SEMINARIO:*ACTUALIZACIÓN*EN*INFECTOLOGÍA ... 2015...Erisipelas* Mordeduras* Foliculis y*...
29
Dr. Manuel Ramírez Cardoce Infectología – UCR Hospital San Juan de Dios [email protected] SEMINARIO: ACTUALIZACIÓN EN INFECTOLOGÍA INFECCIÓN DE PIEL Y TEJIDOS BLANDOS
Transcript of SEMINARIO:*ACTUALIZACIÓN*EN*INFECTOLOGÍA ... 2015...Erisipelas* Mordeduras* Foliculis y*...

Dr. Manuel Ramírez Cardoce Infectología – UCR
Hospital San Juan de Dios
SEMINARIO: ACTUALIZACIÓN EN INFECTOLOGÍA
INFECCIÓN DE PIEL Y TEJIDOS BLANDOS

An5bió5coterapia • Estrictamente empírica hasta el descubrimiento de las bases
microbiológicas de las infecciones (siglo XIX).
• Estrategia válida ante varias en5dades clínicas infecciosas.
INTRODUCCIÓN
Mandell GL et al. Principles and prac5ce of infec5ous diseases, 7th ed. Elsevier 2010. Chapter 18 Principles of an5-‐infec5ve therapy.

AnEbióEcoterapia Empírica
Escenarios clínicos
Meningi5s
Endocardi5s
IVRS IVRI/Neumonía
Infecciones urinarias
Infecciones PTB
Infección intraabdominal

¡IMPORTANTE! Tomar muestras apropiadas para fro5s y cul5vo/PSA previo al inicio de la terapia an5microbiana.
Una vez iniciada la terapia anEmicrobiana, los culEvos suelen ser negaEvos (aunque persistan microorganismos viables en el huésped)
Mandell GL et al. Principles and prac5ce of infec5ous diseases, 7th ed. Elsevier 2010. Chapter 18 Principles of an5-‐infec5ve therapy.

Escogencia del An5microbiano
AIdenEficar al Microorganismo Infectante
B C
Tinción Gram PCR
ELISA o látex
U5lizar la estadís'ca
bacteriológica
¿Cuál sería el agente más probable en este escenario
clínico?
Mandell GL et al. Principles and prac5ce of infec5ous diseases, 7th ed. Elsevier 2010. Chapter 18 Principles of an5-‐infec5ve therapy.

Escogencia del An5microbiano
A BConocer la SuscepEbilidad
C
MIC
Mecanismos de resistencia
Par5cularmente importante en:
S. aureus y GN
Considerar variaciones regionales
Mandell GL et al. Principles and prac5ce of infec5ous diseases, 7th ed. Elsevier 2010. Chapter 18 Principles of an5-‐infec5ve therapy.

Escogencia del An5microbiano
A B CFactores del Huésped
Alergias Edad Trastornos gené5cos Embarazo Función renal y hepá5ca
Abscesos Hematomas
pH Cuerpos extraños
Si5o de Infección
Mandell GL et al. Principles and prac5ce of infec5ous diseases, 7th ed. Elsevier 2010. Chapter 18 Principles of an5-‐infec5ve therapy.

Conocer la farmacocinéEca y farmacodinamia
Uso inapropiado…deletéreo mas que beneficioso
Monoterapia vs terapia combinada: indiferencia/sinergismo/antagonismo. Espectro anEmicrobiano. Dosificación y frecuencia: agentes Eempo o concentración dependientes. Vía de administración y biodisponibilidad. Metabolismo y excreción.
DMandell GL et al. Principles and prac5ce of infec5ous diseases, 7th ed. Elsevier 2010. Chapter 18 Principles of an5-‐infec5ve therapy.

INFECCIONES DE PIEL Y TEJIDOS BLANDOS

CLAS
IFICAC
IÓN
• Amplio espectro de presentación clínica. – Complicadas:
• Por compromiso de estructuras profundas, que requieren intervenciones quirúrgicas y/o que se acompañan de comorbilidades (p.ej. inmunocompromiso).
• Infecciones por anaerobios o GN.
NO COMPLICADAS COMPLICADAS
Celuli5s Heridas traumá5cas
Erisipelas Mordeduras
Foliculi5s y furunculosis Heridas quirúrgicas
Impé5gos Pie diabé5co
Ec5mas Úlceras por presión y venosas
Abscesos simples Perianales
Necro5zantes
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.

IPTB CLASIFICACIÓN
61
RAJAN
early detection and prompt surgical interven-tion.15 Since necrotizing fasciitis is very dif-ficult to diagnose, clinicians must maintain a high level of suspicion and use the LRINEC score to trigger early surgical evaluation. Sur-gical exploration is the only way to definitive-ly diagnose necrotizing fasciitis.
Blood cultures in some casesBlood cultures have a low yield and are usually not cost-effective, but they should be obtained in patients who have lymphedema, immune deficiency, fever, pain out of proportion to the findings on examination, tachycardia, or hy-potension, as blood cultures are more likely to be positive in more serious infections and can help guide antimicrobial therapy. Blood cul-tures are also recommended in patients with infections involving specific anatomic sites, such as the mouth and eyes.19
Aspiration, swabs, incision and drainageFluid aspirated from abscesses and swabs of debrided ulcerated wounds should be sent for Gram stain and culture. Gram stain and culture have widely varying yields, from less than 5% to 40%, depending on the source and technique.19 Cultures were not routinely obtained before MRSA emerged, but knowing antimicrobial susceptibility is now important to guide antibiotic therapy. Unfortunately, in cellulitis, swabs and aspi-rates of the leading edge have a low yield of around 10%.25 One prospective study of 25 hospitalized patients did report a higher yield of positive cultures in patients with fe-ver or underlying disease,26 so aspirates may be used in selected cases. In small studies, the yield of punch biopsies was slightly bet-ter than that of needle aspirates and was as high as 20% to 30%.27
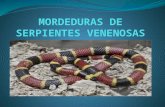
FIGURE 1. Depth of involvement in skin and soft-tissue infections..
Epidermis
Dermis
Superficial fascia
Subcutaneous tissue
Deep fascia
Muscle
Erysipelas Impetigo Folliculitis
Ecthyma Furunculosis Carbunculosis
Cellulitis
Necrotizing fasciitis
Myonecrosis (clostridial and nonclostridial)
Sabitha R. Skin and sol-‐5ssue infec5ons: classifying and trea5ng a spectrum. Clev Clin J Med 2012;79(1):57-‐66.
Erisipelas Impé5go Foliculi5s
Ec5ma Furunculosis Carbunculosis
Celuli5s
Fascii5s necro5zante
Mionecrosis

IPTB MICROBIOLOGÍA Y SUSCEPTIBILIDAD
• La microbiología es dependiente de varios factores: – Huésped. – Ambiente (comunitaria vs. ACS). – Mecanismo de trauma. – Duración y severidad de la enfermedad.
• En general, estreptococos y S. aureus originan la gran mayoría de IPTB no complicadas y complicadas. – Excepción: mordeduras.
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.

• En un estudio mul5céntrico y prospec5vo de IPTB purulenta:
– MRSA fue aislado en 15 a 74% de casos. • 61% de abscesos. • 53% de heridas infectadas. • 47% de celuli5s purulentas.
– MSSA fue aislado en: • 14% de abscesos. • 21% de heridas infectadas. • 34% de celuli5s purulentas.
– Streptococcus spp. fue aislado en: • 7% de abscesos. • 9% de heridas infectadas. • 13% de celuli5s purulentas.
• L a s mo r d edu r a s s u e l e n s e r infecciones mixtas (aerobios y anaerobios).
• De animales: – Pasteurella spp.:
• 50% en perros (P. canis, 26%). • 75% en gatos (P. multocida, 54%).
– Streptococcus spp. en 46% (ambas). – MSSA en 20% (perros) y 4% (gatos). – Anaerobios: Fusobacterium spp.
Bacteroides spp. Prevotella spp.
• De humanos: – Streptococcus spp. en 84%. – S. aureus en 30%. – Eikenella corrodens en 30%. – Prevotella spp. en 36%. – Fusobacterium spp. en 34%.
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.
Moran GJ et al. MRSA infec5ons among pa5ents in the emergency department. N Engl J Med 2006;355(7):666-‐74.

MRSA
Cambio epidemiológico más
significa5vo
Alta prevalencia aún en ausencia de FR “clásicos” clínicos y epidemiológicos
Algunas cepas (MRSA-‐CA) se
asocian a mayor virulencia y
producción de toxinas (p.ej. PVL)
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.

IPTB MICROBIOLOGÍA Y SUSCEPTIBILIDAD
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.
adequate serum levels with respect to the minimum inhibitory concentration(MIC) and maximizing concentration-dependent killing [74]. Although thisrecommendation seems logical and is made to prevent under-dosing, itshould be noted that there are no prospective human trials demonstratingthe superiority of a two double-strength, compared with a one double-strength, regimen. TMP/SMX has been shown to have adequate penetrationinto experimentally made human skin blisters [75,76]; however, the samemay not apply to abscesses even with an increased dosage regimen. Mostimportantly, the issue of penetration into the abscess cavity may bea moot point if they are treated with adequate incision and drainage.Dosage increases may also lead to increased side-effects and potentiallylower patient compliance with the advocated regimen.
Rifampin, a highly active agent against CA-MRSA, is commonly used incombination with TMP/SMX or doxycycline. It should not be used alonebecause of its rapid tendency to select resistant strains [77]. The SanfordGuide recommends the addition of rifampin to TMP/SMX for patientswho have an abscess associated with fever, those with large or multipleabscesses, and in severe infections [74]. The only supporting data are froma retrospective study of CA-MRSA SSTIs, in which clinical resolutionwas achieved in all of six patients treated with a combination of TMP/SMX and rifampin, but in only 6 of 12 patients treated with double-strengthTMP/SMX [78]. Rifampin has numerous drug-drug interactions and an
Table 5In vitro susceptibility patterns of community-associated methicillin-resistant Staphylococcusaureus to a variety of antimicrobial agents
Antibiotic Moran et al [12] Miller et al [21] Naimi et al [23] Ruhe et al [60]
TMP/SMX 100% (n ¼ 217) 100% (n ¼ 120) 95% (n ¼ 106) 99% (n ¼ 322)Rifampin 100% (n ¼ 186) 100% (n ¼ 120) 96% (n ¼ 106) 99% (n ¼ 318)Clindamycin 95% (n ¼ 226)a 95% (n ¼ 102) 83% (n ¼ 106) 98% (n ¼ 482)b
Tetracycline 92% (n ¼ 226) 81% (n ¼ 120) 92% (n ¼ 106) 93% (n ¼ 455)Gentamicin NT 100% (n ¼ 120) 94% (n ¼ 106) 100% (n ¼ 320)Ciprofloxacin 60% (n ¼ 176) 15% (n ¼ 101) 79% (n ¼ 106) 73% (n ¼ 354)Erythromycin 6% (n ¼ 226) 7% (n ¼ 120) 44% (n ¼ 106) 5% (n ¼ 23)Vancomycin NT 100% (n ¼ 120) 100% (n ¼ 106) 100% (n ¼ 492)Linezolid NT 100% (n ¼ 19) NT NT
Susceptibility patterns are dynamic and may vary markedly by geographic regions.Physicians’ familiarity with the prevalence and susceptibility patterns of CA-MRSA in theircommunity is a crucial element in the management of CA-MRSA infections.
Abbreviations: NT, Not tested; TMP/SMX, Trimethoprim/sulfamethoxazole.a Four (approximately 2%; n ¼ 226) MRSA isolates had inducible clindamycin resistance
detected by an antimicrobial susceptibility D-zone disk diffusion test.b Two (3%; n ¼ 59) MRSA isolates had inducible clindamycin resistance detected by an
antimicrobial susceptibility D-zone disk diffusion test.Modified from Abrahamian FM, Snyder EW. Community-associated methicillin-resistant
Staphylococcus aureus: incidence, clinical presentation, and treatment decisions. Curr InfectDis Rep 2007;9(5):391–7; with permission.
104 ABRAHAMIAN et al

0 10 20 30 40 50 60 70 80 90
100
1995 (101 aislamientos) 2004 (956 aislamientos)
Vancomicina Oxacilina Ciprofloxacina TMP/SMX Gentamicina
Histórico de susceptibilidad de S. aureus (Hospital México)
2006-‐08 (2410 aislamientos)
?
72%
48%
34%
87%
74% 66%
72%
87% 88%
74% 79%
69%
Cortesía Dr. Villalobo
s Vinda
s, Servicio de
Infectología Hosp. M
éxico

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
OXA CIP CLI
Susceptibilidad 2410 cepas de S. aureus, Hospital México
LEV TET GEN RIF MOX VAN LZD
66%
SENSIBLE
RESISTENTE
34% 33% 34% 31% 27% 12% 11% 8% 51%
ERI
Cortesía Dr. Villalobos Vindas, Servicio de Infectología Hosp. México
SXT

0
10
20
30
40
50
60
70
80
90
100
1995 2000 2004 2009 2014
% MRSA
Cortesía Lab. Microbiología HSJD y Dr. Boza Cordero
Histórico de susceptibilidad de S. aureus (HSJD)

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100% *2014: Todos los culEvos, de hospitalizados, urgencias y consulta externa.
Susceptibilidad 1292 cepas de S. aureus, HSJD
68% Oxa-‐R
32% R

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CIP
CLI
ERY
GEN
LEV
LZD
MIN
MOX
OXA
Q/D
RIF
TEC
TET
SXT
VAN
2012
2013
*Todos los culEvos de consulta externa.
Susceptibilidad 144 cepas de S. aureus, HSJD
65% Oxa-‐R
20-‐30% R

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CIP
CLI
ERY
GEN
LEV
LZD
MIN
MOX
OXA
Q/D
RIF
TEC
TET
SXT
VAN
2012
2013
2014
*Todos los culEvos de urgencias.
Susceptibilidad 462 cepas de S. aureus, HSJD
65-‐75% Oxa-‐R
20% R

Susceptibilidad 163 cepas de S. aureus aisladas del Servicio de Urgencias, Hospital México
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
OXA CLI SXT CIP TET LEV RIF MOX VAN LZD
53%
SENSIBLE
RESISTENTE
24% 13% 13% 12% 11% 6% 6% 4% 35%
ERI GEN
Cortesía Dr. Villalobos Vindas, Servicio de Infectología Hosp. México

% R % S
Oxacilina Clindamicina Levofloxacina TMP/SMX
% R
% S % R
% S % R
% S
68 79 74 74 74
32 21 26 26 26
Año
2007 2008 2009 2010 Total
0 7 4 0 3
100 93 96 100 97
5 4 0 0 2
95 96 100 100 98
0 0 0 0 0
100 100 100 100 100
(n=22)
(n=28)
(n=27)
(n=77)
Cortesía Dr. Villalobos Vindas, Servicio de Infectología Hosp. México

IPTB ABORDAJE Y MANEJO
• Abscesos no complicados (incluso por MRSA): – Incisión y drenaje solamente
(tasa de curación 85-‐90%). • P r i n c i pa l c au sa de f a l l a
t e r a p é u 5 c a : d r e n a j e inadecuado.
• Cul5vos de heridas, sólo en: – Admisión hospitalaria. – Infecciones complicadas. – Inmunocompromiso. – Enfermedad severa. – Recurrencia o refractariedad.
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.
• Se recomienda el uso de t e r a p i a a n 5m i c r o b i a n a (asociada al manejo quirúrgico de incisión y drenaje) en aquellos abscesos cutáneos:
– Complicados. – Múl5ples. – Con gangrena. – Por mordeduras. – En inmunocomprome5dos. – Con celuli5s extensa. – Con toxicidad sistémica.

IPTB TERAPIA ANTIMICROBIANA TIPO ESCENARIO AGENTES
ImpéEgo
Ambulatorio x 5-‐10 d
Mupirocina al 2% ungüento tópico
CeluliEs No purulenta
Cefalexina VO 500 mg qid +/-‐ TMP-‐SMX 160/800 mg VO 1-‐2 tab bid
CeluliEs Purulenta
TMP-‐SMX 160/800 mg VO 1-‐2 tab bid ó Clindamicina VO 300 mg qid ó Doxiciclina VO 100 mg bid
Absceso con celuliEs leve Incisión y drenaje
Pie diabéEco
Clindamicina VO 300 mg qid + Ciprofloxacina VO 500 bid ó Amox-‐clav 875/125 mg VO 1 tab bid +/-‐ TMP-‐SMX 160/800 mg VO 1-‐2 tab bid
Mordeduras
Amox-‐clav 875/125 mg VO 1 tab bid ó Clindamicina VO 300 mg qid + Ciprofloxacina VO 500 mg bid
Abrahamian FM et al. Management of skin and sol-‐5ssue infec5ons in the emergency department. Infect Dis Clin N Am 2008(22);89-‐116.

M A J O R A R T I C L E
Clinical Trial: Comparative Effectiveness ofCephalexin Plus Trimethoprim-Sulfamethoxazole Versus Cephalexin Alone forTreatment of Uncomplicated Cellulitis: ARandomized Controlled Trial
Daniel J. Pallin,1,2 William D. Binder,3 Matthew B. Allen,1,4 Molly Lederman,1,5 Siddharth Parmar,1 Michael R. Filbin,3
David C. Hooper,6 and Carlos A. Camargo Jr31Department of Emergency Medicine, Brigham and Women’s Hospital, 2Division of Emergency Medicine, Boston Children’s Hospital, and 3Department ofEmergency Medicine, Massachusetts General Hospital, Boston; 4Perelman School of Medicine at the University of Pennsylvania, Philadelphia;5Department of Pediatrics, and 6Division of Infectious Diseases, Department of Medicine, Massachusetts General Hospital, Boston
(See the Editorial Commentary by Chambers on pages 1763–4.)
Background. Community-associated methicillin-resistant S. aureus (CA-MRSA) is the most common organismisolated from purulent skin infections. Antibiotics are usually not beneficial for skin abscess, and national guidelinesdo not recommend CA-MRSA coverage for cellulitis, except purulent cellulitis, which is uncommon. Despite this,antibiotics targeting CA-MRSA are prescribed commonly and increasingly for skin infections, perhaps due, in part,to lack of experimental evidence among cellulitis patients. We test the hypothesis that antibiotics targeting CA-MRSA are beneficial in the treatment of cellulitis.
Methods. We performed a randomized, multicenter, double-blind, placebo-controlled trial from 2007 to 2011.We enrolled patients with cellulitis, no abscesses, symptoms for <1 week, and no diabetes, immunosuppression, pe-ripheral vascular disease, or hospitalization (clinicaltrials.gov NCT00676130). All participants received cephalexin.Additionally, each was randomized to trimethoprim-sulfamethoxazole or placebo. We provided 14 days of antibiot-ics and instructed participants to continue therapy for ≥1 week, then stop 3 days after they felt the infection to becured. Our main outcome measure was the risk difference for treatment success, determined in person at 2 weeks,with telephone and medical record confirmation at 1 month.
Results. We enrolled 153 participants, and 146 had outcome data for intent-to-treat analysis. Median age was29, range 3–74. Of intervention participants, 62/73 (85%) were cured versus 60/73 controls (82%), a risk differenceof 2.7% (95% confidence interval, −9.3% to 15%; P = .66). No covariates predicted treatment response, includingnasal MRSA colonization and purulence at enrollment.
Conclusions. Among patients diagnosed with cellulitis without abscess, the addition of trimethoprim-sulfame-thoxazole to cephalexin did not improve outcomes overall or by subgroup.
Clinical Trials Registration. NCT00676130.
Keywords. cellulitis; community-associated methicillin-resistant Staphylococcus aureus; comparative effectiveness;trimethoprim-sulfamethoxazole; cephalexin.
Community-associated methicillin-resistant Staphylo-coccus aureus (CA-MRSA) is the most common
identifiable cause of purulent skin infections, that is,abscess and purulent cellulitis [1, 2]. The frequency of
Received 5 December 2012; accepted 22 January 2013; electronically published1 March 2013.
Correspondence: Daniel J. Pallin, 75 Francis St, Neville House 304-D, Boston,MA 02115 ([email protected]).
Clinical Infectious Diseases 2013;56(12):1754–62© The Author 2013. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/cit122
1754 • CID 2013:56 (15 June) • Pallin et al
at IDSA
mem
ber on July 11, 2013http://cid.oxfordjournals.org/
Dow
nloaded from
M A J O R A R T I C L E
Clinical Trial: Comparative Effectiveness ofCephalexin Plus Trimethoprim-Sulfamethoxazole Versus Cephalexin Alone forTreatment of Uncomplicated Cellulitis: ARandomized Controlled Trial
Daniel J. Pallin,1,2 William D. Binder,3 Matthew B. Allen,1,4 Molly Lederman,1,5 Siddharth Parmar,1 Michael R. Filbin,3
David C. Hooper,6 and Carlos A. Camargo Jr31Department of Emergency Medicine, Brigham and Women’s Hospital, 2Division of Emergency Medicine, Boston Children’s Hospital, and 3Department ofEmergency Medicine, Massachusetts General Hospital, Boston; 4Perelman School of Medicine at the University of Pennsylvania, Philadelphia;5Department of Pediatrics, and 6Division of Infectious Diseases, Department of Medicine, Massachusetts General Hospital, Boston
(See the Editorial Commentary by Chambers on pages 1763–4.)
Background. Community-associated methicillin-resistant S. aureus (CA-MRSA) is the most common organismisolated from purulent skin infections. Antibiotics are usually not beneficial for skin abscess, and national guidelinesdo not recommend CA-MRSA coverage for cellulitis, except purulent cellulitis, which is uncommon. Despite this,antibiotics targeting CA-MRSA are prescribed commonly and increasingly for skin infections, perhaps due, in part,to lack of experimental evidence among cellulitis patients. We test the hypothesis that antibiotics targeting CA-MRSA are beneficial in the treatment of cellulitis.
Methods. We performed a randomized, multicenter, double-blind, placebo-controlled trial from 2007 to 2011.We enrolled patients with cellulitis, no abscesses, symptoms for <1 week, and no diabetes, immunosuppression, pe-ripheral vascular disease, or hospitalization (clinicaltrials.gov NCT00676130). All participants received cephalexin.Additionally, each was randomized to trimethoprim-sulfamethoxazole or placebo. We provided 14 days of antibiot-ics and instructed participants to continue therapy for ≥1 week, then stop 3 days after they felt the infection to becured. Our main outcome measure was the risk difference for treatment success, determined in person at 2 weeks,with telephone and medical record confirmation at 1 month.
Results. We enrolled 153 participants, and 146 had outcome data for intent-to-treat analysis. Median age was29, range 3–74. Of intervention participants, 62/73 (85%) were cured versus 60/73 controls (82%), a risk differenceof 2.7% (95% confidence interval, −9.3% to 15%; P = .66). No covariates predicted treatment response, includingnasal MRSA colonization and purulence at enrollment.
Conclusions. Among patients diagnosed with cellulitis without abscess, the addition of trimethoprim-sulfame-thoxazole to cephalexin did not improve outcomes overall or by subgroup.
Clinical Trials Registration. NCT00676130.
Keywords. cellulitis; community-associated methicillin-resistant Staphylococcus aureus; comparative effectiveness;trimethoprim-sulfamethoxazole; cephalexin.
Community-associated methicillin-resistant Staphylo-coccus aureus (CA-MRSA) is the most common
identifiable cause of purulent skin infections, that is,abscess and purulent cellulitis [1, 2]. The frequency of
Received 5 December 2012; accepted 22 January 2013; electronically published1 March 2013.
Correspondence: Daniel J. Pallin, 75 Francis St, Neville House 304-D, Boston,MA 02115 ([email protected]).
Clinical Infectious Diseases 2013;56(12):1754–62© The Author 2013. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/cit122
1754 • CID 2013:56 (15 June) • Pallin et al
at IDSA
mem
ber on July 11, 2013http://cid.oxfordjournals.org/
Dow
nloaded from
M A J O R A R T I C L E
Clinical Trial: Comparative Effectiveness ofCephalexin Plus Trimethoprim-Sulfamethoxazole Versus Cephalexin Alone forTreatment of Uncomplicated Cellulitis: ARandomized Controlled Trial
Daniel J. Pallin,1,2 William D. Binder,3 Matthew B. Allen,1,4 Molly Lederman,1,5 Siddharth Parmar,1 Michael R. Filbin,3
David C. Hooper,6 and Carlos A. Camargo Jr31Department of Emergency Medicine, Brigham and Women’s Hospital, 2Division of Emergency Medicine, Boston Children’s Hospital, and 3Department ofEmergency Medicine, Massachusetts General Hospital, Boston; 4Perelman School of Medicine at the University of Pennsylvania, Philadelphia;5Department of Pediatrics, and 6Division of Infectious Diseases, Department of Medicine, Massachusetts General Hospital, Boston
(See the Editorial Commentary by Chambers on pages 1763–4.)
Background. Community-associated methicillin-resistant S. aureus (CA-MRSA) is the most common organismisolated from purulent skin infections. Antibiotics are usually not beneficial for skin abscess, and national guidelinesdo not recommend CA-MRSA coverage for cellulitis, except purulent cellulitis, which is uncommon. Despite this,antibiotics targeting CA-MRSA are prescribed commonly and increasingly for skin infections, perhaps due, in part,to lack of experimental evidence among cellulitis patients. We test the hypothesis that antibiotics targeting CA-MRSA are beneficial in the treatment of cellulitis.
Methods. We performed a randomized, multicenter, double-blind, placebo-controlled trial from 2007 to 2011.We enrolled patients with cellulitis, no abscesses, symptoms for <1 week, and no diabetes, immunosuppression, pe-ripheral vascular disease, or hospitalization (clinicaltrials.gov NCT00676130). All participants received cephalexin.Additionally, each was randomized to trimethoprim-sulfamethoxazole or placebo. We provided 14 days of antibiot-ics and instructed participants to continue therapy for ≥1 week, then stop 3 days after they felt the infection to becured. Our main outcome measure was the risk difference for treatment success, determined in person at 2 weeks,with telephone and medical record confirmation at 1 month.
Results. We enrolled 153 participants, and 146 had outcome data for intent-to-treat analysis. Median age was29, range 3–74. Of intervention participants, 62/73 (85%) were cured versus 60/73 controls (82%), a risk differenceof 2.7% (95% confidence interval, −9.3% to 15%; P = .66). No covariates predicted treatment response, includingnasal MRSA colonization and purulence at enrollment.
Conclusions. Among patients diagnosed with cellulitis without abscess, the addition of trimethoprim-sulfame-thoxazole to cephalexin did not improve outcomes overall or by subgroup.
Clinical Trials Registration. NCT00676130.
Keywords. cellulitis; community-associated methicillin-resistant Staphylococcus aureus; comparative effectiveness;trimethoprim-sulfamethoxazole; cephalexin.
Community-associated methicillin-resistant Staphylo-coccus aureus (CA-MRSA) is the most common
identifiable cause of purulent skin infections, that is,abscess and purulent cellulitis [1, 2]. The frequency of
Received 5 December 2012; accepted 22 January 2013; electronically published1 March 2013.
Correspondence: Daniel J. Pallin, 75 Francis St, Neville House 304-D, Boston,MA 02115 ([email protected]).
Clinical Infectious Diseases 2013;56(12):1754–62© The Author 2013. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/cid/cit122
1754 • CID 2013:56 (15 June) • Pallin et al
at IDSA
mem
ber on July 11, 2013http://cid.oxfordjournals.org/
Dow
nloaded from
that antibiotics be used in such settings was based solely onexpert opinion [7].
The present study is typical of pragmatic trials [11]. Onefeature of comparative effectiveness research is that its pragmat-ic approach can produce results that contradict what would belogically predictable from biological knowledge. We are in themidst of an epidemic of skin infections caused by CA-MRSA,but antibiotics targeting this organism have not been foundhelpful in pragmatic studies.
LimitationsThe chief limitation of our study is intrinsic to most cases ofcellulitis: there is no objective way to make an etiologic diagno-sis. Our study was also limited to outpatients, including, forexample, no patients with cellulitis complicating lymphede-ma, for whom blood cultures and intravenous antibiotics arerecommended [10]. Our study provides no direct informationabout the management of such complicated skin infections inhospitalized patients, though it does provide support for thegeneral concept that CA-MRSA is not important in cellulitis.Treatment of patients with life-threatening infections such asnecrotizing fasciitis is not informed by this study. In this context,it bears mentioning that we avoided the common term “skin andsoft-tissue infections,” in favor of simply, “skin infections.” “Softtissue infections,” which are not “skin infections,” include suchsyndromes as pyomyositis and fasciitis and are rare. This studydoes not inform the treatment of such conditions.
We excluded diabetics. We are aware of no evidence that dia-betics are at higher risk for CA-MRSA–associated skin infec-tions, and thus our results may be generalizable to them.Most episodes of cellulitis in diabetics are treated as in nondia-betics [7]. While diabetic foot infections do require broadercoverage, whether they require coverage for CA-MRSA remainsunknown [10]. We assessed MRSA colonization nasally. Only67% of MRSA-colonized skin infection patients have positivenasal swabs, with other common sites of colonization being theaxillae, groin, and perineum [30]. Had we also swabbed theaxillae and groin, we might have observed an interaction of col-onization and treatment response. While CA-MRSA is almostuniversally susceptible to trimethoprim-sulfamethoxazole invitro, it is possible that other agents, such as clindamycin andtetracyclines, might be more effective in vivo. Using diaries,participants indicated whether they took all of their medica-tions each day until self-reported cure, and this is analyzedabove. However, we did not record the total duration of therapy(ie, we cannot distinguish stopped therapy from a day of partialadherence). This reflects the study’s nature as an effectivenessstudy, rather than an efficacy study, in that the practicing clini-cian controls only the prescription, not subsequent adherence.We did not record lesion area, which would have required
photography and parsing of each lesion into measurable geo-metric shapes.
Though it achieved its target, our study was modest in size.This was not an equivalence study, and when we designed thetrial, we expected to find a benefit from the intervention. Thevalue of the result is that it is the first evidentiary support forthe relevant national guidelines [7]. We know of only 2 otherrelevant trials: NCT00729937 and NCT00730028. If the IDSAguidelines are correct, those trials and meta-analyses combin-ing their results with ours will narrow the confidence interval.However, those studies have posted no results on ClinicalTrials.gov (as of 30 November 2012), and thus we do not know whenthey will contribute relevant data from cellulitis patients or howlarge their samples of cellulitis patients will be.
As clinical trial evidence accumulates, antibiotic prescribingfor skin infection patients might even be a reasonable target forantibiotic stewardship interventions, especially given howcommon skin infections are. Regarding abscesses, the evidencemay already be sufficient to consider use of antibiotics for un-complicated abscesses as a good target for antibiotic steward-ship efforts. Regarding cellulitis, we feel that the present trialalone is not sufficient to motivate a stewardship campaign forcellulitis. If the results of the other studies mentioned aboveecho our own findings, reduction in the use of antibiotics thattarget CA-MRSA for uncomplicated cellulitis may become areasonable target.
CONCLUSIONS
In the first study to provide experimental support for IDSA rec-ommendations against antibiotics targeting CA-MRSA for mostcases of cellulitis, we found that adding trimethoprim-sulfame-thoxazole to cephalexin conferred no benefit relative to therapywith cephalexin alone in the outpatient treatment of cellulitis.Concerns about polypharmacy and antibiotic stewardship maylead us to rely on beta lactams when treating uncomplicated cel-lulitis.
Notes
Acknowledgments. We thank Patricia Kelly, RPh, of Brigham andWomen’s Hospital, for her invaluable help in developing placebos andplanning and executing the study. We are grateful to Shannon Manzi, RPh,of Boston Children’s Hospital, for her help in implementation at that site.John T. Nagurney, MD, provided invaluable support, as did Blair Parry,both of Massachusetts General Hospital. We acknowledge gratefully thework of many research assistants, attending physicians, resident physicians,and nurses who made the study happen. None of these contributors werecompensated for their help. We are very grateful to the participants.Financial support. This work was supported by a grant from the
Eleanor and Miles Shore Fellowship Program of the Brigham and Women’sHospital Department of Emergency Medicine; by the Milton Fund ofHarvard University, Boston, MA; and by seed funding from the Depart-ment of Emergency Medicine of Massachusetts General Hospital.Potential conflicts of interest. All authors: No reported conflicts.
RCT of CA-MRSACoverage in Cellulitis • CID 2013:56 (15 June) • 1761
at IDSA
mem
ber on July 11, 2013http://cid.oxfordjournals.org/
Dow
nloaded from

The new england journal of medicine
n engl j med 372;12 nejm.org March 19, 2015 1093
established in 1812 March 19, 2015 vol. 372 no. 12
From the Los Angeles Biomedical Research Institute (L.G.M., S.J.E.) and Division of Infectious Diseases, Harbor–UCLA (Uni-versity of California, Los Angeles) Medi-cal Center (L.G.M., S.J.E.), Torrance, Da-vid Geffen School of Medicine at UCLA, Los Angeles (L.G.M., S.J.E.), Division of Plastic and Reconstructive Surgery, Uni-versity of California, San Francisco (UCSF) (D.Y.), and Division of Infectious Diseas-es, San Francisco General Hospital and UCSF (M.D.D., H.F.C.), San Francisco — all in California; Division of Pediatric In-fectious Diseases, University of Chicago, Chicago (R.S.D.); Division of Pediatric Infectious Diseases, Vanderbilt Universi-ty, Nashville (C.B.C.); the EMMES Corpo-ration, Rockville, MD (S.P.); and Cota En-terprises, Meriden, KS (R.J.H.). Address reprint requests to Dr. Miller at the Divi-sion of Infectious Diseases, Harbor–UCLA Medical Center, 1000 W. Carson St., Box 466, Torrance, CA 90509, or at lgmiller@ ucla . edu.
*A list of additional members of the Divi-sion of Microbiology and Infectious Dis-eases (DMID) 07-0051 Team is provided in the Supplementary Appendix, available at NEJM.org.
N Engl J Med 2015;372:1093-103.DOI: 10.1056/NEJMoa1403789Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDSkin and skin-structure infections are common in ambulatory settings. However, the efficacy of various antibiotic regimens in the era of community-acquired methicillin-resistant Staphylococcus aureus (MRSA) is unclear.
METHODSWe enrolled outpatients with uncomplicated skin infections who had cellulitis, ab-scesses larger than 5 cm in diameter (smaller for younger children), or both. Patients were enrolled at four study sites. All abscesses underwent incision and drainage. Patients were randomly assigned in a 1:1 ratio to receive either clindamycin or trimethoprim–sulfamethoxazole (TMP-SMX) for 10 days. Patients and investigators were unaware of the treatment assignments and microbiologic test results. The pri-mary outcome was clinical cure 7 to 10 days after the end of treatment.
RESULTSA total of 524 patients were enrolled (264 in the clindamycin group and 260 in the TMP-SMX group), including 155 children (29.6%). One hundred sixty patients (30.5%) had an abscess, 280 (53.4%) had cellulitis, and 82 (15.6%) had mixed infection, de-fined as at least one abscess lesion and one cellulitis lesion. S. aureus was isolated from the lesions of 217 patients (41.4%); the isolates in 167 (77.0%) of these patients were MRSA. The proportion of patients cured was similar in the two treatment groups in the intention-to-treat population (80.3% in the clindamycin group and 77.7% in the TMP-SMX group; difference, −2.6 percentage points; 95% confidence interval [CI], −10.2 to 4.9; P = 0.52) and in the populations of patients who could be evaluated (466 patients; 89.5% in the clindamycin group and 88.2% in the TMP-SMX group; difference, −1.2 percentage points; 95% CI, −7.6 to 5.1; P = 0.77). Cure rates did not differ significantly between the two treatments in the subgroups of children, adults, and patients with abscess versus cellulitis. The proportion of patients with adverse events was similar in the two groups.
CONCLUSIONSWe found no significant difference between clindamycin and TMP-SMX, with respect to either efficacy or side-effect profile, for the treatment of uncomplicated skin infec-tions, including both cellulitis and abscesses. (Funded by the National Institute of Allergy and Infectious Diseases and the National Center for Advancing Translational Sciences, National Institutes of Health; ClinicalTrials.gov number, NCT00730028.)
a bs tr ac t
Clindamycin versus Trimethoprim–Sulfamethoxazole for Uncomplicated Skin Infections
Loren G. Miller, M.D., M.P.H., Robert S. Daum, M.D., C.M., C. Buddy Creech, M.D., M.P.H., David Young, M.D., Michele D. Downing, R.N., M.S.N., Samantha J. Eells, M.P.H., Stephanie Pettibone, B.S., Rebecca J. Hoagland, M.S., and Henry F. Chambers, M.D., for the DMID 07-0051 Team*
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on May 14, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
n engl j med 372;12 nejm.org March 19, 2015 1093
established in 1812 March 19, 2015 vol. 372 no. 12
From the Los Angeles Biomedical Research Institute (L.G.M., S.J.E.) and Division of Infectious Diseases, Harbor–UCLA (Uni-versity of California, Los Angeles) Medi-cal Center (L.G.M., S.J.E.), Torrance, Da-vid Geffen School of Medicine at UCLA, Los Angeles (L.G.M., S.J.E.), Division of Plastic and Reconstructive Surgery, Uni-versity of California, San Francisco (UCSF) (D.Y.), and Division of Infectious Diseas-es, San Francisco General Hospital and UCSF (M.D.D., H.F.C.), San Francisco — all in California; Division of Pediatric In-fectious Diseases, University of Chicago, Chicago (R.S.D.); Division of Pediatric Infectious Diseases, Vanderbilt Universi-ty, Nashville (C.B.C.); the EMMES Corpo-ration, Rockville, MD (S.P.); and Cota En-terprises, Meriden, KS (R.J.H.). Address reprint requests to Dr. Miller at the Divi-sion of Infectious Diseases, Harbor–UCLA Medical Center, 1000 W. Carson St., Box 466, Torrance, CA 90509, or at lgmiller@ ucla . edu.
*A list of additional members of the Divi-sion of Microbiology and Infectious Dis-eases (DMID) 07-0051 Team is provided in the Supplementary Appendix, available at NEJM.org.
N Engl J Med 2015;372:1093-103.DOI: 10.1056/NEJMoa1403789Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDSkin and skin-structure infections are common in ambulatory settings. However, the efficacy of various antibiotic regimens in the era of community-acquired methicillin-resistant Staphylococcus aureus (MRSA) is unclear.
METHODSWe enrolled outpatients with uncomplicated skin infections who had cellulitis, ab-scesses larger than 5 cm in diameter (smaller for younger children), or both. Patients were enrolled at four study sites. All abscesses underwent incision and drainage. Patients were randomly assigned in a 1:1 ratio to receive either clindamycin or trimethoprim–sulfamethoxazole (TMP-SMX) for 10 days. Patients and investigators were unaware of the treatment assignments and microbiologic test results. The pri-mary outcome was clinical cure 7 to 10 days after the end of treatment.
RESULTSA total of 524 patients were enrolled (264 in the clindamycin group and 260 in the TMP-SMX group), including 155 children (29.6%). One hundred sixty patients (30.5%) had an abscess, 280 (53.4%) had cellulitis, and 82 (15.6%) had mixed infection, de-fined as at least one abscess lesion and one cellulitis lesion. S. aureus was isolated from the lesions of 217 patients (41.4%); the isolates in 167 (77.0%) of these patients were MRSA. The proportion of patients cured was similar in the two treatment groups in the intention-to-treat population (80.3% in the clindamycin group and 77.7% in the TMP-SMX group; difference, −2.6 percentage points; 95% confidence interval [CI], −10.2 to 4.9; P = 0.52) and in the populations of patients who could be evaluated (466 patients; 89.5% in the clindamycin group and 88.2% in the TMP-SMX group; difference, −1.2 percentage points; 95% CI, −7.6 to 5.1; P = 0.77). Cure rates did not differ significantly between the two treatments in the subgroups of children, adults, and patients with abscess versus cellulitis. The proportion of patients with adverse events was similar in the two groups.
CONCLUSIONSWe found no significant difference between clindamycin and TMP-SMX, with respect to either efficacy or side-effect profile, for the treatment of uncomplicated skin infec-tions, including both cellulitis and abscesses. (Funded by the National Institute of Allergy and Infectious Diseases and the National Center for Advancing Translational Sciences, National Institutes of Health; ClinicalTrials.gov number, NCT00730028.)
a bs tr ac t
Clindamycin versus Trimethoprim–Sulfamethoxazole for Uncomplicated Skin Infections
Loren G. Miller, M.D., M.P.H., Robert S. Daum, M.D., C.M., C. Buddy Creech, M.D., M.P.H., David Young, M.D., Michele D. Downing, R.N., M.S.N., Samantha J. Eells, M.P.H., Stephanie Pettibone, B.S., Rebecca J. Hoagland, M.S., and Henry F. Chambers, M.D., for the DMID 07-0051 Team*
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on May 14, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
n engl j med 372;12 nejm.org March 19, 2015 1093
established in 1812 March 19, 2015 vol. 372 no. 12
From the Los Angeles Biomedical Research Institute (L.G.M., S.J.E.) and Division of Infectious Diseases, Harbor–UCLA (Uni-versity of California, Los Angeles) Medi-cal Center (L.G.M., S.J.E.), Torrance, Da-vid Geffen School of Medicine at UCLA, Los Angeles (L.G.M., S.J.E.), Division of Plastic and Reconstructive Surgery, Uni-versity of California, San Francisco (UCSF) (D.Y.), and Division of Infectious Diseas-es, San Francisco General Hospital and UCSF (M.D.D., H.F.C.), San Francisco — all in California; Division of Pediatric In-fectious Diseases, University of Chicago, Chicago (R.S.D.); Division of Pediatric Infectious Diseases, Vanderbilt Universi-ty, Nashville (C.B.C.); the EMMES Corpo-ration, Rockville, MD (S.P.); and Cota En-terprises, Meriden, KS (R.J.H.). Address reprint requests to Dr. Miller at the Divi-sion of Infectious Diseases, Harbor–UCLA Medical Center, 1000 W. Carson St., Box 466, Torrance, CA 90509, or at lgmiller@ ucla . edu.
*A list of additional members of the Divi-sion of Microbiology and Infectious Dis-eases (DMID) 07-0051 Team is provided in the Supplementary Appendix, available at NEJM.org.
N Engl J Med 2015;372:1093-103.DOI: 10.1056/NEJMoa1403789Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDSkin and skin-structure infections are common in ambulatory settings. However, the efficacy of various antibiotic regimens in the era of community-acquired methicillin-resistant Staphylococcus aureus (MRSA) is unclear.
METHODSWe enrolled outpatients with uncomplicated skin infections who had cellulitis, ab-scesses larger than 5 cm in diameter (smaller for younger children), or both. Patients were enrolled at four study sites. All abscesses underwent incision and drainage. Patients were randomly assigned in a 1:1 ratio to receive either clindamycin or trimethoprim–sulfamethoxazole (TMP-SMX) for 10 days. Patients and investigators were unaware of the treatment assignments and microbiologic test results. The pri-mary outcome was clinical cure 7 to 10 days after the end of treatment.
RESULTSA total of 524 patients were enrolled (264 in the clindamycin group and 260 in the TMP-SMX group), including 155 children (29.6%). One hundred sixty patients (30.5%) had an abscess, 280 (53.4%) had cellulitis, and 82 (15.6%) had mixed infection, de-fined as at least one abscess lesion and one cellulitis lesion. S. aureus was isolated from the lesions of 217 patients (41.4%); the isolates in 167 (77.0%) of these patients were MRSA. The proportion of patients cured was similar in the two treatment groups in the intention-to-treat population (80.3% in the clindamycin group and 77.7% in the TMP-SMX group; difference, −2.6 percentage points; 95% confidence interval [CI], −10.2 to 4.9; P = 0.52) and in the populations of patients who could be evaluated (466 patients; 89.5% in the clindamycin group and 88.2% in the TMP-SMX group; difference, −1.2 percentage points; 95% CI, −7.6 to 5.1; P = 0.77). Cure rates did not differ significantly between the two treatments in the subgroups of children, adults, and patients with abscess versus cellulitis. The proportion of patients with adverse events was similar in the two groups.
CONCLUSIONSWe found no significant difference between clindamycin and TMP-SMX, with respect to either efficacy or side-effect profile, for the treatment of uncomplicated skin infec-tions, including both cellulitis and abscesses. (Funded by the National Institute of Allergy and Infectious Diseases and the National Center for Advancing Translational Sciences, National Institutes of Health; ClinicalTrials.gov number, NCT00730028.)
a bs tr ac t
Clindamycin versus Trimethoprim–Sulfamethoxazole for Uncomplicated Skin Infections
Loren G. Miller, M.D., M.P.H., Robert S. Daum, M.D., C.M., C. Buddy Creech, M.D., M.P.H., David Young, M.D., Michele D. Downing, R.N., M.S.N., Samantha J. Eells, M.P.H., Stephanie Pettibone, B.S., Rebecca J. Hoagland, M.S., and Henry F. Chambers, M.D., for the DMID 07-0051 Team*
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on May 14, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
n engl j med 372;12 nejm.org March 19, 2015 1093
established in 1812 March 19, 2015 vol. 372 no. 12
From the Los Angeles Biomedical Research Institute (L.G.M., S.J.E.) and Division of Infectious Diseases, Harbor–UCLA (Uni-versity of California, Los Angeles) Medi-cal Center (L.G.M., S.J.E.), Torrance, Da-vid Geffen School of Medicine at UCLA, Los Angeles (L.G.M., S.J.E.), Division of Plastic and Reconstructive Surgery, Uni-versity of California, San Francisco (UCSF) (D.Y.), and Division of Infectious Diseas-es, San Francisco General Hospital and UCSF (M.D.D., H.F.C.), San Francisco — all in California; Division of Pediatric In-fectious Diseases, University of Chicago, Chicago (R.S.D.); Division of Pediatric Infectious Diseases, Vanderbilt Universi-ty, Nashville (C.B.C.); the EMMES Corpo-ration, Rockville, MD (S.P.); and Cota En-terprises, Meriden, KS (R.J.H.). Address reprint requests to Dr. Miller at the Divi-sion of Infectious Diseases, Harbor–UCLA Medical Center, 1000 W. Carson St., Box 466, Torrance, CA 90509, or at lgmiller@ ucla . edu.
*A list of additional members of the Divi-sion of Microbiology and Infectious Dis-eases (DMID) 07-0051 Team is provided in the Supplementary Appendix, available at NEJM.org.
N Engl J Med 2015;372:1093-103.DOI: 10.1056/NEJMoa1403789Copyright © 2015 Massachusetts Medical Society.
BACKGROUNDSkin and skin-structure infections are common in ambulatory settings. However, the efficacy of various antibiotic regimens in the era of community-acquired methicillin-resistant Staphylococcus aureus (MRSA) is unclear.
METHODSWe enrolled outpatients with uncomplicated skin infections who had cellulitis, ab-scesses larger than 5 cm in diameter (smaller for younger children), or both. Patients were enrolled at four study sites. All abscesses underwent incision and drainage. Patients were randomly assigned in a 1:1 ratio to receive either clindamycin or trimethoprim–sulfamethoxazole (TMP-SMX) for 10 days. Patients and investigators were unaware of the treatment assignments and microbiologic test results. The pri-mary outcome was clinical cure 7 to 10 days after the end of treatment.
RESULTSA total of 524 patients were enrolled (264 in the clindamycin group and 260 in the TMP-SMX group), including 155 children (29.6%). One hundred sixty patients (30.5%) had an abscess, 280 (53.4%) had cellulitis, and 82 (15.6%) had mixed infection, de-fined as at least one abscess lesion and one cellulitis lesion. S. aureus was isolated from the lesions of 217 patients (41.4%); the isolates in 167 (77.0%) of these patients were MRSA. The proportion of patients cured was similar in the two treatment groups in the intention-to-treat population (80.3% in the clindamycin group and 77.7% in the TMP-SMX group; difference, −2.6 percentage points; 95% confidence interval [CI], −10.2 to 4.9; P = 0.52) and in the populations of patients who could be evaluated (466 patients; 89.5% in the clindamycin group and 88.2% in the TMP-SMX group; difference, −1.2 percentage points; 95% CI, −7.6 to 5.1; P = 0.77). Cure rates did not differ significantly between the two treatments in the subgroups of children, adults, and patients with abscess versus cellulitis. The proportion of patients with adverse events was similar in the two groups.
CONCLUSIONSWe found no significant difference between clindamycin and TMP-SMX, with respect to either efficacy or side-effect profile, for the treatment of uncomplicated skin infec-tions, including both cellulitis and abscesses. (Funded by the National Institute of Allergy and Infectious Diseases and the National Center for Advancing Translational Sciences, National Institutes of Health; ClinicalTrials.gov number, NCT00730028.)
a bs tr ac t
Clindamycin versus Trimethoprim–Sulfamethoxazole for Uncomplicated Skin Infections
Loren G. Miller, M.D., M.P.H., Robert S. Daum, M.D., C.M., C. Buddy Creech, M.D., M.P.H., David Young, M.D., Michele D. Downing, R.N., M.S.N., Samantha J. Eells, M.P.H., Stephanie Pettibone, B.S., Rebecca J. Hoagland, M.S., and Henry F. Chambers, M.D., for the DMID 07-0051 Team*
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on May 14, 2015. For personal use only. No other uses without permission.
Copyright © 2015 Massachusetts Medical Society. All rights reserved.

IPTB ABORDAJE DE ABSCESOS SIMPLES













![Picaduras y mordeduras [autoguardado]](https://static.fdocuments.ec/doc/165x107/5585018fd8b42a8f078b4f39/picaduras-y-mordeduras-autoguardado.jpg)