






Idiomas
Páginas
Jurídico

Propuesta de ventas de de Adventure Works
Sandra Milena Acevedo RuedaMD Residente Medicina InternaOctubre de 2013Infecciones del SNC
Meningitis bacteriana aguda
Meningitis tuberculosa
Infecciones del SNC en paciente VIHAgenda
Generalidades
Meninges
Lquido cefaloraqudeo
Cerebrospinal fluid (CSF) is considered a part of the transcellular fluids. It is contained in the ventricles and the subarachnoid space and bathes the brainandspinal cord. The CSF is contained within the meningesandacts as a cushion to protect the brain from injury with position or movement. It has been estimated that thiswater bath effectgives the 1400g brain an effective net weight of only 50g.The total volume of CSF is 150 mls. The daily production is 550 mls/day so the CSF turns over about 3 to 4 times per day. The CSF is formed by the choroid plexus (50%) and directly from the walls of the ventricules (50%).CSFflowsthrough the foramens of Magendie & Luschka into the subarachnoid space of the brain and spinal cord. It is absorbed by the arachnoid villi (90%) and directly into cerebral venules (10%).The normal intracerebral pressure (ICP) is 5 to 15 mmHg. The rate of formation of CSF is constant and is not affected by ICP. Absorption of CSF increases linearly as pressure rises above about 7 cmsH2O pressure. At a pressure of about 11cmsH2O, the rate of secretion & absorption are equal.The CSF has a composition identical to that of the brain ECF but this is different from plasma. The major differences from plasma are:The pCO2 is higher (50 mmHg) resulting in a lower CSF pH (7.33)The protein content is normally very low (0.2g/l) resulting in a low buffering capacityThe glucose concentration is lowerThe chloride concentration is higherThe cholesterol content is very lowThere are no lymphatic channels in the brain and CSF fulfils the role of returning interstitial fluid and protein to the circulation.The CSF is separated from blood by the blood-brain barrier. Only lipid soluble substances caneasilycross this barrier and this is important in maintaining the compositional differences
5
Lquido cefaloraqudeo
6
Lquido cefaloraqudeo
7
Meningitis Bacteriana Aguda
Signo de Kerning
Tiene dos variantes
Signo de Brudzinski
Tiene dos variantes
Kernig: S: 5% E: 95% VPP: 27% VPN: 72%Brudzinski: S: 5% E: 95% VPP: 27% VPN: 72% Rig nucal: S: 30% E: 68% VPP:26% VPN: 73%LCR > 6 WBC/ml
LCR > 100 WBC/mlKernig: S: 9% E: 96% VPP: 18% VPN: 91%Brudzinski: S: 9% E: 96% VPP: 18% VPN: 91% Rig nucal: S: 52% E: 71% VPP:16% VPN: 93%
LCR > 1000 WBC/mlKernig: S: 0% E: 95% VPP: 0% VPN: 98%Brudzinski: S: 25% E: 96% VPP: 9% VPN: 99% Rig nucal: S: 100% E: 70% VPP:4% VPN: 100%
It may reach 250 mm H2O in obese adults [w21].bHigher cellularity in tuberculous meningitis has been occasionally observed in immunocompetent and BCG-vaccinated subjects soon after theinitiation of anti-tuberculous therapy.cNeutrophilic response in tuberculous meningitis is known with acute onset and in HIV patients. Lymphocytic pleocytosis in ABM is seen in caseswho have already been partially treated with antibiotics.ABM, acute bacterial meningitis20
Allan R. Tunkel. Practice Guidelines for the Management of Bacterial Meningitis. Clinical Infectious Diseases 2004; 39:126784
Dexametasona: 10 mg ev administrada 15-20 min antes o con la 1 dosis de ABO y continuar 10 mg cada 6 h por 4 das(A1) para meningitis por neumococo en Guias IDSA
Meningitis Tuberculosa
Se estima: 2 billones de personas (tercera parte de la poblacin mundial) est infectada con Mycobacterium tuberculosis
En 2010, 8.8 millones, 1.4 mill murieron
MENINGITIS TB1% de todos los casos, 6% de casos de extrapulmonarMortalidad 10 a 40%
AracnoiditisVasculitisHidrocefalia
Central nervous system tuberculosis. Leonard John, et al. Sept 2013. Wolters Kluwer Health.
A la semana 30 se tiene un acumulado de 7194 casos, el 74,6 % ingresaron como confirmados por laboratorio, el 24,1% confirmados por clnica y el 1,3 % restante ingresaron confirmados por nexo epidemiolgico
79,7 % de los casos corresponde al tipo pulmonar, 17,7 % al tipo extrapulmonar y el 2,6 % restante al tipo meningitis tuberculosa
34
MENINGITIS TBEstado 1: alerta, algunos signos focales o evidencia de hidrocefaliaEstado 2: letargo, confusin, sintomas leves, paralisis facial, hemiparesiaEstado 3: delirium estupor, coma, convulsiones, paralisis varios nervios craneales, hemipleja densa
Central nervous system tuberculosis. Leonard John, et al. Sept 2013. Wolters Kluwer Health.
MENINGITIS TBManifestaciones
PrdromosFase menngeaFase paralitica
Atpica: raro, rpidamente progresiva
Central nervous system tuberculosis. Leonard John, et al. Sept 2013. Wolters Kluwer Health.
The prodromal phase, lasting two to three weeks, is characterized by the insidious onset of malaise,lassitude, headache, low-grade fever, and personality change.The meningitic phase follows with more pronounced neurologic features, such as meningismus, protractedheadache, vomiting, lethargy, confusion, and varying degrees of cranial nerve and long-tract signs.The paralytic phase supervenes as the pace of illness accelerates rapidly; confusion gives way to stupor andcoma, seizures, and often hemiparesis. For the majority of untreated patients, death ensues within five toeight weeks of the onset of illness.36
The presenting clinical features of tuberculousmeningitis in older children and adults as described byrecent clinical series
The presenting clinical features of tuberculousmeningitis in older children and adults as described byrecent clinical series37
Central nervous system tuberculosis. Leonard John, et al. Sept 2013. Wolters Kluwer Health.
38
Meningitis Tuberculosa
The sensitivity of ADA in the diagnosis of TBM was 0.79(95%CI 0.750.83), specifi city 0.91 (95%CI 0.890.93),positive likelihood ratio 6.85 (95%CI 4.1111.41), negativelikelihood ratio 0.29 (95%CI 0.190.44) and diagnosticodds ratio 26.93 (95%CI 12.7356.97)
OBJECTIVE: To determine the accuracy of adenosinedeaminase (ADA) measurements in the diagnosis of tuberculousmeningitis (TBM)DESIGN: After a systematic review of English languagestudies, the sensitivity, specifi city and accuracy of ADAconcentrations in the diagnosis of cerebrospinal fluid(CSF) were evaluated using random effects models. Summaryreceiver operating characteristic curves were usedto summarise overall test performance.RESULTS: Ten studies met our inclusion criteria. Thesensitivity of ADA in the diagnosis of TBM was 0.79(95%CI 0.750.83), specifi city 0.91 (95%CI 0.890.93),positive likelihood ratio 6.85 (95%CI 4.1111.41), negativelikelihood ratio 0.29 (95%CI 0.190.44) and diagnosticodds ratio 26.93 (95%CI 12.7356.97).CONCLUSION: Our data suggest that ADA in the CSFcan be a sensitive and specifi c target and a critical criteriafor the diagnosis of TBM.KEY WORDS: adenosine deaminase; cerebrospinal fl uid;tuberculosis41
Tratamiento
A randomized, double-blind trial in Vietnam compared dexamethasone (for the first six to eight weeks of treatmentin a tapering dose regimen) with placebo in 545 patients over 14 years of age [59]. The following findings werenoted:Mortality was reduced significantly in the dexamethasone-treated group (32 versus 41 percent). The mortalitybenefit was most evident for patients with Stage I disease (17 versus 30 percent), approached significancefor Stage II (31 versus 40 percent), and was not significant in patients with Stage III disease (55 versus 60percent).There was no demonstrable reduction in residual neurologic deficits and disability among surviving patientsevaluated by questionnaire at nine months follow-up.The survival benefit associated with steroid therapy may have been in part due to a reduction in severeadverse events (9.5 versus 16.6 percent), particularly hepatitis that necessitated changes in antituberculosisdrug regimens.No mortality benefit from dexamethasone was evident in 98 HIV-infected patients included in the study.In another randomized trial, 141 children with tuberculous meningitis were assigned to either prednisone (usually 4mg/kg per day) or placebo for the first month of treatment [60]. Prednisone therapy was associated with asignificant reduction in mortality in children with stage III disease (4 versus 17 percent); only two deaths occurred inother patients (see 'Clinical stages' above).42
Tratamiento
A randomized, double-blind trial in Vietnam compared dexamethasone (for the first six to eight weeks of treatmentin a tapering dose regimen) with placebo in 545 patients over 14 years of age [59]. The following findings werenoted:Mortality was reduced significantly in the dexamethasone-treated group (32 versus 41 percent). The mortalitybenefit was most evident for patients with Stage I disease (17 versus 30 percent), approached significancefor Stage II (31 versus 40 percent), and was not significant in patients with Stage III disease (55 versus 60percent).There was no demonstrable reduction in residual neurologic deficits and disability among surviving patientsevaluated by questionnaire at nine months follow-up.The survival benefit associated with steroid therapy may have been in part due to a reduction in severeadverse events (9.5 versus 16.6 percent), particularly hepatitis that necessitated changes in antituberculosisdrug regimens.No mortality benefit from dexamethasone was evident in 98 HIV-infected patients included in the study.In another randomized trial, 141 children with tuberculous meningitis were assigned to either prednisone (usually 4mg/kg per day) or placebo for the first month of treatment [60]. Prednisone therapy was associated with asignificant reduction in mortality in children with stage III disease (4 versus 17 percent); only two deaths occurred inother patients (see 'Clinical stages' above).43
Tratamiento
A randomized, double-blind trial in Vietnam compared dexamethasone (for the first six to eight weeks of treatmentin a tapering dose regimen) with placebo in 545 patients over 14 years of age [59]. The following findings werenoted:Mortality was reduced significantly in the dexamethasone-treated group (32 versus 41 percent). The mortalitybenefit was most evident for patients with Stage I disease (17 versus 30 percent), approached significancefor Stage II (31 versus 40 percent), and was not significant in patients with Stage III disease (55 versus 60percent).There was no demonstrable reduction in residual neurologic deficits and disability among surviving patientsevaluated by questionnaire at nine months follow-up.The survival benefit associated with steroid therapy may have been in part due to a reduction in severeadverse events (9.5 versus 16.6 percent), particularly hepatitis that necessitated changes in antituberculosisdrug regimens.No mortality benefit from dexamethasone was evident in 98 HIV-infected patients included in the study.In another randomized trial, 141 children with tuberculous meningitis were assigned to either prednisone (usually 4mg/kg per day) or placebo for the first month of treatment [60]. Prednisone therapy was associated with asignificant reduction in mortality in children with stage III disease (4 versus 17 percent); only two deaths occurred inother patients (see 'Clinical stages' above).44
Infecciones del SNC en VIH
Infecciones del SNC en VIH33 millones de personas (1millon HIV 2)7000 se infectan cada daAfrica Sub-SaharianaEnfermedad neurolgica:40% a 60% de VIH +Infeccin SNC: Cualquier etapaOportunistas CD4 < 200 clulas / dlInicio agudo, subagudo o crnico
Infecciones del SNC en VIHPrimera manifestacin de SIDA en 10 a 20%Terapia antirretroviral altamente activa: disminucion de enf oportunistas.Sintomas meningeosInfeccion de parenquima sin focalizacionInfeccion de parenquima con focalizacion
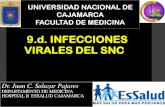
Figure ": Axial MRI of the brain in patients with HIV and CNS opportunistic infections(A) Cryptococcal meningitis in a man aged 58 years who presented with headache, weight loss, anorexia, and ageneralised seizure, with a CD4-cell count of 10 cells per !L. The arrow shows gadolinium enhancement of theposterior meninges on T1-weighted MRI. A cryptococcoma is present in the right basal ganglion. (B) Cerebraltoxoplasmosis in a man aged 39 years who presented with generalised seizure and nadir in CD4-cell count of2 cells per !L. Diagnosis was confi rmed by brain biopsy. Multiple hyperintense lesions with surrounding oedema(arrow), appearing as a hypointense rim, with mass eff ect can be seen on T2-weighted, fl uid-attenuated inversionrecovery MRI. (C) Primary CNS lymphoma in a man aged 21 years who presented with acute-onset left-sidedweakness and a CD4-cell count of 0 cells per !L. Diagnosis was confi rmed by brain biopsy. A rim-enhancing lesion(arrow) is visible in the right temporoparietal lobe on gadolinium-enhanced MRI. (D) Progressive multifocalleukoencephalopathy in a man aged 42 years who presented with lethargy, left hemiparesis, dysphagia, seizures,and visual hallucinations. T2-weighted, fl uid-attenuated inversion recovery MRI shows asymmetric, confl uenthyperintensities involving the cerebral white matter (arrow) without mass eff ect. All patients were started oncombination antiretroviral therapy and appropriate antimicrobials and supportive treatment, and all survive.55
Criptococo Levadura encapsulada:Cryptococcus neoformansMedio ambiente: Tierra Heces de pjaros y palomaNo transmite de persona a personaInfeccin primaria diseminacinRectivacin infeccin latenteNormal 30%
Criptococo Meningitis no exudativa Mnima inflamacinFrecuente ausencia de signos menngeosCriptococoma - masaFormaAgudaPeriodos 2 a 4 semanas insidiosa
Hidrocefalia, HTE 15%
Criptococo Principal infeccin fngica SNC Incidencia < individuos con profilaxis fluconazol y TAR ( desarrollados) 7%Sin terapia antirretroviral 44%CD 4+ 20 Cm H2O)50%Criptococosis extraneuralFrecuente
Criptococo LCR: normal 50% a 72%Ag polisacrido capsular Alta Sensibilidad 97%Tinta china 75 a 90 %Cultivo (dx definitivo) test Ag positivo en LCRRMNAtrofia leveAumento tamao ventricularHidrocefalia obstructivaCriptococoma en espacios perivasculares
Ag polisacrido capsular Alta Sensibilidad 97%( probabilidad de clasificar correctamente a un individuo enfermo si la pba es positiva)62
Criptococo Terapia AgudaFlucitosina + Anfotericina B 2 sem.Anfotericina 0.7 a 1 mg /kg /d IV en 30 a 60 minFlucitocina 100 mgr/kg/d VO en 4 dosis daContinuar Fluconazol 400 mg/d VO 8 a 10 sem.PL 2 semanas despus de Tto valorar presin LCRProfilaxis secundariaFluconazol 200 mgr /da VO Anfotericina B 1 mgr/kgr /da 1 vez por semanaItraconazol 200mgr
Panel de expertos de GESIDA; Prevencin de las infecciones oportunistas en pacientes adultos y adolescentes infectados por el VIH 2008
Ag polisacrido capsular Alta Sensibilidad 97%( probabilidad de clasificar correctamente a un individuo enfermo si la pba es positiva)63
Criptococo
Suspender profilaxis si mejora inmunolgica con TAR CD4 > 200 6 meses Cultivo LCR estril
Tiempo inicio de TAR no establecido, 30% IRIS mas frecuente al inicio en los 30 das siguientes al Tto (Shelburne et al. 2005)
Ag polisacrido capsular Alta Sensibilidad 97%( probabilidad de clasificar correctamente a un individuo enfermo si la pba es positiva)64
CMVFamilia Herpesviridae doble cadena de DNA.Reactivacin infeccin latentePrimo infeccin: mononucleosisInfeccin localizada o diseminadaMononeuritis , encefalitis, radiculomielitis, retinitisG/I : Esofagitis, colitisPulmonar: neumonitis intersticialCD 4 + 100.000 copias / ml
CMV
FormasEncefalitis nodular microglialDemencia (+ comn)Ventriculoencefalitis: agudoFocalizacinParlisis pares cranealesNistagmusProgresin rpida a muertePolirradiculomielopatia Similar a Guillain-Barre Retencin urinariaDebilidad progresiva MsIs
Kaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009
CMV
Kaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009Cuadro clnico Compromiso de otro rgano (retinitis)LCR: InespecficoPleocitosis linfoctica, neutrofilica.Aumento protenasDisminucin glucosa o glucosa normalAnticuerpo contra Ag del CMV (pp65)
PCR en LCR S: 80-100% E: 75-100%Cultivo RMN : Realce meningeo y agrandamiento periventricular
CMV
Kaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009Ganciclovir : 5 mgr /kg tres veces al da 2-4 sem Mantenimiento 5 mgr/kg/da 5 - 7 sem Foscarnet: 60 mgr/kg c/8h 2-6 sem Mantenimiento 90-120mgr/kg /da 6-7 sem
Puede haber sinergia si ganciclovir y foscarnet se usan juntos
Resistencia a ganciclovir en polirradiculopata
Toxoplasmosis
Toxoplasma gondiiParsito intracelular: Taquizoitos 0,4 (3,2) /1000 personas-ao3% negativosInfeccin : Ingesta de carneHeces de gatoEncefalitis necrotizante multifocalMortalidad 20-60%FormasPrimariaReactivacin : Parasitados previamente 47%EstadiosCD 4+ < 100 o < 50
Toxoplasmosis
Cefalea 4963% Fiebre 4168%Dficit neurolgico focal (motor)2280%Convulsiones 1929% Confusin 1552%Ataxia 1525%Letargia1244%Compromiso nervios craneales1219%Defectos visuales 815%Signos menngeos, cerebelososNauseasCompromiso ocular 10 a 50% preceden SNC
Toxoplasmosis
Cuadro clnico compatible
Serologa: alta tasa portadores crnicos Ig G
Estudio LCRNormal o inespecficoElevacin protenas 65%Disminucin glucosa 8 a 52%Pleocitosis (mononuclear) 27 a 40%
Toxoplasmosis
PCR LCRE: 97 a 100%S: 50 a 60%
TAC y RMNImgenes en anillo (ganglios basales y R. frontotemporal)Mltiples (>5)
Toxoplasmosis
Marra, Christina M., Infections of the central nervous system in a pacients infected with Human Immunodeficiency Virus, rev, Continuum abril 2006
Toxoplasmosis
Alternativas para sulfadiazina: Atovaquone: 750 mg VO 4 Veces / da Claritromicina: 1 g VO 2 veces / diaAzitromicina: 1 g , 500 mgr / diaKaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009
Leucoencefalopata Multifocal Progresiva
Kaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009Virus JC (Adultos 50 a 90%) Papova virusInfeccin primaria en la infancia: asintomticaLatente en tej renal y cerebral . ReactivacinContagio por inhalacinDesmielinizacin: afecta oligodendrocitos, astrocitos, cel granularesPrimer condicin definitoria de SIDA 25 a 57%Predominio H7:M1Estado< 100 CD4+/l> 200 CD4+ 25%
Leucoencefalopata Multifocal Progresiva
Kaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009Debilidad 5063%Anormalidades de la marcha 3243%Disfuncin cognitiva 2955%Incoordinacin 25%Alteraciones visuales 2150%, inicialesAlteracin habla 1831%Convulsiones 523% tempranasHemiparesiaProgresivo (meses)
Leucoencefalopata Multifocal Progresiva
Kaplan, Jonathan; Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents 2009PCR en LCRS: 70 a 100%E: 92 a 100%RMN TACSustancia blanca, cerebelo, sustancia grisDesmielinizacin subcorticalNo edema ni efecto de masa
Leucoencefalopata Multifocal Progresiva
Leucoencefalopata Multifocal Progresiva
Terapia antirretroviral Regresin espontneaMayor supervivencia si TARNo recuperacin de dficitTto especfico para el virus an no identificadoCorticosteroides: inflamacin (IRIS)
Linfoma
EN VIH 26 casos / 100.000SIN VIH: 0.38 casos /100.000
Cambios cognitivos, letargo, cefaleaLesin intracraneal efecto de masaCamara anterior ojo: 20%
Toxoplasmosis
ToxoplasmosisLinfoma SNCMltiples 70%Solitarias 50%Ganglios basalesPeriventricularAnular borde delgadoHeterogneoEdema +++Edema +Iso o hipodensaHiperdensa4 cm
Linfoma
Corticosteroides: Biopsia
Terapia antiretroviral
Radioterapia podra servir
Herpes Virus
PCR 1-2%HV y Epstein BarrTemporales, frontal inferiorVigorosa respuesta inflamatoriaActividad epileptiforme
Herpes simplex virus type 1 typicallycauses encephalopathy that might develop subacutelyover several weeks. Herpes simplex virus type 2 typicallycauses a di! use meningoencephalitis that can recur
Herpes Virus
TratamientoAciclovir 30mg/k/d 14 a 21 dasGanciclovir y foscarnetResistencia a aciclovirRecadas a los 3 meses
Infecciones del SNC en VIH
Zunt Joseph R MD, MPH Central Nervous System Infection During Immunosuppression, 2002
Gracias!
Top Related