MITJANS La Relacion Entre Personal Id Ad, Creatividad y Motivacion

of 6
Upload
makolla007Category
view
218download
07/23/2019 Alianza Terapeutico y La Relacion Entre Motivacion...
1/6
Regular article
Therapeutic alliance and the relationship between motivation and
treatment outcomes in patients with alcohol use disorder
Mark A. Ilgen, (Ph.D.)4, John McKellar, (Ph.D.), Rudolf Moos, (Ph.D.), John W. Finney, (Ph.D.)
Center for Health Care Evaluation, Department of Veterans Affairs Palo Alto Health Care System, Menlo Park, CA 94025, USA
Stanford University School of Medicine, Stanford, CA, USA
Received 12 December 2005; received in revised form 11 April 2006; accepted 17 April 2006
Abstract
Although motivational readiness to change predicts alcohol use disorder (AUD) treatment outcomes, little is known about treatment
aspects that are helpful for patients with low motivation. We examined whether a positive therapeutic alliance is particularly beneficial for
patients entering AUD treatment with low motivation. Among Project MATCH outpatients (n = 753), we tested the influence of motivation,
therapeutic alliance, and their interaction on 6-month and 1-year alcohol use. The impact of motivation on alcohol use varied depending on
therapists perceptions of alliance. Interactions involving treatment compliance did not mediate the Motivation Alliance interaction. Thus,
a positive therapeutic relationship may be particularly important for patients with low motivation, but mechanisms underlying this possible
patienttreatment bmatchQremain to be determined. D 2006 Elsevier Inc. All rights reserved.
Keywords:Motivation; Alcohol use disorder; Therapeutic alliance; Treatment
1. Introduction
Motivational readiness to change is theorized to be an
important determinant of treatment outcome for patients
with alcohol use disorders (AUDs;Miller & Rollnick, 2002;
Prochaska, DiClemente, & Norcross, 1992). High motiva-
tion prior to treatment is a strong predictor of treatment
outcomes and foreshadows a better course for several years
following treatment (Carbonari & DiClemente, 2000;
DiClemente, Carbonari, Zweben, Morrel, & Lee, 2001;
McKay & Weiss, 2001). The consistency of these findingshas led researchers to examine how psychosocial interven-
tions can strengthen motivation in patients with AUDs,
particularly in patients who report low motivation at the
beginning of treatment.
Project MATCH tested whether any of three psychosocial
treatments for AUDs was particularly well suited to treat
patients with low motivation (Project MATCH Research
Group, 1993). Specifically, it was hypothesized that patients
with low motivation who were randomized to Motivational
Enhancement Therapy (MET) would do better than those
randomized to either Cognitive Behavioral Treatment (CBT)
or 12-Step Facilitation (TSF). Further, it was hypothesized
that this advantage would occur because the bmatchQ
between MET and patients with low motivation would
produce a better therapeutic alliance and better adherence to
treatment than would be true for patients with low moti-
vation in either of the other two treatment conditions.
However, there was little or no support for the hypothesis
that states that any of the three treatments used in Project
MATCH was particularly well suited to the challenge of
treating patients with AUD who have low motivation
(Babor & Del Boca, 2003; DiClemente et al., 2001).
0740-5472/06/$ see front matterD 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.jsat.2006.04.001
4 Corresponding author. Center for Health Care Evaluation, Depart-
ment of Veterans Affairs Palo Alto Health Care System, 795 Willow Road
(MPD 152), Menlo Park, CA 94025, USA. Tel.: +1 650 493 5000x27575.
E-mail address: [email protected] (M.A. Ilgen).
Journal of Substance Abuse Treatment 31 (2006) 157162
7/23/2019 Alianza Terapeutico y La Relacion Entre Motivacion...
2/6
Rather than focusing on specific treatments or modalities,
an alternative approach for examining patienttreatment
interactions is to focus on common factors across treatments.
One common aspect of treatment, the quality of the thera-
peutic alliance, predicts treatment outcomes in a number of
different domains (Lebow, Kelly, Knobloch-Fedders, &
Moos, 2006; Meier, Barrowclough, & Donmall, 2005).Within Project MATCH, Connors, Carroll, DiClemente,
Longabaugh, and Donovan (1997) found that stronger
therapeutic alliance predicted better AUD treatment com-
pliance and outcomes. Patients with low motivation are
particularlysensitive to aspects ofthe therapeutic relation-
ship (e.g.,Miller & Rollnick, 2002) and, consequently, may
be especially responsive to a strong, positive therapeutic
alliance. Thus, it is likely that therapeutic alliance may
influence the relationship between patient motivation and
outcome. As far as we know, no prior study has examined the
interaction between motivation and therapeutic alliance as a
predictor of AUD treatment outcomes.We hypothesize that a positive therapeutic alliance can
overcome the consequences of low motivation on drinking
outcomes in patients treated for AUDs. We also examine the
role of treatment compliance (treatment sessions attended)
as a potential mediator of a Motivation Alliance inter-
action following steps described in Finney (1995). In these
analyses, we test whether patients with low motivation who
have a strong therapeutic alliance are more likely to achieve
positive outcomes because they are more compliant with
treatment compared with those who have a weak alliance.
We hypothesize that the expected interaction between
patient motivation and therapeutic alliance in predicting
drinking outcomes may be due to increased treatmentcompliance among bmatched Qpatients with low motivation,
the interaction between compliance and therapeutic alliance
on patient outcomes, or both.
2. Materials and methods
Within Project MATCH, independent samples of out-
patient and aftercare patients were randomly assigned to
CBT (Kadden, Carroll, & Donovan, 1992), MET (Miller,
Zweben, DiClemente, & Rychtarik, 1992) , or T SF
(Nowinski, Baker, & Carroll, 1992). We focus on out-patients because of our interest in the role of motivation at
the beginning of treatment and because previous analyses in
Project MATCH found the strongest predictive relationships
for motivation, treatment type, and therapeutic alliance
within the outpatient sample (Connors et al., 2000;
DiClemente et al., 2001; Project MATCH Research Group,
1997). Patients were assessed at multiple time points before,
during, and following treatment (see below). Informed
consent was obtained from all participants, and the pro-
cedures used were in accordance with the standards of the
Committee on Human Experimentation from the Helsinki
Declaration of 1975 (Project MATCH Research Group,
1993). The Stanford University Human Research Protection
Program provided human subjects approval for this specific
set of secondary analyses of Project MATCH data. Detailed
information on sample, eligibility criteria, assessments, and
treatments has been reported previously (see Babor &
Del Boca, 2003).
2.1. Participants
This study included patients in the outpatient sample who
provided usable data on measures of alcohol consumption at
baseline, 6 months, and 1 year after treatment completion.
Data on therapeutic alliance were available for 785 (82.5%)
participants. Prior research on therapeutic alliance in Project
MATCH indicates that outpatients with complete data on
measures of therapeutic alliance are representative of the
overall outpatient Project MATCH sample, with the
exception that they were more likely to be married than
were those without complete data (Connors et al., 1997).
2.2. Measures
2.2.1. Alcohol stages of change version of the University of
Rhode Island Change Assessment (URICA-A; DiClemente
& Hughes, 1990)
This measure contains four 7-item subscales that were
combined to develop a single scale of motivation to change.
This method for scoring the URICA-A has been described
previously in Kadden, Longabaugh, and Wirtz (2003).
Reliability estimates for the four subscales range from .68
to .85 in the Project MATCH data set (Carbonari &
DiClemente, 2000).
2.2.2. Working Alliance Inventory (WAI; Horvath &
Greenberg, 1986)
The WAI is a 36-item measure of the patients capacity to
engage actively in treatment and the patients experience of
the therapeutic relationship as helpful. Both the therapist
and the patient completed theWAI. The WAI demonstrated
good internal consistency (Connors et al., 1997), and,
consistent with past research with the WAI on this sample,
the total scores for therapists and patients reported after the
second session of therapy were used here.
2.2.3. Drinking behavior
Drinking behavior (percentage of days abstinent [PDA]
and drinks per drinking day [DDD]) was measured via
interview at all time points using the Form 90 (Miller,
1996). The Form 90 asks patients to provide retrospective
data on the quantity and frequency of alcohol consumed
per day in the prior 3 months. Consistent with other pub-
lished reports from Project MATCH, we used transformed
versions of these variables (i.e., arcsin transformation for
PDA and square root transformation for DDD) in all
analyses (for more information, see Project MATCH Re-
search Group, 1997).
M.A. Ilgen et al. / Journal of Substance Abuse Treatment 31 (2006) 157162158
7/23/2019 Alianza Terapeutico y La Relacion Entre Motivacion...
3/6
To decrease family-wise error, we generated factor
scores, combining PDA and DDD for each time point.
The two outcomes converged well, producing a unitary
factor (68% of variance in a single factor for 6-month
outcomes and 70% of variance in a single factor for 1-year
outcomes) on which each variable loaded .83 at both
time points.
2.2.4. Type of treatment and number of sessions
Treatment providers reported information about the
number of treatment sessions attended by each patient.
Treatment type (MET, CBT, and TSF) was coded using
orthogonal contrasts (Kraemer & Blasey, 2004). To measure
treatment compliance, we calculated the ratio of number
of treatment sessions attended over number available
(i.e., the number of sessions actually attended was divided
by 12 for CBT and TSF and was divided by 4 for MET).
2.3. Analysis plan
Two regression analyses were conducted, in which the
predictors were baseline motivation, therapeutic alliance,
and the interaction of motivation and therapeutic alliance
and the outcomes were alcohol use at either 6 months or
1 year. Baseline alcohol use and treatment type were
included as covariates. Separate analyses were conducted
for patients and therapists rating of therapeutic alliance. A
series of regression analyses was conducted to test whether
either of the two interactions involving the ratio of treatment
sessions attended over number of available sessions (as a
measure of treatment compliance) mediated the interaction
between motivation and alliance in relation to alcohol use
treatment outcome. All variables were median centered (see
Kraemer & Blasey, 2004).
3. Results
Results from the primary regression analyses are
presented inTable 1. With patient-rated therapeutic alliance
in the model, a significant main effect was found, showing
that stronger patient motivation at baseline was linked to
less alcohol use at both 6 months and 1 year. Patients who
perceived a stronger alliance had better alcohol outcomes at
6 months but not at 1 year. However, no significant inter-
action effect between motivation and patient-rated alliance
was found at either time point.
In analyses involving therapists ratings of the therapeutic
alliance, higher motivation and more positive perception ofthe alliance by the therapist both independently predicted less
alcohol use at the 6-month and 1-year follow-ups. Addition-
ally, there was a significant interaction between motivation
and therapists ratings of alliance at each follow-up. The
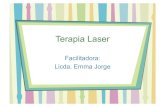
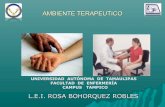
form of these interactions is presented inFigs. 1 and 2, which
show low, medium, and high groups F1SD from the mean
for motivation and therapists reports of therapeutic alliance.
The effects of therapeutic alliance were strongest for patients
Fig. 1. Therapists ratings of alliance are more closely related to less
alcohol use at 6 months in patients with low motivation than in those
with high motivation.
Fig. 2. Therapists ratings of alliance are more closely related to less
alcohol use at 1 year in patients with low motivation than in those with
high motivation.
Table 1
Predictors of alcohol use at 6 months and at 1 year
Predictors
Alcohol use at
6 months (b)
Alcohol use at
1 year (b)
Analyses of patient
ratings of alliancea
Motivation .06344 .07544
Patient rating of alliance .00344 .001
Motivation Patient
rating of alliance
.000 .000
Constant .031 .027
R2 .055 .053
Analyses of therapist
ratings of alliancea
Motivation .06744 .07244
Therapist rating of alliance .00544 .00444
Motivation Therapist
rating of alliance
.0024 .0024
Constant .042 .040
R2 .071 .072
a All analyses included baseline alcohol use and treatment type
as covariates.
4 p = .05.
44 p b .01.
M.A. Ilgen et al. / Journal of Substance Abuse Treatment 31 (2006) 157162 159
7/23/2019 Alianza Terapeutico y La Relacion Entre Motivacion...
4/6
with low motivation. A good therapeutic alliance ameliorated
the negative effects of low baseline motivation in predicting
drinking at the 6-month and 1-year follow-up. In contrast,
variation in the quality of the therapeutic alliance made
relatively little difference in alcohol use outcomes for
individuals with high motivation at treatment entry.
Analyses were conducted to test whether interactionsinvolving treatment compliance (operationalized as number
of sessions attended over the maximum number of available
sessions) might mediate the significant interaction between
motivation and therapists ratings of alliance in relation to
alcohol use outcome. All analyses predicting alcohol use
utilized data from the 1-year follow-up. The first set of
analyses indicated that compliance did not mediate the
outcomes. Specifically, although compliance did predict
1-year alcohol use, the interaction between motivation and
therapists ratings of alliance did not predict compliance,
and the inclusion of compliance in the original model did
not decrease the magnitude of the interaction of motivationand alliance in relation to alcohol use at 1 year. The other set
of regression analyses provided further evidence that show
that another interaction involving compliance did not
mediate the effect of the interaction between motivation
and alliance on alcohol use. Specifically, we found that
motivation did not predict compliance, that the interaction
between alliance and compliance did not predict alcohol
use, and that the addition of the interaction of alliance and
compliance to the original equation did not decrease the
magnitude of the interaction between motivation and
alliance predicting alcohol use.
4. Discussion
Similar to earlier published reports from Project MATCH
(Carbonari & DiClemente, 2000; DiClemente et al., 2001),
motivation at treatment entry predicted a reduction in
alcohol use 6 months and 1 year after AUD treatment.
However, the relationship between low motivation and treat-
ment outcomes depended on the therapists perception of the
therapeutic alliance. Specifically, even after controlling for
baseline alcohol use and treatment type, a high-quality
therapeutic relationship was more strongly associated with
reductions in alcohol use among patients with low moti-vation than among those with high motivation. These
findings suggest that a strong positive therapeutic relation-
ship may be able to overcome much of the negative effect of
low motivation on posttreatment alcohol use. Although it
seems plausible that interactions involving treatment com-
pliance might explain this overall interaction effect, we
found no support for such mediating effects.
Our findings support the growing body of literature
indicating that motivational readiness to changeis important
in influencing treatment outcomes for AUDs (Carbonari &
DiClemente, 2000). As evidence builds for the importance of
motivation as a determinant of treatment outcome, it becomes
increasingly vital to discover aspects of treatment that are
especially beneficial for patients with low motivation. Past
investigations of the role of treatment type may have
underestimated the degree of variability across treatments
in therapists abilities to employ diverse treatment strategies
to engage patients with low motivation in the therapeutic
process (Connors et al., 1997, 2000). Consistent with priorresults from Project MATCH, the present findings indicate
that the quality of the relationship between treatment provider
and patientis important irrespective of the type of treatment
provided (Connors et al., 1997). Providers espousing differ-
ent orientations to treatment must attemptto establish rapport
and a strong therapeutic relationship (Lambert & Barley,
2001; Lebow et al., 2006), and, according to our results, the
quality of the relationship, especially as seen by the therapist,
may be particularly important in patients with low motiva-
tion. However, it is important to note that these findings are
preliminary and more research is needed before concluding
that increased alliance caused the improvements seen inpatients with low motivation.
There are several reasons why patients with low
motivation may be uniquely responsive to the therapeutic
relationship. Such patients tend to be ambivalent about
treatment (Miller & Rollnick, 2002), which may make them
more attuned to contextual influences such as the quality of
the therapeutic relationship (Lebow et al., 2006). Moreover,
responsive therapists are likely to be aware of patients low
motivation and change their behavior to fit these patients
needs. Thus, therapists estimates of alliance may reflect
their general sensitivity to the needs of patients with low
motivation. This conceptualization is consistent with the
finding that therapists perceptions of the relationship, ratherthan patients perceptions, were more closely tied with
improvements in patients with low motivation. Additionally,
such patients may be less attentive to the relationship and,
consequently, provide less accurate ratings of therapeutic
alliance. Others have suggested that ratings of alliance
provided by either therapists or third-party observers may be
more closely related to treatment outcomes in patients with
substance use disorder than patients ratings of alliance
(Fenton, Cecero, Nich, Frankforter, & Carroll, 2001; Shelef,
Diamond, Diamond, & Liddle, 2005).
More research is needed to understand how patients
baseline motivation affects the development of the treatmentalliance and why it is associated with outcomes. A closely
related direction for future research is to examine alternative
causal chains such as whether a positive therapeutic alliance
with patients with low motivation leads to proximal changes
(e.g., increases in approach coping) that foreshadow positive
outcome. In this study, interactions involving treatment
compliance did not mediate the effect of the interaction
between therapists ratings of alliance and motivation on
patients outcome.
Our findings have implications for clinicians and research-
ers. Clearly, because of the association between motivation
and prognosis, therapists need to attend to patients levels of
M.A. Ilgen et al. / Journal of Substance Abuse Treatment 31 (2006) 157162160
7/23/2019 Alianza Terapeutico y La Relacion Entre Motivacion...
5/6
motivation. Additionally, the finding that the relationship
between low motivation and poorer alcohol use outcomes is
not uniform highlights the potential positive influence
therapists can have with patients with low motivation.
Although prior literature on motivation and AUDtreatment
has focused primarily on treatment techniques (Miller &
Rollnick, 2002), our findings indicate that the quality of therelationship may be more important than the therapists
treatment orientation or specific techniques.
These implications notwithstanding, this study has
several limitations. The selection criteria for participants
and the close monitoring of treatment providers in Project
MATCH may have raised patients levels of motivation and
enhanced therapeutic alliances, thus decreasing the general-
izability of our findings. Additionally, the lack of consistent
findings between patient and therapist ratings of alliance
raises the possibility that the findings may have been due to
factors other than the quality of the therapeutic relationship.
The fact that motivation was measured at baseline andalliance was measured after two sessions of treatment leaves
open the possibility that, in addition to alliance, therapists
may have been rating patients motivation or performance
in treatment.
Our findings suggest that treatment providers can work
effectively with patients with low motivation when they are
able to establish a strong alliance with their patient. Better
identification of the mechanisms of action underlying the
interaction between motivation and therapeutic alliance may
help to identify ways in which therapists can enhance their
relationships with patients who are initially hesitant to
engage in treatment, thereby improving patients outcomes.
Acknowledgment
Preparation of this article was supported by the Depart-
ment of Veterans Affairs Health Services Research and
Development Service. The views expressed here are the
authors and do not necessarily represent the views of the
Department of Veterans Affairs. Additionally, the authors
acknowledge that the reported results are based on analyses
of the Project MATCH Public Data Set. These data were
collected as part of a multisite clinical trial of alcoholism
treatments supported by a series of grants from the NationalInstitute on Alcohol Abuse and Alcoholism and made
available to the authors by the Project MATCH Research
Group. This article has not been reviewed or endorsed by
the Project MATCH Research Group and does not
necessarily represent the opinions of its members, who are
not responsible for the contents.
References
Babor, T. F., & Del Boca, F. K. (Eds.). (2003). Treatment matching in
alcoholism. New York, NY7 Cambridge University Press.
Carbonari, J. P., & DiClemente, C. C. (2000). Using transtheoretical model
profiles to differentiate levels of alcohol abstinence success.Journal of
Consulting and Clinical Psychology, 68, 810 817.
Connors, G. J., Carroll, K. M., DiClemente, C. C., Longabaugh, R., &
Donovan, D. M. (1997). The therapeutic alliance and its relationship to
alcoholism treatment participation and outcome. Journal of Consulting
and Clinical Psychology, 65, 588598.
Connors, G. J., DiClemente, C. C., Dermen, K. H., Kadden, R., Carroll,K. M., & Frone, M. R. (2000). Predicting the therapeutic alliance in
alcoholism treatment. Journal of Studies on Alcohol, 61, 139149.
DiClemente, C. C., Carbonari, J. P., Zweben, A., Morrel, T., & Lee, R. E.
(2001). Motivation hypothesis causal chain analysis. In R. Longabaugh,
& P. W. Wirtz (Eds.), Project match hypotheses: Results and causal
chain analyses,(Vol. 8, pp. 206 222). Bethesda, MD: Project MATCH
Monograph Series NIH Pub No. 01-4238.
DiClemente, C. C., & Hughes, S. O. (1990).Stages of change profiles in out-
patient alcoholism treatment.Journal of Substance Abuse,2, 217 235.
Fenton, L. R., Cecero, J. J., Nich, C., Frankforter, T. L., & Carroll, K. M.
(2001). Perspective is everything: The predictive validity of six working
alliance instruments. Journal of Psychotherapy Practice and Research,
10, 262268.
Finney, J. W. (1995). Enhancing substance abuse treatment evaluations:
Examining mediators and moderators of treatment effects. Journal of Substance Abuse, 7, 135150.
Horvath, A. O., & Greenberg, L. S. (1986). The development of the
working alliance inventory. In L. S. Greenberg, & W. M. Pinsof (Eds.),
The psychotherapeutic process: A research handbook (pp. 529556).
New York, NY7 Guilford.
Kadden, R. M., Carroll, K., & Donovan, D. M. (1992). Cognitive
behavioral coping skills therapy manual: A clinical research guide for
therapists treating individuals with alcohol abuse or dependence.
Rockville, MD7 National Institute on Alcohol Abuse and Alcoholism.
Kadden, R. M., Longabaugh, R., & Wirtz, P. W. (2003). The matching
hypotheses: Rationale and predictions. In F. Babor (Ed.), Treatment
matching in alcoholism. International research monographs in the
addictions (pp. 81102). New York, NY7Cambridge University Press.
Kraemer, H. C., & Blasey, C. M. (2004). Centering in regression analyses:
A strategy to prevent errors in statistical inference. InternationalJournal of Methods in Psychiatric Research, 13, 141 151.
Lambert, M. J., & Barley, D. E. (2001). Research summary on the
therapeutic relationship and psychotherapy outcome. Psychotherapy:
Theory, Research, Practice, Training, 38, 357361.
Lebow, J., Kelly, J. F., Knobloch-Fedders, L. M., & Moos, R. (2006).
Relationship factors in treating substance use disorders. In L. B.
Castonguay, & L. E. Beutler (Eds.), Principles of therapeutic change
that work(pp. 293317). New York, NY7 Oxford University Press.
McKay, J. R., & Weiss, R. V. (2001). A review of temporal effects and
outcome predictors in substance abuse treatment studies with long-term
follow-ups: Preliminary results and methodological issues. Evaluation
Review, 25, 113 161.
Meier, P. S., Barrowclough, C., & Donmall, M. C. (2005). The role of the
therapeutic alliance in the treatment of substance misuse: A critical
review of the literature. Addiction, 100, 304 316.Miller, W. R. (1996). Manual for form 90: A structural assessment
interview for drinking and related behaviors (project match monograph
series no. 5). Rockville, MD7 National Institute on Alcohol Abuse
and Alcoholism.
Miller, W. R., & Rollnick, S. (2002). Motivational interviewing: Preparing
people for change(2nd ed.). New York, NY7 US: Guilford Press.
Miller, W. R., Zweben, A., DiClemente, C. C., & Rychtarik, R. G. (1992).
Motivational-enhancement therapy manual: A clinical research guide
for therapists treating individuals with alcohol abuse or dependence.
Rockville, MD7 National Institute on Alcohol Abuse and Alcoholism.
Nowinski, J., Baker, S., & Carroll, K. (1992).The twelve-step facilitation
therapy manual: A clinical research guide for therapists treating
individuals with alcohol abuse or dependence. Rockville, MD7National
Institute on Alcohol Abuse and Alcoholism.
M.A. Ilgen et al. / Journal of Substance Abuse Treatment 31 (2006) 157162 161
7/23/2019 Alianza Terapeutico y La Relacion Entre Motivacion...
6/6
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of
how people change: Applications to addictive behaviors. American
Psychologist, 47, 11021114.
Project MATCH Research Group. (1993). Project match: Rationale and
methods for a multisite clinical trial matching patients to alcoholism
treatment. Alcoholism: Clinical & Experimental Research, 17,
11301145.
Project MATCH Research Group. (1997). Matching alcoholism treatments
to client heterogeneity: Project match posttreatment drinking outcomes.
Journal of Studies on Alcohol, 58, 729.
Shelef, K., Diamond, G. M., Diamond, G. S., & Liddle, H. A. (2005).
Adolescent and parent alliance and treatment outcome in multidimen-
sional family therapy. Journal of Consulting and Clinical Psychology,
73, 689698.
M.A. Ilgen et al. / Journal of Substance Abuse Treatment 31 (2006) 157162162