, SABCS 2011)
HER2-positive
EBC
centrally confirmed
(n = 225)
FEC
Trastuzumab
to complete
1 year
S
u
r
g
e
r
y
• All 3 arms were experimental
• Study dosing q3w:− FEC: 500 mg/m2, 100 mg/m2, 600 mg/m2
− Carboplatin: AUC 6− Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance− Pertuzumab: 840 mg loading dose, 420 mg maintenance− Docetaxel: 75 mg/m2 (escalating to 100 mg/m2 if tolerated, in Arms A and B only)
Docetaxel
Cycles 1‒3 4‒6
Pertuzumab+ trastuzumab
Pertuzumab + trastuzumab
FECDocetaxel
Carboplatin
Docetaxel
Pertuzumab + trastuzumabC
B
A
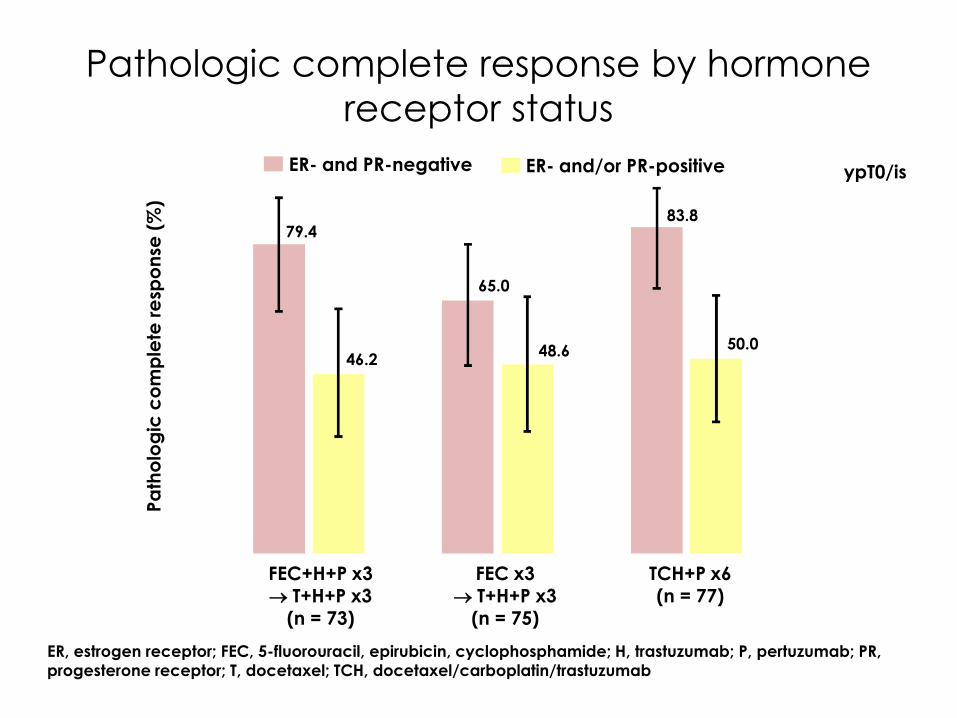
Pathologic complete response by hormone
receptor status
ER, estrogen receptor; FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; PR,
progesterone receptor; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
Pa
tho
log
ic c
om
ple
te r
esp
on
se (
%)
ER- and PR-negative ER- and/or PR-positive
79.4
65.0
46.248.6
83.8
50.0
ypT0/is
FEC+H+P x3 T+H+P x3
(n = 73)
FEC x3 T+H+P x3
(n = 75)
TCH+P x6(n = 77)
Neoadyuvancia en HER2+
• Doble bloqueo HER2 + QT (excepto B41)
• Antraciclinas excepto en casos seleccionados
(Tryphaena)
• Reexplorar la combinación antiHER2 + HT
(Pamela)
• Relevancia de pCR como marcador surrogado?
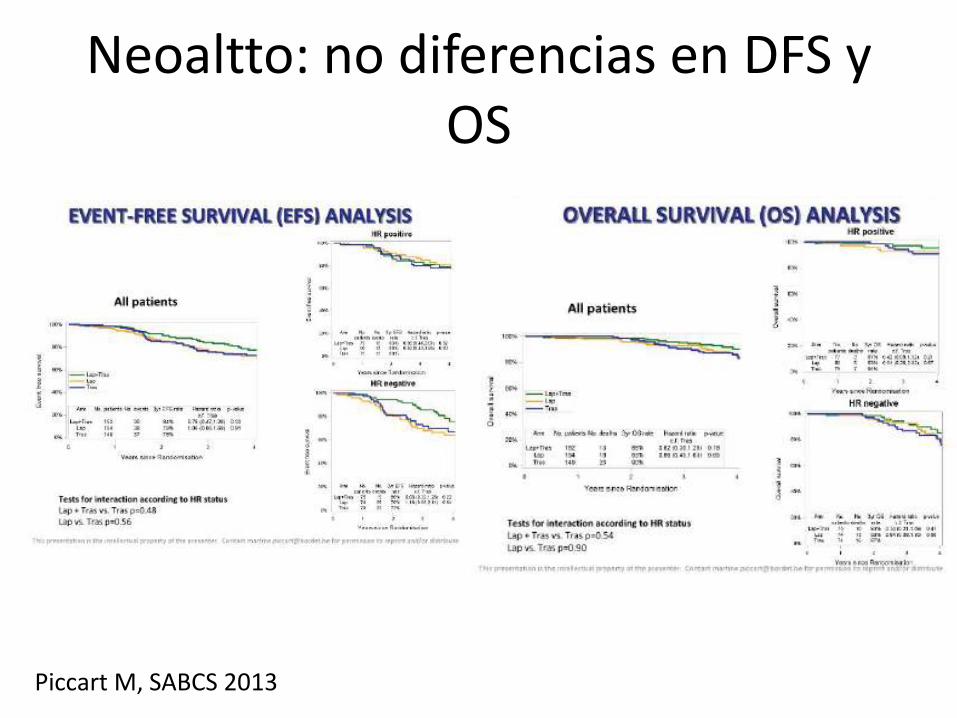
Neoaltto: no diferencias en DFS y OS
Piccart M, SABCS 2013
Fenotipo Triple Negativo

7
16
0
10
20
30
40
50
60
18
30 31
50
.
Grade 1-2 Grade 3
HR+
No Tras Yes Tras
HER2+ HR+
No Tras Yes Tras
HER2+ HR- TRIPLE NEG
34
pCR Rates by Tumor Subtypes
FDA, SABCS 2012
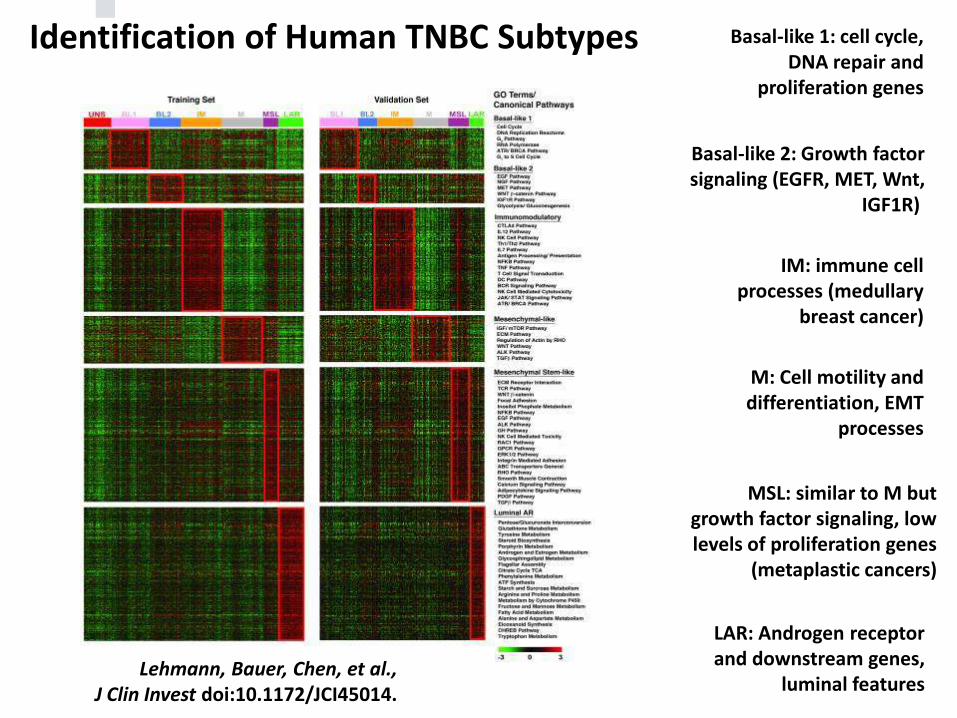
Basal-like 1: cell cycle, DNA repair and
proliferation genes
Basal-like 2: Growth factorsignaling (EGFR, MET, Wnt,
IGF1R)
IM: immune cellprocesses (medullary
breast cancer)
M: Cell motility and differentiation, EMT
processes
MSL: similar to M butgrowth factor signaling, lowlevels of proliferation genes
(metaplastic cancers)
LAR: Androgen receptor and downstream genes,
luminal featuresLehmann, Bauer, Chen, et al.,
J Clin Invest doi:10.1172/JCI45014.
Identification of Human TNBC Subtypes
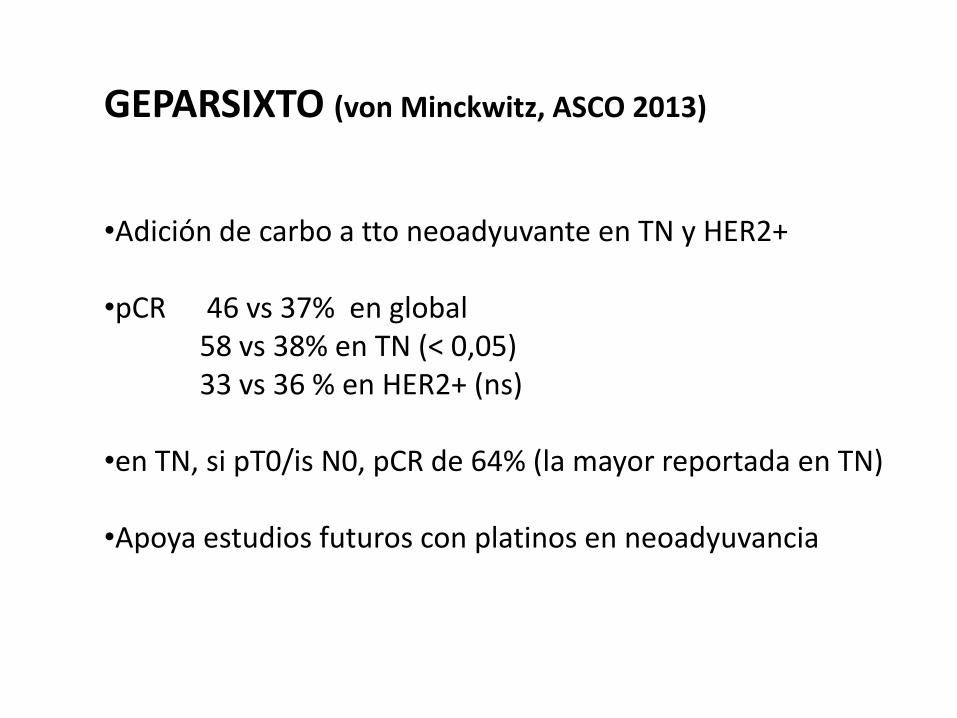
GEPARSIXTO (von Minckwitz, ASCO 2013)
•Adición de carbo a tto neoadyuvante en TN y HER2+
•pCR 46 vs 37% en global58 vs 38% en TN (< 0,05)33 vs 36 % en HER2+ (ns)
•en TN, si pT0/is N0, pCR de 64% (la mayor reportada en TN)
•Apoya estudios futuros con platinos en neoadyuvancia
CALGB 40603 (Sikov, SABCS 2013)
•Adición de carbo y bevacizumab a tto neoadyuvante en TN •Paclitaxel semanal +/-beva +/- carboplatino
seguido ACX4 (dd)•pCR mama y axila:
- 41 vs 54% a favor de carboplatino (p 0,0029)- 44 vs 52% tendencia a favor de beva (NS)
•Junto a datos de Geparsixto, valorar adición de carboplatino
•Necesario mayor seguimiento (SLE)
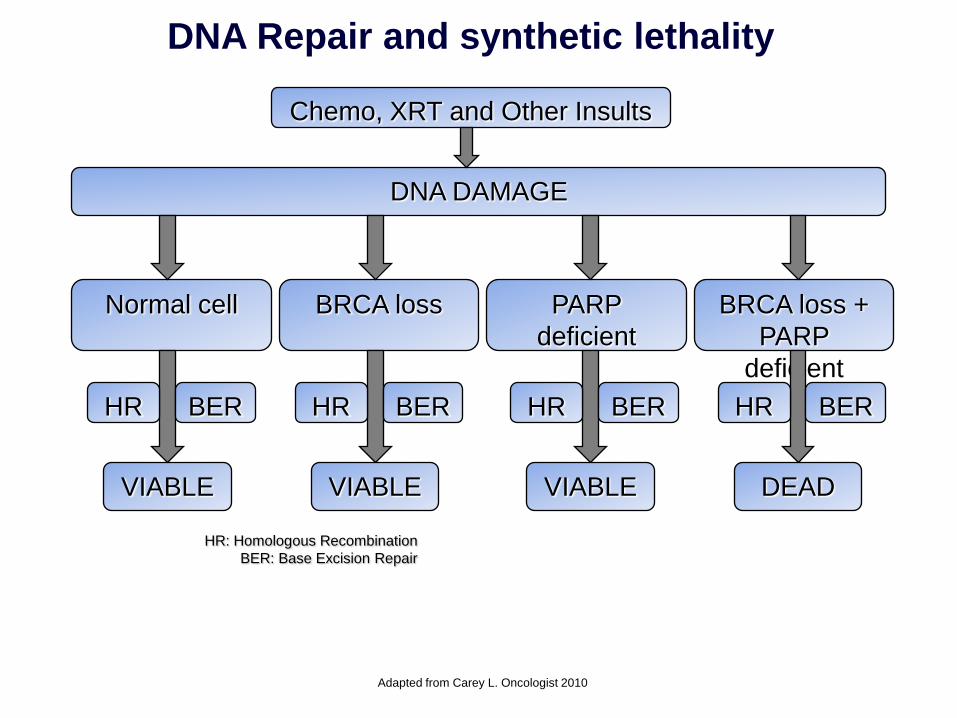
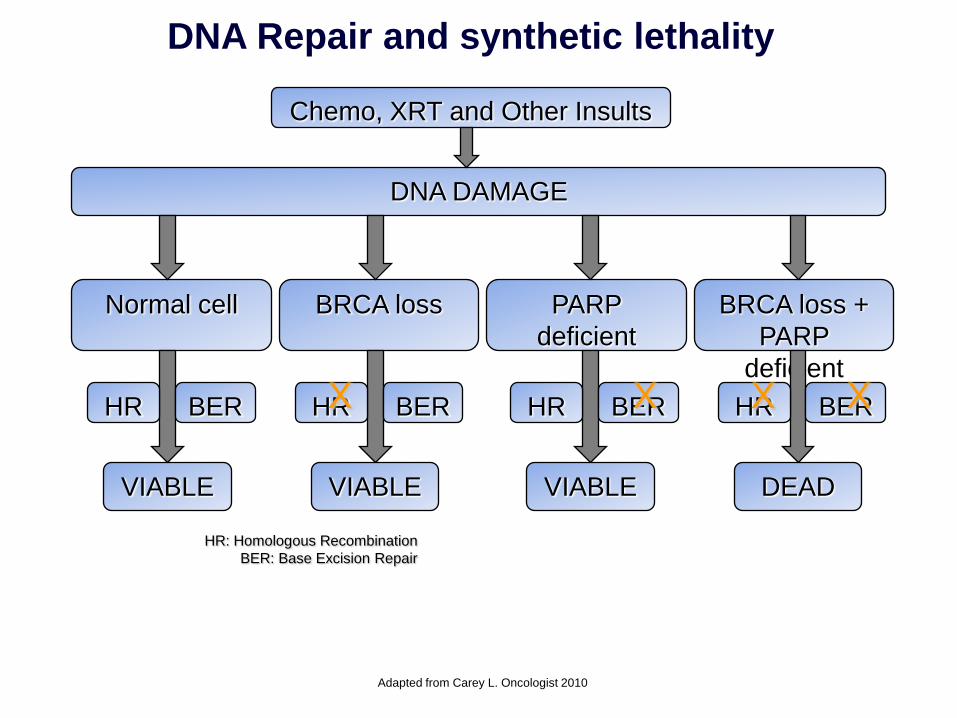
DNA Repair and synthetic lethality
Adapted from Carey L. Oncologist 2010
Chemo, XRT and Other Insults
DNA DAMAGE
Normal cell BRCA loss PARP
deficient
BRCA loss +
PARP
deficient
VIABLE VIABLE VIABLE DEAD
HR BER HR BER HR BER HR BER
HR: Homologous Recombination
BER: Base Excision Repair
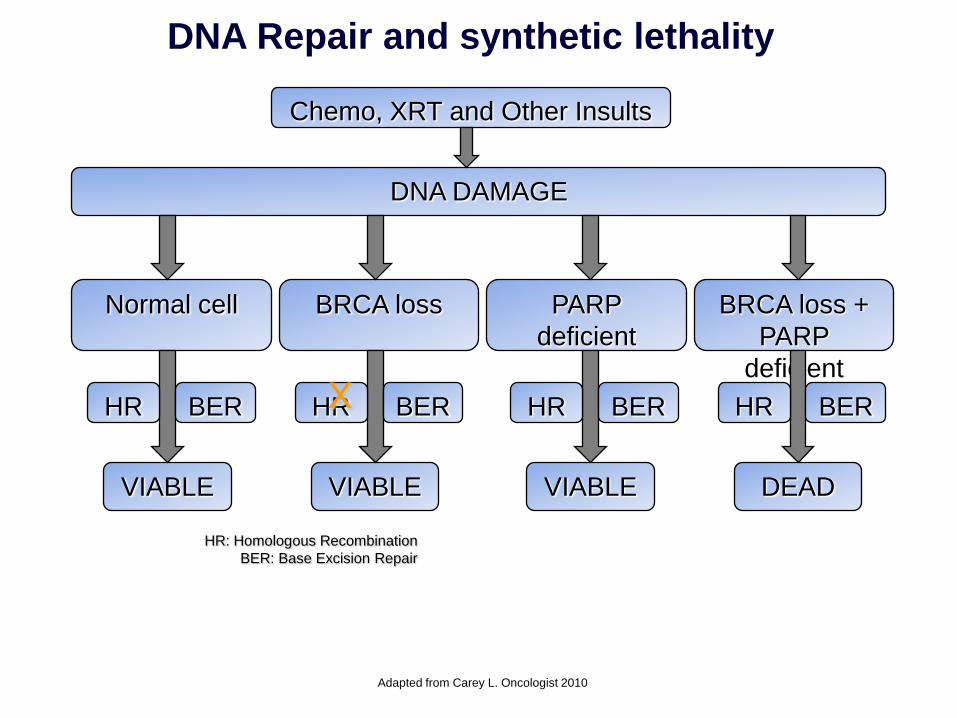
DNA Repair and synthetic lethality
Adapted from Carey L. Oncologist 2010
Chemo, XRT and Other Insults
DNA DAMAGE
Normal cell BRCA loss PARP
deficient
BRCA loss +
PARP
deficient
VIABLE VIABLE VIABLE DEAD
HR BER HR BER HR BER HR BER
HR: Homologous Recombination
BER: Base Excision Repair
X
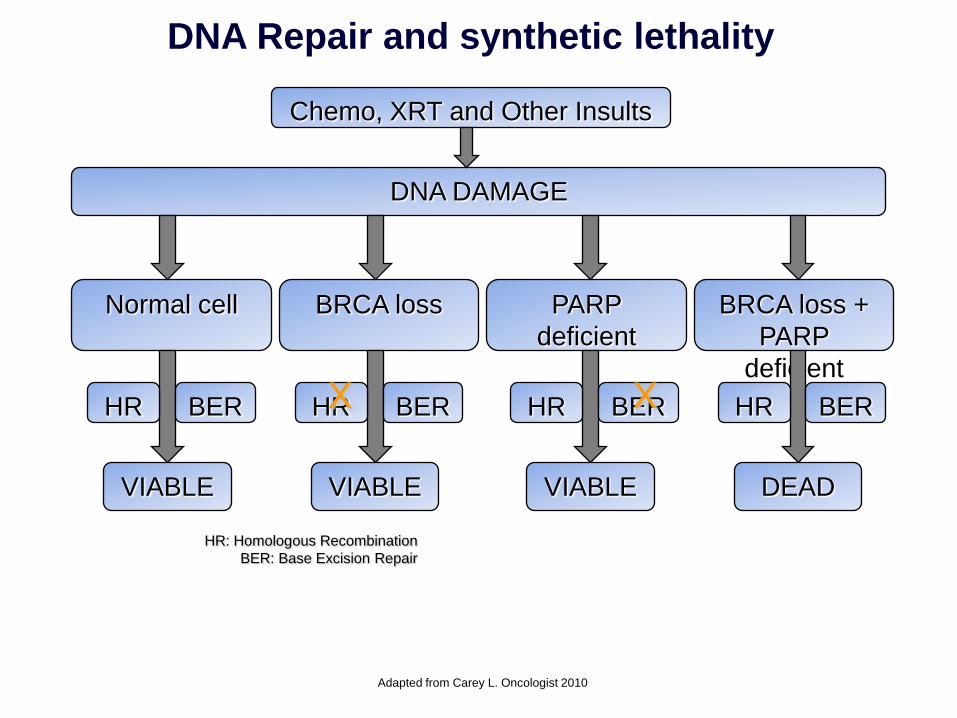
DNA Repair and synthetic lethality
Adapted from Carey L. Oncologist 2010
Chemo, XRT and Other Insults
DNA DAMAGE
Normal cell BRCA loss PARP
deficient
BRCA loss +
PARP
deficient
VIABLE VIABLE VIABLE DEAD
HR BER HR BER HR BER HR BER
HR: Homologous Recombination
BER: Base Excision Repair
X X
DNA Repair and synthetic lethality
Adapted from Carey L. Oncologist 2010
Chemo, XRT and Other Insults
DNA DAMAGE
Normal cell BRCA loss PARP
deficient
BRCA loss +
PARP
deficient
VIABLE VIABLE VIABLE DEAD
HR BER HR BER HR BER HR BER
HR: Homologous Recombination
BER: Base Excision Repair
X X X X
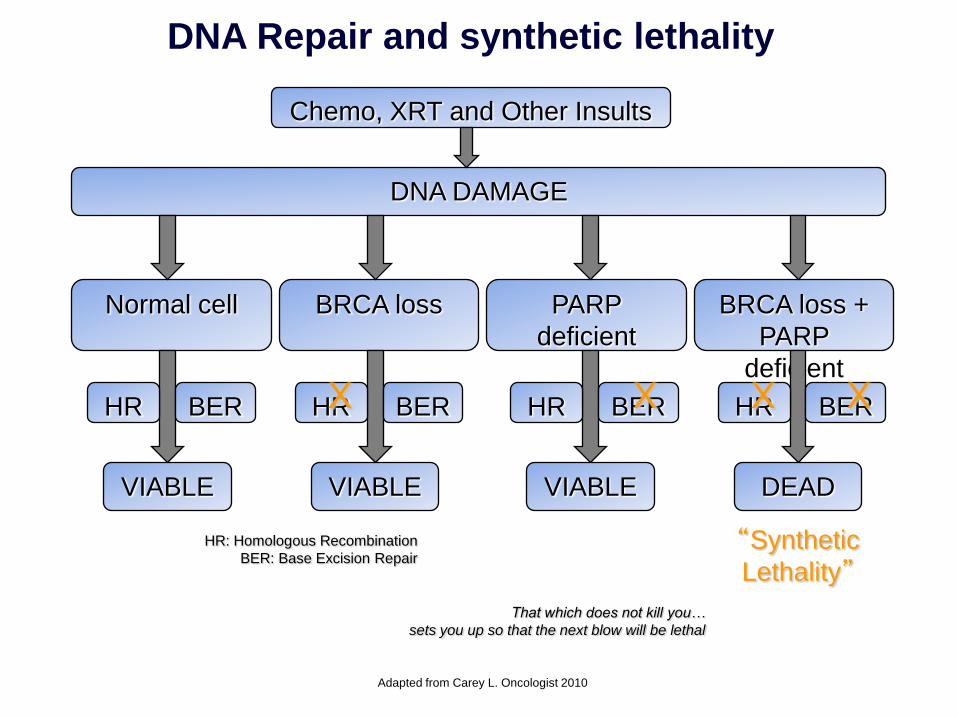
DNA Repair and synthetic lethality
Adapted from Carey L. Oncologist 2010
Chemo, XRT and Other Insults
DNA DAMAGE
Normal cell BRCA loss PARP
deficient
BRCA loss +
PARP
deficient
VIABLE VIABLE VIABLE DEAD
HR BER HR BER HR BER HR BER
HR: Homologous Recombination
BER: Base Excision Repair
X X X X
“Synthetic
Lethality”
That which does not kill you…
sets you up so that the next blow will be lethal
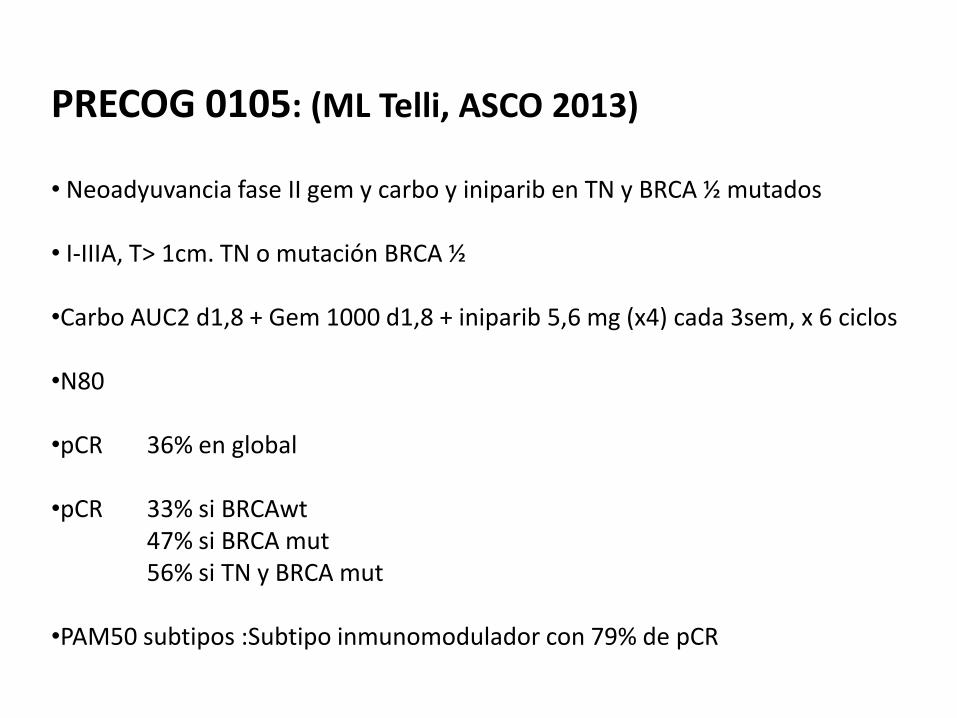
PRECOG 0105: (ML Telli, ASCO 2013)
• Neoadyuvancia fase II gem y carbo y iniparib en TN y BRCA ½ mutados
• I-IIIA, T> 1cm. TN o mutación BRCA ½
•Carbo AUC2 d1,8 + Gem 1000 d1,8 + iniparib 5,6 mg (x4) cada 3sem, x 6 ciclos
•N80
•pCR 36% en global
•pCR 33% si BRCAwt47% si BRCA mut56% si TN y BRCA mut
•PAM50 subtipos :Subtipo inmunomodulador con 79% de pCR
Fenotipo Triple Negativo
• Quimioterapia convencional basada
en antraciclinas y taxanos
• Posible papel para platinos e inhibidores
de PARP
• Subtipos intrínsecos (7)
• Papel dudoso de bevacizumab
Tratamiento hormonal neoadyuvante
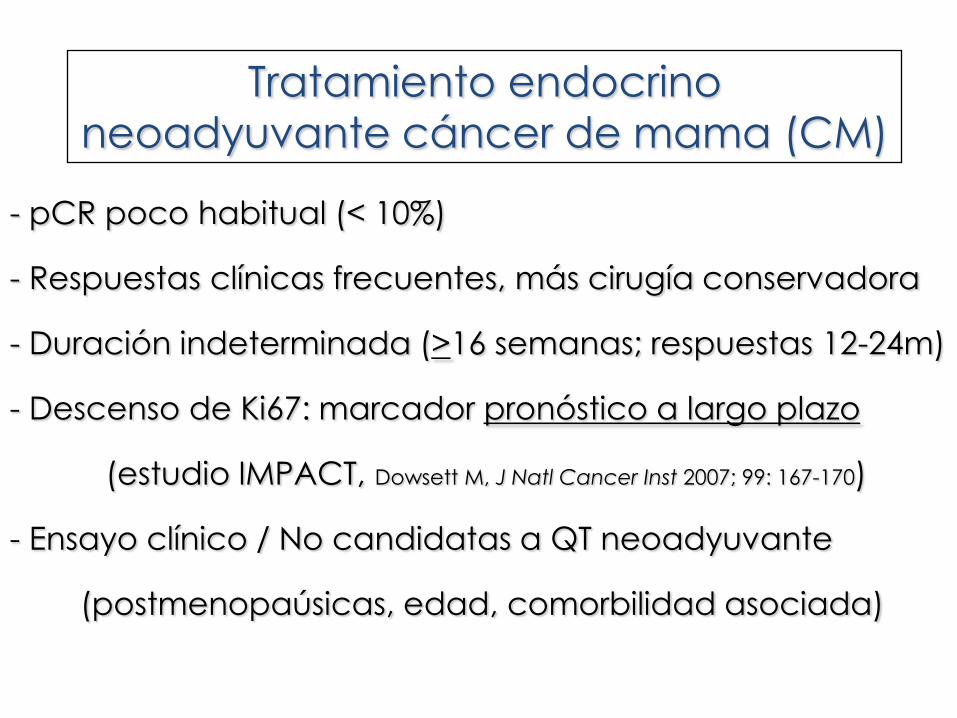
- pCR poco habitual (< 10%)
- Respuestas clínicas frecuentes, más cirugía conservadora
- Duración indeterminada (>16 semanas; respuestas 12-24m)
- Descenso de Ki67: marcador pronóstico a largo plazo
(estudio IMPACT, Dowsett M, J Natl Cancer Inst 2007; 99: 167-170)
- Ensayo clínico / No candidatas a QT neoadyuvante
(postmenopaúsicas, edad, comorbilidad asociada)
Tratamiento endocrino
neoadyuvante cáncer de mama (CM)

ACOSOG Z-1031
Ellis M, SABCS 2010
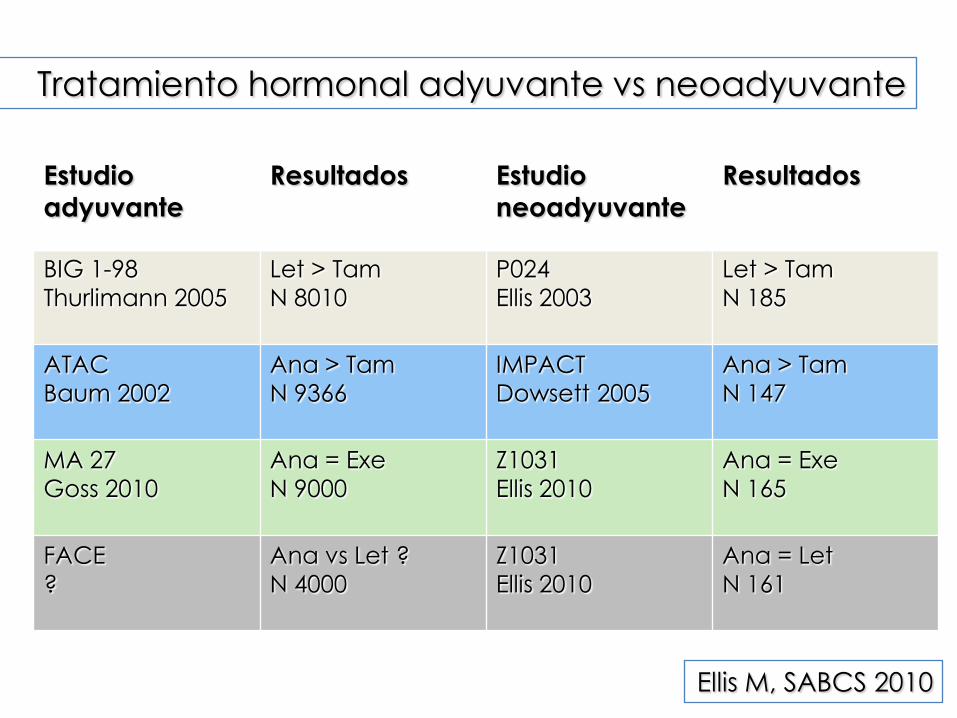
Tratamiento hormonal adyuvante vs neoadyuvante
Estudio
adyuvante
Resultados Estudio
neoadyuvante
Resultados
BIG 1-98
Thurlimann 2005
Let > Tam
N 8010
P024
Ellis 2003
Let > Tam
N 185
ATAC
Baum 2002
Ana > Tam
N 9366
IMPACT
Dowsett 2005
Ana > Tam
N 147
MA 27
Goss 2010
Ana = Exe
N 9000
Z1031
Ellis 2010
Ana = Exe
N 165
FACE
?
Ana vs Let ?
N 4000
Z1031
Ellis 2010
Ana = Let
N 161
Ellis M, SABCS 2010

Ellis MJ, et al. JNCI 2008
Preoperative Endocrine Prognostic Index
Basado en pT, N, ER score, y Ki-67 tras 3-4 meses de Tto
Hormonoterapia Neoadyuvante
Información Pronóstica
PEPI Score
Aspectos de manejo
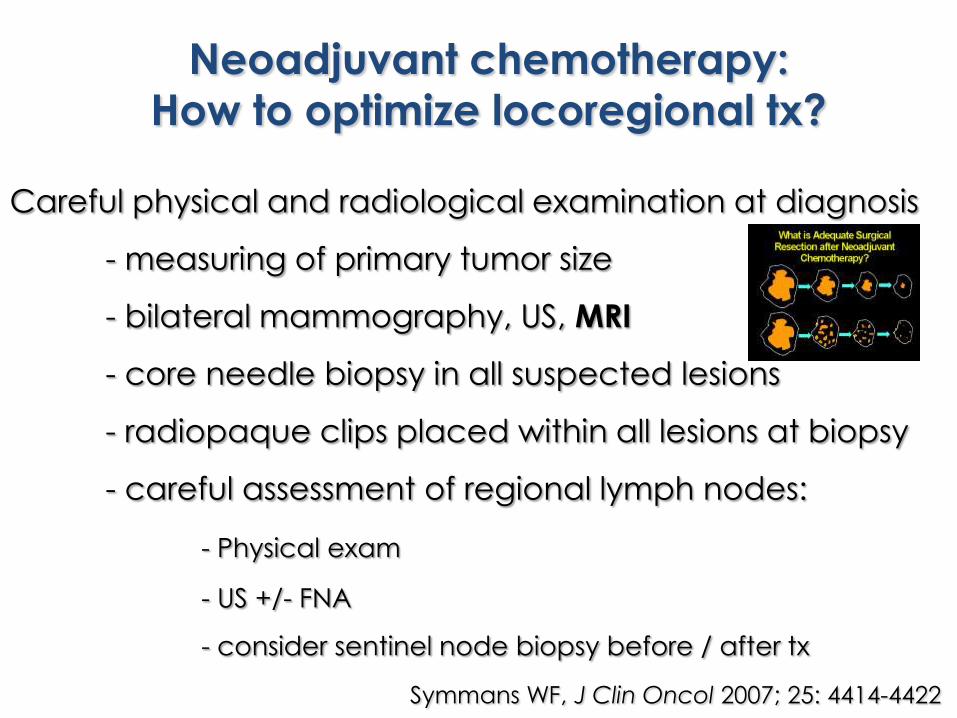
Careful physical and radiological examination at diagnosis
- measuring of primary tumor size
- bilateral mammography, US, MRI
- core needle biopsy in all suspected lesions
- radiopaque clips placed within all lesions at biopsy
- careful assessment of regional lymph nodes:
- Physical exam
- US +/- FNA
- consider sentinel node biopsy before / after tx
Neoadjuvant chemotherapy:
How to optimize locoregional tx?
Symmans WF, J Clin Oncol 2007; 25: 4414-4422
Necesidad de trabajar en Unidades Multidisciplinares

Aspectos regulatorios
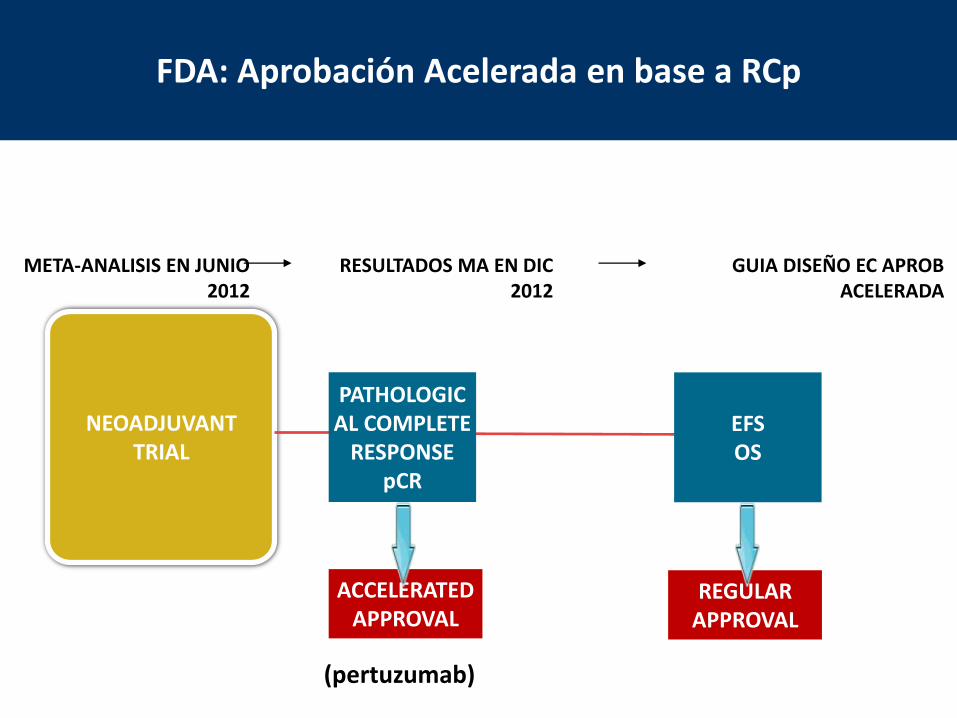
ACCELERATEDAPPROVAL
NEOADJUVANTTRIAL
PATHOLOGICAL COMPLETE
RESPONSEpCR
EFSOS
REGULARAPPROVAL
META-ANALISIS EN JUNIO 2012
RESULTADOS MA EN DIC 2012
GUIA DISEÑO EC APROB ACELERADA
FDA: Aprobación Acelerada en base a RCp
(pertuzumab)
Possibly due to:
• low pCR rates
• small pCR improvements
• heterogeneous population
• lack of targeted therapies
Larger pCR differences between treatment
arms may translate into long-term outcome
and may vary according to breast cancer
subtype (more agressive.: TN, HER2+)
FDA pooled-analysis could not establish
pCR as a surrogate endpoint for EFS/OS



















