FUMC Case Presentation
29
-
Upload
princess-grace-mamplata -
Category
Documents
-
view
224 -
download
0
Transcript of FUMC Case Presentation
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 1/29
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 2/29
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 3/29
CASECASEPRESENTATIONPRESENTATION
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 4/29
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 5/29
P A T I E N T · S P
R O F I L
E
P A T I E N T · S P
R O F I L
EName: Mrs. D
Age: 39 years old
Gender: Female
Address :Bonifacio, Makati City
Date of Birth: July 3, 1972
Civil Status: Married
Religion: Baptist
Nationality: Filipino
Occupation: Accountant
Spouse: Mr. D
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 6/29
Date of Admission: January 16, 2012 (9:12pm)
Mode of Admission: Wheelchair from ER(Accompanied by Husband)
Chief Complaint:
Abdominal Pain
Admitting Diagnosis:
Fatty Liver, Gallbladder Polyp
Patient D has no history of Hypertension, DM,
Asthma, or any allergic reaction to medications. She
has also no history of any discussed diseases on herfamily. The patient was neither a smoker nor a drinker.
She consumes four meals a day, with some foods high
on fats.
P A T I E N T · s H
I S T O
R Y
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 7/29
ANATOMY and PHYSIOLOGYANATOMY and PHYSIOLOGY
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 8/29
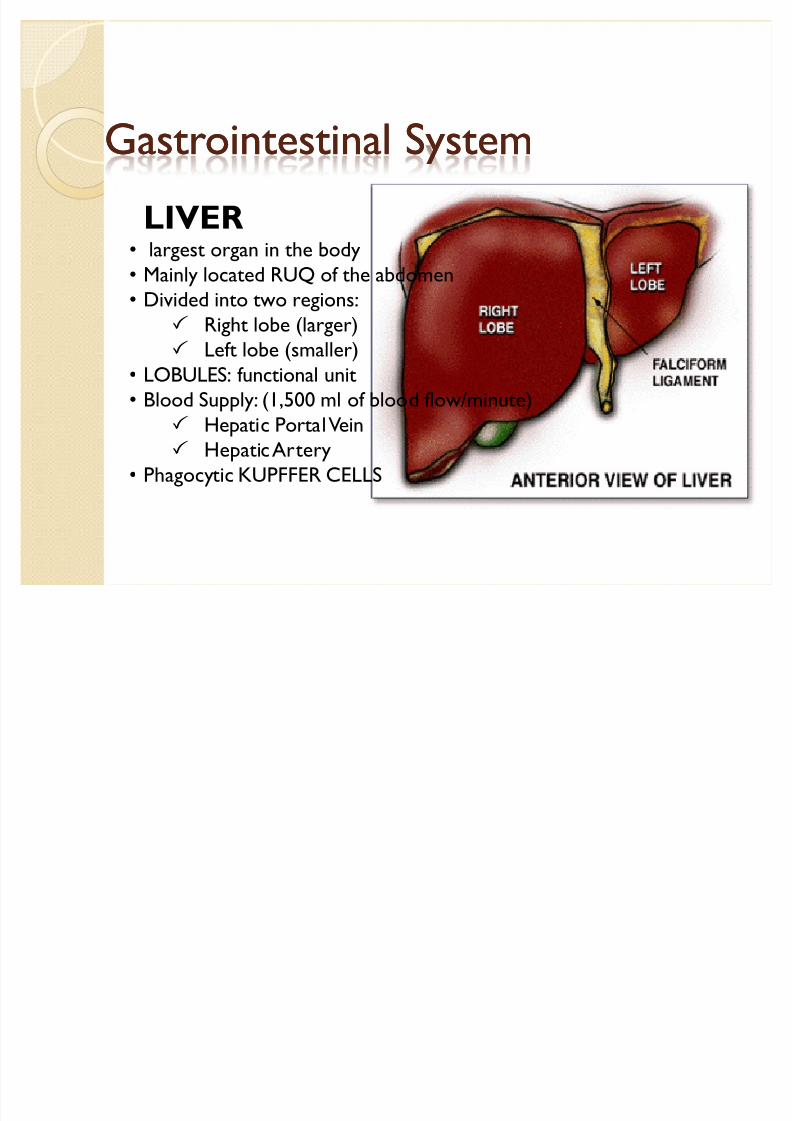
Gastrointestinal SystemGastrointestinal System
LIVER largest organ in the body
Mainly located RUQ of the abdomen
Divided into two regions:
Right lobe (larger)
Left lobe (smaller)
LOBULES: functional unit
Blood Supply: (1,500 ml of blood flow/minute)
Hepatic Portal Vein
Hepatic Artery
Phagocytic KUPFFER CELLS
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 9/29
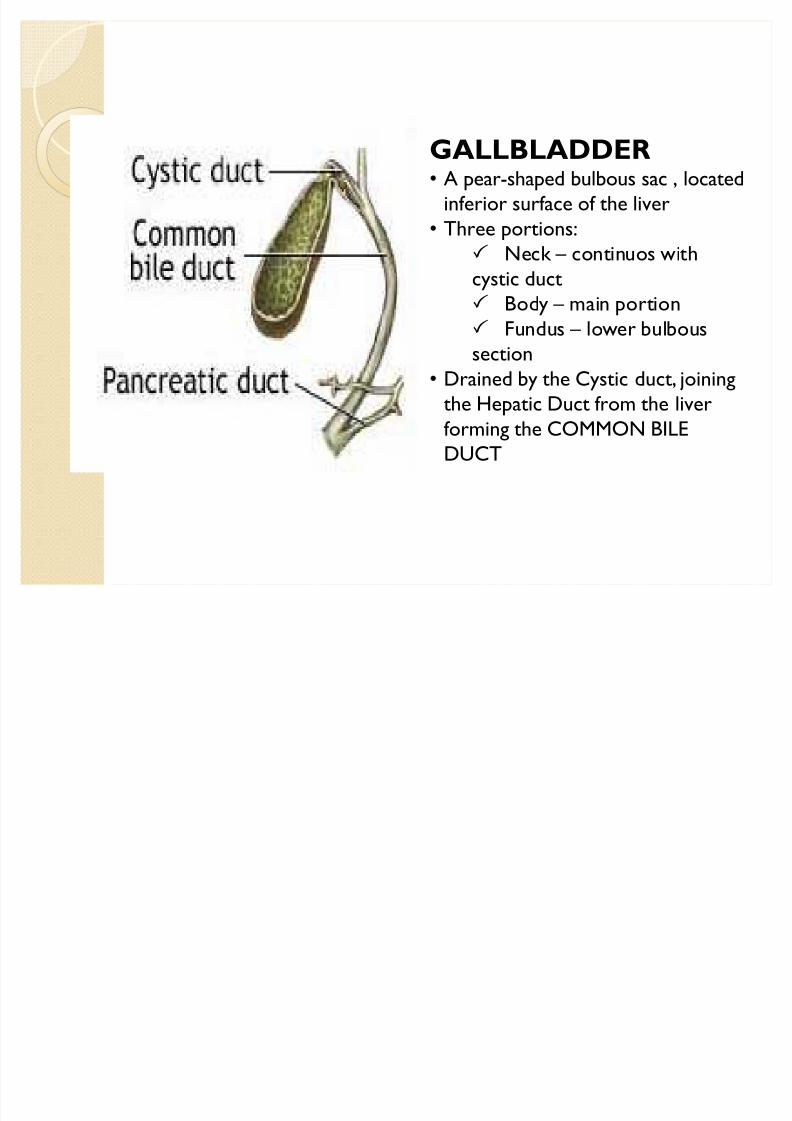
GALLBLADDER A pear-shaped bulbous sac , located
inferior surface of the liver
Three portions:
Neck ² continuos with
cystic duct Body ² main portion
Fundus ² lower bulbous
section
Drained by the Cystic duct, joining
the Hepatic Duct from the liverforming the COMMON BILE
DUCT
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 10/29
y LIVER:
Produces BILES Regulates blood glucose ( Glycogenesis/ Glycogenolysis)
Synthesizes proteins and other AA
Converts Ammonia to Urea for kidney elimination
Stores Vitamins (ADEK) and Minerals
Brakes down certain toxic substances and hormones
(Kupffer cells)
GALLBLADDER:
Collects, concentrates, and stores BILE
Releases the bile into duodenum via common bile duct
when fat is present.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 11/29
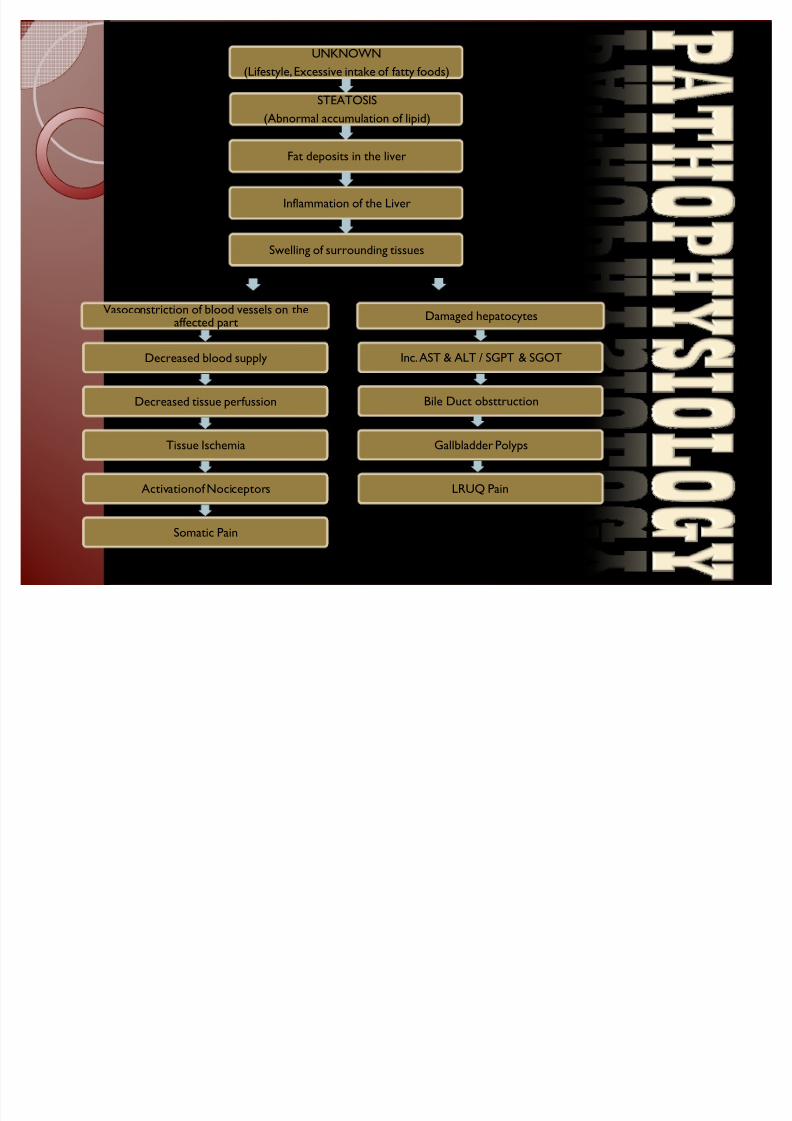
UNKNOWN
(Lifestyle, Excessive intake of fatty foods)
STEATOSIS
(Abnormal accumulation of lipid)
Fat deposits in the liver
Inflammation of the Liver
Swelling of surrounding tissues
Vasoconstriction of blood vessels on theaffected part
Decreased blood supply
Decreased tissue perfussion
Tissue Ischemia
ActivationofNociceptors
Somatic Pain
Damaged hepatocytes
Inc. AST & ALT / SGPT & SGOT
Bile Duct obsttruction
LRUQ Pain
Gallbladder Polyps
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 12/29
LABORATORYLABORATORY
EXAMINATIONSEXAMINATIONS
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 13/29
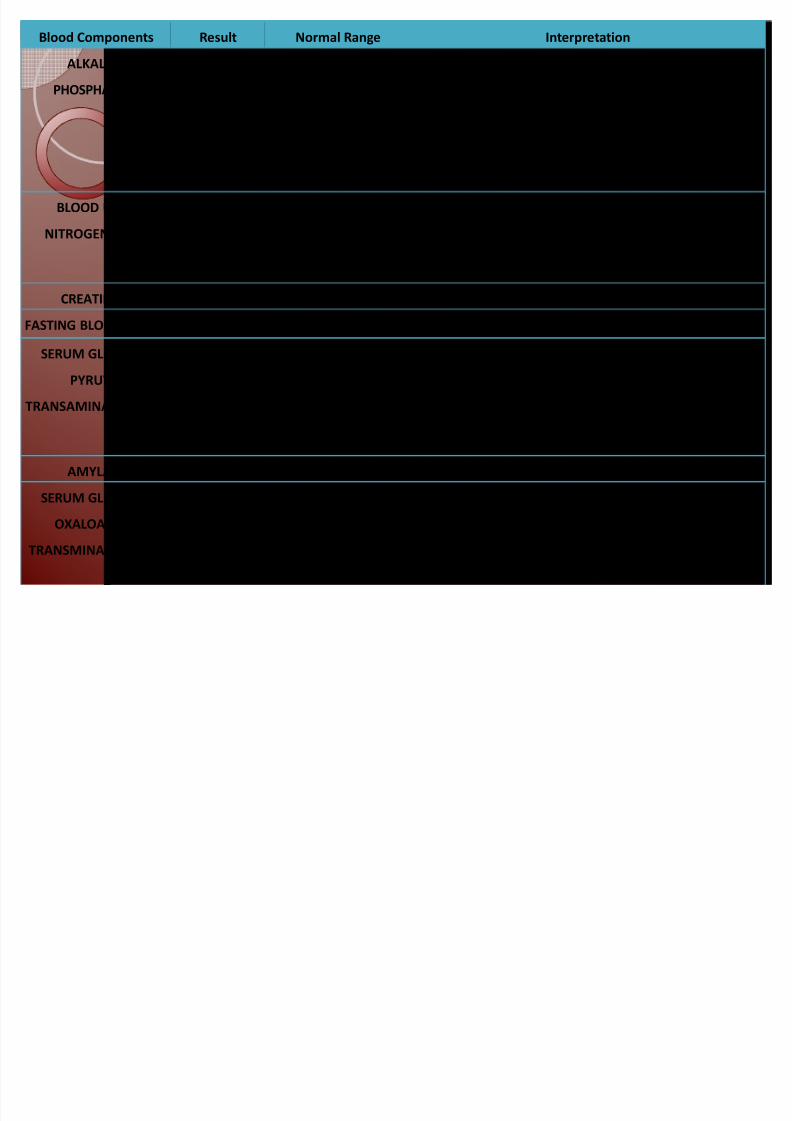
Blood Components Result Normal Range Interpretation
ALKALINE
PHOSPHATASE
156 F: 42-98 µ/L INCREASED
in liver diseases (cholestasis, fatty liver, cholecystitis,
cirrhosis, hepatitis, liver tumor), drug intoxication; drugs
(verapamil, carbamazepine, phenytoin, erythromycin,
allopurinol, ranitidine)
BLOOD UREA
NITROGEN (BUN)
1.4 2.2-7.1 mmol/L DECREASED
in hepatic failure, nephrotic syndrome, cachexia (low
protein and high carbohydrate diets)CREATININE 62 F: 53-97 µmol/L NORMAL
FASTING BLOOD SUGAR 5.0 3.9-5.8 mmol/L NORMAL
SERUM GLUTAMIC
PYRUVIC
TRANSAMINASE (SGPT)
301 F: 3-31µ/L INCREASED
in acute viral hepatitis, diabetes, CHF, liver damage, bile
duct obstructions, infectious mononucleosis, myopathy;
hepatotoxic drug
AMYLASE 69 27-102 µ/L NORMAL
SERUM GLUTAMIC
OXALOACETIC
TRANSMINASE (SGOT)
249 F: 2-31 µ/L INCREASED
in acute viral hepatitis, biliary tract obstraction,
mononucleoisis, alcoholic hepatitis and cirrhosis, liver
abscess, ischemic injury to liver, myopathy
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 14/29
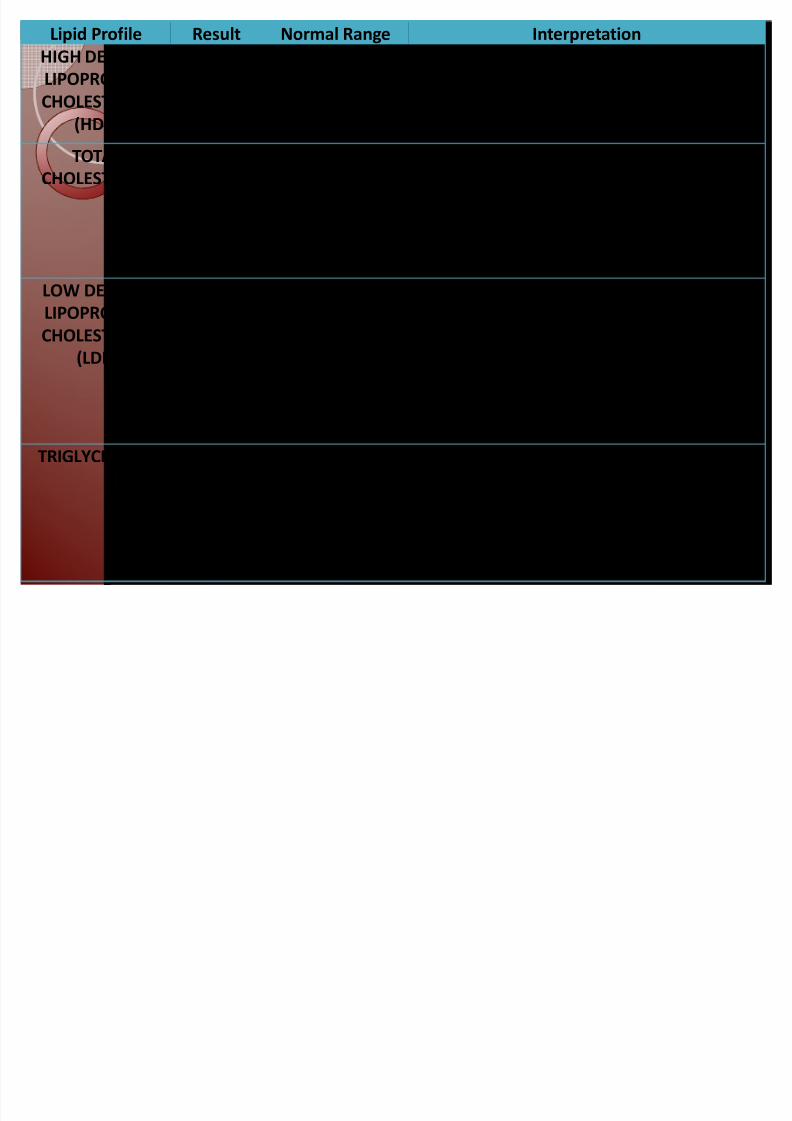
Lipid Profile Result Normal Range Interpretation
HIGH DENSITY
LIPOPROTEIN
CHOLESTEROL
(HDL)
1.36 Low <1.03
Medium 1.03-1.56
High >1.56
MEDIUM / NORMAL
TOTAL
CHOLESTEROL
6.50 Desirable <5.16
Borderline High
5.16-6.17
High >6.18
HIGH
Associated with atherosclerosis, biliary
cirrhosis, high-cholesterol diet,
hypothyroidism, myocardial infarction,
nephritic syndrome, uncontrolled diabetes
LOW DENSITY
LIPOPROTEIN
CHOLESTEROL
(LDL)
4.36 Optimal <2.58
Near/Low Optimal
2.58-3.34
Borderline High
3.35-4.12
High 4.13-4.89
Very High >4.90
HIGH
Connected with heart diseases including
atherosclerosis, heart attack, stroke, and
coronary heart disease
TRIGLYCERIDES 1.72 Normal <1.70
Borderline High
1.70-2.25
High 2.26-5.63
Very High >5.65
BORDERLINE HIGH
Slightly above normal; associated with
cirrhosis, hypothyroidism, low protein in diet
and high carbohydrates, pancreatitis, poorly
controlled diabetes, nephrotic syndrome
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 15/29
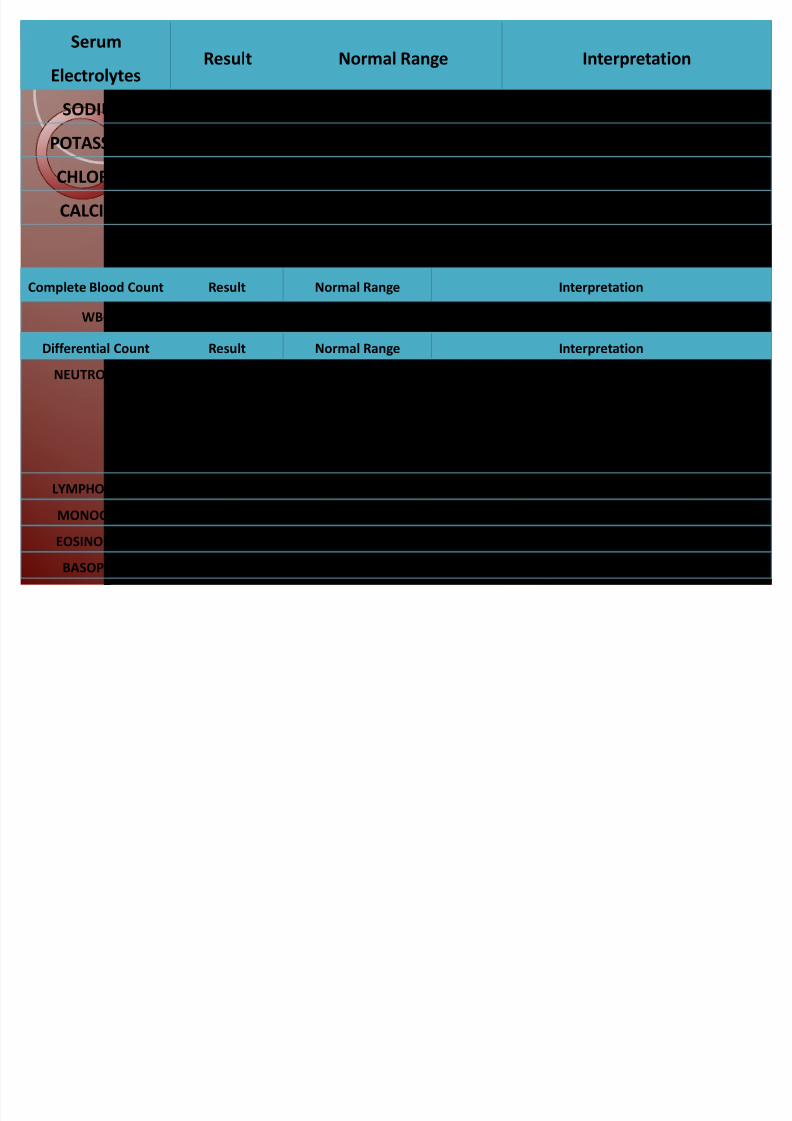
Serum
ElectrolytesResult Normal Range Interpretation
SODIUM 141 138-146 mmol/L NORMAL
POTASSIUM 3.9 3.6-5.0 mmol/L NORMAL
CHLORIDE 101 96-110 mmol/L NORMAL
CALCIUM 1.24 1.15-1.29 mmol/L NORMAL
Complete Blood Count Result Normal Range Interpretation
WBC 9.3 5.0-10.0x10 g/L NORMAL
Differential Count Result Normal Range Interpretation
NEUTROPHILS 0.62 0.40-0.60 INCREASED
in infection (bacterial or early viral), acute stress,
acute and chronic inflammation, tumor, drugs, DKA
LYMPHOCYTES 0.26 0.20-0.40 NORMAL
MONOCYTES 0.08 0.02-0.08 NORMAL
EOSINOPHILS 0.02 0.01-0.03 NORMAL
BASOPHILS 0.02 0-0.02 NORMAL
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 16/29
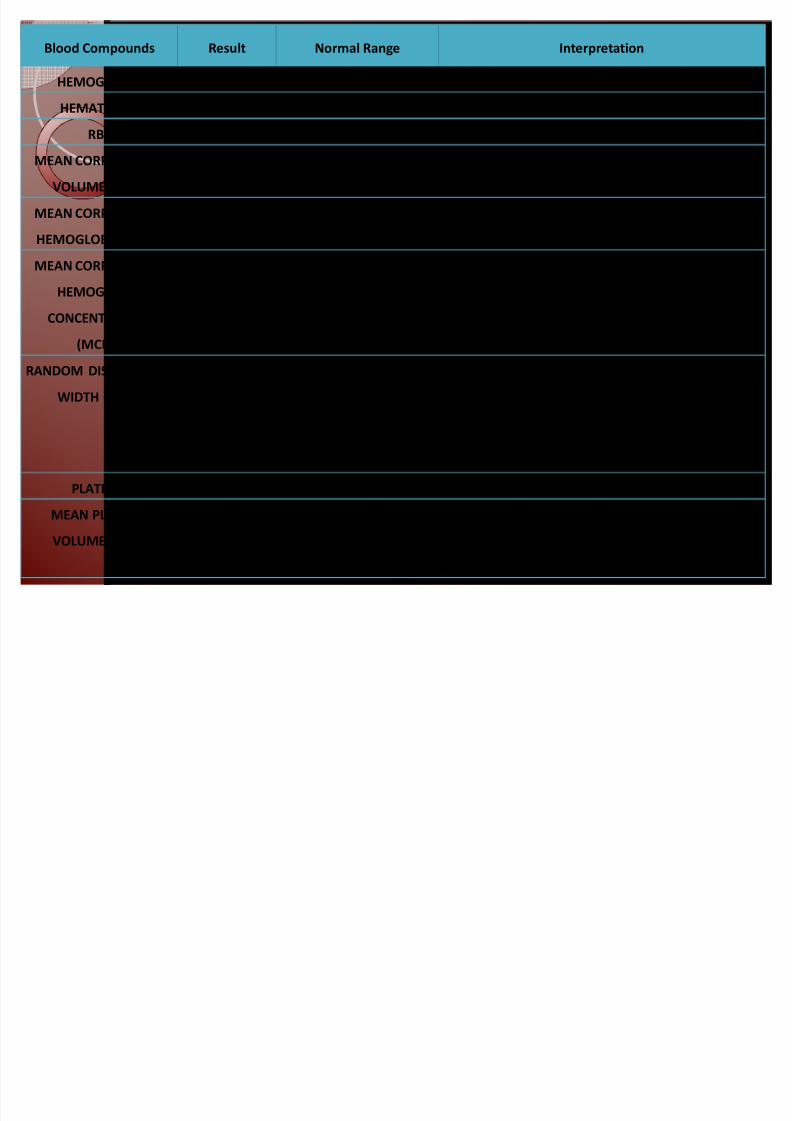
Blood Compounds Result Normal Range Interpretation
HEMOGLOBIN 142 F: 123-152 g/L NORMAL
HEMATOCRIT 0.42 F: 0.37-0.42 NORMAL
RBC 4.88 F: 4.5-5.5x1012
/L NORMALMEAN CORPUSCULAR
VOLUME (MCV)
87 88-96 NORMAL
MEAN CORPUSCULAR
HEMOGLOBIN (MCH)
29.1 27-33 pg NORMAL
MEAN CORPUSCULAR
HEMOGLOBIN
CONCENTRATION
(MCHC)
336 300-360 g/L NORMAL
RANDOM DISTRIBUTION
WIDTH (RDW)
12.5 12.7-22.7% DECREASED
in iron deficiency anemia (blood loss, parasites,poor iron absorption), vitamin B6 anemia, rheumatoid
arthritis
PLATELET 327 150-450x20 g/L NORMAL
MEAN PLATELET
VOLUME (MPV)
4.38 4.5-7.5 fL DECREASED
platelet production problems; thrombocytopenia,
leukemia
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 17/29
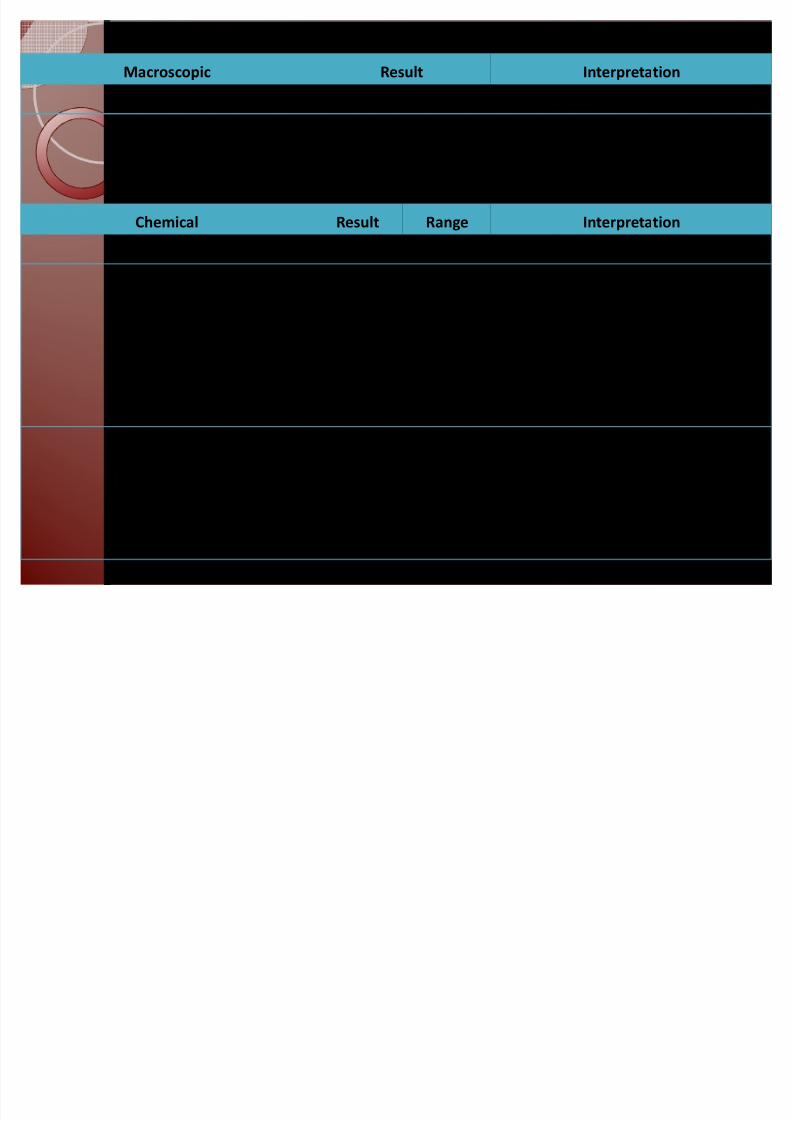
Macroscopic Result Interpretation
COLOR Dark yellow May indicate dehydration
TRANSPARENCY turbid May be a symptom of bacterial infection;
can be caused by crystallization of salts
(calcium phosphate)
Chemical Result Range Interpretation
SPECIFIC GRAVITY 1.010 1.003-1.030 NORMAL
pH 8.5 4.5-8 INCREASED
Alkalinic; kidney failure, UTI, vomiting;
in diet high in citrus, vegetables, dairy;
drugs (acetazolamide, potassium citrate,
sodium bicarbonate)
UROBILINOGEN +2 0.2-1 mg/dL INCREASED
Associated with liver diseases (hepatitis,
cirrhosis), increased RBC destruction
(haemolytic anemia)
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 18/29
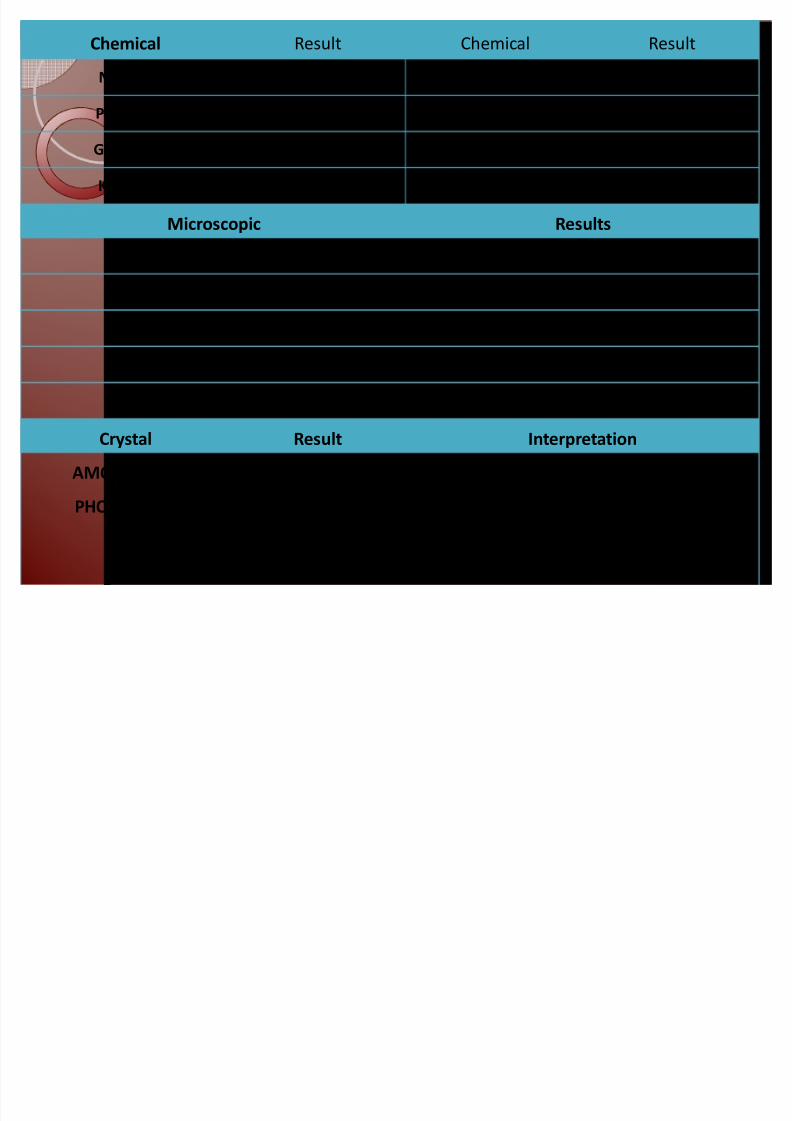
Chemical Result Chemical Result
NITRITE Negative BILIRUBIN Negative
PROTEIN Negative LEUKOCYTES Negative
GLUCOSE Negative BLOOD Negative
KETONE Negative PREGNANCY Negative
Microscopic Results
RBC 0-2 / HPF
PUS CELLS 0-2 / HPF
BACTERIA Few
EPITHELIAL CELLS +1
MUCUS THREADS Few
Crystal Result Interpretation
AMORPHOUS
PHOSPHATES
+1 Present in an alkaline urine; can be caused
by diet (vegetarian, phosphate-rich foods),
or by pathological conditions (UTI, kidney
failure)
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 19/29
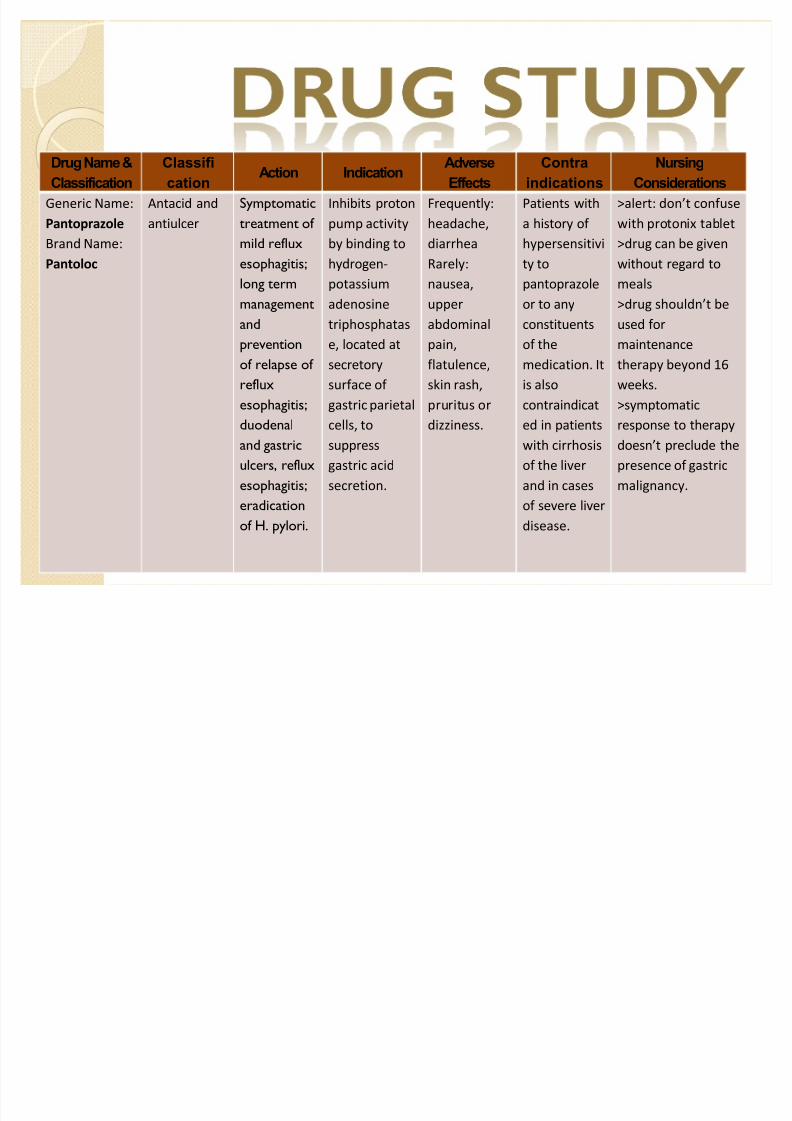
Drug Name &
Classification
Classifi
cationAction Indication
Adverse
Effects
Contra
indications
Nursing
Considerations
Generic Name:
Pantoprazole
Brand Name:
Pantoloc
Antacid and
antiulcer
Symptomatic
treatment of
mild reflux
esophagitis;
long term
management
and
prevention
of relapse of
reflux
esophagitis;
duodenal
and gastric
ulcers, reflux
esophagitis;
eradication
of H. pylori.
Inhibits proton
pump activity
by binding to
hydrogen-
potassium
adenosine
triphosphatas
e, located at
secretory
surface of
gastric parietal
cells, to
suppress
gastric acid
secretion.
Frequently:
headache,
diarrhea
Rarely:
nausea,
upper
abdominal
pain,
flatulence,
skin rash,
pruritus or
dizziness.
Patients with
a history of
hypersensitivi
ty to
pantoprazole
or to any
constituents
of the
medication. It
is also
contraindicat
ed in patients
with cirrhosis
of the liver
and in cases
of severe liver
disease.
>alert: dont confuse
with protonix tablet
>drug can be given
without regard to
meals
>drug shouldnt be
used for
maintenance
therapy beyond 16
weeks.
>symptomatic
response to therapy
doesnt preclude the
presence of gastric
malignancy.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 20/29
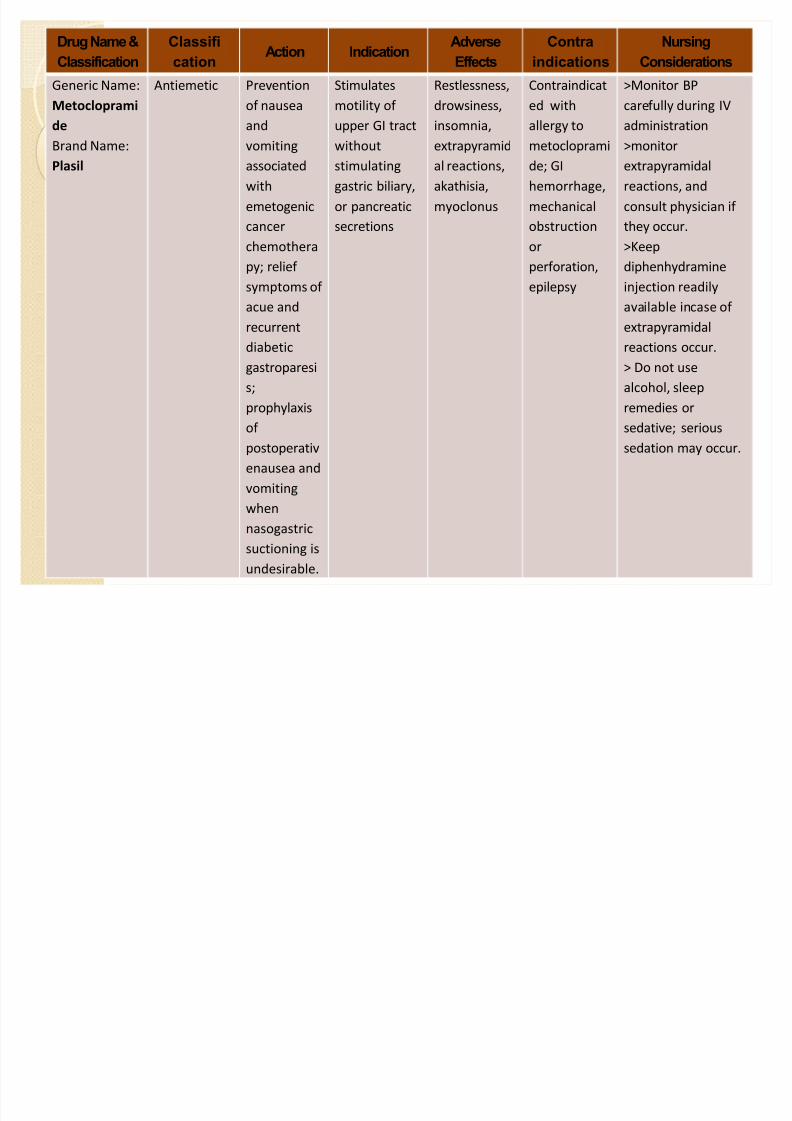
Drug Name &
Classification
Classifi
cationAction Indication
Adverse
Effects
Contra
indications
Nursing
Considerations
Generic Name:
Metocloprami
de
Brand Name:
Plasil
Antiemetic Prevention
of nausea
and
vomiting
associated
with
emetogenic
cancer
chemothera
py; relief
symptoms of
acue and
recurrent
diabetic
gastroparesi
s;
prophylaxis
of
postoperativ
enausea and
vomiting
when
nasogastric
suctioning isundesirable.
Stimulates
motility of
upper GI tract
without
stimulating
gastric biliary,
or pancreatic
secretions
Restlessness,
drowsiness,
insomnia,
extrapyramid
al reactions,
akathisia,
myoclonus
Contraindicat
ed with
allergy to
metocloprami
de; GI
hemorrhage,
mechanical
obstruction
or
perforation,
epilepsy
>Monitor BP
carefully during IV
administration
>monitor
extrapyramidal
reactions, and
consult physician if
they occur.
>Keep
diphenhydramine
injection readily
available incase of
extrapyramidal
reactions occur.
> Do not use
alcohol, sleep
remedies or
sedative; serious
sedation may occur.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 21/29
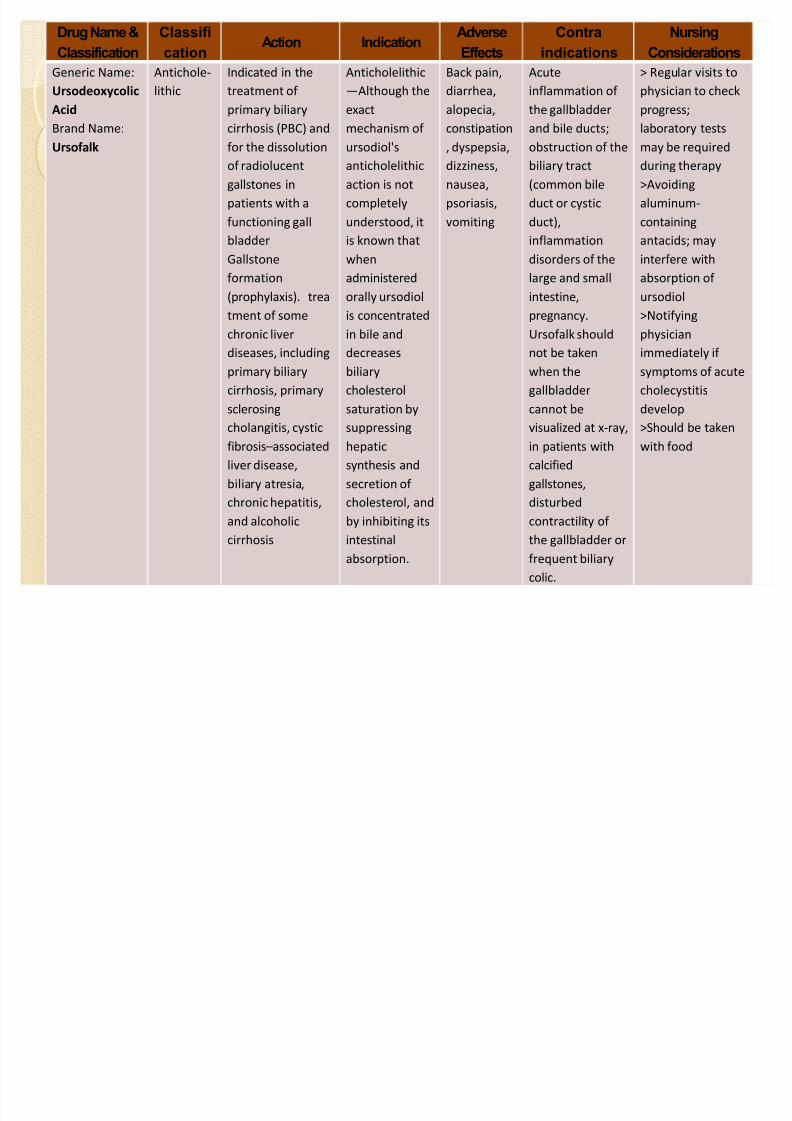
Drug Name &
Classification
Classifi
cationAction Indication
Adverse
Effects
Contra
indications
Nursing
Considerations
Generic Name:
Ursodeoxycolic
Acid
Brand Name:
Ursofalk
Antichole-
lithic
Indicated in the
treatment of
primary biliary
cirrhosis (PBC) and
for the dissolution
of radiolucent
gallstones in
patients with a
functioning gall
bladder
Gallstone
formation(prophylaxis). trea
tment of some
chronic liver
diseases, including
primary biliary
cirrhosis, primary
sclerosing
cholangitis, cystic
fibrosisassociated
liver disease,
biliary atresia,
chronic hepatitis,
and alcoholic
cirrhosis
Anticholelithic
Although the
exact
mechanism of
ursodiol's
anticholelithic
action is not
completely
understood, it
is known that
when
administeredorally ursodiol
is concentrated
in bile and
decreases
biliary
cholesterol
saturation by
suppressing
hepatic
synthesis and
secretion of
cholesterol, and
by inhibiting its
intestinal
absorption.
Back pain,
diarrhea,
alopecia,
constipation
, dyspepsia,
dizziness,
nausea,
psoriasis,
vomiting
Acute
inflammation of
the gallbladder
and bile ducts;
obstruction of the
biliary tract
(common bile
duct or cystic
duct),
inflammation
disorders of the
large and smallintestine,
pregnancy.
Ursofalk should
not be taken
when the
gallbladder
cannot be
visualized at x-ray,
in patients with
calcified
gallstones,
disturbed
contractility of
the gallbladder or
frequent biliary
colic.
> Regular visits to
physician to check
progress;
laboratory tests
may be required
during therapy
>Avoiding
aluminum-
containing
antacids; may
interfere with
absorption of ursodiol
>Notifying
physician
immediately if
symptoms of acute
cholecystitis
develop
>Should be taken
with food
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 22/29
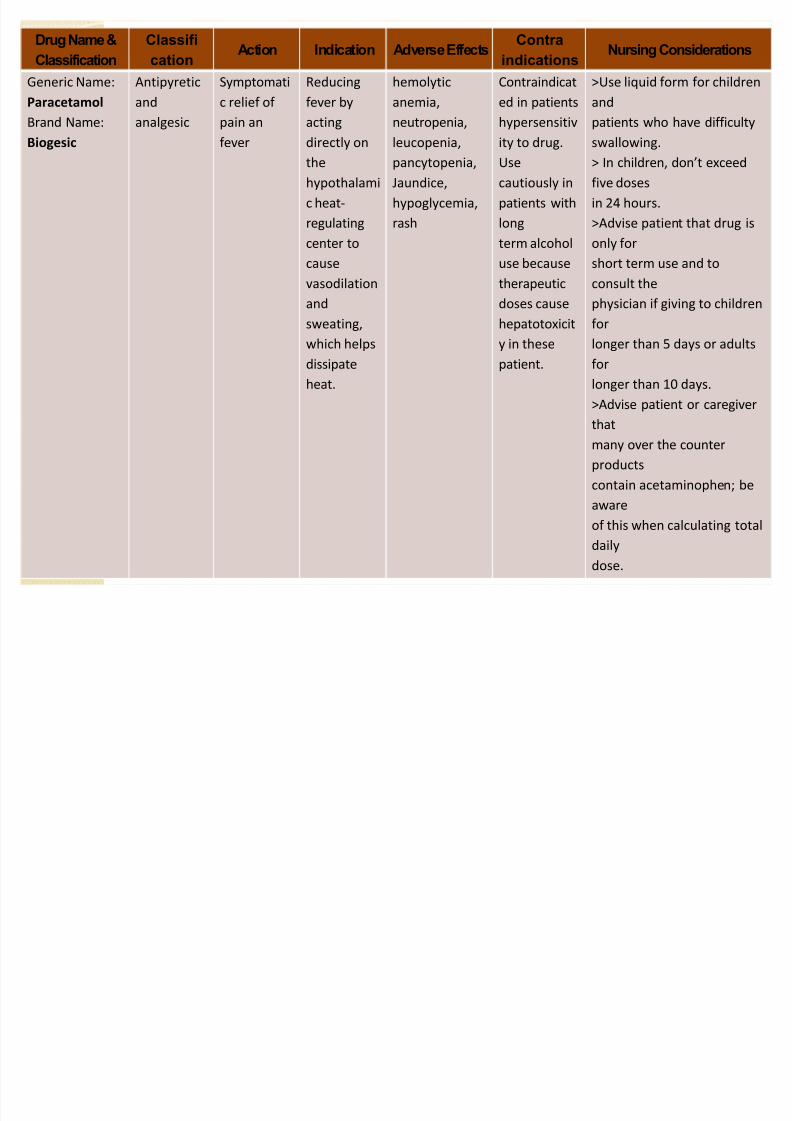
Drug Name &
Classification
Classifi
cationAction Indication Adverse Effects
Contra
indicationsNursing Considerations
Generic Name:
Paracetamol
Brand Name:
Biogesic
Antipyretic
and
analgesic
Symptomati
c relief of
pain an
fever
Reducing
fever by
acting
directly onthe
hypothalami
c heat-
regulating
center to
cause
vasodilation
and
sweating,
which helps
dissipate
heat.
hemolytic
anemia,
neutropenia,
leucopenia,pancytopenia,
Jaundice,
hypoglycemia,
rash
Contraindicat
ed in patients
hypersensitiv
ity to drug.Use
cautiously in
patients with
long
term alcohol
use because
therapeutic
doses cause
hepatotoxicit
y in these
patient.
>Use liquid form for children
and
patients who have difficulty
swallowing.> In children, dont exceed
five doses
in 24 hours.
>Advise patient that drug is
only for
short term use and to
consult the
physician if giving to children
for
longer than 5 days or adults
for
longer than 10 days.
>Advise patient or caregiver
that
many over the counter
products
contain acetaminophen; be
aware
of this when calculating total
daily
dose.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 23/29
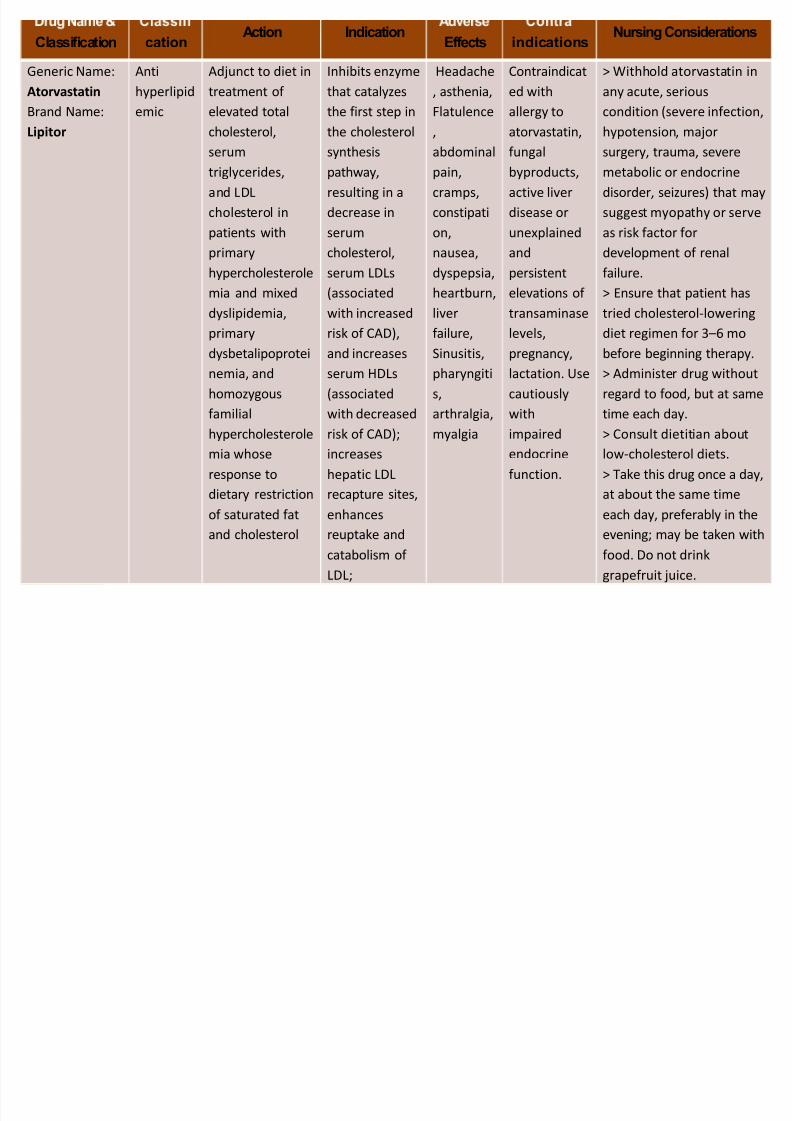
Classification cationAction Indication
Effects indicationsNursing Considerations
Generic Name:
Atorvastatin
Brand Name:
Lipitor
Anti
hyperlipid
emic
Adjunct to diet in
treatment of
elevated total
cholesterol,
serum
triglycerides,
and LDL
cholesterol in
patients with
primary
hypercholesterolemia and mixed
dyslipidemia,
primary
dysbetalipoprotei
nemia, and
homozygous
familialhypercholesterole
mia whose
response to
dietary restriction
of saturated fat
and cholesterol
Inhibits enzyme
that catalyzes
the first step in
the cholesterol
synthesis
pathway,
resulting in a
decrease in
serum
cholesterol,
serum LDLs(associated
with increased
risk of CAD),
and increases
serum HDLs
(associated
with decreasedrisk of CAD);
increases
hepatic LDL
recapture sites,
enhances
reuptake and
catabolism of LDL;
Headache
, asthenia,
Flatulence
,
abdominal
pain,
cramps,
constipati
on,
nausea,
dyspepsia,heartburn,
liver
failure,
Sinusitis,
pharyngiti
s,
arthralgia,myalgia
Contraindicat
ed with
allergy to
atorvastatin,
fungal
byproducts,
active liver
disease or
unexplained
and
persistentelevations of
transaminase
levels,
pregnancy,
lactation. Use
cautiously
withimpaired
endocrine
function.
> Withhold atorvastatin in
any acute, serious
condition (severe infection,
hypotension, major
surgery, trauma, severe
metabolic or endocrine
disorder, seizures) that may
suggest myopathy or serve
as risk factor for
development of renal
failure.> Ensure that patient has
tried cholesterol-lowering
diet regimen for 36 mo
before beginning therapy.
> Administer drug without
regard to food, but at same
time each day.> Consult dietitian about
low-cholesterol diets.
> Take this drug once a day,
at about the same time
each day, preferably in the
evening; may be taken with
food. Do not drinkgrapefruit juice.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 24/29
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 25/29
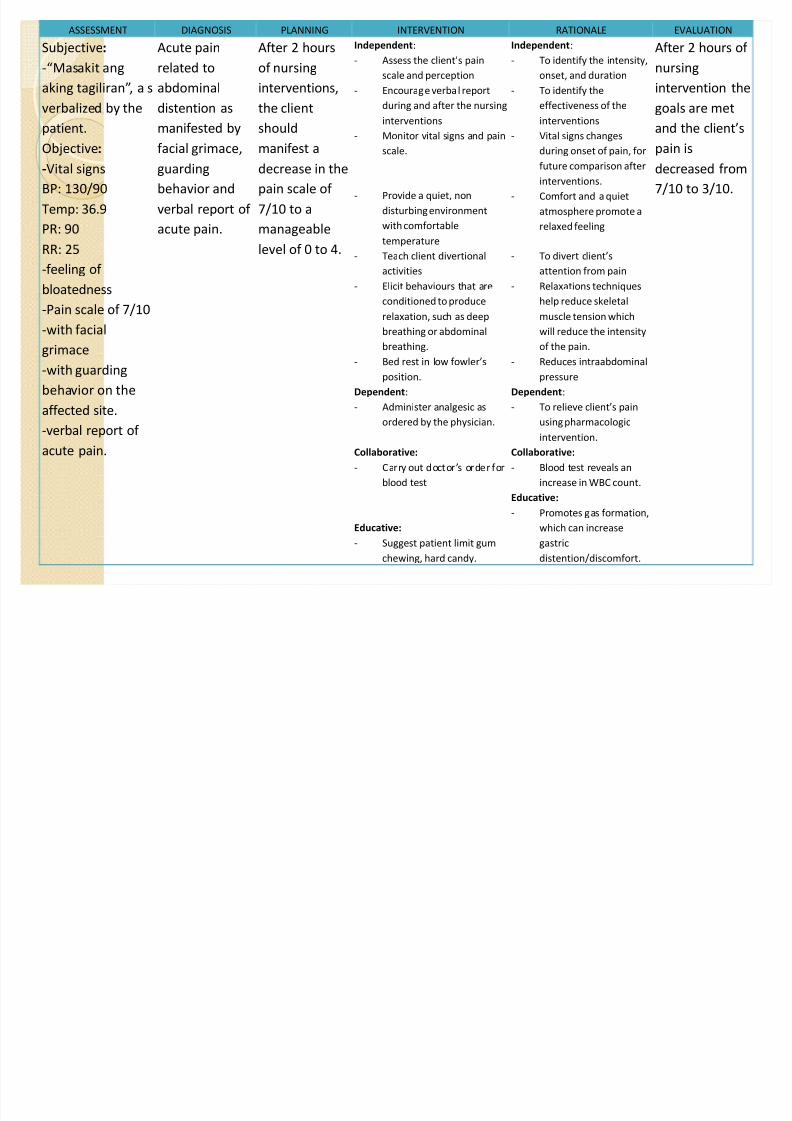
ASSESSMENT DIAGNOSIS PLANNING INTERVENTION RATIONALE EVALUATION
Subjective:
-Masakit ang
aking tagiliran, a s
verbalized by the
patient.
Objective:
-Vital signs
BP: 130/90
Temp: 36.9
PR: 90
RR: 25
-feeling of
bloatedness
-Pain scale of 7/10
-with facial
grimace
-with guarding
behavior on the
affected site.
-verbal report of
acute pain.
Acute pain
related to
abdominal
distention as
manifested by
facial grimace,
guarding
behavior and
verbal report of
acute pain.
After 2 hours
of nursing
interventions,
the client
should
manifest a
decrease in the
pain scale of
7/10 to a
manageable
level of 0 to 4.
Independent:
- Assess the clients pain
scale and perception
- Encourage verbal report
during and after the nursing
interventions
- Monitor vital signs and pain
scale.
- Provide a quiet, non
disturbing environment
with comfortable
temperature
- Teach client divertional
activities
- Elicit behaviours that are
conditioned to produce
relaxation, such as deep
breathing or abdominal
breathing.
- Bed rest in low fowlers
position.
Dependent:
- Administer analgesic as
ordered by the physician.
Collaborative:
- Carry out doctors order for
blood test
Educative:
- Suggest patient limit gum
chewing, hard candy.
Independent:
- To identify the intensity,
onset, and duration
- To identify the
effectiveness of the
interventions
- Vital signs changes
during onset of pain, for
future comparison after
interventions.
- Comfort and a quiet
atmosphere promote a
relaxed feeling
- To divert clients
attention from pain
- Relaxations techniques
help reduce skeletal
muscle tension which
will reduce the intensity
of the pain.
- Reduces intraabdominal
pressure
Dependent:
- To relieve clients pain
using pharmacologic
intervention.
Collaborative:
- Blood test reveals an
increase in WBC count.
Educative:
- Promotes gas formation,
which can increase
gastric
distention/discomfort.
After 2 hours of
nursing
intervention the
goals are met
and the clients
pain is
decreased from
7/10 to 3/10.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 26/29
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 27/29
Be sure the patient understands any medication
prescribed, including names of the drugs, dosage, route,action and side effects.
Advocate the patient to adhere to therapeutic regimens.
Encourage to follow up with his nutritionist regarding his
diet.
Encourage to use of stress management techniques, e.g.,
progressive relaxation, deep-breathing exercises to
promote muscle relaxation and manage any discomfort.
Encourage the patient to routinely exercise digits/joints
distal to injury to enhance circulation.Advocate the patient to report any unusual/sudden pain
or deep, progressive, and poorly localized pain to prevent
further infection/complication.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 28/29
Encourage family members to inform the patient
to attend follow up appointments with his physician.
Advise the patient to have adequate rest and sleep
and to eat a healthy & balanced diet.
Encourage patient to eat high calorie, moderate
protein meal and to have supplementary feedings.Suggest small, frequent feedings and attractive
meals in an aesthetically pleasing setting at meal
time.
Encourage and assist with gradually increasing
periods of exercise.
Provide emotional support to enhance coping
abilities in the management of the stress of injury
and pain.
8/3/2019 FUMC Case Presentation
http://slidepdf.com/reader/full/fumc-case-presentation 29/29