CONTENTS - profaniljain.comprofaniljain.com/pages/pdf2.pdf · CONTENTS - profaniljain.com ......
66
EDITOR SC Goel (Varanasi) ASSOCIATE EDITOR SK Saraf (Varanasi) Sanjay Jain (Jabalpur) EDITORIAL BOARD MEMBERS Rajkumar Amravati, Banglore RC Siwach, Rohtak Rakesh Gupta, Rohtak Sushrut Babhulkar, Nagpur Lalit Maini, New Delhi Anup Khare, Agra RK Kanojia, New Delhi VK Varma, Nagpur ZS Kundu, Rohtak CO-OPTED MEMBERS TK Moitra (Kolkata) AK Jain (New Delhi) S Rajasekaran (Coimbatore) Sanjay Chaturvedi (Agra) GN Khare (Varanasi) A Rastogi (Varanasi) ADVISORY BOARD KT Dholakia (Mumbai) SM Tuli (Delhi) WG Rama Rao (Mumbai) TK Shanmugasundaram (Chennai) DP Baksi (Kolkata) Kamal Bose (Singapore). I NDIAN JOURNAL OF ORTHOPAEDICS CONTENTS Volume 38 : Number 3 July 2004 Editorial Evidence Based Medicine 139 VP Singh Hip Bone grafting for acetabular deficiencies in case of total hip arthoplasty 143 BK Dhaon, Vineet Jain, Jatinder Singla, Anuj Jaiswal, Vishal Nigam Hip arthroplasty following failed dynamic hip screw fixation for 147 per-trochanteric femoral fractures SKS Marya, R Thukral, R Bawari, R Gupta Estimation of femoral neck anteversion in adults – A comparison 151 between preoperative, clinical and biplane X-rays methods AV Maheshwari, AK Jain, MP Singh, SK Bhargava Knee Short and long term results of arthroscopic partial meniscectomy 158 P Sripathi Rao, Sharath K Rao, Shamasunder Bhat N Traumatology Infected nonunions of tibia – management by simple fixator – compressor 162 ZS Kundu, SS Sangwan, Sanjeev Jain, Rajeev Mittal, RC Siwach, Bhardwaj Gaurav Crossed pin fixation in displaced supracondylar humerus fractures in children 166 UB Yadav, R Singhal, G Tonk, T Aggarwal, AN Verma Miscellaneous Coping mechanism and its correlation with quality of life in upper 170 limb post traumatic joint stiffness patients Aditya Aggarwal, Adarsh Kohli, ON Nagi, Arun Kumar Psychological disturbance in Indian low back pain population 175 Ketan C Pande Deep venous thrombosis – A multicentric study 178 S Bhan, BK Dhaon, Yash Gulati, Shkhar Aggarwal
Transcript of CONTENTS - profaniljain.comprofaniljain.com/pages/pdf2.pdf · CONTENTS - profaniljain.com ......

EDITOR
SC Goel (Varanasi)
ASSOCIATE EDITORSK Saraf (Varanasi)Sanjay Jain (Jabalpur)
EDITORIAL BOARD MEMBERSRajkumar Amravati, Banglore
RC Siwach, RohtakRakesh Gupta, RohtakSushrut Babhulkar, Nagpur
Lalit Maini, New DelhiAnup Khare, AgraRK Kanojia, New Delhi
VK Varma, NagpurZS Kundu, Rohtak
CO-OPTED MEMBERSTK Moitra (Kolkata)AK Jain (New Delhi)
S Rajasekaran (Coimbatore)Sanjay Chaturvedi (Agra)GN Khare (Varanasi)
A Rastogi (Varanasi)
ADVISORY BOARDKT Dholakia (Mumbai)
SM Tuli (Delhi)WG Rama Rao (Mumbai)TK Shanmugasundaram (Chennai)DP Baksi (Kolkata)Kamal Bose (Singapore).
INDIAN JOURNAL OFORTHOPAEDICS
CONTENTS
Volume 38 : Number 3July 2004
Editorial
Evidence Based Medicine 139VP Singh
Hip
Bone grafting for acetabular deficiencies in case of total hip arthoplasty 143BK Dhaon, Vineet Jain, Jatinder Singla, Anuj Jaiswal, Vishal Nigam
Hip arthroplasty following failed dynamic hip screw fixation for 147per-trochanteric femoral fractures
SKS Marya, R Thukral, R Bawari, R Gupta
Estimation of femoral neck anteversion in adults – A comparison 151between preoperative, clinical and biplane X-rays methodsAV Maheshwari, AK Jain, MP Singh, SK Bhargava
Knee
Short and long term results of arthroscopic partial meniscectomy 158P Sripathi Rao, Sharath K Rao, Shamasunder Bhat N
Traumatology
Infected nonunions of tibia – management by simple fixator – compressor 162ZS Kundu, SS Sangwan, Sanjeev Jain, Rajeev Mittal, RC Siwach, Bhardwaj Gaurav
Crossed pin fixation in displaced supracondylar humerus fractures in children 166UB Yadav, R Singhal, G Tonk, T Aggarwal, AN Verma
Miscellaneous
Coping mechanism and its correlation with quality of life in upper 170limb post traumatic joint stiffness patientsAditya Aggarwal, Adarsh Kohli, ON Nagi, Arun Kumar
Psychological disturbance in Indian low back pain population 175Ketan C Pande
Deep venous thrombosis – A multicentric study 178S Bhan, BK Dhaon, Yash Gulati, Shkhar Aggarwal

INDIAN JOURNAL OFORTHOPAEDICS
Volume 38 : Number 3July 2004
CONTENTS
Please visit http://www.ijo.ioaindia.org to browse the Journal and for Electronic submission
Case Reports
Osteoid osteoma puzzling presentation & effective and effective management 183S Agarwala, BS Rajput
Desmoplastic fibroma of lumber spine 185MM Prabhakar, Tejas H Thakker
Massive discoid medial meniscus presenting as a meniscal cyst 187Sushil K Sabnis, Anish P Kakadia
Tuberculosis of the patella 189Roop Singh, Rakesh Gupta
Kini Memorial Oration
Principles and practice of deformity correction 191GS Kulkarni
IOA White Paper
Bone grafts and bone substitute in clinical Orthopaedics 199SM Tuli
Published by
Dr. SC Goel
for
Indian OrthopaedicAssociation
from Varanasi
The Journal is published inJanuary, April, July and
October.Subscription price payable in
advance.Inland. Rs. 400 per annum
Rs 125 per copyForeign. $25 per annum
$10 per copy
Indian Journal of Orthopaedicis indexed in Excerpta Medica,
Bibliografia Orthopaedica,Index Medicus SEAR and
Biological abstracts.
iii

“.... I think there is no sense in forming an opinionwhen there is no evidence to form it on. If you build aperson without any bones in him he may look fair enoughto the eye, but he will be limber and cannot stand up; andI consider that evidence are the bones of an opinion”.
Joan of Arc
While we endeavour to improve the quality of healthcare, simultaneously we have been increasingly lamentingover the paucity of solid evidence for most medicalinterventions. As reported in a BMJ editorial, it was observedthat only about 15% of medical interventions are supportedby solid scientific evidence.1
Compounding this fact, are the challenges encounteredin our day to day clinical practice. While caring for patientsmany questions about diagnosis, prognosis and therapy arisethat challenge health professionals to keep up-to-date withmedical literature. It is estimated that the general physicianswho want to keep themselves updated with relevant journalsface the task of examining 19 articles a day, 365 days a year.2
In an era when the so called scientific journals havemushroomed and access through internet is on finger tips,we are confronted by a growing body of information, fewgiving us the useful articles and many producing the junkstuff that is invalid or irrelevant to clinical practice. Oneapproach to meet these challenges and avoid clinical entropyis to learn how to practice evidence based medicine; topractice how to cope with a rapidly changing body of relevantevidence and maximize the quality of medical care despite thereduction in time spent per doctor per patient.
Most good discussions start with definitions. EvidenceBased Medicine (EBM) has been more recently defined as“the integration of best research evidence with clinicalexpertise and patient values”.3
It is a process of turning clinical problems into questionsand then systematically finding, appraising and usingcontemporaneous research findings as the basis for clinical
Editorial
Evidence Based MedicineVP Singh
decisions. It can therefore be used to close the gulf betweengood clinical research and good clinical practice. To stayabreast with the growing scientific advancements, and therapidly changing relevant evidence, the endeavour shouldbe to learn effectively the skill of practicing evidence basedmedicine. The strength of evidence based medicine is that itmoves clinical practice from anecdotal experience and expertopinion to a strong scientific foundation. The elegantrandomized controlled clinical trials, meta analysis, andguidelines have changed the support of our recommendationsfrom “because I said so” towards “because we know so”.
Practicing evidence based medicine
The practice of EBM is a process of self directed learningin which caring for patients leads to the birth of doubts aboutan aspect of clinical diagnosis prognosis or management,therefore creating the need for clinically important informationand its application in the proper situation.
This self directed learning process, for practicing EBMcomprises of five stages.
1. Formulating a clear, focused clinical question from apatient’s problem.
2. Searching the literature for relevant clinical articles, i.e.finding the best evidence.
3. Critically appraise the evidence for its validity (closenessto truth) and usefulness (clinical applicability).
4. Applying the evidence : Integrate the appraisal withclinical expertise and apply the results to clinical practice.
5. Evaluating your performance : “Is my practice evidencebased ?”
Asking (or setting) answerable clinical question
To illustrate how many questions may arise, let usconsider a scenario of a 43 years old active businessman,who has a strong family history of premature heart disease,and presently has no symptoms of coronary disease with anormal electrocardiogram. The individual is normotensive(systolic blood pressure 120 mm Hg), and has never takenlong-term medications for any chronic illnesses. His fastinglipid profile levels reveal total cholesterol of 225 mg perdeciliter, HDL 35 mg per deciliter, triglyceride level of 150 mg
VP Singh, MD, Formerly Professor of Medicine and Director, **Institute of Medical Sciences, BHU, Varanasi.
VOL. 38, NO. 3, JULY 2004 139

INDIAN JOURNAL OF ORTHOPAEDICS140
per deciliter and LDL cholesterol of 160 mg per deciliter. Theperson thought of consulting a physician, after reading anarticle on aspirin’s role in prevention of CAD in a healthmagazine. He wanted to know if he could take aspirin to reducehis risk of coronary events.
Plenty of questions may arise in the treatment of thispatient. Such question that may initiate evidence basedmedicine cover a wide spectrum and may relate to diagnosis,prognosis, treatment, iatrogenic harm or quality of care.4 Giventhis breadth and multitude of questions that may arise, it isimportant to narrow down to the question most interestingto the clinician in perspective of the patient or the questionmost likely to be raised in subsequent patients which couldprovide information for both the clinician and the patient.
In the patient described, two important questions arise.These questions relate to the risks and benefits of offeringlong-term aspirin therapy.
The first question relates to prognosis, “how great is theannual risk of coronary events in a 43 years old man, nonhypertensive non diabetic, non smoker without anyelectrocardiogram abnormality, but with a strong family historyof premature heart disease and an unfavourable lipid profile?”
The other question related to treatment and weighingrisk and benefit, “what is the risk reduction for coronary eventsfrom aspirin therapy in such a patient, and what is the risk ofharming him with a long term therapy ?”
Once the questions are formulated, the next step is tosearch for the best available evidence.
Searching for the evidence
Focused questions sharpen the search for the bestavailable evidence. To conduct searches, clinicians needeffective searching skills and easy access to bibliographicdatabases available both in paper and electronic forms.
Two different types of electronic databases are available.The first is bibliographic type that permits to identify relevantcitations in the clinical literature. Such citations may beextracted from MEDLINE resources. The NLM (NationalLibrary of Medicine) allows access into PUBMED, which canbe used for bibliographic citations. (http://www.nlm.nih.gov).The second sort of database, helps the user in retrieving thevarious primary or secondary publications of the relevantclinical evidence which may be in the form of meta analysis,systematic reviews and practice guidelines, that may beobtained from the internet. The Cochrane library on compactdisk, provides one of the most rigorous of systematic reviewson effects of health care that have been genrated by the
Cochrane collaborations.5 Some evidence-based materialsfrom this collaboration appear on internet(www.cochrane.org.). Various evidence based medicinejournals appear on the internet, and some offer the full textmaterial on the web, such as the evidence based medicinejournal published by the BMJ group (http://www.evidence-basedmedicine.com), ACP journal club published from thehome page of American College of Physicians (http://www.acponline.org.), and from the pages of American MedicalAssociation (http://www.ama-assn.org) etc.6 Guideline basedon evidences, controlled trials and expert consensus may beobtained from various web sites like www.guideline.gov.
Several comprehensive search systems index vastproportions of the web such as Google (http:/ /www.google.com), Lycos (http://www.lycos.com) and Yahoo(http://www.yahoo.com). However these do not discriminatebetween clinical and non clinical information or between apersonal web page and that of a prestigious journal or medicalcenter. Therefore, the more clinically focused web pagesshould be screened through. For this patient, the searchesmay be conducted with MEDLINE and internet, in variousoptions.
The major heading may be looked for by searching thesoftware by entering “primary prevention of coronary arterydisease” and “aspirin” as subjects and “randomized controlledtrial” as a publication type. The search may be further refinedby entering “review” or “meta analysis” as publication typeto further narrow the search.
While it is always easy to obtain a quick-reference guidefrom meta analyais or reviews, the ability to critically appraisepublications of all types will remain an invaluable skill.
Critically appraising the evidence
The central tenet of evidence based medicine is that thetask is achieved by using the best evidence combined withconsideration of the patients individuals needs ? Thequestion therefore arises : “what is the best evidence”.
The third step in EBM is to evaluate or appraise theevidence for its validity (closeness to the truth) andusefulness (clinical applicability). This is important, becauseit lets the clinician decide, whether the article retrieved, canbe relied on to give useful guidance.
Mastering critical appraisal entails learning how to ask afew questions about the validity of the evidence and itsrelevance to a particular patient or group of patients.
EVIDENCE BASED MEDICINE

VOL. 38, NO. 3, JULY 2004 141
In this patient, a typical set of critical appraisal questionsarise of evaluating articles about treatment.
1. Are the results valid ?
• was the assignment of patients to treatmentrandomized
• Were the groups similar at the start of the trail ?
• Was blinding to treatment done ?
• Apart from experimental intervention were the
groups treated equally
2. What was the result ?
• How precise was the treatment effect, and was it
statistically significant ?
3. The applicability of the result to my patient
• Were all clinically important outcomes considered.
• Are the likely benefits worth the potential harms
and costs ?
The considerations for “Which clinical studies providethe best evidence”, have supported a hierarchy of evidencewith randomized controlled trials and derivatives at the top,controlled observational studies in the middle anduncontrolled studies and opinions at the bottom. The best touse in decision making, is the evidence highest in hierarchy.Evidence from a lower level should be used only if there is nogood randomized controlled trial to answer a particular clinicalquestion. However the clinician must use his critical appraisalskill not as a rule of thumb as per the aforementionedhierarchy, but to find the best of the articles obtained. In thisregard ‘small inadequate randomized controlled trials do notautomatically trump any conflicting observational studies’8 .However if high quality randomized controlled trials exist fora clinical question, then they trump any number ofobservational studies.
The evidence sought may not automatically dictatepatient care, but will provide the factual basis on whichdecisions can be made taking all aspects of patient care intoconsideration.
Applying the evidence to individual patients
This is the most important act. It is about integration ofevidence with clinical expertise, and knowledge of the uniquefeatures of patients and their situations, rights andexpectations. Patients preference and actions should be takeninto account because they may have either ‘no views’ or‘unshakable views’ on their treatment options.
Evidence should be personalized. In this case annualrisk of coronary artery events has to be specified, since itwould depend on individual characteristics and various riskfactors i.e. age, hypertension, smoking, lipid abnormalitiesand lifestyles etc.
Moreover the risk of long term aspirin therapy has to bespecified too, for the major risk of bleeding episodes variesas per the individual characteristics i.e. age, history of bleedingdiathesis, active peptic ulcer disease, or presence of any co-morbid conditions.
In the case of this non diabetic patient, the absolute riskof coronary events could be calculated by a scoring systemdescribed from the Framingham heart study (the scoringsystem encompassed variables of age, sex, status as smoker,total cholesterol, HDL cholesterol and systolic bloodpressure).9,10
A recent metaanalysis revealed that when the five yearabsolute risk of coronary events reached 5%, aspirin treatmentreduced the absolute risk of coronary event by 0.3% perstroke, but increased the risk of hemorrhagic stroke by 0.02%per year and the risk of major gastrointestinal bleeding by0.06% per year.11 However, if the five year absolute risk ofcoronary events was only 1%, aspirin treatment resulted in areduction of only 0.06% per year in the absolute risk.
The U.S. Preventive Services Task Force, supported theuse of aspirin for the primary prevention of coronary diseasein patients whose five year risk of disease was estimated tobe 3% or higher.11,12
For the patient described, the risk of acute coronary eventmay appear high, in perspective of the strong family historyand an unfavorable lipid profile, yet the calculated 5 yearabsolute risk of disease was less than 3%. It would thereforebe prudent to withhold aspirin, because the absolute benefitof aspirin use in this case being low was weighed out againstthe risk of major bleeding from long term aspirin use. Howeverthe absolute risk should be reassessed every 3-5 years.
Accordingly, the decision of whether to treat theindividual patient has to be weighed for risk against benefits;preferably with the help of hard data of evidence. Theapplicability of evidence would depend upon the integrationof best research evidence with patient values, clinicalcircumstances and clinical expertise.
Evaluating your performance
Evaluating ones own performance is the final step in thefive stage process of traditional evidence based practice. Atthe end of each cycle it should be asked :
VP SINGH

INDIAN JOURNAL OF ORTHOPAEDICS142
• Whether focused answerable questions were
formulated.
• If good evidence was found quickly. “Do I need to
improve my database access ?
• If evidence was effectively appraised.
• Whether the integration of evidence appraisal withclinical expertise and patient’s unique features ledto a rational and acceptable management strategy
This step of self-evaluation will allow to focus on earliersteps that may need improvement in the future.
Foot note
Often the evidence based answers to may questions arenot clear, thus being branded as “incomplete evidence”. Inour quest for scientific advancements and obtaining harddata, these unknown answers should not be correlated as“no”. If there are no trials carried out for our patient’spredicament, we must follow the trail to the next best externalevidence and work from there.
EBM is not the final description or dictation. Neverthelessthis relatively young discipline, whose positive impacts arejust beginning to be validated, should be prescriptive andact as a guide for thinking about how decisions should bemade.3 Clinical expertise and best available evidence shouldwork together. Without clinical expertise, even excellentexternal evidence may be inapplicable for an individual patient;and without current best evidence. practice become rapidlyout of date, to the detriment of patients.
In the present era where geographical difference persistsfor many diseases, we feel that it will be worthwhile toconstitute small size expert groups separately for variousimportant clinical conditions prevailing in our country, whomay carry out the exercise of retrieving various concernedstudies and do the systemic reviews based on the evidencesdrawn plus their own long standing clinical experiences, andthen decide about the management policies. The outcome ofthis expert group exercise then may be published anddisseminated in a journal identified to report these guidelinesfor practice management.
Lastly, as laid down in the famous incompletenesstheorem of Goldel, ‘that for any suitably complex system ofreasoning there exists truths that are not provable from within
the system; to prove these truths one has to step outside thesystem’, probably holds time for our profession too. Perhapsthis is what clinicians do when applying clinicalcommonsense, and providing care, comfort, compassion andhope to patients’lives. This is what make medicine an art aswell as science. The art should be practiced, rational scienceshould be understood and the growing body of evidencesshould be embraced.
“This is what learning is. You suddenly understandsomething you have understood all your life; But in a newway”.
Dorris Lessing
References
1. Simth R, Where is the wisdom……? the poverty of medical evidence.BMJ 1991; 303: 798-99.
2. Davidoff F, Haybes RB, Sackett DL, Smith R. Evidence based medi-cine: a new journal to help doctors identify the information they need.BMJ 1995; 310: 1085-1086.
3. Clinical expertise in the era of evidence-based medicine and patientchoice. EBM (www.evidenebasedmedicine.com) 2002; 7: 36-38.
4. Rosenberg W, Donald A. Evidence based medicine: an approach toclinical problem-solving. BMJ 1995; 310: 1122-1126.
5. Godlee F. The Cochrane Collaboration, BMJ 1994; 309: 969-70.
6. Evidence based medicine and the internet. ACP Journal Club, 1996July-Aug; 125:A14 (extracted from http://www.acpjc.org/Content/125/1/ISSUE/ACPJC-1996-125-1-A14.htm).
7. Sackett DI, Rosenberg WMC, Gray JAM, Haynes RB, RichardsonWS. Evidence based medicine: what it is and what it isn’t. BMJ 1996;312: 71-72.
8. Barton S. Which clinical studies provide the best evidence ? BMJ 2000;255-256.
9. D’ Agostino RB Sr, Grundy S, Sullivan LM, Wilson P. Validation ofthe Framingham coronary heart disease prediction scores: results of amultiple ethnic groups investigation. JAMA 2001; 286: 180-7.
10. Wilson W, D’ Agostino RB, Levy D, Belanger AM, Silbershatz H,Kannal WB. Prediction of coronary heart disease using risk factorcategories. Circulation 1998; 97: 1937-47.
11. Hayden M, Pigone M, Philips C. Aspirin for the primary prevention ofcardiovascular events: a summary of the evidence for the U.S. Preven-tive Services Task Force. Ann Intern Med. 2002; 136: 161-72.
12. Preventive Services Task Force. Aspirin for the primary prevention ofcardiovascular events: recommendation and rationale. Ann Intern Med.2002; 136: 157-60.
EVIDENCE BASED MEDICINE

Background: Bone-graft is among the most popular methods ofproviding bony support in cases of acetabular bony deficienciesduring total hip arthroplasty. Controversy still exists on the bestmethod for bony reconstruction.Methods: Twenty patients having acetabular deficiency wereoperated from 1998 to 2002 for total hip arthroplasty using bonecement, allograft or autograft. There were 14 males and 6 femalesin the study with an average age of 47 years. Average time offollow up was 3.2 years.Results: There was delayed union in one case each of allograftand autograft. Average Harris hip score pre-operatively was 39.5,which improved to an average of 80 post-operatively.Conclusion: Our study has shown that bone grafting both inform of autograft and allograft, provide excellent results inreconstruction of acetabular bony deficiencies. Graft should notsupport more than 50% of acetabular cup. Also, bone cementcan be good option in cases of mild cavitatory lesion in old patients.Key-words: Revision total hip arthroplasty; Bone graft total hiparthroplasty; Acetabular reconstruction.
Introduction
Acetabular bony deficiencies during total hiparthroplasty often present a surgical dilemma. Acetabulardeficiencies encountered can be primarily in form of protrusioacetabuli or secondary deficiency due to failedhemiarthroplasty or primary total hip arthroplasty. Variousmethods have been described to restore bony support forsuccessful total hip arthroplasty. They vary from cement1,autogenous graft, allograft 2 and metal devices3. Autograft
Bone grafting for acetabular deficiencies in cases of totalhip arthroplastyBK Dhaon, Vineet Jain, Jatinder Singla, Anuj Jaiswal, Vishal Nigam
Maulana Azad Medical College and associated LN Hospital, New Delhi.
BK Dhaon, Dean, Director Professor and Head of Department.Vineet Jain, Post Graduate.Jatinder Singla, Post Graduate.Anuj Jaiswal, Senior Resident.Vishal Nigam, Senior Resident.Maulana Azad Medical College and associated LN Hospital, N. Delhi.Prof. BK Dhaon, House No. 11, Type VI, Maulana Azad Medical CollegeCampus, Bahadur Shah Zafar Marg, New Delhi – 110002. E-mail:[email protected] **
and allograft in the form of structural or morselised bonegraft are one of the most preferred methods of providingbony support. We conducted a study at our center to studythe results of bony reconstruction for acetabular deficienciesusing bone cement, autograft, allograft or both.
Materials and Methods
Twenty patients having acetabular deficiency / protrusioacetabuli were operated from 1998 to 2002 for total hiparthroplasty using bone cement, allograft or autograft.Acetabular bony defects were classified according to AAOSclassification4:
Type 1: Segmental, significant rim deficiency.
Type 2: Cavitatory defect usually medial / posterior.
Type 3: Combined defect.
Type 4: Pelvic discontinuity.
Type 5: Arthrodesis.
In case of Type 1 defect segmental bone grafts wereused, they were fixed with two cancellous screws. In case ofType 2 defect, only bone cement was used in patients morethan 60 years old with poor bone stock, while in a youngerpatients morselised bone graft was used. In cases of Type 3defects rim was usually supplemented with segmental graftwhile cavitatory lesion was filled with either bone cement orbone graft as described earlier for type 2 defects. In cases ofType 4 and Type 5 defects whole acetabular bone graft wasused for reconstruction. Autograft in the form of excisedfemoral head alone was used in patients where it was sufficientto reconstruct the acetabulum while it was combined withallograft in cases where autograft alone was insufficient inthe reconstruction of bony defect. Allograft was used in casesof revision total hip arthroplasty. Grafts were made into slurry,put in acetabular defect and then molded with reverseacetabular reamer. No metallic support was used. All thepatients were assessed preoperatively and postoperativelyclinically using Harris Hip score.
The source of allograft was femoral heads harvested fromprevious cases of total hip arthroplasty and hemiarthroplasty.
VOL. 38, NO. 3, JULY 2004 143
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3: P. 143-146

INDIAN JOURNAL OF ORTHOPAEDICS144
Allografts used were preserved at minus 70oC at the collegebone bank. They were thawed at room temperature usingnormal saline in the operation theatre. Allografts used wereat least 3 weeks old and were taken from patient testednegative for HIV, Hepatitis B and C.
Each patient was assessed during follow-up at 6 weeks,3 months, 6 months and then yearly for evidence ofincorporation of bone graft, as shown by continuity oftrabeculae across the graft and acetabulum. Any evidence ofprogressive loosening of acetabular component was assessedusing technique of DeLee and Charnley in cases of cementedcups5.
Patients were allowed non weight bearing crutch walkingafter 6 weeks and toe touch walking when there was somesign of incorporation of bone graft. Patients were allowedfull weight bearing only on radiological evidence of completeincorporation of the graft.
Results
There were 14 males and 6 females in the study with anaverage age of 47 years. Four cases were having revisionarthroplasty (Table I). Twelve defects were type 2, five type1, two type 3 and one case was having acetabular defect type4. Table II shows various methods used to fill defect.
Table I: Diagnosis of the patients undergoing acetabular reconstruction.Diagnosis Cases
1. Avascular necrosis 82. Ankylosing spondylitis 43. Failed hemiarthroplasty 44. Revision total hip replacement 4
TOTAL 20
Average time for incorporation of autograft was 6 monthswhile that of allograft was 9 months. Segmental graft was
used in seven cases. Partial resorption of segmental graftwas seen in four cases. There was delayed union in one caseeach of allograft and autograft. Longest duration of followup was 5 years with an average of 3.2 years.
Table II: Methods of acetabular reconstruction and results.Method Cases Union Delayed Union
1. Cement 6 62. Autograft 8 7 13. Allograft 4 3 14. Autograft +Allograft 2 2
TOTAL 20 18 2
Among five cases of Type 1 defect where segmental bonegraft was used, partial resorption of graft was seen in threecases. Out of 12 cases of Type 2 defect, bone cement wasused in six cases while morselised bone graft was used in sixcases (Fig. 1). Non-progressive lucency at bone cementinterface was seen in two cases. Bone graft united in all cases.In one case of type 3 defects there was delayed union ofallograft. Patient had undergone revision total hip arthroplastyand whole acetabular allograft was used with morselised andsegmental bone graft. Patient had dislocation, 4 months aftersurgery, due to loosening of acetabular component. Patientagain underwent revision surgery when additional allograftwas used which incorporated (Fig. 2). In one case of type 4defect, a patient of rheumatoid arthritis, total acetabular bonegrafting with morselised bone allograft was done. No metalsupport was used. Patient presented one year after undergoingtotal hip arthroplasty with complaint of mild pain in theoperated hip. X-rays of the patient revealed medial superiormigration of the implant. Patient was advised revision, whichthe patient refused in view of insignificant disability.
There was no case of infection. Average Harris hip scorepre-operatively was 39.5, which improved post-operativelyto an average of 80.
BONE GRAFTING FOR ACETABULAR DEFICIENCIES IN CASES OF TOTAL HIP ARTHROPLASTY
Fig 1 (a). Antero-posterior radiograph of a case of type 2 defect; (b) immediately post-operatively after autogenic and allogenic bonegrafting; (c) full incorporation of bone graft 3 months post-operatively.
(a) (b) (c)

VOL. 38, NO. 3, JULY 2004 145
Discussion
Successful total hip arthroplasty requires satisfactoryprosthetic replacement of both the acetabular and femoralsides of the joint. The reconstruction methods should bedirected to replace loss of bone, to repair the hip biomechanicsto normal, and to obtain stability. Emerson et al6 in 1989reported only two cases of partial graft resorption in 46 hipswith press fit cups, on average follow-up of 22 months. Theyalso concluded that initial success of allograft reconstructiondepends upon stable fixation.
Jasty and Harris, in an earlier report advocated use ofbulk graft7 but after a 10-year review they have condemnedthe use of bulk grafts reporting failure rate of 47%8. Paproskyet al9 reported 100% graft union and no acetabular looseningin 147 revision cases with 5.7 years follow up. Garbuz et al10,while using segmental allograft reported graft union in 97%cases with only 10% acetabular loosening or failure. Gross etal11 reported only 5% acetabular loosening after 5 to 12 yearsin 56 patients.
There were six cases of Type 2 defect (protrusio acetabuli)in which morselised bone graft was used. Bone graft wasincorporated in all the cases. Gates et al12 in review of casesof protrusio acetabuli reconstructed with bone grafting at12.8 years follow up concluded that bone grafting is effectivein arrest of progression of protrusio acetabuli in most hips.Sloff et al13 and Kinzinger et al14 also reported good resultswith bone grafting for protrusio acetabuli.
There were two cases of type 3 defect in whom combinedmorselised bone graft and segmental graft was used. In onecase there was delayed union and dislocation secondary to
acetabular loosening, requiring a revision surgery. Knight etal15 reported 100% graft union and acetabular failure in 21%cases. Hooten et al16 reported 44% loosening of acetabularcup on 4 year follow up. Loosening was more if graftsupported more than 50% of cup. Paprosky et al17 in 1996reported acetabular graft failure in only 2 of 10 cases wherewhole acetabular graft was used.
In our series acetabular loosening was seen in one caseof type 3 and one case of type 4 defect. In both the caseswhole acetabular allograft was used, without metal support.Most studies indicate that an allograft that supports morethan 50% of an uncemented cup is associated with higherrate of failure17-19. Cemented cups with reinforcement ringsare now recommended in cases were graft contact area isgreater than 50%7,8,14,16, 20.
Bone graft both in form of autograft and allograft provideexcellent results in reconstruction of acetabular bonydeficiencies. Graft should not support more than 50% ofacetabular cup. Probably some metallic support implantshould be used in cases of severe acetabular bony deficiency.Also, bone cement can be good option in cases of mildcavitatory lesion in old patients.
References
1. Slooff TJ, Schimmel JW, Buma P. Cemented fixation with bone grafts.Orthop Clin North Am. 1993;24:667-676.
2. Tanzer M, Drucker D, Jasty M et al. Revision of the acetabularcomponent with an uncemented Harris Galante porous-coated cup. JBone Joint Surg (Am). 1992;74:987-994.
3. Berry DJ, Muller ME. Revision arthroplasty using an anti-protrusiocage for massive acetabular bone deficiency. J Bone Joint Surg (Br).1992;74:711-715.
BK DHAON, VINEET JAIN, JATINDER SINGLA, ANUJ JAISWAL, VISHAL NIGAM
Fig 2 (a). Antero-posterior radiograph of type 3 defect in a case of revision total hip arthroplasty; (b). Post-operative dislocation afterallogenic segmental and morselised bone grafting; (c). After reduction and additional bone grafting with incorporation of allograft.
(a) (b) (c)

INDIAN JOURNAL OF ORTHOPAEDICS146
4. D Antonio JA, Capello WN, Borden LS, et al. Classification andmanagement of acetabular abnormalities in total hip arthroplasty. ClinOrthop. 1989;243:126-137.
5. Delee JD, Charnley J. Radiological demarcation of cemented socketsin total hip replacement. Clin Orthop. 1976;121:20-32.
6. Emerson RH, Head WC, Berklacich FM, Malinin TL. Noncementedacetabular revision arthroplasty using bone allograft. Clin Orthop.1989;249:30-43.
7. Jasty MJ, Harris WH. Total hip reconstruction using frozen femoralhead allografts in patients with acetabular bone loss. Orthop Clin NorthAm. 1987;18:291-299.
8. Kwong LM, Jasty MJ, Harris WH. High failure rate of bulk femoralhead allografts in total hip acetabular reconstructions at 10 years. JArtroplasty.1993;8:341-346.
9. Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classifi-cation and surgical reconstruction in revision arthroplasty: A 6- yearfollow up evaluation. J Arthroplasty. 1994;9:33-44.
10. Garbuz DS, Morsi E, Mohamed N, et al. Classification and recon-struction in revision acetabular arthroplasty with bone stock deficiency.Clin Orthop. 1996;324:98-107.
11. Gross AE, Garbuz DS, Morsi ES. Acetabular allografts for restorationof bone stock in revision arthroplasty of the hip. Instruc Course Lect.1996;45:135-142.
12. Gates HS, McCollum MD, Poletti SC, Nunley JA. Bone grafting intotal hip arthroplasty for protrusio acetabuli – A follow up note. J BoneJoint Surg (Am). 1990; 72:248-251.
13. Slooff TJJH, Huiskes R, Horn JV, Lemmens AJ. Bone grafting intotal hip replacement for acetabular protrusion. Acta OrthopScand.1984;55(6):593-596.
14. Kinzinger PJM, Karthaus RP, Sloff TJJH. Bone grafting for acetabu-lar protrusion in total hip arthroplasty. Acta Orthop Scand.1991;62:110-112.
15. Knight JL, Fujii K, Atwater R et al. Bone-grafting for acetabulardeficiency during primary and revision total hip arthroplasty: A radio-graphic and clinical analysis. J Arthroplasty.1993;8:371-382.
16. Hooten JP, Engh CA Jr, Engh CA. Failure of stuctural acetabularallografts in cementless revision hip arthroplasty. J Bone Joint Surg(Am). 1994;76:419-422.
17. Paprosky WG, Bradford MS, Jablonsky WS. Acetabular reconstruc-tion with massive acetabular allografts. Instruc Course Lect.1996;45:149-159.
18. Zmolek JC, Dorr LD. Revision total hip arthroplasty. The use of solidallograft. J Arthroplasty. 1993;8:361-370.
19. Young SK, Dorr LD, Kaufman RL, et al. Factors related to failure ofstructural bone grafts in acetabular reconstruction of total hip arthro-plasty. J Arthroplasty. 1991;6s:73-82.
20. Chandler HP. Structural grafting of the acetabulum. Orthopedics.1995;18:863-864.
BONE GRAFTING FOR ACETABULAR DEFICIENCIES IN CASES OF TOTAL HIP ARTHROPLASTY

Background: Unstable trochanteric fractures have a pooroutcome in patients in whom fixation fails and revision to a totalhip arthroplasty is required. The primary indication for secondarysurgery is relief of pain.Method: A retrospective review was performed on 17 patientswith hip arthroplasty following failure of dynamic hip screw fixationdone for per-trochanteric femoral fractures. Three patientsunderwent bipolar hip arthroplasty and total hip replacement inthe remaining fourteen.Results: Clinical and radiological results at final follow up wereequally good following bipolar or total hip arthroplasty conversions.Extreme care needs to be taken to avoid fracture and penetrationof the femoral shaft. Auto graft, allograft or head and neckreplacement components should be made available forreconstruction of difficult cases.Conclusion: The principles of a successful outcome includepreservation of the functional continuity of the abduction apparatusduring surgery, and early supervised weight bearing.Key-words: Failed fixation; Trochanteric fracture; Revision; Hiparthroplasty
Introduction
Closed reduction and internal fixation is the preferredinitial treatment for young active patients who sustain adisplaced pertrochanteric hip fracture1 . The outcome inpatients in whom this procedure fails and who subsequentlyrequire revision to a total hip arthroplasty has only recentlybeen studied extensively 2. With the increasing life span ofpatients with fixed trochanteric fractures, late complicationsof these surgeries are becoming significant. Within thisscenario, it has been argued that the most effective solution
Hip arthroplasty following failed dynamic hip screwfixation for per-trochanteric femoral fracturesSKS Marya, R Thukral, R Bawari, R Gupta
Max Healthcare, New Delhi
SKS Marya, MS, DNB, MCh Orth, Director Orthopedics & Joint ReplacementInstituteR Thukral, MS, DNB (Orth), Consultant OrthopedicsBawari R, MS (Orth), DA, Consultant OrthopedicsGupta R, MS (Orth), Joint Replacement FellowMax Healthcare, New DelhiDr SKS Marya, 1193A, Sector B-1, Vasant Kunj, New Delhi – 110070;Email: [email protected] **
to the femoral neck fracture in the majority of patients is openreduction and internal fixation, with elective conversion, whennecessary, to total hip arthroplasty in patients who have acomplication 3.
Unstable trochanteric fractures demonstrate overallfailure rates in the range of 3%-12%, with non-union in 2% to5%, device penetration in 2% to 12%, and varus collapse in5%-11% 3-6. The primary indication for secondary surgery isrelief of pain resulting from the aforementionedcomplications5 . Bipolar or total hip arthroplasty may beutilized for the salvage of such failed fracture fixations of theproximal femur.
In the conversion of these cases to hip replacement,various technical difficulties may be encountered7. Also, ahigh incidence of intra- and post-operative complicationsmay occur because of the altered biomechanics and bonestock, including femoral fracture, wound infection, and asepticloosening7. The purpose of this study is to review experiencewith conversion of fractures of the proximal femur (treatedby dynamic hip screw fixation) to hip arthroplasty, assessthe technical difficulties encountered, and to report the short-term outcome in our series of seventeen patients.
Materials and Methods
Six males and 11 females with a mean age of 65 years(range 60-72 years) were reviewed retrospectively for age,gender, type of fracture, complication necessitating hiparthroplasty, status of the acetabulum, time interval toconversion, type of components used, postoperative positionof the components, leg length restoration, technical problemsencountered at surgery, blood loss, postoperativecomplications and clinical end result.
Three patients (all females) had healthy acetabuli, andcemented bipolar arthroplasty was performed in them.Fourteen patients had significant arthritic changes in theiracetabulae necessitating total hip replacement. The meanfollow up was 30 months (range, 9 months to 72 months).
Deficiency of proximal femoral bone was managed usingautogenous graft (femoral head), or use of the long-neck /long-stem replacement prosthesis. Long stemmed prostheses
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 147-150
VOL. 38, NO. 3, JULY 2004 147

INDIAN JOURNAL OF ORTHOPAEDICS148
were used in all our cases, the distal tip extending about 2-3cms. distal to the last screw hole (of the removed dynamichip screw plate). Long neck stems were used in six of thepatients. Distal plug of bone was inserted with the help ofHardinge restrictor holder. Screw holes were blocked withcement (manual pressurization). No neurological or vascularcomplications were encountered. Post-operatively all patientswere made to stand and walk within 3-5 days and were put ona vigorous physiotherapy program.
At final follow-up, patients were analyzed for pain, limp,use of support, distance walked, difficulty with stairs, abilityto dress, sitting pain, and use of transportation. They werealso rated on a 10-point Visual Analog Scale as to their levelof satisfaction.
Results
The time interval from the original internal fixation toconversion to hip arthroplasty averaged 20 months for theentire study group. Charnley cemented Ogee acetabular(except the bipolar patients) and femoral components wereutilized in all cases. Pre-operative shortening of the femuraveraged 16 mm. Restoration of leg length to within 5 mm ofequality was accomplished in all patients.
The average blood loss for bipolar arthroplasty was 400ml, while that for total hip replacement was 600ml. Totaloperative time for conversion to bipolar arthroplastyaveraged 60 minutes compared to 80 minutes for total hipreplacement.
A unique complication occurred in one of our earlierpatients. The stem of the prosthesis followed the path createdby dynamic hip screw and was projecting out on the lateralaspect of the shaft of the femur. This was recognized duringthe surgical procedure, exit holes were cemented and theprosthesis was inserted in proper position.
One patient with failure of operated intertrochantericfracture had dislocation of his converted THR two days aftersurgery (Figs. 1a, b). This was recognized immediately andclosed reduction was successful. Abduction brace wasapplied for 6 weeks. He has had no recurrence of thedislocation since then (Fig. 1c)
No patient had persistence of pain, sitting or otherwise.Reasonably good function was achieved in the majority, andthe patients were themselves quite satisfied with the endresults (Fig. 2a, b).
Discussion
Reduction and internal fixation remains the primarytreatment of displaced pertrochanteric fractures in mostpatients because of the benefits of preservation of the normalhip joint. However, if this method of treatment fails, revisionto a hip arthroplasty is a universally accepted option7-9. Ingeneral, the results of secondary replacement are comparableto those obtained following primary arthroplasty or failedinternal fixation for femoral neck fractures7-9. The risk of earlycomplications is however higher and hip function may bepoorer than if the arthroplasty had been performed as a
Fig. 1(a) Failed DHS done for intertrochanteric fracture femur; (b) Converted THR dislocation; (c) Closed reduction of dislocatedconverted THR
(a) (b) (c)
HIP ARTHROPLASTY FOLLOWING FAILED DYNAMIC HIP SCREW FIXATION

VOL. 38, NO. 3, JULY 2004 149
primary procedure2. Contemporary techniques of fracturefixation with compression screw-plate devices demonstratefailure rates of 5% to 10%4-5. Many patients will thereforerequire hip arthroplasty to salvage failed internal fixation ofproximal femur fractures. This series demonstrates thatsatisfactory results may be achieved in the majority of cases.
The treatment algorithms for displaced fractures of thefemoral neck in the elderly need to be improved if we are toreduce the need for secondary surgery. Primary hipreplacement provides a better outcome than internal fixationfor the elderly, relatively healthy, lucid patients with adisplaced fracture of the femoral neck10. In comparison withosteosynthesis, endoprosthetic replacement is less extensive,the mortality no higher and the complication rate lower. It istherefore the procedure of choice in arthritic hip fractures11.Internal fixation may be only appropriate for those who arevery frail12.
A review of literature on the comparative results ofinternal fixation and arthroplasty for unstable extracapsulartrochanteric femoral fractures show no significant differencesbetween the two methods of treatment for operating time,local wound complications, mortality rate or mobility ofpreviously independent patents. Primary replacementarthroplasty has not been demonstrated to have anysignificant advantage over the sliding hip screw forextracapsular hip fractures6. In a study by Berry 13, final hipscores at 2 years or more after total hip arthroplasty were notstatistically different between patient groups undergoingprimary or conversion hip arthroplasties. The authorsconcluded that total hip replacement is a satisfactory salvageprocedure for failed fracture treatment despite the increasedincidence of operative difficulty and increased incidence ofcomplications9,13.
Salvage of failed intertrochanteric fractures proves to beconsiderably more challenging. Unstable intertrochanteric
fracture patterns tend to heal with distortion of the neck-shaft relationship. Sizable medial displacement of the distalportion of the canal made conventional reaming and broachingdifficult, which has to be done carefully7. The commonlyencountered fracture patterns leave the proximal femurshortened, in varus, and with medial displacement of the neckon the shaft. If the surgeon does not recognize the deformityof the upper femur, penetration of the shaft or fracture of theupper end of the femur may occur7,13. In our series there wasno perforation of the canal.
Endoprostheses are now considered invaluable in thesalvage of failed internal fixation of a subtrochanteric orintertrochanteric fracture7,11,13-15. Preservation of the functionalcontinuity of the abduction apparatus during surgery, andearly weight bearing made possible by the arthroplasty areconsidered to be the major factors contributing to thepublished good results 16.
Reconstruction of the proximal femur is almost alwaysrequired, and may be achieved by various means. One maysimply use a standard component with a long neck (suitablefor simple fracture patterns). Unstable fractures have specialrequirements. The medial displacement of the shaft may notaccommodate the curvature of the conventional femoral stem.In such cases, the surgeon may choose to rebuild the proximalfemur either by using the bone from the femoral head andneck as an intercalary graft or, if this is not of sufficient quality,a femoral allograft7. Autograft, allograft or head and neckreplacement components should be available forreconstruction of difficult cases7,15. Calcar-replacementimplants may also be occasionally required15. We prefer theuse of the long neck prosthesis as a simpler solution,especially in older individuals. This technique has provedsuccessful in the short follow-up period in our series.
Another technical difficulty we encountered iscontainment of the acrylic cement when it is pressurized. The
Fig. 2(a) Failed DHS done forbasicervical fracture neckfemur; (b) Conversion tocemented THR
(a) (b)
SKS MARYA, R THUKRAL, R BAWARI, R GUPTA

INDIAN JOURNAL OF ORTHOPAEDICS150
cement tends to extrude through previous screw holes, butthis can be contained by soft tissue and the pressure affordedby the assistant surgeon’s fingers.
Dislocation can occur following conversion ofintertrochanteric fractures to joint replacement9,13. This maybe prevented by careful component positioning, restorationof leg length, and careful abductor mechanismreconstruction9,13.
In older patients with limited functional demands andnormal acetabulum, a bipolar acetabular component mayafford better stability17-18. Also, rehabilitation is easier andfaster, and the incidence of pressure sores, pulmonaryinfection, and atelectasis are significantly lower with thebipolar prostheses 17-18.
To sum up, the method of treatment chosen for a failedtrochanteric fracture depends on the specific problem:nonunion, aseptic necrosis, infection, degenerative arthritis,or a failed primary prosthesis. Factors influencing treatmentinclude the patient’s chronological and physiological age,his general health, his life pattern, familiarity of the surgeonwith the technique, and, the advantages and disadvantagesof the salvage procedure 19.
The surgeon should be cognizant of the technicaldifficulties that may be encountered in conversion of failedper-trochanteric fractures, as well as the complications andpitfalls. Recognition of distortion of the proximal femur andthe availability of standard implants and head and neckreplacement components allows satisfactory outcome in thesechallenging cases.
References
1. Ecker M, Joyce JJ, Kohl EJ. The treatment of trochanteric hip frac-tures using a compression screw. J Bone Joint Surg (Am). 1975; 57:23.
2. McKinley JC, Robinson CM. Treatment of displaced intracapsular hipfractures with total hip arthroplasty: comparison of primary arthroplastywith early salvage arthroplasty after failed internal fixation. J Bone JointSurg (Am). 2002; 84:2010-5.
3. Estrada LS, Volgas DA, Stannard JP, Alonso JE. Fixation failure infemoral neck fractures. Clin Orthop. 2002; 399:110-8.
4. Johnsson R. Comparison between hemiarthoplasty and total hip re-placement following failure of nailed femoral neck fractures focused ondislocations. Arch Orthop Trauma Surg. 1984; 102:107.
5. Laros GS, Moore JF. Complications of fixation in intertrochantericfractures. Clin Orthop. 1974; 101: 110.
6. Parker MJ, Handoll HH. Replacement arthroplasty versus internalfixation for extracapsular hip fractures. Cochrane Database Syst Rev.2000;(2):CD000086.
7. Mehlhoff T, Landon GC, Tullos HS. Total hip arthroplasty followingfailed internal fixation of hip fractures. Clin Orthop. 1991; 269:32-7.
8. Franzen H, Nilsson LT, Stromqvist B, Johnsson R, Herrlin K.Secondary total hip replacement after fractures of the femoral neck. JBone Joint Surg (Br). 1990;72:784-7.
9. Berry DJ. Salvage of failed hip fractures with total hip replacement.Orthopedics. 2002; 25:949-50.
10. Tidermark J, Ponzer S, Svensson O, Soderqvist A, Tornkvist H.Internal fixation compared with total hip replacement for displaced femo-ral neck fractures in the elderly. A randomized, controlled trial. J BoneJoint Surg (Br). 2003; 85(3):380-8.
11. Broos P, Willemsen PJ, Rommens PM, Stappaerts KH, Gruwez JA.Pertrochanteric fractures in elderly patients. Treatment with a long-stem/long-neck endoprosthesis. Unfallchirurg. 1989; 92(5):234-9.
12. Parker MJ, Khan RJ, Crawford J, Pryor GA. Hemiarthroplasty ver-sus internal fixation for displaced intracapsular hip fractures in the eld-erly. A randomized trial of 455 patients. J Bone Joint Surg (Br). 2002;84(8):1150-5.
13. Tabsh I, Waddell JP, Morton J. Total hip arthroplasty for complica-tions of proximal femoral fractures. J Orthop Trauma. 1997;11(3):166-9.
14. Stoffelen D, Haentjens P, Reynders P, Casteleyn PP, Broos P,Opdecam P. Hip arthroplasty for failed internal fixation of intertrochan-teric and subtrochanteric fractures in the elderly patient. Acta OrthopBelg. 1994; 60 Suppl 1:135-9.
15. Haidukewych GJ, Berry DJ. Hip arthroplasty for salvage of failedtreatment of intertrochanteric hip fractures. J Bone Joint Surg (Am).2003; 85:899-904.
16. Haentjens P, Casteleyn PP, Opdecam P. Hip arthroplasty for failedinternal fixation of intertrochanteric and subtrochanteric fractures in theelderly patient. Arch Orthop Trauma Surg. 1994; 113(4):222-7.
17. Green S, Moore T, Proano F. Bipolar prosthetic replacement for themanagement of unstable intertrochanteric hip fractures in the elderly.Clin Orthop. 1987; 224:169-77.
18. Haentjens P, Casteleyn PP, De Boeck H, Handelberg F, OpdecamP. Treatment of unstable intertrochanteric and subtrochanteric fracturesin the elderly patient. Primary bipolar arthroplasty compared with internalfixation. J Bone Joint Surg (Am). 1989; 71(8):1214-25.
19. Albright JP, Weinstein SL. Treatment for fixation complications: Femo-ral neck fractures. Arch Surg. 1975;110(1):30-6.
HIP ARTHROPLASTY FOLLOWING FAILED DYNAMIC HIP SCREW FIXATION

Background: The accurate estimation of femoral neckanteversion in living subjects has always been difficult with lots ofinter- and intra-method variations. The present study wasundertaken to define the range of normal femoral neck anteversionin our adult population and to draw the relationship between theperoperative, biplane X-rays and clinical methods.Methods: Femoral neck anteversion was evaluated by theperoperative, biplane X-rays and clinical methods on 31 otherwisehealthy and normal adults who underwent closed reduction /open reduction and internal fixation for post traumatic freshintracapsular fracture of the neck of femur.Results: The mean value obtained by peroperative, biplane X-rays and clinical methods were 10.6° (n=31 hips), 11.7° (n=62hips) and 13.0° (n=62 hips) respectively. No statistically significantdifference was found between the sides and the sexes. Theclinical method correlated better with the peroperative methodthan the X-rays method.Conclusion: The average femoral neck anteversion in oursubjects was estimated to be 10.6° (SD 2.2°) by the per-operativemethod, with 83.6% subjects having anteversion between 8.6-12.6°. This is less than most of the western data. Statistical relationshave also been drawn between the peroperative, X-ray and theclinical methods.Key-words: Femoral neck anteversion, Peroperative, Clinical,Radiological measurement
Introduction
The angle of anteversion of the neck of femur in humansexhibits a wide range (-25° to +50°) with the mean angle varying
from 8 to 25 degrees1-7. Racial variations are expected to existin femoral neck anteversion and may have an importantimplication. Since our population is more apt to floor levelactivities with increased external rotation of the hip, our hipswould be evolutionally different from the Westerncounterparts.
The accurate estimation of femoral neck anteversion inliving subjects has always been difficult with lots of inter-and intra-method variations. Estimation of anteversion ondry bone is considered the most accurate method. But theirgreatest drawback is that involvement of femora from someof the skeletons with pathologic conditions can not be ruledout which may influence the statistical analysis. Themeasurement on dry bones may not be relevant for clinicalpractice since clinicoradiological measurements of the angleof anteversion may be different from those obtained on dryfemora. The present study is undertaken to define the rangeof normal femoral neck anteversion in our adult populationand to draw the relationship between the peroperative,biplane X-rays and clinical methods.
Materials and Methods
Thirty one consecutive patients, who underwent closereduction / open reduction and internal fixation for post-traumatic fresh intracapsular fractures of neck of the femur orundisplaced intertrochanteric fractures of the femur in ourdepartment constituted the clinical material for this study.These patients were otherwise medically fit adults, more than18 years of age. Old hip pathology was ruled out by thoroughclinical and radiological assessment. Osteopenic states likeosteomalacia and malignancy were ruled out. Informedconsent was taken in each case. Surgery was done withinthree to four days of trauma. These patients were evaluatedfor the estimation of the angle of anteversion by:
• Peroperative method (on affected side)
• Biplane X-rays method (bilateral hips)
• Clinical method (bilateral hips)
Estimation of femoral neck anteversion in adults -A comparison between peroperative, clinical and biplaneX-rays methodsAV Maheshwari, AK Jain, MP Singh, SK Bhargava
University College of Medical Sciences and Guru Teg Bahadur Hospital, Shahdara, Delhi
Aditya V MaheshwariAK Jain, Professor of OrthopaedicsMP Singh, Professor of OrthopaedicsSK Bhargava, Professor, Department of RadiodiagnosisUniversity College of Medical Sciences and Guru Teg Bahadur Hospital,Shahdara, Delhi-110095 (INDIA).Prof AK Jain,Department of Orthopaedics, University College of MedicalSciences and Guru Teg Bahadur Hospital, Delhi-110095 (INDIA),E-mail: [email protected] **
VOL. 38, NO. 3, JULY 2004 151
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 151-157

INDIAN JOURNAL OF ORTHOPAEDICS152
Evaluation of angle of anteversion by clinical andradiological methods were done three to six months aftersurgery, when there was evidence of radiological union withadequate range of motion.
Peroperative Method
The patients were placed supine on the fracture table. Astandard lateral approach was used to expose the proximalpart of the femur. A guide wire was put in the approximatecenter of the femoral neck after reduction in both theanteroposterior and lateral projections as confirmed by theC-arm image intensifier. The neck was fixed with 6.5 mmcannulated cancellous screws. The limb was then realignedon the spica table till the patella points skywards to get ahorizontal condylar plane. The angle between the guide wireand the horizontal axis was, by definition, the true angle ofanteversion (a). Since defining of horizontal axis was difficulton table, we defined the vertical axis by dropping a plumbline onto the guide wire from above. The angle formedbetween the guide wire and the plumb line was designated as‘b’ and was measured by a variable angle guide, 90° minus ‘b’was the angle of anteversion - ‘a’ (since the plumb linerepresented the true vertical i.e. 90° to the horizontal condylaraxwas). Three different readings were taken for each caseand the average of the three was taken as final for that femur(Fig. a,b).
X-rays method (Ogata et al, 1979)8
The patient was kept supine on the X-rays table. Theknee was flexed to 90° on the edge of the table with the legsperpendicular to the ground. An anteroposterior
roentgenogram of the hip was taken with the tube centeredover the femoral neck and the beam perpendicular to thetable. This position brings the transcondylar axis of the distalend of the femur into the horizontal plane. The true lateralroentgenogram of the femoral neck was made with the patientlying supine on the table with the hip and knee flexed to 90ºand the entire lateral aspect of the leg contacting the tabletop. This positioning rotates the femur 90º on its long axiscompared with the anteroposterior roentgenogram, so thatthe transcondylar plane was perpendicular to the table. APand lateral views for both the sides were obtained on eachpatient. The location of the axes on the roentgenograms wasdone by the technique described by Hubbard and Staheli9,where the central axis of the neck was located on each film bya line connecting the center of the neck at its proximal anddistal ends. To locate the axis of femoral shaft, two sites weremarked – one, just inferior to the lesser trochanter, and thesecond, 10 cms distal to the lesser trochanter. The line joiningthe center of the shaft at these two sites represents the axisof the femoral shaft. The 10 cms mark was chosen as most ofthe X-rays of this region contained these points. The anglebetween the shaft axis and the neck axis was measured oneach film and the angle of anteversion was then determinedby trigonometric calculations or by available normograms.
Clinical Method (Ruwe et al)10
The anteversion was measured clinically by thetrochanteric prominence angle test. The patients were placedprone on a hard surface with knee flexed to 90° and legsvertically up. To measure the right hip the examiner standson the left side of the patient. The left hand was used to
Fig. 1 (a). Measurement of femoral neck anteversion angleperoperatively using a guide wire, a variable angle guide and aplumb line.
Fig. 1 (b). The illustration of figure 1a, whereV = vertical axis or plumb line, H = horizontal axis,b = measured angle; a = anteversion angle = 90°-bG = guide wire in centre of neck; A = variable angle guide
PEROPERATIVE, CLINICAL AND X-RAYS EVALUATION OF FEMORAL ANTEVERSION

VOL. 38, NO. 3, JULY 2004 153
palpate the greater trochanter while the right hand externallyrotates the leg. At the point of maximum trochantericprominence, representing the most lateral position of thetrochanter, the neck of the femur was parallel to the ground.The angle subtended between the tibia and true vertical wasmeasured with a goniometer, and this represents the angle ofanteversion of femoral neck. Three such readings were takenfor each limb and the average of those were considered asfinal reading.
Table II. Distribution of peroperative cases around the mean offemoral neck anteversion
±Degrees Perop. total (n=31) Perop. right (n=15) Perop.left (n=16)of mean No. % No. % No. %±1 12 38.70 7 46.67 5 31.25±2 26 83.87 13 86.67 13 81.25±3 28 90.32 14 93 14 87.50±4 30 96.78 15 100 15 93.75±5 30 96.78 15 100 15 93.75±6 30 96.78 15 100 15 93.75
Mean 10.6° 10.7° 10.5°
Results
Peroperative Method
Thirty one patients (21 males and 10 females), involvingthe right hip in 15 cases and left hip in 16 cases were analysed.The right side was affected in 10 males and 5 females and theleft side was affected in 11 males and 5 females. The mean ofthe peroperative observed angle of femoral neck anteversionwas 10.6° with a standard deviation (SD) of 2.2°. The medianwas 10°, the mode was 9.3° and the range (mean±2SD) wasfrom 6.0° to 15.1°. The mean of males was 10.8° (SD 2.6°) andthe mean of females was 10.1° (SD 1.2°). The mean of right
side was 10.7° (SD 1.6°) and the mean of left side was 10.5°(SD 2.8°). The mean of right sided males was 10.7° (SD 1.7°)and of left sided males was 10.8° (SD 3.3°). The mean of rightsided females was 10.5° (SD 1.4°) and of left sided femaleswas 9.9° (SD 1.2°). Twenty six (83.87%) of observations werewithin ±2° (8.6° to 12.6°) of the mean and 90% (28) were within±3° of the mean (Table I,II).
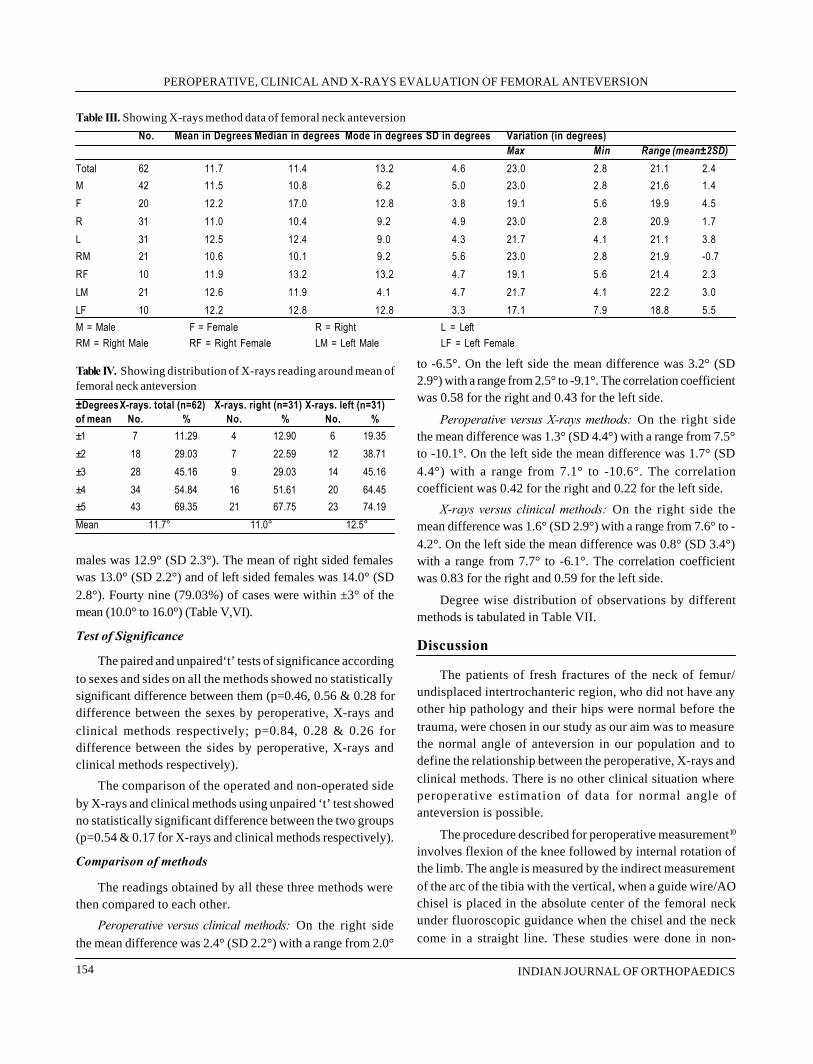
X-rays Method
Since bilateral hips were evaluated, total hips in this groupwere 62, with 42 males and 20 females. Both the right and theleft sides were evaluated in 21 males and 10 females (31 rightsided and 31 left sided hips). The mean of the observed angleof anteversion of femoral neck was 11.7° (SD 4.6°). The medianwas 11.4° and mode was 13.2° with a range (mean±2SD) from2.4° to 21.1°. The mean of males was 11.5° (SD 5.0°) and themean of females was 12.2° (SD 3.8°). The mean of right sidewas 11.0° (SD 4.9°) and the mean of left side was 12.5° (SD4.3°). The mean of right sided males was 10.6° (SD 5.6°) andof left sided males was 12.6° (SD 4.7°). The mean of rightsided females was 11.9° (SD 4.7°) and of left sided femaleswas 12.2° (SD 3.3°). Fourty three (69.3%) of observationswere within ±5° of the mean (6.7° to 16.7°) (Table III,IV).
Clinical Method
Same sets of patients as evaluated by X-rays methodwere clinically examined to measure the angle of anteversion.The mean of the observed angle of anteversion in this groupwas 13.0° (SD 2.7°). The median was 13.0°, the mode was10.5° and the range (mean±2SD) was from 7.6° to 18.4°. Themean of males was 12.7° (SD 2.7°) and the mean of femaleswas 13.5° (SD 2.4°). The mean of right side was 12.7° (SD2.8°) and the mean of left side was 13.3° (SD 2.5°). The meanof right sided males was 12.5° (SD 3.1°) and of left sided
Table I. Per operative method data of femoral neck anteversion
No. Mean in Median Mode in Std. Dev. Variation (in degrees)Degrees in degrees degrees in degrees Max Min Range (mean±2SD)
Total 31 10.6 10.0 9.3 2.2 19.6 7.3 15.1 6.0M 21 10.8 10.1 9.3 2.6 19.6 7.3 16.0 5.5F 10 10.1 9.8 8.6 1.2 12.8 8.6 12.6 7.6R 15 10.7 10.0 9.1 1.6 14.5 8.6 13.9 7.4L 16 10.5 10.0 9.3 2.8 19.6 7.3 16.1 4.8RM 10 10.7 10.6 11.3 1.7 14.5 8.6 14.2 7.2RF 5 10.5 10.0 9.1 1.4 12.8 9.1 13.4 9.6LM 11 10.8 10.1 10.3 3.3 19.6 7.3 17.4 4.1LF 5 9.9 9.5 8.6 1.2 11.8 8.6 12.3 7.4M = Male F = Female R = Right L = LeftRM = Right Male RF = Right Female LM = Left Male LF = Left Female
AV MAHESHWARI, AK JAIN, MP SINGH, SK BHARGAVA
INDIAN JOURNAL OF ORTHOPAEDICS154
males was 12.9° (SD 2.3°). The mean of right sided femaleswas 13.0° (SD 2.2°) and of left sided females was 14.0° (SD2.8°). Fourty nine (79.03%) of cases were within ±3° of themean (10.0° to 16.0°) (Table V,VI).
Test of Significance
The paired and unpaired‘t’ tests of significance accordingto sexes and sides on all the methods showed no statisticallysignificant difference between them (p=0.46, 0.56 & 0.28 fordifference between the sexes by peroperative, X-rays andclinical methods respectively; p=0.84, 0.28 & 0.26 fordifference between the sides by peroperative, X-rays andclinical methods respectively).
The comparison of the operated and non-operated sideby X-rays and clinical methods using unpaired ‘t’ test showedno statistically significant difference between the two groups(p=0.54 & 0.17 for X-rays and clinical methods respectively).
Comparison of methods
The readings obtained by all these three methods werethen compared to each other.
Peroperative versus clinical methods: On the right sidethe mean difference was 2.4° (SD 2.2°) with a range from 2.0°
to -6.5°. On the left side the mean difference was 3.2° (SD2.9°) with a range from 2.5° to -9.1°. The correlation coefficientwas 0.58 for the right and 0.43 for the left side.
Peroperative versus X-rays methods: On the right sidethe mean difference was 1.3° (SD 4.4°) with a range from 7.5°to -10.1°. On the left side the mean difference was 1.7° (SD4.4°) with a range from 7.1° to -10.6°. The correlationcoefficient was 0.42 for the right and 0.22 for the left side.
X-rays versus clinical methods: On the right side themean difference was 1.6° (SD 2.9°) with a range from 7.6° to -4.2°. On the left side the mean difference was 0.8° (SD 3.4°)with a range from 7.7° to -6.1°. The correlation coefficientwas 0.83 for the right and 0.59 for the left side.
Degree wise distribution of observations by differentmethods is tabulated in Table VII.
Discussion
The patients of fresh fractures of the neck of femur/undisplaced intertrochanteric region, who did not have anyother hip pathology and their hips were normal before thetrauma, were chosen in our study as our aim was to measurethe normal angle of anteversion in our population and todefine the relationship between the peroperative, X-rays andclinical methods. There is no other clinical situation whereperoperative estimation of data for normal angle ofanteversion is possible.
The procedure described for peroperative measurement10
involves flexion of the knee followed by internal rotation ofthe limb. The angle is measured by the indirect measurementof the arc of the tibia with the vertical, when a guide wire/AOchisel is placed in the absolute center of the femoral neckunder fluoroscopic guidance when the chisel and the neckcome in a straight line. These studies were done in non-
Table III. Showing X-rays method data of femoral neck anteversion
No. Mean in Degrees Median in degrees Mode in degrees SD in degrees Variation (in degrees)Max Min Range (mean±2SD)
Total 62 11.7 11.4 13.2 4.6 23.0 2.8 21.1 2.4M 42 11.5 10.8 6.2 5.0 23.0 2.8 21.6 1.4F 20 12.2 17.0 12.8 3.8 19.1 5.6 19.9 4.5R 31 11.0 10.4 9.2 4.9 23.0 2.8 20.9 1.7L 31 12.5 12.4 9.0 4.3 21.7 4.1 21.1 3.8RM 21 10.6 10.1 9.2 5.6 23.0 2.8 21.9 -0.7RF 10 11.9 13.2 13.2 4.7 19.1 5.6 21.4 2.3LM 21 12.6 11.9 4.1 4.7 21.7 4.1 22.2 3.0LF 10 12.2 12.8 12.8 3.3 17.1 7.9 18.8 5.5M = Male F = Female R = Right L = LeftRM = Right Male RF = Right Female LM = Left Male LF = Left Female
Table IV. Showing distribution of X-rays reading around mean offemoral neck anteversion
±DegreesX-rays. total (n=62) X-rays. right (n=31) X-rays. left (n=31)of mean No. % No. % No. %±1 7 11.29 4 12.90 6 19.35±2 18 29.03 7 22.59 12 38.71±3 28 45.16 9 29.03 14 45.16±4 34 54.84 16 51.61 20 64.45±5 43 69.35 21 67.75 23 74.19Mean 11.7° 11.0° 12.5°
PEROPERATIVE, CLINICAL AND X-RAYS EVALUATION OF FEMORAL ANTEVERSION

VOL. 38, NO. 3, JULY 2004 155
traumatic conditions like CDH, cerebral palsy andpoliomyelitis where derotation osteotomy was planned forthe patient. Since we have measured the angle of anteversionin cases of traumatic hips, it was unjustified and impossibleto remove the traction and measure the angle between thetibia and the vertical axis. The measurement of tibia with animaginary vertical axis adds lot of subjectivity to themeasurement. We modified this method. We only needed toalign the patella vertically upwards which involved rotationof the whole limb. The anteversion angle is measured betweentwo sharp well defined lines i.e. the suspended thread of theplumb line and a solid guide wire. In our series, seven of thepostoperative patients later on underwent CT scan for hipunrelated pathologies. Retrospectically, femoral neckanteversion was evaluated by the CT method and it hasshown good correlation to our peroperative method (0.92).
The method of Ogata et al8 for the roentgenographicmeasurements of the angle of anteversion has severaladvantages over other radiographic techniques in use. Itrequires no special X-rays equipment or positioningapparatus and can be done quickly and easily. This methodhas been found to be accurate and reproducible in clinicalpractice. The true femoral neck-shaft angle as well as thedegree of femoral anteversion can be determinedsimultaneously.
Clinical measurements were performed by thetrochanteric prominence test10. Since this method is supposedto be influenced by various extrinsic and intrinsic variableslike tension of the hip capsule, inclination of the acetabulum,muscle and fat mass over the trochanter and patients’cooperation, it has often not been used for investigativepurposes. This method has not been used before to estimatethe profile of anteversion angle in a normal population. But
we have also used this method to obtain a correlation ofclinical and other methods due to its simplicity.
Ruwe et al10 compared the peroperative method to theclinical, X-rays and CT methods in pathological hips like CDH,cerebral palsy and poliomyelitis, where there was alreadyincreased angle of anteversion. No study has been everundertaken to estimate the normal angle of anteversion in apopulation by the peroperative method. Standardization ofperoperative method and its relation with clinical and X-raysmethod is of utmost importance so that correct estimationcan be made and correction of rotatory deformities can beundertaken. The position of the patient for a lateral X-rayswas difficult in a postoperative case. The palpation of thegreater trochanter also poses problem due to thepostoperative scar and fibrosis. These factors could affectthe calculation of normal anteversion of operated side. Since,no statistically significant difference was found between theoperated and non-operated side by all the methods, thesevalues thus obtained were combined to get the normalanteversion angle for the sample of patient.
Variable range of normal femoral neck anteversion hasbeen reported by various authors and also by variousmethods. The combined study on 806 dry femora showedthe mean average to be 14.09°3. Kingsley and Olmsted6 intheir study on 630 adult dry femora found the average to be8.021°, with males averaging 7.97° and females 8.11°. Dunlapet al3 used X-rays method on 100 normal adults and foundthe average anteversion to be 8.7° with no mention of therange. This was stated to be 8° to 15 ° by Budin and Chandler2,18° by Gibson4 and 28° by Herrlin et al5 in normal adults.Ruby et al11 compared the radiological methods of Ryder andCrane (biplanar x-rays), Dunn (axial x-rays) and Rogers(fluoroscopy) and found them to be comparable in clinicalpractice. Terjeson12 et al compared the ultrasound method to
Table V. Showing clinical method data of femoral neck anteversion
No. Mean in Median in Mode in Std. Dev. in Variation (in degrees)Degrees degrees degrees degrees Max Min Range (mean±2SD)
Total 62 13.0 13.0 10.5 2.7 20.5 8.0 18.4 7.6M 42 12.7 12.5 10.5 2.7 20.5 8.0 18.3 7.1F 20 13.5 13.5 14.5 2.4 20.0 9.1 18.4 8.6R 31 12.7 12.6 10.5 2.8 20.5 8.0 18.4 6.9L 31 13.3 13.1 13.6 2.5 20.0 8.5 18.3 8.2RM 21 12.5 12.1 13.3 3.1 20.5 8.0 18.9 6.1RF 10 13.0 13.8 14.5 2.2 15.6 9.1 17.5 8.5LM 21 12.9 13.0 13.6 2.3 18.8 8.5 17.6 8.2LF 10 14.0 14.0 9.8 2.8 20.0 9.8 19.6 8.4M = Male F = Female R = Right L = LeftRM = Right Male RF = Right Female LM = Left Male LF = Left Female
AV MAHESHWARI, AK JAIN, MP SINGH, SK BHARGAVA

INDIAN JOURNAL OF ORTHOPAEDICS156
plain X-rays and found discrepancy of less than 10° in morethan 90% of the cases (47 girls and 10 boys). Braten et al1
found the average anteversion to be 18° (SD 7.4°) in normalfemales and 14° (SD 7.8°) in normal males using ultrasound.Using the Murphy13 (1987) method of CT scan, Reikeras etal7 found the anteversion angle to be 18° (SD 6°) in femalesand 16° (SD 5°) in males. Miller et al14 compared the variousmethods on 24 dry femora and the found the average as 16.4°(SD 5.9°) by Kingsley and Olmsted method, 11.4° (SD 6.7°)by CT method of Weiner, 16.8° (SD 4.1°) by flat goniometermethod, 21.1° (SD 4.9) by ultrasound HN Tangent methodand 21.3° (SD 4.5°) by ultrasound flat surface method. Hestated that CT results were lowest that all other methods andthe average difference between the CT and the ultrasoundmethod was 10°. Thus the actual peroperative anteversionvalue in our patient is less than most of the western studies.
The average angle of anteversion by peroperativemethod in our series was 10.6° (SD 2.2°) which was less thanthose obtained by the X-rays method [11.7° (SD 4.6°)] andthe clinical method [13.0° (SD 2.7°)]. More than 83.87% (26hips) of our cases were within ±2° (8.6° to 12.6°) of the meanin peroperative method. Only 2 values were just lower thanthis (7.3° and 8.1°) and 3 values were higher than this (12.8°,14.5° and 19.6°). 48.39% of cases have less than 10° ofanteversion and 80.64% of cases had less than 12° ofanteversion. About 70% of the cases were between 6.7° and16.7° and 95% of the cases between 2.4° to 21.1° by the x-rays method. 79% of the cases were between 10.0° to 16.0°and 95% cases between 7.6° to 18.4° by the clinical method.Since values at extremes of data influence the mean, we havedefined our true range as mean±2SD and extended ourstatistical analysis to find out the range which covers about3/4th of the population. No statistically significant differencewas observed between the sides and the sexes.
In our series, all the three methods showed differentreadings in the same patient. Thus, there is a method specificvariation in the angle of anteversion with a wide range ofmean difference between various methods. The correlationbetween the clinical and peroperative method was howeversuperior to the peroperative and X-rays method. Also therange of mean difference between the peroperative andclinical method is narrower than between the peroperativeand the X-rays method. Thus the clinical method is betterthan the X-rays method for measurement of angle ofanteversion10. Though better modalities like CT scan methodare desirable if any surgical procedure is being contemplated(e.g. restoration osteotomies), its use can be precluded by itscost factor and non-availability at all centres, radiation fearand its less reliability in cases of excessive coxa valga orexcessive anteversion14. Thus the peroperative value stillremains the true available angle of anteversion in livingsubjects.
Conclusions
The average angle of anteversion by peroperativemethod was found to be 10.6° (SD 2.2°) with a range(mean±SD) from 6.0° to 15.1°. By the x-rays method this was11.7° (SD 4.6°) with a range (mean±2SD) from 2.4° to 21.1°.About 70% of the cases were between 6.7° to 16.7°. By theclinical method this was 13.0° (SD 2.7°) with a range (mean±SD)from 7.6° to 18.4°. About 79% of the cases were between10.0° to 16.0°. Peroperative value on an average was found tobe 1.1° less than the x-rays and 2.4° less than the clinicalmethod. It seems to be the value which is more near to thetrue angle of anteversion. Hence 83.8% of population has ananteversion between 8.6° and 12.6°, which is less than mostof the western studies. No statistically significant differencewas found between the sides and the sexes. The clinicalmethod was found to correlate better to the peroperativemethod than the X-rays method.
Table VI. Showing distribution reading by clinical method aroundthe mean of femoral neck anteversion
±Degrees Clinical total Clinical right Clinical left ofmean (n=62) (n=31) (n=31)
No. % No. % No. %±1 18 29.03 8 25.81 9 29.03±2 34 54.84 16 51.61 19 61.3±3 49 79.03 23 74.19 26 83.88±4 54 87.10 27 87.10 27 87.10±5 57 91.93 29 93.55 29 93.55±6 60 96.78 29 93.55 29 93.55
Mean 13.0° 12.7° 13.3°
Table VII. Showing the slabwise distribution of femoral neckanteversion by different methods
Angle in Perop X-rays Clinicaldegrees No. %age No. %age No. %age0-5 0 0 3 4.83 0 05.1-10 16 51.61 21 33.87 8 12.9010.1-15 14 45.16 22 35.48 42 67.74>15 1 3.22 16 25.80 10 32.26Mean 10.6° (n=31) 11.7° (n=62) 13.0° (n=62)
Range 6.0° to 15.1° 2.4° to 21.1° 7.6° to 18.4°
PEROPERATIVE, CLINICAL AND X-RAYS EVALUATION OF FEMORAL ANTEVERSION

VOL. 38, NO. 3, JULY 2004 157
References
1. Braten M, Terjeson T, Rossvoll I. Femoral anteversion in normaladults. Ultrasound measurements in 50 men and 50 women. Acta OrthopScand. 1992; 63(1): 29-32.
2. Budin E, Chandler E. Measurement of femoral neck anteversion by adirect method. Radiol. 1957; 69: 209-13.
3. Dunlap K, Shands AR, Jr., Hollister LC, Jr., et al. A new method fordetermination of torsion of the femur. J Bone Joint Surg (Am.) 1953;35(2): 289-311.
4. Gibson RD. Anteversion of femoral neck. A method of measurement.Aust Radiol. 1967; 11(2): 163-9.
5. Herrlin K, Ekelund L. Radiographic measurements of the femoralneck anteversion. Comparison of two simplified procedures. Acta OrthopScand. 1983; 54: 141-47.
6. Kingsley PC, Olmsted KL. A study to determine the angle of anteversionof the neck of the femur. J Bone Joint Surg (Am). 1948; 30(3): 745-51.
7. Reikeras O, Bjerkremim I, Kolbenstvedt A. Anteversion of the ac-etabular and femoral neck in normal and in patients with osteoarthritis ofthe hip. Acta Orthop Scand. 1983; 54: 18-23.
8. Ogata K, Goldsand EM. A simple biplanar method of measuring femo-ral anteversion and neck shaft angle. J Bone Joint Surg (Am). 1979;61(6): 546-50.
9. Hubbard DD, Staheli LT. The direct radiographic measurement offemoral torsion using axial tomography. Technique and comparison withan indirect method. Clin Orthop. 1972; 86: 16-20.
10. Ruwe PA, Gage JR, Ozonoff MB, et al. Clinical determination offemoral anteversion. A comparison with established techniques. J BoneJoint Surg (Am). 1992; 74(6): 820-30.
11. Ruby L, Mital MA, O’Connor J, et al. Anteversion of the femoralneck. Comparison of methods of measurement in patients. J Bone JointSurg (Am). 1979; 61(1): 46-51.
12. Terjeson T, Anda S. Femoral anteversion in children measured byultrasound. Acta Orthop Scand. 1987; 58: 403-7.
13. Murphy SB, Simon SR, Kijewski PK, et al. Femoral anteversion. JBone Joint Surg (Am). 1987; 69(8): 1169-76.
14. Miller F, Merlo M, Liang Y, et al. Femoral version and neck shaftangle. J Paediatr Orthop. 1993; 13: 382-8.
AV MAHESHWARI, AK JAIN, MP SINGH, SK BHARGAVA

Background: Arthroscopic partial meniscectomy is the treatmentof choice for meniscal tears. The ultimate effect of meniscectomyon the joint has been controversial.Methods: This study was done to determine the short and long-term end results of arthroscopic partial meniscectomy. The resultswere assessed on the basis of Lysholm scoring and Tapper andHoover scoring systems. Detailed questionnaires including differentcriteria like pain, swelling, locking etc. were sent to 323 patientswith meniscal injuries. One hundred and sixty five patientsresponded to the questionnaire. The patients were categorizedas long term for more than 2 years and short term for 2 years orless of follow up. Patients who underwent reconstruction of anteriorcruciate ligament were excluded from the study.Results: The best clinical results were observed in patients whowere operated within 3 months after injury (81.25% excellent &good results). Patients below the age of 40 showed consistentlybetter results than those above the age of 40 years. Associatedcartilage defects and anterior cruciate ligament rupture vitiatedthe results. Results were similar for short-term and long-term.The overall scoring showed 76.06% excellent and good results inthe Lysholm scoring method and 69.72% excellent and goodresults in Tapper and Hoover scoring system.Conclusion: Arthroscopic partial meniscectomy gives good short-and long-term clinical results when performed early and in patientsbelow the age of 40 years for meniscal injuries. Cartilage damageand anterior cruciate ligament injury vitiated clinical end results.Key-words: Meniscal tear; Arthroscopic surgery; Partialmeniscectomy; Anterior cruciate ligament tear; Cartilage defects.
Introduction
The advantages of arthroscopy in the diagnosis andtreatment of meniscal lesions has been accepted for a decade
Short and long term results of arthroscopic partialmeniscectomyP Sripathi Rao, Sharath K Rao, Shyamasunder Bhat NDepartment of Orthopaedics, Kasturba Medical College, Manipal
P Sripathi Rao, MS (Orth), D Orth, ProfessorSharath K Rao MS (Orth), Additional ProfessorShyamasunder Bhat N, MS (Orth), DNB(Orth), Assistant ProfessorDepartment of Orthopaedics, Kasturba Medical College, ManipalDr. Shyamasunder Bhat N, Assistant Professor, Department of Orthopaedics,Kasturba Medical Col lege, Manipal – 576 119, India E-mai l :[email protected] **
now. The first meniscal tear to be partially excised underarthroscopic control was performed in Tokyo in 19621 .Arthroscopic partial meniscectomy allows the detection andremoval of multiple unstable fragments by probing themeniscal remnant under direct vision2 . The majordisadvantage of closed meniscal surgery is its technicaldifficulty while being learnt.
Anatomical forms of the tears include the posterior horntear, the incomplete tear which locks the joint, the completetear which allows full extension and rupture of socket handleitself3. Multiple bucket handle tears of the posterior horn ofthe medial meniscus with peripheral separation can occur4.In some of the patients with tears of the meniscus combinedwith rupture of the anterior cruciate ligament, partialmeniscectomy itself is enough to cure the symptoms ofinstability5.
Many authors have emphasized the advantages of closedas compared with open meniscectomy 6. The aim ofarthroscopic meniscectomy is to remove all ruptured andoffending tissue and to save as much as functioning meniscaltissue with a peripheral rim7. Arthroscopic partialmeniscectomy has been shown to have advantages over totalmeniscectomy in terms of recovery from operation and thelate appearance of radiographic changes 7.
The orthopaedic literature is replete with confusing andcontradictory statements regarding ultimate effect ofmeniscectomy on the live joint. At one extreme is the direprediction that degenerative arthritis and dissolving areinevitable after meniscectomy 8, on the other hand the kneefunction of patients over 60 years have been reported asgood or excellent7.
This study was undertaken to determine the short andlong-term results of arthroscopic partial meniscectomy andto access the difference in clinical results due to associatedcartilage defects and anterior cruciate ligament rupture.
Materials and methods
Detailed questionnaires were sent to 323 patients withmeniscal injuries who were treated arthroscopically atKasturba Hospital, Manipal till December 1998. We received
158 INDIAN JOURNAL OF ORTHOPAEDICS
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 158-161

VOL. 38, NO. 3, JULY 2004 159
163 replies. Twenty-three patients who subsequentlyunderwent anterior cruciate ligament reconstruction wereexcluded from the study.
The total number of patients included was 140 of which127 were males and 13 were females; 55 were left, 82 wereright and 3 were bilateral. The mechanisms of injury of thesepatients included sports related injuries - 47 knees (32.9 %),road traffic accidents - 23 knees (16.1 %) and other injuries /no trauma - 73 knees (51.0 %)
Table I. Lysholm Knee Scoring1) Limp (5 points)
None - 5Slight or periodical - 3Severe or constant - 0
2) Support (5 points)None - 5Stick or crutch - 2Weight bearing impossible - 0
3) Locking (15 points)No locking and no catching sensation - 15Catching sensation but no locking - 10Locking occasionally - 6Locking frequently - 2Locked joint on examination - 0
4) Instability (25 points)Never giving way - 25Rarely during athletics or other severe exertion - 15Occasionally in daily activities - 10Often in daily activities - 5Every step - 0
5) Pain (25 points)None - 25Inconsistent and slight during severe exertion - 20Marked during severe exertion - 15Marked on or after walking more than 2 km - 10Marked on or after walking less than 2 km - 5Constant - 0
6) Swelling (10 points)None - 10On severe exertion - 6On ordinary exertion - 2Constant - 0
7) Stair Climbing (10 points)No problem - 10Slight impaired - 6One step at a time - 2Impossible - 0
8) Squatting (5 points)No problem - 5Slight impaired - 4Not beyond 90 degrees - 2Impossible - 0
The response of the patients were analysed by Lysholm9
score (Table I) and grading system of Tapper and Hoover8
(Table II). Based on the patients’ replies, scores werecalculated according to Lysholm Scoring System and graded
according to Tapper and Hoover system. The results weregraded on the basis of patient’s symptoms and disability.The results were analysed using t test and one way analysisof variance.
Table II. Tapper and Hoover System
Excellent: The patient had no symptoms and no disability related to his knee.
Good: The patient had minimum symptom, such as aching or weaknessafter heavy use/exertion, but there was essentially no disability.
Fair: The patient had symptoms, which had become enough of a prob-lem to interfere somewhat with daily activities and though active,could not participate in vigorous sports.
Poor: The symptoms were severe and included pain at rest, limitedmotion and locking. He was disabled, and all activities includingwalking were definitely limited because of his knee.
Results
These 140 patients (143 knees) had a follow up periodranging from 10 months to 63 months (Mean 32.98 months).Depending on the period of follow-up, they were categorizedinto short term (2 years or less) and long term (more than 2years). Eighty-eight knees were included in the short-termfollow up group and the remaining 55 were in long-term followup group. In 70 knees medial meniscus was torn, in 51 kneeslateral meniscus was torn and in 22 knees both menisci weretorn.
Age: According to Tapper and Hoover grading, patientsbelow the age of 40 years showed better results (Fig 1). ForLysholm scores, there was no statistical significance whilecomparing patients below and above the age of 40 years i.e.,p = 0.052 (null hypothesis accepted). In the short-term group,there was no significant difference between the two agegroups (p = 0.7), however there was significant difference inthe long-term group (p = 0.02).
13
2
58
27 28
81
6
0
10
20
30
40
50
60
No
. of
Kn
ees
Excellent Good Fair Poor
<40 Years>40 Years
Fig 1. Results according to the age of the patient (Tapper andHoover)
P SRIPATHI RAO, SHARATH K RAO, SHYAMASUNDER BHAT N

INDIAN JOURNAL OF ORTHOPAEDICS160
Duration of symptoms: The knees with less than 3 monthsof symptoms had 81.3% good and excellent results incomparison with 61.8% good and excellent results with morethan 2 years of symptom duration (Fig 2).
Associated anterior cruciate ligament tear: Those kneeswith intact anterior cruciate ligament had 78.1% excellent andgood results and those with anterior cruciate ligament tearhad 61.4% excellent and good results (Fig 3).
Associated cartilage damage: Associated cartilagedamage vitiated end results. Those knees with normal articularcartilage had 73.2% excellent and good results whereas thosewith cartilage damage had 63% excellent and good results(Fig 4).
Associated anterior cruciate ligament tear and cartilagedefects: In patients with intact anterior cruciateligament,presence or absence of cartilage damage did not alter the endresults (p = 0.12). In anterior cruciate ligament deficient kneesbetter results were seen without cartilage defects (p = 0.004).
Type of tear: Among the 127 knees with isolated medialmeniscal tear or lateral meniscal tear, those with bucket handletear, longitudinal tear and radial tear had 82.2%, 52.8% and70% excellent and good results respectively; whereas 66.7%of knees with degenerative tear had fair and poor results(Table III).
Table III. Results of different types of meniscal tear
Type of Tear Excellent Good Fair PoorBucket Handle 6/45 (13.3%) 31/45 68.9%) 7/45 (15.6%) 1/45 (2.2%)Longitudinal 2/36 (5.6%) 17/36 (47.2 %) 8/36 (22.2%) 9/36 (25%)Radial 0/10 (0%) 7/10 (70%) 3/10 (30%) 0/10 (0%)Degenerative 0/9 (0%) 3/9 (33.3%) 3/9 (33.3%) 3/9 (33.3%)
Other types 4/27 (14.8%) 16/27 (51.9%) 6/27 (22.2%) 1/27 (3.7%)
Duration of follow up: The results were slightly better inthe short term group (70.9% excellent and good) than longterm group (69.3% excellent and good) (Fig 5).
There was no statistically significant difference inLysholm scores, for short and long-term follow up (p = 0.622);however, patients less than 40 years of age showed betterlong term results (p = 0.02).
Discussion
We are fully cognizant of the pitfalls of a retrospectivequestionnaire study. Only about half of the patients did notreply and there is no way to ascertain that their results wouldhave been identical with those who replied. In the series of494 questionnaires sent by Tapper and Hoover8 with thecorrection for unclaimed letters (returned by the post office),35% returned for examination, 36% replied by questionnaireonly and 30% did not reply.
We have not analysed physical and radiological findingsin this study. Our purpose was to determine the subjectiveend results after arthroscopic partial meniscectomy. The scoredesigned by Tapper and Hoover is the more generalassessment of knee function without focus on specificproblem but is still regarded as reliable for the assessment of
64
33
17
710
2 3
0
5
10
15
20
25
30
35
No
. of
Kn
ees
Excellent Good Fair Poor
< 3 Months> 2 Years
Fig. 2. Results according to the duration of symptoms (Tapper andHoover)
96
34
51
25
11
2 5
0
10
20
30
40
50
60
No
. of
Kn
ees
Excellent Good Fair Poor
ACL TearACL Intact
Fig 3. Results according to tear or intactness of anterior cruciateligament (Tapper and Hoover)
3
12
26
59
11
25
61
0
10
20
30
40
50
60
No
. of
Kn
ees
Excellent Good Fair Poor
CartilageDamageNormalCartilage
Fig 4. Results according to presence or absence of cartilage damage(Tapper and Hoover)
SHORT AND LONG TERM RESULTS OF ARTHROSCOPIC PARTIAL MENISCECTOMY

VOL. 38, NO. 3, JULY 2004 161
knee joints with meniscal lesions10. Partial meniscectomy incombination with the minimal invasive technique ofarthroscopic surgery proves to be an extraordinary effectivesurgical procedure. Real long-term results do not exist yet inliterature because of the still relatively young age of thissurgical technique10.
Tapper and Hoover8 studied the age at the time of openmeniscectomy. In their study, patients who were 20 years orless at the time of operation had significantly fewer excellentor good results than those twenty one and over (p<0.01).Our study showed better results in patients who were lessthan 40 years of age than those more than 40 years.
As expected and akin to earlier reports, the duration ofsymptoms preoperatively seemed to have bearing on the endresults11. Even then, adequate time can be allowed for recoveryfrom the initial injury to ensure accuracy of diagnosis. Thelonger one waits, the more episodes of locking the patienthas, the more specific the diagnosis and the more precise theoperation. Good results occurring after delay in treatment intheir study may possibly be explained by better diagnosis 8.However, we feel that better results will be seen when theduration of symptoms is short as shown in our study.
Cave (as cited by Tapper and Hoover8) stated that anuncomplicated meniscal tear should have 100% cure aftersurgical treatment and that, if it doesn’t, the patient musthave had associated ligament tear. He also noted that cartilagedamage and anterior cruciate ligament rupture are associatedwith poor end results. About 40% of patients withuncomplicated meniscectomy will eventually have a normally
functioning knee and 10% will have a bad outcome.Remaining 50% will have varying degrees of symptoms anddisability8. Schimmer et al10 demonstrated that isolatedmeniscal tears had 94.8% good and excellent results evenafter a mean follow up of 12 years. They also state that highestimpact on the long-term results arises from additional lesionsin the knee joint, in particular cartilage damage or ligamentinjuries. Our study also showed better results in kneeswithout cartilage damage and anterior cruciate ligament tear.
In conclusion, patients below the age of 40 years showconsistently better long-term results than those above 40years after arthroscopic partial meniscectomy. Early partialmeniscectomy yields better short and long-term results.Cartilage defects in anterior cruciate ligament deficient kneesvitiate end results of arthroscopic partial meniscectomy.
References
1. Carson RW. Arthroscopic meniscectomy. Orthop Clin North Am. 1979;10: 619-627.
2. Tregonning RSA. Closed partial meniscectomy – early results forsimple tears with mechanical symptoms. J Bone Joint Surg (Br). 1983;65: 378-387.
3. Dandy DJ. The bucket handle meniscal tear – a technique detachingthe posterior segment first. Orthop Clin North Am. 1982; 13: 369-385.
4. Shakespeare DT, Rigby HS. The bucket-handle tear of the meniscus– a clinical and arthrographic study. J Bone Joint Surg (Br.) 1983; 65:383-387.
5. Paterson FWN, Trickey. Meniscectomy for tears of the meniscuscombined with rupture of the anterior cruciate ligament. J Bone JointSurg (Br). 1983; 65: 388-390.
6. Simpson DA, Thomas NP, Aichroth PM. Open and closed meniscec-tomy – a comparative analysis. J Bone Joint Surg (Br). 1986; 68: 301-304.
7. Gillquist J, Hamberg P, Lysholm J. Endoscopic partial and totalmeniscectomy – a comparative study with a short term follow up. ActaOrthop Scand. 1982; 53: 975-979.
8. Tapper EM, Hoover NW. Late results after meniscectomy. J BoneJoint Surg (Am). 1969; 51: 517-526.
9. Tegner Y, Lysholm J. Rating systems in the evaluation of knee liga-ment injuries. Clin Orthop. 1985; 198, 43-49.
10. Scimmer RC, Brülhart KB, Duff C, Glinz W. Arthroscopic partialmeniscectomy: a 12 year follow up and two step evaluation of the long-term course. Arthroscopy. 1998; 14: 136-142.
11. Gear MWL. Late results of meniscectomy. Br J Surg. 1967; 54: 270-272.
7 8
32
53
14
22
25
0
10
20
30
40
50
60
No
. of
Kn
ees
Excellent Good Fair Poor
Short-term
Long-term
Fig 5. Results according to the duration of follow up (Tapper andHoover)
P SRIPATHI RAO, SHARATH K RAO, SHYAMASUNDER BHAT N

Background : Management of open fractures of tibia complexproblem. It requires stabilisation of fracture and soft tissue cover.Method: Seventeen patients of fractures both bones of leg, whosuffered open fractures at the time of initial injury and weremanaged either by external fixator or pins incorporated in plastercast with window, reported with non-union of either tibia or bothbones of leg. These patients were managed by using simpleexternal fixator-cum-compressor using Steinmann or Denham’spins and compressing the fracture site after doing the osteotomyof fibula and early weight bearing.Results : All fractures united well, however there was shorteningof 3/4 to 1 inch in these cases which was compensated by shoeraise.Conclusion : Simple fixator compressor is a simple, economicaland easy method of treatment of open tibial fractures.Key-words: Infected ununited fractures; External fixator-cum-compressor
Introduction
Tibia, being the subcutaneous bone, is more prone toopen fractures 1. The initial management of such fracture ismost important that needs thorough washing, debridement,coverage of the fracture site with skin graft or flap andstabilization as per personality of the fracture and time delayafter injury. Within 4 to 6 hours these cases can be managedwith unreamed intramedullary nailing2-4 and coverage of thefracture site with flap or skin graft. But situation is difficultwhen the patients report late with already contaminated andinfected wounds. In such cases external fixator using Schanzscrews and connecting rods, leaving the wound open; remains
Infected non-unions of tibia - management bysimple fixator - compressorZS Kundu, SS Sangwan, Sanjeev Jain, Rajeev Mittal, RC Siwach, Gaurav Bhardwaj
Department of Orthopaedics, Pt. B.D. Sharma PGIMS, Rohtak
ZS Kundu, LecturerSS Sangwan, Professor and HeadSanjeev Jain, Senior ResidentRajeev Mittal, Senior ResidentRC Siwach, ProfessorGaurav Bhardwaj, Senior ResidentDepartment of Orthopaedics, Pt. B.D. Sharma PGIMS, Rohtak (Haryana) IndiaDr ZS Kundu, 11J/7 (UH), Medical Campus, Rohtak-124001 (Haryana) **
the standard method of management5-7. Many a times thesepatients remain on fixators and the wounds are allowed toheal either with secondary intention or managed by skingrafting or flap coverage after many days and the end resultis lot of scarring, angulation and infection at fracture site5,8,9.In the developing world, pin tract infection is very commonwhich contraindicates intramedullary nailing for fear of spreadof infection from one end to the other. Plating in the scarredarea with precarious skin condition will not be possible dueto difficulty in skin closure and it may remain exposed.
The method of internal fixation usually requires asignificant surgical exposure by an invasive, technicallydemanding procedure and although joint motion is startedearly, the fixation achieved will not be sufficient to allow earlyweight bearing, which compounds the problems of causingosteoporosis and soft tissue dystrophy. Finally infectionoften persists in presence of implant10.
Ilizarov ring fixator is the best method to treat such casesbut it needs expertise, lot of experience and knowledge ofputting of various wires in the specific portals and overallassembly is quite expensive and cumbersome as well11.
Material and methods
Seventeen male patients of age ranging from 20 to 40years having infected non-unions with dystrophy andscarification at fracture site with a gap of <1 inch were includedin the study.
The apparatus
The apparatus is simple external fixator-cum-compressorhaving three units, made of stainless steel (Fig.1). The centralhexagonal part which is threaded from inside is turnbuckleand two end pieces having holes for passage of Steinmannor Denham’s pin. The two end pieces can be introduced inand out of central turnbuckle. By rotating the centralturnbuckle in one particular direction, one can achievecompression and in opposite direction, the distraction. Sothe apparatus can be used as compressor as well as distractor.But in this series we have used it as compressor only. Onefull turn of the turnbuckle will distract or compress 3mm. So
162 INDIAN JOURNAL OF ORTHOPAEDICS
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 162-165

VOL. 38, NO. 3, JULY 2004 163
one third of the full turn will be equal to 1 mm of compressionor distraction.
Method
All the operations were performed under spinal or generalanaesthesia in supine position. Infected pin tracts of previousexternal fixator were thoroughly curretted. Fracture siteopened through a small incision by raising an osteoperiostealflap and sclerotic bone was osteotomised and piece left assuch at fracture site and medullary canal at both fractureends opened. Cancellous bone grafts were put in at fracturesite. Osteotomy of fibula was done in those cases wherefibula was already united (10 in our series). Two to threeDenham’s pins / Steinmann pins were passed in proximal anddistal fragments. Denham’s pins were used in osteoporoticbones. Any angulation, if present, was corrected. The fixator-cum-compressor in the already distracted mode wasintroduced over these pin which are already passed inhorizontal plane. The fixator-cum-compressor were attachedon both sides. By rotating the central turnbuckle in thecompression mode, maximum possible compression isachieved at fracture site. The skin closure done andcompression bandage given. Gentle knee and anklemovements were done passively while the patient is underanaesthesia to break the previously formed adhesions.
Postoperative care: The limb was raised and active toes,ankle and knee movements were started immediately. Thepatient was mobilized and advised partial weight bearing fromsecond postoperative day. Pin site dressing was taught to
the patients and stitches were removed after two weeks. Afterthat patients were advised to take bath and to wash the limband pin sites with plenty of fluid. Patient were able to bearfull weight after 6 weeks and fracture united within 3 monthsperiod and fixator-cum-compression were removed after 3 to4 months i.e. after full consolidation at fracture site (Fig.2, 3).After that patients were given PTB brace for next 2 to 3 months.
Results
In total 17 patients, all males, with age ranging from 20 to40 years, were operated. All the patients had open fracture ofboth bones of leg and in 13 cases it was initially managedwith external fixator and in four cases with POP cast withwindow and wound were allowed to heal by secondaryintention. Only in two cases skin graft was done at the timeof management of fresh trauma. Non union was infected i.e.pus discharge at fracture site along with sequestrum in 11cases and in 6 cases there were infected pin tracts. Fibulawas already united in 10 cases and in rest of 7 cases it wasun-united. Non-union was in upper 1/3rd of leg in 2 cases,middle 1/3rd in 5 cases and in lower 1/3rd in 10 cases. Bonegrafting was done in 16 cases and in one case the fracturesite was only compressed. The patients were discharged fromhospital on 3rd postoperative day and allowed partial weightbearing on 2nd day and full weight bearing after 6 weeks.
Results were evaluated on the basis of criteria given byPaley et al (Table I).11
KUNDU ZS, SANGWAN SS, JAIN SANJEEV, MITTAL RAJEEV, SIWACH RC, BHARDWAJ GAURAV
Fig.1 Fixatorcum distractor /compressor.
Fig.2. Infected nonunion treated with the appratus and fibularosteotomy done to achieve compression.

INDIAN JOURNAL OF ORTHOPAEDICS164
Table I.Bone results Functional results4 criteria: Union, infection, 5 criteria: Significant limpdeformity and leg length Equinus rigidity of anklediscrepancy Soft tissue dystrophy (skin
hypersensitivity, insensitivity of sole, ordecubitus), pain, inactivity(unemployment because of leg injury orinability to return to daily activitiesbecause of leg injury).
Excellent: Union, no infection, Excellent: Active individual with none ofdeformity of less than 7° and the other 4 criteria.length discrepancy of less than2.5 cm in tibia.Good: Union + any two of the Good: Active individual with one or twoabove of other 4 criteria.Fair: Union + any one of the Fair: Active individual with 3 or 4 of theabove other criteria or an amputation.Poor: Non-union or none of the Poor: Inactive patientothers
Patients were followed up monthly till the apparatus wason and then three monthly after removal of apparatus fornext one year. Range of follow up was 2-4 years. Excellent togood results were achieved in the majority of cases (TableII).
The main complication was a superficial pin tractinfection which was well managed after good cleaning of pinsite. In two cases deeper pin tract infection needed curettageand thorough washing of pin tract.Table II.
Bone results Functional resultsExcellent 13 11Good 2 4Fair 2 2
Poor 0 0
Discussion
Open fractures of tibia are commonest due tosubcutaneous anatomical location of the bone in itsanteromedial aspect12. After open fractures in tibia, non unionis quite common due to factors like force of initial trauma,infection at fracture site, precarious blood supply, particularlyin lower 1/3rd and improper initial management at the time ofinjury. The open fractures initially are usually managed withsimple external fixator5,6 and pin tract infections are quitecommon7,13-15. Extensive management including thoroughdebridement, washing, wound coverage with skin grafting orflap and good stabilization is either delayed or not done inevery case. So the outcome is usually an ununited fracturewith scarification, angulation and infection at fracture site.
This becomes a difficult non union to manage. The fracturesite at non-union becomes sclerotic with blockage ofmedullary canal and rest of the bone becomes osteoporoticdue to non weight bearing and disuse.
Any internal fixation in such a situation in the presenceof infection becomes almost a contraindication. Althoughintramedullary nailing after thorough reaming along withremoval of sequestrae; early weight bearing and bone graftinghas been tried in such cases. But the infection spread fromone end to other along the implant and it persists for quite along time. Plating in scarred area poses the problem of skinclosure, fear of compartment syndrome and it may remainexposed and advantage of early weight bearing is also lost.Iliazarov’s ring fixator and bone transport has become thesolution for every kind of non-union, but is easier said thandone, as this needs knowledge of the instrumentation16 ,technique of application and expertise. It has its owncomplications and disadvantages like pain, pin tract infection,joint stiffness, vascular and neurological injury as describedby Paley as problems, obstacles and complications17. Personworking in periphery may not be able to use this apparatusand it is costlier also in our setup and overall assembly isquite cumbersome.
So with the idea in mind to minimize above mentionedproblems, infected ununited fractures with gaps of less thanone inch were managed by simple fixator-cum-compressorusing multiple Steinmann’s or Denham pins. It can be appliedby any surgeon in the periphery. It has advantages like:
1. It is simple, economical and easy method of treatmentand can be well used even in peripheral set up.
INFECTED NON-UNIONS OF TIBIA - MANAGEMENT BY SIMPLE FIXATOR
Fig.3. Infected nonunion with angulation managed withapparatus (maleolar screw and wire removed simultaneously).

VOL. 38, NO. 3, JULY 2004 165
2. Using 2-3 pins on each side of fracture provides quite astable construct.
3. No bigger incision is needed at fracture site so biologyis well preserved. Only small incision and a osteopriostealflap is raised for fresh cancellous bone grafts insertion.
4. Hospital stay is less and patient can be discharged from2 to 3 days after operation.
5. Early weight bearing started and after compressionfurther load sharing is possible and hence faster fracturehealing.
6. The pins are applied away from fracture site so no chancesof infection with implant at fracture site as is the casewith internal fixation.
7. Construct is very simple in comparison to ring fixatorand easy to apply and dress and cost effective.
8. No need of X-ray/image intensifier.
9. Removal of the apparatus is an OPD procedure.
10. Active knee and ankle movement can be startedimmediately and thus managing the joint stiffnesssimultaneously.
Few disadvantages of this method observed were:
1. Superficial pin sepsis in summer season is commonproblem but can be well managed with good pin sitedressing.
2. As the apparatus is applied in coronal plane so patienthas to keep the limbs part while walking and sleeping.
3. After removal of the apparatus PTB brace is needed toavoid fracture at pin site as these are 4 to 5 mm thick.
The initial results showed that the apparatus is quiteuseful for the management of infected and difficult non-unionswith a gap of less than 1 inch.
References
1. Pintore E, Maffuli N, Petriccicuolo F. Interlocking nailing for fracturesof femur and tibia. Injury. 1992; 23(6): 381-7.
2. Bone LB, Johnson KD. Treatment of tibial fractures by reaming andintramedullary nailing. J Bone Joint Surg (Am). 1986; 68: 877-86.
3. Court-Brown CM, Mcqueen MM, Quaba AA, Christu J. Lockingintrumedullary nailing of open tibial fractures. J Bone Joint Surg (Br).1991;73: 959-64.
4. Deenhan MA, Oppenheim, Auron B. Assessment of prognostic indi-cators in tibia fractures treated with unreamed interlocking intramedul-lary nails. J Orthop Trauma. 1993; 7: 162.
5. Edwards CC, Simmons SC, Browner BD, Weigel MC. Severe opentibia fractures. Results treating 202 injuries with external fixation. ClinOrthop. 1988; 230: 98-114.
6. Behrens F, Searles K. External fixation of the tibia, basic concepts andprospective evaluation. J Bone Joint Surg (Br). 1986; 68: 246-54.
7. Gershuni DH, Halma G. The AO external skeletal fixator in the treat-ment of severe tibia fractures. J Trauma. 1983; 23: 986-90.
8. Hass N, Krettek C, Schandelmaier P, Frigg R, Tscherne H. A newunreamed tibial nail for shaft fractures with severe soft tissue injury.Injury. 1993; 24(1): 44-54.
9. Henley MB, Chapman JR. Comparison of unreamed tibial nails andexternal fixators in the treatment of grade II and III open tibial shaftfractures. Orthop Trans. 1994; 19: 143-4.
10. Paley D, Catagni MA, Argnani F, Villa A, Benedett GB, Callaneo R.Ilizarov treatment of tibial non-unions with bone loss. Clin Orthop. 1999;241: 146.
11. Ilizarov GA. Clinical application of tension-stress effect for limb length-ening. Clin Orthop. 1990; 250: 8.
12. Charles TJ. Fractures of lower extremity. In: Campbell’s OperativeOrthopaedics. 8th ed. Vol.2. Mosby Year Book, 1992: p.785-893.
13. Kimmel RB. Results of treatment using the Hoffman external fixator forfracture of the tibial diaphysis. J Trauma. 1972; 12: 756-61.
14. Melendez EM, Colon C. Treatment of open tibial fractures with theorthofix fixator. Clin Orthop. 1989; 241: 224-30.
15. Rosenthal RE, Macphail JA, Ortiz JE. Non-union in open tibial frac-tures - Analysis of reasons for failure of treatment. J Bone Joint Surg(Am). 1977; 59-A(2): 244.
16. Fleming B, Paley D, Kristiansen T, Pope M. A biomechanical analy-sis of Ilizarov external fixator. Clin Orthop. 1989; 241: 95.
17. Paley D. Problems, obstacles and complications of limb lengthening byIlizarov technique. Clin Orthop. 1990; 250: 81-104.
KUNDU ZS, SANGWAN SS, JAIN SANJEEV, MITTAL RAJEEV, SIWACH RC, BHARDWAJ GAURAV

Background: Displaced supracondylar fractures of the humerusin children are common injuries treated by orthopedic surgeons.Amongst the various methods used for treating these fracturesclosed reduction and crossed pin fixation has shown improvedresults.Method: One hundred ninety seven cases with Gartland grade IIand grade III supracondylar humeral fractures were treated withclosed reduction and percutaneous crossed pin fixation withKirschner wire and followed up for a minimum period of twoyears .Results: Patients were assessed on the basis of Flynn’s criteria.There were 145 excellent and 41 good results.Conclusion: It is concluded that closed reduction and crossedpin fixation is a sound and effective treatment for displacedsupracondylar fractures with several advantages but requirescareful judgement on the part of surgeon to avoid complicationsKey-words: Displaced supracondylar fractures; Closedreduction; Crossed pin fixation
Introduction
Supracondylar fractures of humerus account for 60% ofall fractures about the elbow in children1,2 and representapproximately 3% of all fractures in children3.
Many methods have been proposed for the treatment ofsupracondylar fractures of humerus in children: manipulativereduction and immobilization in a plaster cast with elbowflexed4,5 , axial skeletal traction on the ulna with the elbowflexed5,6,7, Dunlop’s skin traction7 , closed reduction andpercutaneous pinning1,3,8-12 and open reduction and internalfixation9,10. Treatment of this displaced fracture is fraught
Crossed pin fixation in displaced supracondylar humerusfractures in childrenUB Yadav, R Singhal, G Tonk, T Aggarwal, AN Verma
Department of Orthopedics, Motilal Nehru Medical College, Allahabad
Uday Bhan Yadav, MS (Orth), LecturerRohit Singhal, MS (Orth), Ex Junior ResidentGyaneshwar Tonk, MS (Orth), Ex Junior ResidentTribhuwan Aggarwal, MBBS Jr. ResidentA N Verma, MS (Orth), Professor and HeadDepartment of Orthopedics, Motilal Nehru Medical College AllahabadDr. Udaybhan Yadav, L-12, Lecturer Niwas, MLN Medical College CampusAllahabad-211001 **
with many complications including Volkmann’s Ischaemiccontracture 13, nerve injury14, arterial injury, skin slough andcubitus varus2.
Closed reduction and percutaneous crossed Kirschnerwire fixation was initially described by Swenson15 and laterpopularized by Flynn et al8. Because of the concern aboutpossible ulnar nerve injury iatrogenically caused by themedial pin14, other authors 3,9 have advocated that the closedreduction be stabilized by parallel lateral pins. HoweverSwenson technique of crossed pin fixation continues to beused today with excellent results and low morbidity. It isbiomechanically most stable as compared to other pinconfigurations6,16.
The purpose of the study was to evaluate the role ofclosed reduction and percutaneous crossed pin fixation indisplaced supracondylar fractures and to design a simpleand effective protocol for the treatment of these fractures.
Material and Methods
A total of 197 cases with supracondylar fractures werestudied prospectively. All the fractures were closed, unilateraland opposite elbow was taken as control for comparison.
The indication for crossed pin fixation was Gartland4
grade II and grade III displaced fractures. Out of the total 197of fractures, 101 were grade II and 96 were grade III. Fracturesolder than 7 days were not included. There were 126 malesand 71 females. The age of the patients ranged from 3 -13years (mean age 8 years). Left elbow was involved in 128cases and right side in 69 cases. One hundred thirty eighthad postereomedial displacement and 59 had posterolateraldisplacement. Associated injuries and complications wereboth bones fracture forearm in 28 cases radial nerve injury in11 cases, absent / feeble pulses in 21 cases and impendingcompartment syndrome in 9 cases
With the patient under general anaesthesia and in supineposition, closed reduction of supracondylar fracture wasdone. Reduction was checked by fluoroscopy and Baumann’sangle was compared with opposite side. If the difference ofmore than 5o was observed, remanipulation was done. If thelandmarks were obliterated by swelling, a few moments of
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 166-169
166 INDIAN JOURNAL OF ORTHOPAEDICS
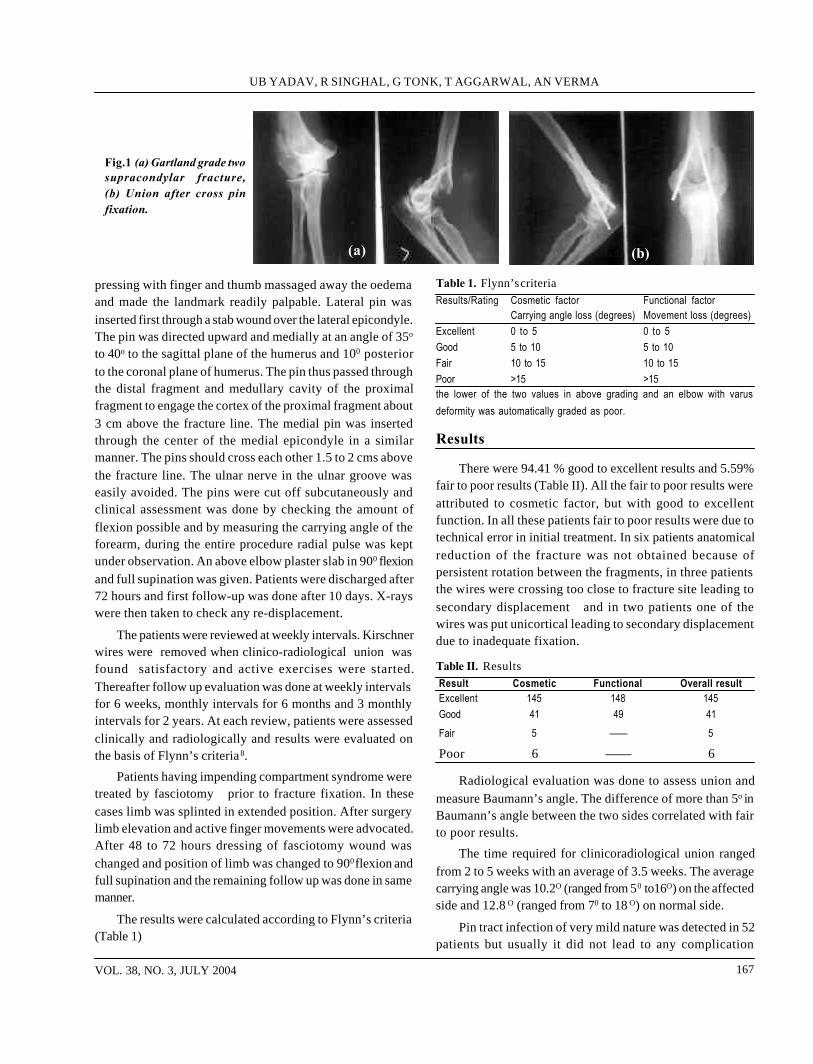
VOL. 38, NO. 3, JULY 2004 167
pressing with finger and thumb massaged away the oedemaand made the landmark readily palpable. Lateral pin wasinserted first through a stab wound over the lateral epicondyle.The pin was directed upward and medially at an angle of 35o
to 40o to the sagittal plane of the humerus and 100 posteriorto the coronal plane of humerus. The pin thus passed throughthe distal fragment and medullary cavity of the proximalfragment to engage the cortex of the proximal fragment about3 cm above the fracture line. The medial pin was insertedthrough the center of the medial epicondyle in a similarmanner. The pins should cross each other 1.5 to 2 cms abovethe fracture line. The ulnar nerve in the ulnar groove waseasily avoided. The pins were cut off subcutaneously andclinical assessment was done by checking the amount offlexion possible and by measuring the carrying angle of theforearm, during the entire procedure radial pulse was keptunder observation. An above elbow plaster slab in 900 flexionand full supination was given. Patients were discharged after72 hours and first follow-up was done after 10 days. X-rayswere then taken to check any re-displacement.
The patients were reviewed at weekly intervals. Kirschnerwires were removed when clinico-radiological union wasfound satisfactory and active exercises were started.Thereafter follow up evaluation was done at weekly intervalsfor 6 weeks, monthly intervals for 6 months and 3 monthlyintervals for 2 years. At each review, patients were assessedclinically and radiologically and results were evaluated onthe basis of Flynn’s criteria8.
Patients having impending compartment syndrome weretreated by fasciotomy prior to fracture fixation. In thesecases limb was splinted in extended position. After surgerylimb elevation and active finger movements were advocated.After 48 to 72 hours dressing of fasciotomy wound waschanged and position of limb was changed to 900 flexion andfull supination and the remaining follow up was done in samemanner.
The results were calculated according to Flynn’s criteria(Table 1)
Table 1. Flynn’s criteriaResults/Rating Cosmetic factor Functional factor
Carrying angle loss (degrees) Movement loss (degrees)Excellent 0 to 5 0 to 5Good 5 to 10 5 to 10Fair 10 to 15 10 to 15Poor >15 >15the lower of the two values in above grading and an elbow with varusdeformity was automatically graded as poor.
Results
There were 94.41 % good to excellent results and 5.59%fair to poor results (Table II). All the fair to poor results wereattributed to cosmetic factor, but with good to excellentfunction. In all these patients fair to poor results were due totechnical error in initial treatment. In six patients anatomicalreduction of the fracture was not obtained because ofpersistent rotation between the fragments, in three patientsthe wires were crossing too close to fracture site leading tosecondary displacement and in two patients one of thewires was put unicortical leading to secondary displacementdue to inadequate fixation.
Table II. ResultsResult Cosmetic Functional Overall resultExcellent 145 148 145Good 41 49 41
Fair 5 —— 5
Poor 6 —— 6
Radiological evaluation was done to assess union andmeasure Baumann’s angle. The difference of more than 5o inBaumann’s angle between the two sides correlated with fairto poor results.
The time required for clinicoradiological union rangedfrom 2 to 5 weeks with an average of 3.5 weeks. The averagecarrying angle was 10.2O (ranged from 50 to16O) on the affectedside and 12.8 O (ranged from 70 to 18 O) on normal side.
Pin tract infection of very mild nature was detected in 52patients but usually it did not lead to any complication
Fig.1 (a) Gartland grade twosupracondylar fracture,(b) Union after cross pinfixation.
(a) (b)
UB YADAV, R SINGHAL, G TONK, T AGGARWAL, AN VERMA

INDIAN JOURNAL OF ORTHOPAEDICS168
because in most of the cases Kirschner wire were removed in3-5 weeks and infection healed without any activeintervention. Ulnar nerve injury was found in six cases. Ofthese six cases, three cases were detected in the immediatepost operative period. One case was deteced as delayedneuropathy of ulnar nerve due to its stretching over themedial pin and in two cases ulnar nerve injury took placewhile withdrawing the pin. In all the cases nerve injury wasmainly of sensory type, no exploration of the nerve was triedin any case. All the cases recovered spontaneously withoutany neurological deficit with in 3-6 weeks.
Discussion
Displaced supracondylar fratures of the humerus are oneof the commonest childhood injuries and good comesticresults and functional recovery are the goals of the treatment.
Although good results have been reported using variousmethods of treatment but high incidence of cubitus varusdeformity remains a significant problem. With closedreduction and cast immobilisation the reported incidence ofcubitus varus defortmity is as high as 24 %5. Studies showpoorest functional and cosmetic outcome with this modalityof treatment12. The result of skeletal traction treatment forthese fractures have been varied. The incidence of cubitusvarus deformity with this modality of treatment varies 0 to57%15,18. Other disadvantages of skeletal traction includeprolonged hospital stay, pin tract infection, ulnar nerve injuryduring insertion of traction pin and elbow stiffness16. Theresults of open reduction and internal fixation have also beenvaried with an incidence of cubitus varus deformity rangingfrom 0 to 35%5. Persistent elbow stiffness after open reductionis also reported19.
Percutaneous pinning after closed reduction ofsupracondylar fractures has got several advantages.Immediate fixation of these fractures reduces the duration ofhospital stay. The technique provides anatomic and stablefixation which prevents cubitus varus deformity. In the
developing countries many patients present with history ofmanipulation and massage. These cases have a high incidenceof compartment syndrome and myositis ossificans. Thissituation poses a dilemma for the surgeon, whether to increasestability of closed reduction by hyperflexion which mayincrease circulatory compromise or whether to apply Dunlop’straction till the swelling subsides. If the fracture is fixedimmediately after closed reduction it can be splinted in a safeposition without any fear of loss of reduction. This minimizesthe risk of compartment syndrome and maximizes circulationOur views and results were in concordance with several otherstudies 4,9,10,13,14.
Swenson1 reported excellent results using crossed pinfixation, but others7 have suggested the pins placed from thelateral condyle in a parallel or crossed configuration tominimize the risk of iatrogenic ulnar nerve injury. Althoughinjury to ulnar nerve from the medial pin is a major concern,its incidence is estimated to be 2% to 3% 6. Recent studiescomparing the relative strength of fixation afforded bydifferent configurations of pin placements have crossedmedial and lateral pins to be the most stable configurationsbiomechanically8,9.
However, Kirschner wire fixation has its owndisadvantages. Complications such as ulnar nerve injury9,11,13.wire extrusion, pin tract infection 4 and heterotropicossification4,9,13 have been reported . Cubitus varus deformityafter this modality of treatment can be prevented by strictlyfollowing the surgical technique. It is usually due to reductionof fixation of fragments in poor position and improperplacement of Kirschner wires9,10,11,13.
From the present study it could be concluded that closedreduction and percutaneous crossed pin fixation is a soundand effective modality for the treatment of displacedsupracondylar fractures. With the advantages of decreasedduration of hospital stay, stable fixation and early mobilizationit also reduces the incidence of cubitus varus deformity if thesurgical technique is followed strictly.
Fig.2 (a) Gartland gradethree supracondylar fracture,(b) Union after cross pinfixation.
(a) (b)
CROSSED PIN FIXATION IN DISPLACED SUPRACONDYLAR HUMERUS FRACTURES IN CHILDREN

VOL. 38, NO. 3, JULY 2004 169
References
1. Mostafavi HR, Spero C. Crossed pin fixation of displaced supracondy-lar humerus fractures in children. Clin Orthop. 2000; 376: 56-61.
2. D’Ambrosia RD. Supracondylar fractures of humerus - prevention ofcubitus varus. J Bone Joint Surg (Am). 1972; 54: 60-66.
3. Aronson DD, Prager BI. Supracondylar fractures of the humerus inchildren –a modified technique of closed pinning. Clin Orthop. 1987;219: 174-184.
4. Gartland JJ. Management of supracondylar fractures of the humerusin children. Surg Gynecol Obstet. 1959; 109: 145-154.
5. Herzenberg Jt, Koreska J , Carroll NC , Rang M. Biochemicaltesting of fixation technique for pediatric supracondylar elbow fractures.Orthop Trans. 1988:12: 678-679.
6. Dodge HS. Displaced supracondylar fractures of the humerus in chil-dren - treatment by Dunlop’s traction. J Bone Joint Surg (Am) 1972; 54:1408-1418.
7. Ippolito E, Caterini R ,Scola E. Supracondylar fractures of the hu-merus in children - analysis at maturity of fifty three patients treatedconservatively. J Bone Joint Surg (Am). 1986; 68: 333-44.
8. Flynn JC, Matthews JG, Benoit RC. Blind pinning of displaced supra-condylar fracture of the humerus in children- sixteen years’ experiencewith long term follow-up. J Boint Joint Surg (Am). 1974; 56 (A): 263-272.
9. Mazda K, Boggione C, Fitoussi F , Pennecot GF. Systematic pin-ning of displaced extention–type Supracondylar fractures of the hu-merus in children –A prospective study of 116 consecutive patients . JBone Joint Surg (Br). 2001; 83:888-893.
10. Davis RT, Gorczyca JT, Pugh K. Supracondylar humerus fractures inchildren– comparison of operative treatment method. Clin Orthop. 2000;376: 49-55.
11. Pirone AM, Graham HK, Krabich JI. Management of displacedextention type supracondylar fractures of humerus in children. J BoneJoint Surg (Am). 1988; 70: 641-650
12. Boyd DW, Aronson DD. Supracondylar fractures of the humerus –aprospective study of percutaneous pinning. J Pediatr Orthop. 1992; 12:789-794.
13. Mubarak SJ, Carroll NC. Volkmann’s contracture in children – aetiol-ogy and prevention. J Bone Joint Surg (Am). 1979; 61: 285-293.
14. Royce RO, Dutkowsky TP, Kasser JR, Rand FR. Neurologic compli-cations after K wire fixation of supracondylar fracture of humerus inchildren J Pediatr Orthop. 1991;11: 191-194.
15. Zoints LE, McKellop HA ,Hathaway R. Torsional strength of pinconfigurations used to fix supracondylar fracture of the humerus inchildren. J Bone Joint Surg (Am). 1994; 76: 253-256.
16. Charnley J. The closed treatment of common fractures . 4th.ed. Cam-bridge : Colt Books .1999; 105 -115.
17. Piggot J, Graham HK, McCoy GF. Supracondylar fractures of thehumerus in children - treatment by straight lateral traction. J Bone JointSurg (Am). 1986; 68: 577-583.
18. Swenson AL. The treatment of supracondylar fractures of the humerusby Kirschner wire transfixion. J Bone Joint Surg (Am). 1948; 30: 993 -997.
19. Wilkins KE. Fractures and dislocations of the elbow region In Fracturesin children vol.3. Ed. Rockwood CA Jr. Wilkins KE, King RE. Philadel-phia: JB.Lippincott. 1991:575-576.
UB YADAV, R SINGHAL, G TONK, T AGGARWAL, AN VERMA

Background: Joint stiffness especially of upper limb jointsfollowing trauma may lead to psychological problems.Method: This study was carried out on twenty-six consecutivepatients between 18-45 years of age, of post-traumatic jointstiffness (PTJS) in upper extremity, to determine the type ofcoping mechanism and its effect on their quality of life. Copingchecklist1 and WHO QOL-Brief Version2 questionnaires were usedto assess the coping strategies and quality of life of these patients.Results: Critical analysis of the data revealed that these patientscommonly employed coping strategies like problem solving, positivecognition, avoidance, religious and magical thinking in that order.Conclusion: The correlation analysis between the scores ofcoping strategies and quality of life showed that patients, whowere high on avoidance coping skills, had better psychologicalfunctioning where as those who were high on external attribution,had low physical health.Key words: Post-traumatic joint stiffness; Upper limbs; Copingstrategies; Quality of life.
Introduction
With the increase in high-speed vehicular trauma, thenumber of patients with multiple fractures includingintraarticular fractures and associated soft tissue injury hasgone up considerably. This has led to considerable morbidityafter the completion of the treatment. Joint stiffness is one ofthe important fall-outs of such injuries. Upper extremityfractures may result in ankylosis of the joints such asshoulder, elbow or hand, which may be quite disabling at
Coping mechanism and its correlation with quality of life inupper limb post traumatic joint stiffness patientsAditya Aggarwal, Adarsh Kohli, ON Nagi, Arun Kumar
Department of Orthopaedic Surgery and Psychiatry, Postgraduate Institute of Medical Education andResearch, Chandigarh
Aditya Aggarwal, MS, DNB, Assistant ProfessorON Nagi, MS, MSc (Oxon), FAMS, Professor and HeadDepartment of Orthopaedic SurgeryAdarsh Kohli, Ph D, Associate ProfessorArun Kumar, MPhil, Social ScientistDepartment of PsychiatryPostgraduate Institute of Medical Education and Research,Chandigarh 160 012Dr. Aditya Aggarwal, # 123-C, Sector 24-A, Chandigarh 160023; **Email: [email protected]
times. This stiffness may hamper routine as well as certainother activities. The functional disability is more marked ifdominant upper limb is affected. Such patient may resort todifferent coping mechanism in order to deal with the situation.
Coping is a process involving efforts on the way towardssolution of the problem. Researchers have systematicallyexamined coping strategies among different people. Someways of coping seem to be better suited to certain kinds ofsituation than others. Coping would occur when an individualconfronts a fairly drastic change or problem that defiesfamiliar ways of behaving, requires the production of newbehaviour and very likely gives rise to uncomfortable effortslike anxiety, despair, guilt, shame or grief, the relief of whichforms part of the needed adaptation.
Pearlin and Schooler3 reported that coping is a behaviourthat protects people from being psychologically harmed byproblematic social experience. They further added that copingprotects by a) eliminating or modifying stresses, b)perpetually controlling the meaning of stressful experience,thus neutralizing its problematic character, or c) keepingemotional consequences within manageable bounds.
Quality of life (QOL) is an important issue for the largenumber of patients who may need to adapt to severe andchronic disability due to joint stiffness. The loss of mobilityin the joints makes patient more dependent on others whichaffects their quality of life. Measuring quality of life canprovide a detailed assessment of physical disability andtreatment effects as well as the global impact of those effectson the person’s daily life.
The data of QOL might be useful to predict patient’sresponse to future treatment or for taking important decisionfor future treatment. For example, Hawker et al4 found thatboth generic and disease specific QOL measurements wereof value in assessing the well-being of patients receivingknee replacement surgery. Their findings demonstrate theabsolute necessity of considering each person’s individualassessment of what makes life worth living for them. Twopeople with the very same objective health status can have
170 INDIAN JOURNAL OF ORTHOPAEDICS
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 170-174

VOL. 38, NO. 3, JULY 2004 171
very different QOL, due to difference in expectations andcoping ability.
Very few studies are available concerning thepsychological variables in patients with orthopaedicproblems. Previous studies are mainly on coping mechanismsin osteoarthritis 5 and psycho-educational interventions inarthritis 6. Thus the present study was conducted to determinethe quality of life and the coping strategies and the correlationbetween them in patients of post-traumatic joint stiffness inupper extremity.
Materials and Methods
Sample
Twenty-six consecutive patients with posttraumatic jointstiffness in upper limbs attending the orthopaedic outpatientdepartment with the following inclusion and exclusion criteria,was undertaken for this study. The patients included for thestudy were in the age group of 18 to 45 years of either sex,diagnosed as having post-traumatic joint stiffness (PTJS) inupper limbs of minimum six months duration after trauma.Post-traumatic joint stiffness (PTJS) is defined as residualsignificant restriction of functional range of motion of thejoints, causing interference in the professional and/or dailyactivities. Exclusion criteria were i) patient with any chronicmedical diseases such as asthma, epilepsy, tuberculosis, heartdiseases etc., ii) patient with any past history of psychiatricillness, iii) head injury patients, iv) any neurological diseasesuch as polio, epilepsy, etc.
Instruments used
1. Sociodemographic profile sheet was used to collect thesociodemographic information i.e. name, age, sex andeducation etc. of the patient.
2. Clinical profile sheet was developed to record the clinicalfeatures such as physical deformity, range of motion ofthe joints and diagnosis.
3. WHO QOL –Brief Version2 questionnaire to measure theQOL. It covers four domains of physical health,psychological functioning, social relationships andenvironment with two additional items of general well-being.
4. Coping Checklist1 instrument was used to assess thecoping strategies like positive cognition, negativecognition, problem solving, distraction, magical thinking,avoidance, religious, help seeking and externalattribution.
Procedure
Each patient was seated comfortably and consent wastaken for participation in the study. All the questionnaireswere administered to each patient individually. Thesociodemographic, clinical features of the patients and theresponses to the coping checklist and quality of life werenoted down. The tests were administered strictly accordingto their prescribed instructions. They were assured that theirresults and the information obtained would be kept strictlyconfidential and used for research purpose only.
Results
Twenty two of 26 patients were males. Twenty weremarried and 17 of them were in the age group of 31-45 years.As per the occupational status, 4 patients were professionals,11 were from clerical background, 5 were from the skilled/semi-skilled workers and 6 were students. As per educationalstatus, 25 were literate.
Clinical examination showed that 11(42.4%) patients werebetween one to two years of duration of treatment. Eighteen(69.23%) patients underwent only one surgery. Fifteen(57.7%) patients presented with arthralgia at the time ofinterview. In terms of union of fractures, 25 (96.15%) patientsshowed complete union of fractures. One case presentedwith non-union. With regard to the presence of stiffness inthe joints, shoulder and elbow joints were predominantlyinvolved. Nineteen (73.1%) showed only one jointinvolvement (Table I).
Severity of stiffness was calculated on the basis of therange of motion of the joint with respect to the normal rangeof motion. Global rating score of 0 was given to those havingrange of motion 75% compared to normal. One was given tothose having ROM 50-75%, 2 to ROM 25-50%, and 3 to below25%.
Table II shows the percentage of coping strategies inpatients with upper limb joint stiffness. Scores are inpercentages of each coping strategy used in such patients.Table III shows mean, standard deviation and range of scoresof dimensions of quality of life. Table IV shows the inter-correlation of coping strategies and the dimensions of theQOL. Pearson’s product moment correlation was calculatedamong all the fourteen variables.
From the inter-correlation table, it can be seen thatpositive cognitive scores have correlations with:
i) Distraction (r=0.57, df=24,p<.01),
ii) Magical thinking (r=0.39, df=24, p<.05)
ADITYA AGGARWAL, ADARSH KOHLI, ON NAGI, ARUN KUMAR

INDIAN JOURNAL OF ORTHOPAEDICS172
iii) Religious (r=0.47, df=24, p<.05) and
iv) Help seeking (r=0.68, df=24, p<.01)
Scores of distraction have significant correlations with:
i) Magical thinking (r=0.50, df=24, p<.01)
ii) Religious (r=0.66, df=24, p<.01), and
iii) Help seeking (r=0.54, df=24, p<.05).
Scores of Magical thinking has significant correlationwith religious (r=0.46, df=24, p<.01).
Scores of avoidance has significant correlation withpsychological functioning (r=0.45, df=24, p<.05).
Scores of religious has significant correlation with helpseeking (r=0.49, df=24,p<.01).
Scores of external attribution has significant negativecorrelation with physical health (r=-0.54, df=24, p<.01).
Scores of physical health have significant correlationswith:
i) Psychological functioning(r=0.60, df=24,p<.01),
ii) Social relationships, (r=0.47, df=24,p<.05),
iii) Environment (r=0.60, df=24,p<.05), and
iv) General well being (r=0.75, df=24,p<.01).
Scores of psychological functioning have significantcorrelations with:
i) Social relationships (r=0.50, df=24,p<.01),
ii) Environment (r=0.72, df=24,p<.01), and
iii) General well-being (r=0.63, df=24,p<.01).
Scores of social relationships has significant correlationwith general well-being i.e. (r=0.39, df=24,p<.05).
Scores of environment has significant correlation withgeneral well being i.e. (r=0.62, df=24,p<.01).
Table III. Mean and standard deviation of the dimensions of quality of lifeQuality of Physical Psychological Social Environment GeneralLife health Functioning Relationships well beingMean 17.96 17.23 11.00 21.73 5.73SD 5.14 4.88 4.45 8.93 2.27Range of 7-35 6-30 3-15 8-40 2-10scores
Discussion
In our study the coping strategies used were mainlyproblem solving (82.8%), positive cognition (66.8%),avoidance (56.3%), religious (55.56%), and magical thinking(50.8%) in that order.
Problem solving strategies in such patients includestalking to friends and family members, doubling efforts, takingactive steps to fight out the problem, analyzing the problem,solving it in steps and taking help of guide-books etc. In astudy done with subjects with spinal cord injuries,predominantly problem solving means of coping wereutilized7.
Positive cognition is the second most used copingstrategy in such patients. In positive cognition there isacceptance, and comparing the self with others and feelingbetter off, looking at brighter side of the things to come.
Table I. Clinical features of the sample. No.(26)No. Percentages
Duration of treatment6-12 months 10 38.412-24 months 11 42.4more than two years 5 19.2
Number of Surgeries performedno surgery 1 3.9one surgery 18 69.2two or more surgeries 7 26.9
Painabsent 15 57.7present 11 42.3
State of unionunion 25 96.2delayed union 0 0.0non union 1 3.9
Joints affectedShoulder 13 50Elbow 13 50Wrist 7 26.2MP Joints 1 3.8
Number of joints affectedOne joint 19 73.1two joints 6 23.1More than two joints 1 3.9
Table II. Coping strategies used in patients having PTJS (Upperlimbs) (N=26)Coping strategies Scores in percentageProblem solving 82.8Positive cognitive 66.8Avoidance 56.5Religious 55.56Magical thinking 50.8External attribution 49.5Negative cognitive 47.11Help seeking 43.52
Distraction 43
COPING & QUALITY OF LIFE IN PTJS

VOL. 38, NO. 3, JULY 2004 173
Avoidance is the third most commonly used copingstrategies in such patients. Here the individual refuses tothink about the problem, seeks isolation, avoids being withpeople, keeps feelings to oneself. These strategies are mostlyproblem focused. It reflects cognitive and behavioralattempts to avoid telling about a stress and its implicationsor to manage the effect associated with it. Patients withosteoarthritis used problem and emotion focused strategiesto manage their problems in their day-to-day life5,8. Howeverin our study, coping strategies were more active problemfocused and less emotion focused.
Religious coping strategies were the next commonlyused, to deal with the stressful situation in the present study.In the Indian context, strategies like going to pilgrimage,attending bhajans, praying, attending religious discussions,making special offerings and reading religious or holy books,are the popular modes of adjustments. Manning9 observedthat spiritual and religious coping strategies in the form ofreappraisal of God’s power were mainly used in patients ofbreast cancer. These were positive in nature and affectedQOL and/or life situations.
Magical thinking is another most commonly copingstrategy used in such patients. Such patients believe insupernatural power, wear lockets or rings with stones, andconsult faith healers with a hope of miracle to happen. Theyalso consult the astrologers for the solution to their problem.Dalal10 observed in the orthopaedic patients that theyfrequently blame themselves and cosmic factors (fate, Karmaand God) for their health problems. Such beliefs played an
important role in various treatment related decisions madeby the patients.
Conversely the coping strategies used less frequentlyin post-traumatic joint stiffness in upper limbs were externalattribution, negative cognitive, help seeking, and distraction.Curran11 found that coping strategies characterized by worry,wishful thinking, and self-blame were associated with higherlevels of depression and anxiety. Strategies focusing onproblem solving and having a positive outlook were relatedto anxiety but to a lesser degree. Felton12 in his study showedsimilar results.
On analysis of the kind of coping strategies used inrelation to severity of illness, it was found that those withmaximum severity (grade III) were usually employing problemsolving, distraction, external attribution and avoidance in thatorder. Patients with moderate severity (grade II) revealedthe use of coping strategies like problem solving and externalattribution mainly. Those with mild severity (grade I) employedproblem solving, positive cognition and external attributionin that order.
On examining the scores of QOL of patients with PTJS,we found that they had positive inclination towards all theaspects of quality of life i.e., physical health, psychologicalfunctioning, social relationships, environment and generalwell-being.
Examining the coping strategies in relation to quality oflife, the study indicates that avoidance coping strategy leadsto better psychological functioning of the patient. On the
Table IV. Inter correlation matrix of the dimensions of coping strategies and quality of life (n=26)
Positive Negative Problem Distraction Magical Avoidance Religious Help External Physical Psychologicalcognitive cognitive Solving thinking e s Seeking Attribution health 1
Positive cognitive - -0.08 0.14 0.57** 0.39* 0.24 0.47* 0.68* 0.05 0.16 0.23Negative cognitive - -0.11 0.03 -0.08 0.24 -0.13 0.00 0.21 -0.20 -0.11Problem solving - 0.24 -0.04 0.27 0.32 0.08 -0.25 0.12 0.21Distraction - 0.50** 0.13 0.66** 0.54** 0.17 0.12 0.14Magical thinking - 0.13 0.46* 0.21 -0.06 0.23 -0.09Avoidance - 0.14 0.10 -0.18 0.22 0.45**Religious - 0.49** 0.01 0.24 -0.05Help seeking - 0.19 0.19 0.03External Attribution - 0.54** 0.03Physical health - 0.60**Psychological Functioning -Social RelationshipsEnvironmentGeneral Well being -Significant at .05 level*, significant 15 .01 level**.
ADITYA AGGARWAL, ADARSH KOHLI, ON NAGI, ARUN KUMAR

INDIAN JOURNAL OF ORTHOPAEDICS174
other hand negative correlation between external attributionand physical health shows that person who is high on externalattribution has poor physical health.
Overall analysis of the inter-correlation matrix doesn’tshow much significant correlations in the dimensions ofcoping checklist and quality of life.
An extensive search of literature has revealed no suchstudy in patients of post-traumatic joint stiffness. Thereappears to be an urgent need for intervention at the individuallevel in such cases. They need general guidelines on how tocope successfully with the problems and considerable stressdue to restriction of joints movements after trauma. Anintegrated assessment of coping skills can be useful informulating clinical case descriptions, treatment planning,and program evaluation. It can help to describe a person’scoping responses to the specific stressful life circumstances,monitor stability and change in coping responses, compareindividuals and groups, and examine how new life eventsaffect a person’s ways of coping as well as how copingresponse change an individual’s life situation and functioningand affect his quality of life.
References
1. Rao K, Prabhu GG, Subhakrishnan DK. Development of copingChecklist. Ind J Psychiatry. 1989; 31(2): 128-133.
2. WHOQOL-Brief Field trial version. Program on mental health.World health Organization; Geneva 1996.
3. Pearlin LL, Schooler C. The structure of coping. J Health SocialBehaviour. 1978; 19:2-21.
4. Hawker G, Melfi C, Paul J, Green R, Bombardier C. Comparison ofa generic (SF-36) and a disease specific (WOMAC) instrument in themeasurement of outcomes after knee replacement surgery. J Rheumatol.1995; 22:1193-1196
5. Downe-Wamboldt B. Stress, emotions, and coping: a study of elderlywomen with osteoarthritis. Health Care Women Int. 1991; 12(1): 85-98.
6. Hawley DJ. Psycho-educational interventions in the treatment of arthri-tis. Clin Rheumatol. 1995; 9(4). 803-23.
7. Wheeler G, Krausher R, Cumming C, Jung V, Steadward R,Cumming D. Personal styles and ways of coping in individuals whouse wheelchairs. Spinal Cord. 1996; 34:351-357.
8. Lazarus R, Folkman S. Stress, appraisal, and coping. New York;Springer Publishing Co. 1984.
9. Manning, Juanita K. The effects of spiritual coping on quality of lifeand life satisfaction in women with breast cancer. Dissertation AbstractInternational-B. 2001 (April); 61/10:5237.
10. Dalal AK. Living with a chronic disease: healing and psychologicaladjustment in Indian society. Psychol Dev Soc. 2000; 12(1), 67-81.
11. Curran CA, Ponsford JL, Crowe S. Coping strategies and emotionaloutcome following traumatic brain injury: A comparison with orthopedicpatients. J Head Tr Rehabil. 2000; 15(6): 1256-74.
12. Felton BJ, Revenson TA, Hinrichsen GA. Stress and coping in theexplanation of psychological adjustment among chronically ill adults.Social Sc Med. 1984; 18:889-898.
COPING & QUALITY OF LIFE IN PTJS

Background: Psychologic disturbance is known to have aninfluence on the outcome of treatment of patients with low backpain.Method: The prevalence of anxiety and depression in 145 Indianlow back pain patients was studied using the Hospital Anxiety andDepression Scale (HADS)Results: Significant correlation was found between the levels ofself reported disability and anxiety and depression which were71.7% and 64.8% respectively.Conclusion: The pain drawing was found to have a low sensitivityand positive predictive value in identifying patients with abnormalanxiety and depression.Key-words: Low back pain, psychologic disturbance, anxiety,depression, pain Drawing.
Introduction
It is well recognised that the outcome of variousinterventions including conservative treatment,1
chemonucleolysis,2 and surgery 3-6 in patients with low backpain is influenced by the presence of psychologicdisturbance.
Anxiety and depression are the two most common formsof psychologic disturbances seen in medical patients.Hospital Anxiety and Depression Scale (HADS)7 is one ofthe most widely used tools in medical practice to identifythese. Scant data is available on the prevalence of anxietyand depression in the Indian low back pain population.
The aims of the present study were i) to assess theprevalence of anxiety and depression in Indian low back painpopulation, ii) to study the correlation between presence ofanxiety, depression and disability and iii) to study thedifferences in anxiety, depression and disability scores inpatients with ‘normal’ and ‘abnormal’ pain drawing with a
Psychological disturbance in Indian low back pain populationKetan C Pande
Sushrut Hospital, Research Centre and Post Graduate Institute of Orthopaedics, Nagpur
K C Pande, MS, DNB, MCh (Orth), **Consultant Orthopaedic & Spinal Surgeon, Division of Spinal Surgery,Sushrut Hospital, Research Centre and Post Graduate Institute ofOrthopaedics, Ramdaspeth, Nagpur 440 010;Email: [email protected]
view to assess the efficacy of pain drawing to identify patientswith anxiety and depression.
Material and Methods
A total of 145 consecutive low back pain patients wereenrolled after obtaining their informed consent. Before clinicalevaluation, all patients completed a questionnaire thatincluded demographic details and the following instruments:
Hospital Anxiety and Depression Scale (HADS) 7
Oswestry Disability Index (ODI) 8
Pain Drawing 9
The details included age and sex of the patient withduration of low back pain. In all the patients the pain wasthought to be related to mechanical back pain, degenerativedisc disease or lumbar canal stenosis. Patients with low backpain related to infection, trauma or tumour were excluded.
The HADS scores were used as a measure of severity ofthe anxiety and depression subscales. The four score rangeswere classified as:
Normal 0-7
Mild 8-10
Moderate 11-14
Severe 15-21
Based on features described by Ransford et al 9, whichinclude pain in sporadic pattern, indicators of pain outsidethe body, incorporation of extra words or symbols to describepain, circumferential thigh pain and bilateral anterior tibialand foot pain, the pain drawing was categorised into ‘normal’and ‘abnormal’ pain drawing by the author blinded to theresults of other assessments.
Statistical analysis: The anxiety and depression scoresare expressed as mean ± standard deviation. To study thecorrelation between different variables the Pearson’sCorrelation Coefficient (r) was used. The sensitivity of thepain drawing was the number of patients with abnormal levelsof anxiety or depression correctly identified (true positive)by a ‘normal’ pain drawing expressed as percentage of thetotal of patients with anxiety or depression. The positivepredictive value of the pain drawing is expressed as the
VOL. 38, NO. 3, JULY 2004 175
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 175-177

INDIAN JOURNAL OF ORTHOPAEDICS176
probability that an individual with ‘normal’ pain drawing hassignificant level of anxiety or depression. The level ofsignificance was taken as p<0.05. The statistical package SPSS10.0 for Windows was used for the statistical analysis.
Results
The response rate for HADS was 100%, while the ODIwas completed by 141 (97.2%) patients. The pain drawingwas completed by 106 (73.1%) patients.
Patient characteristics: There were 69 women (47.6%)and 76 men (52.4%) in the sample. The average age of patientswas 47.5 years with a range of 22 to 84 years. The averageduration of symptoms was 4.15 years with a minimum of 1year and a maximum of 31 years.
Prevalence of anxiety and depression: The percentagenumber of patients with varying degrees of anxiety anddepression according to the cut off recommended is given intable I.
Table 1. Prevalence of anxiety and depression in low back painpopulation (n=145)HADS SubClass Anxiety Subscale Depression SubscaleNormal (0-7) 28.3% 35.2%Mild (8-11) 33.8% 36.6%Moderate (12-14) 31.0% 24.8%
Severe (15-21) 6.9% 3.4%
Correlation between reported disability, anxiety anddepression scores: There was modest but significantcorrelation between disability score assessed by ODI andthe anxiety (r=0.31; p<0.05) and depression (r=0.34; p<0.05)scores assessed by HADS.
Table 2. Disability, anxiety and depression scores in patients with‘normal’ and ‘abnormal’ pain drawing (n=106)
‘Normal’ ‘Abnormal’ p valueAnxiety score 8.7±3.6 10.1±3.7 0.06Depression score 7.8±3.7 8.4±3.3 0.39
ODI 39.8±25.1 47.3±21.3 0.13
Analysis of pain drawing: Of the 106 patients whocompleted the pain drawing, 35 (33%) were scored as havingan ‘abnormal’ pain drawing. The mean±SD of disability,anxiety and depression scores in patients with ‘normal’ and‘abnormal’ pain drawing is given in table II. The sensitivityand positive predictive value of pain drawing with referenceto patients with abnormal levels of anxiety and depression isgiven in table III.
Table 3. The performance of pain drawing expressed as sensitivityand positive predictive value
Anxiety DepressionSensitivity 63% 65%Positive predictive value 63% 63%
Discussion
The present study has found a high prevalence of anxietyand depression in Indian low back pain patients. Abnormallevels of anxiety and depression were found in 71.7% and64.8% respectively.
The rate of major depression in patients with low backpain is between 20% and 45% 10-13 and between 60% to 100%have demonstrable symptoms of a depressive disorder12,14.Although anxiety has primarily been associated with thereaction to acute pain,15,16 it is also found in chronic low backpain14,16,17.
Greenough and Fraser compared eight psychometricinstruments in low back pain patients 18. The patient wasdefined as disturbed if he had three or more of the eight testspositive. Patients with less than three positive tests weredefined as not disturbed. Of 274 patients, 64 (23%) weredefined as psychologically disturbed and the median anxietyand depression score in these patients using HADS was 11and 10 respectively. In the non-disturbed patients the mediananxiety and depression scores were 6 and 3 respectively 18.
In a study of 70 German patients with back pain, Herrmannreported 36% patients with abnormal anxiety (HADS-A >10)and 29% with abnormal depression (HADS-D >8). Abnormalanxiety and / or depression were noted in 47% of patients 19.The present study demonstrates significantly higherprevalence of anxiety and depression though a different cutoff value was used.
In another study, the mean + SD of anxiety and depressionin chronic low back pain patients (n=25) was found to be 9.8+ 5.0 and 6.7 + 3.8 respectively compared to 6.3 + 3.2 and 2.9+ 2.6 in normal patients20. In the present study the mean + SDof anxiety and depression scores were 9.5 + 3.4 respectively.
In the present study there was modest but significantcorrelation between reported disability and levels of anxiety(r=0.31 ; p<0.05) and depression (r=0.34 ; p <0.05). Thissuggests that low back pain patients with significant levelsof anxiety and depression may report increased disabilitycompared to psychologically normal patients. The correlationbetween psychological distress and self reported disabilityhas been explored in the literature. Studies have revealedthat the change in disability after surgery is significantlyrelated to change in psychological distress5,6,21.
PSYCHOLOGICAL DISTURBANCE AND BACK PAIN

VOL. 38, NO. 3, JULY 2004 177
The present study revealed no significant difference inthe anxiety, depression and disability scores in patients whohave a ‘normal’ or ‘abnormal’ pain drawing. This was furthersubstantiated by low sensitivity and positive predictive valueof pain drawing in identifying patients with any degree ofanxiety and depression. The use of pain drawings inassessing patients with low back pain has been supportedby a number of authors22-26, while others have found the paindrawing to be insensitive18, 27.
The results of the present study must be viewed in thelight of the study by Grevitt et al28. In a comparative study ofsubjective and objective psychological assessment of lowback pain patients, it was demonstrated that experiencedspinal surgeons have only 26% sensitivity when trying toidentify distressed patients. Subjective psychologicassessment of back pain patients had a low sensitivity andpredictive value for distressed patients. The same study alsorevealed that a wide variety of instruments are in use, thepain drawing and inappropriate signs being the mostcommonly used.
The results of the present study and the availableliterature highlight the need to detect psychologic disturbancein low back pain patients using objective measures.Psychological screening of all patients with low back pain isrecommended. Pain drawing on its own has poor ability toidentify patients with either anxiety or depression. Thereforepain drawing has limited clinical application as a stand alonetest but it can provide valuable information when used inconjunction with other psychological test like HADS.
References
1. Beals RK, Hickman NW. Industrial injuries of the back and extremities.J Bone Joint Surg (Am). 1972;54:1593-1611.
2. Wiltse LL, Rocchio PD. Preoperative psychological tests as predic-tors of success of chemonucleolysis in the treatment of low backsyndrome. J Bone Joint Surg (Am). 1975;57:478-483.
3. Pheasant HC, Gilbert D, Goldfarb J, Herron L. The MMPI as apredictor of outcome in low back surgery. Spine. 1979;4:78-84.
4. Turner RS, Leiding WC. Correlation of the MMPI with lumbosacralspine fusion results: prospective study. Spine. 1985;10:932-936.
5. Van Susante J, Van de Schaaf D, Pavlov P. Psychological distressdeteriorates the subjective outcome of lumbosacral fusion. A prospec-tive study. Acta Orthop Belg. 1998;64:371-377.
6. Trief PM, Grant W, Fredrickson B. A prospective study of psychologi-cal predictors of lumbar surgery outcome. Spine. 2000;15:2616-2621.
7. Zigmond AS, Snaith RP. The hospital anxiety and depression scale.Acta Psychiatrica Scand. 1983;67:361-370.
8. Fairbank JCT, Couper J, Davies JB, O’Brian JP. The Oswestry lowback pain disability questionnaire. Physiotherapy. 1980;66:271-273.
9. Ransford AO, Cairns D, Mooney V. The pain drawing as an aid to thepsychologic evaluation of patients with low back pain. Spine. 1976;1:127-134.
10. Crue BL, Pinsky JJ. An approach to chronic pain of non-malignantorigin. Postgrad Med J. 1984;60:858-864.
11. Ranga Rama Krishnan K, France RD, Pelton S et al. Chronic painand depression. I. Classification of depression in chronic low back painpatients. Pain. 1985;22:279-287.
12. Atkinson JH Jr, Ingram RE, Kremer EF, Saccuzzo DP. MMPI sub-groups and affective disorder in chronic pain patients. J Nerv Ment Di.s1986;174:408-413.
13. Love AW. Depression in chronic low back pain patients. Diagnosticefficacy of three self-report questionnaires. J Clin Psychol. 1987;43:85-89.
14. Ranga Rama Krishnan K, France RD, Pelton S et al. Chronic painand depression. II. Symptoms of anxiety in chronic low back painpatients and their relationship to subtypes of depression. Pain. 1985; 22:289-294.
15. Hendler N, Viernstein M, Gucer P, Long D. A preoperative screeningtest for chronic back pain patients. Psychosomatics. 1979;20:801-808.
16. Sedlak K. Low back pain: Perception and tolerance. Spine. 1985; 10:440-443.
17. Merskey H, Boyd DB. Emotional adjustment and chronic pain. Pain.1978; 5:173-178.
18. Greenough CG, Fraser RD. Comparison of eight psychometric instru-ments in unselected patients with back pain. Spine. 1991;16:1068-1074.
19. Herrmann C. International experiences with the Hospital Anxiety andDepression Scale - A review of validation data and clinical results. JPsychosom Res. 1997;42:17-41.
20. Morley S, Pallin V. Scaling the affective domain of pain: a study of thedimensionality of verbal descriptors. Pain. 1995;62:39-49.
21. Tandon V, Campbell F, Ross ER. Posterior lumbar interbody fusion.Association between disability and psychological disturbance in non-compensation patients. Spine. 1999;24:1833-1838.
22. Uden A, Landin LA. Pain drawing and myelography in sciatic pain. ClinOrthop. 1987;216:124-130.
23. Uden A, Astrom M, Bergenudd H. Pain drawings in chronic backpain. Spine. 1988;13:389-392.
24. Mooney V. When is surgery appropriate for patients with low back pain.J Musculoskeletal Med. 1990;7:68-89.
25. Goldman S, Merritt JL. Using the pain drawing in evaluating low backdisorders. J Musculoskeletal Med. 1991;16:1039-1043.
26. Chan CW, Goldwin S, Ilstrup DM, Kunselman AR, O’Neill PI. Thepain drawing and Waddell’s Nonorganic physical signs in chronic lowback pain. Spine. 1993;18:1717-1722.
27. Von Baeyer CL, Bergstrom KJ, Brodwin MG, Brodwin SK. Invaliduse of pain drawings in psychological screening of back pain patients.Pain. 1983;16:103-107.
28. Grevitt M, Pande K, O’Dowd J, Webb J. Do first impressions count?A comparison of subjective and psychologic assessment of spinal pa-tients. Eur Spine J. 1998;7:218-223.
KETAN C PANDE

Background : Deep vein thrombosis is a common complicationafter hip and knee surgery. Ideal prophylaxis is still not available.Methods : In a controlled trial, 30 patients in group I were notgiven any thromboprophylaxis while 100 patients in group II wereput on mechanical prophylaxis.Results : Seven patients in group I developed DVT while nopatient in group II had this complications.Conclusion : Mechanical prophylaxis may be a safe tool inpreventing DVT.Key-words : Deep vein thrombosis; Prophylaxis.
Introduction
Deep vein thrombosis or thromboembolism is one of themost common complications in patients who have sustainedskeletal injury1 or who have undergone replacement surgeryof hip2 and knee3. Evidences in literature show that afteroperations of hip replacement arthroplasty, 30 to 50 percentof the cases develop deep vein thrombosis in legs and pelvis 4.Elderly people who have sustained fracture of hip or lowerextremity and pelvis run a greater risk of developingthromboembolism as compared to the younger populationgroup5. Deep vein thrombosis after knee replacements hasbeen reported to range from 40% to 80% 3. Risk factors,which are thought to predispose to this phenomenon, areage over 40 years, increased duration of surgical procedureand severity of underlying systemic disease. It is thoughtthat a hypercoaguable state persists in the body after a traumaor episode of instrumentation in the skeleton. Thishypercoaguability is secondary to the release ofthromboplastin from marrow fat and medullary sinusoids intothe systemic circulation4. Propagation of thrombi proximally
Deep venous thrombosis prophylaxis- A multicentric studyS Bhan, BK Dhaon, Yash Gulati, Shekhar Aggarwal
New Delhi
S Bhan, Professor and Head, Department of Orthopaedics, **All India Institute of Medical Sciences, New DelhiBK Dhaon, Professor and Head, Department of Orthopaedics, Maulana AzadMedical College, New DelhiYash Gulati, Consultant Orthopaedic Surgeon, Apollo Hospital, New DelhiShekhar Aggarwal, Director, Sant Parmanand Hospital, New Delhi
No outside funding or grant was received in support of this research.No professional or personal benefits are received or promised to theauthors or their institutions.
from vein of calf into the popliteal and femoral veins is wellknown, as one of the major factors for fatal pulmonaryembolism6. Prevalence of asymptomatic pulmonary embolismis less certain, but a study of patients undergoing total kneearthroplasty has reported 1.8- 7% prevalence of pulmonaryembolism7. Mortality rate in patients who have developedP.E. ranges from 0.5% to 2%8 In the absence of properdiagnosis and limitations of adequate therapy the mortalitycould be as high as 30%9. It is therefore clear that preventionof DVT is much preferable to treating it10.
Thromboprophylaxis can be achieved by pharmacologicaland non-pharmacological means. No consensus howeverexists on the ideal thromboprophylactic method.Pharmacological agents such as low molecular weight heparinand oral anticoagulants are commonly used for prophylaxisbut may cause bleeding. In cases of polytrauma, institutionof anticoagulants or other pharmacological agents may bedelayed due to the presence of associated cranial or othervisceral bleed. Mechanical means in contrast topharmacological measures are devoid of hemorrhagiccomplications. Various mechanical agents, which have beenused, include active and passive exercise, elastic stockings,graduated pressure, electrical stimulation of the muscles ofthe calf, and intermittent compression of calf by pneumaticstockinet. A more recent mechanical prophylaxis has emergedin form of an electrical stimulator (lymphavision), whichenhances drainage not only from venous system but alsofrom the lymphatic system due to stimulation of striated, andsmooth muscle found in the system network.
This multicenteric study was undertaken to assess theeffectiveness of lymphavision in preventing the phenomenonof thromboembolism in patients operated for total kneereplacement, total hip replacement, major spine surgeryinvolving instrumented spinal fusion and polytrauma withlower limb fracture. Four different hospitals in the city wereinvolved in the study to remove personal bias and to representa wider section of patient population.
Material and methods
This prospective study involving 180 patients of over40 years of age was conducted at four independent hospitalsof the city i.e. The All India Institute of Medical Sciences,
178 INDIAN JOURNAL OF ORTHOPAEDICS
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 178-182

VOL. 38, NO. 3, JULY 2004 179
L.N.J.P. hospital, Sant Parmanand hospital and Apollohospital from June 2001 to March 2003. The first thirty patientswere allocated to Gr. I or control group while the remaininghundred patients were put in Gr. II or study group. Patientswho had history of previous thromboembolic phenomenonor pulmonary embolism were not included in the study. Allpatients undergoing the study were interviewed andcomprehensive clinical history and examination wasconducted on them to rule out presence of risk factors forthromboembolism such as history of smoking, alcoholconsumption, and contraceptive intake, presence of varicosevein, any abdominal tumor, and previous cerebrovascularaccident. There were 81 female and 49 men in the study. Theaverage age of the patients was 61 yrs (range 42 to 80yrs).Cases, which were found suitable for study included 75primary total knee replacement (5 simultaneous bilateral, 65unilateral), 30 primary total hip replacement (all unilateral), 15operated lower limb fracture in polytrauma patients and 10instrumented spinal fusion in traumatic vertebral fractures.The mode of anesthesia for replacement and internal fixationin lower limb fracture was epidural in all the cases whileinstrumented spinal fusion were performed with generalanesthesia. Two-dimensional ultrasound, with color flowmapping and Doppler velocimetry was performed in both thegroups to look for course, contour, compressibility, caliberand flow patterns in veins of lower leg using variablefrequency real time transducer. Veins which were screenedincluded the common femoral, superficial femoral, deepfemoral, popliteal, anterior tibial and the posterior tibial.Written and informed consent was sought in all the cases.
Group I or the control group consisted of thirty patientsin whom no thromboprophylaxis in any form mechanical orpharmaceutical was initiated in the postoperative period.Patients who had undergone either unilateral total kneereplacement (n = 25) or unilateral total hip arthroplasty (n = 5)were included in this group. Doppler studies to rule outthromboembolic phenomenon were carried out on the fourthand the fifteenth postoperative day. There were 18 femalesand 12 males in this group.
Group II or the study group consisted of hundred patientsin whom mechanical prophylaxis (Lymphavision, Aloha,France) was initiated. Sixty-three females and 37 malesparticipated in this group. The distribution of case being: 50total knee replacements (5 Bilateral, 40 unilateral), 25 total hipreplacements, 15 operated polytrauma patients with lowerlimb fracture and 10 cases of instrumented spinal fusions.
Technique: To stimulate the muscles small rubber pads
in form of electrodes were applied either on the calf or theplantar aspect of foot of the patients on both the legs. Lowvoltage current with an intensity of 21mA (range 15 – 27 mA)was used, which could be varied so as stimulate a visiblemuscle in the lower leg. The intensity was nevertheless keptin the comfort zone of the patients. This treatment was givenfor a period of 30 minutes, two to three times daily for aperiod of 10 days. Postoperative rehabilitation program forthe patients was initiated on the day of surgery itself. Patientsoperated with joint replacements and internal fixation weretaught quadriceps drill and ankle ROM exercise on the day ofsurgery, thereafter active range of motion of involved joints,walking with support (partial, full or non weight bearing,depending upon the surgery) were started on the third postoperative day. Patients with spinal instrumentation wereinitiated side turning, sitting and standing with support on2nd postoperative day itself after application of an appropriatebrace.
Ultrasonic Doppler evaluation was performed in patientsof both the groups pre operatively and on 4th day and at theend of second week postoperatively. Interpretation of Dopplerreports of both the groups was made by the same radiologistwho was unaware of the mechanical prophylaxis and thestudy as a deliberate attempt made to remove observer bias.Thrombi were classified as proximal if they involved thepopliteal and or femoral veins. Patients in whom Doppleranalysis showed presence of thrombosis, subcutaneousenoxaparin in the dose of 40 mg twice a day was institutedand continued for a period of 6 weeks.
Patients were also evaluated clinically for presence ofother signs or symptoms of deep vein thrombosis. Calftenderness, with swelling, along with increase in localtemperature was noted for, if any. Homan’s sign or pain incalf with dorsiflexion of ankle was looked for in every patientbut its absence was not considered to be predictive ofabsence of thromboembolic phenomenon. Examination ofboth the lower limbs for daily measurement the calf and thighcircumference was done.
Results
A comparative analysis was made between the controlgroup and study group with reference to presence ofthromboembolism either symptomatic or asymptomatic bymeans of clinical examination and Doppler evaluation.
In group I or the control seven out of 30 patientsdeveloped Doppler evidence of deep venous thrombosis.Five of these patients had undergone total knee replacements
S BHAN, BK DHAON, YASH GULATI, SHEKHAR AGGARWAL

INDIAN JOURNAL OF ORTHOPAEDICS180
while the remaining two had total hip replacements. Threeout of five patients in total knee replacement group had adistal thrombosis involving the extremity, which was operated.Two patients had both proximal and distal thrombus. Onepatient out of these two had evidence of a bilateralinvolvement. In the total hip replacement category, one ofthe patients had both proximal and distal vein involvementwhile the other screened positive only for proximal veins. Inboth these patients the operated limb was affected.Documentation of calf girth was made on a proforma notingit a day before operation and from the day of operation to thefourteenth postoperative day. One patient was clinicallysymptomatic in this group. Calf tenderness was apparent inthis patient on third postoperative day after a right total kneereplacement. There was an increase in calf girth by 2.5 cm ascompared to the preoperative status. This further increasedto 3.0.cm by tenth postoperative day (preoperative girth – 40cm, 10th postoperative day girth 43 cm) and remained staticthereafter. Doppler ultrasound report both on the 4 th day andafter two weeks confirmed presence of thrombus in theanterior and posterior tibial veins with partial involvement ofthe popliteal veins with no further progression.Subcutaneous enoxaparin in a dose of 40 mg twice daily wasinitiated on third postoperative day itself and was continuedfor six weeks. There was a mean increase of calf girth of 1.78cm (range 0.5 cm to 2.4cm) on second postoperative day andan overall increase in calf girth by 1.65 cm (range, 0.0 cm to1.9 cm) was still seen after fourteenth postoperative day inthe asymptomatic patients in this group
Group II patients also underwent Doppler screeningstudies, clinical examination and calf girth measurement asthe previous group. None of the patients screened by Dopplerultrasound showed any evidence of presence of thrombus.
This group of patients showed an increase in calf girthby about 1.50 cm (range 0.5 to 1.8 cm) on secondpostoperative day and by 1.30 cm (range 0.2 to 1.5 cm) ontenth postoperative day. None of the patients in either groupdeveloped any signs or symptoms of pulmonary embolism.
Discussion
Following total joint replacement or internal fixation oflong bones after skeletal trauma, the most feared complicationin the immediate and early postoperative period is probablydeep venous thrombosis. The causes of this phenomenonare summarized under Virchow’s triad. These include stasisand hypercoagulability of the blood as well as damage to theendothelial wall of venous system11 . In normal state
procoagulants such as thrombin are removed by macrophagesin the liver. Clotting is further prevented by endothelial surfacefactors such as thrombomodulin and anticoagulants likeantithrombin III12. This condition may be reversed duringsurgery since stasis and hypoxia, which may be aggravatedwith application of tourniquet, promotes release ofprocoagulants and ultimately may promote intra vascularclotting13. Incidence of deep venous thrombosis withoutprophylaxis has been reported to be as high as 88% aftertotal knee replacement3 and 54% after total hip replacement14.Various methods, both mechanical as well as pharmacologicalare being tried world wide to prevent thromboembolism aftersurgical intervention. Mechanical devices such as pneumaticcompression devices and early post operative mobilizationhave been used to improve venous blood flow therebydecreasing the risk of having a deep vein thrombosis episodepost operatively in elective orthopedic surgery 15. They alsohave advantages over pharmacological agents in thathemorrhagic complications do not occur13.
In the present study a new form of a mechanical devicehas been employed for thromboprophylaxis in patientsundergoing orthopedic surgery to document its efficacy andto compare this form of prophylaxis as against others asillustrated in literature. Our mechanical prophylaxis instrumentconsisted of non-invasive electrical stimulationlymphavision, which used a very low frequency forstimulating striated and smooth muscles of the limb.Stimulation is provided by means of multiple electrodes,which are placed in the desired area. The current generatedby the device reproduces an autonomic nervous systemmessage sent to the smooth muscles located between twocontact electrodes, therefore activating the peristalsis of thelymphatic network of lower limb. This peristalsis correspondsto the cyclic contraction and relaxation of the smooth musclescontrolled by both the sympathetic and parasympatheticnervous system. As it travels through various body tissues,the current would also stimulate striated skeletal muscles.An increase in current intensity causes an elementarycontraction provoking a muscular pump effect. Smoothmuscles are found in practically the whole lymphatic system,in all muscular or distributing arteries and in wall of deep veinnetwork.
The smooth muscles do not have striation and take alonger limb to reach peak contraction. However, they remaincontracted for a longer period of time. This lymphavisiontakes into account these periods producing a stimulationtime of 6 ms, while the rest time is 650 ms. This allows thesmooth muscles to reach peak contraction and to stay there
DEEP VENOUS THROMBOSIS PROPHYLAXIS

VOL. 38, NO. 3, JULY 2004 181
and relax before the next stimulation. This equals to afrequency of 1.52 Hz stimulation of the striated muscle andactivation of the muscle helps the venous as well as thelymphatic system to evacuate early by enhancing interstitialdrainage, restoring disrupted intercellular exchanges andreducing congestion of muscle pump. Enhanced venousreturn by this system is brought primarily by the action ofcurrent over both plantar venous plexus and the calf musclepump. The calf muscle pump action is due to contraction ofthe calf muscle thereby squeezing the veins in the deep calf.This propels the blood in upward direction. Visiblecontractions of the muscles of calf produced by the systemsignify the initiation of the calf pump activity. Foot pumpactivity is also partially activated by the muscular contractionthus created by current. In our patients an intensity of mean21+ 6.4 MA was sufficient to produce visible musculartwitching, thereby initiating muscle pump action. Results ofusing the electrical stimulator have been gratifying in ourstudy.
Four different hospitals from both public and privatesector used this equipment to have different sets ofpopulation belonging to different occupations and socialstatus. Patients who underwent this study included thosewho underwent mainly hip and knee arthroplasty operationas well as those poly trauma cases where internal fixation oflong bones of lower limb were carried out. Patients underwentDoppler ultrasound studies on 4th and 14th postoperative dayto screen for course, contour, compressibility, caliber andflow patterns of lower leg. These were compared with apreoperative Doppler study done a day before surgery of thesame patient to detect presence of thrombosis. None of thepatients included in the study had any evidence of thrombosispreoperatively either clinically or through Doppler ultrasoundmethod. Postoperatively Doppler results in 100 patients wherelymphavision was used showed no evidence of thrombosiseither in proximal or distal veins in any patient. This 100%complication free result is better than other forms ofprophylaxis. Westrich et al13 while reviewing about 138articles on prophylaxis in total knee replacement found anoverall deep vein thrombosis rate of 53% in patients whoreceived aspirin, in 45% of patients who received wafarin,29% in patients who received LMW Heparin and 17% inpatients who received mechanical prophylaxis in form ofpneumatic compression devices. Review of literature inregards to thromboprophylaxis of various forms in total hipreplacement also shows more or less similar results. Whileusing low dose warfarin in their patients Amstutz et al17
reported 0.5% of nonfatal pulmonary embolism where asPaiement et al18 found the incidence to be 16.7% with lowdoses of warfarin. LMW Heparins have been documented togive better results than other pharmaceutical agents minusthe morbidity. Turpie et al19 found that enoxaparin reducedthe incidence of venous thrombosis from 51% to 11% afterelective hip surgery. However use of LMW heparin is limiteddue to the use of epidural or spinal anaesthetic, which arebeing used more commonly in such patients because of riskof spinal hematoma formation.
The calf diameter of the patients on second and onfourteen day postoperatively in patients where lymphavisionwas used was lower than those in whom thethromboprophylaxis was not used. The reason for reductionin the over all calf girth probably is due to complementaryeffect of electrical stimulation both on the lymphatic andvenous system. The activation of lymphatic system inprincipal leads to faster drainage and restores intercellularand interstitial exchanges, which are disruptedintraoperatively. Reduction of edema in turn helpsrehabilitation faster thereby promoting muscle pump and footpump activity. Foot pump activity is principally activated byweight bearing which compresses the veins in the deep layersof plantar surface20. It also flattens the arch thus stretchingthe plantar veins and plexus. This helps in preventinghypercoagulability and stasis during early postoperativestages thus further reducing chances of deep venousthrombosis. Patient compliance in this equipment was alsonot a problem since intensity of the current could be regulatedby a rheostat thus limiting the intensity of the current with inthe comfort zone of individual patients. Our experience withmechanical prophylaxis device such as lymphavision has beenencouraging both in lowering the incidence of deep venousthrombosis and postoperative limb edema. It can safely beused in patients in whom epidural or spinal anesthesia hasbeen used for elective or emergency operations. Absence ofbleeding complications as seen in anticoagulant therapy andits safe use in situations where anticoagulants arecontraindicated such as poly trauma with head injury,haemothorax or abdominal bleeding makes it a favouredmethod for prophylaxis in these conditions. Mechanicalprophylaxis in form of low intensity electrical stimulation maybe a very helpful and a safe tool in preventing DVT followingelective joint replacement surgery and in cases of polytraumawhere anticoagulants are contraindicated.
Acknowledgement: The authors wish to thank Dr. E. Krishna
Kiran, for his help in conducting the study.
S BHAN, BK DHAON, YASH GULATI, SHEKHAR AGGARWAL

INDIAN JOURNAL OF ORTHOPAEDICS182
References
1. Geerts W, Code K, Jay R, Chen E, Szalai J. A prospective study ofvenous thromboembolism after major trauma. N Eng J Med. 1994; 24:1601-1606.
2. Harris WH, Saltzman EW, Desanctis RW, Coutts RD. Prevention ofvenous thromboembolism following total hip replacement. J Am MedAssoc. 1972; 220: 1319-1322.
3. Mc Kenna A, Bachmann F, Kaushal SP, et al. Thromboembolicdisease in patients undergoing total knee replacements. J Bone JointSurg (Am). 1976; 58: 928-932.
4. Love lW. Venous thrombosis and embolism. J Bone Joint Surg (Br).1981; 63: 155-167.
5. Tubiana R, Dupare J. Prevention of thromboembolism complication inorthopaedic and accident surgery. J Bone Joint Surg (Br). 1961; 43 : 7-15.
6. Borow M, Goldson H. Postoperative venous complications. A m JSurg. 1981; 141: 245-251.
7. Clagett GP, Anderson FA, Geerts W et al. Prevention of venousthromboembolism. Chest. 1998; 114 (5 Suppl): 513- 560.
8. Cavendish ME, Charnley J. Review of the complications of lowfriction arthroplasty in the elderly. Wrighttington Int. publication No.37,1972.
9. Sikorski JM, Hampson WG, Staddon GE. The natural history andaetiology of deep vein thrombosis after total hip replacement. J BoneJoint Surg (Br). 1981; 63: 171-177.
10. Gallus AS, Hirsh J. Prevention and treatment of venous thromboem-bolism. Semin Thromb Hemost. 1976; 11:291-331.
11. Virchow R. Neuer fall von tod licher embolic der lungenarterian. ArchPathol Anat. 1856; 10: 225-228.
12. Gross PL, Aird WC. The endothelium and thrombosis. Semin ThrombHemost. 2000; 26: 463-478.
13. Westrich GH, Haes SB, Mosca P, et al. Meta analysis of thromboembolic prophylaxis after total knee arthroplasty . J Bone Joint Surg(Br). 2000; 82: 795-800, 2000.
14. Johnson R, Orth MC, Carmichael JHE et al. Deep venous thrombo-sis following Charnley arthroplasty. Clin Orthop. 1978; 132:24-30.
15. Tamir L, Hendel D, Neyman C, et al. Sequential foot compressionreduces lower limb swelling and pain after total knee arthroplasty. JArthroplasty. 1999; 14:333-338.
16. Francis CW, Pellegrini VD, Marder V, et al. Comparison of Warfarinand external pneumatic compression in the prevention of venous throm-bosis after total hip replacement. J Am Med Assoc. 1992; 267:2911-2922.
17. Amstutz HC, Friscia DA, Dorey F, Carney BT. Warfarin prophylaxisto prevent mortality from pulmonary embolism after total hip replace-ment. J Bone Joint Surg (Am). 1989; 71: 321.
18. Paiement G, Wessinger SJ, Waltman AC, Harris WH. Low dosewarfarin versus external pneumatic compression for prophylaxis againstvenous thromboembolism following total hip arthroplasty. J Arthro-plasty. 1987; 2: 23.
19. Turpie AGG, Levine MN, Hirsh J, et al. A randomized control trial ofa low molecular weight heparin (enoxaparin) to prevent deep-vein throm-bosis in patients undergoing elective hip surgery. N Eng J Med. 1966;315:925.
20. Lundeen S, Lundquist K, Cornwall MW, et al. Plantar pressureduring level walking compared to other ambulatory activities. FootAnkle Int. 1994; 15: 324-328.
DEEP VENOUS THROMBOSIS PROPHYLAXIS

Introduction
Osteoid Osteoma is a benign osteoblastic tumour ofenchondral bones. This is usually found in the patientsbetween the ages of 7 and 25 with a male to female ratio ofapproximately 3:1. The tumour is characterised histologicallyby a central core of vascular osteoid tissue (nidus) surroundedby a zone of sclerotic bone 1. The commonest site ofinvolvement is the femur followed by the tibia, humerus andspine. Hands and feet may also be involved. The hallmark ofosteoid osteoma is the insidious onset of symptoms whichstart as a dull ache and progress to intense and persistentpain. Here we report a case of osteoid osteoma where a doublepathology confused the presentation due to overlappingsymptoms.
Case Report
A young boy of 17 years presented with complaints oflow back ache with pain radiating to left thigh and calf for 6months. On examination SLR was 600 with ankle and kneejerks normal and grade IV power in the extensor hallucislongus with no paraesthesia on the affected side. The hipmovements were full and free with no localized tenderness.X-ray lumbosacral spine was unremarkable while MRI showedL4/5 posterolateral disc prolapse with indentation over leftsided L5 nerve root.
Due to persistence of pain in the left lower limb andinability to attend college in spite of conservative treatment,a lumbar microdiscectomy was performed with disc excisionat L4/5 and left sided L5 root clearance. Post operatively thepatient’s LBA and calf pain disappeared for the first two dayshowever from 3rd post operative day he complained of pain inleft lower limb localizing it now to the front of left thigh withradiation upto the left knee.
Osteoid osteoma- puzzling presentation & effectivemanagement –a case reportS Agarwala, BS Rajput
Department of Orthopaedics, PD Hinduja National Hospital & Research Centre, Mumbai
S Agarwala, MS, MCh Orth, Chief of Orthopaedic SurgeryBS Rajput, D Orth, Associate Consultant **Department of Orthopaedics, PD Hinduja National Hospital & ResearchCentre, MumbaiDr BS Rajput, D Orth, Associate consultant, Department of Orthopaedics,PD Hinduja National Hospital & Research Centre, Mahim, Mumbai, India
A repeat MRI was done and cord and nerve root clearancewere confirmed. The severity of pain warranted a relooksurgical exposure. This confirmed a total clearance aroundthe nerve root. The patient recovered for two days, howeverhe had recurrence of pain on 3rd day. Since the pain wasepisodic and persistent a bone scan was ordered and thisrevealed a high activity zone around lesser trochanter. A CTand MRI of the affected region were done which confirmedan osteolytic lesion surrounded by a zone of sclerosis in theanteromedial part of the femoral neck proximal to lessertrochanter ( Fig 1a,b).
It was elected to excise the nidus as the pain waspersistent. The patient was taken on fracture table andthrough a lateral incision the nidus was localized under C-arm image intensifier. It was in the anteromedial quadrant andonly seen in the 15° external rotation. Recognizing that asurgical defect left behind could result in a stress fracturesubsequently, it was planned to protect this by a spanningDHS plate. The nidus was precisely excised using a highspeed Midas rex cutting K 1 burr (Fig 2).This is a highrevolution pointed bone cutter and helps cutting a precisepiece of bone. Next a DHS plate fixation was done to avoidchances of a stress fracture neck femur. The excised piecewas immediately screened under C arm to confirm the completeremoval of the nidus.The surgically created gap was filled byan exactly sized muscle pedicle corticocancellous bone graftfrom the greater trochanter. The patient was completelyrelieved of his symptoms and discharged on elbow crutches.
Fig 1(a,b) C T of hip showing nidus in the anteromedial part of theneck other than the herniation pit in intertrochanteric region, aphysiological finding.
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 183-184
VOL. 38, NO. 3, JULY 2004 183

INDIAN JOURNAL OF ORTHOPAEDICS184
Discussion
Though posterolateral disc is frequent, the symptoms ofosteoid osteoma can be missed, particularly in the presenceof co-morbid pathology. The spine surgery in this case wasjustified for the persistent pain, distress and the EHLweakness, which recovered after surgery. The annoying painin the thigh led us to suspect a painful hip rather than the
spine as a cause for the pathology. MRI helped in localisingthe lesion2.
The removal of the localized nidus, though simpleenough due to C-Arm localization, would have left a majordefect in the weight bearing bone of this active young man.This was a surgical challenge, as it would entail 3 months ofbedrest but surgical expertise had something else to offer.
Here we elected to buttress and protect the stress raiser(left behind by the defect in the calcar) with a dynamic hipscrew, a device used for fractures in that region of hip , whichoften permits immediate partial weight bearing.
The second important step was the mobilization of aprecisely cut muscle pedicle corticocancellous bone graftthrough the same incision from anterior greater trochanterarea and impacting it in the defect left behind from the excisednidus. This helped bring bone and blood into the defect andpermitted early mobilization. Both of them we feel have helpedin the excellent net outcome.
References
1. Resnick D, Niwayama G. Tumour & tumour like lesions of bone. Phila-delphia, W B Saunders.1995:3620-35.
2. Davies M, Cassar-Pullicino VN et al. The diagnostic accuracy of MRimaging in osteoid osteoma. Skeletal radiology. 2002;31:559-569.
S AGARWALA, BS RAJPUT
Fig 2. Marking of the boundries of nidus by the pointed Midas rex
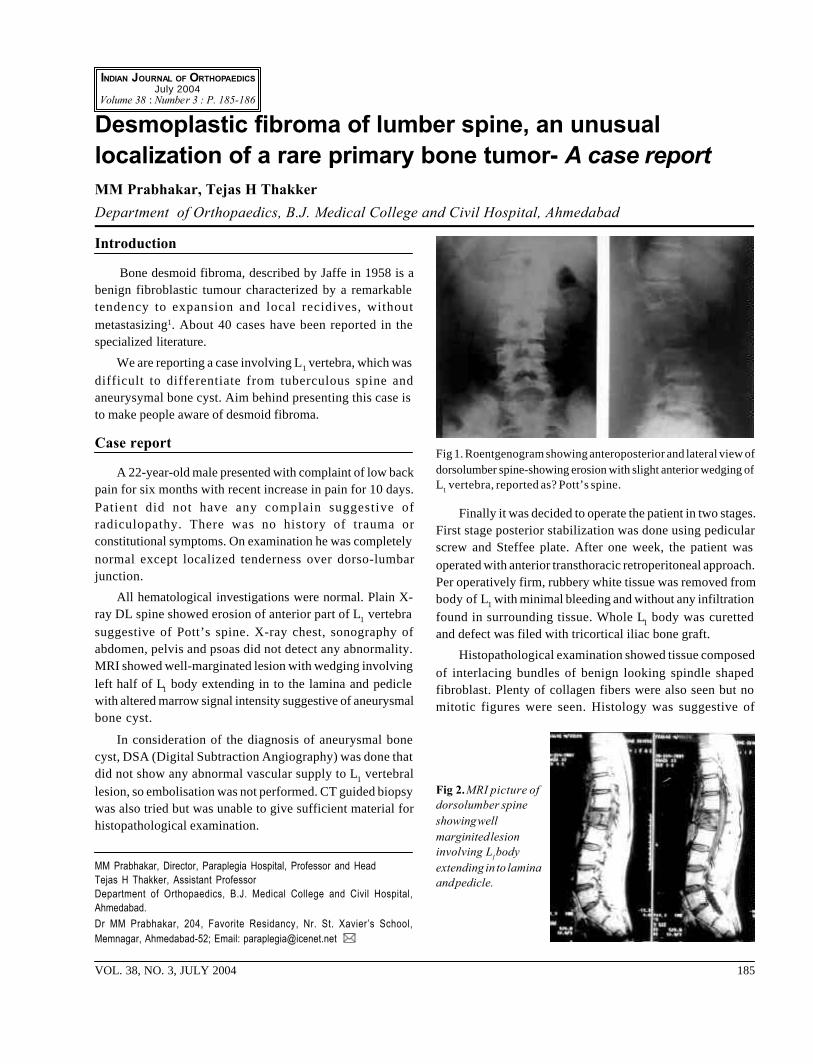
Introduction
Bone desmoid fibroma, described by Jaffe in 1958 is abenign fibroblastic tumour characterized by a remarkabletendency to expansion and local recidives, withoutmetastasizing1. About 40 cases have been reported in thespecialized literature.
We are reporting a case involving L1 vertebra, which wasdifficult to differentiate from tuberculous spine andaneurysymal bone cyst. Aim behind presenting this case isto make people aware of desmoid fibroma.
Case report
A 22-year-old male presented with complaint of low backpain for six months with recent increase in pain for 10 days.Patient did not have any complain suggestive ofradiculopathy. There was no history of trauma orconstitutional symptoms. On examination he was completelynormal except localized tenderness over dorso-lumbarjunction.
All hematological investigations were normal. Plain X-ray DL spine showed erosion of anterior part of L1 vertebrasuggestive of Pott’s spine. X-ray chest, sonography ofabdomen, pelvis and psoas did not detect any abnormality.MRI showed well-marginated lesion with wedging involvingleft half of L1 body extending in to the lamina and pediclewith altered marrow signal intensity suggestive of aneurysmalbone cyst.
In consideration of the diagnosis of aneurysmal bonecyst, DSA (Digital Subtraction Angiography) was done thatdid not show any abnormal vascular supply to L1 vertebrallesion, so embolisation was not performed. CT guided biopsywas also tried but was unable to give sufficient material forhistopathological examination.
Desmoplastic fibroma of lumber spine, an unusuallocalization of a rare primary bone tumor- A case reportMM Prabhakar, Tejas H Thakker
Department of Orthopaedics, B.J. Medical College and Civil Hospital, Ahmedabad
MM Prabhakar, Director, Paraplegia Hospital, Professor and HeadTejas H Thakker, Assistant ProfessorDepartment of Orthopaedics, B.J. Medical College and Civil Hospital,Ahmedabad.Dr MM Prabhakar, 204, Favorite Residancy, Nr. St. Xavier’s School,Memnagar, Ahmedabad-52; Email: [email protected] **
Finally it was decided to operate the patient in two stages.First stage posterior stabilization was done using pedicularscrew and Steffee plate. After one week, the patient wasoperated with anterior transthoracic retroperitoneal approach.Per operatively firm, rubbery white tissue was removed frombody of L1 with minimal bleeding and without any infiltrationfound in surrounding tissue. Whole L1 body was curettedand defect was filed with tricortical iliac bone graft.
Histopathological examination showed tissue composedof interlacing bundles of benign looking spindle shapedfibroblast. Plenty of collagen fibers were also seen but nomitotic figures were seen. Histology was suggestive of
Fig 1. Roentgenogram showing anteroposterior and lateral view ofdorsolumber spine-showing erosion with slight anterior wedging ofL1 vertebra, reported as? Pott’s spine.
Fig 2. MRI picture ofdorsolumber spineshowing wellmarginited lesioninvolving L1 bodyextending in to laminaand pedicle.
VOL. 38, NO. 3, JULY 2004 185
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 185-186

INDIAN JOURNAL OF ORTHOPAEDICS186
desmoplastic fibroma.
At the end of one year follow up patient did not haveany complaint or neurological deficit.
Discussion
Desmoplastic fibroma of bone is a rare, locallyprogressive, nonmetastatic, slowly growing tumor of bone.The term was first introduced by Jaffe in 19581. Since thenonly few cases have been reported in the world. It’s incidenceis about 0.2 to 0.3% of biopsy analyzed primary bone lesion2.
Desmoplastic tumor of the soft tissue and thedesmoplastic fibroma of bone are histologically identical, souse of only one name for a tumor process affecting bothbone and soft tissue is more efficacious than use of twonames. Thus preferred name would be desmoid tumor of bone.Desmoplastic implies a dense matted fibrous texture a featurethat is reflected microscopically by eosinophillic strands ofcollagen that form the characteristic interwoven pattern ofdesmoplastic fibroma3.
It usually affects patients between 15 to 40 years withoutsex predominance. It commonly affects metaphyseal regionof long bone, particularly tibia and femur. Most patients (90%)presents with pain alone, 15% stress or pathological fracture,less than 10% presents with swelling4,5.
Radiological findings of uneven destruction of cortexand medullary bone results in ridges of variable thicknessand as the tumor grows slowly periosteum keeps pace withthe lesion by laying down new bone6. In central tumor areasan inhomogeneous, intermediate to low signal is demonstratedby MRI using T1- and T2-weighted spin-echo and turbo-spin-echo sequences. Contrast-enhanced MRI shows markedenhancement in peripheral areas depicting the extraosseousand intramedullary extension7,8.
Constant histological feature are fibroblasticproliferation, nuclear monotony (no atypia) with ovoid nucleiand well-formed collagen appearance from field to field. Whilecellularity; range of cellularity from case to case is of fair
degree.
The differential of the tumor includes spindle cell tumors,most specifically low grade fibrosarcoma. The desmoplasticfibroma does not have the cellularity, mitotic activity orpleomorphism of a fibrosarcoma but the distinction can bedifficult and is sometimes made clinically. The edge of thetumor may resemble fibrous dysplasia, but under polarizedlight, lamellar structures are obvious4.
Most effective treatment of this tumor is enbloc widelocal excision taking a clear border of normal bone in alldimensions about the lesion. As it is a locally aggressivetumor, following marginal excision 30% to 66% of cases recurone or more times if not excised completely. Recently, onestudy has recommended “aggressive curettage” as a surgicaloption9.
References
1. Jaffe HL. Tumors and Tumorous Conditions of the Bones and Joints.Philadelphia: Lea & Febiger. 1958; 298–303.
2. Gebhardt MC, Campbell CJ, Schiller AL, Mankin HJ. Desmoplasticfibroma of bone: a report of 8 cases and review of the literature. J BoneJoint Surg (Am). 1985; 67:732–747.
3. Bridge JA, Swarts SJ, Buresh C, Nelson M, Degenhardt JM, SpanierS. Trisomies 8 and 20 characterize a subgroup of benign fibrous lesionsarising in both soft tissue and bone. Am J Pathol. 1999; 154:729–733.
4. Bohm P, Krober S, Greschniok A, Laniado M, Kaiserling E. Des-moplastic fibroma of bone: a report of two patients, review of theliterature, and therapeutic implications. Cancer. 1996; 78:1011–1023.
5. Inwards CY, Unni KK, Beabout JW, Sim FH. Desmoplastic fibromaof bone. Cancer. 1991;68:1978–1983.4
6. Taconis WK, Schutte HE, van der Heul RO. Desmoplastic fibroma ofbone: a report of 18 cases. Skeletal Radiol. 1994; 23(4):283-8.
7. Juergens KU,Bullmann V. Desmoplastic fibroma in the thoracicspine:an unusual localization of a rare primary bone tumour.Eur Radiol-ogy. 2000; 11(2):273-5.
8. Kong KY,Kang HS. MR finding of desmoplastic fibroma of the spine.Acase report.Acta Radiol. 2000; 41(1):89-91.
9. Huvos A. Bone tumors: Diagnosis, treatment and prognosis.W.B.Saunders Co., 1991.
Fig 3. Antero-posterior and lateralroentgenogram of1-year-old operatedcase of desmoplasticfibroma of L1 vertebrashoeing wellincorporating bonegraft without anysigns of recurrence.
Fig 4.Photograph ofhistopathology
DESMOPLASTIC FIBROMA OF LUMBER SPINE, AN UNUSUAL LOCALIZATION

Introduction
Medial discoid meniscus is a rare entity, rarer than thelateral discoid variety. Normal meniscus is semilunar in shape.It was once postulated that the discoid form must bedevelopmental in the growing fetus and that the abnormalpersistence of the same would produce the discoid meniscusvariant1. But embryological studies showed that during thedevelopment of the meniscus, there is never a discoid phaseand hence it was thought that the discoid from might be dueto a variety of other etiological factors 2. It was believed bysome that the discoid meniscus is a result of instability of themeniscus with subsequent thickening, gradually assuming adiscoid shape3.
Case Report
A 16 year old male came with history of pain and swellingin right knee for eight months. Pain was present on the medialside of the knee during climbing stairs and getting up fromsquatting position and was dull in nature. There was anoccasional clicking sound from the right knee joint. Therewas no history of fall, trauma, fever of constitutionalsymptoms, or pain in any other bone or joints.
On examination there was localized fullness on the medialside of the right knee joint line. There was no evidence ofjoint effusion. There was medial joint line tenderness and noother positive physical finding. Occasional clicks were,however, heard from the right knee joint. All special testswere negative.
Plain radiograph of the right knee joint showed wideningof the medial joint space (Fig 1). Ultrasonography of the rightknee joint was done in view of the suspected superficialetiology of the localized fullness. Ultrasound showed a medialmeniscal cyst (Fig 2).
Massive discoid medial meniscus presenting as ameniscal cyst – A case reportSushil K Sabnis, Anish P Kadakia
Department of Orthopaedics, Shri Harilal Bhagwati Municipal General Hospital and Sabnis Hospital,Mumbai
Sushil K Sabnis, MS (Orth), DOrth, Honorary Orthopaedic SurgeonAnish P Kadakia, MS (Orth), DNB Orth, FCPS Orth, DOrth, Senior RegistrarDepartment of Orthopaedics, Shri Harilal Bhagwati Municipal General Hospitaland Sabnis Hospital, MumbaiDr. Anish P Kadakia, 3/27, New Ghaswala Building, 493, Sane GurujiMarg. Tardeo, Mumbai 400 034; Email: akadakiao-rediffmail.com **
The patient’s right knee joint was subjected toarthroscopy. It showed a massive medial discoid meniscus,covering the entire medial tibial condylar surface, with noabnormal attachments (Fig 3). There was, however, ahorizontal cleavage tear communicating with the undersurfaceof the meniscus. A partial balanced meniscectomy was done.The patient’s post operative recovery was uneventful andwas pain free with no symptoms at the last follow up.
Fig 1 : Radiograph ofthe right knee showingwidening of the medialjoint space.
Fig 2. Ultrasound of the right knee joint showing medial meniscalcyst.
VOL. 38, NO. 3, JULY 2004 187
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 187-188

INDIAN JOURNAL OF ORTHOPAEDICS188
Discussion
Medial discoid meniscus as against the lateral varianthas not been satisfactorily classified due to the rarity of theentity. Following the lines of the classification for the lateraldiscoid meniscus, medial discoid meniscus could also beclassified into complete or incomplete depending upon thecoverage of the medial tibial plateau.
The classical sign for the lateral discoid meniscus4 is notseen in the medial discoid. Most often the symptoms andclinical findings point towards medial meniscus pathology,usually a tear5.
Massive medial discoid meniscus is subject tocompressive and rotatory strains6. This combined with itsthickness usually results in a mid-substance horizontalcleavage tear often communicating with one of its surfaces6,7.In our case the presenting symptom was suggestive of amedial meniscal cyst which was secondary to the horizontalcleavage tear.
The radiographic findings are inconsistent, draw asurgeon’s attention retrospectively 5,8,9. The definitivediagnosis is made at arthroscopy, though magnetic resonanceimaging, being non-invasive, is being increasingly practicedbefore an arthroscopy9.
The treatment consists of treating the pathologyproducing the symptoms in the discoid meniscus. In our casethe meniscus was shaped to give it an anatomical shape andin this process the cyst had got decompressed too. A varietyof associated congenital intra-articular anomalies have alsobeen observed but whether or not to tackle them at the samesitting is still debatable10.
References
1. Smile IS. The congenital discoid meniscus. J Bone Joint Surg (Br).1948; 30: 671-682.
2. Kaplan EB. Discoid lateral meniscus of the knee joint. J Bone JointSurg (Am). 1957; 39: 77-87.
3. Clark CR, Ogden JA. Development of the menisci of the human kneejoint. J Bone Joint Surg (Am). 1983; 65: 538-547.
4. Jeannopoulos CL. Observations on discoid menisci. J Bone JointSurg (Am). 32: 649-652.
5. Dickson JM, Pizzo WD, Blazina ME et al. A series of ten discoidmedial menisci. Clin Orthop. 1982; 168: 75-79.
6. Johnson RJ, Simmons EH. Discoid medial meniscus. Clin Orthop.1982; 167: 176-179.
7. Comba D, Quaglia F, Magliano G. Massive discoid medial meniscus.Acta Orthop Scand. 1985; 56: 340-341.
8. Weiner B, Rosenberg N. Discoid medial meniscus. Association withbone changes in the tibia. J Bone Joint Surg (Am). 1974; 56: 171-173.
9. Narvekar A, Acharya A, Shroff M. Bilateral discoid menisci with ab-normal attachment to the anterior cruciate ligament – A case report.Acta Orthop Scand. 1999; 70 : 387-389.
10. Kim SJ, Lee YT, Kin DM. Intraarticular anatomic variants associatedwith discoid meniscus in Koreans. Clin Orthop. 1998; 356: 202-207.
Fig 3 : Intraoperativearthroscopicfinding of themedial discoidmeniscus.
MASSIVE DISCOID MEDIAL MENISCUS PRESENTING AS A MENISCAL CYST

Introduction
Extrapulmonary tuberculosis in the form of skeletalinvolvement is fairly common, though isolated patellarinvolvement is rare1-3. Two such cases are discussed withtheir clinical and radiological features which help indifferentiating tuberculosis from other similar lesions.
Case Report
Case I : An apparently healthy 22 year male presentedwith a complaint of pain, swelling and some restriction ofmovements of the right knee for last 2 months. Patient had noconstitutional symptoms and denied any history suggestiveof tuberculosis. Examination of the knee revealed swellingand tenderness over the patella, mild effusion, no synovialthickening and loss of terminal 20-30o of flexion. There wasmild atrophy of the quadriceps and significant inguinallymphadenopathy. Laboratory investigations revealed ahaemoglobin of 11 gm/dl, a total leucocyte count of 8300 mm3
with lymphocytosis and a high erythrocytic sedimentationrate (ESR) of 42 mm/1st hour (Westergren). Mantoux test gavean induration of 20 mm at the end of 72 hours. Chest X-raywas normal. Radiograph of the knee joint demonstrated alytic lesion in the lower pole of patella containing sequestratewithout any marginal sclerosis.
Case II: Our second patient was young female with ruralbackground who presented with progressive pain andswelling over the anterior aspect of the right knee for lastfour months. Patients had no past history of cough orexpectoration, though she had some loss of weight andappetite. On examination knee was found to be swollen andwarm, but the range of knee motion was normal. Tapping onthe patella was painful and no synovial thickening waspresent. Matted inguinal lymphnodes were present.Laboratory investigations revealed a haemoglobin of 7.4 gm/dl, total leucocyte count of 6200/mm3 with mild lymphocytosis
Tuberculosis of the patella – A case reportRoop Singh, Rakesh Gupta
Department of Orthopaedics, Physical Medicine, Parapelgia and Rehabilitation, Pt BD Sharma PostGraduate Institute of Medical Sciences, Rohtak
Roop Singh, MS (Orth), Assistant Professor **Rakesh Gupta, MS (Orth), Associate ProfessorDepartment of Orthopaedics, Physical Medicine, Parapelgia and Rehabilitation,Pt BD Sharma Post Graduate Institute of Medical Sciences, Rohtak 124001,Haryana
and ESR of 52 mm/1st hour. Mantoux test gave an duration of22mm at the end of 72 hours. Chest X-ray was normal.Anteroposterior, lateral and skyline view of the knee jointshowed osteolytic lesion of patella containing sequestrate(Fig. 1). Fine needle aspiration cytology revealed classicaltubercular granulomas.
Both the patients were subjected to surgical debridement.Operative findings consisted of cavities full of unhealthygranulation tissue with few sequestrate lying inside but therewas no communication to the joints. Knees were immobilizedpostoperatively to give rest to the part. Histopathologicalexaminations in both the patients revealed chronicgranulomatous tissue with areas of caseous necrosis andLanghans type giant cells, confirming the diagnosis oftubercular infection. The patients were put on appropriateantitubercular regimen. After a follow up of 12-18 monthslesions healed clinically and radiologically with full kneemovements in both the patients (Fig. 2).
Discussion
Knee joint is the third most common joint affected byosteoarticular tuberculosis after spine and hip joint4. Isolatedtubercular patellar involvement is very uncommon withliterature reporting an incidence of 0.09 to 0.15%1). Differentialdiagnosis of such lesion varies from tumours like
Fig 1 : Anteroposterior and lateral radiograph of the right knee atthe time of presentation showing an osteolytic area in the lowerpole of patella with sequestrate.
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 189-190
VOL. 38, NO. 3, JULY 2004 189

INDIAN JOURNAL OF ORTHOPAEDICS190
chondroblastoma, osteoblastoma, infected aneurysmal bonecyst to metastatic lesions; tumor like conditions eg. Browntumor; and inflammatory lsions such as gout, pyogenic andfungal osteomyelitis 2,5.
Osteolytic lesion with a sequestrum is usually consideredto be infective in nature and absence of marginal sclerosisshould suggest tuberculosis, through, its value as absolutediagnostic criteria is debated in the literature. Althoughradionuclide bone scan and CT scan have been reported inthe literature as excellent diagnostic aids for diagnosing suchlesions2,3, but these are not universally available and areexpensive. Patellar bone is easily accessible bone for the
needle aspiration cytology and it can be used for earlyconfirmation of diagnosis, as was done successfully in oursecond case. Surgical debridement can also serve as adiagnostic tool for confirmation of the diagnosis, besidesbeing therapeutic in nature.
An early diagnosis followed by definitive treatment isdesirable in such cases in view of proximity of the knee jointto such lesions. Results in both of our patients after surgicaldebridement and ATT were good as the diagnosis was madeearly and prior to the involvement of the joint. Tuberculosisis not so common in the west, but is fairly common incountries like India. Hence in osteolytic lesions of the patellapossibility of tuberculosis should always be considered,inspite of it being rare.
References
1. Dhillon MS, Rajsekhar C, Nagi ON. Tuberculosis of patella ; report ofa case and review of literature. Knee. 1995 ; 2 : 53-56.
2. Shah P, Ramakantan R. Tuberculosis of the patella. Br J Radiol. 1990;63 : 363-364.
3. Dhillon MS, Rao SS, Sandhu MS, Vasisht RK, Nagi ON. Tuberculo-sis of the patella. Skeletal Radiol. 1998 ; 27 : 40-42.
4. Tuli SM. Tuberculosis of skeletal system . New Delhi. Jaypee BrothersMedical Publishers. 1991.
5. Ehara S, Khurana JS, Kattapuram SV, Rosenberg AE, El-KhouryGY, Rosenthal DL. Osteolytic lesion of the patella. Am J Roentgenal.1989 ; 153 : 103-106.
Fig 2 : Skyline view radiograph of the same patient shows welldefined osteolytic lesion. No articular involvement is seen.
ROOP SINGH, RAKESH GUPTA
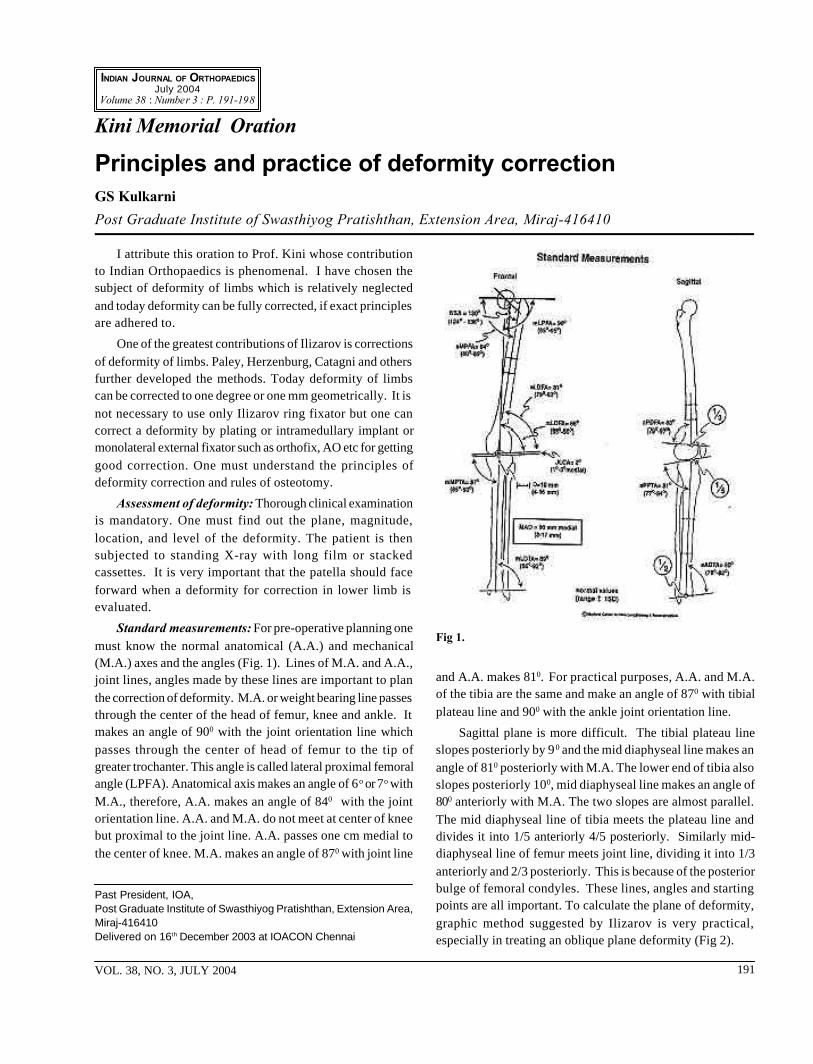
I attribute this oration to Prof. Kini whose contributionto Indian Orthopaedics is phenomenal. I have chosen thesubject of deformity of limbs which is relatively neglectedand today deformity can be fully corrected, if exact principlesare adhered to.
One of the greatest contributions of Ilizarov is correctionsof deformity of limbs. Paley, Herzenburg, Catagni and othersfurther developed the methods. Today deformity of limbscan be corrected to one degree or one mm geometrically. It isnot necessary to use only Ilizarov ring fixator but one cancorrect a deformity by plating or intramedullary implant ormonolateral external fixator such as orthofix, AO etc for gettinggood correction. One must understand the principles ofdeformity correction and rules of osteotomy.
Assessment of deformity: Thorough clinical examinationis mandatory. One must find out the plane, magnitude,location, and level of the deformity. The patient is thensubjected to standing X-ray with long film or stackedcassettes. It is very important that the patella should faceforward when a deformity for correction in lower limb isevaluated.
Standard measurements: For pre-operative planning onemust know the normal anatomical (A.A.) and mechanical(M.A.) axes and the angles (Fig. 1). Lines of M.A. and A.A.,joint lines, angles made by these lines are important to planthe correction of deformity. M.A. or weight bearing line passesthrough the center of the head of femur, knee and ankle. Itmakes an angle of 900 with the joint orientation line whichpasses through the center of head of femur to the tip ofgreater trochanter. This angle is called lateral proximal femoralangle (LPFA). Anatomical axis makes an angle of 6o or 7o withM.A., therefore, A.A. makes an angle of 840 with the jointorientation line. A.A. and M.A. do not meet at center of kneebut proximal to the joint line. A.A. passes one cm medial tothe center of knee. M.A. makes an angle of 870 with joint line
Kini Memorial Oration
Principles and practice of deformity correctionGS Kulkarni
Post Graduate Institute of Swasthiyog Pratishthan, Extension Area, Miraj-416410
and A.A. makes 810. For practical purposes, A.A. and M.A.of the tibia are the same and make an angle of 870 with tibialplateau line and 900 with the ankle joint orientation line.
Sagittal plane is more difficult. The tibial plateau lineslopes posteriorly by 90 and the mid diaphyseal line makes anangle of 810 posteriorly with M.A. The lower end of tibia alsoslopes posteriorly 100, mid diaphyseal line makes an angle of800 anteriorly with M.A. The two slopes are almost parallel.The mid diaphyseal line of tibia meets the plateau line anddivides it into 1/5 anteriorly 4/5 posteriorly. Similarly mid-diaphyseal line of femur meets joint line, dividing it into 1/3anteriorly and 2/3 posteriorly. This is because of the posteriorbulge of femoral condyles. These lines, angles and startingpoints are all important. To calculate the plane of deformity,graphic method suggested by Ilizarov is very practical,especially in treating an oblique plane deformity (Fig 2).
Past President, IOA,Post Graduate Institute of Swasthiyog Pratishthan, Extension Area,Miraj-416410Delivered on 16th December 2003 at IOACON Chennai
Fig 1.
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 191-198
VOL. 38, NO. 3, JULY 2004 191

INDIAN JOURNAL OF ORTHOPAEDICS192
Malalignment and malorientation tests: Malalignmenttest determines the magnitude, level and site of deformity. Itis done by plotting the M.A. line passing through the centerof the head of femur, knee and ankle. Similarly the M.A. oftibia and joint orientation lines of knee and ankle aremeasured.
Hidden deformities
Alongwith an obvious deformity, there may be a hiddendeformity, which can be detected by plotting the axes andjoint lines. When the obvious CORA (center of rotation ofangulation) does not coincide with true apex, there is anotherdeformity at a different level (which may be the hiddendeformity) or there is translational deformity. Hiddendeformities can be detected by plotting the CORA or trueapex and obvious or false apex. When CORA does notcoincide with the obvious apex it indicates two deformities.The deformity is then managed by osteotomy with followingoptions.
Option I – Two osteotomies at two CORAs
Option II – One osteotomy at resolution point.
If there are two CORAs, two osteotomies will correctboth anatomic and mechanical axes (Fig 3).
Rules of osteotomy
Rule 1: Osteotomy should pass through the bisector line.If the hinge is placed on the convex side, opening wedgeosteotomy occurs. If on concave side, closing wedge, if atcenter, half closing and half opening (neutral wedge) is there.The line which bisects the obtuse angle is called a bisector line.
Rule 2: If the osteotomy is done at a different level thanthe CORA, then translation occurs. This is made use of inH.T.O. (Fig. 4a)
Rule 3: If osteotomy is done at a different level thanCORA but hinge placed at osteotomy site, mechanical axisbecomes parallel but anatomical axis becomes zigzag. This isused in certain situations (Fig. 4b).
Rule 4: Where M.A. of proximal and distal segments meet,it is called as resolved CORA. If osteotomy is done at resolvedCORA, the limb is functionally normal and avoids multipleosteotomies.
Rule 5: If the osteotomy is performed through theresolution point CORA rather than the true multiple apices,then the mechanical axis and joint orientation will be correctedwith a residual alteration in the anatomic axis of the bone.This may be a cosmetic problem but it does not affect jointorientation or mechanical axis alignment.
Concept of mid segment: If the M.A. or A.A. of proximaland distal segment coincide and the middle segment may beof any length and any deformity, the limb is functionally normalprovided the limb length is normal (Fig 5). If the mechanicalaxes of proximal and distal fragments are collinear, then themiddle segment of any length and any deformity will notcompromise normal function of the limb provided there is nolimb length discrepancy.
Fig 3.Fig 2.
Fig 4(a).
Fig 4(b).
PRINCIPLES AND PRACTICE OF DEFORMITY CORRECTION

VOL. 38, NO. 3, JULY 2004 193
Correction of bowing deformity: Bowing deformity hasmultiple apices. If there is more than one CORA, completerealignment of mechanical and anatomic axes requires morethan one osteotomy for each CORA. The level of the CORAand the magnitude of correction are dependent on the middleaxis line, which can be drawn at different orientations.Therefore, the level and magnitude of one apex determinesthe level and magnitude of the second apex (Fig 6, 7).
Principle of angulation translation
If the CORA is very near the joint, or in the joint, thentranslation of distal fragment is necessary. If open wedgeosteotomy is done at the CORA, then M.A. is perfect. But itis difficult to fix the small fragment, osteotomy needs to bedone at a distance from true CORA. Keep the hinges at theCORA and do osteotomy at the desired level-automaticallytranslation and correction of deformity occurs. When thehinge is placed at the true CORA and osteotomy is done at adifferent level, the fragment which does not contain the hingemoves towards convexity.
Eversion and inversion of sub talar joint can compensate,to some extent, for varus and valgus deformities of ankle
respectively, but supra-malleolar osteotomy is an excellentosteotomy to correct the deformities of ankle and foot,provided the relation of hind-foot to fore-foot is normal. It issimple, easy to do and rapidly healing as it is throughcancellous bone. Principle of angulation translation is used.
Congenital pseudoarthrosis of tibia
For congenital pseudoarthrosis of tibia Ilizarov methodappears to be superior to vascularised fibular graft. Resectionof the lesion, bone transport and bone grafting are indicatedin dysplastic type with tapering ends (Fig 9). For bone andperiosteal grafting, a three inch incision is made on the iliaccrest. Iliac growth cartilage is separated as a whole. Soft tissueis cut from the outer surface of periosteum, which is separatedfrom bone sub periosteally. Bone graft of 2” by 1” size isobtained. A small 3 mm curette is inserted & cancellous boneis curetted. Enough quantity of graft is obtained. Afterresection and docking of the bony ends, bone graft is laidaround the non union site, over which the periosteum iscovered with smooth surface facing the graft.
In the cystic type with thick bone, compression with orwithout bone transport is necessary. Resection may not be
Fig 6.
Fig. 5
GS KULKARNI

INDIAN JOURNAL OF ORTHOPAEDICS194
needed.
Today there is no problem of union of pseudoarthrosisbut refracture occurs in 30 to 50%. Refracture is due to - i) Ongoing disease, and ii) Residual angular deformity. To preventresidual deformity, an intramedullary nail is passed throughmedial malleolus. Fibular pseudoarthrosis should also betreated similarly. The results of surgery before the age of 4are poor. Our experience is of 33 cases of which 30 unitedwhile 11 had refracture.
Non union
Aseptic non-union: Most of the aseptic non unions canbe treated by internal fixation.
Aseptic hypertrophic non union with deformity: Mostof these can be treated by interlocking nail or a plate. Howeverif there is lot of sclerosis, a nail can not be negotiated and ifthere is a large bump, plating is difficult. These are theindications for Ilizarov method (Fig. 10). Another indicationis hypertrophic non union with deformity which is treated byfirst correcting the deformity, then distraction 0.5 mm dailyfor 20 days, 20 days of no distraction, finally compression(accordion method).
Infected Non-union
I have classified the infected nonunion in 3 types
Type I: Mild infection- A bead of pus is seen on pressing,but no deformity. With debridement, antibiotic and two ringsor functional cast or brace for 6 to 8 weeks, the fracture mightunite.
Type II: Moderate infection but no deformity, noshortening, no gap.
Type III: Severe infection with deformity, gap orshortening. Treatment consists of through debridement,reaming intramedullary canal, vancomycin beads, corticotomyand Ilizarov fixator. Bone transport may be needed, if gap > 2
cms. Thorough debridement consists of removal of implants,infected soft tissues, sequestrii etc. Bony ends are excisedtill punctuate bleeding is seen. Then tourniquet is releasedand medullary canal is reamed. Antibiotic beads and /or a rodis inserted.
To make antibiotic beads 40 grams of bone cementpowder (PMMA) is taken, 2 gms of antibiotic Vancomycin orGentamycin ( in powder form ) or Tobramycin or any newerthermostable antibiotic is added to it. Now the liquid polymeris added to it. When it becomes a paste, it is wrapped around6 mm or 7 mm Kuntschner nail of the required length, measuredclinically or radiologically and smoothened by rolling betweenthe 2 palms. The diameter of the composite nail should beuniform; it is passed through the hole of a nail gauge so thatthe proper diameter is achieved. For tibia we usually take 6mm or 7 mm Knail, for femur 7 mm or 8 mm nail. While thecement is still soft, nail is bent as required, i. e. create Herzog’sangle. The remaining cement is used to prepare chains ofbeads using a 14 gauge wire.
Fig 7. (a) Severebowingdeformity oflimb, (b) aftercorrection
Fig 8. Open wedge or close wedge or dome supramalleolarosteotomy
Fig 9. Congenital pseudoarthrosis of tibia treated with bonetransport
(a) (b)
PRINCIPLES AND PRACTICE OF DEFORMITY CORRECTION

VOL. 38, NO. 3, JULY 2004 195
We have treated total number of 240 cases ; 220 unitedafter multiple operations ; ten lost to follow up and eight didnot united at all inspite of multiple operations. Amputationwas carried out in two.
Chronic osteomyelitis with deformity
Chronic osteomyelitis, a common disease may present inmany ways, as with deformity of the bone; non union of thepathological fracture with or without deformity; shorteningwith or without gap non union; associated joint stiffness ordeformity.
All these problems can be solved in one stage by Ilizarovmethod. A thorough debridement and reaming of the
medullary canal, if infected are mandatory. Dead bone andsoft tissue are boldly excised. Even a large gap can besatisfactorily closed by bone transport and limb lengthening.Placement of vancomycin beads in the debrided area hasgiven excellent results. Beads or antibiotic rod may be insertedin the medullary canal. “Infection burns in the fire ofregenerate”—Ilizarov, is not true in all cases but only whenthe sequestrae are small or absent.
Hip reconstruction by pelvic support osteotomy
This is a good procedure for many hip diseases in ourcountry, especially in the young.
Fig 10. Non union of tibia with hypertrophic fibula treated with distraction with ring fixator. Note new bone formation at the tibialnon union site and union of fracture.
Fig 11. (a) The case of acute osteomyelitis of tibia with pathological fractures at both ends, (b) Severe varus deformity and 8 cm shorteningtreated with resection, (c) Limb lengthening by bone transport, (d) Second Limb lengthening, (e) Limb Lengthening over a nail,(f) Clinical photograph in 1989, 1995 and in 2003
(a) (b) (c)
(d) (e) (f)
GS KULKARNI

INDIAN JOURNAL OF ORTHOPAEDICS196
Indications:
1. Advanced TB hip when both head and acetabulumare destroyed.
2. Old septic arthritis
3. Advanced O.A. hip due to AVN and other causes whentotal hip replacement (THR) is contraindicated or patientrefuses THR because of socio-economic reasons.
Principle is to create an abduction deformity of the hip.An X-ray of pelvis with both hips is taken with the affectedhip in maximum adduction. To maximum adduction 15 degreesis added. This will be the angle of abduction at the sub-trochanteric osteotomy. Distal femoral osteotomy is alsodone to prevent valgus deformity of knee and to restore limblength.
THR is a good operation in the elderly but in the youngit is associated with many complications and socio-economicproblems. Our patients demand squatting and sitting cross-legged.
Club foot
Ponseti technique of correcting club foot has givenexcellent results and is now followed in most of the centersacross the world. This technique eliminates all the compo-nents of the congenital clubfoot deformity so that the patienthas a functional, pain-free, normal-looking, plantigrade foot,with good mobility, without callosities, and requiring nomodified shoes and avoiding major surgery which results instiff painful foot though the patient has a plantigrade foot.
Ponseti manipulation and plaster cast is started on day1, weekly change of cast for 6 weeks. If equinus is not
corrected, percutaneous tenotomy is done under localanesthesia.
Technique: All the components of the clubfoot deformityhave to be corrected simultaneously with the exception ofthe equinus which should be corrected last.
1. The cavus, which results from a pronation of the forefootis corrected as the foot is abducted by supinating theforefoot and thereby placing it in proper alignment withthe hindfoot. Do not pronate forefoot.
2. While the whole-foot is held in supination and in flexion,it can be gently and gradually abducted by applyingcounter-pressure with the thumb against the lateralaspect of the head of the talus.
3. The heel varus and foot supination will correct when theentire foot is fully abducted in maximum external rotationunder the talus. The foot should never be everted.
4. Finally the equinus can be corrected by dorsiflexing thefoot. The tendo Achilles may need to be subcutaneouslysectioned to facilitate this correction.
Calcaneus should never be held while manipulating. Thekite mistake was to hold the thumb at the calcaneo-cuboidjoint. It took 40 years for the orthopaedic surgeons to movethe thumb 1 cm superior to head to talus from calcaneo-cuboid joint.
We have treated 40 cases of CTEV by Ponseti technique,of these 2 needed soft tissue surgery and three needed tibialisanterior transfer to 3rd cuneiform.
PRINCIPLES AND PRACTICE OF DEFORMITY CORRECTION
Fig 12. A case of post polio equinusdeformity with hand to knee gait.Distraction of soft tissues of foot tocorrect the deformity. Note thecorticotomy for limb lengthening.

VOL. 38, NO. 3, JULY 2004 197
Adult club foot
After the age of 12, we treat club-foot by triple osteotomyas in triple arthrodesis. Only subchondral bone is exposed.The talus, calcaneus, cuboid and navicular are compressedfor 6 days then slowly distracted with Ilizarov to correct thedeformity. Excellent regenerate is formed. Finally triplearthrodesis is achieved. We have done 8 cases, withsatisfactory results.
Polio
Ilizarov is an excellent method of treating polio patients.All deformities and limb length discrepencies can be correctedat the same time in one stage. Minimal soft tissue release anddistraction by external fixator give satisfactory results(Fig. 12).
Complications of Ilizarov method: All complicationsare preventable and treatable. Vascular injury is due to faultyinsertion of wire or pins. I never had vascular complications.We had 3 cases of common peroneal nerve injury- allrecovered. Main problem is the stiffness of joints especiallyflexion deformity of knee and equinus of foot while doinglimb lengthening. Extensive physiotherapy from day one andcounselling of patients and parents is important. Refracturesand poor regenerate can be successfully treated by injectionof bone marrow, bone graft or compression and distraction.Treatment of stiff joints by arthrodiatasis (Distractionarthroplasty) is very useful in the management of stiff joints.Other common complications are the pin tract infection andpain.
Fibular hemimelia: Three elements of fibular hemimelianeed to be corrected.
1) Correction of foot deformities by postero lateral softtissue release, which consists of excision of fibular anlage.
This is postero lateral release as opposed to postero medialrelease in CTEV
2) Limb lengthening
3) Correction of bowing deformity of tibia.
All three may be done in one, 2 or 3 stages.
Extra-articular soft tissue releases (tendo-achilles,peroneal tendons, interosseous membrane remenants, andfascial bands ) lead to some improvement in foot position.Supramalleolar osteotomy is done to correct valgus andprocurvatum deformity.
The prognosis is good if there are more than 2 rays. Ifthere is only one ray, amputation is a better option.Unsatisfactory results are due to recurrent residual deformityof the foot.
Proximal femoral focal deficiency
Proximal femoral focal deficiency (PFFD) includes a broadspectrum of defects ranging from minor hypoplasia of thefemur to complete agenesis of the femur. Unstable hip joint,shortening, fibular hemimelia and agenesis of the cruciateligaments of the knee and other anomalies may be associatedwith it.
Bilateral PFFD is best treated non-operatively. Thesepatients can walk well without prostheses, but for social orcosmetic reasons extension prostheses may be provided.Patient learns to accept their short stature and is quitefunctional. Knee fusion is not indicated because the kneefunctions in conjunction with the hip pseudoarthrosisprovides useful motion.
Stability of the hip and knee is important as a determiningfactor in the treatment. Establish continuity between thefemoral head and the femur. This may be technically difficult.Surgery is best delayed till ossification of the femoral head
Fig 13. A case of severe coxa vara and short limb (PFFD). Note the correction of hip and limb length restored by lengthening bothtibia and femur.
GS KULKARNI

INDIAN JOURNAL OF ORTHOPAEDICS198
and proximal metaphysis is adequate. Knee fusion isperformed, creating a one-bone leg. Autogenous bone graftsshould be added to the pseudarthrosis site. With advanceddevelopment of hip reconstruct many of these grotesque limbscan be salvaged (Fig. 13). Subluxation and dislocation duringfemoral lengthening may occur especially with acetabulardysplasia.
Regardless of technique, limb lengthening in patientswith PFFD is difficult with the ever present danger of kneeand hip subluxation. If decided, should be done in 3 or 4stages. Most children with PFFD can learn to walk withoutprosthesis, but prosthesis helps to equalize leg lengths.
Ankle and foot considerations1
In the sagittal plane, the articular surface of the talus iscircular. The three-dimensional shape of this surface is afrustum ( section of a cone ). Therefore, the axis of anklerotation is not parallel to the joint line. The axis normallyruns from the tip of the medial maleolus to the tip of thelateral malleolus, passing through the lateral process of thetalus. Clinically, it is best evaluated from behind.
Frontal plane ankle deformities
Varus and valgus deformities of the tibial plafond arenormally compensated for by the subtalar joint. The normalsubtalar range of motion is 300 inversion and 150 eversion.Therefore, the amount of ankle angulation that can becompensated by the hind-foot is 300 valgus and 150 varuswhen normal subtalar motion is present.
Varus deformity of the tibial plafond is tolerated lessthan is the valgus deformity because there is normally halfthe compensatory range of motion of subtalar eversioncompared with inversion.
Varus deformity of the tibial plafond is unlikely to lead todegenerative changes. This is because the contact area ofweight bearing between the tibia and talus is not decreasedand may actually be increased because of increased loadtransfer from the medial facet of the talus to the very widemedial malleolus.
In contrast, valgus deformity of the tibial plafond maylead to degenerative changes of the ankle joint despite thefoot’s greater ability to compensate for valgus than for varus.
When correcting the severe deformities of the ankle joint,nerves are likely to be compressed. Therefore, tarsal tunneldecompression may be required.
Sagittal plane ankle deformities.
Plantar flexion and dorsiflexion of the ankle jointcompensate for recurvatum and procurvatum deformitiesrespectively, of the distal tibia. The ankle joint normally has200 of dorsiflexion and 500 of plantar flexion range of motion.Therefore, the ankle joint can compensate for more recurvatumthan procurvatum. For this reason, recurvatum of distal tibialdeformity is better tolerated than is procurvatum deformity.Uncompensated procurvatum deformity presents as anequinus deformity. It is symptomatic because the foot is inequinus and also because of impingement of the anteriortibial lip on the neck of the talus.
The closer the CORA is to the ankle joint, the greater isthe malorientation of the ankle joint (greater LDTA )
References
1. Paley D. Principles of Deformity Correction. Springer, 2002
2. Herring JA. Tachdijian’s. Paediatric Orthopaedics. III ed. Vol-III. 2002
3. Bar H F, Hreitfuss H. analysis of angular deformities on radiographs. JBone Joint Surg (Br). 1989 ; 71 : 710.
4. Chao EYS, Neiuheni EVD, Hus RWW, Paley D. Biomechanics ofmalalignment. Orthop Clin North Am. 25 : 379,1994.
5. Coventry M B. Upper tibial osteotomy for osteoarthritis. J Bone JointSurg (Am). 1985; 67 : 1136.
6. Herzeberg J E Waanders N A. Calculating rate and duration ofdistraction for deformity correction with the Ilizarov technique. ClinOrthop. 1991; 22 : 601.
7. Ilizarov G A. The tension stress effect on the genesis and growth oftissues : Part II-The influence of the rate and frequency of distraction.Clin Orthop. 1989 ; 238 : 263.
8. Masr JW Teitge, RA Gowda. Preoperative planning for the treatmentof non-unions and the correction of malunions of the long bones : OrthopClin North Am . 1990; 21; 693, 1990.
9. Paley D, Tetsworth KT. Mechanical axis deviation of the lower limbs-preoperative planning of uniapical angular deformities of the tibia orfemur Clin Orthop. 1992; 280: 48-64.
10. Paley D, Tetsworth KT. Mechanical axis deviation of the lower limbs-preoperative planning of multiapical frontal plane angular and bowingdeformities of the femur and tibia. Clin Orthop 1992 ; 280 ; 65-71.
11. Paley D, Tetsworth KT. Deformity correction by the Ilizarov tech-nique. In Chapman M (Ed): Operative Orthopaedics, 1993; Vol-1. JBLippincott : Philadelphia, 883-948.
12. Paley D. Problem, obstacles and complication of limb lengthening bythe Ilizarov technique. Clin Orthop. 1990 ; 250:81.
13. Shoji H, Insall J. High tibial osteotomy for osteoarthritis of the kneewith valgus deformity. J Bone Joint Surg (Am). 1973 ; 55 : 963.
PRINCIPLES AND PRACTICE OF DEFORMITY CORRECTION

Bone grafting is a standard Orthopaedic procedureperformed in clinical practice. In India, approximately 800,000such procedures are performed annually. Autogenous graftis gold standard and the preferred graft used. However,allograft bone continues to play an important in manyorthopaedic reconstructive procedures. One has to resort tothe allogenic source especially in filling up of large or multiplecontainable cavitary lesions, structural reconstruction of largecircumferential osteoperiosteal defects after tumour resectionand traumatic bone loss, extensive spinal fusions for grossdeformities or severe instabilities and repeat surgeries aftertotal joint replacement1,2. These procedures demand abundantquantity of bone which the recipient’s body cannot supplywithout significant donor area morbidity and risks.
Autogenous bone graft is osteogenic, osteoinductive,osteoconductive and completely biocompatible. Osteogenicactivity implies that the living bone forming cells such asosteoblasts or osteocytes have survived the transplantationand are active in the recipient area. This is possible only inautogenous fresh cancellous bone grafts and to a smalldegree in fresh cortical compact bone grafts. There is nosubstitute to autogenous bone graft yet available whichembodies all these qualities 3 . Some of the alternatives orsubstitutes currently available for clinical use are discussedas follows.
Allogenic bone graft has been the most obviousalternative to autogenous material. It has been widely usedfor structural reconstruction or foar filling up of cavitarylesions. Fresh untreated allografts are presently not usedbecause of immune reaction and the risk of transmission ofdisease. At present popularly allogenic bone is preserved bydeep freezing (-80 to -100 degrees centigrade) or freeze-drying(and vacuum sealed) or by radiation for long termpreservation.
These techniques have been shown to maintain sterility,reduce immunogenicity and provide adequate structuralintegrity, however, these procedures also reduce the boneforming biological activity (Table I). Frozen grafts requirethawing ; freeze dried grafts require hydration before
IOA White paper
Bone grafts and bone substitutes in clinical OrthopaedicsSM Tuli
implantation, and the unused graft can not be represerved ;deproteinated grafts must be composited with BMPs orautogenous cancellous bone.
Demineralised bone matrix provides the most potent bonemorphogenetic (bone induction principles) agents1-9. Itsviability however, depends upon the influence of processesof preparation and preservation. Total demineralization leavesbehind the matrix with leather-like texture and pliability withno mechanical strength.
Partially decalcified allogenic bone (decalbone) appearsto be the most appropriate substitute to autografts becauseit has adequate mechanical strength, is biocompatible,biodegradable, bioactive and the ideal natural scaffold forinduction and growth of new bone. Compactly filled cavitarylesions, and the mass of decalbone used as structural graftsprovide adequate biomechanical strength. The bioactive andexposed bone matrix provides adequate quantity of bonemorphogenetic proteins and other local growth factors at thesite of desired action.
Bone morphogenetic protein (BMP) is considered themost active biological agent responsible for osteoinductionand resultant success of the allografts 10,11. The method ofextraction of BMP is quite complicated and tedious and thequantity of the active agent obtained is very small;approximately one mg from one kilogram wet weight of bone.If one were to use BMPs for posterior spinal fusion the costis approximately US $ 3000 for one case. Having obtained theBMP some workers and manufacturers are recombining itwith other porous biological or synthetic materials which actas ‘spreaders’ of BMP and serve as osteoconductive inertmaterial. The materials with which the biologically activeagent has been combined are bone gelatin, B-tricalciumphosphate, hydroxyapatite, absorbable glass ceramics,collagen matrix, plaster of paris etc1,2,12. However, if one isusing partially demineralised allogenic bone the BMPs arealready spread uniformally on the natural cancellated matrixframe work.
Miscellaneous Materials
Autoclaved and irradiated autogenous bone has beenused successfully under certain circumstances where
Dr. SM Tuli, 6 Park Avenue, Maharani Bagh, New Delhi – 110065Delivered at IOACON 2003, Chennai
VOL. 38, NO. 3, JULY 2004 199
INDIAN JOURNAL OF ORTHOPAEDICSJuly 2004
Volume 38 : Number 3 : P. 199-202
Key-words : Bone graft, Bone substitutes, Allogenic bone, Bone regeneration

INDIAN JOURNAL OF ORTHOPAEDICS200
expertise for resection and reconstruction was availablehowever adequate conventional bone grafts were notavailable13-15. Formaline treated and preserved allograft hasalso been used successfully 16.
Bioabsorbable non-allogenic bone substitutes (ceramics)mainly composed of hydroxyapatite, tricalcium phosphate orcalcium sulphate are now commercially available for clinicaluse17-19. They have intercommunicating micropores for readypenetration and ingrowth of neocapillaries and accompanyingcells. They act essentially as osteoconductive material. Fortheir success autoclaved bone, irradiated bone and ceramicsmust be composited with autogenous cancellous bone, BMP,bone marrow stromal cells or other growth factors.
Contents of bone grafts and their role
There are three major components of a bone graft- themineral, the matrix frame work and the cells. In general calciumhydroxyapatite provides an inert frame work providingmechanical stability and offering a lattice work for penetrationof reparative tissues and osteoconduction. Only the mostsuperficial bone forming cells which survive getting nutritionby tissue perfusion, provide osteogenic activity in the freshautografts. In allografts no viable cells are expected, howeverthe debris of dead cells act as the most potent immunogenicagent. Organic matrix provides the most potent morphogenetic(bone induction principles) agents. Its viability howeverdepends upon the influence of processes of allograftspreparation and preservation (Table II)1,4-9,20.
Table II . Contents of bone grafts and their roleCa Hydroxyapatite Mechanical stabilityCells Auto surviving OsteogenesisCells Allo. Non surviving Immunogenesis
Matrix Bone morphogenetic agents
Immunogenecity of allogenic bone is now betterunderstood. Fresh unmatched and un-treated allogenic boneinevitably evokes an immune response in the host21-23. Theimmune response in general is delayed, mild and developsslowly, however it results in ‘unexplained’ graft resorption
and delay or failure in its incorporation24-27. In clinical practicedeep freezing, freezing, freeze drying and irradiation arecurrently employed to reduce immunogenecity. Pure BMPfrom allogenic source or even xenogenic source is consideredto have negligible immunogenecity.
General principles of operative procedures and postoperative management
Standard principles of orthopaedic operations areemployed with respect to soft tissue dissection and sterilityas observed in major implant surgery. The basic rules are thesame whether one is using autogenous or allogenic bone orbone graft substitutes.
For cavitary lesions and for posterior spinal fusion oneshould preferably shape grafts as long slivers, and placethem in the bed along the direction of loading. The minimumdimension of the graft should be between 4 and 5 mm in anyorientation. The grafts cut smaller than 4mm, minced ormorsellised grafts do not have any mechanical strength andprobably the biological activity of the matrix also getsdamaged. At best such grafts act as fillers. For structural orintercalary defects the volume of the graft should be almostdouble the volume of the bone being replaced. In clinicalpractice however the volume would depend upon theavailability of adequate soft tissue coverage.
Cavitary lesion: The contents of the cavity arethoroughly curetted through an elliptical shaped adequatesize of a window, the cavity is compactly packed with thebone graft slivers or small pieces. The slivers are preferablyplaced along the lines of load bearing.
Osteoperiosteal gaps: In case aggressive tumour anextra-lesional enbloc resection is performed. The graft is cutto a suitable size and shape and fixed in the bed generallywith a long intramedullary implant.
Spinal fusion: The recipient bed is decorticated.Abundant graft is placed oriented along the long axis of spine.In cases with gross mechanical instability suitable implantwith multi-segmental fixation is desirable.
BONE GRAFTS AND BONE SUBSTITUTE IN CLINICAL ORTHOPAEDICS
Table I. Commonly used bone grafts in clinical OrthopaedicsFresh autogenous Fresh unprocessed Frozen/ freeze Partially Deproteinized
allogenic dried allogenic decalcified allogenic allogenicOsteoinduction ++++ +++ +++ ++++ 0Osteoconduction +++ ++ ++ +++ ++Osteogenic ++ 0 0 0 0Immunogenecity 0 +++ ++ + 0Mechanical strength +++ +++ ++ ++ ++Cost ?+ + +++ + +++

VOL. 38, NO. 3, JULY 2004 201
Postoperative protection and functional loading: Forcavitary lesions of upper limb all physiological functions arepermitted (3 to 4 weeks post-operative) with suitable orthosisfor 3 to 6 months. For the lesions in the lower limb graduatedloading with protective splints or braces is required for 4 to 8months. When structural bone grafts are used upper limbmajor bones need protection for 1 to 2 years, the lower limbbones (femur or tibia) require suitable bracing encouragingaxial loading for 2 to 4 years. Depending upon the inherentinstability of the spine, the quality of mechanical stabilityprovided by the implant and the neural status of the patient,for ambulation suitable spinal braces should be continuedfor 2 to 3 years.
Biology of bone graft incorporation
The biological process of incorporation of bone grafts ispractically similar to that of a fracture healing 4,21,28-30. Underfavourable environments following major steps occur in acascadal fashion from the time of placement of bone graft inthe recipient bed to its incorporation and remodelingaccording to the Wolffs Law.
Hematoma formation and its organization by invasion ofneocapillaries surrounded by perivascular mesenchymal(pleuripotent) cells.
Osteoclastic and phagocytic resorption of non-viablemineral (calcium hydroxyapatite) and cellular debris andtunneling of the graft makes channels for ingrowth andpropagation of neocapillaries and osteoprogenitor cells.
Conversion (tissue engineering) of osteoprogenitor cellsto osteoblastic cells under the influence of localosteoinductive agents (bone morphogenetic proteins, andother inductive agents) present in the organic matrix of thebone graft, and laying down of the new bone (neo-osteogenesis) on the surface of matrix frame work and alongwith the vascular spaces or channels.
Remodelling of the newly formed bone to conform to thetrabecular pattern along the lines of functional loading andstress (Wolff’s law).
Role of biological and biochemical environments
The above events are slow processes and the graftedarea needs protection with provision for repetitivephysiological axial or functional loading. The mostchallenging clinical condition of structural bone grafting forlarge osteoperiosteal gaps in the lower limbs may take 2 to 4years for adequate incorporation permitting unprotectedloading5,31-36. The mechanical strength of the reconstruct (dueto resorptive activity) is weak for 1 ½ to 2 years, after which
the strength increases by more neosteogenesis. The leasttime is taken in a cavitary pathology which offers a very largeosteogenic bed and copious surface for intimate contact withthe graft37-39. As incorporation takes place from periphery tothe center the time taken for large cavities and large grafts iscorrespondingly longer. In large undemineralised grafts 20to 30 percent (deepest sector) of the grafted bone may neverget incorporated, it may stay incarcerated surrounded bynewly formed bone22,28,32,35. The biologic environment andbiomechanical influences are most favourable for a singlelevel interbody fusion of spine. The recipient bedenvironments, however, become unfavourable whileattempting intercorporeal fusion for more than two vertebralbodies. Well decorticated postero-lateral gutter is an excellentrecipient bed for successful posterior spinal fusion.
Assessment of success, partial success, failures
For purposes of clinical documentation andcommunication generally acceptable definitions for clinical‘success’, ‘partial success’ and ‘failure’ of the bone graftsare as follows.
For cavitary lesions : Success : Incorporation of the graftand filling up of more than 80% of the cavity ; Partial success:Incorporation of the graft with filling up of 50 to 80% of thecavity; Failure : Less than 50% repair of the cavity needing asupplementary operation.
For structural graft used for osteoperiosteal gaps :Success : Restoration of continuity permitting unaided orpartially aided full function and loading of the limb ; Partialsuccess : Incorporation of the graft bridging 50-30% of thegap requiring supplementary bone graft for further repair ;Failure : Bridging of less than 50% of the operated gaprequiring further procedures.
Assertion of failures in spinal fusion procedures isdifficult even with the modern imaging modalities. The onlysure method appears to be a second look by a formal surgicalexposure as advocated by JIP James. This however appearsimpracticable for general use in clinical practice. Breakage ofthe metal fixation, and radiological demonstration ofinstability in stress X-rays are reliable indicators of failure ofthe graft incorporation. Supplementary procedures forobtaining success in large cavities and for osteoperiostealstructural reconstruction in an accepted norm (10 to 20% forcavitary lesions and 20 to 35% for osteoperiosteal gaps).
Major causes of failures are as follows : (i) Scarring orfibrosis in the recipient bed because of prior infection, earlieroperations, extensive trauma, or radiation; (ii) Activeinfection; (iii) Diabetes and other debilitating conditions ;
SM TULI

INDIAN JOURNAL OF ORTHOPAEDICS202
(iv) Prolonged use of systemic steroids and immun-suppressive drugs; (v) Nicotine, alcohol or drug abuse;(vi) Unstable fixation of the grafted area ; (vii) Immunogenicresponse seen as unexplained resorption (viii) Immunogenicresponse seen as unexplained resorption of graft as happensin fresh allogenic or xenogenic grafts; (ix) Oncologicalrecurrence
References
1. Urist M, O Connor B, Burwell RD Eds. Bone grafts, derivatives andsubstitutes , Ox Ford Butterworth, Heinemann 1994.
2. Habal MB, Reddy AH. Eds. Bone grafts and bone substitutes , Phila-delphia, WB Saunders, 1992.
3. Boden SD, Stevenson S Eds. Bone grafting and bone graft substi-tutes. Orthop Clin North Am. 30, 1999.
4. Ludwig SC, Boden SD. Osteoinductive bone graft substitutes forspinal fusion. Orthop Clin North Am. 1999; 30 : 635-645.
5. Einhorn TA, Lane JM, Burstein AH. The healing of segmental bonedefects induced by demineralised bone matrix. A radiographic and bio-mechanical study. J Bone Joint Surg (Am), 1984; 66 : 274-279.
6. Bolander M, Balian G. The use of demineralised bone matrix in repairof segmental defects. J Bone Joint Surg (Am). 1986 ; 68 : 1264-1274.
7. Gepstein R, Weiss RE, Saba K, Hallel T. Bridging large defects inbone by demineralised bone matrix in the form of a powder. J Bone JointSurg (Am). 1987 ; 69 : 984-992.
8. Johnson EE, Urist MR, Finerman GA. Resistant nonunions and par-tial or complete segmental defects of long bones: treatment with im-plants of a composite of human bone morphogenetic proteins (BMP) andautolysed, antigen extracted, allogenic (AAA) bone. Clin Orthop. 1992 ;277 : 229-237.
9. Edwards JT, Diegmann MH, Scarborough NL. Osteo induction ofhuman demineralised bone : characterization in rat model. Clin Orthop.1989 ; 357 : 219228.
10. Urist MR, Silverman BF, Buring K et al. The bone induction principle.Clin Orthop. Clin Orthop. 1967 ; 53 : 243-283.
11. Urist MR. Surface decalcified allogenic bone (SDAB) implant. Clin Orthop.1968 ; 56 : 37-50.
12. Khan SN, Tomin E, Lane JM. Clinical application of bone graft substi-tutes. Orthop Clin North Am . 2000 ; 3 : 289-298.
13. Tuli SM. Traumatic extrusion of the diaphysis of the radius and ulnasuccessfully treated by replacement. J Bone Joint Surg (Am). 1967 ; 49: 745-749.
14. Harrington KD, Johnson JO, Kaufer HN, Luck JV Jr, More TM.Limb salvage and prosthetic joint reconstruction for low grade and se-lected high grade sarcomas of bone after wide resection and replace-ment by autoclaved autogenic grafts. Clin Orthop. 1986 ; 211 : 180-214.
15. Chen WM, Chen TH, Huang CK, Chiang CC, Lo WH. Treatment ofmalignant bone tumours by extracorporeally irradiated autograft pros-thetic composite arthroplasty. J Bone Joint Surg (Br). 2002 ; 84 : 1156-1161.
16. Maini PS. Formalin treated and preserved allografts. Personal commu-nication.1986.
17. Bucholz RW. Non allograft osteoconductive bone graft substitutes.Clin Orthop. 2002 ; 395 : 44-52.
18. Baurer TW, Smith ST. Bioactive materials in Orthopaedic surgery. ClinOrthop. 2002 ; 395 : 11-22.
19. Goel SC. Bone substitutes. Ind J Orthop. 2003 ; 37 : 143-144.20. Kakiuchi M, Ono K. Preparation of bank bone using defatting freeze
drying and sterilizing with ethylene oxide gas part 2 clinical evaluation ofits efficacy and safety. Int Orthop. 1996 ; 20 : 147-152.
21. Horowitz MC, Friedlaender GL. The induction of specific T cell re-sponsiveness to allogeneic bone. J Bone Joint Surg (Am). 1991 ; 73 :1157 – 1168.
22. Stevenson S, Horowitz MC. Current concepts review ; the responseto bone allografts. J Bone Joint Surg (Am). 1922; 74 : 939-950.
23. Strong DM. Friedlaender GE, Tomford WW et al. Immunologicalresponses in human recipients of osseous and osteochondral allografts.Clin Orthop. 1996 ; 326 : 107-114.
24. Chalmers J. Transplantation immunity in bone homografting. J BoneJoint Surg (Br). 1959 ; 41 : 160-179.
25. Friedlaender GE, Strong DM, Sell KW. Studies on the antigenicity ofbone. H Donor specific anti HLA antibodies in human recipients offreeze dried allografts. J Bone Joint Surg (Am). 1984 ; 66 : 107-112.
26. Friedlaender GE. Bone allografts. The biological consequences ofimmunological events. J Bone Joint Surg (Am). 1991 ; 73 : 1119-1122.
27. Langer F, Gross E, West M et al. The immunogenicity of allograft kneejoint transplant. Clin Orthop. 1978 ; 132 : 157-162.
28. Burwell RG. The fate of bone grafts in Apley AG (ed) Recent Advancesin Orthopaedics, Baltimore, Williams & Wilkins. 1979 ; 115-200.
29. Garbuz DS, Masri BA, Czitrom AA. Biology of allografting. OrthopCIin North Am. 1998 ; 29 : 199-204.
30. Stevensons S. Biology of bone grafts. Orthop Clin North Am. 1994 ; 30: 543 – 552.
31. Friedlaender GE, Mankin HJ, Sell KW. Osteochondral allograft :Biology, banking and clinical applications. Boston, Little Brown. 1993.
32. Friedlaender GE, Strong DM, Tomford WW, Mankin HJ. Long termfollowup of patients with osteochondral allografts. Orthop Clin NorthAm. 1999 ; 30 : 583-588.
33. Mankin HJ, Doppelt SH, Sullivan TR et al. Osteoarticular and inter-calary allograft transplantation in the management of malignant tumorsof bone. Cancer. 1982 ; 50 : 613-630.
34. Mankin HJ, Gebhardt MC, Tomford WW. The use of frozen cadav-eric allografts in the management of patients with bone tumours of theextremities. Orthop Clin North Am . 1987 ; 18 : 275-289.
35. Mankin HJ, Gebhardt MC, Jennings LC et al. Long term results ofallograft replacement in the management of bone tumours. Clin Orthop.1996 ; 324 : 86-97.
36. Tuli SM, Srivastava TP, Sharma SV, Goel SC, Khanna S, Gupta D.Bridging of large osteoperiosteal gaps by allogenic partially decalcifiedbone ‘Decalbone’ in man. Int Orthop. 1988 ; 12 : 119-124.
37. Glancy GL, Daniel JB, Eilert RE, Chang EM. Autograft versus al-lograft for benign lesins in children. Clin Orthop. 1991 ; 262 : 282.
38. Goel SC, Tuli SM, Singh HP, Sharma SV, Saraf SK, Srivastava TP.Allogenic decalbone in the repair of benign cystic lesions of bone. IntOrthop. 1992 ; 16 : 176 – 179.
39. Sethi A, Aggarwal K, Sethi S, Kumar S, Marya SKS, Tuli SM.Allograft in the treatment of benign cystic lesions bone. Arch OrthopTraum Surg. 1993 ; 112 : 167-170.
BONE GRAFTS AND BONE SUBSTITUTE IN CLINICAL ORTHOPAEDICS