Juan Carlos Garcia-Pagán...Trombosis Portal Aguda. Tratamiento I Anticoagulación: Tratamiento de...
41
Juan Carlos Garcia-Pagán Barcelona Hepatic Hemodynamic Laboratory. Liver Unit. IMDIM. Hospital Clinic. IDIBAPS. Ciberehd. Barcelona X Curso de Formación Continuada en Trombosis y Hemostasia. 20 Noviembre 2015. Zaragoza Trombosis Portal y Síndrome de Budd-Chiari
Transcript of Juan Carlos Garcia-Pagán...Trombosis Portal Aguda. Tratamiento I Anticoagulación: Tratamiento de...

Juan Carlos Garcia-PagánBarcelona Hepatic Hemodynamic Laboratory. Liver Unit. IMDIM.
Hospital Clinic. IDIBAPS. Ciberehd. Barcelona
X Curso de Formación Continuada en Trombosis y Hemostasia.
20 Noviembre 2015. Zaragoza
Trombosis Portal y Síndrome de Budd-Chiari

• Enfermedades raras
• Trombosis Venosa
• Causan Hipertensión Portal
• Frecuentemente causa
hematológica subyacente
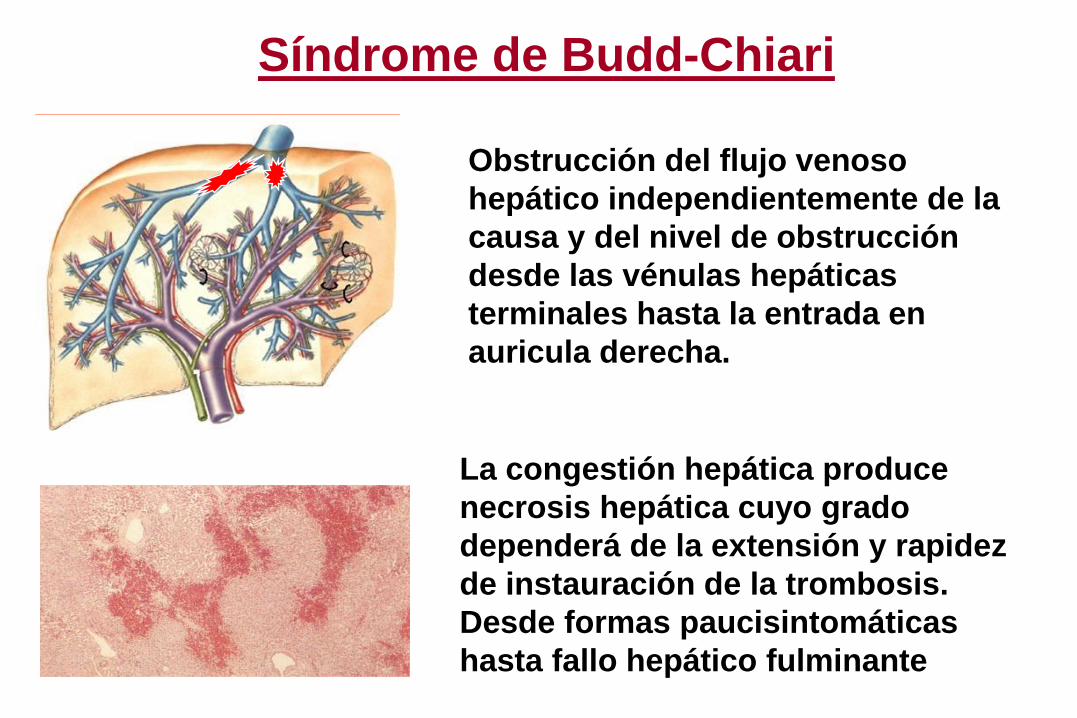
Síndrome de Budd-Chiari
Obstrucción del flujo venoso
hepático independientemente de la
causa y del nivel de obstrucción
desde las vénulas hepáticas
terminales hasta la entrada en
auricula derecha.
La congestión hepática produce
necrosis hepática cuyo grado
dependerá de la extensión y rapidez
de instauración de la trombosis.
Desde formas paucisintomáticas
hasta fallo hepático fulminante

Budd-Chiari Syndrome. Survival
100
50
0
1 3 5 Years
1997-2004Plessier Hepatology 2006
1987-2002Murad Hepatology 2004
1960-1970Tavill Gastroenterology 1975
From D. Valla
Mejoría Supervivencia:
1. Diagnóstico precoz (Elevada Sospecha Diagnóstica;
Mejores pruebas de imagen)
2. Diagnóstico de la causa protrombótica subyacente y su
tratamiento
3. Tratamientos más eficaces (TIPS)
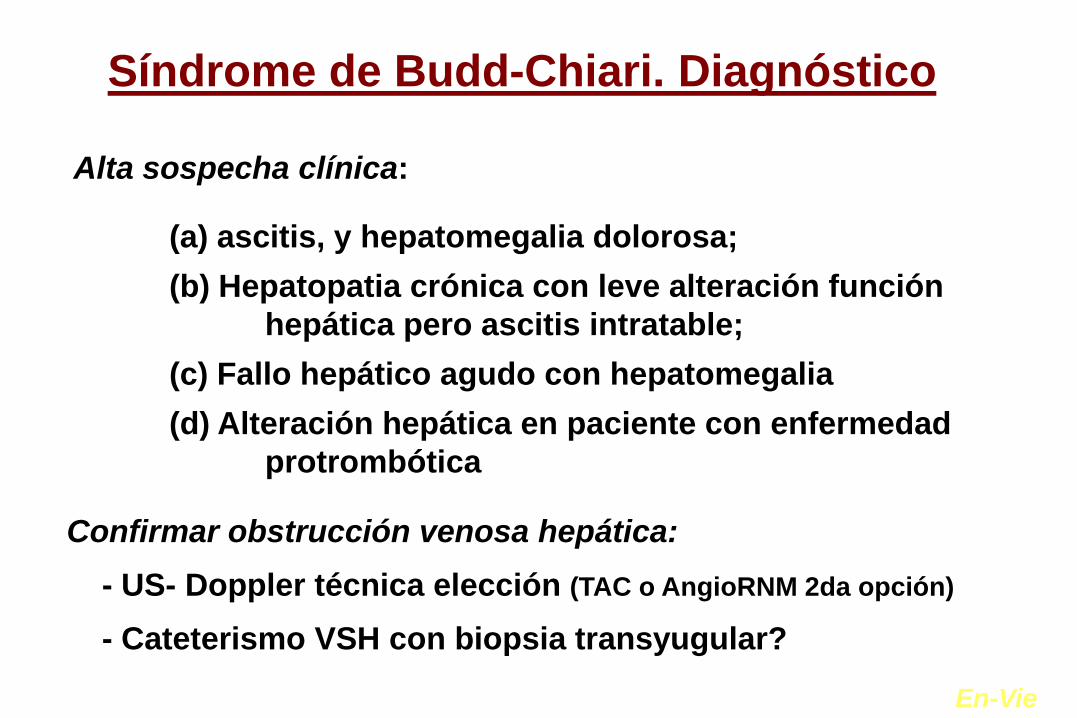
Síndrome de Budd-Chiari. Diagnóstico
Alta sospecha clínica:
(a) ascitis, y hepatomegalia dolorosa;
(b) Hepatopatia crónica con leve alteración función
hepática pero ascitis intratable;
(c) Fallo hepático agudo con hepatomegalia
(d) Alteración hepática en paciente con enfermedad
protrombótica
Confirmar obstrucción venosa hepática:
- US- Doppler técnica elección (TAC o AngioRNM 2da opción)
- Cateterismo VSH con biopsia transyugular?
En-Vie
Síndrome de Budd-Chiari.
Diagnóstico etiológico
Procesos protrombóticos adquiridos
Síndromes mieloproliferativos (P Vera, T Esencial)
Síndrome antifosfolípido; HPN
Estados inflamatorios, hiperhomocisteinemia
Procesos protrombóticos hereditarios
Mutación de factor V de Leiden; de factor II G20210A
Déficits antitrombina III; proteína C y S
65%
• En menos del 10% no se encuentra ninguna causa: Idiopática
• En más del 10% casos más de una causa

Síndrome de Budd-Chiari y TP
Hipertension Portal ocasiona
esplenomegalia con hiperesplenismo y
expansión del volumen plamático con
hemodilución
Esto puede enmascarar aumento en
las células sanguíneas.
JAK2; Calreticulin!!

• CALR + en 4 pacientes
• 1,9% de toda la cohorte
• 31% de las NMPs JAK2 negativo
209 pts con trombosis esplácnica
140 TVP 69 SBC
30 JAK2+ (21%) 31 JAK2+ (45%)
2 Calreticulin+/110 JAK2- (1.8%) 2 Calreticulin+ /38 JAK2- (5.3%)
35 MPN32/35 (91.5% JAK2 o CAL)
39 MPN33/39 (85% JAK2 o CAL)
Turon et al. J Hepatol 2015

Budd-Chiari Treatment
Asymptomatic patients
• BCS may be asymptomatic and diagnosed incidentally
Collateral formation keeps patient
asymptomatic
Underlying Thrombofilia!!!
Rethrombosis may lead to
decompensation
Asymptomatic Patients
• Rx underlying disorder
• Anticoagulation
• Clinical Surveillance

Failure of Medical Rx
• Very close Surveillance
(weekly, monthly…)
TIPS
Transplantation
Stepwise Management of BC Patients
• How much to wait until
considering TIPS and OLT?
• Are there data to recommend
Early-TIPS or Early-OLT in
some severe BC patients?

Prospective Study in 163 BCS patients. Results of
applying Stepwise Rx strategy. Long-Term Follow-up.
Seijo et al. Hepatology 2013
Cu
mu
lative
pro
ba
bili
ty
88%
45%
79%
31%
74%
29%
Overall survival
Survival without OLT
Survival without OLT/TIPS
Survival without
OLT/TIPS or Angioplasty
Anticoagulation
Medical Rx
Angioplasty
TIPS
OLT
Years OLT in BCS. European Registry J Hepatol 2006

Obstrucción de la vena
porta con o sin afectación
de las ramas portales
intrahepáticas que puede
extenderse a vena esplenica
y/o mesentericas
Trombosis eje espleno-portal

TVP. Diagnóstico y estudio de Extensión
US-Doppler.
• Muy sensible y especifica. Pero muy operador
dependiente (falsos negativos)
Angio-TAC/Angio-RNM.
• Muy sensible y especifica. Menos operador
dependiente. Visualiza todo el eje. Falsos
positivos!
US-Doppler técnica inicial y confirmar y evaluar
extensión con Angio-TAC o Angio-RNM.

Thrombosis of the PV System. Etiology
Healthy Liver Diseased Liver
- Cirrhosis (Non-Tumoral PVT)
- IPH/Non-Cirrhotic IntraH. PH

Thrombosis of the PV System. Etiology
Healthy Liver Diseased Liver
Acquired or Inherited Prothrombotic Dis. 40-50%
- Myeloproliferative Syndromes
- Prothrombin gen mutation
- Others
Local Factor: Surgery, abd. inflamation… 20-30%
Idiopathic 20-30%
• 36% of those with a local factor, also had a general
prothrombotic disorder
Plessier for the Envie Group. Hepatology 2010

PVT in Healthy Liver
• Abd. Pain/Intestinal Isch.
• Infarction
Acute PVT Chronic PVT/
Portal Cavernoma
• Variceal Bleeding
• Portal Colangiopathy
• Recurrent Thrombosis
• Others
- Prevent Ischemic Complications
- Prevent Progression to Chronic
Aim of Rx in Acute PVT:
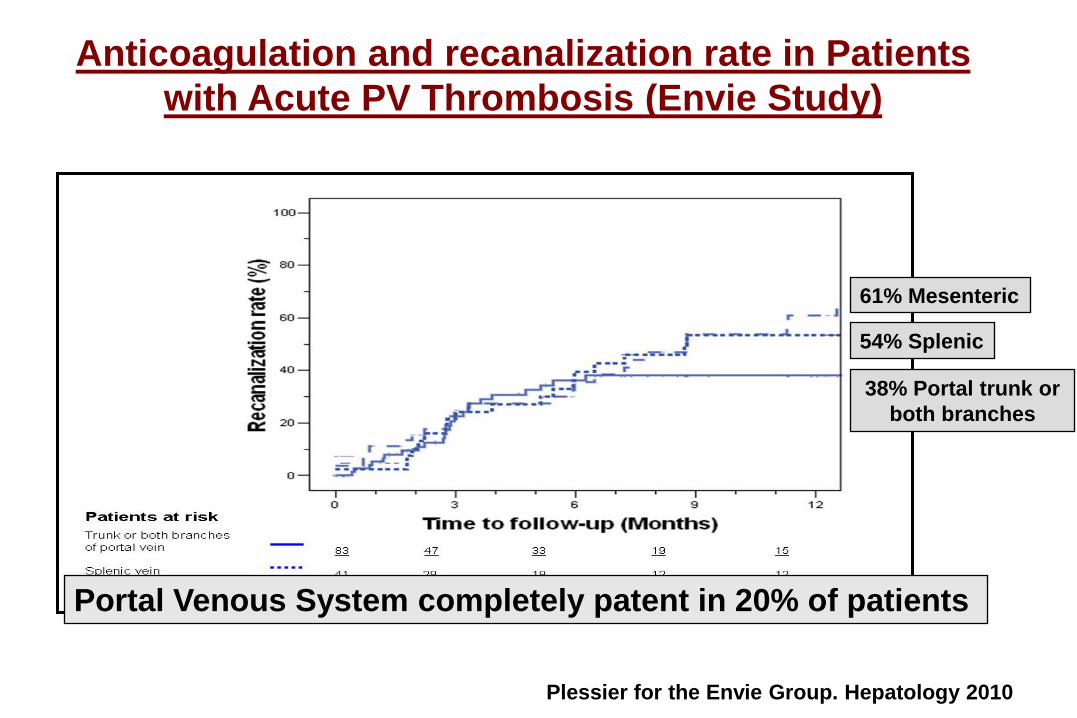
Anticoagulation and recanalization rate in Patients
with Acute PV Thrombosis (Envie Study)
61% Mesenteric
54% Splenic
38% Portal trunk or
both branches
Portal Venous System completely patent in 20% of patients
Plessier for the Envie Group. Hepatology 2010

Predictors for Absence of Recanalization. Envie Study
Plessier for the Envie Group. Hepatology 2009
Envie Study. Anticoagulation in 95 Acute PVT
• 2 Intestinal Infarction, limited intestinal resection,
both pts survived
• 9 bleeding (5 GI; 3 Severe: No mortality)
• 2 death (1 Late malignancy and 1 sepsis)
Low number of adverse events
Plessier for the Envie Group. Hepatology 2009

Thrombolytic Therapy in Acute thrombosis of the PV System
Rate of Recanalization and complications
0
10
20
30
40
50
60
70
Major complications
Minor complications
No
%Complications
Hollingshead et al. J Vasc Interv Radiol 2005 (n=20) Smalberg et al. Thromb Haemost 2008 (n=12)
Different routes and systems of thrombolysis
0
10
20
30
40
50
Complete Partial No Recanalization
Recanalization%
60
70

Trombosis Portal Aguda. Tratamiento I
Anticoagulación: Tratamiento de elección
• Iniciar lo más precozmente posible
• Reduce el riesgo de infarto intestinal y de
muerte y puede lograr la repermeabilización con
escasas complicaciones
• Si existe una enfermedad protrombótica
subyacente o el paciente ha presentado
síntomas de isquemia intestinal, mantener
anticoagulación de por vida
• En otras situaciones 6-12 meses

• En casos de persistencia o empeoramiento de
síntomas a pesar de la anticoagulación (elevado
riesgo de infarto intestinal!)
Trombolisis/Trombectomia:
Trombosis Portal Aguda. Tratamiento II
Chronic Non-Cirrhotic Non-Tumoral PVT
Gastroesophageal Varices (Baveno VI)
• Patients not achieving recanalization, should be screened for varices within 6 months of the acute episode

Gastroesophageal Varices In Chronic PVT
French-Spanish Cohort
178 Chronic PVT pts
• Variceal Bleeding at diagnosis (15%)
• No Varices (29%)
• Small Esophageal Varices (16%)
• Large Gastroesophageal Varices (40%)

Actuarial probability of appearance of varices
Number
at risk40 35 28 20 14 12 9 8 6
22%22%
Chronic Non-Cirrhotic Non-Tumoral PVT
Gastroesophageal Varices (Baveno VI)
• In the absence of varices, endoscopy should be repeated at 12 months and 2 years thereafter
• Primary and secondary prophylaxis and treatment of acute variceal bleeding as for Cirrhosis

Chronic PVT. Portal Cholangiopathy
Biliary tree abnormalities seen in patients with extrahepatic portal vein
obstruction
Collateral Vessels
Cholangio-Angio-MRI
Different degrees of biliary alterations from mild compression to severe
stenosis/dilatations
• Symptomatic: 19% (5-38%)
• Abdominal pain; Jaundice; Cholangitis
• Incidence (CPRE/Cholangio-MRI) • 94% (81-100%)

Recurrent Thrombosis in pts with NCNT-PVT
- Probably much more common than suspected.
- Frequently asymptomatic and only recognized if intentionally
investigated.
- Rethrombosis may deteriorate outcome
- Different risk according with underlying etiology.
Anticoagulation in Chronic PVT if:
• Existence of an underlying prothrombotic disordes
• Previous thrombosis of other vascular territories
• Rethrombosis/thrombosis progression
Prevents recurrent thrombosis without * or with **more risk of GI bleeding
but without increasing the severity of bleeding when it occurs
*Condat et al. Gastroenterology 2001;**Spaander et al. J Thromb Haem 2013

In non-cirrhotic non-tumoral PVT there is an
hypercoagulative state independent of the etiology
Further increase in the risk of new thrombotic events?
Raffa et al. Cclin Gastroenterol Hepatol 2012
• Reduced procoagulant and anticoagulant factors
• Increased vWF
• Increased Thrombin generation
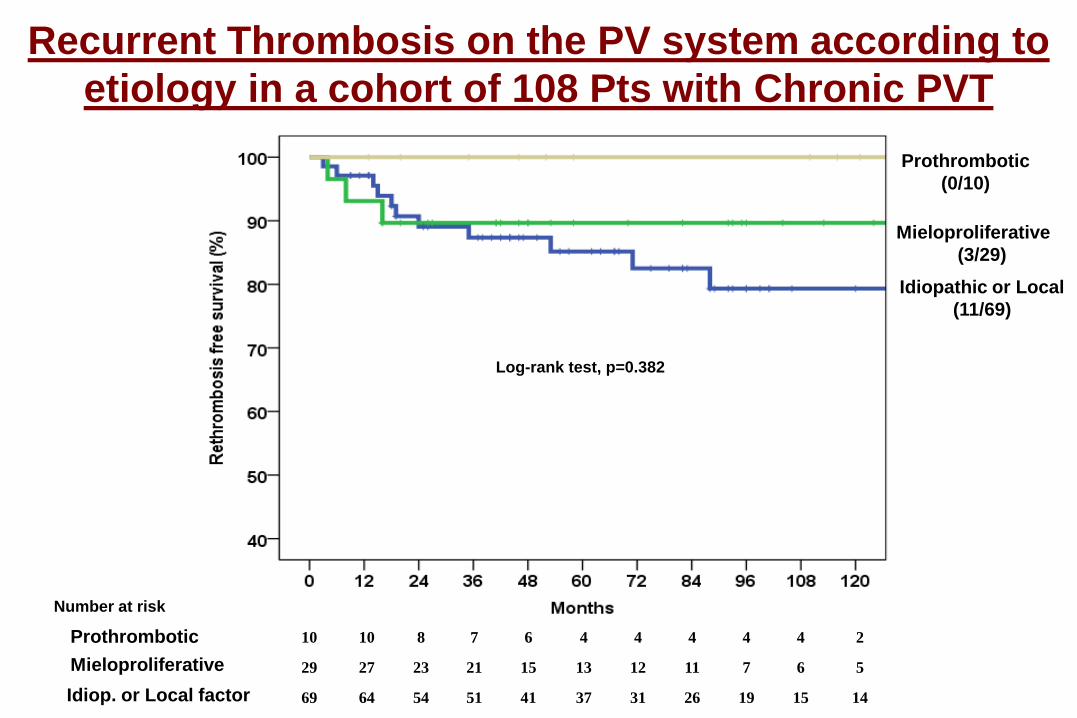
Idiopathic or Local
(11/69)
Log-rank test, p=0.382
Number at risk
10 10 8 7 6 4 4 4 4 4 2
29 27 23 21 15 13 12 11 7 6 5
69 64 54 51 41 37 31 26 19 15 14
Mieloproliferative
(3/29)
Idiop. or Local factor
Mieloproliferative
Prothrombotic
(0/10)
Prothrombotic
Recurrent Thrombosis on the PV system according to
etiology in a cohort of 108 Pts with Chronic PVT

with ACO
(0/12)
Without ACO
(11/57)
Log-rank test, p=0.168
Number at risk
12 11 10 8 5 3 2 2 1 1 1
57 53 44 43 36 34 29 24 18 14 13
Recurrent Thrombosis in patients with Idiopathic or
Underlying Local Factors receiving or not ACO
Anticoagulation
No anticoagulation
Is there a group of patients with Idiopathic
thrombosis or secondary to local factors that
need to be also treated with long-term
anticoagulation?

Janssen et al. Gut 2001
Patients With Non-Cirrhotic Non-Malignant Chronic
Portal Vein Thrombosis had a Good Prognosis
47
Rajani et al. Aliment Pharmacol Ther 2010; 32: 1154-1162
> 85% Survival at 5 y

www.valdig.eu

The Barcelona Portal Hypertension Team
Vascular liver diseases collaborative group
Barcelona Hepatic Hemodynamics Laboratory


JAK2 y Trombosis esplácnica241 pacientes (104 SBC, 137 TVP), 3 centros Europeos.
Kiladjian et Al. Blood, 2008
JAK2V617F + en 91 pacientes (45% de SBC, 34% de TVP)No MPL ni JAK2 exon 12
-Aumentar el dx de NMPs: de 31% a 44%- Evitar el 40% de BMO

TIPS for BCS – Learning Curve
Plessier Hepatology 2006
• TIPS, using PTFE-Covered Stents, is the Treatment
of Choice in BC patients unresponsive to
Supportive Therapy.
• However, TIPS in BC patients needs a particular
training and should be done in Specific Referral
Centers (More than 40% Direct inferior Vena Cava
Punction)

Distribución de las mutaciones JAK2 y CALR en los pacientes
con trombosis esplácnica y neoplasias mieloproliferativas
Turon et al. J Hepatol 2015
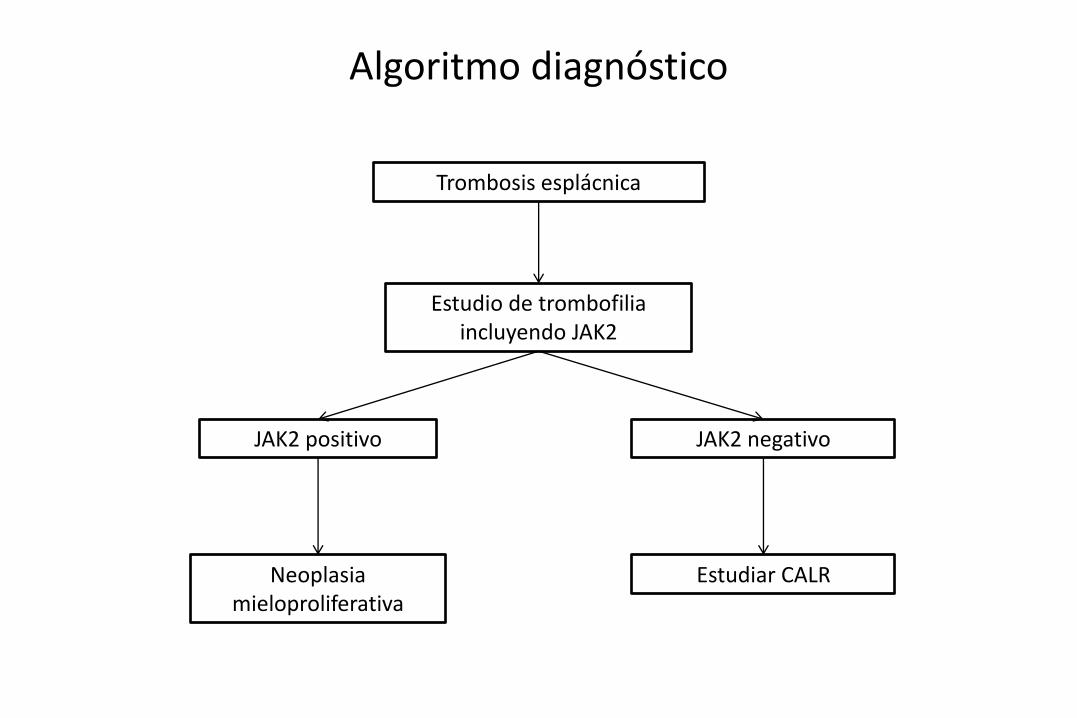
Trombosis esplácnica
Estudio de trombofilia incluyendo JAK2
JAK2 positivo
Neoplasia mieloproliferativa
JAK2 negativo
Estudiar CALR
Algoritmo diagnóstico

• El tratamiento en el SBC debe ser individualizado
• Un porcentaje considerable de pacientes sólo requieren
tratamiento médico con anticoagulación y de la enfermedad
de base
• En pacientes con una obstrucción/estenosis segmentaria de
la vena suprahepática, la angioplastia o la colocación de una
prótesis para en la zona estenosada es la mejor opción
terapéutica
• El TIPS es la opción de elección en pacientes con SBC en los
que fracasa el tratamiento médico
• El TOH debe ser utilizado en los pacientes en los que fracase
el TIPS
Síndrome de Budd-Chiari. Tratamiento

Other PVT Complications
•Overt HE Infrequent. Usually triggered
•More frequent Minimal Hepatic Encephalopathy
Long-Term consequences?
•Mild ascites easily controlled in 20%
• If severe discard other possible causes (e.g.
Cirrhosis + PVT; nephrotic syndrome...)