Muerte súbita en deportistas
61
Muerte súbita en deportistas Vicente R. Cabedo García Centro de Salud “El Barranquet” (Castellón)
-
Upload
vicente-ramon-cabedo-garcia -
Category
Health & Medicine
-
view
62 -
download
2
Transcript of Muerte súbita en deportistas

Muerte súbita en deportistas
Vicente R. Cabedo GarcíaCentro de Salud “El Barranquet” (Castellón)


Mueren 2 atletas en el Maratón de Navajas y otro está en observación
!Francisco Amat, de 57 años y vecino de Alicante, sufrió un infarto fulminante a 17 km de la meta - Juan Barros, de 45, murió en su hotel por un paro cardíaco 11.04.2016 | 13:05

SOCIEDADLos médicos destacan la importancia de la prevención para sortear problemas cardíacos
Expertos, tras el maratón de Ojos Negros: 'El 99% de casos de muerte súbita se puede evitar'
«El 99 por ciento de casos de muerte súbita se puede evitarjefe del servicio de Cardiología del Hospital Nisa Rey Don Jaime de Castellón. El prestigioso médico señaló que la «vital» prevención tiene que partir de uno mismo. «relacionado con la cultura sanitaria que tenemos en Españacarísimas y que después le duela gastarse el dinero en saber cómo está del corazón», remarcó el reputado galeno.

• El ecocardiograma contribuye a evitar la muerte súbita en deportistas de competición !Noticias cardiologíaEl ecocardiograma contribuye a evitar la muerte súbita en deportistas de competiciónLa utilización del ecocardiograma en las revisiones preparticipativas (RPP) de deportistas de competición mejoraría la prevención de la muerte súbita y facilitaría la detección de alteraciones cardiacas que habitualmente pasan inadvertidas en la revisión física y durante el electrocardiograma.

Artıculo original
Utilidad del ecocardiograma en la revision preparticipativade deportistas de competicion
Gonzalo Graziolia, Beatriz Merinoa, Silvia Montserrata, Barbara Vidala,Manel Azquetaa, Carles Parea, Georgia Sarquella-Brugadab, Xavier Yanguasc,Ramon Pic, Lluis Tilc,d, Jaume Escodae, Josep Brugadaa y Marta Sitgesa,*a Grup de Treball Cardiologia Esportiva, Institut del Torax, Hospital Clınic de Barcelona, Universitat de Barcelona, IDIBAPS, Institut d’Investigacions Biomediques August Pi i Sunyer,Barcelona, Espanab Servicio de Cardiologıa, Hospital Sant Joan de Deu, Universitat de Barcelona, Sant Joan Despı, Barcelona, Espanac Servei Medic, Futbol Club Barcelona, Barcelona, Espanad GIRSANE, Consorci Sanitari de Terrassa-Centre d’Alt Rendiment, Sant Cugat del Valles, Barcelona, Espanae Area de Medicina, Consell Catala de l’Esport, Generalitat de Catalunya, Barcelona, Espana
Rev Esp Cardiol. 2014;67(9):701–705
Historia del artıculo:Recibido el 23 de julio de 2013Aceptado el 28 de noviembre de 2013On-line el 13 de abril de 2014
Palabras clave:EcocardiografıaDeporteAtletasMuerte subitaRevision preparticipativa
R E S U M E N
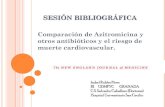
Introduccion y objetivos: A pesar del establecido valor diagnostico del electrocardiograma en la revisionpreparticipativa de sujetos deportistas, algunas alteraciones estructurales cardiacas podrıan pasarinadvertidas, en especial en fases precoces de la enfermedad. El objetivo de este estudio es valorar laprevalencia de alteraciones estructurales cardiacas mediante el uso sistematico de la ecocardiografıa enla revision preparticipativa de deportistas de competicion.Metodos: Se estudio a los deportistas incluidos en un programa de competicion o profesionales. Serealizo a todos los deportistas una revision que incluyo historia familiar y personal, examen fısico,electrocardiograma, prueba de esfuerzo y ecocardiograma Doppler.Resultados: Se incluyo a 2.688 deportistas (el 67% varones; media de edad, 21 ! 10 anos). La mayorıa delos estudios ecocardiograficos (92,5%) fueron estrictamente normales y solo 203 (7,5%) tenıan alteraciones; lamas frecuente de ellas fue la hipertrofia ventricular izquierda, en 50 deportistas (1,8%). En 4 casos (0,14%) seindico el cese de la practica deportiva: 2 por miocardiopatıa hipertrofica (el electrocardiograma mostrabaalteraciones pero no cumplıa criterios diagnosticos), 1 pectus excavatum con compresion del ventrıculoderecho y 1 estenosis valvular pulmonar significativa; el resto de las alteraciones no implicaron el cese de lapractica deportiva y solo requirieron seguimiento periodico.Conclusiones: Algunas alteraciones estructurales cardiacas, aunque poco frecuentes, pueden pasarinadvertidas al examen fısico y en el electrocardiograma; en cambio, son facilmente reconocibles con unecocardiograma. Estas observaciones indican introducir el ecocardiograma al menos en la primeravaloracion preparticipativa de deportistas de competicion para mejorar la eficacia de los programas deprevencion de la muerte subita del deportista.! 2013 Sociedad Espanola de Cardiologıa. Publicado por Elsevier Espana, S.L.U. Todos los derechos reservados.
Usefulness of Echocardiography in Preparticipation Screening of CompetitiveAthletes
Keywords:EchocardiographySportAthletesSudden deathPreparticipation screening
A B S T R A C T
Introduction and objectives: Despite the established diagnostic value of the electrocardiogram inpreparticipation screening of athletes, some cardiac structural changes can be missed, particularly inearly disease stages. The aim of this study was to evaluate the prevalence of cardiac structural changesvia the systematic use of echocardiography in preparticipation screening of competitive athletes.Methods: Professional athletes or participants in a competitive athletic program underwent a screeningthat included family and personal medical history, physical examination, electrocardiography, exercisetesting, and Doppler echocardiography.Results: A total of 2688 athletes (67% men; mean age [standard deviation], 21 [10] years) were included.Most of the echocardiographic evaluations (92.5%) were normal and only 203 (7.5%) showed changes;the most frequent change was left ventricular hypertrophy, seen in 50 athletes (1.8%). Cessation ofathletic activity was indicated in 4 athletes (0.14%): 2 for hypertrophic cardiomyopathy (electro-cardiography had shown changes that did not meet diagnostic criteria), 1 pectus excavatum withcompression of the right ventricle, and 1 significant pulmonary valve stenosis; the rest of the changes didnot entail cessation of athletic activity and only indicated periodic monitoring.
* Autor para correspondencia: Servicio de Cardiologıa, Institut Clınic del Torax, Hospital Clınic, Villarroel 170, 08036 Barcelona, Espana.Correo electronico: [email protected] (M. Sitges).
0300-8932/$ – see front matter ! 2013 Sociedad Espanola de Cardiologıa. Publicado por Elsevier Espana, S.L.U. Todos los derechos reservados.http://dx.doi.org/10.1016/j.recesp.2013.11.023
Documento descargado de http://www.revespcardiol.org el 21/04/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

La utilidad de la ecocardiografıa en manos experimentadas paradescartar alteraciones estructurales cardiacas es incuestionable,ası como el valor del ecocardiograma para el diagnostico deenfermedad cardiaca estructural en presencia de alteracionessignificativas en el ECG, es decir, el grupo 2 de anormalidadesdescritas en el ECG de los deportistas, segun las actualesrecomendaciones8.
Respecto a las alteraciones detectadas en el ecocardiograma, suincidencia en nuestra poblacion es inferior a la descrita en otroestudio realizado en futbolistas9, pero superior a la descrita en elmayor estudio publicado de seguimiento de deportistas de elite10.La mayor incidencia de hallazgos anormales en nuestro estudiorespecto al realizado por Pelliccia et al10 podrıa explicarse por dosmotivos; por un lado, en nuestro estudio se han valoradoalteraciones cardiacas menores, que no descalifican para lacompeticion deportiva pero sı tendrıan importancia para esta-blecer un seguimiento estrecho de estos deportistas. Por otro lado,los deportistas incluidos en el estudio realizado en Italia eran deelite y ya habıan pasado una RPP por obligacion legal, por lo que aaquellos con alteraciones ya detectadas probablemente se losexcluyera. Este valor adicional de la ecocardiografıa, a nuestrocriterio, hace del ecocardiograma una herramienta muy util en elcontrol de los deportistas de competicion.
De hecho, la evolucion de estas alteraciones, por lo comunconsideradas triviales, es completamente desconocida en sujetossometidos a programas de entrenamiento intensivos. En estesentido, estudios previos apuntan a que el entrenamiento nodeberıa inducir una aceleracion de la progresion de estasenfermedades de leves a moderadas11, pero la evidencia alrespecto continua siendo escasa. En deportistas sin cardiopatıaque han participado en uno o mas Juegos Olımpicos, un estudio12
ha demostrado en un seguimiento de 17 anos que no se objetivancambios significativos en el volumen, la masa y la motilidad del VI,y de manera significativa solo hay un leve aumento del tamano dela aurıcula izquierda que no excede el lımite normal.
Recientemente se ha descrito mayor prevalencia de criteriosdiagnosticos de falta de compactacion o hipertrabeculacion apicaldel VI en deportistas13. En nuestra serie, la prevalencia fue menor,pero el diagnostico diferencial con una miocardiopatıa nocompactada se dio en 8 deportistas (0,3%). En este subgrupo, lacombinacion con los datos del ECG, en especial cuando hayalteracion en la repolarizacion ventricular y en el ecocardiograma,particularmente en caso de disminucion de la funcion sistolica delVI, es necesaria para tomar decisiones diagnosticas y deseguimiento.
En cuanto a la valvula aortica bicuspide, a pesar de que suincidencia en deportistas es similar que en poblacion general, unestudio ha mostrado que en el seguimiento a 5 anos los deportistascon valvula aortica bicuspide presentan un incremento significa-tivo de las dimensiones del VI en comparacion con deportistas queposeen una valvula aortica tricuspide, aunque los valores semantienen dentro de la normalidad14. En esa misma lınea, si bienlos deportistas con valvula aortica bicuspide mantienen unafraccion de eyeccion del VI normal, otro trabajo demostro que elstrain rate esta disminuido en los segmentos apicales del VI encomparacion con los que tienen una valvula aortica tricuspide15.Por lo tanto, el impacto del entrenamiento cronico en pequenasalteraciones cardiacas no se conoce bien, pero es probable que lasobrecarga cronica de volumen condicione alguna diferencia en laevolucion de estos sujetos que requieren, como mınimo, unseguimiento, y por ello su deteccion precoz es importante desde elpunto de vista clınico.
La dilatacion de ventrıculo derecho se definio con un diametrodel tracto de salida > 40 mm16, la hipertrabeculacion delventrıculo derecho se diagnostico en presencia de mas de 3 tra-beculaciones > 3 mm17. Respecto a las insuficiencias tricuspıdea ypulmonar, que en el grado ligero son muy frecuentes en lapoblacion sana18, se registraron unicamente cuando eran signifi-cativas y se considero las que eran practicamente moderadas; esdecir, todas las triviales y ligeras no se describieron.
Finalmente, con el avance en la tecnologıa de los equipos deecocardiografıa, la sensibilidad diagnostica para detectar un origenanomalo de las arterias coronarias ha aumentado del 80 a mas del96%19 y, de hecho, es el primer metodo diagnostico no invasivo queintentar ante esta sospecha diagnostica20. En nuestra serie, serealizo la busqueda sistematica de los ostium de ambas arteriascoronarias, que se identificaron en el 99% de los casos.
Limitaciones
Uno de los problemas que se han planteado con el usosistematico de la ecocardiografıa es la limitacion inherente a latecnica ultrasonica: dificultad diagnostica ante ventanas acusticasdifıciles, que por otro lado es poco frecuente en sujetos atleticos ydeportistas. En nuestra serie, la frecuencia de uso complementariode la resonancia magnetica cardiaca como tecnica de diagnosticofue < 1%. Este dato guarda coherencia con la unica serie publicadaen Italia al respecto21, en la que solo se menciona un requerimientode estudios de mayor complejidad < 5%, considerando la
2.688 deportistas
Ecocardiogramanormal, 2.485 (92,50%)
Ecocardiogramaanormal, 203 (7,50%)
Interrumpir prácticadeportiva, 4 (0,14%)
Tratamiento específico, 3 (0,11%)
Sin seguimiento*,44 (1,63)
Seguimiento anual,152 (5,65%)
Figura 2. Diagrama de flujo que muestra el diseno del estudio, los resultados de la ecocardiografıa y la conducta seguida. *Deportistas con insuficiencia tricuspıdea omitral ligera.
G. Grazioli et al / Rev Esp Cardiol. 2014;67(9):701–705704
Documento descargado de http://www.revespcardiol.org el 21/04/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

Sudden cardiac death in athletesChristopher Semsarian professor 1 2 3, Joanna Sweeting PhD student 1 2, Michael J Ackerman doctor 4
1Agnes Ginges Centre for Molecular Cardiology, Centenary Institute, Newtown, NSW, 2042, Australia; 2Sydney Medical School, University of Sydney,Sydney, NSW, Australia; 3Department of Cardiology, Royal Prince Alfred Hospital, Sydney, NSW, Australia; 4Departments of Medicine, Pediatrics,and Molecular Pharmacology and Experimental Therapeutics, Divisions of Cardiovascular Diseases and Pediatric Cardiology, Windland Smith RiceSudden Death Genomics Laboratory, Mayo Clinic, Rochester, MN, USA
Sudden cardiac death is defined as an unexpected death,occurring usually within one hour from onset of symptoms incases where the death is witnessed and in unwitnessed caseswithin 24 hours of the individual last being seen alive and well.1Sudden cardiac death in athletes is the leading cause of medicaldeath in this subgroup, with an estimated incidence of 1 in 50000 to 1 in 80 000 athletes per year, although a wide range hasbeen reported, from 1 in 3000 in some subpopulations to 1 in1 000 000.2 Males, black or African Americans, and basketballplayers seem to be at a higher risk than other subgroups.2
Although rare, sudden cardiac death in athletes is importantbecause of its impact within both the sporting community andthe general community. The widely held perception is thatathletes represent examples of health and vitality, so the suddencardiac death of an athlete can evoke strong emotions anddisbelief. The esteem in which athletes are held, in combinationwith often highly emotive reporting from the media, means thatthese events are tragedies not only on a personal family levelbut also at a public level.3 This review summarises the commoncauses of sudden cardiac death in athletes and examines whethersystematic training can confer increased risk for the condition.Also considered are the measures that can be undertaken toprevent sudden cardiac death.
What is an athlete?A competitive athlete is defined as “one who participates in anorganised team or individual sport that requires regularcompetition against others as a central component, places a highpremium on excellence and achievement, and requires someform of systematic (and usually intense) training.”4 Althoughthis generally includes students in high school, college, anduniversity and those participating in paid professional sports,there is no reason that children and adolescents younger than14 years who satisfy this definition should not be considered asathletes. The distinction between competitive athletes and thoseinvolved in recreational sports is in the ability and freedom ofthe participant to judge when it is prudent to pull back or stopphysical exertion, with competitive athletes more likely to beunder the direction and encouragement of someone else, suchas a coach.4
What are the causes of sudden cardiacdeath in athletes?Sudden cardiac death in athletes is most often caused by anunderlying heart condition, which may or may not have beendiagnosed previously. In athletes aged 35 years or older, mostsudden cardiac death events are due to atherosclerotic coronaryartery disease.5 In those under 35, genetic and other acquiredcardiovascular abnormalities, particularly the cardiomyopathies,are more commonly responsible.3 5-7 The box shows the commoncauses of sudden cardiac death in athletes, including structural,arrhythmogenic, and acquired cardiac abnormalities. For manyof these conditions, the sentinel symptom might be suddencardiac death, whereas other athletes may have experiencedprevious symptoms such as syncope, chest pains, and suddenventricular arrhythmias.8 In cases of sudden cardiac death,non-cardiac causes have been excluded and toxicology screensare negative. Autopsy negative sudden unexplained death, whereno cause of death can be determined at postmortem examination,is also important and accounts for approximately 30% of suddendeaths in athletes.7 Diagnosis in these athletes may be madeafter comprehensive cardiac evaluation of family members, withone study reporting diagnosis based on family screening inapproximately 50% of the unexplained deaths in the cohort.9
Inherited causesStudies in the United Kingdom10 and the United States6 havefound definite or possible hypertrophic cardiomyopathy to beone of the most common causes of sudden cardiac death inathletes in these countries. Hypertrophic cardiomyopathy is agenetic condition, with an estimated prevalence of up to 1 in200 and is characterised by unexplained left ventricularhypertrophy, which can lead to ventriculartachycardia/fibrillation and sudden cardiac death.5 11 Otherstudies undertaken in Italy and Denmark found arrhythmogenicright ventricular cardiomyopathy/dysplasia to be a morecommon cause of death than hypertrophic cardiomyopathy inyoung athletes.7 Arrhythmogenic right ventricularcardiomyopathy/dysplasia is another form of genetic
Correspondence to: C Semsarian [email protected]
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2015;350:h1218 doi: 10.1136/bmj.h1218 (Published 18 March 2015) Page 1 of 7
Clinical Review
CLINICAL REVIEW

La muerte súbita se define como aquella muerte inesperada que se produce en menos de una hora desde el inicio de los síntomas (si hay testigos presenciales) o en 24h desde la última vez que el paciente fue visto vivo y sano si no hay testigos.

• La incidencia de muerte súbita en deportistas (MSD)se estima entre 1/50.000 y 1/80.000 aunque distintas series presentas rangos entre 1/3.000 y 1/1.000.000
• Los varones, de raza negra y jugadores de baloncesto parecen presentar un riesgo mayor.
• En un estudio en USA se contabilizaron 10,9 millones de participantes en maraton y media maraton durante el periodo 2000-2010 se produjeron 59 paradas cardiacas (51 hombres) con una edad media de 42 +/- 13 años. Incidencia mas alta en maraton 1,01 por 100.000 que en media maraton 0,27 por 100.000
• La percepción de los deportistas como ejemplo de salud y vitalidad junto a la presentacion emotiva por parte de los medios de comunicación convierten estos episodios en tragedias no solo familiares sino sociales.

¿Cual es la causa de MSD?• En mayores de 35 años la causa principal es la enfermedad coronaria
arteriosclerótica.
• En menores de 35 años las causas mas frecuentes son las alteraciones genéticas y otras anomalías cardiovasculares adquiridas como miocardiopatías.
• En muchos de estos trastornos la manifestación inicial puede ser la muerte súbita, a veces hay antecedentes de síncope, dolores torácicos o arritmias ventriculares.
• Deberan excluirse la ingesta de tóxicos como causa de muerte.
• En un 30% de los casos la autopsia no llega a explicar la causa de la muerte.
• Se debe hacer un estudio cardiológico familiar, lo que ayuda al diagnostico etiológico en 50% de casos

¿Cual es la causa de MSD?• Un estudio realizado en UK y otro en USA muestran que la miocardiopatía
hipertrófica es una de las causas mas frecuentes de MSD. Se trata de una enfermedad congénita con una prevalencia estimada de 1/200 y se caracteriza por una inexplicada HVI que puede producir taquicardia ventricular, fibrilación y muerte súbita.
• Otros estudios realizados en Dinamarca e Italia señalan que la miocardiopatia/displasia arritmogénica del ventrículo derecho es mas frecuente como causa de MSD jóvenes. Se trata de otra forma congénita de miocardiopatía en la que existe una infiltración fibroadiposa del miocardio con dilatacion del ventrículo derecho (aunque puede haber dilatación VI o de ambos ventrículos) tiene una prevalencia de 1/5000 en población general y puede agravarse con el ejercicio intenso.
• Las anomalías congénitas de las arterias coronarias fueron responsables del 17% de las muertes en una cohorte de deportistas.
• Las enfermedades por afectación de los canales de conducción de impulsos, como el síndrome de QT largo familiar, pueden causar MSD y ser responsables de fallecimientos con autopsia negativa.

¿Cual es la causa de MSD?• Otros trastornos arritmogénicos como WPW o la
Taquicardia ventricular polimórfica catecolaminérgica pueden causar MSD precisando mas estudios que demuestren su contribución a la muerte súbita de deportistas
• Las formas adquiridas de MSD incluyen las infecciones víricas que producen miocarditis, los trastornos vasculares como la disección aortica o el abuso de farmacos (incluyendo aquellos para mejorar rendimiento)
• Otra causa adquirida es la Commotio cordis producida al desencadenarse una fibrilación ventricular y muerte súbita tras un traumatismo torácico.

The bottom lineSudden cardiac death in athletes aged less than 35 years is most commonly caused by an underlying genetic heart disorder, such ashypertrophic cardiomyopathy; however, up to half of all sudden cardiac deaths may be associated with a structurally normal heart atpostmortem examination and are referred to as autopsy negative sudden unexplained deathsSystematic and intense physical training can lead to changes in the heart; however, these are not always detrimentalPathological changes to the heart caused by exercise may mimic characteristics of genetic heart diseases—for example, hypertrophyand fibrosisThere is much debate worldwide regarding the implementation and extent of preparticipation screening for athletes, with the main issuebeing the balance between lives saved; athletes tested; psychological, ethical, and legal issues; and the economic costIncreased education and awareness about sudden cardiac death, training in cardiopulmonary resuscitation, and accessibility to automatedexternal defibrillators can help prevent sudden cardiac death in athletes, as well as non-athletes
Sources and selection criteriaWe searched PubMed and the Cochrane Database of Systematic Reviews using the search terms “sudden cardiac death” and “athletes”.To ensure that we represented a diversity of opinion worldwide, particularly on preparticipation screening, we focused on review articles.Owing to the nature of the subject matter, a substantial proportion of the available literature comes from retrospective studies, which canhave limited data. We also consulted comprehensive consensus guideline documents and population based studies.
Causes of sudden cardiac death in athletes. Adapted from Chandra et al 20135
Inherited: structurally abnormal heartCardiomyopathies
• Arrhythmogenic cardiomyopathy, right ventricular cardiomyopathy, or dysplasia• Dilated cardiomyopathy• Hypertrophic cardiomyopathy
Other• Coronary artery abnormalities• Valvular heart disease (for example, bi-leaflet mitral valve prolapse syndrome)• Aortopathies (for example, ascending aortic aneurysm)
Inherited: structurally normal heartChannelopathies
• Brugada syndrome• Catecholaminergic polymorphic ventricular tachycardia• Idiopathic ventricular fibrillation• Long QT syndrome
Acquired: structurally abnormal heart• Ischaemic heart disease• Myocarditis
Acquired: structurally normal heart• Commotio cordis• Substance misuse• Other environmental factors (for example, hypothermia or hyperthermia)
cardiomyopathy, characterised by fibro-fatty replacement in themyocardium and right ventricular dilatation. Biventricularinvolvement and exclusively left ventricular involvement arealso possible. Arrhythmogenic right ventricularcardiomyopathy/dysplasia has a reported overall prevalence of1 in 5000 in the general population and can be exacerbated byintense endurance training.5 Congenital coronary arteryabnormalities also contribute to sudden cardiac death in athletes,with one study showing coronary artery abnormalities to beresponsible for 17% of cardiovascular deaths in a cohort ofathletes.6
In addition to the structural causes of sudden cardiac death,primary arrhythmogenic diseases, also known as the cardiacchannelopathies, contribute to sudden cardiac death in athletes,especially those with autopsy negative sudden unexplaineddeath. These channelopathies, such as familial long QTsyndrome, can cause life threatening ventricular arrhythmias,
including torsade de pointes and ventricular fibrillation, resultingin sudden cardiac death.3 Other arrhythmogenic disorders includeWolff-Parkinson-White syndrome, which can causesupraventricular tachycardia, atrial fibrillation, ventricularfibrillation, and sudden cardiac death, and catecholamingericpolymorphic ventricular tachycardia, which is characterised byexercise induced (or emotional stress induced) polymorphicventricular tachycardia and syncope.5 Further evaluation isrequired to determine the propensity of these conditions to causesudden cardiac death in athletes.
Acquired causesAcquired forms of cardiac abnormalities may be responsiblefor causing sudden cardiac death, such as viral infection leadingto myocarditis, vascular abnormalities such as aortic dissection,or drug misuse (including performance enhancing drugs).3Commotio cordis also falls into this category and involves the
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2015;350:h1218 doi: 10.1136/bmj.h1218 (Published 18 March 2015) Page 2 of 7
CLINICAL REVIEW

T R A B A J O S O R I G I N A L E S
26
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
La muerte súbita en el deporte. Registro en el Estado españolPEDRO MANONELLES MARQUETAa, BEATRIZ AGUILERA TAPIAb, ARACELI BORAITA PÉREZc, EMILIO LUENGO FERNÁNDEZd, CARLOS PONS DE BERISTAINa Y M.a PAZ SUÁREZ MIERb
aFederación Española de Medicina del Deporte. Zaragoza. España.bInstituto Nacional de Toxicología y Ciencias Forenses. Madrid. España.cCentro Nacional de Medicina del Deporte. Consejo Superior de Deportes. Madrid. España.dHospital de la Defensa. Zaragoza. España.
Trabajo realizado con la beca de investigación cardiovascular 2004/2005 de la Fundación MAPFRE Medicina.
Correspondencia: Pedro Manonelles Marqueta. Federación Española de Medicina del Deporte. Asociación Aragonesa. Paseo de Ruiseñores, 2. 50006Zaragoza. España. Correo electrónico: [email protected]
RESUMENIntroducción y objetivos: Este trabajo investiga las cau-sas de muerte súbita en España recogidas a través del Regis-tro Nacional de Muerte Accidental y Súbita en Deportistas.Métodos: Estudio retrospectivo y prospectivo de 180 ca-sos de muerte desde el año 1995 hasta la fecha actual.Resultados: Ciento ochenta casos de muerte súbita: 164varones, 12 mujeres (4 no determinados). Deportes: fútbol(40), ciclismo (39), atletismo (24), fútbol sala y deportes defrontón (8 cada uno) y educación física (7). Las causas másfrecuentes han sido: enfermedad ateromatosa coronaria(48), la miocardiopatía arritmogénica (11), la miocardiopatíahipertrófica (9), las anomalías coronarias congénitas (5), lahipertrofia ventricular izquierda idiopática (4) y la estenosisvalvular aórtica (4). En mayores de 30 años (96): enferme-dad ateromatosa coronaria (73,43%), miocardiopatía arrit-mogénica (6,25%) y miocardiopatía hipertrófica (4,68%). Enlos fallecidos de 30 años o menos (84): miocardiopatía arrit-mogénica (13,72%), la miocardiopatía hipertrófica (11,76%),anomalías coronarias congénitas (9,8%), la hipertrofia ven-tricular izquierda idiopática (7,84%) y estenosis valvular aór-tica (5,88%). En estas edades la mayoría de las muertes fue-ron de origen indeterminado (27,45%).Conclusiones: Dificultad para obtener datos completos demuerte súbita en deportistas en nuestro país, que muestranuna importante incidencia en jóvenes y en adultos de la quin-ta década. Los deportes más implicados son fútbol, ciclismoy atletismo. Causa más frecuente en mayores de 30 años: en-fermedad ateromatosa coronaria, y en menores de 30 años:la muerte inexplicada en corazón estructuralmente normales lo más frecuente. Es necesario profundizar en la obten-ción de los datos de las muertes súbitas en deportistas a tra-vés de este registro.
PALABRAS CLAVE: Muerte súbita en deportistas. Re-gistro de muerte súbita. Deporte.
ABSTRACTIntroduction and objectives: The present article inves-tigates the causes of sudden death in Spain. The data weredrawn from the National Registry of Accidental and SuddenDeath in Athletes.Methods: There were 180 cases of sudden death from 1995to present.Results: 180 cases of sudden death, 166 in males, 12 in fe-males and 4 in which gender was not recorded. Sports: foot-ball (40 cases), cycling (39), athletics (24), futsal and racquetsports (8 each) and physical education (7). The most commoncases of sudden death were atheromatous coronary disease(48 cases), arrhythmogenic cardiomyopathy (11), hypertro-phic cardiomyopathy (9), congenital coronary anomalies (5),idiopathic left ventricular hypertrophy (4), and aortic valvularstenosis (4). In persons aged more than 30 years old (96): at-heromatous coronary disease (73.43%), arrhythmogenic car-diomyopathy (6.25%) and hypertrophic cardiomyopathy(4.68%). In deaths occurring in persons aged 30 years or less(84): arrhythmogenic cardiomyopathy (13.72%), hypertrophiccardiomyopathy (11.76%), congenital coronary anomalies(9.8%), idiopathic left ventricular hypertrophy (7.84%), andaortic valvular stenosis (5.88%). In this age group, most deathswere of undetermined cause (27.45%).Conclusions: It is difficult to obtain complete data on ca-ses of sudden death in Spanish athletes, the incidence ofwhich is considerable in young persons and adults in thefifth decade of life. The most commonly involved sports arefootball, cycling and athletics. After the age of 30 years, themost frequent cause of sudden death is atheromatous co-ronary disease. Below the age of 30 years, the cause withthe greatest incidence is unexplained death occurring in astructurally normal heart. Mechanisms for obtaining moredetailed information on the causes of sudden death in ath-letes should be established through this register.
KEY WORDS: Sudden death in athletes. Registry of sud-den death. Sport.
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
T R A B A J O S O R I G I N A L E S
26
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
La muerte súbita en el deporte. Registro en el Estado españolPEDRO MANONELLES MARQUETAa, BEATRIZ AGUILERA TAPIAb, ARACELI BORAITA PÉREZc, EMILIO LUENGO FERNÁNDEZd, CARLOS PONS DE BERISTAINa Y M.a PAZ SUÁREZ MIERb
aFederación Española de Medicina del Deporte. Zaragoza. España.bInstituto Nacional de Toxicología y Ciencias Forenses. Madrid. España.cCentro Nacional de Medicina del Deporte. Consejo Superior de Deportes. Madrid. España.dHospital de la Defensa. Zaragoza. España.
Trabajo realizado con la beca de investigación cardiovascular 2004/2005 de la Fundación MAPFRE Medicina.
Correspondencia: Pedro Manonelles Marqueta. Federación Española de Medicina del Deporte. Asociación Aragonesa. Paseo de Ruiseñores, 2. 50006Zaragoza. España. Correo electrónico: [email protected]
RESUMENIntroducción y objetivos: Este trabajo investiga las cau-sas de muerte súbita en España recogidas a través del Regis-tro Nacional de Muerte Accidental y Súbita en Deportistas.Métodos: Estudio retrospectivo y prospectivo de 180 ca-sos de muerte desde el año 1995 hasta la fecha actual.Resultados: Ciento ochenta casos de muerte súbita: 164varones, 12 mujeres (4 no determinados). Deportes: fútbol(40), ciclismo (39), atletismo (24), fútbol sala y deportes defrontón (8 cada uno) y educación física (7). Las causas másfrecuentes han sido: enfermedad ateromatosa coronaria(48), la miocardiopatía arritmogénica (11), la miocardiopatíahipertrófica (9), las anomalías coronarias congénitas (5), lahipertrofia ventricular izquierda idiopática (4) y la estenosisvalvular aórtica (4). En mayores de 30 años (96): enferme-dad ateromatosa coronaria (73,43%), miocardiopatía arrit-mogénica (6,25%) y miocardiopatía hipertrófica (4,68%). Enlos fallecidos de 30 años o menos (84): miocardiopatía arrit-mogénica (13,72%), la miocardiopatía hipertrófica (11,76%),anomalías coronarias congénitas (9,8%), la hipertrofia ven-tricular izquierda idiopática (7,84%) y estenosis valvular aór-tica (5,88%). En estas edades la mayoría de las muertes fue-ron de origen indeterminado (27,45%).Conclusiones: Dificultad para obtener datos completos demuerte súbita en deportistas en nuestro país, que muestranuna importante incidencia en jóvenes y en adultos de la quin-ta década. Los deportes más implicados son fútbol, ciclismoy atletismo. Causa más frecuente en mayores de 30 años: en-fermedad ateromatosa coronaria, y en menores de 30 años:la muerte inexplicada en corazón estructuralmente normales lo más frecuente. Es necesario profundizar en la obten-ción de los datos de las muertes súbitas en deportistas a tra-vés de este registro.
PALABRAS CLAVE: Muerte súbita en deportistas. Re-gistro de muerte súbita. Deporte.
ABSTRACTIntroduction and objectives: The present article inves-tigates the causes of sudden death in Spain. The data weredrawn from the National Registry of Accidental and SuddenDeath in Athletes.Methods: There were 180 cases of sudden death from 1995to present.Results: 180 cases of sudden death, 166 in males, 12 in fe-males and 4 in which gender was not recorded. Sports: foot-ball (40 cases), cycling (39), athletics (24), futsal and racquetsports (8 each) and physical education (7). The most commoncases of sudden death were atheromatous coronary disease(48 cases), arrhythmogenic cardiomyopathy (11), hypertro-phic cardiomyopathy (9), congenital coronary anomalies (5),idiopathic left ventricular hypertrophy (4), and aortic valvularstenosis (4). In persons aged more than 30 years old (96): at-heromatous coronary disease (73.43%), arrhythmogenic car-diomyopathy (6.25%) and hypertrophic cardiomyopathy(4.68%). In deaths occurring in persons aged 30 years or less(84): arrhythmogenic cardiomyopathy (13.72%), hypertrophiccardiomyopathy (11.76%), congenital coronary anomalies(9.8%), idiopathic left ventricular hypertrophy (7.84%), andaortic valvular stenosis (5.88%). In this age group, most deathswere of undetermined cause (27.45%).Conclusions: It is difficult to obtain complete data on ca-ses of sudden death in Spanish athletes, the incidence ofwhich is considerable in young persons and adults in thefifth decade of life. The most commonly involved sports arefootball, cycling and athletics. After the age of 30 years, themost frequent cause of sudden death is atheromatous co-ronary disease. Below the age of 30 years, the cause withthe greatest incidence is unexplained death occurring in astructurally normal heart. Mechanisms for obtaining moredetailed information on the causes of sudden death in ath-letes should be established through this register.
KEY WORDS: Sudden death in athletes. Registry of sud-den death. Sport.
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

T R A B A J O S O R I G I N A L E S
28
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
punta. En los casos sin hallazgos patológicos y en los que elanálisis quimicotoxicológico es negativo, se estudia también elsistema de conducción cardíaco21.
RESULTADOS
En la tabla 2 y en la figura 1 se puede ver la distribución defallecimientos por años. Destaca el hecho de que en más del10% –19 concretamente– de los casos conocidos de MSD nose ha podido averiguar el año del fallecimiento.
El número de fallecimientos, en el período comprendidoentre los años 1995 y 2005, es bastante homogéneo: 14,27 ca-sos por año, excepto en 1998, año en que se recogieron 20 ca-sos (11,21% casos del total).
La distribución de fallecimientos, respecto a la actividadpracticada en el momento de la muerte, ha sido muy amplia.La tabla 3 recoge la distribución de fallecimientos por deporteso actividad física practicada en el momento del episodio deMSD. Destacan sobre los demás el fútbol y el ciclismo, con 40y 39 casos, lo que supone porcentajes de 22,22 y del 21,66%,respectivamente.
El tercer deporte es el atletismo, con 24 casos (13,33%), se-guido del fútbol sala y de los deportes de frontón (8 casos cadauno, 4,44%) y de la educación física (7 casos, 3,88%). En 15casos (8,33%) se desconocía el deporte practicado.
Tabla 1 Distribución por edades
Rango (años) Varón Mujer S.I. Total Porcentaje
0-15 7 4 0 11 6,11
16-20 28 2 1 31 17,22
21-25 16 0 0 16 8,88
26-30 15 1 0 16 8,88
31-35 12 1 0 13 7,22
36-40 13 0 0 13 7,22
41-45 20 1 0 21 11,66
46-50 11 0 0 11 6,11
51-55 11 0 0 11 6,11
56-60 8 0 0 8 4,44
61-65 6 0 0 6 3,33
66-70 3 0 0 3 1,66
71-75 3 0 0 3 1,66
76-80 2 0 0 2 1,11
S.I. 9 3 3 15 8,33
Total 164 12 4 180 100,00
S.I.: sin identificar.
Tabla 2 Fallecimientos por años
Año N Porcentaje
1995 10 5,55
1996 9 5,00
1997 17 9,44
1998 20 11,11
1999 15 8,33
2000 11 6,11
2001 14 7,77
2002 16 8,88
2003 16 8,88
2004 14 7,77
2005 15 8,33
2006 4 2,22
Desconocido 19 10,55
Total 180 100,00
20
18
16
14
12
10
8
6
4
2
0
Desc. 1996 1998 2000 2002 2004 2006Anys
Figura 1 Fallecimientos por año.
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

T R A B A J O S O R I G I N A L E S
28
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
punta. En los casos sin hallazgos patológicos y en los que elanálisis quimicotoxicológico es negativo, se estudia también elsistema de conducción cardíaco21.
RESULTADOS
En la tabla 2 y en la figura 1 se puede ver la distribución defallecimientos por años. Destaca el hecho de que en más del10% –19 concretamente– de los casos conocidos de MSD nose ha podido averiguar el año del fallecimiento.
El número de fallecimientos, en el período comprendidoentre los años 1995 y 2005, es bastante homogéneo: 14,27 ca-sos por año, excepto en 1998, año en que se recogieron 20 ca-sos (11,21% casos del total).
La distribución de fallecimientos, respecto a la actividadpracticada en el momento de la muerte, ha sido muy amplia.La tabla 3 recoge la distribución de fallecimientos por deporteso actividad física practicada en el momento del episodio deMSD. Destacan sobre los demás el fútbol y el ciclismo, con 40y 39 casos, lo que supone porcentajes de 22,22 y del 21,66%,respectivamente.
El tercer deporte es el atletismo, con 24 casos (13,33%), se-guido del fútbol sala y de los deportes de frontón (8 casos cadauno, 4,44%) y de la educación física (7 casos, 3,88%). En 15casos (8,33%) se desconocía el deporte practicado.
Tabla 1 Distribución por edades
Rango (años) Varón Mujer S.I. Total Porcentaje
0-15 7 4 0 11 6,11
16-20 28 2 1 31 17,22
21-25 16 0 0 16 8,88
26-30 15 1 0 16 8,88
31-35 12 1 0 13 7,22
36-40 13 0 0 13 7,22
41-45 20 1 0 21 11,66
46-50 11 0 0 11 6,11
51-55 11 0 0 11 6,11
56-60 8 0 0 8 4,44
61-65 6 0 0 6 3,33
66-70 3 0 0 3 1,66
71-75 3 0 0 3 1,66
76-80 2 0 0 2 1,11
S.I. 9 3 3 15 8,33
Total 164 12 4 180 100,00
S.I.: sin identificar.
Tabla 2 Fallecimientos por años
Año N Porcentaje
1995 10 5,55
1996 9 5,00
1997 17 9,44
1998 20 11,11
1999 15 8,33
2000 11 6,11
2001 14 7,77
2002 16 8,88
2003 16 8,88
2004 14 7,77
2005 15 8,33
2006 4 2,22
Desconocido 19 10,55
Total 180 100,00
20
18
16
14
12
10
8
6
4
2
0
Desc. 1996 1998 2000 2002 2004 2006Anys
Figura 1 Fallecimientos por año.
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

La tabla 4 recoge las causas de MSD en los 115 casos en quese ha podido obtener la información del estudio necrópsico.
La primera causa de MSD es la enfermedad ateromatosa coro-naria, que ha estado presente en 48 casos (41,73%). La edad me-dia de los fallecidos era de 48,02 años, con un rango de 28-72 años.
Sigue en orden de frecuencia la miocardiopatía arritmogé-nica, con 11 casos (9,56%) y una edad media de 25,54 años(rango, 13-39); la miocardiopatía hipertrófica, con 9 casos(7,82%) y una edad media de 28,22 años (rango, 11-45 años);las anomalías coronarias congénitas, con 5 casos (4,34%) y una
edad media de 16,8 años (rango, 12-22 años); la hipertrofiaventricular izquierda idiopática (edad media, 24; rango, 18-30años), y la estenosis valvular aórtica (edad media, 26,75; rango,12-53 años), con 4 casos cada una (3,47%).
Se han encontrado 5 casos de miocarditis, 3 casos en formaaguda (2,60%) y 2 en forma crónica (1,73%). También se hanencontrado 2 casos (1,73%) de disección aórtica y de acciden-te cerebrovascular.
Hay un caso (0,86%) de cada una de estas situaciones: bra-diarritmia, comunicación interauricular, coronaria descenden-
Tabla 3 Deportes/actividad física en el momento de la muerte
Deporte Varón Mujer S.I. Total Porcentaje
Fútbol 40a 0 0 40 22,22
Ciclismo 38 1 0 39 21,66
Atletismo (carrera) 19 3 2 24 13,33
Fútbol sala 8 0 0 8 4,44
Deportes de frontón 8 0 0 8 4,44
Baloncesto 7a 0 0 7 3,88
Educación física 4 3 0 7 3,88
Trabajo de gimnasia personal 6 0 0 6 3,33
Montañismo 5 0 0 5 2,77
Natación 4b 1 0 5 2,77
Buceo 1 1 1 3 1,66
Tenis 3 0 0 3 1,66
Bádminton 0 1 0 1 0,55
Ciclismo de montaña 1 0 0 1 0,55
Triatlón 1 0 0 1 0,55
Esquí 0 1 0 1 0,55
Paddle 0 1 0 1 0,55
Pesca 1 0 0 1 0,55
Senderismo 1 0 0 1 0,55
Vela 1 0 0 1 0,55
Pruebas físicas 1 0 0 1 0,55
Bicicleta estática 1 0 0 1 0,55
Deporte S.I. 11 0 0 11 6,11
Desconocido 3 0 1 4 2,22
Total 164 12 4 180 100,00
a1 árbitro.b1 ahogado.S.I.: sin identificar.
T R A B A J O S O R I G I N A L E S
29
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

T R A B A J O S O R I G I N A L E S
30
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
te anterior intramural (puente miocárdico), posible intoxica-ción por flecainida, hipopotasemia, infarto agudo de miocar-dio junto con golpe de calor, golpe de calor, miocardiopatíapor hemocromatosis, miocardiopatía dilatada, prolapso valvu-lar mitral junto con hipertensión arterial, y rotura aórtica.
En el estudio destacan 14 casos (12,17%) de muerte súbi-ta inexplicada, a pesar de haber practicado el procedimientonecrópsico completo. Este grupo tenía una edad media de18,28 años, con un rango de 9-29 años. En el grupo de edadde menos de 30 años, ésta es la causa más frecuente de muertesúbita.
Finalmente, el Registro tiene recogidos 7 casos de pacientesque pudieron ser resucitados en situaciones de paro cardíaco ode fibrilación ventricular por los servicios de urgencia (tabla 5).
Tabla 5 Casos resucitados
Diagnóstico Sexo Edad Deporte
FV por miocardiopatía hemocromatósica V 47 Natación
Parada cardíaca V 58 Ciclismo
FV por hipopotasemia M 32 Atletismo
FV por cardiopatía no especificada V 72 Tenis
Fibrilación ventricular V 51 Tenis
Fibrilación ventricular V 35 Fútbol
Parada cardíaca V 16 Atletismo
FV: fibrilación ventricular; M: mujer; V: varón.
Tabla 4 Causas de muerte súbita
Causa de muerte Rango edad Edad media Varón Mujer N Porcentaje
Enfermedad ateromatosa coronaria 28-72 48,02 48 0 48 41,73
Miocardiopatía arritmogénica 13-39 25,54 11 0 11 9,56
Miocardiopatía hipertrófica 11-45 28,22 7 2 9 7,82
Anomalía coronaria 12-22 16,8 3 2 5 4,34
Hipertrofia ventricular izquierda 18-30 24 4 0 4 3,47
Estenosis valvular aórtica 12-53 26,75 4 0 4 3,47
Miocarditis aguda 21-54 32 3 0 3 2,60
Miocarditis crónica 20-31 – 2 0 2 1,73
Disección aórtica 20-79 – 2 0 2 1,73
Fibrosis cardíaca 17-20 – 2 0 2 1,73
Accidente cerebrovascular 26-57 – 2 0 2 1,73
Bradiarritmia 32 – 1 0 1 0,86
Comunicación interauricular 17 – 1 0 1 0,86
Coronaria descendente anterior intramural 79 – 1 0 1 0,86
Intoxicación por flecainida 51 – 1 0 1 0,86
IAM y golpe de calor 41 – 1 0 1 0,86
Golpe de calor 22 – 1 0 1 0,86
Miocardiopatía dilatada 14 – 1 0 1 0,86
PVM e HTA 47 – 1 0 1 0,86
Rotura aórtica 16 – 1 0 1 0,86
Inexplicada 9-29 18,28 11 2 14 12,17
Total 9-79 – 108 7 115 100,00
IAM: infarto agudo de miocardio; HTA: hipertensión arterial; PVM: prolapso de la válvula mitral.
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

La edad media de este grupo fue de 35,6 años, con un rango de16-58 años.
El análisis de las causas de MSD difiere según la edad.En sujetos de edad superior a 30 años (tabla 6) la causa más
frecuente de MSD es la enfermedad ateromatosa coronaria,con 47 de los 64 casos estudiados, lo que supone el 73,43%.
Hay 4 casos de miocardiopatía arritmogénica (6,25%) y 3casos (4,68%) de miocardiopatía hipertrófica.
Hay un caso (1,56%) de cada uno de los siguientes diag-nósticos: infarto agudo de miocardio junto con golpe de calor,miocardiopatía por hemocromatosis, prolapso valvular mitraljunto a hipertensión, intoxicación por flecainida, estenosis val-vular aórtica, miocarditis aguda, miocarditis crónica, coronariadescendente anterior intramural, disección aórtica, accidentecerebrovascular, hipopotasemia y bradiarritmia.
En los fallecidos de 30 años o menos (tabla 7), la etiología deMSD difiere notablemente del grupo anterior, como es bien co-nocido. Concretamente en nuestra serie las causas más frecuen-tes han sido la miocardiopatía arritmogénica, con 7 casos(13,72%); la miocardiopatía hipertrófica, con 6 casos (11,76%);
las anomalías coronarias congénitas, con 5 casos (9,8%); la hi-pertrofia ventricular izquierda, con 4 casos (7,84%), y la esteno-sis valvular aórtica, con 3 casos (5,88%).
Se han detectado 2 casos de miocarditis aguda y de fibrosiscardíaca (3,92%). Ha habido un caso (1,96%) de los siguien-tes diagnósticos: disección aórtica, enfermedad ateromatosa co-ronaria, comunicación interauricular, miocarditis crónica, gol-pe de calor, miocardiopatía dilatada, rotura aórtica y accidentecerebrovascular.
Hay que destacar que en este grupo de edad la mayoría de lasmuertes fueron de origen indeterminado (14 casos, 27,45%) apesar de haber practicado el procedimiento necrópsico completo.
DISCUSIÓN
Como sucede en todas las series de estudio de MSD, la in-cidencia en mujeres es extraordinariamente más baja que en va-rones, con el 1,96-8,75% de los fallecimientos27-29. En el pre-sente estudio la incidencia es del 6,81% (12 casos de mujeresde los 176 casos en que se conocía el sexo del fallecido).
Tabla 6 Causas de muerte súbita en deportistasmayores de 30 años
Causa de muerte Varón Mujer N Porcentaje
Enfermedad ateromatosa coronaria 47 0 47 73,43
Miocardiopatía arritmogénica 4 0 4 6,25
Miocardiopatía hipertrófica 2 1 3 4,68
IAM y golpe de calor 1 0 1 1,56
PVM e HTA 1 0 1 1,56
Intoxicación por flecainida 1 0 1 1,56
Estenosis valvular aórtica 1 0 1 1,56
Miocarditis aguda 1 0 1 1,56
Miocarditis crónica 1 0 1 1,56
Coronaria descendente anterior intramural 1 0 1 1,56
Disección aórtica 1 0 1 1,56
Accidente cerebrovascular 1 0 1 1,56
Bradiarritmia 1 0 1 1,56
Total 63 1 64 100,00
IAM: infarto agudo de miocardio; HTA: hipertensión arterial; PVM: prolapso de la vál-vula mitral.
Tabla 7 Causas de muerte súbita en deportistas de 30 años o menos
Causa de muerte Varón Mujer N Porcentaje
Miocardiopatía arritmogénica 7 0 7 13,72
Miocardiopatía hipertrófica 5 1 6 11,76
Anomalía coronaria 3 2 5 9,8
Hipertrofia ventricular izquierda 4 0 4 7,84
Estenosis valvular aórtica 3 0 3 5,88
Miocarditis aguda 2 0 2 3,92
Fibrosis cardíaca 2 0 2 3,92
Disección aórtica 1 0 1 1,96
Enfermedad ateromatosa coronaria 1 0 1 1,96
Comunicación interauricular 1 0 1 1,96
Miocarditis crónica 1 0 1 1,96
Golpe de calor 1 0 1 1,96
Miocardiopatía dilatada 1 0 1 1,96
Rotura aórtica 1 0 1 1,96
Accidente cerebrovascular 1 0 1 1,96
Inexplicada 11 3 14 27,45
Total 45 6 51 100,00
T R A B A J O S O R I G I N A L E S
31
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

La edad media de este grupo fue de 35,6 años, con un rango de16-58 años.
El análisis de las causas de MSD difiere según la edad.En sujetos de edad superior a 30 años (tabla 6) la causa más
frecuente de MSD es la enfermedad ateromatosa coronaria,con 47 de los 64 casos estudiados, lo que supone el 73,43%.
Hay 4 casos de miocardiopatía arritmogénica (6,25%) y 3casos (4,68%) de miocardiopatía hipertrófica.
Hay un caso (1,56%) de cada uno de los siguientes diag-nósticos: infarto agudo de miocardio junto con golpe de calor,miocardiopatía por hemocromatosis, prolapso valvular mitraljunto a hipertensión, intoxicación por flecainida, estenosis val-vular aórtica, miocarditis aguda, miocarditis crónica, coronariadescendente anterior intramural, disección aórtica, accidentecerebrovascular, hipopotasemia y bradiarritmia.
En los fallecidos de 30 años o menos (tabla 7), la etiología deMSD difiere notablemente del grupo anterior, como es bien co-nocido. Concretamente en nuestra serie las causas más frecuen-tes han sido la miocardiopatía arritmogénica, con 7 casos(13,72%); la miocardiopatía hipertrófica, con 6 casos (11,76%);
las anomalías coronarias congénitas, con 5 casos (9,8%); la hi-pertrofia ventricular izquierda, con 4 casos (7,84%), y la esteno-sis valvular aórtica, con 3 casos (5,88%).
Se han detectado 2 casos de miocarditis aguda y de fibrosiscardíaca (3,92%). Ha habido un caso (1,96%) de los siguien-tes diagnósticos: disección aórtica, enfermedad ateromatosa co-ronaria, comunicación interauricular, miocarditis crónica, gol-pe de calor, miocardiopatía dilatada, rotura aórtica y accidentecerebrovascular.
Hay que destacar que en este grupo de edad la mayoría de lasmuertes fueron de origen indeterminado (14 casos, 27,45%) apesar de haber practicado el procedimiento necrópsico completo.
DISCUSIÓN
Como sucede en todas las series de estudio de MSD, la in-cidencia en mujeres es extraordinariamente más baja que en va-rones, con el 1,96-8,75% de los fallecimientos27-29. En el pre-sente estudio la incidencia es del 6,81% (12 casos de mujeresde los 176 casos en que se conocía el sexo del fallecido).
Tabla 6 Causas de muerte súbita en deportistasmayores de 30 años
Causa de muerte Varón Mujer N Porcentaje
Enfermedad ateromatosa coronaria 47 0 47 73,43
Miocardiopatía arritmogénica 4 0 4 6,25
Miocardiopatía hipertrófica 2 1 3 4,68
IAM y golpe de calor 1 0 1 1,56
PVM e HTA 1 0 1 1,56
Intoxicación por flecainida 1 0 1 1,56
Estenosis valvular aórtica 1 0 1 1,56
Miocarditis aguda 1 0 1 1,56
Miocarditis crónica 1 0 1 1,56
Coronaria descendente anterior intramural 1 0 1 1,56
Disección aórtica 1 0 1 1,56
Accidente cerebrovascular 1 0 1 1,56
Bradiarritmia 1 0 1 1,56
Total 63 1 64 100,00
IAM: infarto agudo de miocardio; HTA: hipertensión arterial; PVM: prolapso de la vál-vula mitral.
Tabla 7 Causas de muerte súbita en deportistas de 30 años o menos
Causa de muerte Varón Mujer N Porcentaje
Miocardiopatía arritmogénica 7 0 7 13,72
Miocardiopatía hipertrófica 5 1 6 11,76
Anomalía coronaria 3 2 5 9,8
Hipertrofia ventricular izquierda 4 0 4 7,84
Estenosis valvular aórtica 3 0 3 5,88
Miocarditis aguda 2 0 2 3,92
Fibrosis cardíaca 2 0 2 3,92
Disección aórtica 1 0 1 1,96
Enfermedad ateromatosa coronaria 1 0 1 1,96
Comunicación interauricular 1 0 1 1,96
Miocarditis crónica 1 0 1 1,96
Golpe de calor 1 0 1 1,96
Miocardiopatía dilatada 1 0 1 1,96
Rotura aórtica 1 0 1 1,96
Accidente cerebrovascular 1 0 1 1,96
Inexplicada 11 3 14 27,45
Total 45 6 51 100,00
T R A B A J O S O R I G I N A L E S
31
A P U N T S . M E D I C I N A D E L ’ E S P O R T . 2 0 0 7 ; 1 5 3 : 2 6 - 3 5
Documento descargado de http://www.apunts.org el 07/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

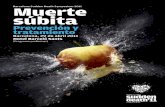
uno de ellos era mujer. Dos fueron formas septales asi-métricas (fig. 2) y otras dos MCH simétricas. En todoslos casos existía extenso desorden de fibras (fig. 3).
En los 3 pacientes con HVI el peso cardíaco era su-perior al 20% del máximo estimado para el peso cor-poral, con una media de 500 ± 36 g. En el primer casoel peso corporal no era conocido, pero el peso cardíacoera tal (512 g) que lo consideramos patológico. Un va-rón de 20 años era jugador profesional de baloncesto yen un chico de 18 años se encontraron, además de lahipertrofia cardíaca, signos de bronquitis asmática conescasos tapones de moco intrabronquiales con intensi-dad insuficiente para explicar la muerte.
En otros 2 corazones, pertenecientes a 2 varones de20 y 17 años, respectivamente, se apreciaron extensaslesiones cicatrizales subepicárdicas en pared libre delventrículo izquierdo, en un caso, y biventricular enotro (tabla 1), con arterias coronarias permeables. Elsegundo había sido sometido a revisión médica pocoantes de su muerte sin que se apreciara nada patológi-co. Un chico de 14 años que falleció jugando al fútbolpresentaba una miocardiopatía dilatada (MCD), proba-ble secuela de una miocarditis que había padecido enla infancia, con hipertrofia y dilatación biventricular.
En 2 varones de 22 y 16 años, respectivamente, seapreciaron anomalías en el origen de las arterias coro-narias. El primero falleció tras recorrer 30 km en bici-cleta y en su corazón se apreció que el ostium corona-rio izquierdo estaba situado en el seno de Valsalvaderecho y la coronaria izquierda discurría dentro de laadventicia aórtica (fig. 4), hasta su división en las co-ronarias descendente anterior y circunfleja. En el se-gundo, el ostium coronario derecho se situaba sobre lacomisura entre los senos de Valsalva derecho e iz-quierdo, con un trayecto de unos 5 mm entre la arteria
350 Rev Esp Cardiol 2002;55(4):347-58 52
Suárez-Mier MP, et al. Causas de muerte súbita asociadas al deporte en España
Fig. 1. Miocardiopatía arritmogénica biventricular. Dilatación del ven-trículo derecho con notable infiltración adiposa transmural. Bandasubepicárdica circunferencial de coloración pardogrisácea en el ven-trículo izquierdo. El estudio microscópico demostró la sustitución delmiocardio por tejido fibroadiposo con arterias coronarias permeables,lo que permitió establecer el diagnóstico.
Fig. 2. Miocardiopatía hipertrófica. Sección transversal biventricular delcorazón de un varón de 30 años que falleció practicando ciclismo. Su co-razón pesaba 405 g y presentaba una hipertrofia septal asimétrica, queprácticamente ocluía la luz ventricular, y parches blanquecinos de fibrosis.
Fig. 3. Aspecto desordenado de las fibras miocárdicas con imágenesen remolino y parches de fibrosis característico de la miocardiopatíahipertrófica. Tricrómico de Masson, MO ×10.
Fig. 4. Origen anómalo de la coronaria izquierda en el seno de Valsalvaderecho. Trayecto inicial en el espesor de la pared de la aorta (flecha).
Documento descargado de http://www.revespcardiol.org el 09/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

uno de ellos era mujer. Dos fueron formas septales asi-métricas (fig. 2) y otras dos MCH simétricas. En todoslos casos existía extenso desorden de fibras (fig. 3).
En los 3 pacientes con HVI el peso cardíaco era su-perior al 20% del máximo estimado para el peso cor-poral, con una media de 500 ± 36 g. En el primer casoel peso corporal no era conocido, pero el peso cardíacoera tal (512 g) que lo consideramos patológico. Un va-rón de 20 años era jugador profesional de baloncesto yen un chico de 18 años se encontraron, además de lahipertrofia cardíaca, signos de bronquitis asmática conescasos tapones de moco intrabronquiales con intensi-dad insuficiente para explicar la muerte.
En otros 2 corazones, pertenecientes a 2 varones de20 y 17 años, respectivamente, se apreciaron extensaslesiones cicatrizales subepicárdicas en pared libre delventrículo izquierdo, en un caso, y biventricular enotro (tabla 1), con arterias coronarias permeables. Elsegundo había sido sometido a revisión médica pocoantes de su muerte sin que se apreciara nada patológi-co. Un chico de 14 años que falleció jugando al fútbolpresentaba una miocardiopatía dilatada (MCD), proba-ble secuela de una miocarditis que había padecido enla infancia, con hipertrofia y dilatación biventricular.
En 2 varones de 22 y 16 años, respectivamente, seapreciaron anomalías en el origen de las arterias coro-narias. El primero falleció tras recorrer 30 km en bici-cleta y en su corazón se apreció que el ostium corona-rio izquierdo estaba situado en el seno de Valsalvaderecho y la coronaria izquierda discurría dentro de laadventicia aórtica (fig. 4), hasta su división en las co-ronarias descendente anterior y circunfleja. En el se-gundo, el ostium coronario derecho se situaba sobre lacomisura entre los senos de Valsalva derecho e iz-quierdo, con un trayecto de unos 5 mm entre la arteria
350 Rev Esp Cardiol 2002;55(4):347-58 52
Suárez-Mier MP, et al. Causas de muerte súbita asociadas al deporte en España
Fig. 1. Miocardiopatía arritmogénica biventricular. Dilatación del ven-trículo derecho con notable infiltración adiposa transmural. Bandasubepicárdica circunferencial de coloración pardogrisácea en el ven-trículo izquierdo. El estudio microscópico demostró la sustitución delmiocardio por tejido fibroadiposo con arterias coronarias permeables,lo que permitió establecer el diagnóstico.
Fig. 2. Miocardiopatía hipertrófica. Sección transversal biventricular delcorazón de un varón de 30 años que falleció practicando ciclismo. Su co-razón pesaba 405 g y presentaba una hipertrofia septal asimétrica, queprácticamente ocluía la luz ventricular, y parches blanquecinos de fibrosis.
Fig. 3. Aspecto desordenado de las fibras miocárdicas con imágenesen remolino y parches de fibrosis característico de la miocardiopatíahipertrófica. Tricrómico de Masson, MO ×10.
Fig. 4. Origen anómalo de la coronaria izquierda en el seno de Valsalvaderecho. Trayecto inicial en el espesor de la pared de la aorta (flecha).
Documento descargado de http://www.revespcardiol.org el 09/05/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.

¿Puede el ejercicio desencadenar una MSD?
• Los trastornos cardiacos, como la hipertrofia o fibrosis constituyen un sustrato y el ejercicio actuaría como desencadenante produciendo arritmias inducidas por cambios fisiológicos con aumento de catecolaminas, acidosis y deshidratación.
• Un estudio prospectivo en Italia muestra un riesgo relativo mas elevado en deportistas competitivos mientras que otro danes no demuestra un aumento de muerte subita entre deportistas competitivos comparado con aquellos que realizan deporte recreativo.

Figures
Fig 1 Important diagnostic features compatible with both physiologically based adaptions to athletic training (athlete’s heart)and cardiomyopathies. Adapted from Maron et al 20033
Fig 2 Important clinical history, examination findings, and basic cardiac investigations that may indicate underlying cardiacdisease in athletes5 37
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2015;350:h1218 doi: 10.1136/bmj.h1218 (Published 18 March 2015) Page 7 of 7
CLINICAL REVIEW

¿Puede el entrenamiento intensivo producir una remodelación cardiaca y MSD?
• Desde el siglo XIX sabemos que el corazon de un deportista difiere del de una persona sedentaria.
• El entrenamiento sistemático induce cambios estructurales, funcionales y remodelación en la conducción electrica que se manifiesta en cambios en ECG: bradicardia y trastornos de repolarización.
• Sin embargo algunos trastornos cardiovasculares (cardiomiopatías) pueden confundirse con el “corazon del deportista”.
• Los cambios estructurales dependen del tipo de actividad: hipertrofia excentrica (hipertrofia con una gran cavidad ventricular izquierda) en practicantes de ejercicio dinámico como corredores de fondo, o hipertrofia concéntrica (con cavidad ventricular cercana a normalidad) en deportistas que realizan ejercicio estático como levantadores de peso.

¿Puede el entrenamiento intensivo producir una remodelación cardiaca y MSD?
• Cambios en remodelación electrica producen bradicardia sinusal y bloqueo incompleto de rama izquierda. Sin embargo la presencia de inversión inferolateral de ondas T, bloqueo completo de rama izquierda y ondas Q patológicas pueden mostrar enfermedad subyacente.
• La displasia/miocardiopatia arritmogénica del ventrículo derecho es un trastorno genético caracterizado por la atrofia del miocardio y la sustitución por tejido fibrosoadiposo del miocardio del ventrículo derecho. En estos pacientes el ejercicio intenso podria inducir lesiones cardiacas microscópicas y dilatacion progresiva de VD produciendo la denominada “displasia/miocardiopatia arritmogénica del ventrículo derechoel ejercicio”.

MYOCARDIAL DISEASE
The athlete’s heartDavid L Prior,1,2 Andre La Gerche2,3
Athlete’s heart is the term given to the complex ofstructural, functional, and electrical remodellingthat accompanies regular athletic training. It is animportant physiological adaption which helpsathletes perform better in physical tasks than non-athletes and one of the physiological changes thatmay make a good athlete great. The fact that theheart of an athlete is different to the non-athlete’swas recognised in the late 19th century based onclinical examination, with the recognition ofcardiac enlargement and bradycardia among morehighly trained athletes. Our understanding of thissyndrome has gradually expanded in parallel withthe development of new invasive and non-invasivetools for the examination of cardiac structure andfunction. Initially, the chest x-ray and ECGdemonstrated important features of cardiacchamber enlargement in athletes. The next stepsincorporated invasive haemodynamic measures atrest and with exercise. An additional source ofunderstanding of the athlete’s heart has beenexamination of cardiac pathology specimens. Morerecently the use of imaging techniques such asechocardiography and cardiac MRI have playeda central role in advancing our understanding ofwhat constitutes an athlete’s heart and in applyingthis information in clinical settings.Study of the athlete’s heart has been undertaken
and is important for a number of key reasons: first,to understand how cardiac adaptation contributesto improved athletic performance; second, to guidedevelopment of training regimens which will opti-mise cardiac adaptation and thus enhance athleticperformance; and third, to allow differentiation ofthe normal athlete’s heart from important diseasestates which may share similar morphologicfeatures. It is the third of these reasons that hasassumed most importance in the cardiology andsports medicine worlds.The aim of this article is for clinicians to learn
about the key features of the athlete’s heart and tounderstand concepts used to differentiate normalfindings in an athlete from the presence of cardiacpathology such as hypertrophy cardiomyopathy(HCM), dilated cardiomyopathy (DCM), andarrhythmogenic right ventricular cardiomyopathy(ARVC) when faced with a specific clinicalscenario. The process of cardiac remodelling will beexamined as will the limits of what may beconsidered normal cardiac structure and function inan athlete.
EFFECT OF EXERCISE ON THE HEARTDifferent forms of exercise impose differing loadson the cardiovascular system. A variety of terms
have been used to describe this, but, put simply,pure endurance sports tend to place a high dynamic(isotonic) load on working muscles, and purestrength sports place a high static (isometric) loadon the muscles. Dynamic exercise results inincreased cardiac output through increases in heartrate and stroke volume, reduced peripheral resis-tance and a moderate increase in systemic bloodpressure. Thus the load to which the heart issubjected is predominantly a volume load (figure 1).In contrast, the major physiological change withstatic exercise is a pronounced increase in bothsystolic and diastolic blood pressure accompaniedby only small increases in heart rate, stroke volume,and cardiac output. Thus, the major load is that ofpressure. The differential effects of pressure andvolume loading during training was first docu-mented in the seminal work by Morganroth,1 inwhich it was identified that although all athleteshad increased left ventricular (LV) mass, in swim-mers and runners the major finding was ofincreased LV dimensions while in wrestlers themajor finding was of increased wall thickness.Although a dichotomous effect of exercise oncardiac structure would be convenient, most sportsare not solely dynamic or static in the load theyimpose on the heart. Sports themselves may vary inthe proportion of each of these components andcan therefore be classified by the relative require-ments for static (strength) and dynamic (endur-ance) demands,2 and this is summarised in table 1.
STRUCTURAL REMODELLINGLeft ventricleNumerous studies examining the structuralchanges in the LV of athletes have defined changescommon to all forms of training in addition tothose which may differ between different sports ortypes of training. Some difficulties in interpretationof the literature result from the fact that manystudies of athlete’s heart involve discrete groups ofathletes undertaking only one specific form ofexercise, and the intensity of activity may also vary.This makes direct comparison of these studiesproblematic.As previously outlined, the hallmark of all forms
of athlete’s heart is hypertrophy of the LV whichmay be eccentric or concentric in nature. Buildingon the work of Morganroth,1 Fagard3 and otherinvestigators, an extensive meta-analysis by Pluimet al, published in 2000, examined changes inparameters of LV structure, comparing endurancetrained athletes, strength trained athletes, andcombined strength and endurance trained athleteswith non-athletic controls.4 They found that LV
< Additional references arepublished online only. To viewthese references please visit thejournal online (http://heart.bmj.com/content/98/12.toc).1Department of Cardiology, StVincent’s Hospital, Melbourne,Australia2Department of Medicine, StVincent’s Hospital, University ofMelbourne, Melbourne,Australia3Department of CardiovascularMedicine, University Hospital,University of Leuven, Leuven,Belgium
Correspondence toAssociate Professor David L Prior,Department of Cardiology, StVincent’s Hospital, Melbourne,PO Box 2900, Fitzroy, VIC 3065,Australia;[email protected]
Heart 2012;98:947e955. doi:10.1136/heartjnl-2011-301329 947
Education in Heart
group.bmj.com on November 19, 2014 - Published by http://heart.bmj.com/Downloaded from
MYOCARDIAL DISEASE
The athlete’s heartDavid L Prior,1,2 Andre La Gerche2,3
Athlete’s heart is the term given to the complex ofstructural, functional, and electrical remodellingthat accompanies regular athletic training. It is animportant physiological adaption which helpsathletes perform better in physical tasks than non-athletes and one of the physiological changes thatmay make a good athlete great. The fact that theheart of an athlete is different to the non-athlete’swas recognised in the late 19th century based onclinical examination, with the recognition ofcardiac enlargement and bradycardia among morehighly trained athletes. Our understanding of thissyndrome has gradually expanded in parallel withthe development of new invasive and non-invasivetools for the examination of cardiac structure andfunction. Initially, the chest x-ray and ECGdemonstrated important features of cardiacchamber enlargement in athletes. The next stepsincorporated invasive haemodynamic measures atrest and with exercise. An additional source ofunderstanding of the athlete’s heart has beenexamination of cardiac pathology specimens. Morerecently the use of imaging techniques such asechocardiography and cardiac MRI have playeda central role in advancing our understanding ofwhat constitutes an athlete’s heart and in applyingthis information in clinical settings.Study of the athlete’s heart has been undertaken
and is important for a number of key reasons: first,to understand how cardiac adaptation contributesto improved athletic performance; second, to guidedevelopment of training regimens which will opti-mise cardiac adaptation and thus enhance athleticperformance; and third, to allow differentiation ofthe normal athlete’s heart from important diseasestates which may share similar morphologicfeatures. It is the third of these reasons that hasassumed most importance in the cardiology andsports medicine worlds.The aim of this article is for clinicians to learn
about the key features of the athlete’s heart and tounderstand concepts used to differentiate normalfindings in an athlete from the presence of cardiacpathology such as hypertrophy cardiomyopathy(HCM), dilated cardiomyopathy (DCM), andarrhythmogenic right ventricular cardiomyopathy(ARVC) when faced with a specific clinicalscenario. The process of cardiac remodelling will beexamined as will the limits of what may beconsidered normal cardiac structure and function inan athlete.
EFFECT OF EXERCISE ON THE HEARTDifferent forms of exercise impose differing loadson the cardiovascular system. A variety of terms
have been used to describe this, but, put simply,pure endurance sports tend to place a high dynamic(isotonic) load on working muscles, and purestrength sports place a high static (isometric) loadon the muscles. Dynamic exercise results inincreased cardiac output through increases in heartrate and stroke volume, reduced peripheral resis-tance and a moderate increase in systemic bloodpressure. Thus the load to which the heart issubjected is predominantly a volume load (figure 1).In contrast, the major physiological change withstatic exercise is a pronounced increase in bothsystolic and diastolic blood pressure accompaniedby only small increases in heart rate, stroke volume,and cardiac output. Thus, the major load is that ofpressure. The differential effects of pressure andvolume loading during training was first docu-mented in the seminal work by Morganroth,1 inwhich it was identified that although all athleteshad increased left ventricular (LV) mass, in swim-mers and runners the major finding was ofincreased LV dimensions while in wrestlers themajor finding was of increased wall thickness.Although a dichotomous effect of exercise oncardiac structure would be convenient, most sportsare not solely dynamic or static in the load theyimpose on the heart. Sports themselves may vary inthe proportion of each of these components andcan therefore be classified by the relative require-ments for static (strength) and dynamic (endur-ance) demands,2 and this is summarised in table 1.
STRUCTURAL REMODELLINGLeft ventricleNumerous studies examining the structuralchanges in the LV of athletes have defined changescommon to all forms of training in addition tothose which may differ between different sports ortypes of training. Some difficulties in interpretationof the literature result from the fact that manystudies of athlete’s heart involve discrete groups ofathletes undertaking only one specific form ofexercise, and the intensity of activity may also vary.This makes direct comparison of these studiesproblematic.As previously outlined, the hallmark of all forms
of athlete’s heart is hypertrophy of the LV whichmay be eccentric or concentric in nature. Buildingon the work of Morganroth,1 Fagard3 and otherinvestigators, an extensive meta-analysis by Pluimet al, published in 2000, examined changes inparameters of LV structure, comparing endurancetrained athletes, strength trained athletes, andcombined strength and endurance trained athleteswith non-athletic controls.4 They found that LV
< Additional references arepublished online only. To viewthese references please visit thejournal online (http://heart.bmj.com/content/98/12.toc).1Department of Cardiology, StVincent’s Hospital, Melbourne,Australia2Department of Medicine, StVincent’s Hospital, University ofMelbourne, Melbourne,Australia3Department of CardiovascularMedicine, University Hospital,University of Leuven, Leuven,Belgium
Correspondence toAssociate Professor David L Prior,Department of Cardiology, StVincent’s Hospital, Melbourne,PO Box 2900, Fitzroy, VIC 3065,Australia;[email protected]
Heart 2012;98:947e955. doi:10.1136/heartjnl-2011-301329 947
Education in Heart
group.bmj.com on November 19, 2014 - Published by http://heart.bmj.com/Downloaded from

RV to generate the same stroke volume at rest.Ambiguities may be resolved by studying RVfunction when under the exercise demands ofincreased pressure and volume load.
ELECTRICAL REMODELLINGIn addition to structural and functional remodel-ling, it is recognised that there is electrical remod-elling of the athlete’s heart in response to training,resulting in distinct changes in the ECG. It isimportant for the clinician to be able to correctlyidentify those changes which result from intensephysical training and do not carry an increased riskof adverse cardiac outcomes, in addition to identi-fying ECG changes which are associated withunderlying cardiac diseases and may result incardiac events, the risk of which may be increasedby participation in sport.w14 HCM, ARVC, and thechannelopathies represent some of the pathologiesmost frequently associated with sudden cardiacdeath in athletes aged <35 years, with HCM beingmost common. ECG changes frequently precedethe phenotypic structural changes of HCM andARVC and may be the sole marker of an increasedrisk of sudden cardiac death early in the diseaseprocess. The channelopathies (long and short QTsyndromes, Brugada syndrome, and catecholamin-ergic polymorphic ventricular tachycardia (VT)) areseldom associated with morphologic abnormalities,and diagnosis depends upon the identification ofcharacteristic ECG changes and/or familial history.Based on this rationale, preparticipation screeningof competitive athletes is mandated in manycountries and sporting competitions, andfrequently includes an ECG in addition to a clinicalassessment. Accurate interpretation of the ECG, inthe light of known changes of electrical remodellingseen with the athlete’s heart, will result in lessunnecessary investigation and exclusion of athletes
based on ECG abnormalities which may beconsidered acceptable in an athlete.The most commonly observed forms of electrical
remodelling include sinus bradycardia, sinusarrhythmia or first degree atrioventricular (AV)block, largely due to high vagal tone at rest. TheEuropean Society of Cardiology recently publishedguidelines for interpretation of the 12 lead ECG inthe athlete. These guidelines provide a clinicallyuseful classification of ECG abnormalities into:those which are considered common and related totraining, and are therefore part of the spectrum ofelectrical remodelling in the athlete’s heart; andthose which are uncommon and training unrelated,and should prompt examination for underlyingcardiac pathology.13 This document provides a verypractical framework for evaluation of electricalremodelling. In short, sinus bradycardia, first degreeAV block, incomplete RBBB, early repolarisationand voltage criteria for LVH may be considerednormal electrical remodelling of the athlete’s heart.Some of these reflect the underlying structuralremodelling such as development of LVH.w14 Otherabnormalities such as T wave inversion, completebundle branch blocks, and left atrial enlargementon ECG are not regarded as training related changesreflecting a normal athlete’s heart, and furtherevaluation for pathology is recommended (table 2).There is, however, variability in what constitutes
normal electrical remodelling based on gender, race,and type of training. There may also be interactionof these factors. Compared to female athletes, maleathletes have a much higher prevalence ofabnormal ECG findings that may reflect, but arenot diagnostic of, cardiac disease.w15 Normal blackathletes have a higher prevalence of voltage criteriafor LVH, ST segment abnormalities, and deep Twave inversion than both male14 w16and female15
white athletes. Endurance training has been asso-ciated with a higher rate of ECG changes than non-endurance sports.w15 It should be noted, however,that many athletes with ECG changes consideredabnormal which are detected at screening andrequiring further cardiac assessment are found tohave no underlying structural cardiac disease, and
Figure 3 An example of right ventricular free wall strain imaging using colour codedtissue Doppler imaging. Peak systolic strain is relatively reduced in the basal segment ofthis healthy endurance athlete’s heart as has been described by Teske et al.w12 Of note,there is also post-systolic shortening with the peak shortening occurring later than themore apical segments and after aortic valve closure.
Table 2 ECG findings considered normal and abnormalfor the athlete’s heart (adapted from Corrado et al13)Normal athlete’s heart Abnormal finding
Sinus bradycardia T wave inversion
First degree AV block ST segment depression
Incomplete RBBB Pathological Q waves
Early repolarisation Left atrial enlargement
Isolated QRS voltagecriteria for LVH
Left axis deviation/left anteriorfascicular block
Right axis deviation/left posteriorfascicular block
Right ventricular hypertrophy
Ventricular pre-excitation
Complete LBBB or RBBB
Long or short QT interval
Brugada-like early repolarisation
AV, atrioventricular; LBBB, left bundle branch block; LVH, left ventricularhypertrophy; RBBB, right bundle branch block.
950 Heart 2012;98:947e955. doi:10.1136/heartjnl-2011-301329
Education in Heart
group.bmj.com on November 19, 2014 - Published by http://heart.bmj.com/Downloaded from

mass was increased in all groups of athletescompared to control subjects, with no difference inLV mass between the three groups of athletes.Although it is usually assumed that strengthtrained athletes who may generate very high bloodpressures during training would develop a concen-tric pattern of LV hypertrophy (LVH) with smallcavity dimensions, increased LV mass and wallthickness, the available evidence does not supportthis. Strength trained athletes in fact have LVcavity sizes that are similar or slightly larger thansedentary controls,1 4 although wall thicknessrelative to cavity size does tend to be higher thancontrols and endurance athletes. This may be usefulin differentiating athlete’s heart from HCM, inwhich cavity sizes tend to be small, and it has beensuggested that a cavity size <45 mm stronglyfavours a diagnosis of HCM.w1
Right ventricleIn endurance trained athletes, the right ventricle(RV) is subjected to the same volume load as the
left side, and increased RV volume, mass, and strokevolume have all been observed in athletes, largelybased on measurements using cardiac MRI. Thephenomenon of balanced dilation of the RV, similarto increases in LV volume, has been described inthese athletes.5 6 w2 Although recent work hassuggested that the RV may remodel slightly morethan the LV in endurance athletes7dpossiblyreflecting the fact that although the volumeload during exercise is the same, RV wall stressincreases more than LV wall stress during exercise,thus placing an additional pressure load on thisventricledthis difference is small. Other researchhas suggested that the common ECG changes seenin athletes of incomplete and complete right bundlebranch block (RBBB) reflect the degree of RVremodelling, even in the absence of significantstructural heart disease.w3 There has been littlework on RV changes in athletes engaged in staticexercise, although one study observed increased RVvolume in sprinters,w4 a finding which requiresfurther study. The challenge in clinical practice hasbeen to measure RV size accurately due to thecomplex three dimensional structure of thischamber, although the use of cardiac MRI and threedimensional echocardiography may make this morepracticable in the future (figure 2).
AtriaIn addition to remodelling of the LVand RV, studieshave shown atrial enlargement to be frequent intrained athletes whether identified by dimen-sionsw5 or volumetric measures.w6 Most studieshave examined the left atrium, although right atrialenlargement has also been described. In general,atrial enlargement is proportional to the enlarge-ment of the ventricles and is affected by the type oftraining undertaken. There is some speculation thatatrial enlargement may not regress completely aftercessation of athletic activity and may predisposeathletes to an increased risk of subsequent atrialfibrillation.
FUNCTIONAL REMODELLINGLeft ventricleWhile structural change within the LV has beenvery clearly and consistently demonstrated, theevidence regarding functional change has been lessconsistent.8 Compared to pathological LV remod-elling which is frequently associated with reducedsystolic and/or diastolic function measures,athlete’s heart has been demonstrated to havepreserved or even enhanced function. Most func-tional studies have used echocardiography anda small subset have used cardiac MRI. LV ejectionfraction (LVEF) is the most common measure ofsystolic function used and athletes generally havevalues for LVEF which are close to the generalpopulation. The exception to this may be thoseendurance athletes with notably dilated leftventricles who may have an LVEF which is ‘lowerthan normal’, and resting values as low as 41% havebeen documented in otherwise normal athletes,although stroke volume is normal. One study of
Figure 1 Apical four chamber echocardiogram comparing the heart of a 23-year-oldnon-athlete (left) with that of a 23-year-old professional cyclist. The volume load ofendurance sport training results in dilation of all four cardiac chambers and a notableincrease in stroke volume despite normal or even reduced resting function. In this case,a normal cardiac output is maintained at rest in spite of a pronounced bradycardia (heartrate 28 beats/min). The 10 cm echocardiographic field depth is marked in red to highlightthe differences in cardiac size.
Table 1 Classification of training type by sport (adapted from Mitchell et al2)Dynamic component
Low Medium High
Static component Low Golf Baseball Hockey
Cricket Fencing Long distance running
Bowling Volleyball Football (soccer)
Tennis
Medium Archery American football Middle distance running
Diving Jumping events Swimming
Equestrian Sprinting Basketball
Rugby Ice hockey
Figure skating Cross country skiing
High Throwing events Downhill skiing Cycling
Weight lifting Body building Triathlon
Gymnastics Snowboarding Rowing
Martial arts Wrestling Boxing
Canoe/kayak
948 Heart 2012;98:947e955. doi:10.1136/heartjnl-2011-301329
Education in Heart
group.bmj.com on November 19, 2014 - Published by http://heart.bmj.com/Downloaded from

Racial variabilityIt is apparent that genetic and racial variabilityaffect the individual’s cardiac response to exercisetraining such that different limits of normality mayneed to be applied depending on an athlete’sbackground. Athletes of Afro-Caribbean back-ground tend to have increased LV mass and wallthickness when compared to white athletes. Infact, the normal distribution of these parameters inAfro-Caribbean athletes is shifted to the right suchthat these athletes may have wall thickness up to15 mm.14 In Basavarajaiah’s study, 25% of blackathletes had LVH based on an end-diastolic wallthickness >12 mm, compared with only 4% ofwhite athletes. Black athletes of East African origin,on the other hand, show a lower frequency of LVHthan those of West African ancestry. There are onlylimited data in other racial groups such as Asians orthe indigenous populations of many countries,despite such populations being disproportionatelywell represented in some elite sports.
EFFECTS OF DETRAININGUpon cessation of training, the changes of athlete’sheart may regress towards more normal struc-ture.17 This has been advocated as a useful methodfor discrimination of the true athlete’s heart froma structurally abnormal heart due to cardiacpathology, in which the expected regression withdetraining will not occur. Regression of changes hasbeen not only with structural, but also with elec-trical remodelling.w19 There is some evidence tosupport this approach, although there is conjectureabout whether longstanding changes of athlete’sheart in an older athlete will regress as effectively asin a younger athlete.
MECHANISMS OF REMODELLINGAthlete’s heart is an adaptive response to exercisetraining which imposes an intermittent volumeand pressure load. This remodelling response to anexercise stimulus is often termed ‘physiological’ incontrast to the hypertrophic response which resultsfrom pathological entities such as systemic hyper-tension, valvular heart disease and cardiomyopathy.In both cases, an increase in cardiac load activatesa variety of molecular mechanisms, activates ribo-somal kinases and increases protein synthesiswhich are necessary for an increase in muscle mass.However, the molecular mediators of ‘pathological’hypertrophy (natriuretic peptides, vasoactivehormones and catecholamines) are quite differentfrom those which mediate hypertrophy in athletes(trophic hormones such as insulin-like growthfactor), possibly as a result of the chronic versusintermittent nature of the load excess.18 w20 Path-ological hypertrophy includes cellular apoptosis,expansion of pro-fibrotic elements and frequentlyprogresses to cardiac dysfunction whereas theincrease in myocyte mass is relatively ‘pure’ inathletes with minimal or no increase in extracel-lular expansion. Microarray techniques have beenused to demonstrate the differences in geneexpression between hypertrophy resulting fromphysiological and pathological stimuli,w21 althoughthe separation remains incomplete and someinvestigators have argued that the distinction issomewhat arbitrary.w22
IS THE ATHLETE’S HEART ALWAYS BENIGN ANDREVERSIBLE?Physiological hypertrophy implies that musclemass has the capacity to both increase and decreasein response to changes in load. Indeed, de-trainingleads to regression of cardiac hypertrophy and canbe a clinically useful tool when attempting toseparate athlete’s heart from structural heartdisease. However, normalisation of cardiac massmay not always be complete, even after many yearsof deconditioning.17 w23 This seems particularlytrue of well practised athletes who have developedprofound cardiac hypertrophy over many years.The lack of longitudinal studies detailing cardiacmorphology before athletic conditioning meansthat one cannot exclude the possibility that these
Figure 5 Flow chart for evaluation of the athlete’s heart. yType 1 ECG changes are thoseconsidered normal for an athlete, and type 2 ECG changes are considered abnormal.13
ARVC, arrhythmogenic right ventricular cardiomyopathy; DCM, dilated cardiomyopathy;EF, ejection fraction; EP, electrophysiology; HCM, hypertrophic cardiomyopathy.
952 Heart 2012;98:947e955. doi:10.1136/heartjnl-2011-301329
Education in Heart
group.bmj.com on November 19, 2014 - Published by http://heart.bmj.com/Downloaded from

¿Se debería realizar cribado preparticipación a todos los deportistas?
• Dado que la muerte súbita puede ser el primer síntoma de una enfermedad subyacente se han planteado muchos programas de cribado preparticipación para deportistas.
• Se ha producido mucho debate acerca de la utilidad y factibilidad de estos programas con pruebas contradictorias.
• El principal argumento a favor del cribado es la posible prevención de muertes mediante la detección de anomalias cardiovasculares inicio de tratamiento de las mismas y prohibición de realizar deporte competitivo.

Documento marco sobre cribado poblacional 5/35
tratamiento, para reducir el riesgo de la enfermedad o sus complicaciones” (NSC, 2009).
Tabla 1. Beneficios y riesgos del cribado (Holland et al. WHO, 2006)
Beneficios Riesgos y Desventajas Mejora del pronóstico de los casos detectados
Mayor tiempo de morbilidad en casos que no mejoran su pronóstico Sobretratamiento de anomalías de pronóstico incierto
Tratamiento menos radical que cura los casos precoces Riesgo de efectos adversos por el
proceso de cribado Ahorro de recursos Costes añadidos Mayor tranquilidad en casos con resultado negativo
Falsa tranquilidad en los casos falsos negativos
Los beneficios del cribado se obtienen mediante un diagnóstico precoz
preciso, con la consiguiente intervención, que permitirá mejorar el pronóstico en gran parte de los pacientes detectados. En esta fase de evolución, el tratamiento puede ser menos radical. Se podría ahorrar recursos de los servicios de salud por el tratamiento precoz de la enfermedad. Aquellos con resultados verdaderos negativos en las pruebas pueden sentir mayor tranquilidad respecto a esa enfermedad concreta.
El cribado también tiene desventajas y riesgos. Los pacientes en los que la detección precoz no suponga una mejora en su pronóstico sufrirán un periodo de morbilidad mayor por el adelanto diagnóstico. La detección de anomalías de pronóstico incierto o lesiones precursoras puede derivar en sobrediagnóstico y sobretratamiento. El aumento inicial en los costes es evidente, no sólo por la infraestructura y los recursos materiales y humanos necesarios, sino también por el aumento de la carga que supone para el sistema de salud la confirmación diagnóstica y el eventual tratamiento de los casos detectados. Sin embargo, si se valora en un horizonte temporal suficientemente largo, el programa podría tener un menor coste global, al disminuir la prevalencia de casos graves que exigen una asistencia más frecuente y costosa. Los casos con resultados falsos negativos pueden sentirse falsamente tranquilizados, lo que podría derivar en retrasos diagnósticos ante la aparición de síntomas. Los casos falsos positivos sufrirán un periodo innecesario de ansiedad, el riesgo de efectos adversos asociados a las pruebas confirmatorias y, en el peor de los casos, un tratamiento inapropiado. Por último, como en todo acto médico, existen potenciales efectos adversos asociados a las pruebas y al tratamiento.
El cribado como programa integral En los criterios clásicos de Wilson y Jungner sobre el cribado ya se establece que “el cribado debe ser un proceso continuo y no una prueba puntual” (Wilson et al, 1968). El resultado de una única prueba de cribado sólo permite discriminar a los individuos con un mayor riesgo de sufrir el problema en cuestión y, por tanto, siempre precisará de una confirmación diagnóstica. La OMS también considera que el cribado se debe enmarcar dentro de un plan más amplio de control de la enfermedad. Debería ser un programa integral que
Documento marco sobre cribado poblacional 5/35
tratamiento, para reducir el riesgo de la enfermedad o sus complicaciones” (NSC, 2009).
Tabla 1. Beneficios y riesgos del cribado (Holland et al. WHO, 2006)
Beneficios Riesgos y Desventajas Mejora del pronóstico de los casos detectados
Mayor tiempo de morbilidad en casos que no mejoran su pronóstico Sobretratamiento de anomalías de pronóstico incierto
Tratamiento menos radical que cura los casos precoces Riesgo de efectos adversos por el
proceso de cribado Ahorro de recursos Costes añadidos Mayor tranquilidad en casos con resultado negativo
Falsa tranquilidad en los casos falsos negativos
Los beneficios del cribado se obtienen mediante un diagnóstico precoz
preciso, con la consiguiente intervención, que permitirá mejorar el pronóstico en gran parte de los pacientes detectados. En esta fase de evolución, el tratamiento puede ser menos radical. Se podría ahorrar recursos de los servicios de salud por el tratamiento precoz de la enfermedad. Aquellos con resultados verdaderos negativos en las pruebas pueden sentir mayor tranquilidad respecto a esa enfermedad concreta.
El cribado también tiene desventajas y riesgos. Los pacientes en los que la detección precoz no suponga una mejora en su pronóstico sufrirán un periodo de morbilidad mayor por el adelanto diagnóstico. La detección de anomalías de pronóstico incierto o lesiones precursoras puede derivar en sobrediagnóstico y sobretratamiento. El aumento inicial en los costes es evidente, no sólo por la infraestructura y los recursos materiales y humanos necesarios, sino también por el aumento de la carga que supone para el sistema de salud la confirmación diagnóstica y el eventual tratamiento de los casos detectados. Sin embargo, si se valora en un horizonte temporal suficientemente largo, el programa podría tener un menor coste global, al disminuir la prevalencia de casos graves que exigen una asistencia más frecuente y costosa. Los casos con resultados falsos negativos pueden sentirse falsamente tranquilizados, lo que podría derivar en retrasos diagnósticos ante la aparición de síntomas. Los casos falsos positivos sufrirán un periodo innecesario de ansiedad, el riesgo de efectos adversos asociados a las pruebas confirmatorias y, en el peor de los casos, un tratamiento inapropiado. Por último, como en todo acto médico, existen potenciales efectos adversos asociados a las pruebas y al tratamiento.
El cribado como programa integral En los criterios clásicos de Wilson y Jungner sobre el cribado ya se establece que “el cribado debe ser un proceso continuo y no una prueba puntual” (Wilson et al, 1968). El resultado de una única prueba de cribado sólo permite discriminar a los individuos con un mayor riesgo de sufrir el problema en cuestión y, por tanto, siempre precisará de una confirmación diagnóstica. La OMS también considera que el cribado se debe enmarcar dentro de un plan más amplio de control de la enfermedad. Debería ser un programa integral que

Documento marco sobre cribado poblacional 10/35
ser independientes y hacer explícita una declaración de conflictos de interés.
Además, debe existir un proceso de revisión previsto, sistemático y periódico.
La factibilidad del programa La implantación de un programa de cribado supone una importante inversión y la intervención en un numeroso grupo de personas para detectar un relativamente pequeño número de casos. Por eso, debe existir una evaluación económica completa del programa. Los costes de un programa de cribado se deben considerar en su conjunto, no analizar únicamente la eficiencia de la prueba inicial.
Además, habrá que hacer una valoración del impacto del programa en el sistema de salud. En primer lugar, habrá que evaluar cómo se está realizando hasta ese momento la prevención y control del problema de salud en cuestión; en segundo lugar habrá que valorar cómo se va a integrar el cribado en esa realidad y qué repercusiones (demanda, uso de recursos, listas de espera,…) tendrá sobre el sistema en su conjunto. Hay que tener en cuenta que los recursos que consuma el programa no podrán ser destinados a otras acciones de salud (coste-oportunidad).
Los aspectos éticos Las consideraciones éticas, como el equilibrio entre beneficios y riesgos del programa completo, la equidad en el acceso, el respeto a la autonomía, y el derecho a la intimidad y la confidencialidad, son de una importancia crucial. Este aspecto cobra especial relevancia en el campo de las enfermedades genéticas. La capacidad técnica para realizar un cribado no implica que sea aceptable desde un punto de vista ético. Además, hay que considerar cuestiones como la posible discriminación o estigmatización de los casos detectados, desde un punto de vista social e incluso laboral o por parte de las compañías aseguradoras. La tabla 2 recoge algunos de los riesgos éticos asociados con el cribado.
Tabla2. Cuestiones éticas del cribado (adaptado de Ruf et al, 2008) Principio ético Riesgo potencial Beneficencia El cribado puede tener un beneficio poblacional, pero
muchos individuos no se beneficiarán directamente Daño psicológico en casos falsos positivos Posibles muertes evitables entre los falsos negativos Iatrogenia del proceso diagnóstico y posterior intervención
No maleficencia
Falsa tranquilidad en falsos negativos (posible retraso diagnóstico, deterioro hábitos saludables…) Aumentar desigualdades si no hay previstas medidas para potenciar la equidad en el acceso Detrimento de la implantación de otras medidas preventivas o de control de la enfermedad más coste-efectivas (coste-oportunidad)
Justicia
Discriminación o estigmatización de casos detectados Autonomía Dada la dificultad en comunicar riesgos, los individuos
pueden no comprender todas las implicaciones de su participación en el programa.
Documento marco sobre cribado poblacional 10/35
ser independientes y hacer explícita una declaración de conflictos de interés.
Además, debe existir un proceso de revisión previsto, sistemático y periódico.
La factibilidad del programa La implantación de un programa de cribado supone una importante inversión y la intervención en un numeroso grupo de personas para detectar un relativamente pequeño número de casos. Por eso, debe existir una evaluación económica completa del programa. Los costes de un programa de cribado se deben considerar en su conjunto, no analizar únicamente la eficiencia de la prueba inicial.
Además, habrá que hacer una valoración del impacto del programa en el sistema de salud. En primer lugar, habrá que evaluar cómo se está realizando hasta ese momento la prevención y control del problema de salud en cuestión; en segundo lugar habrá que valorar cómo se va a integrar el cribado en esa realidad y qué repercusiones (demanda, uso de recursos, listas de espera,…) tendrá sobre el sistema en su conjunto. Hay que tener en cuenta que los recursos que consuma el programa no podrán ser destinados a otras acciones de salud (coste-oportunidad).
Los aspectos éticos Las consideraciones éticas, como el equilibrio entre beneficios y riesgos del programa completo, la equidad en el acceso, el respeto a la autonomía, y el derecho a la intimidad y la confidencialidad, son de una importancia crucial. Este aspecto cobra especial relevancia en el campo de las enfermedades genéticas. La capacidad técnica para realizar un cribado no implica que sea aceptable desde un punto de vista ético. Además, hay que considerar cuestiones como la posible discriminación o estigmatización de los casos detectados, desde un punto de vista social e incluso laboral o por parte de las compañías aseguradoras. La tabla 2 recoge algunos de los riesgos éticos asociados con el cribado.
Tabla2. Cuestiones éticas del cribado (adaptado de Ruf et al, 2008) Principio ético Riesgo potencial Beneficencia El cribado puede tener un beneficio poblacional, pero
muchos individuos no se beneficiarán directamente Daño psicológico en casos falsos positivos Posibles muertes evitables entre los falsos negativos Iatrogenia del proceso diagnóstico y posterior intervención
No maleficencia
Falsa tranquilidad en falsos negativos (posible retraso diagnóstico, deterioro hábitos saludables…) Aumentar desigualdades si no hay previstas medidas para potenciar la equidad en el acceso Detrimento de la implantación de otras medidas preventivas o de control de la enfermedad más coste-efectivas (coste-oportunidad)
Justicia
Discriminación o estigmatización de casos detectados Autonomía Dada la dificultad en comunicar riesgos, los individuos
pueden no comprender todas las implicaciones de su participación en el programa.

800 450
200 8550
Enfermos Sanos
Test +
Test -
1000 9000
1250
8750
10000

800 450
200 8550
Enfermos Sanos
Test +
Test -
1000 9000
1250
8750
10000
Sensibilidad: 800/1000= 80%Especificidad: 8550/9000= 95%
Valor predictivo+: 800/1250= 64%Valor predictivo-: 8550/8750= 97,7%
Prevalencia 10%

80 495
20 9405
Enfermos Sanos
Test +
Test -
100 9900
575
9425
10000

80 495
20 9405
Enfermos Sanos
Test +
Test -
100 9900
575
9425
10000
Sensibilidad: 80/100= 80%Especificidad: 9405/9900= 95%
Valor predictivo+: 80/575= 14%Valor predictivo-: 9405/9425= 99,8%
Prevalencia 1%

Evidencias para el cribado preparticipación• Los programas de cribado pueden incluir:
★ Realización de anamnesis personal y familiar.★ Exploración física★ ECG y aquellos con alguna alteración: ecocardiograma, prueba de esfuerzo, Holter de 24 h y
RNM cardiaca.
• En Italia se introdujo un programa de cribado incorporando todos los aspectos anteriores en 1982.
• Un estudio de 26 años realizado en el Veneto mostró una disminución del 89% en la incidencia de muerte súbita aunque el análisis se realizó de forma retrospectiva y el número de episodios mortales fué pequeño.
• Otro estudio en Israel cuestiona los resultados positivos del cribado.
• En un estudio en UK se realizó cribado a 3500 deportistas y solo se encontraron dos posibles casos de miocardiopatía hipertrófica aunque en una valoración posterior se diagnosticaron de hipertrofia fisiológica del VI. En otros 26 deportistas se encontró alguna anomalía que podía ser relevante lo que nos lleva a una tasa de detección de 0,8% ligeramente por encima de otros estudios.


ORIGINAL CONTRIBUTION
Trends in Sudden Cardiovascular Deathin Young Competitive AthletesAfter Implementation of aPreparticipation Screening ProgramDomenico Corrado, MD, PhDCristina Basso, MD, PhDAndrea Pavei, MDPierantonio Michieli, MD, PhDMaurizio Schiavon, MDGaetano Thiene, MD
THE MAJORITY OF YOUNG ATH-letes who die suddenly havepreviously unsuspected struc-tural heart disease.1-8 Cardi-
omyopathies have been consistently im-plicated as the leading cause of cardiacarrest in young competitive athletes,with hypertrophic cardiomyopathy ac-counting for more than one third offatal cases in the United States1,4-6 andarrhythmogenic right ventricular car-diomyopathy for approximately onefourth of fatal cases in Italy.2,3,7,8
Medical evaluation of athletic popu-lations before competition offers thepotential to identify asymptomatic ath-letes with potentially lethal cardiovas-cular abnormalities and to prevent sud-den death through disqualificationfrom competitive sports.9-13 Italian lawmandates that every participant en-gaged in competitive sports activitymust undergo a clinical evaluation andobtain eligibility.14 Accordingly, a na-tionwide systematic screening pro-gram was launched in Italy in 1982.15,16
This preparticipation screening essen-tially based on 12-lead electrocardio-gram (ECG) has been shown to be ef-fective in identifying athletes withhypertrophic cardiomyopathy and in
For editorial comment see p 1648.
Author Affiliations: Department of Cardiac, Tho-racic, and Vascular Sciences (Drs Corrado andPavei) and Institute of Pathological Anatomy (DrsBasso and Thiene), University of Padua MedicalSchool; and Center for Sports Medicine and
Physical Activity (Drs Michieli and Schiavon),Padua, Italy.Corresponding Author: Gaetano Thiene, MD, Isti-tuto di Anatomia Patologica, Via A. Gabelli, 61-35121 Padova, Italy ([email protected]).
Context A nationwide systematic preparticipation athletic screening was intro-duced in Italy in 1982. The impact of such a program on prevention of sudden car-diovascular death in the athlete remains to be determined.
Objective To analyze trends in incidence rates and cardiovascular causes of suddendeath in young competitive athletes in relation to preparticipation screening.
Design, Setting, and Participants A population-based study of trends in suddencardiovasculardeath inathleticandnonathleticpopulationsaged12to35years intheVenetoregion of Italy between 1979 and 2004. A parallel study examined trends in cardiovascu-lar causesofdisqualification fromcompetitive sports in42 386athletesundergoingprepar-ticipation screening at the Center for Sports Medicine in Padua (22 312 in the early screen-ing period [1982-1992] and 20 074 in the late screening period [1993-2004]).
Main Outcome Measures Incidence trends of total cardiovascular and cause-specific sudden death in screened athletes and unscreened nonathletes of the sameage range over a 26-year period.
Results During the study period, 55 sudden cardiovascular deaths occurred in screenedathletes (1.9 deaths/100 000 person-years) and 265 sudden deaths in unscreened non-athletes (0.79 deaths/100 000 person-years). The annual incidence of sudden cardiovas-cular death in athletes decreased by 89% (from 3.6/100 000 person-years in 1979-1980 to 0.4/100000 person-years in 2003-2004; P for trend!.001), whereas the incidenceof sudden death among the unscreened nonathletic population did not change signifi-cantly. The mortality decline started after mandatory screening was implemented andpersisted to the late screening period. Compared with the prescreening period (1979-1981), the relative risk of sudden cardiovascular death in athletes was 0.56 in the earlyscreening period (95% CI, 0.29-1.15; P=.04) and 0.21 in the late screening period (95%CI, 0.09-0.48; P=.001). Most of the reduced mortality was due to fewer cases of sud-den death from cardiomyopathies (from 1.50/100 000 person-years in the prescreeningperiod to 0.15/100 000 person-years in the late screening period; P for trend=.002). Dur-ing the study period, 879 athletes (2.0%) were disqualified from competition due to car-diovascular causes at the Center for Sports Medicine: 455 (2.0%) in the early screeningperiod and 424 (2.1%) in the late screening period. The proportion of athletes who weredisqualified for cardiomyopathies increased from 20 (4.4%) of 455 in the early screeningperiod to 40 (9.4%) of 424 in the late screening period (P=.005).
Conclusions The incidence of sudden cardiovascular death in young competitive ath-letes has substantially declined in the Veneto region of Italy since the introduction ofa nationwide systematic screening. Mortality reduction was predominantly due to alower incidence of sudden death from cardiomyopathies that paralleled the increas-ing identification of athletes with cardiomyopathies at preparticipation screening.JAMA. 2006;296:1593-1601 www.jama.com
©2006 American Medical Association. All rights reserved. (Reprinted) JAMA, October 4, 2006—Vol 296, No. 13 1593
Downloaded From: http://jama.jamanetwork.com/ by a HOSPITAL UNIV I POLITECNICA User on 04/22/2016

years). In 50 cases (91%), sudden deathoccurred during sports activity (44 cases)or immediately afterward (6 cases).
Number and rates of sudden cardio-vascular death in young competitiveathletes decreased during the 26-yearperiod (FIGURE). The annual rate ofdeath was 3.6 per 100 000 person-
years in 1979-1980 (8 sudden deaths)and 4.0 per 100 000 person-years in1981-1982 (9 sudden deaths). Subse-quently, the annual rate of deathsteadily decreased over time and in the2001-2004 period, it was 0.43 per100 000 person-years (1 sudden deatheach period), which is approximately
a tenth of that recorded 2 decades be-fore (P for trend! .001).
The overall changes in total inci-dence rates of sudden cardiovasculardeath in athletes in relation to the 3screening periods are shown in TABLE 1.The decrease of sudden cardiovascu-lar deaths in the athletic populationstarted after the introduction of prepar-ticipation screening and persisted to thelate screening period. During the pre-screening period, there were 14 deaths(13 males and 1 female; mean [SD] age,22.9 [6] years), 12 of which weresports-related; during the early screen-ing period, there were 29 deaths (26males and 3 females; mean [SD] age,23.7 [5] years), 27 of which weresports-related; and during the latescreening period, 12 deaths (11 malesand 1 female; mean [SD] age, 23.5 [6]years), 11 of which were sports-related.
The average incidence of sudden car-diovascular death in young competitiveathletes in the prescreening period was4.19 (95% CI, 1.78-7.59) per 100 000person-years. The average incidence de-creased to 2.35 (95% CI, 1.94-2.75) per
Figure. Annual Incidence Rates of Sudden Cardiovascular Death in Screened CompetitiveAthletes and Unscreened Nonathletes Aged 12 to 35 Years in the Veneto Region of Italy(1979-2004)
4.5
1.0
2.5
2.0
1.5
3.0
3.5
4.0
0.5
01979-1980
1981-1982
1983-1984
1985-1986
1987-1988
1989-1990
1991-1992
1993-1994
1995-1996
1997-1998
1999-2000
2001-2002
2003-2004
Years
Sud
den D
eath
per
100
000 P
ers
on-Y
ears
Screened AthletesUnscreened Nonathletes
During the study period, the annual incidence of sudden cardiovascular death decreased by 89% in screenedathletes (P for trend!.001). In contrast, the incidence rate of sudden cardiovascular death did not demon-strate consistent changes over time in unscreened nonathletes.
Table 1. Number and Annual Incidence Rates of Total and Cause-Specific Sudden Cardiovascular Death in Screened Athletes and UnscreenedNonathletes in Relation to 3 Screening Periods*
Periods
P forTrend
RR(95% CI)†
Prescreening(1979-1981)
Early Screening(1982-1992)
Late Screening(1993-2004)
No. ofEvents
Incidence Rate(95% CI)
No. ofEvents
Incidence Rate(95% CI)
No. ofEvents
Incidence Rate(95% CI)
Total sudden deaths in athletes 14 4.19 (1.78-7.59) 29 2.35 (1.94-2.75) 12 0.87 (0.46-1.28) .001 0.21 (0.09-0.48)Cardiomyopathies 5 1.50 (0.21-2.78) 7 0.57 (0.26-0.87) 2 0.15 (0-0.36) .002 0.10 (0.01-0.59)Coronary artery disease 3 0.90 (0-3.12) 5 0.41 (0.09-0.72) 3 0.22 (0-0.47) .08 0.24 (0.03-1.81)Cardiac conduction disease 1 0.30 (0-1.56) 2 0.16 (0-0.40) 1 0.07 (0-0.23) .29 0.24 (0.01-19.02)Myocarditis 1 0.30 (0-1.56) 4 0.32 (0.02-0.63) 2 0.15 (0-0.36) .40 0.48 (0.02-28.61)Congenital coronary anomalies 1 0.30 (0-1.56) 4 0.32 (0.02-0.63) 2 0.15 (0-0.36) .40 0.48 (0.02-28.61)Mitral valve prolapse 1 0.30 (0-1.56) 4 0.32 (0.02-0.63) 1 0.07 (0-0.23) .19 0.24 (0.01-19.02)Other‡ 2 0.60 (0-1.87) 3 0.24 (0-0.52) 1 0.07 (0-0.23) .06 0.12 (0.01-2.33)
Total sudden death in nonathletes 29 0.77 (0.26-1.26) 110 0.79 (0.69-0.88) 126 0.81 (0.68-0.94) .80 1.05 (0.69-1.64)Cardiomyopathies 8 0.21 (0.10-0.33) 35 0.25 (0.17-0.33) 40 0.26 (0.19-0.33) .76 1.21 (0.56-2.99)Coronary artery disease 7 0.19 (0.07-0.30) 23 0.17 (0.12-0.22) 25 0.16 (0.12-0.21) .81 0.87 (0.36-2.37)Cardiac conduction disease 3 0.08 (0-0.28) 8 0.06 (0.02-0.10) 12 0.08 (0.03-0.13) .66 0.97 (0.26-5.36)Myocarditis 4 0.10 (0-0.34) 15 0.11 (0.06-0.16) 20 0.13 (0.08-0.18) .58 1.21 (0.41-4.88)Congenital coronary anomalies 2 0.05 (0-0.17) 5 0.04 (0.01-0.06) 7 0.05 (0.01-0.08) .87 0.85 (0.16-8.37)Mitral valve prolapse 2 0.05 (0-0.17) 9 0.06 (0.03-0.11) 8 0.05 (0.02-0.09) .72 0.97 (0.19-9.38)Other‡ 3 0.08 (0-0.28) 15 0.11 (0.07-0.15) 14 0.09 (0.05-0.13) .79 1.13 (0.32-6.15)
Abbreviations: CI, confidence interval; RR, relative risk.*Incidence rates are shown as events per year per 100 000 athletes aged 12 to 35 years. Number of events represent the actual number of events.†Reported for the rates of sudden cardiovascular deaths during the late screening period (1993-2004) using prescreening (1979-1981) rates as the baseline.‡Includes myocardial bridge, aortic stenosis, aortic rupture, and pulmonary thromboembolism.
PARTICIPATION SCREENING AND SUDDEN DEATH IN ATHLETES
1596 JAMA, October 4, 2006—Vol 296, No. 13 (Reprinted) ©2006 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a HOSPITAL UNIV I POLITECNICA User on 04/22/2016

years). In 50 cases (91%), sudden deathoccurred during sports activity (44 cases)or immediately afterward (6 cases).
Number and rates of sudden cardio-vascular death in young competitiveathletes decreased during the 26-yearperiod (FIGURE). The annual rate ofdeath was 3.6 per 100 000 person-
years in 1979-1980 (8 sudden deaths)and 4.0 per 100 000 person-years in1981-1982 (9 sudden deaths). Subse-quently, the annual rate of deathsteadily decreased over time and in the2001-2004 period, it was 0.43 per100 000 person-years (1 sudden deatheach period), which is approximately
a tenth of that recorded 2 decades be-fore (P for trend! .001).
The overall changes in total inci-dence rates of sudden cardiovasculardeath in athletes in relation to the 3screening periods are shown in TABLE 1.The decrease of sudden cardiovascu-lar deaths in the athletic populationstarted after the introduction of prepar-ticipation screening and persisted to thelate screening period. During the pre-screening period, there were 14 deaths(13 males and 1 female; mean [SD] age,22.9 [6] years), 12 of which weresports-related; during the early screen-ing period, there were 29 deaths (26males and 3 females; mean [SD] age,23.7 [5] years), 27 of which weresports-related; and during the latescreening period, 12 deaths (11 malesand 1 female; mean [SD] age, 23.5 [6]years), 11 of which were sports-related.
The average incidence of sudden car-diovascular death in young competitiveathletes in the prescreening period was4.19 (95% CI, 1.78-7.59) per 100 000person-years. The average incidence de-creased to 2.35 (95% CI, 1.94-2.75) per
Figure. Annual Incidence Rates of Sudden Cardiovascular Death in Screened CompetitiveAthletes and Unscreened Nonathletes Aged 12 to 35 Years in the Veneto Region of Italy(1979-2004)
4.5
1.0
2.5
2.0
1.5
3.0
3.5
4.0
0.5
01979-1980
1981-1982
1983-1984
1985-1986
1987-1988
1989-1990
1991-1992
1993-1994
1995-1996
1997-1998
1999-2000
2001-2002
2003-2004
Years
Sud
den D
eath
per
100
000 P
ers
on-Y
ears
Screened AthletesUnscreened Nonathletes
During the study period, the annual incidence of sudden cardiovascular death decreased by 89% in screenedathletes (P for trend!.001). In contrast, the incidence rate of sudden cardiovascular death did not demon-strate consistent changes over time in unscreened nonathletes.
Table 1. Number and Annual Incidence Rates of Total and Cause-Specific Sudden Cardiovascular Death in Screened Athletes and UnscreenedNonathletes in Relation to 3 Screening Periods*
Periods
P forTrend
RR(95% CI)†
Prescreening(1979-1981)
Early Screening(1982-1992)
Late Screening(1993-2004)
No. ofEvents
Incidence Rate(95% CI)
No. ofEvents
Incidence Rate(95% CI)
No. ofEvents
Incidence Rate(95% CI)
Total sudden deaths in athletes 14 4.19 (1.78-7.59) 29 2.35 (1.94-2.75) 12 0.87 (0.46-1.28) .001 0.21 (0.09-0.48)Cardiomyopathies 5 1.50 (0.21-2.78) 7 0.57 (0.26-0.87) 2 0.15 (0-0.36) .002 0.10 (0.01-0.59)Coronary artery disease 3 0.90 (0-3.12) 5 0.41 (0.09-0.72) 3 0.22 (0-0.47) .08 0.24 (0.03-1.81)Cardiac conduction disease 1 0.30 (0-1.56) 2 0.16 (0-0.40) 1 0.07 (0-0.23) .29 0.24 (0.01-19.02)Myocarditis 1 0.30 (0-1.56) 4 0.32 (0.02-0.63) 2 0.15 (0-0.36) .40 0.48 (0.02-28.61)Congenital coronary anomalies 1 0.30 (0-1.56) 4 0.32 (0.02-0.63) 2 0.15 (0-0.36) .40 0.48 (0.02-28.61)Mitral valve prolapse 1 0.30 (0-1.56) 4 0.32 (0.02-0.63) 1 0.07 (0-0.23) .19 0.24 (0.01-19.02)Other‡ 2 0.60 (0-1.87) 3 0.24 (0-0.52) 1 0.07 (0-0.23) .06 0.12 (0.01-2.33)
Total sudden death in nonathletes 29 0.77 (0.26-1.26) 110 0.79 (0.69-0.88) 126 0.81 (0.68-0.94) .80 1.05 (0.69-1.64)Cardiomyopathies 8 0.21 (0.10-0.33) 35 0.25 (0.17-0.33) 40 0.26 (0.19-0.33) .76 1.21 (0.56-2.99)Coronary artery disease 7 0.19 (0.07-0.30) 23 0.17 (0.12-0.22) 25 0.16 (0.12-0.21) .81 0.87 (0.36-2.37)Cardiac conduction disease 3 0.08 (0-0.28) 8 0.06 (0.02-0.10) 12 0.08 (0.03-0.13) .66 0.97 (0.26-5.36)Myocarditis 4 0.10 (0-0.34) 15 0.11 (0.06-0.16) 20 0.13 (0.08-0.18) .58 1.21 (0.41-4.88)Congenital coronary anomalies 2 0.05 (0-0.17) 5 0.04 (0.01-0.06) 7 0.05 (0.01-0.08) .87 0.85 (0.16-8.37)Mitral valve prolapse 2 0.05 (0-0.17) 9 0.06 (0.03-0.11) 8 0.05 (0.02-0.09) .72 0.97 (0.19-9.38)Other‡ 3 0.08 (0-0.28) 15 0.11 (0.07-0.15) 14 0.09 (0.05-0.13) .79 1.13 (0.32-6.15)
Abbreviations: CI, confidence interval; RR, relative risk.*Incidence rates are shown as events per year per 100 000 athletes aged 12 to 35 years. Number of events represent the actual number of events.†Reported for the rates of sudden cardiovascular deaths during the late screening period (1993-2004) using prescreening (1979-1981) rates as the baseline.‡Includes myocardial bridge, aortic stenosis, aortic rupture, and pulmonary thromboembolism.
PARTICIPATION SCREENING AND SUDDEN DEATH IN ATHLETES
1596 JAMA, October 4, 2006—Vol 296, No. 13 (Reprinted) ©2006 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a HOSPITAL UNIV I POLITECNICA User on 04/22/2016

Cardiovascular Causes ofDisqualification at ScreeningThe estimated number of competitiveathletes aged 12 to 35 years in theVeneto region from 1982 to 2004 was385600 (186 700 during 1982-1992and 198 900 during 1993-2004). Ofthese, 42 386 young athletes (11%)were screened at the Center for SportsMedicine in Padua between 1982 and2004 (22 312 in 1982-1992 and 20 074in 1993-2004). Among the 42 386 ath-letes, 3914 (9%) were referred for fur-ther examination because of positivefindings and 879 (2%) were ulti-mately disqualified from participationin competitive sports because of the fol-lowing types of cardiovascular condi-tions: (1) rhythm and conduction ab-normalities, which worsened duringphysical exercise to the extent that theyproduced symptoms, such as im-paired consciousness, significant fa-tigue, or dyspnea, regardless of pres-
ence of an underlying heart disease, andwere inadequately treated with antiar-rhythmic drugs or catheter ablation(39.0%); (2) systemic hypertension(!160/100 mm Hg at rest) unsatisfac-torily controlled with drug therapy orassociated with target organ damage(23.0%); (3) valvular diseases, includ-ing mitral valve prolapse complicatedby ventricular arrhythmias, mitral valveregurgitation, or both (21.0%); (4) car-diomyopathies (6.8%); (5) atheroscle-rotic coronary artery disease (1.3%);and (6) other, such as congenital heartdiseases, vascular diseases, rheumaticdisease, and pericarditis (8.4%)(TABLE 2).
These conditions causing disquali-fication in the 879 athletes were sus-pected at baseline screening on the ba-sis of positive history, physical and ECGfindings, and confirmed by further ex-amination, including echocardiogra-phy and exercise testing in 387 ath-
letes (44%); echocardiography, exercisetesting, and 24-hour Holter monitor-ing in 335 athletes (38%); echocardi-ography in 128 athletes (14%); and ech-ocardiography and 24-hour Holtermonitoring in 29 athletes (3%). Car-diac magnetic resonance imaging, elec-trophysiologic study, or contrast an-giography were required in 47 athletes(5%).
Despite positive findings at first-line screening evaluation, 3035 ath-letes obtained eligibility for competi-tion after cardiovascular disease wasruled out by additional test results(false-positive results), such as echo-cardiography in 2458 athletes (81%);echocardiography and exercise test-ing in 424 athletes (14%); and echo-cardiography, exercise testing, and 24-hour Holter monitoring in 153 athletes(5%). Twenty-nine athletes (0.9%) un-derwent cardiac magnetic resonanceimaging, invasive tests (such as elec-trophysiologic study and contrast an-giography), or both.
The analysis of cardiovascular con-ditions causing disqualification fromcompetitive sports in the 879 athletesduring the early and late screening pe-riods indicated an increasing efficacy ofpreparticipation evaluation in identi-fying athletes who had cardiomyopa-thies over time. The proportion of ath-letes who were disqualified fromcompetition due to cardiomyopathiesincreased from 20 (4.4%) of 455 in theearly screening period to 40 (9.4%) of424 during the late screening period(P=.005) (Table 2). This was predomi-nantly a consequence of the signifi-cantly higher number of athletes whodid not obtain sports eligibility be-cause of a diagnosis of arrhyth-mogenic right ventricular cardiomy-opathy during the late screening periodcompared with the early screening pe-riod (14/424 [3.3%] and 2/455 [0.4%],respectively; P=.004).
An increase (with a nonstatisticallysignificant trend) of the number of ath-letes who were disqualified because ofcoronary artery disease was observed inthe late screening period (2.1% vs 0.4%;P=.05).
Table 2. Cardiovascular Conditions Causing Disqualification From Competitive Sports in 879Athletes Over 2 Consecutive Screening Periods (1982-1992 and 1993-2004) at the Center forSports Medicine in Padua, Italy
Cardiovascular Causesof Disqualification
No. (%) of Disqualified Athetes
PValue
Total StudyPeriod
(1982-2004)
Early ScreeningPeriod
(1982-1992)
Late screeningPeriod
(1993-2004)Total No. screened* 42 386 22 312 20 074Total No. disqualified† 879 (2.0) 455 (2.0) 424 (2.1)Rhythm and conduction abnormalities 345 (39.0) 166 (36.0) 179 (42.2) .13
Ventricular arrhythmias 173 (19.6) 81 (18.0) 92 (21.6) .20Supraventricular arrhythmias 73 (8.3) 39 (8.6) 34 (8.0) .56Wolff-Parkinson-White syndrome 55 (6.3) 29 (6.3) 26 (6.1) .88LBBB or RBBB and LAD 26 (3.0) 8 (1.7) 18 (4.2) .102nd-degree atrioventricular block 13 (1.5) 7 (1.5) 6 (1.4) .89Long QT syndrome 5 (0.6) 2 (0.4) 3 (0.7) .93
Systemic hypertension 205 (23.0) 118 (25.9) 87 (20.5) .96Valvular disease, including MVP 184 (21.0) 106 (23.3) 78 (18.4) .09Cardiomyopathies 60 (6.8) 20 (4.4) 40 (9.4) .005
Hypertrophic 30 (3.4) 14 (3.0) 16 (3.8) .50Arrhythmogenic right ventricular 16 (1.8) 2 (0.4) 14 (3.3) .004Dilated 14 (1.6) 4 (0.9) 10 (2.4) .21
Coronary artery disease 11 (1.3) 2 (0.4) 9 (2.1) .05Other‡ 74 (8.4) 43 (9.5) 31 (7.3) .42Abbreviations: LAD, left axis deviation; LBBB, left bundle-branch block; MVP, mitral valve prolapse; RBBB, right bundle-
branch block.*All athletes were screened at the Center for Sports Medicine in Padua, Italy, between 1982 and 2004.†A total of 721 males and 158 females (age range, 12-35 years; mean [SD] age, 18.9 [6] years; median, 17 years) com-
prised the disqualified athletes for the total study period; 382 males and 73 females (age range, 12-35 years; mean [SD]age, 19.1 [4] years; median, 17 years) comprised the disqualified athletes for the early screening period; and 335 malesand 89 females (age range, 12-35 years; mean [SD] age, 18.6 [5] years; median, 17 years) comprised the disqualifiedathletes for the late screening period.
‡Includes congenital heart diseases, vascular diseases, rheumatic disease, and pericarditis.
PARTICIPATION SCREENING AND SUDDEN DEATH IN ATHLETES
1598 JAMA, October 4, 2006—Vol 296, No. 13 (Reprinted) ©2006 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a HOSPITAL UNIV I POLITECNICA User on 04/22/2016

Pre-Participation Athletic Screening
Mandatory Electrocardiographic Screening ofAthletes to Reduce Their Risk for Sudden DeathProven Fact or Wishful Thinking?
Arie Steinvil, MD,* Tamar Chundadze, MD,* David Zeltser, MD,* Ori Rogowski, MD,*Amir Halkin, MD,† Yair Galily, PHD,‡ Haim Perluk, MD,§ Sami Viskin, MD†
Tel-Aviv, Israel
Objectives The purpose of this study was to determine if pre-participation screening of athletes with a strategy includingresting and exercise electrocardiography (ECG) reduces their risk for sudden death.
Background An increasing number of countries mandate pre-participation ECG screening of athletes for the prevention ofsudden death. However, the evidence showing that such a strategy actually reduces the risk of sudden death inathletes is limited. We therefore analyzed the impact of the National Sport Law enacted in Israel in 1997—which mandates screening of all athletes with resting ECG and exercise testing—on the incidence of suddendeath among competitive athletes.
Methods We conducted a systematic search of the 2 main newspapers in Israel to determine the yearly number of car-diac arrest events among competitive athletes. The size of the population at risk was retrieved from the IsraelSport Authority and was extrapolated to the changes in population size over time.
Results There were 24 documented events of sudden death or cardiac arrest events among competitive athletes duringthe years 1985 through 2009. Eleven occurred before the 1997 legislation and 13 occurred after it. The averageyearly incidence of sudden death or cardiac arrest events was 2.6 events per 100,000 athlete-years. The respec-tive averaged yearly incidence during the decade before and the decade after the 1997 legislation was 2.54 and2.66 events per 100,000 person years, respectively (p ! 0.88).
Conclusions The incidence of sudden death of athletes in our study is within the range reported by others. However, manda-tory ECG screening of athletes had no apparent effect on their risk for cardiac arrest. (J Am Coll Cardiol 2011;57:1291–6) © 2011 by the American College of Cardiology Foundation
Sudden cardiac death in young athletes is a tragic event.Because most cases are the result of ventricular arrhythmiascaused by underlying heart disease (1), an increasing num-ber of countries now enforce medical pre-participationscreening that includes recording of a baseline electrocardi-ography (ECG) results (2), with the aim of detectingspecific cardiac pathologic features associated with suddendeath in athletes (3). However, the evidence showing thatsuch a strategy actually prevents sudden death amongathletes is limited to a single, retrospective Italian study (4).
In 1997, a mandatory pre-participation screening pro-gram was implemented in Israel (5). By law, the obligatoryscreening tests for all athletes include a medical question-naire, physical examination, baseline ECG, and exercisestress testing. The aim of this study was to evaluate theimpact of this extensive mandatory screening on the inci-dence of sudden death and cardiac arrest in athletes.
See page 1297
Methods
Definitions. The Israel Sport Regulations on AthletesMedical Testing, enacted in 1997, calls for the mandatorymedical screening of all athletes in Israel (6). By law, to beallowed participation in sporting activities, every athlete inIsrael must undergo medical screening by specifically ac-credited physicians. The Israel Sport Law defines athletesrequiring screening as “individuals who engage in sportiveactivity at any level of physical endurance” (6). Only
From the *Department of Internal Medicine “D,” Tel-Aviv Sourasky Medical Centerand Sackler School of Medicine, Tel Aviv University, Tel-Aviv, Israel; †Departmentof Cardiology, Tel-Aviv Sourasky Medical Center and Sackler School of Medicine,Tel Aviv University, Tel-Aviv, Israel; ‡Zinman College of Physical Education &Sports Sciences at the Wingate Institute, Tel-Aviv, Israel; and the §Mediton MedicalCenter, Tel-Aviv, Israel. The authors have reported that they have no relationships todisclose. Drs. Steinvil and Chundadze contributed equally to this work.
Manuscript received July 7, 2010; revised manuscript received September 30, 2010,accepted October 23, 2010.
Journal of the American College of Cardiology Vol. 57, No. 11, 2011© 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00Published by Elsevier Inc. doi:10.1016/j.jacc.2010.10.037

now mandating pre-participation screening—with baselineECG—of all athletes. Yet, there is very limited proof thatsuch preventive strategy actually works (17). We thereforeperformed the present study to assess whether the enforce-ment of massive pre-participation screening, including notonly resting ECG, but also an exercise stress test, wouldreduce the risk of sudden cardiac death or cardiac arrest inathletes.Main findings. We found that the average yearly incidencefor a sudden cardiac death event among Israeli competitiveathletes was 2.6 events per 100,000 person-years or 1 event
per 38,000 athletes per year. These numbers are within therange reported by others (see the following text). Impor-tantly, we found that a mandatory screening strategy includ-ing, resting ECG and exercise ECG, had no apparentinfluence on the incidence of sudden death in athletes.Impact of mandatory screening on the incidence ofsudden death of athletes viewed in the context of previousstudies. Figure 2 shows the annual mortality per 100,000person-years in our study and in the only 2 previousstudies—from Italy (4) and from the United States (19)—that evaluated the effects of screening on the mortality ofathletes over time. The Italian study (4) (pink graph inFig. 2) analyzed the effects of a screening strategy thatincludes baseline ECG recording of all athletes on themortality rates of those 35 years of age or younger. In thatItalian study, the sudden death rate among athletes in theprescreening period was 3.6 per 100,000 person-years,which is similar to the 2.6 per 100,000 person-years findingin our study. The Italian investigators reported that after theonset of screening, the annual rate of sudden death amongathletes decreased dramatically. Indeed, the pink graphshows an impressive reduction in the incidence of suddencardiac death from 3.6 per 100,000 person-years in theprescreening period to 0.4 per 100,000 person-years at theend of the study (from point B to point F in Fig. 2) (4).Note that, in the Italian study, the prescreening period usedas a reference value was limited to the 2 years before theenforcement of pre-participation screening (point A topoint B in Fig. 2).
More recently, Maron et al. (19) reported that the suddendeath rate among high school athletes over a 23-year periodin Minnesota was 1 per 100,000 person-years. That studyappears as a yellow graph in Figure 2. The Minnesotasudden death rate of athletes was lower than the ratesreported in Italy and in our study, although the ECGexamination was not part of the screening strategy used inthe United States during that period.
Our study (green graph in Fig. 2) reports the effects of ascreening strategy that includes resting ECG and exercise
Summary of Sudden Cardiac Death or Cardiac ArrestEvents in Israel in the Years 1985 to 2009Table 1 Summary of Sudden Cardiac Death or Cardiac ArrestEvents in Israel in the Years 1985 to 2009
Event DateSex/Age
(yrs) SportCPR
Delivered?On-Site or
Hospital Death?
01/12/1985 M/17 Football Yes Yes
12/21/1988 M/26 Football Yes Yes
01/13/1991 M/33 Handball Yes Yes
12/05/1992 M/16 Football Yes Yes
01/04/1995 M/23 Football Yes No
01/07/1995 M/17 Football Yes Yes
02/26/1995 M/17 Football Yes Yes
04/12/1995 M/31 Football Yes Yes
12/13/1995 M/28 Rugby Yes Yes
01/21/1996 M/15 Football ND Yes
04/04/1997 M/22 Football Yes Yes
03/01/1998 M/44 Football ND Yes
01/24/1999 M/14 Football Yes Yes
02/20/2000 M/14 Football Yes Yes
08/06/2000 M/18 Basketball Yes Yes
05/01/2001 M/12 Football ND No
01/15/2001 M/39 Football ND Yes
01/26/2002 M/21 Football Yes Yes
09/27/2003 M/22 Athletics Yes Yes
02/18/2004 M/27 Football Yes Yes
10/14/2005 M/40 Triathlon Yes Yes
12/09/2005 M/29 Basketball Yes Yes
09/25/2005 M/21 Football Yes Yes
08/29/2007 M/29 Football Yes Yes
CPR ! cardiopulmonary resuscitation; ND ! no data available.
Figure 1 Sudden Death or Cardiac Arrest Events Rates per 100,000 Athlete-Years From 1985 to 2008
The crude rates are depicted by the solid line. The dotted line depicts our results after assumingthat the percentage of the population actively participating in competitive sport doubled during the last 2 decades.
1293JACC Vol. 57, No. 11, 2011 Steinvil et al.March 15, 2011:1291–6 Electrocardiographic Screening of Athletes

stress testing and started at the end of 1997. There ismarked variation in the sudden cardiac death rates thatpeaks at 8.4 per 100,000 person-years 2 years before theenforcement of screening (point D in Fig. 2). Note that ifone compares the sudden death rates during the 2 yearspreceding the enforcement of screening with the mortalityat the end of the study—as was done in the Italianstudy—one would conclude that our screening strategy isextremely effective for preventing sudden death amongathletes because the sudden death rate decreased from 8.4 to1.1 per 100,000 person-years (p ! 0.001) (D to G inFig. 2). It is only when one reviews the entire study periodand compares the 12-year period before screening with the12-year period after screening (from point C to G in Fig. 2)that it becomes obvious that this apparent mortality reduc-tion is most likely related to a large year-to-year variation.What is the evidence that mandatory pre-participationECG screening of athletes prevents sudden death inathletes? The only evidence that a mandatory screeningstrategy that includes a resting ECG reduces the suddencardiac death risk in athletes comes from Italy (4). ThisItalian study is the basis for current guidelines from theEuropean Heart Society advocating mandatory ECGscreening of athletes (2). It is important to note that theconclusions of the Italian study are based on the comparisonof sudden death rates of athletes recorded during the 2 yearspreceding the enforcement of ECG screening with themortality rates 2 decades later (point A to B vs. B to F inFig. 2). Had we adopted a similar strategy, we would havereached similar conclusions simply because the suddencardiac death rates during the 2-year period preceding theenforcement of screening in Israel were unusually high
(point D in Fig. 2). In reality, it is likely that this unusuallyhigh sudden-death rate observed among Israeli athletes in1995 and 1996—and the public outcry that followed—ledto the legislation mandating ECG screening of athletes inIsrael in 1997. Only when one extends the comparison ofsudden death rates to include the decade that preceded theenforcement of screening in Israel (and not only the last 2years) with the decade that followed it does one realize thatthis mortality reduction is the result of a large variation inmortality rates over longer periods of observation. A similarphenomenon could have occurred in Italy. In other words, itis possible that high mortality rates in Italy in 1980 and1981 led to the Italian legislation in 1982 and allowed forsubsequent mortality reduction. Furthermore, immortal-time bias (20), a methodology flaw frequently encounteredin observational studies (21), probably skewed the findingsof the Italian study toward concluding that screeningimproves survival. Studies with time-dependent outcomesin which the test of interest (ECG screening, in this case)and the outcome analyzed (in this case, sudden death) occurduring the same period are susceptible to time-dependentbias, also termed immortality bias. All the athletes who diedsuddenly during the prescreening period never made it tothe first screening; consequently, the population of athleteswho made it alive to the first screening already representeda selected lower-risk population—and their lower-risk char-acteristics contributed to the lower mortality rates in thepost-screening period.Study limitations. Data on the effects of ECG screeningon mortality rates among athletes are observational andretrospective. This is true for our study and for the Italianand Minnesota studies (4,19). Because of the small
Figure 2 Annual Incidence of Sudden Cardiac Death Expressed per 100,000 Person-Yearsin the 3 Studies Evaluating the Effects of Screening on the Mortality of Athletes Over Time
The Italian study (4) (pink graph) concluded that electrocardiography (ECG) screening (started in 1982) significantly reduced the incidence of sudden cardiac death bycomparing the sudden death in the 2-year pre-screening period (A to B) with the post-screening period (B to F). The present study is depicted by the green graph. Wecompared the 12 years before screening (C to E) with the 12 years after the onset of mandatory ECG screening (E to G). Had we limited our comparison of the post-screening period to the 2-year period preceding the enforcement of screening in Israel (D to E vs. E to G, as performed in the Italian study), we would have concludederroneously that screening saved lives of athletes in Israel. The study from Minnesota (19) (yellow graph) shows a low mortality rate in a population of athletes notundergoing systematic ECG screening.
1294 Steinvil et al. JACC Vol. 57, No. 11, 2011Electrocardiographic Screening of Athletes March 15, 2011:1291–6

El ECG como herramienta de cribado• La utilizacion del ECG en screening ha sido cuestionada por los
resultados anormales detectados debidos en parte a las características del corazon de un paciene muy entrenado.
• Para enfrentarnos a la baja especificidad del ECG se han elaborado unos criterios de interpretación que ayudan a diferenciar entre los cambios diagnosticos de enfermedad y aquellas alteraciones benignas en los deportistas entre ellos tenemos los “Criterios de Seattle” y los de la “Sociedad Europea de Cardiología”.
• Sin embargo se han planteado problemas similares con Ecocardiografía tras ECG anormal por sus resultados ambiguos debidos a los cambios fisiológicos observados en el corazón del deportista.
• Estos falsos positivos tambien se dan con la historia personal y familiar (31%) y la exploración física (9,3%)

Electrocardiographic interpretation in athletes:the ‘Seattle Criteria’Jonathan A Drezner,1 Michael John Ackerman,2 Jeffrey Anderson,3 Euan Ashley,4
Chad A Asplund,5 Aaron L Baggish,6 Mats Börjesson,7 Bryan C Cannon,8
Domenico Corrado,9 John P DiFiori,10 Peter Fischbach,11 Victor Froelicher,4
Kimberly G Harmon,1 Hein Heidbuchel,12 Joseph Marek,13 David S Owens,14
Stephen Paul,15 Antonio Pelliccia,16 Jordan M Prutkin,14 Jack C Salerno,17
Christian M Schmied,18 Sanjay Sharma,19 Ricardo Stein,20 Victoria L Vetter,21
Mathew G Wilson22
For numbered affiliations seeend of article.
Correspondence toJonathan A Drezner,Department of FamilyMedicine, University ofWashington, 1959 NE PacificStreet, Box 356390, Seattle,Washington 98195, USA;[email protected]
Received 7 December 2012Revised 7 December 2012Accepted 7 December 2012
To cite: Drezner JA,Ackerman MJ, Anderson J,et al. Br J Sports Med2013;47:122–124.
This document was developed in collaboration between the American Medical Society for Sports Medicine (AMSSM),the Section on Sports Cardiology of the European Association for Cardiovascular Prevention and Rehabilitation(EACPR), a registered branch of the European Society of Cardiology (ESC), the FIFA Medical Assessment and ResearchCenter (F-MARC), and the Pediatric & Congenital Electrophysiology Society (PACES).
ABSTRACTSudden cardiac death (SCD) is the leading cause of deathin athletes during sport. Whether obtained for screeningor diagnostic purposes, an ECG increases the ability todetect underlying cardiovascular conditions that mayincrease the risk for SCD. In most countries, there is ashortage of physician expertise in the interpretation of anathlete’s ECG. A critical need exists for physicianeducation in modern ECG interpretation that distinguishesnormal physiological adaptations in athletes fromabnormal findings suggestive of pathology. On 13–14February 2012, an international group of experts in sportscardiology and sports medicine convened in Seattle,Washington, to define contemporary standards for ECGinterpretation in athletes. The objective of the meetingwas to develop a comprehensive training resource to helpphysicians distinguish normal ECG alterations in athletesfrom abnormal ECG findings that require additionalevaluation for conditions associated with SCD.
INTRODUCTIONCardiovascular-related sudden death is the leadingcause of mortality in athletes during sport.1 2 Themajority of disorders associated with increased riskof sudden cardiac death (SCD), such as cardiomy-opathies and primary electrical diseases, are sug-gested by abnormal findings present on a 12-leadECG. ECG interpretation in athletes requirescareful analysis to properly distinguish physio-logical changes related to athletic training fromfindings suggestive of an underlying pathologicalcondition. Whether used for the diagnostic evalu-ation of cardiovascular-related symptoms, a familyhistory of inheritable cardiac disease or prematureSCD, or for screening of asymptomatic athletes,ECG interpretation is an important skill for physi-cians involved in the cardiovascular care of athletes.
DISTINGUISHING NORMAL FROM ABNORMALA challenge in the interpretation of an athlete’sECG is the ability to accurately differentiate find-ings suggestive of a potentially lethal cardiovascular
disorder from benign physiological adaptationsoccurring as the result of regular, intense training(ie, athlete’s heart). Several reports have outlinedcontemporary ECG criteria intended to distinguishnormal ECG findings in athletes from ECG abnor-malities requiring additional evaluation.3–8 Despitethe publication of these consensus guidelines, mostsports medicine and cardiology training pro-grammes lack a standard educational curriculum onECG interpretation in athletes.
THE IMPACT OF STANDARDISED CRITERIAStudies demonstrate that without further educationthe ability of many physicians to accurately interpretan athlete’s ECG is relatively poor and may lead to anunacceptable rate of false-positive interpretations andunnecessary secondary evaluations.9 10 However, pro-viding physicians standardised criteria with which toevaluate an ECG considerably improves accuracy.10 Ina study involving physicians across different specialties,use of a simple two-page criteria tool to guide ECGinterpretation significantly improved accuracy to dis-tinguish normal from abnormal findings, even in phy-sicians with little or no experience.10 Therefore,physician education in ECG interpretation is feasibleand accompanied by meaningful improvements inaccuracy when a reference standard is used to assistinterpretation. Further education is needed to producea larger physician infrastructure that is skilled andcapable of accurate ECG interpretation in athletes.
SUMMIT ON ECG INTERPRETATION INATHLETESOn 13–14 February 2012, the American MedicalSociety for Sports Medicine (AMSSM) co-sponsoredby the FIFA Medical Assessment and ResearchCenter (F-MARC) held a ‘Summit onElectrocardiogram Interpretation in Athletes’ inSeattle, Washington. Partnering medical societiesincluded the European Society of Cardiology (ESC)Sports Cardiology Subsection and the Pediatric &Congenital Electrophysiology Society (PACES), aswell as other leading cardiologists on ECG
Drezner JA, et al. Br J Sports Med 2013;47:122–124. doi:10.1136/bjsports-2012-092067 1 of 3
Original articles
group.bmj.com on January 10, 2013 - Published by bjsm.bmj.comDownloaded from

interpretation in athletes from the USA, Europe and around theworld. The goals of the summit meeting were to:
1. define ECG interpretation standards to help physiciansdistinguish normal ECG alterations in athletes from abnor-mal ECG findings that require additional evaluation forconditions associated with SCD;
2. outline recommendations for the initial evaluation ofECG abnormalities suggestive of a pathological cardiovas-cular disorder; and
3. assemble this information into a comprehensive resource andonline training course targeted for physicians around the worldto gain expertise and competence in ECG interpretation.
The consensus recommendations developed are presented inthree papers:
4. Normal Electrocardiographic Findings: RecognizingPhysiologic Adaptations in Athletes11
5. Abnormal Electrocardiographic Findings in Athletes:Recognizing Changes Suggestive of Cardiomyopathy12
6. Abnormal Electrocardiographic Findings in Athletes:Recognizing Changes Suggestive of Primary Electrical Disease13
Box 1 summarises a list of normal ECG findings in athletesthat are considered physiological adaptations to regular exerciseand do not require further evaluation. Table 1 summarises a listof abnormal ECG findings unrelated to athletic training thatmay suggest the presence of a pathological cardiac disorder andshould trigger additional evaluation in an athlete.
ONLINE E-LEARNING ECG TRAINING MODULE—FREE!The Seattle Criteria will be used to develop a comprehensiveonline training module for physicians to acquire a commonfoundation in ECG interpretation in athletes. This state of theart E-learning resource provides additional ECG examples,figures and explanations, and is prepared in a user friendly
educational format to optimise learning. This online trainingmodule is accessible at no cost to any physician world-wide at:http://learning.bmj.com/ECGathlete
LIMITATIONS OF THE SEATTLE CRITERIAWhile the ECG increases the ability to detect underlying cardio-vascular conditions that place athletes at increased risk, ECG asa diagnostic tool has limitations in both sensitivity and specifi-city. Even if properly interpreted, an ECG will not detect allconditions predisposing to SCD. In addition, the true preva-lence of specific ECG parameters in athletes and in diseases thatpredispose to SCD is often unknown and requires further study.The Seattle Criteria were developed with thoughtful attentionto balance sensitivity (disease detection) and specificity (false-positives), while maintaining a clear and usable checklist of find-ings to guide ECG interpretation for physicians, including newlearners.
The criteria define ECG findings that warrant further cardio-vascular evaluation for disorders that predispose to SCD. Thecriteria were developed with consideration of ECG interpret-ation in the context of an asymptomatic athlete age 14–35. Anathlete is defined as an individual who engages in regular exer-cise or training for sport or general physical fitness, typicallywith a goal of improving performance. In the presence of
Box 1 Normal ECG findings in athletes
1. Sinus bradycardia (≥ 30 bpm)2. Sinus arrhythmia3. Ectopic atrial rhythm4. Junctional escape rhythm5. 1° AV block (PR interval > 200 ms)6. Mobitz Type I (Wenckebach) 2° AV block7. Incomplete RBBB8. Isolated QRS voltage criteria for LVH
▸ Except: QRS voltage criteria for LVH occurring withany non-voltage criteria for LVH such as left atrialenlargement, left axis deviation, ST segmentdepression, T-wave inversion or pathologicalQ waves
9. Early repolarisation (ST elevation, J-point elevation, J-wavesor terminal QRS slurring)
10. Convex (‘domed’) ST segment elevation combined withT-wave inversion in leads V1–V4 in black/African athletes
These common training-related ECG alterations arephysiological adaptations to regular exercise, considerednormal variants in athletes and do not require furtherevaluation in asymptomatic athletes.AV, atrioventricular; bpm, beats per minute; LVH, left
ventricular hypertrophy; ms, milliseconds; RBBB, right bundlebranch block.
Table 1 Abnormal ECG findings in athletes
Abnormal ECG finding Definition
T-wave inversion >1 mm in depth in two or more leads V2–V6, IIand aVF, or I and aVL (excludes III, aVR and V1)
ST segment depression ≥0.5 mm in depth in two or more leadsPathologic Q waves >3 mm in depth or >40 ms in duration in two or
more leads (except for III and aVR)Complete left bundlebranch block
QRS ≥120 ms, predominantly negative QRScomplex in lead V1 (QS or rS), and uprightmonophasic R wave in leads I and V6
Intraventricular conductiondelay
Any QRS duration ≥140 ms
Left axis deviation −30° to −90°Left atrial enlargement Prolonged P wave duration of >120 ms in leads I
or II with negative portion of the P wave ≥1 mm indepth and ≥40 ms in duration in lead V1
Right ventricularhypertrophy pattern
R−V1+S−V5>10.5 mm AND right axis deviation>120°
Ventricular pre-excitation PR interval <120 ms with a delta wave (slurredupstroke in the QRS complex) and wide QRS(>120 ms)
Long QT interval* QTc≥470 ms (male)QTc≥480 ms (female)QTc≥500 ms (marked QT prolongation)
Short QT interval* QTc≤320 msBrugada-like ECG pattern High take-off and downsloping ST segment
elevation followed by a negative T wave in ≥2leads in V1–V3
Profound sinus bradycardia <30 BPM or sinus pauses ≥ 3 sAtrial tachyarrhythmias Supraventricular tachycardia, atrial-fibrillation,
atrial-flutterPremature ventricularcontractions
≥2 PVCs per 10 s tracing
Ventricular arrhythmias Couplets, triplets and non-sustained ventriculartachycardia
Note: These ECG findings are unrelated to regular training or expectedphysiological adaptation to exercise, may suggest the presence ofpathological cardiovascular disease, and require further diagnostic evaluation.*The QT interval corrected for heart rate is ideally measured with heart rates of60–90 bpm. Consider repeating the ECG after mild aerobic activity for borderline orabnormal QTc values with a heart rate <50 bpm.
2 of 3 Drezner JA, et al. Br J Sports Med 2013;47:122–124. doi:10.1136/bjsports-2012-092067
Original articles
group.bmj.com on January 10, 2013 - Published by bjsm.bmj.comDownloaded from

interpretation in athletes from the USA, Europe and around theworld. The goals of the summit meeting were to:
1. define ECG interpretation standards to help physiciansdistinguish normal ECG alterations in athletes from abnor-mal ECG findings that require additional evaluation forconditions associated with SCD;
2. outline recommendations for the initial evaluation ofECG abnormalities suggestive of a pathological cardiovas-cular disorder; and
3. assemble this information into a comprehensive resource andonline training course targeted for physicians around the worldto gain expertise and competence in ECG interpretation.
The consensus recommendations developed are presented inthree papers:
4. Normal Electrocardiographic Findings: RecognizingPhysiologic Adaptations in Athletes11
5. Abnormal Electrocardiographic Findings in Athletes:Recognizing Changes Suggestive of Cardiomyopathy12
6. Abnormal Electrocardiographic Findings in Athletes:Recognizing Changes Suggestive of Primary Electrical Disease13
Box 1 summarises a list of normal ECG findings in athletesthat are considered physiological adaptations to regular exerciseand do not require further evaluation. Table 1 summarises a listof abnormal ECG findings unrelated to athletic training thatmay suggest the presence of a pathological cardiac disorder andshould trigger additional evaluation in an athlete.
ONLINE E-LEARNING ECG TRAINING MODULE—FREE!The Seattle Criteria will be used to develop a comprehensiveonline training module for physicians to acquire a commonfoundation in ECG interpretation in athletes. This state of theart E-learning resource provides additional ECG examples,figures and explanations, and is prepared in a user friendly
educational format to optimise learning. This online trainingmodule is accessible at no cost to any physician world-wide at:http://learning.bmj.com/ECGathlete
LIMITATIONS OF THE SEATTLE CRITERIAWhile the ECG increases the ability to detect underlying cardio-vascular conditions that place athletes at increased risk, ECG asa diagnostic tool has limitations in both sensitivity and specifi-city. Even if properly interpreted, an ECG will not detect allconditions predisposing to SCD. In addition, the true preva-lence of specific ECG parameters in athletes and in diseases thatpredispose to SCD is often unknown and requires further study.The Seattle Criteria were developed with thoughtful attentionto balance sensitivity (disease detection) and specificity (false-positives), while maintaining a clear and usable checklist of find-ings to guide ECG interpretation for physicians, including newlearners.
The criteria define ECG findings that warrant further cardio-vascular evaluation for disorders that predispose to SCD. Thecriteria were developed with consideration of ECG interpret-ation in the context of an asymptomatic athlete age 14–35. Anathlete is defined as an individual who engages in regular exer-cise or training for sport or general physical fitness, typicallywith a goal of improving performance. In the presence of
Box 1 Normal ECG findings in athletes
1. Sinus bradycardia (≥ 30 bpm)2. Sinus arrhythmia3. Ectopic atrial rhythm4. Junctional escape rhythm5. 1° AV block (PR interval > 200 ms)6. Mobitz Type I (Wenckebach) 2° AV block7. Incomplete RBBB8. Isolated QRS voltage criteria for LVH
▸ Except: QRS voltage criteria for LVH occurring withany non-voltage criteria for LVH such as left atrialenlargement, left axis deviation, ST segmentdepression, T-wave inversion or pathologicalQ waves
9. Early repolarisation (ST elevation, J-point elevation, J-wavesor terminal QRS slurring)
10. Convex (‘domed’) ST segment elevation combined withT-wave inversion in leads V1–V4 in black/African athletes
These common training-related ECG alterations arephysiological adaptations to regular exercise, considerednormal variants in athletes and do not require furtherevaluation in asymptomatic athletes.AV, atrioventricular; bpm, beats per minute; LVH, left
ventricular hypertrophy; ms, milliseconds; RBBB, right bundlebranch block.
Table 1 Abnormal ECG findings in athletes
Abnormal ECG finding Definition
T-wave inversion >1 mm in depth in two or more leads V2–V6, IIand aVF, or I and aVL (excludes III, aVR and V1)
ST segment depression ≥0.5 mm in depth in two or more leadsPathologic Q waves >3 mm in depth or >40 ms in duration in two or
more leads (except for III and aVR)Complete left bundlebranch block
QRS ≥120 ms, predominantly negative QRScomplex in lead V1 (QS or rS), and uprightmonophasic R wave in leads I and V6
Intraventricular conductiondelay
Any QRS duration ≥140 ms
Left axis deviation −30° to −90°Left atrial enlargement Prolonged P wave duration of >120 ms in leads I
or II with negative portion of the P wave ≥1 mm indepth and ≥40 ms in duration in lead V1
Right ventricularhypertrophy pattern
R−V1+S−V5>10.5 mm AND right axis deviation>120°
Ventricular pre-excitation PR interval <120 ms with a delta wave (slurredupstroke in the QRS complex) and wide QRS(>120 ms)
Long QT interval* QTc≥470 ms (male)QTc≥480 ms (female)QTc≥500 ms (marked QT prolongation)
Short QT interval* QTc≤320 msBrugada-like ECG pattern High take-off and downsloping ST segment
elevation followed by a negative T wave in ≥2leads in V1–V3
Profound sinus bradycardia <30 BPM or sinus pauses ≥ 3 sAtrial tachyarrhythmias Supraventricular tachycardia, atrial-fibrillation,
atrial-flutterPremature ventricularcontractions
≥2 PVCs per 10 s tracing
Ventricular arrhythmias Couplets, triplets and non-sustained ventriculartachycardia
Note: These ECG findings are unrelated to regular training or expectedphysiological adaptation to exercise, may suggest the presence ofpathological cardiovascular disease, and require further diagnostic evaluation.*The QT interval corrected for heart rate is ideally measured with heart rates of60–90 bpm. Consider repeating the ECG after mild aerobic activity for borderline orabnormal QTc values with a heart rate <50 bpm.
2 of 3 Drezner JA, et al. Br J Sports Med 2013;47:122–124. doi:10.1136/bjsports-2012-092067
Original articles
group.bmj.com on January 10, 2013 - Published by bjsm.bmj.comDownloaded from


Distinguir entre un corazon normal y anormal
• Debido a la dificultad en distinguir las anomalías cardiovasculares del corazon normal de un deportista incluso utilizando técnicas diagnósticas complejas se plantea el dilema de la exclusión innecesaria de algunos deportistas.
• En otros casos se podria garantizar erroneamente que no había alteraciones cardiovasculares y sufrir el deportista una muerte súbita.
• Ademas en algunos estudios presentan un riesgo similar de muerte súbita cardiaca los deportistas de competición y aquellos que realizan deporte como actividad lúdica por lo que un programa de cribado solo a los primeros no sería ético.
• Otros estudios, en cambio, muestran mayor riesgo de MSD en los competitivos.

Razón coste-beneficio
• Con datos del estudio italiano deberían ser cribados 33.000 deportistas para salvar una vida a un coste por vida salvada de 1.185.000 €.
!
• Se puede argumentar que este dinero podría utilizarse para las necesidades sanitarias que afectan a la población (dieta, obesidad, tabaquismo…)


Recomendaciones internacionales• La “American Heart Association” recomienda realizar una
historia personal y familiar completa junto a una exploración física antes de la participación en deportes competitivos.
• La “European Society of Cardiology” recomienda además la realizacion de ECG con 12 derivaciones.
• Algunas organizaciones deportivas como la FIFA han puesto en marcha programas de cribado para todos los jugadores.
• La OMS ha señalado la necesidad de tener en cuenta los criterios de Wilson y Jungner para poner en marcha programas de cribado en toda la población escolar.
• Un estudio concluye que aunque el cribado en poblacion escolar cumple algunos criterios es prematuro iniciar programas de cribado con ECG en esta población


¿Que mas podemos hacer para prevenir la MSD?• Aumentar los conocimientos y motivacion de MF puede ser un paso
importante para prevenir MSD.
• La historia clinica incluirá preguntas sobre la existencia de síncopes previos, síntomas relacionados con el ejercicio como palpitaciones o presíncope y acerca de historia familiar de cardiopatía o muerte súbita en jóvenes (<40 años)
• La exploracion incluira: TA, FC, búsqueda de latido de apex en torax y auscultacion cuidadosa buscando soplos o ruidos adicionales.
• Algunos deportistas pueden venir a consulta para que les hagamos exploracion preparticipación en deportes competitivos, en esta situacion una historia personal y familiar junto a exploración física y ECG normal es suficiente.
• En algunos deportistas de elite (maraton, triatlon) puede estar indicada ecocardiografía para valorar estructura y función cardiaca

Figures
Fig 1 Important diagnostic features compatible with both physiologically based adaptions to athletic training (athlete’s heart)and cardiomyopathies. Adapted from Maron et al 20033
Fig 2 Important clinical history, examination findings, and basic cardiac investigations that may indicate underlying cardiacdisease in athletes5 37
For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe
BMJ 2015;350:h1218 doi: 10.1136/bmj.h1218 (Published 18 March 2015) Page 7 of 7
CLINICAL REVIEW

¿Que mas podemos hacer para prevenir la MSD?• Los pacientes diagnosticados de cardiopatía deberían dejar el deporte de
competición con excepcion de deportes clase I: billar, golf, bolos… sin embargo algunos estudios demuestran que estas normas pueden ser demasiado restrictiva y tratamiento medico o incluso desfibrilador implantable pueden permitir realización de deporte competitivo.
• A nivel comunitario el acceso a DEA junto al entrenamiento en RCP puede disminuir las MSD
• La FIFA reconoce la necesidad de establecer una atención medica estandarizada de las emergencias y ha establecido una serie de 11 puntos para prevenir MSD incluyendo entrenamiento en RCD y DEA y asegurando la existencia de una “bolsa para las emergencias” en los campos de futbol y que los miembros de los equipos sepan reconocer una posible parada cardiaca y como responder ante ella.
• Grupos de corredores han puesto énfasis en la formacion en RCP y disposición de DEA en escuelas y clubs deportivos así como a lo largo de las carreras
• Algunos paises como Japon y Austria obligan a completar cursos de RCP para obtener carnet de conducir aumentando así el número de personas entrenadas en la comunidad.

GRACIAS POR VUESTRA ATENCIÓN