Sesión Urgencias Psiquiátricas
32
URGENCIAS PSIQUIATRICAS
-
Upload
urgencias-fml -
Category
Health & Medicine
-
view
119 -
download
3
Transcript of Sesión Urgencias Psiquiátricas
URGENCIAS PSIQUIATRICAS
CONCEPTOS FUNDAMENTALES
Perturbación en el pensamiento, los sentimientos o la conducta
que requiere intervención terapéutica urgente.
Anamnesis, expl. Física, pruebas complementarias, exploración
Psiquiátrica, orientación clínica y plan de tratamiento.
DESCARTAR ORGANICIDAD.
CARACTERISTICAS SUGERENTES DE
ORGANICIDAD
Comienzo brusco sin hª previa.
Síntomas en >65 años o síntomas psicóticos en > 45 años.
Alteraciones perceptivas no auditivas.
Síntomas neurológicos: incontinencia de esfínteres.
Fluctuación o alt conciencia, desorientación, alt memoria,
concentración…
Trast. Movimiento, marcha o lenguaje, catatonía.
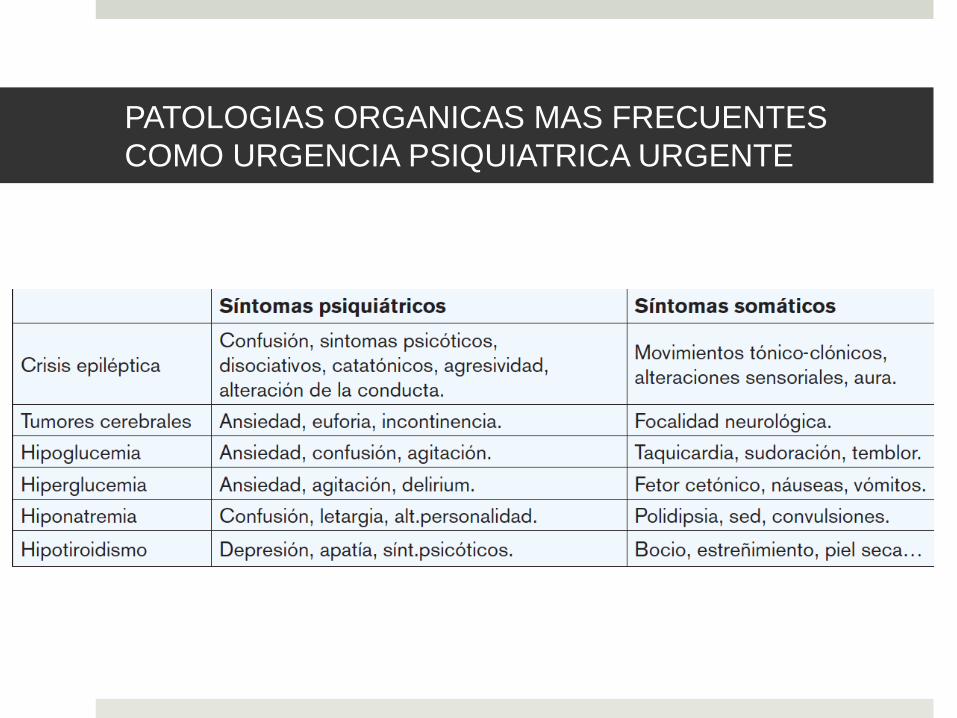
PATOLOGIAS ORGANICAS MAS FRECUENTES
COMO URGENCIA PSIQUIATRICA URGENTE
EXPLORACION PSIQUIATRICA
Información de comunicación verbal y no verbal, de los
acompañantes o terceros presentes o por vía telefónica.
Informar al paciente de que se va a recoger esta información, y
solicitar su permiso.
Appearance, Attitude, Behavior, Mood and affect, Speech,
Thought process, Thought content, Perceptions, Cognition,
Insight,Judgment,
SINDROMES PRINCIPALES EN LA
URGENCIA PSIQUIATRICA
AGITACION Y COMPORTAMIENTOS VIOLENTOS.
COMPORTAMIENTOS AUTOLOTICOS.
CRISIS DE ANGUSTIA.
CRISIS DE ANGUSTIA
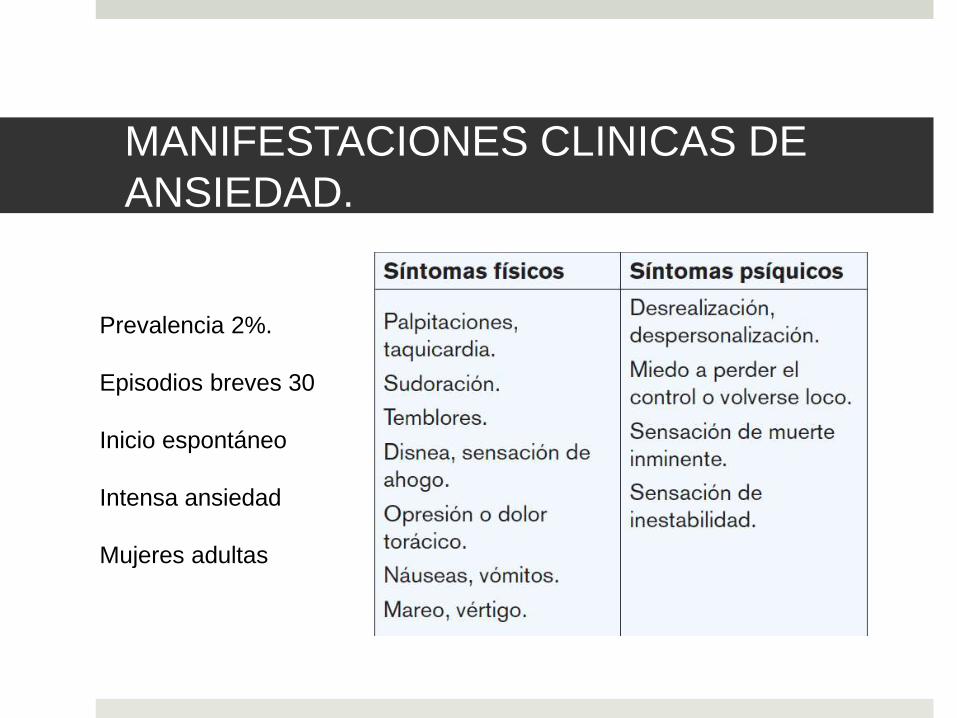
MANIFESTACIONES CLINICAS DE
ANSIEDAD.
Prevalencia 2%.
Episodios breves 30
Inicio espontáneo
Intensa ansiedad
Mujeres adultas
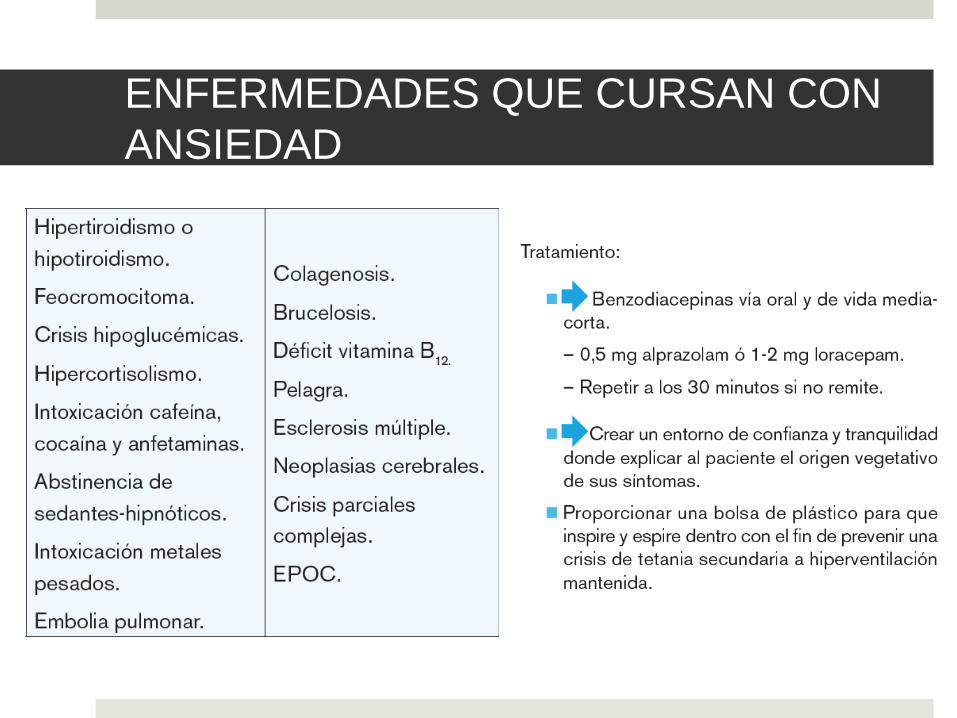
ENFERMEDADES QUE CURSAN CON
ANSIEDAD
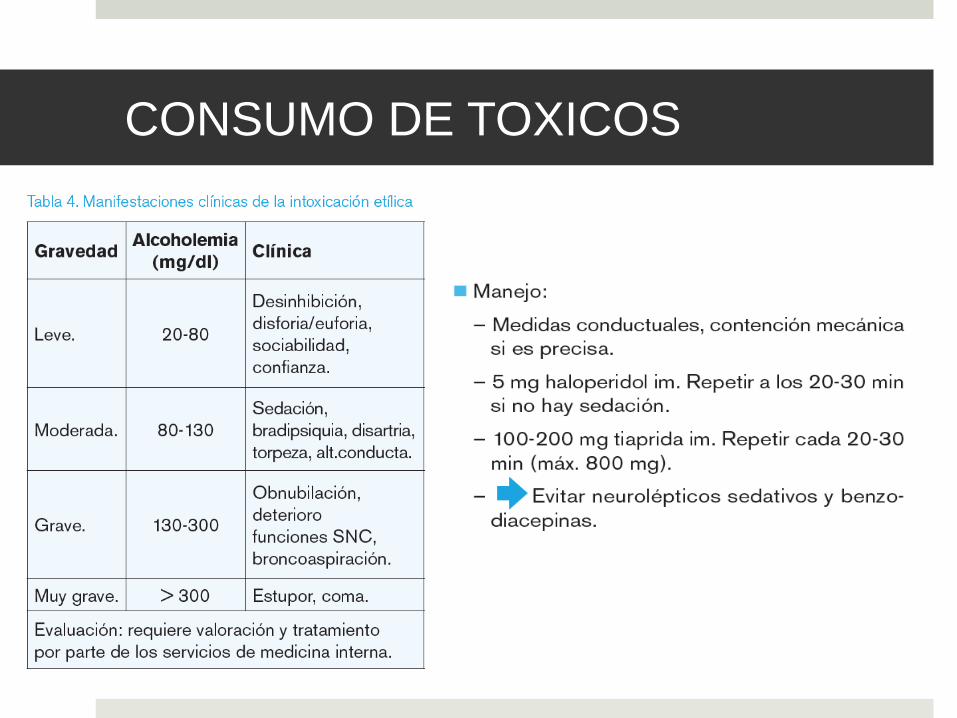
CONSUMO DE TOXICOS
SINDROME DE ABSTINENCIA
Deprivación brusca, parcial o total.
4-12 h Pico 48 h Mejoría 4º día
Primera fase- dolor de cabeza, agitación, temblores graves, náuseas y vómitos gran sudoración, somnolencia, calambres e incluso alucinaciones.
Segunda fase- Síntomas anteriores y actividad convulsiva.
Tercera fase- DELIRIUM TREMENS- confusión, ilusiones extrañas, alucinaciones muy perturbadoras, agitación, midriasis, diaforesis, taquipnea, hipertermia y taquicardia.
MORTAL-20% sin tto y 5% con tto.
TRATAMIENTO ABSTINENCIA
ALCOHOLICA
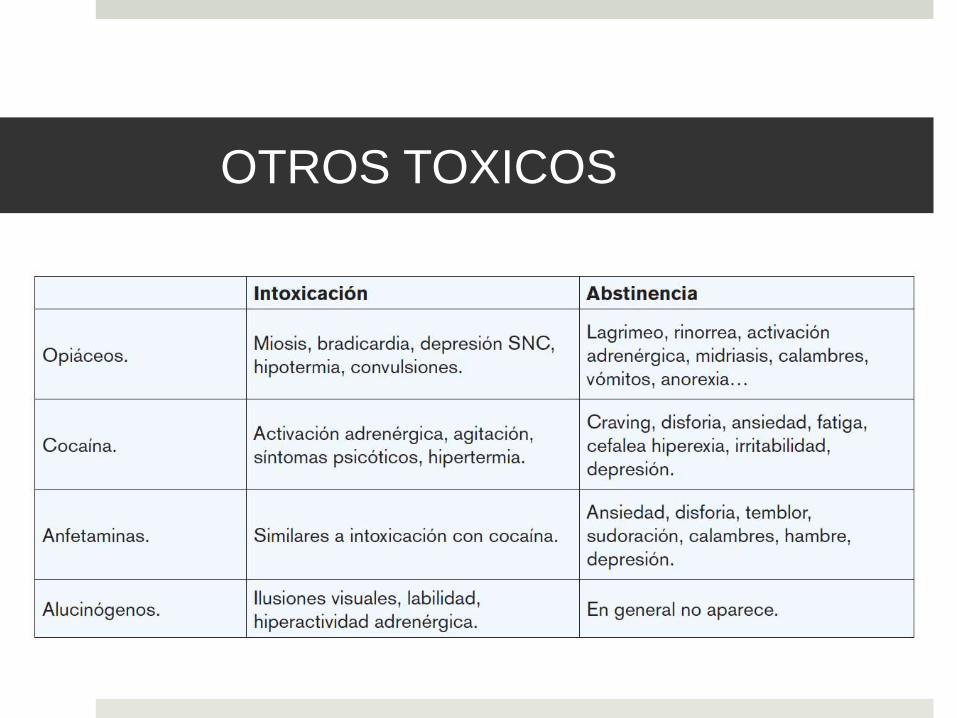
OTROS TOXICOS
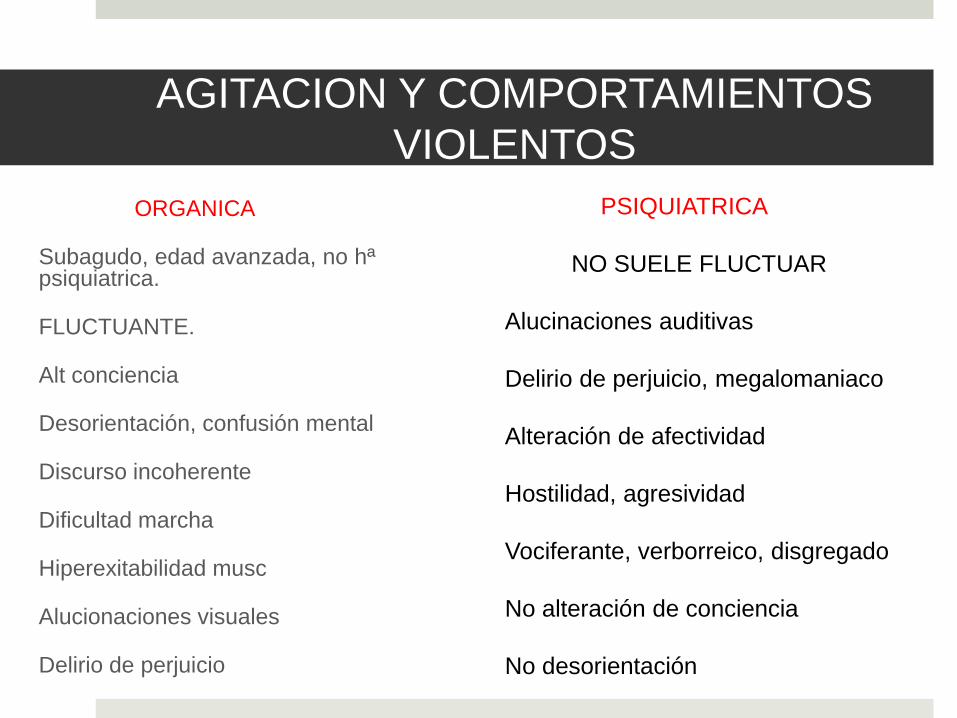
AGITACION Y COMPORTAMIENTOS
VIOLENTOS
ORGANICA
Subagudo, edad avanzada, no hªpsiquiatrica.
FLUCTUANTE.
Alt conciencia
Desorientación, confusión mental
Discurso incoherente
Dificultad marcha
Hiperexitabilidad musc
Alucionaciones visuales
Delirio de perjuicio
PSIQUIATRICA
NO SUELE FLUCTUAR
Alucinaciones auditivas
Delirio de perjuicio, megalomaniaco
Alteración de afectividad
Hostilidad, agresividad
Vociferante, verborreico, disgregado
No alteración de conciencia
No desorientación
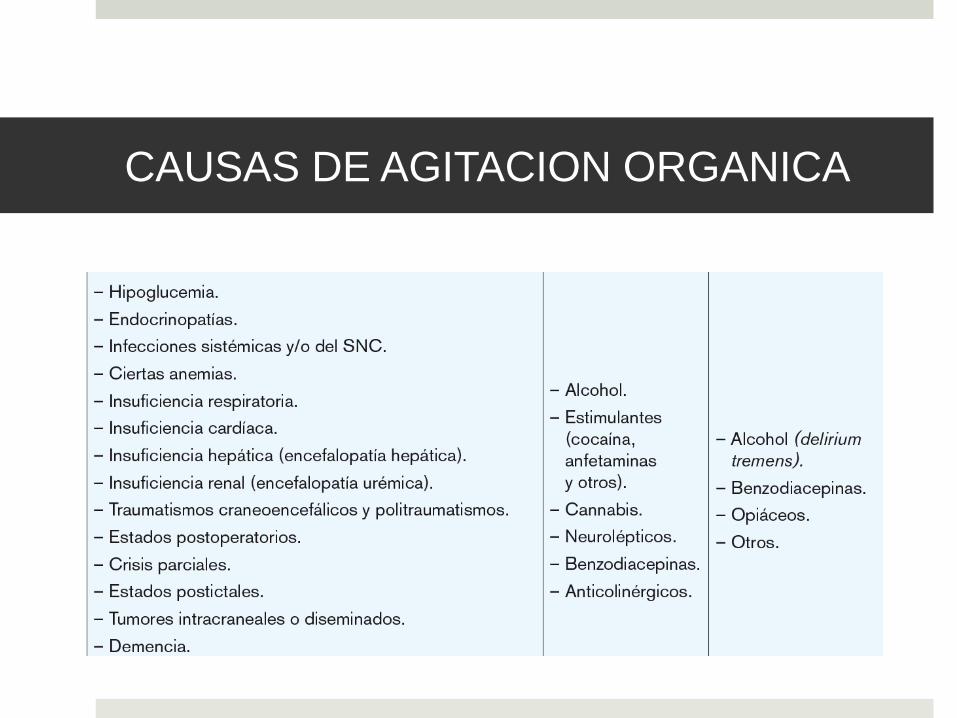
CAUSAS DE AGITACION ORGANICA
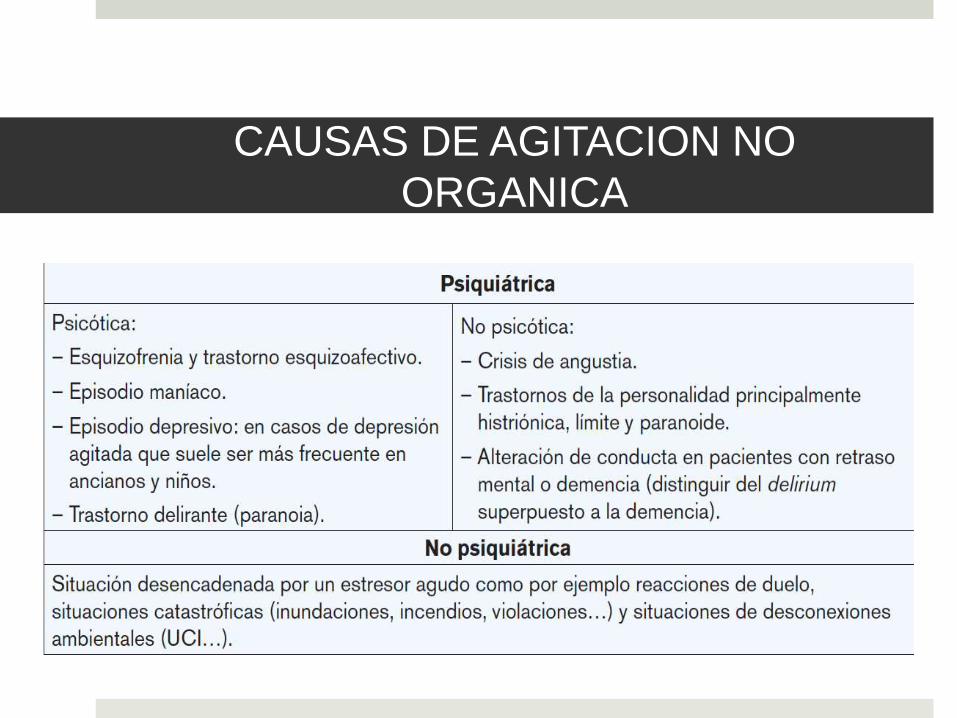
CAUSAS DE AGITACION NO
ORGANICA
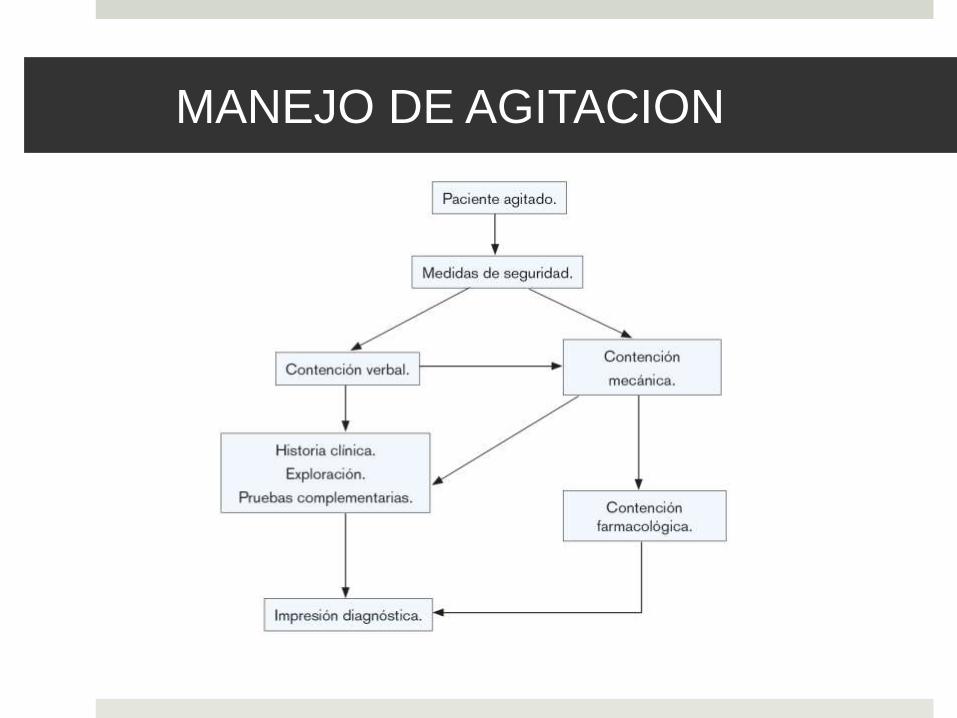
MANEJO DE AGITACION
Facilities
Should ensure routes of safe entry and exit in the event of an
emergency related to disturbed/violent behaviour.
PHYSICAL SKILS
The level of force applied must be justifiable, appropriate,
reasonable and proportionate to a specific situation and should be
applied for the minimum possible amount of time.
Every effort should be made to utilise skills and techniques that do
not use the deliberate application of pain.
The deliberate application of pain has no therapeutic value and
could only be justified for the immediate rescue of staff, service
users and/or others.
Physical intervention
Oneteam member should be responsible for protecting and supporting the head and neck, where required. The team memberwho is responsible for supporting the head and neck should takeresponsibility for leading the team through the physical interventionprocess, and for ensuring that the airway and breathing are notcompromised and that vital signs are monitored.
The management of disturbed/violent behaviour frequently involvesinterventions to which an individual does not – or cannot – consent. Itis especially important that such interventions are in accordance withbest practice.
May have legal consequences

TRATAMIENTO DE LA AGITACION
ORGANICA
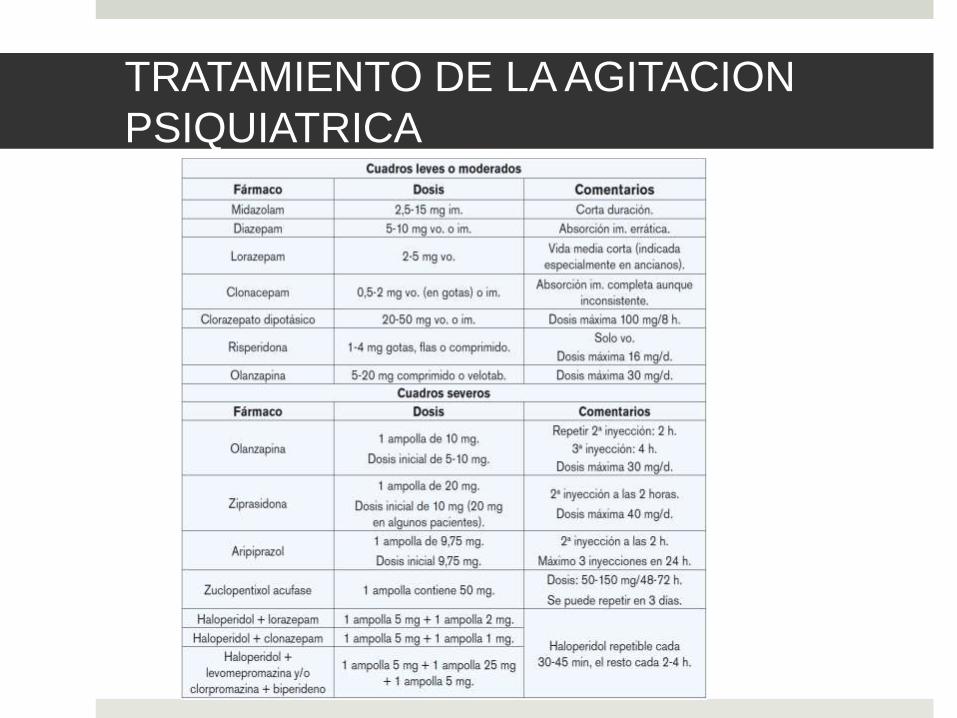
TRATAMIENTO DE LA AGITACION
PSIQUIATRICA
CUIDADOS Y TIPOS DE INTERVENCIÓN EN LAS
URGENCIAS PSIQUIÁTRICAS
Intervención verbal: la comunicación es primordial. Con las transacciones explícitas, la ganancia siempre es alta y los riesgos menores. La comunicación debe ser directa, comprensiva, persuasiva y firme.
Intervención farmacológica: referida al empleo adecuado, seguro y juicioso de los psicofármacos que, en la actualidad, constituyen recurso de privilegio técnico en el tratamiento. Así, es indispensable el conocimiento cabal de la psicofarmacología.
Intervención física: implica restricción por la fuerza humana o contención mecánica. Será necesaria en algunos casos para proteger al paciente mismo o a los demás.
Solicitud de ayuda: cuando la situación lo requiera.

COMPORTAMIENTOS AUTOLITICOS
Conjunto de ideas o actos realizados de manera voluntaria con el propósito aparente de acabar con la propia vida.
IDEACION SUICIDA
AMANAZAS O GESTOS
PARASUICIDIO
INTENTO DE SUICIDIO
SUICIDIO FRUSTRADO
SUICIDIO CONSUMADO
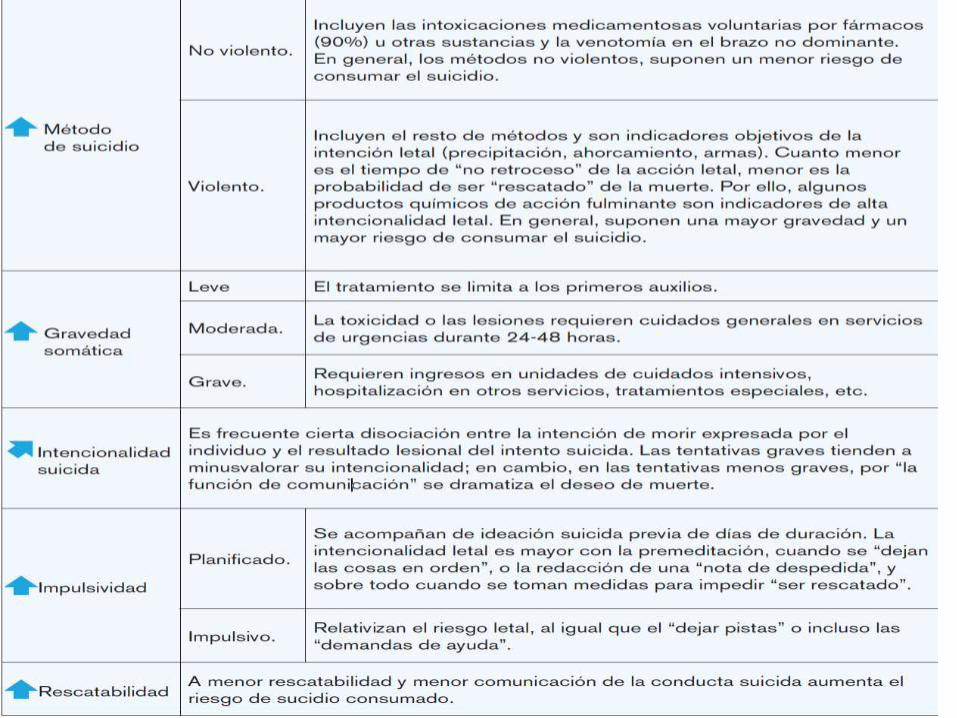
Analizar método, gravedad, rescatabilidad e impulsividad del acto suicida.
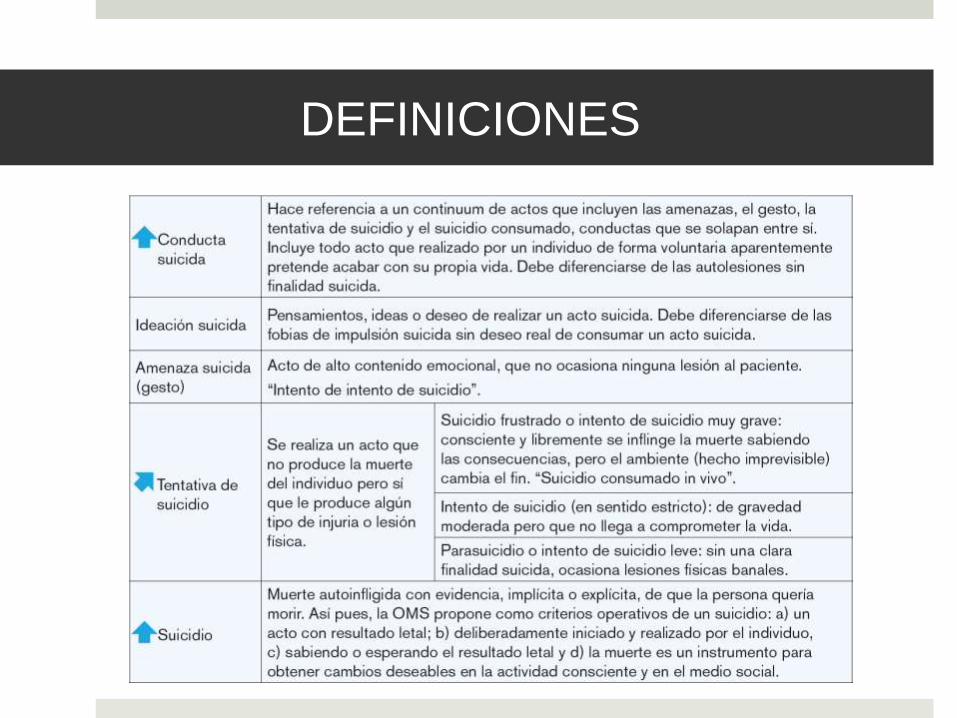
DEFINICIONES
FACTORES DE RIESGO
TRASTORNO PSIQUIATRICO MAYOR- (afectivo) más del 90%.
Hª PREVIA- X6, 3 meses después EDAD: >60 años.
SEXO: Consumado y frustrado- Hombres>mujeres 3:1(no chinas) Parasuicidio- Mujeres>hombres 3:1.5
ESTADO CIVIL: Solteros>viudos>divorciados>casados sin hijos>con hijos.
FACTORES ECONOMICOS
LIFE-EVENTS recientes.
GENETICO/HISTORIA FAMILIAR.
CAMBIOS ESTACIONALES, RELIGION…
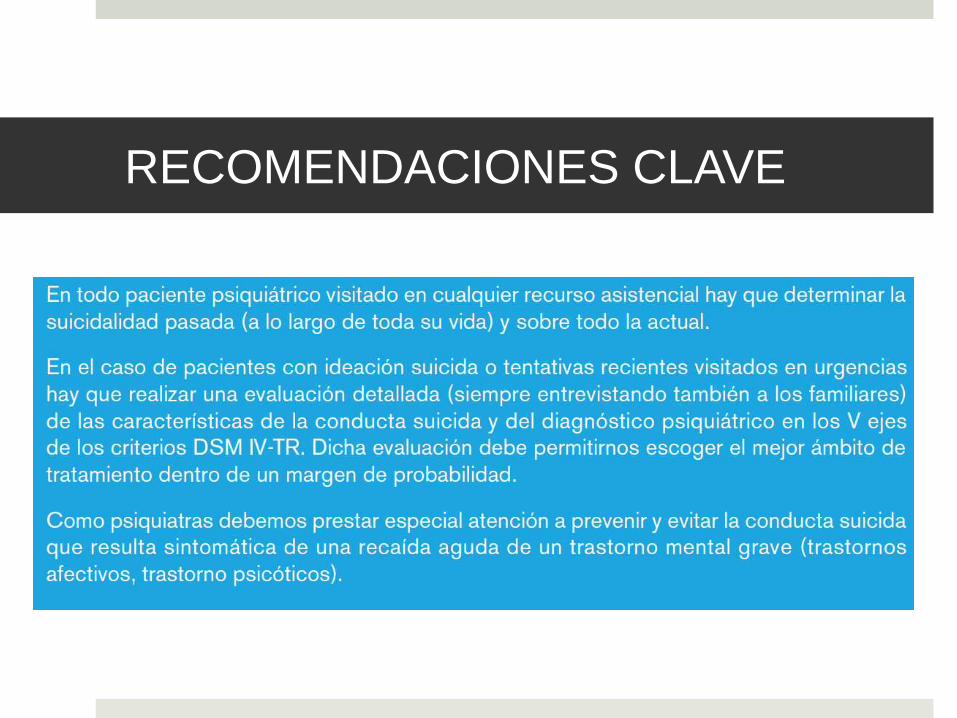
RECOMENDACIONES CLAVE
BIBLIOGRAFIA