Acetato de abiraterona en cáncer de próstata metastásico ...
Upload
mauricio-lemaCategory
view
102download
1
Tratamiento inicial de cáncer de mama en pacientes posmenopáusicas
HR+/Her2- metastásico: una visión panorámica
Mauricio Lema Medina MDClínica de Oncología Astorga / Clínica SOMA, Medellín
Medellín, 11.11.2016

@Onconerd

1970s Tamoxifen 20% 26wks38%
ORR CBR PFS/TTF
Does chemotherapy increase response-rate over hormonal therapy in HR+
aBC?
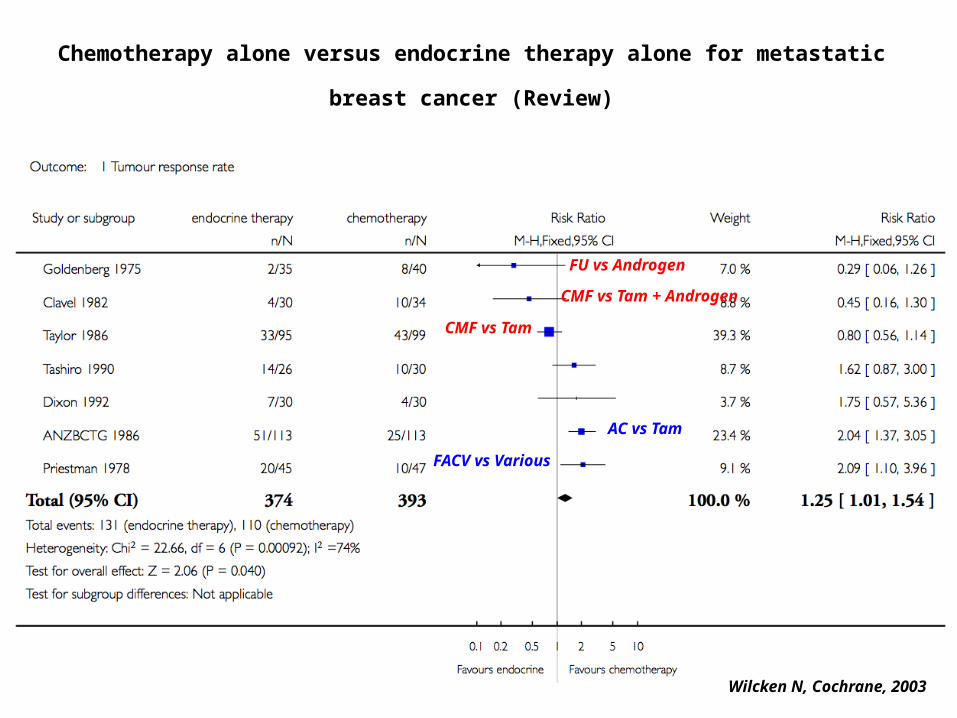
CMF vs Tam
CMF vs Tam + Androgen
FU vs Androgen
AC vs Tam
FACV vs Various
Chemotherapy alone versus endocrine therapy alone for metastatic breast cancer (Review)
Wilcken N, Cochrane, 2003
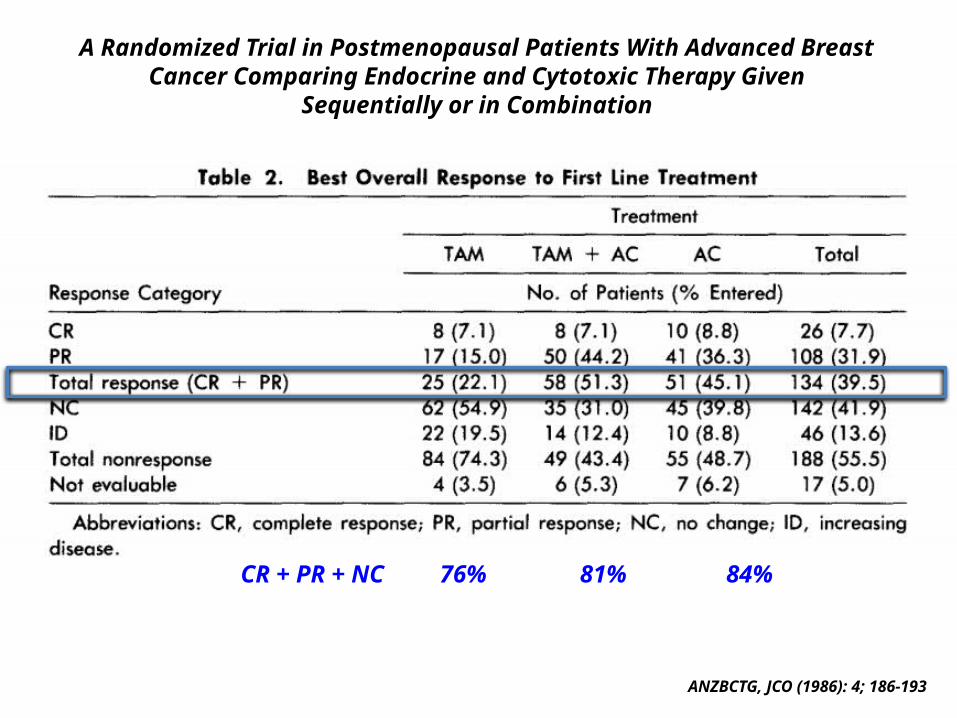
A Randomized Trial in Postmenopausal Patients With Advanced BreastCancer Comparing Endocrine and Cytotoxic Therapy Given
Sequentially or in Combination
ANZBCTG, JCO (1986): 4; 186-193
CR + PR + NC 76% 81% 84%
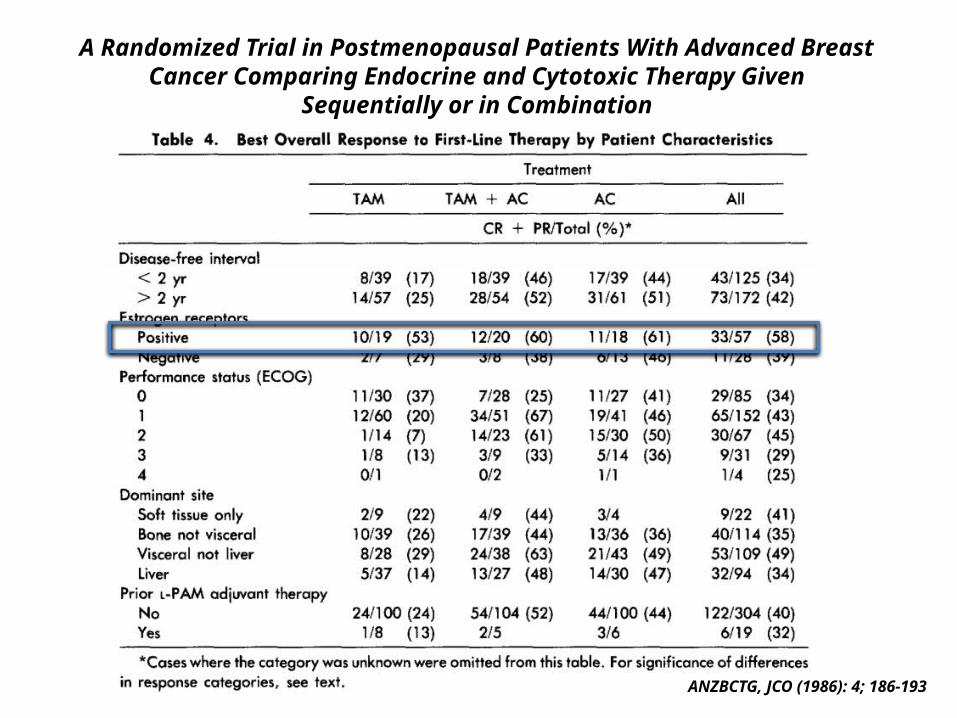
A Randomized Trial in Postmenopausal Patients With Advanced BreastCancer Comparing Endocrine and Cytotoxic Therapy Given
Sequentially or in Combination
ANZBCTG, JCO (1986): 4; 186-193
Does chemotherapy increase response-rate over hormonal therapy in HR+ aBC?
No solid phase III evidence can support this notion
What is the optimal first-line chemotherapy in aBC?
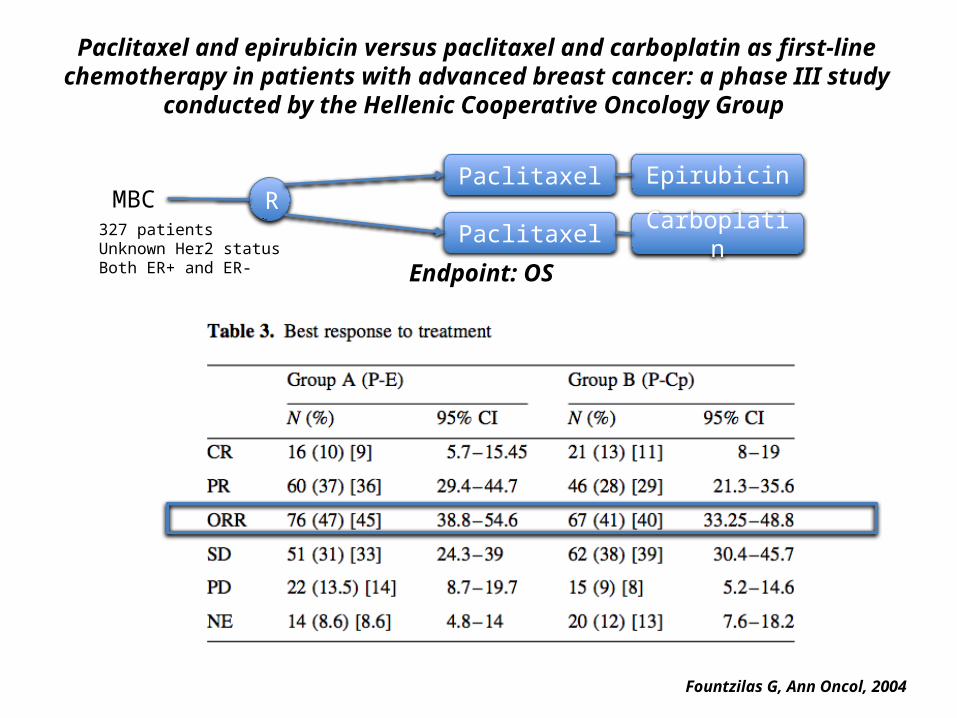
Paclitaxel and epirubicin versus paclitaxel and carboplatin as first-line chemotherapy in patients with advanced breast cancer: a phase III study conducted by the Hellenic
Cooperative Oncology Group
Fountzilas G, Ann Oncol, 2004
Paclitaxel Epirubicin
Paclitaxel CarboplatinRMBC
327 patientsUnknown Her2 statusBoth ER+ and ER- Endpoint: OS
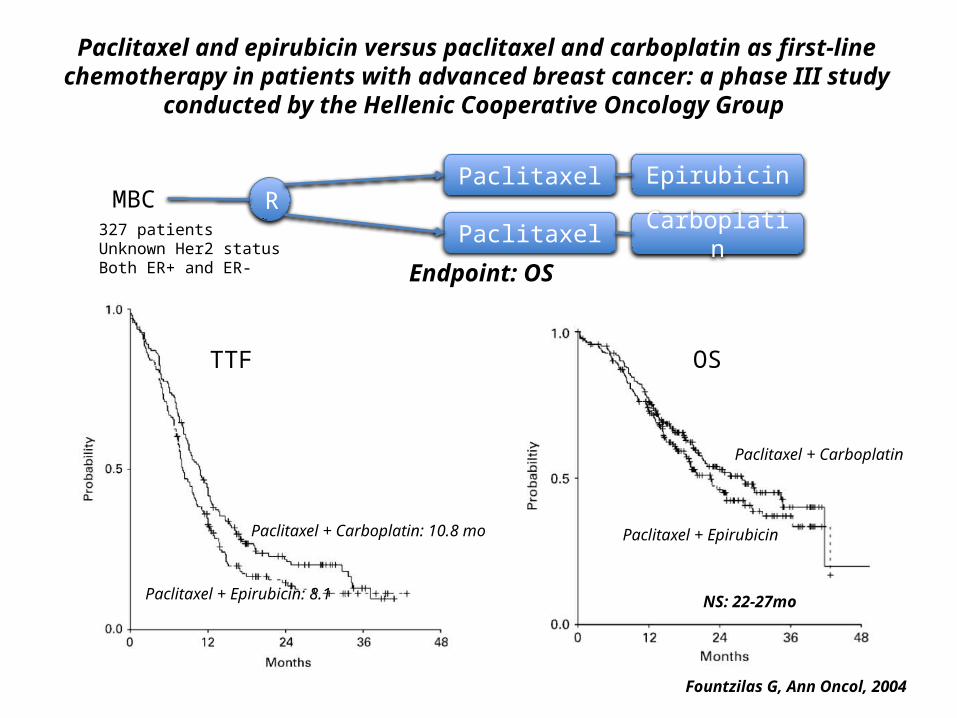
Paclitaxel and epirubicin versus paclitaxel and carboplatin as first-line chemotherapy in patients with advanced breast cancer: a phase III study conducted by the Hellenic
Cooperative Oncology Group
Fountzilas G, Ann Oncol, 2004
Paclitaxel Epirubicin
Paclitaxel CarboplatinRMBC
327 patientsUnknown Her2 statusBoth ER+ and ER- Endpoint: OS
TTF
Paclitaxel + Carboplatin: 10.8 mo
Paclitaxel + Epirubicin: 8.1
OS
Paclitaxel + Carboplatin
Paclitaxel + Epirubicin
NS: 22-27mo
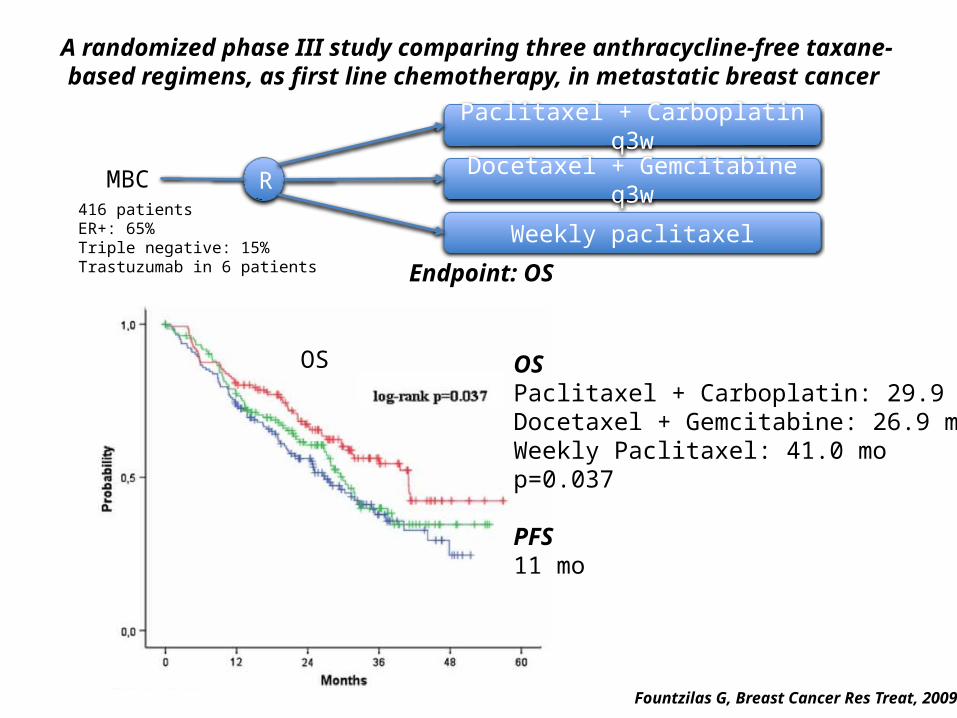
A randomized phase III study comparing three anthracycline-free taxane-based regimens, as first line chemotherapy, in metastatic breast cancer
Fountzilas G, Breast Cancer Res Treat, 2009
Docetaxel + Gemcitabine q3w
Weekly paclitaxel
RMBC416 patientsER+: 65%Triple negative: 15%Trastuzumab in 6 patients Endpoint: OS
OS
Paclitaxel + Carboplatin q3w
OSPaclitaxel + Carboplatin: 29.9 moDocetaxel + Gemcitabine: 26.9 moWeekly Paclitaxel: 41.0 mop=0.037
PFS11 mo
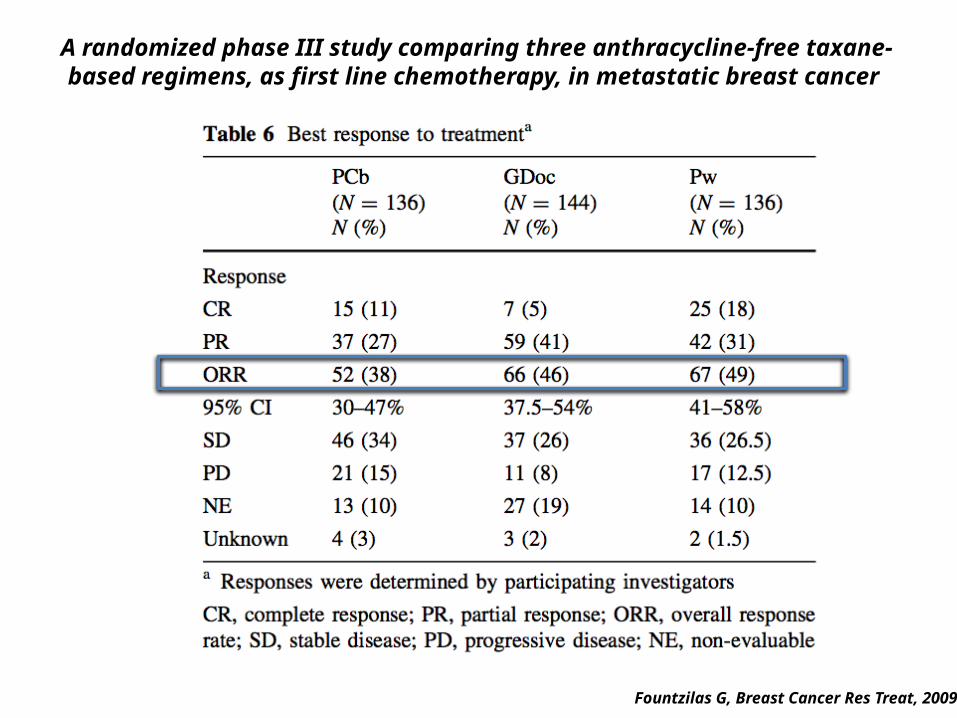
A randomized phase III study comparing three anthracycline-free taxane-based regimens, as first line chemotherapy, in metastatic breast cancer
Fountzilas G, Breast Cancer Res Treat, 2009
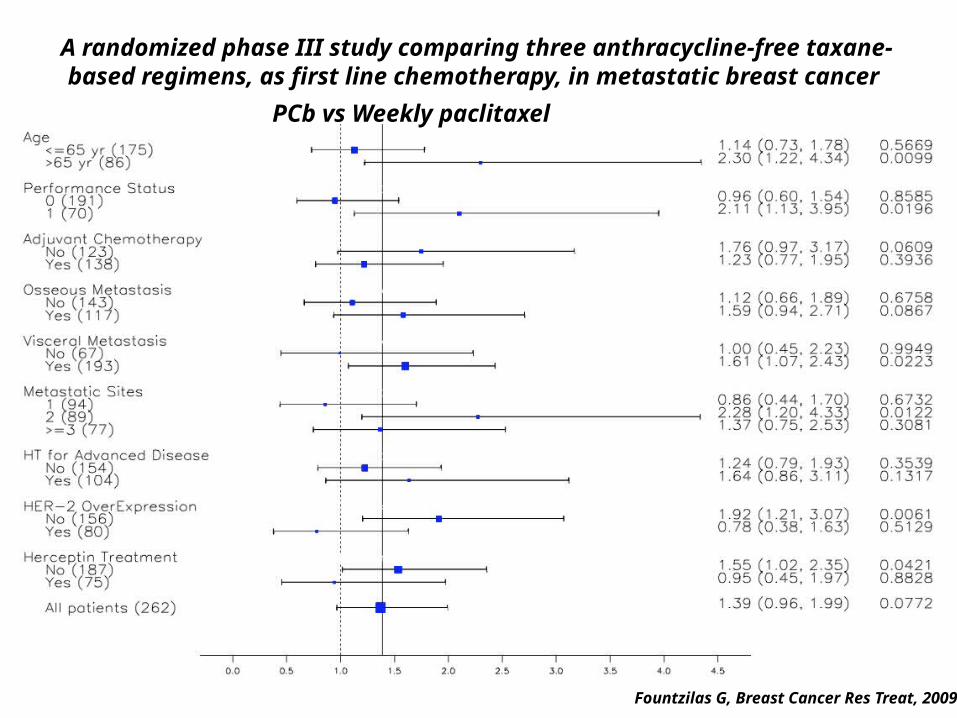
A randomized phase III study comparing three anthracycline-free taxane-based regimens, as first line chemotherapy, in metastatic breast cancer
Fountzilas G, Breast Cancer Res Treat, 2009
PCb vs Weekly paclitaxel
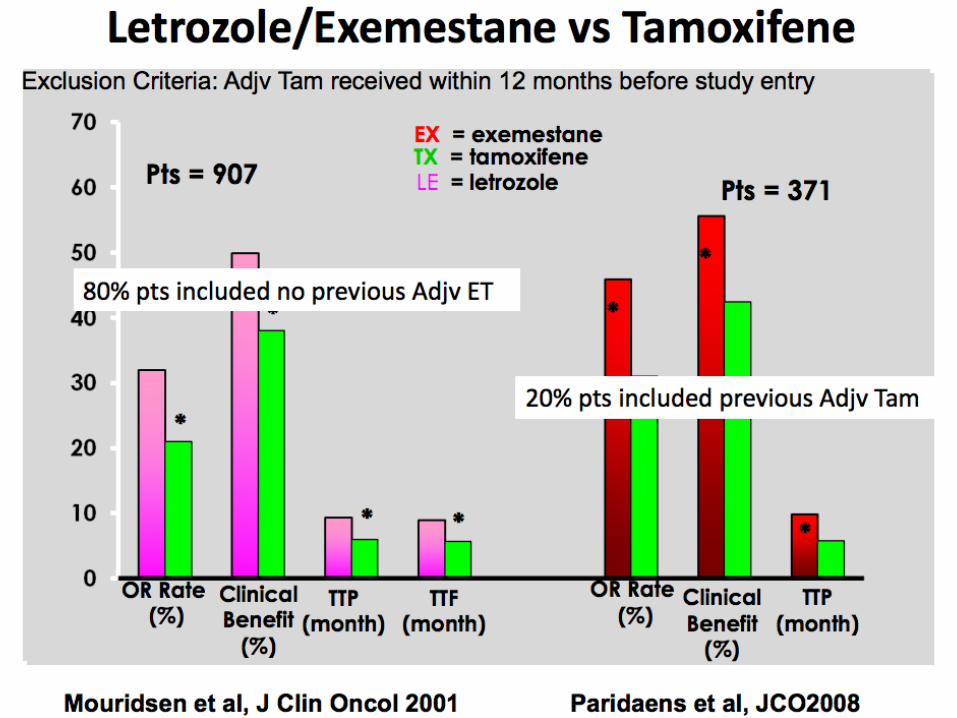
2009 Weekly paclitaxel 49% 47wks75%
Fountzilas, Breast Cancer Res Treat, 2009
ORR CBR PFS/TTF
ER+/ER-/Her2+
What is the optimal first-line chemotherapy in aBC?
Weekly paclitaxel appears to be superior to combination agents in
“all-comers” with aBC
What is the optimal first-line single-agent hormonal therapy in
HR+/Her2- aBC?
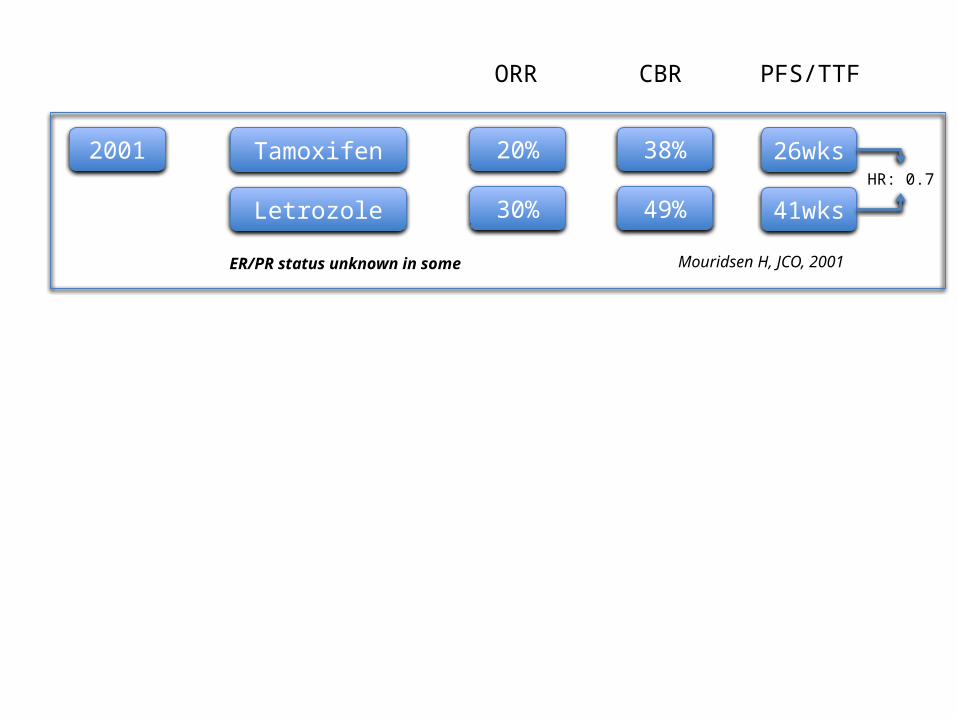
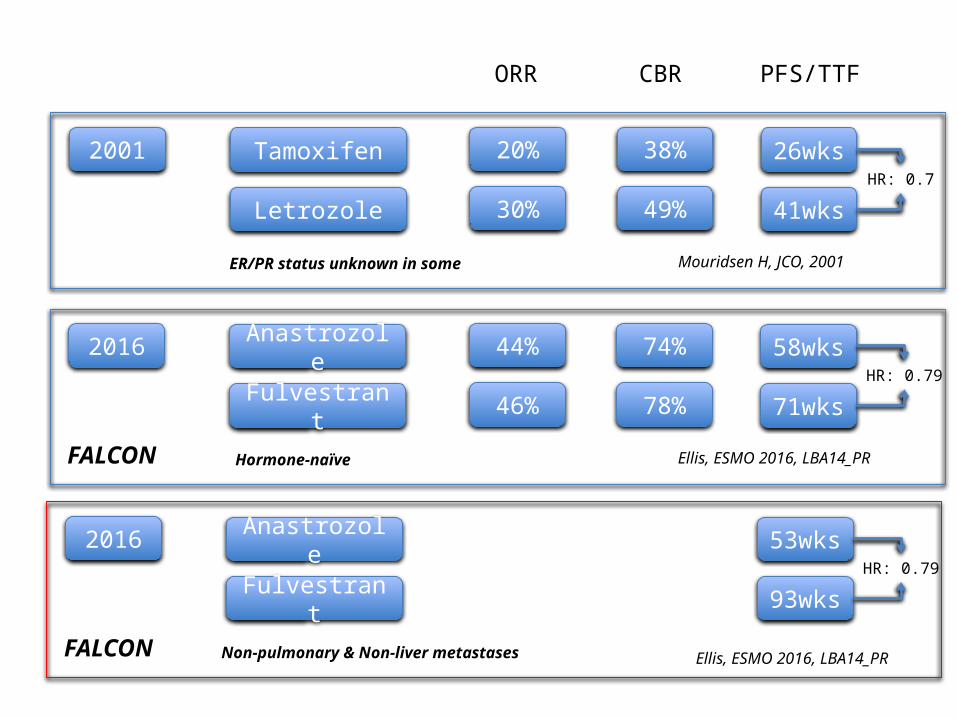
2001 Tamoxifen 20% 26wks38%
Letrozole 30% 41wks49%
Mouridsen H, JCO, 2001
HR: 0.7
ORR CBR PFS/TTF
ER/PR status unknown in some
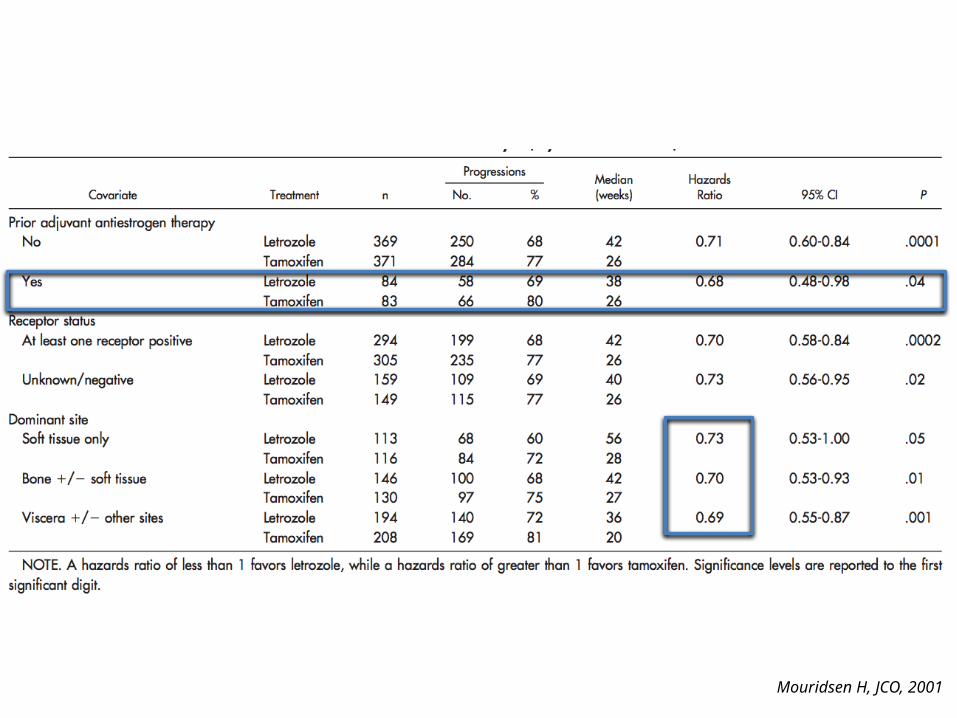
Mouridsen H, JCO, 2001
ESMO-2016, Copenhagen, 7-11 October 2016
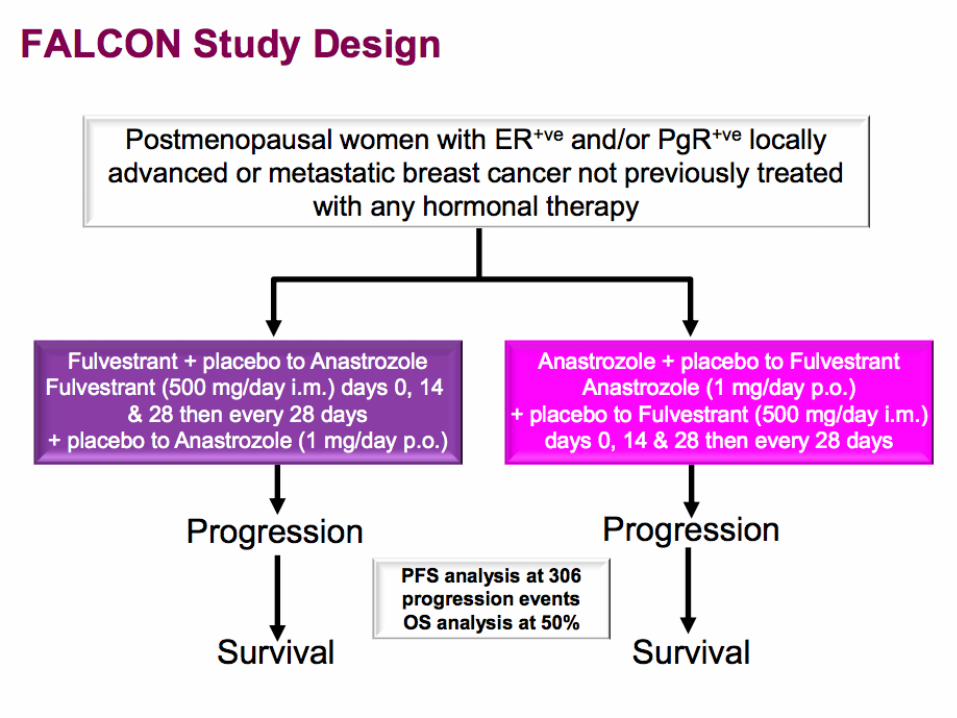
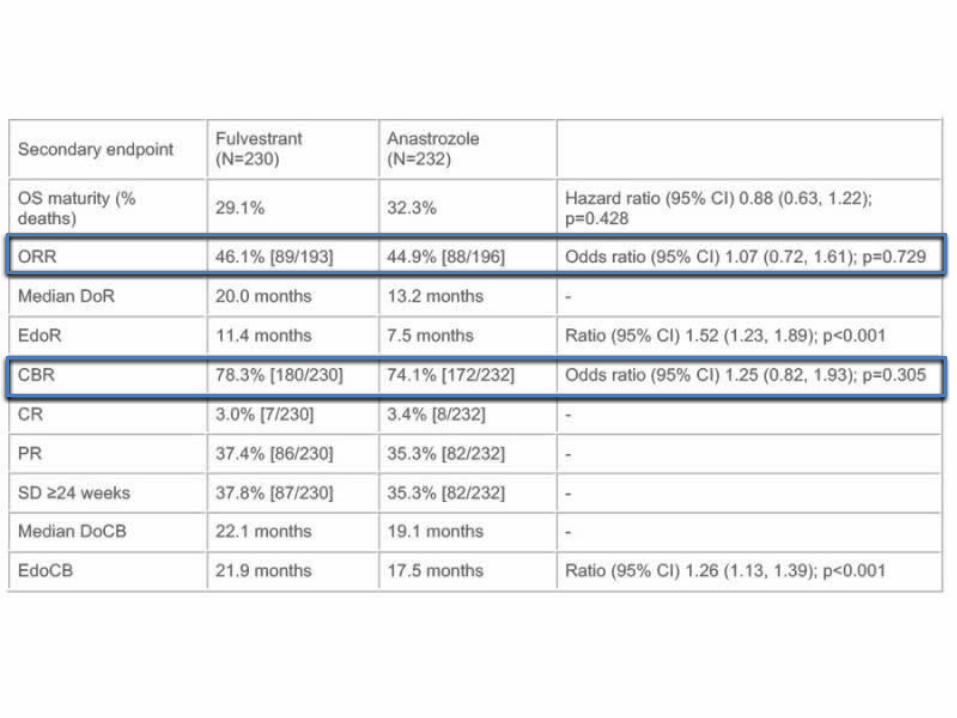
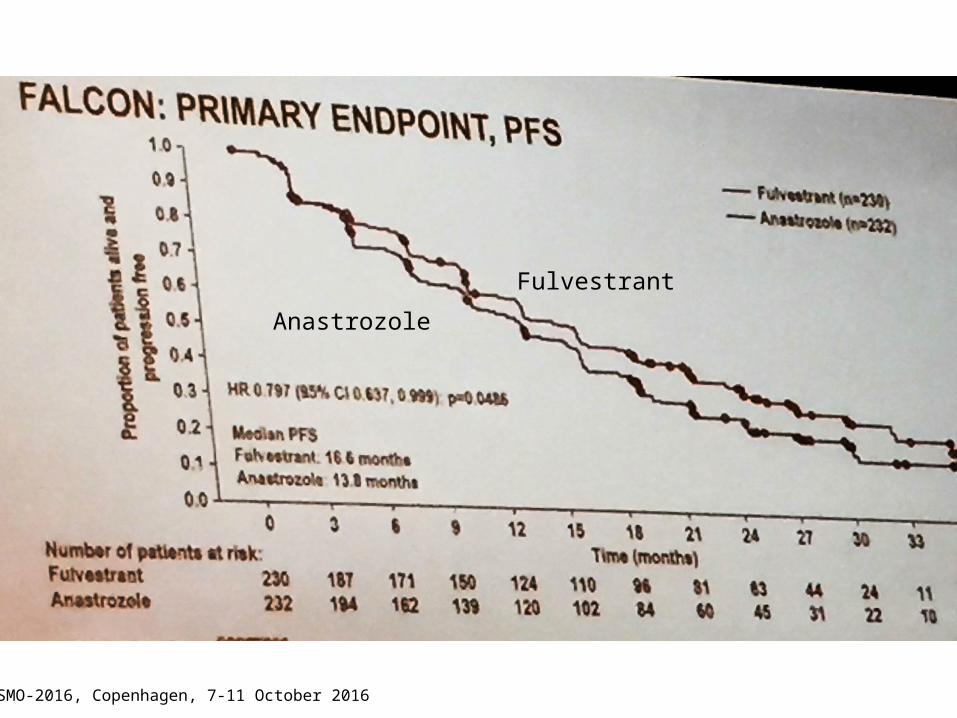
Fulvestrant
Anastrozole
ESMO-2016, Copenhagen, 7-11 October 2016
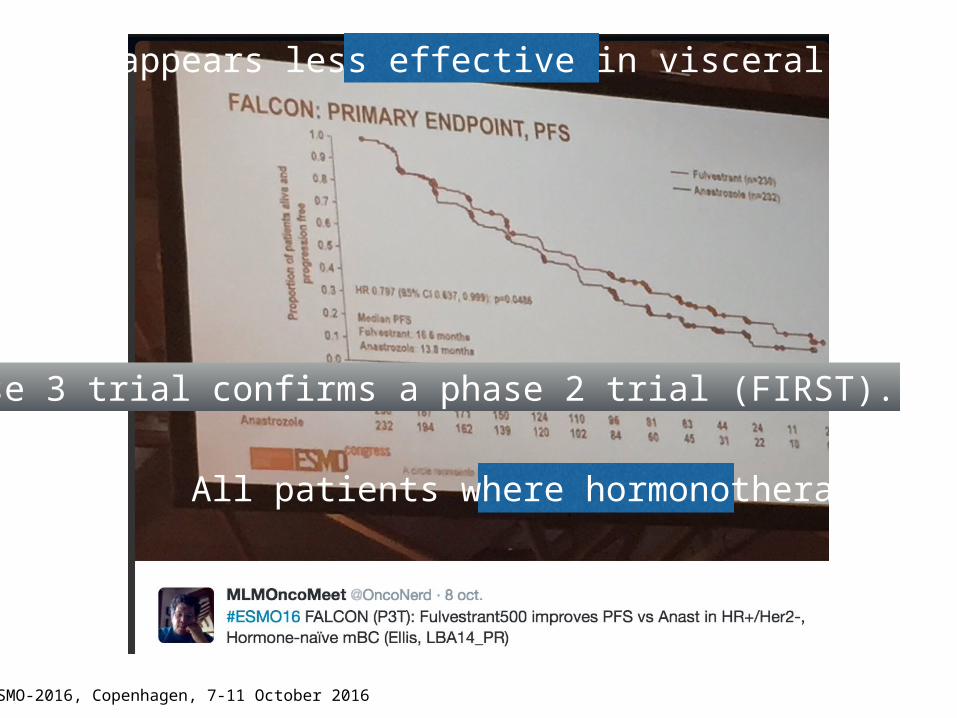
A phase 3 trial confirms a phase 2 trial (FIRST).
Fulvestrant appears less effective in visceral metastases.
All patients where hormonotherapy naïve.
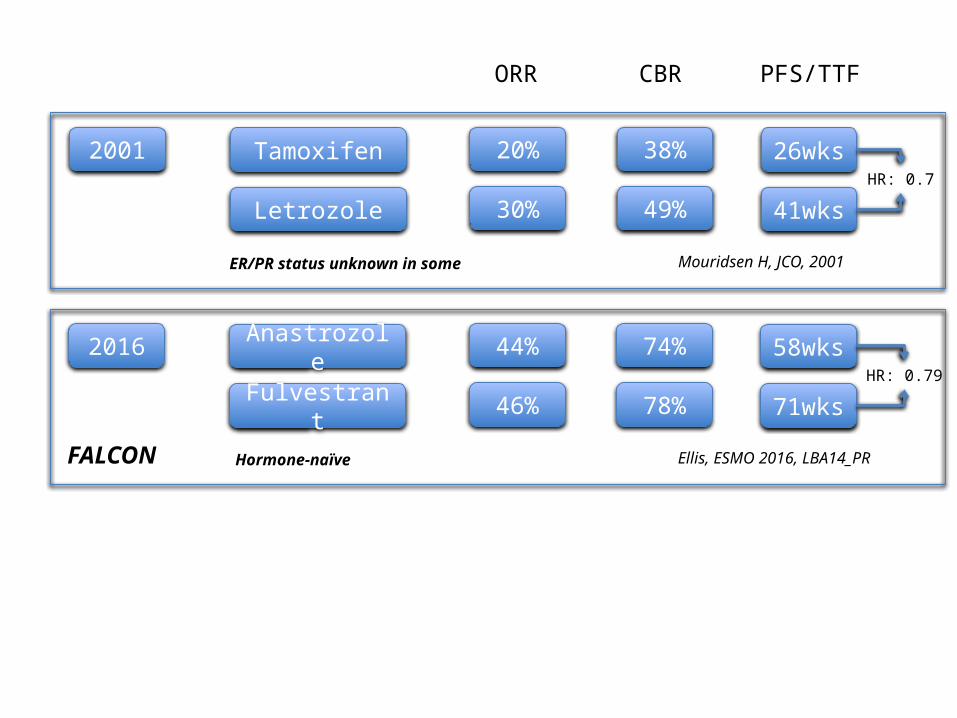
2001 Tamoxifen 20% 26wks38%
Letrozole 30% 41wks49%
Mouridsen H, JCO, 2001
HR: 0.7
2016 Anastrozole 44% 58wks74%
Fulvestrant 46% 71wks78%
Ellis, ESMO 2016, LBA14_PR
HR: 0.79
FALCON Hormone-naïve
ORR CBR PFS/TTF
ER/PR status unknown in some
2001 Tamoxifen 20% 26wks38%
Letrozole 30% 41wks49%
Mouridsen H, JCO, 2001
HR: 0.7
2016 Anastrozole 44% 58wks74%
Fulvestrant 46% 71wks78%
Ellis, ESMO 2016, LBA14_PR
HR: 0.79
FALCON Hormone-naïve
ORR CBR PFS/TTF
ER/PR status unknown in some
2016 Anastrozole 53wks
Fulvestrant 93wksHR: 0.79
FALCON Non-pulmonary & Non-liver metastases Ellis, ESMO 2016, LBA14_PR
What is the optimal first-line single-agent hormonal therapy in
HR+/Her2- aBC?
Fulvestrant is superior to AIs and displays a remarkable OS in non-
visceral metastatic in de-novo aBC
What about non-hormone naïve progressive HR+/Her2- aBC?
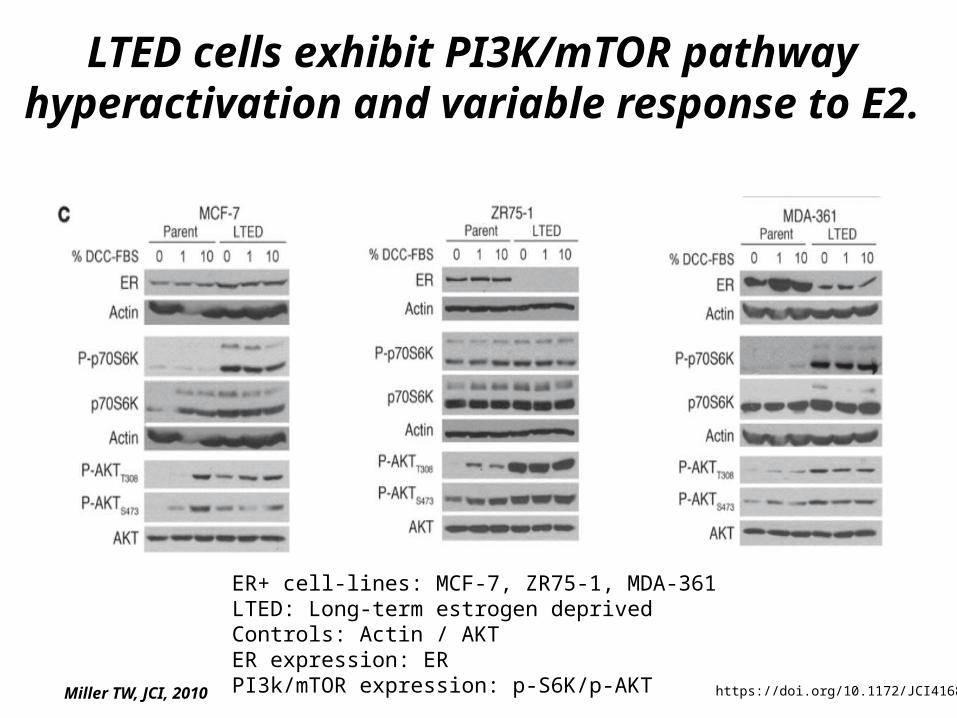
LTED cells exhibit PI3K/mTOR pathway hyperactivation and variable response to E2.
ER+ cell-lines: MCF-7, ZR75-1, MDA-361LTED: Long-term estrogen deprivedControls: Actin / AKTER expression: ERPI3k/mTOR expression: p-S6K/p-AKT https://doi.org/10.1172/JCI41680Miller TW, JCI, 2010

PI3K pathway inhibition suppresses hormone-independent cell growth
ER+ cell-lines: MCF-7, ZR75-1, MDA-361LTED: Long-term estrogen deprivedBEZ235 (Dactolisib): PI3k/mTOR inhibitorRAD0001 (Everolimus): mTOR inhibitorAEW541: IGR-1R inhibitorLapatinib: EGFR/Her2 inhibitor https://doi.org/10.1172/JCI41680Miller TW, JCI, 2010
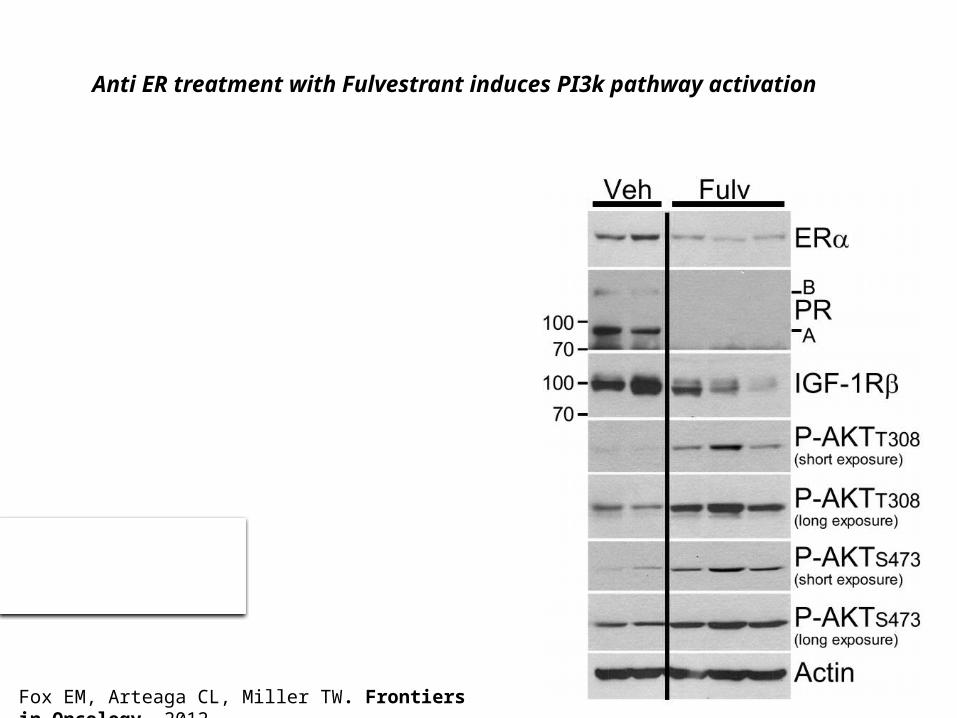
Anti ER treatment with Fulvestrant induces PI3k pathway activation
Fox EM, Arteaga CL, Miller TW. Frontiers in Oncology, 2012
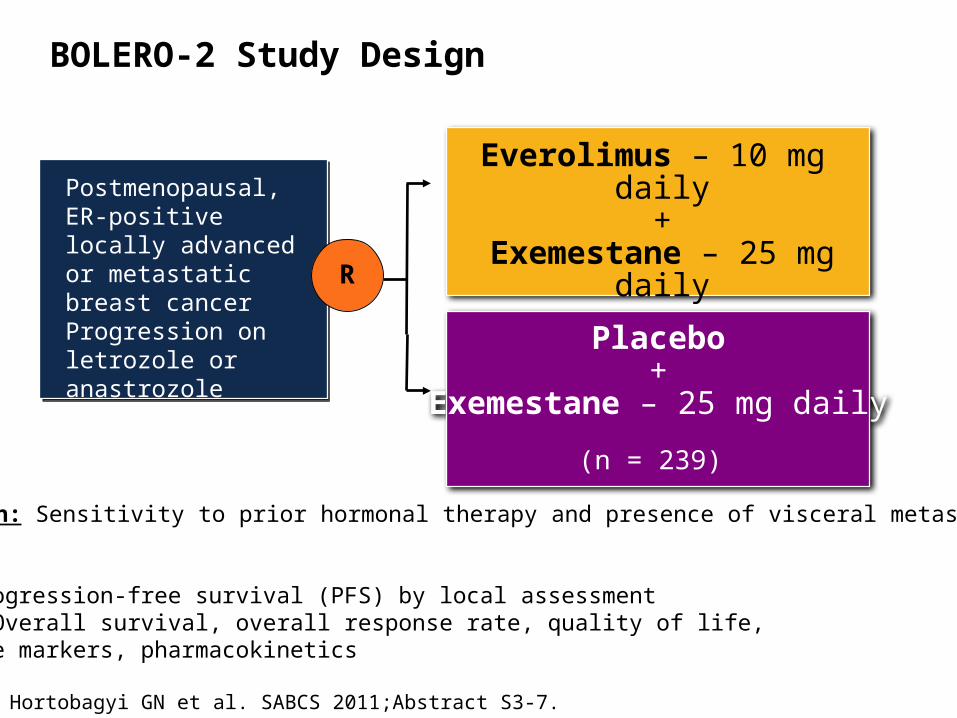
Hortobagyi GN et al. SABCS 2011;Abstract S3-7.
Postmenopausal, ER-positive locally advanced or metastatic breast cancerProgression on letrozole or anastrozole(n = 724)
R
Everolimus – 10 mg daily+
Exemestane – 25 mg daily
(n = 485)
Placebo+
Exemestane – 25 mg daily
(n = 239)
Stratification: Sensitivity to prior hormonal therapy and presence of visceral metastases
Endpoints:• Primary: Progression-free survival (PFS) by local assessment• Secondary: Overall survival, overall response rate, quality of life,
safety, bone markers, pharmacokinetics
BOLERO-2 Study Design
Patients with primary resistance were those relapsing during or within 6
months of stopping adjuvant AI treatment or progressing within 6
months of starting AI treatment in the metastatic setting
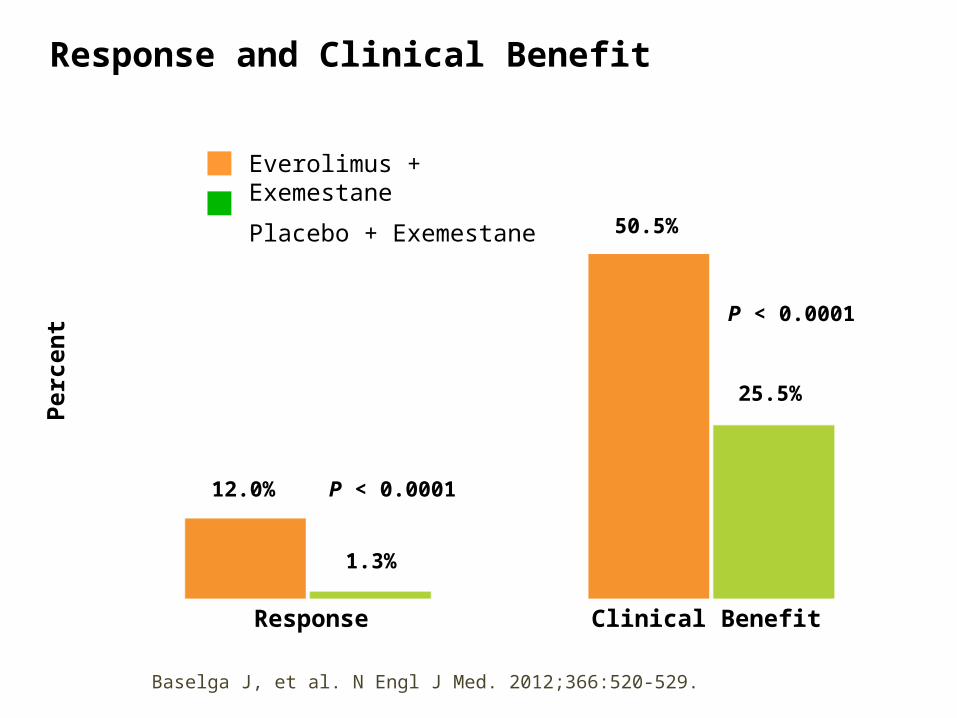
Response and Clinical Benefit
Everolimus + Exemestane
Placebo + Exemestane
Response Clinical Benefit
Perc
ent
12.0%
1.3%
50.5%
25.5%
P < 0.0001
P < 0.0001
Baselga J, et al. N Engl J Med. 2012;366:520-529.
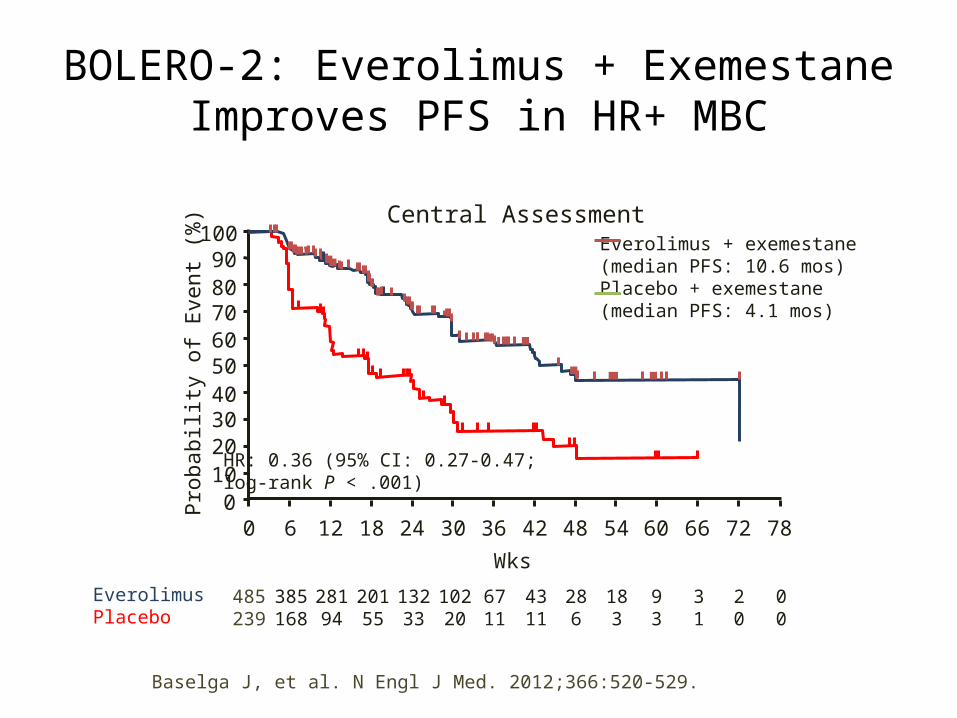
BOLERO-2: Everolimus + Exemestane Improves PFS in HR+ MBC
Baselga J, et al. N Engl J Med. 2012;366:520-529.
0 6 12 18 24 30 36 42 48 54 60 66 72 78Wks
Prob
abili
ty o
f Eve
nt (%
)
Everolimus + exemestane(median PFS: 10.6 mos)Placebo + exemestane(median PFS: 4.1 mos)
HR: 0.36 (95% CI: 0.27-0.47;log-rank P < .001)
Patients at Risk, nEverolimusPlacebo
485239
385168
28194
20155
13233
10220
6711
4311
286
183
93
31
20
00
100908070605040302010
0
Central Assessment
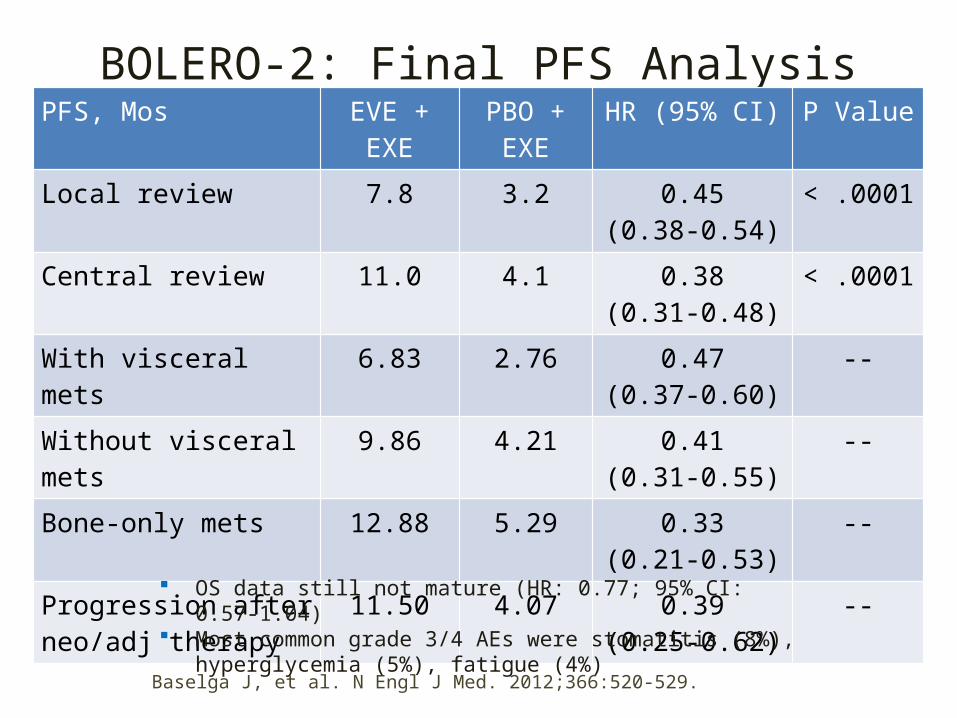
BOLERO-2: Final PFS Analysis (18-Mo Follow-up)PFS, Mos EVE + EXE PBO + EXE HR (95% CI) P Value
Local review 7.8 3.2 0.45(0.38-0.54)
< .0001
Central review 11.0 4.1 0.38(0.31-0.48)
< .0001
With visceral mets 6.83 2.76 0.47(0.37-0.60)
--
Without visceral mets 9.86 4.21 0.41(0.31-0.55)
--
Bone-only mets 12.88 5.29 0.33(0.21-0.53)
--
Progression after neo/adj therapy
11.50 4.07 0.39(0.25-0.62)
--
OS data still not mature (HR: 0.77; 95% CI: 0.57-1.04) Most common grade 3/4 AEs were stomatitis (8%), hyperglycemia
(5%), fatigue (4%)
Baselga J, et al. N Engl J Med. 2012;366:520-529.
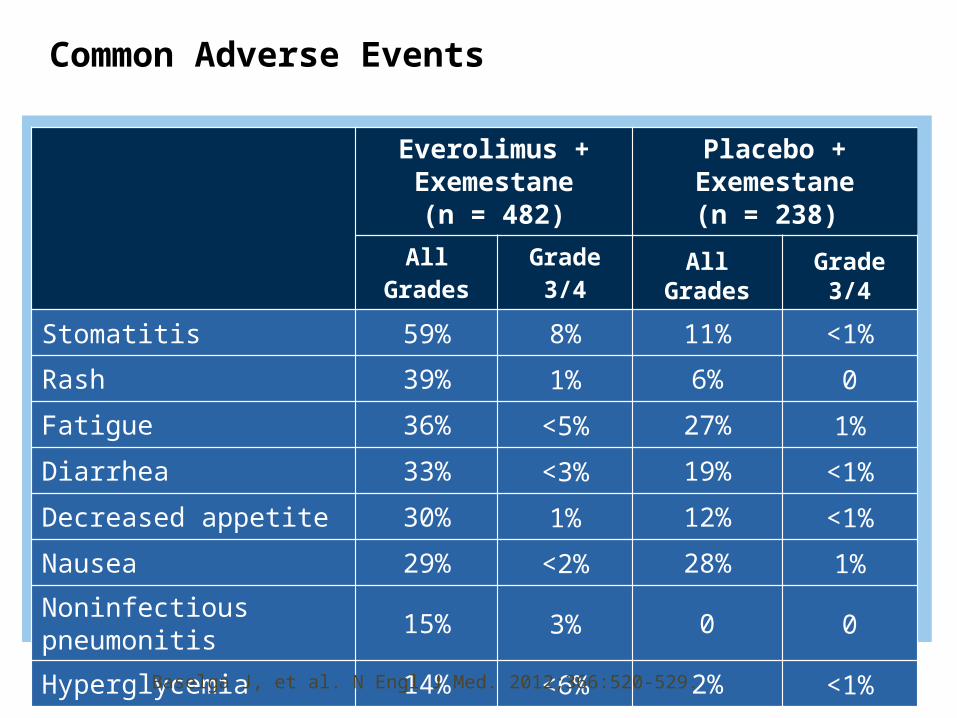
Common Adverse Events
Everolimus + Exemestane
(n = 482)
Placebo + Exemestane
(n = 238) All Grades Grade 3/4 All Grades Grade 3/4
Stomatitis 59% 8% 11% <1%Rash 39% 1% 6% 0Fatigue 36% <5% 27% 1%Diarrhea 33% <3% 19% <1%Decreased appetite 30% 1% 12% <1%Nausea 29% <2% 28% 1%Noninfectious pneumonitis 15% 3% 0 0
Hyperglycemia 14% <6% 2% <1%
Baselga J, et al. N Engl J Med. 2012;366:520-529.
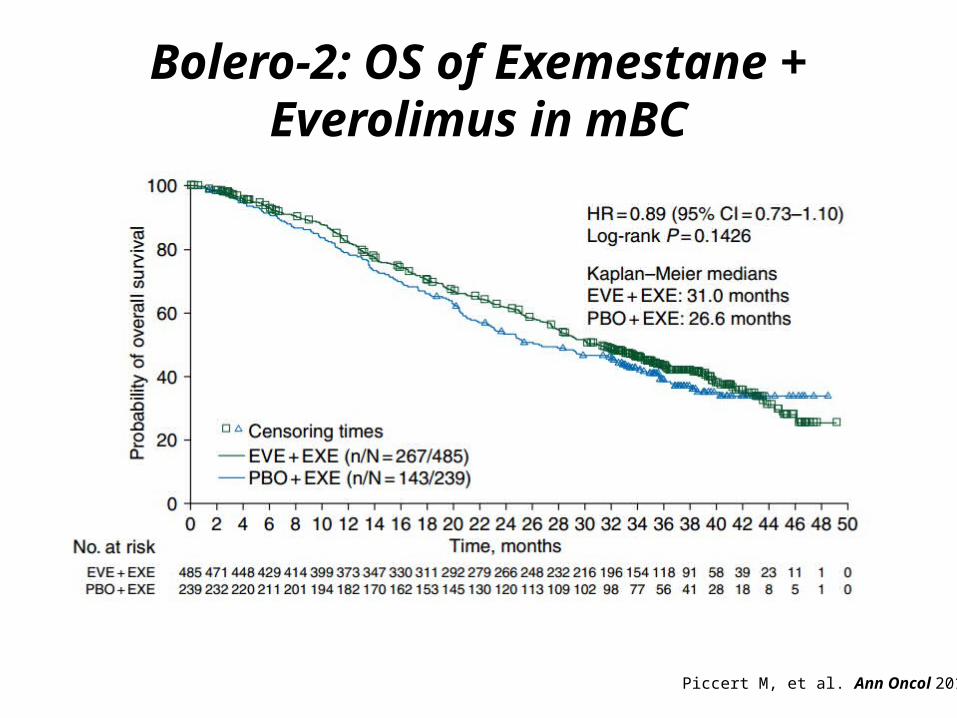
Bolero-2: OS of Exemestane + Everolimus in mBC
Piccert M, et al. Ann Oncol 2014
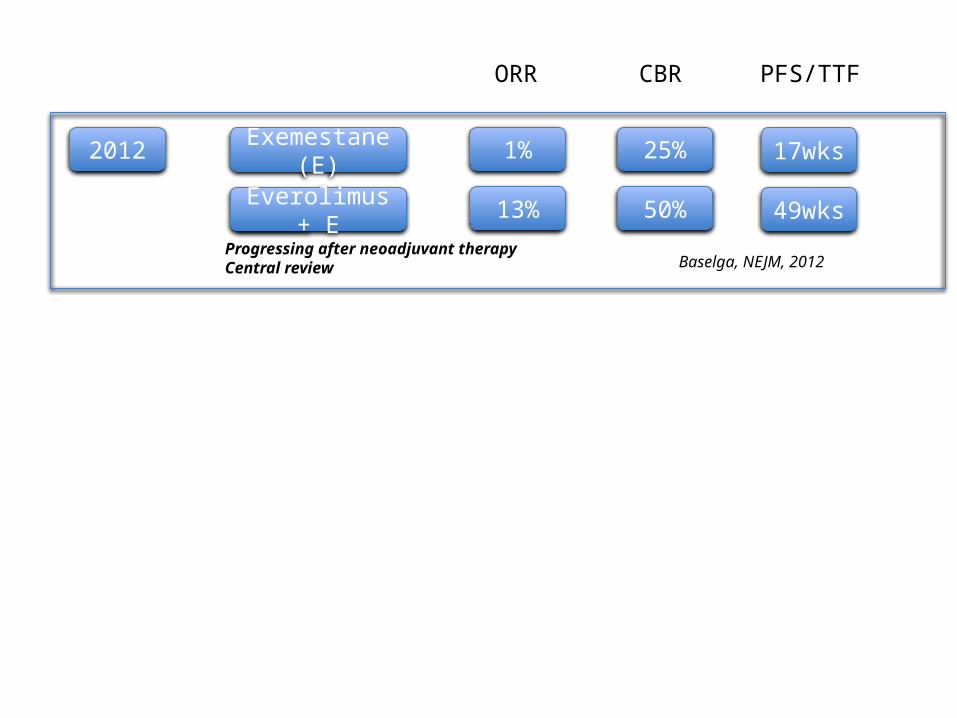
2012 Exemestane (E) 1% 17wks25%
Everolimus + E 13% 49wks50%
Baselga, NEJM, 2012
ORR CBR PFS/TTF
Progressing after neoadjuvant therapyCentral review
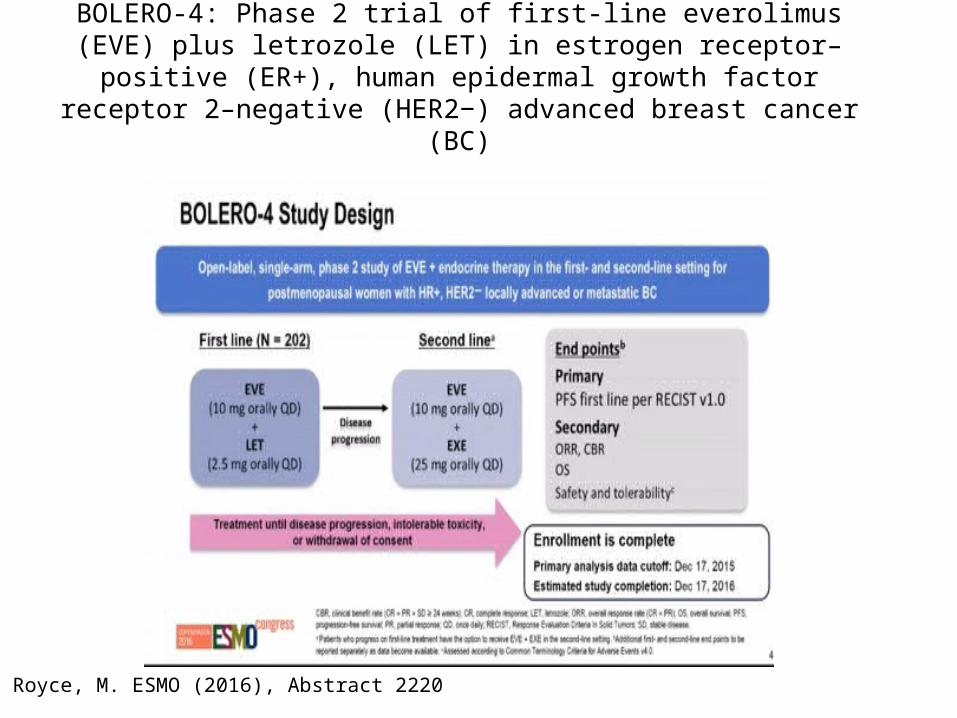
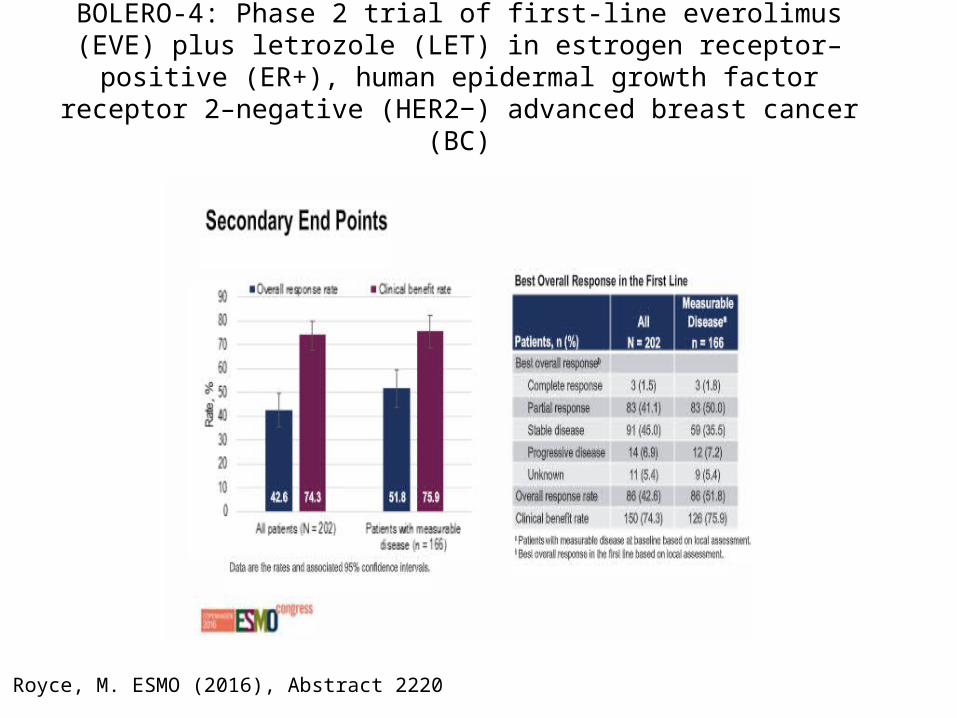
Royce, M. ESMO (2016), Abstract 2220
BOLERO-4: Phase 2 trial of first-line everolimus (EVE) plus letrozole (LET) in estrogen receptor–positive (ER+), human epidermal growth factor receptor
2–negative (HER2−) advanced breast cancer (BC)
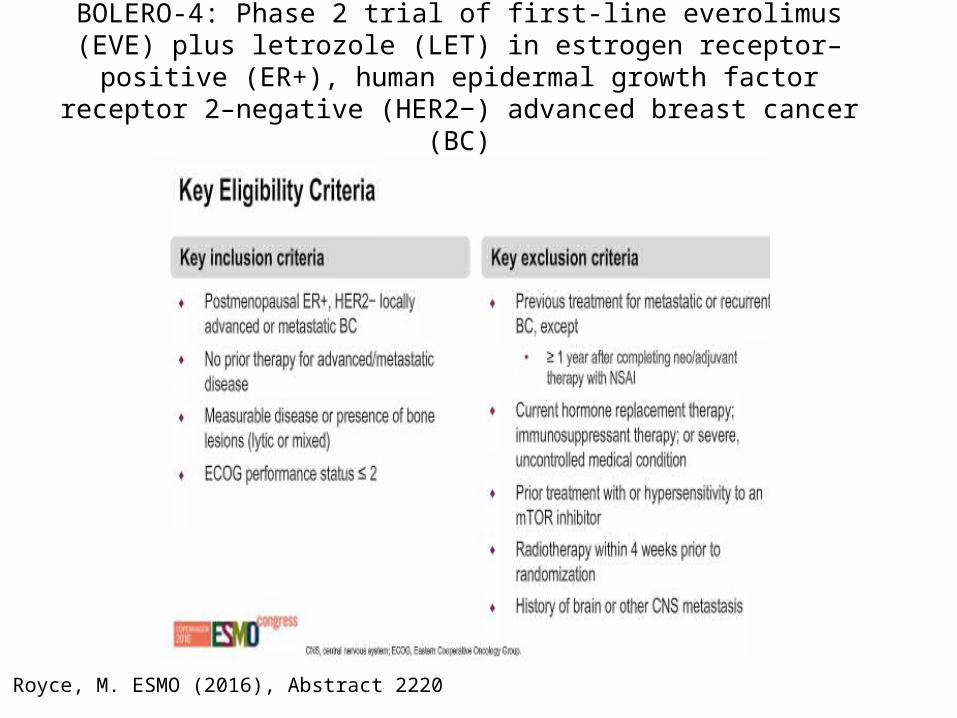
Royce, M. ESMO (2016), Abstract 2220
BOLERO-4: Phase 2 trial of first-line everolimus (EVE) plus letrozole (LET) in estrogen receptor–positive (ER+), human epidermal growth factor receptor
2–negative (HER2−) advanced breast cancer (BC)
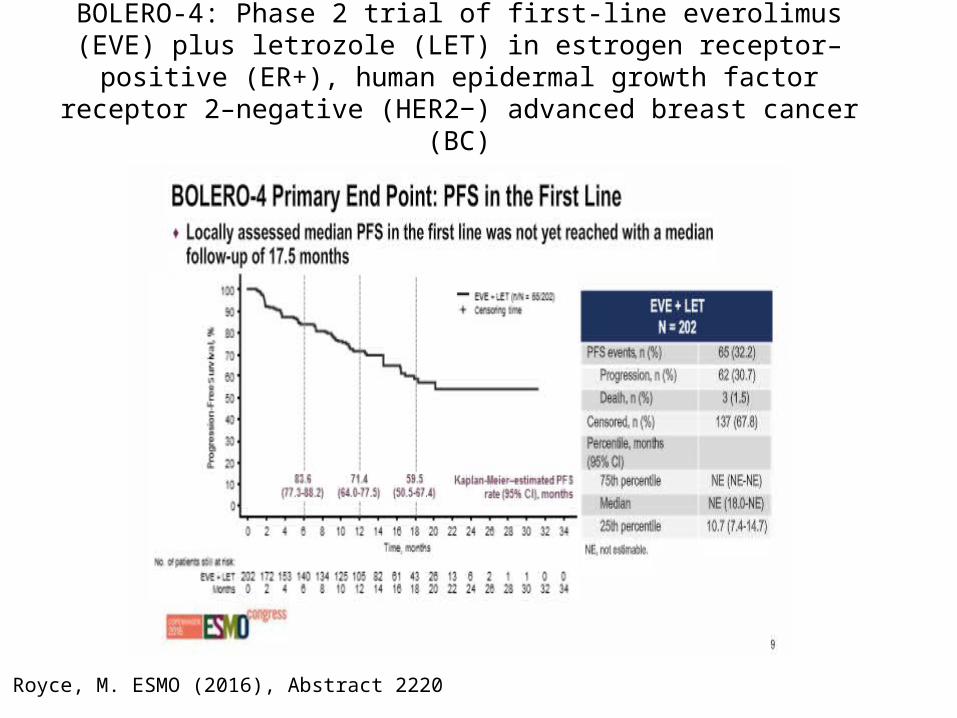
Royce, M. ESMO (2016), Abstract 2220
BOLERO-4: Phase 2 trial of first-line everolimus (EVE) plus letrozole (LET) in estrogen receptor–positive (ER+), human epidermal growth factor receptor
2–negative (HER2−) advanced breast cancer (BC)
Royce, M. ESMO (2016), Abstract 2220
BOLERO-4: Phase 2 trial of first-line everolimus (EVE) plus letrozole (LET) in estrogen receptor–positive (ER+), human epidermal growth factor receptor
2–negative (HER2−) advanced breast cancer (BC)
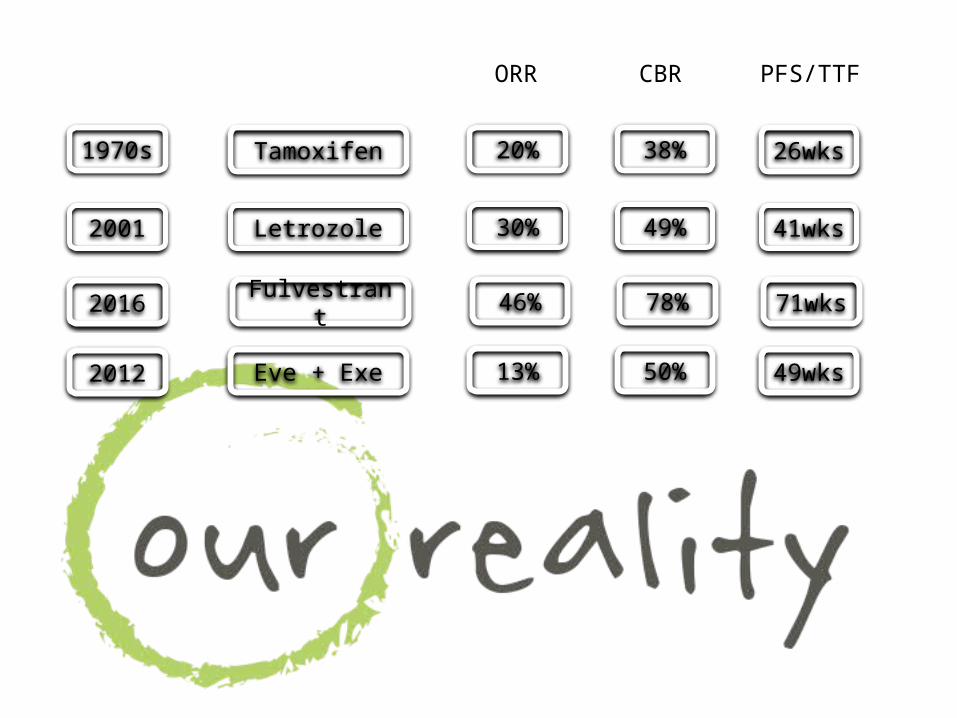
1970s Tamoxifen 20% 26wks38%
ORR CBR PFS/TTF
2016 Fulvestrant 46% 71wks78%
2001 Letrozole 30% 41wks49%
2012 Eve + Exe 13% 49wks50%
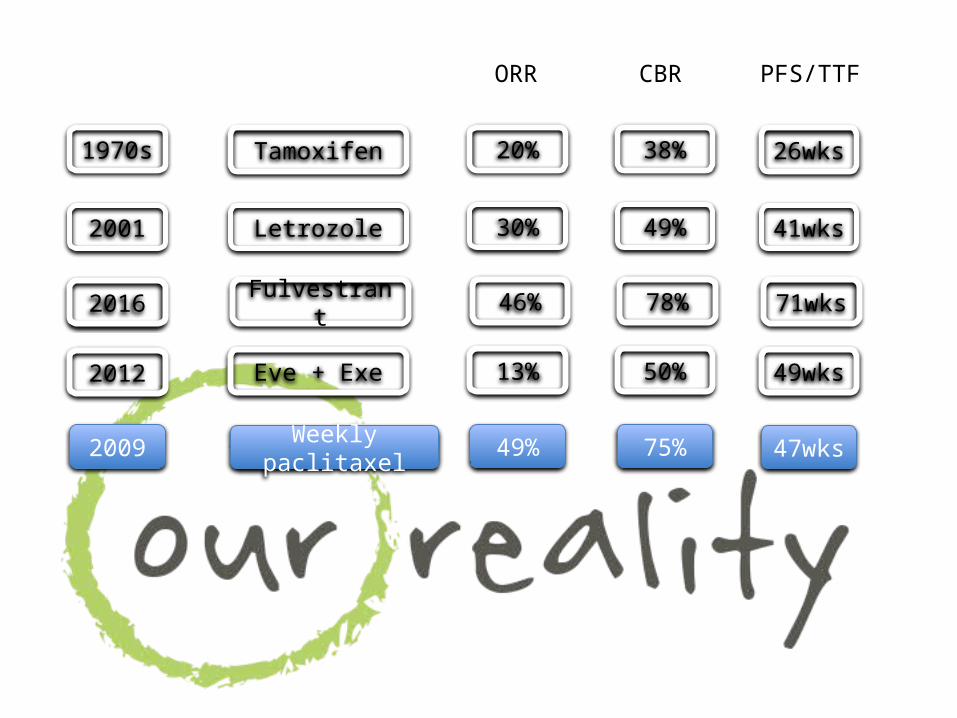
1970s Tamoxifen 20% 26wks38%
ORR CBR PFS/TTF
2016 Fulvestrant 46% 71wks78%
2001 Letrozole 30% 41wks49%
2012 Eve + Exe 13% 49wks50%
2009 Weekly paclitaxel 49% 47wks75%
PALOMA-2: Addition of Palbociclib to Frontline Letrozole Significantly Improves PFS in
Postmenopausal ER+/HER2- Advanced Breast Cancer
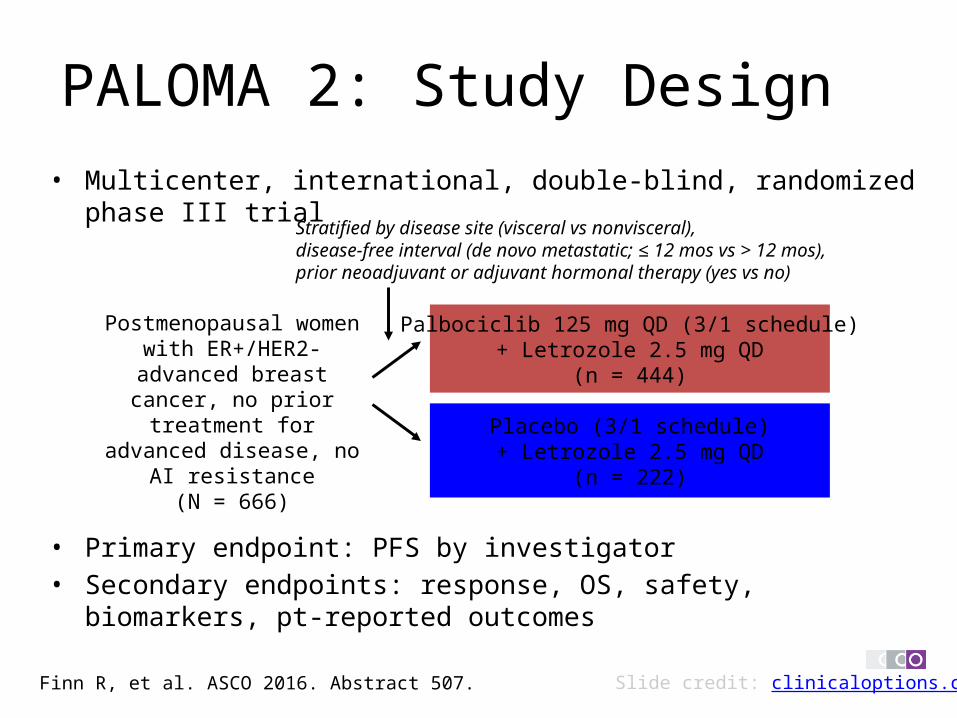
PALOMA 2: Study Design • Multicenter, international, double-blind, randomized phase III trial
• Primary endpoint: PFS by investigator• Secondary endpoints: response, OS, safety, biomarkers, pt-reported
outcomes
Postmenopausal women with ER+/HER2- advanced
breast cancer, no prior treatment for advanced
disease, no AI resistance(N = 666)
Stratified by disease site (visceral vs nonvisceral), disease-free interval (de novo metastatic; ≤ 12 mos vs > 12 mos), prior neoadjuvant or adjuvant hormonal therapy (yes vs no)
Palbociclib 125 mg QD (3/1 schedule)+ Letrozole 2.5 mg QD
(n = 444)
Placebo (3/1 schedule)+ Letrozole 2.5 mg QD
(n = 222)
Slide credit: clinicaloptions.comFinn R, et al. ASCO 2016. Abstract 507.
Slide credit: clinicaloptions.com
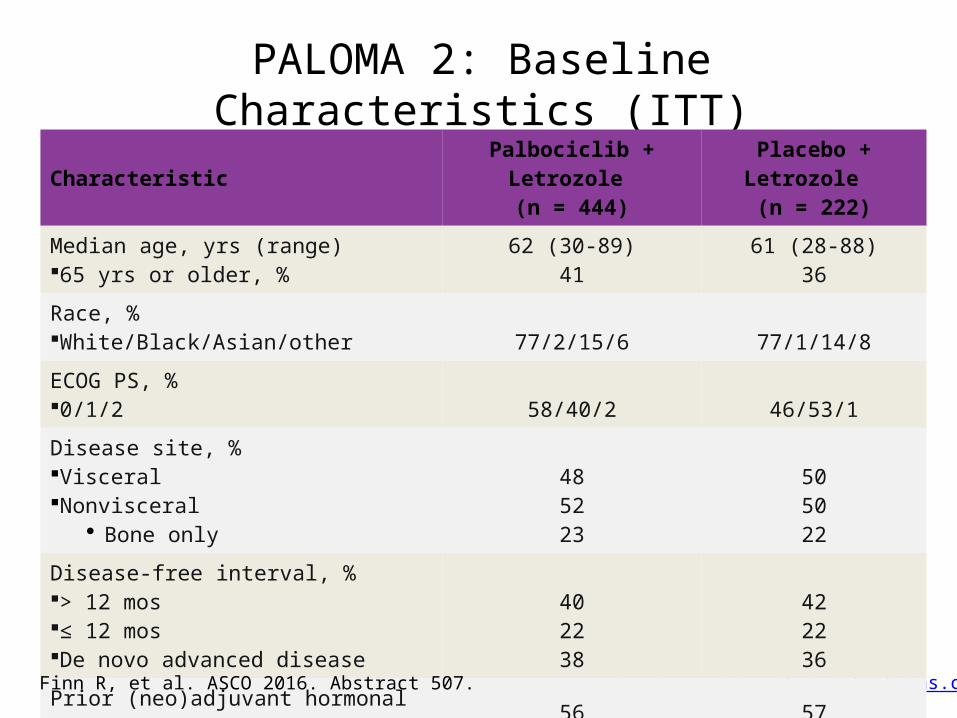
PALOMA 2: Baseline Characteristics (ITT)
CharacteristicPalbociclib + Letrozole
(n = 444)Placebo + Letrozole
(n = 222)
Median age, yrs (range) 65 yrs or older, %
62 (30-89)41
61 (28-88)36
Race, %White/Black/Asian/other 77/2/15/6 77/1/14/8
ECOG PS, %0/1/2 58/40/2 46/53/1
Disease site, %VisceralNonvisceral
• Bone only
485223
505022
Disease-free interval, %> 12 mos≤ 12 mosDe novo advanced disease
402238
422236
Prior (neo)adjuvant hormonal therapy, % 56 57
Finn R, et al. ASCO 2016. Abstract 507.
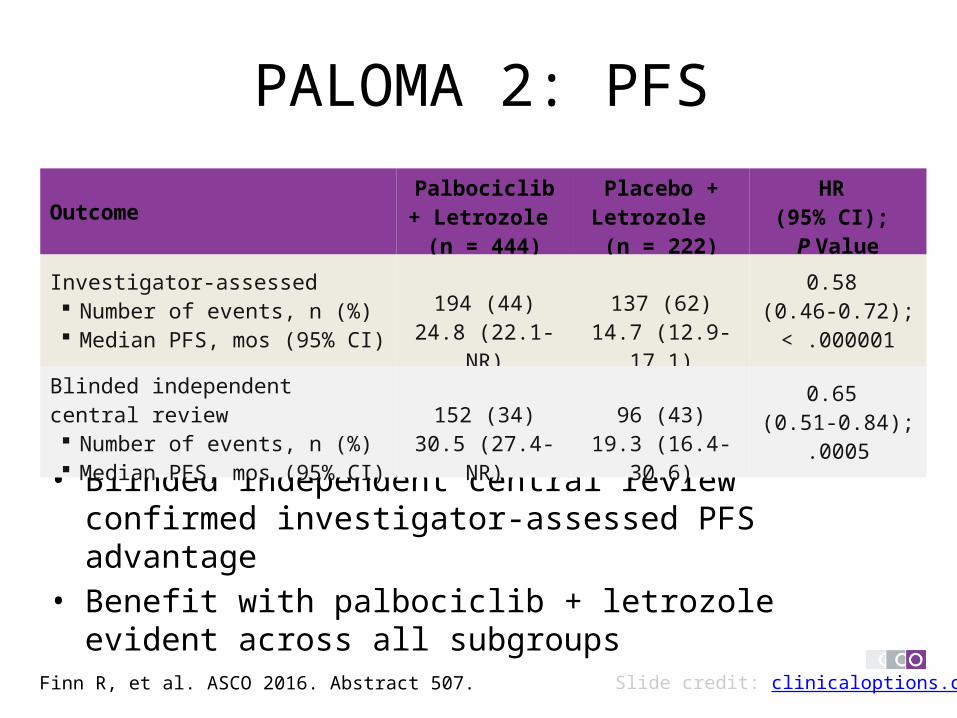
PALOMA 2: PFS
• Blinded independent central review confirmed investigator-assessed PFS advantage
• Benefit with palbociclib + letrozole evident across all subgroups
Slide credit: clinicaloptions.comFinn R, et al. ASCO 2016. Abstract 507.
OutcomePalbociclib +
Letrozole (n = 444)
Placebo + Letrozole (n = 222)
HR (95% CI); P Value
Investigator-assessed Number of events, n (%) Median PFS, mos (95% CI)
194 (44)24.8 (22.1-NR)
137 (62)14.7 (12.9-17.1)
0.58 (0.46-0.72); < .000001
Blinded independent central review Number of events, n (%) Median PFS, mos (95% CI)
152 (34)30.5 (27.4-NR)
96 (43)19.3 (16.4-30.6)
0.65 (0.51-0.84);
.0005
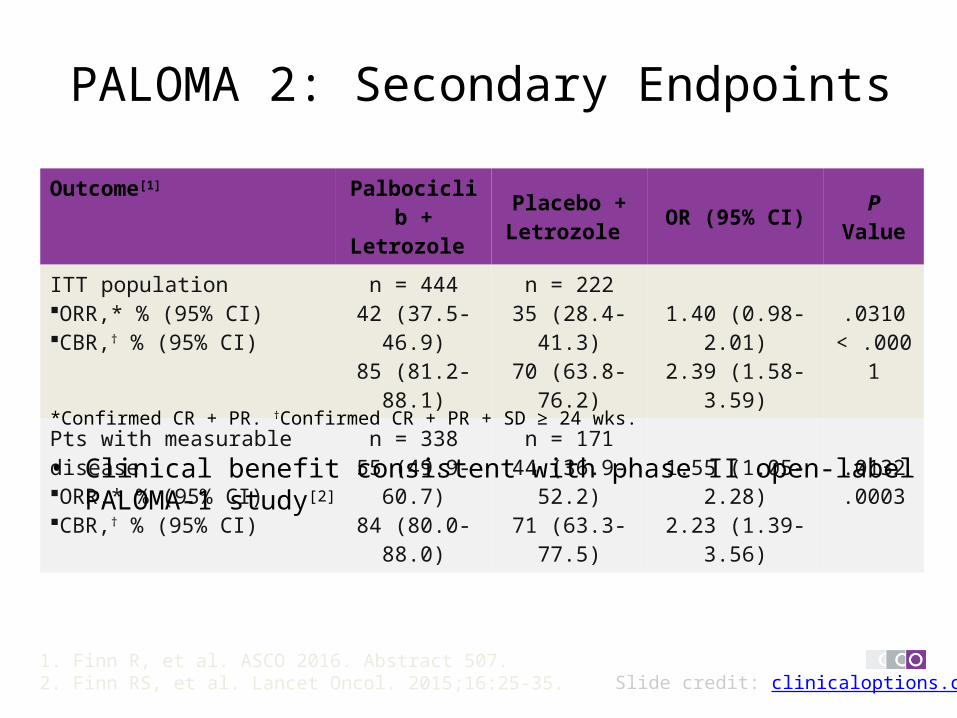
Outcome[1] Palbociclib + Letrozole
Placebo + Letrozole OR (95% CI) P Value
ITT populationORR,* % (95% CI)CBR,† % (95% CI)
n = 44442 (37.5-46.9)85 (81.2-88.1)
n = 22235 (28.4-41.3)70 (63.8-76.2)
1.40 (0.98-2.01)2.39 (1.58-3.59)
.0310< .0001
Pts with measurable diseaseORR,* % (95% CI)CBR,† % (95% CI)
n = 33855 (49.9-60.7)84 (80.0-88.0)
n = 17144 (36.9-52.2)71 (63.3-77.5)
1.55 (1.05-2.28)2.23 (1.39-3.56)
.0132
.0003
PALOMA 2: Secondary Endpoints
• Clinical benefit consistent with phase II open-label PALOMA-1 study[2]
Slide credit: clinicaloptions.com
*Confirmed CR + PR. †Confirmed CR + PR + SD ≥ 24 wks.
1. Finn R, et al. ASCO 2016. Abstract 507. 2. Finn RS, et al. Lancet Oncol. 2015;16:25-35.
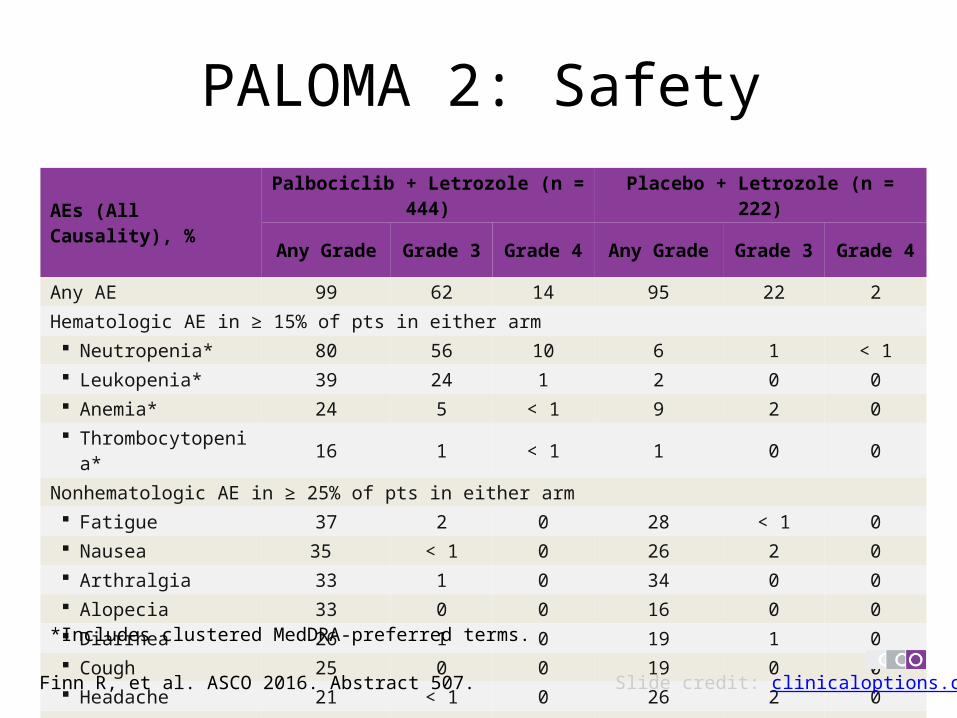
PALOMA 2: Safety
AEs (All Causality), % Palbociclib + Letrozole (n = 444) Placebo + Letrozole (n = 222)Any Grade Grade 3 Grade 4 Any Grade Grade 3 Grade 4
Any AE 99 62 14 95 22 2Hematologic AE in ≥ 15% of pts in either arm Neutropenia* 80 56 10 6 1 < 1 Leukopenia* 39 24 1 2 0 0 Anemia* 24 5 < 1 9 2 0 Thrombocytopenia* 16 1 < 1 1 0 0
Nonhematologic AE in ≥ 25% of pts in either arm Fatigue 37 2 0 28 < 1 0 Nausea 35 < 1 0 26 2 0 Arthralgia 33 1 0 34 0 0 Alopecia 33 0 0 16 0 0 Diarrhea 26 1 0 19 1 0 Cough 25 0 0 19 0 0 Headache 21 < 1 0 26 2 0 Hot flush 21 0 0 31 0 0
*Includes clustered MedDRA-preferred terms.
Finn R, et al. ASCO 2016. Abstract 507. Slide credit: clinicaloptions.com
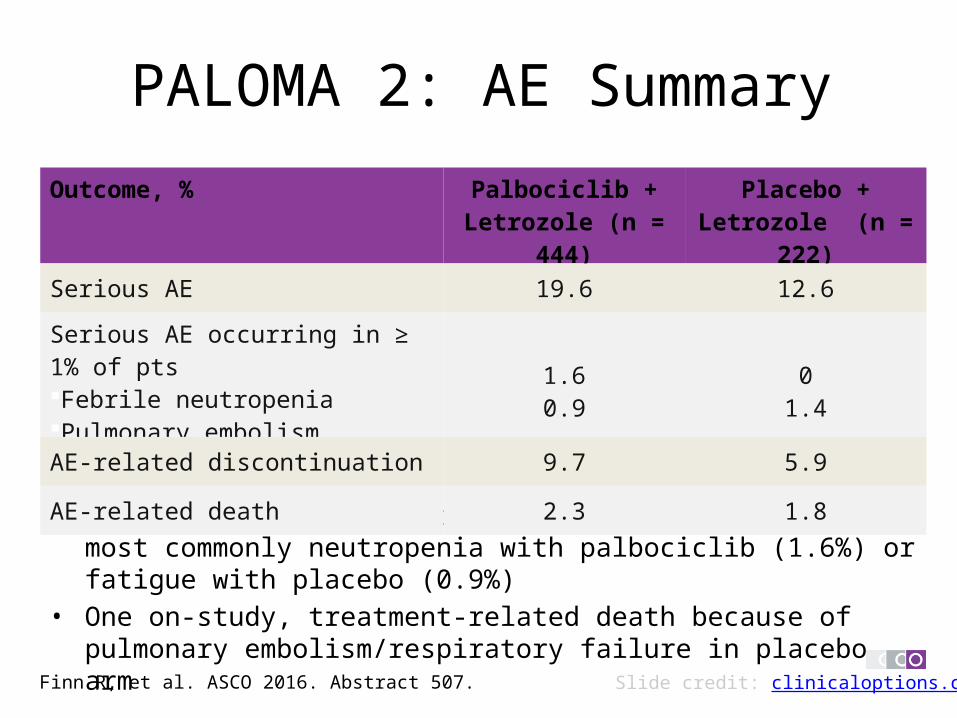
PALOMA 2: AE Summary
• Most AEs resulting in d/c reported as single events, most commonly neutropenia with palbociclib (1.6%) or fatigue with placebo (0.9%)
• One on-study, treatment-related death because of pulmonary embolism/respiratory failure in placebo arm
Slide credit: clinicaloptions.comFinn R, et al. ASCO 2016. Abstract 507.
Outcome, % Palbociclib + Letrozole (n = 444)
Placebo + Letrozole (n = 222)
Serious AE 19.6 12.6
Serious AE occurring in ≥ 1% of ptsFebrile neutropeniaPulmonary embolism
1.60.9
01.4
AE-related discontinuation 9.7 5.9
AE-related death 2.3 1.8
PALOMA 2: Conclusions• First-line palbociclib + letrozole significantly improved median PFS vs
placebo + letrozole in women with ER+/HER2- advanced breast cancer– Median PFS improved by > 10 mos compared to placebo
• 24.8 mos vs 14.5 mos, HR: 0.58 (95% CI: 0.46-0.72; P < .0001)
• Palbociclib clinical benefit observed in all prespecified subgroups• Palbociclib well tolerated with neutropenia, leukopenia the most
frequently reported AEs• PALOMA-2[1] data confirm PALOMA-1[2] results and constitute the longest
median PFS improvement to date in the front-line setting in advanced ER+ breast cancer
Slide credit: clinicaloptions.com1. Finn R, et al. ASCO 2016. Abstract 507.2. Finn RS, et al. Lancet Oncol. 2015;16:25-35.
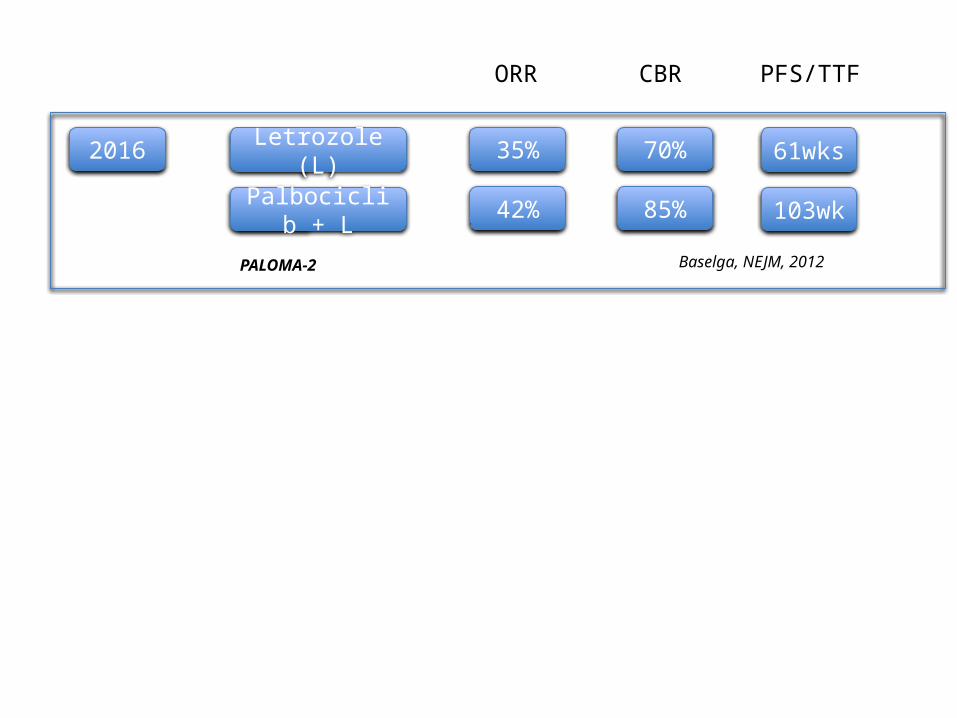
2016 Letrozole (L) 35% 61wks70%
Palbociclib + L 42% 103wk85%
Baselga, NEJM, 2012
ORR CBR PFS/TTF
PALOMA-2
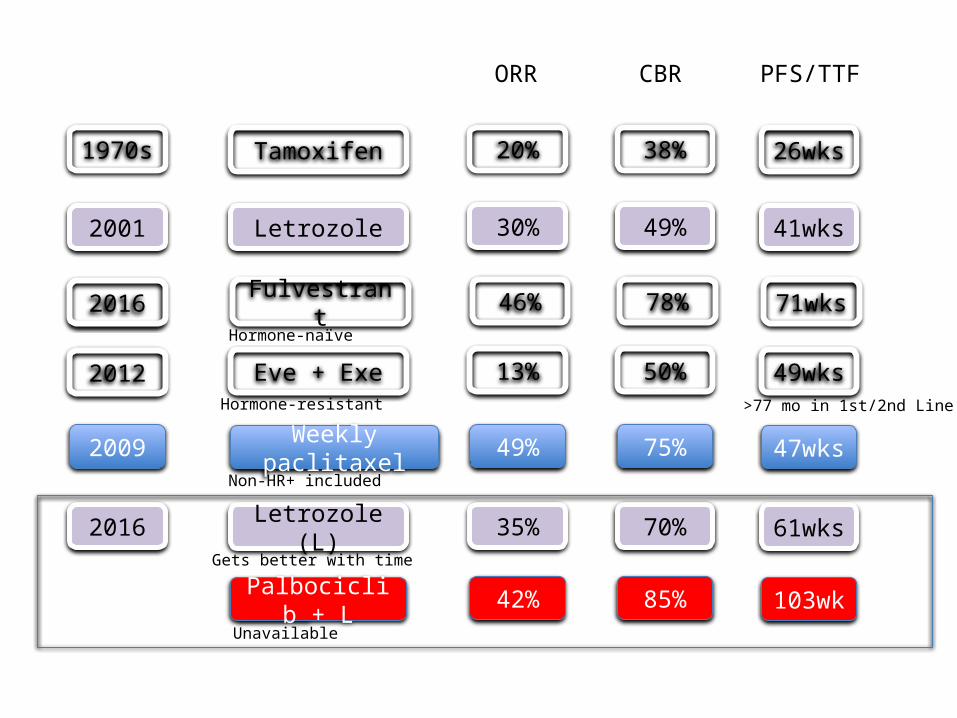
1970s Tamoxifen 20% 26wks38%
ORR CBR PFS/TTF
2016 Fulvestrant 46% 71wks78%
2001 Letrozole 30% 41wks49%
2012 Eve + Exe 13% 49wks50%
2009 Weekly paclitaxel 49% 47wks75%
2016 Letrozole (L) 35% 61wks70%
Palbociclib + L 42% 103wk85%
Hormone-resistant
Hormone-naïve
Non-HR+ included
Gets better with time
Unavailable
>77 mo in 1st/2nd Line

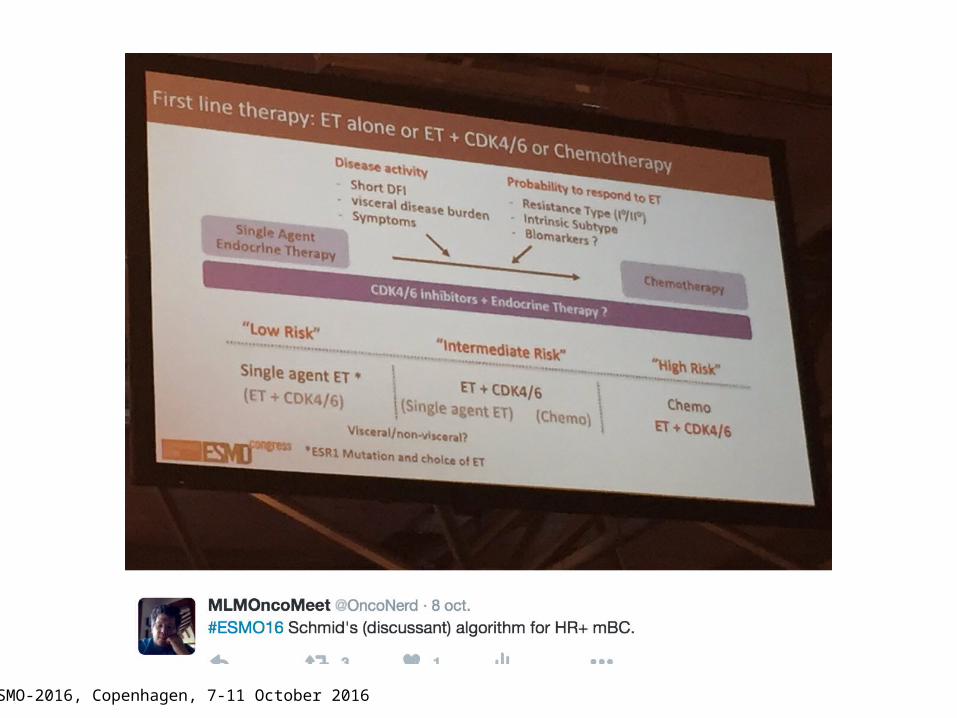
ESMO-2016, Copenhagen, 7-11 October 2016
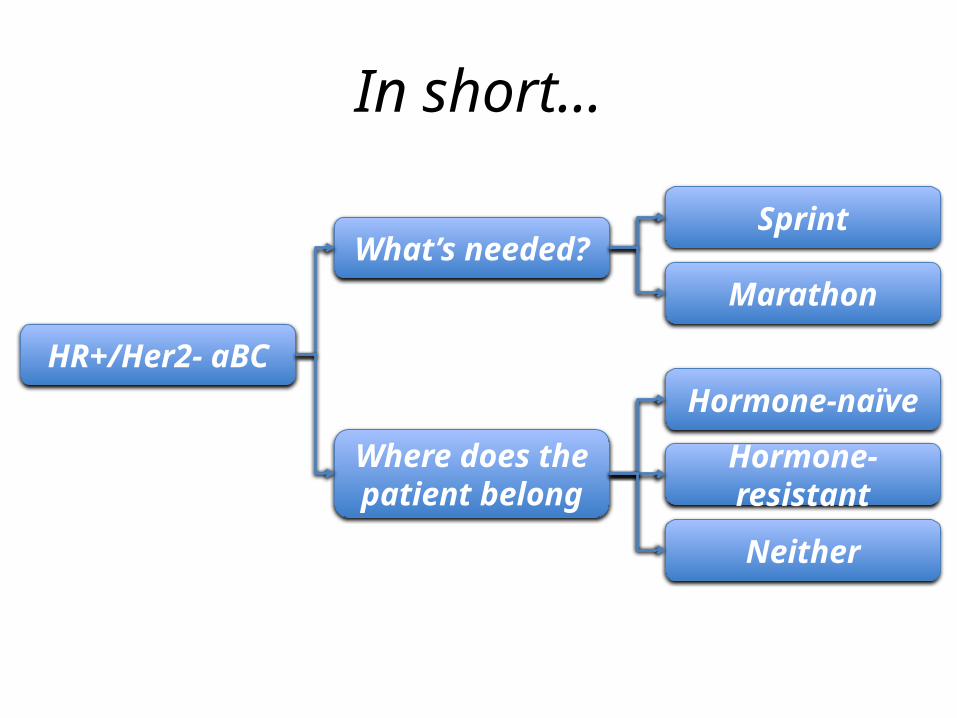
HR+/Her2- aBC
What’s needed?Sprint
Marathon
Hormone-naïve
Hormone-resistant
Neither
Where does the patient belong
In short…
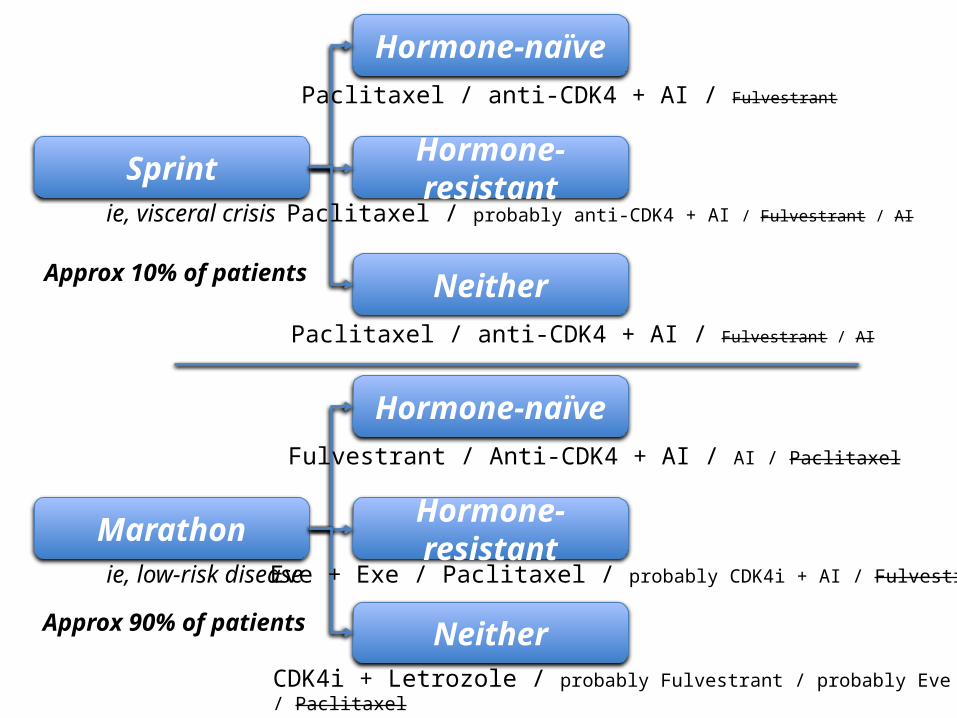
Hormone-naïve
Sprint Hormone-resistant
Neither
Paclitaxel / anti-CDK4 + AI / Fulvestrant
Paclitaxel / probably anti-CDK4 + AI / Fulvestrant / AI
Paclitaxel / anti-CDK4 + AI / Fulvestrant / AI
ie, visceral crisis
Hormone-naïve
Marathon Hormone-resistant
Neither
Fulvestrant / Anti-CDK4 + AI / AI / Paclitaxel
Eve + Exe / Paclitaxel / probably CDK4i + AI / Fulvestrant
CDK4i + Letrozole / probably Fulvestrant / probably Eve + Let / Paclitaxel
ie, low-risk disease
Approx 10% of patients
Approx 90% of patients
@Onconerd